Disease-Specific Care CERTIFICATION PROGRAM
|
|
|
- Lizbeth Haynes
- 8 years ago
- Views:
Transcription
1 Disease-Specific Care CERTIFICATION PROGRAM PERFORMANCE MEASUREMENT IMPLEMENTATION GUIDE January 2014 Copyright, The Joint Commission

2 (ACHF) Set Measures Set Measure Measure Short Name ID ACHF-01 Beta-Blocker Therapy (i.e., Bisoprolol, Carvedilol, or Sustained-Release Metoprolol Succinate) for LVSD Prescribed at Discharge ACHF-02 Post-Discharge Appointment for Heart Failure Patients ACHF-03 Care Transition Record Transmitted ACHF-04 Discussion of Advance Directives/Advance Care Planning ACHF-05 Advance Directive Executed ACHF-06 Post-Discharge Evaluation for Heart Failure Patients General Data Elements Element Name Birthdate Clinical Trial Discharge Date Hispanic Ethnicity ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date Race Sex Collected For All Records, All Records, All Records, Not collected for HBIPS-2 and HBIPS-3 All Records, All Records, Optional for All HBIPS Records; Used in algorithm for PC-01, 02, 04 and 05; All Records, Optional for HBIPS-2 and HBIPS-3; Used in algorithm for PC-01, 02, 03, 04, 05 and PBM-03 All Records, Optional for All HBIPS Records; Used in algorithm for PC-01, 02, 04 and 05 All Records, Optional for All HBIPS and PBM Records All Records, All Records, Measure Set Specific Data Elements Element Name Admission Date Advance Directive Executed Bisoprolol, Carvedilol, or Sustained-Release Metoprolol Prescribed for LVSD at Discharge Care Transition Record Transmitted Collected For ACHF-01, ACHF-02, ACHF-03, ACHF- 04, ACHF-05, ACHF-06, ACHF-05, ACHFOP-07, ACHF-01, ACHF-03, 1

3 Care Transition Record-Discharge Medications ACHF-03, Care Transition Record-Follow-Up Treatment(s) and ACHF-03, Service(s) Needed Care Transition Record-Procedures Performed During ACHF-03, Hospitalization Care Transition Record-Reason for Hospitalization ACHF-03, Care Transition Record-Treatment(s)/Service(s) Provided ACHF-03, Comfort Measures Only ACHF-01, ACHF-02, ACHF-03, ACHF- 04, ACHF-05, ACHF-06, Discharge Disposition ACHF-01, ACHF-02, ACHF-03, ACHF- 04, ACHF-05, ACHF-06, Discussion of Advance Directives/Advance Care Planning ACHF-04, ACHFOP-06, LVSD < 40% ACHF-01, ACHFOP-01, ACHFOP-02, ACHFOP-03, Post-Discharge Appointment Scheduled Within 7 Days ACHF-02, Post-Discharge Evaluation Conducted Within 72 Hours ACHF-06, Reason for No Bisoprolol, Carvedilol, or Sustained-Release ACHF-01, Metoprolol Prescribed for LVSD at Discharge Reason for No Post-Discharge Appointment Within 7 Days ACHF-02, Initial Patient Population 2

4 3
5 HF Sample Size Requirements Hospitals that choose to sample have the option of sampling quarterly or sampling monthly. A hospital may choose to use a larger sample size than is required. Hospitals whose Initial Patient Population size is less than the minimum number of cases per quarter for the measure set cannot sample. Hospitals that have five or fewer HF discharges (both Medicare and non-medicare combined) in a quarter are not required to submit HF patient level data to the QIO Clinical Warehouse 1 and Joint Commission s Data Warehouse. Regardless of the option used, hospital samples must be monitored to ensure that sampling procedures consistently produce statistically valid and useful data. Due to exclusions, hospitals selecting sample cases MUST submit AT LEAST the minimum required sample size. The following sample size tables for each option automatically build in the number of cases needed to obtain the required sample sizes. For information concerning how to perform sampling, refer to the Population and Sampling Specifications section in this manual. Quarterly Sampling Hospitals performing quarterly sampling for HF must ensure that its Initial Patient Population and sample size meet the following conditions: Quarterly Sample Size Based on Initial Patient Population Size for the HF Measure Set Average Quarterly Initial Patient Population Size N Hospital's Measure Minimum Required Sample Size n % of Initial Patient Population size No sampling; 100% Initial Patient Population required 0-5 Submission of patient level data is encouraged but not required: CMS: if submission occurs, 1-5 cases of Initial Patient Population may be submitted 1 The Joint Commission: if submission occurs, 100% Initial Patient Population required Monthly Sampling Hospitals performing monthly sampling for HF must ensure that its Initial Patient Population and sample size meet the following conditions: 4

6 Monthly Sample Size Based on Initial Patient Population Size for the HF Measure Set Average Monthly Initial Patient Population Size N Hospital's Measure Minimum Required Sample Size n % of Initial Patient Population size <26 No sampling; 100% Initial Patient Population required Sample Size Examples Quarterly sampling: The HF Initial Patient Population size for a hospital has been 500 patients per quarter during the past year. The required quarterly sample size would be 100 (twenty percent of 500) heart failure patients per quarter -- as this number is smaller than the maximum condition (i.e., 304 cases) and larger than the minimum condition (i.e., 76 cases). A hospital s HF Initial Patient Population size is 1,482 patients during the third quarter. The required sample size is 20% of the patient population or 297 cases for the quarter (twenty percent of 1,482 equals rounded to the next highest whole number equals 297). A hospital s HF Initial Patient Population size is 5 patients during the first quarter. Submission of patient level data is not required. If the hospital chooses to submit patient level data: CMS: the quarterly sample size would be 1 5 cases for the quarter. 1 The Joint Commission: the required quarterly sample size would be 100% of the patient population or 5 cases for the quarter. Monthly sampling: A hospital s HF Initial Patient Population size is 25 patients during March. Since this is less than the minimum condition (i.e., 26 cases), no sampling is allowed or 100% of the patient population of 25 cases is required. A hospital s HF Initial Patient Population size is 503 patients during July. The required sample size is 20% of the patient population or 101 cases for the month (twenty percent of 503 equals rounded to the next highest whole number equals 101). 1 The Heart Failure (HF) core measure sampling methodology is applicable to both the HF core measures as well as the ACHF measures. The HF sampling methodology is shared by CMS and The Joint Commission; however, data collection for the ACHF measures is required by Joint Commission Disease-Specific Care Certification only. 5
 heart failure patients per quarter -- as this number is smaller than the maximum condition (i.e., 304 cases) and larger than the minimum condition (i.")
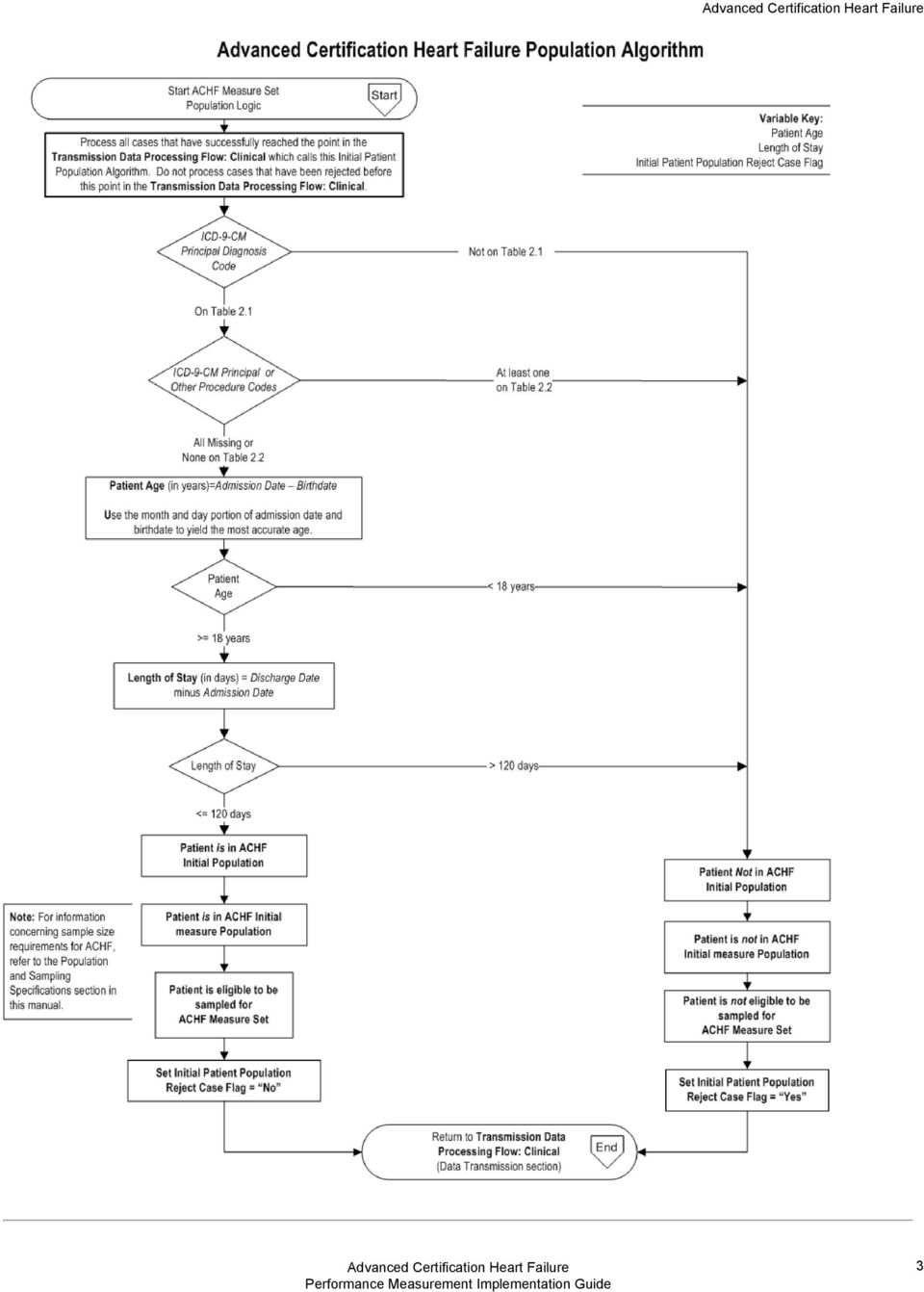
