Does this patient have Parkinsonism? Salvador Cruz-Flores, MD, MPH, FCCM Professor and Founding Chair Department of Neurology
|
|
|
- Tyler Richards
- 7 years ago
- Views:
Transcription

1 Does this patient have Parkinsonism? Salvador Cruz-Flores, MD, MPH, FCCM Professor and Founding Chair Department of Neurology
2 Nothing to disclose
3 Case Scenarios Context The Evidence o Populations o Prior Probability o Reference Standard o Test Characteristics Overview
4 Case 1 70-year-old man with 3-month history of progressive tremor and difficulty writing letters Physical examination Bilateral tremor, otherwise well. Continues to play golf
5 Case 2 68-year-old man with three-month history of right arm tremor and trouble getting up from chair Physical examination: Rigidity, Small steps, limited arm swing and limited facial expression
6 Questions What is the likelihood that these patients have Parkinson disease? Are there other elements of history or physical examination that would help you assess the likelihood of Parkinsonism?
7 Prior Probability Parkinson disease prevalence Aged 65+ years: 1% Aged 85+ years: 2% In older patients presenting with general neurological complaints the prior probability is likely higher
8 Why Do Clinical Evaluation? Diagnosis of Parkinson disease relies on serial clinical assessments No simple tested imaging or markers available Symptoms overlap other conditions o Supranuclear palsy o Multisystem atrophy o Dementia with Lewy bodies
9 Reference Standard Pragmatic standard: Serial clinical examinations performed by a specialist with or without concomitant treatment Neuropathologic standard: Depletion of brain stem pigmented neurons and proliferation of Lewy bodies
10 Pathophysiology Parkinson disease o Primary or idiopathic o Neurons and dopamine lost from substantia nigra and Lewy bodies Parkinsonism o 2 or more features present: tremor, rigidity, bradykinesia o Causes include viral, toxins, heredity, head trauma, hydrocephalus, or medications
11
12 Step one Cardinal features of Parkinsonism Bradykinesia Rigidity Tremor Postural instability Diagnostic? o Reponse to L dopa
13 Bradykinesia in Parkinson disease Slowing of active movement or slowness in initiating movement Postural instability o Presents as changes in gait and balance o Short, shuffling steps o Loss of arm movement o Loss of postural reflex mechanisms leads to falls
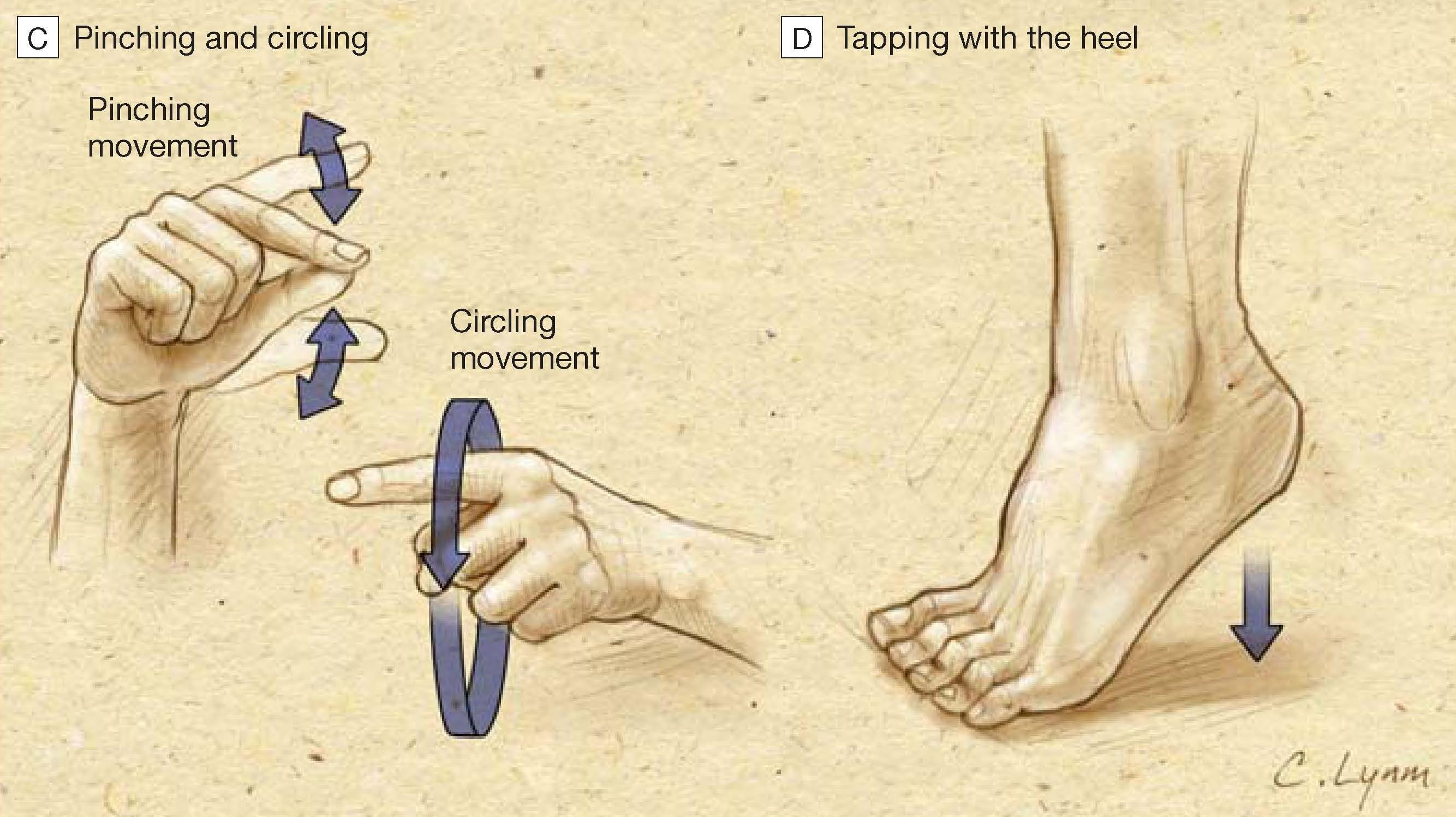
14 How to Elicit Signs Bradykinesia Definition of Bradykinesia A decrease in speed and amplitude of complex movements Four maneuvers to consider o Tapping fingers o Twiddling o Pinching and circling o Tapping with the heel

15 Detecting Bradykinesia
16 Detecting Bradykinesia
17 Rigidity in Parkinson disease Involuntary stiffness of skeletal muscles Cog wheeling o Jerky motion of limbs as constant force is applied across a joint o Similar to ratcheting of clicking cogs or gears Spasticity (not usually present) o Selective increase in tone of flexor muscles in arms and extensor muscles in legs o Suggests diagnosis other than Parkinson
18 How to Elicit Signs Rigidity Examiner places thumb across patient s antecubital fossa to palpate the distal biceps tendon while passively moving the forearm ocog-wheeling rigidity: Intermittent, resistance alternates with relaxation olead-pipe rigidity: Smooth increase tone
19 Differential Diagnosis of Tremor Three common tremor syndromes otremor of Parkinson oclassic essential tremor ophysiologic tremor
20 Classification of Tremors Rest tremor Occurs in a body part not voluntarily activated and supported completely against gravity Action tremor Postural: Occurs while voluntarily maintaining a position against gravity Kinetic Occurs during any voluntary movement: simple, intention, task-specific, isometric
21 Kinetic Tremors Simple: Occurs during voluntary nontarget-directed movement Intention: Amplitude increases during visually guided movement (eg, finger to nose) Task-specific: Appears or is exaggerated by specific tasks (eg, writing) Isometric: Occurs during voluntary muscle contraction against a rigid stationary object (eg, squeezing hand)
22 Common Tremor Syndromes Tremor of Parkinson Slow frequency (4-6/second) Occurs at rest Inhibited during movement and sleep Aggravated by emotional stress Pill-rolling quality
23 The tremor of Parkinson disease 75% of patients complain of initial tremor at rest Usually starts upper extremity Appears intermittently Disappears during sleep Increases with stress or anxiety Signs typically begin unilaterally then progress asymmetrically
24 Common Tremor Syndromes Classic essential tremor Bilateral Usually symmetric postural or kinetic Family history common Tremor attenuated with alcohol
25 Common Tremor Syndromes Physiologic tremor High frequency (8-12/second) Differing degrees in different subjects Enhanced form is easily visible Postural (while maintaining a position against gravity) No evidence underlying neurologic disease Cause may be reversible (eg, caffeine)
26 Definition: How to Elicit Signs Tremor Rhythmical, involuntary, oscillatory movement of body part Observe with hands on lap o Rest or action o Frequency o Symmetry
27 Step two Red flags Pattern and distribution Course Medication response Tremor Myoclonus Dysphagia/dysarthria Dystonia Pyramidal signs Ataxia Gait and balance Polyneuropathy Eye movements Autonomic dysfunction Cognitive dysfunction Sleep disturbances
28 Step three Differential diagnosis
29 Step three Differential diagnosis

30 Step three Differential diagnosis
31 Patients Without Tremor Multisystem atrophy: Asymmetric rigidity, akinesia, autonomic dysfunction, cerebellar symptoms, and possible transient response to levodopa, but minority have tremor Progressive supranuclear palsy: Rigidity and postural instability but rare tremor Lewy body disease: Cognitive impairment is present at the onset with behavioral changes, hallucinations
32 Presentation Early Parkinson disease symptoms o Nonspecific symptoms o Generalized malaise and easy fatigability o Subtle personality changes o May occur years before tremor Next stage Symptoms frequently unilateral asymmetric o Tremor o Limb rigidity and bradykinesia o Postural instability
33 Secondary manifestations Disordered sleep (42%) Constipation (50%) Pain (50%) Depression (40%) Dementia (20%)
34 Prevalence Prior Probability o per population More common with age 1% of persons age > 65 2% of persons age > 85 Prevalence among older people with neurologic symptoms is higher but precise figures unavailable
35 Test Characteristics Sensitivity o SnN( )out: Negative tends to rule out Specificity o SpP(+)in: Positive tends to rule in
36 Test Characteristics Likelihood ratio (LR) o Determined for a particular test result o Conceptually related to how much more (LR > 1) or less (LR < 1) likely the disease is, given a particular test result o LR = 1 will not change your assessment of the likelihood of disease, given a particular test result
37 Using Likelihood Ratios Values of Likelihood Ratio: How much do they affect probability of disease? o LR = 1 o LR = 3-10 o LR = olr > 10 olr < 0.10 No effect on likelihood Disease More Likely Disease Less Likely Disease More Likely Disease Less Likely

38 LR: Impact on Likelihood of Disease 0 LR = 0.01 More Impact LR = 0.1 More Impact LR = 0.2 LR = 5 More Impact LR = 0.3 More Impact Increasing impact LR = 1 No Impact LR = 3 More Impact More Impact LR = 10 More Impact increasing impact LR = 100 More Impact
39 Useful Symptoms Findings (No. of Studies) LR+ LR History of shuffling gait (2) History of bradykinesia and difficulty rising from a chair (2) History of loss of balance (2) History of tremor (4) History of rigidity (3)
40 Useful Signs Findings LR+ (95% CI) LR (95% CI) Rigidity and bradykinesia 4.5 ( ) 0.12 ( ) Glabella tap 4.5 ( ) 0.13 ( ) Difficulty walking heel 2.9 ( ) 0.32 ( ) to toe Rigidity 2.8 ( ) 0.38 ( ) Asymmetry of disease 1.8 ( ) 0.61 ( ) Tremor 1.5 ( ) 0.47 ( )
41 Nomogram for Interpreting LR Plot patient s prior probability on left Draw straight line through LR for given test result Line points to posttest probability
42 70-year-old man Return to Case 1 History 3-month history of progressive tremor Difficulty writing letters Physical examination Bilateral tremor Otherwise well Continues to play golf
43 LR: Tremor History of tremor, LR = % Prior probability of Parkinson disease in 70-year-old man 1.3%-10% Posttest probability
44 Return to Case Scenario 1 Additional physical examination Glabella tap positive (LR = 4.5) Micrographia (LR = 2.8) Difficulty walking heel to toe (LR = 2.9)
45 LR: Glabella Tap/Heel to Toe Heel to toe, LR = 2.9 1% Prior probability of Parkinson disease in 70-year-old man Posttest probability 3% for Heel to toe
46 Return to Case 2 68-year-old man History 3-month history of right arm tremor Trouble getting up from chair Physical examination Rigidity Small steps, limited arm swing Limited facial expression
47 LR: Tremor Bradykinesia LR = 1.9 1% Pretest probability of Parkinson disease in 68-year-old man Posttest probability, 2%
48 Case Scenarios Both cases have many features of Parkinson disease. Given a 1% prior probability, single findings each individually increase likelihood of disease. However, clinical decisions are made based on multiple findings and follow-up over time. Positive symptoms and signs over time may justify a trial of empiric treatment.
49 Take home Classic features when present do help establish the diagnosis otremor origidity obradykinesia combined oloss of balance (postural instability) oresponse to L dopa
50 Take home Diagnosis of Parkinson disease remains challenging and relies on clinical evaluation, signs, and symptoms. Single findings may not alter the prior probability enough to direct diagnosis and management on their own. Combinations of findings, follow-up, and response to therapy guides clinical management, but such strategies have not been tested.
What is PD? Dr Catherine Dotchin MD MRCP Consultant Geriatrician
 What is PD? Dr Catherine Dotchin MD MRCP Consultant Geriatrician Overview of presentation Case history Video example pre and post treatment Historical review PD in the UK Epidemiology and aetiology Making
What is PD? Dr Catherine Dotchin MD MRCP Consultant Geriatrician Overview of presentation Case history Video example pre and post treatment Historical review PD in the UK Epidemiology and aetiology Making
Parkinson s Disease (PD)
") Parkinson s Disease (PD) Parkinson s disease (PD) is a movement disorder that worsens over time. About 1 in 100 people older than 60 has Parkinson s. The exact cause of PD is still not known, but research
Parkinson s Disease (PD) Parkinson s disease (PD) is a movement disorder that worsens over time. About 1 in 100 people older than 60 has Parkinson s. The exact cause of PD is still not known, but research
Parkinson's s disease - a
 Parkinson's Disease Parkinson's s disease - a progressive disorder of the nervous system that affects movement. The most common perception of Parkinson s is the patient having tremors. Hands shaking, inability
Parkinson's Disease Parkinson's s disease - a progressive disorder of the nervous system that affects movement. The most common perception of Parkinson s is the patient having tremors. Hands shaking, inability
PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS
 PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS De Anna Looper, RN CHPN Corporate Clinical Consultant / Legal Nurse Consultant Carrefour Associates L.L.C. PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS
PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS De Anna Looper, RN CHPN Corporate Clinical Consultant / Legal Nurse Consultant Carrefour Associates L.L.C. PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS
Lewy body dementia Referral for a Diagnosis
 THE Lewy Body society The more people who know, the fewer people who suffer Lewy body dementia Referral for a Diagnosis Lewy Body Dementias REFERRAL FOR A DIAGNOSIS In the UK people with all forms of dementia
THE Lewy Body society The more people who know, the fewer people who suffer Lewy body dementia Referral for a Diagnosis Lewy Body Dementias REFERRAL FOR A DIAGNOSIS In the UK people with all forms of dementia
Parkinson's disease. Definition. Symptoms
 Parkinson's disease Definition Parkinson's disease is a progressive disorder of the nervous system that affects your movement. It develops gradually, sometimes starting with a barely noticeable tremor
Parkinson's disease Definition Parkinson's disease is a progressive disorder of the nervous system that affects your movement. It develops gradually, sometimes starting with a barely noticeable tremor
Parkinson s Disease Symptoms Guide
 Parkinson s Disease Symptoms Guide Some symptoms of Parkinson s disease (PD) are hard for even specialists to detect. Others are obvious even to an untrained eye. Parkinson s symptoms are different for
Parkinson s Disease Symptoms Guide Some symptoms of Parkinson s disease (PD) are hard for even specialists to detect. Others are obvious even to an untrained eye. Parkinson s symptoms are different for
PARKINSON S DISEASE AND PARKINSONISM. Dr Phil Wood Geriatrician, Waitemata DHB Clinical Unit Leader, Waikato DHB
 PARKINSON S DISEASE AND PARKINSONISM Dr Phil Wood Geriatrician, Waitemata DHB Clinical Unit Leader, Waikato DHB OUTLINE Covering:- Why this is an important area of Medical and Psychiatric care The variety
PARKINSON S DISEASE AND PARKINSONISM Dr Phil Wood Geriatrician, Waitemata DHB Clinical Unit Leader, Waikato DHB OUTLINE Covering:- Why this is an important area of Medical and Psychiatric care The variety
Parkinson s Disease - A Junior Doctor s Survival Guide
 Parkinson s Disease - A Junior Doctor s Survival Guide Professor Richard Walker Consultant Geriatrician Hon. Professor of Ageing & Interna
Parkinson s Disease - A Junior Doctor s Survival Guide Professor Richard Walker Consultant Geriatrician Hon. Professor of Ageing & Interna
Nursing Care of Patients with Movement Disorders. Catholic Health 2 nd Annual Neurorehab Symposium November 1, 2014
 Nursing Care of Patients with Movement Disorders Catholic Health 2 nd Annual Neurorehab Symposium November 1, 2014 Types of Movement Disorders Parkinson s disease Huntington s disease Dystonia Tremors
Nursing Care of Patients with Movement Disorders Catholic Health 2 nd Annual Neurorehab Symposium November 1, 2014 Types of Movement Disorders Parkinson s disease Huntington s disease Dystonia Tremors
Prevalence of Parkinsonism and its aetiological subtypes within patients with movement disorders
 Research papers Prevalence of and its aetiological subtypes within patients with movement disorders D G S V D Gajasinghe* AL 2002 batch of students, Faculty of Medicine, University of Colombo Abstract
Research papers Prevalence of and its aetiological subtypes within patients with movement disorders D G S V D Gajasinghe* AL 2002 batch of students, Faculty of Medicine, University of Colombo Abstract
NEUROIMAGING in Parkinsonian Syndromes
 NEUROIMAGING in Parkinsonian Syndromes (Focus on Structural Techniques: CT and MRI) Dr. Roberto Cilia Parkinson Institute, ICP, Milan, Italy OUTLINE Primary Parkinsonism Idiopathic Parkinson s Disease
NEUROIMAGING in Parkinsonian Syndromes (Focus on Structural Techniques: CT and MRI) Dr. Roberto Cilia Parkinson Institute, ICP, Milan, Italy OUTLINE Primary Parkinsonism Idiopathic Parkinson s Disease
Chapter 28. Drug Treatment of Parkinson s Disease
 Chapter 28 Drug Treatment of Parkinson s Disease 1. Introduction Parkinsonism Tremors hands and head develop involuntary movements when at rest; pin rolling sign (finger and thumb) Muscle rigidity arthritis
Chapter 28 Drug Treatment of Parkinson s Disease 1. Introduction Parkinsonism Tremors hands and head develop involuntary movements when at rest; pin rolling sign (finger and thumb) Muscle rigidity arthritis
Understanding Parkinson s Disease
 Understanding Parkinson s Disease Irene Oh, MD Neurologist, Movement Disorders Specialist The Neurology Center of Southern California, Encinitas & Escondido Introduction PD was first described in 1817
Understanding Parkinson s Disease Irene Oh, MD Neurologist, Movement Disorders Specialist The Neurology Center of Southern California, Encinitas & Escondido Introduction PD was first described in 1817
Movement disorders and gait disturbances. Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs
 Movement disorders and gait disturbances Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs 1 MD pathophysiology Genetic mutation or environmental injury of basal ganglia functioning Pallidum, thalamus, subthalamic
Movement disorders and gait disturbances Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs 1 MD pathophysiology Genetic mutation or environmental injury of basal ganglia functioning Pallidum, thalamus, subthalamic
Dementia & Movement Disorders
 Dementia & Movement Disorders A/Prof Michael Davis Geriatrician ACT Health & GSAHS ANU Medical School Eastern Dementia Network Aged and Dementia Care Symposium Bateman s Bay, 22 October 2010 Types of Dementia
Dementia & Movement Disorders A/Prof Michael Davis Geriatrician ACT Health & GSAHS ANU Medical School Eastern Dementia Network Aged and Dementia Care Symposium Bateman s Bay, 22 October 2010 Types of Dementia
CLINICAL PRACTICE GUIDELINES FOR PHYSICAL THERAPY IN PATIENTS WITH PARKINSON'S DISEASE
 CLINICAL PRACTICE GUIDELINES FOR PHYSICAL THERAPY IN PATIENTS WITH PARKINSON'S DISEASE Charbel MACARI Physical Therapist, AUBMC Master in Neurological Rehabilitation OUTLINE Definition, Epidemiology and
CLINICAL PRACTICE GUIDELINES FOR PHYSICAL THERAPY IN PATIENTS WITH PARKINSON'S DISEASE Charbel MACARI Physical Therapist, AUBMC Master in Neurological Rehabilitation OUTLINE Definition, Epidemiology and
UNIFIED PARKINSON'S DISEASE RATING SCALE
 UNIFIED PARKINSON'S DISEASE RATING SCALE I. MENTATION, BEHAVIOR AND MOOD 1. Intellectual Impairment ne. 1 = Mild. Consistent forgetfulness with partial recollection of events and no other difficulties.
UNIFIED PARKINSON'S DISEASE RATING SCALE I. MENTATION, BEHAVIOR AND MOOD 1. Intellectual Impairment ne. 1 = Mild. Consistent forgetfulness with partial recollection of events and no other difficulties.
Follow-up Form B3: Evaluation Form Unified Parkinson s Disease Rating Scale (UPDRS 1 ) Motor Exam
 Motor Exam") phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu website: www.alz.washington.edu NACC Uniform Data Set (UDS) Follow-up Form B3: Evaluation Form Unified Parkinson s Disease Rating
phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu website: www.alz.washington.edu NACC Uniform Data Set (UDS) Follow-up Form B3: Evaluation Form Unified Parkinson s Disease Rating
Tone Management in Cerebral Palsy. Jenny Wilson, MD wilsjen@ohsu.edu OHSU and Shriners Hospital for Children October, 2015
 Tone Management in Cerebral Palsy Jenny Wilson, MD wilsjen@ohsu.edu OHSU and Shriners Hospital for Children October, 2015 Disclosures I am involved in a Dysport sponsored research study Goals Describe
Tone Management in Cerebral Palsy Jenny Wilson, MD wilsjen@ohsu.edu OHSU and Shriners Hospital for Children October, 2015 Disclosures I am involved in a Dysport sponsored research study Goals Describe
Sleep Difficulties. Insomnia. By Thomas Freedom, MD and Johan Samanta, MD
 Sleep Difficulties By Thomas Freedom, MD and Johan Samanta, MD For most people, night is a time of rest and renewal; however, for many people with Parkinson s disease nighttime is a struggle to get the
Sleep Difficulties By Thomas Freedom, MD and Johan Samanta, MD For most people, night is a time of rest and renewal; however, for many people with Parkinson s disease nighttime is a struggle to get the
Parkinson s Disease: Factsheet
 Parkinson s Disease: Factsheet Tower Hamlets Joint Strategic Needs Assessment 2010-2011 Executive Summary Parkinson s disease (PD) is a progressive neuro-degenerative condition that affects a person s
Parkinson s Disease: Factsheet Tower Hamlets Joint Strategic Needs Assessment 2010-2011 Executive Summary Parkinson s disease (PD) is a progressive neuro-degenerative condition that affects a person s
Parkinson s Disease and Tremors
 Parkinson s Disease and Tremors Current Strategies Leah Karliner, MD, MAS Division of General Internal Medicine Disclosures I have no conflicts of interest Parkinsonism neurological syndrome: Bradykinesia:
Parkinson s Disease and Tremors Current Strategies Leah Karliner, MD, MAS Division of General Internal Medicine Disclosures I have no conflicts of interest Parkinsonism neurological syndrome: Bradykinesia:
Dr. Enas Elsayed. Brunnstrom Approach
 Brunnstrom Approach Learning Objectives: By the end of this lab, the student will be able to: 1. Demonstrate different reflexes including stimulus and muscle tone response. 2. Demonstrate how to evoke
Brunnstrom Approach Learning Objectives: By the end of this lab, the student will be able to: 1. Demonstrate different reflexes including stimulus and muscle tone response. 2. Demonstrate how to evoke
NEUROLOCALIZATION MADE EASY
 NEUROLOCALIZATION MADE EASY Jared B. Galle, DVM, Diplomate ACVIM (Neurology) Dogwood Veterinary Referral Center 4920 Ann Arbor-Saline Road Ann Arbor, MI 48103 Localizing a neurologic problem to an anatomical
NEUROLOCALIZATION MADE EASY Jared B. Galle, DVM, Diplomate ACVIM (Neurology) Dogwood Veterinary Referral Center 4920 Ann Arbor-Saline Road Ann Arbor, MI 48103 Localizing a neurologic problem to an anatomical
MD pathophysiology. Phenomenology of movement disorders and gait disturbances. Phenomenology in MD. Hyperkinetic movements.
 MD pathophysiology Phenomenology of movement disorders and gait disturbances Genetic mutation or environmental injury of basal ganglia functioning Pallidum, thalamus, subthalamic nucleus, caudate nucleus,
MD pathophysiology Phenomenology of movement disorders and gait disturbances Genetic mutation or environmental injury of basal ganglia functioning Pallidum, thalamus, subthalamic nucleus, caudate nucleus,
PARKINSON S DISEASE INTRODUCTION. Parkinson s disease is defined as a disease of the nervous system that affects voluntary movement.
 PARKINSON S DISEASE INTRODUCTION Parkinson s disease is a disorder of the brain and the nervous system. It is one of the more common neurological diseases in people over the age of 60, and it is more common
PARKINSON S DISEASE INTRODUCTION Parkinson s disease is a disorder of the brain and the nervous system. It is one of the more common neurological diseases in people over the age of 60, and it is more common
Doctor I can t walk properly - a guided walk around some gait problems
 Doctor I can t walk properly - a guided walk around some gait problems Dr Jeremy Rees Consultant Neurologist National Hospital for Neurology and Neurosurgery, Queen Square www.london-neurology.co.uk Walking
Doctor I can t walk properly - a guided walk around some gait problems Dr Jeremy Rees Consultant Neurologist National Hospital for Neurology and Neurosurgery, Queen Square www.london-neurology.co.uk Walking
When it s time to apply for Social Security Disability Insurance: Making a stressful and complicated process easier for you and your family!
 When it s time to apply for Social Security Disability Insurance: Making a stressful and complicated process easier for you and your family! Presenter Disclosures Art Spencer The following personal financial
When it s time to apply for Social Security Disability Insurance: Making a stressful and complicated process easier for you and your family! Presenter Disclosures Art Spencer The following personal financial
ALL ABOUT SPASTICITY. www.almirall.com. Solutions with you in mind
 ALL ABOUT SPASTICITY www.almirall.com Solutions with you in mind WHAT IS SPASTICITY? The muscles of the body maintain what is called normal muscle tone, a level of muscle tension that allows us to hold
ALL ABOUT SPASTICITY www.almirall.com Solutions with you in mind WHAT IS SPASTICITY? The muscles of the body maintain what is called normal muscle tone, a level of muscle tension that allows us to hold
CEREBRAL PALSY CLASSIFICATION BY SEVERITY LEVEL
 Patient Name: Today s Date: CAUSE OF CEREBRAL PALSY Hypoxic-Ischemic Encephalopathy (HIE) or Intrapartum Asphyxia - Brain injury Lack of oxygen to the brain or asphyxia. Intracranial Hemorrhage (IVH) Brain
Patient Name: Today s Date: CAUSE OF CEREBRAL PALSY Hypoxic-Ischemic Encephalopathy (HIE) or Intrapartum Asphyxia - Brain injury Lack of oxygen to the brain or asphyxia. Intracranial Hemorrhage (IVH) Brain
Rörelserubbningar och Parkinson, hur svårt kan det vara. En översikt och problematisering av en folksjukdom Örjan Skogar, MD,PhD
 Rörelserubbningar och Parkinson, hur svårt kan det vara En översikt och problematisering av en folksjukdom Örjan Skogar, MD,PhD Man räknar med att 11-19 personer /100 000 invånare insjuknar i Parkinson
Rörelserubbningar och Parkinson, hur svårt kan det vara En översikt och problematisering av en folksjukdom Örjan Skogar, MD,PhD Man räknar med att 11-19 personer /100 000 invånare insjuknar i Parkinson
Multiple System Atrophy
 Multiple System Atrophy U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Multiple System Atrophy What is multiple system atrophy? Multiple system atrophy
Multiple System Atrophy U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Multiple System Atrophy What is multiple system atrophy? Multiple system atrophy
SLEEP AND PARKINSON S DISEASE
 A Practical Guide on SLEEP AND PARKINSON S DISEASE MICHAELJFOX.ORG Introduction Many people with Parkinson s disease (PD) have trouble falling asleep or staying asleep at night. Some sleep problems are
A Practical Guide on SLEEP AND PARKINSON S DISEASE MICHAELJFOX.ORG Introduction Many people with Parkinson s disease (PD) have trouble falling asleep or staying asleep at night. Some sleep problems are
Cerebellum and Basal Ganglia
 Cerebellum and Basal Ganglia 1 Contents Cerebellum and Basal Ganglia... 1 Introduction... 3 A brief review of cerebellar anatomy... 4 Basic Circuit... 4 Parallel and climbing fiber input has a very different
Cerebellum and Basal Ganglia 1 Contents Cerebellum and Basal Ganglia... 1 Introduction... 3 A brief review of cerebellar anatomy... 4 Basic Circuit... 4 Parallel and climbing fiber input has a very different
Infant reflexes and stereotypies are very important in the process of development
 Infant Reflexes and Stereotypies Infant reflexes and stereotypies are very important in the process of development 2007 McGraw-Hill Higher Education. All rights reserved. Importance of Infant Reflexes
Infant Reflexes and Stereotypies Infant reflexes and stereotypies are very important in the process of development 2007 McGraw-Hill Higher Education. All rights reserved. Importance of Infant Reflexes
ABC s of Parkinson s Disease 4/29/15 Karen Parenti, MS, PsyD
 ABC s of Parkinson s Disease 4/29/15 Karen Parenti, MS, PsyD What is Parkinson s Disease? Parkinson's disease is a progressive disorder of the nervous system that affects movement. It develops gradually,
ABC s of Parkinson s Disease 4/29/15 Karen Parenti, MS, PsyD What is Parkinson s Disease? Parkinson's disease is a progressive disorder of the nervous system that affects movement. It develops gradually,
Current evidence suggests that Parkinson s tends to develop
 About Parkinson's Diagnosing Parkinson s Current evidence suggests that Parkinson s tends to develop gradually and it may be many months, even years, before the symptoms become obvious enough for you to
About Parkinson's Diagnosing Parkinson s Current evidence suggests that Parkinson s tends to develop gradually and it may be many months, even years, before the symptoms become obvious enough for you to
REHABILITATION MEDICINE by PROFESSOR ANTHONY WARD
 REHABILITATION MEDICINE by PROFESSOR ANTHONY WARD What is Rehabilitation Medicine? Rehabilitation Medicine (RM) is the medical specialty with rehabilitation as its primary strategy. It provides services
REHABILITATION MEDICINE by PROFESSOR ANTHONY WARD What is Rehabilitation Medicine? Rehabilitation Medicine (RM) is the medical specialty with rehabilitation as its primary strategy. It provides services
Clinical Research in Parkinson s Disease: The Advances, Challenges, and Importance of Rater Training
 Clinical Research in Parkinson s Disease: The Advances, Challenges, and Importance of Rater Training Marian A. Ormont, MD epharmasolutions, A WIRB-Copernicus Group Company April is Parkinson s disease
Clinical Research in Parkinson s Disease: The Advances, Challenges, and Importance of Rater Training Marian A. Ormont, MD epharmasolutions, A WIRB-Copernicus Group Company April is Parkinson s disease
Michelle H. Cameron, M.D., P.T., M.C.R. Portland VA MS Center of Excellence- West, and Oregon Health & Science University
 Michelle H. Cameron, M.D., P.T., M.C.R. Portland VA MS Center of Excellence- West, and Oregon Health & Science University Ileana Howard, M.D. VA Puget Sound, Seattle, WA and University of Washington PVA
Michelle H. Cameron, M.D., P.T., M.C.R. Portland VA MS Center of Excellence- West, and Oregon Health & Science University Ileana Howard, M.D. VA Puget Sound, Seattle, WA and University of Washington PVA
Neurogenic Disorders of Speech in Children and Adults
 Neurogenic Disorders of Speech in Children and Adults Complexity of Speech Speech is one of the most complex activities regulated by the nervous system It involves the coordinated contraction of a large
Neurogenic Disorders of Speech in Children and Adults Complexity of Speech Speech is one of the most complex activities regulated by the nervous system It involves the coordinated contraction of a large
Reflex Physiology. Dr. Ali Ebneshahidi. 2009 Ebneshahidi
 Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
Management of Parkinson s Disease in Primary Care
 Management of Parkinson s Disease in Primary Care Dr June Tan National University Hospital System (NUHS) Division of Neurology Senior Consultant Topics: Diagnosing PD Choice of medication in the de novo
Management of Parkinson s Disease in Primary Care Dr June Tan National University Hospital System (NUHS) Division of Neurology Senior Consultant Topics: Diagnosing PD Choice of medication in the de novo
SLEEP DIFFICULTIES AND PARKINSON S DISEASE Julie H. Carter, R.N., M.S., A.N.P.
 SLEEP DIFFICULTIES AND PARKINSON S DISEASE Julie H. Carter, R.N., M.S., A.N.P. Problems with sleep are common in Parkinson s disease. They can sometimes interfere with quality of life. It is helpful to
SLEEP DIFFICULTIES AND PARKINSON S DISEASE Julie H. Carter, R.N., M.S., A.N.P. Problems with sleep are common in Parkinson s disease. They can sometimes interfere with quality of life. It is helpful to
Motor dysfunction 2: Spinal cord injury and subcortical motor disorders ANATOMY REVIEW: Basal Ganglia
 Motor dysfunction 2: Spinal cord injury and subcortical motor disorders ANATOMY REVIEW: Basal Ganglia A group of subcortical nuclei caudate, putamen, globus pallidus Caudate & Putamen = Neostriatum caudate
Motor dysfunction 2: Spinal cord injury and subcortical motor disorders ANATOMY REVIEW: Basal Ganglia A group of subcortical nuclei caudate, putamen, globus pallidus Caudate & Putamen = Neostriatum caudate
III./3.1.2. Parkinsonian syndrome (parkinsonism, atypical parkinsonian disorders) in neurodegenerative diseases
 in neurodegenerative diseases") III./3.1.2. Parkinsonian syndrome (parkinsonism, atypical parkinsonian disorders) in neurodegenerative diseases III./3.1.2.1. Multiple System Atrophy (MSA) MSA is a sporadic, adult onset degenerative neurological
III./3.1.2. Parkinsonian syndrome (parkinsonism, atypical parkinsonian disorders) in neurodegenerative diseases III./3.1.2.1. Multiple System Atrophy (MSA) MSA is a sporadic, adult onset degenerative neurological
WHAT IS CEREBRAL PALSY?
 WHAT IS CEREBRAL PALSY? Cerebral Palsy is a dysfunction in movement resulting from injury to or poor development of the brain prior to birth or in early childhood. Generally speaking, any injury or disease
WHAT IS CEREBRAL PALSY? Cerebral Palsy is a dysfunction in movement resulting from injury to or poor development of the brain prior to birth or in early childhood. Generally speaking, any injury or disease
American Chiropractic Association. Commentary on Centers for Medicare and Medicaid Services (CMS)/PART. Clinical Documentation Guidelines
/PART. Clinical Documentation Guidelines") American Chiropractic Association Commentary on Centers for Medicare and Medicaid Services (CMS)/PART Clinical Documentation Guidelines DISCLAIMER The American Chiropractic Association provides this commentary
American Chiropractic Association Commentary on Centers for Medicare and Medicaid Services (CMS)/PART Clinical Documentation Guidelines DISCLAIMER The American Chiropractic Association provides this commentary
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Hemiplegic shoulder pain/shoulder subluxation
 UPPER LIMB NEUROMUSCULAR ELECTRICAL STIMULATION: Electrode positions Please note that the polarity (red and black leads) can be altered according to your clinical reasoning. The area in which you want
UPPER LIMB NEUROMUSCULAR ELECTRICAL STIMULATION: Electrode positions Please note that the polarity (red and black leads) can be altered according to your clinical reasoning. The area in which you want
Coding and Documentation in Practice
 Coding and Documentation in Practice Great Exam Documentation By: Kathy Mills Chang Kathy Mills Chang is a Certified Medical Compliance Expert, Reimbursement Consultant, Medicare Specialist, and a Documentation
Coding and Documentation in Practice Great Exam Documentation By: Kathy Mills Chang Kathy Mills Chang is a Certified Medical Compliance Expert, Reimbursement Consultant, Medicare Specialist, and a Documentation
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Evaluating muscle injuries and residuals of shell fragment and gunshot wounds
 Evaluating muscle injuries and residuals of shell fragment and gunshot wounds Training conducted by: Michael Fishman and Sandrine Fisher 1 Objectives To become familiar with the application of the rating
Evaluating muscle injuries and residuals of shell fragment and gunshot wounds Training conducted by: Michael Fishman and Sandrine Fisher 1 Objectives To become familiar with the application of the rating
Cerebral palsy can be classified according to the type of abnormal muscle tone or movement, and the distribution of these motor impairments.
 The Face of Cerebral Palsy Segment I Discovering Patterns What is Cerebral Palsy? Cerebral palsy (CP) is an umbrella term for a group of non-progressive but often changing motor impairment syndromes, which
The Face of Cerebral Palsy Segment I Discovering Patterns What is Cerebral Palsy? Cerebral palsy (CP) is an umbrella term for a group of non-progressive but often changing motor impairment syndromes, which
Hoehn and Yahr Staging of Parkinson's Disease
 Hoehn and Yahr Staging of Parkinson's Disease, Unified Parkinson Disease Rating Scale (UPDRS), and Schwab and England Activities of Daily Living Disclaimer: The information and reference materials contained
Hoehn and Yahr Staging of Parkinson's Disease, Unified Parkinson Disease Rating Scale (UPDRS), and Schwab and England Activities of Daily Living Disclaimer: The information and reference materials contained
PHYSICAL THERAPY FOR PARKINSON S DISEASE. Ann Zylstra PT
 PHYSICAL THERAPY FOR PARKINSON S DISEASE Ann Zylstra PT PARKINSON S TEAM Nrsg/ MA Psych Family Support MD PT Social/ SW And much more Support Group s I&R Centers Friends/ family Church Other Person w PD
PHYSICAL THERAPY FOR PARKINSON S DISEASE Ann Zylstra PT PARKINSON S TEAM Nrsg/ MA Psych Family Support MD PT Social/ SW And much more Support Group s I&R Centers Friends/ family Church Other Person w PD
Parkinson s Disease and Dementia. Dr N Samaniego Consultant Physician and Geriatrician
 Parkinson s Disease and Dementia Dr N Samaniego Consultant Physician and Geriatrician Case 68 year old female. Off legs for a few months, O/E no neurological deficit. -Slowing down -Needs help with dressing,
Parkinson s Disease and Dementia Dr N Samaniego Consultant Physician and Geriatrician Case 68 year old female. Off legs for a few months, O/E no neurological deficit. -Slowing down -Needs help with dressing,
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
PRESCRIPTION DRUG ABUSE prevention
 PRESCRIPTION DRUG ABUSE prevention Understanding Drug Addiction Many people do not understand how someone could abuse drugs even when their life seems to be falling apart. It is often assumed that those
PRESCRIPTION DRUG ABUSE prevention Understanding Drug Addiction Many people do not understand how someone could abuse drugs even when their life seems to be falling apart. It is often assumed that those
UNIFIED PARKINSON'S DISEASE DATA FORM. 1 Mentation. Date: On Off On Off On Off On Off On Off On Off On Off On Off
 UNIFIED PARKINSON'S DISEASE DATA FORM Name: DOPA mg/day hrs DOPA lasts Date: Unit Number: On Off On Off On Off On Off On Off On Off On Off On Off 1 Mentation 2 Thought Disorder 3 Depression 4 Motivation/Initiative
UNIFIED PARKINSON'S DISEASE DATA FORM Name: DOPA mg/day hrs DOPA lasts Date: Unit Number: On Off On Off On Off On Off On Off On Off On Off On Off 1 Mentation 2 Thought Disorder 3 Depression 4 Motivation/Initiative
Clinical and Therapeutic Cannabis Information. Written by Cannabis Training University (CTU) All rights reserved
 All rights reserved") Clinical and Therapeutic Cannabis Information Written by Cannabis Training University (CTU) All rights reserved Contents Introduction... 3 Chronic Pain... 6 Neuropathic Pain... 8 Movement Disorders...
Clinical and Therapeutic Cannabis Information Written by Cannabis Training University (CTU) All rights reserved Contents Introduction... 3 Chronic Pain... 6 Neuropathic Pain... 8 Movement Disorders...
Treatment of Spastic Foot Deformities
 Penn Comprehensive Neuroscience Center Treatment of Spastic Foot Deformities Penn Neuro-Orthopaedics Service 1 Table of Contents Overview Overview 1 Treatment 2 Procedures 4 Achilles Tendon Lengthening
Penn Comprehensive Neuroscience Center Treatment of Spastic Foot Deformities Penn Neuro-Orthopaedics Service 1 Table of Contents Overview Overview 1 Treatment 2 Procedures 4 Achilles Tendon Lengthening
Factors Influencing Human Postures
 Chapter 3 Factors Influencing Human Postures 3.1 Introduction Postures and motions generated by the human body are very difficult to simulate since the human body has so many interrelated muscles that
Chapter 3 Factors Influencing Human Postures 3.1 Introduction Postures and motions generated by the human body are very difficult to simulate since the human body has so many interrelated muscles that
International Standards for the Classification of Spinal Cord Injury Motor Exam Guide
 C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
GLOSSARY OF TERMS. This glossary explains the terms and words often used in association with Parkinson s.
