Key priorities for implementation are around the diagnosis of hypertension and the recommended use of Ambulatory Blood Pressure Monitoring (ABPM)
|
|
|
- Juniper Simpson
- 7 years ago
- Views:
Transcription
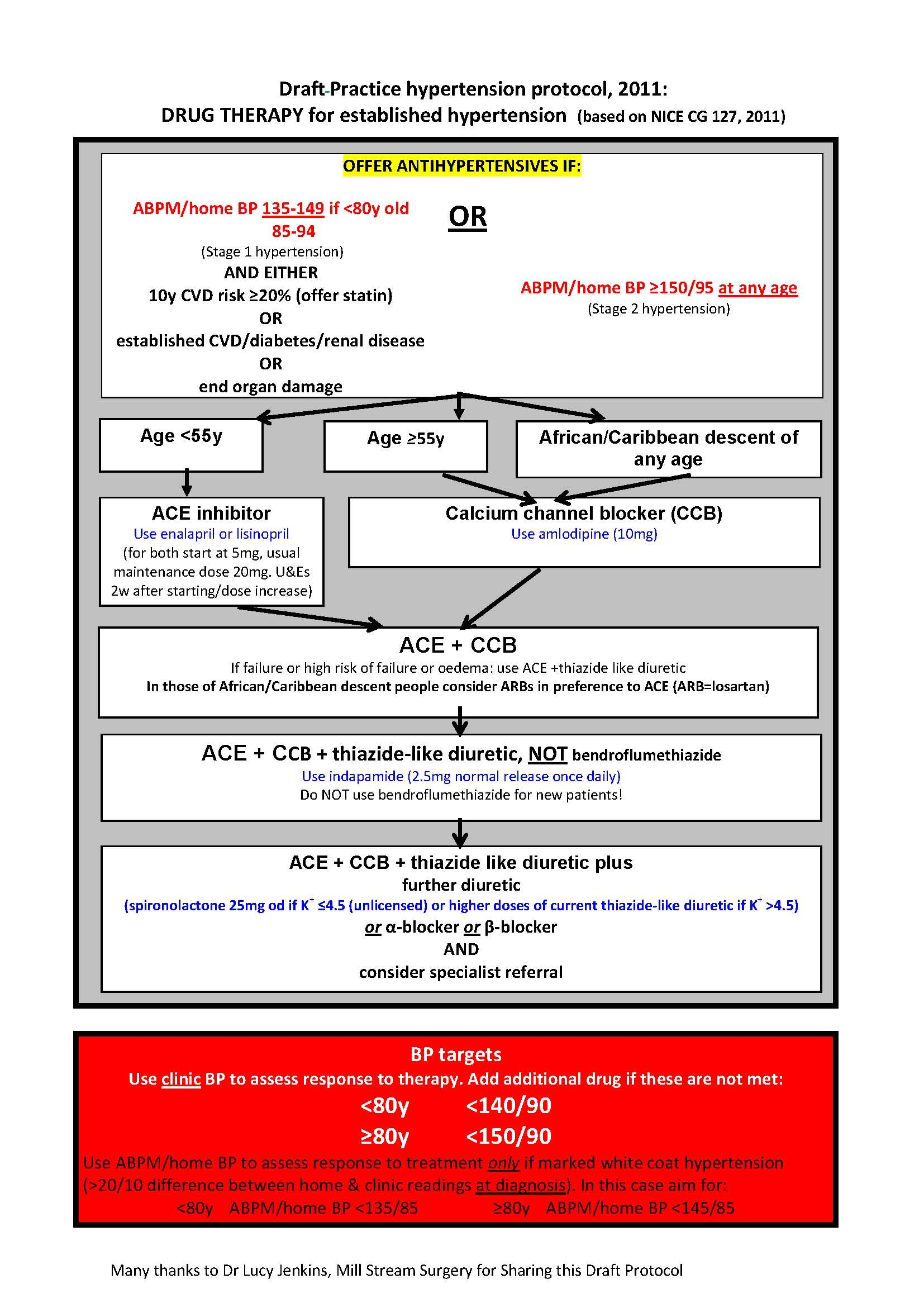
1 Date of issue: December 2011 Written by Sara Wilds & Kathryn Buchanan Prescribing Points A NEWSLETTER FOR ALL HEALTH CARE PROFESSIONALS IN OXFORDSHIRE, WRITTEN BY THE MEDICINES MANAGEMENT TEAM, OXFORDSHIRE PCT, JUBILEE HOUSE, OXFORD BUSINESS PARK SOUTH, OXFORD, OX4 2LH. VOLUME No: Hypertension. This issue covers updated guidance in the management of hypertension in light of NICE CG 127 and recommendations of the Oxfordshire Area Prescribing Committee November 2011 Hypertension - Background The risk associated with increasing blood pressure is continuous, with each 2 mmhg rise in systolic blood pressure associated with a 7% increased risk of mortality from ischaemic heart disease and a 10% increased risk of mortality from stroke. Routine periodic screening for high blood pressure is now commonplace in the UK as part of National Service Frameworks for cardiovascular disease prevention. Consequently, the diagnosis, treatment and follow-up of people with hypertension is one of the most common interventions in primary care, accounting for approximately 12% of Primary Care consultation episodes and approximately 1billion in drug costs in NICE published Clinical Guideline 127 Hypertension in August 2011 The scope being the clinical management of primary hypertension in adults (aged 18 years and older) who may, or may not, have pre-existing cardiovascular disease. Revised Definitions Stage 1 hypertension Clinic blood pressure is 140/90 mmhg or higher and subsequent ambulatory blood pressure monitoring (ABPM) daytime average or home blood pressure monitoring (HBPM) average blood pressure is 135/85 mmhg or higher. Stage 2 hypertension Clinic blood pressure is 160/100 mmhg or higher and subsequent ABPM daytime average or HBPM average blood pressure is 150/95 mmhg or higher. Severe hypertension Clinic systolic blood pressure is 180 mmhg or higher or clinic diastolic blood pressure is 110 mmhg or higher. Key priorities for implementation are around the diagnosis of hypertension and the recommended use of Ambulatory Blood Pressure Monitoring (ABPM) Evidence reviewed by NICE concludes that ABPM is better than home BP monitoring, which is better than clinic BP readings, both in terms of clinical outcomes (CV endpoints) and in terms of costs (QALYs). The NICE Guideline Development Group noted that based on current data, home BP monitoring could not be considered equivalent to ABPM with regard to accuracy of diagnosis and emphasised that that ABPM is the preferred means of confirming or refuting the diagnosis of hypertension. Action required: Practices should review their protocols for diagnosis of hypertension and ensure access to Ambulatory Blood Pressure Monitors. 1

2 If the clinic blood pressure is 140/90mmHg or higher after 2-3 readings, offer ambulatory blood pressure monitoring (ABPM) to confirm the diagnosis of hypertension. HBPM may be an alternative if ABPM not tolerated When using ABPM to confirm a diagnosis, ensure that at least two measurements per hour are taken during the person s usual waking hours (for example, between 08:00 and 22:00). Use the average value of at least 14 measurements. When using HBPM to confirm a diagnosis, ensure that for each blood pressure recording, two consecutive measurements are taken, at least 1 minute apart and with the person seated and blood pressure is recorded twice daily, ideally in the morning and evening and blood pressure recording continues for at least 4 days, ideally for 7 days. Discard the measurements taken on the first day and use the average value of all the remaining measurements to confirm a diagnosis of hypertension In patients with severe hypertension (>180/110) DO NOT wait for results of ABPM, start antihypertensive treatment immediately. If hypertension is not diagnosed but there is evidence of target organ damage such as left ventricular hypertrophy, albuminuria or proteinuria, consider carrying out investigations for alternative causes of the target organ damage. If hypertension is not diagnosed, measure the person s clinic blood pressure at least every 5 years subsequently, and consider measuring it more frequently if the person s clinic blood pressure is close to 140/90 mmhg CBPM 140/90 mmhg & ABPM/HBPM 135/85 mmhg Stage 1 hypertension CBPM 160/100 mmhg & ABPM/HBPM 150/95 mmhg Stage 2 hypertension Care pathway If target organ damage present or 10- year cardiovascular risk > 20% If younger than 40 years Consider specialist referral Offer antihypertensive drug treatment Offer lifestyle interventions Offer patient education and interventions to support adherence to treatment Offer annual review of care to monitor blood pressure, provide support and discuss lifestyle, symptoms and medication For people identified as having a white-coat effect (a discrepancy of more than 20/10 mmhg between clinic and average daytime ABPM or average HBPM blood pressure measurements at the time of diagnosis) consider ABPM or HBPM as an adjunct to clinic blood pressure measurements to monitor the response to antihypertensive treatment with lifestyle modification or drugs. Use clinic blood pressure measurements to monitor the response to antihypertensive treatment with lifestyle modifications or drugs. Aim for a target clinic blood pressure below 140/90 mmhg in people aged under 80 years with treated hypertension. Aim for a target clinic blood pressure below 150/90 mmhg in people aged 80 years and over, with treated hypertension. Aiming for as low as is tolerated will reduce the risk of a cardiac event or stroke 2

