No Financial disclosure
|
|
|
- Emma Tucker
- 8 years ago
- Views:
Transcription
1 Magdy Giurgius.MD
2 No Financial disclosure

3 1-History 2-Gastric Banding 3-Adverse events 4-Multidiscplinary approach
4 The prevalence of obesity in the Western world, especially in the United States, has been increasing. From 1980 to 2004, individuals with a body mass index (BMI) of 30 kg/m 2 doubled, representing almost one-third of the US population. The prevalence of overweight children increased from 1999 to 2004.

5 71% Females Average age 42 Average BMI 45 Average co morbidities % married 62% employed Often overweight since childhood

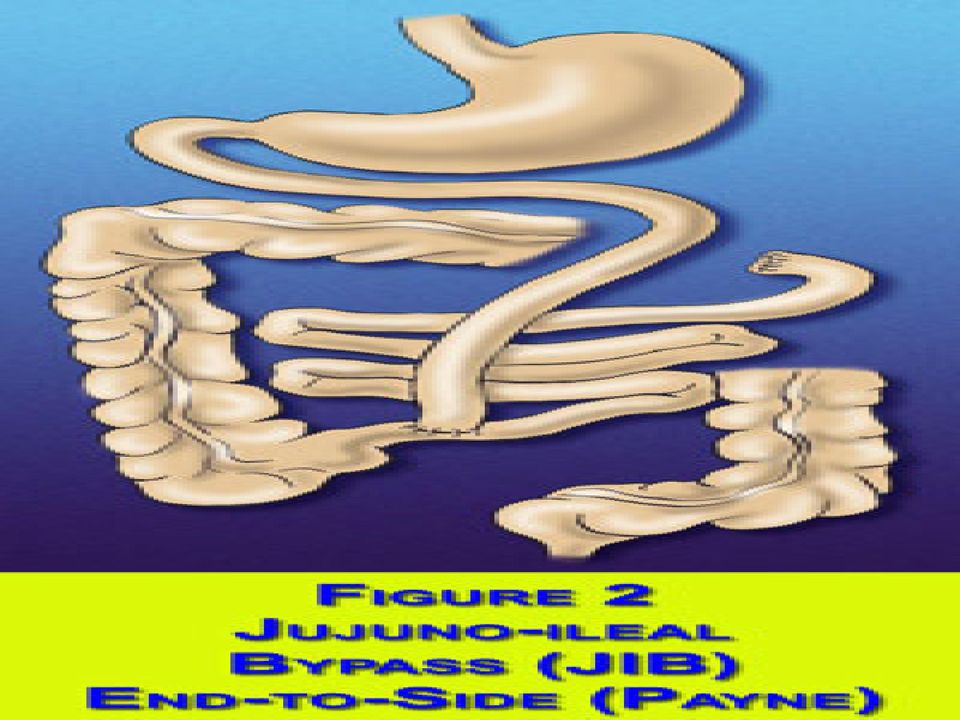
6 The first bariatric procedure to be preceded by animal studies and subsequently presented to a recognized surgical society and published in a peer reviewed journal was that of Kremen and associates in (Kremen, Linner et al. 1954) The story of surgery for Obesity ASBS 1999

7 The case which they presented was of a jejuno-ileal bypass.(jib).

8 Payne et al. reported results of ten patients in whom an end-to-side jejuno-colic shunt had been performed These patients had episodes of uncontrollable diarrhea, dehydration and electrolyte imbalance.

9

10 Payne and Dewind subsequently advised against jejunocolic anastomoses, instead recommending end to side jejuno-ileostomy anastomosing the first 14 inches of jejunum to the last 4 inches of ileum.(payne and DeWind 1969)

11
12 End-to end anastomoses of the proximal jejunum to distal ileum.

13 Both these variants a total of only about 35 cms (18") of normally absorptive small intestine was kept. In consequence, malabsorption of carbohydrate, protein, lipids, minerals and vitamins occur. End-to-side technique was used, reflux of bowel content back up the defunctionalized small intestine allowed absorption of some of the refluxed material resulting in less weight loss initially and greater subsequent weight regain.

14 Bile has an important role in fat digestion, emulsifying fat as the first stage in its digestion. Bypassing the major site of bile acid reabsorption in the small intestine therefore further reduces fat and fat soluble vitamin absorption

15 As a result, huge amounts of fatty acids which are normally absorbed in the small intestine, enter the colon where they cause irritation of the colon wall and the secretion of excessive volumes of water and electrolytes, especially sodium and potassium, leading to diarrhea.

16 Mineral and Electrolyte Imbalance: Decreased serum sodium, potassium, magnesium and bicarbonate. Decreased sodium chloride Osteoporosis and osteomalacia secondary to protein depletion, calcium and vitamin D loss. Protein Calorie Malnutrition Hair loss, anemia, edema, and vitamin depletion Cholelithiasis Enteric Complications: Abdominal distension, irregular diarrhea, increased flatus, pneumatosis intestinalis, colonic pseudo-obstruction, bypass enteropathy, volvulus with mechanical small bowel obstruction.

17 The multiple complications associated with JIB led to a search for alternative procedures Griffen et al. reported a comprehensive series comparing the results of jejuno-ileal bypass with gastric bypass. 11 of 50 patients who underwent JIB required conversion to gastric bypass within 5 years, leading Griffen to abandon jejuno-ileal bypass. (Griffen, Bivins et al. 1983ss)

18 Malabsorption is defined by the incomplete uptake of calories and nutrients and occurs via two mechanisms. First, the bile and pancreatic fluids released into the duodenum to digest food and break down fats, carbohydrates and proteins are diverted away from ingested food hence the name, biliopancreatic diversion The second mechanism through which malabsorption occurs is by decreasing the amount of small intestine through which the ingested food passes

19 A modern improvement of the Jejuno-ileal Bypass (JIB) is Biliopancreatic Diversion,(BPD), a procedure which differs from JIB in that no small intestine is defunctionalized and, consequently, liver problems are much less frequent developed by Professor Nicola Scopinaro, of the University of Genoa, Italy. (Scopinaro, Gianetta et al. 1996)

