12/21/2009. AADEP Abnormal Findings in Normal People Lumbar and Thoracic Spine. Medical Imaging
|
|
|
- Shonda May
- 8 years ago
- Views:
Transcription
1 AADEP Abnormal Findings in Normal People Lumbar and Thoracic Spine Russell L. Travis M. D. Cardinal Hill Rehabilitation Hospital Lexington Back and Neck Clinic Medical Imaging Medical imaging is a growth industry. A 2008 report by the Government Accountability Office (GAO) noted that in just seven years through 2006 Medicare spending for imaging more than doubled to approximately 14 billion dollars. Most of the growth was in advanced imaging such as computed tomography (CT) and magnetic resonance (MR) imaging. Government e Accountability ty Office. Medicare e Part B Imaging g Services: Rapid Spending Growth and Shift to Position Offices Indicate Need for CMS to Consider Additional Management Practices. Washington DC. Government Accountability Office, June Publication: GAO In the particular case of lumbar spine imaging, MR images covered by Medicare increased 307% between 1994 and Deyo, R. A., Mirza, S. K., et. al., Overtreating Chronic Back Pain: Time to Back Off? JAM Board Fam Med. 2009, 22 (1) Spine imaging has come under particular scrutiny because both evidence and expert opinions suggest it is overused. The yield of unexpected findings is low: a ten-year Swedish study estimated that among adults younger than 50 years, one in 2,500 plain lumbar spine films uncovered something that was not expected on clinical rounds. Nachemson, A. L., Lumbar Spine: An Orthopedic Challenge. Spine 1976, (1) The yield of irrelevant findings is alarmingly high. Studying MR images in adults younger than 60 years with no history of back pain or sciatic, Boden and colleagues found that approximately half had bulging discs and degenerative discs and nearly a quarter had herniated discs. In adults older than 60 years, all findings were even more common, and both bulging and degenerative discs were almost ubiquitous. Similar studies by others have produced remarkably similar results. Jensen, M. C., et. al., Magnetic Resonance Imaging of the Lumbar Spine in People Without Back Pain. N Eng J Med 1994, 331 (200), Jarvik, J. J., et. al., Longitudinal Assessment of Imaging and Disability of the Back (LAIDBack) Study: Baseline Data. Spine 2001, 26 (10),
 and magnetic resonance (MR) imaging. Government e Accountability ty Office.")
2 When judged against guidelines, one-third to twothirds of spinal computed tomography imaging and MRI may be inappropriate. Rao, J. K., et. al., Can Guidelines Impact the Ordering of Magnetic Resonance Imaging Studies by Primary Care Providers for Low Back Pain? Am J Manag Care 2002; 8: One of the driving factors underlying the growth of imaging includes patient demand. McPhillips-Tangum C. A., et. al., Reasons for Repeated Medical Visits Among Patients with Chronic Low Back Pain. J Gen Intern Med 1996; 13: There is also the fear of lawsuits which is a compelling reason as well as financial incentives. Mitchell, J. M., Do Financial Incentives Linked to Ownership of Specialty Hospitals Affect Physicians Practice Patterns? Medical Care. 2008; 46: Plain radiographs and CT scans among asymptomatic individuals have shown similar high rates of anatomic abnormalities. van Tulder, M. W., et. al., Spinal Radiographic Findings and Nonspecific Low Back Pain. A Systemic Review of Observational Studies. Spine. 1997; 22 (4) Wiesel, S. W., et. al., A Study of Computer-Assisted Tomography. I: The Incidence of Positive CAT Scans in an Asymptomatic Group of Patients. Spine 1984, 9 (6): In a British randomized controlled trial, 421 patients with at least six weeks of back pain were randomized to receive plain radiography or not. Those who received radiography reported more pain and lower overall health status at three-month follow-up and were more likely to have seen their physician during follow-up. Kendrick, D., et. al., Radiography of the Lumbar Spine in Primary Care Patients with Low Back Pain, Randomized Controlled Trial. BMJ 2001, 322 (7283): In addition to lack of clinical benefit, lumbar imaging is associated with radiation exposure (radiography and CT), may not affect diagnostic or treatment plans, increases direct costs, and may lead to increased use of expensive but potentially unnecessary invasive procedures. 2

3 The notion that imaging might drive surgery is reinforced by studies of geographic variations. Spine imaging rates vary dramatically across geographic regions. Spine surgery rates are highest when spine imaging rates are the highest. This correlation held even if the images specifically associated with surgery were factored out. Lurie, J. D., Weinstein, J.N., et. al., Rates of Advanced Spinal Imaging and Spine Surgery. Spine 2003, 28 (6): Ash and colleagues studied 246 patients with acute back pain or sciatica with MR imaging and randomized them to receive the imaging results or not. Both groups improved over the subsequent year with similar clinical outcomes. However, self rated general health improved significantly more in the group that remained blind to the MR imaging results. However, even more important, increased frequency of lumbar MRI is associated with higher rates of spine surgery without clear differences in patient outcomes. Ash, L. M., et. al., Effects of Diagnostic Information, Per Se, on Patient Outcomes in Acute Radiculopathy and Low Back Pain. Am J Neuroradio. 2008, 28 (6): Probably the most important fact about MR imaging is that in a randomized controlled trial comparing MR imaging with plain radiography as the first imaging test, patients in the two groups had equivalent health outcomes, but those receiving MR imaging were more than twice as likely to undergo surgery in the subsequent year. Kendrick, D., et. al., Radiography of the Lumbar Spine in Primary Care Patients with Low Back Pain, Randomized Controlled Trial. BMJ 2001, 322 (7283): Jarvik, J. G., et. al., Rapid Magnetic Resonance Imaging vs. Radiographs for Patients with Low Back Pain. A Randomized Controlled Trial. JAMA 2003, 289 (21)

4 The question arises, Could there be any harm associated with spine imaging? Beyond the small risk of carcinogenesis or mutagenesis, there is evidence that simply knowing about some abnormality in the spine may adversely affect patient behavior. Someclinicians still dolumbar spine imaging routinely or without a clear indication possibly because they are able to reassure their patients and themselves to meet patient expectations about diagnostic tests, to identify specific anatomical diagnosis for low back pain, or because reimbursement structures provide financial incentives to image. Mitchell, J. M., Do Financial Incentives Linked to Ownership of Specialty Hospitals Affect Physicians Practice Patterns? Medical Care. 2008; 46: Patient Satisfaction: For many clinicians, the conundrum is this: despite the strong evidence against routine spinal imaging, patients like it and sometimes demand it. Patients are often desperate for an explanation of their pain, and visual evidence is particularly compelling. Rhodes, L. A., et. al., The Power of the Visible: The Meaning of Diagnostic Test in Chronic Back Pain. Soc Sci Med. 1999, 48 (9) In the British randomized controlled trial of plain radiography, those in the radiography group were significantly more satisfied with their care, despite having worse outcomes. (Ash, et. al.) In the randomized controlled trial of MR imaging versus plain radiography, those in the MR imaging group felt significantly more reassured and were more satisfied with their care, despite no advantage in outcomes. (Chou, R., et. al.) In a survey of US physicians, 36% said they would order an MR image for a first episode of acute back pain (two days) that began during work around the house if the patient was insistent even after explaining that the test was unnecessary. Campbell, E. G., et. al., Professionalism in Medicine, Results of a National Survey of Physicians. Ann Intern Med. 2007, 147 (11): When disability claims are involved, attorneys and patients are likely to insist on advance imaging regardless of clinical guidelines and the likelihood of discovering an anatomic anomaly is high. Dr. Richard Deyo said, The task is to convince out patients that more is not always better. Deyo, R. A., Imaging Idolatry: The Uneasy Intersection of Patient Satisfaction, Quality of Care, and Overuse. Arch Intern Med/Vol. 169 (No. 10): , May 25,

5 Imaging strategies for low-back pain: systematic review and meta-analysis Roger Chou, Rongwei fu, John A. Carrino, Richard Deyo. Lancet 2009;373: These authors investigated the effects of routine, immediate lumbar imaging versus usual clinical care without immediate imaging on clinical outcomes in patients with low back pain and no indication of serious underlying conditions. The authors analyzed randomized controlled trials that compared immediate lumbar imaging (radiography, MRI, or CT) versus usual clinical i l care without immediate imaging for low back pain. These trials reported pain or function (primary outcomes), quality of life, mental health, overall patient-reported improvement (based on various scales), and patient satisfaction in care received Patient Outcomes: The ultimate goal of imaging is to uncover abnormalities that guide the choice of specific therapies, improving patient outcomes. Unfortunately, spine imaging in patients with no indication of underlying systemic disease or major neurologic compromise appears not to improve patient outcomes. A systematic review of these studies identified six randomized trials comparing some spine imaging strategy to usual care without imaging. These trials involve 804 patients and fail to show any advantage of imaging with regard to pain or function in either the short term or the long term. 5
 versus usual clinical i l care without immediate imaging for low back pain.")
6 The purpose of this systematic review and meta-analysis was to see whether immediate routine lumbar spine imaging is more effective than usual clinical care without immediate lumbar imaging in patients with low back pain and no features suggesting a serious underlying condition. The authors included randomized controlled trials that compared immediate routine lumbar imaging (or routine provision of imaging findings) versus usual clinical care without immediate lumbar imaging (or not routinely providing results of imaging) for low back pain without indications of serious underlying conditions. Six trials met inclusion criteria, four reported in six publications assess lumbar radiography, and two reported in four publications assessed MRI or CT. 1,804 patients were randomly assigned in the six trials. Duration of follow-up ranged from three weeks to two years. Djais and Kalim Modic, et. al., and Ash, et. al. Gilbert, et. al. Kerry, et. al. Interventions Numbers of Exclusion criteria Duration of low Signs of Duration Main outcome measures Country randomized related to markers back pain episode nerve root of patients for serious entrapment follow-up underlying conditions or spinal stenosis Immediate lumbar 101 Age >55 years. <3 months Excluded 3 weeks Pain: VAS (0 to 10). Indonesia spine radiography vs History of cancer. (median 4 weeks, Back-specific function: RDQ usual clinical care Unexplained weight IQR 2 to 9.5) (0 to 24). without lumbar loss or fever. Quality of life: EuroQol-5D radiography Use of oral (0-59 to 1). corticosteroids. Overall improvement History of (dichotomous): overall tuberculosis. assessment (much improved Intravenous drug vs other). use. Symptoms or signs of cauda equina syndrome. Lumbar MRI in all 246 Signs or symptoms <3 weeks 39% 6 weeks Pain: VAS (0 to 10) and SF- USA patients, notification of cauda equina and 36 bodily pain. of results within 48 h syndrome. 1 year Back-specific function: RDQ vs notification only if Polyradiculopathy. (0-24). clinically indicated. History of blunt Mental health: SF-36 mental trauma, previous low health subscale (0 to 100). back surgery. Overall results Use of oral or (dichotomous): patient parenteral symptom assessment (very corticosteroids. pleased or better) Immediate lumbar 782 Need of immediate 18% <3 months 32% 8 months Pain: SF-36 bodily pain. UK MRI or CT vs usual referral for imaging 42% and 2 years Back-specific function: clinical care without (eg, surgical 3-12 months Aberdeen low back pain advanced imaging intervention, those 40% >12 months score (0 to 100) with red flags Quality of life: EuroQol 5D [definition of red (0-59 to 1) flags not reported]) Mental health: SF-36 mental health subscale (0 to 100). Immediate lumbar 153 Not specified 70% <8 weeks Not 6 weeks Pain: SF-36 bodily pain. UK spine radiography vs (clinicians informed reported and Back-specific function: RDQ usual clinical care of the Royal College 1 year (0 to 24) without lumbar of Radiologists 1995 Quality of life: EuroQol radiography guidelines but subjective score (0 to 100) randomization left to Mental health: SF-36 mental their discretion) health subscale (0 to 100). Patient satisfaction: categorical scale (four categories, dissatisfied to very satisfied) Kendrick, et. al. Deyo, et. al. Interventions Numbers of Exclusion criteria Duration of low Signs of randomized related to markers back pain episode nerve root patients for serious entrapment underlying conditions or spinal stenosis Immediate lumbar 421 Age >55 years. >6 weeks and <6 44% spine radiography vs Chronic (>6 months) months (lower limb usual clinical care low back pain. (median 10 pain) without lumbar Unexplained weight weeks, IQR7 to radiography loss or fever. 15) Use of oral steroids. History of cancer, tuberculosis, or HIV infection. Signs or symptoms of cauda equina syndrome. Immediate lumbar 101 Age >50 years. Mean 2 weeks 24% nerve spine radiography vs Temperature root irritation educational >37.8 C. intervention plus Substantial trauma. lumbar spine Neuromotor deficits. radiography if no Unexplained weight improvement within 3 loss. weeks Alcohol or parenteral drug abuse. History of cancer. Use of corticosteroids. Duration of follow-up 3 months and 9 months 3 weeks and 3 months Main outcome measures Country Pain: VAS (0 to 10) UK Back-specific function: RDQ (0 to 24) Quality of life: EuroQol 5D (0-59 to 1) Overall results: (dichotomous): presence of pain (no longer has pain vs pain still present. Patient satisfaction: patient satisfaction score (9 to 27) Pain: categorical scale (1 to USA 6) Function: sickness impact profile (0 to 100) Overall results: (dichotomous): return to normal activities (returned to normal activities vs not returned to normal activities) Patient satisfaction: patient satisfaction score (9 to 27) VAS = visual analogue scale. RDQ = Roland disability questionnaire. Table 1: Characteristics of Randomized Trials. 6
 for low back pain without indications of serious underlying conditions.")
7 Immediate lumbar imaging and usual clinical care without imaging did not differ for short-term or long-term quality of life, mental health, and overall improvement. For quality of life, results slightly favored non-immediate imaging. In the trial that reported extended (two year) follow-up data, immediate MRI or CT was not better than usual clinical care without immediate imaging on any of the scores in unadjusted analyses. The meta-analysis of randomized controlled trials showed that immediate routine lumbar spine imaging in patients with low back pain and no features suggesting serious underlying conditions do not improve clinical outcomes compared with the usual clinical care without immediate imaging. In addition, pooled estimates were small or close to zero, and in some cases, slightly favored the non-imaging strategy. Bottom Line In addition to lack of clinical benefit, lumbar imaging is association with radiation exposure (radiography and CT), may not affect diagnostic or treatment plans, increases direct costs, and may lead to increased use of expensive but potentially unnecessary invasive procedures. Our study confirms that clinicians should refrain from routine, immediate lumbar imaging in patients with low back pain and without features suggesting a serious underlying condition. Conclusions of Systematic Review and Meta-analysis Lumbar imaging for low back pain without indications of serious underlying conditions does not improve clinical outcomes. Therefore, clinicians should refrain from routine, immediate lumbar imaging in patients with acute or subacute low back pain and without features suggesting a serious underlying condition. 7

8 In addition to lack of clinical benefit, lumbar imaging is association with radiation exposure (radiography and CT), may not affect diagnostic or treatment plans, increases direct costs, and may lead to increased use of expensive but potentially unnecessary invasive procedures. 1. Djais, N., et. al., The Role of Lumbar Spine Radiography in the Outcomes of Patients with Simple Acute Low Back Pain. APLAR J of Rheumatology 2005; Vol. 8, Issue 1, Modic, M. T., et. al., Acute Low Back Pain and Radiculopathy: MR Imaging Findings and their Prognostic Role Effect on Outcome. Radiology 2005; 257: Ash, L. M., et. al., Effects of Diagnostic Information, Per Se, on Patient Outcomes and Acute Radiculopathy and Low Back Pain. Am J Neuroradiol; 2008; 29: Gilbert, F. J., et. al., Low Back Pain: Influence of Early MR Imaging or CT on Treatment Outcome Multicenter Randomized Trial. Radiology 2004; 231: Gilbert, F. J., et. al., Does Early Imaging Influence Management and Improve Outcome in Patients with Low Back Pain? A Pragmatic Randomized Controlled Trial. Health Technol Assess (Eng) 2004; 8: Kerry, S., et. al., Radiography for Low Back Pain: Randomized Controlled Trial and Observational Study in Primary Care. Br J Gen Pract 2002; 52: Kerry, S., et. al., Routine Referral for Radiography of Patients Presenting with Low Back Pain: Is Patients Outcome Influenced by GPs Referral for Plain Radiography? Health Technol Assess (Eng) 2000; 4: Kendrick, D., et. al., Radiography of the Lumbar Spine in Primary Care Patients for Low Back Pain: Randomized Controlled Trial. BMJ 2001; 322: Kendrick, D., et. al., Role of Radiography in Primary Care Patients with Low Back Pain of at Least Six Weeks Duration: A Randomized (Unblinded) Controlled Trial. Health Technol Assess (Eng) 2001; 5: Deyo, R. A., et. al., Reducing Roentgenography Use: Can Patient Expectations be Altered? Arch Intern Med 1987; 147: There are six other randomized controlled trials involving a total of 804 patients from primary care without features suggesting a serious underlying disease, comparing some form of lumbar spine imaging with none. In these series, imaging was not associated with an advantage in subsequent pain, function, quality of life, or overall improvement. Djais, N., et. al., The Role of Lumbar Spine Radiography in the Outcomes of Patients with Simple Acute Low Back Pain. APLAR Journal Rheumatology 2005; 8: Gilbert, F. J., Low Back Pain: Influence of Early MR Imaging or CT on Treatment and Outcome Multicenter Randomized Trial. Radiology 2004; 231: Kendrick, D., et. al., Radiography of the Lumbar Spine in Primary Care Patients with Low Back Pain: Randomized Controlled Trial. BMJ 2001, 322 (7283):