3 3
4 4
5 Changes to Drug Treatment Recommendations in line with NICE Give patients with isolated systolic hypertension (systolic BP 160 mmhg) the same treatment as patients with both raised systolic and diastolic BP. For patients > 80 years give the same treatment as patients aged 55 years. Take account of any co morbidity and concurrent drugs. For patients <55 remember ACE, ARBs are teratogenic and best avoided if there is the possibility of pregnancy ACEI and ARB If an ACEI is not tolerated because of cough, give a low cost ARB. Do NOT combine an ACEI with an ARB. Formulary choices:- ACE-I ramipril or lisinopril ARB losartan Calcium channel blocker CCBs are now the preferred treatment option at step 2 as they are cost effective. formulary choice:- amlodipine Diuretics Formulary choice for new patients indapamide 2.5mg once daily (or 1.5mg modified release once daily if side effects such as hypokalaemia). NB Bendroflumethiazide or hydrochlorothiazide are no longer the recommended thiazide-like diuretics for hypertension. For people already taking bendroflumethiazide or hydrochlorothiazide whose BP is stable; continue treatment. Additional treatment options at Step 4 Resistant hypertension (consider specialist advice) Spironolactone Doses of 25mg od may be a useful addition if serum potassium < 4.5mmol/L. Monitor for hyperkalaemia and hyponatraemia as well as renal function. Beta-blockers Beta-blockers are not recommended but can be used in step 1 for: younger people when an ACEI or ARB is contraindicated or not tolerated or, there is evidence of increased sympathetic drive or, in women of child-bearing potential. If a patient on a beta-blocker needs a second drug, add a CCB rather than a thiazide-like diuretic to reduce the risk of developing diabetes Formulary choice:- atenolol (bisoprolol if cardioselective preferred) Alpha-blockers Formulary choice:- doxazosin standard release NB. ALLHAT study showed an increased incidence of heart failure in patients taking doxazosin 5
6 Specialist Referral Refer the same day if: accelerated hypertension i.e. BP >180/110mm/Hg with signs of papilloedema and/or retinal haemorrhage, or suspected phaeochromocytoma. Consider referral in people with signs/symptoms suggesting a secondary cause of hypertension. For people aged under 40 years with stage 1 hypertension and no evidence of target organ damage, cardiovascular disease, renal disease or diabetes, consider seeking specialist evaluation of secondary causes of hypertension and a more detailed assessment of potential target organ damage. This is because 10-year cardiovascular risk assessments can underestimate the lifetime risk of cardiovascular events in these people Assessing target organ damage: updated recommendations For all people with hypertension offer to: initiatives to provide support and promote lifestyle change test urine for presence of protein take blood to measure glucose, electrolytes, creatinine, estimated glomerular filtration rate and lipid screen (fasting) examine fundi for hypertensive retinopathy arrange a 12-lead ECG CV Risk assessment Use a formal CV risk assessment (QRISK2) to discuss prognosis and management options. Assess CV risk in line with NICE CG67; Lipid modification Practice Priorities Review diagnosis and treatment pathways for people with hypertension in order to ensure in line with NICE CG 127 and APCO recommendations & ensure consistency within practice Ensure capacity to deliver ABPM to people who need it Consider use of potential 2011/12 Prescribing Incentive Scheme funds for purchase of ABPM through Oxfordshire wide bulk purchase option Ensure all blood pressure monitoring devices are properly validated, maintained and regularly calibrated 6
Hypertension Guidelines
 Overview Hypertension Guidelines Aim to reduce Blood Pressure to 140/90 or less (140/80 for diabetics), adding drugs as needed until further treatment is inappropriate or declined. N.B. patients do not
Overview Hypertension Guidelines Aim to reduce Blood Pressure to 140/90 or less (140/80 for diabetics), adding drugs as needed until further treatment is inappropriate or declined. N.B. patients do not
From www.gp update.co.uk one day courses for GPs, by GPs
 Hypertension From www.gp update.co.uk one day courses for GPs, by GPs NICE, in conjunction with the British Hypertension Society, have just published new guidelines on the management of hypertension (NICE
Hypertension From www.gp update.co.uk one day courses for GPs, by GPs NICE, in conjunction with the British Hypertension Society, have just published new guidelines on the management of hypertension (NICE
Hypertension. Clinical management of primary hypertension in adults. This guideline partially updates and replaces NICE clinical guideline 34
 Issue date: August 2011 Hypertension Clinical management of primary hypertension in adults This guideline partially updates and replaces NICE clinical guideline 34 NICE clinical guideline 127 Developed
Issue date: August 2011 Hypertension Clinical management of primary hypertension in adults This guideline partially updates and replaces NICE clinical guideline 34 NICE clinical guideline 127 Developed
Cardiovascular Risk in Diabetes
 Cardiovascular Risk in Diabetes Lipids Hypercholesterolaemia is an important reversible risk factor for cardiovascular disease and should be tackled aggressively in all diabetic patients. In Type 1 patients,
