Multiple Myeloma F1 蘇 勇 誠 /MA 林 棟 樑
|
|
|
- Ethelbert Merritt
- 8 years ago
- Views:
Transcription
1 Multiple Myeloma F1 蘇 勇 誠 /MA 林 棟 樑

2 Plasma Cell Disorders Multiple Myeloma Other Disorders Monoclonal gammopathy of undetermined significance (MGUS) Smoldering multiple myeloma (SMM) Solitary Plasmacytoma» Bone» Extramedullary Waldenström s Macroglobulinemia Primary Amyloidosis (AL) Heavy chain disease POEMS syndrome / osteosclerotic myeloma Type I and II cryoglobulinemia Light chain deposition disease

 Amyloidosis (AL) 10% (130) Mayo Clinic Experience SMM, 3.5% (44) Solitary or extramedullary, 1.")
3 Distribution of Monoclonal Gammopathies n=1296 Lymphoproliferative 2.5% (31) Amyloidosis (AL) 10% (130) Mayo Clinic Experience SMM, 3.5% (44) Solitary or extramedullary, 1.5% (20) Macro, 3% (41) Other, 2.5% (34) Myeloma 15% (193) MGUS 62% (803)
 Solitary or extramedullary, 1.")
4 Background and biology

5

6


7 Criteria for Diagnosis of Myeloma MGUS <3 g M spike <10% PC AND Smoldering MM 3 g M spike OR 10% PC Active MM 10% PC M spike + AND No anemia, bone lesions normal calcium and kidney function Anemia, bone lesions, high calcium or abnormal kidney function Kyle RA. N Engl J Med 2002; 346: 564

8 Multiple Myeloma Malignancy of plasma cells Hallmarks: Anemia Renal failure Bone destruction (lytic bone lesions) Hypercalcemia Presence of monoclonal protein Increased risk of infection

9 Multiple Myeloma Prevalence 2nd most common hematologic malignancy 1% of all malignant diseases About 10% of hematologic malignancies Annual incidence: 4/100,000 Median age at diagnosis is 66 years Younger than 50 years: 10% Median survival from diagnosis: 3-5 years 5-year survival: 31% 10-year survival: 10% 5-year survival: 5%

10 Multiple Myeloma Population subgroups Incidence twice as high in African Americans More frequent in men than women This disease remains incurable in most patients


11 Historical Perspective of Multiple Myeloma 1st patient diagnosed with bone pain and heat soluble and "animal matter" in urine Termed MM BM involvement recognized Plasma cell discovered MM associated with plasmacytosis Peak on serum protein electrophoresis noted Bence Jones and MM serum IgG proteins identical


12 Historical Perspective of Multiple Myeloma ABMT VAD High-dose therapy with autologous stem cell support Proteasome inhibitors Other immunomodulatory agents High-dose melphalan Oral melphalan and prednisone High-dose dexamethasone Bisphosphonates Thalidomide

13 Plasma Cell Morphology

14 Normal Serum Protein Electrophoresis

15 Serum Protein Electrophoresis Showing Monoclonal Protein in Myeloma

16 Immunofixation to Determine Type of Monoclonal Protein IgG kappa M protein

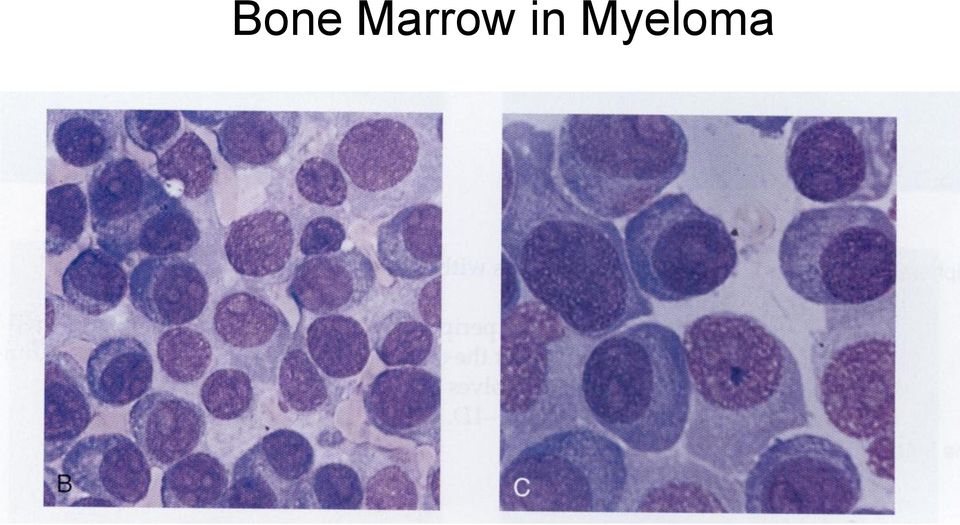
17 Bone Marrow in Myeloma
18 Immunophenotyping Light-chain restriction: kappa/lambda Typically CD 138+ and CD 38+/CD45- Usually CD19-/CD56+ normal plasma cells: CD19+/CD56- CD20(+) in only 15-20% of MM patients (11;14) Lymphoplasmacytic or small mature plasma cells
 Lymphoplasmacytic or small mature")
19 Evolution of MM: The MGUS to Myeloma Progression

20 Distinguishing Multiple Myeloma from MGUS Myeloma MGUS Bone marrow plasma cells 10% on aspirate < 10% on aspirate Serum paraprotein Variable concentration in serum; IgG usually > 3gm/dl IgG usually < 3gm/dl IgA usually <1gm/dl Bence-Jones proteinuria >50% cases Rare Immune paresis > 95% cases Rare Lytic bone lesions Often present Absent Symptoms Frequent Absent Anemia Frequent Absent Hypercalcemia May be present Absent Abnormal renal function May be present Absent

21 MGUS: Rate of Progression to Any Lymphocytic Disorder
22 MGUS: Risk of Progression Based on Initial M-spike
23 MGUS Size of monoclonal (M) protein and risk of progression to myeloma or related malignancy M-Protein Size (g/dl) Risk of Progression at 10 years (%) Risk of Progression at 20 years (%)
24 Relative Risk Diagnosis of Patients Who Have Progressed from MGUS MM 2.4 IgM lymphoma 8.4 Primary amyloidosis 0.9 Chronic lymphocytic leukemia 8.5 Macroglobulinemia Plasmacytoma Disease
25 Chromosomal Abnormalities in Myeloma Incidence Conventional G-banding: 30-50% of patients Difficult due to low proliferative activities Interphase FISH: > 90% of cases Poor prognosis Deletion of chromosome 13 or 13q14 t(4;14) t(14;16) 17p- Chromosome 1q21 aberration
26 Chromosomal Abnormalities 14q32(IgH locus): most common 11q13: most common (bcl-1 locus, 30%) 4p16 (FGFR3, MMSET, 25%) 8q24 (c-myc, 5%) 16q23 (c-maf, 1%) 6p25 (IRF4, rare) P53 Chromosome 1q21 aberration 13 deletion (Rb) 10-20% of patients using conventional cytogenetics and 50% using FISH
27 Clinical presentations and staging
28 Major Symptoms at Diagnosis Bone Pain 58% Fatigue 32% Weight Loss 24% Paresthesias 5% 11% are asymptomatic or have only mild symptoms at diagnosis
29 Clinical Features at Presentation Monoclonal (M) protein (93%) Lytic bone lesions (67%) Increased plasma cells in the bone marrow (96%) Anemia (normochromic normocytic; 73%) Hypercalcemia >11 (13%) Renal failure, serum creatinine >2.0 (19%) Infection
 Serum M spike: 80% Abnormal immunofixation: 90% Detectable urine paraprotein: 75% IgG: 50% 54% IgA: 20% Monoclonal light chain: 16% <20%")
30 Distribution of Monoclonal Proteins in Multiple Myeloma M protein found in serum or urine or both at time of diagnosis in 97% of patients (3% are non-secretory) Serum M spike: 80% Abnormal immunofixation: 90% Detectable urine paraprotein: 75% IgG: 50% 54% IgA: 20% Monoclonal light chain: 16% <20% IgD: 2%
31 Percentage Types of Serum Monoclonal Proteins in 1027 Patients With Multiple Myeloma % % 15 13% 10 8% 9% 7% 7% % 0.2% 1% 1% IgG IgG IgA IgA IgM IgM IgD IgD Free Free Biclonal Negative only only Type of Monoclonal Protein 2%
32 Categories of Multiple Myeloma Classification Characteristics Management MGUS Smoldering MM Serum M protein <3 g/dl Bone marrow plasma cells <10% if done Absence of anemia, renal failure, hypercalcemia, and lytic bone lesions Serum M protein <3 g/dl and/or Bone marrow plasma cells <10% if done Absence of anemia, renal failure, hypercalcemia, and lytic bone lesions Observation with treatment beginning at disease progression Observation, with treatment beginning at disease progression
33 Categories of Multiple Myeloma Classification Characteristics Management Indolent MM Symptomatic MM Presence of serum/urine M protein Bone marrow plasmacytosis Mild anemia or few small lytic bone lesions Absence of symptoms Presence of serum/urine M protein Bone marrow plasmacytosis Anemia, renal failure, hypercalcemia, or lytic bone lesions Patients with primary systematic amyloidosis and bone marrow plasma cells 30% are considered to have both MM and amyloidosis Monitoring every 3 mo, with treatment beginning at disease progression Immediate treatment
34 Durie-Salmon Staging System for Myeloma Stage Criteria Myeloma cell mass ( cells/m 2 ) I All of the following: Hemoglobin >10 g/dl Serum calcium level 12 mg/dl (normal) Normal bone or solitary plasmacytoma on x-ray Low M component production rate: IgG <5 g/dl; IgA <3 g/dl Bence Jones protein <4 g/24 hr <0.6 (low) II Not fitting stage I or III (intermediate) III One or more of the following: Hemoglobin <8.5 g/dl Serum calcium level >12 mg/dl Multiple lytic bone lesions on x-ray High M-component production rate: IgG >7 g/dl; IgA >5 g/dl Bence Jones protein >12 g/24 hr >1.2 (high) Subclassification A B Criteria Normal renal function (serum creatinine level <2.0 mg/dl) Abnormal renal function (serum creatinine level 2.0 mg/dl)
35 International Staging System for Myeloma Stage 1 2 M <3.5 and ALB 3.5 ALB <3.5 and Stage 2 2 M <3.5 ALB <3.5 or 2 M 3.5 <5.5 Stage 3 2 M M=serum 2 microglobulin in mg/dl; ALB=serum albumin in g/dl
36 Major Adverse Prognostic Factors Karyotypic deletion 13 or hypodiploidy High plasma cell labeling index Molecular genetics: t(4;14), t(14;16) or 17p- High LDH, 2 M, or CRP Increased circulating plasma cells Plasmablastic morphology Low albumin
37 Del 13: Unfavorable Prognosis 1 Deletion of chromosome 13 is the single most powerful adverse prognostic factor for all times to events in patients referred for high-dose therapy OS 65.1 ± 9.8 vs 26.7 ± 4.1 months
38 Plasma cell labeling index
39 Plasmablastic Morphology

40 Circulating plasma cells
41 Chemotherapy
42 Initial Therapy Considerations Ensure patient does not have smoldering MM (asymptomatic MM) Approach to therapy for MM is based on whether a patient is a transplant candidate Consider clinical trials if available Improving complete response rates is a key goal of current trials
43 IBMTR (EBMT) Criteria for Complete and Partial Response* Complete response requires all of following No serum/urine M protein by IFE for 6 wk <5% plasma cells in bone marrow aspirate No increase in size or number of lytic bone lesions Disappearance of soft tissue plasmacytomas Partial response requires all of following 50% reduction in serum M protein 6 wk 90% reduction in 24-hr urinary light chain excretion 50% reduction in soft tissue plasmacytomas No increase in size or number of lytic bone lesions *
44 Initial Approach to Treatment of MM Clearly not a transplant candidate based on age, performance status and comorbidity Potential transplant candidate Conventional chemotherapy or clinical trial Non-alkylator based induction x 4 cycles *Thal/Dex, Dex, or VAD if immediate response is needed Stem cell harvest
45 Current Multiple Myeloma Treatment Adapted from NCCN Practice Guidelines Diagnosis Survival 3-5 yrs Survival < 6 mos without Rx ~12,000 deaths per yr Relapsed Disease Transient Response Survival 1-3 yrs Relapsed/Refractory Disease Shorter TTP Survival 6-9 mos Initial Therapy Cyclophosphamide Melphalan, Prednisone VAD, Doxil Dexamethasone (Dex) Thalidomide + Dex Bortezomib Lenalidomide Non- Transplant Candidate Transplant Candidate Salvage Therapy: Repeat primary therapy (if relapse > 6 mos) Cyclophosphamide, VAD, Doxil Etoposide, Dex, Cytarabine, Cisplatin Thalidomide/IMiDs (CC-5013: lenalidomide) +/- Dex Bortezomib +/- Dex Other Novel Therapies Stem cell harvest, subsequent auto SCT ( single vs double) +/- maintenance therapy Investigational therapy (e.g. Allo)
46 Primary Treatment Approaches for Myeloma Combination therapy examples MP VBAP VAD VBMCP Thal/Dex DT-PACE ABCM
47 Challenges in Management Currently incurable in most patients Chemotherapy response rates = 50% to 70% Long-term complete responses = rare Median survival with standard therapy = 3 years Stem cell transplant prolongs survival, but not curative Treatment of relapse No standard therapy Existing options inadequate New treatment options needed.
48 NCCN Treatment Guidelines for Myeloma Primary conventional therapy Melphalan/prednisone (MP) Vincristine/doxorubicin/dexamethasone (VAD) Dexamethasone Thalidomide/dexamethasone (Thal/Dex) Liposomal doxorubicin/vincristine/ dexamethasone (DVD)
49 Melphalan/Prednisone Treatment Alkylating agent + corticosteroid dosing Dosing: 0.25 mg/kg/day melphalan for 4 days + 20 mg prednisone tid for 4 days Duration: every 4 to 6 wk 40% remission (at least 75% reduction in serum myeloma protein, 95% reduction in Bence Jones proteinuria and >5% marrow plasma cells)
50 Melphalan/Prednisone Treatment Median duration of remission about 2 years At least 3 courses Median survival 3 years <10% live longer than 10 years No evidence of disease cured Drug resistance is an issue Not recommended for candidates for SCT Full benefit takes several months
51 Combination Chemotherapy vs Melphalan/Prednisone 3814 patients in 18 trials of combination chemotherapy vs melphalan/prednisone No difference overall Melphalan/prednisone superior for good prognosis patients MP inferior for poor prognosis patients patients in 27 trials of combination chemotherapy vs melphalan/prednisone Higher response rates to combination chemotherapy Equivalent mortality and survival 2
52 Estimated percentage still alive Mortality of Combination Chemotherapy vs Melphalan/Prednisone Years Allocated cct (% ± SD) Allocated MP (% ± SD) 23.0% 24.4% 18.0% 19.4% 1.4% SD 1.4 (log-rank 2P >.1; NS) Deaths/person-years: CCT 642/ / / / / /1130 MP 576/ / / / / /839
53 Thalidomide With Melphalan and Prednisone in Elderly Patients With Multiple Myeloma Response MPT Arm, % MP Arm, % CR + ncr 27.7* 5.4 PR (all combined) 75% to 99% M-protein reduction 50% to 74% M-protein reduction Median EFS, mo 25.2* 13.7 P<0.001 P<0.001 Median follow-up, 13.6 months
54 Thromboembolism in MPT-Treated Elderly Patients Reduced With Prophylaxis More DVT with MPT than with MP (P=0.003) DVT prophylaxis: enoxaparin, 0.4 ml/day for 4 months Adverse Event No Prophylaxis (n=61) Incidence, % With Prophylaxis (n=28) DVT Pulmonary thromboembolism Arterial occlusion
55 Toxicities MPT MP Toxicity, % G 1/2 G 3/4 G 1/2 Gr 3/4 Hematologic Constipation Infection Neurologic Thromboembolism 19 4 Deaths comparable Thal decreased in 28%, discontinued in 42%
56 Thalidomide (Thalomid ) Oral immunomodulator Derivative of glutamic acid Immunomodulatory agent with antiangiogenic and apoptotic properties O O H N N O O
57 Thalidomide in Myeloma: Overview Affects multiple pathways, multiple targets Oral administration Listed by NCCN as Primary conventional therapy with dexamethasone Salvage therapy as monotherapy Optimal dosing and drug combinations being studied

58 Thalidomide in Multiple Myeloma: Multiple Pathways, Multiple Targets Immunomodulatory effects Inhibits TNF Inhibits angiogenesis (bfgp, VEGF) Stimulates T cells (CD8+) Inhibits IL-12 Induces apoptosis Alters cytokines Affects stromal cells Cool RM et al. Pharmacotherapy. 2002;22:1019; D Amato RJ et al. Proc Natl Acad Sci USA. 1994;91:4082; Meierhofer C et al. BioDrugs. 2001;15:681; Thalidomide s various effects in myeloma [figure]. Available at: Weber D et al. J Clin Oncol. 2003;21:16; Bartlett JB et al. Nature Reviews/Cancer. 2004;4:314
59 Thalidomide/Lenalidomide Target MM Cells in the BM Microenvironment C. Thalidomide/IMiD MM cells IL-6 A.Thalidomide /IMiD B.Thalidomide /IMiD ICAM-1 TNF IL-1 Bone Marrow Stromal Cells VEGF bfgf Bone Marrow Vessels PBMC IL-2 IFN D. Thalidomide /IMiD CD8+ T Cells NK Cells E. Thalidomide /IMiD
60 Interaction of MM Cells and Their Bone Marrow Microenvironment MM cell Cytokine-mediated signaling Adhesion-mediated signaling VEGF TNF PI3K/AKT MAPK JAK/STAT3 IL-6 VEGF IGF1 SDF-1 MAPK NF-kB NF-kB Adhesion molecules MM cell ICAM1 VCAM1 LFA1 MUC1 VLA4 CRE c-fos SRE homology BMSC Reprinted with permission from Hideshima T, Anderson KC. Nat Rev Cancer. 2002;2:927
61 Signaling Cascades Mediate Growth, Anti-Apoptosis, and Migration in Myeloma IL-6 IGF1 VEGF TNF IL-21 SDF-1 RAF MEK p42/44 MAPK Proliferation MM cells IL-6 IL-21 JAK STAT3 BCL-X L MCL1 Anti-apoptosis (drug resistance) IL-6 IGF1 VEGF TNF SDF-1 PI3K AKT (PKB) Caspase-9 BAD NF- B FKHR Cyclin D KIP1 Cell cycle PKC Migration BMSC Reprinted with permission from Hideshima T, Anderson KC. Nat Rev Cancer. 2002;2:927
62 Apoptotic Signaling Triggered by Conventional and Novel Agents FAS/FASL, TRAIL Thal/IMiDs PS-341 As 2 O 3 Dexamethasone Caspase-8 Caspase-9 IL-6 IGF1 Conventional chemotherapy Ionizing radiation Caspase-3 PARP cleavage Apoptosis Reprinted with permission from Hideshima T, Anderson KC. Nat Rev Cancer. 2002;2:927
63 Lenalidomide (CC-5013; Revlimid ) More potent immunomodulator than thalidomide Up to 50,000 times more potent inhibitor of TNF 200- to 1000-fold in cytokine modulation Increased stimulation of T-cell proliferation Augmented stimulation OF IL-2 and IFN production Fewer side effects: no significant constipation, neuropathy, or sedation Not teratogenic O N O H N O Marriott JB et al.? 2003;3(3):181 Schey SA et al. J Clin Oncol. 2004;22:16? 2 Richardson P, Anderson K. J Clin Oncol. 2004;22:16? NH
64 Structure Thalidomide Lenalidomide
65 Lenalidomide Phase I Trial in Relapsed Myeloma: Adverse Events Lightheadedness Fatigue Grade 1 Grade 2 Grade 3 Grade 4 Rash Leg Cramps Thrombocytopenia Neutropenia Patients (%) (N=25)
66 NCCN Treatment Guidelines for Multiple Myeloma Exposure to myelotoxic agents (including alkylating agents and nitrosoureas) should be limited to avoid compromising stem-cell reserve prior to stem-cell harvest in patients who may be candidates for transplant

67 Transplant Candidates: Most Commonly Used Induction Regimens VAD Cumbersome Toxicity 55-65% RR 85% of effect secondary to Dex Dexamethasone Oral Less toxicity than VAD or Thal/Dex 43% RR Thal/Dex Oral Increased toxicity compared to Dex 64-72% RR Transplant candidates should not receive alkylator-based therapy
68 VAD Combination of vincristine, Adriamycin (doxorubicin) and dexamethasone, cytotoxic antibiotic, and glucocorticoid steroid Dosing Vincristine: 0.4 mg/day IV daily for 4 days Doxorubicin: 9 mg/m 2 /day IV daily for 4 days Dexamethasone: 40 mg po days 1 4, 9 12, Repeat cycle q 28 days 4 cycles Reduction in tumor mass: 75% in 70% pts Remission: 70% pts Median time to response: 0.9 mo Can be used prior to SCT
69 Thalidomide/Dexamethasone vs Dexamethasone: Best Response Within 4 Cycles Endpoint Thal/Dex (n=99) Dex (n=100) Response rate, %* Adjusted response rate, % Median time to response, mo Disease progression within first 4 mo, % 2 4 *Response rate = Based on intention to treat, 50% reduction in serum and urine M protein, or 90% reduction in urine M protein if only urinary protein was evaluable for response; significantly higher response rate with Thal/Dex compared with Dex alone (P=0.002) Corrected response rate = Allowing for use of serum M protein levels in patients in whom measurable urine M protein was unavailable at follow-up Rajkumar SV et al. Blood. 2004;104(part 1):63a [abstract 205]
70 Thalidomide/Dexamethasone vs Dexamethasone: Drug-Related Adverse Events Drug-Related Adverse Event Thal/Dex, % (n=102) Dex, n % (n=102) DVT grade Rash grade Sinus bradycardia grade Neuropathy grade Any toxicity grade Total* Deaths within 4 cycles: Thal/Dex, 7%; Dex, 11% ]
71 Thalidomide/Dexamethasone vs Dexamethasone: Conclusions Superior response rates with Thal/Dex compared with Dex alone in newly diagnosed MM Thal/Dex associated with higher toxicities than Dex Need for DVT prophylaxis with Thal/Dex Higher response rates of Thal/Dex must be weighed against increased toxicity for individual patients
72 Lenalidomide (CC-5013) and Dexamethasone for Newly Diagnosed Myeloma: Adverse Events Profile Hematologic toxicity, % Grade 1/2 Grade 3/4 Anemia 3 7 Neutropenia 17 3 Lymphopenia 17 3 Non-hematologic toxicity, % Grade 1/2 Grade 3 DVT (all received prophylaxis) 0 0 Constipation 7 0 Sedation 30 7 Rash 3 3 Neuropathy 17 0 Anxiety 7 7 Rajkumar SV et al. Blood. 2004;104(part 1):98a [abstract 331]
73 Bortezomib (PS 341; Velcade ) Mechanism of action Reversible inhibitor of chymotrypsin-like activity of 26S proteasome Inhibition of proteosome prevents proteolysis of ubiquitinated proteins This disrupts homeostasis and can lead to apoptosis
74 Ubiquitin-Proteasome Pathway O Ub OH ATP AMP PP i O NH 2 E2-S E1-SH O Ub E3 E1-S Ub E2-SH HN O Ub n ATP Ub Degraded proteins Lys Protein Substrate isopeptidases Lys 26S Proteasome Complex
75
76 Bortezomib: Mechanism of Action in MM A. PS-341 MM Cell Growth C. PS-341 IL-6 TNF VEGF B. PS-341 ICAM-1 VCAM-1 VEGF bfgf D. PS-341 Bone Marrow Vessels Bone Marrow Stromal Cells
77 Mechanisms of Bortezomib in Treatment of MM Cell adhesion chemosensitizing synergism Modified from NEJM 2004:351:1860
78 Bortezomib: Most Common Adverse Events pts Nausea Diarrhea Constipation Vomiting Anorexia Thrombocytopenia Anemia Neutropenia Fatigue Per. Neuropathy Fever Arthralgia Headache Insomnia Grade 1-2 Grade 3 Grade Richardson, ASH 2002 #385; Richardson NEJM 2003;348:

79 Mean Platelet Count During Treatment
80
81 Autologous stem cell transplant
82 Autologous Stem Cell Transplantation Mel 200/m 2 standard conditioning regimen Sufficient performance status, and adequate liver, pulmonary, cardiac function needed Higher PR and CR rates than conventional chemotherapy Higher overall and event-free survival than conventional Rx Advanced age and impaired renal function are by themselves not contraindications.
83 Transplant versus Conventional Chemotherapy 54 42
84 Total Therapy 1*: Long-term F/U Survival (N = 231) CR Duration (N = 64) 100% 100% 80% 60% Median OS 7 yr 80% 60% Median 3 yr 40% 40% 20% Median EFS 3 yr 0% Years after Registration 20% 0% Years after Onset of CR *Tandem transplant followed by interferon maintenance therapy
85 Single vs Double Autologous Transplantation CR (%) EFS (median, mos) OS (median, mos) Fermand et al Single 37 No difference No difference Double 42 Attal et al Single Double MAG 95 Single 37 No difference No difference* Double 42 Bologna 96 Single No difference* Double Hovon Single Double * Overall survival was improved for pts not achieving CR or near CR with first Auto Fermand JP et al. Blood 2001; 98: 815a Attal M, et al. NEJM 2003; 349: 2495 Fermand JP Mult Myeloma 2004, Torino Italy Cavo M. Mult Myeloma 2004, Torino Italy Sonneveld. Mult Myeloma 2004, Torino Italy Sonneveld P et al. ASH 2004, abst 948
86 Single Versus Tandem Auto SCT: IFM 94 trial 399 pts Single SCT (M 140 mg/m 2 ; 8Gy) vs Tandem SCT (M 140 mg/m 2; ) then (M 140 mg/m 2 ; 8Gy) CR/VGPR 42% 50% p= yr prob EFS 10% 20% p= yr prob OS* 21% 42% p=0.001 *Survival benefit with tandem SCT restricted to patients failing to achieve CR or VGPR with first SCT
87 Attal N Engl J Med 2003; 349:2495 IFM 94 trial
88 Maintenance Therapy
89 Regimens for Maintenance Therapy Interferon alfa (IFN-α) Prednisolone Thalidomide
90 Outcomes with Maintenance Trend for higher OS p of 0.3 (NS) Higher PFS p of Dex did raise the risk of infections, hyperglycemia, and neuropsychiatric complications OS (yrs) Obs Dex PFS (yrs)
MULTIPLE MYELOMA Review & Update for Primary Care. Dr. Joseph Mignone 21st Century Oncology
 MULTIPLE MYELOMA Review & Update for Primary Care Dr. Joseph Mignone 21st Century Oncology OVERVIEW Identify the diagnostic criteria for multiple myeloma Compare first & second line therapies, using data
MULTIPLE MYELOMA Review & Update for Primary Care Dr. Joseph Mignone 21st Century Oncology OVERVIEW Identify the diagnostic criteria for multiple myeloma Compare first & second line therapies, using data
Multiple Myeloma Workshop- Tandem 2014
 Multiple Myeloma Workshop- Tandem 2014 1) Review of Plasma Cell Disorders Asymptomatic (smoldering) myeloma M-protein in serum at myeloma levels (>3g/dL); and/or 10% or more clonal plasma cells in bone
Multiple Myeloma Workshop- Tandem 2014 1) Review of Plasma Cell Disorders Asymptomatic (smoldering) myeloma M-protein in serum at myeloma levels (>3g/dL); and/or 10% or more clonal plasma cells in bone
Current Multiple Myeloma Treatment Adapted From the NCCN Guidelines
 Current Multiple Myeloma Treatment Adapted From the NCCN Guidelines Diagnosis Survival 3-5 yrs Survival
Current Multiple Myeloma Treatment Adapted From the NCCN Guidelines Diagnosis Survival 3-5 yrs Survival
Multiple Myeloma Making Sense of the Report Forms. Parameswaran Hari Medical College of Wisconsin Milwaukee
 Hodgkin CML MDS/Other Leuk CLL Neuroblastoma Multiple Myeloma Making Sense of the Report Forms Parameswaran Hari Medical College of Wisconsin Milwaukee Indications for Blood and Marrow Transplantation
Hodgkin CML MDS/Other Leuk CLL Neuroblastoma Multiple Myeloma Making Sense of the Report Forms Parameswaran Hari Medical College of Wisconsin Milwaukee Indications for Blood and Marrow Transplantation
FastTest. You ve read the book... ... now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. Please refer back to relevant sections
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. Please refer back to relevant sections
UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and
 UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and Blood Disorders La Crosse, WI UNDERSTANDING MULTIPLE
UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and Blood Disorders La Crosse, WI UNDERSTANDING MULTIPLE
Multiple Myeloma: Novel Agents. Robert A. Kyle, M.D. Germany June 28, 2008. Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
 Multiple Myeloma: Novel Agents Robert A. Kyle, M.D. Germany June 28, 2008 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Multiple Myeloma Untreated Initial Therapy Transplant eligible Multiple
Multiple Myeloma: Novel Agents Robert A. Kyle, M.D. Germany June 28, 2008 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Multiple Myeloma Untreated Initial Therapy Transplant eligible Multiple
Multiple Myeloma Patient s Booklet
 1E Kent Ridge Road NUHS Tower Block, Level 7 Singapore 119228 Email : ncis@nuhs.edu.sg Website : www.ncis.com.sg LIKE US ON FACEBOOK www.facebook.com/ nationaluniversitycancerinstitutesingapore Multiple
1E Kent Ridge Road NUHS Tower Block, Level 7 Singapore 119228 Email : ncis@nuhs.edu.sg Website : www.ncis.com.sg LIKE US ON FACEBOOK www.facebook.com/ nationaluniversitycancerinstitutesingapore Multiple
MULTIPLE MYELOMA. Dr Malkit S Riyat. MBChB, FRCPath(UK) Consultant Haematologist
 Consultant Haematologist") MULTIPLE MYELOMA Dr Malkit S Riyat MBChB, FRCPath(UK) Consultant Haematologist Multiple myeloma is an incurable malignancy that arises from postgerminal centre, somatically hypermutated B cells.
MULTIPLE MYELOMA Dr Malkit S Riyat MBChB, FRCPath(UK) Consultant Haematologist Multiple myeloma is an incurable malignancy that arises from postgerminal centre, somatically hypermutated B cells.
Treatment results with Bortezomib in multiple myeloma
 Treatment results with Bortezomib in multiple myeloma Prof. Dr. Orhan Sezer Hamburg University Medical Center Circulating proteasome levels are an independent prognostic factor in MM 1.0 Probability of
Treatment results with Bortezomib in multiple myeloma Prof. Dr. Orhan Sezer Hamburg University Medical Center Circulating proteasome levels are an independent prognostic factor in MM 1.0 Probability of
A Clinical Primer. for Managed Care Stakeholders
 reviews therapy Diagnosing, Staging, and Treating Multiple Myeloma: A Clinical Primer for Managed Care Stakeholders by Ralph V. Boccia, MD, FACP, Medical Director, Center for Cancer and Blood Disorders
reviews therapy Diagnosing, Staging, and Treating Multiple Myeloma: A Clinical Primer for Managed Care Stakeholders by Ralph V. Boccia, MD, FACP, Medical Director, Center for Cancer and Blood Disorders
Outline. Question 1. Question 2. What is Multiple Myeloma? Andrew Eisenberger, MD
 Outline A Disease Overview June 3, 2013 Andrew Eisenberger, MD Assistant Professor of Medicine Hematology/Oncology Columbia Presbyterian Medical Center Introduction Epidemiology/Risk Factors Clinical Features/Diagnostic
Outline A Disease Overview June 3, 2013 Andrew Eisenberger, MD Assistant Professor of Medicine Hematology/Oncology Columbia Presbyterian Medical Center Introduction Epidemiology/Risk Factors Clinical Features/Diagnostic
 MULTIPLE MYELOMA 1 PLASMA CELL DISORDERS Multiple l Myeloma Monoclonal Gammopathy of Undetermined Significance (MGUS) Smoldering Multiple Myeloma (SMM) Solitary Plasmacytoma Waldenstrom s Macroglobulinemia
MULTIPLE MYELOMA 1 PLASMA CELL DISORDERS Multiple l Myeloma Monoclonal Gammopathy of Undetermined Significance (MGUS) Smoldering Multiple Myeloma (SMM) Solitary Plasmacytoma Waldenstrom s Macroglobulinemia
chronic leukemia lymphoma myeloma differentiated 14 September 1999 Pre- Transformed Ig Surface Surface Secreted Myeloma Major malignant counterpart
 Disease Usual phenotype acute leukemia precursor chronic leukemia lymphoma myeloma differentiated Pre- B-cell B-cell Transformed B-cell Plasma cell Ig Surface Surface Secreted Major malignant counterpart
Disease Usual phenotype acute leukemia precursor chronic leukemia lymphoma myeloma differentiated Pre- B-cell B-cell Transformed B-cell Plasma cell Ig Surface Surface Secreted Major malignant counterpart
Multiple Myeloma and Amyloidosis: Optimism for Heretofore Incurable Diseases
 Multiple Myeloma and Amyloidosis: Optimism for Heretofore Incurable Diseases Robert Vescio, MD Director Multiple Myeloma & Bone Metastases Program Samuel Oschin Comprehensive Cancer Center Cedars-Sinai
Multiple Myeloma and Amyloidosis: Optimism for Heretofore Incurable Diseases Robert Vescio, MD Director Multiple Myeloma & Bone Metastases Program Samuel Oschin Comprehensive Cancer Center Cedars-Sinai
TABLE OF CONTENTS. Multiple Myeloma / Plasma Cell Leukemia Pre-HSCT Data
 Instructions for Multiple Myeloma / Plasma Cell Leukemia Pre-HSCT Data (Form 2016) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Multiple Myeloma /
Instructions for Multiple Myeloma / Plasma Cell Leukemia Pre-HSCT Data (Form 2016) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Multiple Myeloma /
SOUTHWEST ONCOLOGY GROUP CLINICAL RESEARCH ASSOCIATE (CRA) MANUAL. MYELOMA CHAPTER 10 REVISED: March 2008
 MANUAL. MYELOMA CHAPTER 10 REVISED: March 2008") Introduction This disease site includes the following three malignancies: multiple myeloma, amyloidosis, and waldenstrom's macroglobulinemia. See pages 4 and 5 for descriptions of the latter two diseases.
Introduction This disease site includes the following three malignancies: multiple myeloma, amyloidosis, and waldenstrom's macroglobulinemia. See pages 4 and 5 for descriptions of the latter two diseases.
Treating myeloma. Dr Rachel Hall Royal Bournemouth Hospital
 Treating myeloma Dr Rachel Hall Royal Bournemouth Hospital Treatment overview When to treat? Aim of treatment Which treatment? Monitoring response to treatment Prevention of complications What happens
Treating myeloma Dr Rachel Hall Royal Bournemouth Hospital Treatment overview When to treat? Aim of treatment Which treatment? Monitoring response to treatment Prevention of complications What happens
Whole Antibody and Free Light Chain Production by Plasma Cells
 MYELOMA Very Good ; Stringent or Complete Navigating the maze of Responses Parameswaran Hari Medical College of Wisconsin Milwaukee Increasing understanding of disease biology in the last few years Deeper
MYELOMA Very Good ; Stringent or Complete Navigating the maze of Responses Parameswaran Hari Medical College of Wisconsin Milwaukee Increasing understanding of disease biology in the last few years Deeper
STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA
 STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA Sundar Jagannath MD Professor of Medicine St. Vincent s Comprehensive Cancer Center New York, NY Where is transplant today in the management of Myeloma? Autologous
STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA Sundar Jagannath MD Professor of Medicine St. Vincent s Comprehensive Cancer Center New York, NY Where is transplant today in the management of Myeloma? Autologous
Cure versus control: Which is the best strategy?
 Cure versus control: Which is the best strategy? Barcelona 8-9-2012 Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY MULTIPLE MYELOMA Cure versus control
Cure versus control: Which is the best strategy? Barcelona 8-9-2012 Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY MULTIPLE MYELOMA Cure versus control
Multiple. Powerful thinking advances the cure
 Multiple Myeloma Treatment OVERVIEW Powerful thinking advances the cure Powerful thinking advances the cure About the Multiple Myeloma Research Foundation The Multiple Myeloma Research Foundation (MMRF)
Multiple Myeloma Treatment OVERVIEW Powerful thinking advances the cure Powerful thinking advances the cure About the Multiple Myeloma Research Foundation The Multiple Myeloma Research Foundation (MMRF)
Background Information Myeloma
 Myeloma FAST FACTS Myeloma, also known as multiple myeloma, is a type of cancer that develops from plasma cells which originate in the bone marrow 1 Myeloma is the second most common type of blood cancer
Myeloma FAST FACTS Myeloma, also known as multiple myeloma, is a type of cancer that develops from plasma cells which originate in the bone marrow 1 Myeloma is the second most common type of blood cancer
MULTIPLE MYELOMA Treatment Overview
 MULTIPLE MYELOMA Treatment Overview ABOUT THE MULTIPLE MYELOMA RESEARCH FOUNDATION After being diagnosed with multiple myeloma in 1998, Kathy Giusti and her sister Karen Andrews, a successful corporate
MULTIPLE MYELOMA Treatment Overview ABOUT THE MULTIPLE MYELOMA RESEARCH FOUNDATION After being diagnosed with multiple myeloma in 1998, Kathy Giusti and her sister Karen Andrews, a successful corporate
Things You Don t Want to Miss in Multiple Myeloma
 Things You Don t Want to Miss in Multiple Myeloma Sreenivasa Chandana, MD, PhD Attending Hematologist and Medical Oncologist West Michigan Cancer Center Assistant Professor, Western Michigan University
Things You Don t Want to Miss in Multiple Myeloma Sreenivasa Chandana, MD, PhD Attending Hematologist and Medical Oncologist West Michigan Cancer Center Assistant Professor, Western Michigan University
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: PS Inj - Velcade Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antineoplastic Client: PS Inj Approval Date: 10/2/2004 Revision Date: 5/22/2007
Prior Authorization Guideline Guideline: PS Inj - Velcade Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antineoplastic Client: PS Inj Approval Date: 10/2/2004 Revision Date: 5/22/2007
Multiple. Powerful thinking advances the cure
 Multiple Myeloma DISEASE OVERVIEW Powerful thinking advances the cure Powerful thinking advances the cure About the Multiple Myeloma Research Foundation The Multiple Myeloma Research Foundation (MMRF)
Multiple Myeloma DISEASE OVERVIEW Powerful thinking advances the cure Powerful thinking advances the cure About the Multiple Myeloma Research Foundation The Multiple Myeloma Research Foundation (MMRF)
Table of Contents Accelerate Your Research Introduction I. From the Real World to the Lab II. Research Challenges III. How Can Conversant Bio Help?
 Table of Contents Accelerate Your Research 2 Introduction 3 I. From the Real World to the Lab 4 A. Diagnosing Multiple Myeloma 4 1. Lab Tests 4 2. Bone Marrow Exams 6 3. Imaging Studies 7 B. Subtypes of
Table of Contents Accelerate Your Research 2 Introduction 3 I. From the Real World to the Lab 4 A. Diagnosing Multiple Myeloma 4 1. Lab Tests 4 2. Bone Marrow Exams 6 3. Imaging Studies 7 B. Subtypes of
Multiple Myeloma. The term multiple myeloma is considered to be synonymous with myeloma, plasma cell myeloma, active and symptomatic myeloma.
 Multiple Myeloma. The term multiple myeloma is considered to be synonymous with myeloma, plasma cell myeloma, active and symptomatic myeloma. The intent is to positively identify patients with active or
Multiple Myeloma. The term multiple myeloma is considered to be synonymous with myeloma, plasma cell myeloma, active and symptomatic myeloma. The intent is to positively identify patients with active or
I've Just Been Diagnosed. with Multiple Myeloma, What s Next?
 I've Just Been Diagnosed with Multiple Myeloma, What s Next? Table of Contents Message from a Survivor Introduction What is Multiple Myeloma? What Causes Multiple Myeloma? Genes & Multiple Myeloma What
I've Just Been Diagnosed with Multiple Myeloma, What s Next? Table of Contents Message from a Survivor Introduction What is Multiple Myeloma? What Causes Multiple Myeloma? Genes & Multiple Myeloma What
Multiple Myeloma. Solving a growing puzzle
 Multiple Myeloma Solving a growing puzzle Disclosures Financial I wish. I eat too much. I did ask who the audience would be. Nurses and Doctors Goals 1. Understand the incidence, symptoms, and pathophysiology
Multiple Myeloma Solving a growing puzzle Disclosures Financial I wish. I eat too much. I did ask who the audience would be. Nurses and Doctors Goals 1. Understand the incidence, symptoms, and pathophysiology
Multiple Myeloma in HUSM. Dr Azlan Husin HUSM
 Multiple Myeloma in HUSM Dr Azlan Husin HUSM Outline Overview Presenting features Progress in myeloma Global HUSM Multiple myeloma is a neoplastic plasma-cell disorder that is characterized by clonal proliferation
Multiple Myeloma in HUSM Dr Azlan Husin HUSM Outline Overview Presenting features Progress in myeloma Global HUSM Multiple myeloma is a neoplastic plasma-cell disorder that is characterized by clonal proliferation
Future strategies for myeloma: An overview of novel treatments In development
 Future strategies for myeloma: An overview of novel treatments In development Dr. Matthew Streetly Guys and St. Thomas NHS Trust How far have we come? Melphalan and prednisolone VAD Autologous SCT Thalidomide
Future strategies for myeloma: An overview of novel treatments In development Dr. Matthew Streetly Guys and St. Thomas NHS Trust How far have we come? Melphalan and prednisolone VAD Autologous SCT Thalidomide
NATIONAL CANCER INSTITUTE. Lenalidomide or Observation in Treating Patients With Asymptomatic High-Risk Smoldering Multiple Myeloma
 NATIONAL CANCER INSTITUTE Lenalidomide or Observation in Treating Patients With Asymptomatic High-Risk Smoldering Multiple Myeloma Basic Trial Information Phase Type Status Age Sponsor Protocol IDs Phase
NATIONAL CANCER INSTITUTE Lenalidomide or Observation in Treating Patients With Asymptomatic High-Risk Smoldering Multiple Myeloma Basic Trial Information Phase Type Status Age Sponsor Protocol IDs Phase
Stem Cell Transplantation
 Harmony Behavioral Health, Inc. Harmony Behavioral Health of Florida, Inc. Harmony Health Plan of Illinois, Inc. HealthEase of Florida, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance
Harmony Behavioral Health, Inc. Harmony Behavioral Health of Florida, Inc. Harmony Health Plan of Illinois, Inc. HealthEase of Florida, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance
A Science Writer s Guide to Multiple Myeloma
 A Science Writer s Guide to Multiple Myeloma 1 A Science Writer s Guide to Multiple Myeloma A Science Writer s Guide to Multiple Myeloma PREFACE Blood cancers and related disorders a serious health risk
A Science Writer s Guide to Multiple Myeloma 1 A Science Writer s Guide to Multiple Myeloma A Science Writer s Guide to Multiple Myeloma PREFACE Blood cancers and related disorders a serious health risk
Shaji Kumar, M.D. Multiple Myeloma: Multiple myeloma (MM) is the second most common hematological
 is the second most common hematological") An update on the management of multiple myeloma and amyloidosis Shaji Kumar, M.D. Multiple Myeloma: Multiple myeloma (MM) is the second most common hematological malignancy in this country affecting nearly
An update on the management of multiple myeloma and amyloidosis Shaji Kumar, M.D. Multiple Myeloma: Multiple myeloma (MM) is the second most common hematological malignancy in this country affecting nearly
Plasma cell dyscrasias Mark Drayson
 Plasma cell dyscrasias Mark Drayson Mortality statistics for England and Wales. Deaths attributed to multiple myeloma from 1988-1997 by age cohort as a percentage of total (21,257) deaths Deaths in age
Plasma cell dyscrasias Mark Drayson Mortality statistics for England and Wales. Deaths attributed to multiple myeloma from 1988-1997 by age cohort as a percentage of total (21,257) deaths Deaths in age
Multiple Myeloma Patient Handbook. www.myeloma.ca
 Multiple Myeloma Patient Handbook www.myeloma.ca Introduction This resource has been designed for: 1. Someone who has been newly diagnosed with myeloma and is wondering what it means and what the future
Multiple Myeloma Patient Handbook www.myeloma.ca Introduction This resource has been designed for: 1. Someone who has been newly diagnosed with myeloma and is wondering what it means and what the future
Waldenström Macroglobulinemia: The Burning Questions. IWMF Ed Forum May 18 2014 Morie Gertz MD, MACP
 Waldenström Macroglobulinemia: The Burning Questions IWMF Ed Forum May 18 2014 Morie Gertz MD, MACP Are my kids going to get this? Familial seen in approximately 5 10% of all CLL patients and can be associated
Waldenström Macroglobulinemia: The Burning Questions IWMF Ed Forum May 18 2014 Morie Gertz MD, MACP Are my kids going to get this? Familial seen in approximately 5 10% of all CLL patients and can be associated
MULTIPLE MYELOMA. Overview
 MULTIPLE MYELOMA Overview Steven R. Schuster, M.D. May 7, 2015 Objectives Give an overview of Multiple Myeloma Everything I know in 15 minutes Explain how genetic information can be used to personalize
MULTIPLE MYELOMA Overview Steven R. Schuster, M.D. May 7, 2015 Objectives Give an overview of Multiple Myeloma Everything I know in 15 minutes Explain how genetic information can be used to personalize
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bortezomib (Velcade) for Multiple Myeloma March 25, 2013
 for Multiple Myeloma March 25, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Bortezomib (Velcade) for Multiple Myeloma March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bortezomib (Velcade) for Multiple Myeloma March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
Intérêt t clinique de l'identification des
 Intérêt t clinique de l'identification des chaînes légères l libres Jean-Fran François Lambert Hematologie - CHUV Healthy 69 yo female Negative past medical history 2/07 acute pulmonary edema Progressive
Intérêt t clinique de l'identification des chaînes légères l libres Jean-Fran François Lambert Hematologie - CHUV Healthy 69 yo female Negative past medical history 2/07 acute pulmonary edema Progressive
Myeloma. Ann Grace, myeloma survivor. This publication was supported in part by a grant from
 Myeloma Ann Grace, myeloma survivor This publication was supported in part by a grant from Revised 2013 A Message From John Walter President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma
Myeloma Ann Grace, myeloma survivor This publication was supported in part by a grant from Revised 2013 A Message From John Walter President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma
Monoclonal Gammopathy of Undetermined Significance (MGUS) Facts
 Facts") Monoclonal Gammopathy of Undetermined Significance (MGUS) Facts Normal plasma cells (a type of white blood cell) produce antibodies (also known as immunoglobulins) which help fight infection. Each type
Monoclonal Gammopathy of Undetermined Significance (MGUS) Facts Normal plasma cells (a type of white blood cell) produce antibodies (also known as immunoglobulins) which help fight infection. Each type
Long-term Results of Response to Therapy, Time to Progression, and Survival With Lenalidomide Plus Dexamethasone in Newly Diagnosed Myeloma
 ORIGINAL ARTICLE LONG-TERM RESULTS OF REV-DEX THERAPY FOR NEWLY DIAGNOSED MYELOMA Long-term Results of Response to Therapy, Time to Progression, and Survival With Lenalidomide Plus Dexamethasone in Newly
ORIGINAL ARTICLE LONG-TERM RESULTS OF REV-DEX THERAPY FOR NEWLY DIAGNOSED MYELOMA Long-term Results of Response to Therapy, Time to Progression, and Survival With Lenalidomide Plus Dexamethasone in Newly
REVLIMID and IMNOVID for Multiple Myeloma
 REVLIMID and IMNOVID for Multiple Myeloma What is Multiple Myeloma? Multiple myeloma (MM) is a persistent and life-threatening blood cancer that is characterised by tumour proliferation and immune suppression.
REVLIMID and IMNOVID for Multiple Myeloma What is Multiple Myeloma? Multiple myeloma (MM) is a persistent and life-threatening blood cancer that is characterised by tumour proliferation and immune suppression.
Multiple Myeloma Something Old, Something New, Something Borrowed
 Multiple Myeloma Something Old, Something New, Something Borrowed UCT Nicolas Novitzky Dip Med, PhD, FCP(SA) Haematology Clinical & Laboratory Science, Department of Medicine University of Cape Town 1.
Multiple Myeloma Something Old, Something New, Something Borrowed UCT Nicolas Novitzky Dip Med, PhD, FCP(SA) Haematology Clinical & Laboratory Science, Department of Medicine University of Cape Town 1.
Bendamustine for the fourth-line treatment of multiple myeloma
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for the fourth-line treatment of multiple myeloma Contents Summary 1 Background 2 Epidemiology 3 Cost 6 References 7 Summary There is no standard
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for the fourth-line treatment of multiple myeloma Contents Summary 1 Background 2 Epidemiology 3 Cost 6 References 7 Summary There is no standard
A Focus on Multiple Myeloma
 A Focus on Multiple Myeloma Guest Expert: Madhav Dhodapkar, MD Professor of Hematology, Yale Cancer Center www.wnpr.org www.yalecancercenter.org Welcome to Yale Cancer Center Answers with Dr. Ed and Dr.
A Focus on Multiple Myeloma Guest Expert: Madhav Dhodapkar, MD Professor of Hematology, Yale Cancer Center www.wnpr.org www.yalecancercenter.org Welcome to Yale Cancer Center Answers with Dr. Ed and Dr.
The Blood Cancer Twice As Likely To Affect African Americans: Multiple Myeloma
 The Blood Cancer Twice As Likely To Affect African Americans: Multiple Myeloma 11 th Annual National Leadership Summit on Health Disparities Innovation Towards Reducing Disparities Congressional Black
The Blood Cancer Twice As Likely To Affect African Americans: Multiple Myeloma 11 th Annual National Leadership Summit on Health Disparities Innovation Towards Reducing Disparities Congressional Black
Multiple Myeloma How to Evaluate Response To Treatment and Relapse
 Multiple Myeloma How to Evaluate Response To Treatment and Relapse D R L. G AR D E R E T Saint Antoine Hospital, Paris Haematology Department 1 What is Multiple Myeloma? 4 Diagnostic Tools 8 Response to
Multiple Myeloma How to Evaluate Response To Treatment and Relapse D R L. G AR D E R E T Saint Antoine Hospital, Paris Haematology Department 1 What is Multiple Myeloma? 4 Diagnostic Tools 8 Response to
Chapter 8. Summary, general discussion and future perspectives
 Summary, general discussion and future perspectives 115 Summary Multiple Myeloma (MM) is characterized by a malignant proliferation of monoclonal plasma cells in the bone marrow, clinical presenting by
Summary, general discussion and future perspectives 115 Summary Multiple Myeloma (MM) is characterized by a malignant proliferation of monoclonal plasma cells in the bone marrow, clinical presenting by
Multiple Myeloma (Event Driven)
") Brochure More information from http://www.researchandmarkets.com/reports/2234830/ Multiple Myeloma (Event Driven) Description: The 2010 multiple myeloma (myeloma) market garnered impressive sales despite
Brochure More information from http://www.researchandmarkets.com/reports/2234830/ Multiple Myeloma (Event Driven) Description: The 2010 multiple myeloma (myeloma) market garnered impressive sales despite
Use of free light chain analysis in the diagnosis, prognosis and therapy of multiple myeloma. Amitabha Mazumder, MD
 Use of free light chain analysis in the diagnosis, prognosis and therapy of multiple myeloma Amitabha Mazumder, MD Monoclonal Gammopathies Multiple Myeloma 18% Light Chain Dep Ds < 1% AL Amyloidosis 9%
Use of free light chain analysis in the diagnosis, prognosis and therapy of multiple myeloma Amitabha Mazumder, MD Monoclonal Gammopathies Multiple Myeloma 18% Light Chain Dep Ds < 1% AL Amyloidosis 9%
PATIENT HANDBOOK. Multiple Myeloma. Improving Lives Finding the Cure. Cancer of the Bone Marrow. Prepared by Brian G.M. Durie, M.D.
 PATIENT HANDBOOK A Publication of the International Myeloma Foundation Dedicated to improving the quality of life of myeloma patients while working toward prevention and a cure. Prepared by Brian G.M.
PATIENT HANDBOOK A Publication of the International Myeloma Foundation Dedicated to improving the quality of life of myeloma patients while working toward prevention and a cure. Prepared by Brian G.M.
Multiple Myeloma Therapy Doublet, Triplet, and beyond October 2013 The IV. International Eurasian Congress of Hematology Rafat Abonour, M.D.
 Multiple Myeloma Therapy Doublet, Triplet, and beyond October 2013 The IV. International Eurasian Congress of Hematology Rafat Abonour, M.D. Multiple Myeloma Facts Second most prevalent hematologic neoplasm,
Multiple Myeloma Therapy Doublet, Triplet, and beyond October 2013 The IV. International Eurasian Congress of Hematology Rafat Abonour, M.D. Multiple Myeloma Facts Second most prevalent hematologic neoplasm,
Special Article. Introduction. Aims. Description of the method used to gather evidence. Background