20 A modern improvement of the Jejuno-ileal Bypass (JIB) is Biliopancreatic
 is")
21
22 72% excess body weight loss maintained for 18 years Disadvantages of the procedure are the association with loose stools, stomal ulcers, and foul smelling stools and flatus. The most serious potential complication is protein malnutrition, which is associated with hypoalbuminemia, anemia, edema, asthenia, generally requires hospitalization and 2-3 weeks hyperalimentation
23 Because of this potential for significant complications, BPD patients require lifelong follow-up
24 In 1988, Hess, using a combination of Scopinaro's BPD and the duodenal switch described by De Meester in 1987, developed a hybrid operation with the advantages of the BPD but without some of the associated problems. The duodenal switch, originally designed for patients with bile reflux gastritis, consists of a suprapapillary Roux-en-Y duodeno-jejunostomy
25 This allows the first portion of the duodenum to remain in the alimentary stream thus reducing the incidence of stomal ulcer. When combined with a 70%-80% greater curvature gastrectomy (sleeve resection of the stomach) continuity of the gastric lesser curve is maintained while simultaneously reducing stomach volume.
26 A long limb Roux-en-Y is then created. The efferent limb acts to decrease overall caloric absorption and the long biliopancreatic limb diverting bile from the alimentary contents, specifically to induce fat malabsorption Hess in 1992 and first published in a paper by Marceau, Biron et al in 1993 is known as Biliopancreatic Diversion with Duodenal Switch (BPDDS)
27
28 BPD/DS Deep vein thrombophlebitis 0.7% pulmonary embolism 0.5% Pneumonia 0.5% Acute respiratory distress syndrome 0.25% Splenectomy 0.9% Gatric leak and fistula 2.0% Duodenal leak 1.5% Distal Roux-en-Y leak 0.25% Postoperative bleeding 0.5% Abcess unrelated to leaks 0.25% Duodenal stomal obstruction 0.75% Small bowel obstruction 2.0%
29 1960s Gastric Bypass (RGB) was developed by Dr Edward E. Mason, of the University of Iowa, based on the observation that females who had undergone partial gastrectomy for peptic ulcer disease, tended to remain underweight following the surgery, and that it was very difficult to achieve weight gain in this patient group Professor of Surgery at the University of Iowa
30 (Mason and Ito 1967) With the availability of surgical staples, he was able to create a partition across the upper stomach using staples, and did not require removal of any of the stomach
31 Subsequent modifications of the technique include a pouch of 50 ml or less, a gastro-enterostomy stoma of 0.9 mm, use of the Roux-en-Y technique to avoid loop gastroenterostomy and the bile reflux which may ensue
32
33
34 Lengthening of the Roux limb to cms to include a greater element of malabsorption and improve weight loss and the use of the retrocolic and retrogastric routing of the gastrojejunostomy to ease the technical difficulties of the procedure and improve long term weight loss results Gastric Bypass has also stood the test of time, with one series of greater than 500 cases, followed for 14 years, maintaining 50% excess weight loss.
35 Early: Leak Acute gastric dilatation Roux-Y obstruction Atelectasis Wound Infection/seroma Late: Stomal Stenosis Anemia Vitamin B12 deficiency Calcium deficiency/osteoporosis
36 The use of rings to control the stoma size, proven with Vertical Banded Gastroplasty, has led to their adoption by some surgeons as an addition to gastric bypass procedures However, because the muscular stomach wall has a tendency to stretch, the stoma can widen thus permitting greater food and calorie intake To reduce this possibility, weight loss surgeons place a silastic ring as a sort of "collar" around the stoma, to prevent stretching and enlarging of the passage into the lower (distal) stomach.
37
38
39 During World War II, the Russians, as part of their war effort, developed a series of surgical instruments which would staple various body tissues together as a simple and rapid method of dealing with injuries. This concept was adapted and refined by American surgical instrument makers after the war, leading to the surgical stapling instruments in use today
40 In Bariatric Surgery The idea being that food which the patient takes in is held up in the segment of stomach above the staple line causing the sensation of fullness. The food then empties slowly through the stoma into the stomach below the staple line. Unfortunately, the stomach wall has a tendency to stretch and the stoma enlarges (Gomez 1981),used this technique which was only partially successful
41
42 The search for a better gastroplasty was pursued by Dr. Edward E. Mason in He realized that the lesser curvature part of the stomach had the thickest wall and was therefore least likely to stretch, so he used a vertical segment of stomach along the lesser curvature for the pouch. Modification which he made was to place a polypropylene band (Marlex Mesh) around the lower end of the vertical pouch, which acts as the stoma, to fix the size of the outlet of the pouch, preventing it from stretching
43
44 He defined the size of the pouch, measuring it at surgery under a standard hydrostatic pressure, and has shown that best results follow the use of a very small pouch, holding only 14 mls of saline at the time of surgery.
45 A surgical variant of the VBG is the Silastic Ring Vertical Gastroplasty (SRVG) which is functionally identical to VBG but uses a silastic ring to control the stoma size.
46
47 Leak Stenosis with persistent vomiting Ulcer Incisional hernia Wound Infection Band erosion
48 Several things all happened in the early 1990s 1993:The first Laparoscopic Gastric bypass Bariatric surgeons learned from each other
49 Laparoscopic Roux GIB with hand sewn gastrojejunostomy First case took them 8 hours
50 Dr. Alan Wittgrove, is known as the father of laparoscopic gastric bypass: he performed the first laparoscopic gastric bypass in the world as primary surgeon in This was performed in San Diego, California
51
52 Vertical Sleeve Gastrectomy (VSG) The earliest forms of this procedure were conceived of by Dr. Jamieson in Australia (Long Vertical Gastroplasty, Obesity Surgery 1993)- and by Dr. Johnston in England in 1996 (Magenstrasse and Mill operation- Obesity Surgery 2003). Dr Gagner in New York, refined the operation to include gastrectomy(removal of stomach) and offered it to high risk patients in 2001
53
54 Alternative to a Roux-en-Y Gastric Bypass The Vertical Gastrectomy is a reasonable alternative to a Roux en Y Gastric Bypass for a number of reasons Because there is no intestinal bypass, the risk of malabsorptive complications such as vitamin deficiency and protein deficiency is minimal. There is no risk of marginal ulcer which occurs in over 2% of Roux en Y Gastric Bypass patients. The pylorus is preserved so dumping syndrome does not occur or is minimal. There is no intestinal obstruction since there is no intestinal bypass. It is relatively easy to modify to an alternative procedure should weight loss be inadequate or weight regain occur. The limited two year and 6 year weight loss data available to date is superior to current Banding and comparable to Gastric Bypass weight loss data(see Lee, Jossart, Cirangle Surgical Endoscopy 2007).
55
56 Effect of Bariatric Surgery on Medical Diseases
57 The global prevalence of Type 2 DM is increasing, and is estimated to reach > 366 million individuals in 2030 The American Diabetes Association estimates that in 2020, the annual cost of caring for persons with diabetes will approach $192 billion Postgrad Med Jan;123(1):24-33
58 Bariatric Surgery in Patients with Type 2 Diabetes Because of its increased safety and efficacy, bariatric surgery, particularly LAGB, has gained acceptance as a potential therapeutic tool in patients with T2DM who have a BMI of > 35 kg/m 2. Roux-en-Y gastric bypass appears to have remained the procedure that has shown the most dramatically effective weight loss when compared with LAGB; however, in one systematic review, LAGB had lower short-term morbidity and higher reoperation rates. Postgrad Med Jan;123(1):24-33
59 IMPACT ON OBESITY-RELATED DISEASES Can improve or resolve more than 30 obesity-related conditions, including Type 2 diabetes, heart disease, sleep apnea, hypertension and high cholesterol Gastric bypass resolves Type 2 diabetes in nearly 87% of patients Band surgery resolves Type 2 diabetes in 73% of patients Cuts risk of developing coronary heart disease in half Resolves obstructive sleep apnea in more than 85% of patients
60 BARIATRIC SURGERY: RISKS VS. BENEFITS In 2007, federal government (Agency for Healthcare Research and Quality) and clinical studies report significant improvements in safety. o Risk of death from bariatric surgery is about 0.1% Bariatric surgery increases lifespan, as compared to those who do not have surgery o Patients may improve life expectancy by 89% Patients may reduce their risk of premature death by 30 to 40% Dramatic reduction in risk of death from obesity-related diseases, as compared to those who do not have surgery o Risk of death from diabetes down 92%, from cancer down 60% and from coronary artery disease down 56%
