New England Pediatric Sickle Cell Consortium
|
|
|
- Sandra Douglas
- 10 years ago
- Views:
Transcription
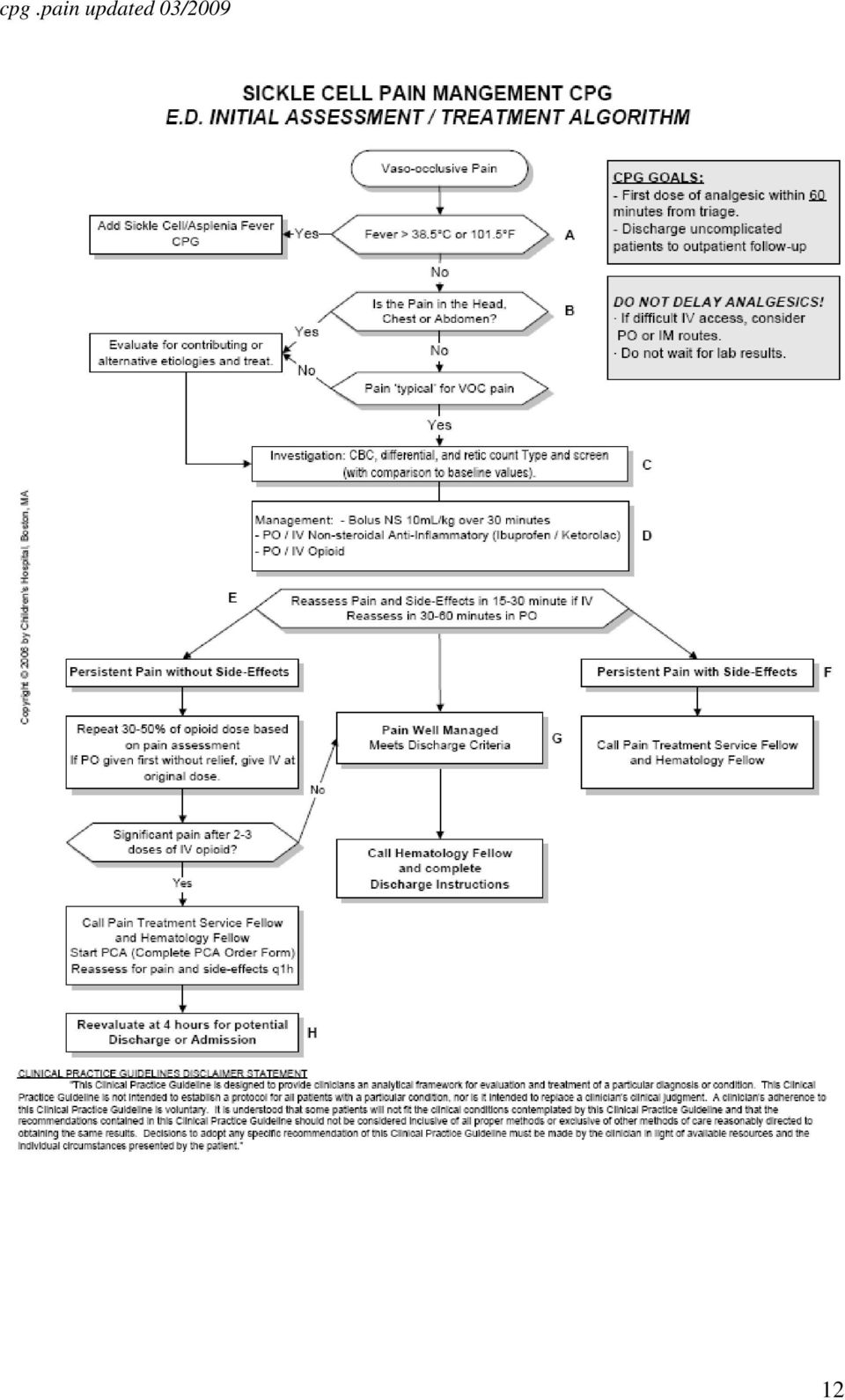
1 New England Pediatric Sickle Cell Consortium Management of Acute Pain in Pediatric Patients with Sickle Cell Disease (Vaso-Occlusive Episodes) Disclaimer Statement: Hospital clinical pathways are designed to assist clinicians by providing an analytical framework for the diagnosis and treatment of specific medical problems. They may be used for patient education and to assist in planning future care. They are not intended to replace a physician s judgment or to establish a protocol for all patients with a particular condition. The ultimate decision regarding the care of any patient should be made in respect to the individual circumstances presented by the patient. Any specific medications and dosing must always be reviewed carefully for each patient in view of any drug allergy or adverse reactions. This document was based on available research and clinical experience at time of its compilation. The following protocol is a regional guideline, and may be adopted by individual institutions as needed. 1

2 BACKGROUND Vaso-occlusive pain episodes (VOE) are the hallmark complication of sickle cell disease. They can be precipitated by exposure to cold, stress, infection, and dehydration. Maybe rebound after incomplete resolution of previous VOE episode. Most VOE symptoms can be managed at home with oral medications. More severe pain requires management in a dedicated Day Hospital, if available or Emergency Room evaluation with possible hospital admission for parenteral opioids, Goal of VOE treatment is to minimize pain and to prevent complications, (acute chest syndrome). APPROPRIATE HOME MANAGEMENT Appropriate home care of the child with sickle cell disease is crucial to optimize best health outcomes for the patient. Pain management begins with avoidance of precipitating factors, importantly, keeping the patient warm, well, hydrated and free from stress Vasoocclusive pain occurs very frequently in SCD and must be anticipated. The family of a child with SCD should have, at all times, a sickle cell care plan that details how to manage a painful crisis including which medicines and what doses to use. The patient must have an adequate supply of pain medications in the house at all times and must know how to ask for a refill before the bottle is finished. Management of an acute painful episode must include adequate oral pain medicines prior to ever giving parenteral narcotics If the child has not received adequate oral medications there must be a trial of oral medicines prior to parenteral narcotics being given. PEDIATRIC EMERGENCY DEPARTMENT (ED) EVALUATION: PATIENTS WITH SICKLE CELL DISEASE AND PAIN SHOULD BE ASSIGNED LEVEL 2 TRIAGE CRITERIA, AS DEFINED BY THE EMERGENCY SEVERITY INDEX (ESI CRITERIA). Rapid triage: immediately on presentation to ED clinic. Age appropriate pain assessment at triage and again before and after each intervention. 2
.")
