MYOCARDIAL PERFUSION SCINTIGRAPHY
|
|
|
- Quentin Allison
- 7 years ago
- Views:
Transcription



1 MYOCARDIAL PERFUSION SCINTIGRAPHY George N. Sfakianakis MD Professor of Radiology and Pediatrics Director Division of Nuclear Medicine, University of Miami, Florida October 2009
2 EVALUATION OF THE FUNCTION AND DISEASES OF THE HEART WITH NUCLEAR MEDICINE PROCEDURES (CARDIAC SCINTIGRAPHY)


3 The real function of the heart The real trouble of the heart
4 PREVENTION
5 CARDIOVASCULAR SCINTIGRAPHY CORONARY ARTERY DISEASE: MYOCARDIAL PERFUSION SCINTIGRAPHY ( 201 Thallium/ 99m Tc-Agents/ 82 Rhubidium) MYOCARDIAL VIABILITY ( 201 Thallium/ 18 FDG-PET) ACUTE MYOCARDIAL INFARCTION ( 99m Tc-Agents) MYOCARDITIS, TRANSPLANT REJECTION 67 Gallium Imaging (Myosin Ab Imaging) GENERAL INDICATIONS (CHEMOTHERAPY etc) Evaluation of EF, Stroke Vol., Chamber Size, Wall Motion (MUGA/First Pass/Myocardial Perfusion)
6 CORONARY ARTERY DISEASE (CAD) ATHEROMATOUS PLAQUES REDUCE MYOCARDIAL BLOOD FLOW
7 THE CLINICAL NEED FOR MPS MANIFESTATIONS OF CAD IN DECLINING SEVERITY (They depend on degree of stenosis, collaterals, demand and formation of acute thrombus) Sudden Death (AMI, Arrhythmias) Acute Myocardial Infarction Unstable Angina Typical Angina Atypical Chest Pain Asymptomatic
8 MYOCARDIAL PERFUSION SCINTIGRAPHY (MPS) FOR CORONARY ARTERY DISEASE (CAD) (using 201 TlCl 2, 99m Tc-MP-Agents, PET-MP-Agents) DIAGNOSIS OF CLINICALLY SIGNIFICANT CAD (>60% lumen) Indications Chronic Stress Pain (Angina), Rest Pain (Unstable Angina), Acute Chest Pain (Acute Myocardial Infarction, Mi), Preoperative Evaluation Of Patients With Risk Factors QUANTITATION OF SEVERITY AND EXTENT OF CAD ASSESS VIABILITY OF ISCHEMIC MYOCARDIUM POST MI OBTAIN PROGNOSIS BEFORE OR AFTER INFARCTION TO HELP THERAPY PLANNING FOLLOW UP EFFECT OF PTCA / CABG / MEDICAL Tx OR JUST THE COURSE OF THE DISEASE


9 Present in only 40-50% of Patients

10 OTHER DISORDERS MAY PRESENT WITH CHEST PAIN

11 MANIFESTATIONS OF CAD: PATHOPHYSIOLOGY MECHANISMS OF ISCHEMIA Ischemia may be the result of decreased supply or increased demand or both of them adenosine
12 MANIFESTATIONS OF CAD: PATHOPHYSIOLOGY RELATION OF CORONARY FLOW TO DEGREE OF STENOSIS
13 MANIFESTATIONS OF CAD: PATHOPHYSIOLOGY CORONARY FLOW - CORONARY FLOW STRESS REST
14 MANIFESTATIONS OF CAD: PATHOPHYSIOLOGY DEGREE OF STENOSIS NORMAL OBSTRUCTION DEGREE OF STENOSIS

15 MANIFESTATIONS OF CAD: PATHOPHYSIOLOGY RELATION OF CORONARY FLOW TO DEGREE OF STENOSIS and ISCHEMIA 60-80% STENOSIS STENOSIS > 60% becomes CLINICALLY SIGNIFICANT CAD ISCHEMIA At STRESS ONLY STENOSIS>80-90% At REST ISCHEMIA


16 THE MANIFESTATIONS OF CAD DEPEND UPON: 1. The Severity and Extend of Stenosis (Angina Pectoris) 2. The development of Collateral Vessels (Asymptomatic) 3. Formation of Thrombus ( Myocardial Infarction)

17 CORONARY ARTERY DISEASE (CAD) MYOCARDIAL INFARCTION THROMBUS FORMATION STOPS MYOCARDIAL BLOOD FLOW AND CAUSES ACUTE INFARCTION
18 THE CLINICAL NEED FOR MPS MANIFESTATIONS OF CAD IN DECLINING SEVERITY (They depend on degree of stenosis, collaterals, demand and formation of acute thrombus) Sudden Death (AMI, Arrhythmias) Acute Myocardial Infarction Unstable Angina Typical Angina Atypical Chest Pain Asymptomatic
19 TESTS FOR MYOCARDIAL ISCHEMIA Old Techniques Assessment Disadvantages ECG Electrical Activity Accuracy 65% Angiography Coronary Anatomy Invasive/Anatomy New Techniques Nuclear Medicine Regional Blood Flow Accuracy 80-90% Echocardiography Regional Wall Motion Sensitivity low CT /CTI Lumen /Calcification Specificity low MRI Flow Myocardial Perfusion Being Evaluated
20 THE CLINICAL NEED FOR MPS Clinical Examination and EKG at Rest and Special Tests are Suboptimal or Invasive
21 TREADMILL ECG TEST Informative, noninvasive, low risk Accuracy 65% Both FP and FN results
22 CARDIAC CATHETERIZATION Excellent anatomic definition of CAD Insufficient physiologic information Limited definition of viability Invasive, expensive, subjective Evaluation and Therapy (Angioplasty)


23 DIAGNOSTIC VISUALIZATION OF THE ISCHEMIC MYOCARDIUM WITH SCINTIGRAPHY
24 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY DIAGNOSIS OF CLINICALLY SIGNIFICANT CAD (>60% lumen) Chronic Stress Pain (Angina), Rest Pain (Unstable Angina), Acute Chest Pain (Acute Myocardial Infarction, Mi), REST & STRESS MYOCARDIAL PERFUSION IMAGING WITH LVEF & WALL MOTION STUDY : Normal: Very low probability for significant CAD or good collateral vessels Abnormal: Cardiac Catheterization ( and revascularization)
25 THALLIUM: EXPERIMENTAL WORK IN DOGS Thallium injected iv had the same distribution with the micro spheres ( 131 I-MAA), which were injected into the left atrium therefore 201 Tl shows REGIONAL MYOCARDIAL PERFUSION non invasively

26 THALLIUM: CLINICAL APPLICATIONS Planar Imaging in volunteers showed the applicability of the method

27 THALLIUM IMAGING: IMPACT ON PATIENT CARE Planar
28 WHY WE NEED MYOCARDIAL PERFUSION SCINTIGRAPHY (MPS) The RESULTS of MPS are DIFFERENT from the ECG The RESULTS of MPS are BETTER than the ECG MPS is NON-INVASIVE as compared to Angiography
29 The RESULTS of MPS are DIFFERENT from the ECG COMPARATIVE STUDY: Exercise SPECT Imaging vs Exercise ECG in 2700 Patients with Suspected CAD POSITIVE NUCLEAR SPECT STUDIES NEGATIVE NUCLEAR SPECT STUDIES Positive EKG inconclusive EKG inconclusive EKG Positive EKG Positive EEG Negative EEG InconclusiveEEG Negative EKG Negative EKG Entire Population 29
30 The RESULTS of MPS are BETTER than the ECG COMPARATIVE STUDY: Exercise SPECT Imaging vs Exercise ECG in 2700 Patients with Suspected CAD POSITIVE NUCLEAR SPECT STUDIES NEGATIVE NUCLEAR SPECT STUDIES Revascularization Death or MCE Death or MCE No Complications No Complications No Complications Revascularization Catheterized Population 30
31 ADVANCES IN PERFUSION IMAGING Introduction of Pharmacologic Tests Introduction of 99m Tc-Radiopharmaceuticals Tomography (SPECT) increased accuracy to 90% Artifact recognition - Attenuation Correction Functional data: EF, Volumes, Wall Motion Reduced Imaging Time (fast 90 o dual detectors)
32 MYOCARDIAL PERFUSION SCINTIGRAPHY More than 3,000,000 procedures done annually Used to assess regional coronary blood flow Usually done with exercise or pharmacologic stress testing Its Safety and efficacy have been proven
33 MYOCARDIAL PERFUSION SCINTIGRAPHY (SPECT) METHODS AND APPLICATIONS
34 MYOCARDIAL PERFUSION SCINTIGRAPHY Radiopharmaceuticals Single Photon Emission Comp. Tomo (SPECT) 201 Thallium ( 201 Tl, 3-4 mci) 99m Tc Sestamibi (Cardiolite, MIBI, 25 mci), 99m Tc Tetrofosmin (Myoview, 25 mci) Positron Emission Tomography (PET) or PET/CT 82 Rb (10-40 mci) by Generator 11 C-FFA (30 mci) by Cyclotron 13 NH 3 (15-25 mci) by Cyclotron
35 Cellular Retention of Myocardial Perfusion Radiopharmaceuticals Thallium Sestamibi Teboroxine Rubidium Tetrofosmin