61 LONG-TERM EFFECTIVENESS OF BARIATRIC SURGERY Typically patients have maximum weight loss within 1-2 years after surgery and maintain a substantial weight loss, with improvements in obesity-related conditions, for years afterwards Patients may lose 30 to 50% of their excess weight 6 months after surgery and 77% of their excess weight as early as 12 months after surgery Long-term studies show up to years after surgery, morbidly obese patients who had surgery maintained a much greater weight loss and more favorable levels of diabetes, cholesterol and hypertension, as compared to those who did not have surgery
62 Meta-Analysis: Surgical Treatment of Obesity Surgery is more effective than nonsurgical treatment for weight loss and control of some comorbid conditions in patients with a BMI of 40 kg/m 2 or greater. More data are needed to determine the efficacy of surgery relative to nonsurgical therapy for less severely obese people. Procedures differ in efficacy and incidence of complications. April 5, 2005 vol. 142 no
63 Original Article Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects The prospective, controlled Swedish Obese Subjects study involved 4047 obese subjects. Of these subjects, 2010 underwent bariatric surgery (surgery group) and 2037 received conventional treatment (matched control group) Maximum weight losses in the surgical subgroups were observed after 1 to 2 years: gastric bypass, 32%; vertical-banded gastroplasty, 25%; and banding, 20%. After 10 years, the weight losses from baseline were stabilized at 25%, 16%, and 14%, respectively. There were 129 deaths in the control group and 101 deaths in the surgery group Bariatric surgery for severe obesity is associated with long-term weight loss and decreased overall mortality N Engl J Med 2007; 357: August 23, 2007
64 Surgery is the only way to obtain consistent,permenant weight loss for morbid obese patients Indications: 1-BMI of 40 or over 2-BMI with significant comorbidity 3-Documented dietary attempts ineffective 4-VBG & Gastric bypass are identified as the safe and effective surgical treatment for obesity
65 The field grew but complications grew as well!!!!!
66 Leak rate 2-5 % Major infections 2-5% Incisional Hernias 10-20% Bleeding less than 2 % Clot related?????
67 Complications Port related Stapler related Tube and dilator related
68 Too many trained too quickly -Lap.Gatsric bypass is a complex operation often done on sick patients -A week end is not enough to learn about the prinicples of Bariatric procedures -People got into Bariatric surgery for wrong reasons. Many for the money
69 Development of courses,fellowships and preceptor ship NIH update-consensus conference May 2004 Meta analysis Creation of surgical review corporation(src) Work with Medicare
70 1. Bariatric surgery is the most effective therapy available for morbid obesity and can result in improvement or complete resolution of obesity co morbidities. 2. Types of operative procedures for morbid obesity have increased since 1991 and are continuously evolving; there are currently four types of procedures that can be used to achieve sustained weight loss: gastric bypass (standard, long-limb, and very long-limb Roux), alone or in combination with vertical banded gastroplasty; laparoscopic adjustable gastric banding; vertical banded gastroplasty; and biliopancreatic diversion and duodenal switch.
71 3. Both open and laparoscopic bariatric operations are effective therapies for morbid obesity and represent complementary state-of-the-art procedures. 4. Bariatric surgery candidates should have attempted to lose weight by nonoperative means, including self-directed dieting, nutritional counseling, and commercial and hospital-based weight loss programs, but should not be required to have completed formal nonoperative obesity therapy as a precondition for the operation. 5. The bariatric surgery patient is best evaluated and subsequently cared for by a multidisciplinary team
72
73 Forsell- March 1996 developed SAGB laparoscopic Technique. Based on Pars Flaccida dissection in open technique. Catona A et Manna L and Forsell P. The Swedish Adjustable Gastric Band: laparoscopic technique and preliminary results. Obes Surg 2000Feb :10(1)15-21
74
75 Position : -Lithotomy vs Supine Surgeon s preference -Operating table in reversed Trendelenberg
76
77
78 Angle of His Dissection Preserve gastro-phrenic attachment
79 Five trocars are placed in the following sequence: a 10 mm trocar for a 30 optical system 6 finger breadths below the xyphoid a 10 mm trocar for the liver retractor (sub-xyphoid) a 10 mm trocar for the grasping forceps and the Lap-Band Closure Tool (in R upper quadrant) a 5 mm trocar for the cautery hook, needle holder and grasping forceps (in L upper quadrant) 10 mm trocar for the atraumatic grasping forceps for band introduction and reservoir placement (on the L anterior axillary line below the costal margin).
80
81 Incise lesser omentum in avascular pars flaccida region Blunt dissection along the medial border of the right crus picture
82
83 Minimal Force should be needed 5 mm articulating dissector (golden finger) other dissectors or a grasper can be used
84
85 Check band and tube for leaks Aspirate all air from the Balloon Tighten Knot on tube
86 15 mm trocar Minimal force Grasp the band flap with the grasper
87 Pass and hook the suture loop arround the endoscopic dissector tip slot Pass Band first instead of tubing first
88
89 Two Balloon types available -Symmetrical -Asymmetrical Inflate with 15 cc saline
90
91 Grab the suture loop Pass and pull through the buckle till locked
92
93 Standard of care in USA In many other countries they do not plicate A curved needle may assist with good bites in the small space between the band and the cardia Deflate and remove the gastric calibration tube before placing sutures.
94
95
96 Bring the free end of the tubing out of the peritoneal cavity through the selected Trocar port site. Leave sufficient tubing length within the peritoneal cavity to avoid tension on the gastric band. Placement of the injection port above the fascia
97
98
99
100
101 1-Slippage/prolapse Anterior Posterior it is uncommon with pars flaccida technique
102 Remove fluid If prolapse small and symptoms improve: -re-train patient,behaviour modification eating rules -Re adjust band slowly If prolapse large -Revision surgery in the form of pulling the stomach through and resuture.
103 Chronic enlargement of gastric pouch Different than slippage/prolapse concentric Presentation -Hunger/Larger portions/no weight loss -Obstructive symptoms: Vomiting/reflux/regurgitaion
104 A. Conservative -Band deflation -Behavior modification -Reinforce eating rules -Frequent follow up visits -slow adjustments Nutritional and psychological support
105 B. Surgical Treatment Reposition the band Band explant Convert to RNY
106 Etiology 1-Serosa injury from dissection 2-Excessive tissue tension 3-Excessive vomiting C/P Asymptomatic Lack of restrictions Latent access port infection
107 Dysphagia Epigatsric pain Diagnosis Barium study Barium is flowing around the eroding band
108 Upper GI endoscopy -Definitive diagnostic tool -A normal barium study does not exclude Erosion
109 A. Laparoscopic : Removal and close gastrotomy B. Endoscopic: -Totally endoscopic removal -Laparoscopic assisted endoscopic removal
110 Etiology Stitch pull through causing gastric leak C/P Acute presentation few days post-op Consistent with peritonitis UGI study may not show a leak CT may be more helpful Laparoscopy best approach &Band explanation
111 Clinical scenario -Usually patient doing well and after adjustments develops obstruction not improving with band deflation -Unusual dysphasia, fluid collection,abscess UGI or CT may be helpful Laparoscopy---inflammatory reaction Turbid fluid or pus. Treatment Band Explanation
112 Uncommon Etiology -May be unclear -Iatrogenic needle, grasper, instrument
113 On Suspicious of leak -Aspirate all fluid -Under fluroscopy inject contrast -If no leak detected aspirate contarst and inject saline instead.
114 Natural Orifice Translumenal Endoscopic Surgery (NOTES ) Under trials
115
116 The multidiscplinary approach is not a luxury but rather mandatory as mandated by various guidelines and criteria.
117 Programs need to address preoperative and long term management Patients require long term follow up including nutritional counseling and biochemical surveillance. Surgeons need to be aware of the needs for morbidly obese patients in terms of facilities,supplies, equipment, staff, and procedures
118 Multidisciplinary approach including medical management of co morbidities, dietary,instruction, exercise training, specialized nursing care and Psychological assistance Well trained team familiar with equipments, instruments and techniques of bariatric surgery
