Psychopathy and the DSM IV Criteria for Antisocial Personality Disorder
|
|
|
- Joseph Sullivan
- 8 years ago
- Views:
Transcription
1 Journal of Abnormal Psychology August 1991 Vol. 100, No. 3, by the American Psychological Association For personal use only--not for distribution. Psychopathy and the DSM IV Criteria for Antisocial Personality Disorder Robert D. Hare University of British Columbia Stephen D. Hart University of British Columbia Timothy J. Harpur University of British Columbia ABSTRACT The Axis II Work Group of the Task Force on DSM IV has expressed concern that antisocial personality disorder (APD) criteria are too long and cumbersome and that they focus on antisocial behaviors rather than personality traits central to traditional conceptions of psychopathy and to international criteria. We describe an alternative to the approach taken in the rev. 3rd ed. of the Diagnostic and Statistical Manual of Mental Disorders ( DSM III R ; American Psychiatric Association, 1987 ), namely, the revised Psychopathy Checklist. We also discuss the multisite APD field trials designed to evaluate and compare four criteria sets: the DSM III R criteria, a shortened list of these criteria, the criteria for dyssocial personality disorder from the 10th ed. of the International Classification of Diseases ( World Health Organization, 1990 ), and a 10-item criteria set for psychopathic personality disorder derived from the revised Psychopathy Checklist. The views expressed in this article are those of the authors and do not represent the official positions of the American Psychiatric Association or its Task Force on DSM IV. This work was supported by Grant MT-4511 from the Medical Research Council of Canada and by the Program of Research on Mental Health and the Law of the John D. and Catherine T. MacArthur Foundation. We gratefully acknowledge the substantial contributions of Adelle E. Forth and Sherrie Williamson to the development of the psychopathic personality disorder criteria. We also appreciate the thoughtful comments made by Thomas A. Widiger and Scott Lilienfeld on an earlier draft of the article. Timothy J. Harpur is now at the University of Illinois at Champaign. Correspondence may be addressed to Robert D. Hare, Department of Psychology, University of British Columbia, 2136 West Mall, Vancouver, British Columbia, Canada, V6T 1Y7. Received: July 24, 1990 Revised: October 30, 1990 Accepted: December 17, 1990 The Axis II Work Group of the American Psychiatric Association's Task Force on DSM IV (the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders ) has identified antisocial personality disorder (APD) as "the personality disorder most likely to undergo major changes in (1 of 14) [11/2/2001 3:27:03 PM]

2 DSM IV" ( American Psychiatric Association, 1990, p. 5). The goals of the work group are to "simplify the criteria for this disorder and at the same time include more traditional items, typical of psychopathy" (p. 6). As part of the second goal, the work group hopes to increase "congruency and compatibility" between the DSM IV and criteria from the International Classification of Diseases and Related Health Problems (ICD-10; World Health Organization, 1990 ). The following four criteria sets have been developed for evaluation and comparison in field trials: the existing criteria in the revised DSM III ( DSM III R ; American Psychiatric Association, 1987 ) for APD (see Table 1 ); a shortened list of the DSM III R criteria, developed by Lee Robins ( Table 2 ); the ICD-10 criteria for dyssocial personality disorder ( Table 3 ); and a set of diagnostic criteria for psychopathic personality disorder ( Table 4 ) derived from the Psychopathy Checklist Revised (PCL R; Hare, 1985a, 1991 ). In this article we discuss the concerns that led the Axis II Work Group to consider making changes in the DSM III R criteria for APD. Next, we describe alternative approaches to the DSM III R criteria, focusing on the PCL R. Finally, we comment briefly on the DSM IV APD field trials, which are currently underway in five North American sites (and which are described by Widiger, Frances, Pincus, Davis, & First, 1991 ). DSM III R Criteria for Antisocial Personality Disorder Four criteria, singly necessary and jointly sufficient, are required for a DSM III R diagnosis of APD (see Table 1 ): (a) the patient is at least 18 years old; (b) there is evidence of conduct problems before age 15 (at least 3 of 12 symptoms); (c) there is evidence of a pattern of antisocial behavior that persists into adulthood (at least 4 of 10 symptoms); and (d) antisocial behavior is not the result of (i.e., not exclusively during the course of) certain acute mental disorders, namely, schizophrenia or manic episodes. One major criticism of the DSM III R criteria for APD is that they are too long and cumbersome. The two inclusion criteria (b and c) take the form of fairly lengthy symptom checklists related to antisocial and delinquent behavior; in turn, most symptoms are defined in terms of a number of specific behavioral indicators. Consequently, the number of discrete clinical judgments required to diagnose APD is rather large. This has led to a concern that some clinicians may ignore the explicit APD criteria and rely instead on their own, idiosyncratic prototypical criteria ( Widiger, Frances, & Trull, 1989 ). There is some empirical evidence to justify this concern (e.g., Ford & Widiger, 1989 ; Morey & Ochoa, 1989 ). Also, because such detailed information is required for a diagnosis, clinicians are generally forced to rely to a large extent on patients' memories and self-reports of their past conduct ( Widiger et al., 1989 ) a state of affairs that is particularly problematic, given that untruthfulness is one of the disorder's symptoms (see Table 1 ). An obvious way to make the DSM IV criteria for APD more accessible to its users, then, is merely to shorten and simplify the existing DSM III R criteria. This task was undertaken by Lee Robins, and the resulting criteria set is presented in Table 2. The DSM III R approach to the diagnosis of APD is based on the assumption that personality traits are difficult to measure reliably and that it is easier to agree on the behaviors that typify a disorder than on the reasons why they occur ( Robins, 1978, p. 256). Although the result has been a diagnostic category with good reliability, concerns have been expressed about its content- and construct-related validity, in particular, about its relation to clinical conceptions of psychopathy, in which inferences about affective and interpersonal processes have long played an important role ( Hare, 1983 ; Millon, 1981 ; Wulach, (2 of 14) [11/2/2001 3:27:03 PM]
.")
3 1983 ). This is the second major criticism of the current DSM III R criteria for APD: They represent a rather radical break with clinical tradition (see Cleckley, 1976 ; Karpman, 1961 ; McCord & McCord, 1964 ; Millon, 1981 ), with clinical practice ( Davies & Feldman, 1981 ; Gray & Hutchison, 1964 ), with earlier versions of the DSM, and with international diagnostic nomenclature ( ICD-9 [ World Health Organization, 1978 ] and ICD-10 ; Sartorius, Jablensky, Cooper, & Burke, 1988 ). Specifically, the DSM III R criteria exclude, or at least do not explicitly include, such characteristics as selfishness, egocentricity, callousness, manipulativeness, lack of empathy, and so forth. The lack of congruence between the DSM III R criteria for APD and other well-established conceptions of psychopathy does not appear to have been intentional. Rather, this construct drift seems to have been the unforeseen result of reliance on a fixed (and possibly biased; see Millon, 1981 ) set of behavioral indicators in the DSM III and the DSM III R. That is, the behavioral indicators do not provide adequate coverage of the construct they were designed to measure. As S. O. Lilienfeld (personal communication, September 15, 1990 ) pointed out, a diagnosis of APD is based largely on the use of closed concepts in which the diagnostician is required to select from a fixed and limited set of indicators of a trait; other, perhaps better indicators cannot be used. The use of closed concepts ignores the fact that a given trait can be reflected in a wide variety of behaviors and that a given behavior can reflect more than one personality trait ( Widiger et al., 1989 ). All of those who fulfill the APD criteria may be antisocial, but they may differ greatly in their motivations for being so and in significant interpersonal, affective, and psychopathological features, such as the capacity for empathy, remorse, guilt, anxiety, or loyalty. Paradoxically, the criteria for APD appear to define a diagnostic category that is at once too broad, encompassing criminals and antisocial persons who are psychologically heterogeneous, and too narrow, excluding those who have the personality structure of the psychopath but who have not exhibited some of the specific antisocial behaviors listed for APD ( Millon, 1981 ). 1 This second concern led to the inclusion of two criteria sets in the APD field trials that are closer to the the traditional clinical construct of psychopathy the dyssocial and psychopathic personality disorder criteria ( Tables 3 and 4 ). An Alternative to Antisocial Personality Disorder: The Psychopathy Checklist Revised Criticisms of the DSM III R criteria for APD would be moot if there were no viable alternatives available. Over the last 10 years, however, a great deal of empirical evidence indicates that at least one viable alternative does exist the PCL R. The original PCL ( Hare, 1980 ) was a 22-item clinical rating scale designed to assess the traditional clinical construct of psychopathy, perhaps best exemplified in the work of Cleckley (1976). More recently, a 20-item revision of the scale has been developed (PCL R; Hare, 1985a, 1991 ). Description The 20 items of the PCL R (see Table 5 ) measure behaviors and inferred personality traits considered fundamental to the clinical construct of psychopathy. Most of the traits are treated as open concepts ( Lilienfeld, 1990 ). That is, the rater is provided with a description of a trait and with some behavioral exemplars and is asked to make a judgment about the extent to which a given person has the trait. Each item is scored on a 3-point scale, for which 0 indicates that it definitely does not apply, 1 that it applies somewhat or only in a limited sense, and 2 that it definitely does apply to the person. (3 of 14) [11/2/2001 3:27:03 PM]
.")