Cardiovascular Risk in Diabetes Lipids Hypercholesterolaemia is an important reversible risk factor for cardiovascular disease and should be tackled aggressively in all diabetic patients. In Type 1 patients,
HYPERTENSION ASSOCIATED WITH RENAL DISEASES
 RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
Hypertension and Heart Failure Medications. Dr William Dooley
 Hypertension and Heart Failure Medications Dr William Dooley Plan Heart Failure Acute vs. chronic Mx Hypertension Common drugs used Method of action Choice of medications Heart Failure Aims; Short term:
Hypertension and Heart Failure Medications Dr William Dooley Plan Heart Failure Acute vs. chronic Mx Hypertension Common drugs used Method of action Choice of medications Heart Failure Aims; Short term:
ADULT HYPERTENSION PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
Chronic Kidney Disease (CKD) Algorithm. Chronic Kidney Disease (CKD) Algorithm Page 1
 Algorithm. Chronic Kidney Disease (CKD) Algorithm Page 1") Chronic Kidney Disease (CKD) Algorithm Chronic Kidney Disease (CKD) Algorithm Page 1 Chronic Kidney Disease (CKD) Algorithm (See NICE Clinical Guideline CG73 1 and Quality Standards 2 ) Who should have
Chronic Kidney Disease (CKD) Algorithm Chronic Kidney Disease (CKD) Algorithm Page 1 Chronic Kidney Disease (CKD) Algorithm (See NICE Clinical Guideline CG73 1 and Quality Standards 2 ) Who should have
Case Study 6: Management of Hypertension
 Case Study 6: Management of Hypertension 2000 Scenario Mr Ellis is a fit 61-year-old, semi-retired market gardener. He is a moderate (10/day) smoker with minimal alcohol intake and there are no other cardiovascular
Case Study 6: Management of Hypertension 2000 Scenario Mr Ellis is a fit 61-year-old, semi-retired market gardener. He is a moderate (10/day) smoker with minimal alcohol intake and there are no other cardiovascular
Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria.
 Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Effects of a fixed combination of the ACE inhibitor, perindopril,
ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Effects of a fixed combination of the ACE inhibitor, perindopril,
DRUG UTILIZATION EVALUATION OF ANTIHYPERTENSIVE DRUGS IN DIABETIC PATIENTS WITH CKD
 WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES Elhami et al. SJIF Impact Factor 5.210 Volume 4, Issue 11, 1159-1166 Research Article ISSN 2278 4357 DRUG UTILIZATION EVALUATION OF ANTIHYPERTENSIVE
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES Elhami et al. SJIF Impact Factor 5.210 Volume 4, Issue 11, 1159-1166 Research Article ISSN 2278 4357 DRUG UTILIZATION EVALUATION OF ANTIHYPERTENSIVE
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8)
") Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) Adapted by Capital Health Plan Approved by Quality Improvement
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) Adapted by Capital Health Plan Approved by Quality Improvement
Measurement of Blood Pressure
 Measurement of Blood Pressure Ambulatory and Home Blood Pressure Monitoring BHS Non Medical Prescribing Update MSc. Management of Hypertension in Primary Care University of Birmingham February 2013 Louise
Measurement of Blood Pressure Ambulatory and Home Blood Pressure Monitoring BHS Non Medical Prescribing Update MSc. Management of Hypertension in Primary Care University of Birmingham February 2013 Louise
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #317: Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented National Quality Strategy Domain: Community / Population Health 2016 PQRS OPTIONS F INDIVIDUAL MEASURES:
Measure #317: Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented National Quality Strategy Domain: Community / Population Health 2016 PQRS OPTIONS F INDIVIDUAL MEASURES:
Hypertension Guideline V4
 Hypertension Guideline V4 Approved 24/06/2008 Version VERSION 4 FINAL Date of First Issue 26/02/08 Review Date 01/03/2010 Date of Issue 24/06/2008 EQIA Yes / No 24/06/2008 Author / Contact Dr Leslie Cruickshank
Hypertension Guideline V4 Approved 24/06/2008 Version VERSION 4 FINAL Date of First Issue 26/02/08 Review Date 01/03/2010 Date of Issue 24/06/2008 EQIA Yes / No 24/06/2008 Author / Contact Dr Leslie Cruickshank
Antihypertensive Drug Management to Achieve Systolic Blood Pressure <120 mmhg in SPRINT
 Antihypertensive Drug Management to Achieve Systolic Blood Pressure
Antihypertensive Drug Management to Achieve Systolic Blood Pressure
HIGH BLOOD PRESSURE AND YOUR KIDNEYS
 HIGH BLOOD PRESSURE AND YOUR KIDNEYS www.kidney.org About the Information in this Booklet Did you know that the National Kidney (NKF) Foundation offers guidelines and commentaries that help your healthcare
HIGH BLOOD PRESSURE AND YOUR KIDNEYS www.kidney.org About the Information in this Booklet Did you know that the National Kidney (NKF) Foundation offers guidelines and commentaries that help your healthcare
Guideline for Microalbuminuria Screening
 East Lancashire Diabetes Network Guideline for Microalbuminuria Screening Produced by: Task and Finish Group, Clinical Standards Group Produced: August 2006 Approved by: East Lancashire Diabetes Network
East Lancashire Diabetes Network Guideline for Microalbuminuria Screening Produced by: Task and Finish Group, Clinical Standards Group Produced: August 2006 Approved by: East Lancashire Diabetes Network
Correspondence to: Rima B Shah (rima_1223@yahoo.co.in) DOI: 10.5455/ijmsph.2013.2.167-172 Received Date: 29.11.2012 Accepted Date: 03.12.