119 To deliver Optimal Bariatric surgical care Education of patients Develop a process to assess each program objectively (know the data)
120 Documented In-service education. Commitment up to the highest level Minimum 50 cases per surgeon per year. Institution maintains Minimum 125 cases /year.
121 Program maintains a program director who participates in the relevant decision making meetings Well equipped ICU with trained personal Obesity safe environment Beds, Radiological equipment,.etc
122 RN Clinical and non-clinical responsibilities. Certified Bariatric nurse.
123 Maximizing adipose tissue loss by minimizing lean muscle mass loss gm of protein daily Cultural preferences Vitamin needs
124 Exercise is a key for maintaining long term weight loss Physical disabilities or limitations should be addressed Motivation, encouragement, reassurance and customization.
125 A systematic approach helps with data recording and reporting. COE requirement Insurance companies requiring data as well Allows opportunities for research.
126 Support the patient Trained to pick up disorders and potential red flags Depth of understanding of Bariatric surgery Available for consultation Pre operative Psych assessment per ASMBS requirements
127 Supports pre and post operative patient care Educates about different aspects of Bariatric needs Coordinates with other members of the team : Nurses, Psychologists, Dietitian, Program coordinator.
128 Specialized and ongoing clinical training Competent in complication recognition Understanding Bariatric procedures Empathy training
129 It has to be a dedicated team focusing in Bariatric patients,understanding their needs and give them the tools and guidance to optimally achieve their goals.
130 The goal is 75% long term follow up at five years. -Provide SRC (Surgical Review Corporation) and annual update -HIPPA compliant -Early and late complications
131 Morbid obesity surgery is a curative tool when indicated. Need for a center of excellence to practice Multidisciplinary approach is the way to go Use of different techniques Fellowship programs Trained nursing staff
132 Thank you
Overview of Bariatric Surgery
 Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Types of Bariatric Procedures. Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012
 Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Vertical Sleeve Gastrectomy (VSG) - Also known as Sleeve Gastrectomy, Vertical Gastrectomy
 - Also known as Sleeve Gastrectomy, Vertical Gastrectomy") Vertical Sleeve Gastrectomy (VSG) - Also known as Sleeve Gastrectomy, Vertical Gastrectomy The Vertical Sleeve Gastrectomy procedure (also called Sleeve Gastrectomy, Vertical Gastrectomy, Greater Curvature
Vertical Sleeve Gastrectomy (VSG) - Also known as Sleeve Gastrectomy, Vertical Gastrectomy The Vertical Sleeve Gastrectomy procedure (also called Sleeve Gastrectomy, Vertical Gastrectomy, Greater Curvature
Some of the diseases and conditions associated with obesity include:
 WEIGHT-LOSS SURGERY facts about obesity Obesity is rapidly becoming the nation s number-one health problem. Of the 97 million Americans who are overweight, 10 million are considered morbidly obese. Obesity
WEIGHT-LOSS SURGERY facts about obesity Obesity is rapidly becoming the nation s number-one health problem. Of the 97 million Americans who are overweight, 10 million are considered morbidly obese. Obesity
Morbid obesity is a chronic condition that
 COSMETIC A Review of Bariatric Surgery Procedures Morbid obesity is a chronic condition that is extremely difficult to treat. In addition to unhealthy food choices and lifestyles, effective treatment for
COSMETIC A Review of Bariatric Surgery Procedures Morbid obesity is a chronic condition that is extremely difficult to treat. In addition to unhealthy food choices and lifestyles, effective treatment for
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Weight Loss Surgery Info for Physicians
 Weight Loss Surgery Info for Physicians As physicians, we see it every day when we see our patients more and more people are obese, and it s affecting their health. It s estimated that at least 2/3 of
Weight Loss Surgery Info for Physicians As physicians, we see it every day when we see our patients more and more people are obese, and it s affecting their health. It s estimated that at least 2/3 of
The Evolution of Bariatric Surgery. History of the Development of a Successful Bariatric Program at the University of Iowa Hospitals & Clinics
 The Evolution of Bariatric Surgery History of the Development of a Successful Bariatric Program at the University of Iowa Hospitals & Clinics It s a BIG Problem & it s Getting Worse Obesity is now a disease
The Evolution of Bariatric Surgery History of the Development of a Successful Bariatric Program at the University of Iowa Hospitals & Clinics It s a BIG Problem & it s Getting Worse Obesity is now a disease
BARIATRIC SURGERY MAY CURE TYPE 2 DIABETES IN SOME PATIENTS
 BARIATRIC SURGERY MAY CURE TYPE 2 DIABETES IN SOME PATIENTS Thomas Rogula MD, Stacy Brethauer MD, Bipand Chand MD, and Philip Schauer, MD. "Gastric bypass surgery has become a popular option for obese
BARIATRIC SURGERY MAY CURE TYPE 2 DIABETES IN SOME PATIENTS Thomas Rogula MD, Stacy Brethauer MD, Bipand Chand MD, and Philip Schauer, MD. "Gastric bypass surgery has become a popular option for obese
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
Transmittal 54 Date: APRIL 28, 2006. SUBJECT: Bariatric Surgery for Treatment of Morbid Obesity
 CMS Manual System Pub 100-03 Medicare National Coverage Determinations Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 54 Date: APRIL 28, 2006 Change
CMS Manual System Pub 100-03 Medicare National Coverage Determinations Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 54 Date: APRIL 28, 2006 Change
Surgical Weight Loss. Mission Bariatrics
 Surgical Weight Loss Mission Bariatrics Obesity is a major health problem in the United States, with more than one in every three people suffering from this chronic condition. Obese adults are at an increased
Surgical Weight Loss Mission Bariatrics Obesity is a major health problem in the United States, with more than one in every three people suffering from this chronic condition. Obese adults are at an increased
Bariatric Weight Loss Surgery
 BARIATRIC SURGERY Bariatric Weight Loss Surgery The heart and science of medicine. Weight loss surgery, also known as bariatric surgery, was developed as a tool to help people with morbid obesity reduce
BARIATRIC SURGERY Bariatric Weight Loss Surgery The heart and science of medicine. Weight loss surgery, also known as bariatric surgery, was developed as a tool to help people with morbid obesity reduce
Gastric Surgery for Clinically Severe (Morbid) Obesity
 Obesity") Origination: 03/28/01 Revised: 01/16/15 Annual Review: 11/12/15 Purpose: The Medical Technology Assessment Committee will review published scientific literature and information from appropriate government
Origination: 03/28/01 Revised: 01/16/15 Annual Review: 11/12/15 Purpose: The Medical Technology Assessment Committee will review published scientific literature and information from appropriate government
Obesity Affects Quality of Life
 Obesity Obesity is a serious health epidemic. Obesity is a condition characterized by excessive body fat, genetic and environmental factors. Obesity increases the likelihood of certain diseases and other
Obesity Obesity is a serious health epidemic. Obesity is a condition characterized by excessive body fat, genetic and environmental factors. Obesity increases the likelihood of certain diseases and other
Roux-en-Y Gastric Bypass
 Roux-en-Y Gastric Bypass Restrictive and malabsorptive procedure Most frequently performed bariatric procedure in the US First done in 1967 Laparoscopic since 1993 75% EWL in 18-24 months 50% EWL is still
Roux-en-Y Gastric Bypass Restrictive and malabsorptive procedure Most frequently performed bariatric procedure in the US First done in 1967 Laparoscopic since 1993 75% EWL in 18-24 months 50% EWL is still
Consent for Treatment/Procedure Laparoscopic Sleeve Gastrectomy
 Patient's Name: Today's Date: / / The purpose of this document is to confirm, in the presence of witnesses, your informed request to have Surgery for obesity. You are asked to read the following document
Patient's Name: Today's Date: / / The purpose of this document is to confirm, in the presence of witnesses, your informed request to have Surgery for obesity. You are asked to read the following document
Consumer summary Laparoscopic adjustable gastric banding for the treatment of obesity (Update and re-appraisal)
") ASERNIP S Australian Safety and Efficacy Register of New Interventional Procedures Surgical Consumer summary Laparoscopic adjustable gastric banding for the treatment of obesity (Update and re-appraisal)
ASERNIP S Australian Safety and Efficacy Register of New Interventional Procedures Surgical Consumer summary Laparoscopic adjustable gastric banding for the treatment of obesity (Update and re-appraisal)
Technical Aspects of Bariatric Surgical Procedures. Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital
 Technical Aspects of Bariatric Surgical Procedures Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital Disclosures Allergan, Inc. (Past) Faculty Member Educational
Technical Aspects of Bariatric Surgical Procedures Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital Disclosures Allergan, Inc. (Past) Faculty Member Educational
Weight Loss Surgery Information Session. WFBH Bariatric Surgery Program
 Weight Loss Surgery Information Session WFBH Bariatric Surgery Program What makes us different? Center of Excellence (COE) High volume center > 1000 procedures since 2003 Less complications than non-coe
Weight Loss Surgery Information Session WFBH Bariatric Surgery Program What makes us different? Center of Excellence (COE) High volume center > 1000 procedures since 2003 Less complications than non-coe
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201420 APRIL 29, 2014
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201420 APRIL 29, 2014 IHCP to cover sleeve gastrectomy surgery The Indiana Health Coverage Programs (IHCP) covers bariatric surgery for individuals with
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201420 APRIL 29, 2014 IHCP to cover sleeve gastrectomy surgery The Indiana Health Coverage Programs (IHCP) covers bariatric surgery for individuals with
WEIGHT LOSS SURGERY. Pre-Clinic Conference Jennifer Kinley, MD 12/15/2010
 WEIGHT LOSS SURGERY Pre-Clinic Conference Jennifer Kinley, MD 12/15/2010 EDUCATIONAL OBJECTIVES: Discuss the available pharmaceutical options for weight loss and risks of these medications Explain the
WEIGHT LOSS SURGERY Pre-Clinic Conference Jennifer Kinley, MD 12/15/2010 EDUCATIONAL OBJECTIVES: Discuss the available pharmaceutical options for weight loss and risks of these medications Explain the
Obesity When to Recommend Surgery. Lily Chang, MD September 27, 2013
 Obesity When to Recommend Surgery Lily Chang, MD September 27, 2013 Obesity BMI >30 Trends Among U.S. Adults Source: Behavioral Risk Factor Surveillance System, CDC, 2012 Obesity Related Co-Morbidities
Obesity When to Recommend Surgery Lily Chang, MD September 27, 2013 Obesity BMI >30 Trends Among U.S. Adults Source: Behavioral Risk Factor Surveillance System, CDC, 2012 Obesity Related Co-Morbidities
2013 RN.ORG, S.A., RN.ORG, LLC
 Obesity: Bariatric Surgical Options WWW.RN.ORG Reviewed September, 2013, Expires September, 2015 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2013 RN.ORG,
Obesity: Bariatric Surgical Options WWW.RN.ORG Reviewed September, 2013, Expires September, 2015 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2013 RN.ORG,
Medical Coverage Policy Bariatric Surgery
 Medical Coverage Policy Bariatric Surgery Device/Equipment Drug Medical Surgery Test Other Effective Date: 9/1/2011 Policy Last Updated: 11/01/2011 Prospective review is recommended/required. Please check
Medical Coverage Policy Bariatric Surgery Device/Equipment Drug Medical Surgery Test Other Effective Date: 9/1/2011 Policy Last Updated: 11/01/2011 Prospective review is recommended/required. Please check
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Dept. of Medical Imaging University of Ottawa
 ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
MEDICAL COVERAGE POLICY. SERVICE: Bariatric (Weight Loss) Surgery Policy Number: 053 Effective Date: 5/27/2014 Last Review: 4/24/2014
 Surgery Policy Number: 053 Effective Date: 5/27/2014 Last Review: 4/24/2014") Page 1 of 6 MEDICAL COVERAGE POLICY Important note Even though this policy may indicate that a particular service or supply is considered covered, this conclusion is not necessarily based upon the terms
Page 1 of 6 MEDICAL COVERAGE POLICY Important note Even though this policy may indicate that a particular service or supply is considered covered, this conclusion is not necessarily based upon the terms
Why the band in the Gastric Bypass Operation.
 Center for Surgical Treatment of Obesity, Los Angeles, California C.S.T.O. Why the band in the Gastric Bypass Operation. M.A.L. Fobi, MD F.A.C.S. H. Lee, MD; B. Felahy, MD; N. Fobi, MD; P. Ako, MD Chi
Center for Surgical Treatment of Obesity, Los Angeles, California C.S.T.O. Why the band in the Gastric Bypass Operation. M.A.L. Fobi, MD F.A.C.S. H. Lee, MD; B. Felahy, MD; N. Fobi, MD; P. Ako, MD Chi
If you are morbidly obese, you should remember these important points:
 What is Morbid Obesity? Morbid obesity is a serious medical condition. If you are morbidly obese, it means that you are severely overweight, usually by at least 100 pounds. It also means that you have
What is Morbid Obesity? Morbid obesity is a serious medical condition. If you are morbidly obese, it means that you are severely overweight, usually by at least 100 pounds. It also means that you have
What is the Sleeve Gastrectomy?
 What is the Sleeve Gastrectomy? The Sleeve Gastrectomy (also referred to as the Gastric Sleeve, Vertical Sleeve Gastrectomy, Partial Gastrectomy, or Tube Gastrectomy) is a relatively new procedure for
What is the Sleeve Gastrectomy? The Sleeve Gastrectomy (also referred to as the Gastric Sleeve, Vertical Sleeve Gastrectomy, Partial Gastrectomy, or Tube Gastrectomy) is a relatively new procedure for
White Paper: Treating Clinical Obesity: When is Bariatric Surgery or Bariatric Surgery Revision Medically Necessary?
 White Paper: Treating Clinical Obesity: When is Bariatric Surgery or Bariatric Surgery Revision Medically Necessary? For Health Plans, Medical Management Organizations and TPAs Introduction More than one
White Paper: Treating Clinical Obesity: When is Bariatric Surgery or Bariatric Surgery Revision Medically Necessary? For Health Plans, Medical Management Organizations and TPAs Introduction More than one
Emergencies in Post- Bariatric Surgery Patients
 Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
5. Conversion Procedures that change from an index procedure to a different type of procedure.
 Benefit Coverage Covered Benefit for lines of business including Health Benefits Exchange (HBE), Rite Care (MED), Children with Special Needs (CSN), Substitute Care (SUB), Rhody Health Partners (RHP),
Benefit Coverage Covered Benefit for lines of business including Health Benefits Exchange (HBE), Rite Care (MED), Children with Special Needs (CSN), Substitute Care (SUB), Rhody Health Partners (RHP),
11/10/2014. I have nothing to Disclose. Covered Stents discussed are NOT FDA approved for the indications covered in my presentation
 I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
Weight loss surgery more than just a gastric band
 Weight loss surgery more than just a gastric band Presented by Ms Beth Murgatroyd Honorary Bariatric Nurse Practitioner Mr Ameet G Patel Consultant Surgeon Director of Bariatric Surgery at King s College
Weight loss surgery more than just a gastric band Presented by Ms Beth Murgatroyd Honorary Bariatric Nurse Practitioner Mr Ameet G Patel Consultant Surgeon Director of Bariatric Surgery at King s College
The weight of the world.
 The weight of the world. SONY ANTHONY Obesity Derived from the Latin word obesus to devour Definition: having a very high amount of body fat in relation to lean body mass Classifications using Body Mass
The weight of the world. SONY ANTHONY Obesity Derived from the Latin word obesus to devour Definition: having a very high amount of body fat in relation to lean body mass Classifications using Body Mass
Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it
 How I do it") CENTER OF EXCELLENCE FOR THE STUDY AND OBESITY TREATMENT Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it Concepts and Results in a series of 11-years experience with 2,200 patients Miguel-A.
CENTER OF EXCELLENCE FOR THE STUDY AND OBESITY TREATMENT Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it Concepts and Results in a series of 11-years experience with 2,200 patients Miguel-A.
Surgical Treatment of Obesity: A Surgeon s View
 Surgical Treatment of Obesity: A Surgeon s View Jenny J. Choi, MD Director of Bariatrics Associate Director of Clinical Affairs Assistant Professor of Surgery Albert Einstein School of Medicine Montefiore
Surgical Treatment of Obesity: A Surgeon s View Jenny J. Choi, MD Director of Bariatrics Associate Director of Clinical Affairs Assistant Professor of Surgery Albert Einstein School of Medicine Montefiore
NHRMC General Surgery Specialists. Minimally Invasive Gastrointestinal Surgery Phone: 910-662-9300 Fax: 910-662-9303
 Minimally Invasive Gastrointestinal Surgery Phone: 910-662-9300 Fax: 910-662-9303 W. Borden Hooks III, MD 1725 New Hanover Medical Park Drive Wilmington, NC 28403 Thank you for choosing NHRMC General Surgery
Minimally Invasive Gastrointestinal Surgery Phone: 910-662-9300 Fax: 910-662-9303 W. Borden Hooks III, MD 1725 New Hanover Medical Park Drive Wilmington, NC 28403 Thank you for choosing NHRMC General Surgery
Weight-Loss Surgery for Adults With Diabetes or Prediabetes Who Are at the Lower Levels of Obesity
 Weight-Loss Surgery for Adults With Diabetes or Prediabetes Who Are at the Lower Levels of Obesity A Review of the Research for Adults With a BMI Between 30 and 35 Is This Information Right for Me? If
Weight-Loss Surgery for Adults With Diabetes or Prediabetes Who Are at the Lower Levels of Obesity A Review of the Research for Adults With a BMI Between 30 and 35 Is This Information Right for Me? If
Bariatric i Surgery: Optimalizing Outcome Results. Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende BARIATRIC SURGERY
 Bariatric i Surgery: Optimalizing i Outcome Results Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende THE OBESE PATIENT : A CHALLENGE FOR ANAESTHESIA, Ostend,14/11/09 BARIATRIC SURGERY 50 s : First Reported
Bariatric i Surgery: Optimalizing i Outcome Results Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende THE OBESE PATIENT : A CHALLENGE FOR ANAESTHESIA, Ostend,14/11/09 BARIATRIC SURGERY 50 s : First Reported
Diabetes and Weight-Loss Surgery
 WHITE PAPER Diabetes and Weight-Loss Surgery Treat the cause. Cure the symptom. Center of Excellence BARIATRIC SURGERY Written July 2011 Bariatric Surgery: The Cure for Type II Diabetes? For most individuals
WHITE PAPER Diabetes and Weight-Loss Surgery Treat the cause. Cure the symptom. Center of Excellence BARIATRIC SURGERY Written July 2011 Bariatric Surgery: The Cure for Type II Diabetes? For most individuals
UW MEDICINE PATIENT EDUCATION. Weight Loss Surgery. What is bariatric surgery?
 UW MEDICINE PATIENT EDUCATION Weight Loss Surgery Divided proximal roux-y-gastric bypass, laparoscopic adjustable gastric banding, and laparoscopic sleeve gastrectomy. This section of the Guide to Your
UW MEDICINE PATIENT EDUCATION Weight Loss Surgery Divided proximal roux-y-gastric bypass, laparoscopic adjustable gastric banding, and laparoscopic sleeve gastrectomy. This section of the Guide to Your
BARIATRIC SURGERY. Prerequisites. Authorization, Notification and Referral
 BARIATRIC SURGERY Policy NHP reimburses participating providers for specific types of medically necessary bariatric surgery when needed to either alleviate or correct medical problems caused by severe
BARIATRIC SURGERY Policy NHP reimburses participating providers for specific types of medically necessary bariatric surgery when needed to either alleviate or correct medical problems caused by severe
Laparoscopic Adjustable Gastric Banding as a Type of Weight Loss
 Laparoscopic Adjustable Gastric Banding as a Type of Weight Loss Abstract Obesity has become a global health crisis. Traditional treatments try to modify behavior in regard to diet and exercise. Laparoscopic
Laparoscopic Adjustable Gastric Banding as a Type of Weight Loss Abstract Obesity has become a global health crisis. Traditional treatments try to modify behavior in regard to diet and exercise. Laparoscopic
Position Statement Weight Loss Surgery (Bariatric Surgery) and its Use in Treating Obesity or Treating and Preventing Diabetes
 and its Use in Treating Obesity or Treating and Preventing Diabetes") Position Statement Weight Loss Surgery (Bariatric Surgery) and its Use in Treating Obesity or Treating and Preventing Diabetes People with diabetes Losing excess weight will assist in the management of
Position Statement Weight Loss Surgery (Bariatric Surgery) and its Use in Treating Obesity or Treating and Preventing Diabetes People with diabetes Losing excess weight will assist in the management of
d EFFECTIVE DATE: 11 5 2014 POLICY LAST UPDATED: 5 29 2015
 Medical Coverage Policy Bariatric Surgery-Not medically necessary procedures d EFFECTIVE DATE: 11 5 2014 POLICY LAST UPDATED: 5 29 2015 OVERVIEW Surgery for obesity, termed bariatric surgery, is a treatment
Medical Coverage Policy Bariatric Surgery-Not medically necessary procedures d EFFECTIVE DATE: 11 5 2014 POLICY LAST UPDATED: 5 29 2015 OVERVIEW Surgery for obesity, termed bariatric surgery, is a treatment
Who s Who in Bariatric Surgery: The Pioneers in the Development of Surgery for Weight Control
 HISTORY Who s Who in Bariatric Surgery: The Pioneers in the Development of Surgery for Weight Control Nelson L. Jenkins, MD, James O. Johnson, MD, Ronald P. Mageau, MD, Josie B. Bowen, MD, and Walter E.
HISTORY Who s Who in Bariatric Surgery: The Pioneers in the Development of Surgery for Weight Control Nelson L. Jenkins, MD, James O. Johnson, MD, Ronald P. Mageau, MD, Josie B. Bowen, MD, and Walter E.
Metabolic and Bariatric Surgery Center
 Metabolic and Bariatric Surgery Center www.bannerhealth.com/universitytucsonsurgicalweightloss 1 Welcome to Banner University Medical Center s Metabolic and Bariatric Surgery Center Thank you for choosing
Metabolic and Bariatric Surgery Center www.bannerhealth.com/universitytucsonsurgicalweightloss 1 Welcome to Banner University Medical Center s Metabolic and Bariatric Surgery Center Thank you for choosing
BILIOPANCREATIC DIVERSION WITH DUODENAL SWITCH SURGERY
 WITH DUODENAL SWITCH SURGERY Disclaimer This movie is an educational resource only and should not be used to manage Obesity. All decisions about surgical management of Obesity must be made in conjunction
WITH DUODENAL SWITCH SURGERY Disclaimer This movie is an educational resource only and should not be used to manage Obesity. All decisions about surgical management of Obesity must be made in conjunction
Endoscopic therapy for obesity and complications of bariatric surgery
 Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
The University of Hong Kong Department of Surgery Division of Esophageal and Upper Gastrointestinal Surgery
 Program Overview The University of Hong Kong Department of Surgery Division of Esophageal and Upper Gastrointestinal Surgery Weight Control and Metabolic Surgery Program The Weight Control and Metabolic
Program Overview The University of Hong Kong Department of Surgery Division of Esophageal and Upper Gastrointestinal Surgery Weight Control and Metabolic Surgery Program The Weight Control and Metabolic
BARIATRIC SURGERY (SURGERY FOR THE TREATMENT OF OBESITY)
") BARIATRIC SURGERY (SURGERY FOR THE TREATMENT OF OBESITY) WHAT IS OBESITY? Obesity is the condition whereby the individual sustains the body weight that is significantly higher than ideal body weight for
BARIATRIC SURGERY (SURGERY FOR THE TREATMENT OF OBESITY) WHAT IS OBESITY? Obesity is the condition whereby the individual sustains the body weight that is significantly higher than ideal body weight for
Treatment for Severely Obese Patients
 Treatment for Severely Obese Patients Associate Professor Jimmy So Senior Consultant Surgeon Director, Centre for Obesity Management and Surgery (COMS) National University Hospital Obesity Shortens Lives
Treatment for Severely Obese Patients Associate Professor Jimmy So Senior Consultant Surgeon Director, Centre for Obesity Management and Surgery (COMS) National University Hospital Obesity Shortens Lives
Gastric Sleeve Surgery
 Gastric Sleeve Surgery Introduction Obesity is associated with many diseases such as diabetes, high blood pressure, heart problems, and degeneration of the joints. These diseases and the obesity itself
Gastric Sleeve Surgery Introduction Obesity is associated with many diseases such as diabetes, high blood pressure, heart problems, and degeneration of the joints. These diseases and the obesity itself
INFORMED CONSENT FOR LAPAROSCOPIC GASTRIC SLEEVE SURGICAL PROCEDURE
 INFORMED CONSENT FOR LAPAROSCOPIC GASTRIC SLEEVE SURGICAL PROCEDURE It is very important to [insert physician, practice name] that you understand and consent to the treatment your doctor is rendering and
INFORMED CONSENT FOR LAPAROSCOPIC GASTRIC SLEEVE SURGICAL PROCEDURE It is very important to [insert physician, practice name] that you understand and consent to the treatment your doctor is rendering and
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Changes to Bariatric Surgery Prior Authorization Guidelines
 Update August 2011 No. 2011-44 Affected Programs: BadgerCare Plus, Medicaid To: Hospital Providers, Physician Assistants, Physician Clinics, Physicians, HMOs and Other Managed Care Programs Changes to
Update August 2011 No. 2011-44 Affected Programs: BadgerCare Plus, Medicaid To: Hospital Providers, Physician Assistants, Physician Clinics, Physicians, HMOs and Other Managed Care Programs Changes to
INFORMATION SHEET FOR A LAPAROSCOPIC SLEEVE GASTRECTOMY
 INFORMATION SHEET FOR A LAPAROSCOPIC SLEEVE GASTRECTOMY You are considering undergoing a laparoscopic sleeve gastrectomy for weight loss. The purpose of this information sheet is to provide you with the
INFORMATION SHEET FOR A LAPAROSCOPIC SLEEVE GASTRECTOMY You are considering undergoing a laparoscopic sleeve gastrectomy for weight loss. The purpose of this information sheet is to provide you with the
Laparoscopic Sleeve gastrectomy
 Restrictive procedure Laparoscopic Sleeve gastrectomy Dr. R. Peterli Professional Education 1 2 Introduction Gastric sleeve resection is the restrictive part of the biliopancreatic diversion duodenal switch,
Restrictive procedure Laparoscopic Sleeve gastrectomy Dr. R. Peterli Professional Education 1 2 Introduction Gastric sleeve resection is the restrictive part of the biliopancreatic diversion duodenal switch,
INFORMED CONSENT FOR POSSIBLE REMOVAL OF ADJUSTABLE GASTRIC BAND AND CONVERSION TO ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE
 INFORMED CONSENT FOR POSSIBLE REMOVAL OF ADJUSTABLE GASTRIC BAND AND CONVERSION TO ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to [insert physician, practice name] that you understand
INFORMED CONSENT FOR POSSIBLE REMOVAL OF ADJUSTABLE GASTRIC BAND AND CONVERSION TO ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to [insert physician, practice name] that you understand
Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of
 Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of Surgery & Associate Residency Program Director UC Irvine
Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of Surgery & Associate Residency Program Director UC Irvine
Weight Loss before Hernia Repair Surgery
 Weight Loss before Hernia Repair Surgery What is an abdominal wall hernia? The abdomen (commonly called the belly) holds many of your internal organs. In the front, the abdomen is protected by a tough
Weight Loss before Hernia Repair Surgery What is an abdominal wall hernia? The abdomen (commonly called the belly) holds many of your internal organs. In the front, the abdomen is protected by a tough
Surgical Weight Loss Program for Teens
 Surgical Weight Loss Program for Teens Surgical Weight Loss Program for Teens The Surgical Weight Loss Program team understands the impact that being severely overweight can have on your life. Our guiding
Surgical Weight Loss Program for Teens Surgical Weight Loss Program for Teens The Surgical Weight Loss Program team understands the impact that being severely overweight can have on your life. Our guiding
Bariatric Surgery. Beth A. Ryder, MD FACS. Assistant Professor of Surgery The Miriam Hospital Warren Alpert Medical School of Brown University
 Bariatric Surgery Beth A. Ryder, MD FACS Assistant Professor of Surgery The Miriam Hospital Warren Alpert Medical School of Brown University April 30, 2013 Why surgery? Eligibility criteria Most commonly
Bariatric Surgery Beth A. Ryder, MD FACS Assistant Professor of Surgery The Miriam Hospital Warren Alpert Medical School of Brown University April 30, 2013 Why surgery? Eligibility criteria Most commonly
Section 2. Overview of Obesity, Weight Loss, and Bariatric Surgery
 Section 2 Overview of Obesity, Weight Loss, and Bariatric Surgery What is Weight Loss? How does surgery help with weight loss? Short term versus long term weight loss? Conditions Improved with Weight Loss
Section 2 Overview of Obesity, Weight Loss, and Bariatric Surgery What is Weight Loss? How does surgery help with weight loss? Short term versus long term weight loss? Conditions Improved with Weight Loss
The Role of Obesity in Bariatric Surgery - Part 1
 MORBID OBESITY: The Role of Bariatric Surgery Rajan V. Nair, MD Medical Director Salem Hospital Bariatric Surgery Program ICL Willamette University Tuesday November 27, 2012 DISCLOSURES Medical Director,
MORBID OBESITY: The Role of Bariatric Surgery Rajan V. Nair, MD Medical Director Salem Hospital Bariatric Surgery Program ICL Willamette University Tuesday November 27, 2012 DISCLOSURES Medical Director,
Understanding Obesity
 Your Guide to Understanding Obesity As your partner in health for your life s journey, we want you to be as informed and confident as possible regarding the disease or medical issue you may be facing.
Your Guide to Understanding Obesity As your partner in health for your life s journey, we want you to be as informed and confident as possible regarding the disease or medical issue you may be facing.
BARIATRIC SURGERY PATIENT GUIDE
 You the patient play a critical role in the long term success of surgery. You will need to: Commit to improving your health. Discuss your health history with your surgeon. Discuss any questions or concerns
You the patient play a critical role in the long term success of surgery. You will need to: Commit to improving your health. Discuss your health history with your surgeon. Discuss any questions or concerns
BRIAN TIU - PGY 5 KING COUNTY HOSPITAL COMPLICATIONS OF LAPAROSCOPIC GASTRIC BANDING
 BRIAN TIU - PGY 5 KING COUNTY HOSPITAL COMPLICATIONS OF LAPAROSCOPIC GASTRIC BANDING PATIENT PRESENTATION HISTORY 36 yo female morbid obesity, laparoscopic gastric banding 2008 Mar 2015 small bowel resection,
BRIAN TIU - PGY 5 KING COUNTY HOSPITAL COMPLICATIONS OF LAPAROSCOPIC GASTRIC BANDING PATIENT PRESENTATION HISTORY 36 yo female morbid obesity, laparoscopic gastric banding 2008 Mar 2015 small bowel resection,
 Redo Banding After Band Erosion Advantages of the MiniMizer Extra Band Conclusion Approximately 67% of the patients suffering from erosion have sought revisional surgery. The choice of redo procedures
Redo Banding After Band Erosion Advantages of the MiniMizer Extra Band Conclusion Approximately 67% of the patients suffering from erosion have sought revisional surgery. The choice of redo procedures
GASTRIC BYPASS SURGERY CONSENT FORM
 Page 1 of 6 I, have been asked to read carefully all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described below on
Page 1 of 6 I, have been asked to read carefully all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described below on
Why a loop and new approach makes sense!
 IP: tomach Intestinal Pylorus paring urgery Why a loop and new approach makes sense! Mitchell Roslin, MD, FAC Chief of Bariatric and Metabolic urgery Lenox Hill Hospital Northern Westchester Hospital Center
IP: tomach Intestinal Pylorus paring urgery Why a loop and new approach makes sense! Mitchell Roslin, MD, FAC Chief of Bariatric and Metabolic urgery Lenox Hill Hospital Northern Westchester Hospital Center
Sudbury Bariatric Regional Assessment & Treatment Centre
 Sudbury Bariatric Regional Assessment & Treatment Centre Outline Obesity as a Chronic Disease 5 A s of Obesity Management OBN & BRATC Referral Process Obesity Definition BMI Normal Weight 18.5-24.9 Overweight
Sudbury Bariatric Regional Assessment & Treatment Centre Outline Obesity as a Chronic Disease 5 A s of Obesity Management OBN & BRATC Referral Process Obesity Definition BMI Normal Weight 18.5-24.9 Overweight
Bariatric Surgery Guide
 One Bariatric Surgery Guide Get back to enjoying the everyday moments. Obesity is one of the nation s leading health issues. More than half of Americans are overweight and roughly 12 million Americans
One Bariatric Surgery Guide Get back to enjoying the everyday moments. Obesity is one of the nation s leading health issues. More than half of Americans are overweight and roughly 12 million Americans
5/9/2012. What is Morbid Obesity? Obesity Trends* Among U.S. Adults BRFSS, 1990, 1998, 2007 (*BMI 30, or about 30 lbs. overweight for 5 4 person)
") Obesity Trends* Among U.S. Adults BRFSS, 1990, 1998, 2007 (*BMI 30, or about 30 lbs. overweight for 5 4 person) 1990 1998 The Bariatric and Metabolic Center of Colorado Bariatric Surgery: Options, Care
Obesity Trends* Among U.S. Adults BRFSS, 1990, 1998, 2007 (*BMI 30, or about 30 lbs. overweight for 5 4 person) 1990 1998 The Bariatric and Metabolic Center of Colorado Bariatric Surgery: Options, Care
www.ghadialisurgery.com
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
BARIATRIC SURGERY AND OTHER INVASIVE TREATMENTS FOR OBESITY
 Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline must be read in its
Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline must be read in its
Bariatric Surgery 101
 Bariatric Surgery 101 Dr. Brent Bell, MD Bariatric / General Surgeon Medical Conditions Caused By Morbid Obesity Type 2 DM Hypertension Cholesterol Sleep Apnea Fatty Liver Asthma Osteoarthritis Reduced
Bariatric Surgery 101 Dr. Brent Bell, MD Bariatric / General Surgeon Medical Conditions Caused By Morbid Obesity Type 2 DM Hypertension Cholesterol Sleep Apnea Fatty Liver Asthma Osteoarthritis Reduced
Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery
 Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Obesity Obesity is defined as having a body mass index (BMI) of 30 or greater. Obesity is a serious medical
Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Obesity Obesity is defined as having a body mass index (BMI) of 30 or greater. Obesity is a serious medical
Scott A. Shikora, MD, FACS. Sleeve Gastrectomy. Sleeve Gastrectomy. Sleeve Gastrectomy 11/8/2013
 DISCLOSURE Scott A. Shikora, MD, FACS Scott A. Shikora, MD, FACS Associate Professor of Surgery Harvard Medical School Director, Center for Metabolic and Bariatric Surgery Brigham and Women s Hospital
DISCLOSURE Scott A. Shikora, MD, FACS Scott A. Shikora, MD, FACS Associate Professor of Surgery Harvard Medical School Director, Center for Metabolic and Bariatric Surgery Brigham and Women s Hospital
really help your physical, social and emotional wellbeing helping you do more of the things you want and feel more confident and relaxed.
 Weight loss surgery If you are seriously overweight, losing excess weight can transform your life. Find out how you can make that change with the help of Spire Healthcare. If you One are off seriously
Weight loss surgery If you are seriously overweight, losing excess weight can transform your life. Find out how you can make that change with the help of Spire Healthcare. If you One are off seriously
Bariatric and Metabolic Surgery
 Bariatric and Metabolic Surgery It may reduce more than just your weight. It may reduce certain risk factors. The information in this brochure is intended as Before Cholesterol 250 Blood pressure 149/95
Bariatric and Metabolic Surgery It may reduce more than just your weight. It may reduce certain risk factors. The information in this brochure is intended as Before Cholesterol 250 Blood pressure 149/95
Bariatric Surgery. OHTAC Recommendation. Bariatric Surgery
 OHTAC Recommendation Bariatric Surgery January 21, 2005 1 The Ontario Health Technology Advisory Committee (OHTAC) met on January 21, 2005 and reviewed bariatric surgery for morbid obesity. Obesity is
OHTAC Recommendation Bariatric Surgery January 21, 2005 1 The Ontario Health Technology Advisory Committee (OHTAC) met on January 21, 2005 and reviewed bariatric surgery for morbid obesity. Obesity is
Morbid obesity is defined as a body mass index (BMI) >40 kg/m2 (normal BMI range: 19-25 kg/m2)
 >40 kg/m2 (normal BMI range: 19-25 kg/m2)") Medical Policy Manual Topic: Bariatric Surgery Date of Origin: January 1996 Section: Surgery Last Reviewed Date: May 2016 Policy No: 58 Effective Date: June 1, 2016 IMPORTANT REMINDER Medical Policies
Medical Policy Manual Topic: Bariatric Surgery Date of Origin: January 1996 Section: Surgery Last Reviewed Date: May 2016 Policy No: 58 Effective Date: June 1, 2016 IMPORTANT REMINDER Medical Policies
Consent Document for Bariatric Surgery
 Consent Document for Bariatric Surgery I,, have read and understand the following document completely. In addition, my surgeon has discussed with me at length and I completely understand the risks, benefits,
Consent Document for Bariatric Surgery I,, have read and understand the following document completely. In addition, my surgeon has discussed with me at length and I completely understand the risks, benefits,
Having a Gastric Band
 Having a Gastric Band Hope Building Upper G.I. / Bariatrics 0161 206 5062 All Rights Reserved 2014. Document for issue as handout. This booklet aims to describe: l What is a gastric band page 2 l How is
Having a Gastric Band Hope Building Upper G.I. / Bariatrics 0161 206 5062 All Rights Reserved 2014. Document for issue as handout. This booklet aims to describe: l What is a gastric band page 2 l How is
biliopancreatic bypass; a surgical procedure involving a gastric restriction diverting bile and pancreatic juice into the distal ileum.
 SURGERY FOR MORBID OBESITY SUR716.003 COVERAGE: Surgical procedures which may be eligible for coverage for the treatment of morbid or clinically severe obesity are: 1. Vertical banded gastroplasty (gastric
SURGERY FOR MORBID OBESITY SUR716.003 COVERAGE: Surgical procedures which may be eligible for coverage for the treatment of morbid or clinically severe obesity are: 1. Vertical banded gastroplasty (gastric
MORTALITY RISK FACTORS IN PATIENTS UNDERGOING GASTRIC BYPASS SURGERY
 Where Do We Stand? Alan M. Brader, MD Lancaster General Bariatrics Introduction The management of a patient with extreme obesity is a challenging task for most health care givers. Unfortunately, there
Where Do We Stand? Alan M. Brader, MD Lancaster General Bariatrics Introduction The management of a patient with extreme obesity is a challenging task for most health care givers. Unfortunately, there
GASTRIC SLEEVE SURGERY FOR WEIGHT LOSS. www.carepointhealth.org GASTRIC SLEEVE SURGERY FOR WEIGHT LOSS. 201-795-8175 CarePointHealth.
 www.carepointhealth.org GASTRIC SLEEVE SURGERY FOR WEIGHT LOSS 201-795-8175 CarePointHealth.org 1 CONTENTS What is sleeve gastrectomy? Why choose sleeve gastrectomy? Health risks associated with excess
www.carepointhealth.org GASTRIC SLEEVE SURGERY FOR WEIGHT LOSS 201-795-8175 CarePointHealth.org 1 CONTENTS What is sleeve gastrectomy? Why choose sleeve gastrectomy? Health risks associated with excess
Bariatric Surgery Guide Dr. Stewart s Weight Loss Specialists of North Texas
 Welcome. This resource is created for you by Dr. Stewart and our bariatric surgery team with input from people who have found success through weight loss surgery. It is not intended to replace consultation
Welcome. This resource is created for you by Dr. Stewart and our bariatric surgery team with input from people who have found success through weight loss surgery. It is not intended to replace consultation
Morbid obesity is defined as a body mass index (BMI) >40 kg/m2 (normal BMI range: 19-25 kg/m2)
 >40 kg/m2 (normal BMI range: 19-25 kg/m2)") Medical Policy Manual Topic: Bariatric Surgery Date of Origin: January 1996 Section: Surgery Last Reviewed Date: August 2015 Policy No: 58 Effective Date: September 1, 2015 IMPORTANT REMINDER Medical Policies
Medical Policy Manual Topic: Bariatric Surgery Date of Origin: January 1996 Section: Surgery Last Reviewed Date: August 2015 Policy No: 58 Effective Date: September 1, 2015 IMPORTANT REMINDER Medical Policies
Weight Loss Surgery Educational Seminar
 Weight Loss Surgery Educational Seminar Attendee Handout Obesity Overview Obesity is on the rise in the US Body Mass Index (BMI) (see chart in this handout, page 9) o 18.5-24.9: Ideal Less than 1/3 of
Weight Loss Surgery Educational Seminar Attendee Handout Obesity Overview Obesity is on the rise in the US Body Mass Index (BMI) (see chart in this handout, page 9) o 18.5-24.9: Ideal Less than 1/3 of
INFORMATION SHEET FOR A LAPAROSCOPIC GASTRIC BAND
 INFORMATION SHEET FOR A LAPAROSCOPIC GASTRIC BAND You are considering undergoing a laparoscopic gastric band for weight loss. The purpose of this information sheet is to provide you with the necessary
INFORMATION SHEET FOR A LAPAROSCOPIC GASTRIC BAND You are considering undergoing a laparoscopic gastric band for weight loss. The purpose of this information sheet is to provide you with the necessary
Weight Loss Surgery. Malabsorptive: Your intestines are rearranged to reduce the amount of food absorbed into the system
 The Region s Leader Weight Loss Surgery Table of Contents About Weight Loss Surgery 1 Laparoscopic Procedures 2 Adjustable Gastric Band 2 Biliopancreatic Diversion With Duodenal Switch 3 Rou-en-Y (RNY)
The Region s Leader Weight Loss Surgery Table of Contents About Weight Loss Surgery 1 Laparoscopic Procedures 2 Adjustable Gastric Band 2 Biliopancreatic Diversion With Duodenal Switch 3 Rou-en-Y (RNY)
Your Practice Online
 P R E S E N T S Your Practice Online Disclaimer This information is an educational resource only and should not be used to manage Obesity. All decisions about surgical management of Obesity must be made
P R E S E N T S Your Practice Online Disclaimer This information is an educational resource only and should not be used to manage Obesity. All decisions about surgical management of Obesity must be made
The obesity epidemic has grown in severity over the. Bariatric Surgery: A Review of Procedures and Outcomes
 GASTROENTEROLOGY 2007;132:2253 2271 Bariatric Surgery: A Review of Procedures and Outcomes KATHERINE A. ELDER and BRUCE M. WOLFE Department of Surgery, Oregon Health & Science University, Portland, Oregon
GASTROENTEROLOGY 2007;132:2253 2271 Bariatric Surgery: A Review of Procedures and Outcomes KATHERINE A. ELDER and BRUCE M. WOLFE Department of Surgery, Oregon Health & Science University, Portland, Oregon
Surgical Weight Loss Program SURG CAL WEIGHT LOSS. at University Medical Center
 Surgical Weight Loss Program 1 SURG CAL WEIGHT LOSS at University Medical Center Welcome to the University Medical Center Surgical Weight Loss Program Thank you for choosing UMC for your weight loss surgery.
Surgical Weight Loss Program 1 SURG CAL WEIGHT LOSS at University Medical Center Welcome to the University Medical Center Surgical Weight Loss Program Thank you for choosing UMC for your weight loss surgery.
HOUSTON METHODIST SURGICAL WEIGHT LOSS
 HOUSTON METHODIST SURGICAL WEIGHT LOSS Why choose surgical weight loss at Houston Methodist? Obesity causes many dangerous diseases and health conditions such as diabetes, high blood pressure, heart disease,
HOUSTON METHODIST SURGICAL WEIGHT LOSS Why choose surgical weight loss at Houston Methodist? Obesity causes many dangerous diseases and health conditions such as diabetes, high blood pressure, heart disease,