36 MYOCARDIAL PERFUSION NORMAL V/S ISCHEMIA Blood supply by a stenotic artery at rest may suffice We must apply stress to increase the need and elicit ischemia NORMAL NO DEFECT ISCHEMIA stress DEFECT
37 MYOCARDIAL STRESS-TEST PROTOCOLS Methods of Stress Testing Physical Exercise Treadmill Bicycle Pharmacologic Stress Vasodilators: Adenosine, Lexiscan Dipyridamole Catecholamines: Dobutamine


38 TREADMILL EXERCISE - INJECTION The radiopharmaceutical is injected at peak exercise, which must continue >1min after injection
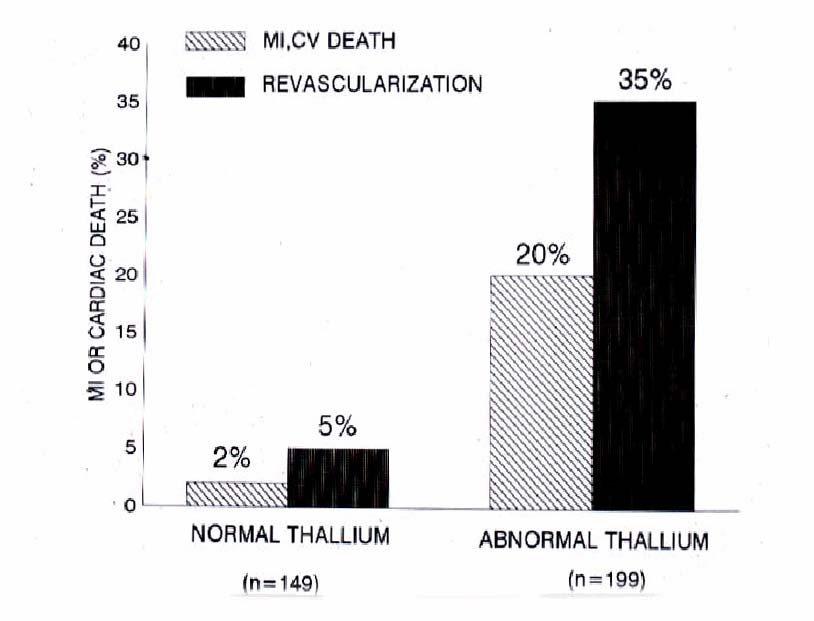
39 MPS DIAGNOSIS and PROGNOSIS Coronary Artery Disease (CAD) may be treatable if diagnosed in time and before myocardial infarction or death occurs. For the diagnosis of CAD Myocardial Perfusion Scintigraphy (MPS) is a Sensitive and Specific method MPS is proven effective for the early Diagnosis and Quantification of CAD, helps in Prognosis, in decision making about mode of Therapy, and can be used for follow up the course of the disease and results of treatment.
40 MPS DIAGNOSIS and PROGNOSIS Myocardial Perfusion Scintigraphy Predicts Major Cardiac Events or The Need for Revascularization 348 patients (75 +/- 4 yo) with suspected CAD, followed for a mean of 2 years Event Rate Revascularization Normal Tl: 149 pts 2% 5% Abnormal Tl: 199 pts 20% 35% Shaw JACC 1985
41
42 MPS DIAGNOSIS and PROGNOSIS There is only a requirement: Adequate stress is essential to uncover ischemia during MPS.
43 MPS DIAGNOSIS and PROGNOSIS Myocardial Perfusion Scintigraphy Predicts Cardiac Events more reliably when the Level of Stress is Adequate 189 patients with typical angina and negative EKG, had cardiac events (death, MI, late revascularization) per year after scintigraphy Event Rate Normal Tl with MPHR > 85%: 108 pts 1.9% / year Normal Tl with MPHR < 85%: 35 pts 8.6% / year Abnormal Tl: 46 pts 15% / year Bairey AJC 1989

44 THE LEVEL OF STRESS MUST BE ADEQUATE
45 LIMITATIONS OF THE PHYSICAL STRESS There is indeed a requirement for a successful MPS: Adequate stress is essential to uncover ischemia However, most of our patients, especially female, are unable to exercise to a level the test becomes diagnostic and fully useful. As a result many examinations are either useless or even misleading. Pharmacologic stress must be used when fitness for physical exercise is anticipated to be low.
46 CONTRAINDICATIONS TO PHYSICAL STRESS Aortic Stenosis Abdominal Aortic Aneurysm Left Bundle Branch Block Ventricular Paced Rhythm Inability to Exercise CNS or Orthopedic Limited Capacity for Exercise Peripheral Vascular Disease, COPD, Medications (eg. β blockers), Poor Motivation, Heart Failure, Previous Submaximal Exercise Test
47 MOST FREQUENT INDICATIONS FOR PHARMACOLOGIC STRESS Inability to Exercise Contraindication to Exercise Limited capacity to Exercise Left Bundle Branch Block: ( use Adenosine, Dipyridamole ) Asthma, Obstructive Lung Disease: ( use Dobutamine )
48 PHARMACOLOGIC STRESS TESTING MEDICATIONS VASODILATORS ADENOSINE or LEXISCAN: Direct receptor Effect, Rapid Onset/Offset DIPYRIDAMOLE: Indirect Effect, Prolonged Action SYMPATHETICOMIMETIC DOBUTAMINE: Indirect Effect (Enhances Myocardial Contraction)
49 PHARMACOLOGIC STRESS TESTING WITH VASODILATORS GENERAL COMMON PROPERTIES Safe with Stable Patients Proven Diagnostic and Prognostic Utility May be Combined with Exercise Avoided with Bronchospasm and AV Block DIFFERENCES DIPYRIDAMOLE: Indirect Effect, Prolonged Action ADENOSINE/LEXISCAN: Direct receptor Effect, Rapid Onset/Offset
50 PHARMACOLOGIC STRESS TESTING PROPERTIES OF VASODILATORS AND DOBUTAMINE LEXISCAN ADENOSINE DIPYRIDAMOLE DOBUTAMINE Half Life 2 min <10 sec Mean time to peak Coronary flow velocity 30 sec 56 sec Onset of action seconds seconds Mechanism of action Direct Direct Patient with side effect 3% 0.6% 2% requiring treatment min 2 min 65 min < 10 min 2 min 1-2 min Indirect Indirect 16% NA



51 INFUSION PROTOCOLS Continuous monitoring ECG, BP, HR, Respiration Until baseline values have returned, usually 1-5min
52 PREPARATION FOR ADENOSINE STRESS At least 24 hr no products containing Caffeine, theophylline and dipyridamole
53 ADENOSINE for Myocardial Stress test MECHANISM OF ACTION Adenosine is a potent vasodilator in most vascular beds. (they exert their effect through activation of purine receptors) Myocardial uptake of perfusion radiopharmaceuticals, like Thallium, Cardiolite, Myoview, and Ammonia, is directly proportional to coronary blood flow Adenosine increases blood flow in normal coronary arteries with little or no increase in stenotic arteries As a result, Adenosine causes relatively less uptake in vascular territories supplied by stenotic arteries, as compared to normal arteries
54 CONTRA-INDICATIONS FOR ADENOSINE PHARMACOLOGIC STRESS 2 nd or 3 rd degree AV Block (except with pacemaker) Sinus node disease (except with pacemaker) Bronchoconstrictive / Bronchospastic Lung disease (asthma) Hypersensitivity to Adenosine
55 ADVERSE REACTIONS TO ADENOSINE MILD REACTIONS Flushing 44% Chest Discomfort 40% Dyspnea or Urge to breathe deeply 28% Headache 18% Throat, Neck, or Jaw Discomfort 15% Gastrointestinal Discomfort 13% Light-headedness/Dizziness 12% SERIOUS REACTIONS AV block 1st-degree 2.9%, 2d-degree 2.6%, 3d-degree 0.8% Cardiac arrest, VT, MI have been reported
56 DISCONTINUE ADENOSINE INFUSION IN CASE OF Persistent or high-grade AV block Persistent or symptomatic hypotension Severe respiratory difficulties TREATMENT OF ADENOSINE SIDE-EFFECTS IV Theophylline mg (needed in less than 2% of patients)
 The effect of Lexiscan on coronary blood flow (a rapid increase to 2.5-fold baseline) is sustained for approximately 2.")

57 LEXISCAN FOR MYOCARDIAL STRESS TEST MECHANISM OF ACTION A2A adenosine receptor agonist ( with at least 10-fold lower affinity for the A1 adenosine receptor) The effect of Lexiscan on coronary blood flow (a rapid increase to 2.5-fold baseline) is sustained for approximately 2.3 minutes, and decreases to less than twice the baseline level within 10 min The combination of low affinity for the A2A adenosine receptor and the presence of a coronary artery A2A adenosine receptor reserve allows rapid induction and sustain maximal coronary blood flow to conduct stress radionuclide MPI.
58 CONTRA-INDICATIONS FOR PHARMACOLOGIC STRESS ADENOSINE or LEXISCAN 2 nd or 3 rd degree AV Block (except with pacemaker Sinus node disease (except with pacemaker) Bronchoconstrictive/Bronchospastic Lung disease (asthma) Hypersensitivity to Adenosine