 DOI: 10.5455/ijmsph.2013.2.167-172 Received Date: 29.11.2012 Accepted Date: 03.12.") RESEARCH ARTICLE STUDY OF UTILIZATION PATTERN OF ANTI-HYPERTENSIVE DRUGS IN HYPERTENSIVE DIABETIC PATIENTS WITH OR WITHOUT REDUCED RENAL FUNCTION AT TERTIARY CARE TEACHING HOSPITAL Jay Shah 1, Tejas Khakhkhar
RESEARCH ARTICLE STUDY OF UTILIZATION PATTERN OF ANTI-HYPERTENSIVE DRUGS IN HYPERTENSIVE DIABETIC PATIENTS WITH OR WITHOUT REDUCED RENAL FUNCTION AT TERTIARY CARE TEACHING HOSPITAL Jay Shah 1, Tejas Khakhkhar
Guidelines for the management of hypertension in patients with diabetes mellitus
 Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
4. Does your PCT provide structured education programmes for people with type 2 diabetes?
 PCT Prescribing Report Drugs used in Type 2 Diabetes Discussion Points 1. Does your PCT have a strategy for prevention of type 2 diabetes? Does your PCT provide the sort of intensive multifactorial lifestyle
PCT Prescribing Report Drugs used in Type 2 Diabetes Discussion Points 1. Does your PCT have a strategy for prevention of type 2 diabetes? Does your PCT provide the sort of intensive multifactorial lifestyle
SPECIALTY : CARDIOLOGY CLINICAL PROBLEM: HEART FAILURE
 SPECIALTY : CARDIOLOGY CLINICAL PROBLEM: HEART FAILURE Summary Heart failure has a worse prognosis than many cancers with an annual mortality of 40% in the first year following diagnosis and 10% thereafter.
SPECIALTY : CARDIOLOGY CLINICAL PROBLEM: HEART FAILURE Summary Heart failure has a worse prognosis than many cancers with an annual mortality of 40% in the first year following diagnosis and 10% thereafter.
Drug Treatment in Type 2 Diabetes with Hypertension
 Hypertension is 1.5 2 times more prevalent in Type 2 diabetes (prevalence up to 80 % in diabetic subjects). This exacerbates the risk of cardiovascular disease by ~ two-fold. Drug therapy reduces the risk
Hypertension is 1.5 2 times more prevalent in Type 2 diabetes (prevalence up to 80 % in diabetic subjects). This exacerbates the risk of cardiovascular disease by ~ two-fold. Drug therapy reduces the risk
High Blood Pressure and Your Kidneys
 High Blood Pressure and Your Kidneys About 65 million Americans have high blood pressure, but as many as one third or three in 10 don't even know it. There are usually no signs or symptoms that your blood
High Blood Pressure and Your Kidneys About 65 million Americans have high blood pressure, but as many as one third or three in 10 don't even know it. There are usually no signs or symptoms that your blood
Diabetic Nephropathy
 Diabetic Nephropathy Kidney disease is common in people affected by diabetes mellitus Definition Urinary albumin excretion of more than 300mg in a 24 hour collection or macroalbuminuria Abnormal renal
Diabetic Nephropathy Kidney disease is common in people affected by diabetes mellitus Definition Urinary albumin excretion of more than 300mg in a 24 hour collection or macroalbuminuria Abnormal renal
Understanding diabetes Do the recent trials help?
 Understanding diabetes Do the recent trials help? Dr Geoffrey Robb Consultant Physician and Diabetologist CMO RGA UK Services and Partnership Assurance AMUS 25 th March 2010 The security of experience.
Understanding diabetes Do the recent trials help? Dr Geoffrey Robb Consultant Physician and Diabetologist CMO RGA UK Services and Partnership Assurance AMUS 25 th March 2010 The security of experience.
Hypertension and Diabetes
 Hypertension and Diabetes C.W. Spellman, D.O., Ph.D., FACOI Professor & Associate Dean Research Dir. Center Diabetes & Metabolic Disorders Texas Tech University Health Science Center Midland-Odessa, Texas
Hypertension and Diabetes C.W. Spellman, D.O., Ph.D., FACOI Professor & Associate Dean Research Dir. Center Diabetes & Metabolic Disorders Texas Tech University Health Science Center Midland-Odessa, Texas
CHAPTER 8 ANTIHYPERTENSIVE DRUGS
 CHAPTER 8 ANTIHYPERTENSIVE DRUGS Classification 1. Diuretics. 2. Beta adrenergic blockers. 3. Calcium channel blockers. 4. Angiotensin converting enzyme inhibitors. 5. Angiotensin receptor blockers. 6.
CHAPTER 8 ANTIHYPERTENSIVE DRUGS Classification 1. Diuretics. 2. Beta adrenergic blockers. 3. Calcium channel blockers. 4. Angiotensin converting enzyme inhibitors. 5. Angiotensin receptor blockers. 6.
Special Communication
 Clinical Review & Education Special Communication 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eighth Joint National
Clinical Review & Education Special Communication 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eighth Joint National
Assess adherence with medication and lifestyle changes at every opportunity and intervene if necessary
 PPR thirty eight Prescribing Practice Review For Primary Care July 2007 Managing hypertension as a cardiovascular risk factor Key Messages Assess absolute cardiovascular risk and manage hypertension along
PPR thirty eight Prescribing Practice Review For Primary Care July 2007 Managing hypertension as a cardiovascular risk factor Key Messages Assess absolute cardiovascular risk and manage hypertension along
Diabetes and the Kidneys
 Diabetes and the Kidneys Aim(s) and objective(s) This guideline focuses on the detection, prevention, and management of kidney disease in people with diabetes. The management of end-stage renal disease
Diabetes and the Kidneys Aim(s) and objective(s) This guideline focuses on the detection, prevention, and management of kidney disease in people with diabetes. The management of end-stage renal disease
Treatment of Hypertension: JNC 8 and More
 PL Detail-Document #300201 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER February 2014 Treatment of
PL Detail-Document #300201 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER February 2014 Treatment of
Renal Disease in Type 2 Diabetes Mellitus
 Renal Disease in Type 2 Diabetes Mellitus 6th Collaborative DiGP/HSE/UCC Conference 25 th September 2013 Dr. Eoin O Sullivan Consultant Endocrinologist Bon Secours Hospital Cork Case 69 year old woman
Renal Disease in Type 2 Diabetes Mellitus 6th Collaborative DiGP/HSE/UCC Conference 25 th September 2013 Dr. Eoin O Sullivan Consultant Endocrinologist Bon Secours Hospital Cork Case 69 year old woman
High Blood Pressure (Essential Hypertension)
") Sacramento Heart & Vascular Medical Associates February 18, 2012 500 University Ave. Sacramento, CA 95825 Page 1 916-830-2000 Fax: 916-830-2001 What is essential hypertension? Blood pressure is the force
Sacramento Heart & Vascular Medical Associates February 18, 2012 500 University Ave. Sacramento, CA 95825 Page 1 916-830-2000 Fax: 916-830-2001 What is essential hypertension? Blood pressure is the force
In many diabetes units, people with type
 Renal Microalbuminuria: Screening and management in type 2 diabetes Julia Arundale Introduction In many diabetes units, patients with type 1 or type 2 diabetes are screened for proteinuria. Screening for
Renal Microalbuminuria: Screening and management in type 2 diabetes Julia Arundale Introduction In many diabetes units, patients with type 1 or type 2 diabetes are screened for proteinuria. Screening for
PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION
 Hull & East Riding Prescribing Committee PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION For guidance on Primary Prevention please see NICE guidance http://www.nice.org.uk/guidance/cg181
Hull & East Riding Prescribing Committee PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION For guidance on Primary Prevention please see NICE guidance http://www.nice.org.uk/guidance/cg181
Vascular Risk Reduction: Addressing Vascular Risk
 Vascular Risk Reduction: Addressing Vascular Risk Vascular Risk Reduction (VRR) Welcome! Presentation & Activities Focus: Managing known risk factors for vascular disease. Engage, collaborate and have
Vascular Risk Reduction: Addressing Vascular Risk Vascular Risk Reduction (VRR) Welcome! Presentation & Activities Focus: Managing known risk factors for vascular disease. Engage, collaborate and have
Trends in Prescribing of Drugs for Type 2 Diabetes in General Practice in England (Chart 1) Other intermediate and long-acting insulins
 Other intermediate and long-acting insulins") Type 2 Diabetes Type 2 diabetes is the most common form of diabetes, accounting for 90 95% of cases. 1 Charts 1 and 2 reflect the effect of increasing prevalence on prescribing and costs of products used
Type 2 Diabetes Type 2 diabetes is the most common form of diabetes, accounting for 90 95% of cases. 1 Charts 1 and 2 reflect the effect of increasing prevalence on prescribing and costs of products used
High Blood Pressure and Kidney Disease
 High Blood Pressure and Kidney Disease National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH The kidneys play a key
High Blood Pressure and Kidney Disease National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH The kidneys play a key
High Blood pressure and chronic kidney disease
 High Blood pressure and chronic kidney disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
High Blood pressure and chronic kidney disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
Using multiple biomarkers to predict renal and cardiovascular drug efficacy: Implications for drug development and registration
 Using multiple biomarkers to predict renal and cardiovascular drug efficacy: Implications for drug development and registration Hiddo Lambers Heerspink Department of Clinical Pharmacology University Medical
Using multiple biomarkers to predict renal and cardiovascular drug efficacy: Implications for drug development and registration Hiddo Lambers Heerspink Department of Clinical Pharmacology University Medical
Chronic Kidney Disease and the Electronic Health Record. Duaine Murphree, MD Sarah M. Thelen, MD
 Chronic Kidney Disease and the Electronic Health Record Duaine Murphree, MD Sarah M. Thelen, MD Definition of Chronic Kidney Disease (CKD) Defined by the National Kidney Foundation Either a decline in
Chronic Kidney Disease and the Electronic Health Record Duaine Murphree, MD Sarah M. Thelen, MD Definition of Chronic Kidney Disease (CKD) Defined by the National Kidney Foundation Either a decline in
Guidance for Industry Hypertension Indication: Drug Labeling for Cardiovascular Outcome Claims
 Guidance for Industry Hypertension Indication: Drug Labeling for Cardiovascular Outcome Claims U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research
Guidance for Industry Hypertension Indication: Drug Labeling for Cardiovascular Outcome Claims U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research
Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results
 Principal Results") Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results Paul K. Whelton, MB, MD, MSc Chair, SPRINT Steering Committee Tulane University School of Public Health and Tropical Medicine, and
Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results Paul K. Whelton, MB, MD, MSc Chair, SPRINT Steering Committee Tulane University School of Public Health and Tropical Medicine, and
Type 2 diabetes and hypertension in older adults:a case study
 If you would like to contribute to the art and science section contact: Gwen Clarke, art and science editor, Nursing Standard, The Heights, 59-65 Lowlands Road, Harrow-on-the-Hill, Middlesex HA1 3AW. email:
If you would like to contribute to the art and science section contact: Gwen Clarke, art and science editor, Nursing Standard, The Heights, 59-65 Lowlands Road, Harrow-on-the-Hill, Middlesex HA1 3AW. email:
Rivaroxaban: Prescribing Guidance for the treatment of provoked venous thromboembolism (VTE)
") Rivaroxaban: Prescribing Guidance for the treatment of provoked venous thromboembolism (VTE) Amber Drug Level 2 Leeds We have started your patient on rivaroxaban for the treatment of provoked VTE (deep
Rivaroxaban: Prescribing Guidance for the treatment of provoked venous thromboembolism (VTE) Amber Drug Level 2 Leeds We have started your patient on rivaroxaban for the treatment of provoked VTE (deep
Identifying and treating long-term kidney problems (chronic kidney disease)
") Understanding NICE guidance Information for people who use NHS services Identifying and treating long-term kidney problems (chronic kidney disease) NICE clinical guidelines advise the NHS on caring for
Understanding NICE guidance Information for people who use NHS services Identifying and treating long-term kidney problems (chronic kidney disease) NICE clinical guidelines advise the NHS on caring for
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates. January 30, 2014
 JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
Prescription Pattern of Anti Hypertensive Drugs used in Hypertensive Patients with Associated Type2 Diabetes Mellitus in A Tertiary Care Hospital
 Research Article Prescription Pattern of Anti Hypertensive Drugs used in Hypertensive Patients with Associated Type2 Diabetes Mellitus in A Tertiary Care Hospital *T. JANAGAN 1, R. KAVITHA 1, S. A. SRIDEVI
Research Article Prescription Pattern of Anti Hypertensive Drugs used in Hypertensive Patients with Associated Type2 Diabetes Mellitus in A Tertiary Care Hospital *T. JANAGAN 1, R. KAVITHA 1, S. A. SRIDEVI
High Blood Pressure and Chronic Kidney Disease. For People With CKD Stages 1 4
 High Blood Pressure and Chronic Kidney Disease For People With CKD Stages 1 4 National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation s Kidney
High Blood Pressure and Chronic Kidney Disease For People With CKD Stages 1 4 National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation s Kidney
Aggressive Lowering of Blood Pressure in type 2 Diabetes Mellitus: The Diastolic Cost
 Aggressive Lowering of Blood Pressure in type 2 Diabetes Mellitus: The Diastolic Cost Naftali Stern Institute of Endocrinology, Metabolism and Hypertension Tel Aviv -Sourasky Medical Center and Sackler
Aggressive Lowering of Blood Pressure in type 2 Diabetes Mellitus: The Diastolic Cost Naftali Stern Institute of Endocrinology, Metabolism and Hypertension Tel Aviv -Sourasky Medical Center and Sackler
Drug treatment of elevated blood pressure
 Drug treatment of elevated blood pressure Mark Nelson, Professor and Chair, Discipline of General Practice Professorial Research Fellow, and Senior Member, Menzies Research Institute, University of Tasmania,
Drug treatment of elevated blood pressure Mark Nelson, Professor and Chair, Discipline of General Practice Professorial Research Fellow, and Senior Member, Menzies Research Institute, University of Tasmania,
CDS Starter Kit: Diabetes f ollow-up care
 CDS Starter Kit: Diabetes f ollow-up care Introduction The delivery of high-quality diabetes care is a complex process that requires a provider to consider many pieces of patient information and treatment
CDS Starter Kit: Diabetes f ollow-up care Introduction The delivery of high-quality diabetes care is a complex process that requires a provider to consider many pieces of patient information and treatment
Combination Antihypertensive Therapy: When to use it Diabetes
 Combination Antihypertensive Therapy: When to use it Diabetes George L. Bakris, MD, F.A.S.N., F.A.S.H. Professor of Medicine Director, ASH Comprehensive Hypertension Center The University of Chicago Medicine
Combination Antihypertensive Therapy: When to use it Diabetes George L. Bakris, MD, F.A.S.N., F.A.S.H. Professor of Medicine Director, ASH Comprehensive Hypertension Center The University of Chicago Medicine
Chronic Illness Benefit application form 2016
 Chronic Illness Benefit application form 2016 This application form is to apply for the Chronic Illness Benefit and is only valid for 2016 Contact details Tel: 0860 116 116, PO Box 652509, Benmore 2010,
Chronic Illness Benefit application form 2016 This application form is to apply for the Chronic Illness Benefit and is only valid for 2016 Contact details Tel: 0860 116 116, PO Box 652509, Benmore 2010,
Board Review: Hypertension Cases
 Board Review: Hypertension Cases Cheryl L. Laffer, MD, PhD, FAHA Associate Professor of Medicine, Texas A&M HSC College of Medicine Senior Staff, S&W Nephrology / Hypertension (Remember, I didn t make
Board Review: Hypertension Cases Cheryl L. Laffer, MD, PhD, FAHA Associate Professor of Medicine, Texas A&M HSC College of Medicine Senior Staff, S&W Nephrology / Hypertension (Remember, I didn t make
Blood Pressure Medication. Barbara Pfeifer Diabetes Programs Manager
 United Indian Health Services Blood Pressure Medication Titration Program Barbara Pfeifer Diabetes Programs Manager Why a Medication titration program? Despite the many antihypertensive medications available,
United Indian Health Services Blood Pressure Medication Titration Program Barbara Pfeifer Diabetes Programs Manager Why a Medication titration program? Despite the many antihypertensive medications available,
Case Study 8: Heart Failure
 Case Study 8: Heart Failure April 2000 Scenario Mr James is a 68 year old man who presents to you for the first time complaining of increasing shortness of breath on exertion. He was prescribed frusemide
Case Study 8: Heart Failure April 2000 Scenario Mr James is a 68 year old man who presents to you for the first time complaining of increasing shortness of breath on exertion. He was prescribed frusemide
Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants
 Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers Relevant Licensed Indications
Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers Relevant Licensed Indications
From Concept to Rapid Visualization a Data Analytics Case Study
 From Concept to Rapid Visualization a Data Analytics Case Study Gregory Wozniak, PhD Director of Outcomes Analytics Health Outcomes Group American Medical Association The Journey Objectives Share experiences
From Concept to Rapid Visualization a Data Analytics Case Study Gregory Wozniak, PhD Director of Outcomes Analytics Health Outcomes Group American Medical Association The Journey Objectives Share experiences
CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE. Las Vegas, Nevada Bellagio March 4 6, 2016. Participating Faculty
 CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE Las Vegas, Nevada Bellagio March 4 6, 2016 Participating Faculty Friday, March 4th: 7:30 am - 8:00 am Registration and Hot Breakfast 8:00 am - 9:00 am Pulmonary
CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE Las Vegas, Nevada Bellagio March 4 6, 2016 Participating Faculty Friday, March 4th: 7:30 am - 8:00 am Registration and Hot Breakfast 8:00 am - 9:00 am Pulmonary
Easy or complex? University Pharmacy. Pharm.D. candidates, 2011
 High Blood Pressure Easy or complex? University Pharmacy Edwin Elliot, Insia Hussain Pharm.D. candidates, 2011 The evolution of mankind 2.5 mn years 50 years and we wonder why our healthcare costs are
High Blood Pressure Easy or complex? University Pharmacy Edwin Elliot, Insia Hussain Pharm.D. candidates, 2011 The evolution of mankind 2.5 mn years 50 years and we wonder why our healthcare costs are
HYPERTENSION MANAGEMENT AND SURVEILLANCE AT PRIMARY CARE LEVEL: A SITUATIONAL ANALYSIS IN THE LIMPOPO PROVINCE
 HYPERTENSION MANAGEMENT AND SURVEILLANCE AT PRIMARY CARE LEVEL: A SITUATIONAL ANALYSIS IN THE LIMPOPO PROVINCE by Dorothy Sekokotla Krisela Steyn Debbie Bradshaw Nolwazi Mbananga Burden of Disease Research
HYPERTENSION MANAGEMENT AND SURVEILLANCE AT PRIMARY CARE LEVEL: A SITUATIONAL ANALYSIS IN THE LIMPOPO PROVINCE by Dorothy Sekokotla Krisela Steyn Debbie Bradshaw Nolwazi Mbananga Burden of Disease Research
Palpitations & AF. Richard Grocott Mason Consultant Cardiologist THH NHS Foundation Trust & Royal Brompton & Harefield NHS Foundation Trust
 Palpitations & AF Richard Grocott Mason Consultant Cardiologist THH NHS Foundation Trust & Royal Brompton & Harefield NHS Foundation Trust Palpitations Frequent symptom Less than 50% associated with arrhythmia
Palpitations & AF Richard Grocott Mason Consultant Cardiologist THH NHS Foundation Trust & Royal Brompton & Harefield NHS Foundation Trust Palpitations Frequent symptom Less than 50% associated with arrhythmia
Managing diabetes in the post-guideline world. Dr Helen Snell Nurse Practitioner PhD, FCNA(NZ)
") Managing diabetes in the post-guideline world Dr Helen Snell Nurse Practitioner PhD, FCNA(NZ) Overview Pathogenesis of T2DM Aims of treatment The place of glycaemic control Strategies to improve glycaemic
Managing diabetes in the post-guideline world Dr Helen Snell Nurse Practitioner PhD, FCNA(NZ) Overview Pathogenesis of T2DM Aims of treatment The place of glycaemic control Strategies to improve glycaemic
Know your Numbers The D5 Goals for Diabetes Care. Shelly Hanson RN, CNS, CDE Cuyuna Regional Medical Center November 6, 2014
 Know your Numbers The D5 Goals for Diabetes Care Shelly Hanson RN, CNS, CDE Cuyuna Regional Medical Center November 6, 2014 The D5 What is it 5 different treatment goals identified for optimal diabetes
Know your Numbers The D5 Goals for Diabetes Care Shelly Hanson RN, CNS, CDE Cuyuna Regional Medical Center November 6, 2014 The D5 What is it 5 different treatment goals identified for optimal diabetes
High blood pressure and stroke
 Stroke Helpline: 0303 3033 100 Website: stroke.org.uk High blood pressure and stroke High blood pressure usually has no symptoms but it is the biggest risk factor for stroke. Both lifestyle changes and
Stroke Helpline: 0303 3033 100 Website: stroke.org.uk High blood pressure and stroke High blood pressure usually has no symptoms but it is the biggest risk factor for stroke. Both lifestyle changes and
High Blood Pressure and Chronic Kidney Disease
 High Blood Pressure and Chronic Kidney Disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
High Blood Pressure and Chronic Kidney Disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Hypertension in anaesthesia Dr Antonia C. Mayell Royal Devon and Exeter Hospital UK Email antoniamayell@hotmail.com
 Hypertension in anaesthesia Dr Antonia C. Mayell Royal Devon and Exeter Hospital UK Email antoniamayell@hotmail.com Self assessment Complete the following questions before reading this tutorial. 1. A 65yr
Hypertension in anaesthesia Dr Antonia C. Mayell Royal Devon and Exeter Hospital UK Email antoniamayell@hotmail.com Self assessment Complete the following questions before reading this tutorial. 1. A 65yr
SUMMARY OF CHANGES TO QOF 2015/16 - ENGLAND CLINICAL
 SUMMARY OF CHANGES TO QOF 2015/1 - ENGLAND KEY No change Retired/replaced Wording and/or change Point or threshold change Indicator ID change 14/15 QOF ID 15/1 QOF ID NICE ID Indicator wording Changes
SUMMARY OF CHANGES TO QOF 2015/1 - ENGLAND KEY No change Retired/replaced Wording and/or change Point or threshold change Indicator ID change 14/15 QOF ID 15/1 QOF ID NICE ID Indicator wording Changes
Getting the most from blood pressure medicines
 P R E S S U R E P O I N T S S E R I E S : NO. 4 Getting the most from blood pressure medicines B L O O D P R E S S U R E A S S O C I AT I O N Pressure Points series Pressure Points is a series of booklets
P R E S S U R E P O I N T S S E R I E S : NO. 4 Getting the most from blood pressure medicines B L O O D P R E S S U R E A S S O C I AT I O N Pressure Points series Pressure Points is a series of booklets
Southern Derbyshire Shared Care Pathology Guidelines. AKI guidelines for primary care
 Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE...2 FLOW DIAGRAM: POST AKI MANAGEMENT
Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE...2 FLOW DIAGRAM: POST AKI MANAGEMENT
CLINICAL GUIDELINE FOR SECONDARY PREVENTION AFTER STROKE OR TIA (PRIMARY AND SECONDARY CARE CORNWALL) MANAGEMENT 1. Aim/Purpose of this Guideline
 MANAGEMENT 1. Aim/Purpose of this Guideline") CLINICAL GUIDELINE FOR SECONDARY PREVENTION AFTER STROKE OR TIA (PRIMARY AND SECONDARY CARE CORNWALL) MANAGEMENT 1. Aim/Purpose of this Guideline The aim of this document to inform clinicians on management
CLINICAL GUIDELINE FOR SECONDARY PREVENTION AFTER STROKE OR TIA (PRIMARY AND SECONDARY CARE CORNWALL) MANAGEMENT 1. Aim/Purpose of this Guideline The aim of this document to inform clinicians on management
Heart Failure: Diagnosis and Treatment
 Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
The Hypertension Treatment Center
 Patricia F. Kao MD MS Asst Professor, EVMS Nephrology & HTN April 26, 2014 The Hypertension Treatment Center I have no conflicts of interest to disclose Objectives Describe the role of Hypertension Treatment
Patricia F. Kao MD MS Asst Professor, EVMS Nephrology & HTN April 26, 2014 The Hypertension Treatment Center I have no conflicts of interest to disclose Objectives Describe the role of Hypertension Treatment
Baskets of Care Diabetes Subcommittee
 Baskets of Care Diabetes Subcommittee Disclaimer: This background information is not intended to be a comprehensive scientific discussion of the topic, but rather an attempt to provide a baseline level
Baskets of Care Diabetes Subcommittee Disclaimer: This background information is not intended to be a comprehensive scientific discussion of the topic, but rather an attempt to provide a baseline level
Tackling the Semantic Interoperability challenge
 European Patient Summaries: What is next? Tackling the Semantic Interoperability challenge Dipak Kalra Cross-border health care The context for sharing health summaries Also useful for within-border health
European Patient Summaries: What is next? Tackling the Semantic Interoperability challenge Dipak Kalra Cross-border health care The context for sharing health summaries Also useful for within-border health
Hypertension Treatment Protocol
 Hypertension Treatment Protocol Need at least one baseline BP with one Pulse value, on 2 different days (if possible), to diagnose HTN. Exception: If need to please patient with some treatment and encourage
Hypertension Treatment Protocol Need at least one baseline BP with one Pulse value, on 2 different days (if possible), to diagnose HTN. Exception: If need to please patient with some treatment and encourage
Summary of QOF indicators
 Summary of QOF indicators Clinical domain Atrial fibrillation (AF) AF001. The contractor establishes and maintains a register of patients with atrial fibrillation AF002. The percentage of patients with
Summary of QOF indicators Clinical domain Atrial fibrillation (AF) AF001. The contractor establishes and maintains a register of patients with atrial fibrillation AF002. The percentage of patients with
EXPLORING THE INTERACTION BETWEEN EXERCISE AND MEDICATION FOR CHRONIC DISEASE: CONSIDERATIONS FOR FITNESS PROFESSIONALS
 EXPLORING THE INTERACTION BETWEEN EXERCISE AND MEDICATION FOR CHRONIC DISEASE: CONSIDERATIONS FOR FITNESS PROFESSIONALS Steven T. Johnson, PhD 1 Introduction The prevalence of chronic diseases like cardiovascular
EXPLORING THE INTERACTION BETWEEN EXERCISE AND MEDICATION FOR CHRONIC DISEASE: CONSIDERATIONS FOR FITNESS PROFESSIONALS Steven T. Johnson, PhD 1 Introduction The prevalence of chronic diseases like cardiovascular
North of Tyne Area Prescribing Committee
 North of Tyne Area Prescribing Committee ANTIPSYCHOTICS IN PSYCHOSIS, BIPOLAR DISORDER AND AUGMENTATION THERAPY IN TREATMENT RESISTANT DEPRESSION Information for Primary Care Updated November 2013 This
North of Tyne Area Prescribing Committee ANTIPSYCHOTICS IN PSYCHOSIS, BIPOLAR DISORDER AND AUGMENTATION THERAPY IN TREATMENT RESISTANT DEPRESSION Information for Primary Care Updated November 2013 This
Initiate Atorvastatin 20mg daily
 Type 2 Diabetes Patient Objectives Stopping Smoking BMI > 25 kg m² Control BP to
Type 2 Diabetes Patient Objectives Stopping Smoking BMI > 25 kg m² Control BP to
Dorset Cardiac Centre
 P a g e 1 Dorset Cardiac Centre Patients with Atrial Fibrillation/Flutter undergoing DC Cardioversion or Ablation procedures- Guidelines for Novel Oral Anti-coagulants (NOACS) licensed for this use February
P a g e 1 Dorset Cardiac Centre Patients with Atrial Fibrillation/Flutter undergoing DC Cardioversion or Ablation procedures- Guidelines for Novel Oral Anti-coagulants (NOACS) licensed for this use February
Let s Do It Well. Nurse Learning Pack
 Let s Do It Well Nurse Learning Pack Let s Do It Well Nurse Learning Pack Reviewed and agreed by the British Hypertension Society (BHS) and the Nurses Hypertension Association (NHA) HIT is an independent
Let s Do It Well Nurse Learning Pack Let s Do It Well Nurse Learning Pack Reviewed and agreed by the British Hypertension Society (BHS) and the Nurses Hypertension Association (NHA) HIT is an independent
ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY
 Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
GUIDELINES FOR THE TREATMENT OF DIABETIC NEPHROPATHY*
 71 GUIDELINES FOR THE TREATMENT OF DIABETIC NEPHROPATHY* Ryuichi KIKKAWA** Asian Med. J. 44(2): 71 75, 2001 Abstract: Diabetic nephropathy is the most devastating complication of diabetes and is now the
71 GUIDELINES FOR THE TREATMENT OF DIABETIC NEPHROPATHY* Ryuichi KIKKAWA** Asian Med. J. 44(2): 71 75, 2001 Abstract: Diabetic nephropathy is the most devastating complication of diabetes and is now the
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below
 RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below") Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Absolute cardiovascular disease risk
 Guidelines for the management of Absolute cardiovascular disease risk An initiative of the National Vascular Disease Prevention Alliance About the National Vascular Disease Prevention Alliance The National
Guidelines for the management of Absolute cardiovascular disease risk An initiative of the National Vascular Disease Prevention Alliance About the National Vascular Disease Prevention Alliance The National
Secondary Stroke Prevention Luke Bradbury, MD 10/4/14 Fall WAPA Conferfence
 Guidelines Secondary Stroke Prevention Luke Bradbury, MD 10/4/14 Fall WAPA Conferfence Stroke/TIA Nearly 700,000 ischemic strokes and 240,000 TIAs every year in the United States Currently, the risk for
Guidelines Secondary Stroke Prevention Luke Bradbury, MD 10/4/14 Fall WAPA Conferfence Stroke/TIA Nearly 700,000 ischemic strokes and 240,000 TIAs every year in the United States Currently, the risk for
Case study 28: Managing hypertension in diabetes
 Case study 28: Managing hypertension in diabetes October 2003 An Independent, Australian organisation for Quality Use of Medicines National Prescribing Service Limited ACN 082 034 393 Level 7/418A Elizabeth
Case study 28: Managing hypertension in diabetes October 2003 An Independent, Australian organisation for Quality Use of Medicines National Prescribing Service Limited ACN 082 034 393 Level 7/418A Elizabeth
Type 2 Diabetes workshop notes
 Group 1 notes Abi / Nicole Type 2 Diabetes workshop notes 4.1 Population The group discussed the following sub groups that may need addressing: Men-as they tend to die earlier compared with women, their
Group 1 notes Abi / Nicole Type 2 Diabetes workshop notes 4.1 Population The group discussed the following sub groups that may need addressing: Men-as they tend to die earlier compared with women, their
Absolute cardiovascular disease risk assessment
 Quick reference guide for health professionals Absolute cardiovascular disease risk assessment This quick reference guide is a summary of the key steps involved in assessing absolute cardiovascular risk
Quick reference guide for health professionals Absolute cardiovascular disease risk assessment This quick reference guide is a summary of the key steps involved in assessing absolute cardiovascular risk
HEART HEALTH WEEK 3 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease HEART FAILURE. Relatively mild, symptoms with intense exercise
 WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
Approaches to the Management of Difficult-to-Control Hypertension
 Approaches to the Management of Difficult-to-Control Theodore D Fraker, Jr, MD Professor of Medicine The Ohio State University Medical Center Orlando, Florida October 7-9, 2011 Case Study: DM 64 year old
Approaches to the Management of Difficult-to-Control Theodore D Fraker, Jr, MD Professor of Medicine The Ohio State University Medical Center Orlando, Florida October 7-9, 2011 Case Study: DM 64 year old
Survey of Canadian Physicians Use of anti-thrombotic therapy for Atrial Fibrillation
 Survey of Canadian Physicians Use of anti-thrombotic therapy for Atrial Fibrillation On the following pages are a number of questions asking about the conditions under which you would prescribe anticoagulation
Survey of Canadian Physicians Use of anti-thrombotic therapy for Atrial Fibrillation On the following pages are a number of questions asking about the conditions under which you would prescribe anticoagulation
Drug Treatment for People with Hypertension
 Treatment algorithm Drug treatment for essential HT Compelling indication / contraindication over choice of drug No Yes Go to Appendix 1 Start with either ACEI (or ARB if ACEI intolerant), calcium channel
Treatment algorithm Drug treatment for essential HT Compelling indication / contraindication over choice of drug No Yes Go to Appendix 1 Start with either ACEI (or ARB if ACEI intolerant), calcium channel