Rise and fall of an evidence based practice: Assertive Community Treatment, a case study in Indiana. John McGrew, Ph.D.
|
|
|
- Ethel Curtis
- 8 years ago
- Views:
Transcription


1 Rise and fall of an evidence based practice: Assertive Community Treatment, a case study in Indiana John McGrew, Ph.D. Psychology IUPUI

2 What is Assertive Community Treatment?

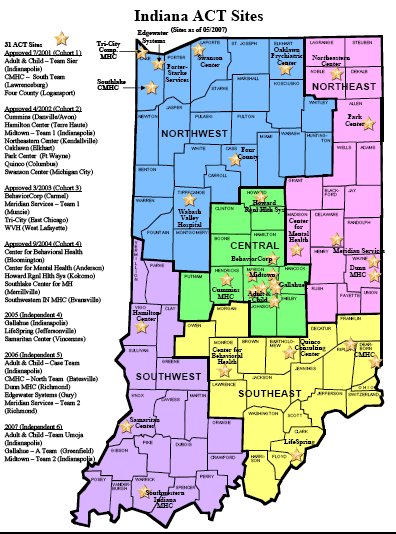
3 ACT History Developed during 1970s in Madison, WI Targeted revolving door client Hospital without Walls 1974, received American Psychiatric Association prestigious Gold Award Over 25 RCTs experimentally demonstrating effectiveness By 2003, implemented in 41 states (NAMI survey) Stein LI, Test MA: Alternative to mental hospital treatment: I. conceptual model, treatment program, and clinical evaluation. Archives of General Psychiatry 37: , 1980 Dixon, L. (2000). Assertive community treatment: Twenty-five years of gold. Psychiatric Services, 51,
. Assertive community treatment: Twenty-five years of gold.")
4 ACT basic elements Multidisciplinary staffing Team approach Integrated services Direct service provider (not brokering) Low client-staff ratios (10:1) More than 75% of contacts in the community Assertive outreach Focus on symptom management and everyday problems in living Ready access in times of crisis Time-unlimited services

5 ACT is reserved for the most severe clients with SMI Frequent psychiatric admissions Frequent use of emergency rooms Homeless or unstable housing Treatment nonadherence Dual diagnosis (SMI + substance abuse) Legal problems Discharge from long-term hospital
 Legal problems Discharge from long-term")
6 ACT attempts to provide comprehensive services Daily activities Housing Work Family/social life Entitlements Financial management Integrated treatment for substance abuse Counseling Medication support Health

7 ACT team is multi-disciplinary Psychiatrist Team Leader Nurse Mental Health Professionals/CMs Therapist/Social Worker/Psychologist Specialist team members Addiction Specialist (sometimes) Employment Specialist (sometimes) Peer Recovery Specialist (infrequently) Administrative Help
 Peer Recovery Specialist (infrequently)")
8 ACT has a strong evidence base Table 1. Comparison of ACT to Controls in 25 RCTs ACT Compared to Controls Better No Diff. Worse Hospital use 17 (74%) 6 (26%) 0 Housing stability 8 (67%) 3 (25%) 1 (8%) Symptoms 7 (44%) 9 (56%) 0 Quality of life 7 (58%) 5 (42%) 0 *Source: Bond, GR, Drake, RE, Mueser, KT, & Latimer, E. (2001). Assertive Community Treatment for People with Severe Mental Illness. Dis Manage Health Outcomes, 9:
 5 (42%) 0 *Source: Bond, GR, Drake, RE, Mueser, KT, & Latimer, E. (2001).")
9 Conclusions About ACT Effectiveness Large impact on: Hospital use Housing Retention in treatment Moderate impact on: Symptoms Quality of life Evidence weak for: Employment Substance use Jail and legal problems Social adjustment

10 Current Status : ACT is Evidence-Based Practice Schizophrenia PORT Recommendations Surgeon General s Report In 1998, PACT made Medicaid reimbursable Identified as EBP by various groups: SAMHSA/RWJ Initiative: ACT identified as one of 6 EBPs SAMSHA registry Society of Clinical Psychology, APA Division 12 Veterans Administration NAMI

11 Some challenges to ACT implementation


12 ACT is very expensive: Actual costs for Indiana urban ACT Team 16 FTEs; 100 consumers Salary & Benefits (direct) =$ 773,027 Indirect costs =$ 343,693 Total costs =$1,116,720 Projected revenue =$1,398,303 Projected profit =$ 281,583 Cost per client =$11, Admin overhead = 10.35% Annual clinician productivity = 1086 hours Turnover rate = 10%

13 ACT is cost-effective only when implemented well and reserved for severe clients Cost per Consumer: $9,000-$12,000 per year ACT reduces hospital costs when: Target heavy users: ACT saves money when programs serve consumers who are heavy users of psychiatric hospitals (>50 hospital days in prior year) High fidelity: ACT saves money if program is faithfully implemented Latimer, E. (1999). Economic impacts of assertive community treatment: A review of the literature. Canadian Journal of Psychiatry, 44,
. Economic impacts of assertive community treatment: A review of the literature.")
14 ACT is hard to implement Failure to implement: Critical but not implemented ingredients (n=108 teams) (McGrew et al., 1996) Rating Ingredient Ideal My team Implementation gap Involved in hosp dischg 88% 46% 42% Work with supports 73% 36% 37% Low staff turnover 76% 50% 26% Psychiatrist involved 78% 52% 26% Shared treatment planning 84% 59% 25% Primary clinical authority 79% 55% 24% Clearly identified pop. 83% 61% 22% Involved in hosp admits 86% 66% 20% Shared treatment provision 82% 62% 20%

15 Implementation tends to worsen over program generations (N=18) Staff Org Service Total Bridge 1st 2nd 3rd McGrew, J., Bond, G., Dietzen, L., & Salyers, M. (1994). Measuring the Fidelity of Implementation of a Mental Health Program Model. Journal of Consulting and Clinical Psychology, 62,

16 Implementation models


17 Implementation Research Proctor, et al. (2009). Implementation research in mental health services: An emerging science with conceptual, methodological and training challenges. Administration and Policy in Mental Health, 36,


18 Diffusion of innovation

19 National EBP Project: Strategies for assessing and ensuring quality Policy and administration Program standards Licensing & certification Financing Dedicated leadership Training and consultation Practice-based training Ongoing consultation Technical assistance centers Operations Selection and retention of qualified workforce Oversight & supervision Supportive organizational climate /culture Program evaluation Outcome monitoring Service-data monitoring Fidelity assessment Monroe-Devita et al. (2012). Program fidelity and beyond: Multiple strategies and criteria for ensuring quality of Assertive Community Treatment. Psychiatric Services, 63,
. Program fidelity and beyond: Multiple strategies and criteria for ensuring quality of Assertive Community Treatment.")
20 Implementing ACT in Indiana The rise of ACT
21 State level: Setting the stage, Factors supporting implementation Strong evidence base in research literature Prior successful research demonstrations of ACT in state Support of National bodies/reports (NASMHPD, Surgeon General, New Freedom Commission Presidential report) Consumer/family advocates (NAMI) (community action grants) Availability of local experts in ACT and in implementation science Ongoing successful public/academic liaison relationships Advocate/champion at DMHA NOTE: Top-down implementation
22 Working Framework The 5 Critical Steps: Implementing a new EBP 1. Provide explicit principles, guidelines, and implementation criteria 2. Ensure administrative and environmental supports for change 3. Provide clinical training 4. Provide ongoing training/supervision/consultation 5. Collect quantitative information on process and outcome (adapted from Drake, Mueser, et al., 2000)
23 1. Provide explicit criteria Contracted with experts to establish state standards and place them into regulatory law Policies, procedures, and resources in place to monitor standards Adopted existing fidelity scale to measure implementation (Dartmouth Assertive Community Treatment Scale) Availability of manuals PACT manual (recently revised, A Manual for ACT Start-up ) EBP toolkit (SAMHSA) Creation of Indiana specific manual ACT Resource Manual (Indiana Guide) Availability of multiple training resources SAMHSA EBP toolkits available on line at:

24 Sample of certification standard
25 Lessons learned: Not all resources are useful EBP toolkits assume basic clinical knowledge and skills (listening skills) Practitioners trained in the National EBP Project and in Indiana often lacked these prerequisites
26 Type of Resource Materials Matters Keep it brief: Detailed workbooks NOT used Practical tools and tips (e.g., posters listing key principles, assessment scales, job descriptions, checklists) eagerly used
27 Sample quick lists
28 2. Ensure supports for change (state level) Funding support Renewable grants to offset startup costs ($300K/year) Established new Medicaid billing rate for certified ACT teams Regulatory change ACT certification rule Tied Medicaid funding to certification Established ACT technical assistance center
29 ACT Center of Indiana Technical assistance center established July 2001 with state grant Collaborative effort (Clinical and Academic partnership) Diverse team (Trainers, Researchers, Clinicians, Consumers, & Family Members) Clinical partner had model program
30 Role of ACT Center Provided consultation, training, fidelity monitoring in Indiana 31 ACT teams between 2001 and Integrated Dual Disorders Treatment programs 8 Illness Management and Recovery Programs In 2008, expanded to general recovery orientation consultation for 5 mental health centers
31 Supports for change (local level) Secure local agency commitment Make information available to stakeholders (tailored information packets) Consensus building prior to implementation Ensure buy-in from key personnel (medical director, nursing director, adult services director, CEO) Willingness to collect fidelity, consumer outcomes, staff outcomes Money talks! Identify and resolve problem areas Meets a clinical need Philosophical match Competing models/priorities (e.g., day treatment, group homes)

32 Tailored messaging
33 More supports (local) Medical staff availability and support (psychiatry/nursing) Ongoing accountability to state/technical assistance Fidelity Outcomes Local Consumer/family advocates (NAMI) Community action grants SAMSHA
34 3. Provide initial clinical training Stepped roll-out, multiple cohorts Key role of ACT Technical Assistance Center Training free Brought in additional outside consultants (MI) Didactic information in multiple formats Written, audio, visual Materials tailored to location EBP toolkit, manuals Job shadowing existing teams Practical applied exercises Availability of model program in state
35 Toolkit
36 4. Provide ongoing support Provided by ACT Center Each site assigned trainer who provided followup consultation visits Training focused on EBP implementation issues as identified by fidelity assessment Established system for training new staff Local, ongoing regular in-service training Statewide, outside workshops & conferences ACT Center newsletter, listserv and monthly phone calls
37 Sample site fidelity report Current Scores Indiana Averages Indiana Averages H1: Small Caseload H2: Team Approach H3: Program Meeting H4: Practicing Team Leader H5: Continuity of Staffing H6: Staff Capacity H7: Psychiatrist on Staff H8: Nurse on Staff H9: Substance Abuse Specialist on Staff H10: Vocational Specialist on Staff H11: Program Size Items Score DACTS Standards Comments H1: Small Caseload 5 DACTS 5 : 1:10 or smaller caseload size Your team is currently serving 34 consumers with 6 staff (excludes psychiatrists) for a ratio of 1: 5.67, which is very good. H2: Team Approach 4 DACTS 5 : At least 90% of clients have contact with more than 1 staff in 2-week period. Based on electronic medical records, extracted by the team leader, 28 out of 34 consumers were seen by 2+ staff in the past 2 weeks, H3: Frequency of team meetings H4: Team leader provides services H5: Continuity of staff 5 DACTS 5 : Must meet at least 4x weekly, review all consumers, full time staff should attend all meetings, part-time staff should attend at least 2 each week. 5 DACTS 5 : TL provides 10 hrs or more of direct service weekly 3 DACTS 5 : Less than 20% turnover in past 2 years which is 82.35%. According to team leader report, criteria fully met. The team meets at least 4x each week, reviews all consumers, full time staff attend meetings, and part time staff attend at least 2 meetings each week. Team leader is reportedly providing about 10.9 hours/week of client direct service, based on an assumed 20 hours available for clinical work and 50% of that available for direct service, which equals 54.5% of time providing services. This meets the standards. According to team leader, the team has had 4 turnovers out of 7 staff positions over the past two years, with two turnovers in the substance abuse position and two turnovers in a case manager position. This equals a 57.14% turnover for the last two years. The acceptable/ideal criteria for this item requires less than 39%/20% turnover in two years.

38 Newsletter
39 Steps not always sequential. Ongoing support/clear standards Change implementation standards when needed Adaptation to feasibility concerns Ongoing changes to standards (e.g., loosening requirements for RNs, to accept LPN; nurse practitioner for psychiatrist) Changing ACT criteria to ensure accurate implementation Establishing clear inclusion criteria

40 Sample section: admission criteria
41 5. Collect quantitative information Monitor fidelity every 6 months Fidelity scales, state standards Identify key components (e.g., service contacts) Monitor key consumer outcomes (COMP software, supplemented by existing state data collection) Hospitalization, Housing, Employment, Substance Use, Incarceration Feedback to team (outcome-based supervision) Graphs, charts, rewards/incentives
42 Some Barriers Funding Staffing Admission criteria Understanding the model Clinical practice
43 Funding Barriers to ACT Lack of compensation for on-call, after hours, and weekend coverage Unrealistic staff productivity expectations Travel time, training time, meetings Billing procedures ACT is expensive (Other EBPs, too) SOLUTION: ACT rate
44 Staffing Barriers Starting a team from scratch vs. retooling existing program/staff Recruiting/hiring appropriate staff, particularly difficult for specialty and medical staff Adequate team size to provide comprehensive services Integrating/defining specialty roles Turnover SOLUTION: Changing standards for medical personnel, different standards for rural and urban teams
45 Starting a New Team Positives: All team members starting at same level Less resistance to change May have previous EBP experience Openness to new model Less likely to keep individual caseload Negatives: May take more time to establish team Less familiar with candidates to be hired
46 Reworking Existing Team Positives: Known staff Use of existing resources Staff knowledgeable of system Negatives: Resistance: We have always done it this way. More likely to keep existing individual caseload Did I volunteer for this?
47 Admission Criteria Barriers (Defining the target population for the EBP) Poorly specified criteria Poorly defined admission process Poorly executed process Admission decision made external to team Rate of new intakes too fast
48 Understanding the Model Barriers Think they are already doing The Model Misperceptions of the model components Following the letter but not the spirit of the model (focus on meeting intensity criterion vs. focus on recovery)
49 Clinical Practice Barriers New program interferes with or is incompatible with existing clinical practice: Shared caseloads Community-based services Weekend/evenings
50 Implementation success
51
52 DACTS Total Fidelity of Indiana ACT Programs improves and meets criterion over time Time 1 Time 2 Time 3 Time A B C D E F G H I J K L M N
53 % of clients hospitalized State Hospital Rates trend down for two cohorts Client Hospitalized in a State Facility 4.0% 3.5% 3.0% 2.5% 2.0% 1.5% 1.0% Total Cohort 1 Cohort 2 Cohort 3 0.5% 0.0% FY 04 Qtr 1 FY 04 Qtr 2 FY 04 Qtr 3 FY 04 Qtr 4 FY 05 Qtr 1
54 % of clients hospitalized Private Hospital Rates Flat Clients Hospitalized in a Private Facility 25.0% 20.0% 15.0% 10.0% Total Cohort 1 Cohort 2 Cohort 3 5.0% 0.0% FY 04 Qtr 1 FY 04 Qtr 2 FY 04 Qtr 3 FY 04 Qtr 4 FY 05 Qtr 1
55 Competitive Employment Rates Increase % of Clients Competitively Employed 20.0% 18.0% 16.0% 14.0% 12.0% 10.0% 8.0% Total Cohort 1 Cohort 2 Cohort 3 6.0% 4.0% 2.0% 0.0% FY 04 Qtr 1 FY 04 Qtr 2 FY 04 Qtr 3 FY 04 Qtr 4 FY 05 Qtr 1
56 % of clients living independently Independent Living Rates Increase Clients Living Independently 120.0% 100.0% 80.0% 60.0% 40.0% Total Cohort 1 Cohort 2 Cohort % 0.0% FY 02 FY 03 FY 04 Qtr 1 FY 04 Qtr 2 FY 04 Qtr 3 FY 04 Qtr 4 FY 05 Qtr 1
57 Areas of weak implementation at one year: Indiana Adequate psychiatric time hour coverage 4.04 Vocational staff 3.92 Intensity of services 3.64 Integrated SA treatment 3.52 Work with supports 3.36
58 De-implementation of ACT The fall of ACT
59 State level factors Loss of champion (Adult Services Director) Changes at the top, new Director, new adult services chief philosophical differences in strategies to achieve recovery outcomes top-down, non-consultative model for change Lack of stakeholder involvement in changes Great recession Funding squeeze (less money for all operations) ACT taking large chunk of discretionary budget
60 State level factors Defacto control of mental health funding by Medicaid, not DMHA Funding changes Discontinuation of DMHA pilot/maintenance funding (300K) Sweeping revisions in Medicaid funding New 5 tiered rates based on client disability level ACT rate discontinued, replaced by much lower psychiatrist consultation rate Reduced and then discontinued funding for ACT center Reduced TA had limited support for phone certification and some onsite followup training
61 Local factors Overall financial squeeze on budgets Discontinuation of state funding support for ACT Lack of compensating financial resources (medical center, private funding)
62 Local factors Tepid support for full model Didn t buy in to all elements of model as critical (psychiatry, daily team meetings) ACT nonsympathetic/noncapable Team leader Lack of accountability from local administrators No internal champion on management team
63 The end of the story ACT Center continues with federal grants, no longer in partnership with local provider or with state, not focused on ACT No certified ACT teams in Indiana Fewer than 10 sites attempting ACT-lite
64 Thanks for your attention! IUPUI: Stop by and be friendly
Assertive Community Treatment The Indiana Experience. Pat Casanova Director, Indiana Office of Medicaid Policy and Planning November 2009
 Assertive Community Treatment The Indiana Experience Pat Casanova Director, Indiana Office of Medicaid Policy and Planning November 2009 Indiana ACT History 2001: Division of Mental Health and Addictions
Assertive Community Treatment The Indiana Experience Pat Casanova Director, Indiana Office of Medicaid Policy and Planning November 2009 Indiana ACT History 2001: Division of Mental Health and Addictions
ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT
 FIDELITY REPORT") ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT Date: /4/201 To: Todd Andre, Clinical Director Stacey Byers, Clinical Coordinator Candise Sorensen, Site Administrator From: Georgia Harris, MAEd Karen
ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT Date: /4/201 To: Todd Andre, Clinical Director Stacey Byers, Clinical Coordinator Candise Sorensen, Site Administrator From: Georgia Harris, MAEd Karen
ASSERTIVE COMMUNITY TREATMENT: ACT 101. Rebecca K. Sartor, LICSW
 ASSERTIVE COMMUNITY TREATMENT: ACT 101 Rebecca K. Sartor, LICSW A LITTLE BIT ABOUT ME HOW I ENDED UP HERE LEARNING OBJECTIVES To develop an understanding of: How ACT Evolved Practice Principles Services
ASSERTIVE COMMUNITY TREATMENT: ACT 101 Rebecca K. Sartor, LICSW A LITTLE BIT ABOUT ME HOW I ENDED UP HERE LEARNING OBJECTIVES To develop an understanding of: How ACT Evolved Practice Principles Services
ASSERTIVE COMMUNITY TREATMENT (ACT) TEAM REQUEST FOR PROPOSALS. October 3, 2014
 TEAM REQUEST FOR PROPOSALS. October 3, 2014") ASSERTIVE COMMUNITY TREATMENT (ACT) TEAM REQUEST FOR PROPOSALS INTRODUCTION October 3, 2014 New York State Office of Mental Health communicated the availability of reinvestment funding associated with
ASSERTIVE COMMUNITY TREATMENT (ACT) TEAM REQUEST FOR PROPOSALS INTRODUCTION October 3, 2014 New York State Office of Mental Health communicated the availability of reinvestment funding associated with
Enhancing Fidelity Assessment to Assertive Community Treatment (ACT): Introducing the TMACT
: Introducing the TMACT") Enhancing Fidelity Assessment to Assertive Community Treatment (ACT): Introducing the TMACT Maria Monroe-DeVita, Ph.D. The Washington Institute for Mental Health Research & Training University of Washington
Enhancing Fidelity Assessment to Assertive Community Treatment (ACT): Introducing the TMACT Maria Monroe-DeVita, Ph.D. The Washington Institute for Mental Health Research & Training University of Washington
ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT
 FIDELITY REPORT") ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT Date: August, 28 2015 To: Derrick Baker, Clinical Coordinator From: Jeni Serrano, BS T.J Eggsware, BSW, MA, LAC ADHS Fidelity Reviewers Method On August
ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT Date: August, 28 2015 To: Derrick Baker, Clinical Coordinator From: Jeni Serrano, BS T.J Eggsware, BSW, MA, LAC ADHS Fidelity Reviewers Method On August
ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT
 FIDELITY REPORT") ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT Date: 8/6/2015 To: Jennifer Starks From: Jeni Serrano, BS T.J. Eggsware, BSW, MA, LAC ADHS Fidelity Reviewers Method On July 13-14, 2015 Jeni Serrano
ASSERTIVE COMMUNITY TREATMENT (ACT) FIDELITY REPORT Date: 8/6/2015 To: Jennifer Starks From: Jeni Serrano, BS T.J. Eggsware, BSW, MA, LAC ADHS Fidelity Reviewers Method On July 13-14, 2015 Jeni Serrano
9/25/2015. Parallels between Treatment Models 2. Parallels between Treatment Models. Integrated Dual Disorder Treatment and Co-occurring Disorders
 Integrated Dual Disorder Treatment and Co-occurring Disorders RANDI TOLLIVER, PHD HEARTLAND HEALTH OUTREACH, INC. ILLINOIS ASSOCIATION OF PROBLEM-SOLVING COURTS OCTOBER 8, 2015 SPRINGFIELD, IL Parallels
Integrated Dual Disorder Treatment and Co-occurring Disorders RANDI TOLLIVER, PHD HEARTLAND HEALTH OUTREACH, INC. ILLINOIS ASSOCIATION OF PROBLEM-SOLVING COURTS OCTOBER 8, 2015 SPRINGFIELD, IL Parallels
ASSERTIVE COMMUNITY TREATMENT TEAMS CERTIFICATION
 ARTICLE 5.2. ASSERTIVE COMMUNITY TREATMENT TEAMS CERTIFICATION Rule 1. Definitions 440 IAC 5.2-1-1 Applicability Sec. 1. The definitions in this rule apply throughout this article. (Division of Mental
ARTICLE 5.2. ASSERTIVE COMMUNITY TREATMENT TEAMS CERTIFICATION Rule 1. Definitions 440 IAC 5.2-1-1 Applicability Sec. 1. The definitions in this rule apply throughout this article. (Division of Mental
ACT Fidelity Scale Protocol (1/16/03) Page 2. Assertive Community Treatment (ACT) Fidelity Scale: Introduction
 Page 2. Assertive Community Treatment (ACT) Fidelity Scale: Introduction") ACT Fidelity Scale Protocol (1/16/03) Page 1 Protocol for Assertive Community Treatment Fidelity Scale (Dartmouth Assertive Community Treatment Scale DACTS) This document is intended to help guide your
ACT Fidelity Scale Protocol (1/16/03) Page 1 Protocol for Assertive Community Treatment Fidelity Scale (Dartmouth Assertive Community Treatment Scale DACTS) This document is intended to help guide your
How To Manage A Case Management
 Step by Step: A Comprehensive Approach to Case Management Written March, 2011 An initiative of the Conrad N. Hilton Foundation, in partnership with The National Center on Family Homelessness, National
Step by Step: A Comprehensive Approach to Case Management Written March, 2011 An initiative of the Conrad N. Hilton Foundation, in partnership with The National Center on Family Homelessness, National
Assistant Director of Alcohol, Drug, and Mental Health Services Clinical Operations Job Bulletin #13-8004-07
 All photographs courtesy of Mark Bright and used by permission. COUNTY OF SANTA BARBARA Assistant Director of Alcohol, Drug, and Mental Health Services Clinical Operations Job Bulletin #13-8004-07 The
All photographs courtesy of Mark Bright and used by permission. COUNTY OF SANTA BARBARA Assistant Director of Alcohol, Drug, and Mental Health Services Clinical Operations Job Bulletin #13-8004-07 The
H.R 2646 Summary and S. 1945 Comparison
 H.R 2646 Summary and S. 1945 Comparison TITLE I ASSISTANT SECRETARY FOR MENTAL HEALTH AND SUBSTANCE USE DISORDERS It establishes an Office of the Assistant Secretary for Mental Health and Substance Use
H.R 2646 Summary and S. 1945 Comparison TITLE I ASSISTANT SECRETARY FOR MENTAL HEALTH AND SUBSTANCE USE DISORDERS It establishes an Office of the Assistant Secretary for Mental Health and Substance Use
How To Run An Active Altruistic Community Care Program
 ACT Fidelity Scale Protocol (1/16/03) Page 1 Protocol for Assertive Community Treatment Fidelity Scale (Dartmouth Assertive Community Treatment Scale DACTS) This document is intended to help guide your
ACT Fidelity Scale Protocol (1/16/03) Page 1 Protocol for Assertive Community Treatment Fidelity Scale (Dartmouth Assertive Community Treatment Scale DACTS) This document is intended to help guide your
Outcomes for People on Allegheny County Community Treatment Teams
 Allegheny HealthChoices, Inc. Winter 2010 Outcomes for People on Allegheny County Community Treatment Teams Community Treatment Teams (CTTs) in Allegheny County work with people who have some of the most
Allegheny HealthChoices, Inc. Winter 2010 Outcomes for People on Allegheny County Community Treatment Teams Community Treatment Teams (CTTs) in Allegheny County work with people who have some of the most
Gerrit van der Leer Director, Mental Health and Substance Use Integrated Primary and Community Care Branch Ministry of Health British Columbia
 Gerrit van der Leer Director, Mental Health and Substance Use Integrated Primary and Community Care Branch Ministry of Health British Columbia November, 4 th, 2014 Presentation Outline Overview of Assertive
Gerrit van der Leer Director, Mental Health and Substance Use Integrated Primary and Community Care Branch Ministry of Health British Columbia November, 4 th, 2014 Presentation Outline Overview of Assertive
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia
 CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
Program of Assertive Community Services (PACT)
") Program of Assertive Community Services (PACT) Service/Program Definition Program of Assertive Community Services (PACT) entails the provision of an array of services delivered by a community-based, mobile,
Program of Assertive Community Services (PACT) Service/Program Definition Program of Assertive Community Services (PACT) entails the provision of an array of services delivered by a community-based, mobile,
What is CCS? Eligibility
 What is CCS? Department of Health Services Division of Mental Health and Substance Abuse Services Bureau of Prevention, Treatment and Recovery Services Comprehensive Community Services (CCS) Comprehensive
What is CCS? Department of Health Services Division of Mental Health and Substance Abuse Services Bureau of Prevention, Treatment and Recovery Services Comprehensive Community Services (CCS) Comprehensive
Peers in Co-Occurring Services: Impact on Fidelity. Jennifer Harrison, LMSW, CAADC Jennifer.harrison@wmich.edu
 Peers in Co-Occurring Services: Impact on Fidelity Jennifer Harrison, LMSW, CAADC Jennifer.harrison@wmich.edu Introduction Co-Occurring Disorders >50% with a Serious Mental Illness (SMI) also have a Substance
Peers in Co-Occurring Services: Impact on Fidelity Jennifer Harrison, LMSW, CAADC Jennifer.harrison@wmich.edu Introduction Co-Occurring Disorders >50% with a Serious Mental Illness (SMI) also have a Substance
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Definition The Assertive Community Treatment (ACT) Team provides high intensity services, and is available to provide treatment, rehabilitation, and support activities
Assertive Community Treatment (ACT) Definition The Assertive Community Treatment (ACT) Team provides high intensity services, and is available to provide treatment, rehabilitation, and support activities
Implementation Resource Kit User s Guide
 Assertive Community Treatment Implementation Resource Kit DRAFT VERSION 2003 Implementation Resource Kit User s Guide Table of Contents Acknowledgments... 2 Foreword... 3 Introduction... 5 Background...
Assertive Community Treatment Implementation Resource Kit DRAFT VERSION 2003 Implementation Resource Kit User s Guide Table of Contents Acknowledgments... 2 Foreword... 3 Introduction... 5 Background...
Implementation Strategies for Effective Integrated Treatment Services
 Implementation Strategies for Effective Integrated Treatment Services Ric Kruszynski, LISW, LICDC Center for Evidence Based Practices at Case/Ohio SAMI CCOE Mandel School of Applied Social Sciences Department
Implementation Strategies for Effective Integrated Treatment Services Ric Kruszynski, LISW, LICDC Center for Evidence Based Practices at Case/Ohio SAMI CCOE Mandel School of Applied Social Sciences Department
ASSERTIVE COMMUNITY TREATMENT TEAMS
 ARTICLE 11. ASSERTIVE COMMUNITY TREATMENT TEAMS Rule 1. Definitions 440 IAC 11-1-1 Applicability Sec. 1. The definitions in this rule apply throughout this article. (Division of Mental Health and Addiction;
ARTICLE 11. ASSERTIVE COMMUNITY TREATMENT TEAMS Rule 1. Definitions 440 IAC 11-1-1 Applicability Sec. 1. The definitions in this rule apply throughout this article. (Division of Mental Health and Addiction;
Overview. AACP Positions on Access to Psychiatric and Psychopharmacologic Services in Underserved Areas 1
 AMERICAN ASSOCIATION OF COMMUNITY PSYCHIATRISTS POSITION PAPER ON ENSURING ACCESS TO RECOVERY ORIENTED SAFETY NET PSYCHIATRIC SERVICES IN UNDERSERVED AND ECONOMICALLY DISTRESSED COMMUNITIES Overview The
AMERICAN ASSOCIATION OF COMMUNITY PSYCHIATRISTS POSITION PAPER ON ENSURING ACCESS TO RECOVERY ORIENTED SAFETY NET PSYCHIATRIC SERVICES IN UNDERSERVED AND ECONOMICALLY DISTRESSED COMMUNITIES Overview The
Treating Co-Occurring Disorders. Stevie Hansen, B.A., LCDC, NCACI Chief, Addiction Services
 Treating Co-Occurring Disorders Stevie Hansen, B.A., LCDC, NCACI Chief, Addiction Services Implementing SAMHSA Evidence-Based Practice Toolkits Integrated Dual Diagnosis Treatment (IDDT) Target group:
Treating Co-Occurring Disorders Stevie Hansen, B.A., LCDC, NCACI Chief, Addiction Services Implementing SAMHSA Evidence-Based Practice Toolkits Integrated Dual Diagnosis Treatment (IDDT) Target group:
Treatment for Co occurring Disorders
 Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention, Treatment, and Recovery and the
Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention, Treatment, and Recovery and the
Integrated Treatment for Co-Occurring Disorders
 Integrated Treatment for Co-Occurring Disorders An Evidence-Based Practice What Are Evidence-Based Practices? Services that have consistently demonstrated their effectiveness in helping people with mental
Integrated Treatment for Co-Occurring Disorders An Evidence-Based Practice What Are Evidence-Based Practices? Services that have consistently demonstrated their effectiveness in helping people with mental
New Developments in Supported Employment San Francisco Behavioral Health Court
 New Developments in Supported Employment San Francisco Behavioral Health Court NADCP National Conference May 27, 2014 Lisa Lightman Kathleen Connolly Lacey, LCSW Gregory Jarasitis, MOT, OTR/L Goals of
New Developments in Supported Employment San Francisco Behavioral Health Court NADCP National Conference May 27, 2014 Lisa Lightman Kathleen Connolly Lacey, LCSW Gregory Jarasitis, MOT, OTR/L Goals of
Optum By United Behavioral Health. 2015 Mississippi Coordinated Access Network (CAN) Medicaid Level of Care Guidelines
 Medicaid Level of Care Guidelines") Optum By United Behavioral Health 2015 Mississippi Coordinated Access Network (CAN) Medicaid Level of Care Guidelines Assertive Community Treatment is a multi-disciplinary, selfcontained clinical team
Optum By United Behavioral Health 2015 Mississippi Coordinated Access Network (CAN) Medicaid Level of Care Guidelines Assertive Community Treatment is a multi-disciplinary, selfcontained clinical team
How to Use. The Treatment of Depression in Older Adults Evidence-Based Practices KITs. The Treatment of Depression in Older Adults
 How to Use The Treatment of Depression in Older Adults Evidence-Based Practices KITs The Treatment of Depression in Older Adults How to Use The Treatment of Depression in Older Adults Evidence-Based Practices
How to Use The Treatment of Depression in Older Adults Evidence-Based Practices KITs The Treatment of Depression in Older Adults How to Use The Treatment of Depression in Older Adults Evidence-Based Practices
Evidence-Based Supported Employment Services in Broward County. Request for Letters of Interest (RLI) Solicitation # 0003
 Solicitation # 0003") Evidence-Based Supported Employment Services in Broward County Request for Letters of Interest (RLI) Solicitation # 0003 Available: November 23, 2015 December 15, 2015 1 P a g e CONTENTS Page Number I.
Evidence-Based Supported Employment Services in Broward County Request for Letters of Interest (RLI) Solicitation # 0003 Available: November 23, 2015 December 15, 2015 1 P a g e CONTENTS Page Number I.
Commission on Alternatives to Incarceration 12-9-2013
 Commission on Alternatives to Incarceration 12-9-2013 Jeff Stenseth Regional Director Southeast and South Central Human Service Center Department of Human Services Outline HSC and the community Services
Commission on Alternatives to Incarceration 12-9-2013 Jeff Stenseth Regional Director Southeast and South Central Human Service Center Department of Human Services Outline HSC and the community Services
GOI Protocol 4-3-04 Page 1. General Organizational Index (GOI) (Expanded) Item Definitions and Scoring
 (Expanded) Item Definitions and Scoring") GOI Protocol 4-3-04 Page 1 General Organizational Index (GOI) (Expanded) Item Definitions and Scoring Note: This version identical to GOI version of 11-25-02 for Items G1-G12. Items G13 & G14 added by
GOI Protocol 4-3-04 Page 1 General Organizational Index (GOI) (Expanded) Item Definitions and Scoring Note: This version identical to GOI version of 11-25-02 for Items G1-G12. Items G13 & G14 added by
Performance Standards
 Performance Standards Co-Occurring Disorder Competency Performance Standards are intended to provide a foundation and serve as a tool to promote continuous quality improvement and progression toward best
Performance Standards Co-Occurring Disorder Competency Performance Standards are intended to provide a foundation and serve as a tool to promote continuous quality improvement and progression toward best
Angela L. Rollins, PhD Research Director, ACT Center of Indiana; Assistant Research Professor, Department of Psychology, IUPUI.
 Integrating ACT and IMR -- 1 Integrating Assertive Community Treatment and Illness Management and Recovery for Consumers with Severe Mental Illness Michelle P. Salyers, PhD Acting Co-Director, VA HSR&D
Integrating ACT and IMR -- 1 Integrating Assertive Community Treatment and Illness Management and Recovery for Consumers with Severe Mental Illness Michelle P. Salyers, PhD Acting Co-Director, VA HSR&D
Integrated Dual Disorder Treatment (IDDT)
") Integrated Dual Disorder Treatment (IDDT) Jeff Stenseth Assistant Regional Director Southeast Human Service Center Department of Human Services Commission on Alternatives to Incarceration 9-13-2012 *Source:
Integrated Dual Disorder Treatment (IDDT) Jeff Stenseth Assistant Regional Director Southeast Human Service Center Department of Human Services Commission on Alternatives to Incarceration 9-13-2012 *Source:
Getting our ACT Together
 Getting our ACT Together Assertive Community Treatment (ACT) for the Seriously Mentally Ill in Iowa Technical Assistance Center for Assertive Community Treatment November 2010 Nancy Williams MD Betsy Hradek
Getting our ACT Together Assertive Community Treatment (ACT) for the Seriously Mentally Ill in Iowa Technical Assistance Center for Assertive Community Treatment November 2010 Nancy Williams MD Betsy Hradek
TREATMENT MODALITIES. May, 2013
 TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
other caregivers. A beneficiary may receive one diagnostic assessment per year without any additional authorization.
 4.b.(8) Diagnostic, Screening, Treatment, Preventive and Rehabilitative Services (continued) Attachment 3.1-A.1 Page 7c.2 (a) Psychotherapy Services: For the complete description of the service providers,
4.b.(8) Diagnostic, Screening, Treatment, Preventive and Rehabilitative Services (continued) Attachment 3.1-A.1 Page 7c.2 (a) Psychotherapy Services: For the complete description of the service providers,
Psychiatric Rehabilitation Services
 DEFINITION Psychiatric or Psychosocial Rehabilitation Services provide skill building, peer support, and other supports and services to help adults with serious and persistent mental illness reduce symptoms,
DEFINITION Psychiatric or Psychosocial Rehabilitation Services provide skill building, peer support, and other supports and services to help adults with serious and persistent mental illness reduce symptoms,
Kenneth Minkoff, MD 100 Powdermill Road, Box 319 Acton, MA 01720 781-932-8792x311 Kminkov@aol.com
 Kenneth Minkoff, MD 100 Powdermill Road, Box 319 Acton, MA 01720 781-932-8792x311 Kminkov@aol.com COMPREHENSIVE, CONTINUOUS, INTEGRATED SYSTEM OF CARE MODEL The Comprehensive, Continuous, Integrated System
Kenneth Minkoff, MD 100 Powdermill Road, Box 319 Acton, MA 01720 781-932-8792x311 Kminkov@aol.com COMPREHENSIVE, CONTINUOUS, INTEGRATED SYSTEM OF CARE MODEL The Comprehensive, Continuous, Integrated System
CABHAs and non-cabha agencies may provide Comprehensive Clinical Assessments, Medication Management, and Outpatient Therapy.
 Page 7c.1b 4.b Early and periodic screening, diagnostic and treatment services for individuals under 21 years of age, and treatment of conditions found. (continued) Critical Access Behavioral Health Agency
Page 7c.1b 4.b Early and periodic screening, diagnostic and treatment services for individuals under 21 years of age, and treatment of conditions found. (continued) Critical Access Behavioral Health Agency
Information for Consumers
 Assertive Community Treatment Implementation Resource Kit DRAFT VERSION 2002 Information for Consumers Who is assertive community treatment for? Assertive community treatment is for people who experience
Assertive Community Treatment Implementation Resource Kit DRAFT VERSION 2002 Information for Consumers Who is assertive community treatment for? Assertive community treatment is for people who experience
DIRECT CARE CLINIC DASHBOARD INDICATORS SPECIFICATIONS MANUAL Last Revised 11/20/10
