Carpal Tunnel Syndrome Medical Treatment Guidelines Proposed by the State of New York Department of Insurance to the Workers Compensation Board
|
|
|
- Austin Potter
- 8 years ago
- Views:
Transcription
1 Carpal Tunnel Syndrome Medical Treatment Guidelines Proposed by the State of New York Department of Insurance to the Workers Compensation Board July 2011 Draft

2 TABLE OF CONTENTS I. INTRODUCTION 1 II. HISTORY TAKING AND PHYSICAL EXAMINATION 1 III. LABORATORY TESTING 3 IV. ESTABLISHING WORK RELATEDNESS 3 V. MAKING THE DIAGNOSIS 4 VI. NON-OPERATIVE TREATMENT PROCEDURES 8 VII. SURGICAL INDICATIONS/CONSIDERATIONS 12 VIII. OPERATIVE PROCEDURES 13 IX. POST-OPERATIVE TREATMENT 13 APPENDIX A

3 CARPAL TUNNEL SYNDROME Medical Treatment Guidelines I. INTRODUCTION This document is a guideline for physicians who treat injured patients with carpal tunnel syndrome ( CTS ). Both documentation of appropriate symptoms and signs and a statement attesting to probable work-relatedness must be present for a CTS claim. II. HISTORY TAKING AND PHYSICAL EXAMINATION establish the foundation/basis for and dictate subsequent stages of diagnostic and therapeutic procedures. When findings of clinical evaluations and those of other diagnostic procedures are not complementing each other, generally the objective clinical findings should have preference. The medical records should reasonably document the following: A. History of Present Injury: i. Age, hand dominance, gender. ii. iii. iv. Onset: date of onset, triggering event (if present) versus gradual onset. Activity at/or before onset of symptoms. Nature of symptoms: pain, numbness, tingling, weakness, swelling, stiffness, temperature change, moisture change, color change. Any history of pain, intermittent or constant, and intensity. A pain scale (0 = no pain, and 10 = worst imaginable pain) may be used. The use of a patient completed pain drawing, Visual Analog Scale (VAS) is highly recommended. Use comprehensive pain diagrams to better localize pain symptoms. Evaluate the patient s overall pain behavior. The behavior should be consistent with the current pain levels reported by the patient. v. Provocative and alleviating factors (occupational and non-occupational): identify the specific physical factors that are aggravating or alleviating the problem, vi. vii. Sleep disturbances. Other associated signs and symptoms noted by the injured worker

4 viii. ix. Ability to perform work activities and activities of daily living (ADL s). Assess the overall degree of restriction or combination of restrictions. Discussion of any symptoms present in the uninjured extremity. B. Past History: i. Prior injuries to the same area including specific prior treatment and any prior supportive devices. ii. iii. iv. Past injury/symptoms involving the upper extremities, trunk and cervical spine. Past personal injury or disease that resulted in temporary or permanent job limitation. Medical conditions associated with CTS: The following are examples of medical conditions which have been commonly seen in association with CTS conditions. These require treatment and may impact the recovery of the work-related injury. A) Amyloidosis; B) Arthropathies including connective tissue disorders, rheumatoid arthritis, systemic lupus erythematosus, gout, osteoarthritis and spondyloathropathy; C) Cancer; D) Diabetes mellitus, including family history or gestational diabetes; E) Hypothyroidism, especially in older females; F) Obesity; G) Pregnancy. v. History of smoking and alcohol use; history of substance abuse; vi. vii. Medication history including, birth control pills, corticosteroid use, and other prescription and non-prescription medication, and Psychosocial history

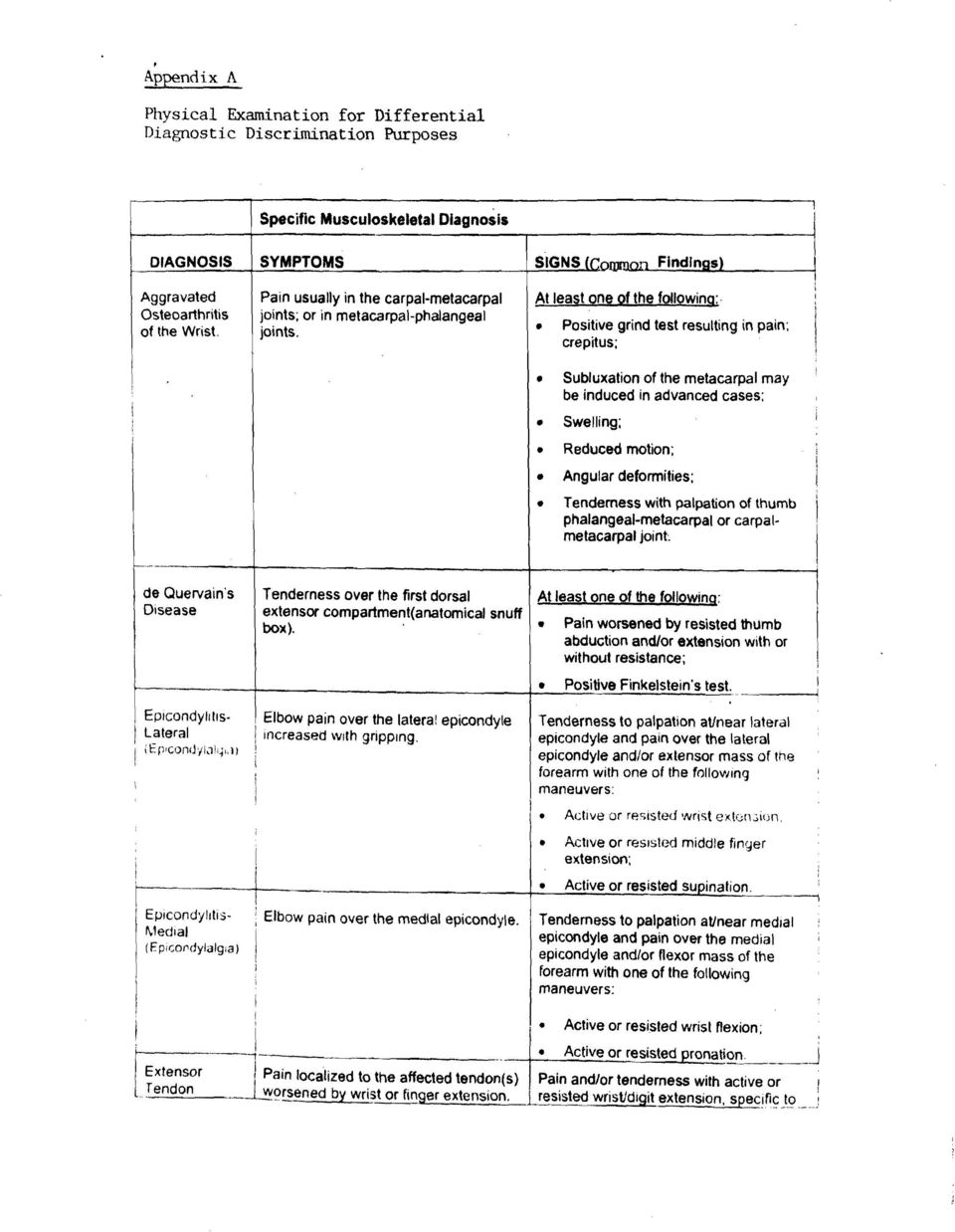
5 C. Physical Examination: The evaluation of any patient with suspected CTS should begin at the neck and upper back and then proceed down to the fingers and include the contralateral region. It should include evaluation of vascular and neurologic status, and describe any dystrophic changes or variation in skin color or turgor. A description of the patient s general posture (e.g., neck rotation, shoulder depression, spine kyphosis), and anthropometric measurements, (e.g. body mass index [BMI]) may prove useful. Behavioral adaptations to symptoms should be documented. Additional physical exam components may be necessary based on past medical history. A neurological examination typically includes bilateral assessments of light touch sensation, pinprick, 2 point sensation as applicable, motor strength and reflexes. Similar assessments of the upper extremities including a vascular assessment may be performed. Special care to evaluate for polyneuropathic processes such as diabetic neuropathy is recommended. Vibratory sense and Achilles reflexes are frequently lost in diabetic neuropathy. For purposes of differential diagnostic discrimination, Appendix A provides a list of other common upper extremity conditions including pertinent signs and symptoms. III. LABORATORY TESTING Laboratory tests are generally accepted, well-established and widely used procedures. Patients should be carefully screened at the initial exam for signs or symptoms of diabetes, hypothyroidism, pregnancy, arthritis, and related inflammatory diseases. Laboratory tests are rarely indicated at the time of initial evaluation unless there is reasonable clinical suspicion of a specific condition listed above. IV. ESTABLISHING WORK RELATEDNESS CTS may result from numerous conditions, including inflammatory or non-inflammatory arthropathies, recent or remote wrist trauma or fractures, diabetes mellitus, obesity, hypothyroidism, pregnancy, and genetic factors. 1 2 In the unusual instance that CTS is acutely, traumatically induced, e.g. a patient has both CTS and concomitant trauma (fracture or dislocation), the treatment may require prompt carpal tunnel release. Work related activities may also cause or contribute to the development of CTS. To establish a diagnosis of work-related carpal tunnel syndrome, all of the following are required: 1 Stevens J, Beard CM, O Failon WM, Kurland LT. Conditions associated with carpal tunnel syndrome. Mayo Clin Proc 1992; 67: Hakim AJ, Cherkas L, El Zayat S, MacGregor AJ, Spector TD. The genetic contribution to carpal tunnel syndrome in women: a twin study. Arthritis and Rheumatism 2002; 47:
![g. body mass index [BMI]) may prove useful. Behavioral adaptations to symptoms should be documented. Additional physical exam components may be necessary based on past medical history.](/docs-images/45/5512336/images/page_5.jpg "A neurological examination typically includes bilateral assessments of light touch sensation, pinprick, 2 point sensation as applicable, motor strength and reflexes.")
6 1. Exposure: Workplace activities that contribute to or cause CTS, and 2. Outcome: A diagnosis of CTS that meets the diagnostic criteria under Section V, and 3. Relationship to work: This includes a statement of the probability that the illness or injury is work-related. The presence of concurrent disease does not eliminate the possibility of work-relatedness of any specific case. Work related CTS is most often associated with activities requiring extensive, forceful, repeated or prolonged use of the hands and wrists, particularly if these potential risk factors are present in combination (e.g., force and repetition or force and posture). Usually, one or more of the following work conditions occurs on a regular basis to support work relatedness: 1. Forceful use, particularly if repeated 2. Repetitive hand use combined with some element of force, especially for prolonged periods 3. Constant firm gripping of objects 4. Moving or using the hand and wrist against resistance or with force 5. Exposing the hand and wrist to strong regular vibrations 6. Regular or intermittent pressure on the wrist V. MAKING THE DIAGNOSIS A. Signs and Symptoms A diagnosis of CTS requires symptoms suggestive of median nerve entrapment at the wrist supported by physical examination findings. Prior to surgery, confirmation of the diagnosis by electrodiagnostic studies (EDS) is required. Typical symptoms of CTS may include numbness, tingling, or pain in the volar aspects of one or both hands, especially noted after work or at night. Nocturnal symptoms are prominent in a majority of patients. Patients frequently awaken at night or early morning and shake their hands to relieve these symptoms. The location of these symptoms may be reported as involving the entire hand or localized to the palmar surfaces of the thumb and first two or three fingers. A hand pain diagram may be useful in localizing sensory symptoms of CTS. B. Specific Physical Exam Findings: No single physical finding is diagnostic of CTS. Multiple tests should be recorded with the patient s exact response. Final diagnosis is dependent on a correlation of symptoms, physical exam findings and EDS testing, where appropriate, as any of these alone can be false positive or false negative. i. The clinical diagnosis should be suspected whenever there are: 1) patient s history of paresthesia in one or more of the following - 4 -

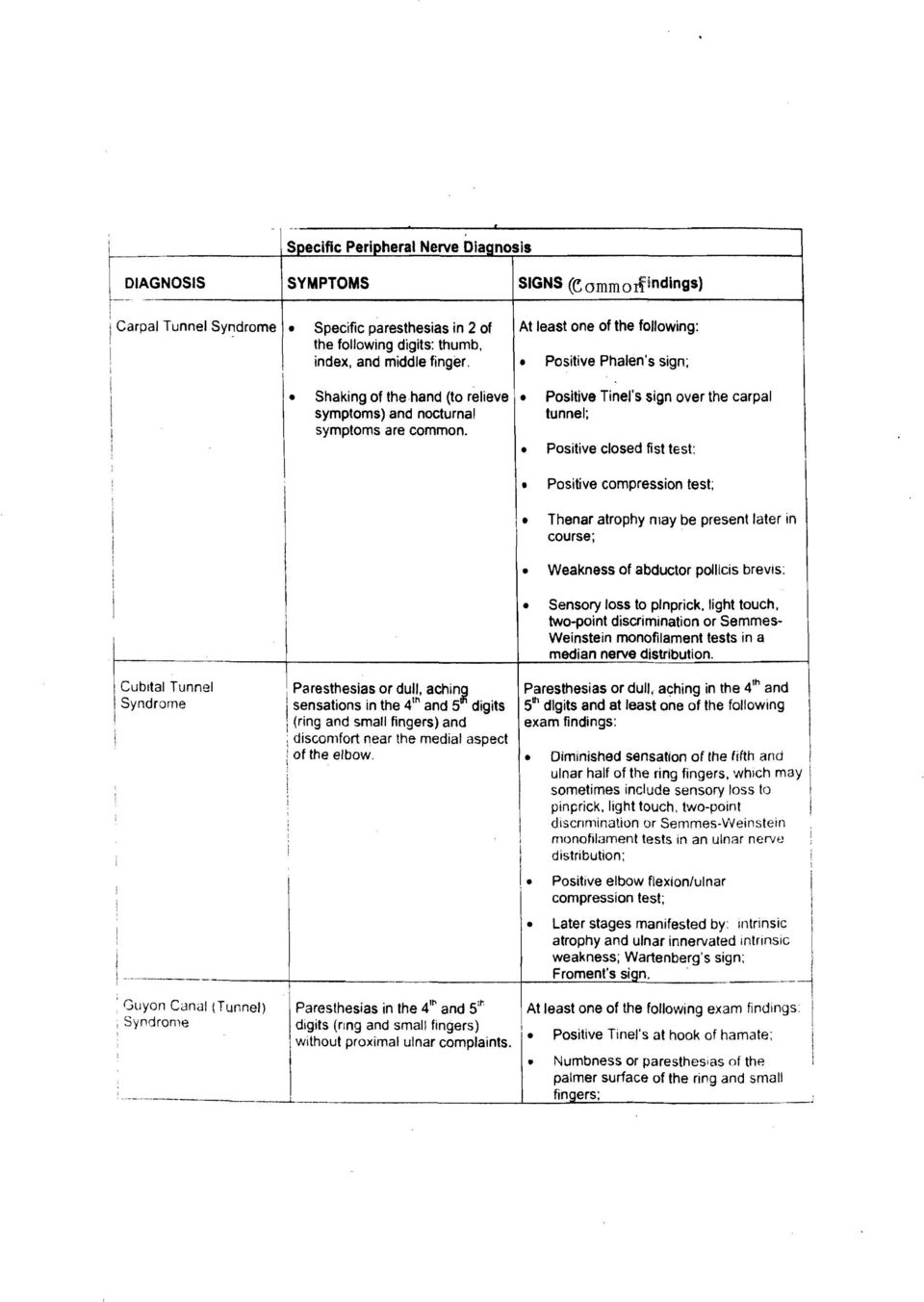
7 digits: thumb, index and middle finger; and 2) at least one of the physical exam signs listed below. Provocative tests must recreate symptoms in the median nerve distribution. Phalen s sign/reverse Phalen s sign. Tinel s sign over the carpal tunnel. Weakness of the abductor pollicis brevis. (see discussion EDS studies) Thenar atrophy may be present, usually late in the course. (see discussion of EDS studies) Sensory loss to pinprick, light touch, two-point discrimination or Semmes Weinstein monofilament test in a median nerve distribution. ii. iii. iv. Evaluation of the contralateral wrist should be performed. Evaluation of the proximal upper extremity and cervical spine for other conditions cervical radiculopathy, thoracic outlet syndrome, other peripheral neuropathies, and other musculoskeletal conditions. Myofascial findings requiring treatment may present in additional soft tissue areas these should be identified and treated in accordance with medical treatment guidelines. C. Diagnostic Testing Procedures: i. Electrodiagnostic (EDS) Testing: are well-established and widely accepted for evaluation of patients suspected of having CTS. The results are sensitive and specific for the diagnosis when clinical symptoms are present. Studies may confirm the diagnosis or direct the examiner to alternative conditions. In those cases where EDS studies are indicated, they should be conducted in accordance with the CTS practice parameters of the American Association of Neuruometer and Electrodiagnostic Medicine. The EDS study is to include median, motor and median sensory conductions (NCV). If abnormal, than comparison to ipsalateral ulnar motor/sensory and contralateral median motor/sensory should be made. Needle electromyography (EMG) of a sample of muscles innervated by the C5 to T1 spinal roots, including paraspinal muscles and a thenar muscle innervated by the median nerve of the symptomatic limb, is required. EDS findings in CTS reflect slowing of median - 5 -
 Sensory loss to pinprick, light touch, two-point discrimination or Semmes Weinstein monofilament test in a median nerve distribution. ii. iii. iv.")
8 motor and sensory conduction across the carpal tunnel region due to demyelination or axonapathy (axonal loss). Axonal loss, when present, is demonstrated by EMG in median nerve supplied thenar muscles. A) To assure accurate testing, hand temperature should be maintained at 30 to 34C preferably recorded from the hand/digits. For temperature below 30C, the hand should be warmed. B) Positive Findings Any of these nerve conduction study findings must be accompanied by median nerve symptoms to establish the diagnosis. 1) Slowing of median distal sensory and/or motor conduction through the carpal tunnel region. 2) Electromyographic changes in the median thenar muscles in the absence of proximal abnormalities. 3) Suggested guidelines for the upper limits of normal latencies: a) Median distal motor latency (DML) at onset - 4.5msec/8cm b) Median distal sensory peak latency (DSL) 3.6msec/14cm c) Median intrapalmar peak latency (palm/wrist) 2.2msec/8cm d) Median-ulnar palmar sensory latency difference greater than 0.3msec. 4) Because laboratories establish their own norms, a degree of variability from the suggested guideline values [as described in 3 above] is acceptable. C) In all cases, normative values are to be provided with the neuron diagnostic evaluation. When there is clinical suspicion of polyneuropathy supported by history or physical examination, it may be worthwhile to perform electrodiagnostic testing in the lower extremities; however, lower extremity studies are not otherwise indicated in the routine - 6 -
 Positive Findings Any of these nerve conduction study findings must be accompanied by median nerve symptoms to establish the diagnosis.")
9 evaluation of suspected CTS. Studies require clinical correlation due to the occurrence of false positive and false negative results. Symptoms of CTS may occur with normal EDS studies, especially early in the clinical course. When expedited surgical intervention is contemplated because of the presence of the following findings: 1) thenar atrophy 2) motor weakness in the muscles supplied by the median nerve an EDS (NCV and EMG) study should be scheduled. For patients who decline surgery, it may be of value in the course of treatment to obtain EDS studies to establish the diagnosis. D) The following EDS studies are not recommended: 1) multiple median F wave parameters 2) median motor nerve residual latency E) The following EDS studies are not recommended and not acceptable to confirm a clinical diagnosis of CTS: 1) hand held conduction devices such as electroneurometer 2) portable automatic electrodiagnostic devices 3) sympathetic skin response 4) current perception threshold measurements 5) quantitative sensory testing F) Frequency of Studies/Maximum Number of Studies: 1) Indications for Initial Testing: a) Patients with clinically significant CTS who do not improve symptomatically or functionally with conservative measures for CTS over a 3 to 4 week period
 study should be scheduled. For patients who decline surgery, it may be of value in the course of treatment to obtain EDS studies to establish the diagnosis.")
10 b) Patients in whom the diagnosis is in question and who are symptomatic for at least 3 weeks. c) To rule out other nerve entrapments, or alternative radiculopathy. d) Patients for whom surgery is contemplated in accordance with Section VII 2) A repeat study may be performed: a) At 3 months or longer when the initial studies were normal and CTS is still suspected. b) At 8 to 12 weeks for inadequate clinical improvement with non-surgical treatment. c) Post-operative 3 to 6 months for persistent or recurrent symptoms following carpal tunnel release, unless an earlier evaluation is required by the surgeon. ii. Other Tests: Imaging, MRI, and sonography are not recommended at this time unless a space occupying lesion is suspected. VI. NON-OPERATIVE TREATMENT PROCEDURES A. Initial Treatment: Medications such as analgesics and over the counter medications for symptomatic relief; wrist splint at night, and restriction of activities such as forceful gripping, awkward wrist posture, and repetitive wrist motion. B. Patient education should include instruction in self-management techniques including sleeping postures which avoid excessive wrist flexion; ergonomics; and a home therapy program to provide symptomatic relief that includes heat treatment, stretching exercises and nerve gliding. C. All patients should be encouraged to return to work as soon as possible. This process may be best facilitated with modified duty particularly when the job demands exceed the patient s capabilities due to the workplace injury. Recommendations for ergonomic assessments to evaluate or reduce exposure may be of value for treatment and future intervention/prevention
 Post-operative 3 to 6 months for persistent or recurrent symptoms following carpal tunnel release, unless an earlier evaluation is required by the surgeon. ii.")
11 D. Medications and Medical Treatment: Use of medications in the treatment of CTS is appropriate for controlling acute and chronic pain and inflammation. All drugs should be used according to patients needs. A thorough medication history, including use of alternative and over the counter medications, should be performed at the time of the initial visit and updated periodically. Use of non-steroidal anti-inflammatory medications (NSAIDs), oral steroids, and diuretics, have not been shown to have significant long-term beneficial effect in treating CTS. Although NSAIDs are not curative, they and other analgesics may provide symptomatic relief. Vitamin B6: Randomized trials have demonstrated conflicting results. Higher doses may result in development of a toxic peripheral neuropathy. In the absence of definitive literature showing a beneficial effect, use of Vitamin B6 cannot be recommended unless there is a documented medical condition that results in the interference of the effects of Vitamin B6 or a significant nutritional problem. Oral Steroids: have been shown to have short-term symptomatic benefit but no long-term functional benefit. There is good evidence that local steroid injection is superior to oral steroids at 3 months. Given this and the problematic systemic effects of oral steroids, they are not recommended. It may occasionally be appropriate to use them for patients with severe CTS symptoms who refuse injections and who have no risk factors for adverse effects. E. Orthotics/Immobilization with Splinting: There is some evidence that splinting leads to more improvement in symptoms and hand function than watchful waiting alone. Because of limited patient compliance with day and night splinting in published studies, evidence of effectiveness is limited to nocturnal splinting. Splints should be loose and soft enough to maintain comfort while supporting the wrist in a relatively neutral position. This can be accomplished using a soft or rigid split with a metal or plastic support. Some splints include immobilization of the metacarpal-phalangeal joints. Splint comfort is critical and may affect compliance. Off-the-shelf splints are usually sufficient, although custom thermoplastic splints may provide a better fit for certain patients. Splints may be effective when worn during sleep hours or during portions of the day, depending on activities. Most studies show that full time night splinting for a total of 4 to 6 weeks is the most effective protocol. Depending on job activities, intermittent daytime splinting can also be helpful. Splint use is rarely mandatory. Providers should be aware that over-usage is counterproductive, and should counsel patients to avoid over-usage
, oral steroids, and diuretics, have not been shown to have significant long-term beneficial effect in treating CTS.")
12 Splinting is generally effective for milder cases of CTS. Long-term benefit beyond 3 months has not been established. An effect should be seen in 1 to 4 weeks. It is more likely to have some long-term benefit in patients who have less severe paresthesias during sleep hours (less than 6/10) and who have had symptoms for less than 1 year. Time to Produce Effect: 1 to 4 weeks. If after 4 weeks, the patient has partial improvement, continue to follow since neuropathy may worsen, even in the face of diminished symptoms. Frequency: During sleep hours. Daytime intermittent, depending on symptoms and activities. Optimum Duration: 4 to 8 weeks. Maximum Duration: 2 to 4 months. If symptoms persist, consideration should be given to either repeating electrodiagnostic studies or to more aggressive treatment. F. Steroid injections: may decrease inflammation and allow the therapist to progress with rehabilitation therapy. Steroid injections under significant pressure should be avoided as the needle may be penetrating the tendon and injection into the tendon can cause possible tendon breakdown, tendon degeneration, or rupture. Injections should be used with caution for patients under 30 years of age. After steroid injections, some patients can have improved symptoms for one year. Lower doses of steroids appear to be as effective as higher doses. There is good evidence that injections have better results at 3 months than oral steroids. If following the first injection, symptomatic relief is followed by recurrent symptoms, the decision to perform a second injection must be weighed against alternative treatments such as surgery. Surgery may give more definitive relief of symptoms. Time to Produce Effect: 1 to 2 injections. If the first injection is unsuccessful and symptoms continue, the second injection should be performed by a specialist with expertise in the anatomy of the upper extremity. Maximum Frequency: 3 injections in one year. Steroid injections should be used cautiously in diabetic patients. Diabetic patients should be reminded to check their blood glucose levels at least daily for 2 weeks after injections

13 G. Nerve Gliding: exercises consist of ROM of the upper extremity and neck that produce tension and longitudinal movement along the length of the median and other nerves of the upper extremity. These exercises are based on the principle that the tissues of the peripheral nervous system are designed for movement, and that tension and glide (excursion) of nerves may have an effect on neurophysiology through alterations in vascular and axoplasmic flow. The exercises are simple to perform and can be done by the patient after brief instruction. Biomechanical principles have been more thoroughly studied than clinical outcomes. Large, well-designed randomized trials have been lacking. There is some evidence from a systematic review that nerve gliding is more effective than no treatment. Time to Produce Effect: 2 to 4 weeks. Frequency: Up to 5 times per day by patient (patient-initiated). Optimum Duration: 2 provider-directed sessions. Maximum Duration: 3 provider-directed sessions. H. Manual Therapy Techniques: There is no evidence supporting manipulation of the spine for treatment of CTS. There is no clear evidence supporting carpal bone mobilization or manual therapy. However, other myofascial components that may occur with CTS may be treated with manual therapy. I. Ultrasound: There is some evidence that ultrasound may be effective in symptom relief and in improving nerve conduction in mild-to-moderate cases of CTS. No studies have demonstrated long-term functional benefit. This treatment may be used in conjunction with an active therapy program for nonsurgical patients who do not improve with splinting and activity modification. It is not known if there are any long-term deleterious neurological effects from ultrasound. It is suggested that treatment by limited to 12 sessions over 6 weeks. J. Low Level Laser: There is no evidence that low level laser therapy alone is beneficial in changing the outcome for patients with CTS and therefore it is not recommended. K. There is no evidence for the use of iontophoresis, magnets or laser acupuncture. Therefore these interventions are not recommended

14 VII. SURGICAL INDICATIONS/CONSIDERATIONS Since cumulative trauma conditions often involve several areas in an upper extremity, surgical treatment of one problem should be performed in conjunction with conservative treatment of other problems in the upper extremity. Overall it is probably reasonable to expect that 40 to 50% of patients with mild exam findings may improve or remain stable over time without surgery. There is strong evidence that surgery is more effective than splinting or injections in producing long-term symptom relief and normalization of median nerve conduction velocity for those patients with clinically significant CTS with positive NCV findings. There is also a positive cost utility for surgery over conservative care for patients with positive nerve conduction studies. There is good evidence that surgery improves symptoms more effectively than steroid injection for up to five months. In one prospective study, duration of symptoms prior to surgery, up to 5 years, did not affect the ability to achieve symptom or functional outcome success with surgery. Patients with more severe symptoms and longer duration of symptoms showed significant improvement with surgery. Patients with thenar atrophy, weakness of the abductor pollicis brevis, and fixed sensory deficits may still improve with surgery. Patients with mild symptoms and functional deficits demonstrated the smallest changes from pre- to post-operative scores. However, their post-operative scores were higher than the postoperative scores of those with more severe symptoms. A. Surgery should be considered as an initial therapy in situations where clinical evidence of CTS is present based on the criteria below. i. Median nerve trauma has occurred; acute carpal tunnel syndrome, or ii Thenar atrophy is present and due to median nerve compression; or iii. Electrodiagnostic evidence of moderate to severe compressive neuropathy of the median nerve is present. EMG findings showing evidence of acute or chronic motor denervation suggest the possibility that irreversible damage may be occurring. There is good evidence that surgery is more beneficial than non-surgical treatment for patients with a motor latency of more than 5.0 ms. B. For cases with positive EDX findings (see sub-paragraph B) of Section V.C.i at page 6) and with a motor latency less than 5.0 ms, non-surgical treatment may be beneficial in some cases; therefore, conservative management, including job alterations, should be tried over 4 to 6 weeks before surgery is considered. C. A clinical impression of moderate to severe CTS with normal EDS studies is very rare and generally indicates a mistaken diagnosis. Surgery may be

15 considered in cases where electrodiagnostic testing is normal and initial nonoperative therapy has failed. The following criteria must be met in deciding whether to proceed to surgery: i. The patients signs and symptoms are specific for CTS; AND ii. The patient experiences significant temporary relief following steroid injection into the carpal tunnel. Under these CTS Guidelines, only carpal tunnel surgeries under this subparagraph C must be pre-authorized by the carrier. VIII. OPERATIVE PROCEDURES: Endoscopic and open carpal tunnel release have low rates of serious complications. The most commonly seen serious complications are incomplete transection of the transverse carpal ligament and inadvertent nerve or vessel injuries. Choice of technique should be left to the discretion of the surgeon. A. Neurolysis: has not been proven advantageous for CTS. Internal neurolysis should never be done. Very few indications exist for external neurolysis. B. Tenosynovectomy: For routine cases of CTS, tenosynovectomy has not proven to be of benefit in CTS. Tenosynovectomy may be considered at the time of carpal tunnel release in the unusual case in which CTS is accompanied by rheumatoid arthritis. Performance of tenosynovectomy in such cases is subject to the existing pre-authorization requirement contained in regulations (12 NYCRR 324.2(d)(3)). IX. POST-OPERATIVE TREATMENT: A. Patients may receive a home therapy protocol involving stretching, ROM, scar management and resistive exercises. Patients should be encouraged to use the hand as much as possible for daily activities, allowing pain to guide their activities. B. There is some evidence showing that immediate mobilization of the wrist following surgery is associated with less scar pain, and faster return to work. Final decisions regarding the need for splinting post-operatively should be left to the discretion of the treating physician based upon the surgical technique used and the specific conditions of the patient

16 C. An individualized rehabilitation program may be helpful in patients who do not show functional improvements post-operatively or in patients with heavy or repetitive job activities. At least 2 visits are recommended to insure appropriate scar management and return to function. The post-operative rehabilitation program should be based upon communication between the treating physician and the therapist. In all cases, communication between the physician and therapist is important to the timing of exercise progressions. Communication is essential between the patient, employer and physician to determine appropriate restrictions and return-to-work dates. It is the responsibility of the physician to provide clear concise restrictions, and it is the employer s responsibility to determine if temporary duties can be provided within the restrictions. Considerations for repeat surgery: The single most important factor in predicting symptomatic improvement following carpal tunnel release is the severity of preoperative neuropathy. Patients with moderate electrodiagnostic abnormalities have better results than those with either very severe and/or mild findings. Incomplete cutting of the transverse carpal ligament or iatrogenic injury to the median nerve are rare. If median nerve symptoms do not improve following initial surgery or symptoms improve initially and then recur, but are unresponsive to non-operative therapy, consider the following: Repetitive work activities may be causing recurrent CTS; Scarring; Work-up for systemic diseases. A second opinion by a hand surgeon and repeat nerve conduction studies are required if repeat surgery is contemplated. The decision to undertake repeat surgery must factor in all of the above possibilities. Results of surgery for recurrent CTS vary widely depending on the etiology of recurrent symptoms. A repeat surgery is subject to the existing regulations (12 NYCRR 324.2(d)(3)) regarding the pre-authorization requirement

17
18

19
20

Carpal Tunnel Syndrome
 New York Carpal Tunnel Syndrome Medical Treatment Guidelines First Edition January 14, 2013 Effective March 1, 2013 Table of Contents A GENERAL GUIDELINE PRINCIPLES... 1 A.1 MEDICAL CARE... 1 A.2 RENDERING
New York Carpal Tunnel Syndrome Medical Treatment Guidelines First Edition January 14, 2013 Effective March 1, 2013 Table of Contents A GENERAL GUIDELINE PRINCIPLES... 1 A.1 MEDICAL CARE... 1 A.2 RENDERING
Carpal Tunnel Syndrome
 New York Carpal Tunnel Syndrome Medical Treatment Guidelines Proposed Second Edition, May 27, 2014 TABLE OF CONTENTS A B C GENERAL GUIDELINE PRINCIPLES... 1 A.1 MEDICAL CARE... 1 A.2 RENDERING OF MEDICAL
New York Carpal Tunnel Syndrome Medical Treatment Guidelines Proposed Second Edition, May 27, 2014 TABLE OF CONTENTS A B C GENERAL GUIDELINE PRINCIPLES... 1 A.1 MEDICAL CARE... 1 A.2 RENDERING OF MEDICAL
Informed Patient Tutorial Copyright 2012 by the American Academy of Orthopaedic Surgeons
 Informed Patient Tutorial Copyright 2012 by the American Academy of Orthopaedic Surgeons Informed Patient - Carpal Tunnel Release Surgery Introduction Welcome to the American Academy of Orthopaedic Surgeons'
Informed Patient Tutorial Copyright 2012 by the American Academy of Orthopaedic Surgeons Informed Patient - Carpal Tunnel Release Surgery Introduction Welcome to the American Academy of Orthopaedic Surgeons'
A Patient s Guide to Carpal Tunnel Syndrome
 A Patient s Guide to Carpal Tunnel Syndrome 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a
A Patient s Guide to Carpal Tunnel Syndrome 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a
CENTER FOR HEALTH AND SAFETY IN THE WORKPLACE
 CENTER FOR HEALTH AND SAFETY IN THE WORKPLACE A study by the RAND Institute for Civil Justice and RAND Health CHILDREN AND FAMILIES EDUCATION AND THE ARTS ENERGY AND ENVIRONMENT HEALTH AND HEALTH CARE
CENTER FOR HEALTH AND SAFETY IN THE WORKPLACE A study by the RAND Institute for Civil Justice and RAND Health CHILDREN AND FAMILIES EDUCATION AND THE ARTS ENERGY AND ENVIRONMENT HEALTH AND HEALTH CARE
Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis
 FPL FCR Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis Thenar motor branch Kaplan s cardinal line: distal TCL thenar branch Superficial palmar arch superficial arch Originates
FPL FCR Proximal border = palmar wrist crease Distal border = Kaplan + ring finger axis Thenar motor branch Kaplan s cardinal line: distal TCL thenar branch Superficial palmar arch superficial arch Originates
APPENDIX F INTERJURISDICTIONAL RESEARCH
 Ontario Scheduled Presumption: Bursitis, listed in Schedule 3, of the Ontario Workers Compensation Act, entry number 18 Description of Disease Bursitis Process Any process involving constant or prolonged
Ontario Scheduled Presumption: Bursitis, listed in Schedule 3, of the Ontario Workers Compensation Act, entry number 18 Description of Disease Bursitis Process Any process involving constant or prolonged
THE WRIST. At a glance. 1. Introduction
 THE WRIST At a glance The wrist is possibly the most important of all joints in everyday and professional life. It is under strain not only in many blue collar trades, but also in sports and is therefore
THE WRIST At a glance The wrist is possibly the most important of all joints in everyday and professional life. It is under strain not only in many blue collar trades, but also in sports and is therefore
 Full version is >>> HERE
Full version is >>> HERE Differentiating Cervical Radiculopathy and Peripheral Neuropathy. Adam P. Smith, MD
 Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
Aetna Nerve Conduction Study Policy
 Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma. Magee, 2008. pg.
 PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
Cervical Spondylosis (Arthritis of the Neck)
") Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Mini Medical School: Focus on Orthopaedics
 from The Cleveland Clinic Mini Medical School: Focus on Orthopaedics Common Disorders of the Hand and Wrist Jeffrey Lawton, MD Associate Staff, Department of Orthopaedic The Cleveland Clinic Appointments:
from The Cleveland Clinic Mini Medical School: Focus on Orthopaedics Common Disorders of the Hand and Wrist Jeffrey Lawton, MD Associate Staff, Department of Orthopaedic The Cleveland Clinic Appointments:
OUTPATIENT PHYSICAL AND OCCUPATIONAL THERAPY PROTOCOL GUIDELINES
 OUTPATIENT PHYSICAL AND OCCUPATIONAL THERAPY PROTOCOL GUIDELINES General Therapy Guidelines 1. Therapy evaluations must be provided by licensed physical and/or occupational therapists. Therapy evaluations
OUTPATIENT PHYSICAL AND OCCUPATIONAL THERAPY PROTOCOL GUIDELINES General Therapy Guidelines 1. Therapy evaluations must be provided by licensed physical and/or occupational therapists. Therapy evaluations
A Patient s Guide to Guyon s Canal Syndrome
 A Patient s Guide to DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or
A Patient s Guide to DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or
Repetitive Strain Injury (RSI)
") Carpal Tunnel Syndrome and Other Musculoskeletal Problems in the Workplace: What s the Solution? by Richard N. Hinrichs, Ph.D. Dept. of Kinesiology Arizona State University Repetitive Strain Injury (RSI)
Carpal Tunnel Syndrome and Other Musculoskeletal Problems in the Workplace: What s the Solution? by Richard N. Hinrichs, Ph.D. Dept. of Kinesiology Arizona State University Repetitive Strain Injury (RSI)
CONSTRUCTION WORK and CUMULATIVE TRAUMA DISORDERS
 Connecticut Department of Public Health Environmental and Occupational Health Assessment Program 410 Capitol Avenue MS # 11OSP, PO Box 340308 Hartford, CT 06134-0308 (860) 509-7740 http://www.ct.gov/dph
Connecticut Department of Public Health Environmental and Occupational Health Assessment Program 410 Capitol Avenue MS # 11OSP, PO Box 340308 Hartford, CT 06134-0308 (860) 509-7740 http://www.ct.gov/dph
ELECTROMYOGRAPHY (EMG), NEEDLE, NERVE CONDUCTION STUDIES (NCS) AND QUANTITATIVE SENSORY TESTING (QST)
, NEEDLE, NERVE CONDUCTION STUDIES (NCS) AND QUANTITATIVE SENSORY TESTING (QST)") AND QUANTITATIVE SENSORY TESTING (QST) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical
AND QUANTITATIVE SENSORY TESTING (QST) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical
.org. Tennis Elbow (Lateral Epicondylitis) Anatomy. Cause
 Anatomy. Cause") Tennis Elbow (Lateral Epicondylitis) Page ( 1 ) Tennis elbow, or lateral epicondylitis, is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can
Tennis Elbow (Lateral Epicondylitis) Page ( 1 ) Tennis elbow, or lateral epicondylitis, is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can
Herniated Cervical Disc
 Herniated Cervical Disc North American Spine Society Public Education Series What Is a Herniated Disc? The backbone, or spine, is composed of a series of connected bones called vertebrae. The vertebrae
Herniated Cervical Disc North American Spine Society Public Education Series What Is a Herniated Disc? The backbone, or spine, is composed of a series of connected bones called vertebrae. The vertebrae
EMG and the Electrodiagnostic Consultation for the Family Physician
 EMG and the Electrodiagnostic Consultation for the Family Physician Stephanie Kopey, D.O., P.T. 9/27/15 The American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) Marketing Committee
EMG and the Electrodiagnostic Consultation for the Family Physician Stephanie Kopey, D.O., P.T. 9/27/15 The American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) Marketing Committee
 Full version is >>> HERE
Full version is >>> HERE Fact Sheet: Occupational Overuse Syndrome (OOS)
") Fact Sheet: Occupational Overuse Syndrome (OOS) What is OOS? Occupational Overuse Syndrome (OOS) is the term given to a range of conditions characterised by discomfort or persistent pain in muscles, tendons
Fact Sheet: Occupational Overuse Syndrome (OOS) What is OOS? Occupational Overuse Syndrome (OOS) is the term given to a range of conditions characterised by discomfort or persistent pain in muscles, tendons
Herniated Lumbar Disc
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Hand Injuries and Disorders
 Hand Injuries and Disorders Introduction Each of your hands has 27 bones, 15 joints and approximately 20 muscles. There are many common problems that can affect your hands. Hand problems can be caused
Hand Injuries and Disorders Introduction Each of your hands has 27 bones, 15 joints and approximately 20 muscles. There are many common problems that can affect your hands. Hand problems can be caused
Medical Report Checklist: Upper Extremities Peripheral Nerve Disorders Impairments (PND)
") http://www.pdratings.com/ Craig Andrew Lange craig@pdratings.com California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
http://www.pdratings.com/ Craig Andrew Lange craig@pdratings.com California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
Ms. Jackson is the Manager of Health Finance and Reimbursement, Division of Health Policy and Practice Services, Washington, DC.
 Electrodiagnostic Testing with Same Day Evaluation Management By: Shane J. Burr, MD; Scott I. Horn, DO; Jenny J. Jackson, MPH, CPC; Joseph P. Purcell, DO Dr. Burr practices general inpatient and outpatient
Electrodiagnostic Testing with Same Day Evaluation Management By: Shane J. Burr, MD; Scott I. Horn, DO; Jenny J. Jackson, MPH, CPC; Joseph P. Purcell, DO Dr. Burr practices general inpatient and outpatient
Standard of Care: Cervical Radiculopathy
 Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
.org. Arthritis of the Hand. Description
 Arthritis of the Hand Page ( 1 ) The hand and wrist have multiple small joints that work together to produce motion, including the fine motion needed to thread a needle or tie a shoelace. When the joints
Arthritis of the Hand Page ( 1 ) The hand and wrist have multiple small joints that work together to produce motion, including the fine motion needed to thread a needle or tie a shoelace. When the joints
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN. Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA
 DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
Whiplash and Whiplash- Associated Disorders
 Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Neck Injuries and Disorders
 Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
International Encyclopedia of Rehabilitation
 International Encyclopedia of Rehabilitation Copyright 2010 by the Center for International Rehabilitation Research Information and Exchange (CIRRIE). All rights reserved. No part of this publication may
International Encyclopedia of Rehabilitation Copyright 2010 by the Center for International Rehabilitation Research Information and Exchange (CIRRIE). All rights reserved. No part of this publication may
Acute Low Back Pain. North American Spine Society Public Education Series
 Acute Low Back Pain North American Spine Society Public Education Series What Is Acute Low Back Pain? Acute low back pain (LBP) is defined as low back pain present for up to six weeks. It may be experienced
Acute Low Back Pain North American Spine Society Public Education Series What Is Acute Low Back Pain? Acute low back pain (LBP) is defined as low back pain present for up to six weeks. It may be experienced
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
.org. Cervical Spondylosis (Arthritis of the Neck) Anatomy. Cause
 Anatomy. Cause") Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
CARPAL TUNNEL SYNDROME A PATIENT GUIDE TO THE NURSE-LED CARPAL TUNNEL SERVICE
 CARPAL TUNNEL SYNDROME A PATIENT GUIDE TO THE NURSE-LED CARPAL TUNNEL SERVICE Information Leaflet Your Health. Our Priority. Page 2 of 6 What is carpal tunnel syndrome? It is entrapment of a nerve at the
CARPAL TUNNEL SYNDROME A PATIENT GUIDE TO THE NURSE-LED CARPAL TUNNEL SERVICE Information Leaflet Your Health. Our Priority. Page 2 of 6 What is carpal tunnel syndrome? It is entrapment of a nerve at the
THORACIC OUTLET SYNDROME
 THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
CARPAL TUNNEL SYNDROME
 CARPAL TUNNEL SYNDROME Background 1. Definition: Entrapment neuropathy of median nerve as it courses through carpal tunnel o Stage I: Predominantly nocturnal symptoms of numbness and /or tingling in fingers
CARPAL TUNNEL SYNDROME Background 1. Definition: Entrapment neuropathy of median nerve as it courses through carpal tunnel o Stage I: Predominantly nocturnal symptoms of numbness and /or tingling in fingers
Carpal Tunnel Syndrome
 Carpal Tunnel Syndrome Information for patients Therapy Services Phone no: 01625 661481 www.eastcheshire.nhs.uk @eastcheshirenhs Ref: 11437 Review: 06/2015 Carpal Tunnel Syndrome Ref: 11437 Page 1 Review:
Carpal Tunnel Syndrome Information for patients Therapy Services Phone no: 01625 661481 www.eastcheshire.nhs.uk @eastcheshirenhs Ref: 11437 Review: 06/2015 Carpal Tunnel Syndrome Ref: 11437 Page 1 Review:
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN
 CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
Carpal Tunnel Release. Relieving Pressure in Your Wrist
 Carpal Tunnel Release Relieving Pressure in Your Wrist Understanding Carpal Tunnel Syndrome Carpal tunnel syndrome (CTS) is a problem that affects the wrist and hand. If you have CTS, tingling and numbness
Carpal Tunnel Release Relieving Pressure in Your Wrist Understanding Carpal Tunnel Syndrome Carpal tunnel syndrome (CTS) is a problem that affects the wrist and hand. If you have CTS, tingling and numbness
Ergonomics Monitor Training Manual
 Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Herniated Disk. This reference summary explains herniated disks. It discusses symptoms and causes of the condition, as well as treatment options.
 Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
.org. Herniated Disk in the Lower Back. Anatomy. Description
 Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Back & Neck Pain Survival Guide
 Back & Neck Pain Survival Guide www.kleinpeterpt.com Zachary - 225-658-7751 Baton Rouge - 225-768-7676 Kleinpeter Physical Therapy - Spine Care Program Finally! A Proven Assessment & Treatment Program
Back & Neck Pain Survival Guide www.kleinpeterpt.com Zachary - 225-658-7751 Baton Rouge - 225-768-7676 Kleinpeter Physical Therapy - Spine Care Program Finally! A Proven Assessment & Treatment Program
INFLUENCE OF SELECTED PHYSICAL EXERCISES TO IMPROVE OUTCOMES IN PATIENTS OPERATED FOR CARPAL TUNNEL SYNDROME IN OWN MATERIAL
 Central European Journal of Sport Sciences and Medicine : 47 51 INFLUENCE OF SELECTED PHYSICAL EXERCISES TO IMPROVE OUTCOMES IN PATIENTS OPERATED FOR CARPAL TUNNEL SYNDROME IN OWN MATERIAL Zbigniew Deskur,
Central European Journal of Sport Sciences and Medicine : 47 51 INFLUENCE OF SELECTED PHYSICAL EXERCISES TO IMPROVE OUTCOMES IN PATIENTS OPERATED FOR CARPAL TUNNEL SYNDROME IN OWN MATERIAL Zbigniew Deskur,
Hand and Upper Extremity Injuries in Outdoor Activities. John A. Schneider, M.D.
 Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Radiculopathy vs. Peripheral Neuropathy. What to do with arm pain? Defining Arm Pain. Arm Pain
 Radiculopathy vs. Peripheral Neuropathy What to do with arm pain? Miriana G. Popadich RN, MSN Clinical Care Coordinator Brachial Plexus Program Department of Neurosurgery University of Michigan Timing
Radiculopathy vs. Peripheral Neuropathy What to do with arm pain? Miriana G. Popadich RN, MSN Clinical Care Coordinator Brachial Plexus Program Department of Neurosurgery University of Michigan Timing
Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA
 Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA 2 offices 805 Sir Thomas Court Harrisburg 3 Walnut Street Lemoyne Mechanism of injury Repetitive overhead activities Falls to the ground Falls with
Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA 2 offices 805 Sir Thomas Court Harrisburg 3 Walnut Street Lemoyne Mechanism of injury Repetitive overhead activities Falls to the ground Falls with
AN EDUCATION BASED ERGONOMIC INTERVENTION PROGRAMME FOR GAUTENG CALL CENTRE WORKERS WITH UPPER EXTREMITY REPETITIVE STRAIN INJURIES.
 AN EDUCATION BASED ERGONOMIC INTERVENTION PROGRAMME FOR GAUTENG CALL CENTRE WORKERS WITH UPPER EXTREMITY REPETITIVE STRAIN INJURIES. Sancha Eliot Johannesburg 2010 DECLARATION I SANCHA ELIOT declare that
AN EDUCATION BASED ERGONOMIC INTERVENTION PROGRAMME FOR GAUTENG CALL CENTRE WORKERS WITH UPPER EXTREMITY REPETITIVE STRAIN INJURIES. Sancha Eliot Johannesburg 2010 DECLARATION I SANCHA ELIOT declare that
Adult Forearm Fractures
 Adult Forearm Fractures Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken. Fractures of the forearm can occur near the wrist at
Adult Forearm Fractures Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken. Fractures of the forearm can occur near the wrist at
Neck Pain Frequently Asked Questions. Moe R. Lim, MD UNC Orthopaedics (919-96B-ONES) UNC Spine Center (919-957-6789)
 UNC Spine Center (919-957-6789)") Neck Pain Frequently Asked Questions Moe R. Lim, MD UNC Orthopaedics (919-96B-ONES) UNC Spine Center (919-957-6789) Neck Pain Human Spine 25 bones Cervical (7) Thoracic (12) Lumbar (5) Sacrum Human Spine
Neck Pain Frequently Asked Questions Moe R. Lim, MD UNC Orthopaedics (919-96B-ONES) UNC Spine Center (919-957-6789) Neck Pain Human Spine 25 bones Cervical (7) Thoracic (12) Lumbar (5) Sacrum Human Spine
1st Edition 2015. Quick reference guide for the management of acute whiplash. associated disorders
 1 1st Edition 2015 Quick reference guide for the management of acute whiplash associated disorders 2 Quick reference guide for the management of acute whiplash associated disorders, 2015. This quick reference
1 1st Edition 2015 Quick reference guide for the management of acute whiplash associated disorders 2 Quick reference guide for the management of acute whiplash associated disorders, 2015. This quick reference
.org. Shoulder Pain and Common Shoulder Problems. Anatomy. Cause
 Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
.org. Rotator Cuff Tears. Anatomy. Description
 Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
Welcome to the July 2012 edition of Case Studies from the files of the Institute for Nerve Medicine in Santa Monica, California.
 Welcome to the July 2012 edition of Case Studies from the files of the Institute for Nerve Medicine in Santa Monica, California. In this issue, we focus on a 23-year-old female patient referred by her
Welcome to the July 2012 edition of Case Studies from the files of the Institute for Nerve Medicine in Santa Monica, California. In this issue, we focus on a 23-year-old female patient referred by her
BEFORE THE APPEALS BOARD FOR THE KANSAS DIVISION OF WORKERS COMPENSATION
 BEFORE THE APPEALS BOARD FOR THE KANSAS DIVISION OF WORKERS COMPENSATION BARBARA SHEREE HUTSON ) Claimant ) ) VS. ) Docket No. 1,035,700 ) CUSTOM CAMPERS, INC. ) Self-Insured Respondent ) ORDER Claimant
BEFORE THE APPEALS BOARD FOR THE KANSAS DIVISION OF WORKERS COMPENSATION BARBARA SHEREE HUTSON ) Claimant ) ) VS. ) Docket No. 1,035,700 ) CUSTOM CAMPERS, INC. ) Self-Insured Respondent ) ORDER Claimant
NOT DESIGNATED FOR PUBLICATION
 NOT DESIGNATED FOR PUBLICATION BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F503749 EVLYNENE KIRKENDOLPH, EMPLOYEE C L A I M ANT DF&A REVENUE SERVICES DIVISION/ OFFICE OF CHILD SUPPORT
NOT DESIGNATED FOR PUBLICATION BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F503749 EVLYNENE KIRKENDOLPH, EMPLOYEE C L A I M ANT DF&A REVENUE SERVICES DIVISION/ OFFICE OF CHILD SUPPORT
Medical Treatment Guidelines Washington State Department of Labor and Industries
 Complex regional pain syndrome (CRPS) Formerly known as reflex sympathetic dystrophy 1. Introduction This bulletin outlines the Department of Labor and Industries guidelines for diagnosing and treating
Complex regional pain syndrome (CRPS) Formerly known as reflex sympathetic dystrophy 1. Introduction This bulletin outlines the Department of Labor and Industries guidelines for diagnosing and treating
Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy. Spine Volume 21(16) August 15, 1996, pp 1877-1883
 August 15, 1996, pp 1877-1883") Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy 1 Spine Volume 21(16) August 15, 1996, pp 1877-1883 Saal, Joel S. MD; Saal, Jeffrey A. MD; Yurth, Elizabeth F. MD FROM
Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy 1 Spine Volume 21(16) August 15, 1996, pp 1877-1883 Saal, Joel S. MD; Saal, Jeffrey A. MD; Yurth, Elizabeth F. MD FROM
Elbow Injuries and Disorders
 Elbow Injuries and Disorders Introduction Your elbow joint is made up of bone, cartilage, ligaments and fluid. Muscles and tendons help the elbow joint move. There are many injuries and disorders that
Elbow Injuries and Disorders Introduction Your elbow joint is made up of bone, cartilage, ligaments and fluid. Muscles and tendons help the elbow joint move. There are many injuries and disorders that
Notice of Independent Review Decision DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE:
 Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
3nd Biennial Contemporary Clinical Neurophysiological Symposium October 12, 2013 Fundamentals of NCS and NMJ Testing
 3nd Biennial Contemporary Clinical Neurophysiological Symposium October 12, 2013 Fundamentals of NCS and NMJ Testing Peter D. Donofrio, M.D. Professor of Neurology Vanderbilt University Medical Center
3nd Biennial Contemporary Clinical Neurophysiological Symposium October 12, 2013 Fundamentals of NCS and NMJ Testing Peter D. Donofrio, M.D. Professor of Neurology Vanderbilt University Medical Center
How To Treat Musculoskeletal Injury In Sonographers
 MUSCULOSKELETAL DISORDERS IN SONOGRAPHERS: ARE WE DOING ENOUGH? Many terms are used to refer to work related injuries among sonographers. Musculosketetal injury (MSI) Repetitive motion injury (RMI) Repetitive
MUSCULOSKELETAL DISORDERS IN SONOGRAPHERS: ARE WE DOING ENOUGH? Many terms are used to refer to work related injuries among sonographers. Musculosketetal injury (MSI) Repetitive motion injury (RMI) Repetitive
ARTHRITIS INTRODUCTION
 ARTHRITIS INTRODUCTION Arthritis is the most common disease affecting the joints. There are various forms of arthritis but the two that are the most common are osteoarthritis (OA), and rheumatoid arthritis
ARTHRITIS INTRODUCTION Arthritis is the most common disease affecting the joints. There are various forms of arthritis but the two that are the most common are osteoarthritis (OA), and rheumatoid arthritis
Hand & Plastics Physiotherapy Department Carpal Tunnel Syndrome Information for patients
 Oxford University Hospitals NHS Trust Hand & Plastics Physiotherapy Department Carpal Tunnel Syndrome Information for patients page 2 What is the Carpal Tunnel? The carpal tunnel is made up of the bones
Oxford University Hospitals NHS Trust Hand & Plastics Physiotherapy Department Carpal Tunnel Syndrome Information for patients page 2 What is the Carpal Tunnel? The carpal tunnel is made up of the bones
Ulnar Neuropathy Differential Diagnosis and Prognosis. Disclosures: None
 Ulnar Neuropathy Differential Diagnosis and Prognosis Disclosures: None Goals of Lecture Describe anatomy: sites of entrapment Ulnar nerve Discuss differential diagnosis of ulnar nerve pathology Identify
Ulnar Neuropathy Differential Diagnosis and Prognosis Disclosures: None Goals of Lecture Describe anatomy: sites of entrapment Ulnar nerve Discuss differential diagnosis of ulnar nerve pathology Identify
.org. Cervical Radiculopathy (Pinched Nerve) Anatomy. Cause
 Anatomy. Cause") Cervical Radiculopathy (Pinched Nerve) Page ( 1 ) Cervical radiculopathy, commonly called a pinched nerve occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal
Cervical Radiculopathy (Pinched Nerve) Page ( 1 ) Cervical radiculopathy, commonly called a pinched nerve occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal
Electrodiagnostic Testing
 Electrodiagnostic Testing Electromyogram and Nerve Conduction Study North American Spine Society Public Education Series What Is Electrodiagnostic Testing? The term electrodiagnostic testing covers a
Electrodiagnostic Testing Electromyogram and Nerve Conduction Study North American Spine Society Public Education Series What Is Electrodiagnostic Testing? The term electrodiagnostic testing covers a
WHEN TO ORDER; HOW TO INTERPRET
 ELECTROMYOGRAPHY AND 1 NERVE CONDUCTION TESTING: WHEN TO ORDER; HOW TO INTERPRET Ronald N. Kent, M.D., Ph.D. 2 ELECTROMYOGRAPHY AND NERVE CONDUCTION TESTING EMG/NCS Testing is a component of a complete
ELECTROMYOGRAPHY AND 1 NERVE CONDUCTION TESTING: WHEN TO ORDER; HOW TO INTERPRET Ronald N. Kent, M.D., Ph.D. 2 ELECTROMYOGRAPHY AND NERVE CONDUCTION TESTING EMG/NCS Testing is a component of a complete
Y O U R S U R G E O N S. choice of. implants F O R Y O U R S U R G E R Y
 Y O U R S U R G E O N S choice of implants F O R Y O U R S U R G E R Y Y O U R S U R G E O N S choice of implants F O R Y O U R S U R G E R Y Your Surgeon Has Chosen the C 2 a-taper Acetabular System The
Y O U R S U R G E O N S choice of implants F O R Y O U R S U R G E R Y Y O U R S U R G E O N S choice of implants F O R Y O U R S U R G E R Y Your Surgeon Has Chosen the C 2 a-taper Acetabular System The
NERVE COMPRESSION DISORDERS
 Common Disorders of the Hand and Wrist Ryan Klinefelter, MD Associate Professor of Orthopaedics Department of Orthopaedics The Ohio State University Medical Center NERVE COMPRESSION DISORDERS 1 Carpal
Common Disorders of the Hand and Wrist Ryan Klinefelter, MD Associate Professor of Orthopaedics Department of Orthopaedics The Ohio State University Medical Center NERVE COMPRESSION DISORDERS 1 Carpal
New York State Workers' Comp Board. Mid and Lower Back Treatment Guidelines. Summary From 1st Edition, June 30, 2010. Effective December 1, 2010
 New York State Workers' Comp Board Mid and Lower Back Treatment Guidelines Summary From 1st Edition, June 30, 2010 Effective December 1, 2010 General Principles Treatment should be focused on restoring
New York State Workers' Comp Board Mid and Lower Back Treatment Guidelines Summary From 1st Edition, June 30, 2010 Effective December 1, 2010 General Principles Treatment should be focused on restoring
Title 40, Part I. Strong Level 1 Evidence We Recommend. Level 2 and Level 3
 Chapter 22. Neurological and Neuromuscular Disorder Medical Treatment Guidelines Subchapter A. Carpal Tunnel Syndrome (CTS) Medical Treatment Guidelines Editor s Note: Form LWC-WC 1009. Disputed Claim
Chapter 22. Neurological and Neuromuscular Disorder Medical Treatment Guidelines Subchapter A. Carpal Tunnel Syndrome (CTS) Medical Treatment Guidelines Editor s Note: Form LWC-WC 1009. Disputed Claim
Role of Electrodiagnostic Tests in Neuromuscular Disease
 Role of Electrodiagnostic Tests in Neuromuscular Disease Electrodiagnostic tests Electroencephalogram (EEG) Electromyography (NCV, EMG) Cerebral evoked potentials (CEP) Motor evoked potentials (MEP) Electronystagmogram
Role of Electrodiagnostic Tests in Neuromuscular Disease Electrodiagnostic tests Electroencephalogram (EEG) Electromyography (NCV, EMG) Cerebral evoked potentials (CEP) Motor evoked potentials (MEP) Electronystagmogram
Keeping the Aging Worker Productive and Injury Free
 Keeping the Aging Worker Productive and Injury Free Peter Goyert PT CCPE Senior Ergonomist WorkSafeBC Aging Some say aging is > 30 years. Everybody is aging. Generally aging workers refer to those in last
Keeping the Aging Worker Productive and Injury Free Peter Goyert PT CCPE Senior Ergonomist WorkSafeBC Aging Some say aging is > 30 years. Everybody is aging. Generally aging workers refer to those in last
Treating Bulging Discs & Sciatica. Alexander Ching, MD
 Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Sample Treatment Protocol
 Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
OVERVIEW. NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. WHAT IS THE MOST IMPORTANT PART OF THE PHYSICAL EXAM?
 NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
Chronic Low Back Pain
 Chronic Low Back Pain North American Spine Society Public Education Series What is Chronic Pain? Low back pain is considered to be chronic if it has been present for longer than three months. Chronic low
Chronic Low Back Pain North American Spine Society Public Education Series What is Chronic Pain? Low back pain is considered to be chronic if it has been present for longer than three months. Chronic low
a) Nerve conduction studies (NCS) test the peripheral nervous system for:
 Nerve conduction studies (NCS) test the peripheral nervous system for:") Health Plan Coverage Policy ARBenefits Approval: 11/02/2011 Effective Date: 01/01/2012 Revision Date: 09/18/2013 Comments: Code additions only. Title: Electrodiagnostic Testing Document: ARB0256 Public
Health Plan Coverage Policy ARBenefits Approval: 11/02/2011 Effective Date: 01/01/2012 Revision Date: 09/18/2013 Comments: Code additions only. Title: Electrodiagnostic Testing Document: ARB0256 Public
SUMMARY. Carpal tunnel syndrome; Permanent impairment [NEL] (rating schedule) (AMA Guides) (functional impairment).
![SUMMARY. Carpal tunnel syndrome; Permanent impairment [NEL] (rating schedule) (AMA Guides) (functional impairment).](/thumbs/25/5513776.jpg "SUMMARY. Carpal tunnel syndrome; Permanent impairment [NEL] (rating schedule) (AMA Guides) (functional impairment).") SUMMARY DECISION NO. 1033/98 Carpal tunnel syndrome; Permanent impairment [NEL] (rating schedule) (AMA Guides) (functional impairment). The worker was a stope miner for four years beginning in 1987. In
SUMMARY DECISION NO. 1033/98 Carpal tunnel syndrome; Permanent impairment [NEL] (rating schedule) (AMA Guides) (functional impairment). The worker was a stope miner for four years beginning in 1987. In
THORACIC OUTLET SYNDROME & BRACHIAL PLEXUS INJURIES
 THORACIC OUTLET SYNDROME & BRACHIAL PLEXUS INJURIES I. THORACIC OUTLET SYNDROME TOS is a compression of nerves or blood vessels, or both, in the thoracic outlet region, which is the space between the collarbone
THORACIC OUTLET SYNDROME & BRACHIAL PLEXUS INJURIES I. THORACIC OUTLET SYNDROME TOS is a compression of nerves or blood vessels, or both, in the thoracic outlet region, which is the space between the collarbone
Multifocal Motor Neuropathy. Jonathan Katz, MD Richard Lewis, MD
 Multifocal Motor Neuropathy Jonathan Katz, MD Richard Lewis, MD What is Multifocal Motor Neuropathy? Multifocal Motor Neuropathy (MMN) is a rare condition in which multiple motor nerves are attacked by
Multifocal Motor Neuropathy Jonathan Katz, MD Richard Lewis, MD What is Multifocal Motor Neuropathy? Multifocal Motor Neuropathy (MMN) is a rare condition in which multiple motor nerves are attacked by
Integra. MCP Joint Replacement PATIENT INFORMATION
 Integra MCP Joint Replacement PATIENT INFORMATION Integra MCP Patient Information This brochure summarizes information about the use, risks, and benefits of the Integra MCP finger implant. Be sure to discuss
Integra MCP Joint Replacement PATIENT INFORMATION Integra MCP Patient Information This brochure summarizes information about the use, risks, and benefits of the Integra MCP finger implant. Be sure to discuss
Evaluation of Disorders of the Hands and Wrists
 Evaluation of Disorders of the Hands and Wrists Case 27 yo female with 6 month history of right forearm and hand pain Works as secretary, symptoms are interfering with her job duties Complains that she
Evaluation of Disorders of the Hands and Wrists Case 27 yo female with 6 month history of right forearm and hand pain Works as secretary, symptoms are interfering with her job duties Complains that she
GUIDANCE AND PROCEDURE FOR HAND ARM VIBRATION
 Department of Human Resources GUIDANCE AND PROCEDURE FOR HAND ARM VIBRATION 1.0 What is Hand-Arm Vibration Syndrome (HAVS)? Hand-Arm Vibration Syndrome (HAVS) is a widespread industrial disease. The Health
Department of Human Resources GUIDANCE AND PROCEDURE FOR HAND ARM VIBRATION 1.0 What is Hand-Arm Vibration Syndrome (HAVS)? Hand-Arm Vibration Syndrome (HAVS) is a widespread industrial disease. The Health
Neck Pain Overview Causes, Diagnosis and Treatment Options
 Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
The Carpal Tunnel CTS. Stålberg 1. Dysfunction of median nerve in the carpal tunnel resulting in
 The Carpal Tunnel CTS Dysfunction of median nerve in the carpal tunnel resulting in 1 Symptoms in CTS pain and numbness in the abd worse on finger activity aggravated by forceful gripping g symptoms more
The Carpal Tunnel CTS Dysfunction of median nerve in the carpal tunnel resulting in 1 Symptoms in CTS pain and numbness in the abd worse on finger activity aggravated by forceful gripping g symptoms more
CTS the Best EDX. Ernest W Johnson MD Emeritus Professor Physical Medicine & Rehabilitation The Ohio State University
 CTS the Best EDX Ernest W Johnson MD Emeritus Professor Physical Medicine & Rehabilitation The Ohio State University 1 Definition of CTS A syndrome 2d to dysfunction of median nerve in carpal tunnel resulting
CTS the Best EDX Ernest W Johnson MD Emeritus Professor Physical Medicine & Rehabilitation The Ohio State University 1 Definition of CTS A syndrome 2d to dysfunction of median nerve in carpal tunnel resulting
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Arthritis of the Shoulder
 Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
How To Cover Occupational Therapy
 Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
1 of 6 1/22/2015 10:06 AM
 1 of 6 1/22/2015 10:06 AM 2 of 6 1/22/2015 10:06 AM This cross-section view of the shoulder socket shows a typical SLAP tear. Injuries to the superior labrum can be caused by acute trauma or by repetitive
1 of 6 1/22/2015 10:06 AM 2 of 6 1/22/2015 10:06 AM This cross-section view of the shoulder socket shows a typical SLAP tear. Injuries to the superior labrum can be caused by acute trauma or by repetitive