December 6, 2010 Pediatric Severe Asthma
|
|
|
- Adrian Cole
- 7 years ago
- Views:
Transcription
1 December 6, 2010 Pediatric Severe Asthma Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens Mercy Hospital Kansas City, Missouri Professor of Pediatrics, Medicine and Basic Science University of Missouri Kansas City School of Medicine

2
3 Disclosure Statement Lanny J. Rosenwasser, MD RESEARCH STUDIES Alcon,A-Z, GlaxoSmithKline, MBBH/MacArthur Foundation, National Institutes of Health CONSULTANT Abbott Corp, Alcon, Alexion, Altana Pharmaceuticals, A-Z,Biogen Idec Corp, Genentech, GlaxoSmithKline, Merck, Novartis, Sanofi-Aventis SPEAKERS BUREAU Alcon, Banyu Pharmaceuticals, Genentech, Merck, Novartis
4 Characteristics of Asthma Narrowing of the airways Airway obstruction Airway inflammation Increased airway responsiveness NHLBI, NAEPP, 1997.
5 Immunohistopathologic Features of Asthma Denudation of airway epithelium Collagen deposition beneath basement membrane Edema Mast cell activation Inflammatory cell infiltration Neutrophils Eosinophils Lymphocytes (TH-2 like cells) NHLBI, NAEPP, 1997.
6 Airway Remodeling Airway Wall Thickening Subepithelial Fibrosis Increased Myocyte Mass Myofibroblast Hyperplasia Mucous Metaplasia
7 Airway Remodeling: Physiologic Consequences Irreversible/Partially Reversible Airway Obstruction Airway Hyper-responsiveness responsiveness Greater Decline in FEV1 than Controls (38ml/yr vs. 22ml/yr)

8

9
10 Regulatory T Lymphocytes CD4 +, CD25 + T lymphocytes Regulatory Express TGFβ, IL-10 Suppressive to other T cells Express Foxp3 transcription factor IL-34, IL-35 growth factors
11 Complexity of Asthma Several orders of magnitude more complex Proteome, Transcriptome, Genome Tissues, Organs, Whole Body, Brain Third and Fourth Dimensions
12 Background First Asthma Guidelines Airway inflammation was central feature of asthma - Characteristics of asthma severity described - Asthma treatment based on disease severity - Proposed outcomes to be achieved
13 Stepwise Approach for Managing Intermittent Asthma Step 1 Preferred: SABA PRN Asthma in Patients Consult with asthma specialist Aged if Step 4 care 12 or higher is requi Years Consider consultation at Step 3. Step 2 Preferred: Low-dose ICS (A) Alternative: Cromolyn (A), LTRA (A), Nedocromil (A), or Theophylline (B) Persistent Asthma: Daily Medication Consult with asthma specialist if Step 4 care or higher is required. red. Step 3 Preferred: Low-dose ICS + LABA (A) OR Medium-dose dose ICS (A) Alternative: Low-dose ICS + either LTRA (A), Theophylline (B), or Zileuton (D) Step 4 Preferred: Medium-dose dose ICS + LABA (B) Alternative: Medium-dose dose ICS + either LTRA (B), Theophylline (B), or Zileuton (D) Step 5 Preferred: High-dose ICS + LABA (B) ICS = inhaled corticosteroids; LABA = long-acting β 2 -agonist; LTRA = leukotriene receptor antagonist. Adapted from National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR ). U.S. Department of Health and Human Services. Available at: Accessed August 29, AND Consider Omalizumab for Patients Who Have Allergies (B) Step 6 Preferred: High-dose ICS + LABA + Oral Corticosteroid AND Consider Omalizumab for Patients Who Have Allergies Each Step: Patient education, environmental control, and management ent of comorbidities Steps 2-4: 2 Consider subcutaneous allergen immunotherapy for patients who have allergic asthma Quick-Relief Medication for All Patients SABA as needed for symptoms. Intensity of treatment depends on severity s of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of systemic oral corticosteroids osteroids may be needed Use of SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control and the need to step up treatment Step Up If Needed (first, check adherence, environmental control, and comorbid conditions) Assess Control Step Down If Possible (and asthma is well controlled at least 3 months)
14 Anti IgE Targets IgE, FCeRI Rhu Mab - E25 - Omalizumab, Xolair Reduces Free IgE (allergen specific) Reduces Eos (sputum, BAL, blood) Reduces FCeRI and FCeRII expression Efficacy - Asthma, AR
15 Major Changes in Long-Term Management Recommendations for three age groups presented separately years years - 12 years Expanded steps of therapy - 6 steps to simplify the action within each step - Medium dose ICS OR low dose ICS + LABA for patients not controlled on low dose ICS - Consider omalizumab for allergic patients not controlled on medium dose ICS + LABA
16 Definitions Severity: the intrinsic intensity of the disease process, measured clinically in untreated patients or by the least amount of medicine required to achieve control Control: the degree to which the manifestations of asthma (symptoms, functional impairment, and risk of untoward events) are minimized and the goals of therapy are met Responsiveness: the ease with which control is achieved by therapy
17 Domains of Severity and Control Impairment - Symptoms (day, night) - Reliever therapy - Activity - Lung function Risk - Exacerbation - Loss of lung function - Medication side effects
18 Steps of Therapy Preferred medications: Best balance of efficacy and safety in clinical trials for patients at that level of severity Must be tailored to individual patients needs, circumstances, and responsiveness
19 Principles of Step Therapy to Achieve Control Step up if not controlled If very poorly controlled, consider increase by 2 steps, oral corticosteroids, or both Before increasing pharmacologic therapy, consider as targets for therapy - Adverse environmental exposures - Poor adherence - Co-morbidities
20 DRAFT Asthma Guidelines Stepwise approach to therapy - 3 age groups Youths 12 years and adults Children 5 to 11 years of age Children 0 to 4 years of age
21 Key Recommendations Managing asthma in children 5-11 years Severity classification should guide initial therapy decisions. ICS are preferred initial long-term controller. Asthma control assessment should guide therapy adjustments.
22 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 5 11 YEARS OF AGE Components of Control Risk Reduction in lung growth Treatment-related adverse effects Recommended Action for Treatment (See figure 4-1bfor treatment steps.) Classification of Asthma Control (5 11 years of age) Well Controlled Maintain current step. Regular followup every 3 6 months. Consider step down if well controlled for at least 3 months. Not Well Controlled Evaluation requires long-termfollowup. Step up at least 1 step and Reevaluate in 2 6 weeks. For side effects: consider alternative treatment options. Very Poorly Controlled Medication side effects can vary in intensity fromnone to very troublesome and worrisome. The level of intensity does not correlate to specificlevels of control but should be considered in the overall assessment of risk. Consider short course of systemic oral corticosteroids, Step up 1 2 steps, and Reevaluate in 2 weeks. For side effects: consider alternative treatment options.
23 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 5 11 YEARS OF AGE Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 care or higher is required. Consider consultation at step 3. Step 1 Preferred: SABA PRN Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn, Nedocromil, or Theophylline Step 3 Preferred: Medium-dose ICS OR Low-dose ICS + either LABA, LTRA, or Theophylline Step 4 Preferred: Medium-dose ICS + LABA Alternative: Medium-dose ICS + either LTRA or Theophylline Step 5 Preferred: High-dose ICS + LABA Alternative: High-dose ICS + either LTRA or Theophylline AND Omalizumab may be considered for patients who have allergies Step 6 Preferred: High-dose ICS + LABA + oral corticosteroid Alternative: High-dose ICS + either LTRA or Theophylline + oral corticosteroid AND Omalizumab may be considered for patients who have allergies Step up if needed (first, check adherence and environmental control and comorbid conditions) Assess control Step down if possible (and asthma is well controlled at least 3 months)
24 Key Recommendations Managing asthma in children 0-4 years Diagnosis is often difficult. Treatment has not been adequately studied. Criteria for initiation of long-term-control therapy: 3 wheezing episodes in past year and positive asthma risk profile. those who require symptomatic treatment > 2 days per week two or more severe exacerbations within 6 months
25 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 0 4 YEARS OF AGE Components of Control Classification of Asthma Control (0 4 years of age) Well Controlled Not Well Controlled Very Poorly Controlled Symptoms 2 days/week >2 days/week Throughout the day Nighttime awakenings 1/month >1x/month >1x/week Impairment Interference with normal activity None Some limitation Extremely limited Short-acting beta 2 -agonist use for symptom control (not prevention of EIB) 2 days/week >2 days/week Several times per day
26 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 0 4 YEARS OF AGE Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 3 care or higher is required. Consider consultation at step 2. Step 1 Preferred: SABA PRN Step 2 Preferred: Low-dose ICS Alternative: Montelukast or Cromolyn Step 3 Preferred: Medium-dose ICS Step 4 Preferred: Medium-dose ICS AND Either: Montelukast or LABA Step 5 Preferred: High-dose ICS AND Either: Montelukast or LABA Step 6 Preferred: High-dose ICS AND Either: Montelukast or LABA AND Oral corticosteroids Step up if needed (first, check adherence and environmental control) Assess control Step down if possible (and asthma is well controlled at least 3 months)
27 ESTIMATED COMPARATIVE DAILY DOSAGES FOR INHALED CORTICOSTEROIDS IN CHILDREN Drug Beclomethasone HFA 40 or 80 mcg/puff Budesonide DPI 200 mcg/inhalation Inhalation suspension for nebulization (child dose) Flunisolide 250 mcg/puff Flunisolide-HFA 80 mcg/puff Fluticasone-HFA MDI: 44, 110, or 220 mcg/puff DPI: 50, 100, or 250 mcg/inhalation Mometasone DPI 200 mcg/inhalation Triamcinolone acetonide 75 mcg/puff Low Daily Dose Medium Daily Dose High Daily Dose Child <5 Child 5 11 Child <5 Child mg Child <5 Child mcg > mcg >320 mcg mcg > mcg >800 mcg 0.5 mg mg 1.0 mg >1.0 mg 2.0 mg mcg 1,000 1,250 mcg >1,250 mcg 160 mcg 320 mcg 640 mcg 176 mcg mcg mcg NA = not approved and no data available for children less than 12 years of age mcg 352 mcg >352 mcg mcg mcg >400 mcg NA NA NA mcg mcg >900 mcg

28
29 Poor Response to Medications Social Issues Patient Related Drug Host Related
30 Poor Response to Medications Social Issues: Barriers to care (lack of insurance) Complexity of Disease/Treatment Poor Provider Patient Interactions Breakdown in Patient Education
31 Poor Response to Medications Patient Related: Non Compliance Psychological Problems (Depression) Poor Perception of Disease and Symptoms
32 Poor Response to Medications Drug/Host Biologic Related: Side Effects Lack of Benefit Cost Lack of Biomarkers Pharmocokinetics (poor absorption, frequent dosing) Pharmocogenetics

33
34 PHARMACOGENETICS STUDIES IN VARIATION OF DRUG RESPONSE Population variations > individual variation Repeatability V g + V Eg r = V P
35 Pharmacogenetics Pathways of AsthmaTreatment Arachidonate Metabolism ALOX 5 LTC 4 Synthase Bronchodilation B 2 AR Immune/Inflammatory IL-4/IL-4R IL-13/IL-13R GCR
36 FCER2 Pleiotropic Effects FCER2 SNP Allele G9782a12 [T/G] G9782a19 [T/C] G9782a26 [C/T] G9782a5 [C/T] G9782a8 [C/A] Forest Haplotype Phenotype Frequency P-Value TTCCC BD % Change TCTCA BD Extremes GTCTA Steroid Extremes CAMP Haplotype Phenotype Frequency P-Value GTCTA BD % Change GTCTA BD % Change 1 yr GTCTA BD % Change 4 yr TCTTA Steroid % Ch. 1 yr TTCCC Steroid % Ch. 4 yr Global P value for Steroid % Change 1 yr = 0.001
37 FCER2 GCTTA Haplotype % with Haplotype Hospitalizations ER Visits Yes No p = (Hosp) and 0.01 (ER)
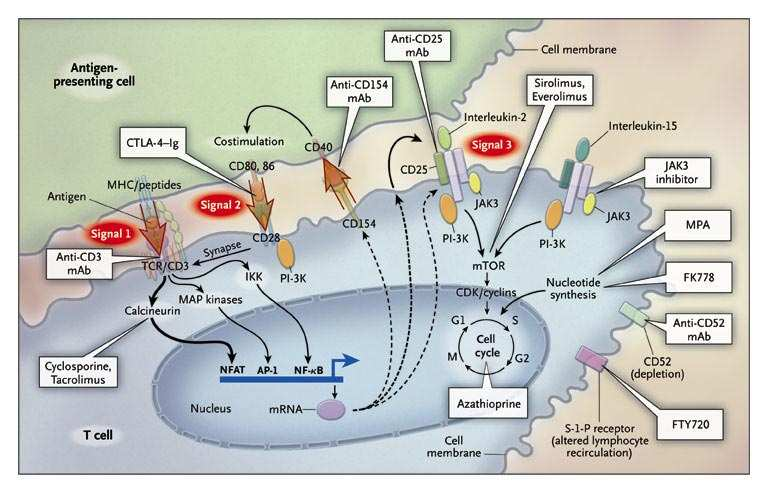
38 IMMUNOMODULATORS Closer to Pathogenesis Disease Altering and Modifying Wave of the future Cost effectiveness will progress Can be applied to Immunotherapy
39 Cytokine Modulation: Therapeutic Implications in Asthma Cytokine/Cytokine Antagonist Mechanism Receptor Antagonists: Interleukin 1 Receptor Antagonist Inhibition of cytokine-mediated Soluble Interleukin-4 Receptor signal transduction Soluble Interleukin-1 receptor Antibodies: Cytokine Inactivation Humanized Anti-IL-5-Antibodies Humanized Anti-TNF Antibodies Cytokines with Anti-allergic inflammatory activities: Interferon-γ Il-4 Antagonist Interleukin-12 TH1-like lymphocyte differentiation Interleukin-10, TGF-β Anti-inflammatory cytokines
40


41 Key Central Role of IL-5 5 in Asthma
42 J ALLERGY IMMUNOL 2010 APR
43 Anti-IL IL-5 5 in Human Asthma: Reduction in Exacerbations Haldar P et al. New Engl J Med 2009;360:973 Nair P et al. New Engl J Med 2009;360:985 Severe (CCS-dependent) asthma Sputum eosinophilia required for enrollment No improvement in FEV1, control, symptoms
44 Anti-IL IL-5 5 in Human Asthma: Haldar P et al. New Engl J Med 2009;360:973 Nair P et al. New Engl J Med 2009;360:985
45
46
47 Allergy Systems Biology Approach to Allergic Cascades Bio Therapeutics Pharmacogenetic Profiling Early Intervention

48
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age
 Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Objectives. Asthma Management
 Objectives Asthma Management BREATHE Conference Allergy and Asthma Specialists PC Christine Malloy MD March 22, 2013 Review the role of inflammation in asthma Discuss the components of the EPR-3 management
Objectives Asthma Management BREATHE Conference Allergy and Asthma Specialists PC Christine Malloy MD March 22, 2013 Review the role of inflammation in asthma Discuss the components of the EPR-3 management
Dear Provider: Sincerely,
 Asthma Toolkit Dear Provider: L.A. Care is pleased to present this updated asthma toolkit. Our goal is to promote the highest level of asthma care, based on the 2007 National Asthma Education and Prevention
Asthma Toolkit Dear Provider: L.A. Care is pleased to present this updated asthma toolkit. Our goal is to promote the highest level of asthma care, based on the 2007 National Asthma Education and Prevention
Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus
 Asthma Pocket Guide for Primary Care Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus POSITION STATEMENT Despite advances in therapy, asthma remains a disease
Asthma Pocket Guide for Primary Care Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus POSITION STATEMENT Despite advances in therapy, asthma remains a disease
Training Manual & Speaker s Guide
 Training Manual & Speaker s Guide Based on National Asthma Education and Prevention Program (NAEPP) Guidelines including the NAEPP s Guidelines Implementation Panel (GIP) Priority Messages. Funded in part
Training Manual & Speaker s Guide Based on National Asthma Education and Prevention Program (NAEPP) Guidelines including the NAEPP s Guidelines Implementation Panel (GIP) Priority Messages. Funded in part
How to Manage Asthma in Children
 Clinical Guideline for the Diagnosis, Evaluation and Management of Adults and Children with Asthma Color Key n Four Components of Asthma Care n Classifying Asthma Severity, Assessing Asthma Control and
Clinical Guideline for the Diagnosis, Evaluation and Management of Adults and Children with Asthma Color Key n Four Components of Asthma Care n Classifying Asthma Severity, Assessing Asthma Control and
Managing Asthma Long Term
 Managing Asthma Long Term TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS F I G U R E 4 2 a. CLASSIFYING ASTHMA SEVERITY AND INITIATING TREATME N T IN CHILDREN 0 4
Managing Asthma Long Term TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS F I G U R E 4 2 a. CLASSIFYING ASTHMA SEVERITY AND INITIATING TREATME N T IN CHILDREN 0 4
An Overview of Asthma - Diagnosis and Treatment
 An Overview of Asthma - Diagnosis and Treatment Asthma is a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness,
An Overview of Asthma - Diagnosis and Treatment Asthma is a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness,
Asthma in Infancy, Childhood and Adolescence. Presented by Frederick Lloyd, MD Palo Alto Medical Foundation Palo Alto, California
 Asthma in Infancy, Childhood and Adolescence Presented by Frederick Lloyd, MD Palo Alto Medical Foundation Palo Alto, California Major Health Problem in Childhood Afflicts 2.7 million children in the USA
Asthma in Infancy, Childhood and Adolescence Presented by Frederick Lloyd, MD Palo Alto Medical Foundation Palo Alto, California Major Health Problem in Childhood Afflicts 2.7 million children in the USA
Asthma (With a little SCID to start) Disclosures Outline Starting with the Immune System The Innate Immune System The Adaptive Immune System
 Disclosures Outline Starting with the Immune System The Innate Immune System The Adaptive Immune System") 1 2 3 4 5 6 7 8 9 Asthma (With a little SCID to start) Lauren Smith, MD CHKD Pediatric Allergy/Immunology Disclosures None Will be discussing some medications that are not yet FDA approved Outline SCID
1 2 3 4 5 6 7 8 9 Asthma (With a little SCID to start) Lauren Smith, MD CHKD Pediatric Allergy/Immunology Disclosures None Will be discussing some medications that are not yet FDA approved Outline SCID
9/16/2014. Anti-Immunoglobulin E (IgE) Omalizumab (Xolair ) Dosing Guidance
 Omalizumab (Xolair ) Dosing Guidance") Disclosure Statement of Financial Interest New Therapies for Asthma Including Omalizumab and Anti-Cytokine Therapies Marsha Dangler, PharmD, BCACP Clinical Pharmacy Specialist James H. Quillen VA Medical
Disclosure Statement of Financial Interest New Therapies for Asthma Including Omalizumab and Anti-Cytokine Therapies Marsha Dangler, PharmD, BCACP Clinical Pharmacy Specialist James H. Quillen VA Medical
Guidance to support the stepwise review of combination inhaled corticosteroid therapy for adults ( 18yrs) in asthma
 in asthma") Guidance to support the stepwise review of combination inhaled corticosteroid therapy for adults ( 18yrs) in asthma Important Complete asthma control needs to be achieved for at least 12 weeks before attempting
Guidance to support the stepwise review of combination inhaled corticosteroid therapy for adults ( 18yrs) in asthma Important Complete asthma control needs to be achieved for at least 12 weeks before attempting
Stanley J. Szefler, MD National Jewish Medical and Research Center
 New Asthma Guidelines: Special Attention to Infant Wheezers Stanley J. Szefler, MD Helen Wohlberg & Herman Lambert Chair in Pharmacokinetics, & Professor of Pediatrics and Pharmacology, University of Colorado
New Asthma Guidelines: Special Attention to Infant Wheezers Stanley J. Szefler, MD Helen Wohlberg & Herman Lambert Chair in Pharmacokinetics, & Professor of Pediatrics and Pharmacology, University of Colorado
understanding the professional guidelines
 SEVERE ASTHMA understanding the professional guidelines This guide includes information on what the European Respiratory Society (ERS) and the American Thoracic Society (ATS) have said about severe asthma.
SEVERE ASTHMA understanding the professional guidelines This guide includes information on what the European Respiratory Society (ERS) and the American Thoracic Society (ATS) have said about severe asthma.
Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis, and asthma
 Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Clinical Research Pediatric Pulmonary Division
 Clinical Research Pediatric Pulmonary Division Hengameh H. Raissy, PharmD Research Associate Professor, Pediatric Pulmonary UNM HSC Director of Clinical Trials Presented at Envision NM Asthma / Pulmonary
Clinical Research Pediatric Pulmonary Division Hengameh H. Raissy, PharmD Research Associate Professor, Pediatric Pulmonary UNM HSC Director of Clinical Trials Presented at Envision NM Asthma / Pulmonary
The Annual Direct Care of Asthma
 The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
How to use FENO-guided asthma control in routine clinical practice
 How to use FENO-guided asthma control in routine clinical practice Asthma is a chronic inflammatory disease of the airways. This has implications for the diagnosis, management and potential prevention
How to use FENO-guided asthma control in routine clinical practice Asthma is a chronic inflammatory disease of the airways. This has implications for the diagnosis, management and potential prevention
Glucocorticoids, Inhaled Therapeutic Class Review (TCR)
") Glucocorticoids, Inhaled Therapeutic Class Review (TCR) July 31, 2015 No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying,
Glucocorticoids, Inhaled Therapeutic Class Review (TCR) July 31, 2015 No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying,
Background information
 Background information Asthma Asthma is a complex disease affecting the lungs that can be managed but cannot be cured. 1 Asthma can be controlled well in most people most of the time, although some people
Background information Asthma Asthma is a complex disease affecting the lungs that can be managed but cannot be cured. 1 Asthma can be controlled well in most people most of the time, although some people
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Glucocorticoids, Inhaled Therapeutic Class Review (TCR) February 7, 2012
 February 7, 2012") Glucocorticoids, Inhaled Therapeutic Class Review (TCR) February 7, 2012 No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying,
Glucocorticoids, Inhaled Therapeutic Class Review (TCR) February 7, 2012 No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying,
Pre-Operative Services Teaching Rounds 2 Jan 2011
 Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Management of Asthma
 Federal Bureau of Prisons Clinical Practice Guidelines May 2013 Clinical guidelines are made available to the public for informational purposes only. The Federal Bureau of Prisons (BOP) does not warrant
Federal Bureau of Prisons Clinical Practice Guidelines May 2013 Clinical guidelines are made available to the public for informational purposes only. The Federal Bureau of Prisons (BOP) does not warrant
Drugs for treatment of respiratory diseases. Huifang Tang Department of pharmacology Zhejiang University, school of medicine tanghuifang@zju.edu.
 Drugs for treatment of respiratory diseases Huifang Tang Department of pharmacology Zhejiang University, school of medicine tanghuifang@zju.edu.cn Antiasthmatic drugs Immunological and non-immunological
Drugs for treatment of respiratory diseases Huifang Tang Department of pharmacology Zhejiang University, school of medicine tanghuifang@zju.edu.cn Antiasthmatic drugs Immunological and non-immunological
Prevention of Acute COPD exacerbations
 December 3, 2015 Prevention of Acute COPD exacerbations George Pyrgos MD 1 Disclosures No funding received for this presentation I have previously conducted clinical trials with Boehringer Ingelheim. Principal
December 3, 2015 Prevention of Acute COPD exacerbations George Pyrgos MD 1 Disclosures No funding received for this presentation I have previously conducted clinical trials with Boehringer Ingelheim. Principal
From the Text. Clinical Indications. Clinical Indications. RSPT 2217 Non-steroidal Anti-asthma Agents. RSPT 2317 Non-steroidal Antiasthma Agents
 From the Text RSPT 2317 Non-steroidal Antiasthma Agents Gardenhire Chapter 12 Key Terms and Definitions Page 226 Nonsteroidal Antiasthma Meds Table 12-1; page 228 Comparative Features of Antileukotriene
From the Text RSPT 2317 Non-steroidal Antiasthma Agents Gardenhire Chapter 12 Key Terms and Definitions Page 226 Nonsteroidal Antiasthma Meds Table 12-1; page 228 Comparative Features of Antileukotriene
COPD MANAGEMENT PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines f the collabative management of patients with a diagnosis of chronic obstructive pulmonary disease (COPD) who are not adequately controlled and to define the roles and
I. PURPOSE To establish guidelines f the collabative management of patients with a diagnosis of chronic obstructive pulmonary disease (COPD) who are not adequately controlled and to define the roles and
Medicaid Health Plans of America Center for Best Practices. Best Practices Compendium in Childhood Asthma Care
 Medicaid Health Plans of America Center for Best Practices Best Practices Compendium in Childhood Asthma Care 2 Childhood Asthma Care Best Practices Compendium table of contents 3 Table of Contents President
Medicaid Health Plans of America Center for Best Practices Best Practices Compendium in Childhood Asthma Care 2 Childhood Asthma Care Best Practices Compendium table of contents 3 Table of Contents President
Autoimmunity and immunemediated. FOCiS. Lecture outline
 1 Autoimmunity and immunemediated inflammatory diseases Abul K. Abbas, MD UCSF FOCiS 2 Lecture outline Pathogenesis of autoimmunity: why selftolerance fails Genetics of autoimmune diseases Therapeutic
1 Autoimmunity and immunemediated inflammatory diseases Abul K. Abbas, MD UCSF FOCiS 2 Lecture outline Pathogenesis of autoimmunity: why selftolerance fails Genetics of autoimmune diseases Therapeutic
COPD and Asthma Differential Diagnosis
 COPD and Asthma Differential Diagnosis Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in America. Learning Objectives Use tools to effectively diagnose chronic obstructive
COPD and Asthma Differential Diagnosis Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in America. Learning Objectives Use tools to effectively diagnose chronic obstructive
5. Treatment of Asthma in Children
 Treatment of sthma in hildren 5. Treatment of sthma in hildren 5.1 Maintenance Treatment 5.1.1 rugs Inhaled Glucocorticoids. Persistent wheezing in children under the age of three can be controlled with
Treatment of sthma in hildren 5. Treatment of sthma in hildren 5.1 Maintenance Treatment 5.1.1 rugs Inhaled Glucocorticoids. Persistent wheezing in children under the age of three can be controlled with
RSPT 2317 Non-steroidal anti-asthma agents
 RSPT 2317 Non-steroidal Anti-asthma Agents Mechanisms of Inflammation in Asthma Mechanisms of Inflammation in Asthma Asthma is a chronic inflammatory disorder of the airways It is divided into extrinsic
RSPT 2317 Non-steroidal Anti-asthma Agents Mechanisms of Inflammation in Asthma Mechanisms of Inflammation in Asthma Asthma is a chronic inflammatory disorder of the airways It is divided into extrinsic
Montelukast Sodium. -A new class of seasonal allergic rhinitis therapy
 Montelukast Sodium -A new class of seasonal allergic rhinitis therapy Symptoms of Seasonal Allergic Rhinitis Nasal itch Sneezing Rhinorrhoea Nasal stuffiness Pathogenesis of Allergic Rhinitis Mast cells,
Montelukast Sodium -A new class of seasonal allergic rhinitis therapy Symptoms of Seasonal Allergic Rhinitis Nasal itch Sneezing Rhinorrhoea Nasal stuffiness Pathogenesis of Allergic Rhinitis Mast cells,
DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A TERTIARY CARE HOSPITAL
 International Journal of Pharmaceutical Applications ISSN 0976-2639, Online ISSN 2278 6023 Vol 3, Issue 2, 2012, pp 297-305 http://www.bipublication.com DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A
International Journal of Pharmaceutical Applications ISSN 0976-2639, Online ISSN 2278 6023 Vol 3, Issue 2, 2012, pp 297-305 http://www.bipublication.com DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A
4 Pharmacological management
 4 Pharmacological management The aim of asthma management is control of the disease. Control of asthma is defined as: no daytime symptoms no night time awakening due to asthma no need for rescue medication
4 Pharmacological management The aim of asthma management is control of the disease. Control of asthma is defined as: no daytime symptoms no night time awakening due to asthma no need for rescue medication
Pharmacology of the Respiratory Tract: COPD and Steroids
 Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Spirometry Workshop for Primary Care Nurse Practitioners
 Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Visiting Assistant
Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Visiting Assistant
Treatment of Asthma. Talk to your doctor about the various medications available to treat asthma.
 Please call 911 if you think you have a medical emergency. Treatment of Asthma The goals of asthma therapy are to prevent your child from having chronic and troublesome symptoms, to maintain your child's
Please call 911 if you think you have a medical emergency. Treatment of Asthma The goals of asthma therapy are to prevent your child from having chronic and troublesome symptoms, to maintain your child's
YOU VE BEEN REFERRED TO AN ASTHMA SPECIALIST...
 YOU VE BEEN REFERRED TO AN ASTHMA SPECIALIST... ...HERE S WHAT TO EXPECT You have been referred to an allergist because you have or may have asthma. The health professional who referred you wants you to
YOU VE BEEN REFERRED TO AN ASTHMA SPECIALIST... ...HERE S WHAT TO EXPECT You have been referred to an allergist because you have or may have asthma. The health professional who referred you wants you to
Bronchodilators in COPD
 TSANZSRS Gold Coast 2015 Can average outcomes in COPD clinical trials guide treatment strategies? Long live the FEV1? Christine McDonald Dept of Respiratory and Sleep Medicine Austin Health Institute for
TSANZSRS Gold Coast 2015 Can average outcomes in COPD clinical trials guide treatment strategies? Long live the FEV1? Christine McDonald Dept of Respiratory and Sleep Medicine Austin Health Institute for
Strategies for Improving Patient Outcomes in Pediatric Asthma Through Education. Pediatric Asthma. Epidemiology. Epidemiology
 Strategies for Improving Patient Outcomes in Pediatric Asthma Through Education Chris Orelup, MS3 Max Project 3/1/01 Pediatric Asthma The leading cause of illness in childhood 10, 000, 000 school absences
Strategies for Improving Patient Outcomes in Pediatric Asthma Through Education Chris Orelup, MS3 Max Project 3/1/01 Pediatric Asthma The leading cause of illness in childhood 10, 000, 000 school absences
Disclosures. Consultant and Speaker for Biogen Idec, TEVA Neuroscience, EMD Serrono, Mallinckrodt, Novartis, Genzyme, Accorda Therapeutics
 Mitzi Joi Williams, MD Neurologist MS Center of Atlanta, Atlanta, GA Disclosures Consultant and Speaker for Biogen Idec, TEVA Neuroscience, EMD Serrono, Mallinckrodt, Novartis, Genzyme, Accorda Therapeutics
Mitzi Joi Williams, MD Neurologist MS Center of Atlanta, Atlanta, GA Disclosures Consultant and Speaker for Biogen Idec, TEVA Neuroscience, EMD Serrono, Mallinckrodt, Novartis, Genzyme, Accorda Therapeutics
Medicines Use Review Supporting Information for Asthma Patients
 Medicines Use Review Supporting Information for Asthma Patients What is asthma? Asthma is a chronic inflammatory disorder of the airways. The inflammation causes an associated increase in airway hyper-responsiveness,
Medicines Use Review Supporting Information for Asthma Patients What is asthma? Asthma is a chronic inflammatory disorder of the airways. The inflammation causes an associated increase in airway hyper-responsiveness,
Logistics. Registration for free continuing education (CE) hours or certificate of attendance through TRAIN at: https://tx.train.
 hours or certificate of attendance through TRAIN at: https://tx.train.") . DSHS Grand Rounds Logistics Registration for free continuing education (CE) hours or certificate of attendance through TRAIN at: https://tx.train.org Streamlined registration for individuals not requesting
. DSHS Grand Rounds Logistics Registration for free continuing education (CE) hours or certificate of attendance through TRAIN at: https://tx.train.org Streamlined registration for individuals not requesting
Pediatric. Updated 2008
 A S T H M A P R O V I D E R M A N U A L Pediatric Updated 2008 Asthma 2 Causes of Asthma 3 Utah Prevalence 3 Diagnosis 7 Managing Asthma 9 Education for Partnership in Care 11 Control of Environmental
A S T H M A P R O V I D E R M A N U A L Pediatric Updated 2008 Asthma 2 Causes of Asthma 3 Utah Prevalence 3 Diagnosis 7 Managing Asthma 9 Education for Partnership in Care 11 Control of Environmental
CCHCS Care Guide: Asthma
 GOALS SHORTNESS OF BREATH, WHEEZE, COUGH NIGHT TIME AWAKENINGS ACTIVITY INTERFERENCE SABA* USE FOR SYMPTOM CONTROL FEV1* OR PEAK FLOW EXACERBATIONS REQUIRING ORAL STEROIDS < 2 DAYS / WEEK 2 TIMES / MONTH
GOALS SHORTNESS OF BREATH, WHEEZE, COUGH NIGHT TIME AWAKENINGS ACTIVITY INTERFERENCE SABA* USE FOR SYMPTOM CONTROL FEV1* OR PEAK FLOW EXACERBATIONS REQUIRING ORAL STEROIDS < 2 DAYS / WEEK 2 TIMES / MONTH
Montelukast Sodium Singulair, Merck. Development and Pharmacology: 1
 Montelukast Sodium Singulair, Merck Development and Pharmacology: 1 Asthma is a chronic inflammatory disease of the airways that is complicated by episodes of acute inflammation. Even patients with mild
Montelukast Sodium Singulair, Merck Development and Pharmacology: 1 Asthma is a chronic inflammatory disease of the airways that is complicated by episodes of acute inflammation. Even patients with mild
Stacie L. Penkova, PharmD, MHSA, BCPS Clinical Pharmacy Manager Critical Care Pharmacy Specialist Drug Information Coordinator Pharmacology Summit
 Stacie L. Penkova, PharmD, MHSA, BCPS Clinical Pharmacy Manager Critical Care Pharmacy Specialist Drug Information Coordinator Pharmacology Summit July 26, 2014 Objectives Classify asthma by severity Prescribe
Stacie L. Penkova, PharmD, MHSA, BCPS Clinical Pharmacy Manager Critical Care Pharmacy Specialist Drug Information Coordinator Pharmacology Summit July 26, 2014 Objectives Classify asthma by severity Prescribe
Severe asthma Definition, epidemiology and risk factors. Mina Gaga Athens Chest Hospital
 Severe asthma Definition, epidemiology and risk factors Mina Gaga Athens Chest Hospital Difficult asthma Defined as asthma, poorly controlled in terms of chronic symptoms, with episodic exacerbations,
Severe asthma Definition, epidemiology and risk factors Mina Gaga Athens Chest Hospital Difficult asthma Defined as asthma, poorly controlled in terms of chronic symptoms, with episodic exacerbations,
RES/006/APR16/AR. Speaker : Dr. Pither Sandy Tulak SpP
 RES/006/APR16/AR Speaker : Dr. Pither Sandy Tulak SpP Definition of Asthma (GINA 2015) Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families
RES/006/APR16/AR Speaker : Dr. Pither Sandy Tulak SpP Definition of Asthma (GINA 2015) Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families
Breathe With Ease. Asthma Disease Management Program
 Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
EVIDENCE-BASED BEST PRACTICES FOR THE MANAGEMENT OF ASTHMA IN PEDIATRIC PRIMARY CARE IN SOUTH CAROLINA
 EVIDENCE-BASED BEST PRACTICES FOR THE MANAGEMENT OF ASTHMA IN PEDIATRIC PRIMARY CARE IN SOUTH CAROLINA Sarah Ball, PharmD Mike Bowman, MD Sandra Garner, PharmD Nancy Hahn, PharmD Sophie Robert, PharmD
EVIDENCE-BASED BEST PRACTICES FOR THE MANAGEMENT OF ASTHMA IN PEDIATRIC PRIMARY CARE IN SOUTH CAROLINA Sarah Ball, PharmD Mike Bowman, MD Sandra Garner, PharmD Nancy Hahn, PharmD Sophie Robert, PharmD
TESTING FOR FOOD ALLERGIES. Laine Keahey, MD Arizona Allergy Associates
 TESTING FOR FOOD ALLERGIES Laine Keahey, MD Arizona Allergy Associates Objectives Understand what blood tests(rast) and skin tests are measuring Learn what the size of a positive skin test really means
TESTING FOR FOOD ALLERGIES Laine Keahey, MD Arizona Allergy Associates Objectives Understand what blood tests(rast) and skin tests are measuring Learn what the size of a positive skin test really means
Monoclonal Antibodies in Asthma Therapy. Yehia El-Gamal MD, PhD
 Monoclonal Antibodies in Asthma Therapy Yehia El-Gamal MD, PhD Conflict of Interest Nothing to disclose Objectives Following this presentation, the audience should be able to: Recognize some important
Monoclonal Antibodies in Asthma Therapy Yehia El-Gamal MD, PhD Conflict of Interest Nothing to disclose Objectives Following this presentation, the audience should be able to: Recognize some important
Guideline on the clinical investigation of medicinal products for the treatment of asthma
 22 October 2015 CHMP/EWP/2922/01 Rev.1 Committee for Medicinal Products for Human Use (CHMP) Guideline on the clinical investigation of medicinal products for the treatment of Draft Agreed by Respiratory
22 October 2015 CHMP/EWP/2922/01 Rev.1 Committee for Medicinal Products for Human Use (CHMP) Guideline on the clinical investigation of medicinal products for the treatment of Draft Agreed by Respiratory
COPD PROTOCOL CELLO. Leiden
 COPD PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives and medication of COPD. The Cello way of working can be viewed on
COPD PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives and medication of COPD. The Cello way of working can be viewed on
InetCE 146-000-01-001-H01
 The National Asthma Education Prevention Program (NAEPP II) Guidelines for the Treatment of Asthma: Implications for the Pharmacist (Manuscript Updated December 2000) InetCE 146-000-01-001-H01 Theresa
The National Asthma Education Prevention Program (NAEPP II) Guidelines for the Treatment of Asthma: Implications for the Pharmacist (Manuscript Updated December 2000) InetCE 146-000-01-001-H01 Theresa
CCHP/CCRMC 2006 Clinical Practice Guideline Outpatient Management of Asthma in Children and Adults
 Clinical Practice Guideline Outpatient Management of ASTHMA in Children and Adults 2007 Contra Costa Health Plan and Contra Costa Regional Medical Center TABLE OF CONTENTS SECTION PAGE ASTHMA GUIDELINE
Clinical Practice Guideline Outpatient Management of ASTHMA in Children and Adults 2007 Contra Costa Health Plan and Contra Costa Regional Medical Center TABLE OF CONTENTS SECTION PAGE ASTHMA GUIDELINE
Factors Associated with Underutilization of Inhalation Corticosteroids. among Asthmatic Patients Attending Tikur Anbessa Specialized Hospital
 Factors Associated with Underutilization of Inhalation Corticosteroids among Asthmatic Patients Attending Tikur Anbessa Specialized Hospital By: Yohanes Ayele (B. Pharm) A thesis submitted to the School
Factors Associated with Underutilization of Inhalation Corticosteroids among Asthmatic Patients Attending Tikur Anbessa Specialized Hospital By: Yohanes Ayele (B. Pharm) A thesis submitted to the School
The Right Medicines Can Help You Get Control of Asthma. BlueCare SM TennCareSelect
 The Right Medicines Can Help You Get Control of Asthma BlueCare SM TennCareSelect WHEEZING. COUGHING. SHORTNESS OF BREATH. CHEST TIGHTNESS. If you or a family member has asthma, you know these symptoms
The Right Medicines Can Help You Get Control of Asthma BlueCare SM TennCareSelect WHEEZING. COUGHING. SHORTNESS OF BREATH. CHEST TIGHTNESS. If you or a family member has asthma, you know these symptoms
In the last few decades, asthma has become epidemic. As the most common
 Licensed School Nurse/ Public Health Nurse/ Registered Nurse In the last few decades, asthma has become epidemic. As the most common chronic childhood disease, asthma affects more than six million children
Licensed School Nurse/ Public Health Nurse/ Registered Nurse In the last few decades, asthma has become epidemic. As the most common chronic childhood disease, asthma affects more than six million children
Montelukast 10mg film-coated tablets PL 17907/0474
 Montelukast 10mg film-coated tablets PL 17907/0474 UKPAR TABLE OF CONTENTS Lay Summary Page 2 Scientific Discussion Page 4 Steps Taken for Assessment Page 11 Steps Taken After Initial Authorisation Page
Montelukast 10mg film-coated tablets PL 17907/0474 UKPAR TABLE OF CONTENTS Lay Summary Page 2 Scientific Discussion Page 4 Steps Taken for Assessment Page 11 Steps Taken After Initial Authorisation Page
T HE ROLE OF THE PHARMACIST IN IMPROVING ASTHMA CARE NIH PUBLICATION NO. 95-3280 JULY 1995 NATIONAL INSTITUTES. National Heart, Lung,
 T HE ROLE OF THE PHARMACIST IN IMPROVING ASTHMA CARE NIH PUBLICATION NO. 95-3280 JULY 1995 NATIONAL INSTITUTES OF HEALTH National Heart, Lung, and Blood Institute TABLE OF CONTENTS Preface.................................i
T HE ROLE OF THE PHARMACIST IN IMPROVING ASTHMA CARE NIH PUBLICATION NO. 95-3280 JULY 1995 NATIONAL INSTITUTES OF HEALTH National Heart, Lung, and Blood Institute TABLE OF CONTENTS Preface.................................i
Understanding Asthma Patients in the Dental Office
 Understanding Asthma Patients in the Dental Office Barbara Fried, RDH, MBA Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce408/ce408.aspx
Understanding Asthma Patients in the Dental Office Barbara Fried, RDH, MBA Continuing Education Units: 1 hour Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce408/ce408.aspx
MEDICATION INFORMATION: CONTROLLER MEDICATIONS
 FRANK J. TWAROG, M.D., Ph.D. CURTIS T. MOODY, M.D. ADULT AND PEDIATRIC ASTHMA AND ALLERGIES Brookline Concord (617) 735-8750 (978) 369-3567 MEDICATION INFORMATION: CONTROLLER MEDICATIONS Asthma medications
FRANK J. TWAROG, M.D., Ph.D. CURTIS T. MOODY, M.D. ADULT AND PEDIATRIC ASTHMA AND ALLERGIES Brookline Concord (617) 735-8750 (978) 369-3567 MEDICATION INFORMATION: CONTROLLER MEDICATIONS Asthma medications
ARIA. At-A-Glance Pocket Reference 2007
 ARIA At-A-Glance Pocket Reference 2007 1 st Edition NEW ARIA UPDATE BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA WORKSHOP REPORT In collaboration with the World Health Organisation, GA 2 LEN,
ARIA At-A-Glance Pocket Reference 2007 1 st Edition NEW ARIA UPDATE BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA WORKSHOP REPORT In collaboration with the World Health Organisation, GA 2 LEN,
Hypersensitivity. TYPE I Hypersensitivity Classic allergy. Allergens. Characteristics of allergens. Allergens. Mediated by IgE attached to Mast cells.
 Gel and Coombs classification of hypersensitivities. Hypersensitivity Robert Beatty Type I Type II Type III Type IV MCB150 IgE Mediated IgG/IgM Mediated IgG Mediated T cell Classic Allergy rbc lysis Immune
Gel and Coombs classification of hypersensitivities. Hypersensitivity Robert Beatty Type I Type II Type III Type IV MCB150 IgE Mediated IgG/IgM Mediated IgG Mediated T cell Classic Allergy rbc lysis Immune
American Thoracic Society Documents
 American Thoracic Society Documents An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations Standardizing Endpoints for Clinical Asthma Trials and
American Thoracic Society Documents An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations Standardizing Endpoints for Clinical Asthma Trials and
PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE
 PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE The content of this booklet was developed by Allergy UK. MSD reviewed this booklet to comment
PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE The content of this booklet was developed by Allergy UK. MSD reviewed this booklet to comment
ASTHMA IN INFANTS AND YOUNG CHILDREN
 ASTHMA IN INFANTS AND YOUNG CHILDREN What is Asthma? Asthma is a chronic inflammatory disease of the airways. Symptoms of asthma are variable. That means that they can be mild to severe, intermittent to
ASTHMA IN INFANTS AND YOUNG CHILDREN What is Asthma? Asthma is a chronic inflammatory disease of the airways. Symptoms of asthma are variable. That means that they can be mild to severe, intermittent to
Drug Class Review on Inhaled Corticosteroids
 Drug Class Review on Inhaled Corticosteroids Final Report January 2006 The purpose of this report is to make available information regarding the comparative effectiveness and safety profiles of different
Drug Class Review on Inhaled Corticosteroids Final Report January 2006 The purpose of this report is to make available information regarding the comparative effectiveness and safety profiles of different
Asthma. Micah Long, MD
 Asthma Micah Long, MD Goals Define the two components of asthma. Describe the method of action and uses for: Steroids (inhaled and IV) Quick Beta Agonists (Nebs and MDIs) The "Others" Magnesium, Epi IM,
Asthma Micah Long, MD Goals Define the two components of asthma. Describe the method of action and uses for: Steroids (inhaled and IV) Quick Beta Agonists (Nebs and MDIs) The "Others" Magnesium, Epi IM,
Tests. Pulmonary Functions
 Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Asthma Intervention. An Independent Licensee of the Blue Cross and Blue Shield Association.
 Asthma Intervention 1. Primary disease education Member will have an increased understanding of asthma and the classification by severity, the risks and the complications. Define asthma Explain how lungs
Asthma Intervention 1. Primary disease education Member will have an increased understanding of asthma and the classification by severity, the risks and the complications. Define asthma Explain how lungs
Asthma Definition. Relationship of Airway Inflammation and Lung Function
 Asthma Guidelines Goals of Medical Care for Adults and Children with Asthma Source: National Institutes of Health, National Heart Lung, and Blood Institute, National Asthma Education and Prevention Program
Asthma Guidelines Goals of Medical Care for Adults and Children with Asthma Source: National Institutes of Health, National Heart Lung, and Blood Institute, National Asthma Education and Prevention Program
Exploratory data: COPD and blood eosinophils. David Price: 9.23-9.35am
 Exploratory data: COPD and blood eosinophils David Price: 9.23-9.35am Blood Eosinophilia in COPD The reliability and utility of blood eosinophils as a marker of disease burden, healthcare resource utilisation
Exploratory data: COPD and blood eosinophils David Price: 9.23-9.35am Blood Eosinophilia in COPD The reliability and utility of blood eosinophils as a marker of disease burden, healthcare resource utilisation
Information for Behavioral Health Providers in Primary Care. Asthma
 What is Asthma? Information for Behavioral Health Providers in Primary Care Asthma Asthma (AZ-ma) is a chronic (long-term) lung disease that inflames and narrows the airways. Asthma causes recurring periods
What is Asthma? Information for Behavioral Health Providers in Primary Care Asthma Asthma (AZ-ma) is a chronic (long-term) lung disease that inflames and narrows the airways. Asthma causes recurring periods
Objectives COPD. Chronic Obstructive Pulmonary Disease (COPD) 4/19/2011
 4/19/2011") Objectives Discuss assessment findings and treatment for: Chronic Obstructive Pulmonary Disease Bronchitis Emphysema Asthma Anaphylaxis Other respiratory issues Provide some definitions Chronic Obstructive
Objectives Discuss assessment findings and treatment for: Chronic Obstructive Pulmonary Disease Bronchitis Emphysema Asthma Anaphylaxis Other respiratory issues Provide some definitions Chronic Obstructive
Pathway for Diagnosing COPD
 Pathway for Diagnosing Visit 1 Registry Clients at Risk Patient presents with symptoms suggestive of Exertional breathlessness Chronic cough Regular sputum production Frequent bronchitis ; wheeze Occupational
Pathway for Diagnosing Visit 1 Registry Clients at Risk Patient presents with symptoms suggestive of Exertional breathlessness Chronic cough Regular sputum production Frequent bronchitis ; wheeze Occupational
RELAPSE MANAGEMENT. Pauline Shaw MS Nurse Specialist 25 th June 2010
 RELAPSE MANAGEMENT Pauline Shaw MS Nurse Specialist 25 th June 2010 AIMS OF SESSION Relapsing/Remitting MS Definition of relapse/relapse rate Relapse Management NICE Guidelines Regional Clinical Guidelines
RELAPSE MANAGEMENT Pauline Shaw MS Nurse Specialist 25 th June 2010 AIMS OF SESSION Relapsing/Remitting MS Definition of relapse/relapse rate Relapse Management NICE Guidelines Regional Clinical Guidelines
COPD Prescribing Guidelines
 South Staffordshire Area Prescribing Group COPD Prescribing Guidelines Inhaler choices in this guideline are different from previous versions produced by the APG. It is not expected patients controlled
South Staffordshire Area Prescribing Group COPD Prescribing Guidelines Inhaler choices in this guideline are different from previous versions produced by the APG. It is not expected patients controlled
Immunology and immunotherapy in allergic disease
 Immunology and immunotherapy in allergic disease Jing Shen, MD Faculty Advisor: Matthew Ryan, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation February 2005
Immunology and immunotherapy in allergic disease Jing Shen, MD Faculty Advisor: Matthew Ryan, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation February 2005
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Making a Difference in the Management of Asthma: A Guide for Respiratory Therapists
 Making a Difference in the Management of Asthma: A Guide for Respiratory Therapists U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Heart, Lung, and Blood Institute
Making a Difference in the Management of Asthma: A Guide for Respiratory Therapists U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Heart, Lung, and Blood Institute
Biologic Treatments for Rheumatoid Arthritis
 Biologic Treatments Rheumatoid Arthritis (also known as cytokine inhibitors, TNF inhibitors, IL 1 inhibitor, or Biologic Response Modifiers) Description Biologics are new class of drugs that have been
Biologic Treatments Rheumatoid Arthritis (also known as cytokine inhibitors, TNF inhibitors, IL 1 inhibitor, or Biologic Response Modifiers) Description Biologics are new class of drugs that have been
STATISTICAL BRIEF #378
 STATISTICAL BRIEF #378 July 212 Asthma Medication Use among Adults with Reported Treatment for Asthma, United States, and 28-29 Frances M. Chevarley, PhD Introduction Asthma is a chronic respiratory disease
STATISTICAL BRIEF #378 July 212 Asthma Medication Use among Adults with Reported Treatment for Asthma, United States, and 28-29 Frances M. Chevarley, PhD Introduction Asthma is a chronic respiratory disease
Chapter 20. Drugs Used in Asthma
 Nitric Oxide (INOmax) Inhalation: 100, 800 ppm gas Katzung PHARMACOLOGY, 9e > Section IV. Drugs with Important Actions on Smooth Muscle > Chapter 19. Nitric Oxide, Donors, & Inhibitors > Chapter 20. Drugs
Nitric Oxide (INOmax) Inhalation: 100, 800 ppm gas Katzung PHARMACOLOGY, 9e > Section IV. Drugs with Important Actions on Smooth Muscle > Chapter 19. Nitric Oxide, Donors, & Inhibitors > Chapter 20. Drugs
Michigan Guidelines for the Use of Controlled Substances for the Treatment of Pain
 Michigan Guidelines for the Use of Controlled Substances for the Treatment of Pain Section I: Preamble The Michigan Boards of Medicine and Osteopathic Medicine & Surgery recognize that principles of quality
Michigan Guidelines for the Use of Controlled Substances for the Treatment of Pain Section I: Preamble The Michigan Boards of Medicine and Osteopathic Medicine & Surgery recognize that principles of quality
Anti-Inflammatory Pharmacotherapy for Wheezing in Preschool Children
 Pediatric Pulmonology Anti-Inflammatory Pharmacotherapy for Wheezing in Preschool Children State of the Art Athanasios G. Kaditis, MD, 1 * Glenna Winnie, MD, 2 and George A. Syrogiannopoulos, MD 1 Summary.
Pediatric Pulmonology Anti-Inflammatory Pharmacotherapy for Wheezing in Preschool Children State of the Art Athanasios G. Kaditis, MD, 1 * Glenna Winnie, MD, 2 and George A. Syrogiannopoulos, MD 1 Summary.
Pharmacogenetics of Topiramate Treatment for Heavy Drinking
 Pharmacogenetics of Topiramate Treatment for Heavy Drinking Henry R. Kranzler, M.D. Perelman School of Medicine of the University of Pennsylvania and VISN 4 MIRECC, Philadelphia VAMC kranzler@mail.med.upenn.edu
Pharmacogenetics of Topiramate Treatment for Heavy Drinking Henry R. Kranzler, M.D. Perelman School of Medicine of the University of Pennsylvania and VISN 4 MIRECC, Philadelphia VAMC kranzler@mail.med.upenn.edu
Supplement Questions asked in the 1st International Basic Allergy Course
 Supplement Questions asked in the 1st International Basic Allergy Course 1. CLINICAL MANIFESTATION What is the percentage of people who have both combined food and inhalant? What is the difference between
Supplement Questions asked in the 1st International Basic Allergy Course 1. CLINICAL MANIFESTATION What is the percentage of people who have both combined food and inhalant? What is the difference between
STAYING ASTHMA FREE. All you need to know about preventers. www.spacetobreathe.co.nz
 STAYING ASTHMA FREE All you need to know about preventers www.spacetobreathe.co.nz HELPING YOUR CHILD BREATHE MORE EASILY GETTING TO KNOW THE PREVENTER What is a preventer? When do you use it? How do they
STAYING ASTHMA FREE All you need to know about preventers www.spacetobreathe.co.nz HELPING YOUR CHILD BREATHE MORE EASILY GETTING TO KNOW THE PREVENTER What is a preventer? When do you use it? How do they
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Updated 2015 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Updated 2015 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
Before prescribing for COPD management, the patient should have had appropriate assessment, including spirometry, as per NICE guidelines.
 Formulary Guidance for Management of COPD patients Before prescribing for COPD management, the patient should have had appropriate assessment, including spirometry, as per NICE guidelines. For inhaler
Formulary Guidance for Management of COPD patients Before prescribing for COPD management, the patient should have had appropriate assessment, including spirometry, as per NICE guidelines. For inhaler
Drug therapy SHORT-ACTING BETA AGONISTS SHORT-ACTING ANTICHOLINERGICS LONG-ACTING BETA AGONISTS LONG-ACTING ANTICHOLINERGICS
 Drug therapy 6 6.1 What is the role of bronchodilators in COPD? 52 SHORT-ACTING BETA AGONISTS 6.2 How do short-acting beta agonists work? 52 6.3 What are the indications for their use? 52 6.4 What is the
Drug therapy 6 6.1 What is the role of bronchodilators in COPD? 52 SHORT-ACTING BETA AGONISTS 6.2 How do short-acting beta agonists work? 52 6.3 What are the indications for their use? 52 6.4 What is the
The National Asthma Education. Overview of Changes to Asthma Guidelines: Diagnosis and Screening
 Overview of Changes to Asthma Guidelines: Diagnosis and Screening SUSAN M. POLLART, MD, MS, and KURTIS S. ELWARD, MD, MPH Department of Family Medicine, University of Virginia School of Medicine, Charlottesville,
Overview of Changes to Asthma Guidelines: Diagnosis and Screening SUSAN M. POLLART, MD, MS, and KURTIS S. ELWARD, MD, MPH Department of Family Medicine, University of Virginia School of Medicine, Charlottesville,
Pulsating Aerosol. The New Wave in SINUSitis Therapy. For the precise, effective and gentle treatment of sinusitis
 The New Wave in SINUSitis Therapy Pulsating Aerosol For the precise, effective and gentle treatment of sinusitis PARI SINUS Inhalation treatment for acute and chronic diseases of the upper airways www.parimedical.co.uk
The New Wave in SINUSitis Therapy Pulsating Aerosol For the precise, effective and gentle treatment of sinusitis PARI SINUS Inhalation treatment for acute and chronic diseases of the upper airways www.parimedical.co.uk
A Genetic Analysis of Rheumatoid Arthritis
 A Genetic Analysis of Rheumatoid Arthritis Introduction to Rheumatoid Arthritis: Classification and Diagnosis Rheumatoid arthritis is a chronic inflammatory disorder that affects mainly synovial joints.
A Genetic Analysis of Rheumatoid Arthritis Introduction to Rheumatoid Arthritis: Classification and Diagnosis Rheumatoid arthritis is a chronic inflammatory disorder that affects mainly synovial joints.
Longitudinal Modeling of Lung Function in Respiratory Drug Development
 Longitudinal Modeling of Lung Function in Respiratory Drug Development Fredrik Öhrn, PhD Senior Clinical Pharmacometrician Quantitative Clinical Pharmacology AstraZeneca R&D Mölndal, Sweden Outline A brief
Longitudinal Modeling of Lung Function in Respiratory Drug Development Fredrik Öhrn, PhD Senior Clinical Pharmacometrician Quantitative Clinical Pharmacology AstraZeneca R&D Mölndal, Sweden Outline A brief