 DIRECT CARE CLINIC DASHBOARD INDICATORS SPECIFICATIONS MANUAL Last Revised 11/20/10 1. ACT Fidelity 2. ISP Current 3. ISP Quality 4. Recipient Satisfaction 5. Staffing Physician 6. Staffing Case Manager
DIRECT CARE CLINIC DASHBOARD INDICATORS SPECIFICATIONS MANUAL Last Revised 11/20/10 1. ACT Fidelity 2. ISP Current 3. ISP Quality 4. Recipient Satisfaction 5. Staffing Physician 6. Staffing Case Manager
THE INTEGRATED DUAL DIAGNOSIS TREATMENT PROGRAM OF VENTURA COUNTY BEHAVIORAL HEALTH. Presented by Linda Gertson, Ph.D. Behavioral Health Manager
 THE INTEGRATED DUAL DIAGNOSIS TREATMENT PROGRAM OF VENTURA COUNTY BEHAVIORAL HEALTH Presented by Linda Gertson, Ph.D. Behavioral Health Manager The California Institute of Mental Health (CIMH) was awarded
THE INTEGRATED DUAL DIAGNOSIS TREATMENT PROGRAM OF VENTURA COUNTY BEHAVIORAL HEALTH Presented by Linda Gertson, Ph.D. Behavioral Health Manager The California Institute of Mental Health (CIMH) was awarded
Dual Diagnosis: Models of Care and Local Pathways AGENDA. Part one: Part two:
 Slide 1 Dual Diagnosis: Models of Care and Local Pathways St. Anne s Community Services Dual Diagnosis Project Slide 2 AGENDA Part one: Models of Care. Clinical Guidelines & Evidence Base Local Care Pathways
Slide 1 Dual Diagnosis: Models of Care and Local Pathways St. Anne s Community Services Dual Diagnosis Project Slide 2 AGENDA Part one: Models of Care. Clinical Guidelines & Evidence Base Local Care Pathways
DDCAT Rating Scale Cover Sheet
 Cover Sheet Program Identification Date Rater(s) Time Spent (Hours) Agency Name Program Name Address Zip Code Contact Person 1) 2) Telephone FAX Email State Region Program ID Time Period 1= Baseline; 2
Cover Sheet Program Identification Date Rater(s) Time Spent (Hours) Agency Name Program Name Address Zip Code Contact Person 1) 2) Telephone FAX Email State Region Program ID Time Period 1= Baseline; 2
Redesigning the Publicly-Funded Mental Health System in Texas
 Redesigning the Publicly-Funded Mental Health System in Texas Access to care when services are needed Choice in health plans for consumers and providers Integration of care at the plan and provider level
Redesigning the Publicly-Funded Mental Health System in Texas Access to care when services are needed Choice in health plans for consumers and providers Integration of care at the plan and provider level
Certified Community Behavioral Health Clinics
 Certified Community Behavioral Health Clinics CCBHCs Stakeholders New Jersey Department of Human Services Division of Mental Health & Addiction Services October, 2015 1 Background on Excellence in Mental
Certified Community Behavioral Health Clinics CCBHCs Stakeholders New Jersey Department of Human Services Division of Mental Health & Addiction Services October, 2015 1 Background on Excellence in Mental
STRUCTURED OUTPATIENT ADDICTION PROGRAM (SOAP)
") STRUCTURED OUTPATIENT ADDICTION PROGRAM (SOAP) Providers contracted for this level of care or service will be expected to comply with all requirements of these service-specific performance specifications.
STRUCTURED OUTPATIENT ADDICTION PROGRAM (SOAP) Providers contracted for this level of care or service will be expected to comply with all requirements of these service-specific performance specifications.
Best Practices in Mental Health State Policy Initiatives
 Best Practices in Mental Health State Policy Initiatives Presentation to the Nevada Senate Legislative Committee on Health Care February 5, 2014 Sita Diehl Director of State Policy and Advocacy National
Best Practices in Mental Health State Policy Initiatives Presentation to the Nevada Senate Legislative Committee on Health Care February 5, 2014 Sita Diehl Director of State Policy and Advocacy National
Marin County s STAR Program: Support and Treatment for Mentally Ill Offenders
 Marin County s STAR Program: Support and Treatment for Mentally Ill Offenders Marcella Velasquez EXECUTIVE SUMMARY Overrepresentation of the mentally ill in prisons and jails and limited mental health
Marin County s STAR Program: Support and Treatment for Mentally Ill Offenders Marcella Velasquez EXECUTIVE SUMMARY Overrepresentation of the mentally ill in prisons and jails and limited mental health
LEVEL III.5 SA: SHORT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE)
") LEVEL III.5 SA: SHT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE) Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders
LEVEL III.5 SA: SHT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE) Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders
Intensive Outpatient Psychotherapy - Adult
 Intensive Outpatient Psychotherapy - Adult Definition Intensive Outpatient Psychotherapy services provide group based, non-residential, intensive, structured interventions consisting primarily of counseling
Intensive Outpatient Psychotherapy - Adult Definition Intensive Outpatient Psychotherapy services provide group based, non-residential, intensive, structured interventions consisting primarily of counseling
Optum By United Behavioral Health. 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines
 Level of Care Guidelines") Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Statewide Inpatient Psychiatric Program Services (SIPP) Statewide Inpatient Psychiatric
Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Statewide Inpatient Psychiatric Program Services (SIPP) Statewide Inpatient Psychiatric
Department of Veterans Affairs VHA DIRECTIVE 2010-010 Veterans Health Administration Washington, DC 20420 March 2, 2010
 Department of Veterans Affairs VHA DIRECTIVE 2010-010 Veterans Health Administration Washington, DC 20420 STANDARDS FOR EMERGENCY DEPARTMENT AND URGENT CARE CLINIC STAFFING NEEDS IN VHA FACILITIES 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2010-010 Veterans Health Administration Washington, DC 20420 STANDARDS FOR EMERGENCY DEPARTMENT AND URGENT CARE CLINIC STAFFING NEEDS IN VHA FACILITIES 1. PURPOSE:
There is mounting interest
 Moving Assertive Community Treatment Into Standard Practice Susan D. Phillips, M.S.W. Barbara J. Burns, Ph.D. Elizabeth R. Edgar, M.S.S.W. Kim T. Mueser, Ph.D. Karen W. Linkins, Ph.D. Robert A. Rosenheck,
Moving Assertive Community Treatment Into Standard Practice Susan D. Phillips, M.S.W. Barbara J. Burns, Ph.D. Elizabeth R. Edgar, M.S.S.W. Kim T. Mueser, Ph.D. Karen W. Linkins, Ph.D. Robert A. Rosenheck,
Program Guidelines and Procedures for Adult Transitional Case Management
 Texas Department of Criminal Justice TCOOMMI Program Guidelines and Procedures for Adult Transitional Case Management Number: PGP 01.07 September Date: 1, 2013 Page: 1 of 5 Supersedes: January 3, 2011
Texas Department of Criminal Justice TCOOMMI Program Guidelines and Procedures for Adult Transitional Case Management Number: PGP 01.07 September Date: 1, 2013 Page: 1 of 5 Supersedes: January 3, 2011
Resident Rotation: Collaborative Care Consultation Psychiatry
 Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD James Basinski, MD With contributions from: Jurgen Unutzer, MD, MPH, MA Jennifer Sexton, MD, Catherine Howe, MD, PhD
Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD James Basinski, MD With contributions from: Jurgen Unutzer, MD, MPH, MA Jennifer Sexton, MD, Catherine Howe, MD, PhD
ACUTE TREATMENT SERVICES (ATS) FOR SUBSTANCE USE DISORDERS LEVEL III.7
 FOR SUBSTANCE USE DISORDERS LEVEL III.7") ACUTE TREATMENT SERVICES (ATS) FOR SUBSTANCE USE DISORDERS LEVEL III.7 Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance
ACUTE TREATMENT SERVICES (ATS) FOR SUBSTANCE USE DISORDERS LEVEL III.7 Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance
Protocol to Support Individuals with a Dual Diagnosis in Central Alberta
 Protocol to Support Individuals with a Dual Diagnosis in Central Alberta Partners David Thompson Health Region Canadian Mental Health Association, Central Alberta Region Persons with Developmental Disabilities
Protocol to Support Individuals with a Dual Diagnosis in Central Alberta Partners David Thompson Health Region Canadian Mental Health Association, Central Alberta Region Persons with Developmental Disabilities
Critical Time Intervention in North Carolina. Barbara B. Smith, MSW, LCSW Clinical Assistant Professor UNC School of Social Work
 Critical Time Intervention in North Carolina Barbara B. Smith, MSW, LCSW Clinical Assistant Professor UNC School of Social Work Critical Time Intervention: Local Pilot and Statewide Championing is funded
Critical Time Intervention in North Carolina Barbara B. Smith, MSW, LCSW Clinical Assistant Professor UNC School of Social Work Critical Time Intervention: Local Pilot and Statewide Championing is funded
CSI Training Supplement Evidence-Based Practices (EBPs) and Service Strategies (SSs) (S-25.0)
 and Service Strategies (SSs) (S-25.0)") CSI Training Supplement Evidence-Based Practices (EBPs) and Service Strategies (SSs) (S-25.0) July 14, 2006 Note: This training supplement is intended to serve as a tool for counties to use in order to
CSI Training Supplement Evidence-Based Practices (EBPs) and Service Strategies (SSs) (S-25.0) July 14, 2006 Note: This training supplement is intended to serve as a tool for counties to use in order to
ILLINOIS DEPARTMENT OF CENTRAL MANAGEMENT SERVICES CLASS SPECIFICATION MENTAL HEALTH RECOVERY SUPPORT SPECIALIST SERIES
 ILLINOIS DEPARTMENT OF CENTRAL MANAGEMENT SERVICES CLASS SPECIFICATION MENTAL HEALTH RECOVERY SUPPORT SPECIALIST SERIES Class Title Position Code Effective Mental Health Recovery Support Specialist I 26921
ILLINOIS DEPARTMENT OF CENTRAL MANAGEMENT SERVICES CLASS SPECIFICATION MENTAL HEALTH RECOVERY SUPPORT SPECIALIST SERIES Class Title Position Code Effective Mental Health Recovery Support Specialist I 26921
I. Introduction. ACT Program Standards
 Montana Standards for Programs of Assertive Community Treatment Adapted in 2011 from National Program Standards for ACT Teams Deborah Allness, M.S.S.W. and William Knoedler, M.D. Revised June 2003 by D.
Montana Standards for Programs of Assertive Community Treatment Adapted in 2011 from National Program Standards for ACT Teams Deborah Allness, M.S.S.W. and William Knoedler, M.D. Revised June 2003 by D.
New York State Health Foundation Center for Excellence in Integrated Care (CEIC): Support for Health Care Institutions
: Support for Health Care Institutions") New York State Health Foundation Center for Excellence in Integrated Care (CEIC): Support for Health Care Institutions Richard N. Rosenthal, MD Chairman, Department of Psychiatry St. Luke s Roosevelt Hospital
New York State Health Foundation Center for Excellence in Integrated Care (CEIC): Support for Health Care Institutions Richard N. Rosenthal, MD Chairman, Department of Psychiatry St. Luke s Roosevelt Hospital
Implementation of IDDT in Vermont Community Rehabilitation and Treatment Programs
 Implementation of IDDT in Vermont Community Rehabilitation and Treatment Programs Report Prepared for: SAMHSA 1500 Fishers Lane 11C 22 Rockville, MD 20857 Project Information Training and Evaluation of
Implementation of IDDT in Vermont Community Rehabilitation and Treatment Programs Report Prepared for: SAMHSA 1500 Fishers Lane 11C 22 Rockville, MD 20857 Project Information Training and Evaluation of
Variance to Minnesota Rules, parts 9520.0500 to 9520.0690 (Rule 36) for Intensive Residential Treatment Services (IRTS) Effective July 1, 2010
 for Intensive Residential Treatment Services (IRTS) Effective July 1, 2010") Variance to Minnesota Rules, parts 9520.0500 to 9520.0690 (Rule 36) for Intensive Residential Treatment Services (IRTS) Effective July 1, 2010 OUTLINE R36V.01 Purpose R36V.02 Applicable Regulations R36V.03
Variance to Minnesota Rules, parts 9520.0500 to 9520.0690 (Rule 36) for Intensive Residential Treatment Services (IRTS) Effective July 1, 2010 OUTLINE R36V.01 Purpose R36V.02 Applicable Regulations R36V.03
Evidence Based Approaches to Addiction and Mental Illness Treatment for Adults
 Evidence Based Practice Continuum Guidelines The Division of Behavioral Health strongly encourages behavioral health providers in Alaska to implement evidence based practices and effective program models.
Evidence Based Practice Continuum Guidelines The Division of Behavioral Health strongly encourages behavioral health providers in Alaska to implement evidence based practices and effective program models.
Evaluating Your Program
 Evaluating Your Program Supported U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Mental Health Services www.samhsa.gov Evaluating Your
Evaluating Your Program Supported U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Mental Health Services www.samhsa.gov Evaluating Your
PERFORMANCE STANDARDS DRUG AND ALCOHOL PARTIAL HOSPITALIZATION PROGRAM. Final Updated 04/17/03
 PERFORMANCE STANDARDS DRUG AND ALCOHOL PARTIAL HOSPITALIZATION PROGRAM Final Updated 04/17/03 Community Care is committed to developing performance standards for specific levels of care in an effort to
PERFORMANCE STANDARDS DRUG AND ALCOHOL PARTIAL HOSPITALIZATION PROGRAM Final Updated 04/17/03 Community Care is committed to developing performance standards for specific levels of care in an effort to
Chapter 1 Implementation Challenges & Opportunities for Evidence Based Practices
 Chapter 1 Implementation Challenges & Opportunities for Evidence Based Practices Anne D. Strode, MSW Diane Norell, MSW, OTR/L Dennis G. Dyck, PhD. Washington State University Spokane Washington Institute
Chapter 1 Implementation Challenges & Opportunities for Evidence Based Practices Anne D. Strode, MSW Diane Norell, MSW, OTR/L Dennis G. Dyck, PhD. Washington State University Spokane Washington Institute
Integrated Dual Disorders Treatment Fidelity Scale
 IDDT Fidelity Scale Protocol (Revision of 11-272-02) Page 1 Integrated Dual Disorders Treatment Fidelity Scale This document is intended to help guide you in administering the Integrated Dual Disorders
IDDT Fidelity Scale Protocol (Revision of 11-272-02) Page 1 Integrated Dual Disorders Treatment Fidelity Scale This document is intended to help guide you in administering the Integrated Dual Disorders
Assertive Community Treatment (ACT) Providing Health Home Care Management Interim Instruction: February 19, 2014
 Providing Health Home Care Management Interim Instruction: February 19, 2014") Assertive Community Treatment (ACT) Providing Health Home Care Management Interim Instruction: February 19, 2014 Introduction The Office of Mental Health (OMH) licensed and regulated Assertive Community
Assertive Community Treatment (ACT) Providing Health Home Care Management Interim Instruction: February 19, 2014 Introduction The Office of Mental Health (OMH) licensed and regulated Assertive Community
OUTPATIENT SERVICES. Components of Service
 OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
Texas Resilience and Recovery. Utilization Management Guidelines: Adult Mental Health Services
 Texas Resilience and Recovery Utilization Management Guidelines: Adult Mental Health Services Effective September 2015 Introduction Texas Resiliency and Recovery, or TRR is a term to describe the service
Texas Resilience and Recovery Utilization Management Guidelines: Adult Mental Health Services Effective September 2015 Introduction Texas Resiliency and Recovery, or TRR is a term to describe the service
LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult
 LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders of the American
LEVEL I SA: OUTPATIENT INDIVIDUAL THERAPY - Adult Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders of the American
Evaluating Your Program
 Evaluating Your Program Assertive Community Treatment U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Mental Health Services www.samhsa.gov
Evaluating Your Program Assertive Community Treatment U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Mental Health Services www.samhsa.gov
Oklahoma Behavioral Healthcare Workforce Study
 Oklahoma Behavioral Healthcare Workforce Study Presented to the Oklahoma Governor s Transformation Advisory Board December 17, 2009 This research was supported by the Mental Health Transformation State
Oklahoma Behavioral Healthcare Workforce Study Presented to the Oklahoma Governor s Transformation Advisory Board December 17, 2009 This research was supported by the Mental Health Transformation State
COMPARISON OF KEY PROVISIONS House and Senate Comprehensive Mental Health Reform Legislation
 COMPARISON OF KEY PROVISIONS House and Senate Comprehensive Mental Health Reform Legislation Note: A full title-by-title summary of H.R. 2646, the Helping Families in Mental Health Crisis Act of 2015 (Murphy/Johnson)
COMPARISON OF KEY PROVISIONS House and Senate Comprehensive Mental Health Reform Legislation Note: A full title-by-title summary of H.R. 2646, the Helping Families in Mental Health Crisis Act of 2015 (Murphy/Johnson)
Building Your Program
 Building Your Program Assertive Community Treatment U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Mental Health Services www.samhsa.gov
Building Your Program Assertive Community Treatment U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Mental Health Services www.samhsa.gov
DUAL DIAGNOSIS CAPABILITY IN ADDICTION TREATMENT (DDCAT) VERSION 3.2 RATING SCALE COVER SHEET
 VERSION 3.2 RATING SCALE COVER SHEET") DUAL DIAGNOSIS CAPABILITY IN ADDICTION TREATMENT (DDCAT) VERSION 3.2 Program Identification RATING SCALE COVER SHEET Date: Rater(s): Time Spent (Hours): Agency Name: Program Name: Address: Zip Code: Contact
DUAL DIAGNOSIS CAPABILITY IN ADDICTION TREATMENT (DDCAT) VERSION 3.2 Program Identification RATING SCALE COVER SHEET Date: Rater(s): Time Spent (Hours): Agency Name: Program Name: Address: Zip Code: Contact
SUPPORTED EMPLOYMENT (SE) FIDELITY REPORT
 FIDELITY REPORT") SUPPORTED EMPLOYMENT (SE) FIDELITY REPORT Date: September 3, 201 To: John Moore From: Georgia Harris, MAEd Karen Voyer-Caravona, MA, MSW ADHS Fidelity Reviewers Method On July 20-22, 201, Georgia Harris
SUPPORTED EMPLOYMENT (SE) FIDELITY REPORT Date: September 3, 201 To: John Moore From: Georgia Harris, MAEd Karen Voyer-Caravona, MA, MSW ADHS Fidelity Reviewers Method On July 20-22, 201, Georgia Harris
Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE
 Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE Subtitle 21 MENTAL HYGIENE REGULATIONS Chapter 26 Community Mental Health Programs Residential Crisis Services Authority: Health-General Article, 10-901
Title 10 DEPARTMENT OF HEALTH AND MENTAL HYGIENE Subtitle 21 MENTAL HYGIENE REGULATIONS Chapter 26 Community Mental Health Programs Residential Crisis Services Authority: Health-General Article, 10-901
Assertive Community Treatment (ACT) Providing Health Home Care Management Interim Instruction: December 6, 2013
 Providing Health Home Care Management Interim Instruction: December 6, 2013") Assertive Community Treatment (ACT) Providing Health Home Care Management Interim Instruction: December 6, 2013 Introduction The OMH licensed and regulated Assertive Community Treatment Program (ACT) will
Assertive Community Treatment (ACT) Providing Health Home Care Management Interim Instruction: December 6, 2013 Introduction The OMH licensed and regulated Assertive Community Treatment Program (ACT) will
The Field of Counseling
 Gainful Employment Information The Field of Counseling Job Outlook Veterans Administration one of the most honorable places to practice counseling is with the VA. Over recent years, the Veteran s Administration
Gainful Employment Information The Field of Counseling Job Outlook Veterans Administration one of the most honorable places to practice counseling is with the VA. Over recent years, the Veteran s Administration
IMPLEMENTING SAMHSA EVIDENCE-BASED PRACTICE TOOLKITS. Integrated Dual Diagnosis Treatment (IDDT)
") This is a DRAFT summary of evidence supporting the IDDT model. It is one of a series of evidence summaries CIMH is creating. IMPLEMENTING SAMHSA EVIDENCE-BASED PRACTICE TOOLKITS Brief description of the
This is a DRAFT summary of evidence supporting the IDDT model. It is one of a series of evidence summaries CIMH is creating. IMPLEMENTING SAMHSA EVIDENCE-BASED PRACTICE TOOLKITS Brief description of the
Development of Health Career Pathway for California. Psychiatric Mental Health Nurse Practitioner/Clinical Nurse Specialist Career Pathway
 Development of Health Career Pathway for California Psychiatric Mental Health Nurse Practitioner/Clinical Nurse Specialist Career Pathway 1 Current State As of February 2011, there were 9,458 psychiatric
Development of Health Career Pathway for California Psychiatric Mental Health Nurse Practitioner/Clinical Nurse Specialist Career Pathway 1 Current State As of February 2011, there were 9,458 psychiatric
Frequently Asked Questions (FAQs) from December 2013 Behavioral Health Utilization Management Webinars
 from December 2013 Behavioral Health Utilization Management Webinars") Frequently Asked Questions (FAQs) from December 2013 Behavioral Health Utilization Management Webinars 1. In the past we did precertifications for Residential Treatment Centers (RTC). Will this change
Frequently Asked Questions (FAQs) from December 2013 Behavioral Health Utilization Management Webinars 1. In the past we did precertifications for Residential Treatment Centers (RTC). Will this change
FACT: A Dutch Version of ACT
 Community Mental Health Journal, Vol. 43, No. 4, August 2007 (Ó 2007) DOI: 10.1007/s10597-007-9089-4 FACT: A Dutch Version of ACT J. Remmers van Veldhuizen, Psychiatrist ABSTRACT: Assertive Community Treatment
Community Mental Health Journal, Vol. 43, No. 4, August 2007 (Ó 2007) DOI: 10.1007/s10597-007-9089-4 FACT: A Dutch Version of ACT J. Remmers van Veldhuizen, Psychiatrist ABSTRACT: Assertive Community Treatment
Employment Opportunities Administrative
 David Lawrence Center is a not-for-profit, behavioral health agency that provides comprehensive, innovative mental health and substance abuse services in Southwest Florida. In addition to helping children
David Lawrence Center is a not-for-profit, behavioral health agency that provides comprehensive, innovative mental health and substance abuse services in Southwest Florida. In addition to helping children
Model Scopes of Practice & Career Ladder for Substance Use Disorder Counseling
 Model Scopes of Practice & Career Ladder for Substance Use Disorder Counseling February 2011 Background and Introduction Treatment of substance use disorders (SUD) is recognized as a multidisciplinary
Model Scopes of Practice & Career Ladder for Substance Use Disorder Counseling February 2011 Background and Introduction Treatment of substance use disorders (SUD) is recognized as a multidisciplinary
MENTAL HEALTH INPATIENT INITIAL CERTIFICATION APPLICATION Chapter DHS 61.71 and 61.79
 DEPARTMENT OF HEALTH SERVICES STATE OF WISCONSIN Division of Quality Assurance Chapter DHS 61.71 and 61.79, Wis. Admin. Code Page 1 of 9 MENTAL HEALTH INPATIENT INITIAL CERTIFICATION APPLICATION Chapter
DEPARTMENT OF HEALTH SERVICES STATE OF WISCONSIN Division of Quality Assurance Chapter DHS 61.71 and 61.79, Wis. Admin. Code Page 1 of 9 MENTAL HEALTH INPATIENT INITIAL CERTIFICATION APPLICATION Chapter
COMPARISON OF KEY PROVISIONS Comprehensive Mental Health Reform Legislation
 COMPARISON OF KEY PROVISIONS Comprehensive Mental Health Reform Legislation Bill Sponsors: Tim Murphy (R-PA) and Eddie Bernice Johnson (D-TX) New position of Assistant Secretary of Mental Health and Substance
COMPARISON OF KEY PROVISIONS Comprehensive Mental Health Reform Legislation Bill Sponsors: Tim Murphy (R-PA) and Eddie Bernice Johnson (D-TX) New position of Assistant Secretary of Mental Health and Substance
Q&A. What Are Co-occurring Disorders?
 What Are Co-occurring Disorders? Some people suffer from a psychiatric or mental health disorder (such as depression, an anxiety disorder, bipolar disorder, or a mood or adjustment disorder) along with
What Are Co-occurring Disorders? Some people suffer from a psychiatric or mental health disorder (such as depression, an anxiety disorder, bipolar disorder, or a mood or adjustment disorder) along with
The Field of Counseling. Veterans Administration one of the most honorable places to practice counseling is with the
 Gainful Employment Information The Field of Counseling Job Outlook Veterans Administration one of the most honorable places to practice counseling is with the VA. Over recent years, the Veteran s Administration
Gainful Employment Information The Field of Counseling Job Outlook Veterans Administration one of the most honorable places to practice counseling is with the VA. Over recent years, the Veteran s Administration
Psychiatric Day Rehabilitation MH - Adult
 Psychiatric Day Rehabilitation MH - Adult Definition Day Rehabilitation services are designed to provide individualized treatment and recovery, inclusive of psychiatric rehabilitation and support for clients
Psychiatric Day Rehabilitation MH - Adult Definition Day Rehabilitation services are designed to provide individualized treatment and recovery, inclusive of psychiatric rehabilitation and support for clients
System Transformation In Philadelphia: A Recovery Revolution
 System Transformation In Philadelphia: A Recovery Revolution Philadelphia Department of Behavioral Health and Mental Retardation Implementation Strategies Roland Lamb, Director Office of Addiction Services
System Transformation In Philadelphia: A Recovery Revolution Philadelphia Department of Behavioral Health and Mental Retardation Implementation Strategies Roland Lamb, Director Office of Addiction Services
ThePACT. Advocacy Guide
 With more than 200,000 members, NAMI is the nation s leading grassroots advocacy organization solely dedicated to improving the lives of persons with severe mental illnesses including schizophrenia, bipolar
With more than 200,000 members, NAMI is the nation s leading grassroots advocacy organization solely dedicated to improving the lives of persons with severe mental illnesses including schizophrenia, bipolar