3 Immediate evaluation with brief history and physical: VS, oximetry, pallor, hydration status, cardio-pulmonary status, spleen size, evidence of infection, medication history: character, nature, location, duration severity of pain. Assessment of medication allergies. Complete a brief, initial psychosocial evaluation. Give pain medication ASAP. (See pain management algorithm)) Goal is first dose of pain medication within 30 minutes of arrival to ED. Can complete H&P when patient s pain is better controlled. If patient is 6 years of age and has received opioids at home, Actiq (transmucosal Fentanyl) can be provided at a dose of 200 mcg every 30 minutes until IV is placed or other pain management is instituted. Pain medication as per chart below. Oral medications if has not previously received any. Opioid bolus and subsequent doses as recommended below. Anti-inflammatory medication when necessary/appropriate. (See Algorithm) IV fluids Consider bolus only if dehydrated 1.25 maintenance (IV + PO), to be modified based on history of fluid intolerance and signs of dehydration. If concerned for the possibility of an acute chest syndrome (ACS) developing, limit volume to 2/3-3/4 maintenance, to avoid fluid overload. Laboratory tests and possible imaging studies: Complete blood count with differential and reticulocyte count Blood culture if febrile CXR- PA and lateral for patients with chest pain, hypoxia, respiratory symptoms- but not as a routine. Additional studies based on history, PE, and clinical presentation SAO 2 and CVR monitors as necessary ACUTE PAIN MANAGEMENT IN THE ED Ensure adequate oral pain medication prior to parenteral therapy (Oral or IV therapy must be determined by pain score) Start with PO Opioids if pain not > 5/10 or equivalent, on other pain scale or faces measure See treatment algorithm below for details 3
 can be provided at a dose of 200 mcg every 30 minutes until IV is placed or other pain management is")
4 MEPERIDINE (DEMEROL) SHOULD NOT BE USED IN SICKLE CELL PATIENTS BECAUSE OF THE INCREASED RISK OF SEIZURES. Disposition Consider discharge home from ED if pain is captured with minimal number of doses ( 2) of IV opioids and then controlled with po medication. see algorithm Consider admission if patient requires multiple boluses of IV opioids without good pain control, or if patient is febrile, or if patient has respiratory symptoms. Start PCA as soon as apparent that patient will not be adequately controlled with oral or bolus pain medicines. INPATIENT MANAGEMENT Medications Continue home medications including penicillin and folic acid when applicable Continue Hydroxyurea if labs are stable (ANC>1500) Opioids Continuous opioid infusion via patient Controlled Analgesia See Pediatric PCA policy of your own institution for guidelines. PCA may not be appropriate for patients < 7 year of age. Most often these patients should be placed on basal rate only. Parent or Nurse controlled PCA should NOT be used. This can result in excessive sedation. Definitions PCA: A technique whereby the patient self- administers opioid medications using a preprogrammed infusion pump. A method of patient-controlled delivery of an opioid which maintains optimal analgesia while minimizing sedation. Bolus dose: a larger dose of opioid given as an initial dose, for persistent or increased pain, before a procedure with an increase in opioid requirement. The goal of a bolus dose is to quickly bring the patient to a therapeutic analgesic blood concentration. PCA dose: Dose of opioid administered when patient activates pump during a drug available interval. Lockout interval: Period during which PCA cannot be activated; the number minutes allowed between PCA doses. Basal dose: Low dose continuous infusion of opioid used to maintain constant background level of analgesia. One hour limit: Predetermined maximum drug amount that can be delivered during any one hour period. 4

5 SEE INSTITUTIONAL PEDIATRIC PCA POLICY FOR INDIVIDUAL DOSING. Morphine Hydromorphone (Dilaudid) Basal rate (mg/kg/hour) PCA dose (mg/kg) Lockout period (min) 6 6 Bolus dose (mg/kg) Use lower dose for opioid naïve patients and higher dose for opioid experienced patients 1 hour limit = basal rate + (PCA dose x # of PCA doses per hour) Select patients may have specific opioid dosing guidelines, refer to patient history PCA teaching sheet should be available for reference for anyone not versed in its use. Patients on PCA need frequent assessment regarding pain intensity and sedation level per individual hospital s policy. Dosing adjustment may be necessary: If patient has increased or persistent pain and is using PCA dosing > 3x/hour consider additional bolus of 0.05 mg/kg/dose morphine or mg/kg/dose hydromorphone and increase basal dose by 10-20%. Re-evaluate q 1 hour until pain is captured and then q 4-6 hours while on PCA. Every hours calculate the total amount of medication given through basal rate vs. total amount of medication given by bolus+ PCA. Adjust the basal rate appropriately so that the PCA and bolus dosing is < 1/3 the total mg received per day. If pain is well controlled and patient is pushing PCA < 3x/hour consider decreasing basal rate by 10-20%, every hours as tolerated. If patient on basal rate is over sedated decrease basal rate by 10-20% For somnolence of respiratory depression stop the infusion, stimulate patient, and apply oxygen. Consider naloxone. Switching from IV to PO analgesics Patients should be changed from IV to PO when pain is well controlled on a total IV Morphine dose (basal+pca+bolus) of approximately 0.025mg/kg/hr (Hydromorphone dose 0.003mg/kg/hr). PO regimen should include a long acting opioid (replaces basal rate) and a short acting opioid (replaces PCA) Give initial dose of oral medication, then discontinue IV medication 1 hour after. For patients who are difficult to transition to po pain medication consider starting long acting opioid, stopping basal rate of PCA, and continuing PCA dose for hours. This regimen can provide the patient with a greater sense of control. If pain is well controlled after hours, d/c PCA dose and give po short acting opioids as needed for breakthrough pain Calculations: Calculate total mg of parenteral opioid given in previous 24 hours. Use table to convert 24-hour parenteral dose to oral equivalent dose. 5

6 Divide 24-hour daily oral dose into appropriate dose per time interval. If using a long acting po opioid be sure to include a short acting opioid breakthrough pain. When switching from IV to PO opioid, dose reductions should be considered if the patient has stable controlled pain. Effective management may be achieved at 50% of the calculated equianagesic dose because there is not complete cross-tolerance among these drugs. SEE ORAL DOSING GUIDELINES FOR MORE ORAL MEDICATION OPTIONS. OPIOD PARENTERAL DOSE/24H ORAL MEDICATION ORAL EQUIVALENT /24H Morphine 20mg 60mg 30mg MS Contin ORAL DOSE INTERVAL Q12H Hydromorphone 3.0 mg 15 mg 1-2mg tablets Q 3-4 h Codeine N/A 400 mg 1-2 T#3 tablets Q 4-6 h Oxycodone N/A 30 mg 5 mg oxycodone Q -6 h Naloxone Must be readily available Dose: Age < 1year- 0.02mg/dose Age 1-12 years- 0.04mg/dose Age 12 years 0.08mg/dose Anti- inflammatory medications Ketorolac- 0.5 mg/kg dose IV max dose 30 mg/dose, 120 mg/day. Max treatment duration 72 hours. May switch to PO NSAID at that time. Ibuprofen 10mg/kg/dose PO q 6 hours. Max dose 800mg Choline magnesium trilisate 25mg/kg/dose PO q 12 hours. Max 1500mg/dose. Do not use for patients with aspirin allergy or G6PD deficiency. Celebrex is also an option if platelets are a concern (50-100mg 1-2x daily) 6