7 Measure Information Form Measure Set: (ACHF) Set Measure ID: ACHF-01 Performance Measure Name: Beta-Blocker Therapy (i.e., Bisoprolol, Carvedilol, or Sustained- Release Metoprolol Succinate) for LVSD Prescribed at Discharge Description: Beta-blocker therapy (i.e., bisoprolol, carvedilol, or sustained-release metoprolol succinate) is prescribed for heart failure patients with LVSD at discharge. For purposes of this measure, LVSD is defined as chart documentation of a left ventricular ejection fraction (LVEF) less than 40% or a narrative description of left ventricular systolic (LVS) function consistent with moderate or severe systolic dysfunction. Rationale: Beta-blocker therapy has been recommended for the treatment of patients with heart failure and reduced left ventricular ejection fraction (LVEF) since the 1970 s (HFSA, 2010). Several large-scale clinical trials have provided unequivocal evidence of important reductions in both morbidity and mortality. The marked beneficial effects of beta blockade has been well demonstrated in large-scale clinical trials of symptomatic patients with New York Heart Association (NYHA) class II-IV heat failure and reduced LVEF using carvedilol, bisoprolol, and sustainedrelease metoprolol succinate (Hunt et al., 2009). These beta-blockers, in addition to ACE inhibitors and diuretics, are considered routine therapy for heart failure patients with reduced LVEF. Betablocker therapy is well tolerated by the majority of patients, even those with co-morbidities such as, diabetes mellitus, chronic obstructive lung disease, and peripheral vascular disease. Type of Measure: Process Improvement Noted As: Increase in the rate Numerator Statement: Patients who are prescribed bisoprolol, carvedilol, or sustained-release metoprolol succinate for LVSD at hospital discharge. Included Populations: Not applicable Excluded Populations: None Data Elements: Bisoprolol, Carvedilol, or Sustained-Release Metoprolol Prescribed for LVSD at Discharge Denominator Statement: Heart failure patients with current or prior documentation of left ventricular ejection fraction (LVSD) < 40%. Included Populations: Discharges with ICD-9-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and Documentation of LVSD < 40% 6

8 Excluded Populations: Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-9-CM procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2) Patients less than 18 years of age Patients who have a Length of Stay greater than 120 days Patients with Comfort Measures Only documented Patients enrolled in a Clinical Trial Patients discharged to another hospital Patients who left against medical advice Patients who expired Patients discharged to home for hospice care Patients discharged to a healthcare facility for hospice care Patients with a documented Reason for No Bisoprolol, Carvedilol, or Sustained- Release Metoprolol Succinate Prescribed for LVSD at Discharge Data Elements: Admission Date Birthdate Clinical Trial Comfort Measures Only Discharge Disposition ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date LVSD < 40% Reason for No Bisoprolol, Carvedilol, or Sustained-Release Metoprolol Prescribed for LVSD at Discharge Risk Adjustment: No. Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. Data Accuracy: Variation may exist in the assignment of ICD-9-CM codes; therefore, coding practices may require evaluation to ensure consistency. Measure Analysis Suggestions: None Sampling: Yes. Please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section. Data Reported As: Aggregate rate generated from count data reported as a proportion. Selected References: American College of Cardiology Foundation, American Heart Association, Physician Consortium for Performance Improvement (PCPI). Heart Failure Performance Measurement Set. Jan. 2011; American Heart Association. Get With The Guidelines Outpatient Fact Sheet

9 3. 4. Hunt SA, Abraham WT, Chin MH, Felman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW Focused update incorporated Into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):e391-e479. Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Klapholz M, MoserDK, Rogers JG, Starling RC, Stevenson WG, Tang WHW, Teerlink JR, Walsh MN. Executive Summary: HFSA 2010 Comphrensive Heart Failure Practice Guideline. J Card Fail 2010;16: Measure Algorithm: 8

10 9

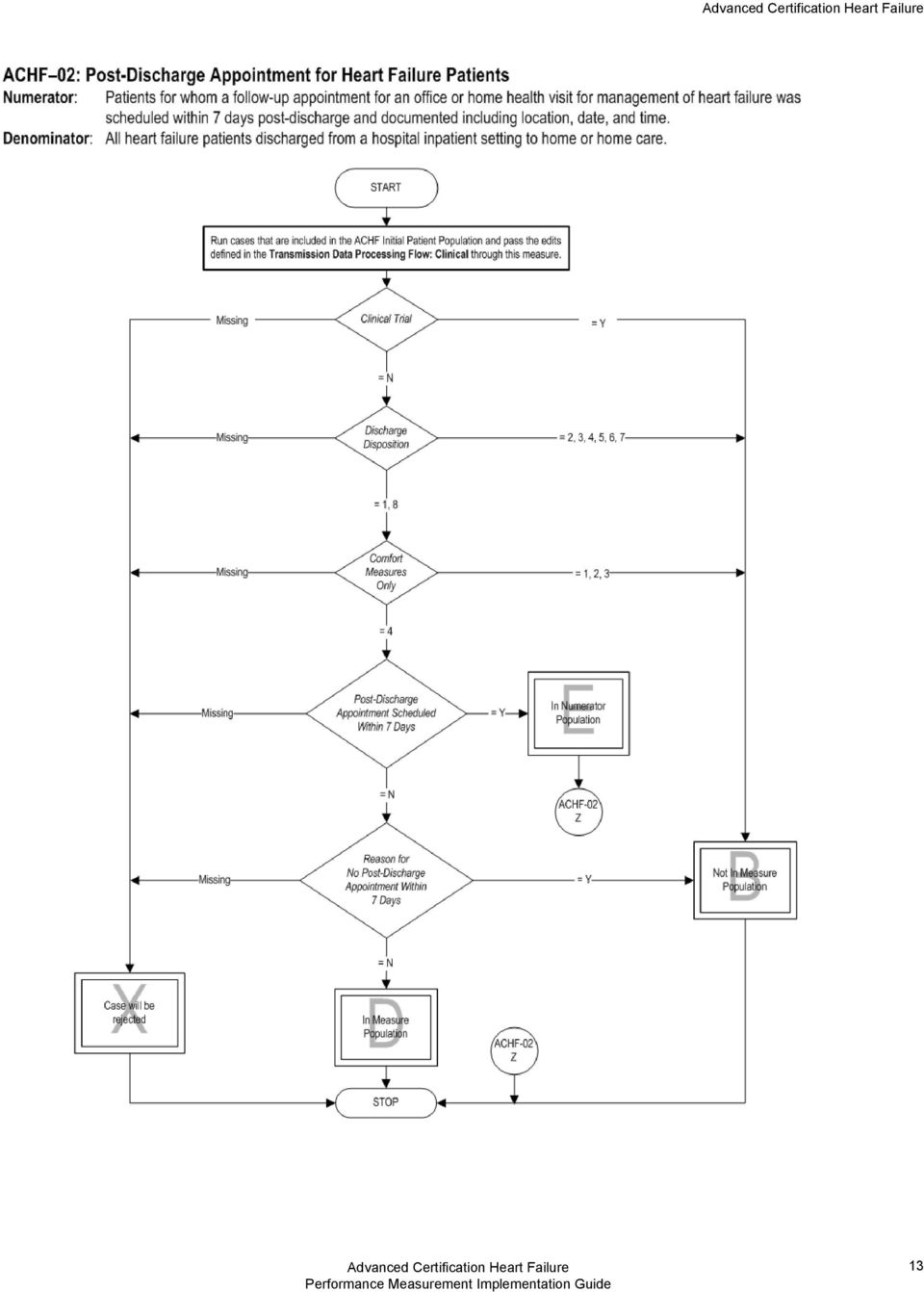
11 Measure Information Form Measure Set: (ACHF) Set Measure ID: ACHF-02 Performance Measure Name: Post-Discharge Appointment for Heart Failure Patients Description: Patients for whom a follow-up appointment for an office or home health visit for management of heart failure was scheduled within 7 days post-discharge and documented including location, date, and time. Rationale: Care coordination is important for all patients, but especially for vulnerable populations, such as patients with heart failure and other chronic diseases. Today, the average Medicare patient sees two primary care and five specialists per year (NQF, 2010). For patients with multiple chronic conditions, the number of healthcare providers involved in the care of the patient is even higher. The exchange of information from one healthcare provider to another should smooth the transition of care from the inpatient to outpatient setting. According to Bell and colleagues (2008), the separation of hospital and ambulatory care may result in significant care discontinuities after discharge. Therefore, it is paramount that discussions between providers summarize the patient s history and communicate the plan for follow-up care after discharge in order to be effective. When done well, this exchange of information can avoid conflicting plans of care; overuse, underuse, and misuse of medications, tests and therapies; reduce costs and potentially adverse events. The Joint Commission s 2013 Disease-Specific Care Certification Manual Advanced Certification in Heart Failure standard DSPR.3 requires: The program [to provide] care coordination services across inpatient and outpatient settings. Scheduling of the initial follow-up appointment with the primary care provider is a first-step to ensuring continuity of care. In addition, standard DSPR.8 requires that care, treatment, and services are provided in a planned and timely manner, which includes the arrangement of a follow-up appointment with a health care provider to occur within seven days after discharge. Type of Measure: Process Improvement Noted As: Increase in the rate Numerator Statement: Patients for whom a follow-up appointment for an office or home health visit for management of heart failure was scheduled within 7 days post-discharge and documented including location, date, and time. Included Populations: Not applicable Excluded Populations: None Data Elements: Post-Discharge Appointment Scheduled Within 7 Days Denominator Statement: All heart failure patients discharged from a hospital inpatient setting to home or home care. 10
.")
12 Included Populations: Discharges with ICD-9-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and A discharge to home, home care, or court/law enforcement Excluded Populations: Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-9-CM procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2) Patients less than 18 years of age Patient who have a Length of Stay greater than 120 days Patients with Comfort Measures Only documented Patients enrolled in a Clinical Trial Patients discharged to locations other than home, home care, or law enforcement Patients with a documented Reason for No Post-Discharge Appointment Within 7 Days Data Elements: Admission Date Birthdate Clinical Trial Comfort Measures Only Discharge Disposition ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date Reason for No Post-Discharge Appointment Within 7 Days Risk Adjustment: No. Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. Data Accuracy: Variation may exist in the assignment of ICD-9-CM codes; therefore, coding practices may require evaluation to ensure consistency. Measure Analysis Suggestions: None Sampling: Yes. Please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section. Data Reported As: Aggregate rate generated from count data reported as a proportion. Selected References: American College of Cardiology Foundation, American Heart Association, Physician Consortium for Performance Improvement (PCPI). Heart Failure Performance Measurement Set. Jan. 2011; American Heart Association. Get With The Guidelines Outpatient Fact Sheet Hunt SA, Abraham WT, Chin MH, Felman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW
 Patients less than 18 years of age Patient who have a Length of Stay greater than 120 days Patients with Comfort Measures Only documented Patients enrolled in a Clinical Trial Patients discharged")
13 4. 5. Focused update incorporated Into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):e391-e479. Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Klapholz M, MoserDK, Rogers JG, Starling RC, Stevenson WG, Tang WHW, Teerlink JR, Walsh MN. Executive Summary: HFSA 2010 Comphrensive Heart Failure Practice Guideline. J Card Fail 2010;16: The Joint Commission. The Joint Commission s 2012 Disease-Specific Care Certification Manual: Advanced Certification in Heart Failure Addendum. Oakbrook Terrace, IL: Author Measure Algorithm: 12

14 13
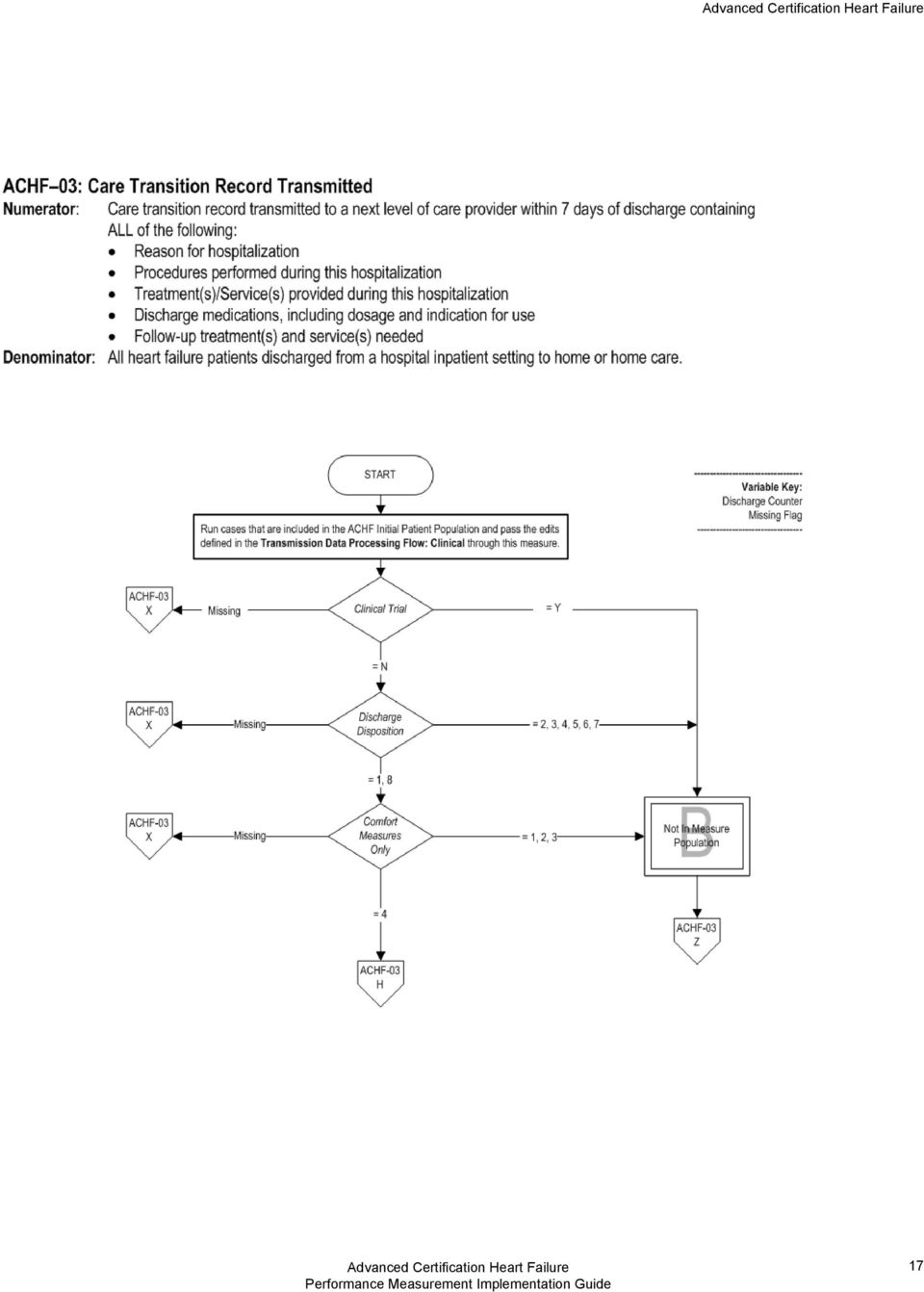
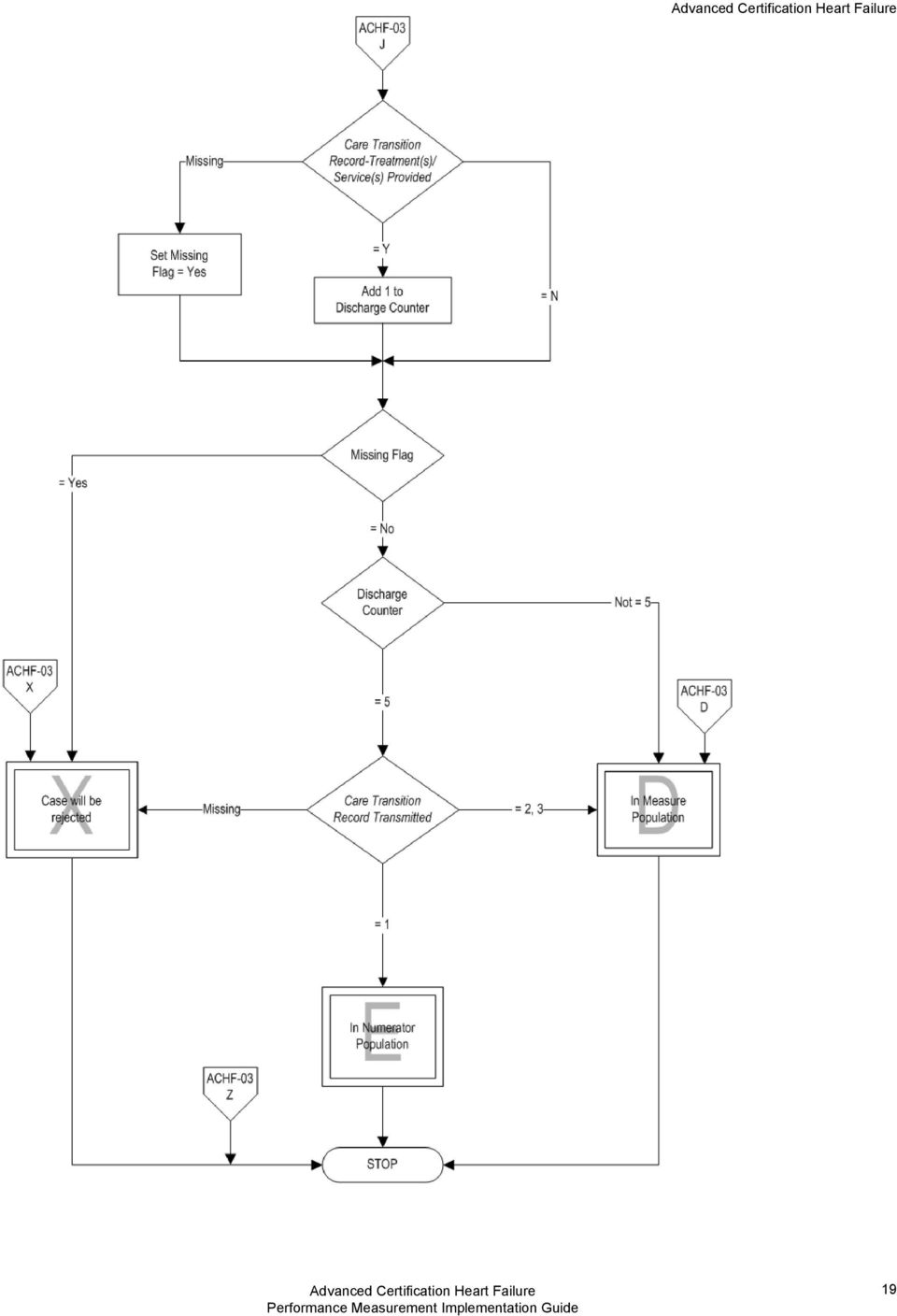
15 Measure Information Form Measure Set: (ACHF) Set Measure ID: ACHF-03 Performance Measure Name: Care Transition Record Transmitted Description: A care transition record is transmitted to a next level of care provider within 7 days of discharge containing ALL of the following: Reason for hospitalization Procedures performed during this hospitalization Treatment(s)/Service(s) provided during this hospitalization Discharge medications, including dosage and indication for use Follow-up treatment and services needed (e.g., post-discharge therapy, oxygen therapy, durable medical equipment) Rationale: The hand-over of care from one healthcare provider to another should smooth the transition of care from the inpatient to outpatient setting (van Walraven et al., 2002). Communication and information exchange should be completed to allow sufficient time for the receiving provider to treat the patient. The timeliness of communication should be consistent with the urgency of follow-up required (Kripalani et al., 2007). Communication and information exchange between providers may be in the form of a phone call, fax, or other secure vehicle, such as, mutual access to an electronic health record (EHR). The Joint Commission s 2013 Disease-Specific Care Certification Manual Advanced Certification in Heart Failure standard DSPR.3 requires: The program [to provide] care coordination services across inpatient and outpatient settings. Requirements specific to heart failure care certification include: The program identifies an individual to coordinate the care of participants. The program provides participants with access to a practitioner 24 hours a day, 7 days a week (access may include use of the telephone and the internet, and referral to urgent care settings). The program communicates important information regarding co-occurring conditions and comorbidities to appropriate practitioner(s) to treat or manage conditions. The program care coordinator(s) is responsible for the communication of relevant information among practitioners and across settings. The program care coordinator(s) is responsible for sharing information among practitioners in a timeframe that meets the participant s needs. The program care coordinator(s) is responsible for confirming practitioner receipt of information and actions taken. Type of Measure: Process Improvement Noted As: Increase in the rate Numerator Statement: Care transition record transmitted to a next level of care provider within 7 days of discharge containing ALL of the following: 14

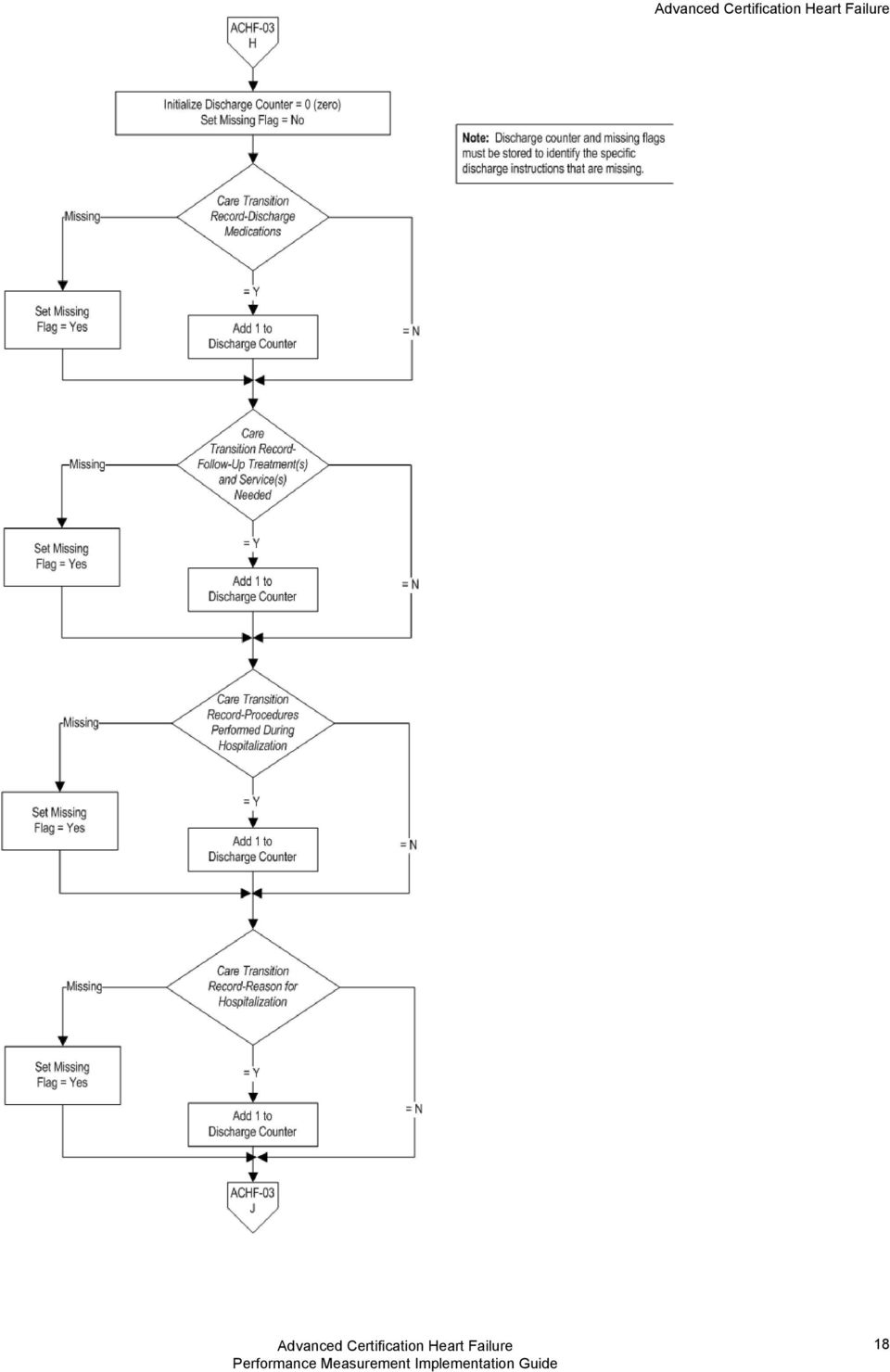
16 Reason for hospitalization Procedures performed during this hospitalization Treatment(s)/Service(s) provided during this hospitalization Discharge medications, including dosage and indication for use Follow-up treatment(s) and service(s) needed Included Populations: Not applicable Excluded Populations: None Data Elements: Care Transition Record Transmitted Care Transition Record-Discharge Medications Care Transition Record-Follow-Up Treatment(s) and Service(s) Needed Care Transition Record-Procedures Performed During Hospitalization Care Transition Record-Reason for Hospitalization Care Transition Record-Treatment(s)/Service(s) Provided Denominator Statement: All heart failure patients discharged from a hospital inpatient setting to home or home care Included Populations: Discharges with ICD-9-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and A discharge to home, home care, or court/law enforcement Excluded Populations: Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-9-CM procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2) Patients less than 18 years of age Patient who have a Length of Stay greater than 120 days Patients with Comfort Measures Only documented Patients enrolled in a Clinical Trial Patients discharged to locations other than home, home care, or law enforcement Data Elements: Admission Date Birthdate Clinical Trial Comfort Measures Only Discharge Disposition ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date Risk Adjustment: No. Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. 15
/Service(s) Provided Denominator Statement: All heart failure patients discharged from a hospital inpatient setting to home or home care Included Populations:")
17 Data Accuracy: Variation may exist in the assignment of ICD-9-CM codes; therefore, coding practices may require evaluation to ensure consistency. Measure Analysis Suggestions: None Sampling: Yes. Please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section. Data Reported As: Aggregate rate generated from count data reported as a proportion. Aggregate rate generated from count data reported as a proportion Selected References: Bell CM, Schnipper JL, Auerback AD, Kaboli PJ, Wetterneck TB, Gonzales DV, Arora VM, Zhang JX, Meltzer DO; Association of communication between hospital-based physicians and Primary care providers with patient outcomes. J Gen Intern Med. 2008; 24(3): Bodenheimer T. Coordinating care a perilous journey through the health care system.nejm. 2008;358(10): Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. JAMA. 2007; 297(8): Ravel AN, Marchiori GE, Arnold JMO. Improving the continuity of care following discharge of patients hospitalized with heart failure: Is the discharge summary adequate? Can J Cardiol. 2003;19(4): van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17(3): The Joint Commission. The Joint Commission s 2012 Disease-Specific Care Certification Manual: Advanced Certification in Heart Failure Addendum. Oakbrook Terrace, IL: Author Measure Algorithm: 16

18 17
19 18
20 19
21 Measure Information Form Measure Set: (ACHF) Set Measure ID: ACHF-04 Performance Measure Name: Discussion of Advance Directives/Advance Care Planning Description: Patients who have documentation in the medical record of a one-time discussion of advance directives/advance care planning with a healthcare provider. Rationale: Heart failure is a progressive, debilitating disease which carries with it a poor prognosis over time and high mortality rate. Physicians should acknowledge the life-threatening nature of the disease and discuss with patients and/or their caregivers prognosis, quality of life, pharmacologic and device therapies, self-management, and supportive care options (HFSA, 2010). According to Heffner and Barbieri, most patients at fourteen cardiac rehabilitation programs across the United States, presumed the need for life-support at some point in the future and wanted to make their own decisions about end-of-life care. Most of the patients were aware of advance directives, desired more information, and preferred to get more information from their lawyers, families, physicians, or cardiac rehabilitation programs (Perkins, 2000). Despite this receptiveness, only 15% of patients had discussed advance directives with their physicians, and 10% had confidence that their physicians understood their wishes (Heffner and Barbieri, 2000). Type of Measure: Process Improvement Noted As: Increase in the rate Numerator Statement: Patients who have documentation in the medical record of a one-time discussion of advance directives/advance care planning with a healthcare provider Included Populations: Not applicable Excluded Populations: None Data Elements: Discussion of Advance Directives/Advance Care Planning Denominator Statement: All heart failure patients Included Populations: Discharges with ICD-9-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1 Patients who left against medical advice (AMA) Patients enrolled in a Clinical Trial Excluded Populations: 20
22 Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-9-CM procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2) Patients less than 18 years of age Patient who have a Length of Stay greater than 120 days Patients with Comfort Measures Only documented Patients discharged to another hospital Patients discharged to home for hospice care Patients discharged to a health care facility for hospice care Patients who expire Data Elements: Admission Date Birthdate Comfort Measures Only Discharge Disposition ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date Risk Adjustment: No. Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. Data Accuracy: Variation may exist in the assignment of ICD-9-CM codes; therefore, coding practices may require evaluation to ensure consistency. Measure Analysis Suggestions: None Sampling: Yes. please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section. Data Reported As: Aggregate rate generated from count data reported as a proportion. Aggregate rate generated from count data reported as a proportion Selected References: Anderson R, Joy S, Carkido A, Anthony S, Smyntek D, Perrine S, Puet TA, Butler ET. Development of a Congestive Heart Failure Protocol in a Rehabilitation Setting. Rehab Nursing 2010;35(1);3-7;30. Hefner JE, Barberi C. End-of-life care preferences of patients enrolled in cardiovascular rehabilitation programs. Chest. 2000;117(5); Kass-Bartelmes BL, Hughes R. Advance Care Planning Preferences for care at the end of life. J Pain Palliat Care Pharmacother. 2004;18(1): Perkins HS. Time to move advance care planning beyond advance directives. Chest. 2000;117(5); Wilkinson A. Living with Advanced Congestive Heart Failure: A Guide for Family Caregivers. The Washington Home Center for Palliative Care Studies (A Division of the RAND Corporation). Nov Measure Algorithm: 21
23 22
24 Measure Information Form Measure Set: (ACHF) Set Measure ID: ACHF-05 Performance Measure Name: Advance Directive Executed Description: Patients who have documentation in the medical record that an advance directive was executed. Rationale: Heart failure is a progressive, debilitating disease which carries with it a poor prognosis over time and high mortality rate. Physicians should acknowledge the life-threatening nature of the disease and discuss with patients and/or their caregivers prognosis, quality of life, pharmacologic and device therapies, self-management, and supportive care options (HFSA, 2010). According to Heffner and Barbieri, most patients at fourteen cardiac rehabilitation programs across the United States, presumed the need for life-support at some point in the future and wanted to make their own decisions about end-of-life care. Most of the patients were aware of advance directives, desired more information, and preferred to get more information from their lawyers, families, physicians, or cardiac rehabilitation programs (Perkins, 2000). Despite this receptiveness, only 15% of patients had discussed advance directives with their physicians, and 10% had confidence that their physicians understood their wishes (Heffner and Barbieri, 2000). Type of Measure: Process Improvement Noted As: Increase in the rate Numerator Statement: Patients who have documentation in the medical record that an advance directive was executed. Included Populations: Not applicable Excluded Populations: None Data Elements: Advance Directive Executed Denominator Statement: All heart failure patients. Included Populations: Discharges with ICD-9-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and Patients who left against medical advice (AMA) Patients enrolled in a Clinical Trial Excluded Populations: 23
25 Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-9-CM procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2) Patients less than 18 years of age Patients who have a Length of Stay Greater than 120 days Patients with Comfort Measures Only documented Patients discharged to another hospital Patients discharged to home for hospice care Patients discharged to a health care facility for hospice care Patients who expire Data Elements: Admission Date Birthdate Comfort Measures Only Discharge Disposition ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date Risk Adjustment: No. Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. Data Accuracy: Variation may exist in the assignment of ICD-9-CM codes; therefore, coding practices may require evaluation to ensure consistency. Measure Analysis Suggestions: None Sampling: Yes. Please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section. Data Reported As: Aggregate rate generated from count data reported as a proportion. Selected References: 1. Anderson R, Joy S, Carkido A, Anthony S, Smyntek d, Perrine S, Puet TA, Butler ET. Development of a Congestive Heart Failure Protocol in a Rehabilitation Setting. Rehab Nursing 2010;35(1);3-7; Hefner JE, Barberi C. End-of-life care preferences of patients enrolled in cardiovascular rehabilitation programs. Chest. 2000;117(5); Kass-Bartelmes BL, Hughes R. Advance Care Planning Preferences for care at the end of life. J Pain Palliat Care Pharmacother. 2004;18(1): Perkins HS. Time to move advance care planning beyond advance directives. Chest. 2000;117 (5); Wilkinson A. Living with Advanced Congestive Heart Failure: A Guide for Family Caregivers. The Washington Home Center for Palliative Care Studies (A Division of the RAND Corporation). Nov Measure Algorithm: 24
26 25
27 Measure Information Form Measure Set: (ACHF) Set Measure ID: ACHF-06 Performance Measure Name: Post-Discharge Evaluation for Heart Failure Patients Description: Patients who receive a re-evaluation for symptoms worsening and treatment compliance by a program team member within 72 hours after inpatient discharge. Rationale: Today, hospitals and providers in the United States are challenged to provide highquality, cost-effective healthcare. Preventing readmissions to the hospital is one opportunity to control costs and deliver quality care. According to Hospital Compare (2010), the national 30-day readmission rate for heart failure is 24.7%. Jha and colleagues (2009) have concluded that data collection for discharge planning and instruction measures has not reduced unnecessary readmissions. Alternative interventions are needed to meet heart failure treatment goals postdischarge. Ongoing evaluation of patient symptoms and their functional consequences may help prevent hospital readmissions The Joint Commission s 2013 Disease-Specific Care Certification Manual Advanced Certification in Heart Failure standard DSPR.8, EP.1a requires that care, treatment, and services are provided in a planned and timely manner. Compliance with this standard is demonstrated through a re-evaluation of the patient by a program team member within 72 hours after inpatient discharge. The reevaluation may be conducted via phone call, home visit, or scheduled office appointment. Type of Measure: Process Improvement Noted As: Increase in the rate Numerator Statement: Patients who have a documented re-evaluation conducted via phone call or home visit within 72 hours after discharge. Included Populations: Not applicable Excluded Populations: None Data Elements: Post-Discharge Evaluation Conducted Within 72 Hours Denominator Statement: All heart failure patients discharged from a hospital inpatient setting to home or home care AND patients leaving against medical advice (AMA). Included Populations: Discharges with ICD-9-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and A discharge to home, home care, or court/law enforcement Patients who left against medical advice (AMA) 26
28 Excluded Populations: Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-9-CM procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2) Patients less than 18 years of age Patient who have a Length of Stay greater than 120 days Patients with Comfort Measures Only documented Patients enrolled in a Clinical Trial Patients discharged to locations other than home, home care, law enforcement, or AMA Data Elements: Admission Date Birthdate Clinical Trial Comfort Measures Only Discharge Disposition ICD-9-CM Other Procedure Codes ICD-9-CM Principal Diagnosis Code ICD-9-CM Principal Procedure Code ICD-9-CM Principal Procedure Date Risk Adjustment: No. Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. Data Accuracy: Variation may exist in the assignment of ICD-9-CM codes; therefore, coding practices may require evaluation to ensure consistency. Measure Analysis Suggestions: None Sampling: Yes. please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section. Data Reported As: Aggregate rate generated from count data reported as a proportion. Aggregate rate generated from count data reported as a proportion Selected References: Hoyt RE, Bowling LS. Reducing Readmissions for Congestive Heart Failure. Am Fam Physician 2001;63(8): Jha AK, Orav EJ, Epstein AM. Public Reporting of Discharge Planning and Rate of Readmissions. N Eng J Med 2009; 361(27): The Joint Commission. The Joint Commission s 2012 Disease-Specific Care Certification Manual: Advanced Certification in Heart Failure Addendum. Oakbrook Terrace, IL: Author Measure Algorithm: 27
29 28
30 Data Elements 29
31 Data Element Name: Admission Date Collected For: Definition: Collection Question: ACHF-01, ACHF-02, ACHF-03, ACHF-04, ACHF-05, ACHF-06, CAH-01.1, CAH-02.1, CAH-03, CAH-04, CAH-05, CAH-06, CAH-08.1, CAH-09.1, CAH -10.1, CSTK, HBIPS, Osteo, PBM, PC, SCA-03, SUB, TOB, The month, day, and year of admission to acute inpatient care. What is the date the patient was admitted to acute inpatient care? Format: Length: 10 MM-DD-YYYY (includes dashes) Allowable Values: Type: Date Occurs: 1 MM = Month (01-12) DD = Day (01-31) YYYY = Year (20xx) Notes for Abstraction: The intent of this data element is to determine the date that the patient was actually admitted to acute inpatient care. Because this data element is critical in determining the population for all measures, the abstractor should NOT assume that the claim information for the admission date is correct. If the abstractor determines through chart review that the date is incorrect, for purposes of abstraction, she/he should correct and override the downloaded value. If using claim information, the Statement Covers Period is not synonymous with the Admission Date and should not be used to abstract this data element. These are two distinctly different identifiers: The Admission Date (Form Locator 12) is purely the date the patient was admitted as an inpatient to the facility. The Statement Covers Period ( From and Through dates in Form Locator 6) identifies the span of service dates included in a particular claim. The From Date is the earliest date of service on the claim. For patients who are admitted to Observation status and subsequently admitted to acute inpatient care, abstract the date that the determination was made to admit to acute inpatient care and the order was written. Do not abstract the date that the patient was admitted to Observation. Example: Medical record documentation reflects that the patient was admitted to observation on xx. On xx the physician writes an order to admit to acute inpatient effective xx. The Admission Date would be abstracted as
32 20xx; the date the determination was made to admit to acute inpatient care and the order was written. If there are multiple inpatient orders, use the order that most accurately reflects the date that the patient was admitted. The admission date should not be abstracted from the earliest admission order without regards to substantiating documentation. If documentation suggests that the earliest admission order does not reflect the date the patient was admitted to inpatient care, the date should not be used. Example: Preoperative Orders are dated as xx with an order to admit to Inpatient. Postoperative Orders, dated xx, state to admit to acute inpatient. All other documentation supports that the patient presented to the hospital for surgery on xx. The admission date would be abstracted as xx. For newborns that are born within this hospital, the admission date is the date the baby was born. Sources: ONLY ALLOWABLE SOURCES Physician orders Face sheet UB-04, Field Location: 12 Excluded Data Sources UB-04, Field Location: 06 Additional Notes: Guidelines for Abstraction: Inclusion Exclusion None Admit to observation Arrival date 31
33 Data Element Name: Collected For: Advance Directive Executed ACHF-05, ACHFOP-07, Definition: Collection Question: Documentation in the medical record that an advance directive was executed. An advance directive are instructions given by individuals specifying what actions should be taken for their health in the event that they are no longer able to make decisions due to illness or incapacity, and appoints a person to make such decisions on their behalf. Was documentation present in the medical record that an advance directive was executed? Format: Length: 1 Type: Alphanumeric Occurs: 1 Allowable Values: Y (Yes) There was documentation present in the medical record of an advance directive. N (No) There was no documentation present in the medical record of an advance directive, or unable to determine from medical record documentation. Notes for Abstraction: If there is documentation of an advance directive present in the medical record, select Yes. See inclusion list for acceptable documentation of advance directive. Sources: History and physical Progress notes Physician orders Discharge summary Care Transition Record Consultation form Discharge planning form MOLST/POLST Forms Hospice referral Outpatient medical record Additional Notes: Collected for both inpatient and outpatient Guidelines for Abstraction: Inclusion Exclusion 32
34 Advance care plan Advance decision Advance directive Advance healthcare directive Health care proxy Living will MOLST (Medical Orders for Life-Sustaining Treatment) Personal directive POLST (Physician Orders for Life-Sustaining Treatment) Power of attorney for healthcare DNR orders Do Not Resuscitate Orders 33
35 Data Element Name: Collected For: Definition: Birthdate All Records The month, day, and year the patient was born. Note: Patient's age (in years) is calculated by Admission Date minus Birthdate. The algorithm to calculate age must use the month and day portion of admission date and birthdate to yield the most accurate age. For HBIPS discharge measures, i.e., HBIPS-1, 4, 5, 6, 7, patient's age (in years) is calculated by Discharge Date minus Birthdate. For event measures, i.e., HBIPS-2, 3, patient's age at time of event (in years) is calculated by Event Date minus Birthdate. The algorithm to calculate age must use the month and day portion of birthdate, and discharge date or event, as appropriate to yield the most accurate age. Collection Question: What is the patient s date of birth? Format: Length: 10 MM-DD-YYYY (includes dashes) Type: Date Occurs: 1 Allowable Values: MM = Month (01-12) DD = Day (01-31) YYYY = Year (1880-Current Year) Notes for Abstraction: Sources: Because this data element is critical in determining the population for all measures, the abstractor should NOT assume that the claim information for the birthdate is correct. If the abstractor determines through chart review that the date is incorrect, she/he should correct and override the downloaded value. If the abstractor is unable to determine the correct birthdate through chart review, she/he should default to the date of birth on the claim information. Emergency department record Face sheet Registration form 34
36 UB-04, Field Location: 10 Additional Notes: Guidelines for Abstraction: Inclusion Exclusion None None 35
37 Data Element Name: Collected For: Definition: Collection Question: Bisoprolol, Carvedilol, or Sustained-Release Metoprolol Prescribed for LVSD at Discharge ACHF-01, Documentation that bisoprolol, carvedilol, or sustained-release metoprolol was prescribed at discharge. Beta-blockers are agents which block betaadrenergic receptors, thereby decreasing the rate and force of heart contractions, and reducing blood pressure. Over time beta-blockers improve the heart s pumping ability. The marked beneficial effects of beta blockade has been well demonstrated in large-scale clinical trials of symptomatic patients with New York Heart Association (NYHA) class II-IV heat failure and reduced LVEF using bisoprolol, carvedilol, and sustainedrelease metoprolol succinate. Was bisoprolol, carvedilol, or sustained-release metoprolol prescribed for LVSD at discharge? Format: Length: 1 Type: Alphanumeric Occurs: 1 Allowable Values: Y (Yes) Bisoprolol, carvedilol, or sustained-release metoprolol was prescribed for LVSD at discharge. N (No) Bisoprolol, carvedilol, or sustained-release metoprolol was not prescribed for LVSD at discharge or unable to determine from medical record documentation. Notes for Abstraction: Only select "Yes" for those beta-blockers identified in the list of inclusions. No other beta-blockers will be accepted for this data element In determining whether bisoprolol, carvedilol, or sustained-release metoprolol succinate was prescribed at discharge, it is not uncommon to see conflicting documentation amongst different medical record sources. For example, the discharge summary may list one of these beta-blockers that is not included in any of the other discharge medication sources (e.g., discharge orders). All discharge medication documentation available in the chart should be reviewed and taken into account by the abstractor. In cases where there is bisoprolol, carvedilol, or sustainedrelease metoprolol succinate in one source that is not mentioned in other sources, it should be interpreted as a discharge medication (select "Yes") unless documentation elsewhere in the medical record suggests that it was NOT prescribed at discharge - Consider it a discharge medication in the absence of contradictory documentation. If documentation is contradictory (e.g., physician noted d/c carvedilol in the discharge orders, but carvedilol is listed in the discharge summary s discharge medication list), or after careful 36
38 examination of circumstances, context, timing, etc, documentation raises enough questions, the case should be deemed " Consider documentation of a hold on bisoprolol, carvedilol, or sustained-release metoprolol succinate after discharge in one location and a listing of that beta-blocker as a discharge medication in another location as contradictory ONLY if the timeframe on the hold is not defined (e.g., Hold bisoprolol ). Examples of a hold with a defined timeframe include Hold Toprol-XL x 2 days and Hold Coreg until after stress test. If bisoprolol, carvedilol, or sustained-release metoprolol succinate is NOT listed as a discharge medication, and there is only documentation of a hold or plan to delay initiation/restarting of the beta-blocker after discharge (e.g., Hold Toprol-XL x 2 days, Start Zebeta as outpatient, Hold Coreg ), select No. If two discharge summaries are included in the medical record, use the one with the latest date/time. If one or both are not dated or timed, and you cannot determine which was done last, use both. This also applies to discharge medication reconciliation forms. Use the dictated date/time over transcribed date/time, file date/time, etc. Examples: Two discharge summaries, one dictated 5/22 (day of discharge) and one dictated 5/27 - Use the 5/27 discharge summary. Two discharge medication reconciliation forms, one not dated and one dated 4/24 (day of discharge) - Use both. Disregard bisoprolol, carvedilol, or sustained-release metoprolol succinate documented only as a recommended medication for discharge (e.g., Recommend sending patient home on Coreg ). Documentation must be more clear that the beta-blocker was actually prescribed at discharge. Disregard documentation of bisoprolol, carvedilol, or sustainedrelease metoprolol succinate prescribed at discharge when noted only by medication class (e.g., Beta-Blocker Prescribed at Discharge: Yes on a core measures form). The beta-blocker prescribed must be listed by name. Sources: Nursing notes Progress notes Physician orders Physician s notes Discharge summary Medication administration record (MAR) Transfer sheet Discharge instruction sheet Medication reconciliation form Additional Notes: Guidelines for Abstraction: 37
39 Inclusion Bisoprolol Bisoprolol/fumarate Bisoprolol/hydrochlorothiazide Carvedilol Carvedilol phosphate Coreg Coreg CR Metoprolol succinate Toprol-XL Zebeta Ziac Exclusion All other beta-blocker medications other than those listed as inclusions. 38