 Antagonist This glossary explains the terms and words often used in association with Parkinson s. Medications which have a negative effect on particular cells in the body. In Parkinson s dopamine antagonists
Antagonist This glossary explains the terms and words often used in association with Parkinson s. Medications which have a negative effect on particular cells in the body. In Parkinson s dopamine antagonists
Mr James Garrard University of Leicester May 2014
 Parkinson s disease exemplifies the art and science of geriatric medicine. Introduction First described by Dr. James Parkinson in the classic essay The Shaking Palsy in 1817 (1), Parkinson s disease is
Parkinson s disease exemplifies the art and science of geriatric medicine. Introduction First described by Dr. James Parkinson in the classic essay The Shaking Palsy in 1817 (1), Parkinson s disease is
Welcome to the Medical Risk Webinar: a taster of Assessing and Managing Medical Risk for Insurers courses. 26 April 2013
 Welcome to the Medical Risk Webinar: a taster of Assessing and Managing Medical Risk for Insurers courses 26 April 2013 1 Parkinson s Disease & Multiple Sclerosis Dr Nick Niven Jenkins 2 Movement Human
Welcome to the Medical Risk Webinar: a taster of Assessing and Managing Medical Risk for Insurers courses 26 April 2013 1 Parkinson s Disease & Multiple Sclerosis Dr Nick Niven Jenkins 2 Movement Human
SLEEP DISTURBANCE AND PSYCHIATRIC DISORDERS
 E-Resource December, 2013 SLEEP DISTURBANCE AND PSYCHIATRIC DISORDERS Between 10-18% of adults in the general population and up to 50% of adults in the primary care setting have difficulty sleeping. Sleep
E-Resource December, 2013 SLEEP DISTURBANCE AND PSYCHIATRIC DISORDERS Between 10-18% of adults in the general population and up to 50% of adults in the primary care setting have difficulty sleeping. Sleep
Medical Treatment Guidelines Washington State Department of Labor and Industries
 Complex regional pain syndrome (CRPS) Formerly known as reflex sympathetic dystrophy 1. Introduction This bulletin outlines the Department of Labor and Industries guidelines for diagnosing and treating
Complex regional pain syndrome (CRPS) Formerly known as reflex sympathetic dystrophy 1. Introduction This bulletin outlines the Department of Labor and Industries guidelines for diagnosing and treating
Spine Care Centre (SCC) protocols for Multiple Sclerosis Update 1 August 2015
 protocols for Multiple Sclerosis Update 1 August 2015") Spine Care Centre (SCC) protocols for Multiple Sclerosis Update 1 August 2015 Introduction Multiple sclerosis (MS) affects nerves in the brain and spinal cord, causing a wide range of symptoms including
Spine Care Centre (SCC) protocols for Multiple Sclerosis Update 1 August 2015 Introduction Multiple sclerosis (MS) affects nerves in the brain and spinal cord, causing a wide range of symptoms including
FUNCTIONAL EEG ANALYZE IN AUTISM. Dr. Plamen Dimitrov
 FUNCTIONAL EEG ANALYZE IN AUTISM Dr. Plamen Dimitrov Preamble Autism or Autistic Spectrum Disorders (ASD) is a mental developmental disorder, manifested in the early childhood and is characterized by qualitative
FUNCTIONAL EEG ANALYZE IN AUTISM Dr. Plamen Dimitrov Preamble Autism or Autistic Spectrum Disorders (ASD) is a mental developmental disorder, manifested in the early childhood and is characterized by qualitative
Role of Electrodiagnostic Tests in Neuromuscular Disease
 Role of Electrodiagnostic Tests in Neuromuscular Disease Electrodiagnostic tests Electroencephalogram (EEG) Electromyography (NCV, EMG) Cerebral evoked potentials (CEP) Motor evoked potentials (MEP) Electronystagmogram
Role of Electrodiagnostic Tests in Neuromuscular Disease Electrodiagnostic tests Electroencephalogram (EEG) Electromyography (NCV, EMG) Cerebral evoked potentials (CEP) Motor evoked potentials (MEP) Electronystagmogram
Webinar title: Know Your Options for Treating Severe Spasticity
 Webinar title: Know Your Options for Treating Severe Spasticity Presented by: Dr. Gerald Bilsky, Physiatrist Medical Director of Outpatient Services and Associate Medical Director of Acquired Brain Injury
Webinar title: Know Your Options for Treating Severe Spasticity Presented by: Dr. Gerald Bilsky, Physiatrist Medical Director of Outpatient Services and Associate Medical Director of Acquired Brain Injury
Personal Health Record
 Personal Health Record Contents Section 1: Personal details (pages 4 6) Within this section you can note all information about you, next of kin, important health information and general medical history.
Personal Health Record Contents Section 1: Personal details (pages 4 6) Within this section you can note all information about you, next of kin, important health information and general medical history.
P U T T I N G T H E P I E C E S T O G E T H E R
 MEDICAL THERAPY PROGRAM P U T T I N G T H E P I E C E S T O G E T H E R CALIFORNIA CHILDREN SERVICES CCS is a statewide program providing medical care and rehabilitation to children with physical disabilities.
MEDICAL THERAPY PROGRAM P U T T I N G T H E P I E C E S T O G E T H E R CALIFORNIA CHILDREN SERVICES CCS is a statewide program providing medical care and rehabilitation to children with physical disabilities.
Unmet Needs for Parkinson s Disease Therapeutics
 Unmet Needs for Parkinson s Disease Therapeutics Coalition Against Major Diseases & FDA Workshop October 20, 2014 Caroline M Tanner MD, PhD Director, Parkinson's Disease Research Education and Clinical
Unmet Needs for Parkinson s Disease Therapeutics Coalition Against Major Diseases & FDA Workshop October 20, 2014 Caroline M Tanner MD, PhD Director, Parkinson's Disease Research Education and Clinical
Developmental delay and Cerebral palsy. Present the differential diagnosis of developmental delay.
 Developmental delay and Cerebral palsy objectives 1. developmental delay Define developmental delay Etiologies of developmental delay Present the differential diagnosis of developmental delay. 2. cerebral
Developmental delay and Cerebral palsy objectives 1. developmental delay Define developmental delay Etiologies of developmental delay Present the differential diagnosis of developmental delay. 2. cerebral
---------------------
 EVERYTHING YOU NEED TO KNOW ABOUT PARKINSON S DISEASE --------------------- THE TOP 101 QUESTIONS ABOUT PARKINSON S DISEASE By Lianna Marie Copyright 2005 Lianna Marie All rights reserved. No part of this
EVERYTHING YOU NEED TO KNOW ABOUT PARKINSON S DISEASE --------------------- THE TOP 101 QUESTIONS ABOUT PARKINSON S DISEASE By Lianna Marie Copyright 2005 Lianna Marie All rights reserved. No part of this
Range of Motion Exercises
 Range of Motion Exercises Range of motion (ROM) exercises are done to preserve flexibility and mobility of the joints on which they are performed. These exercises reduce stiffness and will prevent or at
Range of Motion Exercises Range of motion (ROM) exercises are done to preserve flexibility and mobility of the joints on which they are performed. These exercises reduce stiffness and will prevent or at
Mental health issues in the elderly. January 28th 2008 Presented by Éric R. Thériault etheriau@lakeheadu.ca
 Mental health issues in the elderly January 28th 2008 Presented by Éric R. Thériault etheriau@lakeheadu.ca Cognitive Disorders Outline Dementia (294.xx) Dementia of the Alzheimer's Type (early and late
Mental health issues in the elderly January 28th 2008 Presented by Éric R. Thériault etheriau@lakeheadu.ca Cognitive Disorders Outline Dementia (294.xx) Dementia of the Alzheimer's Type (early and late
Passive Range of Motion Exercises
 Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Physical Therapy Perspective on Ataxia. Roger Fong, MPT University of Chicago Medical Center March, 2010
 Physical Therapy Perspective on Ataxia Roger Fong, MPT University of Chicago Medical Center March, 2010 Definition: Physical Therapist Physical therapy dynamic profession with an established theoretical
Physical Therapy Perspective on Ataxia Roger Fong, MPT University of Chicago Medical Center March, 2010 Definition: Physical Therapist Physical therapy dynamic profession with an established theoretical
Non-Surgical Treatments for Spasticity in Cerebral Palsy and Similar Conditions by Susan Agrawal
 www.complexchild.com Non-Surgical Treatments for Spasticity in Cerebral Palsy and Similar Conditions by Susan Agrawal Children with cerebral palsy and other conditions that affect muscle tone often present
www.complexchild.com Non-Surgical Treatments for Spasticity in Cerebral Palsy and Similar Conditions by Susan Agrawal Children with cerebral palsy and other conditions that affect muscle tone often present
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 Rehabilitation for movement difficulties after stroke bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online.
Rehabilitation for movement difficulties after stroke bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online.
WalkAide. Long term cost effectiveness of FES. J of Rehab Med 2013; 45(2):154 60 Humphreys et al
:154 60 Humphreys et al") WalkAide Long term cost effectiveness of FES J of Rehab Med 2013; 45(2):154 60 Humphreys et al 126 people (62 stroke, 39 MS, 7 SCI, 3 CP, 15 other) Mean time of FES use 3.6 years 33 using FES after 11.1
WalkAide Long term cost effectiveness of FES J of Rehab Med 2013; 45(2):154 60 Humphreys et al 126 people (62 stroke, 39 MS, 7 SCI, 3 CP, 15 other) Mean time of FES use 3.6 years 33 using FES after 11.1
How to identify, approach and assist employees with young onset dementia: A guide for employers
 How to identify, approach and assist employees with young onset dementia: A guide for employers What is dementia? Dementia involves the decline of cognitive functions. Young Onset Dementia, also known
How to identify, approach and assist employees with young onset dementia: A guide for employers What is dementia? Dementia involves the decline of cognitive functions. Young Onset Dementia, also known
An Introduction to Lewy Body Dementia
 An Introduction to Lewy Body Dementia A special publication for people newly diagnosed with Lewy body dementia and those still seeking answers. You don t have to face LBD alone. Increasing Knowledge Sharing
An Introduction to Lewy Body Dementia A special publication for people newly diagnosed with Lewy body dementia and those still seeking answers. You don t have to face LBD alone. Increasing Knowledge Sharing
Check List for identifying Special Needs Children among School age children. Cerebral Palsy
 Check List for identifying Special Needs Children among School age children Cerebral Palsy Sl. 1. The child has drooling? 2. The child has problems in controlling voluntary movements? 3. The child has
Check List for identifying Special Needs Children among School age children Cerebral Palsy Sl. 1. The child has drooling? 2. The child has problems in controlling voluntary movements? 3. The child has
1: Motor neurone disease (MND)
") 1: Motor neurone disease (MND) This section provides basic facts about motor neurone disease (MND) and its diagnosis. The following information is an extracted section from our full guide Living with motor
1: Motor neurone disease (MND) This section provides basic facts about motor neurone disease (MND) and its diagnosis. The following information is an extracted section from our full guide Living with motor
The type of cancer Your specific treatment Your pre training levels before diagnose (your current strength and fitness levels)
") Exercise and Breast Cancer: Things you can do! Cancer within the fire service is one of the most dangerous threats to our firefighter s health & wellness. According to the latest studies firefighters are
Exercise and Breast Cancer: Things you can do! Cancer within the fire service is one of the most dangerous threats to our firefighter s health & wellness. According to the latest studies firefighters are
National Hospital for Neurology and Neurosurgery. Managing Spasticity. Spasticity Service
 National Hospital for Neurology and Neurosurgery Managing Spasticity Spasticity Service If you would like this document in another language or format, or require the services of an interpreter please contact
National Hospital for Neurology and Neurosurgery Managing Spasticity Spasticity Service If you would like this document in another language or format, or require the services of an interpreter please contact
Alzheimer's: The Latest Assessment and Treatment Strategies
 Questions from chapter 1 Alzheimer's: The Latest Assessment and Treatment Strategies 1) What is a loss of cognitive and intellectual powers without changes in consciousness. a) dementia b) delusions c)
Questions from chapter 1 Alzheimer's: The Latest Assessment and Treatment Strategies 1) What is a loss of cognitive and intellectual powers without changes in consciousness. a) dementia b) delusions c)
A GUIDE FOR THE NEW PATIENT. supported by the Neurological Foundation
 PARKINSON S A GUIDE FOR THE NEW PATIENT supported by the Neurological Foundation INTRODUCTION 1 Contents 1. Introduction 2. Parkinson s 3. The main symptoms of Parkinson s 6. What causes Parkinson s? 7.
PARKINSON S A GUIDE FOR THE NEW PATIENT supported by the Neurological Foundation INTRODUCTION 1 Contents 1. Introduction 2. Parkinson s 3. The main symptoms of Parkinson s 6. What causes Parkinson s? 7.
Cerebral Palsy. www.teachinngei.org p. 1
 Cerebral Palsy What is cerebral palsy? Cerebral palsy (CP) is a motor disability caused by a static, non-progressive lesion (encephalopathy) in the brain that occurs in early childhood, usually before
Cerebral Palsy What is cerebral palsy? Cerebral palsy (CP) is a motor disability caused by a static, non-progressive lesion (encephalopathy) in the brain that occurs in early childhood, usually before
Review Last Lecture. Definition of Gait? What are the 2 phases of gait? 5 parts of stance phase? 3 parts of swing phase?
 Abnormal Gait Review Last Lecture Definition of Gait? What are the 2 phases of gait? 5 parts of stance phase? 3 parts of swing phase? Abnormal Gait An altered gait pattern reflecting any lower extremity
Abnormal Gait Review Last Lecture Definition of Gait? What are the 2 phases of gait? 5 parts of stance phase? 3 parts of swing phase? Abnormal Gait An altered gait pattern reflecting any lower extremity
CENTRAL NERVOUS SYSTEM MANAGEMENT OF PARKINSON S DISEASE
 MANAGEMENT CENTRAL NERVOUS SYSTEM MANAGEMENT OF PARKINSON S DISEASE Parkinson s Disease is classically determined by the triad or rest tremor (usually starting in one arm) with bradykinesia (slowing of
MANAGEMENT CENTRAL NERVOUS SYSTEM MANAGEMENT OF PARKINSON S DISEASE Parkinson s Disease is classically determined by the triad or rest tremor (usually starting in one arm) with bradykinesia (slowing of
Muscular Dystrophy. By. Tina Strauss
 Muscular Dystrophy By. Tina Strauss Story Outline for Presentation on Muscular Dystrophy What is Muscular Dystrophy? Signs & Symptoms Types When to seek medical attention? Screening and Diagnosis Treatment
Muscular Dystrophy By. Tina Strauss Story Outline for Presentation on Muscular Dystrophy What is Muscular Dystrophy? Signs & Symptoms Types When to seek medical attention? Screening and Diagnosis Treatment
A 34-year-old female with a history of multiple sclerosis (MS) returns to the neurology clinic for follow-up.
 returns to the neurology clinic for follow-up.") Complementary and Alternative Medicine in Multiple Sclerosis Case Presentation: A 34-year-old female with a history of multiple sclerosis (MS) returns to the neurology clinic for follow-up. The patient
Complementary and Alternative Medicine in Multiple Sclerosis Case Presentation: A 34-year-old female with a history of multiple sclerosis (MS) returns to the neurology clinic for follow-up. The patient
SPECIMEN. Interactive Training DVD-ROM for a standardised, quantified neurological examination and assessment of Kurtzke s Functional Systems and
 Definitions for a standardised, quantified neurological examination and assessment of Kurtzke s Functional Systems and Expanded Disability Status Scale in Multiple Sclerosis Independent Internet Platform
Definitions for a standardised, quantified neurological examination and assessment of Kurtzke s Functional Systems and Expanded Disability Status Scale in Multiple Sclerosis Independent Internet Platform