59 Adverse effect of Lexiscan v/s Adenosine
60 TREATMENT OF LEXISCAN SIDE-EFFECTS IV Theophylline mg

61 PHARMACOLOGIC STRESS TESTING DIAGNOSTIC ACCURACY COMPARISON OF EXERCISE ADENOSINE DIPYRIDAMOLE DOBUTAMINE
62 POTENTIAL ADVANTAGES OF COMBINING LIMITED EXERCISE WITH ADENOSINE No Change in Severity of Myocardial Perfusion Defect Improvement in Detection of Reversibility Reduced Non-cardiac Side Effects and Arrhythmias Improved Image quality from increased T/NT
63 MYOCARDIAL STRESS-TEST PROTOCOLS A REST and a STRESS STUDY are usually performed METHODS OF STRESS TESTING a) Physical Exercise b) Pharmacologic Stress METHODS OF RADIOPHARMACEUTICAL INJECTION a) Thallium protocols (one or two injections) b) Technetium labeled protocols (one day or two days) c) Mixed protocols d) PET protocols ( 82 Rb or 13 N-Ammonia)
64 PROTOCOLS FOR MPS A. THALLIUM ONLY a) Single Injection at Stress(3-4 mci) Redistribution Imaging immediately(stress), and late(4 hr=rest) b) Stress Injection (3-4 mci) and Imaging immediately Reinjection at rest (1.5mCi) and imaging at 4hr c) Rest Injection (3-4 mci) and Imaging at (30min) 4hr Re-imaging at 24 hr
65 PROTOCOLS FOR MPS B. 99m Tc MYOCARDIAL PERFUSION AGENTS a) Two Day Protocols (rest / stress each 20-30mCi) b) Same Day Protocol: Rest injection (8 mci) imaging after 60 min Stress re-injection (24 mci) and imaging after min
66 PROTOCOLS FOR MPS C. MIXED PROTOCOLS or Tc-MYOVIEW Tc-MYOVIEW or REST STUDY 201 Tl (3-4 mci) injection at rest; imaging at 30 min (4hr,24hr) STRESS STUDY 99m Tc-Agents (20-30 mci) injection at peak stress; imaging at 30min-1hr
67 MIXED PROTOCOLS FOR MPS IMPROVED QUALITY ADVANTAGES 201 Tl more sensitive for viability than 99m Tc-Agents 99m Tc-Agents had better photons and short half life, the higher dose increases sensitivity for ischemia, allows functional evaluations (EF, Volumes,WM, ) BETTER LOGISTICS Facilitates imaging, utilizes resources better, shortens time the patient stays in the lab
68 CORONARY ARTERIES

69 CORONARY ANATOMY: Angiography AP Caudal View of Left CA

70 CORONARY ANATOMY: Angiography AP Cranial View of Left CA

71 SPECT STUDIES: THE THREE AXES
72 A 55 yo man with typical angina pectoris has a stress and rest MPS
73 SPECT STUDIES: THE THREE AXES a severe reversible defect Diagnosis Anterior Wall Ischemia
74 ASSESSMENT OF VENTRICULAR FUNCTION IN CONJUNCTION WITH PERFUSION IMAGING GATED SPECT AT REST Global and regional thickening and wall motion LV Ejection Fraction, global and regional LV Volumes: Stroke Volume, ESV, EDV


75 EDGE DETECTION, LVEF, VOLUME MEASUREMENTS EDV, ESV LVEF=58% Germano et al 1995


76 EDGE DETECTION, LVEF, VOLUME MEASUREMENTS EDV, ESV IN CASES WITH PEREFUSION DEFECTS LVEF=28% Germano et al 1995

77 WALL MOTION EVALUATION

78 EF BY MYOCARDIAL PERFUSION SCINTIGRAPHY COMPARISON WITH FPRA

79 EF BY MYOCARDIAL PERFUSION SCINTIGRAPHY INCREMENTAL PROGNOSTIC VALUE
80 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY QUANTITATION OF EXTENT AND SEVERITY OF CAD (Before or after cardiac catheterization ) REST & STRESS MYOCARDIAL PERFUSION IMAGING WITH LVEF & WALL MOTION STUDY IS PERFORMED a) Severity of ischemia: mild, moderate, severe b) Extend of ischemia: percent of total wall found ischemic c) Vessel(s) involved: Single, Two, Multiple, LAD/LCx/RCA d) Function: Wall motion, Volumes, EF ( global and regional)

81 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY QUANTITATION OF EXTENT OF CAD (Before or after cardiac catheterization )
82 EXTEND OF ISCHEMIA AFFECTS PROGNOSIS
83 A 61 yo lady is evaluated for chest pain (not typical)


84 SEVERITY OF ISCHEMIA AFFECTS PROGNOSIS a mild reversible defect Diagnosis: Inferolateral Wall Ischemia
85 A 55 yo man with typical angina pectoris has a stress and rest MPS
86 SEVERITY OF ISCHEMIA AFFECTS PROGNOSIS a severe reversible defect Diagnosis: Severe Anterior Wall Ischemia

87 MPS PROGNOSIS THE SEVERITY OF HYPOPERFUSION ON REST / STRESS MYOCARDIAL SCINTIGRAPHY IS A PREDICTOR OF CARDIAC EVENTS 5000 pts with SPECT studies followed 642 +/- 226 days

88 POLAR MAP OR BULL S EYE

89 POLAR MAP OR BULL S EYE
90 INTERPRETATION OF MYOCARDIAL PERFUSION SCINTIGRAPHY REST STUDY STRESS STUDY CONCLUSION No defect No defect No Ischemia No defect Defect Ischemia Defect Same Defect Infarct or Hibernation Defect Larger Defect Ischemia+Infarct


91 MPS: NO DEFECT = NO ISCHEMIA
92 A 45 yo patient presents with typical angina pectoris Has an exercise and rest MPS

93 MPS: INFEROLATERAL WALL REVERSIBLE DEFECT= ISCHEMIA RCA Inferolateral Wall Reversible Defect
94 A 79 yo man with history af CAD and MI has an Adenosine MPS

95 MPS: ANTERIOR WALL MOSTLY FIXED DEFECT= = INFARCT WITH PERI-INFARCTION ISCHEMIA Anterior Wall Partially Reversible Defect
96 A 45 yo lady with atypical chest pain has an exercise and rest MPS
97 MPS: ANTERIOR WALL FIXED DEFECT = INFARCT OR HIBERNATION Anterior Wall Unchanged (Fixed) Defect
98 THREE DECADES OF EXPERIENCE IN MYOCARDIAL PERFUSION SCINTIGRAPHY Based on tens of thousands of publications The Tests is Considered Safe Accurate Cost Effective

99 First evaluation of our studies

100 Second evaluation of our studies
101 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY PREOPERATIVE SCREENING FOR CAD Before non-cardiac surgery, in patients presented with history or symptoms and signs or EKG findings suspicious for CAD: REST & STRESS MYOCARDIAL PERFUSION IMAGING WITH LVEF & WALL MOTION STUDY : Normal: Very low risk for peri-operative major cardiac events ( MI and death) Abnormal: Cardiac Catheterization ( and revascularization)
102 MPS PROGNOSIS/PREOPERATIVE SCREENING Myocardial Perfusion Scintigraphy(Thallium Dipyridamole) Predicts Perioperative MI / Death (Despite the exclusion of patients who underwent revascularization because of an abnormal Tl study) Among 335 patients with major non-coronary surgery 130 patients with abnormal Tl had such complications And the Extend of Reversibility is Proportional to Perioperative Events Lette AJC 1992
103 Lette AJC 1992
104 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY Acute Chest Pain when there is clinical suspicion of acute MI with inconclusive EKG and enzymes: REST MYOCARDIAL PERFUSION IMAGING NORMAL study : Consider other cause of chest pain May schedule stress scintigraphy ABNORMAL: Patient Admission-Therapy for MI-CAD

105 ACUTE CHEST PAIN
106 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY PROGNOSIS BEFORE OR AFTER MI REST & STRESS MYOCARDIAL PERFUSION IMAGING WITH LVEF & WALL MOTION STUDY: Normal: Less than 0.5% per year major cardiac events Abnormal: PTCA or CABG to prevent ( a high rate of ) major cardiac events ( MI or death)
107 MPS PROGNOSIS (RISK STRATIFICATION) MYOCARDIAL PERFUSION SCINTIGRAPHY (THALLIUM EXERCISE) PREDICTS MAJOR CARDIAC EVENTS In 404 patients with a mean age of 65 years who were followed for a mean of 2 years Incidence of MI or cardiac death was 0.5%in normal, 5% in one vessel, 13% in =>2 vessel disease Iskandrian AJC 1988
108 MPS: PROGNOSIS (RISK STRATIFICATION)
109 MPS PROGNOSIS MYOCARDIAL PERFUSION SCINTIGRAPHY (Tl), WHEN ABNORMAL AND CONCORDANT WITH EKG-TEST, IS ASSOCIATED WITH SHORTER EVENT-FREE SURVIVAL It predicted a 3.6-fold risk for a coronary event (independent of conventional risk factors) for 23 patients with abnormal / concordant Tl / EKG as compared to 384 patients of all the other groups (Along x-axis: numbers of patients at risk / year for 8 years concordant / positive Tl and EKG at bottom and all other group patients at top) Fleg Circulation 1990
110

111 PROGNOSTIC VALUE OF VASODILATOR MYOCARDIAL PERFUSION SCINTIGRAPHY IN PATIENTS WITH LBBB
112 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY FOLLOW UP DISEASE OR THERAPY REST & STRESS MYOCARDIAL PERFUSION IMAGING WITH LVEF & WALL MOTION STUDY: Normal or Stable: Medical Therapy Recurrence or Deterioration: PTCA or CABG or change in Medical Tx
113 A 57 yo man underwent angioplasty because of LAD disease He had MPS before and after Angioplasty

