Canadian Diabetes Association 2013 Clinical Practice Guidelines
|
|
|
- Octavia Copeland
- 7 years ago
- Views:
Transcription
1 Canadian Diabetes Association 2013 Clinical Practice Guidelines Presentation by: Kerry Mansell, PharmD, CDE
2 Learning Objectives By the end of this session, participants will be: 1. familiar with most major changes within the 2013 CDA clinical practice guidelines 2. able to apply the recommendations in clinical practice and be familiar with online resources
3
4 Neither evidence nor clinical judgment alone is sufficient. Evidence without judgment can be applied by a technician. Judgment without evidence can be applied by a friend. But the integration of evidence and judgment is what the healthcare provider does in order to dispense the best clinical care. (Hertzel Gerstein, 2012)
5 What is new in making the diagnosis of diabetes?
6 Diagnosis of Diabetes 2013 FPG 7.0 mmol/l Fasting = no caloric intake for at least 8 hours or A1C 6.5% (in adults) Using a standardized, validated assay, in the absence of factors that affect the accuracy of the A1C and not for suspected type 1 diabetes or 2hPG in a 75-g OGTT 11.1 mmol/l or Random PG 11.1 mmol/l Random= any time of the day, without regard to the interval since the last meal 2hPG = 2-hour plasma glucose; FPG = fasting plasma glucose; OGTT = oral glucose tolerance test; PG = plasma glucose
7 Diagnosis of Prediabetes* 2013 Test Result Prediabetes Category Fasting Plasma Glucose (mmol/l) 2-hr Plasma Glucose in a 75-g Oral Glucose Tolerance Test (mmol/l) Glycated Hemoglobin (A1C) (%) Impaired fasting glucose (IFG) Impaired glucose tolerance (IGT) Prediabetes * Prediabetes = IFG, IGT or A1C % high risk of developing T2DM
8 A1C Level and Future Risk of Diabetes: Systematic Review A1C Category (%) 5-year incidence of diabetes <5 to 9% to 25% to 50% Zhang X et al. Diabetes Care. 2010;33:
9 Screening
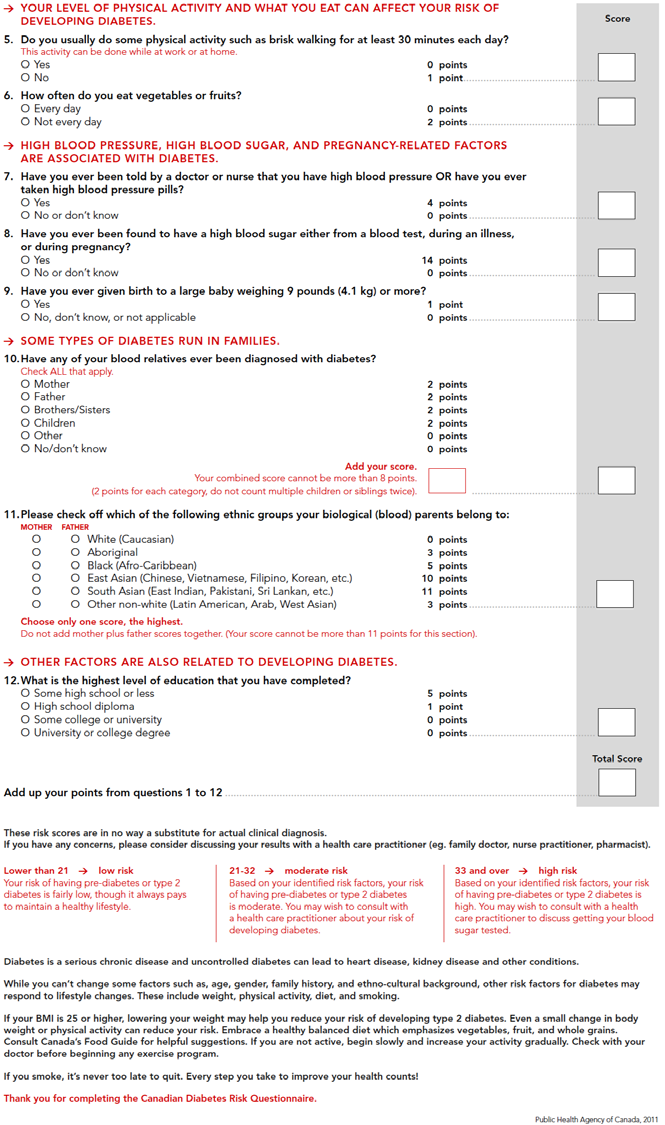
10 If you choose to use a diabetes risk calculator Public Health Agency of Canada CANRISK calculator For people years old Components Age, sex, BMI, waist circumference Physical activity level, eating veg and fruits Hypertension, history of dysglycemia (GDM, acute illness etc.) macrosomia Family history, ethnicity, level of education Calculates low, moderate or high risk groups

11
12 Glycemic Targets: New Targets and why?
13 2013 Targets Checklist A1C 7.0% for MOST people with diabetes A1C 6.5% for SOME people with T2DM A1C % in people with specific features

14 Macro and Microvascular Benefits? diabetes.ca BANTING ( )
15 A1c 7.0% Large trials support this number with reduced complications It can usually be safely achieved in most people with diabetes

16 diabetes.ca BANTING ( )
 Recurrent")
17 A1c 6.5% Encourage in those in whom it is safe to do so Some evidence of reduced microvascular complications (ADVANCE) Recurrent hypoglycemia is associated with detrimental effects on vasculature, increased risk of falls, cognitive decline Benefit Hypoglycemia
18 diabetes.ca BANTING ( )
19 Consider A1C % if 2013 Limited life expectancy High level of functional dependency Extensive coronary artery disease at high risk of ischemic events Multiple co-morbidities History of recurrent severe hypoglycemia Hypoglycemia unawareness Longstanding diabetes for whom is it difficult to achieve an A1C 7%, despite effective doses of multiple antihyperglycemic agents

20 Individualizing A1C Targets 2013 Consider % if: which must be balanced against the risk of hypoglycemia Copyright guidelines.diabetes.ca 2013 Canadian BANTING Diabetes Association ( ) diabetes.ca
21 Diabetes in the Elderly Checklist 2013 ASSESS for level of functional dependency (frailty) INDIVIDUALIZE glycemic targets based on the above (A1C 8.5% for frail elderly) but if otherwise healthy, use the same targets as younger people AVOID hypoglycemia in cognitive impairment, frail elderly SELECT antihyperglycemic therapy carefully caution with sulfonylureas or thiazolidinediones Basal analogues instead of NPH or human 30/70 insulin Premixed insulins instead of mixing insulins separately GIVE regular diets instead of diabetic diets or nutritional formulas in nursing homes
22 Moorhouse P, Rockwood K. J R Coll Physicians Edinb 2012;42:
23 Among frail elderly 2013 Parameter Target A1C 8.5% FPG or preprandial glucose mmol/l (depending on level of frailty) FPG= fasting plasma glucose AVOID HYPOGLYCEMIA
24 owering/a1ctarget Copyright guidelines.diabetes.ca 2013 Canadian BANTING Diabetes Association ( ) diabetes.ca
