Optimizing Therapy in Progressive MS: Treatment Options
|
|
|
- Kenneth Jones
- 8 years ago
- Views:
Transcription
1 Optimizing Therapy in Progressive MS: Treatment Options Neeta Garg, MD Associate Professor of Neurology University of Massachusetts Medical School Associate Director, Multiple Sclerosis Center UMass Memorial Medical Center

2 Multiple Sclerosis Multiple sclerosis is a potentially treatable disorder The recent focus has been on the early diagnosis and treatment Disease modifying therapy can slow down the progression of disability May delay the development of clinically definite MS

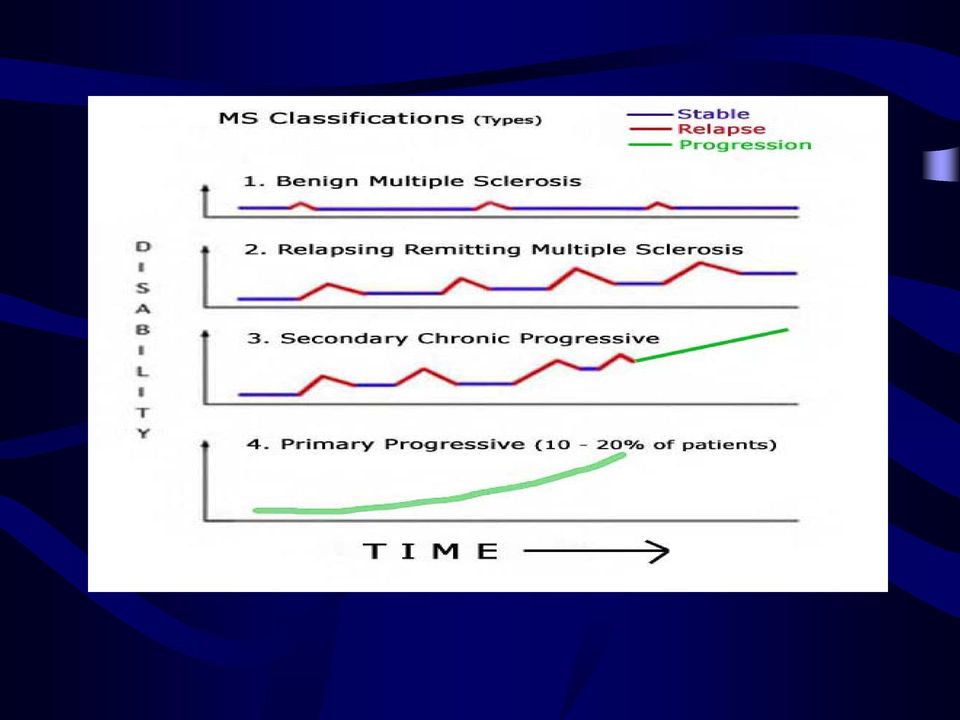
3 Definition of MS Subgroups Relapsing-remitting MS: clear relapses with full recovery or with residual deficit; lack of disease progression in periods between relapses Primary-progressive MS: disease progression from onset with occasional plateaus and temporary minor improvement without relapses Secondary-progressive MS: initial RR course followed by progression with or without occasional relapses, minor remissions and plateaus Progressive-relapsing MS: progressive disease from onset, clear acute relapses, continued progression between relapses Lublin and Reingold, Neurology 1996; 46,

4 MS: Clinical Subtypes Relapsing-remitting Secondary progressive Symptoms Time Symptoms Time Symptoms Time Symptoms Time Primary progressive Progressive-relapsing Symptoms Time Symptoms Time Symptoms Time Symptoms Time Lublin FD, et al. Neurology. 1996;46: Kieseier BC, et al. Semin Neurol. 2003;23: Overview of MS

5
6 Multiple Sclerosis Disease activity heterogeneous and course variable First-line therapy: partially effective, 30% relapse reduction with DMT: stabilization vs. continuous activity in some patients About 50 percent of people with relapsingremitting MS may progress to SPMS within ten years and up to 80 to 90% of people with RRMS would eventually develop SPMS within 25 years slow progressive accumulation of disability fewer or no relapses

7 Optimizing therapy in progressive MS However, this was before the wide-spread use of disease-modifying medications Before DMTs became widely available, the long-term effects of these medications on the progression of MS still not known Proportion of progressive disease probably much lower and slower to develop now

8 MS: Natural history In 60% of patients, MS begins as a relapsing-remitting disease and evolves secondarily into a progressive neurological illness Up to 40% of patients with attacks severe enough to render them nonambulatory may not recover At 15 years from MS onset, 50% of patients are disabled to the point at which they at least require a cane to walk a half block Early age at onset, female sex, relapsing-remitting course at onset, and perhaps optic neuritis or sensory symptoms at onset and relatively few attacks in the first two years are associated with a favorable course Weinshenker et al, Ann Neurol. 1994;36 Suppl:S6-11

9 MS and Disability Fifteen years after diagnosis: 80% of patients have functional impairment 50% of patients are unable to walk 70% of patients are unable to continue working PDRHealth. Multiple Sclerosis. Available at: Overview of MS

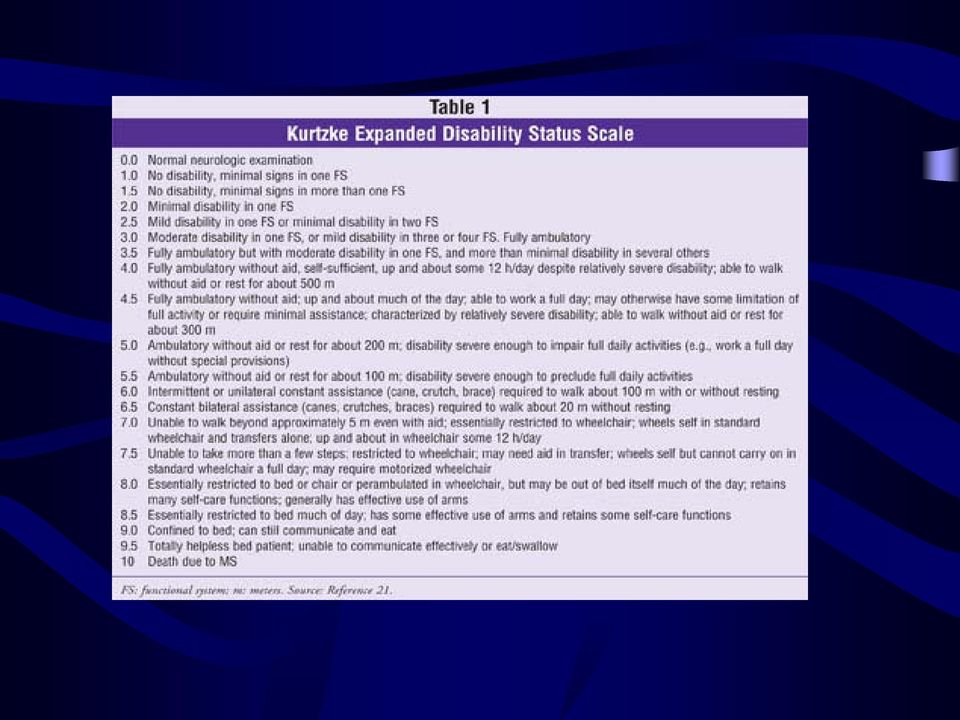
10 Key Parameters in MS Management: Disability Expanded Disability Status Scale Death Normal neurological exam Minimal disability Increased limitation in walking ability Need for walking assistance Restriction to wheelchair Helpless bed patient Patient disability classification Expanded Disability Status Scale (EDSS) = Rating system used by neurologists and clinical trial investigators to follow the progression of disability in MS Kurtzke JF. Neurology. 1983;33: Overview of MS
 = Rating system used by neurologists and clinical trial")
11
12 MS: Natural history Patients with definite relapsing-remitting MS at British- Columbian MS clinic before July 1998 were selected from the population-based database Prognosis and risk factors for progression to and from SPMS were examined Results 87.6% were relapsing-remitting (RR) at onset, 58.2% reaching SPMS, at median 18.9 years The RR phase lasted on average almost two decades, being shorter for males and those older at onset of MS A longer RR phase was a favorable predictor of disease progression in SPMS Longer disease duration, older age, and lower EDSS at onset of SPMS: slower progression to higher disability Tremlett et al, Mult Scler Apr;14(3):314-24

13 MS: Natural history The relationship of relapses to long-term disability in multiple sclerosis is uncertain Relapse reduction is a common therapeutic target but dissociation between relapse suppression and disability accumulation exists Relationships between relapses and disability progression in the preprogressive or relapsing-remitting phase for outcomes of disability (requiring assistance to walk, being bedridden and dying from multiple sclerosis [Disability Status Scale 6, 8, 10) was investigated Results: Frequent relapses in the first 2 years and shorter first inter-attack intervals predicted shorter times to reach hard disability endpoints Time to Disability Status Scale 3 highly and independently predicted time to Disability Status Scale 6, 8 and 10 In contrast, neither total number of relapsing-remitting phase attacks nor of relapses experienced during the relapsing-remitting phase after the second year up to onset of progression showed correlation with progression of disability Scalfari et al, Brain Jun 9. [Epub ahead of print]