114 FOLLOW UP DISEASE OR THERAPY Anteroseptal Wall Defect Resolved (Effect of Angioplasty)
115 INTERPRETATION OF MYOCARDIAL PERFUSION SCINTIGRAPHY REST STUDY STRESS STUDY CONCLUSION No defect No defect No Ischemia No defect Defect Ischemia Defect Same Defect Infarct/Hibernation Defect Larger Defect or Ischemia+Infarct Different Location
116 A 45 yo lady with atypical chest pain has an exercise and rest MPS

")
117 MPS: ANTERIOR WALL FIXED DEFECT = INFARCT OR HIBERNATION Anterior Wall Severe Unchanged (Fixed) Defect
118 A 55 yo man with typical chest pain has an exercise and rest MPS
119 MPS: NO ISCHEMIA ; FIXED SEVERE DEFECT: SCAR v/s HIBERNATING MYOCARDIUM STRESS MIBI REST THALLIUM Anterior Wall Severe Unchanged (Fixed) Defect
120 CLINICAL USE OF MYOCARDIAL SCINTIGRAPHY MYOCARDIAL VIABILITY POST (OR PRE) MI: 1) MPS: a) normal perfusion at rest = viable myocardium b) a fixed rest defect = scar or hibernation to differentiate: 2) 18 F-DEOXY-GLUCOSE (FDG)-PET STUDY : MYOCARDIUM VISIBLE = VIABLE MYOCARDIUM Visible myocardium on FDG with a rest Tl perfusion Defect= MISMATCH WITH Tl= HIBERNATING myocardium FDG+MPS Matching DEFECT = SCAR
121 A 63 yo patient with a history of heart attack and an inconclusive EKG had MPS and FDG/PET study

122 FDG PET FOR MYOCARDIAL VIABILITY MYOCARDIAL SCAR Inferolateral Wall Severe Matching Defect on MPS and FDG STRESS THALLIUM REST THALLIUM FDG PET
123 Compare Perfusion with Viability
 on FDG REST THALLIUM FDG PET Short axis slices from the apex (left) to the base of the heart REVASCULARIZATION")
124 FDG-PET FOR MYOCARDIAL VIABILITY PERFUSION/METABOLISM MISMATCH = = VIABLE HIBERNATING MYOCARDIUM Anteroseptal Wall Severe Defect on MPS but viable (Mismatching) on FDG REST THALLIUM FDG PET Short axis slices from the apex (left) to the base of the heart REVASCULARIZATION INDICATED
125 MPS VIABILITY/PROGNOSIS PERFUSION / 18 FDG MISMACH ES UNDERLINE THE NEED FOR REVASCULARIZATION Among 43 patients with Mismatch in Perfusion/FDG, 26 who were revascularized showed increased survival as compared to those (17/43) with medical therapy Among 70 patients with No-Mismatch in Perfusion/FDG, there was no difference in survival between 17 patients who were revascularized and 53 treated medically DiCarli AJC 1994
126 Please explain to us what we see in the next picture and what lessons we learn from it
127 DiCarli AJC 1994 PERFUSION / 18 FDG MISMATCHES underline the need for Revascularization In Mismatch, Revascularization Increases Survival
128 MYOCARDIAL PERFUSION SCINTIGRAPHY (MPS) FOR CORONARY ARTERY DISEASE (CAD) (using 201 TlCl 2, 99m Tc-MP-Agents, PET-MP-Agents) DIAGNOSIS OF CLINICALLY SIGNIFICANT CAD (>60% lumen) CHRONIC STRESS PAIN (ANGINA), REST PAIN (UNSTABLE ANGINA), ACUTE CHEST PAIN (ACUTE MYOCARDIAL INFARCTION, MI), PREOPERATIVE EVALUATION OF PATIENTS WITH RISK FACTORS QUANTITATION OF SEVERITY AND EXTENT OF CAD ASSESS VIABILITY OF ISCHEMIC MYOCARDIUM POST MI OBTAIN PROGNOSIS BEFORE OR AFTER INFARCTION TO HELP THERAPY PLANNING FOLLOW UP EFFECT OF PTCA / CABG / MEDICAL Tx OR JUST THE COURSE OF THE DISEASE
129 COMPARISON OF ECHO WITH SCINTIGRAPHY Advantages of Scintigraphy Ischemia not required for regional abnormality Quantification of perfusion abnormality - extent and severity Greater reproducibility through quantification Detection of peri-infarction ischemia High success rate Not as dependent on physician s technical expertise Extensive literature on clinical value
130 COMPARISON OF ECHO WITH SCINTIGRAPHY Equal Value Detection of disease in patients with normal function at rest Left ventricular function Advantages of Echocardiography Ease and rapidity of study On-line visualization of the heart Evaluation of pericardium, valves, myocardium

131 MYOCARDIAL PERFUSION SCINTIGRAPHY George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL
123 Main St NY, New York 12345 ph: (202) 555 5555 fax: (202) 555 5555
 555 5555 fax: (202) 555 5555") Patient Name: DOE, JOHN D. Gender: M Date of Study: 4/2/2013 Date of birth: 6/28/1962 Age: 50 Medical Record #: 45869725 Ordering Physician: JANE INTERNIST, MD History: Atypical Angina, Abn ECG, High Cholesterol,
Patient Name: DOE, JOHN D. Gender: M Date of Study: 4/2/2013 Date of birth: 6/28/1962 Age: 50 Medical Record #: 45869725 Ordering Physician: JANE INTERNIST, MD History: Atypical Angina, Abn ECG, High Cholesterol,
Section 8: Clinical Exercise Testing. a maximal GXT?
 Section 8: Clinical Exercise Testing Maximal GXT ACSM Guidelines: Chapter 5 ACSM Manual: Chapter 8 HPHE 4450 Dr. Cheatham Outline What is the purpose of a maximal GXT? Who should have a maximal GXT (and
Section 8: Clinical Exercise Testing Maximal GXT ACSM Guidelines: Chapter 5 ACSM Manual: Chapter 8 HPHE 4450 Dr. Cheatham Outline What is the purpose of a maximal GXT? Who should have a maximal GXT (and
2015 Reimbursement Guide
 Reimbursement Guide - Cardiology 2015 Reimbursement Guide for Myocardial Perfusion Imaging including radiopharmaceuticals and related product information 2015 Reimbursement Guide for Myocardial Perfusion
Reimbursement Guide - Cardiology 2015 Reimbursement Guide for Myocardial Perfusion Imaging including radiopharmaceuticals and related product information 2015 Reimbursement Guide for Myocardial Perfusion
MYOCARDIAL PERFUSION COMPUTED TOMOGRAPHY PhD course in Medical Imaging. Anne Günther Department of Radiology OUS Rikshospitalet
 MYOCARDIAL PERFUSION COMPUTED TOMOGRAPHY PhD course in Medical Imaging Anne Günther Department of Radiology OUS Rikshospitalet CORONARY CT ANGIOGRAPHY (CTA) Accurate method in the assessment of possible
MYOCARDIAL PERFUSION COMPUTED TOMOGRAPHY PhD course in Medical Imaging Anne Günther Department of Radiology OUS Rikshospitalet CORONARY CT ANGIOGRAPHY (CTA) Accurate method in the assessment of possible
Efficient Evaluation of Chest Pain
 Efficient Evaluation of Chest Pain Vikranth Gongidi, DO FACC FACOI Indian River Medical Center Vero Beach, FL No Disclosures Outline Background Chest pain pathway Indications for stress test Stress test
Efficient Evaluation of Chest Pain Vikranth Gongidi, DO FACC FACOI Indian River Medical Center Vero Beach, FL No Disclosures Outline Background Chest pain pathway Indications for stress test Stress test
Pharmacologic Stress Agents
 Pharmacologic Stress Agents Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate family members
Pharmacologic Stress Agents Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate family members
Perioperative Cardiac Evaluation
 Perioperative Cardiac Evaluation Caroline McKillop Advisor: Dr. Tam Psenka 10-3-2007 Importance of Cardiac Guidelines -Used multiple times every day -Patient Safety -Part of Surgical Care Improvement Project
Perioperative Cardiac Evaluation Caroline McKillop Advisor: Dr. Tam Psenka 10-3-2007 Importance of Cardiac Guidelines -Used multiple times every day -Patient Safety -Part of Surgical Care Improvement Project
Diagnostic and Therapeutic Procedures
 Diagnostic and Therapeutic Procedures Diagnostic and therapeutic cardiovascular s are central to the evaluation and management of patients with cardiovascular disease. Consistent with the other sections,
Diagnostic and Therapeutic Procedures Diagnostic and therapeutic cardiovascular s are central to the evaluation and management of patients with cardiovascular disease. Consistent with the other sections,
Pharmacologic Stress Agents: Protocol and Safety
 Pharmacologic Stress Agents: Protocol and Safety Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate
Pharmacologic Stress Agents: Protocol and Safety Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate
The Role Of Early Stress Testing In Assessing Low Risk Chest Pain Patients Admitted Through The Emergency Department
 The Role Of Early Stress Testing In Assessing Low Risk Chest Pain Patients Admitted Through The Emergency Department Simbo Chiadika LAY ABSTRACT A. Study purpose Cardiac stress testing has been recommended
The Role Of Early Stress Testing In Assessing Low Risk Chest Pain Patients Admitted Through The Emergency Department Simbo Chiadika LAY ABSTRACT A. Study purpose Cardiac stress testing has been recommended
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology
 Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics. Yen Tibayan, M.D. Division of Cardiovascular Medicine
 Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics Yen Tibayan, M.D. Division of Cardiovascular Medicine Case Presentation 69 y.o. woman calls 911 with the complaint of
Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics Yen Tibayan, M.D. Division of Cardiovascular Medicine Case Presentation 69 y.o. woman calls 911 with the complaint of
RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department
 RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department Sohil Pothiawala FAMS (EM), MRCSEd (A&E), M.Med (EM), MBBS Consultant Dept. of Emergency Medicine Singapore General Hospital
RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department Sohil Pothiawala FAMS (EM), MRCSEd (A&E), M.Med (EM), MBBS Consultant Dept. of Emergency Medicine Singapore General Hospital
CHEST PAIN EVALUATION TOOL
 CHEST PAIN EVALUATION TOOL Chest pain or discomfort is one of the commonest causes for presentation to the Emergency Room (ER) or physicians office. There are many causes for chest discomfort. The serious
CHEST PAIN EVALUATION TOOL Chest pain or discomfort is one of the commonest causes for presentation to the Emergency Room (ER) or physicians office. There are many causes for chest discomfort. The serious
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Computed Tomography, Head Or Brain; Without Contrast Material, Followed By Contrast Material(S) And Further Sections
 And Further Sections") 1199SEIU BENEFIT AND PENSION FUNDS High Tech Diagnostic Radiology and s # 1 70336 Magnetic Resonance (Eg, Proton) Imaging, Temporomandibular Joint(S) 2 70450 Computed Tomography, Head Or Brain; Without
1199SEIU BENEFIT AND PENSION FUNDS High Tech Diagnostic Radiology and s # 1 70336 Magnetic Resonance (Eg, Proton) Imaging, Temporomandibular Joint(S) 2 70450 Computed Tomography, Head Or Brain; Without
Objectives. Cardiac Substrate Metabolism. 2004 SNM Mid-Winter Educational Symposium
 Myocardial Viability Imaging With PET Marcelo F. Di Carli,, MD Brigham and Women s Hospital Harvard Medical School Boston, MA Conflict of Interest: : No Relations to disclose To review: Basic principles
Myocardial Viability Imaging With PET Marcelo F. Di Carli,, MD Brigham and Women s Hospital Harvard Medical School Boston, MA Conflict of Interest: : No Relations to disclose To review: Basic principles
38 year old female with mild obesity. She is planning an exercise program to loose weight. She has no other known risk factors for CAD.
 Stress Testing: Wael A. Jaber, MD,FACC 38 year old female with mild obesity She is planning an exercise program to loose weight. She has no other known risk factors for CAD. You recommend: A. Exercise
Stress Testing: Wael A. Jaber, MD,FACC 38 year old female with mild obesity She is planning an exercise program to loose weight. She has no other known risk factors for CAD. You recommend: A. Exercise
2/20/2015. Cardiac Evaluation of Potential Solid Organ Transplant Recipients. Issues Specific to Transplantation. Kidney Transplantation.
 DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
12 Lead ECGs: Ischemia, Injury & Infarction Part 2
 12 Lead ECGs: Ischemia, Injury & Infarction Part 2 McHenry Western Lake County EMS Localization: Left Coronary Artery Right Coronary Artery Right Ventricle Septal Wall Anterior Descending Artery Left Main
12 Lead ECGs: Ischemia, Injury & Infarction Part 2 McHenry Western Lake County EMS Localization: Left Coronary Artery Right Coronary Artery Right Ventricle Septal Wall Anterior Descending Artery Left Main
Non Invasive Testing for CAD
 Non Invasive Testing for CAD Wael A. Jaber, MD Section of Cardiac Imaging Heart and Vascular Institute Cleveland Clinic 38 year old female with mild obesity She is planning an exercise program to loose
Non Invasive Testing for CAD Wael A. Jaber, MD Section of Cardiac Imaging Heart and Vascular Institute Cleveland Clinic 38 year old female with mild obesity She is planning an exercise program to loose
Cardiovascular diseases. pathology
 Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Listen to your heart: Good Cardiovascular Health for Life
 Listen to your heart: Good Cardiovascular Health for Life Luis R. Castellanos MD, MPH Assistant Clinical Professor of Medicine University of California San Diego School of Medicine Sulpizio Family Cardiovascular
Listen to your heart: Good Cardiovascular Health for Life Luis R. Castellanos MD, MPH Assistant Clinical Professor of Medicine University of California San Diego School of Medicine Sulpizio Family Cardiovascular
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
Pharmacologic Stress Test: Adenosine
 Pharmacologic Stress Test: Adenosine OVERVIEW The purpose of this document is to specifically identify the critical components involved in performing a pharmacologic stress test with adenosine. This information
Pharmacologic Stress Test: Adenosine OVERVIEW The purpose of this document is to specifically identify the critical components involved in performing a pharmacologic stress test with adenosine. This information
Predictive Implications of Stress Testing (Chapt. 14) 1979, Weiner and coworkers. Factors to improve the accuracy of stress testing
 1979, Weiner and coworkers. Factors to improve the accuracy of stress testing") Predictive Implications of Stress Testing (Chapt. 14) Sensitivity Specificity Predictive Value Patient Risk 1979, Weiner and coworkers Stress testing has very little diagnostic value. A positive stress
Predictive Implications of Stress Testing (Chapt. 14) Sensitivity Specificity Predictive Value Patient Risk 1979, Weiner and coworkers Stress testing has very little diagnostic value. A positive stress
CARDIOLOGY Delineation of Privileges
 CARDIOLOGY Delineation of Privileges APPLICANT: INITIAL APPOINTMENT REQUIREMENTS: BASIC EDUCATION: M.D. or D.O. from an accredited school of medicine or osteopathy. Successful completion of an ACGME or
CARDIOLOGY Delineation of Privileges APPLICANT: INITIAL APPOINTMENT REQUIREMENTS: BASIC EDUCATION: M.D. or D.O. from an accredited school of medicine or osteopathy. Successful completion of an ACGME or
Cardiac Assessment for Renal Transplantation: Pre-Operative Clearance is Only the Tip of the Iceberg
 Cardiac Assessment for Renal Transplantation: Pre-Operative Clearance is Only the Tip of the Iceberg 2 nd Annual Duke Renal Transplant Symposium March 1, 2014 Durham, NC Joseph G. Rogers, M.D. Associate
Cardiac Assessment for Renal Transplantation: Pre-Operative Clearance is Only the Tip of the Iceberg 2 nd Annual Duke Renal Transplant Symposium March 1, 2014 Durham, NC Joseph G. Rogers, M.D. Associate
CPT CODE PROCEDURE DESCRIPTION. CT Scans 70450 CT HEAD/BRAIN W/O CONTRAST 70460 CT HEAD/BRAIN W/ CONTRAST 70470 CT HEAD/BRAIN W/O & W/ CONTRAST
 CPT CODE PROCEDURE DESCRIPTION CT Scans 70450 CT HEAD/BRAIN W/O CONTRAST 70460 CT HEAD/BRAIN W/ CONTRAST 70470 CT HEAD/BRAIN W/O & W/ CONTRAST 70480 CT ORBIT W/O CONTRAST 70481 CT ORBIT W/ CONTRAST 70482
CPT CODE PROCEDURE DESCRIPTION CT Scans 70450 CT HEAD/BRAIN W/O CONTRAST 70460 CT HEAD/BRAIN W/ CONTRAST 70470 CT HEAD/BRAIN W/O & W/ CONTRAST 70480 CT ORBIT W/O CONTRAST 70481 CT ORBIT W/ CONTRAST 70482
What are some common uses of the procedure?
 Scan for mobile link. Cardiac Nuclear Medicine Cardiac nuclear medicine imaging evaluates the heart for coronary artery disease and cardiomyopathy. It also may be used to help determine whether the heart
Scan for mobile link. Cardiac Nuclear Medicine Cardiac nuclear medicine imaging evaluates the heart for coronary artery disease and cardiomyopathy. It also may be used to help determine whether the heart
Effect of Spinal Cord Stimulation on Myocardial Flow Reserve in Patients with Refractory Angina Pectoris
 Effect of Spinal Cord Stimulation on Myocardial Flow Reserve in Patients with Refractory Angina Pectoris Antti Varis, Heikki Ukkonen, Antti Saraste, Tuija Vasankari, Satu Tunturi, Markku Taittonen, Pirkka
Effect of Spinal Cord Stimulation on Myocardial Flow Reserve in Patients with Refractory Angina Pectoris Antti Varis, Heikki Ukkonen, Antti Saraste, Tuija Vasankari, Satu Tunturi, Markku Taittonen, Pirkka
NAME OF THE HOSPITAL: 1. Coronary Balloon Angioplasty: M7F1.1/ Angioplasty with Stent(PTCA with Stent): M7F1.3
: M7F1.3") 1. Coronary Balloon Angioplasty: M7F1.1/ Angioplasty with Stent(PTCA with Stent): M7F1.3 1. Name of the Procedure: Coronary Balloon Angioplasty 2. Select the Indication from the drop down of various indications
1. Coronary Balloon Angioplasty: M7F1.1/ Angioplasty with Stent(PTCA with Stent): M7F1.3 1. Name of the Procedure: Coronary Balloon Angioplasty 2. Select the Indication from the drop down of various indications
AI CPT Codes. x x. 70336 MRI Magnetic resonance (eg, proton) imaging, temporomandibular joint(s)
 imaging, temporomandibular joint(s)") Code Category Description Auth Required Medicaid Medicare 0126T IMT Testing Common carotid intima-media thickness (IMT) study for evaluation of atherosclerotic burden or coronary heart disease risk factor
Code Category Description Auth Required Medicaid Medicare 0126T IMT Testing Common carotid intima-media thickness (IMT) study for evaluation of atherosclerotic burden or coronary heart disease risk factor
PRECOMBAT Trial. Seung-Whan Lee, MD, PhD On behalf of the PRECOMBAT Investigators
 Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease PRECOMBAT Trial Seung-Whan Lee, MD, PhD On behalf
Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease PRECOMBAT Trial Seung-Whan Lee, MD, PhD On behalf
BASIC STANDARDS FOR RESIDENCY TRAINING IN CARDIOLOGY
 BASIC STANDARDS FOR RESIDENCY TRAINING IN CARDIOLOGY American Osteopathic Association and the American College of Osteopathic Internists Specific Requirements For Osteopathic Subspecialty Training In Cardiology
BASIC STANDARDS FOR RESIDENCY TRAINING IN CARDIOLOGY American Osteopathic Association and the American College of Osteopathic Internists Specific Requirements For Osteopathic Subspecialty Training In Cardiology
Part A: Structure and Organization
 Part A: Structure and Organization Radioactive Materials License NRC (or State) radioactive materials license present Personnel Medical Director Meets Medical Director responsibility requirements Meets
Part A: Structure and Organization Radioactive Materials License NRC (or State) radioactive materials license present Personnel Medical Director Meets Medical Director responsibility requirements Meets
Christopher M. Wright, MD, MBA Pioneer Cardiovascular Consultants Tempe, Arizona
 Christopher M. Wright, MD, MBA Pioneer Cardiovascular Consultants Tempe, Arizona Areas to be covered Historical, current, and future treatments for various cardiovascular disease: Atherosclerosis (Coronary
Christopher M. Wright, MD, MBA Pioneer Cardiovascular Consultants Tempe, Arizona Areas to be covered Historical, current, and future treatments for various cardiovascular disease: Atherosclerosis (Coronary
GENERAL HEART DISEASE KNOW THE FACTS
 GENERAL HEART DISEASE KNOW THE FACTS WHAT IS Heart disease is a broad term meaning any disease affecting the heart. It is commonly used to refer to coronary heart disease (CHD), a more specific term to
GENERAL HEART DISEASE KNOW THE FACTS WHAT IS Heart disease is a broad term meaning any disease affecting the heart. It is commonly used to refer to coronary heart disease (CHD), a more specific term to
Scott Hubbell, MHSc, RRT-NPS, C-NPT, CCT Clinical Education Coordinator/Flight RRT EagleMed
 Scott Hubbell, MHSc, RRT-NPS, C-NPT, CCT Clinical Education Coordinator/Flight RRT EagleMed Identify the 12-Lead Views Explain the vessels of occlusion Describe the three I s Basic Interpretation of 12-Lead
Scott Hubbell, MHSc, RRT-NPS, C-NPT, CCT Clinical Education Coordinator/Flight RRT EagleMed Identify the 12-Lead Views Explain the vessels of occlusion Describe the three I s Basic Interpretation of 12-Lead
Non-invasive functional testing in 2014
 Non-invasive functional testing in 2014 Bjarne Nørgaard Department Cardiology B Aarhus University Hospital Skejby, Disclosures: Research grants: Edwards and Siemens Non-invasive functional testing in 2014
Non-invasive functional testing in 2014 Bjarne Nørgaard Department Cardiology B Aarhus University Hospital Skejby, Disclosures: Research grants: Edwards and Siemens Non-invasive functional testing in 2014
Heart Attack: What You Need to Know
 A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
CARDIOLOGY PROCEDURES REQUIRING PRECERTIFICATION
 CLINICAL POLICY CARDIOLOGY PROCEDURES REQUIRING PRECERTIFICATION Policy Number: CARDIOLOGY 026.6 T2 Effective Date: May 1, 2015 Table of Contents CONDITIONS OF COVERAGE... COVERAGE RATIONALE... BENEFIT
CLINICAL POLICY CARDIOLOGY PROCEDURES REQUIRING PRECERTIFICATION Policy Number: CARDIOLOGY 026.6 T2 Effective Date: May 1, 2015 Table of Contents CONDITIONS OF COVERAGE... COVERAGE RATIONALE... BENEFIT
Rb 82 Cardiac PET Scanning Protocols and Dosimetry. Deborah Tout Nuclear Medicine Department Central Manchester University Hospitals
 Rb 82 Cardiac PET Scanning Protocols and Dosimetry Deborah Tout Nuclear Medicine Department Central Manchester University Hospitals Overview Rb 82 myocardial perfusion imaging protocols Acquisition Reconstruction
Rb 82 Cardiac PET Scanning Protocols and Dosimetry Deborah Tout Nuclear Medicine Department Central Manchester University Hospitals Overview Rb 82 myocardial perfusion imaging protocols Acquisition Reconstruction
Exchange solutes and water with cells of the body
 Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Society of Nuclear Medicine Procedure Guideline for Myocardial Perfusion Imaging
 Society of Nuclear Medicine Procedure Guideline for Myocardial Perfusion Imaging version 3.0, approved June 15, 2002 Authors: H. William Strauss, MD (Memorial Sloan Kettering Cancer Center, New York, NY);
Society of Nuclear Medicine Procedure Guideline for Myocardial Perfusion Imaging version 3.0, approved June 15, 2002 Authors: H. William Strauss, MD (Memorial Sloan Kettering Cancer Center, New York, NY);
Osama Jarkas. in Chest Pain Patients. STUDENT NAME: Osama Jarkas DATE: August 10 th, 2015
 STUDENT NAME: Osama Jarkas DATE: August 10 th, 2015 PROJECT TITLE: Analysis of ECG Exercise Stress Testing and Framingham Risk Score in Chest Pain Patients PRIMARY SUPERVISOR NAME: Dr. Edward Tan DEPARTMENT:
STUDENT NAME: Osama Jarkas DATE: August 10 th, 2015 PROJECT TITLE: Analysis of ECG Exercise Stress Testing and Framingham Risk Score in Chest Pain Patients PRIMARY SUPERVISOR NAME: Dr. Edward Tan DEPARTMENT:
Ischemic Heart Disease: Angina Pectoris
 Ischemic Heart Disease: Angina Pectoris Robert J. Straka, Pharm.D. FCCP Associate Professor University of Minnesota College of Pharmacy Minneapolis, Minnesota, USA strak001@umn.edu Learning Objectives
Ischemic Heart Disease: Angina Pectoris Robert J. Straka, Pharm.D. FCCP Associate Professor University of Minnesota College of Pharmacy Minneapolis, Minnesota, USA strak001@umn.edu Learning Objectives
INTRODUCTION TO EECP THERAPY
 INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
ECG may be indicated for patients with cardiovascular risk factors
 eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
LEADING-EDGE Cardiovascular Care
 LEADING-Edge Cardiovascular Care Coral Gables Hospital North Shore Medical Center Hialeah Hospital Delray Medical Center Good Samaritan Medical Center Palm Beach Gardens Medical Center St. Mary s Medical
LEADING-Edge Cardiovascular Care Coral Gables Hospital North Shore Medical Center Hialeah Hospital Delray Medical Center Good Samaritan Medical Center Palm Beach Gardens Medical Center St. Mary s Medical
National Imaging Associates, Inc. Clinical guidelines
 National Imaging Associates, Inc. Clinical guidelines Original Date: February 2010 STRESS ECHOCARDIOLOGY Page 1 of 15 CPT Codes: 93350, 93351, + 93352 Last Reviewed Date: June 2012 Guideline Number: NIA_CG_026
National Imaging Associates, Inc. Clinical guidelines Original Date: February 2010 STRESS ECHOCARDIOLOGY Page 1 of 15 CPT Codes: 93350, 93351, + 93352 Last Reviewed Date: June 2012 Guideline Number: NIA_CG_026
CPT * Codes Included in AIM Preauthorization Program for 2013 With Grouper Numbers
 CPT * Codes Included in AIM Preauthorization Program for 2013 With Grouper Numbers Computerized Tomography (CT) CPT Description Abdomen 74150 CT abdomen; w/o contrast 6 74160 CT abdomen; with contrast
CPT * Codes Included in AIM Preauthorization Program for 2013 With Grouper Numbers Computerized Tomography (CT) CPT Description Abdomen 74150 CT abdomen; w/o contrast 6 74160 CT abdomen; with contrast
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL)
") ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
Cilostazol versus Clopidogrel after Coronary Stenting
 Cilostazol versus Clopidogrel after Coronary Stenting Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea AMC, 2004 Background
Cilostazol versus Clopidogrel after Coronary Stenting Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea AMC, 2004 Background
CARDIA 288 MONTH FOLLOW-UP SUPPLEMENTAL FORM (FORM B) HOSPITALIZATION CASE #: INTERVIEWER ID FY288BIVID2. Page 1 of 6 FY288BH4CN
 HOSPITALIZATION CASE #: INTERVIEWER ID FY288BIVID2. Page 1 of 6 FY288BH4CN") HOSPITALIZATION CASE #: 2 8 8 0 H FY288BH4CN Has the participant indicated any of the following reasons for being admitted overnight for this case? 1. Suspected or confirmed problems with the heart, circulation,
HOSPITALIZATION CASE #: 2 8 8 0 H FY288BH4CN Has the participant indicated any of the following reasons for being admitted overnight for this case? 1. Suspected or confirmed problems with the heart, circulation,
Diagnostic Imaging Prior Review Code List 3 rd Quarter 2016
 Computerized Tomography (CT) Abdomen 6 Abdomen/Pelvis Combination 101 Service 74150 CT abdomen; w/o 74160 CT abdomen; with 74170 CT abdomen; w/o followed by 74176 Computed tomography, abdomen and pelvis;
Computerized Tomography (CT) Abdomen 6 Abdomen/Pelvis Combination 101 Service 74150 CT abdomen; w/o 74160 CT abdomen; with 74170 CT abdomen; w/o followed by 74176 Computed tomography, abdomen and pelvis;
Nuclear Medicine Coding 101 June 16, 2008 Contac me: DENISE@MERLINOHCCC.COM 1-888-60M-HCCC, 1-888-606-4222
 Nuclear Medicine Coding 101 June 16, 2008 Contac me: DENISE@MERLINOHCCC.COM 1-888-60M-HCCC, 1-888-606-4222 Presented by: Denise A. Merlino, MBA, CNMT, CPC, FSNMTS Disclosures SNM ASNC Bracco Diagnostics
Nuclear Medicine Coding 101 June 16, 2008 Contac me: DENISE@MERLINOHCCC.COM 1-888-60M-HCCC, 1-888-606-4222 Presented by: Denise A. Merlino, MBA, CNMT, CPC, FSNMTS Disclosures SNM ASNC Bracco Diagnostics
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
PET PROS PET Professional Resources and Outreach Source. A summary of the recommendations and practice guidelines of professional groups
 PET PROS PET Professional Resources and Outreach Source A summary of the recommendations and practice guidelines of professional groups Background: The SNMMI PET/CT Utilization Task Force (UTF) was formed
PET PROS PET Professional Resources and Outreach Source A summary of the recommendations and practice guidelines of professional groups Background: The SNMMI PET/CT Utilization Task Force (UTF) was formed
Provider Checklist-Outpatient Imaging. Checklist: Nuclear Stress Test, Thallium/Technetium/Sestamibi (CPT Code 78451-78454 78469)
") Provider Checklist-Outpatient Imaging Checklist: Nuclear Stress Test, Thallium/Technetium/Sestamibi (CPT Code 78451-78454 78469) Medical Review Note: Per InterQual, if any of the following are present,
Provider Checklist-Outpatient Imaging Checklist: Nuclear Stress Test, Thallium/Technetium/Sestamibi (CPT Code 78451-78454 78469) Medical Review Note: Per InterQual, if any of the following are present,
CHAPTER 9 DISEASES OF THE CIRCULATORY SYSTEM (I00-I99)
") CHAPTER 9 DISEASES OF THE CIRCULATORY SYSTEM (I00-I99) March 2014 2014 MVP Health Care, Inc. CHAPTER 9 CHAPTER SPECIFIC CATEGORY CODE BLOCKS I00-I02 Acute rheumatic fever I05-I09 Chronic rheumatic heart
CHAPTER 9 DISEASES OF THE CIRCULATORY SYSTEM (I00-I99) March 2014 2014 MVP Health Care, Inc. CHAPTER 9 CHAPTER SPECIFIC CATEGORY CODE BLOCKS I00-I02 Acute rheumatic fever I05-I09 Chronic rheumatic heart
Cardiovascular Guidelines for DOT Physical Exams By Maureen Collins MSN, APRN, BC
 Cardiovascular Guidelines for DOT Physical Exams By Maureen Collins MSN, APRN, BC The Federal Motor Carrier Safety Administration (FMCSA) administers the Federal Motor Carrier Safety Regulations (FMCSRs)
Cardiovascular Guidelines for DOT Physical Exams By Maureen Collins MSN, APRN, BC The Federal Motor Carrier Safety Administration (FMCSA) administers the Federal Motor Carrier Safety Regulations (FMCSRs)
Management of Pacing Wires After Cardiac Surgery
 Management of Pacing Wires After Cardiac Surgery David E. Lizotte, Jr. PA C, MPAS, FAPACVS President, Association of Physician Assistants in Cardiovascular Surgery Conflicts: None Indications 2008 Journal
Management of Pacing Wires After Cardiac Surgery David E. Lizotte, Jr. PA C, MPAS, FAPACVS President, Association of Physician Assistants in Cardiovascular Surgery Conflicts: None Indications 2008 Journal
Heart Center Packages
 Heart Center Packages For more information and appointments, Please contact The Heart Center of Excellence at the American Hospital Dubai Tel: +971-4-377-6571 Email: heartcenter@ahdubai.com www.ahdubai.com
Heart Center Packages For more information and appointments, Please contact The Heart Center of Excellence at the American Hospital Dubai Tel: +971-4-377-6571 Email: heartcenter@ahdubai.com www.ahdubai.com
6/5/2014. Objectives. Acute Coronary Syndromes. Epidemiology. Epidemiology. Epidemiology and Health Care Impact Pathophysiology
 Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Accurate Coding of Nuclear Medicine Procedures. Unravel Coding Basics
 Accurate Coding of Nuclear Medicine Procedures Presented by: Denise A. Merlino, MBA, CNMT, CPC Merlino Healthcare Consulting Corp. 1 Unravel Coding Basics October 27, 2009 2 1 Coding Basic Steps diagnosis
Accurate Coding of Nuclear Medicine Procedures Presented by: Denise A. Merlino, MBA, CNMT, CPC Merlino Healthcare Consulting Corp. 1 Unravel Coding Basics October 27, 2009 2 1 Coding Basic Steps diagnosis
Atrial Fibrillation An update on diagnosis and management
 Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
4/7/2015. Cardiac Rehabilitation: From the other side of the glass door. Chicago, circa 1999. Objectives. No disclosures, no conflicts
 Cardiac Rehabilitation: From the other side of the glass door No disclosures, no conflicts Charles X. Kim, MD, FACC, ABVM Objectives 1. Illustrate common CV benefits of CV rehab in real world practice.
Cardiac Rehabilitation: From the other side of the glass door No disclosures, no conflicts Charles X. Kim, MD, FACC, ABVM Objectives 1. Illustrate common CV benefits of CV rehab in real world practice.
Perioperative Risk Stratification for Noncardiac Surgical Patients with Cardiac Diagnosis. Michael A. Blazing
 Perioperative Risk Stratification for Noncardiac Surgical Patients with Cardiac Diagnosis Michael A. Blazing Outline The coming crush A practical approach to clinical risk assessment Classic approach to
Perioperative Risk Stratification for Noncardiac Surgical Patients with Cardiac Diagnosis Michael A. Blazing Outline The coming crush A practical approach to clinical risk assessment Classic approach to
Automatic External Defibrillators
 Last Review Date: May 27, 2016 Number: MG.MM.DM.10dC2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: May 27, 2016 Number: MG.MM.DM.10dC2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI)
") Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Diagnosis Code Crosswalk : ICD-9-CM to ICD-10-CM Cardiac Rhythm and Heart Failure Diagnoses
 Diagnosis Code Crosswalk : to 402.01 Hypertensive heart disease, malignant, with heart failure 402.11 Hypertensive heart disease, benign, with heart failure 402.91 Hypertensive heart disease, unspecified,
Diagnosis Code Crosswalk : to 402.01 Hypertensive heart disease, malignant, with heart failure 402.11 Hypertensive heart disease, benign, with heart failure 402.91 Hypertensive heart disease, unspecified,
Objectives. Preoperative Cardiac Risk Stratification for Noncardiac Surgery. History
 Preoperative Cardiac Risk Stratification for Noncardiac Surgery Kimberly Boddicker, MD FACC Essentia Health Heart and Vascular Center 27 th Heart and Vascular Conference May 13, 2011 Objectives Summarize
Preoperative Cardiac Risk Stratification for Noncardiac Surgery Kimberly Boddicker, MD FACC Essentia Health Heart and Vascular Center 27 th Heart and Vascular Conference May 13, 2011 Objectives Summarize
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
Ch. 138 CARDIAC CATHETERIZATION SERVICES 28 138.1 CHAPTER 138. CARDIAC CATHETERIZATION SERVICES GENERAL PROVISIONS
 Ch. 138 CARDIAC CATHETERIZATION SERVICES 28 138.1 CHAPTER 138. CARDIAC CATHETERIZATION SERVICES Sec. 138.1 Principle. 138.2. Definitions. GENERAL PROVISIONS PROGRAM, SERVICE, PERSONNEL AND AGREEMENT REQUIREMENTS
Ch. 138 CARDIAC CATHETERIZATION SERVICES 28 138.1 CHAPTER 138. CARDIAC CATHETERIZATION SERVICES Sec. 138.1 Principle. 138.2. Definitions. GENERAL PROVISIONS PROGRAM, SERVICE, PERSONNEL AND AGREEMENT REQUIREMENTS
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY. Guidelines for Use of Intravenous Isoproterenol
 ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
EMR Tutorial Acute Coronary Syndrome
 EMR Tutorial Acute Coronary Syndrome How to find the Acute Coronary Syndrome AAA Home Page 1 of 26 Master Tool Bar Icon When the Template button is clicked you will be presented with the preference list.
EMR Tutorial Acute Coronary Syndrome How to find the Acute Coronary Syndrome AAA Home Page 1 of 26 Master Tool Bar Icon When the Template button is clicked you will be presented with the preference list.
Positron Emission Tomography - For Patients
 Positron Emission Tomography - For Patients A physician s written order is required for any PET-CT tests. How should I prepare for my PET-CT? PET-CT is more complicated than most other tests you may be
Positron Emission Tomography - For Patients A physician s written order is required for any PET-CT tests. How should I prepare for my PET-CT? PET-CT is more complicated than most other tests you may be
Acute Coronary Syndrome. What Every Healthcare Professional Needs To Know
 Acute Coronary Syndrome What Every Healthcare Professional Needs To Know Background of ACS Acute Coronary Syndrome (ACS) is an umbrella term used to cover a spectrum of clinical conditions that are caused
Acute Coronary Syndrome What Every Healthcare Professional Needs To Know Background of ACS Acute Coronary Syndrome (ACS) is an umbrella term used to cover a spectrum of clinical conditions that are caused
Pre-Screening and Risk Stratification
 Pre-Screening and Risk Stratification Chapter 1, 2 and 3 ACSM What is involved in the prescreening process? The Basic Goal To determine if it is safe for an individual to start an exercise program, what
Pre-Screening and Risk Stratification Chapter 1, 2 and 3 ACSM What is involved in the prescreening process? The Basic Goal To determine if it is safe for an individual to start an exercise program, what
FFR CT : Clinical studies
 FFR CT : Clinical studies Bjarne Nørgaard Department Cardiology B Aarhus University Hospital Skejby, Denmark Disclosures: Research grants: Edwards and Siemens Coronary CTA: High diagnostic sensitivity
FFR CT : Clinical studies Bjarne Nørgaard Department Cardiology B Aarhus University Hospital Skejby, Denmark Disclosures: Research grants: Edwards and Siemens Coronary CTA: High diagnostic sensitivity
Physician and other health professional services
 O n l i n e A p p e n d i x e s 4 Physician and other health professional services 4-A O n l i n e A p p e n d i x Access to physician and other health professional services 4 a1 Access to physician care
O n l i n e A p p e n d i x e s 4 Physician and other health professional services 4-A O n l i n e A p p e n d i x Access to physician and other health professional services 4 a1 Access to physician care
Signal-averaged electrocardiography late potentials
 SIGNAL AVERAGED ECG INTRODUCTION Signal-averaged electrocardiography (SAECG) is a special electrocardiographic technique, in which multiple electric signals from the heart are averaged to remove interference
SIGNAL AVERAGED ECG INTRODUCTION Signal-averaged electrocardiography (SAECG) is a special electrocardiographic technique, in which multiple electric signals from the heart are averaged to remove interference
Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR:
 Bruce Protocol - Submaximal GXT Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR: Stage Min. % Grade MPH METs 2min HR 3min HR BP RPE 1 0-3 10 1.7 4.7 2 3-6 12 2.5 7.0 3 6-9 14 3.4 10.1
Bruce Protocol - Submaximal GXT Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR: Stage Min. % Grade MPH METs 2min HR 3min HR BP RPE 1 0-3 10 1.7 4.7 2 3-6 12 2.5 7.0 3 6-9 14 3.4 10.1
CV Disease : A Major Threat to Public Health
 CV Disease : A Major Threat to Public Health International Atomic Energy Agency United Nations, Vienna - Austria João V. Vitola, MD, PhD Cardiologist and Nuclear Medicine Physician QUANTA Diagnostico &
CV Disease : A Major Threat to Public Health International Atomic Energy Agency United Nations, Vienna - Austria João V. Vitola, MD, PhD Cardiologist and Nuclear Medicine Physician QUANTA Diagnostico &
Systematic Approach to 12 Lead EKG Interpretation
 Systematic Approach to 12 Lead EKG Interpretation Maureen Knechtel MPAS, PA-C Wellmont CVA Heart Institute Disclosure Statement of Financial Interest I, Maureen Knechtel, do not have a financial interest/arrangement
Systematic Approach to 12 Lead EKG Interpretation Maureen Knechtel MPAS, PA-C Wellmont CVA Heart Institute Disclosure Statement of Financial Interest I, Maureen Knechtel, do not have a financial interest/arrangement
CPT Radiology Codes Requiring Review by AIM Effective 01/01/2016
 CPT Radiology Codes Requiring Review by AIM Effective 01/01/2016 When a service is authorized only one test per group is payable. *Secondary codes or add-on codes do not require preauthorization or separate
CPT Radiology Codes Requiring Review by AIM Effective 01/01/2016 When a service is authorized only one test per group is payable. *Secondary codes or add-on codes do not require preauthorization or separate
Tachyarrhythmias (fast heart rhythms)
") Patient information factsheet Tachyarrhythmias (fast heart rhythms) The normal electrical system of the heart The heart has its own electrical conduction system. The conduction system sends signals throughout
Patient information factsheet Tachyarrhythmias (fast heart rhythms) The normal electrical system of the heart The heart has its own electrical conduction system. The conduction system sends signals throughout
ST Segment Elevation Nothing is ever as hard (or easy) as it looks
 as it looks") ST Segment Elevation Nothing is ever as hard (or easy) as it looks Cameron Guild, MD Division of Cardiology University of Mississippi Medical Center February 17, 2012 Objectives 1. Describe the electrical
ST Segment Elevation Nothing is ever as hard (or easy) as it looks Cameron Guild, MD Division of Cardiology University of Mississippi Medical Center February 17, 2012 Objectives 1. Describe the electrical
CARDIAC CARE. Giving you every advantage
 CARDIAC CARE Giving you every advantage Getting to the heart of the matter The Cardiovascular Program at Northwest Hospital & Medical Center is dedicated to the management of cardiovascular disease. The
CARDIAC CARE Giving you every advantage Getting to the heart of the matter The Cardiovascular Program at Northwest Hospital & Medical Center is dedicated to the management of cardiovascular disease. The
Pre-Operative Cardiac Evaluation Kalpana Jain, MD
 Pre-Operative Cardiac Evaluation Kalpana Jain, MD Cardiac evaluation is an integral part of pre-op evaluation. Perioperative cardiac events are common causes of mortality. Major cardiac complications associated
Pre-Operative Cardiac Evaluation Kalpana Jain, MD Cardiac evaluation is an integral part of pre-op evaluation. Perioperative cardiac events are common causes of mortality. Major cardiac complications associated
PET and PET/CT in Clinical Trials
 PET and PET/CT in Clinical Trials Nathan C. Hall, M.D., Ph.D. The Ohio State University Medical Center CALGB Imaging Core Lab CALGB Imaging Committee Outline Introduction to PET Positron Emitter Physics
PET and PET/CT in Clinical Trials Nathan C. Hall, M.D., Ph.D. The Ohio State University Medical Center CALGB Imaging Core Lab CALGB Imaging Committee Outline Introduction to PET Positron Emitter Physics
For the NXT Investigators
 Diagnostic performance of non-invasive fractional flow reserve derived from coronary CT angiography in suspected coronary artery disease: The NXT trial Bjarne L. Nørgaard, Jonathon Leipsic, Sara Gaur,
Diagnostic performance of non-invasive fractional flow reserve derived from coronary CT angiography in suspected coronary artery disease: The NXT trial Bjarne L. Nørgaard, Jonathon Leipsic, Sara Gaur,
Chest Pain in Young Athletes. Christopher Davis, MD, PhD Pediatric Cardiology Rady Children s Hospital San Diego cdavis@rchsd.
 Chest Pain in Young Athletes Christopher Davis, MD, PhD Pediatric Cardiology Rady Children s Hospital San Diego cdavis@rchsd.org 858-966-5855 None Disclosures Chest Pain: the good news and the bad news:
Chest Pain in Young Athletes Christopher Davis, MD, PhD Pediatric Cardiology Rady Children s Hospital San Diego cdavis@rchsd.org 858-966-5855 None Disclosures Chest Pain: the good news and the bad news:
Atrial Fibrillation Peter Santucci, MD Revised May, 2008
 Atrial Fibrillation Peter Santucci, MD Revised May, 2008 Atrial fibrillation (AF) is an irregular, disorganized rhythm characterized by a lack of organized mechanical atrial activity. The atrial rate is
Atrial Fibrillation Peter Santucci, MD Revised May, 2008 Atrial fibrillation (AF) is an irregular, disorganized rhythm characterized by a lack of organized mechanical atrial activity. The atrial rate is
Tips and Tricks to Demystify 12 Lead ECG Interpretation
 Tips and Tricks to Demystify 12 Lead ECG Interpretation Mission: Lifeline North Dakota Regional EMS and Hospital Conference Samantha Kapphahn, DO Essentia Health- Interventional Cardiology June 5th, 2014
Tips and Tricks to Demystify 12 Lead ECG Interpretation Mission: Lifeline North Dakota Regional EMS and Hospital Conference Samantha Kapphahn, DO Essentia Health- Interventional Cardiology June 5th, 2014
Management of Atrial Fibrillation in Heart Failure
 Disadvantages of AV Junction Ablation Persistent AFib- no AV synchrony Ongoing risk of thromboembolism Life-long dependency on pacemaker Comparison of LA Ablation vs. AVN Ablation LA Ablation AVN Ablation
Disadvantages of AV Junction Ablation Persistent AFib- no AV synchrony Ongoing risk of thromboembolism Life-long dependency on pacemaker Comparison of LA Ablation vs. AVN Ablation LA Ablation AVN Ablation
Noninvasive testing can provide useful information for
 CONTINUING EDUCATION Roles of Nuclear Cardiology, Cardiac Computed Tomography, and Cardiac Magnetic Resonance: Noninvasive Risk Stratification and a Conceptual Framework for the Selection of Noninvasive
CONTINUING EDUCATION Roles of Nuclear Cardiology, Cardiac Computed Tomography, and Cardiac Magnetic Resonance: Noninvasive Risk Stratification and a Conceptual Framework for the Selection of Noninvasive
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains