1. Introduction. Correspondence should be addressed to Waclaw Kuczmik;
|
|
|
- Diana Gaines
- 7 years ago
- Views:
Transcription
1 BioMed Research International, Article ID , 6 pages Research Article Tension-Free Vaginal Tape, Transobturator Tape, and Own Modification of Transobturator Tape in the Treatment of Female Stress Urinary Incontinence: Comparative Analysis Marcin Zyczkowski, 1 Krzysztof Nowakowski, 1 Waclaw Kuczmik, 2 Tomasz Urbanek, 2 Zbiegniew Kaletka, 1 Piotr Bryniarski, 1 Bartosz Muskala, 1 and Andrzej Paradysz 1 1 Department and Clinic of Urology, Medical University of Silesia, Katowice, Poland 2 DepartmentandClinicofGeneralandVascularSurgery,MedicalUniversityofSilesia,Katowice,Poland Correspondence should be addressed to Waclaw Kuczmik; wkuczmik@interia.pl Received 3 January 2014; Accepted 7 February 2014; Published 16 March 2014 Academic Editor: Jakub Taradaj Copyright 2014 Marcin Zyczkowski et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Introduction. This study is a comparative evaluation of the TVT, TOT, and our own modification of TOT (mtot) in the treatment of female stress urinary incontinence from a single center experience. Material and Methods. The study was conducted on 527 patients with SUI diagnosed on the basis of urodynamic studies. They were divided into three groups TVT: n = 142, (TOT): n = 129,andmTOT:n = 256. All of the patients underwent evaluation at 1, 3, and 6 months after surgery. Results were statistically analysed and compared. Results. Objective and subjective effectiveness after the surgery were not significantly different in the study groups and ranged from 90.1% to 96.4%. Mean surgery time was 32.3, 28.2, and 26.4 in the TVT, TOT, and mtot, respectively. Mean hospitalization time was 2.51 days. Mean catheter maintenance time was significantly higher in the TVT than in other groups. In the TVT group total incidence of complications was 13.4%, and it was significantly higher than that in TOT and mtot (9.3% and 8.6%, resp.). Conclusions. TVT, TOT, and mtot are highly effective and safe methods in the treatment of SUI. There are no differences in the efficacy between the methods with a little higher percentage of complications in the TVT group. 1. Introduction Stress urinary incontinence (SUI) in women is a widespread disease all over the world. It causes many psychosocial problems and generates significant costs to the budget of health in many countries. In 1993 DeLancey as one of the first researchers concluded that its pathophysiology is associated with a defect in bladder neck and urethra due to the laxity of surrounding tissues and the insufficiency of the internal sphincter of urethra [1]. Various factors may affect the development of SUI. The most well known are vaginal births, overweight and obesity, hormonal disorders, andmuscleweaknessofpelvicdiaphragm.firstchoiceof the treatment for SUI is conservative treatment, whose main elements are lifestyle modifications (physical activity, dietary habits, and weight loss), bladder control exercises, and pelvic floor muscle training (PFMT). In the absence of effects in the conservative treatment including medications and physiotherapy, surgical treatment is necessary. In addition to open techniques such as Burch colposuspension, currently themostoftenusedareminimallyinvasivemethods.their aim is the suspension of the bladder neck and urethra using syntheticmaterials,theso-calledsling.abnormalpositioning of the urethra and the bladder neck implied the possibility of introducing the method of correcting this condition and in 1996 Ulmsten and colleagues have published the report describing the TVT (tension-free vaginal tape) technique in thetreatmentofsui[2]. A few years later, TOT (transobturator tape) method was described in which the tape is carried out between the obturator holes [3]. Both methods are now widely accepted methods of surgical treatment of SUI. The transobturator variant, however, has become more popular nowadays due to similar cure rate with relatively less complications.

, and own modification of TOT (mtot). Study is based on over 10 years of experience from a single center. 3.")

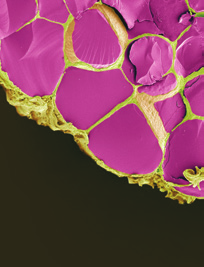
2 2 BioMed Research International Figure 1: Polypropylene mesh used to prepare TOT tape. Figure 2: Close-up of polypropylene mesh shown in Figure Aim of the Study The aim of the study is to evaluate the comparative results of surgical management of the stress urinary incontinence in women using tension-free vaginal tape (TVT), tension-free transobturator tape (TOT), and own modification of TOT (mtot). Study is based on over 10 years of experience from a single center. 3. Materials and Methods In the years in Department of Urology in Zabrze, 527 women with SUI were treated using midurethral slings. The age of patients ranged between 45 and 64 years, mean 55.1 years. All patients before treatment were carefully examined and the diagnosis of SUI and qualification for surgical treatment were established on the basis of physical examination, urinalysis and urine culture, abdominal ultrasound, and urodynamic studies in the form of pressureflow study. 456 patients (86.5%) had pure form of stress urinary incontinence. The remaining 71 (13.5%) presented mixed urinary incontinence (MUI) with urge incontinence component. The treatment option was chosen for the patients according to the routine method used in department at the time when the patients were admitted and treated. Patients were divided into three study groups depending on the type of surgical procedure (Table 1). Group I accounted for 142 patients (26.9%) operated with classical TVT technique. They were treated in the years Group II consisted of 129 patients (24.5%) who have undergone TOT procedure in the years , using original sets dedicated to this type of treatment. Group III included 256 women (48.6%) who underwent TOT in the years with our own modification. In that group instead of the original tape dedicated to TOT, self-prepared tape from a polypropylene mesh destinated for abdominal hernias repair was used. It was prepared just before the procedure by the operator from Dallop PP TDM KTM mesh (Figures 1, 2, and 3). All TOT procedures were performed using Stamey needle. The procedures were performed by three different operators with similar experience in the surgical treatment of stress urinary incontinence. Most procedures were carried out under spinal anesthesia (502, 95.3%) and the other in a short general anesthesia due to anaesthesiological indications. Woman Figure 3: Tape prepared for the mtot procedure with Stamey needle. with MUI after surgery were subjected to pharmacological treatment with antimuscarinic drugs. Postoperative evaluation was performed after one, three months, and then every 6 months after surgery. The subjective cure rate was evaluated by patients satisfaction with surgery interpreted as a patient-reported success rate. Patients answered a short questionnaire consisting of three possible answers: (a) I m very satisfied with treatment results, (b) I m rather satisfied with treatment results, and (c) I m not satisfied with treatment results. Answers (a) and (b) were interpreted as patients related success. Objective cure rate was evaluated on the basis of cough test and one-hour pad test. Completely dry pad after 1 hour of normal day activity was interpreted as a negative result. During the follow-up all of the patients underwent also physical examination, urinalysis, and ultrasound evaluation of postvoiding residual volume. Duration of followup was months. All data were statistically analysed with Kolmogorov-Smirnov test. For analysis of continuous variables without normal distribution nonparametric 𝑈Mann-Whitney test was used. For analysis of categorical variables 𝜒2 was used. Statistical examination was conducted with the aid of Statistica Statsoft v 9.0. 𝑃 values <0.05 were considered as statistically significant. 4. Results First evaluation of the cure rates was obtained in 1 month after surgery (Table 2). Objective (cough test and 1-hour pad
3 BioMed Research International 3 Table 1: Comparison of the study groups. Number of patients 142 (26,9%) 129 (24,5%) 256 (48,6%) Age 55,2 ± 8,3 54,7 ± 7,8 55,9 ± 8,6 0,115 Complications 19 (13,4%) 12 (9,3%) 22 (8,6%) 0,04 Operation time (min) 32,3 28,2 26,4 0,33 Hospitalization time 2,54 2,48 2,50 0,76 Catheter maintenance 1,84 1,58 1,52 0,04 Table 2: Cure rates in 1 month after surgery. Cough test negative 128 (90,1%) 118 (91,5%) 236 (92,2%) 0,09 Pad test negative 133 (93,7%) 122 (94,6%) 241 (94,1%) 0,88 Satisfied with surgery 135 (95,1%) 123 (95,3%) 244 (95,3%) 0,91 Table 3: Cure rates in 3 months after surgery. Cough test negative 129 (90,8%) 120 (93,0%) 238 (92,9%) 0,07 Pad test negative 133 (93,7%) 121 (93,8%) 241 (94,1%) 0,95 Satisfied with surgery 137 (96,4%) 123 (95,3%) 246 (96,1%) 0,88 Table 4: Cure rates in 6 months after surgery. Cough test negative 130 (91,5%) 120 (93,0%) 239 (93,3%) 0,08 Pad test negative 134 (94,4%) 120 (93,0%) 243 (94,9%) 0,12 Satisfied with surgery 137 (96,4%) 124 (96,1%) 247 (96,4%) 0,98 test) and subjective (patient s satisfaction) cure rates were analysed. There were no statistically significant differences in the efficacy of the surgery between the study groups. Dependingonthecurecriteria,efficacyrangedfrom90.1% to 95.3%, with the highest values in the patients satisfaction. Three months after surgery second evaluation was performed (Table 3). Both subjective and objective cure rates were a little higher than 2 months earlier and ranged from 90.8% to 96.4%. No significant differences between the study groups were observed. Last evaluation of the efficacy was performed 6 months after surgery and it contained the same methods as earlier (Table 4). Subjective and objective cure rates ranged from 91.5% to 96.4% without any differences between the study groups. Surgery time ranged from 20 to 42 minutes, with means 32.3, 28.2, and 26.4 in the TVT, TOT, and mtot, respectively. There were no statistical differences between the study groups. Hospitalization time ranged from 2 to 5 days, mean 2.51 days with no significant differences between the groups. Mean catheter maintenance time in the Group I (TVT) was 1.84 days and it was significantly higher than in TOT and mtot groups (1.58 and 1.52, resp.). It occurred probably due to higher percentage of bladder injuries in the TVT group. There were no significant intraoperative and postoperative complications observed in the study groups that required reoperation. Bladder injury, de novo OAB (overactive bladder symptoms), postvoiding residual urine >100 ml, and tape extrusion were analysed as intra- and postoperative complications (Table 5). In the TVT group total incidence of complications was 13.4%, and it was significantly higher than that in TOT and mtot (9.3% and 8.6%, resp.). The analysis of individual complications showed that the only statistical difference was observed in the frequency of bladder injuries during the surgery and it was highest in the TVT group (4.2%);itoccurredonlyinfewcasesinTOTandmTOT (0.7%both).DenovoOABoccurredin %without differences between the groups and was treated pharmacologically after the surgery. Postvoiding residual urine above 100 ml was discovered in the abdominal ultrasound during follow-up in %. Tape extrusion was discovered in 5 casesinthewholestudygroupwithoutstatisticalsignificance between the groups. Analysis between TVT and TOT in total (both TOT and mtot) was also performed in the 6th month after surgery (Table 6). It showed no statistical difference between TVT andtotintotalinbothsubjectiveandobjectivecurerates but it proved higher percentage of complications in the TVT group with statistical significance. Comparison between TOT and mtot was also made in the 6th month after the treatment (Table 7). It revealed no differences in cure rates and complications between
4 4 BioMed Research International Table 5: Complications. Bladder injury 6 (4,2%) 1 (0,7%) 2 (0,7%) 0,01 De novo OAB 5 (3,5%) 6 (4,7%) 11 (4,3%) 0,15 Postvoid residual 7 (4,9%) 3 (2,3%) 7 (2,7%) 0,09 Tape extrusion 1 (0,7%) 2 (1,6%) 2 (0,7%) 0,22 Table 6: Comparison between TVT and overall TOT in 6 months after surgery. TVT (n = 142) OverallTOT(n = 385) P value Cough test negative 130 (91,5%) 359 (93,2%) 0,07 Pad test negative 134 (94,4%) 363 (94,3%) 0,98 Satisfied with surgery 137 (96,4%) 371 (96,4%) 0,99 Complications 19 (13,4%) 34 (8,8%) 0,01 Table 7: Comparison between TOT and TOT with our own modification (mtot). TOT (n = 129) mtot(n = 256) P value Cough test negative 120 (93,0%) 239 (93,3%) 0,09 Pad test negative 120 (93,0%) 243 (94,9%) 0,88 Satisfied with surgery 124 (96,1%) 247 (96,4%) 0,08 Complications 12 (9,3%) 22 (8,6%) 0,07 females operated with classic TOT and TOT with our own modification described above. 5. Discussion World literature reports that TOT has now become a bit more popular, mainly due to the similar efficacy and a slightly lower rate of complications [4, 5]. Published studies show about 80 85% success rate in the efficacy of the TVT method [6, 7]. The most frequently reported complications of this method are bladder perforation, bleeding disorders, and de novo micturition urgency [8]. Published efficacy of the TOT technique is similar, with a slightly lower percentage of complications [9, 10]. Due to the preferences of centers performing such procedures and preferences of individual operators, the number of scientific comparisons of the two methods is low. There are also no standardized uniform methods of follow-up in analysed groups of patients. Depending on study, the level of patients satisfaction, the results of standardized questionnaires, pad tests, or results of urodynamic studies undergone analysis in the efficacy evaluation. Hence, there are few meta-analyses comparing theefficacyofbothmethods.inaprospectiverandomised study comparing the effectiveness of TOT and TVT, based on an analysis of 70 cases, a comparable efficacy of both surgical techniques was achieved, with shorter surgery time and the risk of bladder injury in favor of TOT [11]. Italian researchers, based on a comparative analysis of 148 patients, showed no difference of statistical significance in both the effectiveness and complication rate between the two groups [12]. In the latest publications from 2013 by Darabi et al., no significant differences in efficacy and safety in both groups were shown, except the bladder catheter maintenance time after surgery [13].Thereareafewanalysesbasedonpatientrelatedsuccessrate,sameassubjectivecurerateintheabove article. For example, British analysis from 2012 in prospective randomised controlled trial proved 73% patient-reported success rate for TOT [14]. Large comparative analysis of 1000 cases of SUI treated with TOT and TVT revealed subjective cure rates ranging from 85 to 96% and objective efficacy ranging from 86 91% [15]. Based on 5-year-follow-up evaluation of TOT a study was published in 2013 that showed subjective and objective cure rates at about 90% [16]. The phenomenon of de novo OAB symptoms is a largely debated postoperative complication of midurethral slings. Some studies reported de novo urgency symptoms in 4 33% of operated patients [17, 18]. Confounding role can also play spontaneous development of age-related OAB in a certain percentage of women. In our study de novo OAB was observed in less than 5% of cases and reduced in time during pharmacological treatment. There have also been some assessments of the results in the treatment of patients with mixed urinary incontinence using midurethral slings. Korean authors concluded in 2003 that treatment with TVT and TOT reduced the percentage of daily incontinence from urgency in these patients, with the higher efficacy in the TVT group [19]. This confirmed the Finnish study from 2013, in which 70% of patients with symptoms of detrusor overactivity declared improvement after the surgery; there was no significant difference between the two operating techniques [20]. A meta-analysis of American scientists in 2007, based on 492 cases, showed no significant differences in the efficacy between the two methods. The conclusion was made that a small number of reports are not clear in showing whether any of these methods are effective
5 BioMed Research International 5 in the treatment of urinary incontinence with mixed etiology [4]. The main economical differences between all those three methodswerethecostofmaterialsusedintheprocedure. In mtot we used a tape made from original mesh used inherniasrepair.onetapeformtotmadefromitcosts around 10 EUR. Original TOT tape in Poland costs about 170 EUR. 6. Conclusions (i) All sling procedures are effective in the treatment of stress urinary incontinence and in 6th month after surgeryachievedcureratesrangefrom91.5%to96.4% in subjective and objective parameters of efficacy. (ii) There are no differences in the efficacy of the treatment of SUI between TVT, TOT, and selfmodification of TOT. (iii) There is a little higher risk of bladder injury during thetvtprocedurethaninthetotandmtot. (iv) Self-modification of TOT, which consists of selfprepared polypropylene tape instead of original tape, is as effective and safe as original TOT with a lower cost of the procedure. (v)slingproceduresinthetreatmentofsuiaresafeand do not cause serious complications. Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] J. O. L. DeLancey, Anatomy and biomechanics of genital prolapse, Clinical Obstetrics and Gynecology,vol.36,no.4,pp , [2] U. Ulmsten, L. Henriksson, P. Johnson, and G. Varhos, An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence, International Urogynecology Journal and Pelvic Floor Dysfunction,vol.7,no.2,pp.81 86, [3] E. Delorme, La bandelette trans-obturatricel un procede miniinvasif de traitement de l incontinence urinary de la femme, Progrès en Urologie, vol. 11, pp , [4] V. W. Sung, M. D. Schleinitz, C. R. Rardin, R. M. Ward, and D. L. Myers, Comparison of retropubic vs transobturator approach to midurethral slings: a systematic review and meta-analysis, American Obstetrics and Gynecology, vol.197,no.1, pp. 3 11, [5] D.Waltregny,O.Reul,B.Mathantu,Y.Gaspar,P.Bonnet,and J. de Leval, Inside out transobturator vaginal tape for the treatment of female stress urinary incontinence: interim results of a prospective study after a 1-year minimum followup, Journal of Urology,vol.175,no.6,pp ,2006. [6]C.G.Nilsson,N.Kuuva,C.Falconer,M.Rezapour,andU. Ulmsten, Long-term results of the tension-free vaginal tape (TVT) procedure for surgical treatment of female stress urinary incontinence, International Urogynecology Journal and Pelvic Floor Dysfunction, vol. 12, supplement 2, pp. S5 S8, [7] K. L. Ward and P. Hilton, A prospective multicenter randomized trial of tension-free vaginal tape and colposuspension for primary urodynamic stress incontinence: two-year follow-up, American Obstetrics and Gynecology, vol.190,no.2, pp , [8] M. M. Karram, J. L. Segal, B. J. Vassallo, and S. D. Kleeman, Complications and untoward effects of the tension-free vaginal tape procedure, Obstetrics and Gynecology,vol.101,no.5,part1, pp , [9] E.Delorme,S.Droupy,R.deTayrac,andV.Delmas, Transobturator tape (Uratape): a new minimally-invasive procedure to treat female urinary incontinence, European Urology, vol. 45, no. 2, pp , [10] A. F. Morey, A. R. Medendorp, M. W. Noller et al., Transobturator versus transabdominal mid urethral slings: a multiinstitutional comparison of obstructive voiding complications, Urology,vol.175,no.3,part1,pp ,2006. [11] D. E. Diab, A. M. Zayed, M. N. Allam, A. M. Maroof, E. Ibraheem, and D. E. El-Sayed, A prospective randomized study comparing the safety and efficacy of transobturator tape (TOT) versus tension free vaginal tape (TVT) in treatment of female stress urinary incontinence, European Urology Supplements, vol.11,no.1,p.e177,2012. [12] M. Porena, E. Costantini, B. Frea et al., Tension-free vaginal tape versus transobturator tape as surgery for stress urinary incontinence: results of a multicentre randomised trial, European Urology,vol.52,no.5,pp ,2007. [13] M. R. Darabi, M. Keshvari, and Z. Sheikhi, Evaluation study between Tension Free Vaginal Tape (TVT) and Transobturator Tape (TOT) in treatment stress incontinence in female, European Urology Supplements,vol.12,no.4,p.e1196,2013. [14] M. Abdel-fattah, A. Mostafa, A. Familusi, I. Ramsay, and J. N Dow, Prospective randomised controlled trial of transobturator tapes in management of urodynamic stress incontinence in women: 3-year outcomes from the Evaluation of Transobturator Tapes study, European Urology, vol. 62, no. 5, pp , [15]D.Y.Pushkar,G.Kasyan,M.Gvozdev,andR.Sosnowski, Analysis of 1,000 cases of synthetic midurethral slings used for treatment of female urinary incontinence a single-center experience, Central European Urology,vol.64,no.4, pp ,2011. [16]M.Serati,R.M.Bauer,J.N.L.Cornuetal., TVT-Oforthe treatment of pure urodynamics stress incontinence in females: efficacy and adverse events at 5 years follow-up, European Urology Supplements,vol.12,no.1,p.e726,2013. [17] M. Serati, F. Ghezzi, E. Cattoni et al., Tension-free vaginal tape for the treatment of urodynamic stress incontinence: efficacy and adverse effects at 10-year follow-up, European Urology,vol. 61, no. 5, pp , [18] G. Novara, A. Galfano, R. Boscolo-Berto et al., Complication rates of tension-free midurethral slings in the treatment of female stress urinary incontinence: a systematic review and meta-analysis of randomized controlled trials comparing tension-free midurethral tapes to other surgical procedures and different devices, European Urology,vol.53,no.2,pp , 2008.
6 6 BioMed Research International [19] J. Y. Han, M. S. Choo, Y. S. Lee et al., Effectiveness of retropubic tension-free vaginal tape and transobturator inside-out tape procedures in women with overactive bladder and stress urinary incontinence, International Neurourology Journal, vol. 17,no.3,pp ,2013. [20] V. Nyyssönen, A. Talvensaari-Mattila, and M. Santala, A prospective randomized trial comparing tension-free vaginal tape versus transobturator tape in patients with stress or mixed urinary incontinence: subjective cure rate and satisfaction in median follow-up of 46 months, Scandinavian Urology,2013.
















7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Clinical audit of the use of tension-free vaginal tape as a surgical treatment for urinary stress incontinence, set against NICE guidelines
 GYNAECOLOGY Clinical audit of the use of tension-free vaginal tape as a surgical treatment for urinary stress incontinence, set against NICE guidelines NATALIA PRICE and SIMON R JACKSON The John Radcliffe
GYNAECOLOGY Clinical audit of the use of tension-free vaginal tape as a surgical treatment for urinary stress incontinence, set against NICE guidelines NATALIA PRICE and SIMON R JACKSON The John Radcliffe
SOGC Recommendations for Urinary Incontinence
 The quality of evidence is rated, and recommendations are made using the criteria described by the Canadian Task Force on Preventive Health Care. Clinical Practice Guidelines: The Evaluation of Stress
The quality of evidence is rated, and recommendations are made using the criteria described by the Canadian Task Force on Preventive Health Care. Clinical Practice Guidelines: The Evaluation of Stress
Normal bladder function requires a coordinated effort between the brain, spinal cord, and the bladder.
 .. Urinary Incontinence Urinary incontinence is not an inevitable part of aging, and it is not a disease. The loss of bladder control - called urinary incontinence - affects between 13 and 17 million adult
.. Urinary Incontinence Urinary incontinence is not an inevitable part of aging, and it is not a disease. The loss of bladder control - called urinary incontinence - affects between 13 and 17 million adult
Mixed urinary incontinence - sling or not sling
 Mixed urinary incontinence - sling or not sling 吳 銘 斌 Ming-Ping Wu, M.D.,Ph.D. Director, Div. Urogynecology & Pelvic Floor Reconstruction, Chi Mei Foundation Hospital, Tainan, Taiwan Assistant Professor,
Mixed urinary incontinence - sling or not sling 吳 銘 斌 Ming-Ping Wu, M.D.,Ph.D. Director, Div. Urogynecology & Pelvic Floor Reconstruction, Chi Mei Foundation Hospital, Tainan, Taiwan Assistant Professor,
Transobturator mid urethral sling surgery for stress urinary incontinence: our experience
 International Journal of Reproduction, Contraception, Obstetrics and Gynecology Bettaiah R et al. Int J Reprod Contracept Obstet Gynecol. 2015 Dec;4(6):1831-1835 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Bettaiah R et al. Int J Reprod Contracept Obstet Gynecol. 2015 Dec;4(6):1831-1835 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
Patient-Reported Outcomes of Retropubic versus Trans-Obturator Mid-Urethral Slings for Urinary Stress Incontinence: The Malaysian Experience
 Patient-Reported Outcomes of Retropubic versus Trans-Obturator Mid-Urethral Slings for Urinary Stress Incontinence: The Malaysian Experience Zalina N a, Kamal N b, Aruku N b, Jamaluddin AR c a Obstetrics
Patient-Reported Outcomes of Retropubic versus Trans-Obturator Mid-Urethral Slings for Urinary Stress Incontinence: The Malaysian Experience Zalina N a, Kamal N b, Aruku N b, Jamaluddin AR c a Obstetrics
URINARY INCONTINENCE CASE PRESENTATION #1. Urinary Incontinence - History 2014/10/07. Structure of the Female Lower Urinary Tract
 Bladder pressure 2014/10/07 Structure of the Female Lower Urinary Tract Ureter URINARY INCONTINENCE Clinical Clerkship Lecture Series Outer peritoneal coat Detrusor smooth muscle Mucosa Trigone Proximal
Bladder pressure 2014/10/07 Structure of the Female Lower Urinary Tract Ureter URINARY INCONTINENCE Clinical Clerkship Lecture Series Outer peritoneal coat Detrusor smooth muscle Mucosa Trigone Proximal
Position Statement on Mesh Midurethral Slings for Stress Urinary Incontinence
 Position Statement on Mesh Midurethral Slings for Stress Urinary Incontinence The polypropylene mesh midurethral sling is the recognized worldwide standard of care for the surgical treatment of stress
Position Statement on Mesh Midurethral Slings for Stress Urinary Incontinence The polypropylene mesh midurethral sling is the recognized worldwide standard of care for the surgical treatment of stress
Urinary Incontinence (Involuntary Loss of Urine) A Patient Guide
 A Patient Guide") Urinary Incontinence (Involuntary Loss of Urine) A Patient Guide Urinary Incontinence (Urine Loss) This booklet is intended to give you some facts on urinary incontinence - what it is, and is not, and
Urinary Incontinence (Involuntary Loss of Urine) A Patient Guide Urinary Incontinence (Urine Loss) This booklet is intended to give you some facts on urinary incontinence - what it is, and is not, and
Female Urinary Disorders and Pelvic Organ Prolapse
 Female Urinary Disorders and Pelvic Organ Prolapse Richard S. Bercik, M.D. Director, Division of Urogynecology & Reconstruction Pelvic Surgery Department of Obstetrics, Gynecology & Reproductive Sciences
Female Urinary Disorders and Pelvic Organ Prolapse Richard S. Bercik, M.D. Director, Division of Urogynecology & Reconstruction Pelvic Surgery Department of Obstetrics, Gynecology & Reproductive Sciences
Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline
/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline") Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline RECOMMENDATIONS 1 Conditional: Clinicians who are making
Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline RECOMMENDATIONS 1 Conditional: Clinicians who are making
Should SUI Surgery be Combined with Pelvic Organ Prolapse Surgery?
 Should SUI Surgery be Combined with Pelvic Organ Prolapse Surgery? Geoffrey W. Cundiff, M.D. 36 th National Congress of the South African Society of Obstetricians and Gynaecologists SASOG 2014 Learning
Should SUI Surgery be Combined with Pelvic Organ Prolapse Surgery? Geoffrey W. Cundiff, M.D. 36 th National Congress of the South African Society of Obstetricians and Gynaecologists SASOG 2014 Learning
2/21/2016. Prolapse Surgery after Transvaginal Mesh: The Evolving Landscape. Disclosures. Objectives. No Relevant Disclosures
 Prolapse Surgery after Transvaginal Mesh: The Evolving Landscape David R. Ellington, MD, FACOG Assistant Professor Division of Urogynecology and Pelvic Reconstructive Surgery Disclosures No Relevant Disclosures
Prolapse Surgery after Transvaginal Mesh: The Evolving Landscape David R. Ellington, MD, FACOG Assistant Professor Division of Urogynecology and Pelvic Reconstructive Surgery Disclosures No Relevant Disclosures
Tension-free vaginal tape sling for recurrent stress incontinence after transobturator tape sling failure
 Int Urogynecol J (2007) 18:309 313 DOI 10.1007/s00192-006-0149-z ORIGINAL ARTICLE Tension-free vaginal tape sling for recurrent stress incontinence after transobturator tape sling failure Robert D. Moore
Int Urogynecol J (2007) 18:309 313 DOI 10.1007/s00192-006-0149-z ORIGINAL ARTICLE Tension-free vaginal tape sling for recurrent stress incontinence after transobturator tape sling failure Robert D. Moore
Female Urinary Incontinence
 Female Urinary Incontinence Molly Heublein, MD Assistant Professor Clinical Medicine UCSF Women s Health Primary Care Disclosures I have nothing to disclose. 1 Objectives Review the problem Feel confident
Female Urinary Incontinence Molly Heublein, MD Assistant Professor Clinical Medicine UCSF Women s Health Primary Care Disclosures I have nothing to disclose. 1 Objectives Review the problem Feel confident
In the mid-1990s, Ulmsten and Petros 1 introduced the synthetic,
 Surgical Intervention for Stress Urinary Incontinence: Comparison of Midurethral Sling Procedures Joseph M. Novi, DO Beth H.K. Mulvihill, DO Context: The synthetic, tension-free midurethral sling was introduced
Surgical Intervention for Stress Urinary Incontinence: Comparison of Midurethral Sling Procedures Joseph M. Novi, DO Beth H.K. Mulvihill, DO Context: The synthetic, tension-free midurethral sling was introduced
1 in 3 women experience Stress Urinary Incontinence.
 A PATIENT S GUIDE 1 in 3 women experience Stress Urinary Incontinence. It s time to talk about SUI Get the facts. This Patient s Guide is intended as a public resource on the issue of Stress Urinary Incontinence
A PATIENT S GUIDE 1 in 3 women experience Stress Urinary Incontinence. It s time to talk about SUI Get the facts. This Patient s Guide is intended as a public resource on the issue of Stress Urinary Incontinence
FEMALE UROLOGY Suprapubic sling adjustment: minimally invasive method of curing recurrent stress incontinence after sling surgery
 FEMALE UROLOGY Suprapubic sling adjustment: minimally invasive method of curing recurrent stress incontinence after sling surgery Choe JM Urodynamics and Continence Center, Division of Urology, University
FEMALE UROLOGY Suprapubic sling adjustment: minimally invasive method of curing recurrent stress incontinence after sling surgery Choe JM Urodynamics and Continence Center, Division of Urology, University
VAGINAL TAPE PROCEDURES FOR THE TREATMENT OF STRESS INCONTINENCE
 VAGINAL TAPE PROCEDURES FOR THE TREATMENT OF STRESS INCONTINENCE AN INFORMATION LEAFLET Written by: Department of Urology May 2011 Stockport: 0161 419 5698 Website: w w w. s t o c k p o r t. n h s. u k
VAGINAL TAPE PROCEDURES FOR THE TREATMENT OF STRESS INCONTINENCE AN INFORMATION LEAFLET Written by: Department of Urology May 2011 Stockport: 0161 419 5698 Website: w w w. s t o c k p o r t. n h s. u k
Tension-Free Vaginal Tape: Outcomes Among Women With Primary Versus Recurrent Stress Urinary Incontinence
 Tension-Free Vaginal Tape: Outcomes Among Women With Versus Stress Urinary Incontinence C. R. Rardin, MD, N. Kohli, MD, P. L. Rosenblatt, MD, J. R. Miklos, MD, R. Moore, MD, and W. C. Strohsnitter, MS
Tension-Free Vaginal Tape: Outcomes Among Women With Versus Stress Urinary Incontinence C. R. Rardin, MD, N. Kohli, MD, P. L. Rosenblatt, MD, J. R. Miklos, MD, R. Moore, MD, and W. C. Strohsnitter, MS
Overactive Bladder (OAB)
") Overactive Bladder (OAB) Overactive bladder is a problem with bladder storage function that causes a sudden urge to urinate. The urge may be difficult to suppress, and overactive bladder can lead to the
Overactive Bladder (OAB) Overactive bladder is a problem with bladder storage function that causes a sudden urge to urinate. The urge may be difficult to suppress, and overactive bladder can lead to the
Consumer summary Minimally invasive techniques for the relief of stress urinary incontinence
 ASERNIP S Australian Safety and Efficacy Register of New Interventional Procedures Surgical Consumer summary Minimally invasive techniques for the relief of stress urinary incontinence (Adapted from the
ASERNIP S Australian Safety and Efficacy Register of New Interventional Procedures Surgical Consumer summary Minimally invasive techniques for the relief of stress urinary incontinence (Adapted from the
Stress incontinence. Supported by an unrestricted grant from
 Stress incontinence As a health care provider you can make a significant difference to the quality of life of patients like these by addressing urinary incontinence, introducing conservative therapies
Stress incontinence As a health care provider you can make a significant difference to the quality of life of patients like these by addressing urinary incontinence, introducing conservative therapies
Received June 18, 2007; Revised August 30, 2007; Accepted August 30, 2007; Published September 17, 2007
 Case Study TheScientificWorldJOURNAL (2007) 7, 1575 1578 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2007.253 Unusual Complication of Suprapubic Cystostomy in a Male Patient with Tetraplegia: Traction
Case Study TheScientificWorldJOURNAL (2007) 7, 1575 1578 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2007.253 Unusual Complication of Suprapubic Cystostomy in a Male Patient with Tetraplegia: Traction
Surgical Treatment for Female Stress Urinary. Continence. Consumer Education
 Surgical Treatment for Female Stress Urinary Incontinence By: Amy Rosenman, MD Geffen School of Medicine at UCLA Santa Monica, California Promoting Quality Continence Care through Consumer Education Always
Surgical Treatment for Female Stress Urinary Incontinence By: Amy Rosenman, MD Geffen School of Medicine at UCLA Santa Monica, California Promoting Quality Continence Care through Consumer Education Always
MANAGEMENT OF SLING COMPLICATIONS IN FEMALES. Jorge L. Lockhart M.D. Program Director Division of Urology University of South Florida
 MANAGEMENT OF SLING COMPLICATIONS IN FEMALES Jorge L. Lockhart M.D. Program Director Division of Urology University of South Florida INTRODUCTION The traditional gold standard treatments for stress urinary
MANAGEMENT OF SLING COMPLICATIONS IN FEMALES Jorge L. Lockhart M.D. Program Director Division of Urology University of South Florida INTRODUCTION The traditional gold standard treatments for stress urinary
Prevention & Treatment of De Novo Stress Incontinence after POP. Andy Vu, DO, FACOG UNT Health Science Center Fort Worth, TX.
 Prevention & Treatment of De Novo Stress Incontinence after POP Andy Vu, DO, FACOG UNT Health Science Center Fort Worth, TX Surgery Presenter Disclosure No Conflict of Interest to disclose No Financial
Prevention & Treatment of De Novo Stress Incontinence after POP Andy Vu, DO, FACOG UNT Health Science Center Fort Worth, TX Surgery Presenter Disclosure No Conflict of Interest to disclose No Financial
Mesh Erosion and What to do
 Disclosures Mesh Erosion and What to do None Michelle Y. Morrill, MD Chief of Urogynecology, TPMG Director of Urogynecology, Kaiser San Francisco Assistant Professor, Volunteer Faculty Dept of Ob/Gyn,
Disclosures Mesh Erosion and What to do None Michelle Y. Morrill, MD Chief of Urogynecology, TPMG Director of Urogynecology, Kaiser San Francisco Assistant Professor, Volunteer Faculty Dept of Ob/Gyn,
Learning Resource Guide. Understanding Incontinence. 2000 Prism Innovations, Inc. All Rights Reserved
 Learning Resource Guide Understanding Incontinence 2000 Prism Innovations, Inc. All Rights Reserved ElderCare Online s Learning Resource Guide Understanding Incontinence Table of Contents Introduction
Learning Resource Guide Understanding Incontinence 2000 Prism Innovations, Inc. All Rights Reserved ElderCare Online s Learning Resource Guide Understanding Incontinence Table of Contents Introduction
Y O R K. Health Economics MEDICINES AND HEALTHCARE PRODUCTS REGULATORY AGENCY
 Y O R K Health Economics C O N S O R T I U M MEDICINES AND HEALTHCARE PRODUCTS REGULATORY AGENCY Summaries of the Safety/Adverse Effects of Vaginal Tapes/Slings/Meshes for Stress Urinary Incontinence and
Y O R K Health Economics C O N S O R T I U M MEDICINES AND HEALTHCARE PRODUCTS REGULATORY AGENCY Summaries of the Safety/Adverse Effects of Vaginal Tapes/Slings/Meshes for Stress Urinary Incontinence and
Women s Health. The TVT procedure. Information for patients
 Women s Health The TVT procedure Information for patients What is a TVT procedure? A TVT (Tension-free Vaginal Tape) procedure is an operation to help women with stress incontinence the leakage of urine
Women s Health The TVT procedure Information for patients What is a TVT procedure? A TVT (Tension-free Vaginal Tape) procedure is an operation to help women with stress incontinence the leakage of urine
LOSS OF BLADDER CONTROL IS TREATABLE TAKE CONTROL AND RESTORE YOUR LIFESTYLE
 LOSS OF BLADDER CONTROL IS TREATABLE TAKE CONTROL AND RESTORE YOUR LIFESTYLE TALKING ABOUT STRESS INCONTINENCE (SUI) Millions of women suffer from stress incontinence (SUI). This condition results in accidental
LOSS OF BLADDER CONTROL IS TREATABLE TAKE CONTROL AND RESTORE YOUR LIFESTYLE TALKING ABOUT STRESS INCONTINENCE (SUI) Millions of women suffer from stress incontinence (SUI). This condition results in accidental
Get the Facts, Be Informed, Make YOUR Best Decision. Pelvic Organ Prolapse
 Pelvic Organ Prolapse ETHICON Women s Health & Urology, a division of ETHICON, INC., a Johnson & Johnson company, is dedicated to providing innovative solutions for common women s health problems and to
Pelvic Organ Prolapse ETHICON Women s Health & Urology, a division of ETHICON, INC., a Johnson & Johnson company, is dedicated to providing innovative solutions for common women s health problems and to
Urinary Incontinence in Women. Susan Hingle, M.D. Department of Medicine
 Urinary Incontinence in Women Susan Hingle, M.D. Department of Medicine Background Estimated 13 million Americans with urinary incontinence Women are affected twice as frequently as men Only 25% will seek
Urinary Incontinence in Women Susan Hingle, M.D. Department of Medicine Background Estimated 13 million Americans with urinary incontinence Women are affected twice as frequently as men Only 25% will seek
Primary Care Management Guidelines Female Urinary Incontinence. Overview of Lecture
 Primary Care Management Guidelines Female Urinary Incontinence Professor Don Wilson Department of Women s and Children s Health Dunedin School of Medicine University of Otago GP Teaching for Roy Morris,
Primary Care Management Guidelines Female Urinary Incontinence Professor Don Wilson Department of Women s and Children s Health Dunedin School of Medicine University of Otago GP Teaching for Roy Morris,
Urinary Incontinence. Anatomy and Terminology Overview. Moeen Abu-Sitta, MD, FACOG, FACS
 Urinary Incontinence Anatomy and Terminology Overview Moeen Abu-Sitta, MD, FACOG, FACS Purpose Locate and describe the anatomy of the Female Urinary System Define terminology related to Incontinence Describe
Urinary Incontinence Anatomy and Terminology Overview Moeen Abu-Sitta, MD, FACOG, FACS Purpose Locate and describe the anatomy of the Female Urinary System Define terminology related to Incontinence Describe
Stress Urinary Incontinence: Treatment Manisha Patel, MD April 10, 2006
 Stress Urinary Incontinence: Treatment Manisha Patel, MD April 10, 2006 What treatment options are available for a woman with stress urinary incontinence (SUI)? Behavioral therapy, medication, pessary,
Stress Urinary Incontinence: Treatment Manisha Patel, MD April 10, 2006 What treatment options are available for a woman with stress urinary incontinence (SUI)? Behavioral therapy, medication, pessary,
Transobturator tape sling Female sling system
 Transobturator tape sling Female sling system Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Transobturator tape sling Female sling system Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Regain Control of Your Active Life Treatment Options for Incontinence and Pelvic Organ Prolapse
 Regain Control of Your Active Life Treatment Options for Incontinence and Pelvic Organ Prolapse Nearly one quarter of all women in the United States have some sort of pelvic floor disorder such as urinary
Regain Control of Your Active Life Treatment Options for Incontinence and Pelvic Organ Prolapse Nearly one quarter of all women in the United States have some sort of pelvic floor disorder such as urinary
Chief Executives, NHS Boards General Practitioners Medical Directors, NHS Boards
 Directorate of Chief Medical Officer and Public Health Sir Harry Burns MPH FRCS (Glas) FRCP(Ed) FFPH Chief Medical Officer T: 0131-244 2287 E: Sara.Davies@scotland.gsi.gov.uk David.Bishop@scotland.gsi.gov.uk
Directorate of Chief Medical Officer and Public Health Sir Harry Burns MPH FRCS (Glas) FRCP(Ed) FFPH Chief Medical Officer T: 0131-244 2287 E: Sara.Davies@scotland.gsi.gov.uk David.Bishop@scotland.gsi.gov.uk
PHYSICIAN / HEALTH CARE PROVIDER POCKET GUIDE. Stress Urinary Incontinence
 PHYSICIAN / HEALTH CARE PROVIDER POCKET GUIDE Stress Urinary Incontinence 1 in 3 women experience Stress Urinary Incontinence. This pocket guide is intended as a resource for physicians on the complex
PHYSICIAN / HEALTH CARE PROVIDER POCKET GUIDE Stress Urinary Incontinence 1 in 3 women experience Stress Urinary Incontinence. This pocket guide is intended as a resource for physicians on the complex
What you should know about Stress Urinary Incontinence
 Gynecare TVT Stop coping. Start living. What you should know about Stress Urinary Incontinence Have you ever leaked urine when you laughed, coughed or sneezed? You are not alone. Many women suffer from
Gynecare TVT Stop coping. Start living. What you should know about Stress Urinary Incontinence Have you ever leaked urine when you laughed, coughed or sneezed? You are not alone. Many women suffer from
9/24/2015. Incontinence and Prolapse 2015 Primary Care Update CME Symposium. Objectives. Mark Memo, DO, FACS NEO Urology September 25-27
 Incontinence and Prolapse 2015 Primary Care Update CME Symposium Mark Memo, DO, FACS NEO Urology September 25-27 Objectives Incontinence Pelvic Organ Prolapse Vaginal Mesh Litigation 1 Urinary Incontinence
Incontinence and Prolapse 2015 Primary Care Update CME Symposium Mark Memo, DO, FACS NEO Urology September 25-27 Objectives Incontinence Pelvic Organ Prolapse Vaginal Mesh Litigation 1 Urinary Incontinence
5-Year Continence Rates, Satisfaction and Adverse Events of Burch Urethropexy and Fascial Sling Surgery for Urinary Incontinence
 5-Year Continence Rates, Satisfaction and Adverse Events of Burch Urethropexy and Fascial Sling Surgery for Urinary Incontinence L. Brubaker,*, H. E. Richter, P. A. Norton, M. Albo, H. M. Zyczynski, T.
5-Year Continence Rates, Satisfaction and Adverse Events of Burch Urethropexy and Fascial Sling Surgery for Urinary Incontinence L. Brubaker,*, H. E. Richter, P. A. Norton, M. Albo, H. M. Zyczynski, T.
Topic review: Clinical presentation and diagnosis of urinary incontinence in the elderly. Prapa Pattrapornpisut 7 June 2012
 1 Topic review: Clinical presentation and diagnosis of urinary incontinence in the elderly Prapa Pattrapornpisut 7 June 2012 2 Urinary incontinence Definition the complaint of any involuntary leakage of
1 Topic review: Clinical presentation and diagnosis of urinary incontinence in the elderly Prapa Pattrapornpisut 7 June 2012 2 Urinary incontinence Definition the complaint of any involuntary leakage of
Health Policy Advisory Committee on Technology
 Health Policy Advisory Committee on Technology Technology Brief Single-incision mini-sling system for female stress urinary incontinence August 2013 State of Queensland (Queensland Department of Health)
Health Policy Advisory Committee on Technology Technology Brief Single-incision mini-sling system for female stress urinary incontinence August 2013 State of Queensland (Queensland Department of Health)
TRANSVAGINAL MESH IN PELVIC ORGAN PROLAPSE REPAIR.
 TRANSVAGINAL MESH IN PELVIC ORGAN PROLAPSE REPAIR. Spanish full text SUMMARY Introduction: Pelvic organ prolapse (POP) is characterised by the descent or herniation of the uterus, vaginal vault, bladder
TRANSVAGINAL MESH IN PELVIC ORGAN PROLAPSE REPAIR. Spanish full text SUMMARY Introduction: Pelvic organ prolapse (POP) is characterised by the descent or herniation of the uterus, vaginal vault, bladder
Stress Urinary Incontinence
 Saint Mary s Hospital Gynaecology Service Warrell Unit Stress Urinary Incontinence Information for patients What is Stress Incontinence? Stress incontinence is a leakage of urine occurring on physical
Saint Mary s Hospital Gynaecology Service Warrell Unit Stress Urinary Incontinence Information for patients What is Stress Incontinence? Stress incontinence is a leakage of urine occurring on physical
Urinary Incontinence
 Urinary Incontinence Q: What is urinary Urinary (YOOR-in-air-ee) incontinence (in-kahn-tih-nens) is when urine leaks out before you can get to a bathroom. If you have urinary incontinence, you re not alone.
Urinary Incontinence Q: What is urinary Urinary (YOOR-in-air-ee) incontinence (in-kahn-tih-nens) is when urine leaks out before you can get to a bathroom. If you have urinary incontinence, you re not alone.
Comparison of TOA and TOT for Treating Female Stress Urinary Incontinence: Short-Term Outcomes
 www.kjurology.org DOI:10.4111/kju.2010.51.8.544 Comparison of TOA and TOT for Treating Female Stress Urinary Incontinence: Short-Term Outcomes Chang Shik Youn, Ju Hyun Shin, Yong Gil Na Department of Urology,
www.kjurology.org DOI:10.4111/kju.2010.51.8.544 Comparison of TOA and TOT for Treating Female Stress Urinary Incontinence: Short-Term Outcomes Chang Shik Youn, Ju Hyun Shin, Yong Gil Na Department of Urology,
Name of Policy: Urodynamic Testing to Evaluate Urinary Incontinence
 Name of Policy: Urodynamic Testing to Evaluate Urinary Incontinence Policy #: 315 Latest Review Date: September 2011 Category: Medical Policy Grade: Active Policy but no longer scheduled for regular literature
Name of Policy: Urodynamic Testing to Evaluate Urinary Incontinence Policy #: 315 Latest Review Date: September 2011 Category: Medical Policy Grade: Active Policy but no longer scheduled for regular literature
TRANSOBSTURATOR TAPE (TOT) PROCEDURE: THE IPOH EXPERIENCE
 PROCEDURE: THE IPOH EXPERIENCE") TRANSOBSTURATOR TAPE (TOT) PROCEDURE: THE IPOH EXPERIENCE Zalina Nusee¹, Aruku Naidu 2, Ranjudham SN², Hamizah Ismail 1 1 Division of Urogynecology, Department of Obstetrics and Gynecology, Kulliyyah of
TRANSOBSTURATOR TAPE (TOT) PROCEDURE: THE IPOH EXPERIENCE Zalina Nusee¹, Aruku Naidu 2, Ranjudham SN², Hamizah Ismail 1 1 Division of Urogynecology, Department of Obstetrics and Gynecology, Kulliyyah of
Postoperative. Voiding Dysfunction
 Postoperative Voiding Trial Voiding Dysfunction Stephanie Pickett, MD Fellow Female Pelvic Medicine and Reconstructive Surgery Objectives Define postoperative voiding dysfunction Describe how to evaluate
Postoperative Voiding Trial Voiding Dysfunction Stephanie Pickett, MD Fellow Female Pelvic Medicine and Reconstructive Surgery Objectives Define postoperative voiding dysfunction Describe how to evaluate
Urinary Incontinence FAQ Sheet
 Urinary Incontinence FAQ Sheet Are you reluctant to talk to your doctor about your bladder control problem? Don t be. There is help. Loss of bladder control is called urinary incontinence. It can happen
Urinary Incontinence FAQ Sheet Are you reluctant to talk to your doctor about your bladder control problem? Don t be. There is help. Loss of bladder control is called urinary incontinence. It can happen
Synthetic Vaginal Mesh Mid-urethral Tape Procedure for the Surgical Treatment of Stress Urinary Incontinence in Women
 Synthetic Vaginal Mesh Mid-urethral Tape Procedure for the Surgical Treatment of Stress Urinary Incontinence in Women PATIENT INFORMATION AND CONSENT BOOKLET Patient Label Patient Information and Consent
Synthetic Vaginal Mesh Mid-urethral Tape Procedure for the Surgical Treatment of Stress Urinary Incontinence in Women PATIENT INFORMATION AND CONSENT BOOKLET Patient Label Patient Information and Consent
Overactive bladder and urgency incontinence
 Overactive bladder and urgency incontinence As a health care provider you can make a significant difference to the quality of life of patients like these by addressing urinary incontinence, introducing
Overactive bladder and urgency incontinence As a health care provider you can make a significant difference to the quality of life of patients like these by addressing urinary incontinence, introducing
URINARY INCONTINENCE
 URINARY INCONTINENCE What is urinary incontinence? Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only a few drops when you cough or sneeze to entirely
URINARY INCONTINENCE What is urinary incontinence? Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only a few drops when you cough or sneeze to entirely
Women suffer in silence
 Women suffer in silence Stress urinary incontinence is the involuntary loss of urine resulting from increased intra-abdominal pressure. In people who suffer with this condition, forms of exertion such
Women suffer in silence Stress urinary incontinence is the involuntary loss of urine resulting from increased intra-abdominal pressure. In people who suffer with this condition, forms of exertion such
Bladder Health Promotion
 Bladder Health Promotion Community Awareness Presentation Content contributions provided by the Society of Urologic Nurses (SUNA) National Association for Continence (NAFC) Simon Foundation for Continence
Bladder Health Promotion Community Awareness Presentation Content contributions provided by the Society of Urologic Nurses (SUNA) National Association for Continence (NAFC) Simon Foundation for Continence
Complications of the tension-free vaginal tape procedure for stress urinary incontinence
 Int Urogynecol J (2010) 21:1353 1357 DOI 10.1007/s00192-010-1210-5 ORIGINAL ARTICLE Complications of the tension-free vaginal tape procedure for stress urinary incontinence Ingrid Kristensen & Maysoon
Int Urogynecol J (2010) 21:1353 1357 DOI 10.1007/s00192-010-1210-5 ORIGINAL ARTICLE Complications of the tension-free vaginal tape procedure for stress urinary incontinence Ingrid Kristensen & Maysoon
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 Initial assessment and investigation of urinary incontinence bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used
Initial assessment and investigation of urinary incontinence bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used
FEMALE INCONTINENCE REVIEW
 200 S. Wenona Suite 298 Steven L. Jensen, M.D. 5400 Mackinaw, Suite 4302 Bay City, MI 48706 Frank H. Kim, M.D. Saginaw, MI 48604 Telephone (989) 895-2634 Adult & Pediatric Urologists (989) 791-4020 Fax
200 S. Wenona Suite 298 Steven L. Jensen, M.D. 5400 Mackinaw, Suite 4302 Bay City, MI 48706 Frank H. Kim, M.D. Saginaw, MI 48604 Telephone (989) 895-2634 Adult & Pediatric Urologists (989) 791-4020 Fax
Quality of Life Impact of Using Tension-free Vaginal Tape for Stress Urinary Incontinence
 Original Article Quality of Life Impact of Using Tension-free Vaginal Tape for Stress Urinary Incontinence Shi-Wei Huang, Hong-Jeng Yu, Wai-Yan Wong, Jun Chen Department of Urology, National Taiwan University
Original Article Quality of Life Impact of Using Tension-free Vaginal Tape for Stress Urinary Incontinence Shi-Wei Huang, Hong-Jeng Yu, Wai-Yan Wong, Jun Chen Department of Urology, National Taiwan University
Minimally invasive synthetic suburethral sling operations for stress urinary incontinence in women (Review)
") Minimally invasive synthetic suburethral sling operations for stress urinary incontinence in women (Review) Ogah J, Cody JD, Rogerson L This is a reprint of a Cochrane review, prepared and maintained by
Minimally invasive synthetic suburethral sling operations for stress urinary incontinence in women (Review) Ogah J, Cody JD, Rogerson L This is a reprint of a Cochrane review, prepared and maintained by
An operation for stress incontinence Tension-free Vaginal Tape (TVT)
") Saint Mary s Hospital The Warrell Unit An operation for stress incontinence Tension-free Vaginal Tape (TVT) Information for Patients 1 Stress Incontinence Stress incontinence is a leakage of urine occurring
Saint Mary s Hospital The Warrell Unit An operation for stress incontinence Tension-free Vaginal Tape (TVT) Information for Patients 1 Stress Incontinence Stress incontinence is a leakage of urine occurring
Beverly E Hashimoto, M.D. Virginia Mason Medical Center, Seattle, WA
 Pelvic Floor Relaxation Beverly E Hashimoto, M.D. Virginia Mason Medical Center, Seattle, WA Disclosures Beverly Hashimoto: GE Medical Systems: research support and consultant (all fees given to Virginia
Pelvic Floor Relaxation Beverly E Hashimoto, M.D. Virginia Mason Medical Center, Seattle, WA Disclosures Beverly Hashimoto: GE Medical Systems: research support and consultant (all fees given to Virginia
URINARY INCONTINENCE IN WOMEN
 URINARY INCONTINENCE IN WOMEN Definition Urinary incontinence (UI) is defined as involuntary loss of urine that is a social or hygienic problem (International Continence Society, 1973) Magnitude of the
URINARY INCONTINENCE IN WOMEN Definition Urinary incontinence (UI) is defined as involuntary loss of urine that is a social or hygienic problem (International Continence Society, 1973) Magnitude of the
Bladder Health Promotion
 Bladder Health Promotion Community Awareness Presentation endorsed by the Society of Urologic Nurses (SUNA) National Association for Continence( NAFC) Simon Foundation for Continence This presentation
Bladder Health Promotion Community Awareness Presentation endorsed by the Society of Urologic Nurses (SUNA) National Association for Continence( NAFC) Simon Foundation for Continence This presentation
previous surgery for incontinence.
 Predictive Title page Authors procedure value for of urinary urethra stress mobility incontinence before sub-urethra in women tape Xavier Khalid Alain Fabien Jean-Louis Pigné, Demaria, Zabak, Fritel, MD
Predictive Title page Authors procedure value for of urinary urethra stress mobility incontinence before sub-urethra in women tape Xavier Khalid Alain Fabien Jean-Louis Pigné, Demaria, Zabak, Fritel, MD
GENERAL OBSTETRICS AND GYNECOLOGY: GYNECOLOGY
 American Journal of Obstetrics and Gynecology (2004) 190, 602e8 www.elsevier.com/locate/ajog GENERAL OBSTETRICS AND GYNECOLOGY: GYNECOLOGY A prospective randomized trial comparing tension-free vaginal
American Journal of Obstetrics and Gynecology (2004) 190, 602e8 www.elsevier.com/locate/ajog GENERAL OBSTETRICS AND GYNECOLOGY: GYNECOLOGY A prospective randomized trial comparing tension-free vaginal
COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP)
") The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 18 December 2002 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON THE
The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 18 December 2002 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON THE
Midurethral Slings for Women with Stress Urinary Incontinence
 Ontario Health Technology Assessment Series 2006; Vol. 6, No. 3 Midurethral Slings for Women with Stress Urinary Incontinence An Evidence-Based Analysis February 2006 Medical Advisory Secretariat Ministry
Ontario Health Technology Assessment Series 2006; Vol. 6, No. 3 Midurethral Slings for Women with Stress Urinary Incontinence An Evidence-Based Analysis February 2006 Medical Advisory Secretariat Ministry
Patient. Frequently Asked Questions. Transvaginal Surgical Mesh for Pelvic Organ Prolapse
 Patient Frequently Asked Questions Transvaginal Surgical Mesh for Pelvic Organ Prolapse Frequently Asked Questions WHAT IS PELVIC ORGAN PROLAPSE AND HOW IS IT TREATED? Q: What is pelvic organ prolapse
Patient Frequently Asked Questions Transvaginal Surgical Mesh for Pelvic Organ Prolapse Frequently Asked Questions WHAT IS PELVIC ORGAN PROLAPSE AND HOW IS IT TREATED? Q: What is pelvic organ prolapse
Urinary incontinence during sexual intercourse: a common, but rarely volunteered, symptom
 British Journal of Obstetrics and Gynaecology April 1988, Vol. 95, pp. 77-81 Urinary incontinence during sexual intercourse: a common, but rarely volunteered, symptom PAUL HILTON Summary. A total of 4
British Journal of Obstetrics and Gynaecology April 1988, Vol. 95, pp. 77-81 Urinary incontinence during sexual intercourse: a common, but rarely volunteered, symptom PAUL HILTON Summary. A total of 4
Stress incontinence in Women
 Stress incontinence in Women Exceptional healthcare, personally delivered Operations for Stress Incontinence Introduction Stress incontinence is a medical word used to describe the type of leakage that
Stress incontinence in Women Exceptional healthcare, personally delivered Operations for Stress Incontinence Introduction Stress incontinence is a medical word used to describe the type of leakage that
Urinary Incontinence Dr. Leffler
 Urinary Incontinence Dr. Leffler The involuntary loss of urine at socially unacceptable times occurs in both women and men, but more commonly in women. It has multiple, far-reaching effects on daily activities,
Urinary Incontinence Dr. Leffler The involuntary loss of urine at socially unacceptable times occurs in both women and men, but more commonly in women. It has multiple, far-reaching effects on daily activities,
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 21 CBULP 2011 068 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 21 CBULP 2011 068 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse
 Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse July 2011 I. EXECUTIVE SUMMARY...3 II. OVERVIEW...3 III. SURGICAL MESH FOR UROGYNECOLOGIC
Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse July 2011 I. EXECUTIVE SUMMARY...3 II. OVERVIEW...3 III. SURGICAL MESH FOR UROGYNECOLOGIC
TIBIAL NERVE STIMULATION: ONE OF SEVERAL NEW OPTIONS FOR THE MANAGEMENT OF OVERACTIVE BLADDER IN WOMEN
 TIBIAL NERVE STIMULATION: ONE OF SEVERAL NEW OPTIONS FOR THE MANAGEMENT OF OVERACTIVE BLADDER IN WOMEN Scott A Farrell MD Professor Dept of Obstetrics and Gynaecology Dalhousie University Declaration of
TIBIAL NERVE STIMULATION: ONE OF SEVERAL NEW OPTIONS FOR THE MANAGEMENT OF OVERACTIVE BLADDER IN WOMEN Scott A Farrell MD Professor Dept of Obstetrics and Gynaecology Dalhousie University Declaration of
Bard: Continence Therapy. Stress Urinary Incontinence. Regaining Control. Restoring Your Lifestyle.
 Bard: Continence Therapy Stress Urinary Incontinence Regaining Control. Restoring Your Lifestyle. Stress Urinary Incontinence Becoming knowledgeable about urinary incontinence Uterus Normal Pelvic Anatomy
Bard: Continence Therapy Stress Urinary Incontinence Regaining Control. Restoring Your Lifestyle. Stress Urinary Incontinence Becoming knowledgeable about urinary incontinence Uterus Normal Pelvic Anatomy
Urinary Incontinence: an overview!! Neil Harris Consultant Urological Surgeon, Leeds
 Urinary Incontinence: an overview!! Neil Harris Consultant Urological Surgeon, Leeds Content 1. Epidemiology of pelvic floor dysfunction Urinary incontinence Bowel dysfunction Sexual dysfunction 2. Treatment
Urinary Incontinence: an overview!! Neil Harris Consultant Urological Surgeon, Leeds Content 1. Epidemiology of pelvic floor dysfunction Urinary incontinence Bowel dysfunction Sexual dysfunction 2. Treatment
Classification of Mixed Incontinence
 european urology supplements 5 (2006) 837 841 available at www.sciencedirect.com journal homepage: www.europeanurology.com Classification of Mixed Incontinence Christopher Chapple * Sheffield Hallam University,
european urology supplements 5 (2006) 837 841 available at www.sciencedirect.com journal homepage: www.europeanurology.com Classification of Mixed Incontinence Christopher Chapple * Sheffield Hallam University,
Surgery for stress incontinence:
 Surgery for stress incontinence: information for you Published February 2005 by the RCOG Contents Page number Key points 1 About this information 2 What is stress incontinence? 2 Do I need an operation?
Surgery for stress incontinence: information for you Published February 2005 by the RCOG Contents Page number Key points 1 About this information 2 What is stress incontinence? 2 Do I need an operation?
Vaginal Mesh: The FDA Decision and Repurcussions. Roger Dmochowski MD, FACS Dept of Urology Vanderbilt University Medical Center Nashville, TN
 Vaginal Mesh: The FDA Decision and Repurcussions Roger Dmochowski MD, FACS Dept of Urology Vanderbilt University Medical Center Nashville, TN 1 ANATOMY FUNCTION 2 Mesh vs No Mesh Outcomes Sivaslioglu 2007
Vaginal Mesh: The FDA Decision and Repurcussions Roger Dmochowski MD, FACS Dept of Urology Vanderbilt University Medical Center Nashville, TN 1 ANATOMY FUNCTION 2 Mesh vs No Mesh Outcomes Sivaslioglu 2007
Treatments for Urinary Incontinence in Women
 Treatments for Urinary Incontinence in Women National Kidney and Urologic Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH
Treatments for Urinary Incontinence in Women National Kidney and Urologic Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH
MiniArc Single-Invasive Sling in the Treatment of UTI
 Neurourology Mini-Invasive Sling in The Treatment of Urinary Incontinence International Braz J Urol Vol. 35 (3): 334-343, May - June, 2009 The MiniArc Sling System in the Treatment of Female Stress Urinary
Neurourology Mini-Invasive Sling in The Treatment of Urinary Incontinence International Braz J Urol Vol. 35 (3): 334-343, May - June, 2009 The MiniArc Sling System in the Treatment of Female Stress Urinary
Female Urinary Incontinence
 Focus on CME at the University of British Columbia Approach to Female Urinary Incontinence Although the majority of incontinence patients can be diagnosed and treated effectively by family doctors, there
Focus on CME at the University of British Columbia Approach to Female Urinary Incontinence Although the majority of incontinence patients can be diagnosed and treated effectively by family doctors, there
Stress Urinary Incontinence & Sexual Function
 Stress Urinary Incontinence & Sexual Function Lior Lowenstein, MD, MS Associate Professor Deputy Chairman of Obstetrics and Gynecology Department Rambam Health Care Campus Haifa Israel No Disclosures Disclosures
Stress Urinary Incontinence & Sexual Function Lior Lowenstein, MD, MS Associate Professor Deputy Chairman of Obstetrics and Gynecology Department Rambam Health Care Campus Haifa Israel No Disclosures Disclosures
Urinary Incontinence. Types
 Urinary Incontinence Leakage of urine is called urinary incontinence. It is a common problem in women. Some women occasionally leak small amounts of urine. At other times, leakage of urine is frequent
Urinary Incontinence Leakage of urine is called urinary incontinence. It is a common problem in women. Some women occasionally leak small amounts of urine. At other times, leakage of urine is frequent
symptoms of Incontinence
 Types, causes and symptoms of Urinary Incontinence Aims and Objectives Aim: To have an understanding of the types and causes of urinary incontinence. Objectives: To be aware of the incidence and prevalence
Types, causes and symptoms of Urinary Incontinence Aims and Objectives Aim: To have an understanding of the types and causes of urinary incontinence. Objectives: To be aware of the incidence and prevalence
Refer to Coaptite Injectable Implant Instructions for Use provided with product for complete instructions for use.
 Questions for my Doctor Refer to Coaptite Injectable Implant Instructions for Use provided with product for complete instructions for use. INDICATIONS: Coaptite Injectable Implant is indicated for soft
Questions for my Doctor Refer to Coaptite Injectable Implant Instructions for Use provided with product for complete instructions for use. INDICATIONS: Coaptite Injectable Implant is indicated for soft
Operations for Stress Incontinence. Mid-Urethral Tapes (Retropubic and Obturator)
") Operations for Stress Incontinence Mid-Urethral Tapes (Retropubic and Obturator) Patient Information Leaflet BSUG Patient Information Sheet Disclaimer This patient information sheet was put together by
Operations for Stress Incontinence Mid-Urethral Tapes (Retropubic and Obturator) Patient Information Leaflet BSUG Patient Information Sheet Disclaimer This patient information sheet was put together by
Sonographic Evaluation of Anatomic Results After the Pubovaginal Sling Procedure for Stress Urinary Incontinence
 Article Sonographic Evaluation of Anatomic Results After the Pubovaginal Sling Procedure for Stress Urinary Incontinence Hann-Chorng Kuo, MD Objective. To investigate the anatomic changes after the pubovaginal
Article Sonographic Evaluation of Anatomic Results After the Pubovaginal Sling Procedure for Stress Urinary Incontinence Hann-Chorng Kuo, MD Objective. To investigate the anatomic changes after the pubovaginal
Improving access and reducing costs of care for overactive bladder through a multidisciplinary delivery model
 Improving access and reducing costs of care for overactive bladder through a multidisciplinary delivery model Trafford Crump, Ph.D. Department of Surgery, University of Calgary Presentation to: Canadian
Improving access and reducing costs of care for overactive bladder through a multidisciplinary delivery model Trafford Crump, Ph.D. Department of Surgery, University of Calgary Presentation to: Canadian
Urinary Continence. Second edition FAST FACTS. by Julian Shah and Gary Leach. Anatomy and physiology 7. Investigations and diagnosis 11
 FAST FACTS Urinary Continence Second edition Indispensable Guides to by Julian Shah and Gary Leach Clinical Practice Anatomy and physiology 7 Investigations and diagnosis 11 Detrusor instability 28 Primary
FAST FACTS Urinary Continence Second edition Indispensable Guides to by Julian Shah and Gary Leach Clinical Practice Anatomy and physiology 7 Investigations and diagnosis 11 Detrusor instability 28 Primary
Research Article Inconsistencies Exist in National Estimates of Eye Care Services Utilization in the United States
 Ophthalmology Volume 2015, Article ID 435606, 4 pages http://dx.doi.org/10.1155/2015/435606 Research Article Inconsistencies Exist in National Estimates of Eye Care Services Utilization in the United States
Ophthalmology Volume 2015, Article ID 435606, 4 pages http://dx.doi.org/10.1155/2015/435606 Research Article Inconsistencies Exist in National Estimates of Eye Care Services Utilization in the United States
TRANSVAGINAL MESH TVM HEALTH CONCERNS AND LITIGATION
 TRANSVAGINAL MESH TVM HEALTH CONCERNS AND LITIGATION PRESENTED BY: THE PINKERTON LAW FIRM, PLLC The Pinkerton Law Firm is located in Houston, Texas. The firm specializes in mass tort litigation, including
TRANSVAGINAL MESH TVM HEALTH CONCERNS AND LITIGATION PRESENTED BY: THE PINKERTON LAW FIRM, PLLC The Pinkerton Law Firm is located in Houston, Texas. The firm specializes in mass tort litigation, including
Periurethral bulking agent for stress urinary incontinence (macroplastique)
") PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Who is this leaflet for? This leaflet provides information about having an injection
PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Who is this leaflet for? This leaflet provides information about having an injection
Urinary incontinence. The management of urinary incontinence in women. Issued: September 2013 last modified: January 2015. NICE clinical guideline 171
 Urinary incontinence The management of urinary incontinence in women Issued: September 2013 last modified: January 2015 NICE clinical guideline 171 guidance.nice.org.uk/cg171 NICE has accredited the process
Urinary incontinence The management of urinary incontinence in women Issued: September 2013 last modified: January 2015 NICE clinical guideline 171 guidance.nice.org.uk/cg171 NICE has accredited the process
Treatment for Stress Incontinence Patient Decision Aid
 Treatment for Stress Incontinence Patient Decision Aid Patient Information Author ID: JD/NS Leaflet Number: Gyn 056 Version: 1 Name of Leaflet: Treatment for stress incontinence - Patient decision aid
Treatment for Stress Incontinence Patient Decision Aid Patient Information Author ID: JD/NS Leaflet Number: Gyn 056 Version: 1 Name of Leaflet: Treatment for stress incontinence - Patient decision aid