14 MS: Natural history Relapse frequency beyond Year 2 does not appear to predict the key outcome of secondary progression or times to higher disability highlighting two distinct disease phases related to late outcome These appear to be separated by a watershed within the relapsing-remitting phase, just a few years after clinical onset Higher early relapse frequencies and shorter first inter-attack intervals herald more rapid deterioration via interaction with the neurodegeneration characterizing secondary progression Scalfari et al, Brain Jun 9. [Epub ahead of print]

15 How to diagnose progressive disease
16 Progressive disease: Diagnosis Subjective Worsening symptoms with or without continued attacks Increasing disability Physical Cognitive Objective Increased number and severity of relapses Worsening (sustained) baseline disability Walking: 25-foot walk time Hand function: 9-hole peg time Cognitive impairment Greater lesion burden on MRI

17 Key Parameters in MS Management MRI Activity and Area Assesses MS disease activity in the brain and helps track disease progression* Relapse With each relapse in MS, the probability of permanent disability increases Disability Progression The unpredictable course of MS eventually leads to significant functional disability for many patients *The exact correlation between MRI findings and the current or future clinical status of patients, including disability progression, is unknown. Overview of MS

18 Definition of Breakthrough disease Clinical activity in 6 months after therapy Occurrence of a confirmed relapse with findings on neurologic examination consistent with the symptoms or Objective neurologic impairment (1-point increase in EDSS) MRI activity is defined as appearance of Combined unique activity (CUA) CAU: Number of lesions that were new or enlarging in T2- weighted images and Gd enhancing lesions Durelli et al, J Neurol Neurosurg Psychiatry 2008;79: Rio et al, Mult Scler 2008;14:

19 Key Parameters in MS Management: Relapse Relapse = New or worsening symptoms, lasting >24 hours in the absence of fever, attributed to MS activity, preceded by stability or improvement for 30 days. 1 Common clinical trial outcome measures: Relapse rate Time to relapse Risk of relapse Percent of patients remaining relapse free 1. Schumacher GA, et al. Ann NY Acad Sci. 1965;122: Overview of MS

20 Key Parameters in MS Management: MRI T1-weighted scan with gadolinium (Gd) enhancement Shows number of new lesions (currently active disease) T2-weighted scan Shows number and size of new as well as older (inactive) lesions The exact correlation between MRI findings and the current or future clinical status of patients, including disability progression, is unknown. Overview of MS

21 MS: Breakthrough disease Disease activity is highly heterogeneous among patients with multiple sclerosis Average reduction in relapse rate of 30% induced by interferon (IFN)- treatment encompasses stabilization of disease in some patients and continuous disease activity in others The effect of IFN is provable on MRI even within the first weeks of treatment Presence of MRI disease activity within the first 6 12 months treatment appears predictive of subsequent clinical disease activity Nonresponders: High-titer of Nabs or other factors for biologic nonresponse Inherent high disease activity may underlie on-treatment disease activity Durelli et al, J Neurol Neurosurg Psychiatry 2008;79: Rio et al, Mult Scler 2008;14: , Hesse et al, Neurology 2010;74;
22 MS: Breakthrough disease In published phase III trials 62% to 75% of patients with relapsing-remitting MS had one or more relapses within two years while on disease-modifying drug therapy about one fourth had a sustained increase in Expanded Disability Status Scale score one fourth had one or more gadolinium (Gd)-enhancing lesions more than half had one or more new T2 lesions Rudick et al, CNS Drugs. 2008;22(10): Malucchi et al, Neurology. 2008;70(13 pt 2):
23 Therapeutic Options
24
25
26 Other Therapy Options for MS Other potential MS therapies Corticosteroids Cyclophosphamide (Cytoxan ) Azathioprine (Imuran ) Methotrexate Mycophenolate mofetil (Cellcept ) Monoclonal antibodies Intravenous immunoglobulin G (IVIG) Plasmapheresis Cladribine
27 Case history 64 yo male with progressive leg stiffness, weakness, walking difficulties, and urinary urgency and hesitancy for last 20 years Started using cane 10 years ago, currently able to walk with the cane although walking slower and limited for last 2 years Exam: moderate spasticity and weakness in legs with ataxia CSF: positive OCB and elevated IgG index
28 Cervical MRI: T2WI
29 Thoracic MRI
30 Primary Progressive MS
31 PPMS: Natural history Seen in 10-15% of patients Age of onset 10 years older than RRMS (40 vs 30) Peak age of onset of years for men versus years for women Different sex ratio (M:F=1:1.3), men affected more frequently in PPMS than RRMS (M:F = 1:3) This distinction also blurs with advancing age of onset Weinshenker et al, Brain 1989, Cottrell et al, Brain 1999 Ebers GC, Neurol Sci 2000, Tremlett et al, Neurology 2005
32 Primary Progressive MS Seen in 10-15% of patients Age of onset 10 years older than RRMS (40 vs 30) Peak age of onset of years for men versus years for women Different sex ratio (M:F=1:1.3), men affected more frequently in PPMS than RRMS (M:F = 1:3) This distinction also blurs with advancing age of onset
33 PPMS: Clinical presentation Progressive myelopathy in 80-90% over monthsyears Less common: Pancerebellar syndrome with progressive ataxia Rarely progressive visual loss due to optic neuropathy Cognitive impairment with attention, working memory, and other deficits frequently seen with any presentation
34 PPMS: Disease modifying therapy PROMise (Placebo-controlled trial of glatiramer acetate in PPMS): largest study in PPMS Randomized, placebo-controlled 3 year trial 943 patients, Glatiramer acetate vs. placebo Number of patients with sustained increase in disability low No significant reduction in treatment arm Study stopped at 2 years Subgroup analysis showed some effect in males Wolinsky et al, Ann Neurol 2007
35 PPMS: Treatment Corticosteroids tried empirically, no evidence Beta-interferon Study IFN-β-1a of 50 patients: no effect on disability, brain or spinal cord atrophy (Leary et al, Neurology 2003) IFN-β-1b studied in 73 patients: non-significant trend for disability (EDSS) and significant effect on MSFC (Montalban X, Mult Scler 2004, suppl)
36 PPMS: Treatment Placebo-controlled trial of mitoxantrone (Kita et al, Neurology 2004, abst.) Negative Cladribine Not effective in PPMS and SPMS (Rice et al, Neurology 2000) Methotrexate (low dose-7.5 mg weekly) Small beneficial effect on arm function (Goodkin et al, Ann Neurol 1995) IVIG PPMS patients showed a slight favorable IVIG effect on the best EDSS score (Pohlau et al, Mult Scler. 2007;13(9): ) Riluzole Stabilization of cervical cord area and T1 lesion volume in 16 patients (Kalkers et al, Mult Scler 2002)
37 Rituximab (Rituxan ) in PPMS OLYMPUS trial: Phase II/III randomized, double-blind, placebocontrolled, multi-center study was designed to evaluate the efficacy, safety and tolerability of four courses of Rituximab in patients with PPMS Study of 439 patients for 96 weeks, Rituximab didn't significantly slow the course of the disease Subgroup analysis showed time to CDP was delayed in rituximab-treated patients aged <51 years (hazard ratio [HR] = 0.52; p = 0.010) those with gadolinium-enhancing lesions (HR = 0.41; p = 0.007) and those aged <51 years with gadolinium-enhancing lesions (HR = 0.33; p = 0.009) compared with placebo Hawker et al, Ann Neurol Oct;66(4):460-71
38 PPMS: Treatment Uncontrolled studies: disease stabilization Autologous hematopoetic stem cell transplantation (Saccardi et al, Mult Scler 2006) Cyclophosphamide (Zephir et al, J Neurol Sci 2004)
39 PPMS: Future therapies Ongoing trials FTY720 or Fingolimod in Patients With Primary Progressive Multiple Sclerosis (INFORMS) Canabinoids: phase III study in UK Natalizumab Treatment of Progressive Multiple Sclerosis (NAPMS): phase II trial to study safety and efficacy of natalizumab in treatment of primary and secondary progressive multiple sclerosis Double Blind Placebo-Controlled Phase I/II Clinical Trial of Idebenone (compound similar to coenzyme Q10) in Patients With Primary Progressive Multiple Sclerosis
40 Secondary Progressive MS
41
42 SPMS: Mitoxantrone Mitoxantrone (Novantrone ) has cytotoxic and immunosuppressive effects and has been used for the management of acute myeloid leukemia and symptomatic hormone-resistant prostate cancer MIMS trial: Effect of mitoxantrone in 194 patients with worsening RRMS or SPMS studied At 2 years, the mitoxantrone group experienced benefits compared with the placebo group for the primary outcome: multivariate composite consisting of EDSS change, Ambulation Index change, the number of treated relapses, the time to the first treated relapse, and the change in the Scripps Neurologic Rating Scale Mitoxantrone at a dose of 12 mg/m2 given every 3 months reduces progression of disability and clinical exacerbations To avoid cardiotoxicity, it is recommended that a lifetime cumulative dose of 140 mg/m2 should not be exceeded
43 SPMS: Beta-IFN-1b The European trial In the treatment arm a significant reduction of the confirmed 1-point EDSS progression rate was found The clinical and MRI attack rates and the volume of white matter disease as seen on MRI were significantly reduced Subgroup analysis of patients who did or did not experience clinical attacks in the 2 years before study initiation, or who did or did not have attacks during the study, demonstrated similar effects of IFN beta-1b The benefit, however, in patients with EDSS 6.0 was less convincing. North American trial The study design was similar but the trial failed to demonstrate a statistically significant reduction in the confirmed 1-point EDSS progression rate The reason for this discrepancy between these two trials is unclear It is possible that the North American cohort of patients had more advanced disease and significantly fewer superimposed attacks than their European counterparts and that IFN beta is most effective in the relapsing phase of the disease, but this is speculative European study group on IFN-beta-1b in SPMS, Lancet 1998;352:1491 7
44 SPMS: Beta-IFN-1a Similarly, the trial of subcutaneous IFN beta-1a in SPMS (the SPECTRIMS trial) failed to find a statistically significant reduction in the confirmed 1- point EDSS progression rate In a post hoc subgroup analysis, separating patients into those with or without relapses, a beneficial treatment effect on the confirmed 1- point EDSS progression rate was noted (P = 0.027) in patients with attacks The effect of intramuscular IFN beta 1a was investigated in 436 subjects with SPMS and EDSS 3.5 to 6.5 in the IMPACT trial IFN beta-1a was found to be beneficial (P = 0.033), an effect driven mainly by the nine-hole peg test, whereas there was no discernible benefit on the EDSS Patients in the treatment arm experienced 33% fewer relapses (P = 0.008) (SPECTRIMS) Study Group Neurology 2001;56:
45 SPMS: Beta-interferon The results of interferon b trials in patients with SP-MS have thus been mixed This is particularly striking with the two Betaseron studies, which appear superficially similar and use an identical interferon b product administered with the same dose schedule The European study showed a highly significant, though modest, benefit on disability progression, whereas the North American Study showed no differences This discrepancy has led to comparison between the two study populations. The North American population was significantly older at entry, had a longer disease duration, fewer relapses in the previous 2 years, greater change in EDSS in the 2 years before study entry, and fewer MRI enhancing lesions at study entry These differences suggest that the North American population showed less inflammation and possibly more noninflammatory axonal degeneration
46 SPMS: Beta-interferon Although speculative, this analysis would conclude that interferon b therapy is most effective in the earlier inflammatory stage of MS, and increasingly less effective in later stages characterized by progressive disability In conclusion, it is appropriate to consider IFN beta for treatment with SPMS patients still experiencing relapses (Type A) The FDA has approved IFN beta-1b for SPSM, and the European agency EMEA has approved IFN beta-1b and subcutaneous IFN beta-1a for SPSM with superimposed relapses. The utility of IFN beta in patients with SPMS that do not suffer superimposed relapses is uncertain at present (Type U)
47 SPMS: Dirucotide (MBP8298) Dirucotide induces antigen-specific immunological tolerance Phase 3, double-blind, randomized, placebocontrolled trial MAESTRO-01 Failed to meet the primary endpoint of delaying disease progression No difference after 2 years of treatment between groups on the Expanded Disability Status Scale or on any secondary endpoints
48 Case history 42 yo WF diagnosed with MS in 1996, initial symptoms left sided tingling and numbness BETASERON , discontinued (patient was stable no longer wanted to continue medication) Relapse after four years, numbness in legs Off therapy until 2006
49 Case history Received Copaxone from October 2006 to February 2007, discontinued due to allergic reaction December 2006: Relapse with left leg parasthesias and back pain April 2007 to September 2007: Avonex along with pulse steroids from June to September 2007 for increased lesion load on brain MRI September 2007: Relapse with dizziness and gait problems, MRI showed new midbrain lesion
50 RRMS with breakthrough disease
51 Breakthrough disease: Treatment approach Check compliance Check neutralizing antibodies Positive Copaxone might be a better choice Switching Between interferon products and glatiramer acetate: no studies to support Switch to Tysabri Combination therapy for suboptimal responders is also common but not supported by strong evidence Symptomatic therapy and rehabilitation Rudick et al, CNS Drugs. 2008;22(10): Malucchi et al, Neurology. 2008;70(13 pt 2):
52
53
54 Breakthrough disease in MS: Treatment options Cyclophosphamide (Cy) is an alkylating agent, high doses of Cy produce marked immunosuppression and an anti-inflammatory immune deviation Cy is most effective in young patients, with very active MS frequent relapses, rapid accumulation of disability, and gad+ lesions on brain MRI Monthly intravenous pulses of Cy for 1 year, followed by bimonthly pulses for the second year are a well-tolerated protocol in MS Most side effects (mild alopecia, nausea and vomiting, and cystitis) are transient, dose dependent, and reversible. Permanent amenorrhoea and bladder cancer have rarely been described As second-line therapy, Cy can be used in non-responders to IFN-beta or glatiramer acetate As induction therapy, a short course (6-12 months) of Cy can precede immunomodulatory drugs in selected patients with an aggressive MS onset Rinaldi et al, Neurol Sci Oct;30 Suppl 2:S171-3
55 Breakthrough disease in MS: Treatment options Mitoxantrone (MTX) is a synthetic antineoplastic cytotoxic drug, active both on proliferative and non-proliferative cells The efficacy of MTX has been suggested by many open-label or observational studies and demonstrated in four randomized controlled clinical trials It is indicated for reducing neurological disability and the frequency of clinical relapses in patients with progressive relapsing and worsening relapsing-remitting MS patients The short-term adverse events Nausea/vomiting, alopecia, an increased risk of urinary and respiratory tract infections, phlebitis, transitory leukopenia, amenorrhea in female patients and infertility Most serious risks of the drug Cardiotoxicity and leukaemia, whose incidence seems to be higher than previously reported Martinelli et al, Neurol Sci Oct;30 Suppl 2:S167-70
56 Corticosteroids in treatment of MS Chronic use of high dose intravenous methylprednisolone (IVMP) in patients with MS may limit brain atrophy progression over the long-term In patients with RR-MS, treatment with pulses of IVMP (given every 4 months for 3 years and then every 6 months for the subsequent 2 years) vs. IVMP only for relapses slows development of T1 black holes prevents or delays whole-brain atrophy prevents or delays disability progression Zivadinov et al, Neurology Oct 9;57(7):
57 Corticosteroids in treatment of MS NORMIMS (NORdic trial of oral Methylprednisolone as add-on therapy to Interferon beta-1a for treatment of relapsing-remitting Multiple Sclerosis) Multicenter, randomized trial in RRMS patients with breakthrough disease on Rebif Oral 200 mg methylprednisolone or placebo for 5 consecutive days every 4 weeks for 96 weeks 62% reduction in relapse rates Sorensen et al, Lancet Neurol Jun;8(6):519-29
58 Corticosteroids in treatment of MS However recent ACT trial with weekly IFNβ-1a 30 µg IM and adjunctive steroid therapy was negative Patients with continued disease activity on weekly IFNβ- 1a 30 µg IM were randomized in a 2 x 2 factorial design to adjunctive weekly placebo or MTX 20 mg PO, with or without bimonthly IVMP 1,000 mg/day for 3 days No benefit of adding low-dose oral methotrexate or every other month IV methylprednisolone to interferon beta-1a in relapsing-remitting multiple sclerosis Cohen et al, Neurology 2009;72:
59
60
61 Progressive MS: Conclusion Disease-modifying drugs for relapsing-remitting multiple sclerosis are only partly effective Breakthrough disease common despite treatment Breakthrough disease is predictive of continued disease activity and a poor prognosis More aggressive therapy warranted in these patients Randomized controlled trials of alternative monotherapies or combination therapies needed Not many options for progressive MS Symptomatic therapy and rehabilitation
62
Disease Modifying Therapies for MS
 Disease Modifying Therapies for MS The term disease-modifying therapy means a drug that can modify or change the course of a disease. In other words a DMT should be able to reduce the number of attacks
Disease Modifying Therapies for MS The term disease-modifying therapy means a drug that can modify or change the course of a disease. In other words a DMT should be able to reduce the number of attacks
Medication Policy Manual. Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012
 Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
Medication Policy Manual. Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012
 Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 11, 2015 Next Review Date: December 2016 Effective Date: January
Medication Policy Manual Policy No: dru283 Topic: Aubagio, teriflunomide Date of Origin: November 9, 2012 Committee Approval Date: December 11, 2015 Next Review Date: December 2016 Effective Date: January
Disease Modifying Therapies for MS
 Disease Modifying Therapies for MS The term disease-modifying therapy (DMT) means a drug that can modify or change the course of a disease. In other words a DMT should be able to reduce the number of attacks
Disease Modifying Therapies for MS The term disease-modifying therapy (DMT) means a drug that can modify or change the course of a disease. In other words a DMT should be able to reduce the number of attacks
National MS Society Information Sourcebook www.nationalmssociety.org/sourcebook
 National MS Society Information Sourcebook www.nationalmssociety.org/sourcebook Chemotherapy The literal meaning of the term chemotherapy is to treat with a chemical agent, but the term generally refers
National MS Society Information Sourcebook www.nationalmssociety.org/sourcebook Chemotherapy The literal meaning of the term chemotherapy is to treat with a chemical agent, but the term generally refers
Relapsing-remitting multiple sclerosis Ambulatory with or without aid
 AVONEX/BETASERON/COPAXONE/EXTAVIA/GILENYA/REBIF/TYSABRI Applicant must be covered on an Alberta Government sponsored drug program. Page 1 of 5 PATIENT INFMATION Surname First Name Middle Initial Sex Date
AVONEX/BETASERON/COPAXONE/EXTAVIA/GILENYA/REBIF/TYSABRI Applicant must be covered on an Alberta Government sponsored drug program. Page 1 of 5 PATIENT INFMATION Surname First Name Middle Initial Sex Date
Using the MS Clinical Course Descriptions in Clinical Practice
 Using the MS Clinical Course Descriptions in Clinical Practice Mark J. Tullman, MD Director of Clinical Research The MS Center for Innovations in Care Missouri Baptist Medical Center Disclosures Consultant/speaking
Using the MS Clinical Course Descriptions in Clinical Practice Mark J. Tullman, MD Director of Clinical Research The MS Center for Innovations in Care Missouri Baptist Medical Center Disclosures Consultant/speaking
Progress in MS: Current and Emerging Therapies
 Progress in MS: Current and Emerging Therapies Presented by: Dr. Kathryn Giles, MD MSc FRCPC The MS Society gratefully acknowledges the grant received from Biogen Idec Canada, which makes possible the
Progress in MS: Current and Emerging Therapies Presented by: Dr. Kathryn Giles, MD MSc FRCPC The MS Society gratefully acknowledges the grant received from Biogen Idec Canada, which makes possible the
Integrating New Treatments: A Case Based Approach
 Integrating New Treatments: A Case Based Approach JILL CONWAY, MD, MA, MSCE DIRECTOR, MS CENTER DIRECTOR, NEUROLOGY CLERKSHIP AT UNCSOM- CHARLOTTE CAMPUS CAROLINAS HEALTHCARE CENTER Objectives Provide
Integrating New Treatments: A Case Based Approach JILL CONWAY, MD, MA, MSCE DIRECTOR, MS CENTER DIRECTOR, NEUROLOGY CLERKSHIP AT UNCSOM- CHARLOTTE CAMPUS CAROLINAS HEALTHCARE CENTER Objectives Provide
Committee Approval Date: December 12, 2014 Next Review Date: December 2015
 Medication Policy Manual Policy No: dru299 Topic: Tecfidera, dimethyl fumarate Date of Origin: May 16, 2013 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
Medication Policy Manual Policy No: dru299 Topic: Tecfidera, dimethyl fumarate Date of Origin: May 16, 2013 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
Managing Relapsing Remitting MS Risks & benefits of emerging therapies. Dr Mike Boggild The Walton Centre
 Managing Relapsing Remitting MS Risks & benefits of emerging therapies Dr Mike Boggild The Walton Centre MS: Facts and figures Affects 1 in 800 in the UK Commonest cause of acquired neurological disability
Managing Relapsing Remitting MS Risks & benefits of emerging therapies Dr Mike Boggild The Walton Centre MS: Facts and figures Affects 1 in 800 in the UK Commonest cause of acquired neurological disability
Conflict of Interest Declaration. Overview of New Medications for Multiple Sclerosis. Assessment Question. Objectives 4/1/2011
 Conflict of Interest Declaration Overview of New Medications for Multiple Sclerosis I or my spouse have no actual or potential conflict of interest in relation to this activity. Crystal Obering, Pharm.D.,
Conflict of Interest Declaration Overview of New Medications for Multiple Sclerosis I or my spouse have no actual or potential conflict of interest in relation to this activity. Crystal Obering, Pharm.D.,
Advanced Multiple Sclerosis: Progressive MS Epidemiology
 Advanced Multiple Sclerosis: Progressive MS Epidemiology CMSC 2007-Washington, DC Mitchell T. Wallin, MD, MPH Associate Director-Clinical Care VA MS Center of Excellence-East East Associate Professor of
Advanced Multiple Sclerosis: Progressive MS Epidemiology CMSC 2007-Washington, DC Mitchell T. Wallin, MD, MPH Associate Director-Clinical Care VA MS Center of Excellence-East East Associate Professor of
Treatment in Relapsing MS: Choosing Among the Options. Donald Negroski, MD
 Treatment in Relapsing MS: Choosing Among the Options Donald Negroski, MD Disclosures Research Grants Educational activities and lectures Consulting or other services including Continuing Medical Education
Treatment in Relapsing MS: Choosing Among the Options Donald Negroski, MD Disclosures Research Grants Educational activities and lectures Consulting or other services including Continuing Medical Education
acquired chronic immune-mediated inflammatory condition of CNS. MS in children: 10% +secondary progressive MS: rare +primary progressive MS: rare
 Immunomodulatory Therapies in Pediatric MS Vuong Chinh Quyen Neurology Department Medscape Mar 8, 2013 Multiple Sclerosis in Children. Iran J Child Neurol. 2013 Spring Introduction acquired chronic immune-mediated
Immunomodulatory Therapies in Pediatric MS Vuong Chinh Quyen Neurology Department Medscape Mar 8, 2013 Multiple Sclerosis in Children. Iran J Child Neurol. 2013 Spring Introduction acquired chronic immune-mediated
Disease Modifying Therapies (DMTs) in Multiple Sclerosis
 in Multiple Sclerosis") Disease Modifying Therapies (DMTs) in Multiple Sclerosis Gary Stobbe, MD Medical Director, MS Project ECHO Clinical Assistant Professor, UW Neurology Conflict of Interest Dr. Stobbe has no conflicts of
Disease Modifying Therapies (DMTs) in Multiple Sclerosis Gary Stobbe, MD Medical Director, MS Project ECHO Clinical Assistant Professor, UW Neurology Conflict of Interest Dr. Stobbe has no conflicts of
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Gold R, Giovannoni G, Selmaj K, et al, for
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Gold R, Giovannoni G, Selmaj K, et al, for
Multiple Sclerosis Update. Bridget A. Bagert, MD, MPH Director, Ochsner Multiple Sclerosis Center
 Multiple Sclerosis Update Bridget A. Bagert, MD, MPH Director, Ochsner Multiple Sclerosis Center None Disclosures First of All. Why is my talk in the Neurodegenerative hour? I respectfully object! Case
Multiple Sclerosis Update Bridget A. Bagert, MD, MPH Director, Ochsner Multiple Sclerosis Center None Disclosures First of All. Why is my talk in the Neurodegenerative hour? I respectfully object! Case
Medication Policy Manual. Topic: Betaseron, Extavia, interferon beta-1b Date of Origin: June 18, 2004
 Medication Policy Manual Policy No: dru108 Topic: Betaseron, Extavia, interferon beta-1b Date of Origin: June 18, 2004 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective
Medication Policy Manual Policy No: dru108 Topic: Betaseron, Extavia, interferon beta-1b Date of Origin: June 18, 2004 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective
Multiple Sclerosis (MS) Class Update
 Class Update") Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119 Multiple Sclerosis (MS) Class Update Month/Year of
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119 Multiple Sclerosis (MS) Class Update Month/Year of
Medication Policy Manual. Topic: Plegridy, peginterferon beta-1a Date of Origin: December 12, 2014
 Medication Policy Manual Policy No: dru376 Topic: Plegridy, peginterferon beta-1a Date of Origin: December 12, 2014 Committee Approval Date: December 11, 2015 Next Review Date: December 2016 Effective
Medication Policy Manual Policy No: dru376 Topic: Plegridy, peginterferon beta-1a Date of Origin: December 12, 2014 Committee Approval Date: December 11, 2015 Next Review Date: December 2016 Effective
Which injectable medication should I take for relapsing-remitting multiple sclerosis?
 Which injectable medication should I take for relapsing-remitting multiple sclerosis? A decision aid to discuss options with your doctor This decision aid is for you if you: Have multiple sclerosis Have
Which injectable medication should I take for relapsing-remitting multiple sclerosis? A decision aid to discuss options with your doctor This decision aid is for you if you: Have multiple sclerosis Have
Multiple Sclerosis (MS) Aprile Royal, Novartis Pharma Canada Inc. September 21, 2011 Toronto, ON
 Aprile Royal, Novartis Pharma Canada Inc. September 21, 2011 Toronto, ON") Multiple Sclerosis (MS) Aprile Royal, Novartis Pharma Canada Inc. September 21, 2011 Toronto, ON First-line DMTs Reduce Relapse Frequency by ~30% vs. Placebo Frequency of relapse with various DMTs, based
Multiple Sclerosis (MS) Aprile Royal, Novartis Pharma Canada Inc. September 21, 2011 Toronto, ON First-line DMTs Reduce Relapse Frequency by ~30% vs. Placebo Frequency of relapse with various DMTs, based
SECTION 2. Section 2 Multiple Sclerosis (MS) Drug Coverage
 Drug Coverage") SECTION 2 Multiple Sclerosis (MS) Drug Coverage Section 2 Multiple Sclerosis (MS) Drug Coverage ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST Selected Drug Products used in the treatment of patients with
SECTION 2 Multiple Sclerosis (MS) Drug Coverage Section 2 Multiple Sclerosis (MS) Drug Coverage ALBERTA HEALTH AND WELLNESS DRUG BENEFIT LIST Selected Drug Products used in the treatment of patients with
Life with MS: Striving for Maximal Independence & Fulfillment
 Life with MS: Striving for Maximal Independence & Fulfillment St. Louis, May 7, 2005 Florian P. Thomas, MA, MD, PhD MS Center, Department of Neurology Associate Professor, Saint Louis University Brain
Life with MS: Striving for Maximal Independence & Fulfillment St. Louis, May 7, 2005 Florian P. Thomas, MA, MD, PhD MS Center, Department of Neurology Associate Professor, Saint Louis University Brain
What is MS? 1. disease that affects the central nervous. Is a disease that affects both white and gray matter
 What is MS? 1 Neuron Damaged myelin due to inflammation MS is a chronic immunemediated disease that affects the central nervous system (CNS) Is a disease that affects both white and gray matter Interrupted
What is MS? 1 Neuron Damaged myelin due to inflammation MS is a chronic immunemediated disease that affects the central nervous system (CNS) Is a disease that affects both white and gray matter Interrupted
FastTest. You ve read the book... ... now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
Personalised Medicine in MS
 Personalised Medicine in MS Supportive Evidence from Therapeutic Trials Ludwig Kappos Neurology and Department of Biomedicine University Hospital CH-4031 Basel LKappos@uhbs.ch Established partially effective
Personalised Medicine in MS Supportive Evidence from Therapeutic Trials Ludwig Kappos Neurology and Department of Biomedicine University Hospital CH-4031 Basel LKappos@uhbs.ch Established partially effective
PCORI Workshop on Treatment for Multiple Sclerosis. Breakout Group Topics and Questions Draft 3-27-15
 PCORI Workshop on Treatment for Multiple Sclerosis Breakout Group Topics and Questions Draft 3-27-15 Group 1 - Comparison across DMTs, including differential effects in subgroups Consolidated straw man
PCORI Workshop on Treatment for Multiple Sclerosis Breakout Group Topics and Questions Draft 3-27-15 Group 1 - Comparison across DMTs, including differential effects in subgroups Consolidated straw man
Disclosures. Consultant and Speaker for Biogen Idec, TEVA Neuroscience, EMD Serrono, Mallinckrodt, Novartis, Genzyme, Accorda Therapeutics
 Mitzi Joi Williams, MD Neurologist MS Center of Atlanta, Atlanta, GA Disclosures Consultant and Speaker for Biogen Idec, TEVA Neuroscience, EMD Serrono, Mallinckrodt, Novartis, Genzyme, Accorda Therapeutics
Mitzi Joi Williams, MD Neurologist MS Center of Atlanta, Atlanta, GA Disclosures Consultant and Speaker for Biogen Idec, TEVA Neuroscience, EMD Serrono, Mallinckrodt, Novartis, Genzyme, Accorda Therapeutics
Version History. Previous Versions. Drugs for MS.Drug facts box fingolimod Version 1.0 Author
 Version History Policy Title Drugs for MS.Drug facts box fingolimod Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review Date Supersedes/New (Further fields as required
Version History Policy Title Drugs for MS.Drug facts box fingolimod Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review Date Supersedes/New (Further fields as required
ß-interferon and. ABN Guidelines for 2007 Treatment of Multiple Sclerosis with. Glatiramer Acetate
 ABN Guidelines for 2007 Treatment of Multiple Sclerosis with ß-interferon and Glatiramer Acetate Published by the Association of British Neurologists Ormond House, 27 Boswell Street, London WC1N 3JZ Contents
ABN Guidelines for 2007 Treatment of Multiple Sclerosis with ß-interferon and Glatiramer Acetate Published by the Association of British Neurologists Ormond House, 27 Boswell Street, London WC1N 3JZ Contents
How To Use A Drug In Multiple Sclerosis
 Revised (2009) guidelines for prescribing in multiple sclerosis INTRODUCTION In January 2001, the (ABN) first published guidelines for the use of licensed disease modifying treatments (ß-interferon and
Revised (2009) guidelines for prescribing in multiple sclerosis INTRODUCTION In January 2001, the (ABN) first published guidelines for the use of licensed disease modifying treatments (ß-interferon and
Version History. Previous Versions. Policy Title. Drugs for MS.Drug facts box Glatiramer Acetate Version 1.0 Author
 Version History Policy Title Drugs for MS.Drug facts box Glatiramer Acetate Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review Date Supersedes/New (Further fields
Version History Policy Title Drugs for MS.Drug facts box Glatiramer Acetate Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review Date Supersedes/New (Further fields
Multiple Sclerosis - Relapsing and Remissioning
 DISEASE-MODIFYING THERAPIES IN RELAPSING-REMITTING MULTIPLE SCLEROSIS* Benjamin M. Greenberg, MD, MHS ABSTRACT Four major disease-modifying therapies are discussed within the context of relapsing and remitting
DISEASE-MODIFYING THERAPIES IN RELAPSING-REMITTING MULTIPLE SCLEROSIS* Benjamin M. Greenberg, MD, MHS ABSTRACT Four major disease-modifying therapies are discussed within the context of relapsing and remitting
Medication Policy Manual. Topic: Gilenya, fingolimod Date of Origin: November 22, 2010
 Medication Policy Manual Policy No: dru229 Topic: Gilenya, fingolimod Date of Origin: November 22, 2010 Committee Approval Date: December 11, 2015 Next Review Date: December 2016 Effective Date: January
Medication Policy Manual Policy No: dru229 Topic: Gilenya, fingolimod Date of Origin: November 22, 2010 Committee Approval Date: December 11, 2015 Next Review Date: December 2016 Effective Date: January
Version History. Previous Versions. for secondary progressive MS (SPMS) Policy Title. Drugs for MS.Drug facts box Interferon beta 1b
 Policy Title. Drugs for MS.Drug facts box Interferon beta 1b") Version History Policy Title Drugs for MS.Drug facts box Interferon beta 1b for secondary progressive MS (SPMS) Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review
Version History Policy Title Drugs for MS.Drug facts box Interferon beta 1b for secondary progressive MS (SPMS) Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review
New and Emerging Immunotherapies for Multiple Sclerosis: Oral Agents
 New and Emerging Immunotherapies for Multiple Sclerosis: Oral Agents William Tyor, M.D. Chief, Neurology Atlanta VA Medical Center Professor, Department of Neurology Emory University School of Medicine
New and Emerging Immunotherapies for Multiple Sclerosis: Oral Agents William Tyor, M.D. Chief, Neurology Atlanta VA Medical Center Professor, Department of Neurology Emory University School of Medicine
Treatment Optimization in MS: When to Start, When to Shift, when to Stop
 Treatment Optimization in MS: When to Start, When to Shift, when to Stop Mark S. Freedman MSc MD FAAN FANA FRCPC Director, Multiple Sclerosis Research Unit University of Ottawa Sr. Scientist, Ottawa Hospital
Treatment Optimization in MS: When to Start, When to Shift, when to Stop Mark S. Freedman MSc MD FAAN FANA FRCPC Director, Multiple Sclerosis Research Unit University of Ottawa Sr. Scientist, Ottawa Hospital
What is Multiple Sclerosis? Gener al information
 What is Multiple Sclerosis? Gener al information Kim, diagnosed in 1986 What is MS? Multiple sclerosis (or MS) is a chronic, often disabling disease that attacks the central nervous system (brain and spinal
What is Multiple Sclerosis? Gener al information Kim, diagnosed in 1986 What is MS? Multiple sclerosis (or MS) is a chronic, often disabling disease that attacks the central nervous system (brain and spinal
Review Date: March 2012. Issue Status: Approved Issue No: 2 Issue Date: March 2010
 Title: Multiple Sclerosis guidelines for the use of beta-interferon, glatiramer acetate, natalizumab, mitoxantrone and other disease Authors Name: Dr P Talbot Contact Name: Dr Paul Talbot Contact Phone
Title: Multiple Sclerosis guidelines for the use of beta-interferon, glatiramer acetate, natalizumab, mitoxantrone and other disease Authors Name: Dr P Talbot Contact Name: Dr Paul Talbot Contact Phone
Summary HTA. Interferons and Natalizumab for Multiple Sclerosis Clar C, Velasco-Garrido M, Gericke C. HTA-Report Summary
 Summary HTA HTA-Report Summary Interferons and Natalizumab for Multiple Sclerosis Clar C, Velasco-Garrido M, Gericke C Health policy background Multiple sclerosis (MS) is a chronic inflammatory disease
Summary HTA HTA-Report Summary Interferons and Natalizumab for Multiple Sclerosis Clar C, Velasco-Garrido M, Gericke C Health policy background Multiple sclerosis (MS) is a chronic inflammatory disease
06/06/2012. The Impact of Multiple Sclerosis in the Pacific Northwest. James Bowen, MD. Swedish Neuroscience Institute
 The Impact of Multiple Sclerosis in the Pacific Northwest James Bowen, MD Multiple Sclerosis Center Multiple Sclerosis Center Swedish Neuroscience Institute 1 2 Motor Symptoms of MS Weakness Spasticity
The Impact of Multiple Sclerosis in the Pacific Northwest James Bowen, MD Multiple Sclerosis Center Multiple Sclerosis Center Swedish Neuroscience Institute 1 2 Motor Symptoms of MS Weakness Spasticity
NHS BOURNEMOUTH AND POOLE AND NHS DORSET
 NHS BOURNEMOUTH AND POOLE AND NHS DORSET COMMISSIONING STATEMENT ON THE USE OF BETA-INTERFERON IN RELAPSING-REMITTING MULTIPLE SCLEROSIS OR SECONDARY PROGRESSIVE MULTIPLE SCLEROSIS, WHERE RELAPSES ARE
NHS BOURNEMOUTH AND POOLE AND NHS DORSET COMMISSIONING STATEMENT ON THE USE OF BETA-INTERFERON IN RELAPSING-REMITTING MULTIPLE SCLEROSIS OR SECONDARY PROGRESSIVE MULTIPLE SCLEROSIS, WHERE RELAPSES ARE
CNS DEMYLINATING DISORDERS
 CNS DEMYLINATING DISORDERS Multiple sclerosis A Dutch saint named Lidwina, who died in 1433, may have been one of the first known MS patients. After she fell while ice skating, she developed symptoms such
CNS DEMYLINATING DISORDERS Multiple sclerosis A Dutch saint named Lidwina, who died in 1433, may have been one of the first known MS patients. After she fell while ice skating, she developed symptoms such
Sensitive and reproducible clinical rating
 CLINICAL AND MRI MARKERS OF MS DISEASE PROGRESSION * Richard A. Rudick, MD ABSTRACT Sensitive and reproducible measures of multiple sclerosis (MS) severity and progression are important in the treatment
CLINICAL AND MRI MARKERS OF MS DISEASE PROGRESSION * Richard A. Rudick, MD ABSTRACT Sensitive and reproducible measures of multiple sclerosis (MS) severity and progression are important in the treatment
Lemtrada (alemtuzumab)
") Lemtrada (alemtuzumab) Policy Number: 5.02.517 Last Review: 08/2015 Origination: 08/2015 Next Review: 08/2016 Policy BCBSKC will provide coverage for Lemtrada (alemtuzumab) when it is determined to be
Lemtrada (alemtuzumab) Policy Number: 5.02.517 Last Review: 08/2015 Origination: 08/2015 Next Review: 08/2016 Policy BCBSKC will provide coverage for Lemtrada (alemtuzumab) when it is determined to be
Multiple Sclerosis: What You Need To Know. For Professionals
 Multiple Sclerosis: What You Need To Know For Professionals What will I learn today? The Basics: What is MS? Living with MS: A Family Affair We Can Help: The National MS Society What MS Is: MS is thought
Multiple Sclerosis: What You Need To Know For Professionals What will I learn today? The Basics: What is MS? Living with MS: A Family Affair We Can Help: The National MS Society What MS Is: MS is thought
How To Treat Ms With Ifnb-1B
 Disease Modifying Therapies in Multiple Sclerosis Report of The Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and The MS Council for Clinical Practice Guidelines
Disease Modifying Therapies in Multiple Sclerosis Report of The Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and The MS Council for Clinical Practice Guidelines
Original Policy Date
 MP 5.01.20 Tysabri (natalizumab) Medical Policy Section Prescription Drug Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Local Policy/12:2013 Return to Medical Policy Index Disclaimer
MP 5.01.20 Tysabri (natalizumab) Medical Policy Section Prescription Drug Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Local Policy/12:2013 Return to Medical Policy Index Disclaimer
Multiple Sclerosis: An imaging review and update on new treatments.
 Multiple Sclerosis: An imaging review and update on new treatments. Dr Marcus Likeman Consultant Neuroradiologist North Bristol NHS Trust Bristol Royal Hospital for Children MRI appearances - White Matter
Multiple Sclerosis: An imaging review and update on new treatments. Dr Marcus Likeman Consultant Neuroradiologist North Bristol NHS Trust Bristol Royal Hospital for Children MRI appearances - White Matter
A blood sample will be collected annually for up to 2 years for JCV antibody testing.
 Mellen Center Currently Enrolling Non-Treatment Trials STRATIFY-2 JCV Antibody Program in Patients with Relapsing Multiple Sclerosis Receiving or Considering Treatment with Tysabri Primary Investigator:
Mellen Center Currently Enrolling Non-Treatment Trials STRATIFY-2 JCV Antibody Program in Patients with Relapsing Multiple Sclerosis Receiving or Considering Treatment with Tysabri Primary Investigator:
Chapter 10. Summary & Future perspectives
 Summary & Future perspectives 123 Multiple sclerosis is a chronic disorder of the central nervous system, characterized by inflammation and axonal degeneration. All current therapies modulate the peripheral
Summary & Future perspectives 123 Multiple sclerosis is a chronic disorder of the central nervous system, characterized by inflammation and axonal degeneration. All current therapies modulate the peripheral
MSTAC Initial Application
 MSTAC Initial Application Please send applications to: Facsimile 04 916 7571 Further Contact Details: Address The Co-ordinator MSTAC PHARMAC P O Box 10-254 WELLINGTON Phone 04 460 4990 Email mstaccoordinator@pharmac.govt.nz
MSTAC Initial Application Please send applications to: Facsimile 04 916 7571 Further Contact Details: Address The Co-ordinator MSTAC PHARMAC P O Box 10-254 WELLINGTON Phone 04 460 4990 Email mstaccoordinator@pharmac.govt.nz
Laquinimod Polman, C. et al. Neurology 2005;64:987-991
 Laquinimod Polman, C. et al. Neurology 2005;64:987-991 Multicenter, double-blind, randomized trial, patients with RR MS received 0.1 mg or 0.3 mg laquinimod or placebo as three daily tablets for 24 weeks
Laquinimod Polman, C. et al. Neurology 2005;64:987-991 Multicenter, double-blind, randomized trial, patients with RR MS received 0.1 mg or 0.3 mg laquinimod or placebo as three daily tablets for 24 weeks
Two-Year Phase III Data Presented at AAN 61st Annual Meeting Show Positive Outcome of Cladribine Tablets in Patients with Multiple Sclerosis
 Your contact News Release Barbara Fry Phone +1 905 919 0163 April 29/30, 2009 Two-Year Phase III Data Presented at AAN 61st Annual Meeting Show Positive Outcome of Cladribine Tablets in Patients with Multiple
Your contact News Release Barbara Fry Phone +1 905 919 0163 April 29/30, 2009 Two-Year Phase III Data Presented at AAN 61st Annual Meeting Show Positive Outcome of Cladribine Tablets in Patients with Multiple
MS ECHO: Update on MS treatment. Gary Stobbe, MD Medical Director, MS Project ECHO Clinical Assistant Professor, UW Neurology 10 14 2015
 MS ECHO: Update on MS treatment Gary Stobbe, MD Medical Director, MS Project ECHO Clinical Assistant Professor, UW Neurology 10 14 2015 Conflict of Interest Dr. Stobbe has no conflicts of interest to disclose
MS ECHO: Update on MS treatment Gary Stobbe, MD Medical Director, MS Project ECHO Clinical Assistant Professor, UW Neurology 10 14 2015 Conflict of Interest Dr. Stobbe has no conflicts of interest to disclose
Immunex Corporation Novantrone (Mitoxantrone HCL) P&CNS Advisory Committee Briefing Document. Page 020
 P&CNS Advisory Committee Briefing Document. Page 020") Page 020 4.0 Efficacy of Mitoxantrone in Multiple Sclerosis The efficacy of mitoxantrone in MS was demonstrated in two well-designed, randomized trials: Studies 901 and 902. The study design and efficacy
Page 020 4.0 Efficacy of Mitoxantrone in Multiple Sclerosis The efficacy of mitoxantrone in MS was demonstrated in two well-designed, randomized trials: Studies 901 and 902. The study design and efficacy
The Changing Face of Multiple Sclerosis and Disease-modifying Therapies
 Multiple Sclerosis The Changing Face of Multiple Sclerosis and Disease-modifying Therapies a report by Jack S Burks, MD President, Multiple Sclerosis Alliance (MSA) and Chief Medical Officer, Multiple
Multiple Sclerosis The Changing Face of Multiple Sclerosis and Disease-modifying Therapies a report by Jack S Burks, MD President, Multiple Sclerosis Alliance (MSA) and Chief Medical Officer, Multiple
teriflunomide, 14mg, film-coated tablets (Aubagio ) SMC No. (940/14) Genzyme Ltd.
 SMC No. (940/14) Genzyme Ltd.") teriflunomide, 14mg, film-coated tablets (Aubagio ) SMC No. (940/14) Genzyme Ltd. 10 January 2014 (Issued 07 February 2014) The Scottish Medicines Consortium (SMC) has completed its assessment of the above
teriflunomide, 14mg, film-coated tablets (Aubagio ) SMC No. (940/14) Genzyme Ltd. 10 January 2014 (Issued 07 February 2014) The Scottish Medicines Consortium (SMC) has completed its assessment of the above
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Daclizumab for treating relapsing-remitting multiple Draft scope (pre-referral) Draft remit/appraisal objective To
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Daclizumab for treating relapsing-remitting multiple Draft scope (pre-referral) Draft remit/appraisal objective To
Treatment guidelines for relapsing MS and the two step approach for disease modifying therapy
 Treatment guidelines for relapsing MS and the two step approach for disease modifying therapy Klaus Schmierer, PhD FRCP Blizard Institute, Barts and The London School of Medicine & Dentistry Barts Health
Treatment guidelines for relapsing MS and the two step approach for disease modifying therapy Klaus Schmierer, PhD FRCP Blizard Institute, Barts and The London School of Medicine & Dentistry Barts Health
Understanding How Existing and Emerging MS Therapies Work
 Understanding How Existing and Emerging MS Therapies Work This is a promising and hopeful time in the field of multiple sclerosis (MS). Many new and different therapies are nearing the final stages of
Understanding How Existing and Emerging MS Therapies Work This is a promising and hopeful time in the field of multiple sclerosis (MS). Many new and different therapies are nearing the final stages of
How to S.E.A.R.C.H. SM for the Right MS Therapy For You!
 How to S.E.A.R.C.H. SM for the Right MS Therapy For You! The Changing Landscape The first treatment for relapsing-remitting multiple sclerosis (RRMS) was approved by the United States Food and Drug Administration
How to S.E.A.R.C.H. SM for the Right MS Therapy For You! The Changing Landscape The first treatment for relapsing-remitting multiple sclerosis (RRMS) was approved by the United States Food and Drug Administration
The MS Disease- Modifying Drugs. Gener al information
 The MS Disease- Modifying Drugs Gener al information Current as of October 30, 2009. This online version is updated as breaking news requires. If you have downloaded and printed a copy from the web, please
The MS Disease- Modifying Drugs Gener al information Current as of October 30, 2009. This online version is updated as breaking news requires. If you have downloaded and printed a copy from the web, please
A Letter From the MS Coalition
 0 A Letter From the MS Coalition The treatment of multiple sclerosis (MS) requires a comprehensive management strategy. One important component of that strategy is modifying the disease course. When deciding
0 A Letter From the MS Coalition The treatment of multiple sclerosis (MS) requires a comprehensive management strategy. One important component of that strategy is modifying the disease course. When deciding
Disease-modifying therapies in Chinese children with multiple sclerosis
 The Turkish Journal of Pediatrics 2014; 56: 482-486 Original Disease-modifying therapies in Chinese children with multiple sclerosis Fen Yang 1, De-hui Huang 2, Yang Yang 1, Wei-ping Wu 1 1 Department
The Turkish Journal of Pediatrics 2014; 56: 482-486 Original Disease-modifying therapies in Chinese children with multiple sclerosis Fen Yang 1, De-hui Huang 2, Yang Yang 1, Wei-ping Wu 1 1 Department
News on modifying diseases therapies. Michel CLANET CHU Toulouse France ECTRIMS
 News on modifying diseases therapies Michel CLANET CHU Toulouse France ECTRIMS Current treatment strategies Future oral treatments Future non oral treatments Drug safety and risks CIS at risk of MS Active
News on modifying diseases therapies Michel CLANET CHU Toulouse France ECTRIMS Current treatment strategies Future oral treatments Future non oral treatments Drug safety and risks CIS at risk of MS Active
Oxford University Hospitals. NHS Trust. Department of Neurology Natalizumab (Tysabri) for Multiple Sclerosis. Information for patients
 for Multiple Sclerosis. Information for patients") Oxford University Hospitals NHS Trust Department of Neurology Natalizumab (Tysabri) for Multiple Sclerosis Information for patients page 2 What is Natalizumab and what is it used for? Natalizumab is an
Oxford University Hospitals NHS Trust Department of Neurology Natalizumab (Tysabri) for Multiple Sclerosis Information for patients page 2 What is Natalizumab and what is it used for? Natalizumab is an
PROCEEDINGS TREATING RELAPSING-REMITTING MULTIPLE SCLEROSIS II: STRATEGIES FOR PATIENTS NOT RESPONDING TO PRIMARY TREATMENTS *
 TREATING RELAPSING-REMITTING MULTIPLE SCLEROSIS II: STRATEGIES FOR PATIENTS NOT RESPONDING TO PRIMARY TREATMENTS * Jeffrey L. Bennett, MD, PhD ABSTRACT Many patients with multiple sclerosis (MS) will eventually
TREATING RELAPSING-REMITTING MULTIPLE SCLEROSIS II: STRATEGIES FOR PATIENTS NOT RESPONDING TO PRIMARY TREATMENTS * Jeffrey L. Bennett, MD, PhD ABSTRACT Many patients with multiple sclerosis (MS) will eventually
Resources for the Primary Care Provider. Please print these out for reference
 Resources for the Primary Care Provider Please print these out for reference Resources for providers American Academy of Neurology www.aan.com Provides education and resources, such as guidelines for clinical
Resources for the Primary Care Provider Please print these out for reference Resources for providers American Academy of Neurology www.aan.com Provides education and resources, such as guidelines for clinical
Committee Approval Date: December 12, 2014 Next Review Date: December 2015
 Medication Policy Manual Policy No: dru381 Topic: Lemtrada TM, alemtuzumab Date of Origin: December 12, 2014 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
Medication Policy Manual Policy No: dru381 Topic: Lemtrada TM, alemtuzumab Date of Origin: December 12, 2014 Committee Approval Date: December 12, 2014 Next Review Date: December 2015 Effective Date: January
How to S.E.A.R.C.H. for the Right MS Therapy for You!
 How to S.E.A.R.C.H. for the Right MS Therapy for You! How to S.E.A.R.C.H. for the Right MS Therapy for You! Copyright Multiple Sclerosis Association of America, 2012. All rights reserved. This booklet
How to S.E.A.R.C.H. for the Right MS Therapy for You! How to S.E.A.R.C.H. for the Right MS Therapy for You! Copyright Multiple Sclerosis Association of America, 2012. All rights reserved. This booklet
Cost-effectiveness of teriflunomide (Aubagio ) for the treatment of adult patients with relapsing remitting multiple sclerosis
 for the treatment of adult patients with relapsing remitting multiple sclerosis") Cost-effectiveness of teriflunomide (Aubagio ) for the treatment of adult patients with relapsing remitting multiple sclerosis The NCPE has issued a recommendation regarding the cost-effectiveness of teriflunomide
Cost-effectiveness of teriflunomide (Aubagio ) for the treatment of adult patients with relapsing remitting multiple sclerosis The NCPE has issued a recommendation regarding the cost-effectiveness of teriflunomide
In considering the managed care perspective of
 MANAGED CARE CONSIDERATIONS IN TREATING MULTIPLE SCLEROSIS * Sheldon J. Rich, RPh, PhD ABSTRACT The lifelong treatment that is required for patients with multiple sclerosis (MS) presents numerous managed
MANAGED CARE CONSIDERATIONS IN TREATING MULTIPLE SCLEROSIS * Sheldon J. Rich, RPh, PhD ABSTRACT The lifelong treatment that is required for patients with multiple sclerosis (MS) presents numerous managed
The Nuts and Bolts of Multiple Sclerosis. Rebecca Milholland, M.D., Ph.D. Center for Neurosciences
 The Nuts and Bolts of Multiple Sclerosis Rebecca Milholland, M.D., Ph.D. Center for Neurosciences Objectives Discuss which patients are at risk for Multiple Sclerosis Discuss the diagnostic criteria for
The Nuts and Bolts of Multiple Sclerosis Rebecca Milholland, M.D., Ph.D. Center for Neurosciences Objectives Discuss which patients are at risk for Multiple Sclerosis Discuss the diagnostic criteria for
fingolimod, 0.5mg, hard capsules (Gilenya ) SMC No. (992/14) Novartis Pharmaceuticals UK
 SMC No. (992/14) Novartis Pharmaceuticals UK") fingolimod, 0.5mg, hard capsules (Gilenya ) SMC No. (992/14) Novartis Pharmaceuticals UK 08 August 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
fingolimod, 0.5mg, hard capsules (Gilenya ) SMC No. (992/14) Novartis Pharmaceuticals UK 08 August 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
Current and future options of MS treatment Prof. Dr. Karl Vass, AKH Wien
 Current and future options of MS treatment Prof. Dr. Karl Vass, AKH Wien European Health Forum, Gastein 6 th October 2010 Multiple Sclerosis is the most common neurological disorder in young Caucasian
Current and future options of MS treatment Prof. Dr. Karl Vass, AKH Wien European Health Forum, Gastein 6 th October 2010 Multiple Sclerosis is the most common neurological disorder in young Caucasian
Issues Regarding Use of Placebo in MS Drug Trials. Peter Scott Chin, MD Novartis Pharmaceuticals Corporation
 Issues Regarding Use of Placebo in MS Drug Trials Peter Scott Chin, MD Novartis Pharmaceuticals Corporation Context of the Guidance The draft EMA Guidance mentions placebo as a comparator for superiority
Issues Regarding Use of Placebo in MS Drug Trials Peter Scott Chin, MD Novartis Pharmaceuticals Corporation Context of the Guidance The draft EMA Guidance mentions placebo as a comparator for superiority
National Multiple Sclerosis Society. Disease Modification in Multiple Sclerosis. Current as of January 2, 2013
 National Multiple Sclerosis Society Disease Modification in Multiple Sclerosis Current as of January 2, 2013 Since 1993, the U.S. Food and Drug Administration (FDA) has approved several medications for
National Multiple Sclerosis Society Disease Modification in Multiple Sclerosis Current as of January 2, 2013 Since 1993, the U.S. Food and Drug Administration (FDA) has approved several medications for
TITLE: Treatment of Patients with Multiple Sclerosis: A Review of Guidelines
 TITLE: Treatment of Patients with Multiple Sclerosis: A Review of Guidelines DATE: 13 March 2013 CONTEXT AND POLICY ISSUES Multiple sclerosis (MS) is an unpredictable, often disabling disease of the central
TITLE: Treatment of Patients with Multiple Sclerosis: A Review of Guidelines DATE: 13 March 2013 CONTEXT AND POLICY ISSUES Multiple sclerosis (MS) is an unpredictable, often disabling disease of the central
Multiple Sclerosis (MS) is a disease of the central nervous system (including the brain and spinal cord) in which the nerves degenerate.
 is a disease of the central nervous system (including the brain and spinal cord) in which the nerves degenerate.") What is Multiple Sclerosis? Multiple Sclerosis (MS) is a disease of the central nervous system (including the brain and spinal cord) in which the nerves degenerate. A disease of the central nervous system
What is Multiple Sclerosis? Multiple Sclerosis (MS) is a disease of the central nervous system (including the brain and spinal cord) in which the nerves degenerate. A disease of the central nervous system
A neurologist would assess your eligibility and suitability for the DMTs.
 Choices Disease Modifying Treatments Disease modifying treatments (DMTs) are medications which modify the disease course. They target inflammation and are designed to reduce the damage caused by relapses.
Choices Disease Modifying Treatments Disease modifying treatments (DMTs) are medications which modify the disease course. They target inflammation and are designed to reduce the damage caused by relapses.
Supplementary Online Content
 Supplementary Online Content Burt RK, Balabanov R, Han X, et al. Association of nonmyeloablative hematopoietic stem cell transplantation with neurological disability in patients with relapsing-remitting
Supplementary Online Content Burt RK, Balabanov R, Han X, et al. Association of nonmyeloablative hematopoietic stem cell transplantation with neurological disability in patients with relapsing-remitting
Multiple sclerosis (MS) is a chronic, neurodegenerative
 is a chronic, neurodegenerative") FORMULARY MANAGEMENT Cost-effectiveness of Four Immunomodulatory Therapies for Relapsing-Remitting Multiple Sclerosis: Christopher Bell, MS; Jonathan Graham, MS; Stephanie Earnshaw, PhD; MerriKay Oleen-Burkey,
FORMULARY MANAGEMENT Cost-effectiveness of Four Immunomodulatory Therapies for Relapsing-Remitting Multiple Sclerosis: Christopher Bell, MS; Jonathan Graham, MS; Stephanie Earnshaw, PhD; MerriKay Oleen-Burkey,
A Definition of Multiple Sclerosis
 English 182 READING PRACTICE by Alyx Meltzer, Spring 2009 Vocabulary Preview (see bolded, underlined words) gait: (n) a particular way of walking transient: (adj) temporary; synonym = transitory remission:
English 182 READING PRACTICE by Alyx Meltzer, Spring 2009 Vocabulary Preview (see bolded, underlined words) gait: (n) a particular way of walking transient: (adj) temporary; synonym = transitory remission:
RELAPSE MANAGEMENT. Pauline Shaw MS Nurse Specialist 25 th June 2010
 RELAPSE MANAGEMENT Pauline Shaw MS Nurse Specialist 25 th June 2010 AIMS OF SESSION Relapsing/Remitting MS Definition of relapse/relapse rate Relapse Management NICE Guidelines Regional Clinical Guidelines
RELAPSE MANAGEMENT Pauline Shaw MS Nurse Specialist 25 th June 2010 AIMS OF SESSION Relapsing/Remitting MS Definition of relapse/relapse rate Relapse Management NICE Guidelines Regional Clinical Guidelines
The New England Journal of Medicine
 The New England Journal of Medicine Copyright, 2, by the Massachusetts Medical Society VOLUME 343 N OVEMBER 16, 2 NUMBER 2 RELAPSES AND PROGRESSION OF DISABILITY IN MULTIPLE SCLEROSIS CHRISTIAN CONFAVREUX,
The New England Journal of Medicine Copyright, 2, by the Massachusetts Medical Society VOLUME 343 N OVEMBER 16, 2 NUMBER 2 RELAPSES AND PROGRESSION OF DISABILITY IN MULTIPLE SCLEROSIS CHRISTIAN CONFAVREUX,
Understanding Relapse in Multiple Sclerosis. A guide for people with MS and their families
 Understanding Relapse in Multiple Sclerosis A guide for people with MS and their families Introduction You have been given this booklet because you have been diagnosed with Multiple Sclerosis (MS) and
Understanding Relapse in Multiple Sclerosis A guide for people with MS and their families Introduction You have been given this booklet because you have been diagnosed with Multiple Sclerosis (MS) and
Rational basis for early treatment in MS. Bonaventura Casanova Estruch Unitat d Esclerosi Múltiple Hospital Universitari la Fe València
 Rational basis for early treatment in MS Bonaventura Casanova Estruch Unitat d Esclerosi Múltiple Hospital Universitari la Fe València Bonaventura Casanova Department of Neurology University Hospital La
Rational basis for early treatment in MS Bonaventura Casanova Estruch Unitat d Esclerosi Múltiple Hospital Universitari la Fe València Bonaventura Casanova Department of Neurology University Hospital La
Disclosure Statement. Multiple Sclerosis: Current Trends in Treatment. Epidemiology of MS. Multiple Sclerosis. Viral Link to MS.
 Disclosure Statement Multiple Sclerosis: Current Trends in Treatment Member of Speaker s Bureau Biogen Idec Will discuss non FDA approved therapies Christine St Laurent MSN, RN, MSCN 19 th Annual Mud Season
Disclosure Statement Multiple Sclerosis: Current Trends in Treatment Member of Speaker s Bureau Biogen Idec Will discuss non FDA approved therapies Christine St Laurent MSN, RN, MSCN 19 th Annual Mud Season
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency London, 16 November 2006 Doc. Ref. CPMP/EWP/561/98 Rev. 1 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL INVESTIGATION OF MEDICINAL PRODUCTS FOR THE
European Medicines Agency London, 16 November 2006 Doc. Ref. CPMP/EWP/561/98 Rev. 1 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL INVESTIGATION OF MEDICINAL PRODUCTS FOR THE
- Patients treated with alemtuzumab in CARE-MS II were more than twice as likely to experience disability improvement compared to Rebif -
 PRESS RELEASE Significant Improvement in Disability Scores Observed in Multiple Sclerosis Patients Who Received Lemtrada TM* (Alemtuzumab) Compared With Rebif in Phase lll Trial - Patients treated with
PRESS RELEASE Significant Improvement in Disability Scores Observed in Multiple Sclerosis Patients Who Received Lemtrada TM* (Alemtuzumab) Compared With Rebif in Phase lll Trial - Patients treated with
Progress in the field: therapeutic improvements for all patients?
 Progress in the field: therapeutic improvements for all patients? Krzysztof Selmaj, Department of Neurology, Medical University of Lodz, PL Warsaw 15 May, 2015 Main features of MS Inflammation Demyelination
Progress in the field: therapeutic improvements for all patients? Krzysztof Selmaj, Department of Neurology, Medical University of Lodz, PL Warsaw 15 May, 2015 Main features of MS Inflammation Demyelination
Therapeutic Class Overview Multiple Sclerosis Agents
 Therapeutic Class Overview Multiple Sclerosis Agents Therapeutic Class Overview/Summary: Several biologic response modifiers are Food and Drug Administration (FDA)- approved for the treatment of relapsing-remitting
Therapeutic Class Overview Multiple Sclerosis Agents Therapeutic Class Overview/Summary: Several biologic response modifiers are Food and Drug Administration (FDA)- approved for the treatment of relapsing-remitting
Natalizumab (Tysabri)
") Natalizumab (Tysabri) Spirella Building, Letchworth, SG6 4ET 01462 476700 www.mstrust.org.uk reg charity no. 1088353 Natalizumab (Tysabri) Date of issue: July 2010 Review date: July 2011 Contents Section
Natalizumab (Tysabri) Spirella Building, Letchworth, SG6 4ET 01462 476700 www.mstrust.org.uk reg charity no. 1088353 Natalizumab (Tysabri) Date of issue: July 2010 Review date: July 2011 Contents Section
Department of Health. Rheynn Slaynt. Clinical Recommendations Committee
 Recommendation 06/13 Department of Health Rheynn Slaynt Clinical Recommendations Committee The Isle of Man Department of Health recommend Gilenya (fingolimod) as a HIGH PRIORITY - as an option for the
Recommendation 06/13 Department of Health Rheynn Slaynt Clinical Recommendations Committee The Isle of Man Department of Health recommend Gilenya (fingolimod) as a HIGH PRIORITY - as an option for the
1. Comparative effectiveness of alemtuzumab
 Cost-effectiveness of alemtuzumab (Lemtrada ) for the treatment of adult patients with relapsing remitting multiple sclerosis with active disease defined by clinical or imaging features The NCPE has issued
Cost-effectiveness of alemtuzumab (Lemtrada ) for the treatment of adult patients with relapsing remitting multiple sclerosis with active disease defined by clinical or imaging features The NCPE has issued
Clinical Trials of Disease Modifying Treatments
 MS CENTER CLINICAL RESEARCH The UCSF MS Center is an internationally recognized leader in multiple sclerosis clinical research. We conduct clinical trials involving the use of experimental treatments,
MS CENTER CLINICAL RESEARCH The UCSF MS Center is an internationally recognized leader in multiple sclerosis clinical research. We conduct clinical trials involving the use of experimental treatments,
peginterferon 63, 94 and 125 microgram solution for injection in pre-filled syringe (Plegridy ) SMC No. (1018/14) Biogen Idec Ltd.
 SMC No. (1018/14) Biogen Idec Ltd.") peginterferon 63, 94 and 125 microgram solution for injection in pre-filled syringe (Plegridy ) SMC No. (1018/14) Biogen Idec Ltd. 05 December 2014 The Scottish Medicines Consortium (SMC) has completed
peginterferon 63, 94 and 125 microgram solution for injection in pre-filled syringe (Plegridy ) SMC No. (1018/14) Biogen Idec Ltd. 05 December 2014 The Scottish Medicines Consortium (SMC) has completed