25 Self-Monitoring of Blood Glucose (SMBG) What should we tell patients to do?

26 Regular SMBG is Required for:

27 Increased frequency of SMBG may be required: Daily SMBG is not usually required if patient:


28
29 Medications for glycemia How do we choose?
30 Pharmacotherapy in T2DM checklist 2013 CHOOSE initial therapy based on glycemia START with Metformin +/- others INDIVIDUALIZE your therapy choice based on characteristics of the patient and the agent REACH TARGET within 3-6 months of diagnosis
31 AT DIAGNOSIS OF TYPE 2 DIABETES L I F E S T Y L E 2013 Start lifestyle intervention (nutrition therapy and physical activity) +/- Metformin A1C <8.5% If not at glycemic target (2-3 mos) Start / Increase metformin A1C 8.5% Start metformin immediately Consider initial combination with another antihyperglycemic agent If not at glycemic targets Add an agent best suited to the individual: Patient Characteristics Degree of hyperglycemia Risk of hypoglycemia Overweight or obesity Comorbidities (renal, cardiac, hepatic) Preferences & access to treatment Other See next page Symptomatic hyperglycemia with metabolic decompensation Agent Characteristics BG lowering efficacy and durability Risk of inducing hypoglycemia Effect on weight Contraindications & side-effects Cost and coverage Other Initiate insulin +/- metformin
32 From prior page L I F E S T Y L E If not at glycemic target Add another agent from a different class Add/Intensify insulin regimen 2013 Make timely adjustments to attain target A1C within 3-6 months
33 Antihyperglycemic agents and Renal Function CKD Stage: GFR (ml/min): < Acarbose 25 Metformin Linagliptin Saxagliptin mg Sitagliptin mg mg Exenatide Liraglutide 50 Gliclazide/Glimepiride Glyburide Repaglinide Thiazolidinediones Not recommended / contraindicated Caution and/or dose reduction Safe Adapted Copyright from: Product 2013 Canadian Monographs Diabetes as of Association March 1, 2013; CDA Guidelines 2008; and Yale JF. J Am Soc Nephrol 2005; 16:S7-S10.
34 coselowering/pharmacologyt2
35 Macrovascular Disease Vascular Protection: Who and When?
36 Vascular Protection Checklist 2013 A A1C optimal glycemic control (usually 7%) B BP optimal blood pressure control (<130/80) C Cholesterol LDL 2.0 mmol/l if decided to treat D Drugs to protect the heart A ACEi or ARB S Statin A ASA if indicated E Exercise regular physical activity, healthy diet, achieve and maintain healthy body weight S Smoking cessation
37 Who Should Receive Statins? yrs old or Macrovascular disease or Microvascular disease or DM >15 yrs duration and age >30 years or Warrants therapy based on the 2012 Canadian Cardiovascular Society lipid guidelines Among women with childbearing potential, statins should only be used in the presence of proper preconception counseling & reliable contraception. Stop statins prior to conception.
38 If on a statin: target is LDL 2 mmol/l or >50% reduction in LDL 2013 If Triglycerides > 10.0 mmol/l: Use a FIBRATE to reduce the risk of pancreatitis Optimize glycemic control Implement lifestyle interventions Weight loss Optimal dietary strategies Reduce alcohol
39 Who Should Receive ACEi or ARB Therapy? 55 years of age or Macrovascular disease or Microvascular disease At doses that have shown vascular protection (ramipril 10 mg daily, perindopril 8 mg daily, telmisartan 80 mg daily) Among women with childbearing potential, ACEi or ARB should only be used in the presence of proper preconception counseling & reliable contraception. Stop ACEi or ARB either prior to conception or immediately upon detection of pregnancy 2013
40 Summary of Pharmacotherapy for Hypertension in Patients with Diabetes Threshold equal or over 130/80 mmhg and Target below 130/80 mmhg Diabetes With Nephropathy, CVD or CV risk factors Without the above ACE Inhibitor or ARB 1. ACE Inhibitor or ARB or 2. Thiazide diuretic or DHP-CCB Combination of 2 first line drugs may be considered as initial therapy if the blood pressure is >20 mmhg systolic or >10 mmhg diastolic above target > 2-drug combinations Monitor serum potassium and creatinine carefully in patients with CKD prescribed an ACEI or ARB Combinations of an ACEI with an ARB are specifically not recommended in the absence of proteinuria More than 3 drugs may be needed to reach target values If Creatinine over 150 µmol/l or creatinine clearance below 30 ml/min ( 0.5 ml/sec), a loop diuretic should be substituted for a thiazide diuretic if control of volume is desired
41 No. of events/no. in group ASA for 1⁰ Prevention in Diabetes Meta analysis of 6 studies No overall benefit for: Major CV events MI Stroke CV mortality All-cause mortality arprotection/riskassessment JPAD POPADAD WHS PPP ETDRS Total JPAD POPADAD PPP ETDRS Total De Beradis G, et al. BMJ 2009; 339:b4531. ASA Control/placebo RR (95% CI) RR (95% CI) Major CV events 68/ /638 58/514 20/ / /4789 Myocardial infarction JPAD POPADAD WHS PPP ETDRS PHS Total Stroke JPAD POPADAD WHS PPP ETDRS Total 28/ /638 36/514 5/ / / / / /638 15/514 9/519 92/ /4789 Death from CV causes JPAD POPADAD PPP ETDRS Total 1/ /638 10/ / /4275 All-cause mortality 34/ /638 25/ / / / /638 62/513 22/ / / / /638 24/513 10/ / / / / /638 31/513 10/512 78/ / / /638 8/ / / / /638 20/ / / Favors ASA 0.80 ( ) 0.97 ( ) 0.90 ( ) 0.90 ( ) 0.90 ( ) 0.90 ( ) 0.87 ( ) 1.10 ( ) 1.48 ( ) 0.49 ( ) 0.82 ( ) 0.40 ( ) 0.86 ( ) 0.89 ( ) 0.74 ( ) 0.46 ( ) 0.89 ( ) 1.17 ( ) 0.83 ( ) 0.10 ( ) 1.23 ( ) 1.23 ( ) 0.87 ( ) 0.94 ( ) 0.90 ( ) 0.93 ( ) 1.23 ( ) 0.91 ( ) 0.93 ( ) 2 8 Favors control/placebo
42 tion/riskassessment
43 What are the benefits if we do all of the vascular protective steps?



44 Use a Multifaceted Vascular Protection Strategy Healthy Lifestyle/weight Smoking Cessation Physical Activity BP <130/80 A1C 7% Rx: Statins ACEi/ARB
45 STENO-2: Intensive Group had Improved CV Outcomes Any CV event NNT = RRR= relative risk reduction Gaede et al. NEJM. 2003: 348; P = Conventional therapy Intensive therapy Months of Follow-up 53 % RRR
46 What about Microvascular Disease? Nephropathy
47 Chronic Kidney Disease (CKD) Checklist 2013 SCREEN regularly with random urine albumin creatinine ratio (ACR) and serum creatinine for estimated glomerular filtration rate (egfr) DIAGNOSE with repeat confirmed ACR 2.0 mg/mmol and/or egfr < 60 ml/min DELAY onset and/or progression with glycemic and blood pressure control and ACE inhibitor or angiotensin receptor blocker (ARB) PREVENT complications with sick day management counselling and referral when appropriate

48 Counsel all Patients About Sick Day Medication List 2013
49 2013 ACR 2.0 mg/mmol CKD in diabetes and/or egfr < 60 ml/min
50 How can we keep track of all these parameters for our patients?
51 Tools to help us keep track of our patients
52 Cheat Sheet of Targets and Goals
The Canadian Diabetes Association s 2013 Clinical Practice Guidelines and the Pharmacist Rob Roscoe, B.Sc.Pharm., ACPR, CDE, CPT
 Welcome! Thank you for joining the webinar: The Canadian Diabetes Association s 2013 Clinical Practice Guidelines and the Pharmacist Rob Roscoe, B.Sc.Pharm., ACPR, CDE, CPT The webinar will begin shortly.
Welcome! Thank you for joining the webinar: The Canadian Diabetes Association s 2013 Clinical Practice Guidelines and the Pharmacist Rob Roscoe, B.Sc.Pharm., ACPR, CDE, CPT The webinar will begin shortly.
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated March 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated March 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Diabetes sections of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Diabetes sections of the Guidelines) Authors: Dr. M. Love, Kathy Harrigan Reviewers:
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Diabetes sections of the Guidelines) Authors: Dr. M. Love, Kathy Harrigan Reviewers:
Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria.
 Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Take a moment Confer with your neighbour And try to solve the following word picture puzzle slides.
 Take a moment Confer with your neighbour And try to solve the following word picture puzzle slides. Example: = Head Over Heels Take a moment Confer with your neighbour And try to solve the following word
Take a moment Confer with your neighbour And try to solve the following word picture puzzle slides. Example: = Head Over Heels Take a moment Confer with your neighbour And try to solve the following word
Vascular Risk Reduction: Addressing Vascular Risk
 Vascular Risk Reduction: Addressing Vascular Risk Vascular Risk Reduction (VRR) Welcome! Presentation & Activities Focus: Managing known risk factors for vascular disease. Engage, collaborate and have
Vascular Risk Reduction: Addressing Vascular Risk Vascular Risk Reduction (VRR) Welcome! Presentation & Activities Focus: Managing known risk factors for vascular disease. Engage, collaborate and have
Understanding diabetes Do the recent trials help?
 Understanding diabetes Do the recent trials help? Dr Geoffrey Robb Consultant Physician and Diabetologist CMO RGA UK Services and Partnership Assurance AMUS 25 th March 2010 The security of experience.
Understanding diabetes Do the recent trials help? Dr Geoffrey Robb Consultant Physician and Diabetologist CMO RGA UK Services and Partnership Assurance AMUS 25 th March 2010 The security of experience.
TYPE 2 DIABETES MELLITUS: NEW HOPE FOR PREVENTION. Robert Dobbins, M.D. Ph.D.
 TYPE 2 DIABETES MELLITUS: NEW HOPE FOR PREVENTION Robert Dobbins, M.D. Ph.D. Learning Objectives Recognize current trends in the prevalence of type 2 diabetes. Learn differences between type 1 and type
TYPE 2 DIABETES MELLITUS: NEW HOPE FOR PREVENTION Robert Dobbins, M.D. Ph.D. Learning Objectives Recognize current trends in the prevalence of type 2 diabetes. Learn differences between type 1 and type
嘉 義 長 庚 醫 院 藥 劑 科 Speaker : 翁 玟 雯
 The Clinical Efficacy and Safety of Sodium Glucose Cotransporter-2 (SGLT2) Inhibitors in Adults with Type 2 Diabetes Mellitus 嘉 義 長 庚 醫 院 藥 劑 科 Speaker : 翁 玟 雯 Diabetes Mellitus : A group of diseases characterized
The Clinical Efficacy and Safety of Sodium Glucose Cotransporter-2 (SGLT2) Inhibitors in Adults with Type 2 Diabetes Mellitus 嘉 義 長 庚 醫 院 藥 劑 科 Speaker : 翁 玟 雯 Diabetes Mellitus : A group of diseases characterized
ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Effects of a fixed combination of the ACE inhibitor, perindopril,
ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Effects of a fixed combination of the ACE inhibitor, perindopril,
CASE A1 Hypoglycemia in an Elderly T2DM Patient with Heart Failure
 Hypoglycemia in an Elderly T2DM Patient with Heart Failure 1 I would like to introduce you to Sophie, an elderly patient with long-standing type 2 diabetes, who has a history of heart failure, a common
Hypoglycemia in an Elderly T2DM Patient with Heart Failure 1 I would like to introduce you to Sophie, an elderly patient with long-standing type 2 diabetes, who has a history of heart failure, a common
Guidelines for the management of hypertension in patients with diabetes mellitus
 Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
Diabetic Nephropathy
 Diabetic Nephropathy Kidney disease is common in people affected by diabetes mellitus Definition Urinary albumin excretion of more than 300mg in a 24 hour collection or macroalbuminuria Abnormal renal
Diabetic Nephropathy Kidney disease is common in people affected by diabetes mellitus Definition Urinary albumin excretion of more than 300mg in a 24 hour collection or macroalbuminuria Abnormal renal
Management of Diabetes in the Elderly. Sylvia Shamanna Internal Medicine (R1)
") Management of Diabetes in the Elderly Sylvia Shamanna Internal Medicine (R1) Case 74 year old female with frontal temporal lobe dementia admitted for prolonged delirium and frequent falls (usually in the
Management of Diabetes in the Elderly Sylvia Shamanna Internal Medicine (R1) Case 74 year old female with frontal temporal lobe dementia admitted for prolonged delirium and frequent falls (usually in the
Managing diabetes in the post-guideline world. Dr Helen Snell Nurse Practitioner PhD, FCNA(NZ)
") Managing diabetes in the post-guideline world Dr Helen Snell Nurse Practitioner PhD, FCNA(NZ) Overview Pathogenesis of T2DM Aims of treatment The place of glycaemic control Strategies to improve glycaemic
Managing diabetes in the post-guideline world Dr Helen Snell Nurse Practitioner PhD, FCNA(NZ) Overview Pathogenesis of T2DM Aims of treatment The place of glycaemic control Strategies to improve glycaemic
Adult Diabetes Clinician Guide
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction JANUARY 2016 This evidence-based guideline summary is based on the 2016 National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction JANUARY 2016 This evidence-based guideline summary is based on the 2016 National Diabetes Guideline.
SHORT CLINICAL GUIDELINE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SHORT CLINICAL GUIDELINE SCOPE 1 Guideline title Type 2 diabetes: newer agents for blood glucose control in type 2 diabetes 1.1 Short title Type 2
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SHORT CLINICAL GUIDELINE SCOPE 1 Guideline title Type 2 diabetes: newer agents for blood glucose control in type 2 diabetes 1.1 Short title Type 2
Cardiovascular Risk in Diabetes
 Cardiovascular Risk in Diabetes Lipids Hypercholesterolaemia is an important reversible risk factor for cardiovascular disease and should be tackled aggressively in all diabetic patients. In Type 1 patients,
Cardiovascular Risk in Diabetes Lipids Hypercholesterolaemia is an important reversible risk factor for cardiovascular disease and should be tackled aggressively in all diabetic patients. In Type 1 patients,
CASE B1. Newly Diagnosed T2DM in Patient with Prior MI
 Newly Diagnosed T2DM in Patient with Prior MI 1 Our case involves a gentleman with acute myocardial infarction who is newly discovered to have type 2 diabetes. 2 One question is whether anti-hyperglycemic
Newly Diagnosed T2DM in Patient with Prior MI 1 Our case involves a gentleman with acute myocardial infarction who is newly discovered to have type 2 diabetes. 2 One question is whether anti-hyperglycemic
DM Management in Elderly- What are the glucose targets?
 DM Management in Elderly- What are the glucose targets? AFSHAN ZAHEDI, BASC, MD, FRCP(C) ENDOCRINOLOGY WOMEN S COLLEGE HOSPITAL ASSISTANT PROFESSOR OF MEDICINE UNIVERSITY OF TORONTO NOVEMBER 2, 2011 Disclosures
DM Management in Elderly- What are the glucose targets? AFSHAN ZAHEDI, BASC, MD, FRCP(C) ENDOCRINOLOGY WOMEN S COLLEGE HOSPITAL ASSISTANT PROFESSOR OF MEDICINE UNIVERSITY OF TORONTO NOVEMBER 2, 2011 Disclosures
Diabetes Complications
 Managing Diabetes: It s s Not Easy But It s s Worth It Presenter Disclosures W. Lee Ball, Jr., OD, FAAO (1) The following personal financial relationships with commercial interests relevant to this presentation
Managing Diabetes: It s s Not Easy But It s s Worth It Presenter Disclosures W. Lee Ball, Jr., OD, FAAO (1) The following personal financial relationships with commercial interests relevant to this presentation
Diabetes and the Kidneys
 Diabetes and the Kidneys Aim(s) and objective(s) This guideline focuses on the detection, prevention, and management of kidney disease in people with diabetes. The management of end-stage renal disease
Diabetes and the Kidneys Aim(s) and objective(s) This guideline focuses on the detection, prevention, and management of kidney disease in people with diabetes. The management of end-stage renal disease
Metabolic Syndrome Overview: Easy Living, Bitter Harvest. Sabrina Gill MD MPH FRCPC Caroline Stigant MD FRCPC BC Nephrology Days, October 2007
 Metabolic Syndrome Overview: Easy Living, Bitter Harvest Sabrina Gill MD MPH FRCPC Caroline Stigant MD FRCPC BC Nephrology Days, October 2007 Evolution of Metabolic Syndrome 1923: Kylin describes clustering
Metabolic Syndrome Overview: Easy Living, Bitter Harvest Sabrina Gill MD MPH FRCPC Caroline Stigant MD FRCPC BC Nephrology Days, October 2007 Evolution of Metabolic Syndrome 1923: Kylin describes clustering
Definition of Diabetes Mellitus
 Definition of Diabetes Mellitus Diabetes mellitus consists of a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action or both. U.S. Diabetes
Definition of Diabetes Mellitus Diabetes mellitus consists of a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action or both. U.S. Diabetes
Guideline for Microalbuminuria Screening
 East Lancashire Diabetes Network Guideline for Microalbuminuria Screening Produced by: Task and Finish Group, Clinical Standards Group Produced: August 2006 Approved by: East Lancashire Diabetes Network
East Lancashire Diabetes Network Guideline for Microalbuminuria Screening Produced by: Task and Finish Group, Clinical Standards Group Produced: August 2006 Approved by: East Lancashire Diabetes Network
DIABETES MELLITUS GUIDELINES
 DIABETES MELLITUS GUIDELINES Virginia Premier Health Plan Virginia Premier Health Plan, Clinical Practice Guideline-Diabetes 1. Population screening a. Indications i. Adults of any age with body mass index
DIABETES MELLITUS GUIDELINES Virginia Premier Health Plan Virginia Premier Health Plan, Clinical Practice Guideline-Diabetes 1. Population screening a. Indications i. Adults of any age with body mass index
Baskets of Care Diabetes Subcommittee
 Baskets of Care Diabetes Subcommittee Disclaimer: This background information is not intended to be a comprehensive scientific discussion of the topic, but rather an attempt to provide a baseline level
Baskets of Care Diabetes Subcommittee Disclaimer: This background information is not intended to be a comprehensive scientific discussion of the topic, but rather an attempt to provide a baseline level
Renal Disease in Type 2 Diabetes Mellitus
 Renal Disease in Type 2 Diabetes Mellitus 6th Collaborative DiGP/HSE/UCC Conference 25 th September 2013 Dr. Eoin O Sullivan Consultant Endocrinologist Bon Secours Hospital Cork Case 69 year old woman
Renal Disease in Type 2 Diabetes Mellitus 6th Collaborative DiGP/HSE/UCC Conference 25 th September 2013 Dr. Eoin O Sullivan Consultant Endocrinologist Bon Secours Hospital Cork Case 69 year old woman
CME Test for AMDA Clinical Practice Guideline. Diabetes Mellitus
 CME Test for AMDA Clinical Practice Guideline Diabetes Mellitus Part I: 1. Which one of the following statements about type 2 diabetes is not accurate? a. Diabetics are at increased risk of experiencing
CME Test for AMDA Clinical Practice Guideline Diabetes Mellitus Part I: 1. Which one of the following statements about type 2 diabetes is not accurate? a. Diabetics are at increased risk of experiencing
Type 2 diabetes Definition
 Type 2 diabetes Definition Type 2 diabetes is a lifelong (chronic) disease in which there are high levels of sugar (glucose) in the blood. Type 2 diabetes is the most common form of diabetes. Causes Diabetes
Type 2 diabetes Definition Type 2 diabetes is a lifelong (chronic) disease in which there are high levels of sugar (glucose) in the blood. Type 2 diabetes is the most common form of diabetes. Causes Diabetes
Cardiovascular Disease in Diabetes
 Cardiovascular Disease in Diabetes Where Do We Stand in 2012? David M. Kendall, MD Distinguished Medical Fellow Lilly Diabetes Associate Professor of Medicine University of MInnesota Disclosure - Duality
Cardiovascular Disease in Diabetes Where Do We Stand in 2012? David M. Kendall, MD Distinguished Medical Fellow Lilly Diabetes Associate Professor of Medicine University of MInnesota Disclosure - Duality
Starting Insulin Sooner Than Later
 Starting Insulin Sooner Than Later Rotorua GP Insulin Seminar 13 June 2014 Kingsley Nirmalaraj MBBS, FRACP, FACE Consultant Endocrinologist and Physician Tauranga Hospital/ Bay Endocrinology Ltd Declaration
Starting Insulin Sooner Than Later Rotorua GP Insulin Seminar 13 June 2014 Kingsley Nirmalaraj MBBS, FRACP, FACE Consultant Endocrinologist and Physician Tauranga Hospital/ Bay Endocrinology Ltd Declaration
ADULT HYPERTENSION PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
Type 2 Diabetes Mellitus and Insulin resistance syndrome in Children
 Type 2 Diabetes Mellitus and Insulin resistance syndrome in Children Anil R Kumar MD Pediatric Endocrinology MCV/VCU, Richmond VA Introduction Type 2 diabetes mellitus (T2 DM) has increased in children
Type 2 Diabetes Mellitus and Insulin resistance syndrome in Children Anil R Kumar MD Pediatric Endocrinology MCV/VCU, Richmond VA Introduction Type 2 diabetes mellitus (T2 DM) has increased in children
DR. Trinh Thi Kim Hue
 TYPE 2 DIABETES IN THE CHILD AND ADOLESCENT DR. Trinh Thi Kim Hue CONTENTS Definition Diagnosis Treatment Comorbidities and Complications Comorbidities and Complications Screening for T2D References DEFINITION
TYPE 2 DIABETES IN THE CHILD AND ADOLESCENT DR. Trinh Thi Kim Hue CONTENTS Definition Diagnosis Treatment Comorbidities and Complications Comorbidities and Complications Screening for T2D References DEFINITION
David Shu, MD, FRCPC Endocrinology, Royal Columbian Hospital October 8 th, 2010
 David Shu, MD, FRCPC Endocrinology, Royal Columbian Hospital October 8 th, 2010 Objectives At the end of the talk, the participants will be able to: 1. Identify the increasing prevalence of type 2 diabetes
David Shu, MD, FRCPC Endocrinology, Royal Columbian Hospital October 8 th, 2010 Objectives At the end of the talk, the participants will be able to: 1. Identify the increasing prevalence of type 2 diabetes
Trends in Prescribing of Drugs for Type 2 Diabetes in General Practice in England (Chart 1) Other intermediate and long-acting insulins
 Other intermediate and long-acting insulins") Type 2 Diabetes Type 2 diabetes is the most common form of diabetes, accounting for 90 95% of cases. 1 Charts 1 and 2 reflect the effect of increasing prevalence on prescribing and costs of products used
Type 2 Diabetes Type 2 diabetes is the most common form of diabetes, accounting for 90 95% of cases. 1 Charts 1 and 2 reflect the effect of increasing prevalence on prescribing and costs of products used
Diabetes Mellitus 1. Chapter 43. Diabetes Mellitus, Self-Assessment Questions
 Diabetes Mellitus 1 Chapter 43. Diabetes Mellitus, Self-Assessment Questions 1. A 46-year-old man presents for his annual physical. He states that he has been going to the bathroom more frequently than
Diabetes Mellitus 1 Chapter 43. Diabetes Mellitus, Self-Assessment Questions 1. A 46-year-old man presents for his annual physical. He states that he has been going to the bathroom more frequently than
Updates for your practice March, 2013. Vol 2, Issue 14 TLALELETSO. Managing Complicated Diabetes
 dates for your practice March, 2013. Vol 2, Issue 14 TLALELETSO Managing Complicated Diabetes Diabetes is increasingly common Managing diabetes and working as part of a multidisciplinary team is essential
dates for your practice March, 2013. Vol 2, Issue 14 TLALELETSO Managing Complicated Diabetes Diabetes is increasingly common Managing diabetes and working as part of a multidisciplinary team is essential
Comparing Medications for Adults With Type 2 Diabetes Focus of Research for Clinicians
 Clinician Research Summary Diabetes Type 2 Diabetes Comparing Medications for Adults With Type 2 Diabetes Focus of Research for Clinicians A systematic review of 166 clinical studies published between
Clinician Research Summary Diabetes Type 2 Diabetes Comparing Medications for Adults With Type 2 Diabetes Focus of Research for Clinicians A systematic review of 166 clinical studies published between
Secondary Stroke Prevention Luke Bradbury, MD 10/4/14 Fall WAPA Conferfence
 Guidelines Secondary Stroke Prevention Luke Bradbury, MD 10/4/14 Fall WAPA Conferfence Stroke/TIA Nearly 700,000 ischemic strokes and 240,000 TIAs every year in the United States Currently, the risk for
Guidelines Secondary Stroke Prevention Luke Bradbury, MD 10/4/14 Fall WAPA Conferfence Stroke/TIA Nearly 700,000 ischemic strokes and 240,000 TIAs every year in the United States Currently, the risk for
CHAPTER V DISCUSSION. normal life provided they keep their diabetes under control. Life style modifications
 CHAPTER V DISCUSSION Background Diabetes mellitus is a chronic condition but people with diabetes can lead a normal life provided they keep their diabetes under control. Life style modifications (LSM)
CHAPTER V DISCUSSION Background Diabetes mellitus is a chronic condition but people with diabetes can lead a normal life provided they keep their diabetes under control. Life style modifications (LSM)
Absolute cardiovascular disease risk
 Guidelines for the management of Absolute cardiovascular disease risk An initiative of the National Vascular Disease Prevention Alliance About the National Vascular Disease Prevention Alliance The National
Guidelines for the management of Absolute cardiovascular disease risk An initiative of the National Vascular Disease Prevention Alliance About the National Vascular Disease Prevention Alliance The National
Diabetes is a. A case for prevention of type 2 diabetes mellitus
 A case for prevention of type 2 diabetes mellitus Joseph Cook, DO Diabetes is a disease that has reached epidemic proportions in the United States and around the world. This is troubling because, as bad
A case for prevention of type 2 diabetes mellitus Joseph Cook, DO Diabetes is a disease that has reached epidemic proportions in the United States and around the world. This is troubling because, as bad
HIGH BLOOD PRESSURE AND YOUR KIDNEYS
 HIGH BLOOD PRESSURE AND YOUR KIDNEYS www.kidney.org About the Information in this Booklet Did you know that the National Kidney (NKF) Foundation offers guidelines and commentaries that help your healthcare
HIGH BLOOD PRESSURE AND YOUR KIDNEYS www.kidney.org About the Information in this Booklet Did you know that the National Kidney (NKF) Foundation offers guidelines and commentaries that help your healthcare
Absolute cardiovascular disease risk management
 Quick reference guide for health professionals Absolute cardiovascular disease risk management This quick reference guide is for use by health professionals for primary prevention of cardiovascular disease
Quick reference guide for health professionals Absolute cardiovascular disease risk management This quick reference guide is for use by health professionals for primary prevention of cardiovascular disease
HYPERTENSION ASSOCIATED WITH RENAL DISEASES
 RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
Chronic Kidney Disease (CKD) Algorithm. Chronic Kidney Disease (CKD) Algorithm Page 1
 Algorithm. Chronic Kidney Disease (CKD) Algorithm Page 1") Chronic Kidney Disease (CKD) Algorithm Chronic Kidney Disease (CKD) Algorithm Page 1 Chronic Kidney Disease (CKD) Algorithm (See NICE Clinical Guideline CG73 1 and Quality Standards 2 ) Who should have
Chronic Kidney Disease (CKD) Algorithm Chronic Kidney Disease (CKD) Algorithm Page 1 Chronic Kidney Disease (CKD) Algorithm (See NICE Clinical Guideline CG73 1 and Quality Standards 2 ) Who should have
Managing Patients Newly Diagnosed with Diabetes. Sud Dharmalingam MD, FRCPC Staff Endocrinologist William Osler Health System Brampton, ON
 Managing Patients Newly Diagnosed with Diabetes Sud Dharmalingam MD, FRCPC Staff Endocrinologist William Osler Health System Brampton, ON 1 Conflict Disclosure Information Conflict Disclosure Information
Managing Patients Newly Diagnosed with Diabetes Sud Dharmalingam MD, FRCPC Staff Endocrinologist William Osler Health System Brampton, ON 1 Conflict Disclosure Information Conflict Disclosure Information
Initiate Atorvastatin 20mg daily
 Type 2 Diabetes Patient Objectives Stopping Smoking BMI > 25 kg m² Control BP to
Type 2 Diabetes Patient Objectives Stopping Smoking BMI > 25 kg m² Control BP to
Hypertension Guideline V4
 Hypertension Guideline V4 Approved 24/06/2008 Version VERSION 4 FINAL Date of First Issue 26/02/08 Review Date 01/03/2010 Date of Issue 24/06/2008 EQIA Yes / No 24/06/2008 Author / Contact Dr Leslie Cruickshank
Hypertension Guideline V4 Approved 24/06/2008 Version VERSION 4 FINAL Date of First Issue 26/02/08 Review Date 01/03/2010 Date of Issue 24/06/2008 EQIA Yes / No 24/06/2008 Author / Contact Dr Leslie Cruickshank
Nutrition Therapy in Diabetes Mellitus. Dorothy Debrah Diabetes Specialist Dietitian University Hospital, Llandough. Wales, UK February 2012
 Nutrition Therapy in Diabetes Mellitus. Dorothy Debrah Diabetes Specialist Dietitian University Hospital, Llandough. Wales, UK February 2012 University Hospital Llandough DIABETES MELLITUS. Definition:
Nutrition Therapy in Diabetes Mellitus. Dorothy Debrah Diabetes Specialist Dietitian University Hospital, Llandough. Wales, UK February 2012 University Hospital Llandough DIABETES MELLITUS. Definition:
A Simplified Approach to Initiating Insulin. 4. Not meeting glycemic goals with oral hypoglycemic agents or
 A Simplified Approach to Initiating Insulin When to Start Insulin: 1. Fasting plasma glucose (FPG) levels >250 mg/dl or 2. Glycated hemoglobin (A1C) >10% or 3. Random plasma glucose consistently >300 mg/dl
A Simplified Approach to Initiating Insulin When to Start Insulin: 1. Fasting plasma glucose (FPG) levels >250 mg/dl or 2. Glycated hemoglobin (A1C) >10% or 3. Random plasma glucose consistently >300 mg/dl
PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION
 Hull & East Riding Prescribing Committee PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION For guidance on Primary Prevention please see NICE guidance http://www.nice.org.uk/guidance/cg181
Hull & East Riding Prescribing Committee PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION For guidance on Primary Prevention please see NICE guidance http://www.nice.org.uk/guidance/cg181
Absolute cardiovascular disease risk assessment
 Quick reference guide for health professionals Absolute cardiovascular disease risk assessment This quick reference guide is a summary of the key steps involved in assessing absolute cardiovascular risk
Quick reference guide for health professionals Absolute cardiovascular disease risk assessment This quick reference guide is a summary of the key steps involved in assessing absolute cardiovascular risk
Chronic Kidney Disease and the Electronic Health Record. Duaine Murphree, MD Sarah M. Thelen, MD
 Chronic Kidney Disease and the Electronic Health Record Duaine Murphree, MD Sarah M. Thelen, MD Definition of Chronic Kidney Disease (CKD) Defined by the National Kidney Foundation Either a decline in
Chronic Kidney Disease and the Electronic Health Record Duaine Murphree, MD Sarah M. Thelen, MD Definition of Chronic Kidney Disease (CKD) Defined by the National Kidney Foundation Either a decline in
DIABETES MELLITUS TYPE 2 PROTOCOL CELLO
 DIABETES MELLITUS TYPE 2 PROTOCOL CELLO Leiden November 2010 Mw. M. van Mierlo, practice nurse Mw. C. Gieskes, diabetes nurse 1 Contents Introduction 1. Way of working at CELLO for patients with Diabetes
DIABETES MELLITUS TYPE 2 PROTOCOL CELLO Leiden November 2010 Mw. M. van Mierlo, practice nurse Mw. C. Gieskes, diabetes nurse 1 Contents Introduction 1. Way of working at CELLO for patients with Diabetes
High Blood pressure and chronic kidney disease
 High Blood pressure and chronic kidney disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
High Blood pressure and chronic kidney disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
Technology Assessment
 Technology Assessment Lifestyle Interventions for Four Conditions: Type 2 Diabetes, Metabolic Syndrome, Breast Cancer, and Prostate Cancer Technology Assessment Program Prepared for: Agency for Healthcare
Technology Assessment Lifestyle Interventions for Four Conditions: Type 2 Diabetes, Metabolic Syndrome, Breast Cancer, and Prostate Cancer Technology Assessment Program Prepared for: Agency for Healthcare
ASN DIALYSIS ADVISORY GROUP ASN DIALYSIS CURRICULUM
 ASN DIALYSIS ADVISORY GROUP ASN DIALYSIS CURRICULUM Management of Traditional Cardiovascular Risk Factors in ESRD (Hypertension, Dyslipidemia, Glycemic Control) ROBERT D. TOTO, M.D. PROFESSOR OF MEDICINE
ASN DIALYSIS ADVISORY GROUP ASN DIALYSIS CURRICULUM Management of Traditional Cardiovascular Risk Factors in ESRD (Hypertension, Dyslipidemia, Glycemic Control) ROBERT D. TOTO, M.D. PROFESSOR OF MEDICINE
DRUG UTILIZATION EVALUATION OF ANTIHYPERTENSIVE DRUGS IN DIABETIC PATIENTS WITH CKD
 WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES Elhami et al. SJIF Impact Factor 5.210 Volume 4, Issue 11, 1159-1166 Research Article ISSN 2278 4357 DRUG UTILIZATION EVALUATION OF ANTIHYPERTENSIVE
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES Elhami et al. SJIF Impact Factor 5.210 Volume 4, Issue 11, 1159-1166 Research Article ISSN 2278 4357 DRUG UTILIZATION EVALUATION OF ANTIHYPERTENSIVE
Treating Type 2 Diabetes Mellitus: a New York State Medicaid Clinical Guidance Document
 Treating Type 2 Diabetes Mellitus: a New York State Medicaid Clinical Guidance Document Disclaimer: This document is offered as a service to New York State Prescribers to inform about the most current
Treating Type 2 Diabetes Mellitus: a New York State Medicaid Clinical Guidance Document Disclaimer: This document is offered as a service to New York State Prescribers to inform about the most current
Gayle Curto, RN, BSN, CDE Clinical Coordinator
 Gayle Curto, RN, BSN, CDE Clinical Coordinator INTRODUCTION Historical Program Overview Leadership Team Mission Statement Diabetes Center Demographics for 2011 Older Adult Population HISTORICAL PROGRAM
Gayle Curto, RN, BSN, CDE Clinical Coordinator INTRODUCTION Historical Program Overview Leadership Team Mission Statement Diabetes Center Demographics for 2011 Older Adult Population HISTORICAL PROGRAM
Treatment of Type 2 Diabetes
 Improving Patient Care through Evidence Treatment of Type 2 Diabetes This information is based on a comprehensive review of the evidence for best practices in the treatment of type 2 diabetes and is sponsored
Improving Patient Care through Evidence Treatment of Type 2 Diabetes This information is based on a comprehensive review of the evidence for best practices in the treatment of type 2 diabetes and is sponsored
DISCLOSURES RISK ASSESSMENT. Stroke and Heart Disease -Is there a Link Beyond Risk Factors? Daniel Lackland, MD
 STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
Type 2 Diabetes workshop notes
 Group 1 notes Abi / Nicole Type 2 Diabetes workshop notes 4.1 Population The group discussed the following sub groups that may need addressing: Men-as they tend to die earlier compared with women, their
Group 1 notes Abi / Nicole Type 2 Diabetes workshop notes 4.1 Population The group discussed the following sub groups that may need addressing: Men-as they tend to die earlier compared with women, their
Diabetes and Your Kidneys
 American Kidney Fund reaching out giving hope improving lives Diabetes and Your Kidneys reaching out giving hope improving lives Diabetes: The #1 Cause of Kidney Failure Your doctor told you that you have
American Kidney Fund reaching out giving hope improving lives Diabetes and Your Kidneys reaching out giving hope improving lives Diabetes: The #1 Cause of Kidney Failure Your doctor told you that you have
High Blood Pressure and Your Kidneys
 High Blood Pressure and Your Kidneys About 65 million Americans have high blood pressure, but as many as one third or three in 10 don't even know it. There are usually no signs or symptoms that your blood
High Blood Pressure and Your Kidneys About 65 million Americans have high blood pressure, but as many as one third or three in 10 don't even know it. There are usually no signs or symptoms that your blood
DCCT and EDIC: The Diabetes Control and Complications Trial and Follow-up Study
 DCCT and EDIC: The Diabetes Control and Complications Trial and Follow-up Study National Diabetes Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What
DCCT and EDIC: The Diabetes Control and Complications Trial and Follow-up Study National Diabetes Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What
Hypertension Guidelines
 Overview Hypertension Guidelines Aim to reduce Blood Pressure to 140/90 or less (140/80 for diabetics), adding drugs as needed until further treatment is inappropriate or declined. N.B. patients do not
Overview Hypertension Guidelines Aim to reduce Blood Pressure to 140/90 or less (140/80 for diabetics), adding drugs as needed until further treatment is inappropriate or declined. N.B. patients do not
High Blood Pressure and Kidney Disease
 High Blood Pressure and Kidney Disease National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH The kidneys play a key
High Blood Pressure and Kidney Disease National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH The kidneys play a key
Pharmacy and the Medicaid Accountable Care Organization
 RCCO Pilot Project CDC Grant Increase engagement of non-physician team members (ie., pharmacists) in Hypertension (HTN) and Diabetes Mellitus (DM) management in health care systems; Increase the proportion
RCCO Pilot Project CDC Grant Increase engagement of non-physician team members (ie., pharmacists) in Hypertension (HTN) and Diabetes Mellitus (DM) management in health care systems; Increase the proportion
Drug Treatment in Type 2 Diabetes with Hypertension
 Hypertension is 1.5 2 times more prevalent in Type 2 diabetes (prevalence up to 80 % in diabetic subjects). This exacerbates the risk of cardiovascular disease by ~ two-fold. Drug therapy reduces the risk
Hypertension is 1.5 2 times more prevalent in Type 2 diabetes (prevalence up to 80 % in diabetic subjects). This exacerbates the risk of cardiovascular disease by ~ two-fold. Drug therapy reduces the risk
Add: 2 nd generation sulfonylurea or glinide or Add DPP-4 inhibitor Start or intensify insulin therapy if HbA1c goals not achieved with the above
 Guidelines for Type Diabetes - Diagnosis Fasting Plasma Glucose (confirm results if borderline) HbAIC Normal FPG < 00 < 5.5 Impaired Fasting Glucose (IFG) 00 to < 5.7%-.5% Diabetes Mellitus (or random
Guidelines for Type Diabetes - Diagnosis Fasting Plasma Glucose (confirm results if borderline) HbAIC Normal FPG < 00 < 5.5 Impaired Fasting Glucose (IFG) 00 to < 5.7%-.5% Diabetes Mellitus (or random
Diabetes in Primary Care course MCQ Answers 2016
 Diabetes in Primary Care course MCQ Answers 2016 Diagnosis of Diabetes HbA1C should not be used as a diagnostic tool in the following situations: (answer each TRUE or FALSE) 1. Gestational Diabetes TRUE
Diabetes in Primary Care course MCQ Answers 2016 Diagnosis of Diabetes HbA1C should not be used as a diagnostic tool in the following situations: (answer each TRUE or FALSE) 1. Gestational Diabetes TRUE
EFFIMET 1000 XR Metformin Hydrochloride extended release tablet
 BRAND NAME: Effimet XR. THERAPEUTIC CATEGORY: Anti-Diabetic PHARMACOLOGIC CLASS: Biguanides EFFIMET 1000 XR Metformin Hydrochloride extended release tablet COMPOSITION AND PRESENTATION Composition Each
BRAND NAME: Effimet XR. THERAPEUTIC CATEGORY: Anti-Diabetic PHARMACOLOGIC CLASS: Biguanides EFFIMET 1000 XR Metformin Hydrochloride extended release tablet COMPOSITION AND PRESENTATION Composition Each
High Blood Pressure and Chronic Kidney Disease. For People With CKD Stages 1 4
 High Blood Pressure and Chronic Kidney Disease For People With CKD Stages 1 4 National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation s Kidney
High Blood Pressure and Chronic Kidney Disease For People With CKD Stages 1 4 National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation s Kidney
TYPE 2 DIABETES IN CHILDREN DIAGNOSIS AND THERAPY. Ines Guttmann- Bauman MD Clinical Associate Professor, Division of Pediatric Endocrinology, OHSU
 TYPE 2 DIABETES IN CHILDREN DIAGNOSIS AND THERAPY Ines Guttmann- Bauman MD Clinical Associate Professor, Division of Pediatric Endocrinology, OHSU Objectives: 1. To discuss epidemiology and presentation
TYPE 2 DIABETES IN CHILDREN DIAGNOSIS AND THERAPY Ines Guttmann- Bauman MD Clinical Associate Professor, Division of Pediatric Endocrinology, OHSU Objectives: 1. To discuss epidemiology and presentation
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates. January 30, 2014
 JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused by too little insulin, resistance to insulin, or both.
 Diabetes Definition Diabetes is a chronic (lifelong) disease marked by high levels of sugar in the blood. Causes Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused
Diabetes Definition Diabetes is a chronic (lifelong) disease marked by high levels of sugar in the blood. Causes Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused
Strengthening the Pharmacist Skills in Managing Diabetes Practice Based Program 27 Contact Hours
 Strengthening the Pharmacist Skills in Managing Diabetes Practice Based Program 27 Contact Hours Presented by New York State Council of Health system Pharmacists October 18 19, 2013 St. John s University,
Strengthening the Pharmacist Skills in Managing Diabetes Practice Based Program 27 Contact Hours Presented by New York State Council of Health system Pharmacists October 18 19, 2013 St. John s University,
New in Diabetes. Diabetes is becoming more common. By the. What s. Presented at McMaster University, Hamilton, Ontario, October 2001.
 Focus on CME at McMaster University What s New in Diabetes By Sarah Capes, MD, FRCPC Presented at McMaster University, Hamilton, Ontario, October 2001. Diabetes is becoming more common. By the year 2025,
Focus on CME at McMaster University What s New in Diabetes By Sarah Capes, MD, FRCPC Presented at McMaster University, Hamilton, Ontario, October 2001. Diabetes is becoming more common. By the year 2025,
Overview and update of modern type 2 Diabetes philosophy and management. Dr Steve Stanaway Consultant Endocrinologist BCU
 Overview and update of modern type 2 Diabetes philosophy and management Dr Steve Stanaway Consultant Endocrinologist BCU Diabetes economics 2009: 2.6M adults with DM in UK (90% type 2) 2025: est. > 4M
Overview and update of modern type 2 Diabetes philosophy and management Dr Steve Stanaway Consultant Endocrinologist BCU Diabetes economics 2009: 2.6M adults with DM in UK (90% type 2) 2025: est. > 4M
AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM
 AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM 2013 TASK FORCE Alan J. Garber, MD, PhD, FACE, Chair Martin J. Abrahamson, MD Joshua I. Barzilay, MD, FACE Lawrence Blonde, MD, FACP, FACE Zachary T. Bloomgarden,
AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM 2013 TASK FORCE Alan J. Garber, MD, PhD, FACE, Chair Martin J. Abrahamson, MD Joshua I. Barzilay, MD, FACE Lawrence Blonde, MD, FACP, FACE Zachary T. Bloomgarden,
Treatment Issues of Diabetes, Hypertension, and Lipids in the Elderly Patient
 Treatment Issues of Diabetes, Hypertension, and Lipids in the Elderly Patient 17 th Primary Care Conference March 26, 2013 L. Brian Cross, PharmD, BCACP, CDE Chad K. Gentry, PharmD, BCACP, CDE Objectives
Treatment Issues of Diabetes, Hypertension, and Lipids in the Elderly Patient 17 th Primary Care Conference March 26, 2013 L. Brian Cross, PharmD, BCACP, CDE Chad K. Gentry, PharmD, BCACP, CDE Objectives
Britni Hebert, MD PGY-1
 Britni Hebert, MD PGY-1 Importance of Diabetes treatment Types of treatment Comparison of treatment/article Review Summary Example cases 1 out of 13 Americans have diabetes Complications include blindness,
Britni Hebert, MD PGY-1 Importance of Diabetes treatment Types of treatment Comparison of treatment/article Review Summary Example cases 1 out of 13 Americans have diabetes Complications include blindness,
MEDICATION THERAPY ADHERENCE CLINIC : DIABETES
 MEDICATION THERAPY ADHERENCE CLINIC : DIABETES PHARMACEUTICAL SERVICES DIVISION MINISTRY OF HEALTH MALAYSIA First Edition, 2010 Pharmaceutical Services Division Ministry of Health, Malaysia ALL RIGHT RESERVED
MEDICATION THERAPY ADHERENCE CLINIC : DIABETES PHARMACEUTICAL SERVICES DIVISION MINISTRY OF HEALTH MALAYSIA First Edition, 2010 Pharmaceutical Services Division Ministry of Health, Malaysia ALL RIGHT RESERVED
Use of Glycated Hemoglobin and Microalbuminuria in the Monitoring of Diabetes Mellitus
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Number 84 Use of Glycated Hemoglobin and Microalbuminuria in the Monitoring of Diabetes Mellitus Summary Overview Clinical
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Number 84 Use of Glycated Hemoglobin and Microalbuminuria in the Monitoring of Diabetes Mellitus Summary Overview Clinical
Management of Diabetes: A Primary Care Perspective. Presentation Outline
 Management of Diabetes: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Presentation Outline
Management of Diabetes: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Presentation Outline
Diabetes, Type 2. RelayClinical Patient Education Sample Topic Diabetes, Type 2. What is type 2 diabetes? How does it occur?
 What is type 2 diabetes? Type 2 diabetes is a disorder that happens when your body does not make enough insulin or is unable to use its own insulin properly. The inability to use insulin is called insulin
What is type 2 diabetes? Type 2 diabetes is a disorder that happens when your body does not make enough insulin or is unable to use its own insulin properly. The inability to use insulin is called insulin
AACE/ACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM
 ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been accepted for publication in an issue of Endocrine Practice. This version
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been accepted for publication in an issue of Endocrine Practice. This version
Causes, incidence, and risk factors
 Causes, incidence, and risk factors Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused by too little insulin, resistance to insulin, or both. To understand diabetes,
Causes, incidence, and risk factors Insulin is a hormone produced by the pancreas to control blood sugar. Diabetes can be caused by too little insulin, resistance to insulin, or both. To understand diabetes,
Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results
 Principal Results") Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results Paul K. Whelton, MB, MD, MSc Chair, SPRINT Steering Committee Tulane University School of Public Health and Tropical Medicine, and
Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results Paul K. Whelton, MB, MD, MSc Chair, SPRINT Steering Committee Tulane University School of Public Health and Tropical Medicine, and
Mary Bruskewitz APN, MS, RN, BC-ADM Clinical Nurse Specialist Diabetes
 Mary Bruskewitz APN, MS, RN, BC-ADM Clinical Nurse Specialist Diabetes Objectives Pathophysiology of Diabetes Acute & Chronic Complications Managing acute emergencies Case examples 11/24/2014 UWHealth
Mary Bruskewitz APN, MS, RN, BC-ADM Clinical Nurse Specialist Diabetes Objectives Pathophysiology of Diabetes Acute & Chronic Complications Managing acute emergencies Case examples 11/24/2014 UWHealth
Microalbuminuria: We are in the midst of an epidemic: the epidemic. So What s a Little Protein? Malcolm s diabetes. How much is too much?
 Focus on CME at the University of Saskatchewan Microalbuminuria: So What s a Little Protein? By Judith T. Klassen, BSc, MD, FRCPC University of Saskatchewan Practical Management of Common Medical Problems
Focus on CME at the University of Saskatchewan Microalbuminuria: So What s a Little Protein? By Judith T. Klassen, BSc, MD, FRCPC University of Saskatchewan Practical Management of Common Medical Problems
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Cardiovascular disease physiology. Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011
 Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
New Non-Insulin Therapies for Type 2 Diabetes Mellitus
 New Non-Insulin Therapies for Type 2 Diabetes Mellitus Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Disclosure Relationships
New Non-Insulin Therapies for Type 2 Diabetes Mellitus Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Disclosure Relationships
Nutrition. Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT
 1 Nutrition Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT 2 Type 2 Diabetes: A Growing Challenge in the Healthcare Setting Introduction and background of type 2 diabetes:
1 Nutrition Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT 2 Type 2 Diabetes: A Growing Challenge in the Healthcare Setting Introduction and background of type 2 diabetes: