Cáncer Renal avanzado. Nuevas estrategias para el tratamiento individualizado.
|
|
|
- Brett Summers
- 8 years ago
- Views:
Transcription
1 Cáncer Renal avanzado. Nuevas estrategias para el tratamiento individualizado. Daniel Castellano Oncología Médica.Unidad de Tumores GenitoUrinarios Hospital Universitario 12 de Octubre. I + 12 Research Institute

 1 Temsirolimus (May 2007) 3 Bevacizumab + IFN-α (Jul 2009) 5 Everolimus (Mar 2009) 4 Axitinib")
")
2 Treatment options for metastatic RCC have been revolutionised in a short period of time Sunitinib (Jan 2006) 2 Pazopanib (Oct 2009) 6 High dose interleukin-2 IFN-α Sorafenib (Dec 2005) 1 Temsirolimus (May 2007) 3 Bevacizumab + IFN-α (Jul 2009) 5 Everolimus (Mar 2009) 4 Axitinib (Jan 2012) US FDA. Sorafenib, US FDA. Sunitinib malate, US FDA. Temsirolimus, US FDA. Everolimus, US FDA. Bevacizumab, US FDA. Pazopanib, US FDA. Axitinib, Tivozanib (2012??)
")
3 RCC: efficacy proven across histological subtypes Tumour type Clear cell Papillary (type I + II) Chromophobic Histology 1 Incidence (% of all RCCs) Note: patients may have more than one histological subtype 1. Linehan WM, et al. J Urol 2003; 2. Motzer RJ, et al. N Engl J Med Escudier B, et al. N Engl J Med 2007; 4. Beck J, et al. ECCO Knox JJ, et al. EMUC 2007; 6. Chouieri TK, et al. J Clin Oncol Golshayan AR, et al. ASCO-GU 2008; 8. Motzer RJ, et al. J Clin Oncol 2002

4


5

6
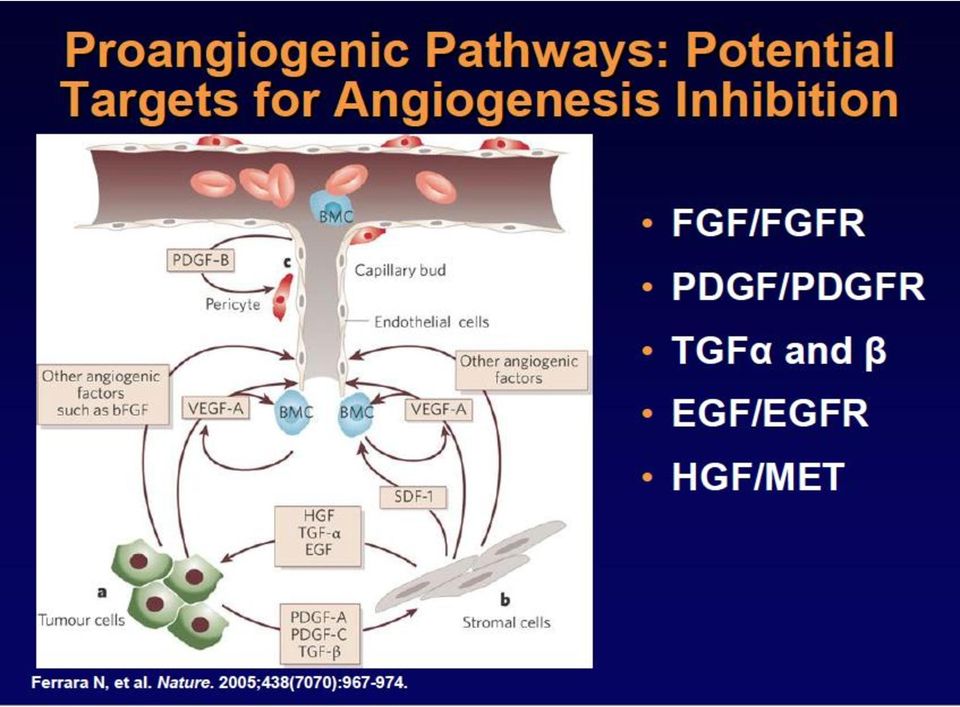
7 Overview of targeted agents in mrcc1 5 Bevacizumab Anti-angiogenesis VEGF-A VEGF-B VEGF-C VEGF-D VEGF-E VEGFR-2 VEGFR-1 PDGFR-α VEGFR-3 PDGFR-ß c-kit Flt-3 References are in slide notes Pazopanib Raf Sorafenib Sunitinib Preclinical in vitro data need to be validated in a clinical setting 5

8 Patient-focused treatment strategy Need to define the optimal setting for each treatment the best treatment for each given patient For any given patient, treatment decisions require consideration of multiple factors disease characteristics patient characteristics treatment aim and previous treatment history

9 Which parameters potentially influence treatment choices? Disease characteristics sites and number of metastases tumour histology MSKCC risk Patient characteristics age cardiac risk renal impairment general comorbidities/overall health of patient Treatment aim and previous treatment history objective of treatment suitability for cytokine therapy failure of prior therapy

10 Proposed schema: factors to consider prior to prescribing treatment for RCC DISEASE MSKCC Good Intermediate Poor No. met sites >4 Site of mets Lymph nodes Liver Lung Bone Brain Histology Clear cell Non-clear cell PATIENT Age P.S. Comorbidity Haematological Wound healing <65 years 65 years Controlled HT Cardiac disease grade 2* > grade 2* Diabetes Fatigue Thyroid Cirrhosis Renal Naive TREATMENT History Suitable for CK Unsuitable for CK Prior CK Prior targeted therapy Aim Prolong survival Tumour shrinkage Disease stabilisation Maintain QoL * Including controlled arrhythmias CK = cytokine; HT = hypertension; mets = metastases; PS = performance status; QoL = quality of life

11 Aim of treatment for RCC Naive TREATMENT History Suitable for CK Unsuitable for CK Prior CK Prior targeted therapy Aim Prolong survival Tumour shrinkage Disease stabilisation Maintain QoL

12 Selecting first-line treatment: A clinician s perspective Efficacy is key when selecting first-line treatment, but there are also other considerations Robust evidence and guidelines Experience Patient characteristics Patient preference

13 Algoritmo CCRm Setting Patients Therapy Options First-line Favourable- or Sunitinib HD IL-2 intermediate-risk Pazopanib Tivozanib? Cytokines Sorafenib Beva - IFN-α Poor-risk Temsirolimus Sunitinib Second-line Prior cytokine Axitinib Pazopanib Sorafenib Sunitinib Prior VEGF TKI Axitinib Sorafenib? Prior VEGF TKI Everolimus Clinical trial Adapted from EAU guidelines 2010, ESMO Clinical Recommendations 2009, NCCN guidelines 2010 SOGUG 2010

14 Recommended targeted agents for first-line treatment: Results from pivotal trials Agent n Median PFS (months) Median OS (months) ORR (%) Sunitinib vs IFN-α vs 5 p<0.001 Bevacizumab + IFN-α vs IFN-α 2, vs 5.4 p< Bevacizumab + IFN-α vs IFN-α 4, vs 5.2 p< Pazopanib vs placebo 6, vs 2.8 p< Poor-risk patients Temsirolimus vs IFN-α vs 3.1 p<0.001 *Includes cytokine refractory and treatment-naïve patients; Poor-risk patients (modified MSKCC criteria) NS, not studied 26.4 vs 21.8 p= vs 21.3 p= vs 17.4 p= vs 20.5* p= vs 7.3 p= vs 12 p< vs 13 p= vs 13 p< vs 3* p< vs 4.8 NS 1. Motzer RJ, et al. J Clin Oncol 2009;27: ; 2. Escudier B, et al. Lancet 2007;370: ; 3. Escudier B, et al. J Clin Oncol 2010;28: ; 4. Rini BI, et al. J Clin Oncol 2008;26:5422 8; 5. Rini BI, et al. J Clin Oncol 2010;28: ; 6. Sternberg C, et al. J Clin Oncol 2010;28:1061 8; 7. Sternberg C, et al. Eur J Cancer 2013;49: ; 8. Hudes G, et al. New Engl J Med 2007;356:

15 Probabilidad de SLP Probability of survival Sunitinib : Estudio fase III como tratamiento de primera línea en el CCR avanzado Criterios de elegibilidad 18 años de edad CCRm Histología de células claras Sin tratamiento sistémico previo Enfermedad medible por RECIST ECOG PS 0 o 1 Función orgánica adecuada Mediana de la SLP (revisión central independiente) Sunitinib Mediana: 11.0 meses (95% IC: ) IFN-α Mediana: 5.1 meses (95% IC: ) N=750 A L E A T O R I Z A C I Ó N Sunitinib 50 mg diario (Esquema 4/2) N=375 IFN-α 3 MU SC, TIW primera semana, 6 MU SC, TIW segunda semana, 9 MU SC, TIW a partir de entonces N=375 Mediana de SG Sunitinib (n=375) Mediana: 26.4 meses (95% IC: ) IFN-α (n=375) Mediana: 21.8 meses (95% IC: ) HR=0.538 (95% IC ) P< Tiempo (meses) No. en riesgo Sunitinib: IFN-α: HR=0.821 (95% IC: ) P=0.051 (log-rank) Total deaths Sunitinib 190 IFN-α Tiempo (meses) nmuertes/nriesgo Sunitinib /326 38/283 48/229 42/180 14/61 4/2 IFN-α /295 46/242 52/187 25/149 15/53 1/1 RECIST = Response Evaluation Criteria in Solid Tumors; ECOG = Eastern Cooperative Oncology Group; SLP = supervivencia libre de progresión; SG = supervivencia global Motzer RJ, et al. N Engl J Med 2007 Motzer RJ, et al. ASCO 2007; Motzer RJ, et al. J Clin Oncol 2009
 N=375 IFN-α 3 MU SC, TIW primera semana, 6 MU SC, TIW segunda semana, 9 MU SC, TIW a partir de entonces N=375 Mediana de SG Sunitinib (n=375) Mediana: 26.")
 1.0 0.8 SG Mediana: 18.4 meses (95% lc: 17.4 19.2) 0.6 0.4 0.2 0 0 10 20 30 Tiempo (meses) No. en riesgo 4,349 1,316 136 0 0.6 0.4 0.2 0 0 10 20 30 Tiempo (meses) 4,349 2,429 525 0 Gore ME, et al.")
16 Probabilidad Probabilidad Programa de acceso expandido de Sunitinib: Escenario Real Programa internacional que incluyó 4,564 pacientes con CCRm (vírgenes al tratamiento o refractarios a citokinas) SLP Mediana: 10.9 meses (95% lc: ) SG Mediana: 18.4 meses (95% lc: ) Tiempo (meses) No. en riesgo 4,349 1, Tiempo (meses) 4,349 2, Gore ME, et al. Lancet Oncol 2009
 No. en riesgo 4,349 1,316 136 0 0.6 0.4 0.")
 p value (1-sided) 2.8 11.1 0.40 (0.27, 0.60) <0.0001 0.6 0.4 Pazopanib 11.1 mo 0.2 0.")
 11 2 1 1. Sternberg et al.")
17 Proportion progression-free Progression-free survival in the treatment-naïve subpopulation 1.0 Median PFS (months) 0.8 Placebo Pazopanib Hazard ratio (95% CI) p value (1-sided) (0.27, 0.60) < Pazopanib 11.1 mo Pazopanib Placebo Number at risk, n Pazopanib Placebo Time (month) In the treatment-naïve subpopulation, PFS was significantly greater in pazopanib- versus placebotreated patients (p<0.0001) Sternberg et al. J Clin Oncol 2010;28:
 11 2 1 1. Sternberg et al.")
18 COMPARZ study design: Phase III, open-label, non-inferiority trial Enrolment criteria: Locally advanced or mrcc Clear-cell histology No prior systemic therapy Measurable disease (RECIST 1.0) KPS 70 Adequate organ function N=927 N=1,110 Randomised 1:1 Pazopanib 800 mg QD Continuous daily dosing Sunitinib 50 mg QD Schedule 4/2 Study start: August 2008 VEG Phase III n=927 VEG Phase II (Asia) n=183 COMPARZ: 1,110 patients KPS, Karnofsky Performance Scale; RECIST, Response Evaluation Criteria in Solid Tumors; Schedule 4/2, 4 weeks on treatment, 2 weeks off (NCT ; NCT )
 n=183 COMPARZ: 1,110 patients KPS, Karnofsky Performance Scale; RECIST, Response")
19 Proportion progression-free COMPARZ primary endpoint: PFS (IRC-assessed) 1.0 N Median PFS (95% CI) 0.8 Pazopanib mo (8.3, 10.9) Sunitinib mo (8.3, 11.1) HR (95% CI ) = (0.898,1.220) Months Number at risk Pazopinib Sunitinib Motzer RJ, et al. Presented at ESMO 2012; Abstract LBA8

20 COMPARZ: PFS (IRC-assessed) 1,2 Non-inferiority met if upper bound of 95% CI for HR <1.25 (EMA requested ) PFS (ITT population) Pazopanib (n=557) Sunitinib (n=553) Median PFS, months (95% CI) 8.4 (8.3, 10.9) 9.5 (8.3, 11.1) HR (95% CI) (0.8982, ) PFS (PP population) Pazopanib (n=501) Sunitinib (n=494) Median PFS, months (95% CI) 8.4 (8.3, 10.9) 10.2 (8.3, 11.1) HR (95% CI) (0.910, 1.255) PP, per-protocol 1. GSK. Clinical Study Register. Study Available at: (last accessed February 2013); 2. Motzer RJ, et al. Presented at ESMO 2012; Abstract LBA8; 3. Available at (last accessed April 2013)
; 2. Motzer RJ, et al.")
21 Laboratory Abnormalities Chemistry labs ( 35%) ALT AST Hypoalbuminemia Bilirubin Creatinine Hyperglycemia Hyponatremia Hypophosphatemia Hematology labs Leukopenia Neutropenia Thrombocytopenia Lymphopenia Anemia Pazopanib (n = 554), % All Grades Sunitinib (n = 548),% All Grades Yellow highlight: Risk greater for pazopanib and 95% CI for relative risk does not cross 1
22 Laboratory Abnormalities Chemistry labs ( 35%) ALT AST Hypoalbuminemia Bilirubin Creatinine Hyperglycemia Hyponatremia Hypophosphatemia Hematology labs Leukopenia Neutropenia Thrombocytopenia Lymphopenia Anemia Pazopanib (n = 554), % All Grades Sunitinib (n = 548),% All Grades Blue highlight: Risk greater for sunitinib and 95% CI for relative risk does not cross 1
23 COMPARZ: Common AEs (treatment-emergent) AE* Pazopanib (n=554), % Sunitinib (n=548), % Risk ratio All grades Grade 3/4 All grades Grade 3/4 All grades 95% CI Any event >99 59/15 >99 57/17 NA NA Diarrhoea 63 9/0 57 7/< , 1.20 Fatigue 55 10/< /< , 0.96 Hypertension 46 15/< /< , 1.31 Nausea 45 2/0 46 2/ , 1.11 Decreased appetite 37 1/0 37 3/0 NA NA ALT increased 31 10/2 18 2/< , 2.17 Hair colour changes 30 0/0 10 <1/0 NA NA HFS 29 6/ /< , 0.68 Taste alteration 26 <1/0 36 0/0 NA NA Thrombocytopenia 10 2/< / , 0.40 *AE 30% in either arm; 2% of patients in pazopanib arm and 3% of patients in sunitinib arm had grade 5 AEs ALT, alanine transaminase; AST, aspartate transaminase; HFS, hand foot syndrome; NA, not applicable
24 TIVO-1 Trial: Phase III Head-to-Head Trial of Tivozanib Vs. Sorafenib Eligibility Requirements Advanced clear cell RCC Prior nephrectomy No prior VEGF treatment ECOG PS: 0 1 First head-to-head RCC registration trial vs. an active comparator Primary end point: PFS Secondary end points: OS, ORR, QOL Treatment schedule (1 cycle = 4 wks) Tivozanib: 1.5 mg/day for 3 wks, followed by 1-wk break Sorafenib: 800 mg/day for 4 wks R A N D O M I Z E 1:1 Tivozanib (n = 250) Sorafenib (n = 250) PD Tivozanib Extension Protocol Continue tivozanib until PD Continue sorafenib until PD QOL = quality of life. US NIH, 2011a, 2011b.
25 [TITLE]
26 Study design* Previously untreated metastatic RCC R A N D O M I Z E 2:1 Axitinib 5 mg BID (n=192) Sorafenib 400 mg BID (n=96) Randomization stratified by ECOG PS (0 vs 1). * ClinicalTrials.gov: NCT Titrated stepwise to 7 mg BID and then 10 mg BID in patients without grade 3 or 4 (CTCAE v3.0) axitinib-related AEs for a consecutive 2-week period, unless BP >150/90 mmhg. Hutson TE et al. Abstract No. 348, ASCO-GU
27 PFS (probability) Progression-free survival (IRC Assessment) = censored for axitinib = censored for sorafenib Axitinib Sorafenib Time (months) No. events (%) 111 (58) 60 (63) Stratified HR, 0.77* (95% CI ) 1-sided P= mpfs, mo (95%CI) 10.1 ( ) 6.5 ( ) *Stratified by ECOG PS; assuming proportional hazards, HR <1 indicates a reduction in favor of axitinib and HR >1 indicates a reduction in favor of sorafenib. IRC = independent radiology committee; mpfs = median progression-free survival Patients at risk, n Axitinib Sorafenib
28 Conclusions Study did not achieve its primary endpoint statistically Statistical design: HR=0.56 (high bar) Actual: HR=0.77 (95% CI );1-sided P=0.038 PFS difference observed in subgroups vs sorafenib Patients with nephrectomy: 10.3 vs 6.4 mo* (P=0.009) PS 0: 13.7 vs 6.6 mo (P=0.022) ~90% patients from outside the US (variability in PS 0 vs 1) First-line therapy with axitinib demonstrated Numerically longer PFS (3.6-mo improvement) Significantly higher ORR Acceptable safety profile OS data not yet mature * Unstratified HR, 0.67 (95% CI ) Unstratified HR, 0.64 (95% CI ) Hutson TE et al. Abstract No. 348, ASCO-GU
29 Selecting first-line treatment: A clinician s perspective Efficacy is key when selecting first-line treatment, but there are also other considerations Robust evidence and guidelines Experience Patient characteristics Patient preference
30 Modelos Integrados de Predicción Pronóstica en CCR avanzado
31 Comorbidities Are Common In Patients With RCC 54% of patients with kidney cancer have at least one comorbidity. 1 72% of patients 75 years of age with kidney cancer have at least one comorbidity. 1 The most common comorbidities are heart disease, hypertension, and diabetes Coebergh JWW, et al. J Clin Epidemiol. 1999;52:
32 P e r c e n t S u r v i v i n g Extent of Comorbidities Correlates with OS in RCC Patients Undergoing Nephrectomy Retrospective study of patients with RCC who underwent radical or partial nephrectomy (N = 697) Cormorbidities were scored based on the Adult Comorbidity Evaluation-27 (ACE-27) validated tool 75% of patients had at least 1 comorbidity Median follow-up was 36.5 months Overall survival for all patients at 1, 3, and 5 years was 92.0%, 75.3%, and 52.7%, respectively N o n e M i l d M o d e r a t e S e v e r e Severe vs. None Adjusted HR: % CI: P < D u r a t i o n ( Y e a r s ) Berger DA, et al. Urology. 2008;72(2):
33 Multivariate models of associations between AEs and survival in patients with mrcc on sunitinib Schedule 4/2 Results of a retrospective analysis of pooled data from 770 patients AE at any time point AE by the 12-week landmark AE Endpoint HR 95% CI p value* HR 95% CI p value* Hypertension PFS OS , , 0.43 < < , 0.84 NS Hand foot syndrome PFS OS , , , 0.98 NS Asthenia/fatigue *Wald chi-square test PFS 0.49 OS 0.72 Donskov F, et al. Presented at ESMO 2012; Abstract 785O 0.38, , 0.96 < NS NS
34 Selecting first-line treatment: A clinician s perspective Efficacy is key when selecting first-line treatment, but there are also other considerations Robust evidence and guidelines Experience Patient characteristics Patient preference
35 PISCES Study Pazopanib versus sunitinib patient preference study in treatment naïve advanced or metastatic renal cell carcinoma (A randomised, double-blind, cross-over patient preference study of pazopanib versus sunitinib in treatment-naïve locally advanced or metastatic renal cell carcinoma) ONCE/PAZ/0049/12 Date of preparation:may 2012
36 Study design1 Randomisation n=169 Pazopanib 800 mg once daily, 10 weeks Sunitinib 50 mg 4/2, 10 weeks Period 1 Sunitinib 50 mg 4/2, 10 weeks Pazopanib 800 mg once daily, 10 weeks 2-week washout Period 2 Double-blind Patient choice of treatment to progression Off study :1 randomisation Time (weeks) Both drugs were over-encapsulated Patients on sunitinib received placebo during 2-week off-period 1. ClinicalTrials.gov. NCT
37 Patients (%) Primary endpoint: Patient preference for study treatments (Primary analysis population) % CI (for difference): ; p< % (n=80) 22% (n=25) 8% (n=9) Preferred pazopanib Preferred sunitinib No preference 1. Escudier B, et al. ASCO 2012 oral presentation;abstract 4502.
38 Temsirolimus: Estudio Fase III de 1º línea en MSKCC-mal pronóstico 3/6 Poor Risk Features LDH >1.5 x ULN Randomize IFN 3 MU-18 MU (n=207) CR + PR 7% CR + PR + SD 29% Med. OS 7.3 months Hgb < LLN Ca ++ (cor) >10 KPS <70% DFI <1 year TEM 25 mg QW (n=209) CR + PR 9% CR + PR + SD 46% Med. OS 10.9 months 1.0 Multiple sites of metastases Metastatic RCC (N=626) IFN 6 MU + TEM 15 mg QW (n=210) CR + PR 11% CR + PR + SD 41% Med. OS 8.4 months Survival distribution function Arm 1: IFN Arm 3: IFN + Temsirolimus Arm 2: Temsirolimus Parameter IFN Arm 1 (n=207) TEMSR Arm 2 (n=209) TEMSR + IFN Arm 3 (n=210) Median survival (mos) Comparisons Arm 2:Arm 1 Arm 3:Arm 1 Stratified log-rank p Time to death *Modified MSKCC poor risk; Stratification by country and nephrectomy status SD 16 weeks; p= Hudes G et al. N Engl J Med. 2007;356:
39 Median PFS: 1st Line Treatement in mrcc from Pivotal Studies Progression Free Survival BCS 2 3 Kane 2006 INF-α alone Multiple studies Present INF-α+ IL-2+5-FU Temsirolimus Sorafenib Bevacizumab + INF-α Gore ASCO 2008 Torisel PI Nexavar PI EscudierASCO Sunitinib Figlin ASCO Pazopanib StembergASCO Tivozanib Motzer Kane et al. Clin Cancer Res. 2006;12:7271, Gore et al. ASCO 2008, Nexavar PI, Figlin et al. ASCO 2008, Escudier ASCO Time (months)
40 Beyond the first Line: Understanding resistance mechanisms can allow identification of optimal treatment strategies Potential approaches to overcoming resistance include Adjust dose or scheduling of TKI 1,2 Switch from one TKI to another 3 Switch from a TKI to an mtor inhibitor 4 Use of novel agents Combination of traditional agents with new agents? 1 Escudier B, et al. J Clin Oncol 2009; 2 Escudier B, et al. J Clin Oncol Rini BI, et al. J Clin Oncol 2009; 4 Motzer RJ, et al. Lancet Hainsworth JD, et al. J Clin Oncol 2010; 6 Rini BI, et al ASCO GU 2010
41 AXIS1032: Axitinib pivotal trial in second-line setting First Phase III, head-to-head study vs a targeted agent in second-line mrcc Eligibility: mrcc clear-cell histology Failure of one first-line regimen containing: Sunitinib Bevacizumab + IFN-α Temsirolimus, or Cytokines Stratification by prior regimen and ECOG PS n=723 R A N D O M I S E 1:1 Axitinib 5 mg BID* Sorafenib 400 mg BID Primary endpoint: PFS ECOG PS, Eastern Cooperative Oncology Group performance status; *Starting dose 5 mg BID with option for dose titration to 10 mg BID Rini BI, et al. Lancet 2011;378:1931 9
42 PFS (probability) Axitinib* showed greater efficacy in extending mpfs vs sorafenib PFS in overall ITT population Axitinib Sorafenib mpfs, mo p< (log-rank) Stratified HR % CI 6.4, , 6.3 (95% CI, 0.56, 0.81) Time (months) 90% power to show improvement in PFS using a one-sided log-rank test at a significance of * Axitinib is indicated for advanced RCC after failure of prior treatment with sunitinib or a cytokine; ITT, intention-to-treat; mpfs, median progression-free survival Axitinib European SmPC
43 OS: Overall population 43
44 Probability (%) Probability (%) Switch from a tyrosine kinase inhibitor to an mtor inhibitor: RECORD-1 PFS* OS HR=0.33 (95% CI: ) Median PFS Everolimus: 4.90 months Placebo: 1.87 months HR=0.87 (95% CI: ) Median OS Everolimus: months Placebo: months Log-rank P value <0.001 Log-rank P value = Everolimus (n=277) Placebo (n=139) Everolimus (n=277) Placebo (n=139) Months *Central radiology review OS = overall survival; PFS = progression-free survival Months Motzer R, et al. Cancer 2010
45 Probability (%) Probability (%) RECORD-1: Phase III evidence for the sequence of sunitinib or sorafenib followed by everolimus PFS in patients with prior sunitinib treatment PFS in patients with prior sorafenib treatment HR = 0.34 (95% CI: ) Median PFS Everolimus: 3.88 months Placebo: 1.84 months Log-rank P value = <0.001 Everolimus (n=124) Placebo (n=60) HR = 0.25 (95% CI: ) Median PFS Everolimus: 5.88 months Placebo: 2.83 months Log-rank P value = <0.001 Everolimus (n=81) Placebo (n=43) Months Patients at risk Everolimus Placebo Months Motzer R, et al. Cancer 2010; Escudier B, et al. ESMO 2008

46 RECORD-1: representative of second line? In RECORD-1 almost 80% of patients were treated with everolimus third-line or later 1,2 Firstline Secondline Thirdline Fourthline mtor fifthline n=82 Firstline Secondline Thirdline mtor fourthline n=104 79% Firstline Secondline mtor thirdline n=141 Firstline mtor secondline n=89 21% 1 Zustovich F, et al. Crit Rev Oncol Hematol 2011;83: ; 2 Motzer RJ, et al. Cancer 2010;18:
47 Beyond the second Line: Understanding resistance mechanisms can allow identification of optimal treatment strategies Potential approaches to overcoming resistance include New pathways Switch from one TKI to another 3 Switch from a TKI to an mtor inhibitor 4 Combination of traditional agents with new agents?
48 Enhancing Immune Responsiveness
49 Ipilimumab Ipilimumab is a human monoclonal antibody that blocks CTLA-4 CTLA-4 is an immune check point molecule that downregulates pathways of T-cell activation T-cell activation T-cell inactivation A B C T-cell activation T cell T cell T cell CTLA4 TCR CD28 CTLA4 TCR CTLA4 MHC B7 CD28 B7 MHC Anti-CTLA4 mab APC APC APC Fong L and Small E, J Clin Oncol 2008
50 Ipilimumab in mrcc Phase II study of ipilimumab in patients with mrcc Patients received either 3 mg/kg followed by 1 mg/kg or all doses at 3 mg/kg every 3 weeks Lower dose schedule 1/21 patients had a partial response Higher dose schedule 5/40 patients had a partial response Responses observed in patients who had not responded to IL-2 therapy previously Toxicity Grade 3/4 immune-mediated toxicity observed in 33% of patients Significant association between auto-immune events and tumour regression was observed Yang J et al. J Immunother 2007
51 Enhancing Immune Responsiveness
52 Programmed Death (PD)-1 pathway PD-1 downregulates T-cell function upon binding to its ligand (PD-L1) APC/ tumour cell PD-L1 PD-1 T-cell T-cell inactivation PD-L1 has been shown to be overexpressed in RCC In patients with mrcc, overexpression of PD-L1 has been shown to be associated with Adverse pathology Aggressive tumour behaviour Poor survival Thompson RH, et al. Clin Cancer Res 2007
53 Thompson et al, Increased B7H1 Expression in RCC Diminishes Survival
 3/25/08 4/14/09 Responses may")

54 Resolving RCC Lytic Bone Metastasis in Patient Treated With Anti-PD-1 (10 mg/kg) 3/25/08 4/14/09 Responses may be correlated with PD- L1 expression 3/4 PRs in PDL-1+ tumors, 0/5 PDL-1 negative Control Ig B7H1 Brahmer et al, 2010.
55 3º Line Treatment Phase III TKI258 (dovitinib) Study Design: International, Prospective, Randomized, Openlabel, Multicenter Patients with advanced RCC, PD to prior VEGF and m- TOR targeted therapy -Primary end point: PFS -Prior Cytokines allowed R A N D O M I Z A T I O N 1:1 Dovitinib n=275 Sorafenib n=275

56 3º Line Treatment Phase III Anti-PD-1 study Study Design: International, Prospective, Randomized, Openlabel, Multicenter Patients with advanced RCC, PD to prior 2 VEGF targeted therapy -Primary end point: PFS/OS -Prior Cytokines allowed R A N D O M I Z A T I O N 1:1 Anti-PD-1 N=350 Everolimus n=350
57 Adapted from EAU guidelines 2010, ESMO Clinical Recommendations 2012, NCCN guidelines 2013 SOGUG 2010 Algoritmo CCRm 2014? Setting Patients Therapy Options First-line Favourable- or intermediate-risk Sunitinib Pazopanib Tivozanib? Beva - IFN-α HD IL-2 Cytokines Sorafenib Poor-risk Temsirolimus Sunitinib Second-line Prior cytokine Axitinib Pazopanib Sorafenib Sunitinib Prior VEGF TKI Axitinib Sorafenib? Prior VEGF TKI Everolimus Clinical trial Third-line Prior TKI TKI Everolimus Anti-PD1?? Clinical Trial Prior TKI mtor Sorafenib/Dovitinib Clinical trial
58 Future Treatment options for metastatic RCC Anti-PD1 Dovitinib Sunitinib (Adjuvant Treatment)
59 Possible areas of unmet medical need Currently approved treatments are not curative, and Patients develop progressive disease Evolving need for effective therapeutics with unique mechanisms of action for patients who progress Non clear cell histologies Few studies are available to determine efficacy Biomarkers, new pathways, gene profile, mechanisms of resistance!!! 18
60 Manejo Integral Multidisciplinar del Carcinoma Renal Avanzado Manejo Efectos Adversos Medicina Basada Evidencia (Est.Clínicos) Tipo Tratamiento: - Secuencial - Individualización Tratamiento Integral Beneficio Clínico Uso Racional de Recursos Control Complicaciones Tumorales
61 Muchas Gracias
62
Background. t 1/2 of 3.7 4.7 days allows once-daily dosing (1.5 mg) with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4
 with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4") Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Tumori rari del rene: trattamento per stadio ed istologia Dr. Camillo Porta
 Tumori rari del rene: trattamento per stadio ed istologia Dr. Camillo Porta S.C. di Oncologia Medica, Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia Non-Clear Cell Renal Cell Carcinoma (nccrcc) nccrcc
Tumori rari del rene: trattamento per stadio ed istologia Dr. Camillo Porta S.C. di Oncologia Medica, Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia Non-Clear Cell Renal Cell Carcinoma (nccrcc) nccrcc
What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center
 What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center The Case for Immunotherapy in mrcc 1. Achieves patient s goal 2.
What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center The Case for Immunotherapy in mrcc 1. Achieves patient s goal 2.
Per gentile concessione del Dr. P. Zucali
 La seconda linea di trattamento: scenario attuale e prospettive future Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano mrcc: second line SECOND-LINE SYSTEMIC THERAPY
La seconda linea di trattamento: scenario attuale e prospettive future Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano mrcc: second line SECOND-LINE SYSTEMIC THERAPY
Sorafenib. Bernard ESCUDIER Institut Gustave Roussy Villejuif, France
 Sorafenib for renal cell carcinoma Bernard ESCUDIER Institut Gustave Roussy Villejuif, France Renal Cell Carcinoma: Drugs and Targets pvhl = HIFα CCI-779 Bevacizumab VEGF KDR PDGF PDGFR TGFα EGFR Sunitinib,
Sorafenib for renal cell carcinoma Bernard ESCUDIER Institut Gustave Roussy Villejuif, France Renal Cell Carcinoma: Drugs and Targets pvhl = HIFα CCI-779 Bevacizumab VEGF KDR PDGF PDGFR TGFα EGFR Sunitinib,
PROSPETTIVE FUTURE NEL TRATTAMENTO. Cinzia Ortega Dipartimento di Oncologia Medica Fondazione del Piemonte per l Oncologia I.R.C.C.S.
 PROSPETTIVE FUTURE NEL TRATTAMENTO MEDICO DEL mrcc Cinzia Ortega Dipartimento di Oncologia Medica Fondazione del Piemonte per l Oncologia I.R.C.C.S. Candiolo Future strategies in mrcc Improve therapeutic
PROSPETTIVE FUTURE NEL TRATTAMENTO MEDICO DEL mrcc Cinzia Ortega Dipartimento di Oncologia Medica Fondazione del Piemonte per l Oncologia I.R.C.C.S. Candiolo Future strategies in mrcc Improve therapeutic
Precision oncology: identifying predictive biomarkers for the treatment of metastatic renal cell carcinoma
 Perspective Precision oncology: identifying predictive biomarkers for the treatment of metastatic renal cell carcinoma Parth K. Modi 1, Nicholas J. Farber 1, Eric A. Singer 1,2 1 Division of Urology, Rutgers
Perspective Precision oncology: identifying predictive biomarkers for the treatment of metastatic renal cell carcinoma Parth K. Modi 1, Nicholas J. Farber 1, Eric A. Singer 1,2 1 Division of Urology, Rutgers
Horizon Scanning in Oncology
 Horizon Scanning in Oncology Pazopanib (Votrient ) for the treatment of locally advanced and/or metastatic renal cell carcinoma DSD: Horizon Scanning in Oncology Nr. 013 ISSN online 2076-5940 Horizon
Horizon Scanning in Oncology Pazopanib (Votrient ) for the treatment of locally advanced and/or metastatic renal cell carcinoma DSD: Horizon Scanning in Oncology Nr. 013 ISSN online 2076-5940 Horizon
Tratamiento actual del Cáncer Renal.
 Tratamiento actual del Cáncer Renal. Daniel Castellano Servicio de Oncología Médica Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre Diagnóstico en CCR Mejor pronóstico en estadios
Tratamiento actual del Cáncer Renal. Daniel Castellano Servicio de Oncología Médica Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre Diagnóstico en CCR Mejor pronóstico en estadios
mrcc: Tratamiento HOY de segunda línea Pablo Maroto Htal Sant Pau
 mrcc: Tratamiento HOY de segunda línea Pablo Maroto Htal Sant Pau El CCRm precisa de una estrategia de tratamiento Los agentes anti-diana constituyen el tratamiento estandar del CCRm. Pero.. Cómo combinarlos?
mrcc: Tratamiento HOY de segunda línea Pablo Maroto Htal Sant Pau El CCRm precisa de una estrategia de tratamiento Los agentes anti-diana constituyen el tratamiento estandar del CCRm. Pero.. Cómo combinarlos?
Carcinoma papilar renal, cromófobo y otras histologías. Maria José Méndez Vidal Servicio de oncología Medica Hospital Reina Sofía Córdoba
 Carcinoma papilar renal, cromófobo y otras histologías. Maria José Méndez Vidal Servicio de oncología Medica Hospital Reina Sofía Córdoba Europe 121 629 new cases RCC 2012, 75 676 affected men Slide 3
Carcinoma papilar renal, cromófobo y otras histologías. Maria José Méndez Vidal Servicio de oncología Medica Hospital Reina Sofía Córdoba Europe 121 629 new cases RCC 2012, 75 676 affected men Slide 3
Maintenance therapy in in Metastatic NSCLC. Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai
 Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
54,390 estimated new cases of RCC 13,010 estimated deaths. Incidence is increasing 2.0% per year
 Advanced Renal Cell Carcinoma Individualizing Treatment Selection in the Era of Targeted Therapy Renal Cell Carcinoma In the United States in 28: 54,9 estimated new cases of RCC, estimated deaths Median
Advanced Renal Cell Carcinoma Individualizing Treatment Selection in the Era of Targeted Therapy Renal Cell Carcinoma In the United States in 28: 54,9 estimated new cases of RCC, estimated deaths Median
Targeted Molecular Therapy for Renal Cell Carcinoma: Impact on Existing Treatment Paradigms
 Targeted Molecular Therapy for Renal Cell Carcinoma: Impact on Existing Treatment Paradigms Wolfram Samlowski, MD For a CME/CEU version of this article please go to www.namcp.org/cmeonline.htm, and then
Targeted Molecular Therapy for Renal Cell Carcinoma: Impact on Existing Treatment Paradigms Wolfram Samlowski, MD For a CME/CEU version of this article please go to www.namcp.org/cmeonline.htm, and then
Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015. (minutes for web publishing)
") Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the
Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the
Anti-PD1 Agents: Immunotherapy agents in the treatment of metastatic melanoma. Claire Vines, 2016 Pharm.D. Candidate
 + Anti-PD1 Agents: Immunotherapy agents in the treatment of metastatic melanoma Claire Vines, 2016 Pharm.D. Candidate + Disclosure I have no conflicts of interest to disclose. + Objectives Summarize NCCN
+ Anti-PD1 Agents: Immunotherapy agents in the treatment of metastatic melanoma Claire Vines, 2016 Pharm.D. Candidate + Disclosure I have no conflicts of interest to disclose. + Objectives Summarize NCCN
Immunotherapy for Metastatic Renal Cell Carcinoma
 Immunotherapy for Metastatic Renal Cell Carcinoma Timothy M. Kuzel, MD Professor of Medicine and Dermatology Feinberg School of Medicine Northwestern University Chicago, Ilinois ICLIO 1 st Annual National
Immunotherapy for Metastatic Renal Cell Carcinoma Timothy M. Kuzel, MD Professor of Medicine and Dermatology Feinberg School of Medicine Northwestern University Chicago, Ilinois ICLIO 1 st Annual National
Successes and Limitations of Targeted Therapies in Renal Cell Carcinoma
 g Tumor Res. Basel, Karger, 2014, vol 41, pp 98 112 (DOI: 10.1159/000355906) Successes and Limitations of Targeted Therapies in Renal Cell Carcinoma Marc Pracht Dominik Berthold Medical Oncology Unit,
g Tumor Res. Basel, Karger, 2014, vol 41, pp 98 112 (DOI: 10.1159/000355906) Successes and Limitations of Targeted Therapies in Renal Cell Carcinoma Marc Pracht Dominik Berthold Medical Oncology Unit,
BJUI. Optimal management of metastatic renal cell carcinoma: an algorithm for treatment
 2009 The Authors; Journal compilation 2009 BJU International Mini-review Article MANAGEMENT ALGORITHMS FOR METASTATIC RCC BELLMUNT et al. BJUI BJU INTERNATIONAL Optimal management of metastatic renal cell
2009 The Authors; Journal compilation 2009 BJU International Mini-review Article MANAGEMENT ALGORITHMS FOR METASTATIC RCC BELLMUNT et al. BJUI BJU INTERNATIONAL Optimal management of metastatic renal cell
2. Background This was the fourth submission for everolimus requesting listing for clear cell renal carcinoma.
 PUBLIC SUMMARY DOCUMENT Product: Everolimus, tablets, 5 mg and 10 mg, Afinitor Sponsor: Novartis Pharmaceuticals Australia Pty Ltd Date of PBAC Consideration: November 2011 1. Purpose of Application To
PUBLIC SUMMARY DOCUMENT Product: Everolimus, tablets, 5 mg and 10 mg, Afinitor Sponsor: Novartis Pharmaceuticals Australia Pty Ltd Date of PBAC Consideration: November 2011 1. Purpose of Application To
Targeting angiogenesis in NSCLC: Clinical trial update Martin Reck Lung Clinic Grosshansdorf Grosshansdorf, Germany
 Targeting angiogenesis in NSCLC: Clinical trial update Martin Reck Lung Clinic Grosshansdorf Grosshansdorf, Germany This presentation was selected by the 15 th World Conference on Lung Cancer Program Committee
Targeting angiogenesis in NSCLC: Clinical trial update Martin Reck Lung Clinic Grosshansdorf Grosshansdorf, Germany This presentation was selected by the 15 th World Conference on Lung Cancer Program Committee
Ovarian Cancer and Modern Immunotherapy: Regulatory Strategies for Drug Development
 Ovarian Cancer and Modern Immunotherapy: Regulatory Strategies for Drug Development Sanjeeve Bala, MD, MPH Ovarian Cancer Endpoints Workshop FDA White Oak September 3, 2015 Overview Immune agents from
Ovarian Cancer and Modern Immunotherapy: Regulatory Strategies for Drug Development Sanjeeve Bala, MD, MPH Ovarian Cancer Endpoints Workshop FDA White Oak September 3, 2015 Overview Immune agents from
NEW CLINICAL RESEARCH OPTIONS IN PANCREATIC CANCER IMMUNOTHERAPY. Alan Melcher Professor of Clinical Oncology and Biotherapy Leeds
 NEW CLINICAL RESEARCH OPTIONS IN PANCREATIC CANCER IMMUNOTHERAPY Alan Melcher Professor of Clinical Oncology and Biotherapy Leeds CANCER IMMUNOTHERAPY - Breakthrough of the Year in Science magazine 2013.
NEW CLINICAL RESEARCH OPTIONS IN PANCREATIC CANCER IMMUNOTHERAPY Alan Melcher Professor of Clinical Oncology and Biotherapy Leeds CANCER IMMUNOTHERAPY - Breakthrough of the Year in Science magazine 2013.
Title: Making Optimal Therapeutic Decisions in Patients with Advanced Renal Cell Carcinoma
 Overall Aim and Objectives: Program Synopsis Title: Making Optimal Therapeutic Decisions in Patients with Advanced Renal Cell Carcinoma Clinical Synopsis: New options for targeted treatment of metastatic
Overall Aim and Objectives: Program Synopsis Title: Making Optimal Therapeutic Decisions in Patients with Advanced Renal Cell Carcinoma Clinical Synopsis: New options for targeted treatment of metastatic
Come valutare la risposta o la progressione nei pazienti in trattamento con terapie biologiche
 Come valutare la risposta o la progressione nei pazienti in trattamento con terapie biologiche Andrea Busolo U.O. di Radiologia Rocco De Vivo U.O. di Oncologia Medica ULSS 6 - Vicenza Activity and efficacy
Come valutare la risposta o la progressione nei pazienti in trattamento con terapie biologiche Andrea Busolo U.O. di Radiologia Rocco De Vivo U.O. di Oncologia Medica ULSS 6 - Vicenza Activity and efficacy
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
ONCOLOGIA: esperienze cliniche a confronto. Il carcinoma mammario metastatico
 ONCOLOGIA: esperienze cliniche a confronto. Il carcinoma mammario metastatico Sequenza ottimale del trattamento Maria Teresa Scognamiglio U.O.C. Clinica Oncologica Chieti-Ortona Chieti 12 novembre 213
ONCOLOGIA: esperienze cliniche a confronto. Il carcinoma mammario metastatico Sequenza ottimale del trattamento Maria Teresa Scognamiglio U.O.C. Clinica Oncologica Chieti-Ortona Chieti 12 novembre 213
Trials in Elderly Melanoma Patients (with a focus on immunotherapy)
") Trials in Elderly Melanoma Patients (with a focus on immunotherapy) Where we were Immunotherapy Trials: past and present Relevance for real world practice Where we are SIOG October 2012 James Larkin FRCP
Trials in Elderly Melanoma Patients (with a focus on immunotherapy) Where we were Immunotherapy Trials: past and present Relevance for real world practice Where we are SIOG October 2012 James Larkin FRCP
Stage IV Renal Cell Carcinoma. Changing Management in A Comprehensive Community Cancer Center. Susquehanna Health Cancer Center
 Stage IV Renal Cell Carcinoma Changing Management in A Comprehensive Community Cancer Center Susquehanna Health Cancer Center 2000 2009 Warren L. Robinson, MD, FACP January 27, 2014 Introduction 65,150
Stage IV Renal Cell Carcinoma Changing Management in A Comprehensive Community Cancer Center Susquehanna Health Cancer Center 2000 2009 Warren L. Robinson, MD, FACP January 27, 2014 Introduction 65,150
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GENITOURINARY RENAL CELL CARCINOMA GU Site Group Renal Cell Carcinoma Date Guideline Created: June 2012 Author: Dr. Charles Catton 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GENITOURINARY RENAL CELL CARCINOMA GU Site Group Renal Cell Carcinoma Date Guideline Created: June 2012 Author: Dr. Charles Catton 1. INTRODUCTION
National Horizon Scanning Centre. Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer. December 2007
 for advanced or metastatic non-small cell lung cancer. December 2007") Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer December 2007 This technology summary is based on information available at the time of research and a limited literature search.
Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer December 2007 This technology summary is based on information available at the time of research and a limited literature search.
The New Kid on the Block for Advanced Renal Cell Carcinoma
 The New Kid on the Block for Advanced Renal Cell Carcinoma Wyeth Pharmaceuticals recently launched Torisel (temsirolimus), a targeted, first-in-class mtor inhibitor. This new treatment for metastatic renal
The New Kid on the Block for Advanced Renal Cell Carcinoma Wyeth Pharmaceuticals recently launched Torisel (temsirolimus), a targeted, first-in-class mtor inhibitor. This new treatment for metastatic renal
Clinical Management Guideline Management of locally advanced or recurrent Renal cell carcinoma. Protocol for Planning and Treatment
 Protocol for Planning and Treatment The process to be followed in the management of: LOCALLY ADVANCED OR METASTATIC RENAL CELL CARCINOMA Patient information given at each stage following agreed information
Protocol for Planning and Treatment The process to be followed in the management of: LOCALLY ADVANCED OR METASTATIC RENAL CELL CARCINOMA Patient information given at each stage following agreed information
Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer
 LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer Everolimus plus exemestane for second-line
LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer Everolimus plus exemestane for second-line
How To Understand The Effects Of A Drug On Your Health
 Farmacologia degli inibitori TK e mtor Romano Danesi Professore ordinario di Farmacologia UOC Farmacologia Universitaria Azienda Ospedaliero-Universitaria Pisana Dipartimento di Medicina Interna Università
Farmacologia degli inibitori TK e mtor Romano Danesi Professore ordinario di Farmacologia UOC Farmacologia Universitaria Azienda Ospedaliero-Universitaria Pisana Dipartimento di Medicina Interna Università
What is the optimal sequence of anti-her2 therapy in metastatic breast cancer?
 What is the optimal sequence of anti-her2 therapy in metastatic breast cancer? David Miles Mount Vernon Cancer Centre Northwood Middlesex UKBCM mee)ng: London 2013 Herceptin plus a taxoid extends survival
What is the optimal sequence of anti-her2 therapy in metastatic breast cancer? David Miles Mount Vernon Cancer Centre Northwood Middlesex UKBCM mee)ng: London 2013 Herceptin plus a taxoid extends survival
MOLOGEN AG. Q1 Results 2015 Conference Call Dr. Matthias Schroff Chief Executive Officer. Berlin, 12 May 2015
 Q1 Results 2015 Conference Call Dr. Matthias Schroff Chief Executive Officer Berlin, 12 May 2015 V1-6 Disclaimer Certain statements in this presentation contain formulations or terms referring to the future
Q1 Results 2015 Conference Call Dr. Matthias Schroff Chief Executive Officer Berlin, 12 May 2015 V1-6 Disclaimer Certain statements in this presentation contain formulations or terms referring to the future
Guidelines for Management of Renal Cancer
 Guidelines for Management of Renal Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Versions 2 and 3 Section 5 updated bullets 5.3 and 5.4 Section 6 updated
Guidelines for Management of Renal Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Versions 2 and 3 Section 5 updated bullets 5.3 and 5.4 Section 6 updated
Drug/Drug Combination: Bevacizumab in combination with chemotherapy
 AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
Advances In Chemotherapy For Hormone Refractory Prostate Cancer. TAX 327 study results & SWOG 99-16 study results presented at ASCO 2004
 Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
BNC105 PHASE II RENAL CANCER TRIAL RESULTS
 ABN 53 075 582 740 ASX ANNOUNCEMENT 19 March 2014 BNC105 PHASE II RENAL CANCER TRIAL RESULTS Results show BNC105 utility in patients with advanced disease Identified biomarkers which correlate with patient
ABN 53 075 582 740 ASX ANNOUNCEMENT 19 March 2014 BNC105 PHASE II RENAL CANCER TRIAL RESULTS Results show BNC105 utility in patients with advanced disease Identified biomarkers which correlate with patient
Foundational Issues Related to Immunotherapy and Melanoma
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
January 2013 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Summary. Contents
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
18.5 Percent Overall Response Rate Observed in Pembrolizumab-Treated Patients with this Aggressive Form of Breast Cancer
 News Release Media Contacts: Annick Robinson Investor Contacts: Joseph Romanelli (514) 837-2550 (908) 740-1986 Stephanie Lyttle NATIONAL Public Relations (514) 843-2365 Justin Holko (908) 740-1879 Merck
News Release Media Contacts: Annick Robinson Investor Contacts: Joseph Romanelli (514) 837-2550 (908) 740-1986 Stephanie Lyttle NATIONAL Public Relations (514) 843-2365 Justin Holko (908) 740-1879 Merck
Kanıt: Klinik çalışmalarda ZYTIGA
 mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
New Treatment Options for Breast Cancer
 New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
Clinical Trial Design. Sponsored by Center for Cancer Research National Cancer Institute
 Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Preliminary Results from a Phase 2 Study of ARQ 197 in Patients with Microphthalmia Transcription Factor Family (MiT) Associated Tumors
 Associated Tumors") Preliminary Results from a Phase 2 Study of ARQ 197 in Patients with Microphthalmia Transcription Factor Family (MiT) Associated Tumors John Goldberg 1 *, George Demetri 2, Edwin Choy 3, Lee Rosen 4, Alberto
Preliminary Results from a Phase 2 Study of ARQ 197 in Patients with Microphthalmia Transcription Factor Family (MiT) Associated Tumors John Goldberg 1 *, George Demetri 2, Edwin Choy 3, Lee Rosen 4, Alberto
Clinical Spotlight in Breast Cancer
 2015 European Oncology Congress in Vienna Clinical Spotlight in Breast Cancer Reference Slide Deck Abstract #1815 Impact of Palbociclib Plus Fulvestrant on Global QOL, Functioning, and Symptoms Compared
2015 European Oncology Congress in Vienna Clinical Spotlight in Breast Cancer Reference Slide Deck Abstract #1815 Impact of Palbociclib Plus Fulvestrant on Global QOL, Functioning, and Symptoms Compared
DECISION AND SUMMARY OF RATIONALE
 DECISION AND SUMMARY OF RATIONALE Indication under consideration Clinical evidence Everolimus in combination with exemestane hormone therapy for oestrogen receptor positive locally advanced or metastatic
DECISION AND SUMMARY OF RATIONALE Indication under consideration Clinical evidence Everolimus in combination with exemestane hormone therapy for oestrogen receptor positive locally advanced or metastatic
Clinical Trials in non-clear cell RCC: ESPN, ASPEN and beyond
 Clinical Trials in non-clear cell RCC: ESPN, ASPEN and beyond Toni K. Choueiri, MD Clinical Director and Kidney Cancer Center Director The Lank Center for Genitourinary Oncology Dana-Farber Cancer Institute
Clinical Trials in non-clear cell RCC: ESPN, ASPEN and beyond Toni K. Choueiri, MD Clinical Director and Kidney Cancer Center Director The Lank Center for Genitourinary Oncology Dana-Farber Cancer Institute
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer September 3, 2015
 for Gastric Cancer September 3, 2015") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer September 3, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer September 3, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
IMMUNOMEDICS, INC. February 2016. Advanced Antibody-Based Therapeutics. Oncology Autoimmune Diseases
 IMMUNOMEDICS, INC. Advanced Antibody-Based Therapeutics Oncology Autoimmune Diseases February 2016 Forward-Looking Statements This presentation, in addition to historical information, contains certain
IMMUNOMEDICS, INC. Advanced Antibody-Based Therapeutics Oncology Autoimmune Diseases February 2016 Forward-Looking Statements This presentation, in addition to historical information, contains certain
Avastin in breast cancer: Summary of clinical data
 Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Renal Cell Carcinoma (Event Driven)
") Brochure More information from http://www.researchandmarkets.com/reports/2365661/ Renal Cell Carcinoma (Event Driven) Description: The Renal Cell Carcinoma market is highly lucrative. We anticipate that
Brochure More information from http://www.researchandmarkets.com/reports/2365661/ Renal Cell Carcinoma (Event Driven) Description: The Renal Cell Carcinoma market is highly lucrative. We anticipate that
NCCN Task Force Report: Optimizing Treatment of Advanced Renal Cell Carcinoma With Molecular Targeted Therapy
 S-1 NCCN Task Force Report: Optimizing Treatment of Advanced Renal Cell Carcinoma With Molecular Targeted Therapy Gary R. Hudes, MD; Michael A. Carducci, MD; Toni K. Choueiri, MD; Peg Esper, MSN, MSA,
S-1 NCCN Task Force Report: Optimizing Treatment of Advanced Renal Cell Carcinoma With Molecular Targeted Therapy Gary R. Hudes, MD; Michael A. Carducci, MD; Toni K. Choueiri, MD; Peg Esper, MSN, MSA,
How valuable is a cancer therapy? It depends on who you ask.
 How valuable is a cancer therapy? It depends on who you ask. Comparing and contrasting the ESMO Magnitude of Clinical Benefit Scale with the ASCO Value Framework in Cancer Ram Subramanian Kevin Schorr
How valuable is a cancer therapy? It depends on who you ask. Comparing and contrasting the ESMO Magnitude of Clinical Benefit Scale with the ASCO Value Framework in Cancer Ram Subramanian Kevin Schorr
Approccio multidisciplinare nel carcinoma della vescica. D. Amoroso Dip. di Oncologia Medica Ospedale Versilia Lido di Camaiore (LU)
") Approccio multidisciplinare nel carcinoma della vescica D. Amoroso Dip. di Oncologia Medica Ospedale Versilia Lido di Camaiore (LU) Disclosures Advisory Role, Honoraria: ü Roche ü Italfarmaco Outline v
Approccio multidisciplinare nel carcinoma della vescica D. Amoroso Dip. di Oncologia Medica Ospedale Versilia Lido di Camaiore (LU) Disclosures Advisory Role, Honoraria: ü Roche ü Italfarmaco Outline v
Attached from the following page is the press release made by BMS for your information.
 July 22, 2015 CheckMate -025 (global clinical trial), a Pivotal Phase III Opdivo (nivolumab) Renal Cancer Trial Stopped Early (PRINCETON, NJ, July 20, 2015) Bristol-Myers Squibb Company (NYSE:BMY) announced
July 22, 2015 CheckMate -025 (global clinical trial), a Pivotal Phase III Opdivo (nivolumab) Renal Cancer Trial Stopped Early (PRINCETON, NJ, July 20, 2015) Bristol-Myers Squibb Company (NYSE:BMY) announced
Avastin in Metastatic Breast Cancer
 Non-interventional study Avastin in Metastatic Breast Cancer ML 21165 / 2007 Clinical Study Report Synopsis ROCHE ML21165 / WiSP Project RH09 / V. 1.0 / 24.06.2013 ROCHE ML21165-2 - Name of Sponsor Roche
Non-interventional study Avastin in Metastatic Breast Cancer ML 21165 / 2007 Clinical Study Report Synopsis ROCHE ML21165 / WiSP Project RH09 / V. 1.0 / 24.06.2013 ROCHE ML21165-2 - Name of Sponsor Roche
Comparing Immunotherapy with High Dose IL-2 and Ipilimumab
 Comparing Immunotherapy with High Dose IL-2 and Ipilimumab Michael K Wong MD PhD FRCPC mike.wong@med.usc.edu Disclosures Speaker s Bureau, Advisory Boards, Consultant: Prometheus Bristol Myers Squibb Novartis
Comparing Immunotherapy with High Dose IL-2 and Ipilimumab Michael K Wong MD PhD FRCPC mike.wong@med.usc.edu Disclosures Speaker s Bureau, Advisory Boards, Consultant: Prometheus Bristol Myers Squibb Novartis
NOUVEAUTES THERAPEUTIQUES DANS LES TUMEURS NEUROENDOCRINES DIGESTIVES (Radiothérapie vectorisée et loco-régionale exclue) Philippe RUSZNIEWSKI
 Philippe RUSZNIEWSKI") NOUVEAUTES THERAPEUTIQUES DANS LES TUMEURS NEUROENDOCRINES DIGESTIVES (Radiothérapie vectorisée et loco-régionale exclue) Réunion APRAMEN, Paris, 2 février 2013 Philippe RUSZNIEWSKI Pôle des Maladies de
NOUVEAUTES THERAPEUTIQUES DANS LES TUMEURS NEUROENDOCRINES DIGESTIVES (Radiothérapie vectorisée et loco-régionale exclue) Réunion APRAMEN, Paris, 2 février 2013 Philippe RUSZNIEWSKI Pôle des Maladies de
Targeted Therapy What the Surgeon Needs to Know
 Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)
 in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)") Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
 Understanding Clinical Trials HR =.6 (CI :.51.7) p
Understanding Clinical Trials HR =.6 (CI :.51.7) p Prior Authorization Guideline
 Prior Authorization Guideline Guideline: PS Inj - Alimta Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antifolates Client: PS Inj Approval Date: 8/2/2004 Revision Date: 12/5/2006 I. BENEFIT
Prior Authorization Guideline Guideline: PS Inj - Alimta Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antifolates Client: PS Inj Approval Date: 8/2/2004 Revision Date: 12/5/2006 I. BENEFIT
Sur les nouveaux médicaments et les perspectives qu ils offrent (traitement à la carte et survie longue)
") Sur les nouveaux médicaments et les perspectives qu ils offrent (traitement à la carte et survie longue) Professeur Jean Trédaniel Unité de cancérologie thoracique Hôpital Saint-Louis Comparison of Four
Sur les nouveaux médicaments et les perspectives qu ils offrent (traitement à la carte et survie longue) Professeur Jean Trédaniel Unité de cancérologie thoracique Hôpital Saint-Louis Comparison of Four
Prognostic factors in patients receiving third-line targeted therapy for metastatic renal cell carcinoma.
 Prognostic factors in patients receiving third-line targeted therapy for metastatic renal cell carcinoma. Iacovelli R 1, Farcomeni A 2, Sternberg CN 3, Carteni G 4, Milella M 5, Santoni M 6, Cerbone L
Prognostic factors in patients receiving third-line targeted therapy for metastatic renal cell carcinoma. Iacovelli R 1, Farcomeni A 2, Sternberg CN 3, Carteni G 4, Milella M 5, Santoni M 6, Cerbone L
GENETIC PROFILES AND TARGETED TREATMENT OF CANCER - PERSONALIZED MEDICINE
 GENETIC PROFILES AND TARGETED TREATMENT OF CANCER - PERSONALIZED MEDICINE Branko Zakotnik MD, PhD Department of Medical Oncology Institute of Oncology Ljubljana 1 I have no conflict of interest to declare
GENETIC PROFILES AND TARGETED TREATMENT OF CANCER - PERSONALIZED MEDICINE Branko Zakotnik MD, PhD Department of Medical Oncology Institute of Oncology Ljubljana 1 I have no conflict of interest to declare
Seconda linea di trattamento
 XVIII Congresso Nazionale CIPOMO Roma, Giugno 2013 Nuovo paradigma terapeutico nel trattamento del carcinoma mammario HER2+ metastatico: dagli studi alla pratica clinica Seconda linea di trattamento Giorgio
XVIII Congresso Nazionale CIPOMO Roma, Giugno 2013 Nuovo paradigma terapeutico nel trattamento del carcinoma mammario HER2+ metastatico: dagli studi alla pratica clinica Seconda linea di trattamento Giorgio
ALCHEMIST (Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials)
") ALCHEMIST (Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials) 3 Integrated Trials Testing Targeted Therapy in Early Stage Lung Cancer Part of NCI s Precision Medicine Effort in
ALCHEMIST (Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials) 3 Integrated Trials Testing Targeted Therapy in Early Stage Lung Cancer Part of NCI s Precision Medicine Effort in
Come è cambiata la storia naturale della malattia
 Malattia Metastatica del Carcinoma del Grosso Intestino Tecniche e terapie Innovative Come è cambiata la storia naturale della malattia Antonio Frassoldati Oncologia Clinica - Ferrara 29 ottobre 2011 Colorectal
Malattia Metastatica del Carcinoma del Grosso Intestino Tecniche e terapie Innovative Come è cambiata la storia naturale della malattia Antonio Frassoldati Oncologia Clinica - Ferrara 29 ottobre 2011 Colorectal
Pharmacogenomic markers in EGFR-targeted therapy of lung cancer
 Pharmacogenomic markers in EGFR-targeted therapy of lung cancer Rafal Dziadziuszko, MD, PhD University of Colorado Cancer Center, Aurora, CO, USA Medical University of Gdansk, Poland EMEA Workshop on Biomarkers,
Pharmacogenomic markers in EGFR-targeted therapy of lung cancer Rafal Dziadziuszko, MD, PhD University of Colorado Cancer Center, Aurora, CO, USA Medical University of Gdansk, Poland EMEA Workshop on Biomarkers,
Corporate Presentation June 2, 2015
 Corporate Presentation June 2, 2015 SAFE HARBOR STATEMENT This presentation contains forward-looking statements. Although the Company believes its expectations are based on reasonable assumptions, these
Corporate Presentation June 2, 2015 SAFE HARBOR STATEMENT This presentation contains forward-looking statements. Although the Company believes its expectations are based on reasonable assumptions, these
Before, Frank's immune cells could
 Before, Frank's immune cells could barely recognize a prostate cancer cell. Now, they are focused on it. Stimulate an immune response against advanced prostate cancer Extend median survival beyond 2 years
Before, Frank's immune cells could barely recognize a prostate cancer cell. Now, they are focused on it. Stimulate an immune response against advanced prostate cancer Extend median survival beyond 2 years
DECISION AND SUMMARY OF RATIONALE
 DECISION AND SUMMARY OF RATIONALE Indication under consideration Clinical evidence Clofarabine in the treatment of relapsed acute myeloid leukaemia (AML) The application was for clofarabine to remain in
DECISION AND SUMMARY OF RATIONALE Indication under consideration Clinical evidence Clofarabine in the treatment of relapsed acute myeloid leukaemia (AML) The application was for clofarabine to remain in
Immunotherapy for High-Risk and Metastatic Melanoma
 Immunotherapy for High-Risk and Metastatic Melanoma Timothy M. Kuzel, MD Professor of Medicine and Dermatology Feinberg School of Medicine Northwestern University Chicago ICLIO 1 st Annual National Conference
Immunotherapy for High-Risk and Metastatic Melanoma Timothy M. Kuzel, MD Professor of Medicine and Dermatology Feinberg School of Medicine Northwestern University Chicago ICLIO 1 st Annual National Conference
Sequential Treatment Strategies and Combination Therapy Regimens in Metastatic Renal Cell Carcinoma
 Sequential Treatment Strategies and Combination Therapy Regimens in Metastatic Renal Cell Carcinoma Sumanta Kumar Pal, MD, and Nicholas J. Vogelzang, MD Dr. Pal is an Assistant Professor of Genitourinary
Sequential Treatment Strategies and Combination Therapy Regimens in Metastatic Renal Cell Carcinoma Sumanta Kumar Pal, MD, and Nicholas J. Vogelzang, MD Dr. Pal is an Assistant Professor of Genitourinary
OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ
 OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ Study Overview Inhibition of poly(adenosine diphosphate [ADP]-ribose) polymerase
OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ Study Overview Inhibition of poly(adenosine diphosphate [ADP]-ribose) polymerase
Avastin in breast cancer: Summary of clinical data
 Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Activity of pemetrexed in thoracic malignancies
 Activity of pemetrexed in thoracic malignancies Results of phase III clinical studies of pemetrexed in malignant pleural mesothelioma and non-small cell lung cancer show benefit P emetrexed (Alimta) is
Activity of pemetrexed in thoracic malignancies Results of phase III clinical studies of pemetrexed in malignant pleural mesothelioma and non-small cell lung cancer show benefit P emetrexed (Alimta) is
Drug treatments for kidney cancer
 James Whale Fund for Kidney Cancer Drug treatments for kidney cancer Before your doctors can discuss treatment options with you they need to know how far your cancer has progressed. Staging is used to
James Whale Fund for Kidney Cancer Drug treatments for kidney cancer Before your doctors can discuss treatment options with you they need to know how far your cancer has progressed. Staging is used to
Treatment Paradigm in NSCLC Treatment
 Treatment Paradigm in NSCLC Treatment Era of Targeted Therapy Aumkhae Sookprasert, MD Medicine Department, KKU Which factors taken to be account in NSCLC treatment? 1. Staging 2. ECOG performance status
Treatment Paradigm in NSCLC Treatment Era of Targeted Therapy Aumkhae Sookprasert, MD Medicine Department, KKU Which factors taken to be account in NSCLC treatment? 1. Staging 2. ECOG performance status
Melanoma and Immunotherapy
 Melanoma and Immunotherapy Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA The Transformed Landscape
Melanoma and Immunotherapy Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA The Transformed Landscape
Public-Private Partnerships in early phase clinical research: Spurring access to innovative therapeutics
 EPAAC WP8 Research Forum - 2 July, Sofitel Hotel Europe, Brussels Public-Private Partnerships in early phase clinical research: Spurring access to innovative therapeutics JY Blay, Past President EORTC
EPAAC WP8 Research Forum - 2 July, Sofitel Hotel Europe, Brussels Public-Private Partnerships in early phase clinical research: Spurring access to innovative therapeutics JY Blay, Past President EORTC
Qu avons-nous appris du développement des anti-her2? Ahmad Awada MD, PhD Medical Oncology Clinic Institut Jules Bordet Université Libre de Bruxelles
 Qu avons-nous appris du développement des anti-her2? Ahmad Awada MD, PhD Medical Oncology Clinic Institut Jules Bordet Université Libre de Bruxelles FOM Lille 2013 1 Her2 breast cancer expression = Poor
Qu avons-nous appris du développement des anti-her2? Ahmad Awada MD, PhD Medical Oncology Clinic Institut Jules Bordet Université Libre de Bruxelles FOM Lille 2013 1 Her2 breast cancer expression = Poor
Cancercare Connect Booklet Series. Renal Cell Cancer. www.cancercare.org
 Cancercare Connect Booklet Series Treatment Update Renal Cell Cancer www.cancercare.org Treatment Update Renal Cell Cancer Table of Contents The CancerCare Connect Booklet Series offers up-to-date, easy-to-read
Cancercare Connect Booklet Series Treatment Update Renal Cell Cancer www.cancercare.org Treatment Update Renal Cell Cancer Table of Contents The CancerCare Connect Booklet Series offers up-to-date, easy-to-read
10 th EADO Congress Vilnius, 7-10 May 2014. Ipilimumab update. Michele Maio
 10 th EADO Congress Vilnius, 7-10 May 2014 Ipilimumab update Michele Maio Medical Oncology and Immunotherapy, Department of Oncology University Hospital of Siena, Istituto Toscano Tumori SIENA, ITALY Evolving
10 th EADO Congress Vilnius, 7-10 May 2014 Ipilimumab update Michele Maio Medical Oncology and Immunotherapy, Department of Oncology University Hospital of Siena, Istituto Toscano Tumori SIENA, ITALY Evolving
Translocation Renal Cell Carcinomas
 Translocation Renal Cell Carcinomas Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Kidney cancer is not a single disease Clear cell (75%)
Translocation Renal Cell Carcinomas Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Kidney cancer is not a single disease Clear cell (75%)
Current Status of Immunotherapy For the Treatment of Metastatic Melanoma
 Current Status of Immunotherapy For the Treatment of Metastatic Melanoma The 2016 Arizona Clinical Oncology Society Meeting Richard W. Joseph, MD Assistant Professor Mayo Clinic Florida joseph.richard@mayo.edu
Current Status of Immunotherapy For the Treatment of Metastatic Melanoma The 2016 Arizona Clinical Oncology Society Meeting Richard W. Joseph, MD Assistant Professor Mayo Clinic Florida joseph.richard@mayo.edu
Treating Hepatocellular Carcinoma: Medical Oncology Options
 Treating Hepatocellular Carcinoma: Medical Oncology Options W. Thomas Purcell, MD, MBA Gastrointestinal Oncology Phase I / Developmental Therapeutics Group Executive Medical Director University of Colorado
Treating Hepatocellular Carcinoma: Medical Oncology Options W. Thomas Purcell, MD, MBA Gastrointestinal Oncology Phase I / Developmental Therapeutics Group Executive Medical Director University of Colorado
Kidney Cancer Research: Developing a New Vision for the Future
 Kidney Cancer Research: Developing a New Vision for the Future A symposium for young investigators, hosted by the Kidney Cancer Association, September 7, 2011 Introduction Since the founding of the Kidney
Kidney Cancer Research: Developing a New Vision for the Future A symposium for young investigators, hosted by the Kidney Cancer Association, September 7, 2011 Introduction Since the founding of the Kidney
MOLOGEN AG. Dr. Matthias Schroff Chief Executive Officer Dr. Alfredo Zurlo Chief Medical Officer. Roadshow Abu Dhabi, Dubai April 2015
 Dr. Matthias Schroff Chief Executive Officer Dr. Alfredo Zurlo Chief Medical Officer Roadshow Abu Dhabi, Dubai April 2015 Disclaimer Certain statements in this presentation contain formulations or terms
Dr. Matthias Schroff Chief Executive Officer Dr. Alfredo Zurlo Chief Medical Officer Roadshow Abu Dhabi, Dubai April 2015 Disclaimer Certain statements in this presentation contain formulations or terms
Cure versus control: Which is the best strategy?
 Cure versus control: Which is the best strategy? Barcelona 8-9-2012 Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY MULTIPLE MYELOMA Cure versus control
Cure versus control: Which is the best strategy? Barcelona 8-9-2012 Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY MULTIPLE MYELOMA Cure versus control
Third-line or fourth-line chemotherapy in non-small-cell lung cancer patients with relatively good performance status
 Available online at www.sciencedirect.com Journal of the Chinese Medical Association 74 (2011) 209e214 Original Article Third-line or fourth-line chemotherapy in non-small-cell lung cancer patients with
Available online at www.sciencedirect.com Journal of the Chinese Medical Association 74 (2011) 209e214 Original Article Third-line or fourth-line chemotherapy in non-small-cell lung cancer patients with
Technology Assessment Report commissioned by the NHS R&D HTA Programme on behalf of the National Institute for Health and Clinical Excellence
 Technology Assessment Report commissioned by the NHS R&D HTA Programme on behalf of the National Institute for Health and Clinical Excellence Protocol 26 October 2007 PROJECT TITLE Bevacizumab, sorafenib
Technology Assessment Report commissioned by the NHS R&D HTA Programme on behalf of the National Institute for Health and Clinical Excellence Protocol 26 October 2007 PROJECT TITLE Bevacizumab, sorafenib
Clinical development of AZD9291 in non-small cell lung cancer
 Clinical development of AZD9291 in non-small cell lung cancer Rachael Lawrance (AstraZeneca) PSI One Day Meeting: The Innovative, Challenging and Diversified World of Respiratory Disease 13 Nov 2015 Overview
Clinical development of AZD9291 in non-small cell lung cancer Rachael Lawrance (AstraZeneca) PSI One Day Meeting: The Innovative, Challenging and Diversified World of Respiratory Disease 13 Nov 2015 Overview
Nieuwe ontwikkelingen op het gebied van de angiogeneseremmers
 Nieuwe ontwikkelingen op het gebied van de angiogeneseremmers Emile Voest, MD, PhD Department of Medical Oncology University Medical Center Utrecht the Netherlands 4e Nascholing Targeted Therapy April
Nieuwe ontwikkelingen op het gebied van de angiogeneseremmers Emile Voest, MD, PhD Department of Medical Oncology University Medical Center Utrecht the Netherlands 4e Nascholing Targeted Therapy April
Management of low grade glioma s: update on recent trials
 Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,