9 Gilbert, Fiona, J., et. al., Low Back Pain: Influence of Early MR Imaging or CT on Treatment Outcome Multicenter Randomized Trial. Radiology. 2004; 231: Purpose: To establish whether early use of magnetic resonance (MR) imaging or computed tomography (CT) influences treatment and outcome of patients with low back pain (LBP) and whether it is cost effective. This is a multicenter randomized study, two imaging policies for LBP were compared in 782 participants with symptomatic lumbar spine disorders who were referred to orthopedists or neurosurgeons. Participants were randomly allocated to early or delayed imaging groups. Delayed selective imaging referred to imaging restricted to patients in whom a clear clinical need subsequently developed. Main outcome measures were multiple tests, scores, and healthcare resource use at 8 and 24 months after randomization. One of the primary measurements was the Aberdeen Low Back Pain (ALBP) score. Conclusion: Early use of imaging does not appear to affect treatment overall. Decisions about the use of imaging depend on judgments concerning whether the small observed improvement in outcome justifies additional cost. The same conclusion applies to CT imaging. Elkayam, O., et. al., The Lack of Prognostic Value of Computerized Tomography Imaging Examinations in Patients with Chronic Nonprogressive Back Pain. Rheumatol Int 1996; 16: The 1994 Agency For Health Care Policy and Research (AHCPR) guidelines made recommendations against lumbar MR imaging in the first month of acute low back pain in the absence of so called red flags suggestive of a serious underlying condition (such as cancer, infection, or cauda equina syndrome). Some guidelines have actually advised against lumbar imaging for chronic low back pain without red flags 9

10 Some Current Guidelines for MRI Use 1. Occupational Medicine Practice Guidelines (ACOEM- Revised 2007 and currently) 2. ODG Treatment in Worker s Comp Clinical Practice Guidelines : For the Diagnosis and Treatment of LOW BACK PAIN. Work Safe, Workers Comp Board of B. C. The Thoracic and Lumbar Disc (Cervical is Another Talk!) Disc Herniations Annular Tears Disc Bulges Degenerative Disc Disease Normal Abnormal Abnormal Findings Cervical, Thoracic and Lumbar Discs in healthy people without symptoms Two types of studies 1. Imaging studies of asymptomatic people 2. Studies of people with symptoms but studies reveal abnormalities not related to the symptoms 10
 Disc Herniations Annular Tears Disc Bulges Degenerative Disc Disease Normal Abnormal Abnormal Findings Cervical, Thoracic and Lumbar Discs in healthy people without")
11 With discography, myelography, CT, MRI and studies comparing these techniques with each other 15%-81% of asymptomatic people with abnormalities D.L. Kent, et. al.,1992, H. Paajanen, et. Al., 1989 N.C. Powell, et. al., 1986 J.W. Simmons,et.al., 1991 T.R. Walsh, et. Al., 1990 S.W. Wiesel, et. al,., 1984 K.B.Woodall, et.al., 1995 Boden et. Al., 1990 Stadnik, et. Al., 1998 The Thoracic Spine Findings in Asymptomatic People Herniation....37% Bulging g disc 53% Annular tear 58% Deformation of spinal cord by disc..29% Scheurmann end-plate irregularities or kyphosis..38% Degenerative changes...56% Wood KB et al., Magnetic Resonance Imaging of the Thoracic Spine. Journal of Bone and Joint Surgery (Am). 1995;77A (4): Asymptomatic Thoracic Disc 11
. 1995;77A (4):1631-1638. Asymptomatic Thoracic Disc 11")
12 THE LUMBAR SPINE: Notable studies of the lumbar spine in asymptomatic individuals include: Boden, et. al., 1990; Hitselberger, et. al., 1968; Jensen, et. al., 1994; McRae, et. al., 1956; Weinrab, et. al., 1989; Paajanen, et. al.,1989; Wiesel, et. al., 1984; Stadnik, et. al., Lumbar Spine Oblique (Partial Rotation) 12
 12")
13 Lateral Sagittal view Images of Spine for Normal Volunteers Herniation of the lumbar disc is found in 25 to 50% of asymptomatic subjects Bulges in up to 81% of asymptomatic people Extrusion of the disc material is found in 1 to 18% Definitions Protrusion was defined as a focal or asymptomatic extension of the disc beyond the interspace. Extrusion as a more extreme extension of the disc beyond the interspace. Bulge A circumferential extension of the disc beyond the interspace around the end plates 13

14 bulge Bulge 14
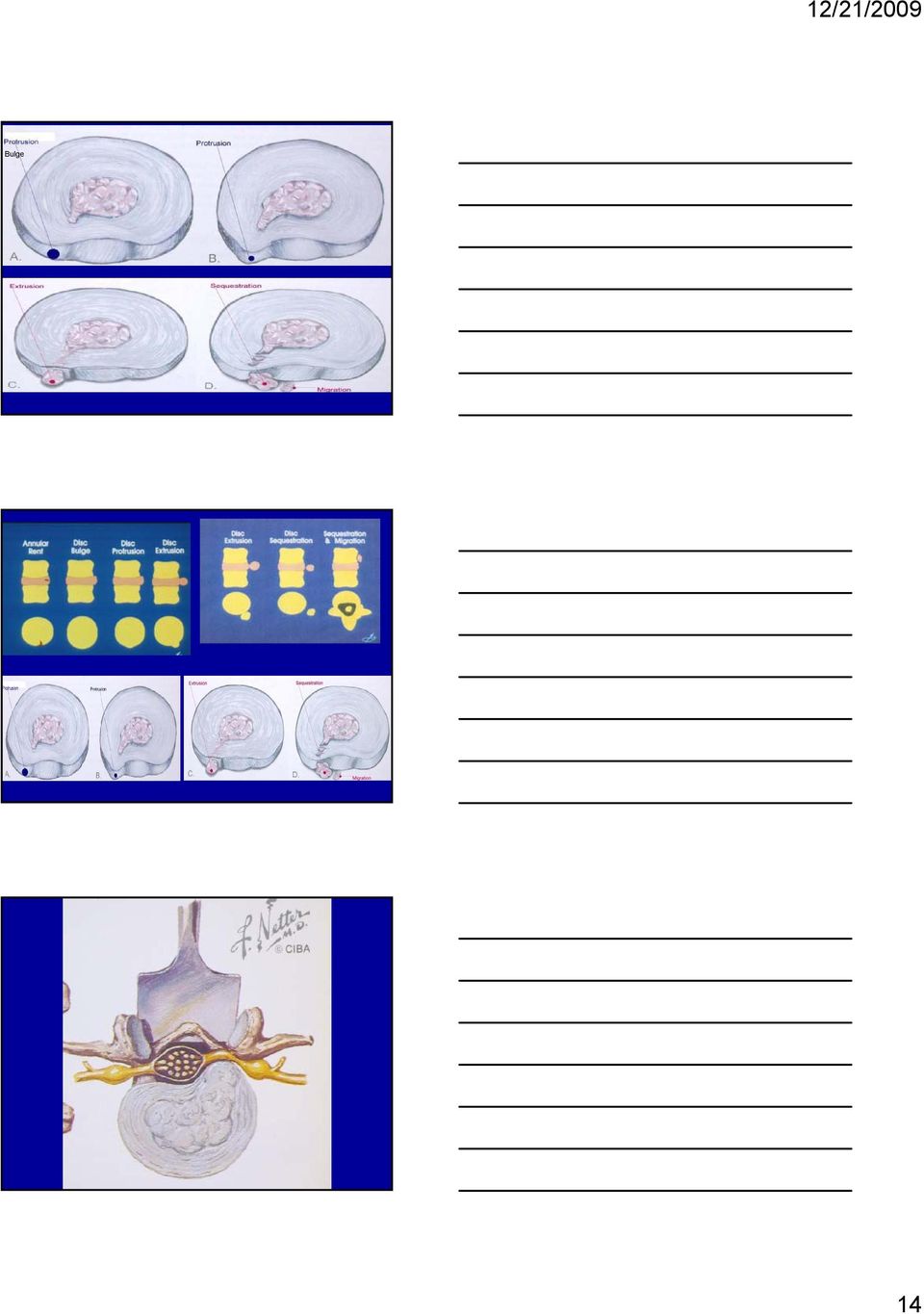
15 Disc Herniation/migration/Sequestration Disc Herniation 15

16 Caudal Migrated Fragment Sequestered Fragment-Migrated Axial-Fragment 16

17 Fragment Migrated Caudally Free Fragment Migrating Sequestered Fragment 17

18 Far Lateral Disc Far Lateral HNP 18

19 Far Lateral Disc Exiting v. Traversing Root Know the direction of saggital images (Right to Left Here) Negative on right Negative at midline 19
 Negative on right Negative at")
20 Large hnp on left parasagittal Large hnp left axial Why are most hnp Parasagittal (lateral)? 20

21 Cauda Equina Syndrome Herniations- Bulges - Protrusions Boden found a 24% prevalence of herniated nucleus pulposus on the MR images of 67 asymptomatic individuals. 21% of volunteers 20 to 39 years of age 36% for subjects older than 60 years. Jensen, et. al., reported 27% prevalence of protrusions 1% extrusion in 90 asymptomatic subjects. Lumbar Disc Herniations McRae Performed autopsy studies on persons who were free of back pain prior to death. He found a 33% prevalence of posterior disc protrusions. Wiesel found that the lumbar spine in asymptomatic individuals demonstrated abnormalities on MR images in 35%. He Found herniated discs in 19.5% of the people under the age of 40 and greater than 27% in those over 40 years of age. He studied only the L4-5 and L5-S1 disc. Weinrab, in asymptomatic females found 54% with bulges or herniations at one or more disc spaces. 21
22 Lumbar MRI Studies of Asymptomatic Subjects 21 Studies Disc Degeneration 30y old 30% 60y old 100% Disc Bulging 50-81% Disc Prolapse 40-70% Bulging Disc & Annular Tear The Right Diagnosis!? 22
23 Degenerative Disc Disease As the disc loses some of its shock absorber capacity, more load is transferred from the previously gelatinous nucleus pulposus to the peripheral annulus. Narrowing of the disc space occurs with the decreased volume of the intervertebral disc.. Weakening of the annulus may lead to bulging of the disc Bulging Discs are Normal Phenomena Intervertebral Disc ( Bulging Discs Not Abnormal) Bending of the spine, (flexion, extension or lateral bending) causes an eccentric ti deformation in the disc Fluid pressure has 2 components, hydrostatic and osmotic. Axial loading=fluid out of NP After axial loading the osmotic pressure causes fluid to flow back into the disc, restoring its height. Bulging discs seen in 81% of normal Asx. persons 23
24 Intervertebral Disc ( Bulging Discs-Not Necessarily Pathologic) The normal nucleus is under pressure, even at rest, and this increases to balance axial loads, which produces tension and slight bulging of the annulus. The disc bulge is normal and reflects the balance between the mechanical forces applied to the spine and the osmotic forces in the nucleus. There is about 20% diurnal variation in disc height and volume. During the day, load increases, overcomes osmotic forces and disc is squashed. Night-osmotic force restores disc height Bulging Disc Bulging Disc 24
25 Lumbar Disc Bulges/Protrusions Most authors report abnormalities as a prevalence increasing with age. Boden found bulging in 34% of the 20 to 39 year range and 50% in the age groups. For protrusions, 24% for volunteers, 29 to 39 years of age, and 36% for subjects older than 60 years. Stadnik also found a relationship to age. Total prevalence of bulging disc was 81%. 33% had at least one disc protrusion. The frequency of protrusion increased as a function of age. 16% of volunteers aged 30 years or younger and 80% of the volunteers older than 60 years had disc protrusions. Summary About one third (36%) of asymptomatic subjects over the age of 20 years have a normal disc at every level. 38% have an abnormality in more than one disc level. The prevalence of bulges and protrusions was higher at the L4-5 and L5-S1 spaces. Up to 80% 67% of the people 50 years or older had multiple abnormalities Bulging-Protruded discs in Asymptomatic People Stadnik 81% Boden JBJS 1990 %54% Jensen NEJM % Weinrab Radiology % 25
26 Do protrusions and herniations in asymptomatic people predict future problems? MRIs were done, and the patients were followed for five years and MRI repeated. Disc degeneration increased, but neural compromise and symptoms did not. The MRI did not predict episodes of low back pain. In Another study of 67 asymptomatic volunteers, MRIs were done in 1989 and a second MRI in 1996 (seven years later). Results: Findings of herniated nucleus pulposus, degeneration increased with time (age) Degeneration, bulge, herniated nucleus pulposus did not predict future symptoms (1989 MRI) Did not correlate with current symptoms (1996 MRI ) Norbert Boos, Natural History of Individuals with Asymptomatic Disc Abnormalities and Magnetic Resonance Imaging, Spine. 2000; 25 (12): 1482 The Back Letter in 1998; (8): The Back Letter, 13., #5, 49 Epidemiology of Low Back Pain Compounding this problem of common abnormalities in asymptomatic people is the overall incidence of low back pain in the general population The annual incidence of lifetime prevalence or lifetime incidence of low back pain varied from 1% to 5%. 3.7% experienced low back pain for two weeks or more duration. 1.5% with low back pain experienced sciatica. Of those with sciatica, over 90% had complete recovery by 2 weeks to 30 days with conservative, nonoperative treatment. Dayo, R. A., Tsui-Wu, Y. J.: Descriptive Epidemiology of Low Back Pain and Its Related Medical Care in the United States, Spine. 12: 264, Fromoier, John W., et. al., An Overview of the Incidence and Cost of Low Back Pain, Orthopedic Clinics North America. Vol. 22, No. 2, April 1991, Recent data: Expenditures and Health Status among Adults with Back and Neck Problems Brook I. Martin, Richard A. Deyo, et, al. JAMA, Feb. 13,2008-Vol299, No.6: Back and neck problems are among symptoms most commonly encountered in clinical practice. In a 2002 survey of US adults, 26% reported low back pain and 14% reported neck pain in the precious 3 months. Low back pain alone counted for approximately 2% of all physician office visits Only routine examinations, hypertension, and diabetes resulted in more office visits. LBP is the fifth most common reason for all physician visits in the U.S. 26
