Your Cost If You Use a Participating Provider
|
|
|
- James Hutchinson
- 10 years ago
- Views:
Transcription
1

2
3
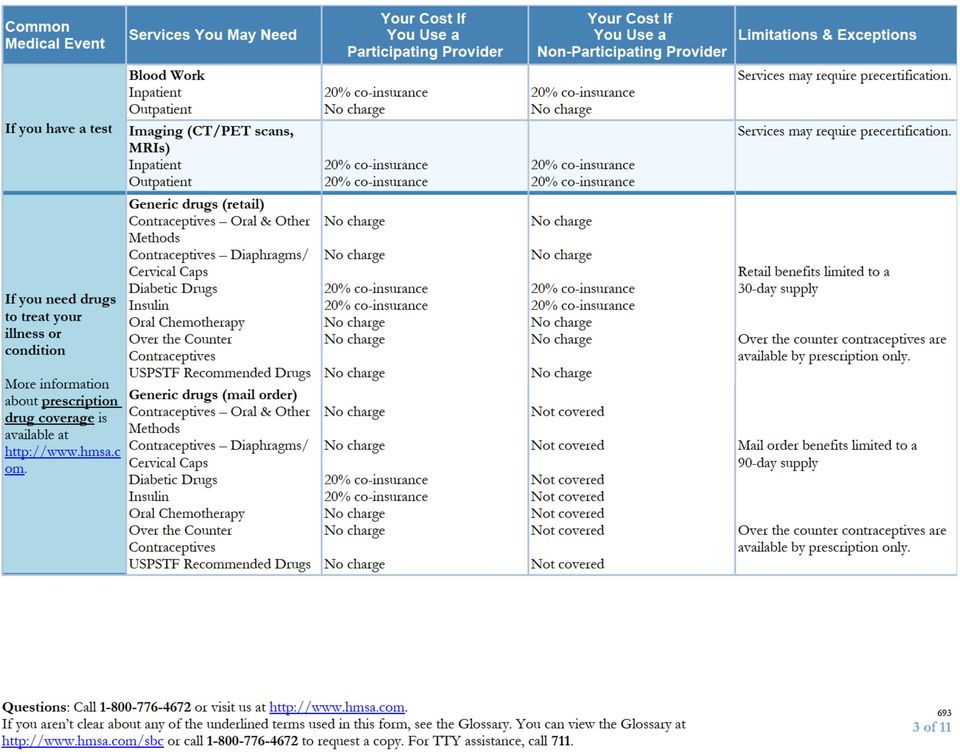
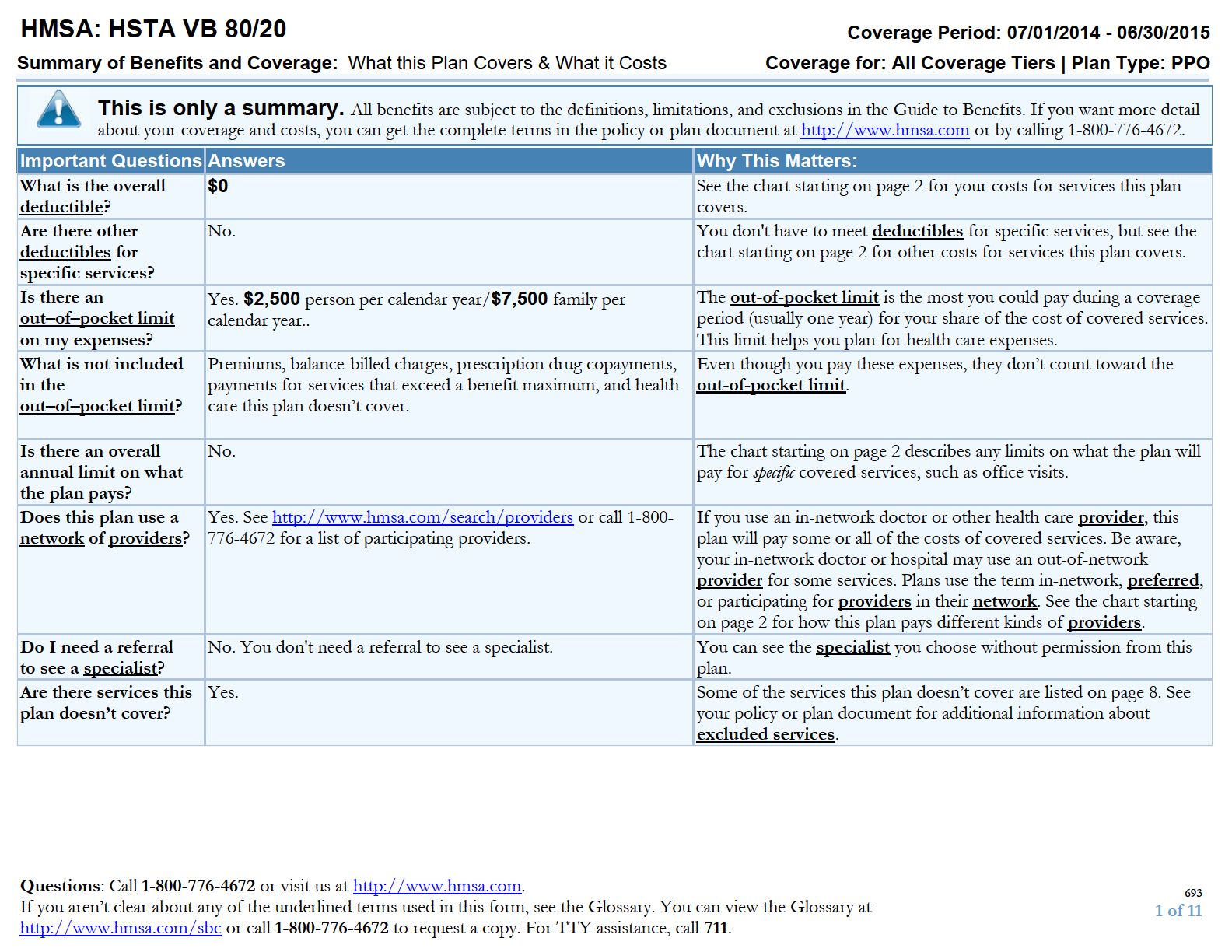
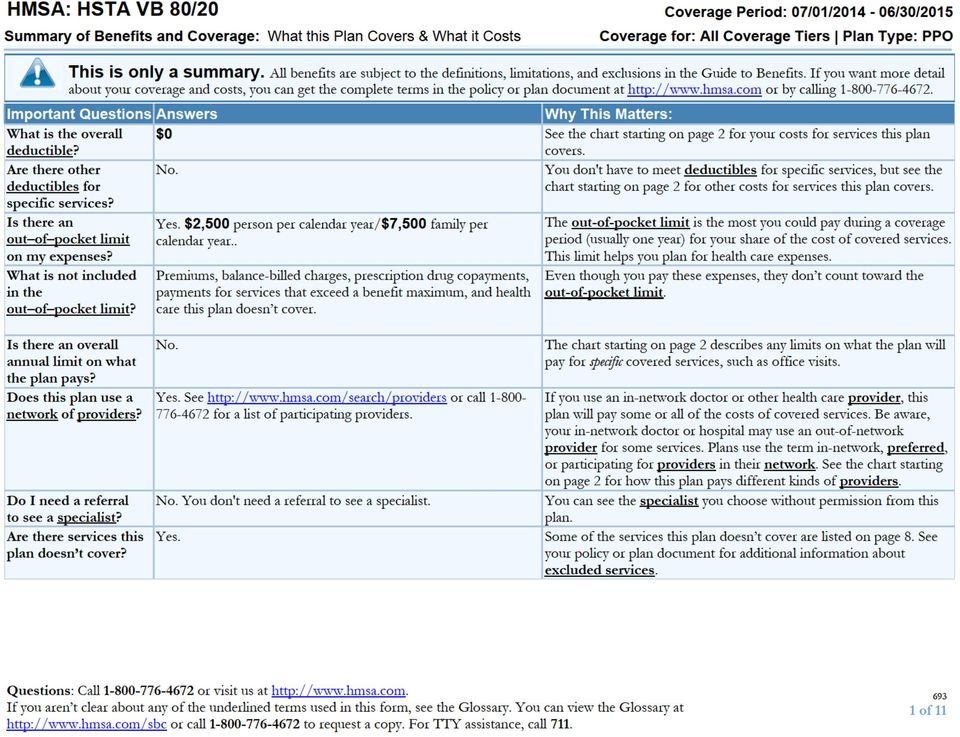
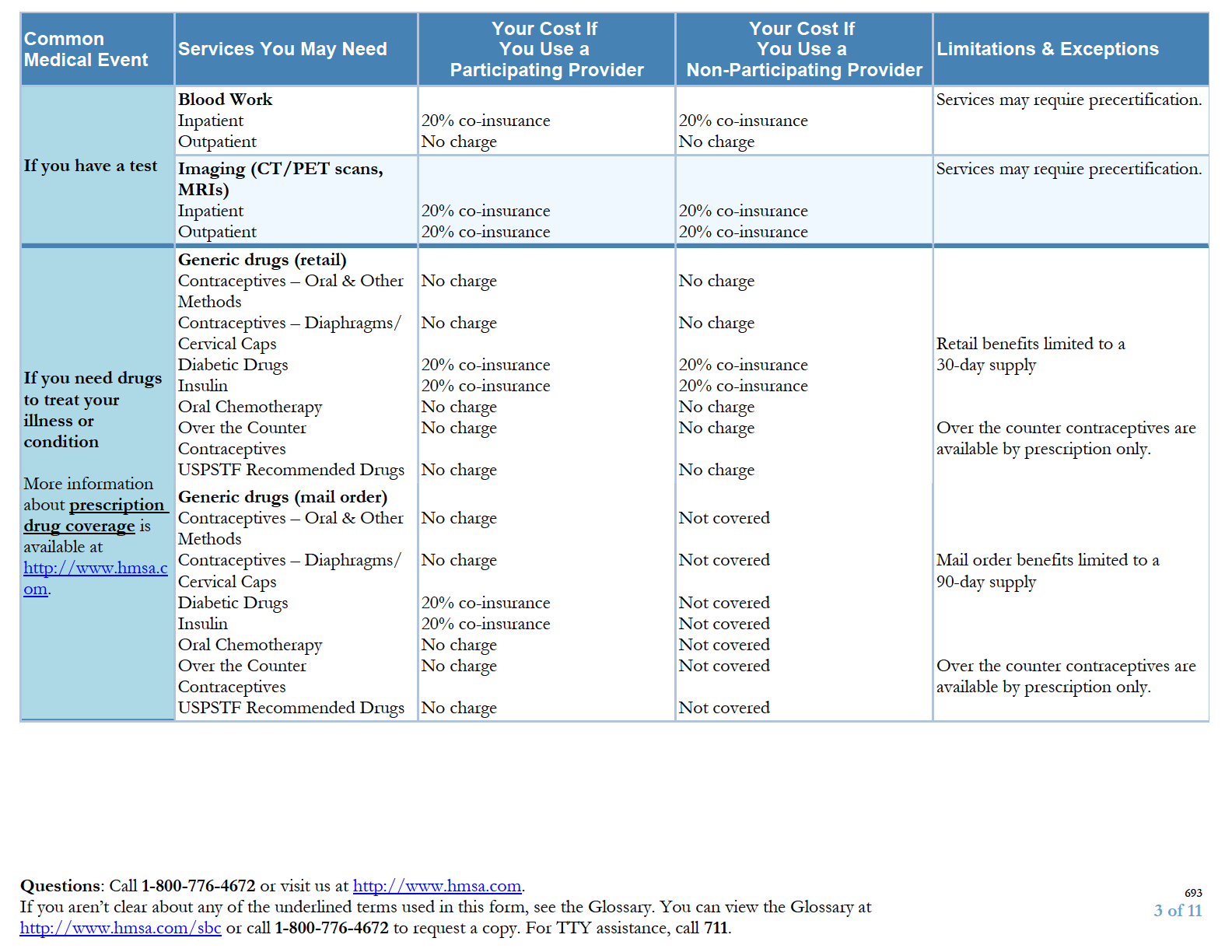
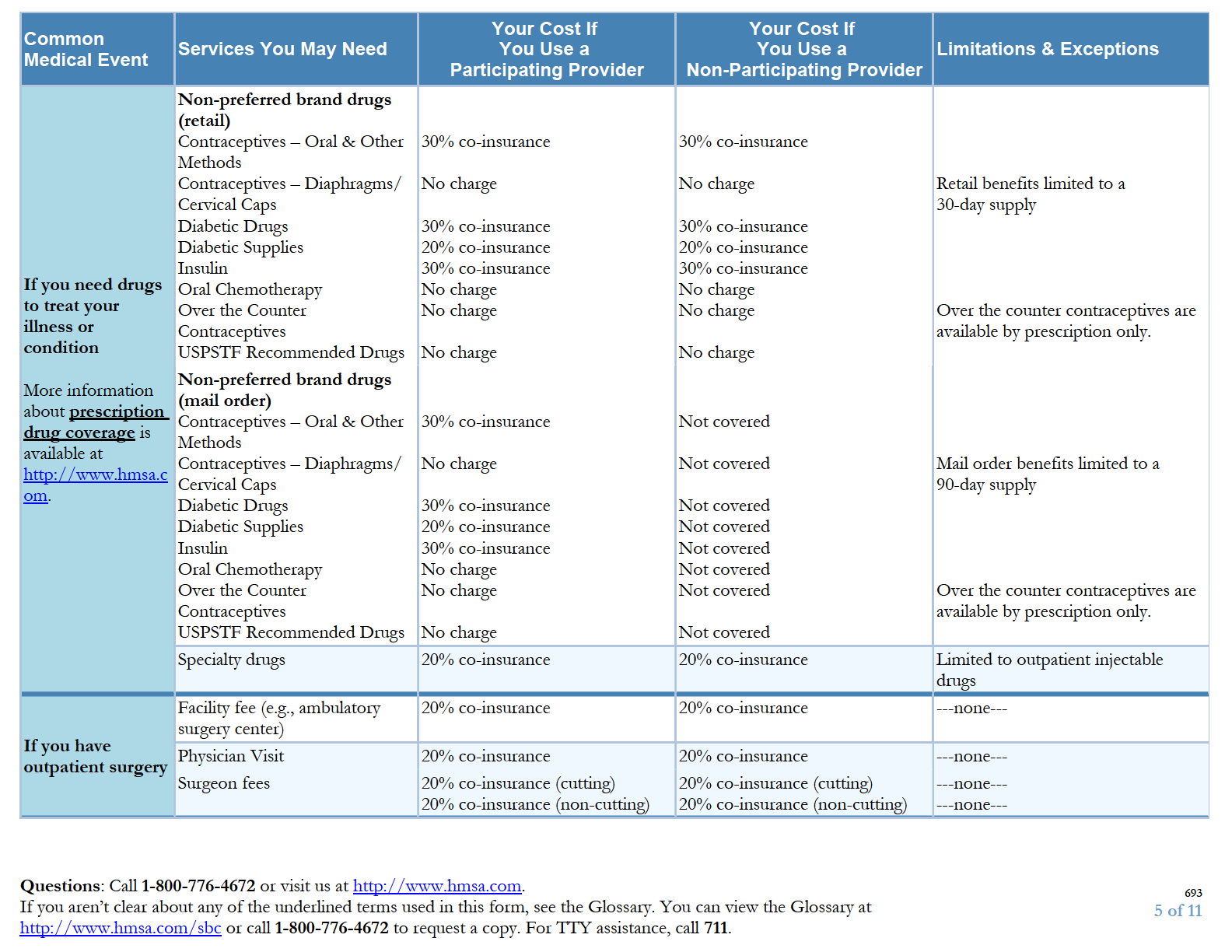
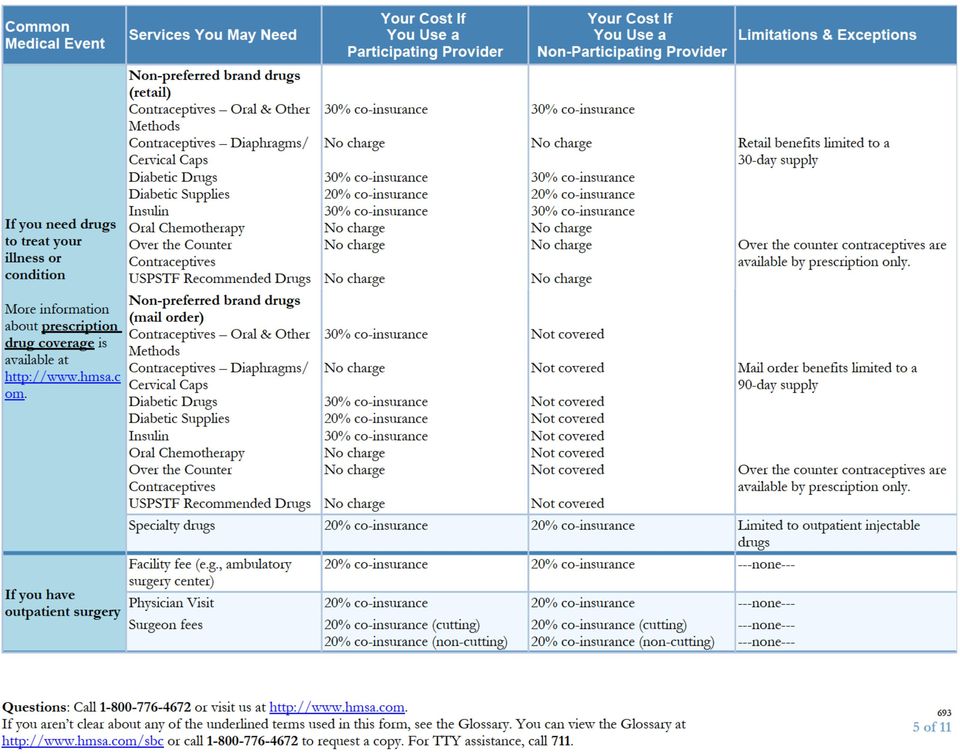
4 Common Medical Event Services You May Need Your Cost If You Use a Participating Provider Your Cost If You Use a Non-Participating Provider Limitations & Exceptions If you need drugs to treat your illness or condition More information about prescription drug coverage is available at om. Preferred brand drugs (retail) Contraceptives Oral & Other Methods Contraceptives Diaphragms/ Cervical Caps Diabetic Drugs Diabetic Supplies Insulin Oral Chemotherapy Over the Counter Contraceptives USPSTF Recommended Drugs Preferred brand drugs (mail order) Contraceptives Oral & Other Methods Contraceptives Diaphragms/ Cervical Caps Diabetic Drugs Diabetic Supplies Insulin Oral Chemotherapy Over the Counter Contraceptives USPSTF Recommended Drugs Retail benefits limited to a 30-day supply Over the counter contraceptives are available by prescription only. Mail order benefits limited to a 90-day supply Over the counter contraceptives are available by prescription only. Questions: Call or visit us at If you aren t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at or call to request a copy. For TTY assistance, call of 11
 Contraceptives Oral & Other Methods Contraceptives Diaphragms/ Cervical Caps Diabetic Drugs Diabetic Supplies Insulin Oral Chemotherapy")
5

6


7

8

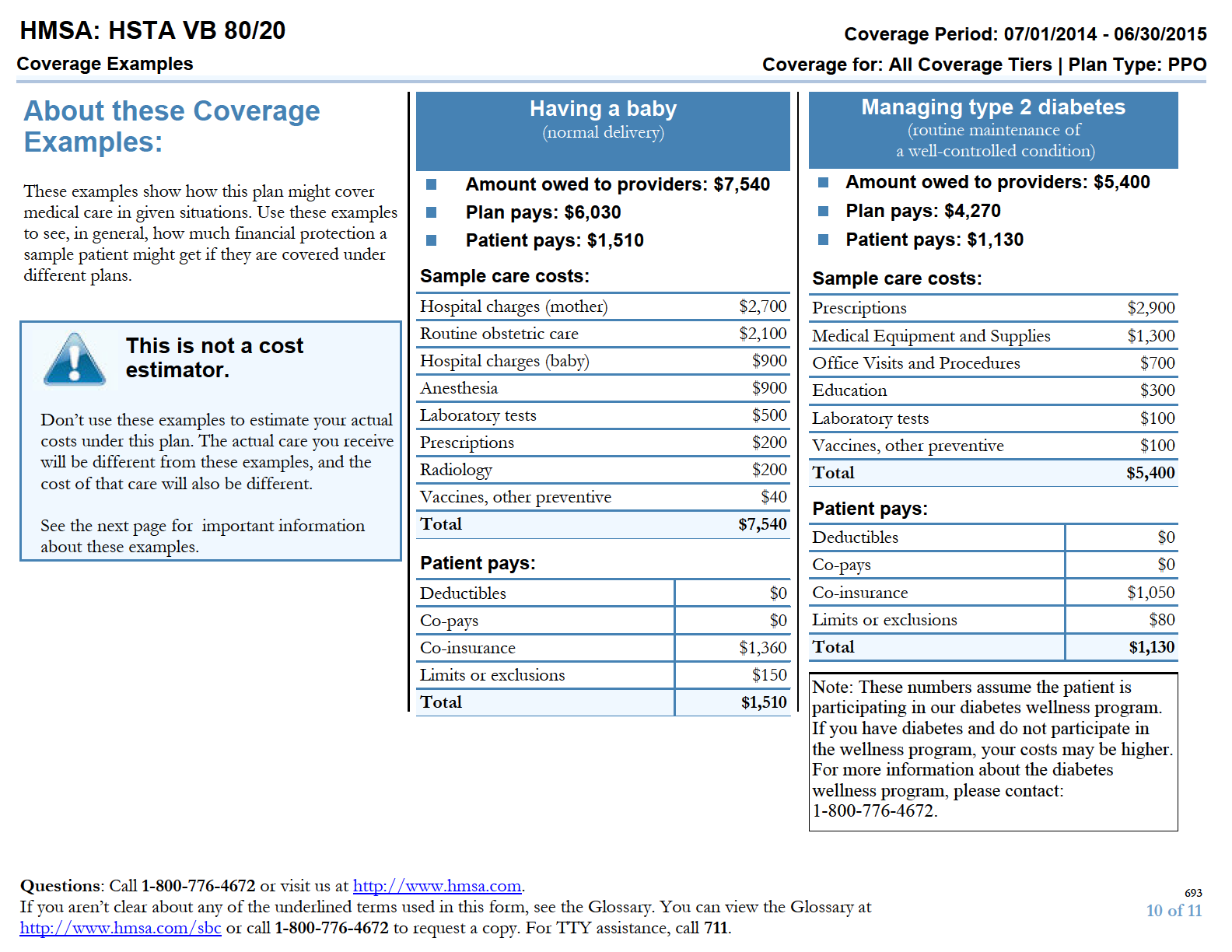
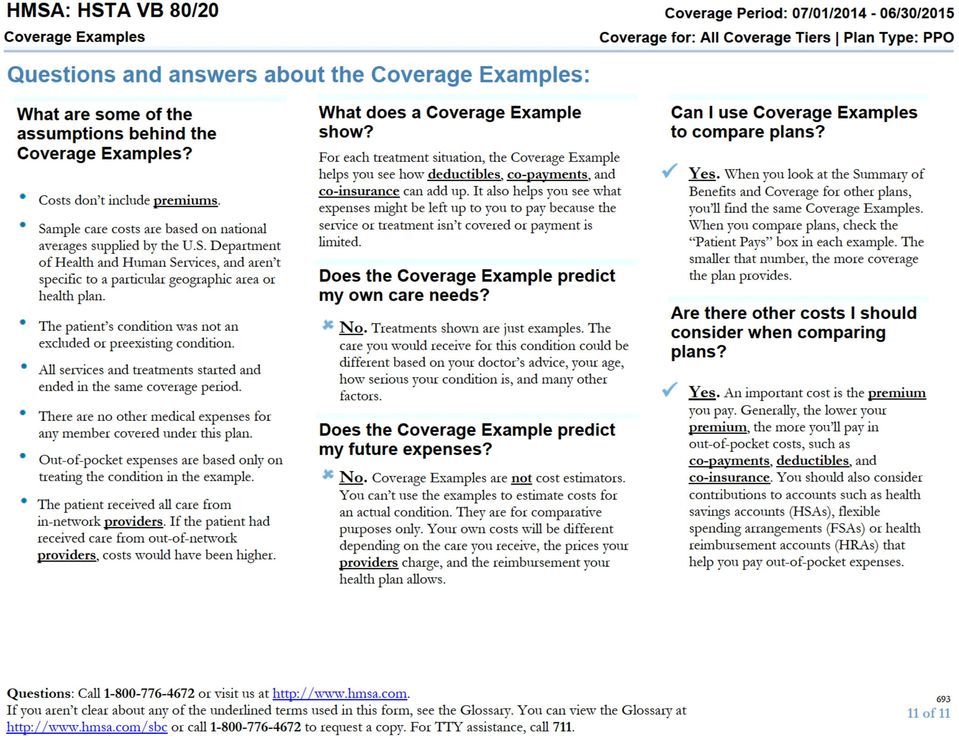
9 Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact: For group health coverage subject to ERISA, you must submit a written request for an appeal to: HMSA Member Advocacy and Appeals, P.O. Box 1958, Honolulu, Hawaii If you have any questions about appeals, you can call us at (808) or toll free at You may also contact the Department of Labor s Employee Benefits Security Administration at EBSA (3272) or You may also file a grievance with the Insurance Commissioner. You must send the request to the Insurance Commissioner at: Hawaii Insurance Division, ATTN: Health Insurance Branch External Appeals, 335 Merchant Street, Room 213, Honolulu, Hawaii Telephone: (808) For non-federal governmental group health plans and church plans that are group health plans, you must submit a written request for an appeal to: HMSA Member Advocacy and Appeals, P.O. Box 1958, Honolulu, Hawaii If you have any questions about appeals, you can call us at (808) or toll free at You may also file a grievance with the Insurance Commissioner. You must send the request to the Insurance Commissioner at: Hawaii Insurance Division, ATTN: Health Insurance Branch External Appeals, 335 Merchant Street, Room 213, Honolulu, Hawaii Telephone: (808) If you disagree with our appeals decision and coverage is insured (i.e. fully insured) you must request review by an Independent Review Organization (IRO) selected by the Insurance Commissioner. You must send the request to the Insurance Commissioner at: Hawaii Insurance Division, ATTN: Health Insurance Branch External Appeals, 335 Merchant Street, Room 213, Honolulu, Hawaii Telephone: (808) If coverage is self-funded, you must request review by an Independent Review Organization (IRO) selected by HMSA at random from a panel of three IROs. Send written requests to: HMSA Member Advocacy and Appeals, P.O. Box 1958, Honolulu, Hawaii, Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as "minimum essential coverage". This plan or policy does provide minimum essential coverage. Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides. Language Access Services: Spanish (Español): Para obtener asistencia en Español, llame al Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa Chinese ( 中 文 ): 如 果 需 要 中 文 的 帮 助, 请 拨 打 这 个 号 码 Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' To see examples of how this plan might cover costs for a sample medical situation, see the next page. Questions: Call or visit us at If you aren t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at or call to request a copy. For TTY assistance, call of 11
 or http://www.dol.gov/ebsa/healthreform.")
10

11
HMSA: MED 867/DRG 777 Coverage Period: 01/01/2016-12/31/2016
 HMSA: MED 867/DRG 777 Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual / Family Plan Type: PPO This is only a summary.
HMSA: MED 867/DRG 777 Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual / Family Plan Type: PPO This is only a summary.
HMSA's Bronze PPO 6600
 HMSA's Bronze PPO 6600 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage for: Individual / Family Plan Type: PPO This is only a summary.
HMSA's Bronze PPO 6600 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2015-12/31/2015 Coverage for: Individual / Family Plan Type: PPO This is only a summary.
Ultimate PPO Coverage Period: Beginning on or after 1/1/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-888-256-3650. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-888-256-3650. Important
Enhanced Exclusive HMO for Small Business $55 Coverage Period: Beginning On or After 1/1/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-888-256-3520. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-888-256-3520. Important
Panther Basic: UPMC Health Plan Coverage Period: 07/01/2015-06/30/2016 Summary of Coverage: What this Plan Covers & What it Costs
 Panther Basic: UPMC Health Plan Coverage Period: 07/01/2015-06/30/2016 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: All coverage levels Plan Type: HSA PPO This is only a summary.
Panther Basic: UPMC Health Plan Coverage Period: 07/01/2015-06/30/2016 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: All coverage levels Plan Type: HSA PPO This is only a summary.
Sutter Health Plus: SG Silver Copay $45 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling 1-855-315-5800. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling 1-855-315-5800. Important
Important Questions Answers Why this Matters:
 Sutter Health Plus: Schools Insurance Group_HDHP_HE06/HE56 Coverage Period: 07/01/2015 06/30/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete
Sutter Health Plus: Schools Insurance Group_HDHP_HE06/HE56 Coverage Period: 07/01/2015 06/30/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: Other
 Kaiser Permanente: Kaiser Permanente Oregon Standard Gold Plan Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family
Kaiser Permanente: Kaiser Permanente Oregon Standard Gold Plan Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family
Sutter Health Plus: SG Gold Copay $30 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling 1-855-315-5800. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling 1-855-315-5800. Important
Coverage for: Large Group Plan Type: HMO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling 1-855-315-5800. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling 1-855-315-5800. Important
BlueOptions 03769. In-Network: $600 Per Person/$1,800 Family. Out-Of-Network: Combined with In-Network. Does not apply to In-Network preventive care.
 BlueOptions 03769 Coverage Period: 01/01/2015-12/31/2015 with Rx $15/$45/$65 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: PPO
BlueOptions 03769 Coverage Period: 01/01/2015-12/31/2015 with Rx $15/$45/$65 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: PPO
BlueOptions 05360. What is the overall deductible?
 BlueOptions 05360 Coverage Period: 10/01/2014-09/30/2015 with Rx $10/$30/$50 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: PPO
BlueOptions 05360 Coverage Period: 10/01/2014-09/30/2015 with Rx $10/$30/$50 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: PPO
BlueCare 61. In-Network: $1,250 Per Person/$2,500 Family. Out-Of-Network: Not Applicable Does not apply to In-Network preventive care.
 BlueCare 61 Coverage Period: 09/01/2014-08/31/2015 with Rx $10/$30/$50 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: HMO This
BlueCare 61 Coverage Period: 09/01/2014-08/31/2015 with Rx $10/$30/$50 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: HMO This
Health Net Life Ins. Co.: PPO HSA C6B HD 1300/2600
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthnet.com or by calling 1-800-522-0088. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthnet.com or by calling 1-800-522-0088. Important
BlueOptions 03160. Coverage Period: 01/01/2015-12/31/2015 HSA Compatible with Rx $15/$50/$80 after In-network Deductible
 BlueOptions 03160 Coverage Period: 01/01/2015-12/31/2015 HSA Compatible with Rx $15/$50/$80 after In-network Deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
BlueOptions 03160 Coverage Period: 01/01/2015-12/31/2015 HSA Compatible with Rx $15/$50/$80 after In-network Deductible Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual+Family Plan Type: DHMO
 Kaiser Permanente: DEDUCTIBLE PLAN Coverage Period: 06/01/2015-05/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual+Family Plan Type: DHMO Kaiser
Kaiser Permanente: DEDUCTIBLE PLAN Coverage Period: 06/01/2015-05/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual+Family Plan Type: DHMO Kaiser
PENDING REGULATORY APPROVAL. Coverage for: Individual Plan Type: HMO. Important Questions Answers Why this Matters: What is the overall deductible?
 PENDING REGULATORY APPROVAL This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling
PENDING REGULATORY APPROVAL This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling
Kaiser Permanente: Platinum 90 HMO
 Kaiser Permanente: Platinum 90 HMO Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO
Kaiser Permanente: Platinum 90 HMO Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO
Excellus BCBS:Simply Blue HDHP
 Excellus BCBS:Simply Blue HDHP A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs HOBART & WILLIAM SMITH
Excellus BCBS:Simply Blue HDHP A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs HOBART & WILLIAM SMITH
$1,250person/ $2,500Family. Doesn t apply to preventive care. Important Questions. Why this Matters:
 Virginia Mason Medical Center: Health Savings Plan Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Virginia Mason Medical Center: Health Savings Plan Coverage Period: 01/01/2014 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Panther Gold Advantage: UPMC Health Plan Coverage Period: 07/01/2016-06/30/2017 Summary of Coverage: What this Plan Covers & What it Costs
 Panther Gold Advantage: UPMC Health Plan Coverage Period: 07/01/2016-06/30/2017 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: All coverage levels Plan Type: HMO This is only
Panther Gold Advantage: UPMC Health Plan Coverage Period: 07/01/2016-06/30/2017 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: All coverage levels Plan Type: HMO This is only
PENDING REGULATORY APPROVAL. Coverage for: Individual Plan Type: HMO. Important Questions Answers Why this Matters: What is the overall deductible?
 PENDING REGULATORY APPROVAL This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling
PENDING REGULATORY APPROVAL This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at sutterhealthplus.org or by calling
Trustmark Life Insurance Company: LewerMark Coverage Period: Beginning on or after Aug 1, 2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.lewermark.com or by calling 1-800-821-7710. Request a
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.lewermark.com or by calling 1-800-821-7710. Request a
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthnet.com or by calling 1-800-522-0088. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthnet.com or by calling 1-800-522-0088. Important
Excellus BCBS:Healthy Blue HDHP
 Excellus BCBS:Healthy Blue HDHP A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs St. John Fisher College
Excellus BCBS:Healthy Blue HDHP A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs St. John Fisher College
Blue Shield of CA Life & Health Insurance: Shield Spectrum PPO SM 250-70/50 Foundation Coverage Period: 1/1/2014-12/31/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-800-200-3242. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-800-200-3242. Important
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthnet.com/uc or by calling 1-800-539-4072. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthnet.com/uc or by calling 1-800-539-4072. Important
Highmark Blue Cross Blue Shield: PPO Coverage Period: 01/01/2015-12/31/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbs.com or by calling 1-800-241-5704. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbs.com or by calling 1-800-241-5704. Important
Blue Shield of California Life & Health Insurance: Active Start Plan 25 - G Coverage Period: Beginning on or after 1/1/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-800-431-2809. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-800-431-2809. Important
Preferred Full PPO for Small Business 0 Coverage Period: Beginning On or After 1/1/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-888-319-5999. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-888-319-5999. Important
Important Questions Answers Why this Matters: $2,400 per individual / $4,800 per family Does not apply to preventive care and generic drugs.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-800-431-2809. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.blueshieldca.com or by calling 1-800-431-2809. Important
Important Questions Answers Why this Matters:
 Harken Health Insurance Company: Care Gold II Coverage Period: Beginning on or after 1/1/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Harken Health Insurance Company: Care Gold II Coverage Period: Beginning on or after 1/1/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-866-403-6183. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com/ca or by calling 1-866-403-6183. Important
Companion Life Insurance Co.: Platinum Plan - St. Louis College of Pharmacy Coverage Period: 8/1/15 7/31/16
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpstudent.com or by calling 1-800-633-7867. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpstudent.com or by calling 1-800-633-7867. Important
City of New York CBP Basic Program
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.emblemhealth.com or by calling 1-800-624-2414. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.emblemhealth.com or by calling 1-800-624-2414. Important
Important Questions Answers Why this Matters: What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsil.com/hsbc or by calling 1-888-979-2057. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bcbsil.com/hsbc or by calling 1-888-979-2057. Important
Yes. $125 per person for prescription drug expenses Yes. HSHS Facility/HSHS Preferred PCP/Network Specialist
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www. hshs.org/benefits or by calling Dean Health Plan at
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www. hshs.org/benefits or by calling Dean Health Plan at
LifeWise HP of Oregon: PST Silver HSA 3000 Coverage Period: Beginning on or after 01/01/2014
 LifeWise HP of Oregon: PST Silver HSA 3000 Coverage Period: Beginning on or after 01/01/2014 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: Individual or Family Plan Type: High-Deductible
LifeWise HP of Oregon: PST Silver HSA 3000 Coverage Period: Beginning on or after 01/01/2014 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: Individual or Family Plan Type: High-Deductible
Coverage for: Individual/Family Plan Type: PPO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at Marcia McMahon or by calling (814) 452-5673. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at Marcia McMahon or by calling (814) 452-5673. Important Questions
$2,000 person /$4,000 family. Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mycigna.com or by calling 1-800- Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.mycigna.com or by calling 1-800- Important Questions
Excellus BCBS:Excellus BluePPO
 Excellus BCBS:Excellus BluePPO A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs COLGATE UNIVERSITY Coverage
Excellus BCBS:Excellus BluePPO A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs COLGATE UNIVERSITY Coverage
: Self-Funded Aetna Open Access Managed Choice HIGH DEDUCTIBLE HEALTH PLAN Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthreformplansbc.com or by calling 1-800-334-0299.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthreformplansbc.com or by calling 1-800-334-0299.
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.cigna.com/individuals-families/connecticut or by calling
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.cigna.com/individuals-families/connecticut or by calling
HealthPartners: Peak HSA $3,650/$10,950-100% Silver Coverage Period: 01/01/2014-12/31/2014
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthpartners.com or by calling 1-877-838-4949. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthpartners.com or by calling 1-877-838-4949. Important
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.emblemhealth.com or by calling 1-800-447-8255. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.emblemhealth.com or by calling 1-800-447-8255. Important
Even though you pay these expenses, they don t count toward the out-ofpocket limit.
 Cigna Health and Life Insurance Co.:myCigna Health Savings 3400 Coverage Period: 01/01/2015-12/31/15 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family
Cigna Health and Life Insurance Co.:myCigna Health Savings 3400 Coverage Period: 01/01/2015-12/31/15 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family
Silver 70 HMO. Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.cchphmo.com or by calling 1-888-681-3888. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.cchphmo.com or by calling 1-888-681-3888. Important Questions
Unity Prime Bronze HSA 9028746 - HMO HSA
 Unity Prime Bronze HSA 9028746 - HMO HSA Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 1/1/2016-12/31/2016 Coverage for: Single/Family Plan Type: HMO This is
Unity Prime Bronze HSA 9028746 - HMO HSA Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 1/1/2016-12/31/2016 Coverage for: Single/Family Plan Type: HMO This is
City of New York CBP w/ Opt. Rider
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.emblemhealth.com or by calling 1-800-624-2414. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.emblemhealth.com or by calling 1-800-624-2414. Important
Coventry Health Care of Louisiana, Inc.: Gold $5 Copay HMO SH PD
 Coventry Health Care of Louisiana, Inc.: Gold $5 Copay HMO SH PD Coverage Period : 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary.
Coventry Health Care of Louisiana, Inc.: Gold $5 Copay HMO SH PD Coverage Period : 01/01/2015-12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary.
Coventry: Silver $5 Copay 2750 Cornerstone
 Coventry: Silver $5 Copay 2750 Cornerstone Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period : 01/01/2015-12/31/2015 Coverage for: Ivl, Ivl/Sp., Ivl/1Ch., Fam. Plan
Coventry: Silver $5 Copay 2750 Cornerstone Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period : 01/01/2015-12/31/2015 Coverage for: Ivl, Ivl/Sp., Ivl/1Ch., Fam. Plan
Premera BC: Balance Gold 1300 HSA Coverage Period: Beginning on or after 01/01/2014
 Premera BC: Balance Gold 1300 HSA Coverage Period: Beginning on or after 01/01/2014 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: Individual or Family Plan Type: High-Deductible
Premera BC: Balance Gold 1300 HSA Coverage Period: Beginning on or after 01/01/2014 Summary of Coverage: What this Plan Covers & What it Costs Coverage for: Individual or Family Plan Type: High-Deductible
BlueSelect 1449. No. Even though you pay these expenses, they don t count toward the out-of-pocket limit.
 BlueSelect 1449 Coverage Period: 01/01/2015-12/31/2015 Everyday Health Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: PPO/EPO
BlueSelect 1449 Coverage Period: 01/01/2015-12/31/2015 Everyday Health Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and/or Family Plan Type: PPO/EPO
Coventry: Bronze $15 Copay Regional Health Plus
 Coventry: Bronze $15 Copay Regional Health Plus Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period : 01/01/2015-12/31/2015 Coverage for: Ivl, Ivl/Sp., Ivl/1Ch., Fam.
Coventry: Bronze $15 Copay Regional Health Plus Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period : 01/01/2015-12/31/2015 Coverage for: Ivl, Ivl/Sp., Ivl/1Ch., Fam.
Coverage Period : 01/01/2014-12/31/2014. Plan Type: HMO. Coverage for: E, ES, EE/1Ch, EE/Chn, Fam
 Altius Health Plans: 73607 - UT Catastrophic Deductible Only Peak Preference - (ON) Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary. If you want more detail
Altius Health Plans: 73607 - UT Catastrophic Deductible Only Peak Preference - (ON) Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary. If you want more detail
Excellus BCBS:Classic Blue
 Excellus BCBS:Classic Blue A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs MONROE COUNTY Coverage Period:
Excellus BCBS:Classic Blue A nonprofit independent licensee of the Blue Cross Blue Shield Association Summary of Benefits and Coverage: What this Plan Covers & What it Costs MONROE COUNTY Coverage Period:
Moda Health Plan, Inc.: Be Rugged (Select) (Catastrophic) Coverage Period: 01/01/2015 12/31/2015
 (Catastrophic) Coverage Period: 01/01/2015 12/31/2015") This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.modahealth.com or by calling 1-888-873-1395. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.modahealth.com or by calling 1-888-873-1395. Important
Preferred PPO Blue Options Health Insurance Plan Coverage Period: 04/01/2015 03/31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at http://icubabenefits.org or by calling 1-866-377-5102. In
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at http://icubabenefits.org or by calling 1-866-377-5102. In
HealthPartners: State of WI Ded - High Deductible Health Plan (HDHP) Coverage Period: 01/01/2015-12/31/2015
 Coverage Period: 01/01/2015-12/31/2015") This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthpartners.com or by calling 1-800-883-2177. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthpartners.com or by calling 1-800-883-2177. Important
How To Pay For A Health Care Plan With A Macy Insurance Plan
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthreformplansbc.com or by calling 1-855-586-6963.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.healthreformplansbc.com or by calling 1-855-586-6963.
National Guardian Life Insurance Company - Platinum Plan for: Texas Wesleyan University Coverage Period: 8/1/15 7/31/16
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpstudent.com or by calling 1-800-633-7867. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.chpstudent.com or by calling 1-800-633-7867. Important