 Special Article Guidelines on the diagnosis and management of multiple myeloma treatment: Associação Brasileira de Hematologia e Hemoterapia e Terapia Celular Vânia Tietsche de Moraes Hungria 1 Edvan de
Special Article Guidelines on the diagnosis and management of multiple myeloma treatment: Associação Brasileira de Hematologia e Hemoterapia e Terapia Celular Vânia Tietsche de Moraes Hungria 1 Edvan de
Multiple Myeloma. What is cancer?
 What is cancer? Multiple Myeloma The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early years of a person's life,
What is cancer? Multiple Myeloma The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early years of a person's life,
MULTIPLE MYELOMA. Version Date: February, 2015
 MULTIPLE MYELOMA Version Date: February, 2015 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted approaches
MULTIPLE MYELOMA Version Date: February, 2015 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted approaches
Myeloma. A guide for patients and families. 1800 620 420 leukaemia.org.au
 Myeloma A guide for patients and families 1800 620 420 leukaemia.org.au Notes Contents Acknowledgments 4 Introduction 5 The Leukaemia Foundation 6 Blood cancers 10 What is myeloma? 16 Who gets myeloma?
Myeloma A guide for patients and families 1800 620 420 leukaemia.org.au Notes Contents Acknowledgments 4 Introduction 5 The Leukaemia Foundation 6 Blood cancers 10 What is myeloma? 16 Who gets myeloma?
Plasma Cell Disorders
 Plasma Cell Disorders 2015 Subtypes of Plasma Cell Disorders Increased Plasma Cells Monoclonal Gammopathy Myeloma Macroglobulinemia (IgM) Increased / Altered Products of Plasma Cells Light Chain Amyloidosis
Plasma Cell Disorders 2015 Subtypes of Plasma Cell Disorders Increased Plasma Cells Monoclonal Gammopathy Myeloma Macroglobulinemia (IgM) Increased / Altered Products of Plasma Cells Light Chain Amyloidosis
Multiple Myeloma and Other Plasma Cell
 CANCER MANAGEMENT: 13TH EDITION Multiple Myeloma and Other Plasma Cell Dyscrasias By Sundar Jagannath, MD 1, Paul Richardson, MD 2, Nikhil C. Munshi, MD 3 2011t325å 1 Multiple Myeloma Program, The Mount
CANCER MANAGEMENT: 13TH EDITION Multiple Myeloma and Other Plasma Cell Dyscrasias By Sundar Jagannath, MD 1, Paul Richardson, MD 2, Nikhil C. Munshi, MD 3 2011t325å 1 Multiple Myeloma Program, The Mount
Malignant Lymphomas and Plasma Cell Myeloma
 Malignant Lymphomas and Plasma Cell Myeloma Dr. Bruce F. Burns Dept. of Pathology and Lab Medicine Overview definitions - lymphoma lymphoproliferative disorder plasma cell myeloma pathogenesis - translocations
Malignant Lymphomas and Plasma Cell Myeloma Dr. Bruce F. Burns Dept. of Pathology and Lab Medicine Overview definitions - lymphoma lymphoproliferative disorder plasma cell myeloma pathogenesis - translocations
Patient Handbook. Multiple Myeloma. International Myeloma Foundation. Until There is a Cure... There is the IMF. Cancer of the Bone Marrow
 Until There is a Cure... There is the IMF. Patient Handbook Published by the International Myeloma Foundation (IMF) International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, CA
Until There is a Cure... There is the IMF. Patient Handbook Published by the International Myeloma Foundation (IMF) International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, CA
Myeloma. Anne Grace, myeloma survivor. Support for this publication provided by
 Myeloma Anne Grace, myeloma survivor Support for this publication provided by Revised 2015 Publication Update Myeloma The Leukemia & Lymphoma Society wants you to have the most up-to-date information about
Myeloma Anne Grace, myeloma survivor Support for this publication provided by Revised 2015 Publication Update Myeloma The Leukemia & Lymphoma Society wants you to have the most up-to-date information about
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)
 in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)") Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
Understanding Revlimid
 Understanding Revlimid International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, CA 91607 USA Telephone: 800-452-CURE (2873) (USA & Canada) 818-487-7455 Fax: 818-487-7454 TheIMF@myeloma.org
Understanding Revlimid International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, CA 91607 USA Telephone: 800-452-CURE (2873) (USA & Canada) 818-487-7455 Fax: 818-487-7454 TheIMF@myeloma.org
Pro Cure in Multiple Myeloma. Nicolaus Kröger Dept. of Stem Cell Transplantation University Hospital Hamburg Hamburg, Germany
 Pro Cure in Multiple Myeloma Nicolaus Kröger Dept. of Stem Cell Transplantation University Hospital Hamburg Hamburg, Germany Pro Cure in Multiple Myeloma Several hematological malignancies can be cured
Pro Cure in Multiple Myeloma Nicolaus Kröger Dept. of Stem Cell Transplantation University Hospital Hamburg Hamburg, Germany Pro Cure in Multiple Myeloma Several hematological malignancies can be cured
Glossary of Multiple Myeloma Terms
 Some things that make multiple myeloma (MM) difficult to understand are the unfamiliar medical terms that some experts and healthcare providers use to explain it. You may come across words like these when
Some things that make multiple myeloma (MM) difficult to understand are the unfamiliar medical terms that some experts and healthcare providers use to explain it. You may come across words like these when
Chapter 2. S. Hovenga 1, J.Th.M. de Wolf 1, J.E.J. Guikema 4, H. Klip 2, J.W. Smit 3, C.Th. Smit Sibinga 5, N.A. Bos 4, E.
 Chapter 2 Autologous stem cell transplantation in multiple myeloma after VAD and EDAP courses; a high incidence of oligoclonal serum immunoglobulins post transplantation S. Hovenga, J.Th.M. de Wolf, J.E.J.
Chapter 2 Autologous stem cell transplantation in multiple myeloma after VAD and EDAP courses; a high incidence of oligoclonal serum immunoglobulins post transplantation S. Hovenga, J.Th.M. de Wolf, J.E.J.
Asymptomatic or smoldering myeloma with no symptoms and slow growing cancer cells
 ESSENTIALS Multiple Myeloma Diagnosed with Multiple Myeloma? It s important to understand everything you can about your diagnosis, possible treatments, and places to go for support and care. Cancer is
ESSENTIALS Multiple Myeloma Diagnosed with Multiple Myeloma? It s important to understand everything you can about your diagnosis, possible treatments, and places to go for support and care. Cancer is
AUTOLOGOUS STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA: IS IT STILL THE RIGHT CHOICE?
 AUTOLOGOUS STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA: IS IT STILL THE RIGHT CHOICE? *Patrizia Tosi Hematology Unit, Department of Oncology and Hematology, Infermi Hospital, Rimini, Italy *Correspondence
AUTOLOGOUS STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA: IS IT STILL THE RIGHT CHOICE? *Patrizia Tosi Hematology Unit, Department of Oncology and Hematology, Infermi Hospital, Rimini, Italy *Correspondence
Phase II: Carfilzomib, Lenalidomide, and Dexamethasone in Newly Diagnosed Multiple Myeloma Neha Korde, MD, Clinical Investigator Ola Landgren, MD
 Phase II: Carfilzomib, Lenalidomide, and Dexamethasone in Newly Diagnosed Multiple Myeloma Neha Korde, MD, Clinical Investigator Ola Landgren, MD PhD, Principal Investigator Multiple Myeloma Section, NCI/NIH,
Phase II: Carfilzomib, Lenalidomide, and Dexamethasone in Newly Diagnosed Multiple Myeloma Neha Korde, MD, Clinical Investigator Ola Landgren, MD PhD, Principal Investigator Multiple Myeloma Section, NCI/NIH,
Multiple Myeloma. Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida CP1123175-1
 Multiple Myeloma 8 th Annual Living with Myeloma Conference New Developments in Multiple Myeloma Treatment Scottsdale, AZ March 22, 2014 Robert A. Kyle, MD Scottsdale, Arizona Rochester, Minnesota Jacksonville,
Multiple Myeloma 8 th Annual Living with Myeloma Conference New Developments in Multiple Myeloma Treatment Scottsdale, AZ March 22, 2014 Robert A. Kyle, MD Scottsdale, Arizona Rochester, Minnesota Jacksonville,
Multiple Myeloma. What is multiple myeloma? Low blood counts
 Multiple Myeloma What is multiple myeloma? Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer, and can spread to other areas of the
Multiple Myeloma What is multiple myeloma? Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer, and can spread to other areas of the
Proteins. Protein Trivia. Optimizing electrophoresis
 Proteins ELECTROPHORESIS Separation of a charged particle in an electric field Michael A. Pesce, Ph.D Department of Pathology New York-Presbyterian Hospital Columbia University Medical Center Rate of migration
Proteins ELECTROPHORESIS Separation of a charged particle in an electric field Michael A. Pesce, Ph.D Department of Pathology New York-Presbyterian Hospital Columbia University Medical Center Rate of migration
The following investigations are required at diagnosis, so that a disease category and stage can be assigned (see below).
.") 3 MULTIPLE MYELOMA Clinical features Multiple myeloma (MM) is a disease with a peak incidence in the 6 th and seventh decades of life, but can also occur in younger patients. It is characterised by infiltration
3 MULTIPLE MYELOMA Clinical features Multiple myeloma (MM) is a disease with a peak incidence in the 6 th and seventh decades of life, but can also occur in younger patients. It is characterised by infiltration
ADVANCES IN MULTIPLE MYELOMA:
 MYELOMA AND THE NEWLY DIAGNOSED PATIENT: A FOCUS ON TREATMENT AND MANAGEMENT S. Vincent Rajkumar, MD LEARNING OBJECTIVES Upon completion of this educational activity, participants should be able to: Discuss
MYELOMA AND THE NEWLY DIAGNOSED PATIENT: A FOCUS ON TREATMENT AND MANAGEMENT S. Vincent Rajkumar, MD LEARNING OBJECTIVES Upon completion of this educational activity, participants should be able to: Discuss
The Role of Bisphosphonates in Multiple Myeloma: 2007 Update Clinical Practice Guideline
 The Role of Bisphosphonates in Multiple Myeloma: 2007 Update Clinical Practice Guideline Introduction ASCO convened an Update Committee to review and update the 2002 recommendations for the role of bisphosphonates
The Role of Bisphosphonates in Multiple Myeloma: 2007 Update Clinical Practice Guideline Introduction ASCO convened an Update Committee to review and update the 2002 recommendations for the role of bisphosphonates
Multiple Myeloma Understanding your diagnosis
 Multiple Myeloma Understanding your diagnosis Multiple Myeloma Understanding your diagnosis When you first hear that you have cancer you may feel alone and afraid. You may be overwhelmed by the large amount
Multiple Myeloma Understanding your diagnosis Multiple Myeloma Understanding your diagnosis When you first hear that you have cancer you may feel alone and afraid. You may be overwhelmed by the large amount
FEIST- WEILLER CANCER CENTER MULTIPLE MYELOMA GUIDELINES. Updated December, 2011. Authors: Nebu Koshy, MD. Binu Nair, MD. Gerhard Hildebrandt, MD
 FEIST- WEILLER CANCER CENTER MULTIPLE MYELOMA GUIDELINES Updated December, 2011 Authors: Nebu Koshy, MD Binu Nair, MD Gerhard Hildebrandt, MD Reinhold Munker, MD Glenn Mills, MD Mandatory initial tests
FEIST- WEILLER CANCER CENTER MULTIPLE MYELOMA GUIDELINES Updated December, 2011 Authors: Nebu Koshy, MD Binu Nair, MD Gerhard Hildebrandt, MD Reinhold Munker, MD Glenn Mills, MD Mandatory initial tests
Momentum in Multiple Myeloma Treatment
 WHITE PAPER Momentum in Multiple Myeloma Treatment Dr. Harish P. Dave, MD, MBA Dr. Ben Manderman, MD Quintiles examines promising new approaches to more effective multiple myeloma treatments. HIGH RESPONSE
WHITE PAPER Momentum in Multiple Myeloma Treatment Dr. Harish P. Dave, MD, MBA Dr. Ben Manderman, MD Quintiles examines promising new approaches to more effective multiple myeloma treatments. HIGH RESPONSE
Revving up the Revlimid Debate Lenalidomide as Maintenance Therapy for Multiple Myeloma after Autologous Stem Cell Transplant
 Revving up the Revlimid Debate Lenalidomide as Maintenance Therapy for Multiple Myeloma after Autologous Stem Cell Transplant Sarah M. Villarreal, Pharm.D. PGY2 Hematology/Oncology Pharmacy Resident Department
Revving up the Revlimid Debate Lenalidomide as Maintenance Therapy for Multiple Myeloma after Autologous Stem Cell Transplant Sarah M. Villarreal, Pharm.D. PGY2 Hematology/Oncology Pharmacy Resident Department
MYEL NEWL OMA Y DIA GNOSED
 Information on NEWLY DIAGNOSED MYELOMA UAMS 1 ABOUT THE MYELOMA INSTITUTE The Myeloma Institute at the University of Arkansas for Medical Sciences (UAMS) is a leading center in the world for comprehensive
Information on NEWLY DIAGNOSED MYELOMA UAMS 1 ABOUT THE MYELOMA INSTITUTE The Myeloma Institute at the University of Arkansas for Medical Sciences (UAMS) is a leading center in the world for comprehensive
Multiple myeloma and other plasma cell dyscrasias
 CHAPTER 33 Multiple myeloma and other plasma cell dyscrasias Raman Desikan, MD, Sundar Jagannath, MD, Paul Richardson, MD, and Nikhil C. Munshi, MD MYELOMA MULTIPLE MYELOMA Multiple myeloma is a disseminated
CHAPTER 33 Multiple myeloma and other plasma cell dyscrasias Raman Desikan, MD, Sundar Jagannath, MD, Paul Richardson, MD, and Nikhil C. Munshi, MD MYELOMA MULTIPLE MYELOMA Multiple myeloma is a disseminated
Mantle Cell Lymphoma Understanding Your Treatment Options
 New Developments in Mantle Cell Lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Vice Chairman, Department
New Developments in Mantle Cell Lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Vice Chairman, Department
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES
 NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
THE MANY FACES OF MONOCLONAL GAMMOPATHIES
 THE MANY FACES OF MONOCLONAL GAMMOPATHIES Marion S. Sternbach, MD, FRCP(C), FACP Presented at Medicine Grand Rounds, St Joseph s Hospital Sept 19, 2007 Monoclonal Gammopathies Objectives. 1. Getting acquainted
THE MANY FACES OF MONOCLONAL GAMMOPATHIES Marion S. Sternbach, MD, FRCP(C), FACP Presented at Medicine Grand Rounds, St Joseph s Hospital Sept 19, 2007 Monoclonal Gammopathies Objectives. 1. Getting acquainted
Clinical Course of Patients With Relapsed Multiple Myeloma. Mayo Clin Proc. July 2004;79(7):867-874 www.mayo.edu/proceedings 867
:867-874 www.mayo.edu/proceedings 867") ORIGINAL RELAPSED MULTIPLE ARTICLE MYELOMA Clinical Course of Patients With Relapsed Multiple Myeloma SHAJI K. KUMAR, MD; TERRY M. THERNEAU, PHD; MORIE A. GERTZ, MD; MARTHA Q. LACY, MD; ANGELA DISPENZIERI,
ORIGINAL RELAPSED MULTIPLE ARTICLE MYELOMA Clinical Course of Patients With Relapsed Multiple Myeloma SHAJI K. KUMAR, MD; TERRY M. THERNEAU, PHD; MORIE A. GERTZ, MD; MARTHA Q. LACY, MD; ANGELA DISPENZIERI,
Recent Advances in Diagnosis and Management of Multiple Myeloma: An Update
 Chapter 80 Recent Advances in Diagnosis and Management of Multiple Myeloma: An Update PS Ghalaut, Soumik Chaudhuri, Ragini Singh INTRODUCTION Multiple myeloma (from Greek myelo bonemarrow) is one of the
Chapter 80 Recent Advances in Diagnosis and Management of Multiple Myeloma: An Update PS Ghalaut, Soumik Chaudhuri, Ragini Singh INTRODUCTION Multiple myeloma (from Greek myelo bonemarrow) is one of the
Personalized, Targeted Treatment Options Offer Hope of Multiple Myeloma as a Chronic Disease
 /publications/targeted-therapy-news/2012/november-2012/personalized-targeted-treatment-options- Offer-Hope-of-Multiple-Myeloma-as-a-Chronic-Disease Personalized, Targeted Treatment Options Offer Hope of
/publications/targeted-therapy-news/2012/november-2012/personalized-targeted-treatment-options- Offer-Hope-of-Multiple-Myeloma-as-a-Chronic-Disease Personalized, Targeted Treatment Options Offer Hope of
New diagnostic criteria for myeloma
 New diagnostic criteria for myeloma Dr Guy Pratt Senior Lecturer/Honorary Consultant Haematologist University of Birmingham/Heart of England NHS Trust International Myeloma Working Group (IMWG) define
New diagnostic criteria for myeloma Dr Guy Pratt Senior Lecturer/Honorary Consultant Haematologist University of Birmingham/Heart of England NHS Trust International Myeloma Working Group (IMWG) define
Understanding the Immune System in Myeloma
 Brian GM Durie Understanding the Immune System in Myeloma Living Well with Myeloma Teleconference Series Thursday, March 19 th 2015 1 The Immune System is Like a Swiss Watch B Cell T Cell Plasma Cell Changing
Brian GM Durie Understanding the Immune System in Myeloma Living Well with Myeloma Teleconference Series Thursday, March 19 th 2015 1 The Immune System is Like a Swiss Watch B Cell T Cell Plasma Cell Changing
Comparison of Serum Beta 2-Microglobulin and 24 hour Urinary Creatinine Clearance as a Prognostic Factor in Multiple Myeloma
 J Korean Med Sci 2006; 21: 639-44 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences Comparison of Serum Beta 2-Microglobulin and 24 hour Urinary Creatinine Clearance as a Prognostic Factor
J Korean Med Sci 2006; 21: 639-44 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences Comparison of Serum Beta 2-Microglobulin and 24 hour Urinary Creatinine Clearance as a Prognostic Factor
2014; 5(3): 248-252. doi: 10.7150/jca.8541 Research Paper
: 248-252. doi: 10.7150/jca.8541 Research Paper") 248 Ivyspring International Publisher Journal of Cancer 2014; 5(3): 248-252. doi: 10.7150/jca.8541 Research Paper Partial Response at Completion of Bortezomib- Thalidomide-Dexamethasone (VTd) Induction
248 Ivyspring International Publisher Journal of Cancer 2014; 5(3): 248-252. doi: 10.7150/jca.8541 Research Paper Partial Response at Completion of Bortezomib- Thalidomide-Dexamethasone (VTd) Induction
Multiple Myeloma: Charging Toward a Bright Future
 CA Cancer J Clin 2007;57:301 318 Multiple Myeloma: Charging Toward a Bright Future Jed A. Katzel, MD; Parameswaran Hari, MD; David H. Vesole, MD, PhD Dr. Katzel is Fellow, Hematology/ Oncology, St. Vincent
CA Cancer J Clin 2007;57:301 318 Multiple Myeloma: Charging Toward a Bright Future Jed A. Katzel, MD; Parameswaran Hari, MD; David H. Vesole, MD, PhD Dr. Katzel is Fellow, Hematology/ Oncology, St. Vincent
MULTIPLE MYELOMA A new era for an old disease
 Emerging trends and recommendations MULTIPLE MYELOMA A new era for an old disease Nizar J. Bahlis, MD and Douglas A. Stewart, MD, FRCPC Top-line summary Multiple myeloma (MM) is the second most common
Emerging trends and recommendations MULTIPLE MYELOMA A new era for an old disease Nizar J. Bahlis, MD and Douglas A. Stewart, MD, FRCPC Top-line summary Multiple myeloma (MM) is the second most common
Frequency of NHL Subtypes in Adults
 Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Why discuss CLL? Common: 40% of US leukaemia. approx 100 pa in SJH / MWHB 3 inpatients in SJH at any time
 Why discuss CLL? Common: 40% of US leukaemia approx 100 pa in SJH / MWHB 3 inpatients in SJH at any time Median age of dx is 65 (30s. Incurable, survival 2-202 20 years Require ongoing supportive care
Why discuss CLL? Common: 40% of US leukaemia approx 100 pa in SJH / MWHB 3 inpatients in SJH at any time Median age of dx is 65 (30s. Incurable, survival 2-202 20 years Require ongoing supportive care