27 MRI availability and use: The number of MRI scanners in the U. S. more than tripled during from 7.6 to 26.5 per million people Early MRI frequently detects low back abnormalities, and sometimes that information is valuable, but often the abnormalities detected are not the cause of the symptoms. Low back MRI is frequently implicated in treatment cascades, in which the use of advanced imaging produces findings that call for follow-up and set the stage for treatments, particulary back surgery, that are of uncertain efficacy for many patients. Expenditures and Health Status among Adults with Back and Neck Problems Brook I. Martin, Richard A. Deyo, et, al.jama, Feb. 13,2008-Vol299, No.6: MRI Availability and Use per MS (318 Metropolitan Statistical Areas) Between 2000 and 2006 MRI was one of the fastest growing sets of services paid for under Medicare Part B physician fee schedule. 1999, median number of units per million population= median had grown to 22.4 MSAs with largest growth in MRI units also had largest growth in LB MRIs billed to Medicare Each additional MRI added between 1999 and 2004 is associated with about 40 additional MRI per additional scanner among all Medicare beneficiaries with nonspecific LBP MRI Availability and Use of Surgery Adding an additional MRI scanner is associated with about 1 additional surgery in the sample which suggests about 5 additional in the whole population of traditional Medicare patients with nonspecific LBP. Authors extrapolate to entire population of Medicare and estimate that 1,825 fewer back surgeries would have taken place if all the LBP patients living in the highest MRI availability areas in had instead lived in the lowest MRI-availability areas. 27
28 MRI Connection to Surgery Guidelines since 1994 have recommended delaying MRI use for most patients for at least 1 month, because the natural history of more than 90 percent of LBP is spontaneous improvement within 4 weeks. Expanding MRI availability leads to increased use of MRI for LBP, and the high frequency of incidental findings on MRI scans may induce a cascade 0f subsequent use of LBP care, including surgery. Prevalence Low Back Pain Last Month Age Country Yes% Sweden France Switzerland, Finland Swe, Den, GB GB, Ger, Swe, Fin Austria GB, Holland Sweden Sweden 40 Does the Accelerated Rates of Surgery Indicate A Growing Back Pain Epidemic? Survey of Northern Germany taken a year apart. Overall prevalence of back pain today % One year prevalence 75.3% Prevalence of severe pain 9.9% % One year prevalence 73.8% Prevalence of severe pain 10.2% Angelika Huppe et al., European Journal of Public Health, 2006;September 23;epub ahead of print version. 28
29 Epidemiology of Low Back Pain (More recent survey) About ¼ of U.S. adults reported LBP in the last 3 months 41% of American adults between the ages of 26 and 44 years had back pain in the last 6 months. Several European studies of the prevalence of LBP in the last month produced estimates that center around 40% The proportion of all physician visits related to LBP has changed very little in the past decade. In contrast there is evidence of increasing use of back surgery, and injection procedures. One hypothesis would be that the prevalence of back pain is relatively stable but therapy is becoming more intensive, with greater per patient use of these treatments. Richard Deyo et al., Back Pain Prevalence and Visit Rates. Estimates from U.S. National Surveys, Spine 31: 23; How Bulging Disc Become a Problem! Jan 2000 Aug 2001 MVA 4/26/02 MRI 6/20/02 MVA 4/26/02 Surgery 7/10/02 MRI 9/1/02 29
30 Annular Tear/Bulge Identified as an area of hyperintensity in the posterior annulus Disc with bright signal in annular fissure represents degenerative changes found in 14 to 33% of asymptomatic subjects. Annular Tear/Bulge Identified as an area of hyperintensity in the posterior annulus Annular Tear 30
31 Annular Tear Annular Tears Pain?-IDET? Annular tears are frequently identified on MR images in patients without low back pain or sciatica. The annulus fibrosis is innervated by the recurrent meningeal nerve and by the small branches of the ventral ramus of the somatic spinal nerve. Annular tears, however, are frequently found in asymptomatic populations. Annular Tears Yu and others in 1989 reported on autopsy examinations of 31 cadavers: In a majority of adult disc, transverse and concentric tears are present in the annulus, whether or not changes are evident in the nucleus pulposus. These tears are probably incidental findings. Carl Hirsh in 1952 examined 120 lumbar discs in autopsies of people with no history of low back pain or sciatica. Hirsh and colleagues found the prevalence of radial and annular tears to be 40% for people between the ages of 50 and 60 years and 75% for those over 60 years of age Jensen, in her studies of younger asymptomatic people found annular tears in 14%. Hirsh, Carl, et. al., Studies in Structural Changes in the Lumbar Annulus Fibrosis, Acta Orthopedica Scand. 1952, 22 ( ): Yu, Schi Wei, et. al., Radiology. 1989; 170:
32 Changes in the Intervertebral disc By age of 50 years 95% 0f people have evidence of degeneration: Water and proteoglycan content of nucleus pulposis decreases Water and proteoglycan content of annulus decreases Collagen fibers of annulus become distorted Tears may occur in lamella, may result in loss of annular strength Disc loses its normal height and volume Discography & High Intensity Zone Spine 2000; 25 (23): Some literature suggests high intensity zone on T2 MRI correlates with pain on discography. Study: 42 symptomatic patients 54 asymptomatic volunteers, all had discography. Presence of 1 high intensity zone on MRI Symptomatic patients 59 % Asymptomatic Volunteers 24 % Discography & High Intensity Zone Spine 2000; 25 (23): If Psychometrics were NORMAL, 50 % of discs with a HIZ were painful on discography. If Psychometrics were ABNORMAL, 100 % of discs with a HIZ were painful. Conclusion: The presence of a high intensity zone does not reliably indicate the presence of symptomatic internal disc disruption. 32
33 "Annular Tears and Disc Herniation: Prevalence and Contrast Enhancement on MRI Images in the absence of Low Back Pain or Sciatica" Journal of Radiology;Neuroradiology Tadeuszw Stadnik, M.D., et al. Annular Tears Stadnik: Asymptomatic=56% Conclusion: In the majority of the adult discs, transverse and concentric tears are present in the annulus, whether or not degenerative changes were evident in the nucleus pulposis, these tears are incidental findings. There was no correlation between the discovery of annular tear and the history of low back pain or sciatica. Autopsy studies, asx people: Yu, Hirsch,-found 40%-50% between ages 50 & % between ages of Stadnic,Tadeuszw,et al. Annular Tears and disc herniation: Prevalence and contrast enhancement on MRI images in the absence of low back pain or sciatica. Journal of Radiology; Neuroradiology, Degenerative Disc Disease 33
34 Degenerative Disc Disease The term degenerative disc disease is like whiplash, probably an unfortunate name for a normal process. It refers to the loss of normal tissue structure and function as the result of the aging process. The normal aging of tissue implies that an accumulation of changes will occur to the anatomy over a course of time and is not usually associated with symptoms. Cadaver studies reveal lumbar DDD begins in the second decade for males and in the third decade in females. By age 50, 97% of all lumbar discs will demonstrate some evidence of DDD Miller JAA, et.al. Lumbar disc degeneration: correlation with age, sex, and spine level in 600 autopsy specimens." Spine 1988;13(2): Degenerative Disc Disease Proteoglycans, the water binding proteins in the nucleus pulposus, are replaced by collagen, and cracks and fissures then appear in the annulus. The water content in young people is 90%. In older people, the water content may be less than 25%. Vertebra and Intervertebral disc of a young child 34
35 The Vertebral Body Vertebral loads are conducted from the disc through the vertebral endplate to the body of the vertebral body. Transmittal via 2 pathways: 1. Cortical-small portion 2. Spongy trabecular bone-major load Trabeculla in cancellous bone recover after load removed Disc Nutrition Endplate formed in concave surfaces on ends of vertebral bodies. Thickest near cortical rim-thinnest in central region 2 layers: as transition between disc and vertebra Inner bony layer Outer cartilaginous ag layer Nutrition to disc diffuses across surface from bony layer. Degeneration of endplates may affect nutrition to disc and affect motion segment 35
36 Degenerative Disc Disease Despite a very high correlation between radiographic or MRI evidence of DDD and increasing age, no clinical correlation exists with pain. Several studies have demonstrated DDD in a high percentage of asymptomatic individuals. Hult found radiographic evidence of DDD in 90% of lumbar radiographs in a group of year old patients. Only 47% reported any history of low back pain. Hult L. Cervical, dorsal, and lumbar spine syndromes. Acta Orthop Scand [suppl 17] 1954: Degenerative Disc Disease There are eight randomized control studies and two reviews from the 1950s, 1960s, 1970s, and 1980s that showed very little relationship between clinical symptoms and radiological signs of degeneration. 1. Fullenlove, TM, Williams, AJ: Comparative Roentgen Findings in Symptomatic and Asymptomatic Backs, JAMA 168: , Horal, J: The Clinical Appearance of Low Back Pain Disorders in the City of Bothenburg, Sweden. Acta Orthop Scand (Suppl) 118, 1-109, Hult, L: The Munkfors Investigation. Acta Orthop Scand (Suppl) 16, La Rocca, H., MacNab, I: Value of Pre-Employment Radiographic Assessment of the Lumbar Spine. Can Med Assoc J 101: , Magora, A., Schwartz, A.: Relationship Between the Low Back Pain Syndrome and X-ray Findings. Scand J Rehabili Med 8: , Mensor, M. C., Duvall, G: Absence of Motion at the Fourth and Fifth Lumbar Interspaces. J Bone Joint Surg 41A: Splithoff, C. A.: Lumbosacral Junction: Roentrographic Comparison of Patients With and Without Backache. JAMA 152: , Torgeson, W. R., Dotler, W. E.: Comparative Roentrographic Study of the Asymptomatic and Symptomatic Lumbar Spine. J Bone Joint Surg 58A: , 1976 Degenerative Disc Disease Review Articles 1. Meyer, A: Progress in Teaching Psychiatry. JAMA 69: , Wiltse, L. L: The Effect of the Common Anomalies of the Lumbar Spine Upon Disc Degeneration and Low Back Pain. Orthop Clin North Am 2: ,