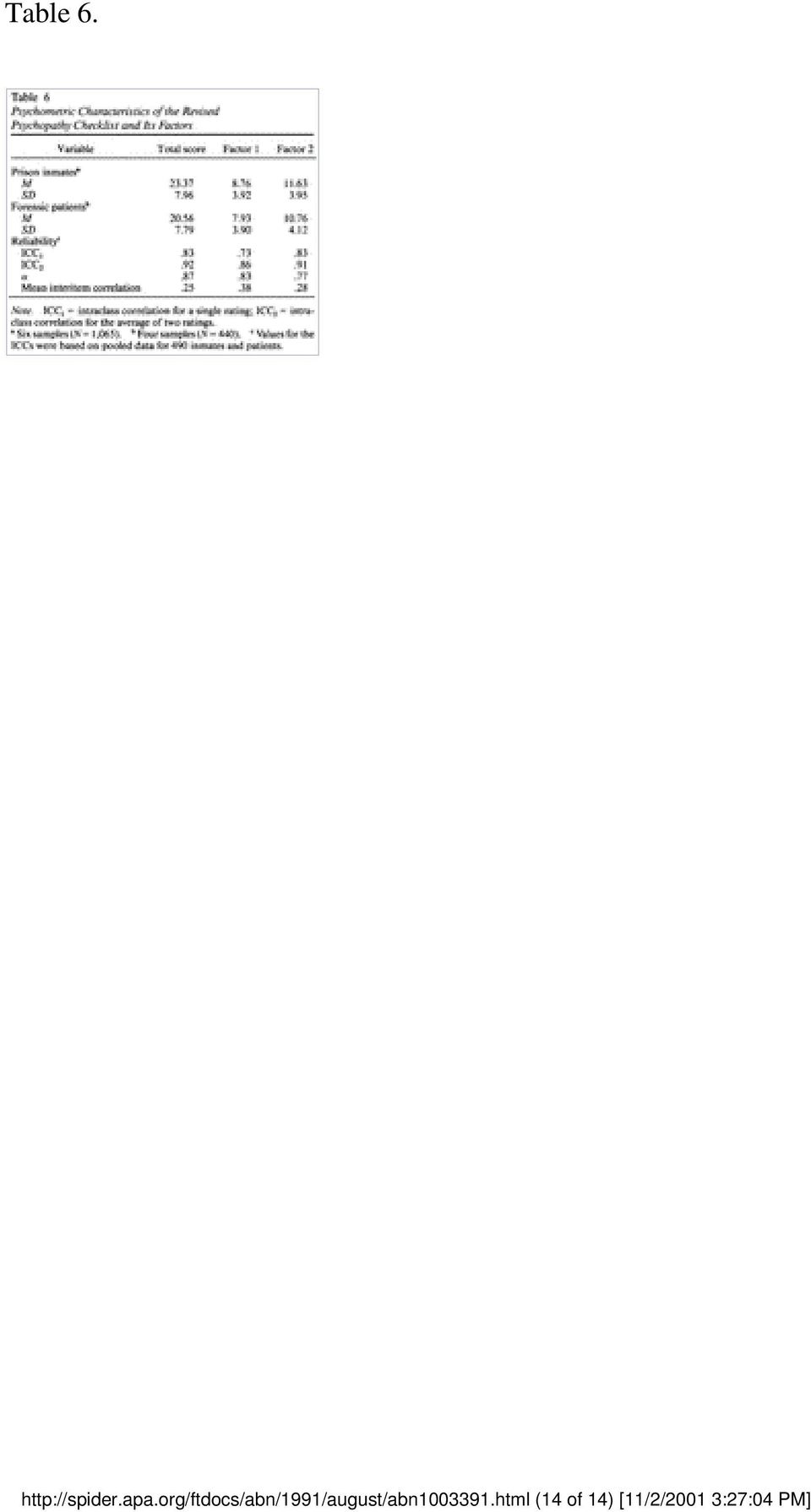
4 The information needed to score the items is obtained from a semistructured interview and institutional files. Detailed instructions for scoring the items are contained in the manual for the PCL R ( Hare, 1991 ). Although clinical judgment and inference are required, the scoring criteria are quite explicit, and with some training, the items are not difficult to score. Descriptive Statistics and Reliability PCL R total scores can range from 0 to 40 and represent the extent to which a person matches the prototypical psychopath. In most forensic samples the distribution of scores is approximately normal, with a slight negative skew. Although the total scores are dimensional, they can be used to provide a categorical diagnosis of psychopathy. A cutoff score of 30 has proven useful for this purpose. Mean PCL R scores are relatively consistent across samples of prison inmates and forensic patients from different institutions and countries. The mean total score for six samples of male prison inmates ( N = 1,065) and four samples of male forensic patients ( N = 440), described by Hare (1991), is presented in Table 6. Despite the subjective nature of most of the PCL R items, each has reasonable interrater reliability (see Table 5 ). The internal consistency of the scale and the interrater reliability of total scores are high in samples of inmates and patients (see Table 6 ). (As values for inmates and patients were much the same, only combined data are presented). Factors There is strong evidence that the PCL R consists of two stable, oblique factors ( Hare et al., 1990 ; Harpur, Hakstian, & Hare, 1988 ). The correlation between the factors is about the same in samples of prison inmates (.56 on average) as it is in samples of forensic patients (.53 on average). The items that define each factor are identified in Table 5. Both factors are psychologically meaningful facets of the higher order construct of psychopathy. Factor 1 clearly reflects a set of interpersonal and affective characteristics, such as egocentricity, lack of remorse, callousness, and so forth, considered fundamental to clinical conceptions of psychopathy. In spite of the relatively small number (8) of items involved, Factor 1 scores, obtained by summing the individual item scores, are reliable in samples of prison inmates and forensic patients (see Table 2 ). Evidence presented elsewhere ( Hare, 1991 ; Harpur, Hare, & Hakstian, 1989 ; Hart & Hare, 1989 ) indicates that Factor 1 is positively correlated with clinical ratings of psychopathy, with prototypicality ratings of narcissistic and histrionic personality disorder, and with self-report measures of machiavellianism and narcissism. It is also negatively correlated with measures of empathy and anxiety. Factor 2 reflects those aspects of psychopathy related to an impulsive, antisocial, and unstable lifestyle. It is positively correlated with diagnoses of APD, criminal behaviors, socioeconomic background, and self-report measures of socialization and antisocial behavior ( Hare, 1991 ; Harpur et al., 1989 ). Validity Evidence for the validity of the PCL and PCL R is reviewed in detail elsewhere ( Hare, 1991 ; Hart, Hare, & Harpur, in press ), and space limitations permit only a very brief outline of this evidence to be (4 of 14) [11/2/2001 3:27:03 PM]

5 presented here. 2 When possible, we examine the comparative validity of the PCL R and APD criteria. Content-related evidence. It is apparent from examination of the criteria sets (see Tables 1 and 5 ) and from our description of these criteria that the PCL R provides more complete coverage of the traditional construct of psychopathy than do the APD criteria. The social deviance or antisociality facet of psychopathy is assessed reasonably well by both the APD criteria and by Factor 2 of the PCL R, but APD neglects the facet of psychopathy assessed by PCL R Factor 1. Concurrent criterion-related evidence. Total scores on the PCL and PCL R are strongly related to other clinical behavioral measures of psychopathy: Point-biserial correlations between total scores and DSM III or DSM III R diagnoses of APD in eight samples of male offenders ( N = 1,603) and in two samples of female offenders ( N = 120) averaged about.55 ( Hare, 1991 ); Factor 2 scores typically correlated higher with APD diagnoses than did Factor 1 scores (about.60 vs..40). Total scores are also correlated with various self-report measures related to psychopathy, including the Psychopathic Deviate and Hypomania scales of the Minnesota Multiphasic Personality Inventory, the California Psychological Inventory Socialization scale, and the Millon Clinical Multiaxial Inventory II Antisocial scale ( Hare, 1985b, 1991 ; Harpur et al., 1989 ). However, the magnitude of these correlations typically is small (about.30.35), as are the correlations between APD and self-reports ( Hare, 1985b ). In general, these self-report scales are more strongly correlated with Factor 2 than with Factor 1. Predictive criterion-related evidence. Hart, Kropp, and Hare (1988) found that the PCL predicted postrelease behavior in a sample of 231 federal offenders, even after they controlled for such variables as criminal history, previous conditional-release violations, and relevant demographic characteristics. Outcome (failure vs. success) correlated.33 with PCL total scores,.25 with PCL diagnoses of psychopathy and.20 with diagnoses of APD. Similar results were obtained by Serin, Peters, and Barbaree (in press) and by Serin (1990). Harris, Rice, and Cormier (in press) reported that the PCL R predicted postrelease violent offending in a sample of 169 male forensic patients. The violent recidivism rate for psychopaths (77%) was almost four times that of nonpsychopaths (21%). The PCL R significantly improved the prediction of outcome over and above the use of criminal history variables and DSM III diagnoses of APD. Violent recidivism correlated.42 with PCL R total scores,.56 with PCL R diagnoses of psychopathy, and.26 with diagnoses of APD. In another study Rice, Harris, and Quinsey (1990) studied 54 rapists released from a maximum security psychiatric hospital. PCL R total scores were significantly correlated with recidivism for violent offenses in general and with recidivism for sexual offenses in particular. A combination of PCL R scores and a phallometric index of arousal (based on penile plethysmography) predicted recidivism as well as did a large battery of criminal history and demographic variables. Ogloff, Wong, and Greenwood (1990) performed an outcome study of 80 men enrolled in a therapeutic community program designed to treat criminals with personality disorders. The data were prospective for (5 of 14) [11/2/2001 3:27:04 PM]

6 some patients and retrospective for others, and the results indicated that PCL R psychopaths remained in the program for a shorter period of time, put in less effort, and showed less improvement than did other inmates. Other construct-related evidence. Total scores typically correlate positively with scores on various measures of impulsivity, machiavellianism, narcissism, and sensation-seeking ( Hare, 1991 ; Harpur et al., 1989 ). Foreman (1988) found that PCL R total scores ( N = 79) were positively correlated ( r =.45) with staff ratings of dominance and negatively correlated ( r =.46) with ratings of nurturance on the Interpersonal Adjective Scales ( Wiggins, Trapnell, & Phillips, 1988 ). The PCL R shows good convergent and discriminant validity with respect to diagnoses of mental disorder. Hart and Hare (1989) found that PCL R total scores were positively correlated with diagnoses of substance use disorder, histrionic personality disorder, and APD; they were also correlated with prototypicality ratings of histrionic personality disorder, narcissistic personality disorder, and APD. (Positive correlations between the PCL R and substance use have also been reported by Smith & Newman, 1990.) Psychopaths were less likely than other patients to receive a DSM III Axis I diagnosis (other than substance use disorder). PCL R total and factor scores were either uncorrelated or negatively correlated with prototypicality ratings of schizophrenia and personality disorders (except histrionic, narcissistic, and antisocial, as noted earlier). Further evidence of the discriminant validity of the PCL and PCL R comes from studies with standardized psychological tests. Total scores are uncorrelated or negatively correlated with self-report measures of empathy, anxiety, depression, and general distress or neuroticism ( Hare, 1991 ; Harpur et al., 1989 ; Hart, Forth, & Hare, 1990 ). The results of over a dozen studies indicate that there is no association between total scores and performance on various intelligence tests ( Hare, 1991 ). Also, two studies have reported that total scores are not associated with any impairment in performance on standard neuropsychological tests ( Hare, 1984 ; Hart, Forth, & Hare, 1991). The PCL and PCL R have a strong and stable association with various indexes of criminality. Psychopaths are charged with a greater number and variety of criminal offenses than nonpsychopaths, regardless of race ( Kosson, Smith, & Newman, 1990 ; Wong, 1984 ) or psychiatric status ( Hare, 1991 ; Hart & Hare, 1989 ). Psychopaths commit violent and aggressive offenses at a particularly high rate. For example, in a sample of 244 inmates, Hare and McPherson (1984) found that PCL-defined psychopaths were significantly more likely than other criminals to engage in physical violence and other forms of aggressive behavior, including verbal abuse, threats, and intimidation, both in and out of prison. Williamson, Hare, and Wong (1987) examined the nature of the violent offenses committed by psychopaths. Official police reports were used to analyze the circumstances of the most serious of inmates' instant offenses. Most of the murders and serious assaults committed by the nonpsychopaths occurred during a domestic dispute or during a period of extreme emotional arousal, whereas this was seldom true of the psychopaths. The victims of the nonpsychopaths were likely to be women and known to them, but the victims of the psychopaths were likely to be men and unknown to them. The violence of the psychopaths frequently had revenge or retribution as the motive or occurred during a drinking bout. In general, it appeared that most of the psychopaths' violence was callous and cold-blooded or part of an (6 of 14) [11/2/2001 3:27:04 PM]
 found that PCL R total scores ( N = 79) were positively correlated ( r =.45) with staff ratings of dominance and negatively correlated ( r =.")
7 aggressive, macho display, without the affective coloring that accompanied the violence of nonpsychopaths. Laboratory studies have generated a body of data that is theoretically meaningful with respect to psychopathy and that provides particularly important evidence for the construct validity of the PCL and PCL R. For example, psychopathy is associated with abnormal processing of the affective components of language in a variety of laboratory tasks ( Williamson, Harpur, & Hare, 1990, in press ; see also review by Hare, Williamson, & Harpur, 1988 ). Psychophysiological aspects of affective functioning in psychopaths have also been examined by Patrick and his colleagues ( Patrick, Bradley, & Cuthbert, 1990 ; Patrick, Cuthbert, & Lang, 1990 ). They have reported that psychopaths, defined with the PCL R, gave smaller autonomic responses during fearful imagery than did other offenders and failed to show normal modulation of the blink reflex to an acoustic startle stimulus presented while slides with affective content were viewed. A third line of research has investigated Hare's (1982) hypothesis that psychopaths may be unusually proficient at selectively focusing attention on events that interest them. Several PCL and PCL R studies have produced results that are generally consistent with the hypothesis (for a review, see Harpur & Hare, 1990 ). Finally, Newman and his colleagues have published a series of studies of passive-avoidance learning, disinhibition, and dominant-response set in psychopaths, as defined by the PCL or PCL R (e.g., Kosson & Newman, 1986 ; Newman, Patterson, & Kosson, 1987 ). Consistent with the theoretical model that underlies this research, there was general support for the hypothesis that the disinhibited behavior of psychopaths is related to a dominant-response set for reward. Summary The PCL R assesses both the affective or interpersonal and the social deviance facets of psychopathy, whereas the DSM III R focuses on the latter. The incremental validity obtained by including explicit inferences about key personality traits in the diagnosis of psychopathy is substantial, even when the criterion involves antisocial or criminal behaviors. This is an important point, given that the items that define APD are from much the same domain as, and therefore ought to predict, criterion variables related to criminality, violence, and recidivism. The fact that the PCL and PCL R generally are more strongly related to these criterion variables than is APD attests to the value of including inferences about personality traits in the assessment of psychopathy. Equally important here is the evidence that laboratory tests of hypotheses about the nature of psychopathy are supported when assessment is based on the PCL or PCL R. Although there is no similar body of systematic laboratory research on APD, several of the laboratory studies of psychopathy discussed above also obtained DSM III or DSM III R diagnoses of APD (C. J. Patrick, personal communication, October 23, 1990; Williamson et al., 1990, in press ). In each case, the effects that were significant with the PCL or PCL R were not significant when the presence or absence of APD was the basis for group selection. Development of the Criteria Set for Psychopathic Personality Disorder The extensive evidence on the psychometric properties of the PCL R clearly indicates that it is possible to obtain reliable and valid measures of the personality traits and behaviors associated with psychopathy. However, it is important to note that completion of the PCL R requires a relatively long semistructured interview and access to a considerable amount of collateral information. There is some evidence that the PCL R can be shortened and simplified for clinical use without an unacceptable decrease in reliability or validity. As part of a large-scale study on the risk of violence in (7 of 14) [11/2/2001 3:27:04 PM]

8 the mentally disordered, funded by the John D. and Catherine T MacArthur Foundation and directed by John Monahan (see Monahan, 1990 ), a 12-item screening version of the PCL R (the PCL:SV; Hare, Cox, & Hart, 1989 ) has been tested in seven samples (three prison, two forensic psychiatric, and two civil psychiatric). The items were designed to tap each of the PCL R factors and are scored on the basis of a 30- to 45-min interview and minimal collateral information. Preliminary analyses of data from 331 subjects indicate that the PCL:SV has good psychometric properties. Thus, the average intraclass correlation coefficient (ICC) for a single rating and for the average of two ratings was about.80 and.85, respectively. The average alpha coefficient was about.80 and the mean inter-item correlation (MIC) about.25. The correlation between independent ratings on the PCL:SV and the PCL R averaged about.80. Encouraged by these results, we used the PCL R and the PCL:SV as the basis for development of the 10-item criteria set for psychopathic personality disorder (PPD) presented in Table 4. These items are substantively the same as those in the PCL:SV, and a reasonable reflection of the constructs measured by PCL R Factors 1 and 2. Specific, though relatively brief, instructions are used to score each PPD item on a 3-point scale (2 = item applies, 1 = item applies somewhat, or evidence is mixed, 0 = item does not apply). Total scores can range from 0 to 20 and represent the extent to which the person matches the clinical prototype of the psychopath. Despite the advantages that dimensional ratings have in clinical research and practice, DSM IV plans to continue using simple categorical diagnoses. On the basis of some preliminary analyses, we determined that a diagnosis of PPD must require that 7 of the 10 criteria be satisfied (i.e., scored 2). We estimate that it will yield a base rate for psychopathy of about 25% 30% among federal prisoners and about 15% among forensic psychiatric inpatients; these values are similar to those obtained with the PCL R and PCL:SV, and less than one-half the prevalence of APD. 3 DSM IV Field Trials As we noted earlier, Widiger et al. (1991) describe the APD field trials in some detail. Briefly, they noted that the four criteria sets presented in Tables 1 to 4 will be tested at five different sites. At each site approximately 100 patients (total N = 500) will be administered structured interviews and subsequently assessed with all four criteria sets, wherein about half of subjects will receive an independent reassessment at a later date. This will allow a determination of the interrater reliability, internal consistency, concurrent validity, and coverage of the various criteria sets. In addition, self-report, demographic, and psychosocial history data will be collected to evaluate the construct validity of the criteria sets. If no single criteria set is clearly superior to the others, the Task Force may test various combinations of symptoms from the different criteria sets. We concur with Widiger et al. (1991) that these field trials represent a significant advance over committee or expert consensus approaches to decision making with respect to the content of diagnostic criteria: "The results will not be unambiguous with respect to which criteria set is preferable, but the field trial will provide reliability and validity data that will be informative for their evaluation, and together with the results provided by the literature review and data reanalyses, the study will facilitate the effort to have the decisions of the work group be empirically based" (pp. 286). Perhaps the biggest strength of the field trials is the attempt made to sample subjects from diverse populations (e.g., prisoners, psychiatric inpatients, substance abusers, and adopted-away offspring), so that reliability and validity data can be compared across various settings. (8 of 14) [11/2/2001 3:27:04 PM]

9 Of course, a single study even a large, multicenter study cannot answer all the relevant questions. An important limitation of the field trials is that they will be unable to examine some important aspects of validity, for example, predictive validity with respect to criminal behavior, or experimental validity with respect to psychophysiological or cognitive variables. (As noted earlier, it is in precisely these areas that the PCL and PCL R approach appears superior to APD.) Full evaluation of the construct validity of the criteria sets will be a lengthy (and, some may argue, a never-ending) process, however, and we recognize that the publication of the DSM IV is a practical necessity that cannot be postponed indefinitely. Concluding Comments Despite the successes of the DSM III and DSM III R APD criteria, conceptual and empirical arguments exist for evaluating alternative approaches to the assessment of psychopathy. The field trials described are an important but not final step in this direction, and the data collected may play a crucial role in the selection of the DSM IV APD criteria. However, our hope is that the information presented here will stimulate further research on the comparative validity of diagnostic criteria for psychopathy; although too late to influence DSM IV, this research may well play a decisive role in subsequent versions or revisions of the DSM. References American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (Rev.3rd ed.).(washington DC: Author) American Psychiatric Association. (1990, January/February). DSM IV Update. (Washington, DC: Author) Cleckley, H. (1976). The mask of sanity (5th ed.).(st. Louis MO: Mosby) Correctional Service of Canada. (1990). A mental health profile of federally sentenced offenders. Forum on Corrections Research, 2, 7-8. Davies, W. & Feldman, P. (1981). The diagnosis of psychopathy by forensic specialists. British Journal of Psychiatry, 138, Ford, M. R. & Widiger, T. A. (1989). Sex bias in the diagnosis of histrionic and antisocial personality disorders. Journal of Consulting and Clinical Psychology, 57, Foreman, M. (1988). Psychopathy and interpersonal behavior. (Unpublished doctoral dissertation, University of British Columbia, Vancouver, Canada) Gray, K. C. & Hutchison, H. C. (1964). The psychopathic personality: A survey of Canadian psychiatrists' opinions. Canadian Psychiatric Association Journal, 9, Hare, R. D. (1980). A research scale for the assessment of psychopathy in criminal populations. Personality and Individual Differences, 1, Hare, R. D. (1982). Psychopathy and physiological activity during anticipation of an aversive stimulus in a distraction paradigm. Psychophysiology, 19, Hare, R. D. (1983). Diagnosis of antisocial personality disorder in two prison populations. American Journal of Psychiatry, 140, Hare, R. D. (1984). Performance of psychopaths on cognitive tasks related to frontal-lobe functioning. Journal of Abnormal Psychology, 93, Hare, R. D. (1985a). Comparison of procedures for the assessment of psychopathy. Journal of (9 of 14) [11/2/2001 3:27:04 PM]
 Full evaluation of the construct validity of the criteria sets will be a lengthy (and, some may argue, a never-ending) process, however, and we recognize that the publication of the DSM IV is a")
10 Consulting and Clinical Psychology, 53, Hare, R. D. (1985b). The Psychopathy Checklist. (Unpublished manuscript, University of British Columbia, Vancouver, Canada) Hare, R. D. (1991). The Hare Psychopathy Checklist Revised. (Toronto: Multi-Health Systems) Hare, R. D., Cox, D. N. & Hart, S. D. (1989). Preliminary manual for the Psychopathy Checklist Screening Version (PCL SV). (Unpublished manuscript, University of British Columbia, Vancouver, Canada) Hare, R. D., Harpur, T. J., Hakstian, A. R., Forth, A. E., Hart, S. D. & Newman, J. P. (1990). The revised Psychopathy Checklist: Reliability and factor structure. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 2, Hare, R. D. & McPherson, L. M. (1984). Violent and aggressive behavior by criminal psychopaths. International Journal of Law and Psychiatry, 7, Hare, R. D., Williamson, S. E. & Harpur, T. J. (1988). Psychopathy and language.(in T. E. Moffitt & S. A. Mednick (Eds.), Biological contributions to crime causation (pp ). Dordrecht, the Netherlands: Martinus Nijhoff.) Harpur, T. J., Hakstian, A. R. & Hare, R. D. (1988). Factor structure of the Psychopathy Checklist. Journal of Consulting and Clinical Psychology, 56, Harpur, T. J. & Hare, R. D. (1990). Psychopathy and attention.(in J. Enns (Ed.), The development of attention: Research and theory (pp ). New York: North Holland.) Harpur, T. J., Hare, R. D. & Hakstian, A. R. (1989). Two-factor conceptualization of psychopathy: Construct validity and assessment implications. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 1, Harpur, T. J., Hare, R. D., Zimmerman, M. & Coryell, W. (1990, August). Dimensions underlying DSM III personality disorders: Cluster 2.(Paper presented at the 98th Annual Convention of the American Psychological Association, Boston, MA) Harris, G. T., Rice, M. E. & Cormier, C (in press). Psychopathy and violent recidivism.(law and Human Behavior. ) Hart, S. D., Forth, A. E. & Hare, R. D. (1990). Performance of male psychopaths on selected neuropsychological tests. Journal of Abnormal Psychology, 99, Hart, S. D. & Hare, R. D. (1989). Discriminant validity of the Psychopathy Checklist in a forensic psychiatric population. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 1, Hart, S. D., Hare, R. D. & Harpur, T. J. (in press). The Psychopathy Checklist: An overview for researchers and clinicians.(in J. Rosen & P. McReynolds (Eds.), Advances in psychological assessment (Vol. 8). New York: Plenum Press.) Hart, S. D., Kropp, P. R. & Hare, R. D. (1988). Performance of male psychopaths following conditional release from prison. Journal of Consulting and Clinical Psychology, 56, Karpman, B. (1961). The structure of neurosis: With special differentials between neurosis, psychosis, homosexuality, alcoholism, psychopathy, and criminality. Archives of Criminal Psychodynamics, 4, Kosson, D. S. & Newman, J. P. (1986). Psychopathy and allocation of attentional capacity in a divided-attention situation. Journal of Abnormal Psychology, 95, Kosson, D. S., Smith, S. S. & Newman, J. P. (1990). Evaluation of the construct validity of psychopathy in Black and White male inmates: Three preliminary studies. Journal of Abnormal Psychology, 99, Lilienfeld, S. O. (1990). Conceptual and empirical issues in the assessment of psychopathy. (10 of 14) [11/2/2001 3:27:04 PM]
.")
11 (Unpublished manuscript, University of Albany, State University of New York) McCord, W. & McCord, J. (1964). The psychopath: An essay on the criminal mind. (Princeton, NJ: Van Nostrand) Millon, T. (1981). Disorders of personality: DSM III, Axis II.(New York: Wiley) Monahan, J. (1990). Risk of violence among the mentally disordered: A description of the MacArthur Risk Study. (Unpublished manuscript, University of Virginia School of Law, Charlottesville, VA) Morey, L. C. (1988). The categorical representation of personality disorder: A cluster analysis of DSM III Personality features. Journal of Abnormal Psychology, 97, Morey, L. C. & Ochoa, E. S. (1989). An investigation of adherence to diagnostic criteria: Clinical diagnosis of the DSM III personality disorders. Journal of Personality Disorders, 3, Newman, J. P., Patterson, C. M. & Kosson, D. S. (1987). Response perseveration in psychopaths. Journal of Abnormal Psychology, 96, Ogloff, J. P. R., Wong, S. & Greenwood, A. (1990). Treating criminal psychopaths in a therapeutic community program. Behavioral Sciences and the Law, 8, Patrick, C. J., Bradley, M. & Cuthbert, B. N. (1990). The criminal psychopath and startle modulation. Psychophysiology, 72, (suppl. 4a) S7 Patrick, C. J., Cuthbert, B. N. & Lang, P. J. (1990). Emotion in the criminal psychopath: Fear imagery. Psychophysiology, 27, (suppl. 4a) S55 Rice, M. E., Harris, G. T. & Quinsey, V. L. (1990). A follow-up of rapists assessed in a maximum security psychiatric facility. Journal of Interpersonal Violence, 4, Robins, L. N. (1978). Etiological implications in childhood histories relating to antisocial personality.(in R. D. Hare & D. Schalling (Eds.), Psychopathic behavior: Approaches to research (pp ). Chichester, United Kingdom: Wiley.) Sartorius, N., Jablensky, A., Cooper, J. E. & Burke, J. D. (Eds.) (1988). Psychiatric classification in an international perspective.(the British Journal of Psychiatry 152 (Suppl. 1).) Serin, R.C. (in press). Psychopathy and violence in criminals.(journal of Interpersonal Violence. ) Serin, R., Peters, R. D. & Barbaree, H. E. (1990). Predictors of psychopathy and release outcome in a criminal population. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 2, Smith, S. S. & Newman, J. P. (1990). Alcohol and drug abuse dependence disorders in psychopathic and nonpsychopathic criminal offenders. Journal of Abnormal Psychology, 99, Widiger, T. A., Frances, A. J. & Trull, T. J. (1989). Personality disorders.(in R. J. Craig (Ed.), Clinical and diagnostic interviewing (pp ). Northvale, NJ: Jason Aronson.) Widiger, T. A., Frances, A. J., Pincus, H. A., Davis, W. W. & First, M. (1991). Toward an empirical classification for DSM IV. Journal of Abnormal Psychology, 100, Wiggins, J. S., Trapnell, P. & Phillips, N. (1988). Psychometric and geometric characteristics of the Revised Interpersonal Adjective Scale (IAS-R). Multivariate Behavioral Research, 23, Williamson, S., Hare, R. D. & Wong, S. (1987). Violence: Criminal psychopaths and their victims. Canadian Journal of Behavioral Science, 19, Williamson, S., Harpur, T. J. & Hare, R. D. (in press). Abnormal processing of affective words by psychopaths. Psychophysiology.,, Williamson, S., Harpur, T. J. & Hare, R. D. (1990, August). Sensitivity to emotional valence in psychopaths. (Paper presented at the 98th Annual Convention of the American Psychological Association, Boston, M) Wong, S. (1984). Criminal and institutional behaviors of psychopaths.(programs Branch Users Report. Ottawa, Ontario, Canada: Ministry of the Solicitor-General of Canada.) (11 of 14) [11/2/2001 3:27:04 PM]
.")
12 World Health Organization. (1978). International classification of diseases, injuries and causes of death (9th ed.).(geneva: Author) World Health Organization. (1990). International classification of diseases and related health problems (10th ed.).(geneva: Author) Wulach, J. (1983). Diagnosing the DSM III antisocial personality disorder. Professional Psychology: Research and Practice, 14, It is worth noting here that the DSM III and DSM III R antisocial personality disorder symptoms lack internal consistency and do not appear to form a natural cluster. Rather, some of the antisocial personality disorder symptoms covary with certain symptoms of narcissistic personality disorder such as exploitativeness, grandiosity, and a lack of empathy to form a syndrome very similar to the traditional clinical construct of psychopathy ( Harpur, Hare, Zimmerman, & Coryell, 1990 ; Morey, 1988 ). 2 Data presented elsewhere ( Hare, 1991 ; Hare et al., 1990 ) indicate that the Psychopathy Checklist and its revision are highly correlated and can be considered measures of the same construct. For this reason, we do not distinguish between the two scales in our review of validity-related evidence. 3 A recent study by the Correctional Service of Canada (1990) found that approximately 75% of the male inmates in Canadian federal prisons met the criteria for antisocial personality disorder. Table 1. (12 of 14) [11/2/2001 3:27:04 PM]

13 Table 2. Table 3. Table 4. Table 5. (13 of 14) [11/2/2001 3:27:04 PM]

14 Table 6. (14 of 14) [11/2/2001 3:27:04 PM]
How To Write A Psychopathy Checklist
 Journal of Abnormal Psychology 1991, Vol. 100, No 3,391-398 Copyright 1991 by Ihe Am n Psychological Association. Inc. 002l-g43X/91/H.OO Psychopathy and the DSM-IV Criteria for Antisocial Personality Disorder
Journal of Abnormal Psychology 1991, Vol. 100, No 3,391-398 Copyright 1991 by Ihe Am n Psychological Association. Inc. 002l-g43X/91/H.OO Psychopathy and the DSM-IV Criteria for Antisocial Personality Disorder
Treatment responsivity in criminal psychopaths
 Treatment responsivity in criminal psychopaths Despite general pessimism in the research community about the effectiveness of psychopathy treatment, (2) correctional staff are encouraged to pursue intervention
Treatment responsivity in criminal psychopaths Despite general pessimism in the research community about the effectiveness of psychopathy treatment, (2) correctional staff are encouraged to pursue intervention
PYSCHOPATHY AND ANTISOCIAL PERSONALITY DISORDER. Lisann Nolte & Justine Paeschen
 PYSCHOPATHY AND ANTISOCIAL PERSONALITY DISORDER Lisann Nolte & Justine Paeschen PSYCHOPATHY THE PSYCHOPATH TEST http://www.youtube.com/watch?v=e_va2tl6czwth E PSYCHOPATH TEST - are you a psychopath? PSYCHOPATHY
PYSCHOPATHY AND ANTISOCIAL PERSONALITY DISORDER Lisann Nolte & Justine Paeschen PSYCHOPATHY THE PSYCHOPATH TEST http://www.youtube.com/watch?v=e_va2tl6czwth E PSYCHOPATH TEST - are you a psychopath? PSYCHOPATHY
Personality Disorders
 Personality Disorders Chapter 11 Personality Disorders: An Overview The Nature of Personality and Personality Disorders Enduring and relatively stable predispositions (i.e., ways of relating and thinking)
Personality Disorders Chapter 11 Personality Disorders: An Overview The Nature of Personality and Personality Disorders Enduring and relatively stable predispositions (i.e., ways of relating and thinking)
Co occuring Antisocial Personality Disorder and Substance Use Disorder: Treatment Interventions Joleen M. Haase
 Co occuring Antisocial Personality Disorder and Substance Use Disorder: Treatment Interventions Joleen M. Haase Abstract: Substance abuse is highly prevalent among individuals with a personality disorder
Co occuring Antisocial Personality Disorder and Substance Use Disorder: Treatment Interventions Joleen M. Haase Abstract: Substance abuse is highly prevalent among individuals with a personality disorder
Compiled by Julie Ann Romero AS 91 Spring 2010
 Compiled by Julie Ann Romero AS 91 Spring 2010 Antisocial personality disorder is a psychiatric condition in which a person manipulates, exploits, or violates the rights of others. This behavior is often
Compiled by Julie Ann Romero AS 91 Spring 2010 Antisocial personality disorder is a psychiatric condition in which a person manipulates, exploits, or violates the rights of others. This behavior is often
Working Definitions APPRECIATION OF THE ROLE OF EARLY TRAUMA IN SEVERE PERSONALITY DISORDERS
 Working Definitions PERSONALITY TRAIT a stable, recurring pattern of human behavior - e.g. a tendency to joke in serious situations, hypersensitivity to criticism, talkativeness in groups. PERSONALITY
Working Definitions PERSONALITY TRAIT a stable, recurring pattern of human behavior - e.g. a tendency to joke in serious situations, hypersensitivity to criticism, talkativeness in groups. PERSONALITY
The responsivity principle and offender rehabilitation
 The responsivity principle and offender rehabilitation Researchers began to seriously question the effectiveness of correctional programs in reducing recidivism in the mid-1970s. Many had come to believe
The responsivity principle and offender rehabilitation Researchers began to seriously question the effectiveness of correctional programs in reducing recidivism in the mid-1970s. Many had come to believe
CHAPTER 2: CLASSIFICATION AND ASSESSMENT IN CLINICAL PSYCHOLOGY KEY TERMS
 CHAPTER 2: CLASSIFICATION AND ASSESSMENT IN CLINICAL PSYCHOLOGY KEY TERMS ABC chart An observation method that requires the observer to note what happens before the target behaviour occurs (A), what the
CHAPTER 2: CLASSIFICATION AND ASSESSMENT IN CLINICAL PSYCHOLOGY KEY TERMS ABC chart An observation method that requires the observer to note what happens before the target behaviour occurs (A), what the
Antisocial personality disorder
 Page 1 of 7 Diseases and Conditions Antisocial personality disorder By Mayo Clinic Staff Antisocial personality disorder is a type of chronic mental condition in which a person's ways of thinking, perceiving
Page 1 of 7 Diseases and Conditions Antisocial personality disorder By Mayo Clinic Staff Antisocial personality disorder is a type of chronic mental condition in which a person's ways of thinking, perceiving
Borderline Personality: Traits and Disorder
 Journal of Abnormal Psychology Copyright 2000 by the American Psychological Association, Inc. 2000, Vol. 109, No. 4, 733-737 0021-843X/00/$5.00 DOI: 10.1037//0021-843X.109.4.733 Borderline Personality:
Journal of Abnormal Psychology Copyright 2000 by the American Psychological Association, Inc. 2000, Vol. 109, No. 4, 733-737 0021-843X/00/$5.00 DOI: 10.1037//0021-843X.109.4.733 Borderline Personality:
Sue/Sue/Sue Understanding Abnormal Behavior, 9 th edition 2010 Cengage Learning CHAPTER EIGHT. Personality Disorders
 Sue/Sue/Sue Understanding Abnormal Behavior, 9 th edition 2010 Cengage Learning CHAPTER EIGHT Personality Disorders PERSONALITY DISORDERS Personality Disorder: Sue/Sue/Sue Understanding Abnormal Behavior,
Sue/Sue/Sue Understanding Abnormal Behavior, 9 th edition 2010 Cengage Learning CHAPTER EIGHT Personality Disorders PERSONALITY DISORDERS Personality Disorder: Sue/Sue/Sue Understanding Abnormal Behavior,
California Sex Offender Management Board. Sex Offender Treatment Training Requirements
 California Sex Offender Management Board Sex Offender Treatment Training Requirements August 2013 CASOMB Certification and Re-certification Requirements for Sex Offender Treatment Providers (Revised July,
California Sex Offender Management Board Sex Offender Treatment Training Requirements August 2013 CASOMB Certification and Re-certification Requirements for Sex Offender Treatment Providers (Revised July,
Anti-Social Personality Disorder
 Anti-Social Personality Disorder Definition Anti-Social Personality Disorder is a type of chronic mental condition in which a person's ways of thinking, perceiving situations and relating to others are
Anti-Social Personality Disorder Definition Anti-Social Personality Disorder is a type of chronic mental condition in which a person's ways of thinking, perceiving situations and relating to others are
Presently, there are no means of preventing bipolar disorder. However, there are ways of preventing future episodes: 1
 What is bipolar disorder? There are two main types of bipolar illness: bipolar I and bipolar II. In bipolar I, the symptoms include at least one lifetime episode of mania a period of unusually elevated
What is bipolar disorder? There are two main types of bipolar illness: bipolar I and bipolar II. In bipolar I, the symptoms include at least one lifetime episode of mania a period of unusually elevated
Dusty L Humes, Ph.D., Licensed Psychologist
 ! Dusty L Humes, Ph.D., Licensed Psychologist 2201 San Pedro NE, Building 4-102, Albuquerque, NM 87110 512.917.3126 dustyhumesphd@gmail.com www.dustyhumes.com Profile I am a clinical psychologist who recently
! Dusty L Humes, Ph.D., Licensed Psychologist 2201 San Pedro NE, Building 4-102, Albuquerque, NM 87110 512.917.3126 dustyhumesphd@gmail.com www.dustyhumes.com Profile I am a clinical psychologist who recently
Mental Health Needs Assessment Personality Disorder Prevalence and models of care
 Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
STATE OF OHIO. DEPARTMENT OF REHABILITATION RELATED ACA STANDARDS: EFFECTIVE DATE: AND CORRECTION February 19, 2011 I. AUTHORITY
 STATE OF OHIO SUBJECT: PAGE 1 OF 7. Specialized Assessments and Screenings NUMBER: 67-MNH-16 RULE/CODE REFERENCE: SUPERSEDES: AR 5120-11-03, 07, 21 67-MNH-16 dated 01/13/10 ORC 5120.031; 5120.032; 5120.033
STATE OF OHIO SUBJECT: PAGE 1 OF 7. Specialized Assessments and Screenings NUMBER: 67-MNH-16 RULE/CODE REFERENCE: SUPERSEDES: AR 5120-11-03, 07, 21 67-MNH-16 dated 01/13/10 ORC 5120.031; 5120.032; 5120.033
The effects of neuropsychological impairment on offender performance in substance abuse treatment
 The effects of neuropsychological impairment on offender performance in substance abuse treatment A recent mental health survey (2) of Canadian federal offenders indicated a 4.3% lifetime prevalence rate
The effects of neuropsychological impairment on offender performance in substance abuse treatment A recent mental health survey (2) of Canadian federal offenders indicated a 4.3% lifetime prevalence rate
Guidelines for Physical and Psychological Evaluations
 Guidelines for Physical and Psychological Evaluations The purpose of this document is to inform licensees, applicants, petitioners, and the public about the Board s requirements and procedures regarding
Guidelines for Physical and Psychological Evaluations The purpose of this document is to inform licensees, applicants, petitioners, and the public about the Board s requirements and procedures regarding
Statistics on Women in the Justice System. January, 2014
 Statistics on Women in the Justice System January, 2014 All material is available though the web site of the Bureau of Justice Statistics (BJS): http://www.bjs.gov/ unless otherwise cited. Note that correctional
Statistics on Women in the Justice System January, 2014 All material is available though the web site of the Bureau of Justice Statistics (BJS): http://www.bjs.gov/ unless otherwise cited. Note that correctional
DSM-V: DISRUPTIVE BEHAVIORS, PERSONALITY DISORDERS AND V-CODES
 DSM-V: DISRUPTIVE BEHAVIORS, PERSONALITY DISORDERS AND V-CODES STEPHEN SOLTYS, MD PROFESSOR AND CHAIRMAN DEPARTMENT OF PSYCHIATRY SOUTHERN ILLINOIS UNIVERSITY SCHOOL OF MEDICINE DISCLOSURES No conflicts
DSM-V: DISRUPTIVE BEHAVIORS, PERSONALITY DISORDERS AND V-CODES STEPHEN SOLTYS, MD PROFESSOR AND CHAIRMAN DEPARTMENT OF PSYCHIATRY SOUTHERN ILLINOIS UNIVERSITY SCHOOL OF MEDICINE DISCLOSURES No conflicts
Personality Disorders (PD) Summary (print version)
 Summary (print version)") Personality Disorders (PD) Summary (print version) 1/ Definition A Personality Disorder is an abnormal, extreme and persistent variation from the normal (statistical) range of one or more personality attributes
Personality Disorders (PD) Summary (print version) 1/ Definition A Personality Disorder is an abnormal, extreme and persistent variation from the normal (statistical) range of one or more personality attributes
TREATING ASPD IN THE COMMUNITY: FURTHERING THE PD OFFENDER STRATEGY. Jessica Yakeley Portman Clinic Tavistock and Portman NHS Foundation Trust
 TREATING ASPD IN THE COMMUNITY: FURTHERING THE PD OFFENDER STRATEGY Jessica Yakeley Portman Clinic Tavistock and Portman NHS Foundation Trust Treating the untreatable? Lack of evidence base for ASPD Only
TREATING ASPD IN THE COMMUNITY: FURTHERING THE PD OFFENDER STRATEGY Jessica Yakeley Portman Clinic Tavistock and Portman NHS Foundation Trust Treating the untreatable? Lack of evidence base for ASPD Only
Chapter 16 Mental Health Services: Legal & Ethical Issues
 Chapter 16 Mental Health Services: Legal & Ethical Issues Civil Commitment Civil Commitment Laws Detail when a person can be: Legally declared to have a mental illness + Placed in a hospital for treatment
Chapter 16 Mental Health Services: Legal & Ethical Issues Civil Commitment Civil Commitment Laws Detail when a person can be: Legally declared to have a mental illness + Placed in a hospital for treatment
Psychopathic Traits in a Large Community Sample: Links to Violence, Alcohol Use, and Intelligence. Craig S. Neumann. University of North Texas
 Psychopathic Traits in a Large Community Sample: Links to Violence, Alcohol Use, and Intelligence Craig S. Neumann University of North Texas & Robert D. Hare University of British Columbia Darkstone Research
Psychopathic Traits in a Large Community Sample: Links to Violence, Alcohol Use, and Intelligence Craig S. Neumann University of North Texas & Robert D. Hare University of British Columbia Darkstone Research
Cindy C. Cottle, Ph.D. 6500 Creedmoor Rd cindy.cottle@gmail.com Ste. 106 Phone: (919) 827-2148 Raleigh, N.C. 27613 Fax: (919) 882-1685
 827-2148 Raleigh, N.C. 27613 Fax: (919) 882-1685") Cindy C. Cottle, Ph.D. 6500 Creedmoor Rd cindy.cottle@gmail.com Ste. 106 Phone: (919) 827-2148 Raleigh, N.C. 27613 Fax: (919) 882-1685 Education 1998 2003 Drexel University Philadelphia, PA Ph.D., Clinical
Cindy C. Cottle, Ph.D. 6500 Creedmoor Rd cindy.cottle@gmail.com Ste. 106 Phone: (919) 827-2148 Raleigh, N.C. 27613 Fax: (919) 882-1685 Education 1998 2003 Drexel University Philadelphia, PA Ph.D., Clinical
A Review of Conduct Disorder. William U Borst. Troy State University at Phenix City
 A Review of 1 Running head: A REVIEW OF CONDUCT DISORDER A Review of Conduct Disorder William U Borst Troy State University at Phenix City A Review of 2 Abstract Conduct disorders are a complicated set
A Review of 1 Running head: A REVIEW OF CONDUCT DISORDER A Review of Conduct Disorder William U Borst Troy State University at Phenix City A Review of 2 Abstract Conduct disorders are a complicated set
Applied Psychology. Course Descriptions
 Applied Psychology s AP 6001 PRACTICUM SEMINAR I 1 CREDIT AP 6002 PRACTICUM SEMINAR II 3 CREDITS Prerequisites: AP 6001: Successful completion of core courses. Approval of practicum site by program coordinator.
Applied Psychology s AP 6001 PRACTICUM SEMINAR I 1 CREDIT AP 6002 PRACTICUM SEMINAR II 3 CREDITS Prerequisites: AP 6001: Successful completion of core courses. Approval of practicum site by program coordinator.
Assessment, Case Conceptualization, Diagnosis, and Treatment Planning Overview
 Assessment, Case Conceptualization, Diagnosis, and Treatment Planning Overview The abilities to gather and interpret information, apply counseling and developmental theories, understand diagnostic frameworks,
Assessment, Case Conceptualization, Diagnosis, and Treatment Planning Overview The abilities to gather and interpret information, apply counseling and developmental theories, understand diagnostic frameworks,
Abnormal Psychology PSY-350-TE
 Abnormal Psychology PSY-350-TE This TECEP tests the material usually taught in a one-semester course in abnormal psychology. It focuses on the causes of abnormality, the different forms of abnormal behavior,
Abnormal Psychology PSY-350-TE This TECEP tests the material usually taught in a one-semester course in abnormal psychology. It focuses on the causes of abnormality, the different forms of abnormal behavior,
Cindy C. Cottle, Ph.D. 5500 McNeely Dr. cindy.cottle@gmail.com Ste. 101 Phone: (919) 827-2148 Raleigh, N.C. 27612 Fax: (919) 882-1685
 827-2148 Raleigh, N.C. 27612 Fax: (919) 882-1685") Cindy C. Cottle, Ph.D. 5500 McNeely Dr. cindy.cottle@gmail.com Ste. 101 Phone: (919) 827-2148 Raleigh, N.C. 27612 Fax: (919) 882-1685 Education 1998 2003 Drexel University Philadelphia, PA Ph.D., Clinical
Cindy C. Cottle, Ph.D. 5500 McNeely Dr. cindy.cottle@gmail.com Ste. 101 Phone: (919) 827-2148 Raleigh, N.C. 27612 Fax: (919) 882-1685 Education 1998 2003 Drexel University Philadelphia, PA Ph.D., Clinical
Describing Ted Bundy s Personality and Working towards DSM-V. Douglas B. Samuel and Thomas A. Widiger. Department of Psychology
 Describing Ted Bundy s Personality 1 Describing Ted Bundy s Personality and Working towards DSM-V Douglas B. Samuel and Thomas A. Widiger Department of Psychology University of Kentucky Published in the
Describing Ted Bundy s Personality 1 Describing Ted Bundy s Personality and Working towards DSM-V Douglas B. Samuel and Thomas A. Widiger Department of Psychology University of Kentucky Published in the
A PROSPECTIVE EVALUATION OF THE RELATIONSHIP BETWEEN REASONS FOR DRINKING AND DSM-IV ALCOHOL-USE DISORDERS
 Pergamon Addictive Behaviors, Vol. 23, No. 1, pp. 41 46, 1998 Copyright 1998 Elsevier Science Ltd Printed in the USA. All rights reserved 0306-4603/98 $19.00.00 PII S0306-4603(97)00015-4 A PROSPECTIVE
Pergamon Addictive Behaviors, Vol. 23, No. 1, pp. 41 46, 1998 Copyright 1998 Elsevier Science Ltd Printed in the USA. All rights reserved 0306-4603/98 $19.00.00 PII S0306-4603(97)00015-4 A PROSPECTIVE
Treatment of DUI s A Swedish Evaluation Study
 Treatment of DUI s A Swedish Evaluation Study 1 A. Andrén, 1 H. Bergman and 2 F. Schlyter, 3 H. Laurell 1 Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden, 2 Swedish Prison
Treatment of DUI s A Swedish Evaluation Study 1 A. Andrén, 1 H. Bergman and 2 F. Schlyter, 3 H. Laurell 1 Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden, 2 Swedish Prison
Personality Disorders
 Abnormal Psychology PSYCH 40111 s s: An Overview The Nature of Personality and s A personality is all the ways we have of acting, thinking, believing, and feeling that make each of us unique and different
Abnormal Psychology PSYCH 40111 s s: An Overview The Nature of Personality and s A personality is all the ways we have of acting, thinking, believing, and feeling that make each of us unique and different
Introduction to the DSM-IV and Psychological Testing
 Introduction to the DSM-IV and Psychological Testing Significance of Mental Illness In any given year, how many Americans will suffer with a diagnosable mental illness? How many will suffer with a serious
Introduction to the DSM-IV and Psychological Testing Significance of Mental Illness In any given year, how many Americans will suffer with a diagnosable mental illness? How many will suffer with a serious
[KQ 804] FEBRUARY 2007 Sub. Code: 9105
![[KQ 804] FEBRUARY 2007 Sub. Code: 9105](/thumbs/26/8053833.jpg "[KQ 804] FEBRUARY 2007 Sub. Code: 9105") [KQ 804] FEBRUARY 2007 Sub. Code: 9105 (Revised Regulations) Theory : Two hours and forty minutes Q.P. Code: 419105 Maximum : 100 marks Theory : 80 marks M.C.Q. : Twenty minutes M.C.Q. : 20 marks 1. A
[KQ 804] FEBRUARY 2007 Sub. Code: 9105 (Revised Regulations) Theory : Two hours and forty minutes Q.P. Code: 419105 Maximum : 100 marks Theory : 80 marks M.C.Q. : Twenty minutes M.C.Q. : 20 marks 1. A
offenders had more classically criminal personality characteristics
 AMERICAN JOURNAL OF FORENSIC PSYCHOLOGY, VOLUME 28, ISSUE 3, 2010 / 1 PERSONALITY DISORDER PROFILES IN INCARCERATED MALE RAPISTS AND CHILD MOLESTERS Charlotte A. Francia, Frederick L. Coolidge, Ph.D.,
AMERICAN JOURNAL OF FORENSIC PSYCHOLOGY, VOLUME 28, ISSUE 3, 2010 / 1 PERSONALITY DISORDER PROFILES IN INCARCERATED MALE RAPISTS AND CHILD MOLESTERS Charlotte A. Francia, Frederick L. Coolidge, Ph.D.,
Child Pornography Offender Characteristics and Risk to Reoffend. Michael C. Seto, Ph.D., C.Psych. Royal Ottawa Health Care Group
 Seto 1 Child Pornography Offender Characteristics and Risk to Reoffend Michael C. Seto, Ph.D., C.Psych. Royal Ottawa Health Care Group Prepared for the United States Sentencing Commission Draft dated February
Seto 1 Child Pornography Offender Characteristics and Risk to Reoffend Michael C. Seto, Ph.D., C.Psych. Royal Ottawa Health Care Group Prepared for the United States Sentencing Commission Draft dated February
Chapter 12 Personality Disorders
 The Nature of Personality Disorders Chapter 12 Personality Disorders Enduring patterns of perceiving, relating to, and thinking about the world and oneself Manifest across many life areas Are inflexible
The Nature of Personality Disorders Chapter 12 Personality Disorders Enduring patterns of perceiving, relating to, and thinking about the world and oneself Manifest across many life areas Are inflexible
The Goal of Correctional Counseling
 41140_CH03_Pass2.qxd 8/9/07 12:21 PM Page 45 Jones and Bartlett Publishers. NOT FOR SALE OR DISTRIBUTION The Goal of Correctional Counseling 3 The goal of correctional counseling is usually based on two
41140_CH03_Pass2.qxd 8/9/07 12:21 PM Page 45 Jones and Bartlett Publishers. NOT FOR SALE OR DISTRIBUTION The Goal of Correctional Counseling 3 The goal of correctional counseling is usually based on two
Rachel A. Klein, Psy.D Licensed Clinical Psychologist (610) 368-4041 rachel.klein81@gmail.com
 368-4041 rachel.klein81@gmail.com") Rachel A. Klein, Psy.D Licensed Clinical Psychologist (610) 368-4041 rachel.klein81@gmail.com EDUCATION Widener University, Institute of Graduate Clinical Psychology, Doctor of Psychology, 5/2012 Widener
Rachel A. Klein, Psy.D Licensed Clinical Psychologist (610) 368-4041 rachel.klein81@gmail.com EDUCATION Widener University, Institute of Graduate Clinical Psychology, Doctor of Psychology, 5/2012 Widener
Department of Psychology
 Colorado State University 1 Department of Psychology Office in Behavioral Sciences Building, Room 201 (970) 491-3799 colostate.edu/depts/psychology (http://www.colostate.edu/depts/ Psychology) Professor
Colorado State University 1 Department of Psychology Office in Behavioral Sciences Building, Room 201 (970) 491-3799 colostate.edu/depts/psychology (http://www.colostate.edu/depts/ Psychology) Professor
MENTAL IMPAIRMENT RATING
 MENTAL IMPAIRMENT RATING Lev.II Curriculum Rev. 6/09 155 OBJECTIVES MENTAL AND BEHAVIORAL DISORDERS 1. Identify the axes used in the diagnostic and statistical manual of mental disorders - DSM. 2. Understand
MENTAL IMPAIRMENT RATING Lev.II Curriculum Rev. 6/09 155 OBJECTIVES MENTAL AND BEHAVIORAL DISORDERS 1. Identify the axes used in the diagnostic and statistical manual of mental disorders - DSM. 2. Understand
Personality Disorders
 Personality s The Good, the Bad and the Really, Really Ugly: Borderline and other Cluster B Personality s BY CHRIS OKIISHI, MD! Long standing! Often life long! Developmental origins! Genetic origins! Resistant
Personality s The Good, the Bad and the Really, Really Ugly: Borderline and other Cluster B Personality s BY CHRIS OKIISHI, MD! Long standing! Often life long! Developmental origins! Genetic origins! Resistant
APPIC APPLICATION Summary of Practicum Experiences
 APPIC APPLICATION Summary of Practicum Experiences 1. Intervention Experience How much experience do you have with different types of psychological interventions? NOTE: Remember that hours accrued while
APPIC APPLICATION Summary of Practicum Experiences 1. Intervention Experience How much experience do you have with different types of psychological interventions? NOTE: Remember that hours accrued while
Rehabilitation programs for young offenders: Towards good practice? Andrew Day. Forensic Psychology Research Group. University of South Australia
 1 Rehabilitation programs for young offenders: Towards good practice? Andrew Day Forensic Psychology Research Group University of South Australia Andrew.day@unisa.edu.au Invited paper for the Understanding
1 Rehabilitation programs for young offenders: Towards good practice? Andrew Day Forensic Psychology Research Group University of South Australia Andrew.day@unisa.edu.au Invited paper for the Understanding
DSM-5: A Comprehensive Overview
 1) The original DSM was published in a) 1942 b) 1952 c) 1962 d) 1972 DSM-5: A Comprehensive Overview 2) The DSM provides all the following EXCEPT a) Guidelines for the treatment of identified disorders
1) The original DSM was published in a) 1942 b) 1952 c) 1962 d) 1972 DSM-5: A Comprehensive Overview 2) The DSM provides all the following EXCEPT a) Guidelines for the treatment of identified disorders
Evidence Based Correctional Practices
 Evidence Based Correctional Practices What works in corrections is not a program or a single intervention but rather a body of knowledge that is accessible to criminal justice professionals. 1 The National
Evidence Based Correctional Practices What works in corrections is not a program or a single intervention but rather a body of knowledge that is accessible to criminal justice professionals. 1 The National
Psychological Correlates of Substance Abuse among First-admission. Patients with Substance Use Disorders
 The International Journal of Indian Psychology ISSN 2348-5396 (e) ISSN: 2349-3429 (p) Volume 3, Issue 1, DIP: C00226V3I12015 http://www.ijip.in October December, 2015 Psychological Correlates of Substance
The International Journal of Indian Psychology ISSN 2348-5396 (e) ISSN: 2349-3429 (p) Volume 3, Issue 1, DIP: C00226V3I12015 http://www.ijip.in October December, 2015 Psychological Correlates of Substance
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)
") The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) Cardwell C Nuckols, PhD cnuckols@elitecorp1.com Cardwell C. Nuckols, PhD www.cnuckols.com SECTION I-BASICS DSM-5 Includes
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) Cardwell C Nuckols, PhD cnuckols@elitecorp1.com Cardwell C. Nuckols, PhD www.cnuckols.com SECTION I-BASICS DSM-5 Includes
Co-Occurring Substance Use and Mental Health Disorders. Joy Chudzynski, PsyD UCLA Integrated Substance Abuse Programs
 Co-Occurring Substance Use and Mental Health Disorders Joy Chudzynski, PsyD UCLA Integrated Substance Abuse Programs Introduction Overview of the evolving field of Co-Occurring Disorders Addiction and
Co-Occurring Substance Use and Mental Health Disorders Joy Chudzynski, PsyD UCLA Integrated Substance Abuse Programs Introduction Overview of the evolving field of Co-Occurring Disorders Addiction and
STANDARDS FOR FORENSIC PSYCHOLOGICAL EVALUATIONS OF ADULT SEXUAL OFFENDERS
 STANDARDS FOR FORENSIC PSYCHOLOGICAL EVALUATIONS OF ADULT SEXUAL OFFENDERS Approved on March 24, 2003 by: The San Diego County Sex Offender Management Council Submitted by the Legal Process Subcommittee
STANDARDS FOR FORENSIC PSYCHOLOGICAL EVALUATIONS OF ADULT SEXUAL OFFENDERS Approved on March 24, 2003 by: The San Diego County Sex Offender Management Council Submitted by the Legal Process Subcommittee
VISITING EXPERTS PAPERS
 139TH INTERNATIONAL TRAINING COURSE ISSUES IN THE ASSESSMENT OF JUVENILE OFFENDERS Robert D. Hoge* I. INTRODUCTION The assessment process involves the collection, processing, and synthesis of information
139TH INTERNATIONAL TRAINING COURSE ISSUES IN THE ASSESSMENT OF JUVENILE OFFENDERS Robert D. Hoge* I. INTRODUCTION The assessment process involves the collection, processing, and synthesis of information
Overview of Domestic Violence (DV) Risk Assessment Instruments (Frequently Asked Questions) Kristin Bechtel and Bill Woodward
 Risk Assessment Instruments (Frequently Asked Questions) Kristin Bechtel and Bill Woodward") The author(s) shown below used Federal funds provided by the U.S. Department of Justice, National Institute of Corrections (NIC) and prepared the following final report: Document Title: Author: Overview
The author(s) shown below used Federal funds provided by the U.S. Department of Justice, National Institute of Corrections (NIC) and prepared the following final report: Document Title: Author: Overview
CAGE. AUDIT-C and the Full AUDIT
 CAGE In the past have you ever: C tried to Cut down or Change your pattern of drinking or drug use? A been Annoyed or Angry because of others concern about your drinking or drug use? G felt Guilty about
CAGE In the past have you ever: C tried to Cut down or Change your pattern of drinking or drug use? A been Annoyed or Angry because of others concern about your drinking or drug use? G felt Guilty about
WESTERN UNIVERSITY LONDON CANADA Department of Psychology 2013-2014
 WESTERN UNIVERSITY LONDON CANADA Department of Psychology 2013-2014 Psychology 3314G Section 001 Forensic Psychology Psychology 3314G Course Syllabus 1 1.0 CALENDAR DESCRIPTION This course introduces students
WESTERN UNIVERSITY LONDON CANADA Department of Psychology 2013-2014 Psychology 3314G Section 001 Forensic Psychology Psychology 3314G Course Syllabus 1 1.0 CALENDAR DESCRIPTION This course introduces students
Criminal Justice - Law Enforcement
 Criminal Justice - Law Enforcement Dr. Charles Adair, Acting Chair Criminal Justice Department adaircn@farmingdale.edu 631-420-2692 School of Arts & Sciences Associate in Science Degree The goal of this
Criminal Justice - Law Enforcement Dr. Charles Adair, Acting Chair Criminal Justice Department adaircn@farmingdale.edu 631-420-2692 School of Arts & Sciences Associate in Science Degree The goal of this
C. Chyrelle Martin, Psy.D
 C. Chyrelle Martin, Psy.D Licensed Clinical and Forensic Psychologist OPAL Institute Oregon Passionate Aging and Living 14780 SW Osprey Dr. #285 Beaverton, OR 97007 Clinical and Forensic Experience Licensed
C. Chyrelle Martin, Psy.D Licensed Clinical and Forensic Psychologist OPAL Institute Oregon Passionate Aging and Living 14780 SW Osprey Dr. #285 Beaverton, OR 97007 Clinical and Forensic Experience Licensed
CORRELATES AND COSTS
 ANOTHER LOOK AT MENTAL ILLNESS AND CRIMINAL JUSTICE INVOLVEMENT IN TEXAS: CORRELATES AND COSTS Decision Support Unit Mental Health and Substance Abuse Services Another Look at Mental Illness and Criminal
ANOTHER LOOK AT MENTAL ILLNESS AND CRIMINAL JUSTICE INVOLVEMENT IN TEXAS: CORRELATES AND COSTS Decision Support Unit Mental Health and Substance Abuse Services Another Look at Mental Illness and Criminal
How To Find Out How Different Groups Of People Are Different
 Determinants of Alcohol Abuse in a Psychiatric Population: A Two-Dimensionl Model John E. Overall The University of Texas Medical School at Houston A method for multidimensional scaling of group differences
Determinants of Alcohol Abuse in a Psychiatric Population: A Two-Dimensionl Model John E. Overall The University of Texas Medical School at Houston A method for multidimensional scaling of group differences
PSYC PSYCHOLOGY. 2011-2012 Calendar Proof
 PSYC PSYCHOLOGY PSYC1003 is a prerequisite for PSYC1004 and PSYC1004 is a prerequisite for all remaining Psychology courses. Note: See beginning of Section F for abbreviations, course numbers and coding.
PSYC PSYCHOLOGY PSYC1003 is a prerequisite for PSYC1004 and PSYC1004 is a prerequisite for all remaining Psychology courses. Note: See beginning of Section F for abbreviations, course numbers and coding.
Con-Quest Residential Substance Abuse Treatment Program Outcome Evaluation. February 2004
 Residential Substance Abuse Treatment Program Outcome Evaluation February 2004 Introduction The link between drugs and crime in the United States is widely accepted. Drug users frequently commit crime
Residential Substance Abuse Treatment Program Outcome Evaluation February 2004 Introduction The link between drugs and crime in the United States is widely accepted. Drug users frequently commit crime
Metropolitan Detention Center (MDC) DWI Addiction Treatment Programs (ATP) Outcome Study for DWI Offenders
 DWI Addiction Treatment Programs (ATP) Outcome Study for DWI Offenders") Metropolitan Detention Center (MDC) DWI Addiction Treatment Programs (ATP) Outcome Study for DWI Offenders Prepared for: The DWI Addiction Treatment Programs (ATP) Metropolitan Detention Center Prepared
Metropolitan Detention Center (MDC) DWI Addiction Treatment Programs (ATP) Outcome Study for DWI Offenders Prepared for: The DWI Addiction Treatment Programs (ATP) Metropolitan Detention Center Prepared
Suicide Assessment in the Elderly Geriatric Psychiatric for the Primary Care Provider 2008
 Suicide Assessment in the Elderly Geriatric Psychiatric for the Primary Care Provider 2008 Lisa M. Brown, Ph.D. Aging and Mental Health Louis de la Parte Florida Mental Health Institute University of South
Suicide Assessment in the Elderly Geriatric Psychiatric for the Primary Care Provider 2008 Lisa M. Brown, Ph.D. Aging and Mental Health Louis de la Parte Florida Mental Health Institute University of South
Understanding 5 High Conflict Personality Disorders
 Understanding 5 High Conflict Personality Disorders Bill Eddy, LCSW, Esq. Attorney, Mediator, Therapist, Author Family Law Institute March 19, 2013 - Minneapolis Copyright 2013 High Conflict Institute
Understanding 5 High Conflict Personality Disorders Bill Eddy, LCSW, Esq. Attorney, Mediator, Therapist, Author Family Law Institute March 19, 2013 - Minneapolis Copyright 2013 High Conflict Institute
ANTISOCIAL PERSONALITY DISORDER: IS IT TREATABLE? JESSICA YAKELEY PORTMAN CLINIC TAVISTOCK AND PORTMAN NHS FOUNDATION TRUST
 ANTISOCIAL PERSONALITY DISORDER: IS IT TREATABLE? JESSICA YAKELEY PORTMAN CLINIC TAVISTOCK AND PORTMAN NHS FOUNDATION TRUST ANTISOCIAL PERSONALITY DISORDER: IS IT TREATABLE? Why care about ASPD? Why care
ANTISOCIAL PERSONALITY DISORDER: IS IT TREATABLE? JESSICA YAKELEY PORTMAN CLINIC TAVISTOCK AND PORTMAN NHS FOUNDATION TRUST ANTISOCIAL PERSONALITY DISORDER: IS IT TREATABLE? Why care about ASPD? Why care
University of Michigan Dearborn Graduate Psychology Assessment Program
 University of Michigan Dearborn Graduate Psychology Assessment Program Graduate Clinical Health Psychology Program Goals 1 Psychotherapy Skills Acquisition: To train students in the skills and knowledge
University of Michigan Dearborn Graduate Psychology Assessment Program Graduate Clinical Health Psychology Program Goals 1 Psychotherapy Skills Acquisition: To train students in the skills and knowledge
Guidelines for Documentation of a A. Learning Disability
 Guidelines for Documentation of a Learning Disability A. Learning Disability B. Attention Deficit Disorder C. Psychiatric Disabilities D. Chronic Health Disabilities A. Learning Disability Students who
Guidelines for Documentation of a Learning Disability A. Learning Disability B. Attention Deficit Disorder C. Psychiatric Disabilities D. Chronic Health Disabilities A. Learning Disability Students who
Mental Health Fact Sheet
 Mental Health Fact Sheet Substance Abuse and Treatment Branch (SATB), Community Supervision Services Re-Entry and Sanctions Center (RSC), Office of Community Justice Programs Adult Probationers / Parolees
Mental Health Fact Sheet Substance Abuse and Treatment Branch (SATB), Community Supervision Services Re-Entry and Sanctions Center (RSC), Office of Community Justice Programs Adult Probationers / Parolees
DSM-5 and its use by chemical dependency professionals
 + DSM-5 and its use by chemical dependency professionals Greg Bauer Executive Director Alpine Recovery Services Inc. President Chemical Dependency Professionals Washington State (CDPWS) NAADAC 2014 Annual
+ DSM-5 and its use by chemical dependency professionals Greg Bauer Executive Director Alpine Recovery Services Inc. President Chemical Dependency Professionals Washington State (CDPWS) NAADAC 2014 Annual
Professors Ellen Dwyer* (History), Roger J. R. Levesque, Harold E. Pepinsky*, Leon E. Pettiway*, Hilliard Trubitt* (Emeritus)
, Roger J. R. Levesque, Harold E. Pepinsky*, Leon E. Pettiway*, Hilliard Trubitt* (Emeritus)") University Graduate School 2005-2006 Academic Bulletin Criminal Justice University Graduate School Kirkwood Hall 111 Indiana University Bloomington, IN 47405 (812) 855-8853 Contact: grdschl@indiana.edu
University Graduate School 2005-2006 Academic Bulletin Criminal Justice University Graduate School Kirkwood Hall 111 Indiana University Bloomington, IN 47405 (812) 855-8853 Contact: grdschl@indiana.edu
Pragmatic Evidence Based Review Substance Abuse in moderate to severe TBI
 Pragmatic Evidence Based Review Substance Abuse in moderate to severe TBI Reviewer Emma Scheib Date Report Completed November 2011 Important Note: This report is not intended to replace clinical judgement,
Pragmatic Evidence Based Review Substance Abuse in moderate to severe TBI Reviewer Emma Scheib Date Report Completed November 2011 Important Note: This report is not intended to replace clinical judgement,
Current Issues in Forensic Psychology Stephen F. Austin State University
 Current Issues in Forensic Psychology Stephen F. Austin State University PSY 498.001 MWF 11:00-11:50 McKibben Education Building: Room 269 Instructor: Sylvia Middlebrook, Ph.D., BCBA-D Office: McKibben
Current Issues in Forensic Psychology Stephen F. Austin State University PSY 498.001 MWF 11:00-11:50 McKibben Education Building: Room 269 Instructor: Sylvia Middlebrook, Ph.D., BCBA-D Office: McKibben
COURSE DESCRIPTIONS 2014-2015
 COURSE DESCRIPTIONS 2014-2015 Course Definitions, Designators and Format Courses approved at the time of publication are listed in this bulletin. Not all courses are offered every term. Refer to the online
COURSE DESCRIPTIONS 2014-2015 Course Definitions, Designators and Format Courses approved at the time of publication are listed in this bulletin. Not all courses are offered every term. Refer to the online
DR. ALEKS MILOSEVIC, C.PSYCH. CLINICAL & FORENSIC PSYCHOLOGIST
 DR. ALEKS MILOSEVIC, C.PSYCH. CLINICAL & FORENSIC PSYCHOLOGIST 1804 Highway 2 East, Brockville, ON, KGV 5W7 388 Albert Street, Unit 2, Ottawa, ON, K1R 5B2 (613) 345-1461, ext. 2647 (613) 680-2079 aleksandar.milosevic@theroyal.ca
DR. ALEKS MILOSEVIC, C.PSYCH. CLINICAL & FORENSIC PSYCHOLOGIST 1804 Highway 2 East, Brockville, ON, KGV 5W7 388 Albert Street, Unit 2, Ottawa, ON, K1R 5B2 (613) 345-1461, ext. 2647 (613) 680-2079 aleksandar.milosevic@theroyal.ca
PREDICTORS OF NON-EPILEPTIC SEIZURES IN AN INPATIENT EPILEPSY PROGRAM
 PREDICTORS OF NON-EPILEPTIC SEIZURES IN AN INPATIENT EPILEPSY PROGRAM Robert C. Doss, PsyD John R. Gates, M.D This paper has been prepared specifically for: American Epilepsy Society Annual Meeting Philadelphia,
PREDICTORS OF NON-EPILEPTIC SEIZURES IN AN INPATIENT EPILEPSY PROGRAM Robert C. Doss, PsyD John R. Gates, M.D This paper has been prepared specifically for: American Epilepsy Society Annual Meeting Philadelphia,
Advanced Abnormal Psychology (PSY 46000-01) CRN 12239 Fall Semester 2015 Dr. David Young, Professor of Psychology. Course Syllabus
 CRN 12239 Fall Semester 2015 Dr. David Young, Professor of Psychology. Course Syllabus") Advanced Abnormal Psychology (PSY 46000-01) CRN 12239 Fall Semester 2015 Dr. David Young, Professor of Psychology Course Syllabus (Presentation Rubric) Monday, Wednesday, Friday, 10-10:50 a.m. Office:
Advanced Abnormal Psychology (PSY 46000-01) CRN 12239 Fall Semester 2015 Dr. David Young, Professor of Psychology Course Syllabus (Presentation Rubric) Monday, Wednesday, Friday, 10-10:50 a.m. Office:
HEALTH LICENSING OFFICE Sex Offender Treatment Board
 BOARD APPROVED BEHAVIORAL SCIENCE DEGREES The Sex Offender Treatment Board met on March 6, 2015 and approved Behavioral Science degrees to include, but not limited to, the following: MULTI/INTERDISCIPLINARY
BOARD APPROVED BEHAVIORAL SCIENCE DEGREES The Sex Offender Treatment Board met on March 6, 2015 and approved Behavioral Science degrees to include, but not limited to, the following: MULTI/INTERDISCIPLINARY
ANTISOCIAL PERSONALITY DISORDER BY: MACKENZIE
 ANTISOCIAL PERSONALITY DISORDER BY: MACKENZIE RESEARCH QUESTIONS Main: What is antisocial personality disorder? What are the symptoms of antisocial personality disorder? What are some everyday complications
ANTISOCIAL PERSONALITY DISORDER BY: MACKENZIE RESEARCH QUESTIONS Main: What is antisocial personality disorder? What are the symptoms of antisocial personality disorder? What are some everyday complications
DESCRIPTION OF FORENSIC POPULATION
 SERVICES FOR FORENSIC CLIENTS GENERAL LEGAL RIGHTS CHAPTER 13 DESCRIPTION OF FORENSIC POPULATION The forensic program for the State of Missouri is designed to provide services to all circuit courtordered
SERVICES FOR FORENSIC CLIENTS GENERAL LEGAL RIGHTS CHAPTER 13 DESCRIPTION OF FORENSIC POPULATION The forensic program for the State of Missouri is designed to provide services to all circuit courtordered
What is Domestic Violence?
 Reentry in the State of Connecticut: Partners in Progress February 24-26, 2009 Rachelle Giguere and Becki Ney What is Domestic Violence? The Centers for Disease Control (CDC) defines intimate partner violence
Reentry in the State of Connecticut: Partners in Progress February 24-26, 2009 Rachelle Giguere and Becki Ney What is Domestic Violence? The Centers for Disease Control (CDC) defines intimate partner violence
Master of Arts, Counseling Psychology Course Descriptions
 Master of Arts, Counseling Psychology Course Descriptions Advanced Theories of Counseling & Intervention (3 credits) This course addresses the theoretical approaches used in counseling, therapy and intervention.
Master of Arts, Counseling Psychology Course Descriptions Advanced Theories of Counseling & Intervention (3 credits) This course addresses the theoretical approaches used in counseling, therapy and intervention.
Influenced by - Alfred Binet intelligence testing movement
 SA1 Trait Psychology Influenced by - Alfred Binet intelligence testing movement Origins - Psychologists became interested in seeing whether the success achieved with mental measurement might be repeated
SA1 Trait Psychology Influenced by - Alfred Binet intelligence testing movement Origins - Psychologists became interested in seeing whether the success achieved with mental measurement might be repeated
HOW TO ASSESS AND COMPENSATE PSYCHIATRIC INJURIES IN THE WORKPLACE Grace Lawson 1
 1 HOW TO ASSESS AND COMPENSATE PSYCHIATRIC INJURIES IN THE WORKPLACE Grace Lawson 1 Introduction Mental illness has become a major health problem in Australia. Work-related mental injuries have also become
1 HOW TO ASSESS AND COMPENSATE PSYCHIATRIC INJURIES IN THE WORKPLACE Grace Lawson 1 Introduction Mental illness has become a major health problem in Australia. Work-related mental injuries have also become
Running head: SAMPLE FOR STUDENTS 1. Sample APA Paper for Students Interested in Learning APA Style 6th Edition. Jeffrey H. Kahn
 Running head: SAMPLE FOR STUDENTS 1 Sample APA Paper for Students Interested in Learning APA Style 6th Edition Jeffrey H. Kahn Illinois State University Author Note Jeffrey H. Kahn, Department of Psychology,
Running head: SAMPLE FOR STUDENTS 1 Sample APA Paper for Students Interested in Learning APA Style 6th Edition Jeffrey H. Kahn Illinois State University Author Note Jeffrey H. Kahn, Department of Psychology,
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Curriculum Vitae. University at Buffalo, The State University of New York Psychology (major); Sociology (minor)
; Sociology (minor)") Curriculum Vitae License #36024 The Physician s Centre 3131 University Drive East Bryan, TX 77802 (979) 450-5320 drjenniferrockett@tsecuremail.com www.drrockett.org Education Ph.D. (2009) M.A. (2005) B.A.
Curriculum Vitae License #36024 The Physician s Centre 3131 University Drive East Bryan, TX 77802 (979) 450-5320 drjenniferrockett@tsecuremail.com www.drrockett.org Education Ph.D. (2009) M.A. (2005) B.A.
EDUCATION WORKSHOP SEXUAL BEHAVIOURS CLINIC November 20 th & 21 st, 2014
 EDUCATION WORKSHOP SEXUAL BEHAVIOURS CLINIC November 20 th & 21 st, 2014 DAY 1 Ms. Stephanie Swayne, MSW, RSW Social Worker, Sexual Behavious Clinic, CAMH Detective Paul Krawczyk, Sex Crimes Child - Exploitation
EDUCATION WORKSHOP SEXUAL BEHAVIOURS CLINIC November 20 th & 21 st, 2014 DAY 1 Ms. Stephanie Swayne, MSW, RSW Social Worker, Sexual Behavious Clinic, CAMH Detective Paul Krawczyk, Sex Crimes Child - Exploitation
Long-term Impact Evaluation of Specialized Sex Offender Probation Programs In Lake, DuPage and Winnebago Counties
 Long-term Impact Evaluation of Specialized Sex Offender Probation Programs In Lake, DuPage and Winnebago Counties Prepared for the The Illinois Criminal Justice Information Authority By: Loretta J. Stalans,
Long-term Impact Evaluation of Specialized Sex Offender Probation Programs In Lake, DuPage and Winnebago Counties Prepared for the The Illinois Criminal Justice Information Authority By: Loretta J. Stalans,
Association of Marital and Family Therapy Regulatory Boards (AMFTRB) Evaluating Ongoing Process and Terminating Treatment (7.5%)
 Evaluating Ongoing Process and Terminating Treatment (7.5%)") Association of Marital and Family Therapy Regulatory Boards (AMFTRB) Test Specifications for the Examination in Marital and Family Therapy Practice s 01 The Practice of Marital and Family Therapy (22.5%)
Association of Marital and Family Therapy Regulatory Boards (AMFTRB) Test Specifications for the Examination in Marital and Family Therapy Practice s 01 The Practice of Marital and Family Therapy (22.5%)
Frequently Asked Questions (FAQs) of Drug Abuse Treatment for Criminal Justice Populations
 of Drug Abuse Treatment for Criminal Justice Populations") Frequently Asked Questions (FAQs) of Drug Abuse Treatment for Criminal Justice Populations From The National Institute on Drug Abuse (NIDA) 2. Why should drug abuse treatment be provided to offenders?
Frequently Asked Questions (FAQs) of Drug Abuse Treatment for Criminal Justice Populations From The National Institute on Drug Abuse (NIDA) 2. Why should drug abuse treatment be provided to offenders?
PSYCHOLOGICAL AND NEUROPSYCHOLOGICAL TESTING
 Status Active Medical and Behavioral Health Policy Section: Behavioral Health Policy Number: X-45 Effective Date: 01/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
Status Active Medical and Behavioral Health Policy Section: Behavioral Health Policy Number: X-45 Effective Date: 01/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
Comparison of External Correlates of MMPI Substance Abuse Scales Across Sex and Race
 Journal of Consulting and Qinical Psychology 985, Vol. 53, No. 4, 5-55 Copyright 985 by the American Psychological Association, Inc. -6X/85/S.75 Comparison of External Correlates of MMPI Substance Abuse
Journal of Consulting and Qinical Psychology 985, Vol. 53, No. 4, 5-55 Copyright 985 by the American Psychological Association, Inc. -6X/85/S.75 Comparison of External Correlates of MMPI Substance Abuse
Requirements. Elective Courses (minimum 9 cr.) Psychology Major. Capstone Sequence (14 cr.) Required Courses (21 cr.)
 Psychology Major. Capstone Sequence (14 cr.) Required Courses (21 cr.)") PSYCHOLOGY, B.A. Requirements Total minimum number of credits required for a major in leading to the B.A. degree 120. Total minimum number of credits for a minor in psychology 18. Total minimum number
PSYCHOLOGY, B.A. Requirements Total minimum number of credits required for a major in leading to the B.A. degree 120. Total minimum number of credits for a minor in psychology 18. Total minimum number
GENDER-RESPONSIVE ASSESSMENT AND TREATMENT FOR JUSTICE-INVOLVED WOMEN IN COMMUNITY SUPERVISION
 GENDER-RESPONSIVE ASSESSMENT AND TREATMENT FOR JUSTICE-INVOLVED WOMEN IN COMMUNITY SUPERVISION Krista Gehring, Ph.D. Assistant Professor Department of Criminal Justice University of Houston-Downtown January
GENDER-RESPONSIVE ASSESSMENT AND TREATMENT FOR JUSTICE-INVOLVED WOMEN IN COMMUNITY SUPERVISION Krista Gehring, Ph.D. Assistant Professor Department of Criminal Justice University of Houston-Downtown January
Personality Difficulties
 Personality Difficulties The essential features of a personality disorder are impairments in personality (self and interpersonal) functioning and the presence of pathological personality traits. There
Personality Difficulties The essential features of a personality disorder are impairments in personality (self and interpersonal) functioning and the presence of pathological personality traits. There
A Conceptual Framework for Co- Occurring Disorders within a Behavioral Health Care System
 A Conceptual Framework for Co- Occurring Disorders within a Behavioral Health Care System Reference: National Dialogue on Co-occurring Mental Health and Substance Abuse Disorder, June 16-17, 1998, Washington,
A Conceptual Framework for Co- Occurring Disorders within a Behavioral Health Care System Reference: National Dialogue on Co-occurring Mental Health and Substance Abuse Disorder, June 16-17, 1998, Washington,
Psychology 3314G Course Syllabus 1 Dr. Peter Hoaken
 1.0 CALENDAR DESCRIPTION THE UNIVERSITY OF WESTERN ONTARIO LONDON CANADA Department of Psychology 2012-2013 Psychology 3314G (formerly 368G & 3390G) Section 001 Forensic Psychology Psychology 3314G Course
1.0 CALENDAR DESCRIPTION THE UNIVERSITY OF WESTERN ONTARIO LONDON CANADA Department of Psychology 2012-2013 Psychology 3314G (formerly 368G & 3390G) Section 001 Forensic Psychology Psychology 3314G Course