Teeth extracting instruments
|
|
|
- Simon Cameron
- 7 years ago
- Views:
Transcription
1 Teeth extracting instruments Content of the lecture Teeth extracting instruments A. Dental elevators a. Component parts b. Types of elevators 1) the straight type 2) the triangle or pennant-shape type 3) the pick type The heavy version of the pick is the Crane pick the root-tip pick or the apex elevator B. Periotomes C. Extraction forceps a. Uses b. Component parts and the types of each part c. Maxillary forceps No. 150 No. 150A No. 1 forceps No. 53 right and left No. 88 right and left forceps No. 210S forceps No. 65, are also known as root-tip forceps No. 150S d. Mandibular forceps lower universal forceps or the No. 151 English style of vertical-hinge forceps No. 151A forceps No. 17 forceps No. 87, the so-called cowhorn forceps No. 151S forceps Prepared by Ali Mansur Ali Collage of dentistry university of kufa / Iraq For more, please visit my page at academia:
 teeth from surrounding bone.")
2 Teeth extracting instruments One of the most important instruments used in the extraction procedure is the dental elevator.these instruments are used to: 1- luxate (loosen) teeth from surrounding bone. 2- dental elevators are also used to expand alveolar bone 3- elevators are used to remove broken or surgically sectioned roots from their sockets. Dental Elevators The three major components of the elevator are (Figure 6-30).: 1) the handle : The handle of the elevator is usually of generous size. In some situations, cross-bar or T-bar handles are used. These instruments must be used with great caution because they can generate an excessive amount of force (Figure 6-31). 2) shank 3) blade
 teeth. The blade of the straight elevator has a concave surface on one side that is placed toward the tooth to be elevated.")
3 Types of Elevators The biggest variation in the type of elevator is in the shape and size of the blade. The three basic types of elevators are: 1) the straight type (Figure 6-32).: is the most commonly used elevator to luxate (loosen) teeth. The blade of the straight elevator has a concave surface on one side that is placed toward the tooth to be elevated. The small straight elevator, No. 301, is frequently used for beginning the luxation of an erupted tooth before application of the forceps Larger straight elevators are used to displace roots from their sockets and are also used to luxate teeth that are more widely spaced or once a smaller-sized straight elevator becomes less effective. The most commonly used large straight elevator is the No. 34S, but the No. 46 and the No. 77R are also used occasionally.

4 2) the triangle or pennant-shape type (Figure 6-34).: The second most commonly used type of elevator is the triangular elevator. These elevators are provided in pairs: a left and a right. The triangular elevator is most useful when a broken root remains in the tooth socket and the adjacent socket is empty. A typical example would be when a mandibular first molar is fractured, leaving the distal root in the socket but the mesial root removed with the crown. The tip of the triangular elevator is placed into the socket, with the shank of the elevator resting on the buccal plate of bone. The elevator is then turned in a wheel-and-axle rotation, with the sharp tip of the elevator engaging the cementum of the remaining distal root; the elevator is then turned, and the root is delivered. How to use it the Cryer elevator is the most common type (pairs of these elevators are also commonly referred to as east-west elevators ). 3) the pick type, used to remove roots. Have two types: a) The heavy version of the pick is the Crane pick (Figure 6-35). This instrument is used as a lever to elevate a broken root from the tooth socket. Usually, it is necessary to drill a hole with a bur (purchase point) approximately 3 mm How to deep into the root just at the bony crest. use it The tip of the pick is then inserted into the hole, and with the buccal plate of bone as a fulcrum, the root is elevated from the tooth socket. b) the root-tip pick or the apex elevator (Figure 6-36). a delicate instrument that is used to tease small root tips from their sockets. It must be emphasized that this is a thin instrument and should not be used as a wheel-and axle or lever type of elevator such as the Cryer elevator or the Crane pick. How to use it The root tip pick is used to tease the very small root end of a tooth by inserting the tip into the periodontal ligament space between the root tip and the socket wall.

5 Periotomes (Figure 6-37). Periotomes are instruments used to extract teeth while preserving the anatomy of the tooth s socket. The general principle behind their useis to sever some of the periodontal ligaments of the tooth to facilitate its removal. How to use it The tip of the periotome blade is inserted into the periodontal ligament space and advanced using pressure in the apical direction along the long axis of the tooth. It is advanced about 2 to 3 millimeters (mm) and then removed and reinserted into an adjacent accessible site. The process is continued around the tooth, gradually advancing the depth of the periotome tip while progressing apically. Once sufficient severance of periodontal ligaments has been accomplished, the tooth is removed by using a dental elevator, extraction forceps, or both, taking care to avoid excessive expansion or fracture of bone.
 Ideally, forceps are used to lift elevator-luxated teeth from their sockets, rather than to pull teeth from their sockets. 3) They also can help to expand bone when properly used.")
6 Extraction Forceps The extraction forceps are instruments used for: 1) removing the tooth from alveolar bone. 2) Ideally, forceps are used to lift elevator-luxated teeth from their sockets, rather than to pull teeth from their sockets. 3) They also can help to expand bone when properly used. The basic components of dental extraction forceps are: (Figure 6-38) 1) the handle 2) hinge 3) beaks
.")
7 The handles of the forceps are held differently, depending on the position of the tooth to be removed: 1) Maxillary forceps are held with the palm underneath the forceps so that the beak is directed in a superior direction (Figure 6-39). 2) The forceps used for removal of mandibular teeth are held with the palm on top of the forceps so that the beak is pointed down toward teeth (Figure 6-40).
 The English preference is for a vertical hinge and a corresponding vertically positioned handle Thus, the English-style handle and hinge are used with the hand held in a vertical direction as")
8 Two distinct types of hinge present in the forceps: 1) The usual American type of forceps has a hinge in a horizontal direction and is used as has been described. 2) The English preference is for a vertical hinge and a corresponding vertically positioned handle Thus, the English-style handle and hinge are used with the hand held in a vertical direction as opposed to a horizontal direction.
9 The beaks of the extraction forceps are the source of the greatest variation among forceps. The beak is designed to adapt to the tooth root near the junction of the crown and root. It must be remembered that the beaks of the forceps are designed to be adapted to the root structure of the tooth and not to the crown of the tooth. The more closely the beaks of the forceps adapt to the tooth roots, the more efficient is the extraction and the lower is the chance for undesired outcomes. A final design variation is in the width of the beak: 1) Some forceps beaks are narrow because their primary use is to remove narrow teeth such as incisor teeth. Forceps designed to remove a lower incisor can theoretically be used to remove a lower molar, but the beaks are so narrow that they will be inefficient for that application. 2) Other forceps beaks are broader because the teeth they are designed to remove are substantially wider, for example, lower molar teeth. The broad molar forceps will not adapt to the narrow space occupied by the lower incisor and, therefore, cannot be used in that situation without damage to adjacent teeth. The beaks of forceps are angled such that they can be placed parallel to the long axis of the tooth, with the handle in a comfortable position. Therefore: 1) the beaks of maxillary forceps are usually parallel to the handles. 2) The beaks of mandibular forceps are usually set perpendicular to the handles, which allows the surgeon to reach lower teeth and maintain a comfortable, controlled position. Maxillary forceps The removal of maxillary teeth requires the use of instruments designed for single-rooted teeth and for teeth with three roots: 1) Maxillary incisors, canine teeth, and premolar teeth are considered single-rooted teeth. 2) The maxillary first premolar frequently has a bifurcated root, but because this occurs in the apical one third, it has no influence on the design of the forceps. 3) The maxillary molars have trifurcated roots, and there are extraction forceps that will adapt to that configuration. The types of maxillary forceps used for maxillary teeth: 1) single-rooted maxillary teeth No. 150 (Figure6-43). After proper elevation they are usually removed with maxillary universal forceps, usually No. 150 (Figure6-43). The No. 150 forceps are slightly S-shaped when viewed from the side and are essentially straight when viewed from above. The beaks of the forceps curve to meet only at the tip. The slight curve of the No. 150 allows the operator to comfortably reach not only incisors but also premolars. 2) maxillary premolar teeth No. 150A (Figure6-44) The beaks of the No. 150 forceps come in a style that has been modified slightly to form the No. 150A (Figure6-44) forceps useful for maxillary premolar teeth and should not be used for incisors because of its poor adaptation to the roots of incisors.
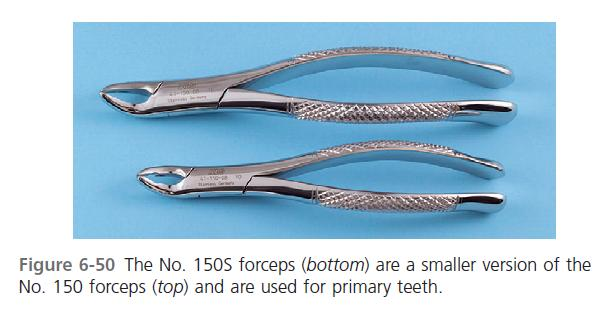
10 3) Maxillary incisors and canines The No. 1 forceps (Figure 6-45) which can be used for maxillary incisors and canines, are easier to use compared with the No. 150 for upper incisors. 4) Maxillary molar teeth the molar forceps come in pairs: a left and a right, because: Maxillary molar teeth are three-rooted teeth, with a single palatal root and a buccal bifurcation. Therefore, forceps that are specifically adapted to fit maxillary molars must have a smooth, concave surface for the palatal root and a beak with a pointed design that will fit into the buccal bifurcation. This requires that the molar forceps come in pairs: a left and a right. Additionally, the maxillary molar forceps should be offset so that the surgeon can reach the posterior aspect of the mouth and remain in the correct position. No. 53 right and left (Figure 6-46). The most commonly used molar forceps are the No. 53 right and left. These forceps are designed to fit anatomically around the palatal beak, and the pointed buccal beak fits into the buccal bifurcation. The beak is offset to allow for good surgeon positioning. No. 88 right and left forceps (Figure 6-47). A design variation is shown in the No. 88 right and left forceps, which have a longer, more accentuated, pointed beak formation. They are particularly useful for maxillary molars with crowns that are severely carious. The sharply pointed beaks may reach deeper into the trifurcation to sound dentin. The major disadvantage is that they crush crestal alveolar bone, and when used on intact teeth without due caution, fracture of large amounts of buccal alveolar bone may occur. The No. 210S forceps (Figure 6-48). On occasion, maxillary second molars and erupted third molars have a single conical root. In this situation, forceps with broad, smooth beaks that are offset from the handle can be useful. The No. 210S forceps exemplify this design. The No. 65, are also known as root-tip forceps (Figure 6-49). the offset molar forceps with very narrow beaks. These forceps are used primarily to remove broken maxillary molar roots but can be used for the removal of narrow premolars and for lower incisors. 5) maxillary primary (deciduous) teeth No. 150S (Figure 6-50). A smaller version of the No. 150 These forceps adapt well to all maxillary primary teeth and can be used as universal primary tooth forceps.

11

12

13 Prepared by Ali Mansur Ali Collage of dentistry university of kufa / Iraq For more, please visit my page at academia:
14
15 Mandibular forceps Extraction of mandibular teeth requires forceps that can be used for single-rooted teeth for the incisors, canines, and premolars, as well as for two-rooted teeth for the molars. The types of mandibular forceps used for mandibular teeth: 1) the single-rooted teeth lower universal forceps or the No. 151 (Figure 6-51). most commonly used for the single-rooted teeth. These forceps have handles similar in shape to the No. 150, but the beaks are pointed inferiorly for lower teeth. The beaks are smooth and narrow and meet only at the tip. This allows the beaks to fit near the cervical line of the tooth to grasp the root. English style of vertical-hinge forceps (Figure 6-53). can be used for the single-rooted teeth in the mandible Great force can be generated with these forceps. Unless great care is exercised, the incidence of root fracture is higher with this instrument. 2) Mandibular premolar teeth No. 151A forceps (Figure 6-52). These forceps should not be used for other lower teeth because their form prevents adaptation to the roots of teeth. 3) Mandibular molars Mandibular molars are bifurcated, two-rooted teeth that allow the use of forceps that anatomically adapt to the tooth. Because the bifurcation is on the buccal and the lingual sides, only a single molar forceps are necessary for the both sides, in contradistinction to the maxilla, for which a right- and left-paired molar forceps set is required. No. 17 forceps (Figure 6-54). Useful lower molar forceps. The beaks have pointed tips in the center to be set into the bifurcation of lower molar teeth. Because of the pointed tips, the No. 17 forceps cannot be used for molar teeth which have fused conical roots. No. 151 forceps used for molar teeth which have fused conical roots. No. 87, the so-called cowhorn forceps (Figure 6-55). Have major design variation These instruments are designed with two pointed, heavy beaks that enter the bifurcation of lower molars. After the forceps are seated into the correct position, usually while gently pumping the handles up and down, the tooth is actually elevated by squeezing the handles of the forceps together tightly. As the beaks are squeezed into the bifurcation, they use the buccal and lingual cortical plates as fulcrums, and the tooth can be literally squeezed out of the socket.

16 As with the English style of forceps, improper use of the cowhorn forceps can result in an increase in the incidence of untoward effects such as fractures of alveolar bone or damage to maxillary teeth if the forceps are not properly controlled by the surgeon as the molar exits the socket. The beginning surgeon should, therefore, use the cowhorn forceps with caution. 4) mandibular primary (deciduous) teeth The No. 151 is also adapted for primary teeth. No. 151S forceps (Figure 6-56). the same general design as the No. 151 but is scaled down to adapt to primary teeth. These forceps are adequate for the removal of all primary mandibular teeth

17

18 Prepared by Ali Mansur Ali Collage of dentistry university of kufa / Iraq For more, please visit my page at academia:
Fast and Predictable Tooth Extraction Technique
 Fast and Predictable Tooth Extraction Technique When I first saw the ads for Physics Forceps, I did not believe the claims could be true. At first glance, I didn t see how this strange looking instrument
Fast and Predictable Tooth Extraction Technique When I first saw the ads for Physics Forceps, I did not believe the claims could be true. At first glance, I didn t see how this strange looking instrument
CHAPTER 10 RESTS AND PREPARATIONS. 4. Serve as a reference point for evaluating the fit of the framework to the teeth.
 CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
SURGICAL EXTRACTIONS: TECHNIQUE AND CAUTIONS By Tony M. Woodward, DVM, AVDC
 SURGICAL EXTRACTIONS: TECHNIQUE AND CAUTIONS By Tony M. Woodward, DVM, AVDC We continue describing the five basic dental services that all general practitioners should be able to provide for their patients.
SURGICAL EXTRACTIONS: TECHNIQUE AND CAUTIONS By Tony M. Woodward, DVM, AVDC We continue describing the five basic dental services that all general practitioners should be able to provide for their patients.
Molar Uprighting Dr. Margherita Santoro Division of Orthodontics School of Dental and Oral surgery. Consequences of tooth loss.
 Molar Uprighting Dr. Margherita Santoro Division of Orthodontics School of Dental and Oral surgery Molars The wide occlusal surface is designed for food grinding. The surface needs to be aligned with the
Molar Uprighting Dr. Margherita Santoro Division of Orthodontics School of Dental and Oral surgery Molars The wide occlusal surface is designed for food grinding. The surface needs to be aligned with the
porcelain fused to metal crown
 Lectur.5 Dr.Adel F.Ibraheem porcelain fused to metal crown the most widely used fixed restoration,it is full metal crown having facial surface (or all surfaces) covered by ceramic material. It consist
Lectur.5 Dr.Adel F.Ibraheem porcelain fused to metal crown the most widely used fixed restoration,it is full metal crown having facial surface (or all surfaces) covered by ceramic material. It consist
Bitewing Radiography B.E. DIXON. B.D.S., M.Sc., D.P.D.S.
 Bitewing Radiography B.E. DIXON B.D.S., M.Sc., D.P.D.S. Main Indications Detection of Dental Caries Monitoring progression of caries Assessment of existing restorations Assessment of Periodontal status
Bitewing Radiography B.E. DIXON B.D.S., M.Sc., D.P.D.S. Main Indications Detection of Dental Caries Monitoring progression of caries Assessment of existing restorations Assessment of Periodontal status
Powertome Assisted Atraumatic Tooth Extraction
 Powertome Assisted Atraumatic Tooth Extraction White et al Jason White, DDS 1 2 3 Abstract Background: While traditional dental extraction techniques encourage minimal trauma, luxated elevation and forceps
Powertome Assisted Atraumatic Tooth Extraction White et al Jason White, DDS 1 2 3 Abstract Background: While traditional dental extraction techniques encourage minimal trauma, luxated elevation and forceps
Introduction to Dental Anatomy
 Introduction to Dental Anatomy Vickie P. Overman, RDH, MEd Continuing Education Units: N/A This continuing education course is intended for dental students and dental hygiene students. Maintaining the
Introduction to Dental Anatomy Vickie P. Overman, RDH, MEd Continuing Education Units: N/A This continuing education course is intended for dental students and dental hygiene students. Maintaining the
SURGICAL MANUAL. Step By Step Techniques
 SURGICAL MANUAL Step By Step Techniques TABLE OF CONTENTS PRE-SURGICAL 1 8 MEASUREMENT OF BONE.......................... 2 BONE CLASSIFICATION........................... 3 IMPLANT SIZE SELECTION.........................
SURGICAL MANUAL Step By Step Techniques TABLE OF CONTENTS PRE-SURGICAL 1 8 MEASUREMENT OF BONE.......................... 2 BONE CLASSIFICATION........................... 3 IMPLANT SIZE SELECTION.........................
DEVELOPMENT AND GROWTH OF THE MANDIBLE
 2012-2013 ORAL BIOLOGY DEVELOPMENT AND GROWTH OF THE MANDIBLE Ass. Prof. Dr. Heba M. Elsabaa Development and Growth of the Mandible DEVELOPMENT OF THE MANDIBLE The Mandible Is the largest and strongest
2012-2013 ORAL BIOLOGY DEVELOPMENT AND GROWTH OF THE MANDIBLE Ass. Prof. Dr. Heba M. Elsabaa Development and Growth of the Mandible DEVELOPMENT OF THE MANDIBLE The Mandible Is the largest and strongest
A. DEVELOPMENT OF THE DENTAL ORGAN (ENAMEL ORGAN):
:") A. DEVELOPMENT OF THE DENTAL ORGAN (ENAMEL ORGAN): AS EARLY AS THE SECOND MONTH OF FETAL LIFE, THE DEVELOPMENT OF THE DECIDUOUS TEETH MAY FIRST BECOME EVIDENT. 1. Dental lamina and Bud stage At about six
A. DEVELOPMENT OF THE DENTAL ORGAN (ENAMEL ORGAN): AS EARLY AS THE SECOND MONTH OF FETAL LIFE, THE DEVELOPMENT OF THE DECIDUOUS TEETH MAY FIRST BECOME EVIDENT. 1. Dental lamina and Bud stage At about six
In Class IV arch: Fulcrum line passes through two abutments adjacent to single edentulous space.
 It is that part of removable partial denture which assists the direct retainers in preventing displacement of distal extension denture bases by resisting lever action from the opposite side of the fulcrum
It is that part of removable partial denture which assists the direct retainers in preventing displacement of distal extension denture bases by resisting lever action from the opposite side of the fulcrum
Implants in your Laboratory: Abutment Design
 1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
Headgear Appliances. Dentofacial Orthopedics and Orthodontics. A Common Misconception. What is Headgear? Ideal Orthodontic Treatment Sequence
 Ideal Orthodontic Treatment Sequence Headgear Appliances Natalie A. Capan, D.M.D. 580 Sylvan Avenue, Suite 1M Englewood Cliffs, New Jersey 07632 (201)569-9055 www.capanorthodontics.com CapanOrtho@nj.rr.com
Ideal Orthodontic Treatment Sequence Headgear Appliances Natalie A. Capan, D.M.D. 580 Sylvan Avenue, Suite 1M Englewood Cliffs, New Jersey 07632 (201)569-9055 www.capanorthodontics.com CapanOrtho@nj.rr.com
Classification of Malocclusion
 Classification of Malocclusion What s going on here? How would you describe this? Dr. Robert Gallois REFERENCE: Where Do We Begin? ESSENTIALS FOR ORTHODONTIC PRACTICE By Riolo and Avery Chapter 6 pages
Classification of Malocclusion What s going on here? How would you describe this? Dr. Robert Gallois REFERENCE: Where Do We Begin? ESSENTIALS FOR ORTHODONTIC PRACTICE By Riolo and Avery Chapter 6 pages
IMPLANT DENTISTRY EXAM BANK
 IMPLANT DENTISTRY EXAM BANK 1. Define osseointegration. (4 points, 1/4 2. What are the critical components of an acceptable clinical trial? (10 points) 3. Compare the masticatory performance of individuals
IMPLANT DENTISTRY EXAM BANK 1. Define osseointegration. (4 points, 1/4 2. What are the critical components of an acceptable clinical trial? (10 points) 3. Compare the masticatory performance of individuals
Calibrated Periodontal Probes and Basic Probing Technique
 Module 11 Calibrated Periodontal Probes and Basic Probing Technique MODULE OVERVIEW This module presents the (1) design characteristics of calibrated periodontal probes and (2) step-by-step instructions
Module 11 Calibrated Periodontal Probes and Basic Probing Technique MODULE OVERVIEW This module presents the (1) design characteristics of calibrated periodontal probes and (2) step-by-step instructions
Complications Associated with Tooth Extraction
 1 Complications Associated with Tooth Extraction Mark M. Smith, VMD, DACVS, DAVDC Center for Veterinary Dentistry and Oral Surgery 9041 Gaither Road Gaithersburg, MD 20877 Introduction Tooth extraction
1 Complications Associated with Tooth Extraction Mark M. Smith, VMD, DACVS, DAVDC Center for Veterinary Dentistry and Oral Surgery 9041 Gaither Road Gaithersburg, MD 20877 Introduction Tooth extraction
The extraction of teeth in Pets
 Ban0108_043-050 2/1/08 8:51 AM Page 43 Techniques for dental extractions Refined techniques allow practitioners to perform successful extractions and enhance a Pet s well-being. The extraction of teeth
Ban0108_043-050 2/1/08 8:51 AM Page 43 Techniques for dental extractions Refined techniques allow practitioners to perform successful extractions and enhance a Pet s well-being. The extraction of teeth
General Technique of Third Molar Removal
 Oral Maxillofacial Surg Clin N Am 19 (2007) 23 43 General Technique of Third Molar Removal Sam E. Farish, DMD a,b, *, Gary F. Bouloux, MD, BDS, MDSc, FRACDS, FRACDS(OMS) b a Division of Oral and Maxillofacial
Oral Maxillofacial Surg Clin N Am 19 (2007) 23 43 General Technique of Third Molar Removal Sam E. Farish, DMD a,b, *, Gary F. Bouloux, MD, BDS, MDSc, FRACDS, FRACDS(OMS) b a Division of Oral and Maxillofacial
Full Crown Module: Learner Level 1
 Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / 30 Extensions: Porcelain Fused to Metal (PFM) / 12 All Ceramic / 8 Learner Level 1 Mastery of Tooth Preparation Estimated Set Up Time: 30
Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / 30 Extensions: Porcelain Fused to Metal (PFM) / 12 All Ceramic / 8 Learner Level 1 Mastery of Tooth Preparation Estimated Set Up Time: 30
Periapical radiography
 8 Periapical radiography Periapical radiography describes intraoral techniques designed to show individual teeth and the tissues around the apices. Each film usually shows two to four teeth and provides
8 Periapical radiography Periapical radiography describes intraoral techniques designed to show individual teeth and the tissues around the apices. Each film usually shows two to four teeth and provides
Activity: Can You Identify the Age?
 Activity: Can You Identify the Age? Skeletons are good age markers because teeth and bones mature at fairly predictable rates. How Teeth Reveal Age For toddler to age 21, teeth are the most accurate age
Activity: Can You Identify the Age? Skeletons are good age markers because teeth and bones mature at fairly predictable rates. How Teeth Reveal Age For toddler to age 21, teeth are the most accurate age
Prosthodontist s Perspective
 Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION.
 CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION. ١ G.V. BLACK who is known as the father of operative dentistry,he classified carious lesions into groups according to their locations in permanent
CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION. ١ G.V. BLACK who is known as the father of operative dentistry,he classified carious lesions into groups according to their locations in permanent
Treatment planning for the class 0, 1A, 1B dental arches
 Treatment planning for the class 0, 1A, 1B dental arches Dr.. Peter Hermann Dr Reminder: Torquing movement on tooth supported denture : no movement Class 1 movement in one direction (depression) Class
Treatment planning for the class 0, 1A, 1B dental arches Dr.. Peter Hermann Dr Reminder: Torquing movement on tooth supported denture : no movement Class 1 movement in one direction (depression) Class
Anatomic Anomalies. Anomalies. Anomalies. Anomalies. Supernumerary Teeth. Supernumerary Teeth. Steven R. Singer, DDS 212.305.5674 srs2@columbia.
 Anatomic Anomalies Steven R. Singer, DDS 212.305.5674 srs2@columbia.edu Anomalies! Anomalies are variations in the:! Size! Morphology! Number! Eruption of the teeth Anomalies Anomalies There are two categories:!
Anatomic Anomalies Steven R. Singer, DDS 212.305.5674 srs2@columbia.edu Anomalies! Anomalies are variations in the:! Size! Morphology! Number! Eruption of the teeth Anomalies Anomalies There are two categories:!
Simplified Positioning for Dental Radiology
 Simplified Positioning for Dental Radiology Prepared by: Animal Dental Care Tony M. Woodward DVM, Dipl. AVDC 5520 N. Nevada Ave. Suite 150 Colorado Springs, CO 80918 (719) 536-9949 tw@wellpets.com www.wellpets.com
Simplified Positioning for Dental Radiology Prepared by: Animal Dental Care Tony M. Woodward DVM, Dipl. AVDC 5520 N. Nevada Ave. Suite 150 Colorado Springs, CO 80918 (719) 536-9949 tw@wellpets.com www.wellpets.com
Introduction of Removable Partial Denture - Design and Retention
 Introduction of Removable Partial Denture - Design and Retention By : Dr Zaihan Ariffin BDS(Malaya), GDCDent (Adelaide), Doctor of Clinical Dentistry (Adelaide), FRACDS (Australia) Type of denture Full
Introduction of Removable Partial Denture - Design and Retention By : Dr Zaihan Ariffin BDS(Malaya), GDCDent (Adelaide), Doctor of Clinical Dentistry (Adelaide), FRACDS (Australia) Type of denture Full
Universal Crown and Bridge Preparation
 Universal Crown and Bridge Preparation The All-Ceramic Crown Preparation Technique for Predictable Success According to Dr. Ronald E. Goldstein Expect the Best. Buy Direct. The Universal * Crown and Bridge
Universal Crown and Bridge Preparation The All-Ceramic Crown Preparation Technique for Predictable Success According to Dr. Ronald E. Goldstein Expect the Best. Buy Direct. The Universal * Crown and Bridge
LATERAL BONE EXPANSION FOR IMMEDIATE PLACEMENT OF ENDOSSEOUS DENTAL IMPLANTS
 LATERAL BONE EXPANSION FOR IMMEDIATE PLACEMENT OF ENDOSSEOUS DENTAL IMPLANTS Department of Oral Maxillofacial Surgery, Chisinau Abstract: The study included 10 using the split control expansion technique
LATERAL BONE EXPANSION FOR IMMEDIATE PLACEMENT OF ENDOSSEOUS DENTAL IMPLANTS Department of Oral Maxillofacial Surgery, Chisinau Abstract: The study included 10 using the split control expansion technique
Advanced Pediatric Emergency Medicine Assembly. March 11 14, 2013 Lake Buena Vista, FL
 Michael Witt, MD, MPH, FACEP Medical Director, Pediatric Emergency Medicine, New Hampshire's Hospital for Children Elliot Health System Advanced Pediatric Emergency Medicine Assembly March 11 14, 2013
Michael Witt, MD, MPH, FACEP Medical Director, Pediatric Emergency Medicine, New Hampshire's Hospital for Children Elliot Health System Advanced Pediatric Emergency Medicine Assembly March 11 14, 2013
Bone augmentation procedure without wound closure
 THE CREATION OF ATTACHED GINGIVA IMMEDIATELY AFTER EXTRACTION Bone augmentation procedure without wound closure One of the characteristics of wound healing after an extraction is that the alveolar process
THE CREATION OF ATTACHED GINGIVA IMMEDIATELY AFTER EXTRACTION Bone augmentation procedure without wound closure One of the characteristics of wound healing after an extraction is that the alveolar process
Dental-based Injuries
 Dental-based Injuries LUXATIONS CROWN FRACTURE CROWN/ROOT FRACTURE ROOT FRACTURE ALVEOLAR BONE FRACTURE AVULSIONS LUXATIONS The tooth is loose, now what? 1. Concussive-not loose or displaced, but tender
Dental-based Injuries LUXATIONS CROWN FRACTURE CROWN/ROOT FRACTURE ROOT FRACTURE ALVEOLAR BONE FRACTURE AVULSIONS LUXATIONS The tooth is loose, now what? 1. Concussive-not loose or displaced, but tender
Removable Partial Dentures 101 Back to the Basics. Luther A. Ison, CDT University of Minnesota School of Dentistry
 Removable Partial Dentures 101 Back to the Basics Luther A. Ison, CDT University of Minnesota School of Dentistry Anterior-Posterior Palatal Strap Major connector Lingual Bar Major Connector, Kennedy Class
Removable Partial Dentures 101 Back to the Basics Luther A. Ison, CDT University of Minnesota School of Dentistry Anterior-Posterior Palatal Strap Major connector Lingual Bar Major Connector, Kennedy Class
CLASSIFICATION OF REMOVABLE PARTIAL DENTURES
 Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Table of Contents Section 6 Table of Contents
 Table of Contents Section Table of Contents Victory Series First Molar Bands...2 Victory Series Second Molar Bands... Unitek General Purpose Molar Bands...10 Unitek Pedodontic Molar Bands...11 Unitek Proportioned
Table of Contents Section Table of Contents Victory Series First Molar Bands...2 Victory Series Second Molar Bands... Unitek General Purpose Molar Bands...10 Unitek Pedodontic Molar Bands...11 Unitek Proportioned
Dental Updates. Excerpted Article e-mail: re777@comcast.net. Why Implant Screws Loosen Part 1. Richard Erickson, MS, DDS
 ¼ ½ ¾ µ mw/cm 2 Volume 17; 2007 Dental Updates "CUTTING EDGE INFORMATION FOR THE DENTAL PROFESSIONAL " 200 SEMINARS AND 30 JOURNALS REVIEWED YEARLY FOR THE LATEST, CUTTING EDGE INFORMATION Excerpted Article
¼ ½ ¾ µ mw/cm 2 Volume 17; 2007 Dental Updates "CUTTING EDGE INFORMATION FOR THE DENTAL PROFESSIONAL " 200 SEMINARS AND 30 JOURNALS REVIEWED YEARLY FOR THE LATEST, CUTTING EDGE INFORMATION Excerpted Article
Dental Anatomy: A Review
 Dental Anatomy: A Review Antoinette Metivier, CDA; Kimberly Bland, CDA, EFDA, M.Ed. Continuing Education Units: 2 hours Disclaimer: Participants must always be aware of the hazards of using limited knowledge
Dental Anatomy: A Review Antoinette Metivier, CDA; Kimberly Bland, CDA, EFDA, M.Ed. Continuing Education Units: 2 hours Disclaimer: Participants must always be aware of the hazards of using limited knowledge
Healing Abutment Selection. Perio Implant Part I. Implant Surface Characteristics. Single Tooth Restorations. Credit and Thanks for Lecture Material
 Healing Abutment Selection Perio Implant Part I Credit and Thanks for Lecture Material Implant Surface Characteristics!CAPT Robert Taft!CAPT Greg Waskewicz!Periodontal Residents NPDS and UMN!Machined Titanium!Tiunite!Osseotite
Healing Abutment Selection Perio Implant Part I Credit and Thanks for Lecture Material Implant Surface Characteristics!CAPT Robert Taft!CAPT Greg Waskewicz!Periodontal Residents NPDS and UMN!Machined Titanium!Tiunite!Osseotite
Secondary dentition permanent teeth - 32. Primary dentition deciduous teeth - 20
 Department of Histology and Embryology, P. J. Šafárik University, Medical Faculty, Košice DEVELOPMENT OF TEETH: Sylabus for foreign students Dental medicine Author: doc. MVDr. Iveta Domoráková, PhD. Primary
Department of Histology and Embryology, P. J. Šafárik University, Medical Faculty, Košice DEVELOPMENT OF TEETH: Sylabus for foreign students Dental medicine Author: doc. MVDr. Iveta Domoráková, PhD. Primary
Principles of Partial Denture Design
 Principles of Partial Denture Design 1. Keep the RPD design as simple as possible Simple those design elements which promote function, esthetics, comfort, ease of fabrication, and ease of maintenance,
Principles of Partial Denture Design 1. Keep the RPD design as simple as possible Simple those design elements which promote function, esthetics, comfort, ease of fabrication, and ease of maintenance,
Technique Guide. Screw Removal Set. Instruments for removing Synthes screws.
 Technique Guide Screw Removal Set. Instruments for removing Synthes screws. Table of Contents Introduction Screw Removal Set 2 Surgical Technique Preoperative Planning and Preparation 6 Removal of Intact
Technique Guide Screw Removal Set. Instruments for removing Synthes screws. Table of Contents Introduction Screw Removal Set 2 Surgical Technique Preoperative Planning and Preparation 6 Removal of Intact
Cysts of the Jaws. Cyst. Types. Effects on adjacent structures. Non-Odontogenic cysts. Odontogenic Cysts
 Cyst A Cyst is a benign pathologic cavity filled with fluid, lined by epithelium, and surrounded by a connective tissue wall A = connective tissue wall Cysts of the Jaws B = epithelium Effects on adjacent
Cyst A Cyst is a benign pathologic cavity filled with fluid, lined by epithelium, and surrounded by a connective tissue wall A = connective tissue wall Cysts of the Jaws B = epithelium Effects on adjacent
Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6
 12 5 Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6 This final article in the series describes the modification of teeth to improve
12 5 Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6 This final article in the series describes the modification of teeth to improve
ATLANTIS abutments design guide CAD/CAM patient-specific abutments
 ATLANTIS abutments design guide CAD/CAM patient-specific abutments Contents Introduction 4 This manual helps you to explore all the benefits of ATLANTIS CAD/CAM patient-specific abutments. It gives you
ATLANTIS abutments design guide CAD/CAM patient-specific abutments Contents Introduction 4 This manual helps you to explore all the benefits of ATLANTIS CAD/CAM patient-specific abutments. It gives you
E. Richard Hughes, D.D.S.
 E. Richard Hughes, D.D.S. Docket No. FDA-2012-N-0677 Blade Form Endosseous Dental Implants E. Richard Hughes, D.D.S. 46440 Benedict Dr.,# 201 Sterling, Va. 20164 USA 703-444-1152 erhughesdds@aol.com Diplomate,
E. Richard Hughes, D.D.S. Docket No. FDA-2012-N-0677 Blade Form Endosseous Dental Implants E. Richard Hughes, D.D.S. 46440 Benedict Dr.,# 201 Sterling, Va. 20164 USA 703-444-1152 erhughesdds@aol.com Diplomate,
Camelid Dentistry. Stephen R. Purdy, DVM Director of Camelid Studies UMass Amherst President Nunoa Project Peru
 Camelid Dentistry Stephen R. Purdy, DVM Director of Camelid Studies UMass Amherst President Nunoa Project Peru Learning objectives To describe the normal dentition of camelids To explain common corrective
Camelid Dentistry Stephen R. Purdy, DVM Director of Camelid Studies UMass Amherst President Nunoa Project Peru Learning objectives To describe the normal dentition of camelids To explain common corrective
Congenital absence of mandibular second premolars
 CLINICIAN S CORNER Congenitally missing mandibular second premolars: Clinical options Vincent G. Kokich a and Vincent O. Kokich b Seattle, Wash Introduction: Congenital absence of mandibular second premolars
CLINICIAN S CORNER Congenitally missing mandibular second premolars: Clinical options Vincent G. Kokich a and Vincent O. Kokich b Seattle, Wash Introduction: Congenital absence of mandibular second premolars
What is a dental implant?
 What is a dental implant? Today, the preferred method of tooth replacement is a dental implant. They replace missing tooth roots and form a stable foundation for replacement teeth that look, feel and function
What is a dental implant? Today, the preferred method of tooth replacement is a dental implant. They replace missing tooth roots and form a stable foundation for replacement teeth that look, feel and function
Resorptive Changes of Maxillary and Mandibular Bone Structures in Removable Denture Wearers
 Resorptive Changes of Maxillary and Mandibular Bone Structures in Removable Denture Wearers Dubravka KnezoviÊ-ZlatariÊ Asja»elebiÊ Biserka LaziÊ Department of Prosthodontics School of Dental Medicine University
Resorptive Changes of Maxillary and Mandibular Bone Structures in Removable Denture Wearers Dubravka KnezoviÊ-ZlatariÊ Asja»elebiÊ Biserka LaziÊ Department of Prosthodontics School of Dental Medicine University
Histologic comparison of biologic width around teeth versus implants: The effect on bone preservation
 Clinical Histologic comparison of biologic width around teeth versus implants: The effect on bone preservation Kazuto Makigusa 1 Abstract Histological analysis of the biological width surrounding primate
Clinical Histologic comparison of biologic width around teeth versus implants: The effect on bone preservation Kazuto Makigusa 1 Abstract Histological analysis of the biological width surrounding primate
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment
 Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Southern California Veterinary Dental Specialties & Oral Surgery
 Southern California Veterinary Dental Specialties & Oral Surgery Dental Radiology a Primer January 29, 2015 Brook A. Niemiec, DVM Diplomate, American Veterinary Dental College Diplomate, European Veterinary
Southern California Veterinary Dental Specialties & Oral Surgery Dental Radiology a Primer January 29, 2015 Brook A. Niemiec, DVM Diplomate, American Veterinary Dental College Diplomate, European Veterinary
Removal of a fractured instrument with a new extractor: clinical cases
 Clinical Removal of a fractured instrument with a new extractor: clinical cases Dominique Martin 1 Introduction The fracture of a root canal instrument during endodontic treatment is a surgical accident
Clinical Removal of a fractured instrument with a new extractor: clinical cases Dominique Martin 1 Introduction The fracture of a root canal instrument during endodontic treatment is a surgical accident
MEDICAID DENTAL PROGRAMS CODING, POLICY AND RELATED FEE REVISION INFORMATION
 MEDICAID DENTAL PROGRAMS CODING, POLICY AND RELATED FEE REVISION INFORMATION Effective for dates of service on and after November 1, 2005, the following dental coding, policy and related fee revisions
MEDICAID DENTAL PROGRAMS CODING, POLICY AND RELATED FEE REVISION INFORMATION Effective for dates of service on and after November 1, 2005, the following dental coding, policy and related fee revisions
LESSON ASSIGNMENT. Topography of the Mouth and Tooth Structure. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Topography of the Mouth and Tooth Structure. LESSON ASSIGNMENT Paragraphs 3-1 through 3-9. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify
LESSON ASSIGNMENT LESSON 3 Topography of the Mouth and Tooth Structure. LESSON ASSIGNMENT Paragraphs 3-1 through 3-9. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify
Chapter 9: Instrument Sharpening
 Chapter 9: Instrument Sharpening There have been a number of interesting developments in periodontal treatment in the past few years. However, the cornerstone of periodontal treatment remains the mechanical
Chapter 9: Instrument Sharpening There have been a number of interesting developments in periodontal treatment in the past few years. However, the cornerstone of periodontal treatment remains the mechanical
Full Crown Module: Learner Level 3
 Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / mesially tilted 30 Extensions: Porcelain Fused to Metal (PFM) / lingually 21 All Ceramic / rotated 12 Learner Level 3 Preparation of Malpositioned
Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / mesially tilted 30 Extensions: Porcelain Fused to Metal (PFM) / lingually 21 All Ceramic / rotated 12 Learner Level 3 Preparation of Malpositioned
Seminar 10 expectations
 Seminar 10 expectations Diagnosis 1. Explain why the transverse dimensions are so important when doing mandibular advancement surgery? How do you determine if maxillary expansion is needed to accept the
Seminar 10 expectations Diagnosis 1. Explain why the transverse dimensions are so important when doing mandibular advancement surgery? How do you determine if maxillary expansion is needed to accept the
Maxillary Sinus. (Antrum of Higmore)
") Maxillary Sinus (Antrum of Higmore) The maxillary sinus is a pneumatic space. It is the largest bilateral air sinus located in the body of the maxilla and opens in the middle nasal meatus of the nasal
Maxillary Sinus (Antrum of Higmore) The maxillary sinus is a pneumatic space. It is the largest bilateral air sinus located in the body of the maxilla and opens in the middle nasal meatus of the nasal
ALL-CERAMIC DENTAL IMPLANT SOLUTIONS
 ALL-CERAMIC DENTAL IMPLANT SOLUTIONS Scientific Evidence Bone-to-implant contact of 78% at 3 months. One piece implant = no prosthetic connections References 1. One-year follow-up of first consecutive
ALL-CERAMIC DENTAL IMPLANT SOLUTIONS Scientific Evidence Bone-to-implant contact of 78% at 3 months. One piece implant = no prosthetic connections References 1. One-year follow-up of first consecutive
Maxillofacial Surgery Basics for the Dental Team: Part II
 Maxillofacial Surgery Basics for the Dental Team: Part II Natalie Kaweckyj, LDARF, CDA, CDPMA, COA, COMSA, MADAA, BA Continuing Education Units: 4 hours Oral and maxillofacial surgery (OMS) is one of the
Maxillofacial Surgery Basics for the Dental Team: Part II Natalie Kaweckyj, LDARF, CDA, CDPMA, COA, COMSA, MADAA, BA Continuing Education Units: 4 hours Oral and maxillofacial surgery (OMS) is one of the
OCCLUSION IN COMPLETE DENTURES
 1 OCCLUSION IN COMPLETE DENTURES C P Owen Introduction Occlusion has been described as the most important subject in all the disciplines of dentistry, and for good reason, because the way the teeth come
1 OCCLUSION IN COMPLETE DENTURES C P Owen Introduction Occlusion has been described as the most important subject in all the disciplines of dentistry, and for good reason, because the way the teeth come
Removing fixed prostheses using the ATD automatic crown and bridge remover
 Removing fixed prostheses using the ATD automatic crown and bridge remover By Dr. Ian E. Shuman, Baltimore, MD. Information provided by J. Morita USA When removing cemented provisionals and final fixed
Removing fixed prostheses using the ATD automatic crown and bridge remover By Dr. Ian E. Shuman, Baltimore, MD. Information provided by J. Morita USA When removing cemented provisionals and final fixed
Introduction to Charting. Tooth Surfaces: M = mesial D = distal O = Occlusal B = buccal F = facial I = incisal L = lingual
 Tooth Surfaces: M = mesial D = distal O = Occlusal B = buccal F = facial I = incisal L = lingual When combining tooth surfaces, as in defining cavity preparations or restorations, there are some spelling
Tooth Surfaces: M = mesial D = distal O = Occlusal B = buccal F = facial I = incisal L = lingual When combining tooth surfaces, as in defining cavity preparations or restorations, there are some spelling
Replacing Hopeless Retained Deciduous Teeth in Adults Utilizing Dental Implants: Concepts and Case Presentation
 Replacing Hopeless Retained Deciduous Teeth in Adults Utilizing Dental Implants: Concepts and Case Presentation by Michael Tischler, DDS Published: Dentistry Today November 2005 Photos at end of article
Replacing Hopeless Retained Deciduous Teeth in Adults Utilizing Dental Implants: Concepts and Case Presentation by Michael Tischler, DDS Published: Dentistry Today November 2005 Photos at end of article
ABSTRACT INTRODUCTION. Facial Esthetics. Dental Esthetics
 ABSTRACT The FACE philosophy is characterized by clearly defined treatment goals. This increases diagnostic ability and improves the quality and stability of the end result. The objective is to establish
ABSTRACT The FACE philosophy is characterized by clearly defined treatment goals. This increases diagnostic ability and improves the quality and stability of the end result. The objective is to establish
Implant Systems MAX LOGIC MONO. Today s name in tomorrow s implant technology
 Implant Systems MAX LOGIC MONO Today s name in tomorrow s implant technology Implant Systems Etgar Medical Implant Systems brings to the market an entire spectrum of dental implant products based on its
Implant Systems MAX LOGIC MONO Today s name in tomorrow s implant technology Implant Systems Etgar Medical Implant Systems brings to the market an entire spectrum of dental implant products based on its
INTRAOSSEOUS ANESTHESIA
 ENDODONTICS: Colleagues for Excellence Winter 2009 Bonus Material F INTRAOSSEOUS ANESTHESIA Intraosseous Anesthesia With the Stabident and X Tip Systems The intraosseous injection allows placement of a
ENDODONTICS: Colleagues for Excellence Winter 2009 Bonus Material F INTRAOSSEOUS ANESTHESIA Intraosseous Anesthesia With the Stabident and X Tip Systems The intraosseous injection allows placement of a
ORTHODONTIC MINI IMPLANTS Clinical procedure for positioning. Orthodontics and Implantology
 ORTHODONTIC MINI IMPLANTS Clinical procedure for positioning Orthodontics and Implantology 2 All rights are reserved. Any reproduction of the present publication is prohibited in whole or in part and by
ORTHODONTIC MINI IMPLANTS Clinical procedure for positioning Orthodontics and Implantology 2 All rights are reserved. Any reproduction of the present publication is prohibited in whole or in part and by
Influence of Biomechanical Factors on Restoration of Devitalized Teeth
 Influence of Biomechanical Factors on Restoration of Devitalized Teeth Adnan atoviê 1 Davor Seifert 1 Renata Poljak-Guberina 1 Boris KvasniËka 2 1 Department of Fixed Prosthodontics School of Dental Medicine
Influence of Biomechanical Factors on Restoration of Devitalized Teeth Adnan atoviê 1 Davor Seifert 1 Renata Poljak-Guberina 1 Boris KvasniËka 2 1 Department of Fixed Prosthodontics School of Dental Medicine
CLASS II AMALGAM. Design Principles
 CLASS II AMALGAM Design Principles CLASS II Class II cavitated caries lesions Class II cavitated caries lesions opaque white haloes identify areas of enamel undermining and decalcification from within
CLASS II AMALGAM Design Principles CLASS II Class II cavitated caries lesions Class II cavitated caries lesions opaque white haloes identify areas of enamel undermining and decalcification from within
Taking Out a Tooth. Before You Begin: Ask Questions! CHAPTER11
 159 CHAPTER11 Taking Out a Tooth Not every painful tooth needs to come out. You must decide how serious the problem is, and then decide if you can treat and save the tooth. Some problems such as root canal
159 CHAPTER11 Taking Out a Tooth Not every painful tooth needs to come out. You must decide how serious the problem is, and then decide if you can treat and save the tooth. Some problems such as root canal
Straumann Dental Implant System. Implant Selection Guide.
 Straumann Dental Implant System. Implant Selection Guide. STRAUMANN's IMPLANT PORTFOLIO The Straumann Dental Implant System offers two implant lines with diverse body and neck designs ranging from the
Straumann Dental Implant System. Implant Selection Guide. STRAUMANN's IMPLANT PORTFOLIO The Straumann Dental Implant System offers two implant lines with diverse body and neck designs ranging from the
1. day. New horizons in prevention and treatment of tooth impaction and tooth retention. Friday March 7 th, 2014
 1. day Friday March 7 th, 2014 New horizons in prevention and treatment of tooth impaction and tooth retention. 8.00 9.00 registration and coffee/bread 9.00 9.30 1 Classification of tooth eruption in disturbances
1. day Friday March 7 th, 2014 New horizons in prevention and treatment of tooth impaction and tooth retention. 8.00 9.00 registration and coffee/bread 9.00 9.30 1 Classification of tooth eruption in disturbances
Orthodontic mini-implants, or temporary anchorage devices
 Anchors, away by John Marshall Grady, DMD, Dan E. Kastner, DMD, and Matthew C. Gornick, DMD Drs. John Marshall Grady (center), Dan E. Kastner (left), and Matthew C. Gornick (right). Drs. John Marshall
Anchors, away by John Marshall Grady, DMD, Dan E. Kastner, DMD, and Matthew C. Gornick, DMD Drs. John Marshall Grady (center), Dan E. Kastner (left), and Matthew C. Gornick (right). Drs. John Marshall
Intraoral Radiographic Techniques
 Intraoral Radiographic Techniques Allan G. Farman, BDS, EdS., MBA, PhD; Sandra A. Kolsom, CDA-Emeritus, RDA; ADAA 2014 Council on Education Continuing Education Units: 4 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce119/ce119.aspx
Intraoral Radiographic Techniques Allan G. Farman, BDS, EdS., MBA, PhD; Sandra A. Kolsom, CDA-Emeritus, RDA; ADAA 2014 Council on Education Continuing Education Units: 4 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce119/ce119.aspx
Waxing up. Waxing up. Crown and bridgework. Friedrich Jetter Christian Pilz. Ideas for dental technology
 Waxing up Waxing up Crown and bridgework Friedrich Jetter Christian Pilz Ideas for dental technology Waxing-up units Waxing-up units Waxlectric II The Waxlectric II is an electrically regulated sculpting
Waxing up Waxing up Crown and bridgework Friedrich Jetter Christian Pilz Ideas for dental technology Waxing-up units Waxing-up units Waxlectric II The Waxlectric II is an electrically regulated sculpting
Expansion screws. Standard expansion screws. Expansion screw Mini. Expansion screw Mini
 Standard expansion screws Expansion screw Mini holes in body of screws for better retention in acrylic built-in stops prevent screws from coming apart Indication: for transversal expansion and distalization
Standard expansion screws Expansion screw Mini holes in body of screws for better retention in acrylic built-in stops prevent screws from coming apart Indication: for transversal expansion and distalization
In the past decade, there has been a remarkable
 TECHNO BYTES Principles of cosmetic dentistry in orthodontics: Part 1. Shape and proportionality of anterior teeth David M. Sarver, DMD, MS Vestavia Hills, Ala In the past decade, there has been a remarkable
TECHNO BYTES Principles of cosmetic dentistry in orthodontics: Part 1. Shape and proportionality of anterior teeth David M. Sarver, DMD, MS Vestavia Hills, Ala In the past decade, there has been a remarkable
The gingival flap technique,
 Ban0108_034-041.qxd 2/1/08 4:47 PM Page 34 Creating effective dental flaps Practitioners can use this surgery to visualize and treat dental problems. By Beatriz Woodall, DVM Contributing Author The gingival
Ban0108_034-041.qxd 2/1/08 4:47 PM Page 34 Creating effective dental flaps Practitioners can use this surgery to visualize and treat dental problems. By Beatriz Woodall, DVM Contributing Author The gingival
ORAL SURGERY ASSISTANCE
 CHAPTER 5 ORAL SURGERY ASSISTANCE INTRODUCTION Oral surgery deals with the surgical treatment or correction of diseases, defects, or injuries of the oral cavity, teeth, and adjacent tissues. A sound knowledge
CHAPTER 5 ORAL SURGERY ASSISTANCE INTRODUCTION Oral surgery deals with the surgical treatment or correction of diseases, defects, or injuries of the oral cavity, teeth, and adjacent tissues. A sound knowledge
Straumann Bone Level Tapered Implant Peer-to-peer communication
 Straumann Bone Level Tapered Implant Peer-to-peer communication Clinical cases April, 2015 Clinical Cases Case No. Site 1 Single unit; Anterior Maxilla 2 Multi-unit; Anterior Maxilla Implant placement
Straumann Bone Level Tapered Implant Peer-to-peer communication Clinical cases April, 2015 Clinical Cases Case No. Site 1 Single unit; Anterior Maxilla 2 Multi-unit; Anterior Maxilla Implant placement
Local Anesthesia in Oral Surgery. Animal Dental Care
 Local Anesthesia in Oral Surgery Presented by: Animal Dental Care Tony M. Woodward DVM, Dipl. AVDC 5520 N. Nevada Ave. Suite 150 Colorado Springs, CO 80918 (719) 536-9949 tw@wellpets.com www.wellpets.com
Local Anesthesia in Oral Surgery Presented by: Animal Dental Care Tony M. Woodward DVM, Dipl. AVDC 5520 N. Nevada Ave. Suite 150 Colorado Springs, CO 80918 (719) 536-9949 tw@wellpets.com www.wellpets.com
Dental Radiology Related With Pedodontics
 Dental Radiology Related With Pedodontics Presented by: Dr. Rajeev Kumar Singh Radiology The branch of medicine that deals with the use of X- rays and radioactive substances in the diagnosis and treatment
Dental Radiology Related With Pedodontics Presented by: Dr. Rajeev Kumar Singh Radiology The branch of medicine that deals with the use of X- rays and radioactive substances in the diagnosis and treatment
Friday 29 th April 2016
 8.00 9.00 Registration and coffee/bread 9.00 9.45 1. Status of Dental Traumatology worldwide. Is prevention realistic? Lars Andersson Presently almost all countries have published data on the dental trauma
8.00 9.00 Registration and coffee/bread 9.00 9.45 1. Status of Dental Traumatology worldwide. Is prevention realistic? Lars Andersson Presently almost all countries have published data on the dental trauma
The Obvious and the Obscure:Diagnostic Steps for Crack Confirmation
 Cracking the Cracked Tooth Code In response to your requests... At the end of each issue of ENDODONTICS: Colleagues for Excellence, the American Association of Endodontists (AAE) asks readers to send in
Cracking the Cracked Tooth Code In response to your requests... At the end of each issue of ENDODONTICS: Colleagues for Excellence, the American Association of Endodontists (AAE) asks readers to send in
Periodontal surgery report for crown lengthening of tooth number 24,25
 411 PDS Periodontal surgery report for crown lengthening of tooth number -Course director : Dr. Nahid Ashri - instructor: Dr.Fatin Awaratani - - Student Name: Hanadi Alyami Computer Number: K S U - D E
411 PDS Periodontal surgery report for crown lengthening of tooth number -Course director : Dr. Nahid Ashri - instructor: Dr.Fatin Awaratani - - Student Name: Hanadi Alyami Computer Number: K S U - D E
The Lower Free End Saddle (distal extension saddle)
") Giles Perryer 1997 I The Lower Free End Saddle (distal extension saddle) Free end saddle dentures move Excessive movement of the denture can cause pain, tissue damage, and complaints of instability and
Giles Perryer 1997 I The Lower Free End Saddle (distal extension saddle) Free end saddle dentures move Excessive movement of the denture can cause pain, tissue damage, and complaints of instability and
Development of Teeth
 Development of Teeth Dr. Khaldoun Darwich Specialist in Oral and Maxillo-Facial Surgery Hamburg University PhD Hamburg University Academic Teacher - Department of OMF Surgery in Damascus University Instructor
Development of Teeth Dr. Khaldoun Darwich Specialist in Oral and Maxillo-Facial Surgery Hamburg University PhD Hamburg University Academic Teacher - Department of OMF Surgery in Damascus University Instructor
Case Report(s): Uncomplicated Crown Fractures
: Uncomplicated Crown Fractures") Case Report(s): Uncomplicated Crown Fractures Tooth fractures can be classified as follows: Uncomplicated crown fracture = fracture limited to the crown of the tooth with dentin exposure but no pulp exposure.
Case Report(s): Uncomplicated Crown Fractures Tooth fractures can be classified as follows: Uncomplicated crown fracture = fracture limited to the crown of the tooth with dentin exposure but no pulp exposure.
Transportation and Lifting of Liquefied Gas Dewars
 Transportation and Lifting of Liquefied Gas Dewars FN000475/OJ 1 Fermilab uses liquefied gasses or cryogenics in various forms around the lab. These liquefied gasses are sometimes transported in large
Transportation and Lifting of Liquefied Gas Dewars FN000475/OJ 1 Fermilab uses liquefied gasses or cryogenics in various forms around the lab. These liquefied gasses are sometimes transported in large
Simple Machines. What are simple machines?
 Definitions to know: Simple Machines Work done when an applied force causes an object to move in the direction of the force Energy ability to cause change; can change the speed, direction, shape, or temperature
Definitions to know: Simple Machines Work done when an applied force causes an object to move in the direction of the force Energy ability to cause change; can change the speed, direction, shape, or temperature
The Mandibular Two-Implant Overdenture First-Choice. Standard of Care for the Edentulous Denture Patient
 The Mandibular Two-Implant Overdenture First-Choice Standard of Care for the Edentulous Denture Patient Joseph R. Carpentieri, DDS Dennis P. Tarnow, DDS ii Preface Preface The prosthetic management of
The Mandibular Two-Implant Overdenture First-Choice Standard of Care for the Edentulous Denture Patient Joseph R. Carpentieri, DDS Dennis P. Tarnow, DDS ii Preface Preface The prosthetic management of
Equine Dentistry. P.O.Box 10338, Salinas, CA, 93912
 Modern Equine, Inc. P.O.Box 10338, Salinas, CA, 93912 Phone: (831) 345-4895 Email: contact@modernequine.com Website: www.modernequine.com Equine Dentistry Horses and ponies are efficient herbivores and
Modern Equine, Inc. P.O.Box 10338, Salinas, CA, 93912 Phone: (831) 345-4895 Email: contact@modernequine.com Website: www.modernequine.com Equine Dentistry Horses and ponies are efficient herbivores and
Appropriate soft tissue closure represents a critical
 Periosteoplasty for Soft Tissue Closure and Augmentation in Preprosthetic Surgery: A Surgical Report Albino Triaca, Dr Med, Dr Med Dent 1 /Roger Minoretti, Dr Med, Dr Med Dent 1 / Mauro Merli, DMD 2 /Beat
Periosteoplasty for Soft Tissue Closure and Augmentation in Preprosthetic Surgery: A Surgical Report Albino Triaca, Dr Med, Dr Med Dent 1 /Roger Minoretti, Dr Med, Dr Med Dent 1 / Mauro Merli, DMD 2 /Beat
Introduction to Veterinary Dental Radiology. Animal Dental Care
 Introduction to Veterinary Dental Radiology Presented by: Animal Dental Care Tony M. Woodward DVM, Dipl. AVDC 5520 N. Nevada Ave. Suite 150 Colorado Springs, CO 80918 (719) 536-9949 tw@wellpets.com www.wellpets.com
Introduction to Veterinary Dental Radiology Presented by: Animal Dental Care Tony M. Woodward DVM, Dipl. AVDC 5520 N. Nevada Ave. Suite 150 Colorado Springs, CO 80918 (719) 536-9949 tw@wellpets.com www.wellpets.com
An overview of classification of dental trauma
 Review Article An overview of classification of dental trauma Sasikala Pagadala 1*, Deepti Chaitanya Tadikonda 2 1 Assistant Professor, Department t of Periodontics, Nanded Rural Dental College and Research
Review Article An overview of classification of dental trauma Sasikala Pagadala 1*, Deepti Chaitanya Tadikonda 2 1 Assistant Professor, Department t of Periodontics, Nanded Rural Dental College and Research