37 Disc Degeneration Stadnik et. al., in 1998 also studied degenerative changes in asymptomatic persons. The authors defined disc degeneration as: Mild a decrease in signal intensity of the nucleus pulposus p on T2 weighted images. Moderate hypointense nucleus pulposus on T2 weighted images with normal disc height. Severe hypointense nucleus pulposus with narrowing of the disc space. Stadnik, Tadeusz W., et. Al., Annular tears and disc herniation:prevalence and contrast enhancement with MRI images in the absence of low-back pain or sciatica. Radiology.1998,Neuroradiology; 206: Three in One! Mild Asx. Volunteers 30 y/o or younger 22% Moderate Asx y/o= 86% >60 y/o=100% Severe Asx y/o=62% 45-60y/o=80% >60=100% 37
38 Asymptomatic Volunteers Disc Degeneration Mild to Moderate 30 years or younger=22% years=86% Over 60 years=100% years=62% Severe years=80% Over60years=100% When Does Disc Degeneration Begin? Powell, et. al., studied MRI scans of the lumbar spine in asymptomatic women and showed that at least one third have significant degenerative changes by the age of 21 to 40 years of age. (Begins in 30s) Paajanen, et. al., studied MR imaging scans of the lumbar spine in asymptomatic 20 year old men. The authors showed 35% had abnormalities. (Begins in 20s) Malette,P.C. et. l., Comparison of High Resolution Computer Tomography with Discography in the Evaluation of Lumbar Disc Herniations., Spine. 1990: 15(6): Paajanen, H., et.al.,magnetic Resonance Study of Disc Degeneration in the Young Low-Back Pain Patients,Spine,1989: 14(9): Powell, N. C., et.al., Prevelance of Lumbar Disc Degeneration Obsereved by Magnetic Resonance in Asymptomatic Women. Lancet,1986;2: When Does Disc Degeneration Begin? An Epidemiologic Study of MRI and Low Back Pain in 13-Year-Old Children. Spine 30:7; ,2005. Per Kjaer, PT, MSc et al., Signs of disc degeneration were found in approximately 1/3 of subjects 38
39 Is Degenerative Disc Disease Associated with Pain? Hult found radiographic evidence of DDD in 90% of lumbar radiographs in a group of year old patients. Despite a very high correlation between radiographic or MRI evidence of DDD and increasing age, no clinical correlation exists with pain. Hult L. Cervical, dorsal, and lumbar spine syndromes. Acta Orthop Scand [suppl 17] 1954: Is Degenerative Disc Disease Associated with Pain and/or Occupation? MRI study in female subjects aged 45 to 62 years with persistent LBP and in age matched controls. Selected from nursing and administrative professions Evaluated: Disc degeneration, disc herniation, nerve root compromise, high intensity it zones, end plate changes and facet joint arthritis. MRI findings did not differ between the 4 groups i.e., nurses and secretaries with and without LBP. Disc degeneration, disc herniation, nerve root compromise and facet joint osteoarthritis were present in over 50% of the intervertebral spaces studied. Patterns of lumbar disc degeneration are not associated with the job type and characteristic physical loading. Peter Schenk, PhD, et al., Magnetic Resonance Imaging of the Lumbar Spine. Spine 31:23; The Latest News About Degenerative Disc Disease in the WC Population Cumulative trauma and DDD Latest Information About DDD 39
40 Intervertebral Disc Degeneration. Summary of an AAOS/NIH/ORS Workshop Back pain has enormous socioeconomic consequences. The cost to society is very high, both directly and indirectly (wages, productivity, etc.) The cost in the United States exceeds $100 billion per year Intervertebral Disc Degeneration. Summary of an AAOS/NIH/ORS Workshop Over the past decade a great shift has occurred in the understanding of the etiology of disc degeneration from an epidemiologic perspective. Studies from twins have suggested that heredity has a dominant role in disc degeneration, while physical loading and environmental factors play a lesser role It appears that disc degeneration can be characterized as a common, oligogenic, multifactorial genetic condition. J Bone Joint /\Surg AM. 88: , Lumbar Disc Degeneration: Epidemiology and Genetics Research conducted over the last decade has led to a dramatic shift in the understanding of disc degeneration and its etiology. Previously, heavy physical loading-often associated with occupation-was the main suspected risk factor for disc degeneration, which was commonly viewed as a wear and tear phenomenon exacerbated by the precarious nutrition of the disc. However, results of studies on twins suggest that physical loading specific to occupation and sport plays a relatively minor role in disc degeneration. Recent research indicates that heredity has a dominant role in disc degeneration. J Bone Joint Surg Am. 88:3-9,
41 Lumbar Disc Degeneration: Epidemiology and Genetics In a multivariate analysis of the T12-L4 region, physical loading exposures explained 7% of variance in summary of disc degeneration scores, this rose to 16% with the addition of age and to 77% with addition of a variable representing familial aggregation. In the L4-L5 and L5-S1 region, measures of occupational and leisure physical loading explained only 2% of variance in disc degeneration. This rose to 9% with addition of age and 43% with addition of familial aggregation. Lumbar Disc Degeneration: Epidemiology and Genetics The additional effects of specific loading exposures beyond those of daily living appear to be relatively minor. J Bone Joint Surg Am. 88:3-9, 2006 Monozygotic Twin Siblings 44 y/o Journalist Severe end plate pathology at L5-S1 (arrow) Farmer anterior bulge at L3-L4 (arrow) Both narrow disc height T11- T12 (upper arrow) 48 y/o programmer Plumber Both have similar anterior and posterior bulging and end plate changes, mostly at higher lumbar levels. Programmer has wedged T 12 vertebra 41
42 49 y/o Bus Carpenter Driver Both have severe disc height narrowing, disc bulging, and some end plate changes. Overall the degenerative changes are quite similar. 61 y/o Farmer Chauffeur Both have severe disc-height narrowing, bulging, and end plate changes at the same disc levels. Disc at L4-5 is narrower in farmer, while disc at L1-2 is narrower in the chaffeur. Lumbar Disc Degeneration: Epidemiology and Genetics The prevalence of disc bulging ranged from 10% to 80% of subjects in the asymptomatic samples studied, and the prevalence of annular tears varied from 6% to 56%. J Bone Joint Surg Am. 88:3-9, 2006 Lumbar Disc Degeneration: Epidemiology and Genetics Age and Gender Degenerative changes in women appear to lag behind those found in men by approximately ten years Signs of DDD can be identified in childhood Histopathologic results from autopsy and surgical samples revealed presence of annular tears and end-plate cartilage pathology among three to ten year children. Degeneration scores steadily increase from 2 to 88 years of age. 42
43 Lumbar Disc Degeneration: Epidemiology and Genetics Annular tears Autopsy study risk of inner annular tear at age of 20 years is 65% Risk of full annular rupture 36% at 50 years of age Further References Beneke R. et al., Spondylitis Deformans. Versammlung deutscher Naturforscher uind Arzte ;4-69 Boos N, et al., Classification of age related changes in lumbar Intervertebral discs. Spine. 2002;27: Videman T et al., The occurrence of annular tears and their relation to lifetime back pain history: a cadaver study using BaSO4 discography. Spine. 2004;29: The Twin Study: Contributions to a changing view of disc degeneration Michele C. Battié, PhD, Tapio Videman et, al. the Spine Journal 9 (2009) Research program on the etiology and pathogenesis of disc degeneration. The most significant investigations related determinants of disc degeneration included: Occupational exposure Driving and whole- body vibration exposure Smoking exposure Anthropomorphic factors Heritability Identification of genotypes associated with DD 43
44 Twin Spine Study, Results..Most significant findings were a substantial influence of heredity on lumbar disc degeneration and identification of first gene associated with disc degeneration. Conversely, despite extraordinary discordance between twin siblings in occupational and leisure physical loading conditions throughout adulthood, surprisingly little effect on disc degeneration was observed. Twin Spine Study Results Effects of smoking demonstrated increase on DD associated with smoking, But this effect was small No evidence was found that whole-body vibration through motorized vehicles led to accelerated DD More recent results indicate that the effect of anthropometric factors, such as body weight and muscle strength on DD although modest, appear to be greater than those of occupational physical demands. In fact, some indications were found that routine loading may actually have some benefits to the disc! 44
45 Can degenerative disc disease become a cause of symptoms? The answer is yes. Degenerative disc disease can become symptomatic for a variety of reasons, the most common of which is the resultant spinal stenosis. The anatomical changes seen in degenerative disc disease are numerous and involve the motion segment. Composed of: Two adjacent vertebra The intervertebral disc Connecting ligaments Two facet joints Osteophytes or Traction Spurs Found near the attachment points of annulus fibrosis to the cortical rim of the vertebra. May have beneficial mechanical effect In stabilizing motion segment as disc space loses height and volume. However Detrimental effect if project into area occupied by a neurological structure Degenerative Disc Disease Not all spurs or bulges are a cause of pain. 45
Measure Title X RAY PRIOR TO MRI OR CAT SCAN IN THE EVAULATION OF LOWER BACK PAIN Disease State Back pain Indicator Classification Utilization
 Client HMSA: PQSR 2009 Measure Title X RAY PRIOR TO MRI OR CAT SCAN IN THE EVAULATION OF LOWER BACK PAIN Disease State Back pain Indicator Classification Utilization Strength of Recommendation Organizations
Client HMSA: PQSR 2009 Measure Title X RAY PRIOR TO MRI OR CAT SCAN IN THE EVAULATION OF LOWER BACK PAIN Disease State Back pain Indicator Classification Utilization Strength of Recommendation Organizations
Health Benchmarks Program Clinical Quality Indicator Specification 2013
 Health Benchmarks Program Clinical Quality Indicator Specification 2013 Measure Title USE OF IMAGING STUDIES FOR LOW BACK PAIN Disease State Musculoskeletal Indicator Classification Utilization Strength
