Upper Extremity MMI and Impairment Rating
|
|
|
- Lambert Craig
- 10 years ago
- Views:
Transcription
1 Upper Extremity MMI and Impairment Rating 1

2 How to Determine Maximum Medical Improvement 1. Understand the definition of MMI 2. Review the DWC Form-032, Request for Designated Doctor Examination 3. Review the medical records 4. Perform the Designated Doctor exam 2

3 How to Determine Maximum Medical Improvement 4. Based on the records reviewed and the exam findings, consider the Official Disability Guidelines (ODG) to see if injured employee (IE) needs additional treatment to reach MMI 5. If at MMI, what is the date? 6. Answer the question from the DWC Form-32: yes or no and why 3

4 MMI and DWC Adopted Guidelines ODG = Treatment MDGuidelines = Return to Work Consider whether additional treatment (per ODG, including Appendix D) may reasonably be anticipated to result in further material recovery or lasting improvement Disability Duration does not equate to MMI - Don t use MDGuidelines for MMI 4

5 Maximum Medical Improvement The earlier of: Clinical MMI - The earliest date, after which based on reasonable medical probability, further material recovery from or lasting improvement to an injury can no longer reasonably be anticipated; or Statutory MMI (listed on DWC Form-032) weeks from date on which income benefits begin to accrue. May be extended by TDI-DWC due to spinal surgery (28 TAC and Texas Labor Code ). 5

6 Maximum Medical Improvement Use TDI-DWC definition of MMI; NOT AMA Guides definition (change of impairment of more than 3% in the next year). Texas Labor Code and rules of the TDI-DWC prevail over the Guides. 6

7 Maximum Medical Improvement Review the records prior to taking history and performing medical exam Provide a justifiable rationale with medical evidence for the MMI date based on the records reviewed and the exam findings, use Official Disability Guideline to see if injured employee (IE) has reached MMI The date of MMI certified as the date of the exam, without reasonable justification, is a common error 7

8 MMI/IR Upper Extremity Case 1 History of Injury 28 y.o. male was working as a tractor driver 3 months ago and was loading a pallet when another tractor smashed him against a wall. He sustained crush injuries to his right wrist and right upper arm. He had severe pain and loss of function in the wrist and shoulder. 8

9 9
10 10

11 MMI/IR - Upper Extremity Case 1 Treatment History He was seen at the Medical Center Hospital ER He was found to have open wounds and fractures of the right wrist and humerus He was taken to the OR by the orthopedic department He underwent debridement of the wounds and open reduction of the fractures He was discharged from the hospital 3 days later after IV meds When he was discharged from the Trauma Center he was told to follow up with an orthopedic surgeon for his shoulder (The University does not take workers comp!). 11

12 MMI/IR - Upper Extremity Case 1 Treatment History He was unable to find an orthopedic doctor The company sent him the next day to an occupational medicine clinic for evaluation He was placed on work restrictions and followed There is no light duty Come back when you are 100% The occupational medicine clinic follows him while he is in a cast Six weeks later he sees an orthopedic surgeon 12

13 MMI/IR - Upper Extremity Case 1 Treatment History The ortho removes the cast and performs x-rays showing healed fractures The ortho refers him for PT He maintains him on restricted work No use of right arm There is no light duty, so he is told to stay home After 3 weeks of PT (9 sessions), the insurance company denies additional PT and submits a DWC 32 requesting a DD exam for MMI & IR The insurance adjustor says he has healed and is at MMI The insurance adjustor says restricted work is available, but he has not worked. 13

14 MMI/IR - Upper Extremity Case 1 Designated Doctor examination - 4 months post injury Medical history: He states he cannot use his right arm well at all, especially above shoulder level It is really weak His right shoulder and wrist are stiff He has no complaints of pain The PT helped, but he has not had any PT in about 3 weeks - he is doing it a home He says he wants to work, but my boss won t let me. 14

15 MMI/IR - Upper Extremity Case 1 Designated Doctor Physical examination: X-rays (UE) - fractures healed hardware in good position Shoulder flexion 80, extension 20, Adduction 20, abduction 80, IR 10, ER 40. Wrist flexion 20, extension 20, radial deviation 10, ulnar deviation 10. Major weakness in shoulder abduction and flexion Some muscle atrophy forearm and upper arm 15

16 Maximum Medical Improvement Upper Extremity Case 1 Log on to ODG. 16

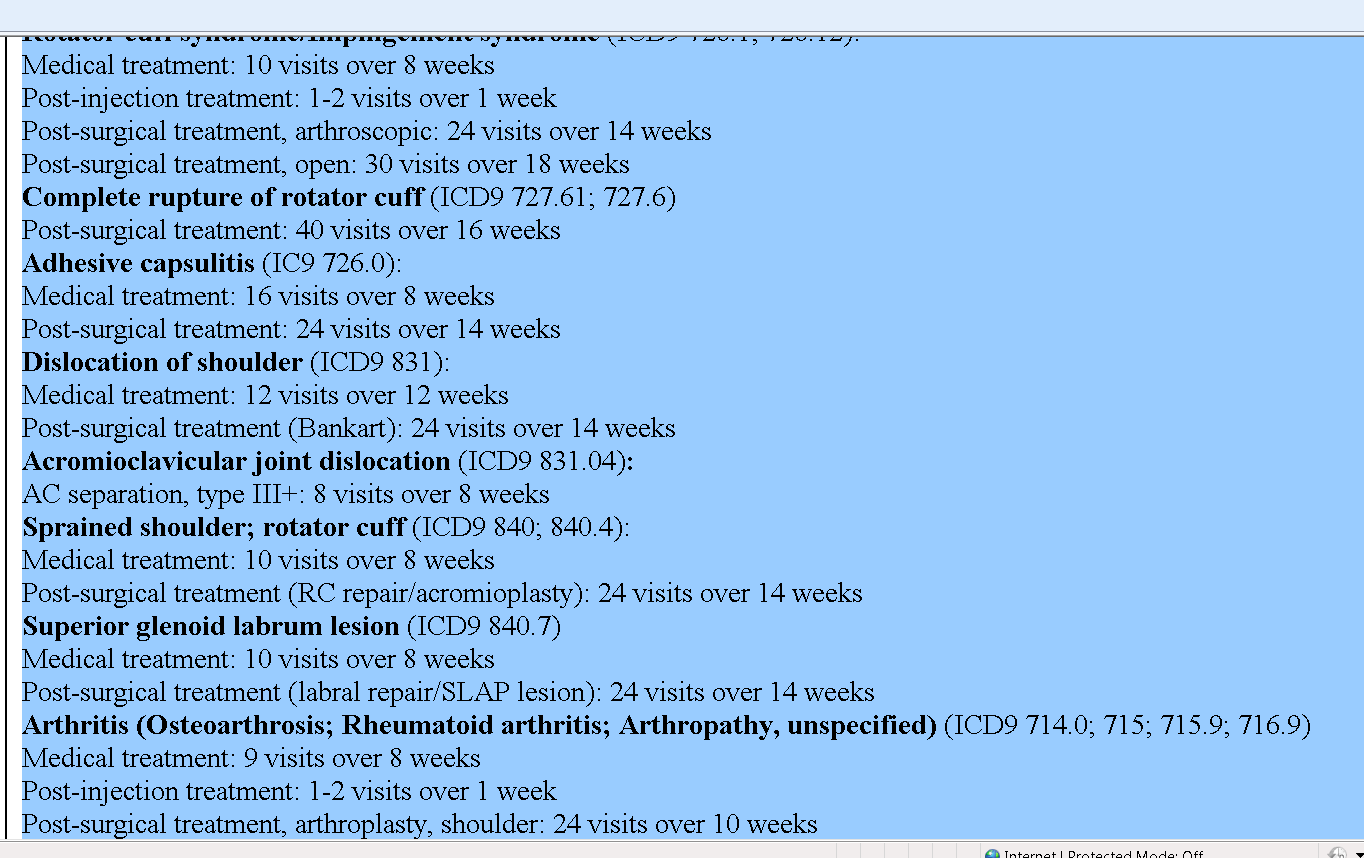
17 Diagnosis? MMI? Sprained shoulder; rotator cuff (ICD9 840; 840.4) Adhesive Capsulitis 726.0: Fracture of radius/ulna (forearm) (ICD9 813): Fracture of humerus (ICD9 812) 17
 (ICD9")
18 MMI? PT ODG recommendation for Dx? Sprained shoulder; rotator cuff (ICD9 840; 840.4): Medical treatment: 10 visits over 8 weeks Post-surgical treatment (RC repair/acromioplasty): 24 visits over 14 weeks Adhesive Capsulitis (ICD9 840; 840.4): Medical treatment: 16 visits over 8 weeks Post-surgical treatment: 24 visits over 14 weeks 18
: Medical treatment: 16 visits over 8 weeks Post-surgical treatment: 24 visits")
19 MMI? PT ODG recommendation for Dx? Fracture of radius/ulna (forearm) (ICD9 813): Medical treatment: 16 visits over 8 weeks Post-surgical treatment: 16 visits over 8 weeks Fracture of humerus (ICD9 812): Medical treatment: 18 visits over 12 weeks Post-surgical treatment: 24 visits over 14 weeks 19
: Medical treatment: 18 visits over 12 weeks")
20 20

21 21
22 22
23 23
24 24
25 25
26 26

27 27
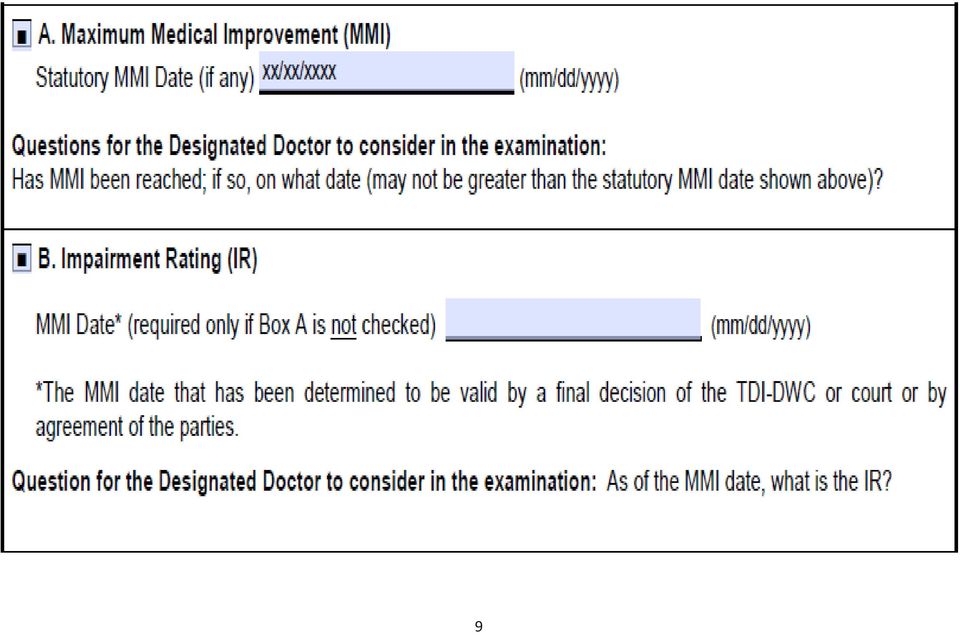
28 MMI - UE Case 1 Question for designated doctor: Has MMI been reached; if so, on what date? If not at MMI, why not and what is needed to reach MMI? Is this consistent with ODG (including Appendix D)? If at MMI, why and what is the date? Explain and give rationale for your MMI date Complete DWC Form-069 and narrative report 28
29 Questions about MMI? 29
30 Impairment Rating 30
31 How to determine Impairment Rating Must rate impairment as of date of MMI. Review the DWC Form-032 Must rate all compensable injuries per DWC or Carrier (See Box 37 of DWC Form-032). Review records to ensure consistency Based on the DD s examination use AMA Guides, 4 th Edition to rate impairment Must be whole person impairment rating 31
32 How to Determine Impairment Rating Show your work! so that any knowledgeable person can compare the clinical findings with the guides criteria and Determine whether or not the impairment estimates reflect those criteria. Guides (p. 8) Document the findings and explain the impairment rating in your narrative report, plus relevant worksheets Complete and sign the DWC Form
33 How to Determine Impairment Rating Hand and Upper Extremity No rating for hand/upper extremity dominance No specific requirement (or prohibition) to measure the uninvolved contralateral upper extremity in the 4 th Ed. of Guides (as per 3 rd, 5 th and 6 th Editions) 33
34 How to Determine Impairment Rating Hand and Upper Extremity Measurements must be consistent Between examiners (pp. 7, 8, 9) By the same examiner with repeated measurements may be expected to lie within 10% of each other (p. 9) Plausible and relate to the impairment being evaluated (p. 8) 34
35 How to Determine Impairment Rating Hand and Upper Extremity Active, not passive range of motion (ROM) should be measured/rated; page 15 Round UE ROM to nearest 10 degrees per written instructions AMA Guides 4 th ed., pp ; also page 15 (NOT 5 degree increments per Figure 29, p. 38 wrist RD/UD) Appeals Panel decision s, decided November 12,
36 How to Determine Impairment Rating Hand and Upper Extremity UE ROM Guides, 4 th do not directly address rounding 5 degrees; however generally recommended that <5 degrees round down, >5 degrees round up Do not round the WHOLE PERSON impairment rating in DWC system as instructed in AMA Guides (p. 9) Use Figure 1 pp
37 37
38 38
39 39
40 40
41 41
42 42
43 Hand and Upper Extremity Impairment Sections Are Different Than The Other Chapters 43
44 Whole Person Concept Upper Extremity Thumb Index Middle Ring Hand Wrist Elbow Upper Extremity x 60% Little Shoulder Whole Person 44
45 These Impairment Values Have to be Converted to Whole Person by Using: Table 1 (p. 18) Table 2 (p. 19) Table 3 (p. 20) 45
46 46
47 47
48 48
49 Hand and Upper Extremity Methods for Evaluating Impairment Amputation Sensory loss of digits ROM Peripheral nerve disorders Cervical Spinal Nerve Roots Brachial Plexus Major Peripheral Nerves Vascular Disorders Other Disorders 49
50 Amputation Loss of entire UE = 60% WP Rate amputation per Figure 7 (thumb), Figure 17 (finger), Figure 3 ( Impairments of the digits and hand), or Figure 2 (Impairments of the UE) Use Figure 1 For digits Convert digit to hand using Table 1, p. 18 Covert hand to UE, using Table 2, p. 19 Convert UE to WP if there are no other UE ratings, using Table 3, p
51 51
52 52
53 Figure 3. p
54 54

55 MMI/IR Upper Extremity Case 2 History of Injury 26 y.o. female punch press operator 4 months ago accidentally amputated the tip of the left index finger with punch press machine. 55
56 MMI/IR - Upper Extremity Case 2 Review Lower Extremity Case 1 with DWC Form
57 57
58 58
59 MMI/IR Upper Extremity Case 2 Treatment History She was seen in the ER, evaluated and was referred to a hand surgeon. A day later, she was taken to the OR for debridement. The operative report noted traumatic amputation of left index finger tip with complete loss of fingernail, and the tip of the distal phalanx. Case 2 59
60 MMI/IR Upper Extremity Case 2 Treatment History She was followed by him with adequate healing. There were 24 post op PT visits. She has returned to work with restrictions per her surgeon. He also recommended additional PT. 60
61 MMI/IR Upper Extremity Case 2 Designated Doctor exam 8 months post-injury Occasional swelling / aching left index Meds: Metformin /vicodin Well healed scar, no redness / swelling Absence tip / fingernail. 61
62 MMI/IR Upper Extremity Case 2 Designated Doctor exam 8 months post-injury Transverse sensory loss tip of index finger rest of hand intact DIP ROM = unable to accurately measure due to amputation PIP ROM = 0 extension / 100 flexion MCP ROM = 0 extension / 90 flexion Normal strength, sensation, neurovasc intact 62
63 MMI/IR Upper Extremity Case 2 Question for designated doctor: Has MMI been reached; if so, on what date? Question for designated doctor: As of the certified MMI date, what is the impairment rating? Show Your Work! 63
64 Finger Impairment Amputation Compare length with Fig. 17 (p. 3/30) Convert using: Table 1 (p. 3/18) Table 2 (p. 3/19) Table 3 (p. 3/20) 64
65 Whole Person Concept Upper Extremity Thumb Index Middle Ring Hand Wrist Elbow Upper Extremity x 60% Little Shoulder Whole Person 65
66 Convert using: Table 1 (p. 3/18) - Digit to Hand 30% Index Impairment = 6% Hand 66
67 Using Table 2: Convert: 6% Hand =5% Upper Extremity 67
68 Convert: 5% Upper Extremity Using Table 3 = 3% Whole Person 68
69 Nerve Injury? Digital Nerve injuries use the Tables and Figures in the Hand Section of Chapter 3 Used for laceration injuries / tendon injuries where distal sensation compromised Not applicable in amputation amputation is MAX rating 69
70 Pg. 30: ROM of the DIP? (if it could be measured) If an amputation affects the measurements of abnormal motion, then only the amputation impairment is acknowledged Not applicable in amputation amputation is MAX rating 70
71 71
72 72

73 Questions about amputation? 73
74 Hand and Upper Extremity Methods for Evaluating Impairment Amputation Sensory loss of digits ROM Peripheral nerve disorders Cervical Spinal Nerve Roots Brachial Plexus Major Peripheral Nerves Vascular Disorders Other Disorders 74
75 Sensory loss of digits Must be unequivocal and permanent, page 20 Dorsal surface not considered impairing 75
76 Sensory loss of digits Impairments are estimated according to the sensory quality and its distribution on the PALMAR aspect of the digits. Sensory loss on the DORSAL surface of the digits is NOT considered to be an impairment. Page 20 76
77 Sensory loss of digits Determine Quality of Loss- page 21 Determine by two-point exam If greater than 15 mm = total sensory loss, 100% sensory impairment 15 mm 7 mm = partial sensory loss, 50% sensory impairment <6mm is normal, 0% sensory impairment 77
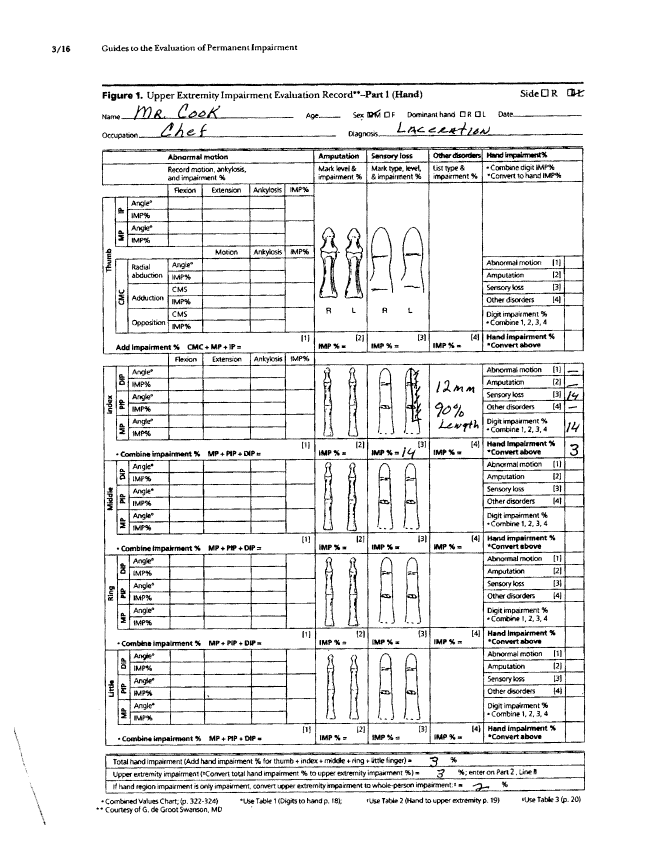
78 78
79 Sensory loss of digits Different Types: 1) Transverse Loss a. Loss of function in both digital nerves b. 100% sensory loss and receive 50% value of amputation at that level c. Thumb - Figure 7, p. 24 d. Fingers - Figure 17, p
80 80
81 81
82 Sensory loss of digits Different Types: 2) Longitudinal Loss a. One Digital Nerve b. Impairment value varies as to side injured (radial vs. ulnar side of digit) c. Be sure to read sections on proper use of Tables d. Thumb/little - Table 4, p.25; and Table 8, p. 31 e. Index, middle, ring Table 9, p
83 Table 4, p.25 83
84 Table 8, p
85 Table 9, p
86 Sensory loss of digits Total Transverse and Longitudinal Sensory Loss Rated using Figure 5, p
87 87
88 Upper Extremity Case 3 MMI/IR History of Injury 28 year old chef sustained a laceration to the radial aspect of his left index finger while slicing some meat. He was seen at a local emergency department where the wound was irrigated and debrided The wound healed without complication and he returned to work. 88
89 89
90 90
91 Upper Extremity Case 3 MMI/IR The IE reached statutory MMI and a designated doctor examination was requested Designated Doctor Physical Exam Well healed scar between the PIP and MP of the left index finger, with 12 mm 2 point discrimination on the radial side of the left index finger 91
92 Upper Extremity Case 3 MMI/IR Designated Doctor Physical Exam Full ROM of the index finger 5/5 strength of the fingers and wrist 92
93 93
94 MMI/IR Upper Extremity Case 3 Question for designated doctor: Has MMI been reached; if so, on what date? Question for designated doctor: As of the certified MMI date, what is the impairment rating? Show Your Work! 94
95 Table 9, p. 31 Left index finger radial digital nerve longitudinal loss 90% digit length 12 mm = partial loss 14% digit impairment 95
96 Convert using: Table 1 (p. 3/18) - Digit to Hand 14% Index Impairment = 3% Hand 96
97 Using Table 2: Convert: 3% Hand =3% Upper Extremity 97
98 Convert: 3% Upper Extremity Using Table 3 = 2% Whole Person 98
99 Case 3 99
100 100
101 Case 3 101
102 Questions about sensory of the digits? 102
103 Hand and Upper Extremity Methods for Evaluating Impairment Amputation Sensory loss of digits ROM Peripheral nerve disorders Cervical Spinal Nerve Roots Brachial Plexus Major Peripheral Nerves Vascular Disorders Other Disorders 103
104 Hand and Upper Extremity Range of Motion Most values are recorded in degrees of motion as measured with a goniometer, with a corresponding pie chart Thumb adduction, opposition and radial abduction are the exceptions (Figs 9,12,14,16 pp 26-29) 104
105 Hand and Upper Extremity Range of Motion Round UE ROM to nearest 10 degrees per written instructions AMA Guides 4 th ed., pp Appeals Panel decision s, decided November 12, 2002 affirmed rounding to nearest 10 degrees 105
106 106
107 Hand and Upper Extremity Range of Motion 1. Measure active motion of the joints 2. Use tables, figures and pie charts for each joint to determine impairment of upper extremity 3. Use of opposite, uninvolved joint as a baseline is optional 107
108 Hand and Upper Extremity Range of Motion 4. Add impairments in same joint 5. Combine impairments in different joints 6. Combine different types of impairments 108
109 Each ROM has its own picture of how to perform measurement 109
110 Reading Hand and Upper Extremity ROM tables Pie charts I A % = impairment value for ankylosis I E % = impairment value for extension I F % = impairment value for flexion V = value measured (degrees) 110
111 Reading Hand and Upper Extremity ROM tables Example: Index finger PIP has extension lag of -20 degrees and 60 of flexion Figure 21. page 33 I E %=7%+ I F %=24 7%+24% = 31% index finger impairment Fig 1 (page 16) states "Combine impairment % MP+PIP+DIP= ". ROM impairment value for more than one finger joint should be combined. See description on p. 34, 2nd column at the top of the page above Fig
112 Reading Hand and UE ROM tables 112
113 Abnormal Motion Thumb FIVE AREAS OF MOTION 1. IP JOINT 2. MP JOINT 3. ADDUCTION 4. ABDUCTION 5. OPPOSITION 113
114 114
115 115
116 116
117 117
118 Abnormal Motion Thumb Five Areas of Motion Add Impairment Losses Thumb Convert Using Tables 1, 2, & 3 Use Figure 1 118
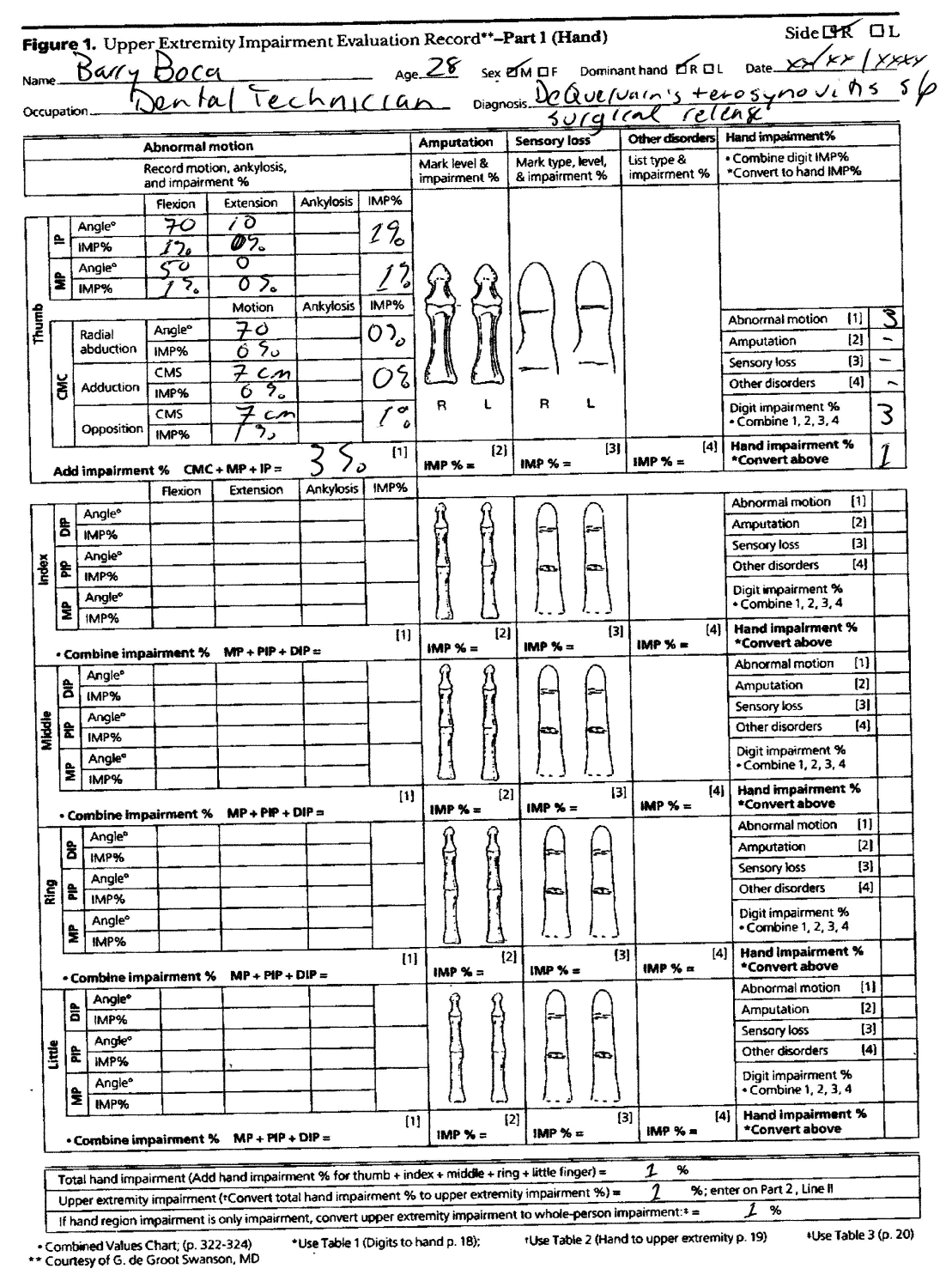
119 119
120 Finger Range of Motion Each joint has its own pie chart to determine impairment value Motion falling between values in pie charts may be rounded or interpolated 120
121 Finger Range of Motion Add impairments in same joint Combine impairments in different joints 121
122 Finger Range of Motion Obtain total digit impairment Convert to whole person using Tables 1, 2, & 3 Use Figure 1 122
123 What do you do with multiple types of impairments (range of motion, sensory, etc.)? Determine impairment from each type of impairment (sensory, range of motion, etc.) Combine the different types to arrive at a total impairment for that digit. Convert using Tables 1, 2, & 3 Use Figure 1 123
124 What if more than one digit has an impairment? 1. Determine the impairment of each individual digit. 2. Convert each digit impairment to a hand impairment using Table 1 124
125 What if more than one digit has an impairment? 3. Add the hand impairments for each digit for a total hand impairment 4. Convert hand to UE using Table 2 5. Convert UE to whole person using Table 3 (NOTE: if more than one UE impairment is involved combine before converting) 6. No deduction for nonpreferred extremity 125
126 126
127 127
128 128
129 Upper Extremity Case 4 MMI/IR History of Injury 35 y.o. male one year ago developed pain over the dorsal hand overlying the first metacarpal. He was diagnosed with DeQuervain s tenosynovitis of the right thumb secondary to repetitive injury. Occupation is dental technician. 129
130 130
131 131
132 Upper Extremity Case 4 MMI/IR Treatment History He has had 12 PT sessions and 2 steroid injections followed by abductor pollicis longus tendon sheath released 6 months ago. This was followed by 16 PT sessions post surgery. He was released by his surgeon to return to work 3 months ago without restrictions. He is now being followed by a family physician who is recommending additional PT and work conditioning. 132
133 Upper Extremity Case 4 MMI/IR The insurance carrier adjustor requested a Designated Doctor examination for MMI and IR. The accepted/compensable injuries/conditions are: DeQuervain s Tenosynovitis of the right thumb. 133
134 Upper Extremity Case 4 MMI/IR Designated Doctor Medical History He presents to the office with complaints of occasional thumb discomfort but indicates some relief with OTC NSAIDS as needed for pain. He is working without restrictions. He has no other complaints but reported his family physician is suggesting additional PT and WC. 134
135 Upper Extremity Case 4 MMI/IR Designated Doctor Physical Examination Your examination shows a well healed scar consistent with his surgery. There is mild tenderness over the scar. Sensory is normal. Neurovascular is intact. 135
136 Upper Extremity Case 4 MMI/IR Designated Doctor Physical Examination Right thumb exam Normal strength IP flexion 70 degrees, extension 10 degrees MP flexion 50 degrees, MP extension 0 degrees Abduction 70 degrees Adduction is carried to between ring and little finger MIP joints, 7cm. Able to oppose to 7cm from the palm 136
137 MMI/IR Upper Extremity Case 4 Question for designated doctor: Has MMI been reached; if so, on what date? Question for designated doctor: As of the certified MMI date, what is the impairment rating? Show Your Work! 137
138 Figure 10, p. 26 IP flexion 70 0 = 1% IP extension 10 0 = 0% Add 1% +0% = 0% thumb impairment 138
139 Figure 13, p. 27 MP flexion 50 0 = 1% MP extension 0 0 = 0% Add 0% +1% = 1% thumb impairment 139
140 Table 6, p. 28 Abduction 70 0 = 0% thumb impairment 140
141 Figure 14, p. 28 Measure adduction to MP joint 141
142 Table 5, p. 28 Adduction to between ring and little finger MP joints, 7 cm Lacks 1 cm = 0% thumb impairment 142
143 Table 7, p. 29 Able to oppose to 7cm from the palm= 1% thumb impairment 143
144 Thumb ROM Impairment IP flexion 70 0 of 1%+ IP extension 10 0 of 0% = 1% MP flexion 50 0 of 1%+ IP extension 0 0 of 0% = 1% Abduction 70 0 = 0% Adduction to 7 cm (lacks 1 cm) = 0% thumb Opposition to 7cm from the palm= 1% 1%+1%+1%= 3% thumb impairment 144
145 Convert using: Table 1 (p. 3/18) - Digit to Hand 3% Thumb Impairment = 1% Hand 145
146 Using Table 2: Convert: 1% Hand =1% Upper Extremity 146
147 Convert: 1% Upper Extremity Using Table 3 = 1% Whole Person 147
148 148
149 149

150 150
151 Any Questions about Thumb ROM? 151
152 Wrist Range of Motion 4 RANGES OF MOTION Measure: a) Flexion (Fig. 24, p. 36) b) Extension (Fig. 24, p. 36) c) Radial Deviation (Fig.27, p. 27) d) Ulnar Deviation (Fig.27, p. 27) 152
153 153
154 154
155 Wrist Range of Motion Determine impairment values based on pie charts Fig. 26 (p. 36) & Fig 29 (p. 38) Round ROM to nearest 10 degrees per written instructions for UD and RD, rather than 5 degree increments in Fig. 29 Appeals Panel decision s Use Figure 1 combine with other UE impairments and convert to whole person using table 3 155
156 156
157 157
158 158
159 159
160 Elbow Range of Motion Measure based on Fig. 30 (p. 29), Fig. 33 (p. 40) Measure: 1) Flexion 2) Extension 3) Pronation 4) Supination 160
161 Elbow Range of Motion Determine impairment values based on pie charts Fig. 32 (p. 40) & Fig 35 (p. 41) Use Figure 1 combine with other UE impairments and convert to whole person using Table 3 161
162 Shoulder Range of Motion 6 Measurements of Range of Motion 1) Flexion (Fig. 36, p. 42) 2) Extension (Fig. 36, p. 42) 3) Adduction (Fig. 39, p. 45) 4) Abduction (Fig. 39, p. 45) 5) Internal Rotation (Fig. 42, p. 44) 6) External Rotation (Fig. 42, p. 44) 162
163 Shoulder Range of Motion Determine Impairment Values Based on Pie Charts: 1) Flexion (Fig. 38, p. 43) 2) Extension (Fig. 38, p. 43) 3) Adduction (Fig. 41, p. 44) 4) Abduction (Fig. 41, p. 44) 5) Internal Rotation (Fig. 44, p. 45) 6) External Rotation (Fig. 44, p. 45) Use Figure 1 combine with other UE impairments and convert to Whole Person using Table 3 163
164 Upper Extremity Case 1 MMI/IR (The Sequel) Crush injury Right wrist & upper arm Open fractures humerus & radius 2 nd DD appointment (+20wks later) 164
165 165
166 166
167 Upper Extremity Case 1 MMI/IR (The Sequel) Designated Doctor Medical History Extra 4 months of PT helped a lot, UE stronger and more mobile Back at work full duty (can t reach overhead the same) 167
168 Upper Extremity Case 1 MMI/IR (The Sequel) Designated Doctor Physical Examination Shoulder ROM Flexion 130 Extension 40 Abduction 120 Adduction 50 IR 20 ER
169 Upper Extremity Case 1 MMI/IR (The Sequel) Designated Doctor Physical Examination Wrist ROM Flexion 30 Extension 40 Radial deviation 10 Ulnar deviation
170 Upper Extremity Case 1 MMI/IR (The Sequel) Designated Doctor Physical Examination Good strength abduction and flexion No atrophy forearm and upper arm No tenderness 170
171 Upper Extremity Case 1 MMI/IR (The Sequel) Question for designated doctor: Has MMI been reached; if so, on what date? Question for designated doctor: As of the certified MMI date, what is the impairment rating? Show Your Work! 171
172 IR ROM loss Shoulder & wrist 172
173 Fig. 38 (pg. 3/43) Fig. 41 (pg. 3/44) Fig. 44 (pg. 3/45) 173
174
175 30 Fig. 24 (pg. 3/36) Fig. 27 (pg. 3/37) = 9% = 4% = 13% UE Fig. 26 (pg. 3/36) Fig. 29 (pg. 3/38) 175
176 176
177
178
179 Whole Person Concept Upper Extremity Thumb Index Middle Ring Hand Wrist Elbow Upper Extremity x 60% Little Shoulder Whole Person 179
180 Different Joints Combine: 13% (Wrist) with 11% (Shoulder) = 23% UE impairment 180
181 Relationship of Imp. of Upper Extremity to Imp. of Whole Person Table 3 (p. 20) Convert 23% UE = 14% Whole Person 181
182 (Combined Values chart Pgs 322/3) 14%
183 Any Questions about Shoulder or Wrist ROM? 183
184 Hand and Upper Extremity Methods for Evaluating Impairment Amputation Sensory loss of digits ROM Peripheral nerve disorders Cervical Spinal Nerve Roots Brachial Plexus Major Peripheral Nerves Vascular Disorders Other Disorders 184
185 Peripheral Nerve Disorders Section 3.1k p. 46 for the Upper Extremity has specific Tables. Three Main Areas: 1) Cervical Spinal Nerve Roots 2) Brachial Plexus 3) Major Peripheral Nerves 185
186 Peripheral Nerve Disorders Restricted UE ROM strictly due to peripheral nerve lesion should not be rated with ROM method p. 46 If restricted ROM is not strictly due to peripheral nerve disorder, then ROM can be combined with peripheral nerve disorder impairment Rate pain/sensory deficits and/or motor deficits 186
187 Peripheral Nerve Disorders Pain/Sensory deficits page 46 How does deficit interfere with ADL that is present at MMI? Does it follow a defined, specific anatomic distribution? (nerve root, plexus, peripheral nerve) Is the injury/condition consistent with a peripheral nerve disorder? 187
188 Peripheral Nerve Disorders Motor deficits Is there a loss of strength, or specific muscle loss of function, that is present and reproducible on the clinical exam? Is this consistent with the injury, clinical condition and prior medical records? Is the strength loss in a defined, specific anatomic pathway of the injured nerve? (nerve root, plexus, peripheral nerve) Do not combine with loss of strength section 3.1m (Impairment due to other disorders of the UE)(which is rarely used) 188
189 Peripheral Nerve Disorders Cervical Spinal Nerve Roots Determine that there is a specific single spinal nerve root injury/deficit, that is not ratable per the Spine section Estimate the sensory deficit/pain from Table 11, p. 48 and motor deficit from Table 12, p. 49 Multiply the severity of the sensory or motor deficit by the appropriate percentage from Table 13, p.51 Combine the sensory and motor deficits to give an UE IR value Use Figure 1 combine with other UE impairments and convert to Whole Person using Table 3 189
190 Peripheral Nerve Disorders Brachial Plexus Determine that there is a specific brachial plexus injury/deficit Estimate the sensory deficit/pain from Table 11, p. 48 and motor deficit from Table 12, p. 49 Multiply the severity of the sensory or motor deficit by the appropriate percentage from Table 14, p.52 Combine the sensory and motor deficits to give an UE IR value Use Figure 1 combine with other UE impairments and convert to Whole Person using Table 3 190
191 Peripheral Nerve Disorders Major Peripheral Nerves Determine that there is a specific peripheral injury/deficit Identify the nerve involved and the level of the lesion per Table 10, p. 47 and Figs. 45 & 48 (pp. 50 & 55) Estimate the sensory deficit/pain from Table 11, p. 48 and motor deficit from Table 12, p. 49 Multiply the severity of the sensory or motor deficit by the appropriate percentage from Table 15, p.54 For mixed nerves, combine the sensory and motor deficits to give an UE IR value If more than one nerve is involved combine the UE values for each nerve Use Figure 1 combine with other UE impairments and convert to Whole Person using Table 3 191
192 Entrapment Neuropathy Table 16, p. 57 alternative method for rating entrapment neuropathy; no definitions of mild, moderate or severe Explain your reason for selecting the severity degree category SHOW YOUR WORK 192
193 RSD/CRPS Rate ROM loss (must be maximal and reproducible/consistent ) Rate the sensory deficit/pain from Table 11, p. 48 Rate the motor deficit of the injured peripheral nerve, if it applies, from Table 12, p. 49 Combine sensory deficit/pain and motor deficit Combine ROM with value from sensory deficit/pain and motor deficit 193
194 Carpal Tunnel Syndrome Carpal tunnel syndrome and other major peripheral nerve disorders should be evaluated by sensory and motor nerve loss Don t use ROM Best Practice don t use Table 16 p. 57 no definitions of mild, moderate or severe 194
195 Upper Extremity Case 5 MMI/IR History of the Injury CTS A 48 year old right handed male meatpacking worker presents to the family physician who is also providing workers compensation care for the local company with a 2 month duration of slow progressive onset of numbness and tingling of the right thumb, index finger, and middle fingers 195
196 196
197 197
198 Upper Extremity Case 5 MMI/IR CTS Treatment History The patient has been a meatpacking worker for 30 years. His most recent job is with a whizzard knife cutting shoulder flanks of pork product. This involves a line speed of 780 per hour. He is right handed, using the whizzard knife with the right hand and a hook with the left hand. 198
199 Upper Extremity Case 5 MMI/IR CTS Medical History 10 year history of diabetes mellitus (takes oral medicine, not insulin) Family history of hypothyroidism Obese ( #) Family practitioner exam: Positive Tinel's and Phalen s test on right No thenar muscle wasting Night time wakening with hand/finger numbness 199
200 Upper Extremity Case 5 MMI/IR CTS Medical History Diagnosis of right CTS Family practitioner recommends: Night time wrist splint Ibuprofen Occupational therapy for 3x per week for 2 weeks Alternate duty (no knife or hook work) Off work status for 2 weeks 200
201 Upper Extremity Case 5 MMI/IR Medical History CTS The worker returns after 2 weeks with no improvement Family practitioner treatment: Injection of the carpal tunnel Narcotic pain medicine Continued use of splint Being completely off work for 4 more weeks 201
202 Extremity Case 5 MMI/IR CTS Medical History The worker returns 4 weeks later (6 weeks post injury) with no change Family practice doctor refers to orthopedic surgeon for consultation regarding release surgery Hand surgeon recommends endoscopic carpal tunnel release Injured worker declines surgery 202
203 Extremity Case 5 MMI/IR CTS The insurance carrier adjustor requested a designated doctor examination to determine MMI and IR The accepted/compensable injuries/conditions are: Right carpal tunnel syndrome. The Designated Doctor examination - 12 weeks post injury to determine MMI and IR 203
204 Upper Extremity Case 5 MMI/IR CTS Designated Doctor Medical history: He presents to the DD exam with c/o bilateral numbness and tingling worse at night. He has been able to return to playing frisbee golf. He is not working. His surgeon recommended surgery but he does not want to do this. 204
205 Extremity Case 5 MMI/IR CTS Designated Doctor Physical Examination: He is a pleasant male 5 8 tall and 300 pounds. Examination of both hands indicated no thenar atrophy. He has full ROM of both wrists 205
206 Extremity Case 5 MMI/IR CTS Designated Doctor Physical Examination: Good grip strength bilaterally at position 2 right 110#, left 102# Sensory exam shows decreased sensation to median nerve distribution of the palmar aspects of the radial and ulnar distributions right thumb, index and middle fingers Tinel s and Phalen s tests are positive on the right 206
207 Upper Extremity Case 5 MMI/IR CTS Question for designated doctor: Has MMI been reached; if so, on what date? Question for designated doctor: As of the certified MMI date, what is the impairment rating? Show Your Work! 207
208 Table 11, P. 48 Sensory deficit which interferes with activity use maximum value (p.48) 60% sensory deficit 208
209 Table 15, p. 54 Decreased sensation to median nerve distribution of the palmar aspects of the radial and ulnar distributions right thumb, index and middle fingers = 36% UE 209
210 UE IR = 60% x 36% UE = 22% UE 22% UE converts to 13% WP 210
211 Relationship of Imp. of Upper Extremity to Imp. of Whole Person Table 3 (p. 20) Convert 23% UE = 14% Whole Person 211
212 Any Questions about Peripheral Nerve Injuries? 212
213 Hand and Upper Extremity Methods for Evaluating Impairment Amputation Sensory loss of digits ROM Peripheral nerve disorders Cervical Spinal Nerve Roots Brachial Plexus Major Peripheral Nerves Vascular Disorders Other Disorders 213
214 Vascular Disorders Section 3.1 L Use Table 17, p. 57 Difficult to find exact situation with every patient Combine vascular rating with amputation when amputation is due to peripheral vascular disease, p
215 215
216 216
217 Hand and Upper Extremity Methods for Evaluating Impairment Amputation Sensory loss of digits ROM Peripheral nerve disorders Cervical Spinal Nerve Roots Brachial Plexus Major Peripheral Nerves Vascular Disorders Other Disorders 217
218 UPPER EXTREMITY Other Disorders Section 3.1m (p. 58) Impairments are under two different classes of disorders: I. Bone And Joint Deformities, p. 58 II. Musculotendinous Impairments, p
219 Impairment Due to Other Disorders of The Upper Extremity I. Bone & Joint Deformities A. Joint Crepitation with Motion B. Joint Swelling due to synovial hypertrophy C. Digit Lateral Deviation D. Digit rotational deformity 219
220 Impairment Due to Other Disorders of The Upper Extremity Bone & Joint Deformities continued. E. Persistent joint subluxation or dislocation F. Joint instability G. Wrist and elbow joint radial and ulnar deviation H. Carpal instability I. Arthroplasty 220
221 Table 27, p
222 Impairment Due to Other Disorders of The Upper Extremity II. Musculotendinous Impairments A. Intrinsic Tightness B. Constrictive Tenosynovitis C. Extensor Tendon Subluxation at the MP Joint 222
223 UPPER EXTREMITY Other Disorders Usually range of motion is the best determination of impairment Have to be cautious in using different tables and values The criteria described in this section should be used only when other criteria have not adequately encompassed the extent of the impairments, p. 58. SHOW YOUR WORK! 223
224 UPPER EXTREMITY Other Disorders Some disorders may be combined with range of motion impairments and some may not be combined 224
225 UPPER EXTREMITY Other Disorders Tables are different and have: Joint impairments Digit impairments Upper extremity impairments 225
226 Upper Extremity 3.1 m (p ) - Strength Evaluation Rarely Used Do not double rate with strength loss from nerve injury Use Tables and formulas on p. 64 & 65 to determine loss 226
227 Upper Extremity Use measurements taken over time, three times each hand. Repeat tests at intervals during your exam 20 % Variation assume patient not exerting full effort. 227
228 Upper Extremity 3.1 m (p ) - Strength Evaluation Determine valid effort 5 position grip producing bellshaped curve Rapid exchange grip test 228
229 Extremity Case 6 MMI/IR RCR with distal clavicle resection History of Injury A 57 year old teacher slipped and fell into the wall with her arm to her right side, contacting her dominant right shoulder 16 months ago 229

230 230
231 231
232 Extremity Case 6 MMI/IR RCR with distal clavicle resection Treatment History She initially saw an occupational medicine physician and was found to have significant tenderness over the right AC joint and reduced right shoulder ROM. Right shoulder X-rays revealed a Type III acromion but no fracture or dislocation. Initial treatment included the use of a sling and NSAIDs, followed by 12 visits of physical therapy, with some improvement. She was able to return to work with restrictions. 232
233 Extremity Case 6 MMI/IR RCR with distal clavicle resection Treatment History Her symptoms persisted and a right shoulder MRI scan was obtained 2 months post injury, revealing a partial thickness tear of the supraspinatus tendon, increased signal in the subacromial bursa, type III acromion, and degenerative changes of the AC joint. Orthopedic surgical consultation was obtained, where arthroscopic acromioplasty with distal clavicle resection and rotator cuff repair were performed. 233
234 Extremity Case 6 MMI/IR RCR with distal clavicle resection Treatment History She completed a course of post-operative PT, consisting of 30 visits over 6 months She returned to work full time as a teacher while in PT 234
235 Extremity Case 6 MMI/IR RCR with distal clavicle resection Designated Doctor Medical history: She is working full time as a teacher with restrictions to avoid lifting overhead with right arm Reports she has not been able to successfully complete yoga class Her QuickDASH score is
236 Extremity Case 6 MMI/IR RCR with distal clavicle resection Designated Doctor Physical Examination: Active goniometric right shoulder ROM: flexion 160 degrees extension 40 degrees abduction 120 degrees adduction 30 degrees internal rotation 30 degrees external rotation 30 degrees all with complaints of increased right shoulder pain. Passive shoulder motions are greater than active motion and less painful. 236
237 Extremity Case 6 MMI/IR RCR with distal clavicle resection Designated Doctor Physical examination: Active and resisted left shoulder ROM is full and pain- free. She has 5/5 strength of bilateral upper extremities, with the exception of right shoulder flexion, abduction and external rotation which were 4/5 due to pain. Resisted empty can, Hawkin s and Neer s are positive for increased pain and weakness Upper extremity sensation and DTRs are normal. There is no atrophy and upper extremity pulses are normal. 237
238 Extremity Case 6 MMI/IR RCR with distal clavicle resection Question for designated doctor: Has MMI been reached; if so, on what date? Question for designated doctor: As of the certified MMI date, what is the impairment rating? Show Your Work! 238
239 Extremity Case 6 MMI/IR RCR with distal clavicle resection Shoulder ROM flexion 160 degrees = 1% UE extension 40 degrees = 1% UE abduction 120 degrees = 3% UE adduction 30 degrees = 1% UE internal rotation 30 degrees = 4% UE external rotation 30 degrees = 1% UE Total = 11% UE 239
240 Extremity Case 6 MMI/IR RCR with distal clavicle resection 11% UE for ROM 10% UE for distal clavicle resection (Table 27, p. 61) 11% cw 10% = 20% UE 20% UE converts to 12% WP 240
241 Distal Clavicle Resection Arthroplasty By definition, requires resection of the distal clavicular portion of the AC joint (not the same as acromioplasty) Carefully review and cite relevant portions of the operative report Can combine with ROM see p
242 Any Questions about Other Disorders? 242
243 Hand and Upper Extremity Pearls (see Summary p. 66) Use Fig 1 (and submit with 69 and report) Add thumb ROM values, combine ROM values for other digits Combine digit impairments, then convert to hand Add the hand impairment values for the digits 243
244 Hand and Upper Extremity Pearls (see Summary p. 66) Convert hand to UE, combine with other UE impairments Convert to whole person impairment Combine with whole person impairments from other regions 244
245 Hand and Upper Extremity Pearls Multiple Upper Extremities Determine whole person impairment from each upper extremity Combine whole person impairment from each upper extremity to give total whole person impairment APD s 245
246 Hand and Upper Extremity Pearls Round UE ROM to nearest 10 degrees vs. wrist radial/ulnar deviation Fig 29 p. 38 in 5 0 increments Carpal tunnel syndrome and other nerve disorders should be evaluated by sensory and motor nerve loss (not ROM; entrapment neuropathy Table 16 p. 57 not recommended no definitions of mild, moderate or severe) 246
247 Hand and Upper Extremity Pearls Grip Strength loss for rare cases only, not recommended, must document validity criteria (with measurements) 5 position grip Rapid exchange grip 247
248 Questions? 248
Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA
 Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA 2 offices 805 Sir Thomas Court Harrisburg 3 Walnut Street Lemoyne Mechanism of injury Repetitive overhead activities Falls to the ground Falls with
Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA 2 offices 805 Sir Thomas Court Harrisburg 3 Walnut Street Lemoyne Mechanism of injury Repetitive overhead activities Falls to the ground Falls with
Hand and Upper Extremity Injuries in Outdoor Activities. John A. Schneider, M.D.
 Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma. Magee, 2008. pg.
 PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
Medical Report Checklist: Upper Extremities Peripheral Nerve Disorders Impairments (PND)
") http://www.pdratings.com/ Craig Andrew Lange [email protected] California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
http://www.pdratings.com/ Craig Andrew Lange [email protected] California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
Notice of Independent Review Decision DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE:
 Notice of Independent Review Decision DATE OF REVIEW: 12/10/10 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for right
Notice of Independent Review Decision DATE OF REVIEW: 12/10/10 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for right
Informed Patient Tutorial Copyright 2012 by the American Academy of Orthopaedic Surgeons
 Informed Patient Tutorial Copyright 2012 by the American Academy of Orthopaedic Surgeons Informed Patient - Carpal Tunnel Release Surgery Introduction Welcome to the American Academy of Orthopaedic Surgeons'
Informed Patient Tutorial Copyright 2012 by the American Academy of Orthopaedic Surgeons Informed Patient - Carpal Tunnel Release Surgery Introduction Welcome to the American Academy of Orthopaedic Surgeons'
NERVE COMPRESSION DISORDERS
 Common Disorders of the Hand and Wrist Ryan Klinefelter, MD Associate Professor of Orthopaedics Department of Orthopaedics The Ohio State University Medical Center NERVE COMPRESSION DISORDERS 1 Carpal
Common Disorders of the Hand and Wrist Ryan Klinefelter, MD Associate Professor of Orthopaedics Department of Orthopaedics The Ohio State University Medical Center NERVE COMPRESSION DISORDERS 1 Carpal
LSU Health Sciences Center Occupational Therapy Flexor Tendon Injury Treatment Protocol
 . LSU Health Sciences Center Occupational Therapy Flexor Tendon Injury Treatment Protocol DIP PIP MCP Zone 1 Zone 2 T 1 T 2 Zone 3 T 3 Zone 4 Zone 5 Zone 5 cs Carla M. Saulsbery LOTR, CHT Dr. A. Hollister,
. LSU Health Sciences Center Occupational Therapy Flexor Tendon Injury Treatment Protocol DIP PIP MCP Zone 1 Zone 2 T 1 T 2 Zone 3 T 3 Zone 4 Zone 5 Zone 5 cs Carla M. Saulsbery LOTR, CHT Dr. A. Hollister,
BEFORE THE APPEALS BOARD FOR THE KANSAS DIVISION OF WORKERS COMPENSATION
 BEFORE THE APPEALS BOARD FOR THE KANSAS DIVISION OF WORKERS COMPENSATION BARBARA SHEREE HUTSON ) Claimant ) ) VS. ) Docket No. 1,035,700 ) CUSTOM CAMPERS, INC. ) Self-Insured Respondent ) ORDER Claimant
BEFORE THE APPEALS BOARD FOR THE KANSAS DIVISION OF WORKERS COMPENSATION BARBARA SHEREE HUTSON ) Claimant ) ) VS. ) Docket No. 1,035,700 ) CUSTOM CAMPERS, INC. ) Self-Insured Respondent ) ORDER Claimant
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis
 FPL FCR Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis Thenar motor branch Kaplan s cardinal line: distal TCL thenar branch Superficial palmar arch superficial arch Originates
FPL FCR Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis Thenar motor branch Kaplan s cardinal line: distal TCL thenar branch Superficial palmar arch superficial arch Originates
 Full version is >>> HERE
Full version is >>> HERE Scaphoid Fracture of the Wrist
 Page 1 of 6 Scaphoid Fracture of the Wrist Doctors commonly diagnose a sprained wrist after a patient falls on an outstretched hand. However, if pain and swelling don't go away, doctors become suspicious
Page 1 of 6 Scaphoid Fracture of the Wrist Doctors commonly diagnose a sprained wrist after a patient falls on an outstretched hand. However, if pain and swelling don't go away, doctors become suspicious
Injuries to Upper Limb
 Injuries to Upper Limb 1 The following is a list of common sporting conditions and injuries. The severity of each condition may lead to different treatment protocols and certainly varying levels of intervention.
Injuries to Upper Limb 1 The following is a list of common sporting conditions and injuries. The severity of each condition may lead to different treatment protocols and certainly varying levels of intervention.
How To Know If You Can Get A Carpal Tunnel Injury Compensation
 U. S. DEPARTMENT OF LABOR Employees Compensation Appeals Board In the Matter of BARBARA SNYDER and DEPARTMENT OF THE TREASURY, INTERNAL REVENUE SERVICE, Germansville, PA Docket No. 03-1467; Submitted on
U. S. DEPARTMENT OF LABOR Employees Compensation Appeals Board In the Matter of BARBARA SNYDER and DEPARTMENT OF THE TREASURY, INTERNAL REVENUE SERVICE, Germansville, PA Docket No. 03-1467; Submitted on
A Patient s Guide to Shoulder Pain
 A Patient s Guide to Shoulder Pain Part 2 Evaluating the Patient James T. Mazzara, M.D. Shoulder and Elbow Surgery Sports Medicine Occupational Orthopedics Patient Education Disclaimer This presentation
A Patient s Guide to Shoulder Pain Part 2 Evaluating the Patient James T. Mazzara, M.D. Shoulder and Elbow Surgery Sports Medicine Occupational Orthopedics Patient Education Disclaimer This presentation
A Patient s Guide to Carpal Tunnel Syndrome
 A Patient s Guide to Carpal Tunnel Syndrome 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 [email protected] DISCLAIMER: The information in this booklet is compiled from a
A Patient s Guide to Carpal Tunnel Syndrome 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 [email protected] DISCLAIMER: The information in this booklet is compiled from a
Adult Forearm Fractures
 Adult Forearm Fractures Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken. Fractures of the forearm can occur near the wrist at
Adult Forearm Fractures Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken. Fractures of the forearm can occur near the wrist at
Ergonomics Monitor Training Manual
 Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
8 th Annual W/C Spine Summit. Ted A. Lennard, MD Feb. 12, 2015
 8 th Annual W/C Spine Summit Ted A. Lennard, MD Feb. 12, 2015 Case Study 45 y.o. male Truck Accident on 1/15/12 Slid on ice and crossed median. Case Study Taken by ambulance to ER in Texas +Loss of consciousness
8 th Annual W/C Spine Summit Ted A. Lennard, MD Feb. 12, 2015 Case Study 45 y.o. male Truck Accident on 1/15/12 Slid on ice and crossed median. Case Study Taken by ambulance to ER in Texas +Loss of consciousness
THORACIC OUTLET SYNDROME
 THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
Symptoms and Signs of Irritation of the Brachial Plexus in Whiplash Injuries
 1 Symptoms and Signs of Irritation of the Brachial Plexus in Whiplash Injuries J Bone Joint Surg (Br) 2001 Mar;83(2):226-9 Ide M, Ide J, Yamaga M, Takagi K Department of Orthopaedic Surgery, Kumamoto University
1 Symptoms and Signs of Irritation of the Brachial Plexus in Whiplash Injuries J Bone Joint Surg (Br) 2001 Mar;83(2):226-9 Ide M, Ide J, Yamaga M, Takagi K Department of Orthopaedic Surgery, Kumamoto University
A Simplified Approach to Common Shoulder Problems
 A Simplified Approach to Common Shoulder Problems Objectives: Understand the basic categories of common shoulder problems. Understand the common patient symptoms. Understand the basic exam findings. Understand
A Simplified Approach to Common Shoulder Problems Objectives: Understand the basic categories of common shoulder problems. Understand the common patient symptoms. Understand the basic exam findings. Understand
Elbow Examination. Haroon Majeed
 Elbow Examination Haroon Majeed Key Points Inspection Palpation Movements Neurological Examination Special tests Joints above and below Before Starting Introduce yourself Explain to the patient what the
Elbow Examination Haroon Majeed Key Points Inspection Palpation Movements Neurological Examination Special tests Joints above and below Before Starting Introduce yourself Explain to the patient what the
Differentiating Cervical Radiculopathy and Peripheral Neuropathy. Adam P. Smith, MD
 Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
The Hand Exam: Tips and Tricks
 The Hand Exam: Tips and Tricks Nikki Strauss Schroeder, MD Assistant Clinical Professor, UCSF Department of Orthopaedic Surgery November 4, 2013 Outline Surface Anatomy Hand Anatomy Exam Management of
The Hand Exam: Tips and Tricks Nikki Strauss Schroeder, MD Assistant Clinical Professor, UCSF Department of Orthopaedic Surgery November 4, 2013 Outline Surface Anatomy Hand Anatomy Exam Management of
CUMMULATIVE DISORDERS OF UPPER EXTIMITY DR HABIBOLLAHI
 CUMMULATIVE DISORDERS OF UPPER EXTIMITY DR HABIBOLLAHI Definition Musculoskeletal disorder (MSD) is an injury or disorder of the muscles, nerves, tendons, joints, cartilage,ligament and spinal discs. It
CUMMULATIVE DISORDERS OF UPPER EXTIMITY DR HABIBOLLAHI Definition Musculoskeletal disorder (MSD) is an injury or disorder of the muscles, nerves, tendons, joints, cartilage,ligament and spinal discs. It
Evaluation of Disorders of the Hands and Wrists
 Evaluation of Disorders of the Hands and Wrists Case 27 yo female with 6 month history of right forearm and hand pain Works as secretary, symptoms are interfering with her job duties Complains that she
Evaluation of Disorders of the Hands and Wrists Case 27 yo female with 6 month history of right forearm and hand pain Works as secretary, symptoms are interfering with her job duties Complains that she
SHOULDER PAIN. Procedures: Subacromial, Glenohumeral and Acromioclavicular Injections Nonprocedural Treatments
 SHOULDER PAIN Anatomy Conditions: Muscular Spasm Pinched Nerve Rotator Cuff Tendonitis Procedures: Subacromial, Glenohumeral and Acromioclavicular Injections Nonprocedural Treatments Surgery: Rotator Cuff
SHOULDER PAIN Anatomy Conditions: Muscular Spasm Pinched Nerve Rotator Cuff Tendonitis Procedures: Subacromial, Glenohumeral and Acromioclavicular Injections Nonprocedural Treatments Surgery: Rotator Cuff
 Full version is >>> HERE
Full version is >>> HERE THORACIC OUTLET SYNDROME & BRACHIAL PLEXUS INJURIES
 THORACIC OUTLET SYNDROME & BRACHIAL PLEXUS INJURIES I. THORACIC OUTLET SYNDROME TOS is a compression of nerves or blood vessels, or both, in the thoracic outlet region, which is the space between the collarbone
THORACIC OUTLET SYNDROME & BRACHIAL PLEXUS INJURIES I. THORACIC OUTLET SYNDROME TOS is a compression of nerves or blood vessels, or both, in the thoracic outlet region, which is the space between the collarbone
THE WRIST. At a glance. 1. Introduction
 THE WRIST At a glance The wrist is possibly the most important of all joints in everyday and professional life. It is under strain not only in many blue collar trades, but also in sports and is therefore
THE WRIST At a glance The wrist is possibly the most important of all joints in everyday and professional life. It is under strain not only in many blue collar trades, but also in sports and is therefore
CONSTRUCTION WORK and CUMULATIVE TRAUMA DISORDERS
 Connecticut Department of Public Health Environmental and Occupational Health Assessment Program 410 Capitol Avenue MS # 11OSP, PO Box 340308 Hartford, CT 06134-0308 (860) 509-7740 http://www.ct.gov/dph
Connecticut Department of Public Health Environmental and Occupational Health Assessment Program 410 Capitol Avenue MS # 11OSP, PO Box 340308 Hartford, CT 06134-0308 (860) 509-7740 http://www.ct.gov/dph
WRIST EXAMINATION. Look. Feel. Move. Special Tests
 WRIST EXAMINATION Look o Dorsum, side, palmar- palmar flex wrist to exacerbate dorsal swellings o Deformity e.g. radial deviation after colles, prominent ulna o Swellings e.g. ganglion o Scars, muscle
WRIST EXAMINATION Look o Dorsum, side, palmar- palmar flex wrist to exacerbate dorsal swellings o Deformity e.g. radial deviation after colles, prominent ulna o Swellings e.g. ganglion o Scars, muscle
Chapter 7 The Wrist and Hand Joints
 Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
A Patient s Guide to Guyon s Canal Syndrome
 A Patient s Guide to DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or
A Patient s Guide to DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or
Lean-Ergonomic methods to reduce workers compensation costs (Part 2 of 2) Cumulative trauma disorders can be classified as: What is CTD?
 Cumulative trauma disorders can be classified as: What is CTD?") #425 Lean-ergonomic methods to reduce workers compensation costs, Part 2 of 2 Lean-Ergonomic methods to reduce workers compensation costs (Part 2 of 2) Govid Bharwani, Ph.D, Biomedical Engineering Thursday,
#425 Lean-ergonomic methods to reduce workers compensation costs, Part 2 of 2 Lean-Ergonomic methods to reduce workers compensation costs (Part 2 of 2) Govid Bharwani, Ph.D, Biomedical Engineering Thursday,
Elbow Injuries and Disorders
 Elbow Injuries and Disorders Introduction Your elbow joint is made up of bone, cartilage, ligaments and fluid. Muscles and tendons help the elbow joint move. There are many injuries and disorders that
Elbow Injuries and Disorders Introduction Your elbow joint is made up of bone, cartilage, ligaments and fluid. Muscles and tendons help the elbow joint move. There are many injuries and disorders that
.org. Rotator Cuff Tears. Anatomy. Description
 Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
Wrist Fracture. Please stick addressograph here
 ORTHOPAEDIC UNIT: 01-293 8687 /01-293 6602 UPMC BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS FOLLOWING WRIST FRACTURE Please stick addressograph
ORTHOPAEDIC UNIT: 01-293 8687 /01-293 6602 UPMC BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS FOLLOWING WRIST FRACTURE Please stick addressograph
Upper Limb. The following case studies relate to injuries to the Upper Limb.
 Upper Limb The following case studies relate to injuries to the Upper Limb. More detailed information regarding the assessment of injuries to the upper limb may be found at Chapter 2 of the MAA s Permanent
Upper Limb The following case studies relate to injuries to the Upper Limb. More detailed information regarding the assessment of injuries to the upper limb may be found at Chapter 2 of the MAA s Permanent
Employees Compensation Appeals Board
 U. S. DEPARTMENT OF LABOR Employees Compensation Appeals Board In the Matter of SHEILA WILSON and U.S. POSTAL SERVICE, POST OFFICE, Gaithersburg, MD Docket No. 99-735; Submitted on the Record; Issued December
U. S. DEPARTMENT OF LABOR Employees Compensation Appeals Board In the Matter of SHEILA WILSON and U.S. POSTAL SERVICE, POST OFFICE, Gaithersburg, MD Docket No. 99-735; Submitted on the Record; Issued December
Elbow, Forearm, Wrist, & Hand. Bony Anatomy. Objectives. Bones. Bones. Bones
 Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
ACUTE HAND INJURY PROTOCOLS
 ACUTE HAND INJURY PROTOCOLS I. FRACTURES OF THE HAND AND DIGITS Digital and hand fractures are seen in workers who use their hands, due to the exposed nature of the hand (in most functions) at work. Most
ACUTE HAND INJURY PROTOCOLS I. FRACTURES OF THE HAND AND DIGITS Digital and hand fractures are seen in workers who use their hands, due to the exposed nature of the hand (in most functions) at work. Most
.org. Shoulder Pain and Common Shoulder Problems. Anatomy. Cause
 Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
WORKCOVER DIVISION Case No. A12596889 --- S GARNETT LATROBE VALLEY REASONS FOR DECISION ---
 !Undefined Bookmark, I IN THE MAGISTRATES COURT OF VICTORIA AT LATROBE VALLEY WORKCOVER DIVISION Case No. A12596889 LEE ANNE SHEARS Plaintiff v STATE OF VICTORIA Defendant --- MAGISTRATE: S GARNETT WHERE
!Undefined Bookmark, I IN THE MAGISTRATES COURT OF VICTORIA AT LATROBE VALLEY WORKCOVER DIVISION Case No. A12596889 LEE ANNE SHEARS Plaintiff v STATE OF VICTORIA Defendant --- MAGISTRATE: S GARNETT WHERE
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Hand Injuries and Disorders
 Hand Injuries and Disorders Introduction Each of your hands has 27 bones, 15 joints and approximately 20 muscles. There are many common problems that can affect your hands. Hand problems can be caused
Hand Injuries and Disorders Introduction Each of your hands has 27 bones, 15 joints and approximately 20 muscles. There are many common problems that can affect your hands. Hand problems can be caused
SHOULDER ACROMIOPLASTY/ SHOULDER DECOMPRESSION
 ORTHOPAEDIC WARD: 01-293 8687 /01-293 6602 BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS HAVING A SHOULDER ACROMIOPLASTY/ SHOULDER DECOMPRESSION
ORTHOPAEDIC WARD: 01-293 8687 /01-293 6602 BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS HAVING A SHOULDER ACROMIOPLASTY/ SHOULDER DECOMPRESSION
Common Hand and Wrist Conditions: When to Refer? Dr Tim Heath
 Common Hand and Wrist Conditions: When to Refer? Dr Tim Heath Difficult Balance Many hand conditions can be managed non-operatively / simply Missed injury or delayed diagnosis not uncommon Common Problems
Common Hand and Wrist Conditions: When to Refer? Dr Tim Heath Difficult Balance Many hand conditions can be managed non-operatively / simply Missed injury or delayed diagnosis not uncommon Common Problems
Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario
 Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Treatment Options for Rotator Cuff Tears A Guide for Adults
 Treatment Options for Rotator Cuff Tears A Guide for Adults Is This Guide for Me? YES, if your doctor has told you that you have a rotator cuff tear, which is an injury to one or more of the muscles and
Treatment Options for Rotator Cuff Tears A Guide for Adults Is This Guide for Me? YES, if your doctor has told you that you have a rotator cuff tear, which is an injury to one or more of the muscles and
Rotator Cuff Tears in Football
 Disclosures Rotator Cuff Tears in Football Roger Ostrander, MD Consultant: Mitek Consultant: On-Q Research Support: Arthrex Research Support: Breg Research Support: Arthrosurface 2 Anatomy 4 major muscles:
Disclosures Rotator Cuff Tears in Football Roger Ostrander, MD Consultant: Mitek Consultant: On-Q Research Support: Arthrex Research Support: Breg Research Support: Arthrosurface 2 Anatomy 4 major muscles:
Examination of the Elbow. Elbow Examination. Structures to Examine. Active Range of Motion. Active Range of Motion 8/22/2012
 Examination of the Elbow The elbow is a complex modified hinge joint The humero-ulnar joint is a hinge joint allowing flexion and extension The radio-ulnar joint allows for pronation and supination of
Examination of the Elbow The elbow is a complex modified hinge joint The humero-ulnar joint is a hinge joint allowing flexion and extension The radio-ulnar joint allows for pronation and supination of
The Elbow, Forearm, Wrist, and Hand
 Elbow - Bones The Elbow, Forearm, Wrist, and Hand Chapters 23 & 24 Humerus Distal end forms the medial & lateral condyles Lateral: capitulum Medial: trochlea Radius Ulna Sports Medicine II Elbow - Bones
Elbow - Bones The Elbow, Forearm, Wrist, and Hand Chapters 23 & 24 Humerus Distal end forms the medial & lateral condyles Lateral: capitulum Medial: trochlea Radius Ulna Sports Medicine II Elbow - Bones
BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F102457 OPINION FILED JULY 20, 2004
 BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F102457 KEN WATERS, EMPLOYEE CENTURY TUBE CORPORATION, EMPLOYER CROCKETT ADJUSTMENT, CARRIER CLAIMANT RESPONDENT RESPONDENT OPINION FILED
BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F102457 KEN WATERS, EMPLOYEE CENTURY TUBE CORPORATION, EMPLOYER CROCKETT ADJUSTMENT, CARRIER CLAIMANT RESPONDENT RESPONDENT OPINION FILED
Refer to Specialist. The Diagnosis and Management of Shoulder Pain 1. SLAP lesions, types 1 through 4
 The Diagnosis Management of Shoulder Pain 1 Significant Hisry -Age -Extremity Dominance -Hisry of trauma, dislocation, subluxation -Weakness, numbness, paresthesias -Sports participation -Past medical
The Diagnosis Management of Shoulder Pain 1 Significant Hisry -Age -Extremity Dominance -Hisry of trauma, dislocation, subluxation -Weakness, numbness, paresthesias -Sports participation -Past medical
Completing the Loop: Management of the Adolescent Sports Injury. Adam Thomas, PT, DPT, ATC
 : Management of the Adolescent Sports Injury Adam Thomas, PT, DPT, ATC https://www.youtube.com/watch?v=vbufpo 8s3As On field assessment can be the most efficient when the health care provider has observed
: Management of the Adolescent Sports Injury Adam Thomas, PT, DPT, ATC https://www.youtube.com/watch?v=vbufpo 8s3As On field assessment can be the most efficient when the health care provider has observed
Carpal Tunnel Release. Relieving Pressure in Your Wrist
 Carpal Tunnel Release Relieving Pressure in Your Wrist Understanding Carpal Tunnel Syndrome Carpal tunnel syndrome (CTS) is a problem that affects the wrist and hand. If you have CTS, tingling and numbness
Carpal Tunnel Release Relieving Pressure in Your Wrist Understanding Carpal Tunnel Syndrome Carpal tunnel syndrome (CTS) is a problem that affects the wrist and hand. If you have CTS, tingling and numbness
what do you mean by Acute Carpal Tunnel Syndrome? 7/14/2012 Acute Variants of Typically Chronic Conditions
 what do you mean by DMK Acute Causes of Chronic Conditions Acute Carpal Tunnel Syndrome? Acute Variants of Typically Chronic Conditions Acute Variants of Typically Chronic Conditions Kennedy-White Orthopaedic
what do you mean by DMK Acute Causes of Chronic Conditions Acute Carpal Tunnel Syndrome? Acute Variants of Typically Chronic Conditions Acute Variants of Typically Chronic Conditions Kennedy-White Orthopaedic
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy Front View Long head of bicep Acromion Figure 1 Shoulder anatomy Supraspinatus Image Copyright 2010 UW Health Sports Medicine Center. Short head of bicep
Rehabilitation Guidelines for Shoulder Arthroscopy Front View Long head of bicep Acromion Figure 1 Shoulder anatomy Supraspinatus Image Copyright 2010 UW Health Sports Medicine Center. Short head of bicep
RADIOGRAPHIC EVALUATION
 Jeff Husband MD Objectives Evaluate, diagnose and manage common wrist injuries due to high energy trauma in athletes Appropriately use radiographs, CT scans and MRI Know when to refer patients for additional
Jeff Husband MD Objectives Evaluate, diagnose and manage common wrist injuries due to high energy trauma in athletes Appropriately use radiographs, CT scans and MRI Know when to refer patients for additional
.org. Tennis Elbow (Lateral Epicondylitis) Anatomy. Cause
 Anatomy. Cause") Tennis Elbow (Lateral Epicondylitis) Page ( 1 ) Tennis elbow, or lateral epicondylitis, is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can
Tennis Elbow (Lateral Epicondylitis) Page ( 1 ) Tennis elbow, or lateral epicondylitis, is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can
Ms. Ruth Delaney ROTATOR CUFF DISEASE Orthopaedic Surgeon, Shoulder Specialist
 WHAT DOES THE ROTATOR CUFF DO? WHAT DOES THE ROTATOR CUFF DO? WHO GETS ROTATOR CUFF TEARS? HOW DO I CLINICALLY DIAGNOSE A CUFF TEAR? WHO NEEDS AN MRI? DOES EVERY CUFF TEAR NEED TO BE FIXED? WHAT DOES ROTATOR
WHAT DOES THE ROTATOR CUFF DO? WHAT DOES THE ROTATOR CUFF DO? WHO GETS ROTATOR CUFF TEARS? HOW DO I CLINICALLY DIAGNOSE A CUFF TEAR? WHO NEEDS AN MRI? DOES EVERY CUFF TEAR NEED TO BE FIXED? WHAT DOES ROTATOR
Shoulder Arthroscopy
 Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Arthroscopy Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint. The word
Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Arthroscopy Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint. The word
TOWN CENTER ORTHOPAEDIC ASSOCIATES P.C. Labral Tears
 Labral Tears The shoulder is your body s most flexible joint. It is designed to let the arm move in almost any direction. But this flexibility has a price, making the joint prone to injury. The shoulder
Labral Tears The shoulder is your body s most flexible joint. It is designed to let the arm move in almost any direction. But this flexibility has a price, making the joint prone to injury. The shoulder
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Integra. MCP Joint Replacement PATIENT INFORMATION
 Integra MCP Joint Replacement PATIENT INFORMATION Integra MCP Patient Information This brochure summarizes information about the use, risks, and benefits of the Integra MCP finger implant. Be sure to discuss
Integra MCP Joint Replacement PATIENT INFORMATION Integra MCP Patient Information This brochure summarizes information about the use, risks, and benefits of the Integra MCP finger implant. Be sure to discuss
BEFORE THE ARKANSAS WORKERS COMPENSATION COMMISSION CLAIM NUMBER F205928 DOUGLAS EUGENE WHIPKEY, EMPLOYEE CLAIMANT XPRESS BOATS, EMPLOYER RESPONDENT
 BEFORE THE ARKANSAS WORKERS COMPENSATION COMMISSION CLAIM NUMBER F205928 DOUGLAS EUGENE WHIPKEY, EMPLOYEE CLAIMANT XPRESS BOATS, EMPLOYER RESPONDENT CONTINENTAL CASUALTY CO., INSURANCE CARRIER RESPONDENT
BEFORE THE ARKANSAS WORKERS COMPENSATION COMMISSION CLAIM NUMBER F205928 DOUGLAS EUGENE WHIPKEY, EMPLOYEE CLAIMANT XPRESS BOATS, EMPLOYER RESPONDENT CONTINENTAL CASUALTY CO., INSURANCE CARRIER RESPONDENT
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1602/11
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1602/11 BEFORE: M. M. Cohen: Vice-Chair HEARING: August 16, 2011 at Toronto Written DATE OF DECISION: August 23, 2011 NEUTRAL CITATION: 2011
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1602/11 BEFORE: M. M. Cohen: Vice-Chair HEARING: August 16, 2011 at Toronto Written DATE OF DECISION: August 23, 2011 NEUTRAL CITATION: 2011
Shoulder Impingement/Rotator Cuff Tendinitis
 Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints
Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints
Hand and Wrist Injuries and Conditions
 Hand and Wrist Injuries and Conditions Julia Wild Hand Therapist www.southernhandtherapy.com.au 02 9553 8597 POSI Position of Safe Immobilisation So everything is balanced Wrist 30⁰ ext MCP 70⁰ flex for
Hand and Wrist Injuries and Conditions Julia Wild Hand Therapist www.southernhandtherapy.com.au 02 9553 8597 POSI Position of Safe Immobilisation So everything is balanced Wrist 30⁰ ext MCP 70⁰ flex for
J F de Beer, K van Rooyen, D Bhatia. Rotator Cuff Tears
 1 J F de Beer, K van Rooyen, D Bhatia Rotator Cuff Tears Anatomy The shoulder consists of a ball (humeral head) and a socket (glenoid). The muscles around the shoulder act to elevate the arm. The large
1 J F de Beer, K van Rooyen, D Bhatia Rotator Cuff Tears Anatomy The shoulder consists of a ball (humeral head) and a socket (glenoid). The muscles around the shoulder act to elevate the arm. The large
Rotator Cuff Repair Protocol
 Rotator Cuff Repair Protocol Anatomy and Biomechanics The shoulder is a wonderfully complex joint that is made up of the ball and socket connection between the humerus (ball) and the glenoid portion of
Rotator Cuff Repair Protocol Anatomy and Biomechanics The shoulder is a wonderfully complex joint that is made up of the ball and socket connection between the humerus (ball) and the glenoid portion of
Evaluating muscle injuries and residuals of shell fragment and gunshot wounds
 Evaluating muscle injuries and residuals of shell fragment and gunshot wounds Training conducted by: Michael Fishman and Sandrine Fisher 1 Objectives To become familiar with the application of the rating
Evaluating muscle injuries and residuals of shell fragment and gunshot wounds Training conducted by: Michael Fishman and Sandrine Fisher 1 Objectives To become familiar with the application of the rating
GALLAND/KIRBY UCL RECONSTRUCTION (TOMMY JOHN) POST-SURGICAL REHABILITATION PROTOCOL
 POST-SURGICAL REHABILITATION PROTOCOL") GALLAND/KIRBY UCL RECONSTRUCTION (TOMMY JOHN) POST-SURGICAL REHABILITATION PROTOCOL INTRODUCTION The ulnar collateral ligament reconstruction is a tendon transfer procedure. No muscles are transected during
GALLAND/KIRBY UCL RECONSTRUCTION (TOMMY JOHN) POST-SURGICAL REHABILITATION PROTOCOL INTRODUCTION The ulnar collateral ligament reconstruction is a tendon transfer procedure. No muscles are transected during
Treatment Guide Understanding Elbow Pain. Using this Guide. Choosing Your Care. Table of Contents:
 Treatment Guide Understanding Elbow Pain Elbow pain is extremely common whether due to aging, overuse, trauma or a sports injury. When elbow pain interferes with carrying the groceries, participating in
Treatment Guide Understanding Elbow Pain Elbow pain is extremely common whether due to aging, overuse, trauma or a sports injury. When elbow pain interferes with carrying the groceries, participating in
The opinions expressed in the report are solely those of the physician performing the examination.
 401 Second Avenue South, Suite 110 Seattle, WA 98104 Telephone: 206.324.6622 Toll Free: 1.800.331.6622 Fax: 206.726.8605 Medical Examination of Employer: : of Exam: of Birth: of Injury: Location of Exam:
401 Second Avenue South, Suite 110 Seattle, WA 98104 Telephone: 206.324.6622 Toll Free: 1.800.331.6622 Fax: 206.726.8605 Medical Examination of Employer: : of Exam: of Birth: of Injury: Location of Exam:
Arthritis of the Shoulder
 Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
NOT DESIGNATED FOR PUBLICATION
 NOT DESIGNATED FOR PUBLICATION BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F412221 BARBARA FARMER, EMPLOYEE WAL-MART STORES, INC., EMPLOYER CLAIMS MANAGEMENT, INC., INSURANCE CARRIER
NOT DESIGNATED FOR PUBLICATION BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F412221 BARBARA FARMER, EMPLOYEE WAL-MART STORES, INC., EMPLOYER CLAIMS MANAGEMENT, INC., INSURANCE CARRIER
Fractures around wrist
 Fractures around wrist Colles Fracture Smiths fracture Barton s fracture Chauffer s fracture Scaphoid fracture Lunate dislocation Vivek Pandey Colles fracture Definition: Fracture of the distal end radius
Fractures around wrist Colles Fracture Smiths fracture Barton s fracture Chauffer s fracture Scaphoid fracture Lunate dislocation Vivek Pandey Colles fracture Definition: Fracture of the distal end radius
RETURN TO WORK SCHEME Impairment Assessment Guidelines
 RETURN TO WORK SCHEME Impairment Assessment Guidelines March 2015 www.rtwsa.com IMPAIRMENT ASSESSMENT GUIDELINES Return to Work scheme Contents Foreword 2 1 Introduction 3 2 Upper extremity 15 3 Lower
RETURN TO WORK SCHEME Impairment Assessment Guidelines March 2015 www.rtwsa.com IMPAIRMENT ASSESSMENT GUIDELINES Return to Work scheme Contents Foreword 2 1 Introduction 3 2 Upper extremity 15 3 Lower
Ms. Jackson is the Manager of Health Finance and Reimbursement, Division of Health Policy and Practice Services, Washington, DC.
 Electrodiagnostic Testing with Same Day Evaluation Management By: Shane J. Burr, MD; Scott I. Horn, DO; Jenny J. Jackson, MPH, CPC; Joseph P. Purcell, DO Dr. Burr practices general inpatient and outpatient
Electrodiagnostic Testing with Same Day Evaluation Management By: Shane J. Burr, MD; Scott I. Horn, DO; Jenny J. Jackson, MPH, CPC; Joseph P. Purcell, DO Dr. Burr practices general inpatient and outpatient
L. R. v. Fletcher Allen Health Care (January 4, 2007) STATE OF VERMONT DEPARTMENT OF LABOR
 STATE OF VERMONT DEPARTMENT OF LABOR") L. R. v. Fletcher Allen Health Care (January 4, 2007) STATE OF VERMONT DEPARTMENT OF LABOR L. R. Opinion No. 57-06WC By: Margaret A. Mangan v. Hearing Officer Fletcher Allen Health Care For: Patricia Moulton
L. R. v. Fletcher Allen Health Care (January 4, 2007) STATE OF VERMONT DEPARTMENT OF LABOR L. R. Opinion No. 57-06WC By: Margaret A. Mangan v. Hearing Officer Fletcher Allen Health Care For: Patricia Moulton
MAJOR DYSFUNCTION OF JOINTS TREATING PHYSICIAN DATA SHEET
 MAJOR DYSFUNCTION OF JOINTS TREATING PHYSICIAN DATA SHEET Long form FOR REPRESENTATIVE USE ONLY REPRESENTATIVE S NAME AND ADDRESS REPRESENTATIVE S TELEPHONE REPRESENTATIVE S EMAIL PHYSICIAN S NAME AND
MAJOR DYSFUNCTION OF JOINTS TREATING PHYSICIAN DATA SHEET Long form FOR REPRESENTATIVE USE ONLY REPRESENTATIVE S NAME AND ADDRESS REPRESENTATIVE S TELEPHONE REPRESENTATIVE S EMAIL PHYSICIAN S NAME AND
The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
 TOPIC OUTLINE 9- THE WRIST AND HAND. Introduction. The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
TOPIC OUTLINE 9- THE WRIST AND HAND. Introduction. The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
Request for Designated Doctor Examination Type (or print in black ink) each item on this form
 each item on this form") Texas Department of Insurance Division of Workers Compensation 7551 Metro Center Drive, Suite 100 MS-603 Austin, TX 78744-1645 (512) 804-4380 phone (512) 804-4121 fax Complete, if known: DWC Claim # Carrier
Texas Department of Insurance Division of Workers Compensation 7551 Metro Center Drive, Suite 100 MS-603 Austin, TX 78744-1645 (512) 804-4380 phone (512) 804-4121 fax Complete, if known: DWC Claim # Carrier
APPENDIX F INTERJURISDICTIONAL RESEARCH
 Ontario Scheduled Presumption: Bursitis, listed in Schedule 3, of the Ontario Workers Compensation Act, entry number 18 Description of Disease Bursitis Process Any process involving constant or prolonged
Ontario Scheduled Presumption: Bursitis, listed in Schedule 3, of the Ontario Workers Compensation Act, entry number 18 Description of Disease Bursitis Process Any process involving constant or prolonged
AN EDUCATION BASED ERGONOMIC INTERVENTION PROGRAMME FOR GAUTENG CALL CENTRE WORKERS WITH UPPER EXTREMITY REPETITIVE STRAIN INJURIES.
 AN EDUCATION BASED ERGONOMIC INTERVENTION PROGRAMME FOR GAUTENG CALL CENTRE WORKERS WITH UPPER EXTREMITY REPETITIVE STRAIN INJURIES. Sancha Eliot Johannesburg 2010 DECLARATION I SANCHA ELIOT declare that
AN EDUCATION BASED ERGONOMIC INTERVENTION PROGRAMME FOR GAUTENG CALL CENTRE WORKERS WITH UPPER EXTREMITY REPETITIVE STRAIN INJURIES. Sancha Eliot Johannesburg 2010 DECLARATION I SANCHA ELIOT declare that
Mini Medical School: Focus on Orthopaedics
 from The Cleveland Clinic Mini Medical School: Focus on Orthopaedics Common Disorders of the Hand and Wrist Jeffrey Lawton, MD Associate Staff, Department of Orthopaedic The Cleveland Clinic Appointments:
from The Cleveland Clinic Mini Medical School: Focus on Orthopaedics Common Disorders of the Hand and Wrist Jeffrey Lawton, MD Associate Staff, Department of Orthopaedic The Cleveland Clinic Appointments:
Notice of Independent Review Decision DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE:
 Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Treatment Guide Understanding Hand and Wrist Pain. Using this Guide. Choosing Your Care
 Treatment Guide Understanding Hand and Wrist Pain With how much we rely on our hands, there s no wonder hand and wrist pain can be so disabling and frustrating. When this pain interferes with typing on
Treatment Guide Understanding Hand and Wrist Pain With how much we rely on our hands, there s no wonder hand and wrist pain can be so disabling and frustrating. When this pain interferes with typing on