7 Side Effect Management Bowel Regimen: mandatory unless medically contraindicated. Ducosate divided into 1-4 doses/24 hours < 3 years: 10-40mg/day 3-6 years: mg/day 6-12 years: mg/day > 12 years: mg/day Add other meds as needed Senna ml/dose or 1-2 tabs PO QHS or BID. Max 2 tabs BID. Milk of Magnesia 5-15 ml/dose PO BID Lactulose 5-20g/ day divided TID-QID. Patient must be taking PO fluids Bisacodyl 5-10mg/dose PO/PR QD Miralax 0.8 g/kg/day Itching: Diphenhydramine 1mg/kg/dose IV/PO q 6 hours PRN itching Hydroxyzine 0.5-1mg/dose IV q 4-6 hours; or 2 mg/kg/day PO divided q 6-8 hours PRN itching. Max 600 mg/day Claritin/ Zyrtec: 2-5 years 5mg daily, 6 years and older 10 mg daily GI Discomfort/Nausea Ondansetron (Zofran) < 10 kg give 0.1 mg/dose PO or IV q8 hours 10 kg give 1 mg/dose PO or IV q8 hour Prochlorperazine if > 2y of age, 0.1mg/kg/dose PO/PR q 6h, max 10mg/dose Promethazine if > 2y of age, mg/kg/dose q 4-6h, max 25mg/dose Anxiolytics Can be used in conjunction with opioids, should not replace opioids. Watch for increased respiratory suppression when used in conjunction with opioids. Monitoring Baseline VS: HR, RR, BP, O2 sat (room air), pain, and sedation level. HR, RR, BP, O2 sat (room air), pain, and sedation level every 15 minutes x2 initially and with any dose change. HR, RR, pain level Q 4h RR, sedation level Q 2h Continues SaO 2 monitor Patients on PCA must be accompanied by nurse or physician during transport to clinical or non-clinical areas. Oxygen and appropriate BMV must be readily available Fluids IV + PO at maintenance. Adjust based on history of fluid intolerance and signs of dehydration. Close monitoring of fluid status including strict I s & O s and weights Consider decreasing IVF after 24 hours. Limit fluid if patient at risk for ACS. 7

8 Labs CBC with diff and retic q hours or more frequently if clinically indicated Blood cultures with CBC for T>101 F Psychiatric, Behavioral, Physical therapy interventions as indicated. Respiratory Incentive spirometry 10x/hour while awake Ambulation at least twice a shift Oxygen to keep SaO2 >95%. Nurse to inform MD immediately if patient has an increasing O2 requirement Consider BiPAP in patients with history of ACS or with chest pain OUTPATIENT MANAGEMENT Patients can be sent home on PO pain medications (NSAID and opioid) if the following criteria are met: Able to hydrate with PO fluids CBC stable (baseline) Pain has been controlled for at least 1 hour after last dose of PO opioid medication Patient and family comfortable with discharge and feel pain can be controlled with PO medications at home. Stable respiratory status Plan for pain treatment at home. Make sure medications are available at home Give meds around the clock for hours to make sure pain is captured and the give PRN Provide instructions for pain management in writing Alternate opioid and Non- opioid medications 8
 if the following criteria are met: Able to hydrate with PO fluids CBC stable (baseline) Pain has been controlled for at least 1 hour after last dose of PO opioid")
9 Oral Analgesia Dosing Guidelines Opioids Medication Dose Preparations Codeine (but beware of its pharmacogenetic profile and its lack of efficacy. Ultram: 0.5-1mg/kg/dose PO q4h Max 60 mg/dose Tylenol + Codeine Elixir (120 mg Acetaminophen +12mg codeine/5ml) Tylenol+Codeine#2(300mg acetaminophen/15mg codeine) Tylenol+Codeine#3 (300mg acetaminophen/30mg codeine) Tylenol+Codeine#4 (300mg acetaminophen/60mg codeine) Codeine Elixir 15mg/5ml Codeine 15, 30, 60mg tablets Dilaudid 1,2,3,4mg tablets Usual adult dose 2-4 mg Hydromorphone ( Dilaudid) mg/kg/dose PO q3 4h Methadone 0.2mg/kg/dose PO q4-6h Oral solution 5mg/5ml,10mg/5ml Oral concentrate 10mg/ml 5,10,40 mg Morphine (immediate release) mg/kg dose PO q3-4h Oral solution 10mg/5ml, 20mg/5ml Oral concentrate 20mg/ml 15,30 mg tablets Morphine sustained release) mg/kg/dose PO q12h MS Contin 15, 30mg tablets Oxycodone (immediate release) mg/kg/dose Oxycodone 5mg tablets Percocet/Roxicet 9325 mg acetaminophen+5mg oxycodone tablets) Roxicet Non- Opioid Medication Dose Preparation Acetaminophen 15mg/kg/dose po /PR q 4h Max 4g/day Tylenol elixir 160mg/5ml Tylenol drops 80mg/0.8ml Tylenol 325, 750, 100mg tablets Choline magnesium 25mg/kg/dose BID Max Trilisate 500, 750, 1000mg trilisate Ibuprofen 1500mg/dose 10mg/kg/dose PO q6h Max 800mg/dose tablets Children s Motrin/Advil Elixir (100mg/5ml) Motrin: 200mg tablets OTC. 400,600,800mg tablets with Rx 9
 0.2-0.")
10 REFERENCES Boston Medical Center, Pain Free Pediatric Reference Card Buchanan ID, Woodward M, Reed GW Opioid Selection during Sickle Cell Pain Crisis and its Impact on the Development of Acute Chest Syndrome Ped. Blood Ca; 45: Co JPT, Johnson KB, Duggan A, Casella J, Wilson M. Does a Clinical Pathway Improve Quality of Care for Sickle Cell Anemia? 2003 Joint Comm J Quality and Safety; 29 (4): Emergency Severity Index: Implementation Handbook, Agency for Health Care Research and Quality Version 4 Frank LS, Treadwell M, Jacob E, Vichinsky E Assessment of Sickle Cell Pain in Children and Young Adults using Adolescent Pediatric Pain Tool. J Pain and Symp. Manag.; 23 (2); NHLBI. The Management of Sickle Cell Disease. NIH guidelines, 4 th edition (NIH Publication Revised. June 2002) Pain in Sickle Cell Diseases Pain Clinical Updates from the International Association for the Study of Pain V (2), Pediatric Patient Controlled Analgesia, Boston Medical Center Medication Guidelines Preboth, M. Practice Guidelines Management of Pain in Sickle cell Disease. American Family Physician, 3: 2001 Shulman E, at al. Pathophysiology and Management of Sickle Cell Pain Crisis Lancet; 364(8987): Specific Guidelines for the Management of Pain in the Emergency Room THE GOAL OF THE CONSORTIUM MEMBERS IS TO HAVE INITIAL PAIN THERAPY PROVIDED WITHIN 30 MINUTES OF THE PATIENT S PRESENTATION TO THE EMERGENCY WITH A MAXIMUM TIME ELAPSED BETWEEN PRESENTATION AND FIRST TREATMENT OF 60 MINUTES. Please see below two different options for the initial management of pain in the Emergency Room. 10
: 181-190 Emergency Severity Index: Implementation Handbook, Agency for Health Care Research and Quality Version 4 Frank LS, Treadwell M, Jacob E,")
11 Guidelines for the Management of Uncomplicated Vaso-Occlusive Pain in Children with Sickle Cell Disease in the E.D. The purpose of these guidelines is to provide an educational resource for clinicians at BMC. Clinicians are encouraged to follow these guidelines. It is recognized however, that at times there will be exceptions to the guidelines that make different medical management appropriate. 0 minutes 30 minutes Triage Basic demographics. Vital Signs. Pain Scale. Give oral analgesia (see table). Complete initial evaluation. Place Saline Lock Obtain CBC, retic., BB hold Re-evaluate 20 minutes-30 minutes after oral dosing. Oral Analgesics If patient expresses a preference for a given analgesic, please provide that one. If not, provide from the list below: Medication Morphine Sulfate (immediate release) Oxycodone (immediate release) Hydromorphone (Dilaudid) Codeine Dose mg/kg mg/kg mg/kg mg/kg Pain significantly improved? No Yes If no other issues identified, give oxycodone +/- Long acting Morphine in ER as appropriate, ensure adequate supply pain home. Notify Pedi. Hematology & discharge. Long acting morphine: mg/kg/dose Q minutes 90 minutes Give first dose of: IV Morphine (0.1mg/kg) [Max. dose 10mg] or IV Hydromorphone (0.015mg/kg) [Max. dose 1.2mg] & re-evaluate in 30 minutes Pain significantly improved? No Give 2nd dose of: IV Morphine (0.1mg/kg) [Max. dose 10mg] or IV Hydromorphone (0.015mg/kg) [Max. dose 1.2mg] & First dose of IV Ketorolac (0.5mg/kg) [Max. dose 15mg child/30mg adolescent] & re-evaluate in 30 minutes Yes Recommended Max. Single Doses I.V. Morphine max.: 10 mg Hydromorphone: 2mg Oral Long acting Morphine: 60mg Short acting Morphine: 60mg Oxycodone: 15mg Acetaminophen: 1gm Codeine: 60mg Hydromorphone: 2mg Ibuprofen: 800mg Pain significantly improved? Yes Call Pedi. Hematology to discuss further management No Prepare for admission. If necessary, give bolus dose while PCA being prepared. 120 minutes Start PCA. See PCA Orders. 12/18/2008 / Version-1 / Dr.Sprinz 11

12 12
Clinical Algorithm & Preferred Medications to Treat Pain in Dialysis Patients
 Clinical Algorithm & Preferred Medications to Treat Pain in Dialysis Patients Developed by the Mid Atlantic Renal Coalition and the Kidney End of Life Coalition September 2009 This project was supported,
Clinical Algorithm & Preferred Medications to Treat Pain in Dialysis Patients Developed by the Mid Atlantic Renal Coalition and the Kidney End of Life Coalition September 2009 This project was supported,
WITHDRAWAL OF ANALGESIA AND SEDATION
 WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening drug doses
WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening drug doses
MUSC Opioid Analgesic Comparison Chart
 MUSC Opioid Analgesic Comparison Chart Approved by the Pharmacy and Therapeutics Committee (February 2006, November 2009, March 2010, December 2011) Prepared by the MUSC Department of Pharmacy Services
MUSC Opioid Analgesic Comparison Chart Approved by the Pharmacy and Therapeutics Committee (February 2006, November 2009, March 2010, December 2011) Prepared by the MUSC Department of Pharmacy Services
VA SAN DIEGO HEALTHCARE SYSTEM MEMORANDUM 118-28 SAN DIEGO, CA
 GUIDELINES FOR PATIENT-CONTROLLED ANALGESIA (PCA) AND PATIENT- CONTROLLED EPIDURAL ANALGESIA (PCEA) FOR ACUTE PAIN MANAGEMENT 1. PURPOSE: To assure the safe and effective use of patient controlled analgesia
GUIDELINES FOR PATIENT-CONTROLLED ANALGESIA (PCA) AND PATIENT- CONTROLLED EPIDURAL ANALGESIA (PCEA) FOR ACUTE PAIN MANAGEMENT 1. PURPOSE: To assure the safe and effective use of patient controlled analgesia
MANAGEMENT OF CHRONIC NON MALIGNANT PAIN
 MANAGEMENT OF CHRONIC NON MALIGNANT PAIN Introduction The Manitoba Prescribing Practices Program (MPPP) recognizes the important role served by physicians in relieving pain and suffering and acknowledges
MANAGEMENT OF CHRONIC NON MALIGNANT PAIN Introduction The Manitoba Prescribing Practices Program (MPPP) recognizes the important role served by physicians in relieving pain and suffering and acknowledges
OPIOID CONVERSIONS. 2. Add a rescue doses (IR) of same opioid if possible should be~10 20% of total daily opioid dose
 of same opioid if possible should be~10 20% of total daily opioid dose") OPIOID CONVERSIONS 1. Converting Short acting Long Acting (IR SR) when pain is well controlled *Use for : CHRONIC pain Pts on scheduled IR opioids pain that recurs before the next dose PP: Can use equianalgesic
OPIOID CONVERSIONS 1. Converting Short acting Long Acting (IR SR) when pain is well controlled *Use for : CHRONIC pain Pts on scheduled IR opioids pain that recurs before the next dose PP: Can use equianalgesic
Nurses Self Paced Learning Module on Pain Management
 Nurses Self Paced Learning Module on Pain Management Dominican Santa Cruz Hospital Santa Cruz, California Developed by: Strategic Planning Committee Dominican Santa Cruz Hospital 1555 Soquel Drive Santa
Nurses Self Paced Learning Module on Pain Management Dominican Santa Cruz Hospital Santa Cruz, California Developed by: Strategic Planning Committee Dominican Santa Cruz Hospital 1555 Soquel Drive Santa
Review of Pharmacological Pain Management
 Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Care Guide: Cancer Pain
 Care Guide: Cancer Pain Key Points: Cancer Pain Specific Pain Problems 1. Pain is defined as an independent and emotional experience associated with actual or potential tissue damage or described in terms
Care Guide: Cancer Pain Key Points: Cancer Pain Specific Pain Problems 1. Pain is defined as an independent and emotional experience associated with actual or potential tissue damage or described in terms
1. Which of the following would NOT be an appropriate choice for postoperative pain. C. Oral oxycodone 5 mg po every 4 to 6 hours as needed for pain
 Pain Management 1 Chapter 34. Pain Management, Self-Assessment Questions 1. Which of the following would NOT be an appropriate choice for postoperative pain management in a patient dependent on opioids?
Pain Management 1 Chapter 34. Pain Management, Self-Assessment Questions 1. Which of the following would NOT be an appropriate choice for postoperative pain management in a patient dependent on opioids?
POST-TEST Pain Resource Professional Training Program University of Wisconsin Hospital & Clinics
 POST-TEST University of Wisconsin Hospital & Clinics True/False/Don't Know - Circle the correct answer T F D 1. Changes in vital signs are reliable indicators of pain severity. T F D 2. Because of an underdeveloped
POST-TEST University of Wisconsin Hospital & Clinics True/False/Don't Know - Circle the correct answer T F D 1. Changes in vital signs are reliable indicators of pain severity. T F D 2. Because of an underdeveloped
Paramedic Pediatric Medical Math Test
 Paramedic Pediatric Medical Math Test Name: Date: Problem 1 Your 4 year old pediatric patient weighs 40 pounds. She is febrile. You need to administer acetaminophen (Tylenol) 15mg/kg. How many mg will
Paramedic Pediatric Medical Math Test Name: Date: Problem 1 Your 4 year old pediatric patient weighs 40 pounds. She is febrile. You need to administer acetaminophen (Tylenol) 15mg/kg. How many mg will
How To Treat An Alcoholic Patient
 Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 Discontinue all lorazepam
Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 Discontinue all lorazepam
Acute Pain Management in the Opioid Dependent Patient. Maripat Welz-Bosna MSN, CRNP-BC
 Acute Pain Management in the Opioid Dependent Patient Maripat Welz-Bosna MSN, CRNP-BC Relieving Pain in America (IOM) More then 116 Million Americans have pain the persists for weeks to years $560-635
Acute Pain Management in the Opioid Dependent Patient Maripat Welz-Bosna MSN, CRNP-BC Relieving Pain in America (IOM) More then 116 Million Americans have pain the persists for weeks to years $560-635
General PROVIDER INITIALS: PHYSICIAN ORDERS
 Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 General Vital Signs
Height Weight Allergies If appropriate for patient condition, please consider the following order sets: Initiate Electrolyte Replcement: Med/Surg, Med/Surg Tele Physician Order #842 General Vital Signs
Welcome to the Internal Medicine Intern Teaching Conference Series
 Welcome to the Internal Medicine Intern Teaching Conference Series Melissa (Moe) Hagman, MD, FACP University of Washington Internal Medicine & Palliative Care [email protected] pager 206-540-9725 Intern Teaching
Welcome to the Internal Medicine Intern Teaching Conference Series Melissa (Moe) Hagman, MD, FACP University of Washington Internal Medicine & Palliative Care [email protected] pager 206-540-9725 Intern Teaching
The TIRF REMS Access program is a Food and Drug Administration (FDA) required risk management program
 required risk management program") Subject: Important Drug Warning Announcement of a single shared REMS (Risk Evaluation and Mitigation Strategy) program for all Transmucosal Immediate Release Fentanyl (TIRF) products due to the potential
Subject: Important Drug Warning Announcement of a single shared REMS (Risk Evaluation and Mitigation Strategy) program for all Transmucosal Immediate Release Fentanyl (TIRF) products due to the potential
October 2012. We hope that our tool will be a useful aid in your efforts to improve pain management in your setting. Sincerely,
 October 2012 he Knowledge and Attitudes Survey Regarding Pain tool can be used to assess nurses and other professionals in your setting and as a pre and post test evaluation measure for educational programs.
October 2012 he Knowledge and Attitudes Survey Regarding Pain tool can be used to assess nurses and other professionals in your setting and as a pre and post test evaluation measure for educational programs.
INR: RUPTURED ANEURYSM: POST EMBOLIZATION Patient Identification Page 1 of 5. Allergies: Weight: kg Diagnosis:
 Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
NEONATAL ABSTINENCE SYNDROME. Osama Naga, M.D. PGY2
 NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
9/16/2010. Contact Information. Objectives. Analgesic Ketamine (Ketalar )
") Analgesic Ketamine (Ketalar )..the long and winding road to clinical practice Contact Information Lois Pizzi BSN, RN-BC Inpatient Pain Management Clinician UPMC Presbyterian Shadyside [email protected]
Analgesic Ketamine (Ketalar )..the long and winding road to clinical practice Contact Information Lois Pizzi BSN, RN-BC Inpatient Pain Management Clinician UPMC Presbyterian Shadyside [email protected]
The Pharmacological Management of Cancer Pain in Adults. Clinical Audit Tool
 The Pharmacological Management of Cancer Pain in Adults Clinical Audit Tool 2015 This clinical audit tool accompanies the Pharmacological Management of Cancer Pain in Adults NCEC National Clinical Guideline
The Pharmacological Management of Cancer Pain in Adults Clinical Audit Tool 2015 This clinical audit tool accompanies the Pharmacological Management of Cancer Pain in Adults NCEC National Clinical Guideline
4/18/14. Background. Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients. Background. Signs and Symptoms of Withdrawal
 Background 1 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Alyssa Cavanaugh, PharmD PGY1 Pharmacy Resident Children s Hospital of Michigan **The speaker has no actual or
Background 1 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Alyssa Cavanaugh, PharmD PGY1 Pharmacy Resident Children s Hospital of Michigan **The speaker has no actual or
Pain Medication Taper Regimen Time frame to taper off 30-60 days
 Pain Medication Taper Regimen Time frame to taper off 30-60 days Medication to taper Taper Regimen Comments Methadone Taper by no more than 25% Morphine Taper by no more than 25% Tramadol Taper by no more
Pain Medication Taper Regimen Time frame to taper off 30-60 days Medication to taper Taper Regimen Comments Methadone Taper by no more than 25% Morphine Taper by no more than 25% Tramadol Taper by no more
Emergency and inpatient treatment of migraine: An American Headache Society
 Emergency and inpatient treatment of migraine: An American Headache Society survey. The objective of this study was to determine the practice preferences of AHS members for acute migraine treatment in
Emergency and inpatient treatment of migraine: An American Headache Society survey. The objective of this study was to determine the practice preferences of AHS members for acute migraine treatment in
Lora McGuire MS, RN Educator and Consultant [email protected]. Barriers to effective pain relief
 Lora McGuire MS, RN Educator and Consultant [email protected] Barriers to effective pain relief Freedom from pain is a basic human right -WHO Pain is whatever the experiencing person says it is and exists
Lora McGuire MS, RN Educator and Consultant [email protected] Barriers to effective pain relief Freedom from pain is a basic human right -WHO Pain is whatever the experiencing person says it is and exists
MODERATE SEDATION RECORD (formerly termed Conscious Sedation)
") (POLICY #DOC-051) Page 1 of 6 WELLSPAN HEALTH - YORK HOSPITAL NURSING POLICY AND PROCEDURE Dates: Original Issue: September 1998 Annual Review: March 2012 Revised: March 2010 Submitted by: Brenda Artz
(POLICY #DOC-051) Page 1 of 6 WELLSPAN HEALTH - YORK HOSPITAL NURSING POLICY AND PROCEDURE Dates: Original Issue: September 1998 Annual Review: March 2012 Revised: March 2010 Submitted by: Brenda Artz
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
Cancer Pain Role Model Program Case Studies and Faculty Guides. Wisconsin Cancer Pain Initiative Madison, Wisconsin
 Cancer Pain Role Model Program Case Studies and Faculty Guides Wisconsin Cancer Pain Initiative Madison, Wisconsin Developed by: David Weissman, MD June L. Dahl, PhD WISCONSIN CANCER PAIN INITIATIVE CANCER
Cancer Pain Role Model Program Case Studies and Faculty Guides Wisconsin Cancer Pain Initiative Madison, Wisconsin Developed by: David Weissman, MD June L. Dahl, PhD WISCONSIN CANCER PAIN INITIATIVE CANCER
Opioid Conversion Ratios - Guide to Practice 2013
 Opioid s - Guide to Practice 2013 Released 1 st October 2013 2013. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that the Eastern
Opioid s - Guide to Practice 2013 Released 1 st October 2013 2013. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that the Eastern
GUIDELINE FOR ADMINISTRATION OF FENTANYL FOR PAIN RELIEF IN LABOUR
 GUIDELINE FOR ADMINISTRATION OF FENTANYL FOR PAIN RELIEF IN LABOUR INTRODUCTION Intravenous (IV) Fentanyl is a good option for pain management during labour and should be administered in a safe and competent
GUIDELINE FOR ADMINISTRATION OF FENTANYL FOR PAIN RELIEF IN LABOUR INTRODUCTION Intravenous (IV) Fentanyl is a good option for pain management during labour and should be administered in a safe and competent
The Outpatient Knee Replacement Program at Orlando Orthopaedic Center. Jeffrey P. Rosen, MD
 The Outpatient Knee Replacement Program at Orlando Orthopaedic Center Jeffrey P. Rosen, MD Anesthesia Pain Management Post-Op / Discharge Protocols The Orlando Orthopaedic Center Joint Replacement Team
The Outpatient Knee Replacement Program at Orlando Orthopaedic Center Jeffrey P. Rosen, MD Anesthesia Pain Management Post-Op / Discharge Protocols The Orlando Orthopaedic Center Joint Replacement Team
Acute & Chronic Pain Management (requiring opioid analgesics) in Patients Receiving Pharmacotherapy for Opioid Addiction
 in Patients Receiving Pharmacotherapy for Opioid Addiction") Acute & Chronic Pain Management (requiring opioid analgesics) in Patients Receiving Pharmacotherapy for Opioid Addiction June 9, 2011 Tufts Health Care Institute Program on Opioid Risk Management Daniel
Acute & Chronic Pain Management (requiring opioid analgesics) in Patients Receiving Pharmacotherapy for Opioid Addiction June 9, 2011 Tufts Health Care Institute Program on Opioid Risk Management Daniel
OPIOIDS CONVERSION GUIDELINES 2007
 Opioid analgesics vary in potency, side effect and pharmacokinetic profile. Therefore the Opioid Conversion Guidelines has been developed to assist when changing opioid drug therapy. When opioid rotating
Opioid analgesics vary in potency, side effect and pharmacokinetic profile. Therefore the Opioid Conversion Guidelines has been developed to assist when changing opioid drug therapy. When opioid rotating
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Condition/Status This powerplan is only intended for use in those patients having symptoms related to alcohol withdrawal. See DSM-IV-TR criteria listed in the Alcohol Withdrawal ICU
DRUG AND TREATMENT Condition/Status This powerplan is only intended for use in those patients having symptoms related to alcohol withdrawal. See DSM-IV-TR criteria listed in the Alcohol Withdrawal ICU
Pain Management Case Studies. Adapted from: IMPROVING END-OF-LIFE CARE A RESOURCE GUIDE FOR PHYSICIAN EDUCATION
 Pain Management Case Studies Adapted from: IMPROVING END-OF-LIFE CARE A RESOURCE GUIDE FOR PHYSICIAN EDUCATION 3rd Edition David E. Weissman, MD Director, Palliative Care Program Medical College of Wisconsin
Pain Management Case Studies Adapted from: IMPROVING END-OF-LIFE CARE A RESOURCE GUIDE FOR PHYSICIAN EDUCATION 3rd Edition David E. Weissman, MD Director, Palliative Care Program Medical College of Wisconsin
Collaborative Practice Agreement for Nurse Practitioner Management of Patients in the Specialty of Pediatric Critical Care
 Collaborative Practice Agreement for Nurse Practitioner Management of Patients in the Specialty of Pediatric Critical Care Purpose Section I Introduction/Overview This document authorizes the nurse practitioner
Collaborative Practice Agreement for Nurse Practitioner Management of Patients in the Specialty of Pediatric Critical Care Purpose Section I Introduction/Overview This document authorizes the nurse practitioner
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Abstral Prescriber and Pharmacist Guide
 Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
Abstral Prescriber and Pharmacist Guide fentanyl citrate sublingual tablets Introduction The Abstral Prescriber and Pharmacist Guide is designed to support healthcare professionals in the diagnosis of
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Union EMS Local Formulary July 18, 2014
 July 18, 2014 Forward The intent of the Union EMS Local Formulary is to provide guidance during the implementation and use of the 2012 NCCEP Protocols, Policies and Procedures to the ALS and BLS Professionals
July 18, 2014 Forward The intent of the Union EMS Local Formulary is to provide guidance during the implementation and use of the 2012 NCCEP Protocols, Policies and Procedures to the ALS and BLS Professionals
Implementing Prescribing Guidelines in the Emergency Department. April 16, 2013
 Implementing Prescribing Guidelines in the Emergency Department April 16, 2013 Housekeeping Note: Today s presentation is being recorded and will be provided within 48 hours. Two ways to ask questions
Implementing Prescribing Guidelines in the Emergency Department April 16, 2013 Housekeeping Note: Today s presentation is being recorded and will be provided within 48 hours. Two ways to ask questions
SAFE PAIN MEDICATION PRESCRIBING GUIDELINES
 Prescription drug abuse has been declared an epidemic by the Centers for Disease Control. According to 2012 San Diego Medical Examiner data, the number one cause of non-natural death is due to drug overdoses
Prescription drug abuse has been declared an epidemic by the Centers for Disease Control. According to 2012 San Diego Medical Examiner data, the number one cause of non-natural death is due to drug overdoses
Transitioning Chronic Pain Patients Out of the Hospital. Rosemary Quirk, MD, DTMH ACP, November 7, 2014
 Transitioning Chronic Pain Patients Out of the Hospital Rosemary Quirk, MD, DTMH ACP, November 7, 2014 Patients rate baseline chronic pain between 4/10-8/10 on clinic surveys This fact should fundamentally
Transitioning Chronic Pain Patients Out of the Hospital Rosemary Quirk, MD, DTMH ACP, November 7, 2014 Patients rate baseline chronic pain between 4/10-8/10 on clinic surveys This fact should fundamentally
2. The prescribing clinician will register with the designated manufacturer.
 Clozapine Management Program Description Magellan of Arizona Pharmacy Program Background: Magellan Health Services of Arizona recognizes the importance of a clozapine program. Clozapine received increased
Clozapine Management Program Description Magellan of Arizona Pharmacy Program Background: Magellan Health Services of Arizona recognizes the importance of a clozapine program. Clozapine received increased
UNIT VIII NARCOTIC ANALGESIA
 UNIT VIII NARCOTIC ANALGESIA Objective Review the definitions of Analgesic, Narcotic and Antagonistic. List characteristics of Opioid analgesics in terms of mechanism of action, indications for use and
UNIT VIII NARCOTIC ANALGESIA Objective Review the definitions of Analgesic, Narcotic and Antagonistic. List characteristics of Opioid analgesics in terms of mechanism of action, indications for use and
KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE
 KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE 201 KAR 9:260. Professional standards for prescribing and dispensing controlled substances.
KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE 201 KAR 9:260. Professional standards for prescribing and dispensing controlled substances.
Narcotic drugs used for pain treatment Version 4.3
 Narcotic drugs used for pain treatment Version 4.3 Strategy to restrict the pack sizes or the type of packaging available in public pharmacies. 1. Introduction The document describing the strategy of the
Narcotic drugs used for pain treatment Version 4.3 Strategy to restrict the pack sizes or the type of packaging available in public pharmacies. 1. Introduction The document describing the strategy of the
Pain Management after Surgery Patient Information Booklet
 Pain Management after Surgery Patient Information Booklet PATS 509-15-05 Your Health Care Be Involved Be involved in your healthcare. Speak up if you have questions or concerns about your care. Tell a
Pain Management after Surgery Patient Information Booklet PATS 509-15-05 Your Health Care Be Involved Be involved in your healthcare. Speak up if you have questions or concerns about your care. Tell a
Electronic Medication Administration Record (emar) (For Cerner Sites Only)
 (For Cerner Sites Only)") POLICY NO. 1009 Approved: 12/05 Effective: 12/05 Reviewed: 9/10; 5/12 1. Purpose: Electronic Medication Administration Record (emar) (For Cerner Sites Only) To provide direction for the transcription and
POLICY NO. 1009 Approved: 12/05 Effective: 12/05 Reviewed: 9/10; 5/12 1. Purpose: Electronic Medication Administration Record (emar) (For Cerner Sites Only) To provide direction for the transcription and
BCCA Protocol Summary for Advanced Therapy for Relapsed Testicular Germ Cell Cancer Using PACLitaxel, Ifosfamide and CISplatin (TIP)
") BCCA Protocol Summary for Advanced Therapy for Relapsed Testicular Germ Cell Cancer Using PACLitaxel, Ifosfamide and CISplatin (TIP) Protocol Code Tumour Group Contact Physician UGUTIP Genitourinary Dr.
BCCA Protocol Summary for Advanced Therapy for Relapsed Testicular Germ Cell Cancer Using PACLitaxel, Ifosfamide and CISplatin (TIP) Protocol Code Tumour Group Contact Physician UGUTIP Genitourinary Dr.
Upstate University Health System Medication Exam - Version A
 Upstate University Health System Medication Exam - Version A Name: ID Number: Date: Unit: Directions: Please read each question below. Choose the best response for each of the Multiple Choice and Medication
Upstate University Health System Medication Exam - Version A Name: ID Number: Date: Unit: Directions: Please read each question below. Choose the best response for each of the Multiple Choice and Medication
PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain
 P a g e 1 PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain Clinical Phase 4 Study Centers Study Period 25 U.S. sites identified and reviewed by the Steering Committee and Contract
P a g e 1 PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain Clinical Phase 4 Study Centers Study Period 25 U.S. sites identified and reviewed by the Steering Committee and Contract
SELECTED OPIATES TOXICITY A MODERN DAY EPIDEMIC
 SELECTED OPIATES TOXICITY A MODERN DAY EPIDEMIC Learning Objectives: 1. Identify the names and reasons/circumstances for additional toxicity of SELECTED OPIATES hydromorphone DILAUDID Methadone Fentanyl/DURAGESIC
SELECTED OPIATES TOXICITY A MODERN DAY EPIDEMIC Learning Objectives: 1. Identify the names and reasons/circumstances for additional toxicity of SELECTED OPIATES hydromorphone DILAUDID Methadone Fentanyl/DURAGESIC
Objectives. Pain Management Knowing How To Help Yourself. Patients and Family Requirements. Your Rights As A Consumer
 Objectives Pain Management Knowing How To Help Yourself Jackie Carter, RN MSN CNS Become familiar with the definitions of pain Be aware of your rights to have your pain treated Become familiar with the
Objectives Pain Management Knowing How To Help Yourself Jackie Carter, RN MSN CNS Become familiar with the definitions of pain Be aware of your rights to have your pain treated Become familiar with the
Pediatric Dosages CHAPTER 18 ALERT LEARNING OBJECTIVES
 CHAPTER 18 Pediatric Dosages LEARNING OBJECTIVES On completion of the materials provided in this chapter, you will be able to perform computations accurately by mastering the following mathematical concepts:
CHAPTER 18 Pediatric Dosages LEARNING OBJECTIVES On completion of the materials provided in this chapter, you will be able to perform computations accurately by mastering the following mathematical concepts:
Opioid Conversion Ratios - Guide to Practice 2013 Updated as Version 2 - November 2014
 Opioid s - Guide to Practice 2013 Updated as Version 2 - November 2014 2013. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that the
Opioid s - Guide to Practice 2013 Updated as Version 2 - November 2014 2013. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that the
Treatment of Opioid Dependence: A Randomized Controlled Trial. Karen L. Sees, DO, Kevin L. Delucchi, PhD, Carmen Masson, PhD, Amy
 Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Quiz 4 Arrhythmias summary statistics and question answers
 1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
Opioid Conversion Ratios - Guide to Practice 2010
 Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
PALLIATIVE CARE PAIN MANAGEMENT AND NON-PAIN SYMPTOMS ONLY
 AN EXAMINATION OF KNOWLEDGE IN: PALLIATIVE CARE PAIN MANAGEMENT AND NON-PAIN SYMPTOMS ONLY (EPERC TEST #1) 40 QUESTIONS; MULTIPLE CHOICE; SINGLE-BEST ANSWER Supplied by: End of Life Physician Education
AN EXAMINATION OF KNOWLEDGE IN: PALLIATIVE CARE PAIN MANAGEMENT AND NON-PAIN SYMPTOMS ONLY (EPERC TEST #1) 40 QUESTIONS; MULTIPLE CHOICE; SINGLE-BEST ANSWER Supplied by: End of Life Physician Education
Opioid Addiction & Methadone Maintenance Treatment. What is Methadone? What is an Opioid?
 Opioid Addiction & Methadone Maintenance Treatment Dr. Nick Wong MD, CCFP AADAC Edmonton ODP AADAC AHMB Concurrent Disorder Series September 13, 2007 1 What is Methadone? What is methadone? Synthetic opioid.
Opioid Addiction & Methadone Maintenance Treatment Dr. Nick Wong MD, CCFP AADAC Edmonton ODP AADAC AHMB Concurrent Disorder Series September 13, 2007 1 What is Methadone? What is methadone? Synthetic opioid.
Appendix 4: Guidelines for Prescribing and Administering Drugs:
 Appendix 4: Guidelines for Prescribing and Administering Drugs: A midwife may prescribe and administer the following substances in accordance with the guidelines approved by the Board. This list indicates
Appendix 4: Guidelines for Prescribing and Administering Drugs: A midwife may prescribe and administer the following substances in accordance with the guidelines approved by the Board. This list indicates
HEADACHES IN CHILDREN AND ADOLESCENTS. Brian D. Ryals, M.D.
 HEADACHES IN CHILDREN AND ADOLESCENTS Brian D. Ryals, M.D. Frequency and Type of Headaches in Schoolchildren 8993 children age 7-15 in Sweden Migraine in 4% Frequent Nonmigrainous in 7% Infrequent Nonmigrainous
HEADACHES IN CHILDREN AND ADOLESCENTS Brian D. Ryals, M.D. Frequency and Type of Headaches in Schoolchildren 8993 children age 7-15 in Sweden Migraine in 4% Frequent Nonmigrainous in 7% Infrequent Nonmigrainous
Pain Control Aims. General principles of pain control. Basic pharmacokinetics. Case history demo. Opioids renal failure John Welsh 8/4/2010
 Pain Control Aims General principles of pain control Basic pharmacokinetics Case history demo Opioids renal failure John Welsh 8/4/2010 Pain Control Morphine is gold standard treatment for moderate to
Pain Control Aims General principles of pain control Basic pharmacokinetics Case history demo Opioids renal failure John Welsh 8/4/2010 Pain Control Morphine is gold standard treatment for moderate to
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: Frenchay 0117 340 6692 Southmead 0117 323
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: Frenchay 0117 340 6692 Southmead 0117 323
CH CONSCIOUS SEDATION
 Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Dosage Calculations INTRODUCTION. L earning Objectives CHAPTER
 CHAPTER 5 Dosage Calculations L earning Objectives After completing this chapter, you should be able to: Solve one-step pharmaceutical dosage calculations. Set up a series of ratios and proportions to
CHAPTER 5 Dosage Calculations L earning Objectives After completing this chapter, you should be able to: Solve one-step pharmaceutical dosage calculations. Set up a series of ratios and proportions to
!!! BOLUS DOSE IV. Use 5-10 mcg IV boluses STD ADRENALINE INFUSION. Use IM adrenaline in advance of IV dosing!
 ADRENALINE IVI BOLUS IV Open a vial of 1:1000 ADRENALINE 1 mg /ml Add 1 ml to 9 ml N/Saline = 1mg adrenaline in 10 ml (or 100 mcg/ml) Add 1 ml 1:10,000 to 9 ml N/Saline = 100 mcg adrenaline in 10 ml (or
ADRENALINE IVI BOLUS IV Open a vial of 1:1000 ADRENALINE 1 mg /ml Add 1 ml to 9 ml N/Saline = 1mg adrenaline in 10 ml (or 100 mcg/ml) Add 1 ml 1:10,000 to 9 ml N/Saline = 100 mcg adrenaline in 10 ml (or
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Update on Buprenorphine: Induction and Ongoing Care
 Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
How To Get A Tirf
 Transmucosal Immediate Release Fentanyl (TIRF) Products Risk Evaluation and Mitigation Strategy (REMS) Education Program for Prescribers and Pharmacists Products Covered Under This Program Abstral (fentanyl)
Transmucosal Immediate Release Fentanyl (TIRF) Products Risk Evaluation and Mitigation Strategy (REMS) Education Program for Prescribers and Pharmacists Products Covered Under This Program Abstral (fentanyl)
University of Michigan Alcohol Withdrawal Guidelines Overview
 University of Michigan Alcohol Withdrawal Guidelines Overview The following document contains the University of Michigan Alcohol Withdrawal Guidelines. These guidelines were developed through an intensive
University of Michigan Alcohol Withdrawal Guidelines Overview The following document contains the University of Michigan Alcohol Withdrawal Guidelines. These guidelines were developed through an intensive
A Patient s Guide to PAIN MANAGEMENT. After Surgery
 A Patient s Guide to PAIN MANAGEMENT After Surgery C o m p a s s i o n a n d C o m m i t m e n t A Patient s Guide to Pain Management After Surgery If you re facing an upcoming surgery, it s natural to
A Patient s Guide to PAIN MANAGEMENT After Surgery C o m p a s s i o n a n d C o m m i t m e n t A Patient s Guide to Pain Management After Surgery If you re facing an upcoming surgery, it s natural to
Reducing harm from high-alert medications
 Institute for Healthcare Improvement s 5 Million Lives Campaign Best-practice protocols: Reducing harm from high-alert medications The Institute for Healthcare Improvement challenges clinicians and administrators
Institute for Healthcare Improvement s 5 Million Lives Campaign Best-practice protocols: Reducing harm from high-alert medications The Institute for Healthcare Improvement challenges clinicians and administrators
Ultram (tramadol), Ultram ER (tramadol extended-release tablets); Conzip (tramadol extended-release capsules), Ultracet (tramadol / acetaminophen)
, Ultram ER (tramadol extended-release tablets); Conzip (tramadol extended-release capsules), Ultracet (tramadol / acetaminophen)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.02.35 Subject: Tramadol Acetaminophen Page: 1 of 8 Last Review Date: September 18, 2015 Tramadol Acetaminophen
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.02.35 Subject: Tramadol Acetaminophen Page: 1 of 8 Last Review Date: September 18, 2015 Tramadol Acetaminophen
Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients
 Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Jennifer Kuhns, Pharm.D. Pharmacy Practice Resident Children s Hospital of Michigan **The speaker has no actual or potential
Evaluation of a Morphine Weaning Protocol in Pediatric Intensive Care Patients Jennifer Kuhns, Pharm.D. Pharmacy Practice Resident Children s Hospital of Michigan **The speaker has no actual or potential
Drugs & Everything Else
 Pain Relief, Common Drugs & Everything Else Henrik Jörnvall MD, PhD MKAIC November 11 2011 Lidocaine Noradrenaline Isoflurane Morphine Ropivacaine Platelets l t Pethidine Dobutamine Propofol Normal Saline
Pain Relief, Common Drugs & Everything Else Henrik Jörnvall MD, PhD MKAIC November 11 2011 Lidocaine Noradrenaline Isoflurane Morphine Ropivacaine Platelets l t Pethidine Dobutamine Propofol Normal Saline
Naloxone treatment of opioid overdose
 Naloxone treatment of opioid overdose Opioids Chemicals that act in the brain to relieve pain, often use to suppress cough, treat addiction, and provide comfort After prolonged use of opioids, increasing
Naloxone treatment of opioid overdose Opioids Chemicals that act in the brain to relieve pain, often use to suppress cough, treat addiction, and provide comfort After prolonged use of opioids, increasing
MEDICATION ABUSE IN OLDER ADULTS
 MEDICATION ABUSE IN OLDER ADULTS Clifford Milo Singer, MD Adjunct Professor, University of Maine, Orono ME Chief, Division of Geriatric Mental Health and Neuropsychiatry The Acadia Hospital and Eastern
MEDICATION ABUSE IN OLDER ADULTS Clifford Milo Singer, MD Adjunct Professor, University of Maine, Orono ME Chief, Division of Geriatric Mental Health and Neuropsychiatry The Acadia Hospital and Eastern
INPATIENT DIABETES MANAGEMENT Robert J. Rushakoff, MD Professor of Medicine Director, Inpatient Diabetes University of California, San Francisco
 INPATIENT DIABETES MANAGEMENT Robert J. Rushakoff, MD Professor of Medicine Director, Inpatient Diabetes University of California, San Francisco CLINICAL RECOGNITION Background: Appropriate inpatient glycemic
INPATIENT DIABETES MANAGEMENT Robert J. Rushakoff, MD Professor of Medicine Director, Inpatient Diabetes University of California, San Francisco CLINICAL RECOGNITION Background: Appropriate inpatient glycemic
Opioid Analgesics. Week 19
 Opioid Analgesics Week 19 Analgesic Vocabulary Analgesia Narcotic Opiate Opioid Agonist Antagonist Narcotic Analgesics Controlled substances Opioid analgesics derived from poppy Opiates include morphine,
Opioid Analgesics Week 19 Analgesic Vocabulary Analgesia Narcotic Opiate Opioid Agonist Antagonist Narcotic Analgesics Controlled substances Opioid analgesics derived from poppy Opiates include morphine,
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence
 Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Calculations Practice Problems
 Calculations Practice Problems Note: A variety of types of problems are provided for practice. Not all situations will be encountered in all states, depending on state limitations to LPN/LVN practice.
Calculations Practice Problems Note: A variety of types of problems are provided for practice. Not all situations will be encountered in all states, depending on state limitations to LPN/LVN practice.
Considerations when Using Controlled Substances to Treat Chronic Pain
 Considerations when Using Controlled Substances to Treat Chronic Pain By Mary-Beth F. Plum, Pharm.D. Impact of Chronic Pain Acute pain is the body s response to environmental dangers, and it helps protect
Considerations when Using Controlled Substances to Treat Chronic Pain By Mary-Beth F. Plum, Pharm.D. Impact of Chronic Pain Acute pain is the body s response to environmental dangers, and it helps protect
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)
 SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)") Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Instructor Guide: CPOE (Order Entry) for the Nurse. Trainer Notes. Objective Learn about PowerPlans. Benefits of CPOE. Learn about Nurse Review
 for the Nurse. Trainer Notes. Objective Learn about PowerPlans. Benefits of CPOE. Learn about Nurse Review") Instructor Guide: CPOE (Order Entry) for the Nurse Trainer Notes Section Name Duration Order Entry 45 minutes Objective Learn about PowerPlans Benefits of CPOE Learn about Nurse Review You ll Need Parking
Instructor Guide: CPOE (Order Entry) for the Nurse Trainer Notes Section Name Duration Order Entry 45 minutes Objective Learn about PowerPlans Benefits of CPOE Learn about Nurse Review You ll Need Parking
[ ] Cardiac monitoring Routine, Until discontinued, Starting today, PACU (only)
![[ ] Cardiac monitoring Routine, Until discontinued, Starting today, PACU (only)](/thumbs/26/8687689.jpg "[ ] Cardiac monitoring Routine, Until discontinued, Starting today, PACU (only)") If appropriate for patient condition, please consider the following order sets: Hydration Order for Reducing Risk of Radiocontrast Induced Nephrotoxicity #683 Over the Counter Patient Care Products #767
If appropriate for patient condition, please consider the following order sets: Hydration Order for Reducing Risk of Radiocontrast Induced Nephrotoxicity #683 Over the Counter Patient Care Products #767
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain
 Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain Division of Workers Compensation 04.01.2015 Background Opioids
Appendix to Tennessee Department of Health: Tennessee Clinical Practice Guidelines for Outpatient Management of Chronic Non- Malignant Pain Division of Workers Compensation 04.01.2015 Background Opioids
Collaborative Care Plan for PAIN
 1. Pain Assessment *Patient s own description of pain is the most reliable indicator for pain assessment. Pain intensity to be assessed using the ESAS (Edmonton Symptom Assessment Scale) Use 5 th Vital
1. Pain Assessment *Patient s own description of pain is the most reliable indicator for pain assessment. Pain intensity to be assessed using the ESAS (Edmonton Symptom Assessment Scale) Use 5 th Vital
Medical Coverage Policy Monitored Anesthesia Care (MAC)
") Medical Coverage Policy Monitored Anesthesia Care (MAC) Device/Equipment Drug Medical Surgery Test Other Effective Date: 9/1/2004 Policy Last Updated: 1/8/2013 Prospective review is recommended/required.
Medical Coverage Policy Monitored Anesthesia Care (MAC) Device/Equipment Drug Medical Surgery Test Other Effective Date: 9/1/2004 Policy Last Updated: 1/8/2013 Prospective review is recommended/required.
How To Improve Care For Bronchiolitis
 Implementation of an Evidence- Based Care Guideline for Inpatient Bronchiolitis Management J E A N E T T E J O N E S, R N + T H O M A S M A Y E S, M D, M B A * + M A R I S S A M A R T I N E Z, M D + S
Implementation of an Evidence- Based Care Guideline for Inpatient Bronchiolitis Management J E A N E T T E J O N E S, R N + T H O M A S M A Y E S, M D, M B A * + M A R I S S A M A R T I N E Z, M D + S