40 Data Element Name: Collected For: Care Transition Record Transmitted ACHF-03, Definition: Collection Question: A care transition record is a document or set of documents containing standardized components specific to the patient s diagnosis, treatment, and care. A care transition record is transmitted to the next level of care provider no later than the seventh post-discharge day. Was a care transition record transmitted to the next level of care provider no later than the seventh post-discharge day? Format: Length: 1 Type: Alphanumeric Occurs: 1 Allowable Values: 1 The medical record contains a care transition record that was transmitted to the next level of care provider no later than the seventh post-discharge day. 2 The medical record contains a care transition record but was not transmitted to the next level of care provider by the seventh postdischarge day. 3 The medical record does not contain a care transition record, or unable to determine from medical record documentation. Notes for Abstraction: A care transition record may consist of one document or several documents which could be considered a care transition packet. The hospital must be able to identify which document(s) make up the care transition record and the hospital must identify what specific documents are transmitted to the next level of care provider. The care transition record could be in the form of a continuing care plan, discharge instruction form, or another patient-specific document (s) contained in the medical record. The first post-discharge day is defined as the day after discharge. The next level of care provider is the clinician, hospital or clinic responsible for managing the patient s heart failure after hospital discharge. The next level of care provider may be a primary care physician, cardiologist, advanced practice nurse (APN), or physician assistant (PA). If the patient has referrals to more than one provider for followup after discharge, transmission of the care transition record must include the next level of care provider. Methods for transmitting the care transition record include, but are not limited to: U.S. mail, , fax, EMR access, doctor's mailbox, medical transport personnel. Giving a copy of the care transition record to the patient DOES NOT comprise transmission. 39
41 If the hospital has an electronic medical record (EMR), abstraction is a two-step process: 1. Make a list of those next level of care providers who have complete access to the hospital EMR. 2. Check the list of those providers who have EMR access against the providers named on the care transition record. If the next level of provider noted on the care transition record matches the list of providers who have EMR access, select allowable value '1'. Sources: Aftercare discharge plan Care transition record Continuing care plan Discharge plan Discharge summary Medication reconciliation form Physician orders Progress notes Referral form Additional Notes: Guidelines for Abstraction: None Inclusion None Exclusion 40
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Heart Failure: Diagnosis and Treatment
 Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15
 Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services. Discharge Planning
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Medicare Patients: Overview The Centers for Medicare & Medicaid Services (), an agency within the Department
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Medicare Patients: Overview The Centers for Medicare & Medicaid Services (), an agency within the Department
Overview of the TJC/CMS VTE Core Measures
 Overview of the TJC/CMS VTE Core Measures CMS Specification Manual 4.2 January 1, 2013 June 30, 2013 Victoria Agramonte, RN, MSN Project Manager, IPRO VTE Regional Learning Sessions NYS Partnership for
Overview of the TJC/CMS VTE Core Measures CMS Specification Manual 4.2 January 1, 2013 June 30, 2013 Victoria Agramonte, RN, MSN Project Manager, IPRO VTE Regional Learning Sessions NYS Partnership for
November 15, 2013. Ann Laramee MS ANP-BC ACNS-BC CHFN FletcherAllen.org
 Advance Care Planning with Heart Failure: Results of a Primary Care Practitioners Needs Survey 5 th Annual Nursing Research and Evidence Based Practice Symposium November 15, 2013 Ann Laramee MS ANP-BC
Advance Care Planning with Heart Failure: Results of a Primary Care Practitioners Needs Survey 5 th Annual Nursing Research and Evidence Based Practice Symposium November 15, 2013 Ann Laramee MS ANP-BC
Heart Failure & Cardiac Rehabilitation
 Heart Failure & Cardiac Rehabilitation Karen Lui, RN, MS, MAACVPR SCACVPR Greenville May 3, 2014 1 I have no disclosures. 2 Outline New Professional Certification New AACVPR CR Guidelines New Heart Failure
Heart Failure & Cardiac Rehabilitation Karen Lui, RN, MS, MAACVPR SCACVPR Greenville May 3, 2014 1 I have no disclosures. 2 Outline New Professional Certification New AACVPR CR Guidelines New Heart Failure
OBJECTIVES AGING POPULATION AGING POPULATION AGING IMPACT ON MEDICARE AGING POPULATION
 OBJECTIVES Kimberly S. Hodge, PhDc, MSN, RN, ACNS-BC, CCRN- K Director, ACO Care Management & Clinical Nurse Specialist Franciscan ACO, Inc. Central Indiana Region Indianapolis, IN By the end of this session
OBJECTIVES Kimberly S. Hodge, PhDc, MSN, RN, ACNS-BC, CCRN- K Director, ACO Care Management & Clinical Nurse Specialist Franciscan ACO, Inc. Central Indiana Region Indianapolis, IN By the end of this session
Congestive Heart Failure Management Program
 Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1
 Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Numerator Details. - An acute or nonacute inpatient admission with a diagnosis of AOD (AOD Dependence
 Description Measure 0004: Initiation and Engagement of Alcohol and Other Drug Dependence Treatment (IET) (National Committee for Quality Assurance) The percentage of adolescent and adult patients with
Description Measure 0004: Initiation and Engagement of Alcohol and Other Drug Dependence Treatment (IET) (National Committee for Quality Assurance) The percentage of adolescent and adult patients with
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Mar. 31, 2011 (202) 690-6145. Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 690-6145. Improving Quality of Care for Medicare Patients: Accountable Care Organizations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
Advanced Heart Failure & Transplantation Fellowship Program
 Advanced Heart Failure & Transplantation Fellowship Program Curriculum I. Patient Care When on the inpatient Heart Failure and Transplant Cardiology service, the cardiology fellow will hold primary responsibility
Advanced Heart Failure & Transplantation Fellowship Program Curriculum I. Patient Care When on the inpatient Heart Failure and Transplant Cardiology service, the cardiology fellow will hold primary responsibility
Clarification of Patient Discharge Status Codes and Hospital Transfer Policies
 The Acute Inpatient Prospective Payment System Fact Sheet (revised November 2007), which provides general information about the Acute Inpatient Prospective Payment System (IPPS) and how IPPS rates are
The Acute Inpatient Prospective Payment System Fact Sheet (revised November 2007), which provides general information about the Acute Inpatient Prospective Payment System (IPPS) and how IPPS rates are
Communication and Information Deficits in Patients Discharged to Rehabilitation Facilities: An Evaluation of Five Acute Care Hospitals
 ORIGINAL RESEARCH Communication and Information Deficits in Patients Discharged to Rehabilitation Facilities: An Evaluation of Five Acute Care Hospitals Esteban Gandara, MD 1,2 Thomas Moniz, PharmD 1,3
ORIGINAL RESEARCH Communication and Information Deficits in Patients Discharged to Rehabilitation Facilities: An Evaluation of Five Acute Care Hospitals Esteban Gandara, MD 1,2 Thomas Moniz, PharmD 1,3
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology
 Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs)
") Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs) Senate Bill 832 directed the Oregon Health Authority (OHA) to develop standards for achieving integration of behavioral health
Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs) Senate Bill 832 directed the Oregon Health Authority (OHA) to develop standards for achieving integration of behavioral health
Preferred Practices and Performance Measures for Measuring and Reporting Care Coordination A CONSENSUS REPORT
 Preferred Practices and Performance Measures for Measuring and Reporting Care Coordination A CONSENSUS REPORT National Quality Forum The mission of the National Quality Forum is to improve the quality
Preferred Practices and Performance Measures for Measuring and Reporting Care Coordination A CONSENSUS REPORT National Quality Forum The mission of the National Quality Forum is to improve the quality
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
HEART FAILURE PERFORMANCE MEASURES: NEW AND UPDATED. Connie White-Williams, PhD, RN, FAAN University of Alabama at Birmingham
 HEART FAILURE PERFORMANCE MEASURES: NEW AND UPDATED Connie White-Williams, PhD, RN, FAAN University of Alabama at Birmingham DEVELOPMENT OF PERFORMANCE MEASURES American College of Cardiology Foundation
HEART FAILURE PERFORMANCE MEASURES: NEW AND UPDATED Connie White-Williams, PhD, RN, FAAN University of Alabama at Birmingham DEVELOPMENT OF PERFORMANCE MEASURES American College of Cardiology Foundation
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes
 Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
Maryland MOLST. Guide for Health Care Professionals. Maryland MOLST Training Task Force
 Maryland MOLST Guide for Health Care Professionals Maryland MOLST Training Task Force May 2012 Health Care Decision Making Guide for Health Care Professionals Introduction Section I: The Health Care Decision
Maryland MOLST Guide for Health Care Professionals Maryland MOLST Training Task Force May 2012 Health Care Decision Making Guide for Health Care Professionals Introduction Section I: The Health Care Decision
Meaningful Use. Medicare and Medicaid EHR Incentive Programs
 Meaningful Use Medicare and Medicaid Table of Contents What is Meaningful Use?... 1 Table 1: Patient Benefits... 2 What is an EP?... 4 How are Registration and Attestation Being Handled?... 5 What are
Meaningful Use Medicare and Medicaid Table of Contents What is Meaningful Use?... 1 Table 1: Patient Benefits... 2 What is an EP?... 4 How are Registration and Attestation Being Handled?... 5 What are
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
caresy caresync Chronic Care Management
 caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Follow-Up Visits after Heart Failure Hospitalizations: Impact of a Medication Reconciliation Clinic
 Follow-Up Visits after Heart Failure Hospitalizations: Impact of a Medication Reconciliation Clinic Sherry K. Milfred-LaForest, PharmD, BCPS Clinical Pharmacy Specialist, Cardiology and Organ Transplantation
Follow-Up Visits after Heart Failure Hospitalizations: Impact of a Medication Reconciliation Clinic Sherry K. Milfred-LaForest, PharmD, BCPS Clinical Pharmacy Specialist, Cardiology and Organ Transplantation
See page 331 of HEDIS 2013 Tech Specs Vol 2. HEDIS specs apply to plans. RARE applies to hospitals. Plan All-Cause Readmissions (PCR) *++
 *++") Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Transitions of Care Management Coding (TCM Code) Tutorial. 1. Introduction Meaning of moderately and high complexity 2
 Tutorial. 1. Introduction Meaning of moderately and high complexity 2") Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
KIH Cardiac Rehabilitation Program
 KIH Cardiac Rehabilitation Program For any further information Contact: +92-51-2870361-3, 2271154 Feedback@kih.com.pk What is Cardiac Rehabilitation Cardiac rehabilitation describes all measures used to
KIH Cardiac Rehabilitation Program For any further information Contact: +92-51-2870361-3, 2271154 Feedback@kih.com.pk What is Cardiac Rehabilitation Cardiac rehabilitation describes all measures used to
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
UB-04 Claim Form Instructions
 UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Provider Manual. Section 18.0 - Case Management and Disease Management
 Section 18.0 - Case Management and Disease Management 18.1.1 Introduction 18.2.1 Scope 18.3.1 Objectives 18.4.1 Procedures Case Management 18.4.1-A. Referrals 18.4.1-B. Case Management Mercy Maricopa Acute
Section 18.0 - Case Management and Disease Management 18.1.1 Introduction 18.2.1 Scope 18.3.1 Objectives 18.4.1 Procedures Case Management 18.4.1-A. Referrals 18.4.1-B. Case Management Mercy Maricopa Acute
Regulatory Compliance Policy No. COMP-RCC 4.03 Title:
 I. SCOPE: Regulatory Compliance Policy No. COMP-RCC 4.03 Page: 1 of 10 This policy applies to (1) Tenet Healthcare Corporation and its wholly-owned subsidiaries and affiliates (each, an Affiliate ); (2)
I. SCOPE: Regulatory Compliance Policy No. COMP-RCC 4.03 Page: 1 of 10 This policy applies to (1) Tenet Healthcare Corporation and its wholly-owned subsidiaries and affiliates (each, an Affiliate ); (2)
Update on New Coordination of Care and Transition of Care Coding
 Update on New Coordination of Care and Transition of Care Coding Michele Olivier ACP Colorado Chapter February 5, 2015 (303) 801-0123 Agenda Introduction Chronic Care Management Coding Advanced Care Planning
Update on New Coordination of Care and Transition of Care Coding Michele Olivier ACP Colorado Chapter February 5, 2015 (303) 801-0123 Agenda Introduction Chronic Care Management Coding Advanced Care Planning
V. Utilization Management (UM) Program
 Program") V. Utilization Management (UM) Program Overview Better Health Network s Utilization Management (UM) Program is designed to provide quality, cost-effective and medically necessary services while meeting
V. Utilization Management (UM) Program Overview Better Health Network s Utilization Management (UM) Program is designed to provide quality, cost-effective and medically necessary services while meeting
RECOMMENDATIONS FOR DEFINING AND DEMONSTRATING MEANINGFUL USE OF CERTIFIED ELECTRONIC HEALTH RECORDS (EHRs)
") RECOMMENDATIONS FOR DEFINING AND DEMONSTRATING MEANINGFUL USE OF CERTIFIED ELECTRONIC HEALTH RECORDS (EHRs) I. Guiding Principles for Ensuring Widespread Use of Certified EHRs A. Timing of EHR Implementation
RECOMMENDATIONS FOR DEFINING AND DEMONSTRATING MEANINGFUL USE OF CERTIFIED ELECTRONIC HEALTH RECORDS (EHRs) I. Guiding Principles for Ensuring Widespread Use of Certified EHRs A. Timing of EHR Implementation
ATLANTIC and OPTIMUS ACCOUNTABLE CARE ORGANIZATIONs CMS QUALITY MEASURES
 CARE / PATIENT SAFETY ATLANTIC and OPTIMUS ACCOUNTABLE CARE ORGANIZATIONs CMS QUALITY MEASURES This tool is for REFERENCE USE ONLY and serves as an Emergency Backup Documentation Tool (downtime procedure
CARE / PATIENT SAFETY ATLANTIC and OPTIMUS ACCOUNTABLE CARE ORGANIZATIONs CMS QUALITY MEASURES This tool is for REFERENCE USE ONLY and serves as an Emergency Backup Documentation Tool (downtime procedure
EMR Name/ Model. meridianemr 4.2 CCHIT 2011 certified
 EMR Name/ Model EMR Vendor meridianemr 4.2 CCHIT 2011 certified meridianemr, Inc Core Set of Measures Objective Stage 1 Objectives Stage 1 Measures EMR Module/ Feature 1 Use CPOE for medication orders
EMR Name/ Model EMR Vendor meridianemr 4.2 CCHIT 2011 certified meridianemr, Inc Core Set of Measures Objective Stage 1 Objectives Stage 1 Measures EMR Module/ Feature 1 Use CPOE for medication orders
GAO HOSPITAL QUALITY DATA. HHS Should Specify Steps and Time Frame for Using Information Technology to Collect and Submit Data
 GAO United States Government Accountability Office Report to the Committee on Finance, U.S. Senate April 2007 HOSPITAL QUALITY DATA HHS Should Specify Steps and Time Frame for Using Information Technology
GAO United States Government Accountability Office Report to the Committee on Finance, U.S. Senate April 2007 HOSPITAL QUALITY DATA HHS Should Specify Steps and Time Frame for Using Information Technology
An Overview of Meaningful Use: FAQs
 An Overview of Meaningful Use: FAQs On Feb. 17, 2009, President Obama signed the American Recovery and Reinvestment Act of 2009 (ARRA) into law. This new law includes provisions (known as the HITECH Act)
An Overview of Meaningful Use: FAQs On Feb. 17, 2009, President Obama signed the American Recovery and Reinvestment Act of 2009 (ARRA) into law. This new law includes provisions (known as the HITECH Act)
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medicare Savings and Reductions in Rehospitalizations Associated with Home Health Use
 Medicare Savings and Reductions in Rehospitalizations Associated with Home Health Use June 23, 2011 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Table of
Medicare Savings and Reductions in Rehospitalizations Associated with Home Health Use June 23, 2011 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Table of
Pushing the Envelope of Population Health
 Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
"2015 ACO quality measures- What's new? How can we be successful?"
 "2015 ACO quality measures- What's new? How can we be successful?" ACO Announcements Reminders: ACO Notifications, Requests for Tax ID information from PECOS, Upcoming Boardline Upcoming Specialty Initiative
"2015 ACO quality measures- What's new? How can we be successful?" ACO Announcements Reminders: ACO Notifications, Requests for Tax ID information from PECOS, Upcoming Boardline Upcoming Specialty Initiative
Section 6. Medical Management Program
 Section 6. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Section 6. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
Measure Information Form (MIF) #275, adapted for quality measurement in Medicare Accountable Care Organizations
 #275, adapted for quality measurement in Medicare Accountable Care Organizations") ACO #9 Prevention Quality Indicator (PQI): Ambulatory Sensitive Conditions Admissions for Chronic Obstructive Pulmonary Disease (COPD) or Asthma in Older Adults Data Source Measure Information Form (MIF)
ACO #9 Prevention Quality Indicator (PQI): Ambulatory Sensitive Conditions Admissions for Chronic Obstructive Pulmonary Disease (COPD) or Asthma in Older Adults Data Source Measure Information Form (MIF)
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary. http://www.cms.gov/ehrincentiveprograms/
 Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary 2010 What are the Requirements of Stage 1 Meaningful Use? Basic Overview of Stage 1 Meaningful Use: Reporting period
Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary 2010 What are the Requirements of Stage 1 Meaningful Use? Basic Overview of Stage 1 Meaningful Use: Reporting period
Functional Improvement for Heart Failure Patients After Left Ventricular Assistive Device Placement in a Free Standing Rehabilitation Hospital
 Functional Improvement for Heart Failure Patients After Left Ventricular Assistive Device Placement in a Free Standing Rehabilitation Hospital Vittal R. Nagar, M.D, PhDc PGY II Mentor: Robert Nickerson,
Functional Improvement for Heart Failure Patients After Left Ventricular Assistive Device Placement in a Free Standing Rehabilitation Hospital Vittal R. Nagar, M.D, PhDc PGY II Mentor: Robert Nickerson,
Chapter 2. Medical Management and Quality Improvement
 Medical Management Overview...3 Introduction...3 Objectives...3 Important Program Points...3 Prior Authorization...4 Overview...4 MedicareBlue PPO Covered Items and Services...4 Medical Policy...5 Prior
Medical Management Overview...3 Introduction...3 Objectives...3 Important Program Points...3 Prior Authorization...4 Overview...4 MedicareBlue PPO Covered Items and Services...4 Medical Policy...5 Prior
Successful Heart Failure Management Nurse/NP Run Clinics
 Dagmar Knot RN BScN CCCN Transplant Coordination Team Leader Organ Transplant Center KFSHRC Riyadh, KSA Heart Failure Nurses Role, responsibilities & education Successful Heart Failure Management Nurse/NP
Dagmar Knot RN BScN CCCN Transplant Coordination Team Leader Organ Transplant Center KFSHRC Riyadh, KSA Heart Failure Nurses Role, responsibilities & education Successful Heart Failure Management Nurse/NP
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety
: Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety") Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Community health care services Alternatives to acute admission & Facilitated discharge options. Directory
 Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Implementing Chronic Care Management (CCM) - CPT 99490
 - CPT 99490") Implementing Chronic Care Management (CCM) - CPT 99490 Dulcian, Inc. May 2015 The Need Population-based statistics published by the Centers for Medicare and Medicaid Services (CMS) tell the story. Most
Implementing Chronic Care Management (CCM) - CPT 99490 Dulcian, Inc. May 2015 The Need Population-based statistics published by the Centers for Medicare and Medicaid Services (CMS) tell the story. Most
CMS-1600-P 201. As we discussed in the CY 2013 PFS final rule with comment period, we are
 CMS-1600-P 201 I. Complex Chronic Care Management Services As we discussed in the CY 2013 PFS final rule with comment period, we are committed to primary care and we have increasingly recognized care management
CMS-1600-P 201 I. Complex Chronic Care Management Services As we discussed in the CY 2013 PFS final rule with comment period, we are committed to primary care and we have increasingly recognized care management
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014
 CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
Oregon Statewide Performance Improvement Project: Diabetes Monitoring for People with Diabetes and Schizophrenia or Bipolar Disorder
 Oregon Statewide Performance Improvement Project: Diabetes Monitoring for People with Diabetes and Schizophrenia or Bipolar Disorder November 14, 2013 Prepared by: Acumentra Health 1. Study Topic This
Oregon Statewide Performance Improvement Project: Diabetes Monitoring for People with Diabetes and Schizophrenia or Bipolar Disorder November 14, 2013 Prepared by: Acumentra Health 1. Study Topic This
National Hospital Inpatient Quality Reporting Measures Specifications Manual
 National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.2 Release Notes Completed: June 25, 2012 Guidelines for Using Release Notes Release Notes 4.2 provide
National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.2 Release Notes Completed: June 25, 2012 Guidelines for Using Release Notes Release Notes 4.2 provide
Clinical pathway concept - a key to seamless care
 SECTION 5: PATIENT SAFETY AND QUALITY ASSURANCE 1 Clinical pathway concept - a key to seamless care Audrey Janoly-Dumenil, Hôpital Edouard Herriot, CHU Lyon Marie-Camille Chaumais, Hôpital Antoine Béclère,
SECTION 5: PATIENT SAFETY AND QUALITY ASSURANCE 1 Clinical pathway concept - a key to seamless care Audrey Janoly-Dumenil, Hôpital Edouard Herriot, CHU Lyon Marie-Camille Chaumais, Hôpital Antoine Béclère,
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION
 LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
Reducing Readmissions with Predictive Analytics
 Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
2016 Physician Quality Reporting System (PQRS) Measure Specification and Measure Flow Guide for Claims and Registry Reporting of Individual Measures
 Measure Specification and Measure Flow Guide for Claims and Registry Reporting of Individual Measures") 2016 Physician Quality Reporting System (PQRS) Measure Specification and Measure Flow Guide for Claims and Registry Reporting of Individual Measures Utilized by Individual Eligible Professionals for Claims
2016 Physician Quality Reporting System (PQRS) Measure Specification and Measure Flow Guide for Claims and Registry Reporting of Individual Measures Utilized by Individual Eligible Professionals for Claims
IC 3 : Improving Continuous Cardiac Care Quality Improvement in Practice
 IC 3 : Improving Continuous Cardiac Care Quality Improvement in Practice Presenter Disclosure Information Paul Chan, MD FINANCIAL DISCLOSURE: None FUNDING FOR THE IC3 PROGRAM: Bristol-Myers Squibb / Sanofi
IC 3 : Improving Continuous Cardiac Care Quality Improvement in Practice Presenter Disclosure Information Paul Chan, MD FINANCIAL DISCLOSURE: None FUNDING FOR THE IC3 PROGRAM: Bristol-Myers Squibb / Sanofi
Psychiatrists and Reporting on Meaningful Use Stage 1. August 6, 2012
 Psychiatrists and Reporting on Meaningful Use Stage 1 August 6, 2012 Quick Overview Functional Measures Providers (tracked by NPI) must report on 15 core objectives and associated measures and 5 objectives
Psychiatrists and Reporting on Meaningful Use Stage 1 August 6, 2012 Quick Overview Functional Measures Providers (tracked by NPI) must report on 15 core objectives and associated measures and 5 objectives
Chapter Three Accountable Care Organizations
 Chapter Three Accountable Care Organizations One of the most talked-about changes in health care delivery in recent decades is Accountable Care Organizations, or ACOs. Having gained the attention of both
Chapter Three Accountable Care Organizations One of the most talked-about changes in health care delivery in recent decades is Accountable Care Organizations, or ACOs. Having gained the attention of both
Breathe With Ease. Asthma Disease Management Program
 Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Chapter 4 Health Care Management Unit 1: Care Management
 Chapter 4 Health Care Unit 1: Care In This Unit Topic See Page Unit 1: Care Care 2 6 Emergency 7 4.1 Care Healthcare Healthcare (HMS), Highmark Blue Shield s medical management division, is responsible
Chapter 4 Health Care Unit 1: Care In This Unit Topic See Page Unit 1: Care Care 2 6 Emergency 7 4.1 Care Healthcare Healthcare (HMS), Highmark Blue Shield s medical management division, is responsible
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
WHAT IS MEDICAL MANAGEMENT? WHAT IS THE PURPOSE OF MEDICAL MANAGEMENT?
 WHAT IS MEDICAL MANAGEMENT? How health plans make decisions to approve payment for medical treatment is a poorly understood part of the healthcare system. One part of the process, known as medical management,
WHAT IS MEDICAL MANAGEMENT? How health plans make decisions to approve payment for medical treatment is a poorly understood part of the healthcare system. One part of the process, known as medical management,
Accountable Care Organization 2015 Program Analysis Quality Performance Standards Narrative Measure Specifications
 January 9, 2015 Accountable Care Organization 2015 Program Analysis Quality Performance Standards Narrative Measure Specifications Prepared for (The Pioneer ACO Model) Division of Accountable Care Organization
January 9, 2015 Accountable Care Organization 2015 Program Analysis Quality Performance Standards Narrative Measure Specifications Prepared for (The Pioneer ACO Model) Division of Accountable Care Organization
Taming Of The Queue VI. Christine Struthers APN Cardiac Telehealth University of Ottawa Heart Institute
 Taming Of The Queue VI Christine Struthers APN Cardiac Telehealth University of Ottawa Heart Institute March 2009 The Heart Failure Continuum 2 Leadership. Knowledge. Community. HF Readmissions Hospital
Taming Of The Queue VI Christine Struthers APN Cardiac Telehealth University of Ottawa Heart Institute March 2009 The Heart Failure Continuum 2 Leadership. Knowledge. Community. HF Readmissions Hospital
Data Collection Guide Emergency Department Transfer Communication Measures
 Data Collection Guide Emergency Department Transfer Communication Measures January 2015 Prepared by Stratis Health in collaboration with Dr. Jill Klingner from the University of Minnesota Rural Health
Data Collection Guide Emergency Department Transfer Communication Measures January 2015 Prepared by Stratis Health in collaboration with Dr. Jill Klingner from the University of Minnesota Rural Health
The Joint Commission Advanced DSC Certification for Inpatient Diabetes Care
 The Joint Commission Advanced DSC Certification for Inpatient Diabetes Care November 12, 2013 Caroline Isbey RN, MSN, CDE Associate Director Teresa Gomez Associate Project Director Specialist-SSM Carol
The Joint Commission Advanced DSC Certification for Inpatient Diabetes Care November 12, 2013 Caroline Isbey RN, MSN, CDE Associate Director Teresa Gomez Associate Project Director Specialist-SSM Carol
Frequently Asked Questions Regarding At Home and Inpatient Hospice Care
 Frequently Asked Questions Regarding At Home and Inpatient Hospice Care Contents Page: Topic Overview Assistance in Consideration Process Locations in Which VNA Provides Hospice Care Determination of Type
Frequently Asked Questions Regarding At Home and Inpatient Hospice Care Contents Page: Topic Overview Assistance in Consideration Process Locations in Which VNA Provides Hospice Care Determination of Type
BlueAdvantage SM Health Management
 BlueAdvantage SM Health Management BlueAdvantage member benefits include access to a comprehensive health management program designed to encompass total health needs and promote access to individualized,
BlueAdvantage SM Health Management BlueAdvantage member benefits include access to a comprehensive health management program designed to encompass total health needs and promote access to individualized,
DRAFT POLICY & PROCEDURE
 DRAFT POLICY & PROCEDURE Current Version Effective Date: Next Review Date: Page 1 of 5 Title: Author: The Physician Orders for Life- Sustaining Treatment (POLST) Creation Date: Introduction: The Nevada
DRAFT POLICY & PROCEDURE Current Version Effective Date: Next Review Date: Page 1 of 5 Title: Author: The Physician Orders for Life- Sustaining Treatment (POLST) Creation Date: Introduction: The Nevada
8/14/2012 California Dual Demonstration DRAFT Quality Metrics
 Stakeholder feedback is requested on the following: 1) metrics 69 through 94; and 2) withhold measures for years 1, 2, and 3. Steward/ 1 Antidepressant medication management Percentage of members 18 years
Stakeholder feedback is requested on the following: 1) metrics 69 through 94; and 2) withhold measures for years 1, 2, and 3. Steward/ 1 Antidepressant medication management Percentage of members 18 years
Summary Evaluation of the Medicare Lifestyle Modification Program Demonstration and the Medicare Cardiac Rehabilitation Benefit
 The Centers for Medicare & Medicaid Services' Office of Research, Development, and Information (ORDI) strives to make information available to all. Nevertheless, portions of our files including charts,
The Centers for Medicare & Medicaid Services' Office of Research, Development, and Information (ORDI) strives to make information available to all. Nevertheless, portions of our files including charts,
Introduction. Mary Collier RN, MSN. Monica Worrell RN,MSN
 UC Health Introduction Mary Collier RN, MSN Monica Worrell RN,MSN OBJECTIVES Discuss Evidence Based Practice Highlight UC Health Medical Centers Heart Failure Clinical Practice Guidelines Share our Heart
UC Health Introduction Mary Collier RN, MSN Monica Worrell RN,MSN OBJECTIVES Discuss Evidence Based Practice Highlight UC Health Medical Centers Heart Failure Clinical Practice Guidelines Share our Heart
Population Health Management
 Population Health Management 1 Population Health Management At a Glance The MedStar Medical Management Department is responsible for managing health care resources for MedStar Select Health Plan. Our goal
Population Health Management 1 Population Health Management At a Glance The MedStar Medical Management Department is responsible for managing health care resources for MedStar Select Health Plan. Our goal
General Practitioner
 Palliative Care/End of Life Related Fees Service Type Fee code When to use General Practitioner Palliative Care Planning 14063 Once a patient living in the community (own or family home or assisted living;
Palliative Care/End of Life Related Fees Service Type Fee code When to use General Practitioner Palliative Care Planning 14063 Once a patient living in the community (own or family home or assisted living;
Reporting Period: For Stage 2, the reporting period must be the entire Federal Fiscal Year.
 Eligible Hospital and Critical Access Hospital (CAH) Attestation Worksheet for Stage 2 of the Medicare Electronic Health Record (EHR) Incentive Program The Eligible Hospital and CAH Attestation Worksheet
Eligible Hospital and Critical Access Hospital (CAH) Attestation Worksheet for Stage 2 of the Medicare Electronic Health Record (EHR) Incentive Program The Eligible Hospital and CAH Attestation Worksheet
GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS
 GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the