Health Benchmarks Program Clinical Quality Indicator Specification 2013 Measure Title USE OF IMAGING STUDIES FOR LOW BACK PAIN Disease State Musculoskeletal Indicator Classification Utilization Strength
Cervical Spine Surgery. Orthopaedic Nursing Seminar. Dr Michelle Atkinson. Friday October 21 st 2011. Cervical Disc Herniation
 Cervical Spine Surgery Dr Michelle Atkinson The Sydney and Dalcross Adventist Hospitals Orthopaedic Nursing Seminar Friday October 21 st 2011 Cervical disc herniation The most frequently treated surgical
Cervical Spine Surgery Dr Michelle Atkinson The Sydney and Dalcross Adventist Hospitals Orthopaedic Nursing Seminar Friday October 21 st 2011 Cervical disc herniation The most frequently treated surgical
How To Get An Mri Of The Lumbar Spine W/O Contrast
 Date notice sent to all parties: May 27, 2014 IRO CASE #: ReviewTex, Inc. 1818 Mountjoy Drive San Antonio, TX 78232 (phone) 210-598-9381 (fax) 210-598-9382 reviewtex@hotmail.com Notice of Independent Review
Date notice sent to all parties: May 27, 2014 IRO CASE #: ReviewTex, Inc. 1818 Mountjoy Drive San Antonio, TX 78232 (phone) 210-598-9381 (fax) 210-598-9382 reviewtex@hotmail.com Notice of Independent Review
Discogenic Low Backache A clinical and MRI correlative study A DISSERTATION SUBMITTED TO UNIVERSITY OF SEYCHELLES AMERICAN INSTITUTE OF MEDICINE
 Discogenic Low Backache A clinical and MRI correlative study A DISSERTATION SUBMITTED TO UNIVERSITY OF SEYCHELLES AMERICAN INSTITUTE OF MEDICINE IN PARTIAL FULFILLMENT OF THE REGULATIONS FOR THE AWARD
Discogenic Low Backache A clinical and MRI correlative study A DISSERTATION SUBMITTED TO UNIVERSITY OF SEYCHELLES AMERICAN INSTITUTE OF MEDICINE IN PARTIAL FULFILLMENT OF THE REGULATIONS FOR THE AWARD
MN Community Measurement Low Back Pain Measure Impact and Recommendation Document June 2010
 MN Community Measurement Low Back Pain Measure Impact and Recommendation Document June 2010 Impact Relevance to Consumers, Employers and Payers Improvability Inclusiveness Mechanical low back pain (LBP)
MN Community Measurement Low Back Pain Measure Impact and Recommendation Document June 2010 Impact Relevance to Consumers, Employers and Payers Improvability Inclusiveness Mechanical low back pain (LBP)
White Paper: Reducing Utilization Concerns Regarding Spinal Fusion and Artificial Disc Implants
 White Paper: Reducing Utilization Concerns Regarding Spinal Fusion and Artificial Disc Implants For Health Plans, Medical Management Organizations and TPAs Executive Summary Back pain is one of the most
White Paper: Reducing Utilization Concerns Regarding Spinal Fusion and Artificial Disc Implants For Health Plans, Medical Management Organizations and TPAs Executive Summary Back pain is one of the most
Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy. Spine Volume 21(16) August 15, 1996, pp 1877-1883
 August 15, 1996, pp 1877-1883") Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy 1 Spine Volume 21(16) August 15, 1996, pp 1877-1883 Saal, Joel S. MD; Saal, Jeffrey A. MD; Yurth, Elizabeth F. MD FROM
Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy 1 Spine Volume 21(16) August 15, 1996, pp 1877-1883 Saal, Joel S. MD; Saal, Jeffrey A. MD; Yurth, Elizabeth F. MD FROM
Sample Treatment Protocol
 Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Nomenclature and Standard Reporting Terminology of Intervertebral Disk Herniation
 167 Nomenclature and Standard Reporting Terminology of Intervertebral Disk Herniation Richard F. Costello, DO a, *, Douglas P. Beall, MD a,b MAGNETIC RESONANCE IMAGING CLINICS Magn Reson Imaging Clin N
167 Nomenclature and Standard Reporting Terminology of Intervertebral Disk Herniation Richard F. Costello, DO a, *, Douglas P. Beall, MD a,b MAGNETIC RESONANCE IMAGING CLINICS Magn Reson Imaging Clin N
Imaging degenerative disk disease in the lumbar spine. Elaine Besancon MS III Dr. Gillian Lieberman
 Imaging degenerative disk disease in the lumbar spine Elaine Besancon MS III Dr. Gillian Lieberman Learning Objectives Anatomy review Pathophysiology of degenerative disc disease Common sequelae of disk
Imaging degenerative disk disease in the lumbar spine Elaine Besancon MS III Dr. Gillian Lieberman Learning Objectives Anatomy review Pathophysiology of degenerative disc disease Common sequelae of disk
SPINE ANATOMY AND PROCEDURES. Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132
 SPINE ANATOMY AND PROCEDURES Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132 SPINE ANATOMY The spine consists of 33 bones called vertebrae. The top 7 are cervical, or neck
SPINE ANATOMY AND PROCEDURES Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132 SPINE ANATOMY The spine consists of 33 bones called vertebrae. The top 7 are cervical, or neck
Treating Bulging Discs & Sciatica. Alexander Ching, MD
 Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Low Back Pain (LBP) Prevalence. Low Back Pain (LBP) Prevalence. Lumbar Fusion: Where is the Evidence?
 Prevalence. Low Back Pain (LBP) Prevalence. Lumbar Fusion: Where is the Evidence?") 15 th Annual Cleveland Clinic Pain Management Symposium Sarasota, Florida Lumbar Fusion: Where is the Evidence? Gordon R. Bell, M.D. Director, Cleveland Clinic Low Back Pain (LBP) Prevalence Lifetime prevalence:
15 th Annual Cleveland Clinic Pain Management Symposium Sarasota, Florida Lumbar Fusion: Where is the Evidence? Gordon R. Bell, M.D. Director, Cleveland Clinic Low Back Pain (LBP) Prevalence Lifetime prevalence:
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
Low Back Injury in the Industrial Athlete: An Anatomic Approach
 Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
A Patient s Guide to Artificial Cervical Disc Replacement
 A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
Spine University s Guide to Kinetic MRIs Detect Disc Herniations
 Spine University s Guide to Kinetic MRIs Detect Disc Herniations 2 Introduction Traditionally, doctors use a procedure called magnetic resonance imaging (MRI) to diagnose disc injuries. Kinetic magnetic
Spine University s Guide to Kinetic MRIs Detect Disc Herniations 2 Introduction Traditionally, doctors use a procedure called magnetic resonance imaging (MRI) to diagnose disc injuries. Kinetic magnetic
Spinal Surgery 2. Teaching Aims. Common Spinal Pathologies. Disc Degeneration. Disc Degeneration. Causes of LBP 8/2/13. Common Spinal Conditions
 Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
OUTLINE. Anatomy Approach to LBP Discogenic LBP. Treatment. Herniated Nucleus Pulposus Annular Tear. Non-Surgical Surgical
 DISCOGENIC PAIN OUTLINE Anatomy Approach to LBP Discogenic LBP Herniated Nucleus Pulposus Annular Tear Treatment Non-Surgical Surgical Facet Joints: bear 20% of weight Discs bear 80% of weight Neural Foramen
DISCOGENIC PAIN OUTLINE Anatomy Approach to LBP Discogenic LBP Herniated Nucleus Pulposus Annular Tear Treatment Non-Surgical Surgical Facet Joints: bear 20% of weight Discs bear 80% of weight Neural Foramen
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
.org. Herniated Disk in the Lower Back. Anatomy. Description
 Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Cervical Disc
 Herniated Cervical Disc North American Spine Society Public Education Series What Is a Herniated Disc? The backbone, or spine, is composed of a series of connected bones called vertebrae. The vertebrae
Herniated Cervical Disc North American Spine Society Public Education Series What Is a Herniated Disc? The backbone, or spine, is composed of a series of connected bones called vertebrae. The vertebrae
Information on the Chiropractic Care of Lower Back Pain
 Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
NON SURGICAL SPINAL DECOMPRESSION. Dr. Douglas A. VanderPloeg
 NON SURGICAL SPINAL DECOMPRESSION Dr. Douglas A. VanderPloeg CONTENTS I. Incidence of L.B.P. II. Anatomy Review III. IV. Disc Degeneration, Bulge, and Herniation Non-Surgical Spinal Decompression 1. History
NON SURGICAL SPINAL DECOMPRESSION Dr. Douglas A. VanderPloeg CONTENTS I. Incidence of L.B.P. II. Anatomy Review III. IV. Disc Degeneration, Bulge, and Herniation Non-Surgical Spinal Decompression 1. History
https://www.laserspineinstitute.com/back_problems/foraminal_stenosis/e...
 Questions? Call toll free 1-866-249-1627 Contact us today. We're here for you seven days a week. MRI Review Consultation Live help Call 1-866-249-1627 Chat Live Home Laser Spine Institute Laser Spine Institute's
Questions? Call toll free 1-866-249-1627 Contact us today. We're here for you seven days a week. MRI Review Consultation Live help Call 1-866-249-1627 Chat Live Home Laser Spine Institute Laser Spine Institute's
Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study
 Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine
Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine
The Petrylaw Lawsuits Settlements and Injury Settlement Report
 The Petrylaw Lawsuits Settlements and Injury Settlement Report BACK INJURIES How Minnesota Juries Decide the Value of Pain and Suffering in Back Injury Cases The Petrylaw Lawsuits Settlements and Injury
The Petrylaw Lawsuits Settlements and Injury Settlement Report BACK INJURIES How Minnesota Juries Decide the Value of Pain and Suffering in Back Injury Cases The Petrylaw Lawsuits Settlements and Injury
Options for Cervical Disc Degeneration A Guide to the M6-C. clinical study
 Options for Cervical Disc Degeneration A Guide to the M6-C clinical study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause
Options for Cervical Disc Degeneration A Guide to the M6-C clinical study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause
Soft-tissue injuries of the neck in automobile accidents: Factors influencing prognosis
 Soft-tissue injuries of the neck in automobile accidents: Factors influencing prognosis 1 Mason Hohl, MD FROM ABSTRACT: Journal of Bone and Joint Surgery (American) December 1974;56(8):1675-1682 Five years
Soft-tissue injuries of the neck in automobile accidents: Factors influencing prognosis 1 Mason Hohl, MD FROM ABSTRACT: Journal of Bone and Joint Surgery (American) December 1974;56(8):1675-1682 Five years
Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, The Cervical Spine. What is the Cervical Spine?
 Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness in the neck, shoulders, arms, and even hands. This patient
Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness in the neck, shoulders, arms, and even hands. This patient
Minimally Invasive Spine Surgery For Your Patients
 Minimally Invasive Spine Surgery For Your Patients Lukas P. Zebala, M.D. Assistant Professor Orthopaedic and Neurological Spine Surgery Department of Orthopaedic Surgery Washington University School of
Minimally Invasive Spine Surgery For Your Patients Lukas P. Zebala, M.D. Assistant Professor Orthopaedic and Neurological Spine Surgery Department of Orthopaedic Surgery Washington University School of
Lumbar Disc Herniation/Bulge Protocol
 Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
On Cervical Zygapophysial Joint Pain After Whiplash. Spine December 1, 2011; Volume 36, Number 25S, pp S194 S199
 On Cervical Zygapophysial Joint Pain After Whiplash 1 Spine December 1, 2011; Volume 36, Number 25S, pp S194 S199 Nikolai Bogduk, MD, PhD FROM ABSTRACT Objective To summarize the evidence that implicates
On Cervical Zygapophysial Joint Pain After Whiplash 1 Spine December 1, 2011; Volume 36, Number 25S, pp S194 S199 Nikolai Bogduk, MD, PhD FROM ABSTRACT Objective To summarize the evidence that implicates
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
Low Back Pain Protocols
 Low Back Pain Protocols Introduction: Diagnostic Triage And 1. Patient Group Adults aged 18 years and over with routine low back problems. Patients who have had recent surgery should be referred directly
Low Back Pain Protocols Introduction: Diagnostic Triage And 1. Patient Group Adults aged 18 years and over with routine low back problems. Patients who have had recent surgery should be referred directly
Spine DJD Nomenclature. Sonia K Ghei, MD
 Spine DJD Nomenclature Sonia K Ghei, MD Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology http://www.asnr.org/spine_nomenclature/
Spine DJD Nomenclature Sonia K Ghei, MD Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology http://www.asnr.org/spine_nomenclature/
Advances In Spine Care. James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery
 Advances In Spine Care James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery Introduction The Spine - A common source of problems Back pain is the #2 presenting
Advances In Spine Care James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery Introduction The Spine - A common source of problems Back pain is the #2 presenting
X Stop Spinal Stenosis Decompression
 X Stop Spinal Stenosis Decompression Am I a candidate for X Stop spinal surgery? You may be a candidate for the X Stop spinal surgery if you have primarily leg pain rather than mostly back pain and your
X Stop Spinal Stenosis Decompression Am I a candidate for X Stop spinal surgery? You may be a candidate for the X Stop spinal surgery if you have primarily leg pain rather than mostly back pain and your
Appropriate Use of Lumbar Imaging for Evaluation of Low Back Pain
 Appropriate Use of Lumbar Imaging for Evaluation of Low Back Pain Roger Chou, MD a,b, *, Richard A. Deyo, MD, MPH a,c,d,e,f,g, Jeffrey G. Jarvik, MD, MPH h,i,j KEYWORDS Low back pain Radiography MRI CT
Appropriate Use of Lumbar Imaging for Evaluation of Low Back Pain Roger Chou, MD a,b, *, Richard A. Deyo, MD, MPH a,c,d,e,f,g, Jeffrey G. Jarvik, MD, MPH h,i,j KEYWORDS Low back pain Radiography MRI CT
ARTICLES. Prevalence of Herniated Intervertebral Discs of the Cervical Spine in Asymptomatic Subjects Using MRI Scans: A Qualitative Systematic Review
 Please note that this electronic prepublication galley may contain typographical errors and may be missing artwork, such as charts, photographs, etc. Pagination in this version will differ from the published
Please note that this electronic prepublication galley may contain typographical errors and may be missing artwork, such as charts, photographs, etc. Pagination in this version will differ from the published
Lower Back Pain. Introduction. Anatomy
 Lower Back Pain Introduction Back pain is the number one problem facing the workforce in the United States today. To illustrate just how big a problem low back pain is, consider these facts: Low back pain
Lower Back Pain Introduction Back pain is the number one problem facing the workforce in the United States today. To illustrate just how big a problem low back pain is, consider these facts: Low back pain
Hitting a Nerve: The Triggers of Sciatica. Bruce Tranmer MD FRCS FACS
 Hitting a Nerve: The Triggers of Sciatica Bruce Tranmer MD FRCS FACS Disclosures I have no financial disclosures Objectives - Sciatica Historical Perspective What is Sciatica What can cause Sciatica Clinical
Hitting a Nerve: The Triggers of Sciatica Bruce Tranmer MD FRCS FACS Disclosures I have no financial disclosures Objectives - Sciatica Historical Perspective What is Sciatica What can cause Sciatica Clinical
Biomechanical Basis of Lumbar Pain. Prepared by S. Pollak. Introduction:
 Biomechanical Basis of Lumbar Pain Prepared by S. Pollak Introduction: The lumbar area of the back is made up of five movable L1-L5 vertebrae which have intervertebral discs in between them 1. The intervertebral
Biomechanical Basis of Lumbar Pain Prepared by S. Pollak Introduction: The lumbar area of the back is made up of five movable L1-L5 vertebrae which have intervertebral discs in between them 1. The intervertebral
Patient Guide to Neck Surgery
 The following is a sampling of products offered by Zimmer Spine for use in Anterior Cervical Fusion procedures. Patient Guide to Neck Surgery Anterior Cervical Fusion Trinica Select With the Trinica and
The following is a sampling of products offered by Zimmer Spine for use in Anterior Cervical Fusion procedures. Patient Guide to Neck Surgery Anterior Cervical Fusion Trinica Select With the Trinica and
Spine Trauma: When to Transfer. Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU
 Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Neck Pain Overview Causes, Diagnosis and Treatment Options
 Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
.org. Cervical Radiculopathy (Pinched Nerve) Anatomy. Cause
 Anatomy. Cause") Cervical Radiculopathy (Pinched Nerve) Page ( 1 ) Cervical radiculopathy, commonly called a pinched nerve occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal
Cervical Radiculopathy (Pinched Nerve) Page ( 1 ) Cervical radiculopathy, commonly called a pinched nerve occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal
There are four main regions of the back; the cervical (C), thoracic (T), lumbar (L), and sacral (S) regions
, thoracic (T), lumbar (L), and sacral (S) regions") Low Back Pain Overview Low back pain is one of the most common disorders in the United States. About 80 percent of people have at least one episode of low back pain during their lifetime. Factors that
Low Back Pain Overview Low back pain is one of the most common disorders in the United States. About 80 percent of people have at least one episode of low back pain during their lifetime. Factors that
LOW BACK PAIN; MECHANICAL
 1 ORTHO 16 LOW BACK PAIN; MECHANICAL Background This case definition was developed by the Armed Forces Health Surveillance Center (AFHSC) for the purpose of epidemiological surveillance of a condition
1 ORTHO 16 LOW BACK PAIN; MECHANICAL Background This case definition was developed by the Armed Forces Health Surveillance Center (AFHSC) for the purpose of epidemiological surveillance of a condition
1 REVISOR 5223.0070. (4) Pain associated with rigidity (loss of motion or postural abnormality) or
 Pain associated with rigidity (loss of motion or postural abnormality) or") 1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
Lumbar Spine Anatomy. eorthopod.com 228 West Main St., Suite D Missoula, MT 59802-4345 Phone: 406-721-3072 Fax: 406-721-2619 info@eorthopod.
 A Patient s Guide to Lumbar Spine Anatomy 228 West Main St., Suite D Missoula, MT 59802-4345 Phone: 406-721-3072 Fax: 406-721-2619 info@eorthopod.com DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Lumbar Spine Anatomy 228 West Main St., Suite D Missoula, MT 59802-4345 Phone: 406-721-3072 Fax: 406-721-2619 info@eorthopod.com DISCLAIMER: The information in this booklet is compiled
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time.
 If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
Orthopaedic Spine Center. Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs
 Normal Discs") Orthopaedic Spine Center Graham Calvert MD James Woodall MD PhD Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs The cervical spine consists of the bony vertebrae, discs, nerves and other structures.
Orthopaedic Spine Center Graham Calvert MD James Woodall MD PhD Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs The cervical spine consists of the bony vertebrae, discs, nerves and other structures.
Discogenic Pain: Diagnosis and Treatment
 Discogenic Pain: Diagnosis and Treatment James P. Rathmell, M.D. Professor of Anesthesiology University of Vermont College of Medicine Burlington, Vermont, USA Cottage Sunrise Westford, Vermont 2005 Learning
Discogenic Pain: Diagnosis and Treatment James P. Rathmell, M.D. Professor of Anesthesiology University of Vermont College of Medicine Burlington, Vermont, USA Cottage Sunrise Westford, Vermont 2005 Learning
Spinal Decompression
 Spinal Decompression Spinal decompression is just one more tool we have to treat radiculopathy. With appropriate education and exercises, this modality has been proven to assist in the resolution of symptoms
Spinal Decompression Spinal decompression is just one more tool we have to treat radiculopathy. With appropriate education and exercises, this modality has been proven to assist in the resolution of symptoms
Herniated Disk in the Lower Back
 Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
FLORIDA MCA PROVIDER EDUCATION BULLETIN APRIL
 NETWORK NOTES NEW REPORTING REQUIREMENTS Effective 6/1/2010, Coventry's Network directories will look slightly different. On April 12, 2010, the agency sent notice to all MCAs regarding modifications for
NETWORK NOTES NEW REPORTING REQUIREMENTS Effective 6/1/2010, Coventry's Network directories will look slightly different. On April 12, 2010, the agency sent notice to all MCAs regarding modifications for
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN
 CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
UPPER LUMBAR DISC HERNIATION WITH CENTRAL AND FAR LATERAL STENOTIC CHANGES RESULTING IN ANTERIOR THIGH PAIN
 Cox Technic Case Report #60 sent 5/13/08 1 UPPER LUMBAR DISC HERNIATION WITH CENTRAL AND FAR LATERAL STENOTIC CHANGES RESULTING IN ANTERIOR THIGH PAIN History, Examination & Imaging Review: A 53-year-old
Cox Technic Case Report #60 sent 5/13/08 1 UPPER LUMBAR DISC HERNIATION WITH CENTRAL AND FAR LATERAL STENOTIC CHANGES RESULTING IN ANTERIOR THIGH PAIN History, Examination & Imaging Review: A 53-year-old
Practice Guidelines For Low Back Pain
 Consumers Guide Practice Guidelines For Low Back Pain Copyright 2008 American Chronic Pain Association Page 1 Written by: Penney Cowan Founder Executive Director American Chronic Pain Association Editors:
Consumers Guide Practice Guidelines For Low Back Pain Copyright 2008 American Chronic Pain Association Page 1 Written by: Penney Cowan Founder Executive Director American Chronic Pain Association Editors:
Cervical Spondylosis (Arthritis of the Neck)
") Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Whiplash and Whiplash- Associated Disorders
 Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
TREATMENT OF AN L5/S1 EXTRUDED DISC HERNIATION USING SPINAL DECOMPRESSION: A CASE STUDY. Jack Choate, DC
 TREATMENT OF AN L5/S1 EXTRUDED DISC HERNIATION USING SPINAL DECOMPRESSION: A CASE STUDY Jack Choate, DC ABSTRACT Objective: To discuss a case of an acute lumbar disc herniation that was successfully treated
TREATMENT OF AN L5/S1 EXTRUDED DISC HERNIATION USING SPINAL DECOMPRESSION: A CASE STUDY Jack Choate, DC ABSTRACT Objective: To discuss a case of an acute lumbar disc herniation that was successfully treated
Back & Neck Pain Survival Guide
 Back & Neck Pain Survival Guide www.kleinpeterpt.com Zachary - 225-658-7751 Baton Rouge - 225-768-7676 Kleinpeter Physical Therapy - Spine Care Program Finally! A Proven Assessment & Treatment Program
Back & Neck Pain Survival Guide www.kleinpeterpt.com Zachary - 225-658-7751 Baton Rouge - 225-768-7676 Kleinpeter Physical Therapy - Spine Care Program Finally! A Proven Assessment & Treatment Program
Evidence Based Medicine in Spinal Surgery
 Evidence Based Medicine in Spinal Surgery Roger Härtl, MD Associate Professor of Neurosurgery Chief of Spinal Surgery Neurosurgeon to the GIANTS Football team Brain & Spine Center Weill Cornell Medical
Evidence Based Medicine in Spinal Surgery Roger Härtl, MD Associate Professor of Neurosurgery Chief of Spinal Surgery Neurosurgeon to the GIANTS Football team Brain & Spine Center Weill Cornell Medical
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1708/15
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1708/15 BEFORE: E. Kosmidis : Vice-Chair E. Tracey : Member Representative of Employers C. Salama : Member Representative of Workers HEARING:
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1708/15 BEFORE: E. Kosmidis : Vice-Chair E. Tracey : Member Representative of Employers C. Salama : Member Representative of Workers HEARING:
Herniated Lumbar Disc
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN. Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA
 DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
CERVICAL SPONDYLOSIS
 CERVICAL SPONDYLOSIS Dr. Sahni B.S Dy. Chief Medical Officer, ONGC Hospital Panvel-410221,Navi Mumbai,India Introduction The cervical spine consists of the top 7 vertebrae of the spine. These are referred
CERVICAL SPONDYLOSIS Dr. Sahni B.S Dy. Chief Medical Officer, ONGC Hospital Panvel-410221,Navi Mumbai,India Introduction The cervical spine consists of the top 7 vertebrae of the spine. These are referred
BODY BODY PEDICLE PEDICLE TRANSVERSE TRANSVERSE PROCESS PROCESS
 Learning Objective Radiology Anatomy of the Spine and Upper Extremity Identify anatomic structures of the spine and upper extremities on standard radiographic and cross-sectional images Timothy J. Mosher,
Learning Objective Radiology Anatomy of the Spine and Upper Extremity Identify anatomic structures of the spine and upper extremities on standard radiographic and cross-sectional images Timothy J. Mosher,
Do you have Back Pain? Associated with:
 Do you have Back Pain? Associated with: Herniated Discs? Protruding Discs? Degenerative Disk Disease? Posterior Facet Syndrome? Sciatica? You may be a candidate for Decompression Therapy The Dynatronics
Do you have Back Pain? Associated with: Herniated Discs? Protruding Discs? Degenerative Disk Disease? Posterior Facet Syndrome? Sciatica? You may be a candidate for Decompression Therapy The Dynatronics
Standard of Care: Cervical Radiculopathy
 Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS?
 SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS? The spinal canal is best imagined as a bony tube through which nerve fibres pass. The tube is interrupted between each pair of adjacent
SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS? The spinal canal is best imagined as a bony tube through which nerve fibres pass. The tube is interrupted between each pair of adjacent
Cervical Spine: Postmortem Assessment of Accident Injuries Comparison of Radiographic, MR Imaging, Anatomic, and Pathologic Findings
 Cervical Spine: Postmortem Assessment of Accident Injuries Comparison of Radiographic, MR Imaging, Anatomic, and Pathologic Findings 1 Radiology, November, 2001;221:340-346. Axel Stäbler, MD, Jurik Eck,
Cervical Spine: Postmortem Assessment of Accident Injuries Comparison of Radiographic, MR Imaging, Anatomic, and Pathologic Findings 1 Radiology, November, 2001;221:340-346. Axel Stäbler, MD, Jurik Eck,
How To Get A Medical Insurance Policy For A Spinal Injury
 Spondylosis, Facet Joint Arthropathy and Pain Jim Borowczyk Department of Orthopaedics and Musculoskeletal Medicine Christchurch School of Medicine University of Otago Do Age Related Changes in the Spinal
Spondylosis, Facet Joint Arthropathy and Pain Jim Borowczyk Department of Orthopaedics and Musculoskeletal Medicine Christchurch School of Medicine University of Otago Do Age Related Changes in the Spinal
Non-Surgical Spinal Decompression with Computerized Spinal Table (Traction, Deep heat and Massage)
") Non-Surgical Spinal Decompression with Computerized Spinal Table (Traction, Deep heat and Massage) for Treating and Rehabilitating Spinal patients New treatment for back problems not just medicines and
Non-Surgical Spinal Decompression with Computerized Spinal Table (Traction, Deep heat and Massage) for Treating and Rehabilitating Spinal patients New treatment for back problems not just medicines and
Degenerative Lumbar Spine Disease
 Beth Israel Deaconess Medical Center A Member of Caregroup Harvard Medical School Degenerative Lumbar Spine Disease Michael Barnett, HMS III Core Radiology Clerkship BIDMC PCE Overview Patient Presentation:
Beth Israel Deaconess Medical Center A Member of Caregroup Harvard Medical School Degenerative Lumbar Spine Disease Michael Barnett, HMS III Core Radiology Clerkship BIDMC PCE Overview Patient Presentation:
.org. Fractures of the Thoracic and Lumbar Spine. Cause. Description
 Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
Thoracic Spine Anatomy
 A Patient s Guide to Thoracic Spine Anatomy 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Thoracic Spine Anatomy 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
How To Understand The Anatomy Of A Lumbar Spine
 Sciatica: Low back and Leg Pain Diagnosis and Treatment Options Presented by Devesh Ramnath, MD Orthopaedic Associates Of Dallas Baylor Spine Center Sciatica Compression of the spinal nerves in the back
Sciatica: Low back and Leg Pain Diagnosis and Treatment Options Presented by Devesh Ramnath, MD Orthopaedic Associates Of Dallas Baylor Spine Center Sciatica Compression of the spinal nerves in the back
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Musculoskeletal: Acute Lower Back Pain
 Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
VCA Animal Specialty Group 5610 Kearny Mesa Rd., Suite B San Diego, CA 92111 858-560-8006 www.vcaanimalspecialtygroup.com.
 Disk Disease While not limited to small breeds, disc disease is much more prevalent among Dachshunds, Lhasa Apsos, Poodles, Beagles and Pekingese primarily due to genetic factors. These traits result in
Disk Disease While not limited to small breeds, disc disease is much more prevalent among Dachshunds, Lhasa Apsos, Poodles, Beagles and Pekingese primarily due to genetic factors. These traits result in
Herniated Disk. This reference summary explains herniated disks. It discusses symptoms and causes of the condition, as well as treatment options.
 Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
A review of spinal problems
 Dr Ulrich R Hähnle MD, FCS Orthopaedic Surgeon, Wits Facharzt für Orthopädie, Berlin Phone: +27 11 485 3236 Fax: +27 11 485 2446 Suite 102, Medical Centre, Linksfield Park Clinic P.O. Box 949, Johannesburg
Dr Ulrich R Hähnle MD, FCS Orthopaedic Surgeon, Wits Facharzt für Orthopädie, Berlin Phone: +27 11 485 3236 Fax: +27 11 485 2446 Suite 102, Medical Centre, Linksfield Park Clinic P.O. Box 949, Johannesburg
.org. Cervical Spondylosis (Arthritis of the Neck) Anatomy. Cause
 Anatomy. Cause") Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
Information for the Patient About Surgical
 Information for the Patient About Surgical Decompression and Stabilization of the Spine Aging and the Spine Daily wear and tear, along with disc degeneration due to aging and injury, are common causes
Information for the Patient About Surgical Decompression and Stabilization of the Spine Aging and the Spine Daily wear and tear, along with disc degeneration due to aging and injury, are common causes
Spine Injury and Back Pain in Sports
 Spine Injury and Back Pain in Sports DAVID W. GRAY, MD 1 Back Pain Increases with Age Girls>Boys in Teenage years Anywhere from 15 to 80% of children and adolescents have back pain depending on the studies
Spine Injury and Back Pain in Sports DAVID W. GRAY, MD 1 Back Pain Increases with Age Girls>Boys in Teenage years Anywhere from 15 to 80% of children and adolescents have back pain depending on the studies
Spinal Surgery Functional Status and Quality of Life Outcome Specifications 2015 (01/01/2013 to 12/31/2013 Dates of Procedure) September 2014
 September 2014") Description Methodology For patients ages 18 years and older who undergo a lumbar discectomy/laminotomy or lumbar spinal fusion procedure during the measurement year, the following measures will be calculated:
Description Methodology For patients ages 18 years and older who undergo a lumbar discectomy/laminotomy or lumbar spinal fusion procedure during the measurement year, the following measures will be calculated:
CORRELATION OF PAIN AND DISABILITY WITH MRI FINDINGS IN PATIENTS WITH LUMBAR DISCOGENIC BACK PAIN Surendra K. Wani 1, Neha Deshpande * 2.
 Original Article CORRELATION OF PAIN AND DISABILITY WITH MRI FINDINGS IN PATIENTS WITH LUMBAR DISCOGENIC BACK PAIN Surendra K. Wani 1, Neha Deshpande * 2. 1 Assistant Professor, *2 Post Graduate Student,
Original Article CORRELATION OF PAIN AND DISABILITY WITH MRI FINDINGS IN PATIENTS WITH LUMBAR DISCOGENIC BACK PAIN Surendra K. Wani 1, Neha Deshpande * 2. 1 Assistant Professor, *2 Post Graduate Student,
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis North American Spine Society Public Education Series What Is Lumbar Spinal Stenosis? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
Lumbar Spinal Stenosis North American Spine Society Public Education Series What Is Lumbar Spinal Stenosis? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
Effects of vertebral axial decompression on intradiscal pressure
 This article is reprinted with the permission of the authors from the Journal of Neurosurgery, Volume 81. J Neurosurg 81:350-353, 1994 Effects of vertebral axial decompression on intradiscal pressure GUSTAVO
This article is reprinted with the permission of the authors from the Journal of Neurosurgery, Volume 81. J Neurosurg 81:350-353, 1994 Effects of vertebral axial decompression on intradiscal pressure GUSTAVO
BACK PAIN: WHAT YOU SHOULD KNOW
 BACK PAIN: WHAT YOU SHOULD KNOW Diane Metzer LOWER BACK PAIN Nearly everyone at some point has back pain that interferes with work, recreation and routine daily activities. Four out of five adults experience
BACK PAIN: WHAT YOU SHOULD KNOW Diane Metzer LOWER BACK PAIN Nearly everyone at some point has back pain that interferes with work, recreation and routine daily activities. Four out of five adults experience
How To Treat Pain With Pain Management
 SUTTER PHYSICIANS ALLIANCE (SPA) 2800 L Street, 7 th Floor Sacramento, CA 95816 SPA PCP Treatment & Referral Guidelines Pain Management Developed June 1, 2003 Revised - (Format Revisions) November 13,
SUTTER PHYSICIANS ALLIANCE (SPA) 2800 L Street, 7 th Floor Sacramento, CA 95816 SPA PCP Treatment & Referral Guidelines Pain Management Developed June 1, 2003 Revised - (Format Revisions) November 13,
Neck Injuries and Disorders
 Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
Management of spinal cord compression
 Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
American Journal of Pain Management Vol. 7 No. 2 April 1997
 American Journal of Pain Management Vol. 7 No. 2 April 1997 Emerging Technologies: Preliminary Findings DECOMPRESSION, REDUCTION, AND STABILIZATION OF THE LUMBAR SPINE: A COST-EFFECTIVE TREATMENT FOR LUMBOSACRAL
American Journal of Pain Management Vol. 7 No. 2 April 1997 Emerging Technologies: Preliminary Findings DECOMPRESSION, REDUCTION, AND STABILIZATION OF THE LUMBAR SPINE: A COST-EFFECTIVE TREATMENT FOR LUMBOSACRAL