PROSTATE CANCER GRADING: An Update from the 2014 ISUP Consensus Conference
|
|
|
- Buddy Maxwell
- 7 years ago
- Views:
Transcription
1 PROSTATE CANCER GRADING: An Update from the 2014 ISUP Consensus Conference Dr. J. Merrimen Associate Professor Depts of Pathology and Urology Dalhousie University Div of AP Videoconference Feb 16, 2016
2 Disclosures None
3 Prostate Cancer Grading Review of Evolution of Prostate Cancer Grading 1966 Gleason Grading System for Prostate Cancer 2005 ISUP Modified Gleason Grading Proposal for New Grade Grouping ISUP Nov 2014: Prostate Cancer Grading Panel, Chicago Clarification of Previous ambiguous grading issues Intraductal carcinoma New Grade Grouping
4 Gleason Grading System 1966 Donald F. Gleason Based solely on architectural pattern Overall grade (Gleason score) based on sum of 2 most common patterns 86% had advanced disease PNB Sampling limited to a couple of large core biopsies directed to palpable abnormalities Before immunohistochemical stains that would highlight basal cells
5
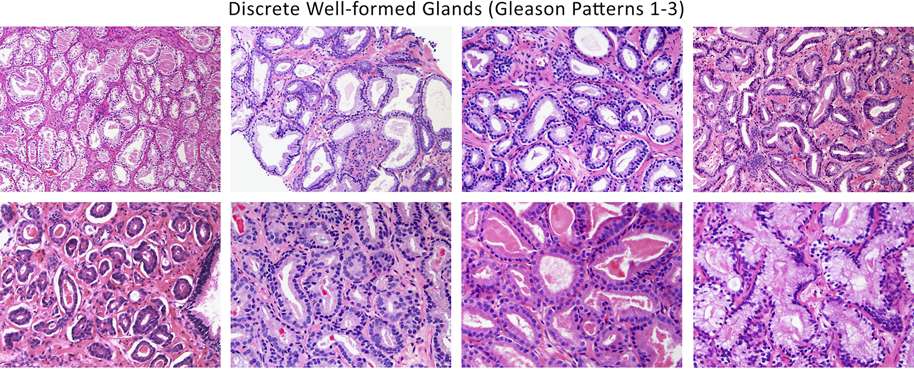
6 TABLE 1. Gleason System Original Gleason System: 1966 & 1967 Pattern 1: Very well differentiated, small, closely packed, uniform, glands in essentially circumscribed masses Pattern 2: Similar (to pattern 1) but with moderate variation in size and shape of glands and more atypia in the individual cells; cribriform pattern may be present, still essentially circumscribed, but more loosely arranged Pattern 3: Similar to pattern 2 but marked irregularity in size and shape of glands, with tiny glands or individual cells invading stroma away from circumscribed masses, or solid cords and masses with easily identifiable glandular differentiation within most of them Pattern 4: Large clear cells growing in a diffuse pattern resembling hypernephroma; may show gland formation Pattern 5: Very poorly differentiated tumors; usually solid masses or diffuse growth with little or no differentiation into glands Gleason s Modifications: 1974 & 1977 Patterns 1 & 2: Unchanged Pattern 3: Adds to earlier description: may be papillary or cribriform (1974), which vary in size and may be quite large, but the essential feature is the smooth and usually rounded edge around all the circumscribed masses of tumor (1977) Pattern 4: Adds to earlier description: raggedly infiltrating, fused-glandular tumor (1974); glands are not single and separate, but coalesce and branch (1977) Pattern 5: Adds to earlier description: can resemble comedocarcinoma of the breast (1977); almost absent gland pattern with few tiny glands or signet cells (1977)
7 Many cases are adenosis (mimic of PCa) Some cases HGPIN
8 ISUP 2005: Gleason Grading International group of more than 70 leading urological pathologists Attempt to achieve consensus in controversial areas related to the Gleason grading system New tools for grading prostate cancer: Diagram Written descriptions Reference images
9 2005
10
11

12 Gleason score = 3 nodule of cancer on TURP

13 Gleason score = 5 adenocarcinoma on needle biopsy

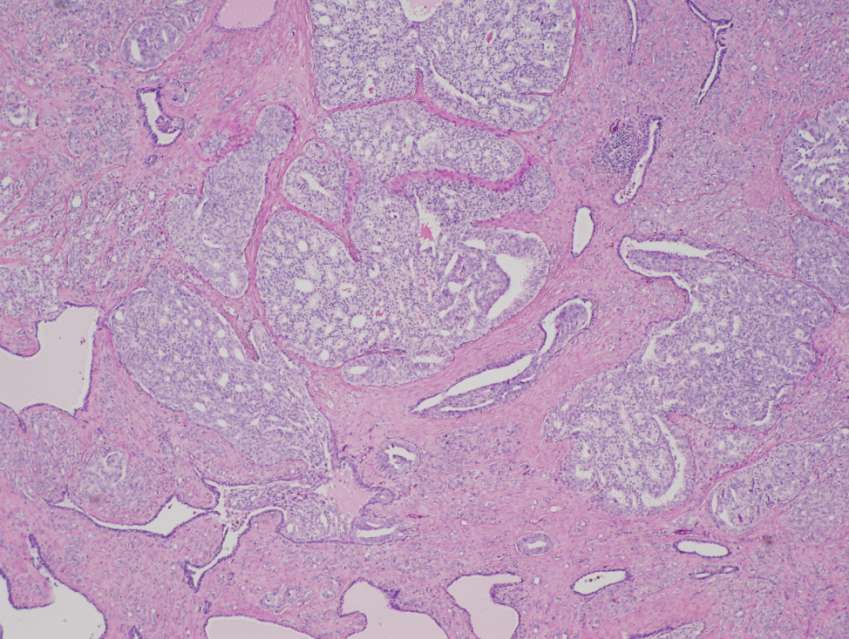
14 Gleason score = 6
15 Cribriform structures

16 Gleason score = 7 adenocarcinoma, where pattern 4 component consists of discrete yet poorly formed glands

17 Gleason score = 8 adenocarcinoma with fused glands

18 Gleason score = 8 with large irregular cribriform glands

19 Gleason grade 5+4 = score of 9 adenocarcinoma

20 Gleason grade 5+5 = score of 10 adenocarcinoma

21 Gleason pattern 5 cancer with cribriform gland containing central comedonecrosis
22 Assigning Gleason Score Primary pattern is the one that is predominant in area, by simple visual inspection Secondary pattern is the second most common pattern If only one pattern is in the tissue sample, that grade is multiplied by two to give the score If the secondary pattern is less than 5% of the total tumor and a lower grade, it is ignored, and the primary grade is again doubled to give the Gleason score
23 Assigning Gleason Score Tertiary pattern is the third most common pattern and in many situations it is < 5% On PNB, highest Gleason pattern must be incorporated into the score Tumor composed of patterns 3 (60%), 4 (35%) and 5 (<5%) Gleason score = 3+5=8 On RP, if tertiary pattern is <5% of the tumor and a higher Gleason pattern; report as tertiary pattern Tumor composed of 3 (60%), 4 (35%) and 5 (<5%) Gleason score = 3+4=7 with a tertiary pattern 5 On RP, if tertiary pattern is a significant percentage of the tumor (>5%), include it in the score Tumor composed of 3 (50%), 4 (30%) and 5 (20%) Gleason score = 3+5=8

24 Epstein et al. AJSP, 2015
25 2014 ISUP Prostate Cancer Grading Panel
26 2014 Chicago ISUP Consensus Meeting Why further modifications? Lack of consensus regarding certain grading issues at 2005 meeting Some grading issues not covered in 2005 New pertinent research and data since 2005 Changes in prostate cancer practice has led some clinicians to challenge the existing grading system
27 Chicago ISUP Consensus Meeting November 1, prostate cancer pathology experts from 19 countries 17 clinical leaders (urologists, radiation oncologists, medical oncologists) Different issues: Grading cribriform glands Grading glomeruloid glands Grading intraductal carcinoma Grading mucinous carcinoma
28 2014 ISUP Prostate Cancer Grading Panel Cribriform pattern adenocarcinoma Pattern 3 vs Pattern 4? 2005 Modified Criteria Pattern 3: Small cribriform glands with regular contour and round evenly spaced lumina Pattern 4: Large cribriform glands or cribriform glands with an irregular border

29 Cribriform structures

30 On one (1) of 3590 cases of prostate cancer was there consensus agreement of Gleason pattern 3 cribriform growth among experts

31

32 Cribriform pattern had the highest OR for PSA failure at 5.89 Both large and small cribriform patterns linked to failure Every mm 2 of cribriform pattern increased the OR for PSA failure
33 2014 ISUP Prostate Cancer Grading Panel Cribriform pattern adenocarcinoma associated with earlier biochemical recurrence, metastases and death All cribriform patterns graded as pattern 4 (Eur J Cancer 2014;50: Am J Surg Pathol 2013; 37:1855-6)
34
35 2014 ISUP Prostate Cancer Grading Panel Glomeruloid structures Pattern 3 vs pattern 4 No consensus reached in 2005

36 2014 ISUP Prostate Cancer Grading Panel Glomeruloid structures Favored to be early cribriform structures, therefore graded as pattern 4

37 45 needle biopsies with glomeruloid features 84% of cases associated with Gleason pattern 4 or 5 on the same core
38 2014 ISUP Prostate Cancer Grading Panel Glomeruloid structures Favored to be early cribriform structures, therefore graded as pattern 4

39 2015 Modified ISUP Gleason Patterns
40 2014 ISUP Prostate Cancer Grading Panel Other discussions and recommendations Mucinous carcinoma should be graded based on underlying pattern; not more aggressive than non-mucinous carcinoma Retire hypernephromatoid term
41 2014 ISUP Prostate Cancer Grading Panel Other discussions and recommendations How do we report and grade intraductal growth?
42 Intraductal Carcinoma of the Prostate Intraductal spread of conventional/acinar type prostatic adenocarcinoma Not prostatic duct carcinoma Not high grade prostatic intraepithelial neoplasia Not cribriform pattern (GP 4) of conventional/acinar type carcinoma

43 Intraductal Carcinoma of the Prostate Spread of prostatic adenocarcinoma within prostatic ducts Kovi et al. Cancer 1985;56: Diagnostic criteria formalized Guo, Epstein. Mod Pathol. 2006;19:
44

45
46
47
48

49
50 How do we report and grade intraductal growth?

51 How do we report and grade intraductal growth?
52 2014 ISUP Prostate Cancer Grading Panel How do we report and grade intraductal growth? Intraductal carcinoma without invasive carcinoma in the background, should not be assigned a Gleason grade Report presence of intraductal carcinoma and comment on its invariable association with aggressive prostate cancer Eg Invasive prostatic adenocarcinoma, conventional type with intraductal growth; Gleason score 8/10 (4,4) [see comment] Intraductal carcinoma [see comment]
53 Proposal for New Prostate Cancer Grading System
54 Why a New Grading System? Problems with Gleason grading system scale Use of inaccurate grade combinations for prognosis and therapy Response to proposals to redefine Gleason score 6 as not cancer
55 Problems with the Gleason Grading System Original scores: 2-10 Reporting of GS 2-5 has virtually disappeared Gleason s original data 27.9% (Recent Results Cancer Res 1977; (60):61-72) Pathologists reporting of GS 2-4: 24% in 1991 vs 2.4% in 2001 (Eur Urol 2005;47: ) Biopsy assignment of GS 2-4: 22.3% in 1994 vs 1.6% in 2003 (J Urol 2008;179:1335-8) Biopsy assignment of GS 2-5 GS2-4: 2.7% ( ) vs 0% (2005) GS5: 12.2% ( ) vs 0.3% (2005) (Virchows Arch 2006;449:62-627)
56 Problems with the Gleason Grading System GS 2-5 are virtually nonexistant and cannot be diagnosed on biopsies GS 6 is the lowest score currently assigned GS 6/10 may imply an intermediate risk disease in patient s mind.
57 Use of inaccurate grade combinations for prognosis and therapy In literature and for therapeutic purposes, various scores have been grouped together (prognostic models/nomograms/risk stratification models) with the assumption that they have a similar prognosis 2-4; 5-7; 8-10 Prostate Cancer Outcomes Study; N Engl J Med 2013; 368: ; 7-10 Prostate Cancer Prevention Trial & Prostate Cancer Intervention vs Observation Trial; N Engl J Med 2014; 370: ; 7; 8-10 Scandinavian Prostate Cancer Group Study; NCCN; D Amico classification system
58 Use of inaccurate grade combinations for prognosis and therapy 2-4; 5-7; 8-10 Prostate Cancer Outcomes Study; N Engl J Med 2013; 368: ; 7-10 Prostate Cancer Prevention Trial & Prostate Cancer Intervention vs Observation Trial; N Engl J Med 2014; 370: ; 7; 8-10 Scandinavian Prostate Cancer Group Study; NCCN; D Amico classification system GS 2-4 virtually never exists
59 Use of inaccurate grade combinations for prognosis and therapy 2-4; 5-7; 8-10 Prostate Cancer Outcomes Study; N Engl J Med 2013; 368: ; 7-10 Prostate Cancer Prevention Trial & Prostate Cancer Intervention vs Observation Trial; N Engl J Med 2014; 370: ; 7; 8-10 Scandinavian Prostate Cancer Group Study; NCCN; D Amico classification system Combining GS 6 (Excellent prognosis) with GS 7
60 Use of inaccurate grade combinations for prognosis and therapy 2-4; 5-7; 8-10 Prostate Cancer Outcomes Study; N Engl J Med 2013; 368: ; 7-10 Prostate Cancer Prevention Trial & Prostate Cancer Intervention vs Observation Trial; N Engl J Med 2014; 370: ; 7; 8-10 Scandinavian Prostate Cancer Group Study; NCCN; D Amico classification system No distinction between 3+4 and 4+3 Urology 2000;56: Urology 2006;67: J Urol 2001;166:
61 Use of inaccurate grade combinations for prognosis and therapy 2-4; 5-7; 8-10 Prostate Cancer Outcomes Study; N Engl J Med 2013; 368: ; 7-10 Prostate Cancer Prevention Trial & Prostate Cancer Intervention vs Observation Trial; N Engl J Med 2014; 370: ; 7; 8-10 Scandinavian Prostate Cancer Group Study; NCCN; D Amico classification system Combining GS 7 with GS 8
62 Use of inaccurate grade combinations for prognosis and therapy 2-4; 5-7; 8-10 Prostate Cancer Outcomes Study; N Engl J Med 2013; 368: ; 7-10 Prostate Cancer Prevention Trial & Prostate Cancer Intervention vs Observation Trial; N Engl J Med 2014; 370: ; 7; 8-10 Scandinavian Prostate Cancer Group Study; NCCN; D Amico classification system Combining GS 8 with GS 9-10
63 Response to proposals to redefine Gleason score 6 as not cancer Proposal to consider GS 6 as not cancer Excellent prognosis Ameliorate the fear associated with the term cancer Response to frequent overtreatment of GS 6 Proposed term IDLE (indolent lesion of epithelial origin) (Lancet Oncol 2014;15:e )

64 Response to proposals to redefine Gleason score 6 as not cancer
65 Response to proposals to redefine Gleason score 6 as not cancer Indolent lesion of epithelial origin IDLE Remove the term cancer from indolent, low malignant potential lesions or minimal risk lesions detected by screening Prevent overtreatment since although small volume, well-diff PCa has a 5 and 10yr survival of 99 and 97%, over 90% of patients receive surgery and/or radiation
66 2014 ISUP Prostate Cancer Grading Panel Issues with removing the cancer label 20-25% of Gleason 6 PCa on biopsy are upgraded on the RP Ie. Some may be significant cancers Risk of patients being lost to follow-up when labeled with IDLE
67 2014 ISUP Prostate Cancer Grading Panel It may be easier to discuss surveillance options with patients if they are in.. Grade Group 1 [Range 1-5] vs Gleason Score 6/10 (3,3) [Range 2-10] GG 1 * 5 GS 2 * 10 Better cancer Worse cancer
68 Grouping Gleason Scores 2-6 vs vs 6-7 vs vs 5-7 vs vs 5-6 vs vs 7 vs vs 6 vs 7 vs vs 4-6 vs 7 vs vs 5-6 vs 7 vs vs 5 vs 6 vs 7 vs vs 4-5 vs 6 vs 7-8 vs vs 3+4 vs 4+3 vs vs 3+4 vs 4+3 vs 8 vs 9-10 Epstein 1993; Hanks 1995 Pilepich 1987 Russel 1991; Catalona 1994 Freedland 2000 D Amico 1998; Tefilli 1999 Bagshaw 1990 Zagars 1995 Ohori 1994; Epstein 1996 Partin 1997 Gleason 1977 Makarov/Partin 2007 Eifler/Partin 2012
69
70
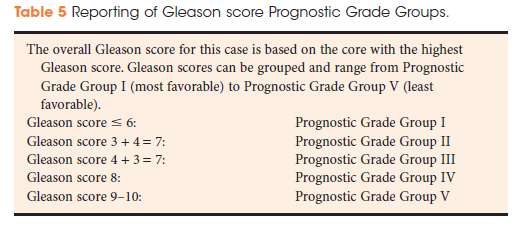
71 New Grading System (Novel Grouping) Grade Group 1 (GS 3+3=6) Excellent prognosis with no risk of lymph node mets (AJSP 2012;36: ) Grade Group 2 (GS 3+4=7) Very good prognosis, rare mets Grade Group 3 (GS 4+3=7) Significantly worse prognosis Grade Group 4 (GS 8) Bad prognosis, significantly better than group 5 Grade Group 5 (GS 9-10)
72 Gleason Grade Grouping Am J Surg Path 2016; 40 (2):

73 Gleason Grade Grouping
74 RP data from five institutions Total RPs Pittsburg Karolinska Hopkins MSKCC CCF
75 Biochemical Recurrence-Free Survival after Radical Prostatectomy
76 Gleason Grade Grouping Grade Group Hazard Ratio 5-Year Biochemical Recurrence-free Survival Grade Group 1 96% Grade Group % Grade Group % Grade Group % Grade Group %
77 Gleason Grade Grouping Founded on the Gleason system with many differences in the definitions and application of original system Disappearance of GS 2-5 Poorly formed glands = GG4 All invasive cribriform glands = GG4 Summing Gleason patterns on RP vs PNB New grading system vs novel grouping of a modified Gleason grading system
78 Gleason Grade Grouping Advantages More accurately reflects prostate cancer biology (eg 3+4 vs 4+3; 8 vs 9-10) Lower number of grade categories 2, 3, 4, 5, 6, 7 (3+4), 7 (4+3), 8, 9, 10 vs 1-5 Lowest grade is Grade group 1 vs Gleason score 6/10 when discussing cancer grade with patients Even though many patients will have an excellent prognosis, the decision to go on active surveillance involves other factors than only Gleason score/grade group (eg extent, PSA) 20% may have unsampled higher grade disease
79 Gleason Grade Grouping 90% of participants in Chicago meeting: Yes Accepted by the WHO for the 2016 edition Pathology and Genetics: Tumours of the Urinary System and Male Genital Organs Used in conjunction with the Gleason system Gleason score 3+3=6 (ISUP Grade Group 1)
80 Prostate Cancer Grading Review of Evolution of Prostate Cancer Grading 1966 Gleason Grading System for Prostate Cancer 2005 ISUP Modified Gleason Grading Proposal for New Grade Grouping ISUP Nov 2014: Prostate Cancer Grading Panel, Chicago Clarification of previous ambiguous grading issues Intraductal carcinoma New Grade Grouping

81 Prostate Cancer Grading: A Contemporary Photomontage JI Epstein AJSP :137-8
82 PROSTATE CANCER GRADING: An Update from the 2014 ISUP Consensus Conference Dr. J. Merrimen Associate Professor Depts of Pathology and Urology Dalhousie University Div of AP Videoconference Feb 16, 2016

83
84

85

86
Intraobserver and Interobserver Reproducibility of WHO and Gleason Histologic Grading Systems in Prostatic Adenocarcinomas
 International Urology and Nephrology 28 (1), pp. 73-77 (1996) Intraobserver and Interobserver Reproducibility of WHO and Gleason Histologic Grading Systems in Prostatic Adenocarcinomas $. O. OZDAMAR,*
International Urology and Nephrology 28 (1), pp. 73-77 (1996) Intraobserver and Interobserver Reproducibility of WHO and Gleason Histologic Grading Systems in Prostatic Adenocarcinomas $. O. OZDAMAR,*
A New Biomarker in Prostate Cancer Care: Oncotype Dx. David M Albala, MD Chief of Urology Crouse Hospital Syracuse, NY
 A New Biomarker in Prostate Cancer Care: Oncotype Dx David M Albala, MD Chief of Urology Crouse Hospital Syracuse, NY Learning Objectives Review the current challenges in the prediction and prognosis of
A New Biomarker in Prostate Cancer Care: Oncotype Dx David M Albala, MD Chief of Urology Crouse Hospital Syracuse, NY Learning Objectives Review the current challenges in the prediction and prognosis of
Beyond the PSA: Genomic Testing in Localized Prostate Cancer
 Beyond the PSA: Genomic Testing in Localized Prostate Cancer Kelvin A. Moses, MD, PhD Vanderbilt University Medical Center Wednesday, December 2, 2015 5:00 p.m. ET/2:00 p.m. PT About ZERO ZERO s mission
Beyond the PSA: Genomic Testing in Localized Prostate Cancer Kelvin A. Moses, MD, PhD Vanderbilt University Medical Center Wednesday, December 2, 2015 5:00 p.m. ET/2:00 p.m. PT About ZERO ZERO s mission
OBJECTIVES By the end of this segment, the community participant will be able to:
 Cancer 101: Cancer Diagnosis and Staging Linda U. Krebs, RN, PhD, AOCN, FAAN OCEAN Native Navigators and the Cancer Continuum (NNACC) (NCMHD R24MD002811) Cancer 101: Diagnosis & Staging (Watanabe-Galloway
Cancer 101: Cancer Diagnosis and Staging Linda U. Krebs, RN, PhD, AOCN, FAAN OCEAN Native Navigators and the Cancer Continuum (NNACC) (NCMHD R24MD002811) Cancer 101: Diagnosis & Staging (Watanabe-Galloway
The 4Kscore blood test for risk of aggressive prostate cancer
 The 4Kscore blood test for risk of aggressive prostate cancer Prostate cancer tests When to use the 4Kscore Test? Screening Prior to 1 st biopsy Prior to negative previous biopsy Prognosis in Gleason 6
The 4Kscore blood test for risk of aggressive prostate cancer Prostate cancer tests When to use the 4Kscore Test? Screening Prior to 1 st biopsy Prior to negative previous biopsy Prognosis in Gleason 6
Prostate Cancer. Treatments as unique as you are
 Prostate Cancer Treatments as unique as you are UCLA Prostate Cancer Program Prostate cancer is the second most common cancer among men. The UCLA Prostate Cancer Program brings together the elements essential
Prostate Cancer Treatments as unique as you are UCLA Prostate Cancer Program Prostate cancer is the second most common cancer among men. The UCLA Prostate Cancer Program brings together the elements essential
An Introduction to PROSTATE CANCER
 An Introduction to PROSTATE CANCER Being diagnosed with prostate cancer can be a life-altering experience. It requires making some very difficult decisions about treatments that can affect not only the
An Introduction to PROSTATE CANCER Being diagnosed with prostate cancer can be a life-altering experience. It requires making some very difficult decisions about treatments that can affect not only the
Newly Diagnosed Prostate Cancer: Understanding Your Risk
 Newly Diagnosed Prostate Cancer: Understanding Your Risk When the urologist calls with the life-changing news that your prostate biopsy is positive for prostate cancer, an office appointment is made to
Newly Diagnosed Prostate Cancer: Understanding Your Risk When the urologist calls with the life-changing news that your prostate biopsy is positive for prostate cancer, an office appointment is made to
Changes in Breast Cancer Reports After Second Opinion. Dr. Vicente Marco Department of Pathology Hospital Quiron Barcelona. Spain
 Changes in Breast Cancer Reports After Second Opinion Dr. Vicente Marco Department of Pathology Hospital Quiron Barcelona. Spain Second Opinion in Breast Pathology Usually requested when a patient is referred
Changes in Breast Cancer Reports After Second Opinion Dr. Vicente Marco Department of Pathology Hospital Quiron Barcelona. Spain Second Opinion in Breast Pathology Usually requested when a patient is referred
Title: Immunohistochemical staining of radixin and moesin in prostatic adenocarcinoma
 Author's response to reviews Title: Immunohistochemical staining of radixin and moesin in prostatic adenocarcinoma Authors: Tanner L Bartholow (bartholow.tanner@medstudent.pitt.edu) Uma R Chandran (chandranur@msx.upmc.edu)
Author's response to reviews Title: Immunohistochemical staining of radixin and moesin in prostatic adenocarcinoma Authors: Tanner L Bartholow (bartholow.tanner@medstudent.pitt.edu) Uma R Chandran (chandranur@msx.upmc.edu)
Do Not Misinterpret Intraductal Carcinoma of the Prostate as High-grade Prostatic Intraepithelial Neoplasia!
 EUROPEAN UROLOGY 62 (2012) 518 522 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial Do Not Misinterpret Intraductal Carcinoma of the Prostate as High-grade Prostatic
EUROPEAN UROLOGY 62 (2012) 518 522 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial Do Not Misinterpret Intraductal Carcinoma of the Prostate as High-grade Prostatic
Prostate Cancer Screening in Taiwan: a must
 Prostate Cancer Screening in Taiwan: a must 吳 俊 德 基 隆 長 庚 醫 院 台 灣 醫 學 會 105 th What is the PSA test? The blood level of PSA is often elevated in men with prostate cancer, and the PSA test was originally
Prostate Cancer Screening in Taiwan: a must 吳 俊 德 基 隆 長 庚 醫 院 台 灣 醫 學 會 105 th What is the PSA test? The blood level of PSA is often elevated in men with prostate cancer, and the PSA test was originally
PSA Screening for Prostate Cancer Information for Care Providers
 All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
Historical Basis for Concern
 Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
Individual Prediction
 Individual Prediction Michael W. Kattan, Ph.D. Professor of Medicine, Epidemiology and Biostatistics, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University Chairman, Department
Individual Prediction Michael W. Kattan, Ph.D. Professor of Medicine, Epidemiology and Biostatistics, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University Chairman, Department
Does my patient need more therapy after prostate cancer surgery?
 Does my patient need more therapy after prostate cancer surgery? Contact the GenomeDx Patient Care Team at: 1.888.792.1601 (toll-free) or e-mail: client.service@genomedx.com Prostate Cancer Classifier
Does my patient need more therapy after prostate cancer surgery? Contact the GenomeDx Patient Care Team at: 1.888.792.1601 (toll-free) or e-mail: client.service@genomedx.com Prostate Cancer Classifier
Saturation Biopsy for Diagnosis and Staging of Prostate Cancer. Original Policy Date
 MP 7.01.101 Saturation Biopsy for Diagnosis and Staging of Prostate Cancer Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date /12/2013 Return to Medical Policy
MP 7.01.101 Saturation Biopsy for Diagnosis and Staging of Prostate Cancer Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date /12/2013 Return to Medical Policy
These rare variants often act aggressively and may respond differently to therapy than the more common prostate adenocarcinoma.
 Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Prostate cancer. Christopher Eden. The Royal Surrey County Hospital, Guildford & The Hampshire Clinic, Old Basing.
 Prostate cancer Christopher Eden The Royal Surrey County Hospital, Guildford & The Hampshire Clinic, Old Basing. Screening Screening men for PCa (prostate cancer) using PSA (Prostate Specific Antigen blood
Prostate cancer Christopher Eden The Royal Surrey County Hospital, Guildford & The Hampshire Clinic, Old Basing. Screening Screening men for PCa (prostate cancer) using PSA (Prostate Specific Antigen blood
Wisconsin Cancer Data Bulletin Wisconsin Department of Health Services Division of Public Health Office of Health Informatics
 Wisconsin Cancer Data Bulletin Wisconsin Department of Health Services Division of Public Health Office of Health Informatics In Situ Breast Cancer in Wisconsin INTRODUCTION This bulletin provides information
Wisconsin Cancer Data Bulletin Wisconsin Department of Health Services Division of Public Health Office of Health Informatics In Situ Breast Cancer in Wisconsin INTRODUCTION This bulletin provides information
Interobserver Reproducibility of Gleason Grading of Prostatic Carcinoma: Urologic Pathologists
 Interobserver Reproducibility of Gleason Grading of Prostatic Carcinoma: Urologic Pathologists WILLIAM C. ALLSBROOK, JR, MD, KATHY A. MANGOLD, PHD, MARIBETH H. JOHNSON, MS, ROGER B. LANE, MD, CYNTHIA G.
Interobserver Reproducibility of Gleason Grading of Prostatic Carcinoma: Urologic Pathologists WILLIAM C. ALLSBROOK, JR, MD, KATHY A. MANGOLD, PHD, MARIBETH H. JOHNSON, MS, ROGER B. LANE, MD, CYNTHIA G.
Robert Bristow MD PhD FRCPC
 Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Us TOO University Presents: Understanding Diagnostic Testing
 Us TOO University Presents: Understanding Diagnostic Testing for Prostate Cancer Patients Today s speaker is Manish Bhandari, MD Program moderator is Pam Barrett, Us TOO International Made possible by
Us TOO University Presents: Understanding Diagnostic Testing for Prostate Cancer Patients Today s speaker is Manish Bhandari, MD Program moderator is Pam Barrett, Us TOO International Made possible by
The PSA Controversy: Defining It, Discussing It, and Coping With It
 The PSA Controversy: Defining It, Discussing It, and Coping With It 11 TH ANNUAL SYMPOSIUM ON MEN S HEALTH June 12, 2013 The PSA Controversy Defining It, Discussing It and Coping With It As of May 2012,
The PSA Controversy: Defining It, Discussing It, and Coping With It 11 TH ANNUAL SYMPOSIUM ON MEN S HEALTH June 12, 2013 The PSA Controversy Defining It, Discussing It and Coping With It As of May 2012,
Early Prostate Cancer: Questions and Answers. Key Points
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Early Prostate Cancer:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Early Prostate Cancer:
Nicole Kounalakis, MD
 Breast Disease: Diagnosis and Management Nicole Kounalakis, MD Assistant Professor of Surgery Goal of Breast Evaluation The goal of breast evaluation is to classify findings as: normal physiologic variations
Breast Disease: Diagnosis and Management Nicole Kounalakis, MD Assistant Professor of Surgery Goal of Breast Evaluation The goal of breast evaluation is to classify findings as: normal physiologic variations
HER2 Status: What is the Difference Between Breast and Gastric Cancer?
 Ask the Experts HER2 Status: What is the Difference Between Breast and Gastric Cancer? Bharat Jasani MBChB, PhD, FRCPath Marco Novelli MBChB, PhD, FRCPath Josef Rüschoff, MD Robert Y. Osamura, MD, FIAC
Ask the Experts HER2 Status: What is the Difference Between Breast and Gastric Cancer? Bharat Jasani MBChB, PhD, FRCPath Marco Novelli MBChB, PhD, FRCPath Josef Rüschoff, MD Robert Y. Osamura, MD, FIAC
GENERAL CODING. When you review old cases that were coded to unknown, make corrections based on guidelines in effect at the time of diagnosis.
 GENERAL CODING When you review old cases that were coded to unknown, make corrections based on guidelines in effect at the time of diagnosis. Exception: You must review and revise EOD coding for prostate
GENERAL CODING When you review old cases that were coded to unknown, make corrections based on guidelines in effect at the time of diagnosis. Exception: You must review and revise EOD coding for prostate
HAVE YOU BEEN NEWLY DIAGNOSED with DCIS?
 HAVE YOU BEEN NEWLY DIAGNOSED with DCIS? Jen D. Mother and volunteer. Diagnosed with DCIS breast cancer in 2012. An educational guide prepared by Genomic Health This guide is designed to educate women
HAVE YOU BEEN NEWLY DIAGNOSED with DCIS? Jen D. Mother and volunteer. Diagnosed with DCIS breast cancer in 2012. An educational guide prepared by Genomic Health This guide is designed to educate women
Understanding your pathology report
 Understanding your pathology report 2 Contents Contents Introduction 3 What is a pathology report? 3 Waiting for your results 4 What s in a pathology report? 4 Information about your breast cancer 5 What
Understanding your pathology report 2 Contents Contents Introduction 3 What is a pathology report? 3 Waiting for your results 4 What s in a pathology report? 4 Information about your breast cancer 5 What
Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma
 Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma Medical Expert: Breast Rotation Specific Competencies/Objectives 1.0 Medical History
Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma Medical Expert: Breast Rotation Specific Competencies/Objectives 1.0 Medical History
The 4Kscore blood test for risk of aggressive prostate cancer
 The 4Kscore blood test for risk of aggressive prostate cancer Early detection of aggressive prostate cancer Challenges Serum PSA has a high false positive rate Over 1 million prostate biopsies performed
The 4Kscore blood test for risk of aggressive prostate cancer Early detection of aggressive prostate cancer Challenges Serum PSA has a high false positive rate Over 1 million prostate biopsies performed
Analysis of Prostate Cancer at Easter Connecticut Health Network Using Cancer Registry Data
 The 2014 Cancer Program Annual Public Reporting of Outcomes/Annual Site Analysis Statistical Data from 2013 More than 70 percent of all newly diagnosed cancer patients are treated in the more than 1,500
The 2014 Cancer Program Annual Public Reporting of Outcomes/Annual Site Analysis Statistical Data from 2013 More than 70 percent of all newly diagnosed cancer patients are treated in the more than 1,500
Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical
 Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Jurisdiction Virginia
 PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Prolaris Prostate Cancer Genomic Assay (DL35629) Please note: This is a Proposed/Draft policy. Proposed/Draft LCDs are works in progress that are
PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Prolaris Prostate Cancer Genomic Assay (DL35629) Please note: This is a Proposed/Draft policy. Proposed/Draft LCDs are works in progress that are
Lung Carcinomas New 2015 WHO Classification. Spasenija Savic Pathology
 Lung Carcinomas New 2015 WHO Classification Spasenija Savic Pathology ***EXPECTED SPRING 2015*** This authoritative, concise reference book provides an international standard for oncologists and pathologists
Lung Carcinomas New 2015 WHO Classification Spasenija Savic Pathology ***EXPECTED SPRING 2015*** This authoritative, concise reference book provides an international standard for oncologists and pathologists
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD
 SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
A918: Prostate: adenocarcinoma
 A918: Prostate: adenocarcinoma General facts of prostate cancer The prostate is about the size of a walnut. It is just below the bladder and in front of the rectum. The tube that carries urine (the urethra)
A918: Prostate: adenocarcinoma General facts of prostate cancer The prostate is about the size of a walnut. It is just below the bladder and in front of the rectum. The tube that carries urine (the urethra)
TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER
 TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER DILEMMA Thomas J Stormont MD January 2012 http://www.youtube.com/watch?v=8jd 7bAHVp0A&feature=related related INTRODUCTION A government health panel (the
TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER DILEMMA Thomas J Stormont MD January 2012 http://www.youtube.com/watch?v=8jd 7bAHVp0A&feature=related related INTRODUCTION A government health panel (the
Oncology Annual Report: Prostate Cancer 2005 Update By: John Konefal, MD, Radiation Oncology
 Oncology Annual Report: Prostate Cancer 25 Update By: John Konefal, MD, Radiation Oncology Prostate cancer is the most common cancer in men, with 232,9 new cases projected to be diagnosed in the U.S. in
Oncology Annual Report: Prostate Cancer 25 Update By: John Konefal, MD, Radiation Oncology Prostate cancer is the most common cancer in men, with 232,9 new cases projected to be diagnosed in the U.S. in
Outline. Workup for metastatic breast cancer. Metastatic breast cancer
 Metastatic breast cancer Immunostain Update: Diagnosis of metastatic breast carcinoma, emphasizing distinction from GYN primary 1/3 of breast cancer patients will show metastasis 1 st presentation or 20-30
Metastatic breast cancer Immunostain Update: Diagnosis of metastatic breast carcinoma, emphasizing distinction from GYN primary 1/3 of breast cancer patients will show metastasis 1 st presentation or 20-30
ATLAS OF HEAD AND NECK PATHOLOGY THYROID PAPILLARY CARCINOMA
 Papillary carcinoma is the most common of thyroid malignancies and occurs in all age groups but particularly in women under 45 years of age. There is a high rate of cervical metastatic disease and yet
Papillary carcinoma is the most common of thyroid malignancies and occurs in all age groups but particularly in women under 45 years of age. There is a high rate of cervical metastatic disease and yet
Prostate cancer volume at biopsy vs. findings at Prostatectomy
 Prostate cancer volume at biopsy vs. findings at Prostatectomy May 2005 By Shelly Smits, RHIT, CCS, CTR Ian Thompson, MD Data Source: Cancer registry data of prostate cancer treated with prostatectomy
Prostate cancer volume at biopsy vs. findings at Prostatectomy May 2005 By Shelly Smits, RHIT, CCS, CTR Ian Thompson, MD Data Source: Cancer registry data of prostate cancer treated with prostatectomy
Update on Prostate Cancer: Screening, Diagnosis, and Treatment Making Sense of the Noise and Directions Forward
 Update on Prostate Cancer: Screening, Diagnosis, and Treatment Making Sense of the Noise and Directions Forward 33 rd Annual Internal Medicine Update December 5, 2015 Ryan C. Hedgepeth, MD, MS Chief of
Update on Prostate Cancer: Screening, Diagnosis, and Treatment Making Sense of the Noise and Directions Forward 33 rd Annual Internal Medicine Update December 5, 2015 Ryan C. Hedgepeth, MD, MS Chief of
Breast Cancer. Presentation by Dr Mafunga
 Breast Cancer Presentation by Dr Mafunga Breast cancer in the UK Breast cancer is the second most common cancer in women. Around 1 in 9 women will develop breast cancer It most commonly affects women over
Breast Cancer Presentation by Dr Mafunga Breast cancer in the UK Breast cancer is the second most common cancer in women. Around 1 in 9 women will develop breast cancer It most commonly affects women over
PSA Testing 101. Stanley H. Weiss, MD. Professor, UMDNJ-New Jersey Medical School. Director & PI, Essex County Cancer Coalition. weiss@umdnj.
 PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
Renal Cell Carcinoma: Advances in Diagnosis B. Iványi, MD
 Renal Cell Carcinoma: Advances in Diagnosis B. Iványi, MD Department of Pathology University of Szeged, Hungary ISUP Vancouver Classification of Renal Neoplasia Am J Surg Pathol 37:14691489, 2013 13 histologic
Renal Cell Carcinoma: Advances in Diagnosis B. Iványi, MD Department of Pathology University of Szeged, Hungary ISUP Vancouver Classification of Renal Neoplasia Am J Surg Pathol 37:14691489, 2013 13 histologic
Breast Cancer: from bedside and grossing room to diagnoses and beyond. Adriana Corben, M.D.
 Breast Cancer: from bedside and grossing room to diagnoses and beyond Adriana Corben, M.D. About breast anatomy Breasts are special organs that develop in women during puberty when female hormones are
Breast Cancer: from bedside and grossing room to diagnoses and beyond Adriana Corben, M.D. About breast anatomy Breasts are special organs that develop in women during puberty when female hormones are
Prostate Cancer Screening. Dr. J. McCracken, Urologist
 Prostate Cancer Screening Dr. J. McCracken, Urologist USPSTF Lifetime risk for diagnosis currently estimated at 15.9% Llifetime risk of dying of prostate cancer is 2.8% Seventy percent of deaths due to
Prostate Cancer Screening Dr. J. McCracken, Urologist USPSTF Lifetime risk for diagnosis currently estimated at 15.9% Llifetime risk of dying of prostate cancer is 2.8% Seventy percent of deaths due to
4/8/13. Pre-test Audience Response. Prostate Cancer 2012. Screening and Treatment of Prostate Cancer: The 2013 Perspective
 Pre-test Audience Response Screening and Treatment of Prostate Cancer: The 2013 Perspective 1. I do not offer routine PSA screening, and the USPSTF D recommendation will not change my practice. 2. In light
Pre-test Audience Response Screening and Treatment of Prostate Cancer: The 2013 Perspective 1. I do not offer routine PSA screening, and the USPSTF D recommendation will not change my practice. 2. In light
BREAST CANCER PATHOLOGY
 BREAST CANCER PATHOLOGY FACT SHEET Version 4, Aug 2013 This fact sheet was produced by Breast Cancer Network Australia with input from The Royal College of Pathologists of Australasia I m a nurse and know
BREAST CANCER PATHOLOGY FACT SHEET Version 4, Aug 2013 This fact sheet was produced by Breast Cancer Network Australia with input from The Royal College of Pathologists of Australasia I m a nurse and know
Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy
 Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy W. Fraser Symmans, M.D. Associate Professor of Pathology UT M.D. Anderson Cancer Center Pathologic Complete Response (pcr) Proof
Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy W. Fraser Symmans, M.D. Associate Professor of Pathology UT M.D. Anderson Cancer Center Pathologic Complete Response (pcr) Proof
Advances in Diagnostic and Molecular Testing in Prostate Cancer
 Advances in Diagnostic and Molecular Testing in Prostate Cancer Ashley E. Ross MD PhD Assistant Professor Urology, Oncology, Pathology Johns Hopkins School of Medicine September 24, 2015 1 Disclosures
Advances in Diagnostic and Molecular Testing in Prostate Cancer Ashley E. Ross MD PhD Assistant Professor Urology, Oncology, Pathology Johns Hopkins School of Medicine September 24, 2015 1 Disclosures
AFTER DIAGNOSIS: PROSTATE CANCER Understanding Your Treatment Options
 AFTER DIAGNOSIS: PROSTATE CANCER Understanding Your Treatment Options INTRODUCTION This booklet describes how prostate cancer develops, how it affects the body and the current treatment methods. Although
AFTER DIAGNOSIS: PROSTATE CANCER Understanding Your Treatment Options INTRODUCTION This booklet describes how prostate cancer develops, how it affects the body and the current treatment methods. Although
Gleason Score. Oncotype DX GPS. identified for. about surveillance. time to get sophisticated
 patient: MARK SMITH PSA 6.2 Gleason Score 6 Oncotype DX GPS 8 identified for active surveillance time to get sophisticated about surveillance Accurate prediction of prostate cancer risk is needed at the
patient: MARK SMITH PSA 6.2 Gleason Score 6 Oncotype DX GPS 8 identified for active surveillance time to get sophisticated about surveillance Accurate prediction of prostate cancer risk is needed at the
How to report Upper GI EMR/ESD specimens
 Section of Pathology and Tumour Biology How to report Upper GI EMR/ESD specimens Dr.H.Grabsch Warning. Most of the criteria, methodologies, evidence presented in this talk are based on studies in early
Section of Pathology and Tumour Biology How to report Upper GI EMR/ESD specimens Dr.H.Grabsch Warning. Most of the criteria, methodologies, evidence presented in this talk are based on studies in early
A Woman s Guide to Prostate Cancer Treatment
 A Woman s Guide to Prostate Cancer Treatment Supporting the man in your life Providing prostate cancer support and resources for women and families WOMEN AGAINST PROSTATE CANCER A Woman s Guide to Prostate
A Woman s Guide to Prostate Cancer Treatment Supporting the man in your life Providing prostate cancer support and resources for women and families WOMEN AGAINST PROSTATE CANCER A Woman s Guide to Prostate
SRO Tutorial: Prostate Cancer Treatment Options
 SRO Tutorial: Prostate Cancer Treatment Options May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible,
SRO Tutorial: Prostate Cancer Treatment Options May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible,
Prostate Cancer 2014
 Prostate Cancer 2014 Eric A. Klein, M.D. Chairman Glickman Urological and Kidney Institute Professor of Surgery Cleveland Clinic Lerner College of Medicine Incidence rates, US Men Mortality Rates, US Men
Prostate Cancer 2014 Eric A. Klein, M.D. Chairman Glickman Urological and Kidney Institute Professor of Surgery Cleveland Clinic Lerner College of Medicine Incidence rates, US Men Mortality Rates, US Men
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC)
") Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies
 Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies John F. Ward, MD Assistant Professor University of Texas M. D. Anderson Cancer Center Ablation
Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies John F. Ward, MD Assistant Professor University of Texas M. D. Anderson Cancer Center Ablation
The Diagnosis of Cancer in the Pathology Laboratory
 The Diagnosis of Cancer in the Pathology Laboratory Dr Edward Sheffield Christmas Select 74 Meeting, Queen s Hotel Cheltenham, 3 rd December 2014 Agenda Overview of the pathology of cancer How specimens
The Diagnosis of Cancer in the Pathology Laboratory Dr Edward Sheffield Christmas Select 74 Meeting, Queen s Hotel Cheltenham, 3 rd December 2014 Agenda Overview of the pathology of cancer How specimens
Understanding ductal carcinoma in situ (DCIS) and deciding about treatment
 and deciding about treatment") Understanding ductal carcinoma in situ (DCIS) and deciding about treatment Developed by National Breast and Ovarian Cancer Centre Funded by the Australian Government Department of Health and Ageing Understanding
Understanding ductal carcinoma in situ (DCIS) and deciding about treatment Developed by National Breast and Ovarian Cancer Centre Funded by the Australian Government Department of Health and Ageing Understanding
Questions to ask my doctor: About prostate cancer
 Questions to ask my doctor: About prostate cancer Being diagnosed with prostate cancer can be scary and stressful. You probably have a lot of questions and concerns. Learning about the disease, how it
Questions to ask my doctor: About prostate cancer Being diagnosed with prostate cancer can be scary and stressful. You probably have a lot of questions and concerns. Learning about the disease, how it
Something Old, Something New.
 Something Old, Something New. Michelle A. Fajardo, D.O. Loma Linda University Medical Center Clinical Presentation 6 year old boy, presented with hematuria Renal mass demonstrated by ultrasound & CT scan
Something Old, Something New. Michelle A. Fajardo, D.O. Loma Linda University Medical Center Clinical Presentation 6 year old boy, presented with hematuria Renal mass demonstrated by ultrasound & CT scan
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER?
 PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
PSA screening in asymptomatic men the debate continues www.bpac.org.nz keyword: psa
 PSA screening in asymptomatic men the debate continues www.bpac.org.nz keyword: psa Key messages: PSA is present in the benign and malignant prostate There is currently no national screening programme
PSA screening in asymptomatic men the debate continues www.bpac.org.nz keyword: psa Key messages: PSA is present in the benign and malignant prostate There is currently no national screening programme
Seton Medical Center Hepatocellular Carcinoma Patterns of Care Study Rate of Treatment with Chemoembolization 2007 2012 N = 50
 General Data Seton Medical Center Hepatocellular Carcinoma Patterns of Care Study Rate of Treatment with Chemoembolization 2007 2012 N = 50 The vast majority of the patients in this study were diagnosed
General Data Seton Medical Center Hepatocellular Carcinoma Patterns of Care Study Rate of Treatment with Chemoembolization 2007 2012 N = 50 The vast majority of the patients in this study were diagnosed
Introduction Breast cancer is cancer that starts in the cells of the breast. Breast cancer happens mainly in women. But men can get it too.
 Male Breast Cancer Introduction Breast cancer is cancer that starts in the cells of the breast. Breast cancer happens mainly in women. But men can get it too. Many people do not know that men can get breast
Male Breast Cancer Introduction Breast cancer is cancer that starts in the cells of the breast. Breast cancer happens mainly in women. But men can get it too. Many people do not know that men can get breast
Local Coverage Determination (LCD): MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153)
: MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153)") Local Coverage Determination (LCD): MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153) Contractor Information Contractor Name Palmetto GBA LCD Information Document Information LCD ID L36153
Local Coverage Determination (LCD): MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153) Contractor Information Contractor Name Palmetto GBA LCD Information Document Information LCD ID L36153
NCCN Prostate Cancer Early Detection Guideline
 NCCN Prostate Cancer Early Detection Guideline Joan McClure Senior Vice President National Comprehensive Cancer Network African American Prostate Cancer Disparity Summit September 22, 2006 Washington,
NCCN Prostate Cancer Early Detection Guideline Joan McClure Senior Vice President National Comprehensive Cancer Network African American Prostate Cancer Disparity Summit September 22, 2006 Washington,
Kidney Cancer OVERVIEW
 Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
PSA screening: Controversies and Guidelines
 PSA screening: Controversies and Guidelines John Phillips, MD, FACS Department of Urology Urology Center of Westchester New York Medical College Historical PerspecGve Cancer of the prostate, although rare,
PSA screening: Controversies and Guidelines John Phillips, MD, FACS Department of Urology Urology Center of Westchester New York Medical College Historical PerspecGve Cancer of the prostate, although rare,
STATE OF MICHIGAN DEPARTMENT OF INSURANCE AND FINANCIAL SERVICES Before the Director of Insurance and Financial Services
 STATE OF MICHIGAN DEPARTMENT OF INSURANCE AND FINANCIAL SERVICES Before the Director of Insurance and Financial Services In the matter of: Petitioner, v Blue Care Network of Michigan, Respondent. File
STATE OF MICHIGAN DEPARTMENT OF INSURANCE AND FINANCIAL SERVICES Before the Director of Insurance and Financial Services In the matter of: Petitioner, v Blue Care Network of Michigan, Respondent. File
Male. Female. Death rates from lung cancer in USA
 Male Female Death rates from lung cancer in USA Smoking represents an interesting combination of an entrenched industry and a clearly drug-induced cancer Tobacco Use in the US, 1900-2000 5000 100 Per Capita
Male Female Death rates from lung cancer in USA Smoking represents an interesting combination of an entrenched industry and a clearly drug-induced cancer Tobacco Use in the US, 1900-2000 5000 100 Per Capita
Understanding Metastatic Disease
 Supported by an unrestricted educational grant from Pfizer Understanding Metastatic Disease Metastatic disease or metastases are phrases that mean the same as Secondary cancer. This means that the cancer
Supported by an unrestricted educational grant from Pfizer Understanding Metastatic Disease Metastatic disease or metastases are phrases that mean the same as Secondary cancer. This means that the cancer
Primary -Benign - Malignant Secondary
 TUMOURS OF THE LUNG Primary -Benign - Malignant Secondary The incidence of lung cancer has been increasing almost logarithmically and is now reaching epidemic levels. The overall cure rate is very low
TUMOURS OF THE LUNG Primary -Benign - Malignant Secondary The incidence of lung cancer has been increasing almost logarithmically and is now reaching epidemic levels. The overall cure rate is very low
ductal carcinoma in situ (DCIS)
") Understanding ductal carcinoma in situ (DCIS) and deciding about treatment Understanding ductal carcinoma in situ (DCIS) and deciding about treatment Developed by National Breast and Ovarian Cancer Centre
Understanding ductal carcinoma in situ (DCIS) and deciding about treatment Understanding ductal carcinoma in situ (DCIS) and deciding about treatment Developed by National Breast and Ovarian Cancer Centre
A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score
 EUROPEAN UROLOGY 69 (2016) 428 435 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Prostate Cancer Editorial by Markus Graefen, Thorsten Schlomm, Guido Sauter
EUROPEAN UROLOGY 69 (2016) 428 435 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Prostate Cancer Editorial by Markus Graefen, Thorsten Schlomm, Guido Sauter
Introduction to Pathology and Diagnostic Medicine
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Introduction to Pathology and Diagnostic Medicine Spring 2003 What is pathology?
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Introduction to Pathology and Diagnostic Medicine Spring 2003 What is pathology?
Your bladder cancer diary. WA Cancer and Palliative Care Network
 Your bladder cancer diary WA Cancer and Palliative Care Network Patient information and persons to contact Your Name Date of Birth URMN (Patient Hospital Unit Number) Address Phone Mobile GP Name Phone
Your bladder cancer diary WA Cancer and Palliative Care Network Patient information and persons to contact Your Name Date of Birth URMN (Patient Hospital Unit Number) Address Phone Mobile GP Name Phone
PSA Screening and the USPSTF Understanding the Controversy
 PSA Screening and the USPSTF Understanding the Controversy Peter C. Albertsen Division of Urology University of Connecticut Farmington, CT, USA USPSTF Final Report 1 Four Key Questions 1. Does PSA based
PSA Screening and the USPSTF Understanding the Controversy Peter C. Albertsen Division of Urology University of Connecticut Farmington, CT, USA USPSTF Final Report 1 Four Key Questions 1. Does PSA based
CMScript. Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014
 Background CMScript Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014 Prostate cancer is second only to lung cancer as the leading cause of cancer-related deaths in men. It is
Background CMScript Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014 Prostate cancer is second only to lung cancer as the leading cause of cancer-related deaths in men. It is
Fact sheet 10. Borderline ovarian tumours. The difficult cases. What is borderline ovarian cancer (BOC)?
?") For this reason, some doctors prefer the term borderline ovarian tumour rather than borderline ovarian cancer. Fact sheet 10 Borderline ovarian tumours We, Ovacome, are a support network for people affected
For this reason, some doctors prefer the term borderline ovarian tumour rather than borderline ovarian cancer. Fact sheet 10 Borderline ovarian tumours We, Ovacome, are a support network for people affected
Advanced Prostate Cancer Treatments
 Advanced Prostate Cancer Treatments Guest Expert: Kevin, DO Associate Professor of Medical Oncology, Yale Cancer Center www.wnpr.org www.yalecancercenter.org Welcome to Yale Cancer Center Answers with
Advanced Prostate Cancer Treatments Guest Expert: Kevin, DO Associate Professor of Medical Oncology, Yale Cancer Center www.wnpr.org www.yalecancercenter.org Welcome to Yale Cancer Center Answers with
Technical Advices for Prostate Needle Biopsy Under Transrectal Ultrasound Guidance
 Technical Advices for Prostate Needle Biopsy Under Transrectal Ultrasound Guidance Makoto Ohori 1 and Ayako Miyakawa 2 1 Dept. of Urology, Tokyo Medical University 2 Dept. of Molecular Medicine and Surgery,
Technical Advices for Prostate Needle Biopsy Under Transrectal Ultrasound Guidance Makoto Ohori 1 and Ayako Miyakawa 2 1 Dept. of Urology, Tokyo Medical University 2 Dept. of Molecular Medicine and Surgery,
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Updates in Mesothelioma By Samieh Amer, MD Professor of Cardiothoracic Surgery Faculty of Medicine, Cairo University History Wagner and his colleagues (1960) 33 cases of mesothelioma
بسم هللا الرحمن الرحيم Updates in Mesothelioma By Samieh Amer, MD Professor of Cardiothoracic Surgery Faculty of Medicine, Cairo University History Wagner and his colleagues (1960) 33 cases of mesothelioma
Breast Cancer. Sometimes cells keep dividing and growing without normal controls, causing an abnormal growth called a tumor.
 Breast Cancer Introduction Cancer of the breast is the most common form of cancer that affects women but is no longer the leading cause of cancer deaths. About 1 out of 8 women are diagnosed with breast
Breast Cancer Introduction Cancer of the breast is the most common form of cancer that affects women but is no longer the leading cause of cancer deaths. About 1 out of 8 women are diagnosed with breast
PCA3 DETECTION TEST FOR PROSTATE CANCER DO YOU KNOW YOUR RISK OF HAVING CANCER?
 PCA3 DETECTION TEST FOR PROSTATE CANCER DO YOU KNOW YOUR RISK OF HAVING CANCER? PCA3 DETECTION TEST FOR PROSTATE CANCER There is a range of methods available to your healthcare professional to verify the
PCA3 DETECTION TEST FOR PROSTATE CANCER DO YOU KNOW YOUR RISK OF HAVING CANCER? PCA3 DETECTION TEST FOR PROSTATE CANCER There is a range of methods available to your healthcare professional to verify the
Medullary Renal Cell Carcinoma Case Report
 Bahrain Medical Bulletin, Vol. 27, No. 4, December 2005 Medullary Renal Cell Carcinoma Case Report Mohammed Abdulla Al-Tantawi MBBCH, CABS* Abdul Amir Issa MBBCH, CABS*** Mohammed Abdulla MBBCH, CABS**
Bahrain Medical Bulletin, Vol. 27, No. 4, December 2005 Medullary Renal Cell Carcinoma Case Report Mohammed Abdulla Al-Tantawi MBBCH, CABS* Abdul Amir Issa MBBCH, CABS*** Mohammed Abdulla MBBCH, CABS**
Kanıt: Klinik çalışmalarda ZYTIGA
 mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
PATIENT GUIDE. Localized Prostate Cancer
 PATIENT GUIDE Localized Prostate Cancer The prostate* is part of the male reproductive system. It is about the same size as a walnut and weighs about an ounce. As pictured in Figure 1, the prostate is
PATIENT GUIDE Localized Prostate Cancer The prostate* is part of the male reproductive system. It is about the same size as a walnut and weighs about an ounce. As pictured in Figure 1, the prostate is
Low-dose CT Imaging. Edgar Fearnow, M.D. Section Chief, Computed Tomography, Lancaster General Hospital
 Lung Cancer Screening with Low-dose CT Imaging Edgar Fearnow, M.D. Section Chief, Computed Tomography, Lancaster General Hospital Despite recent declines in the incidence of lung cancer related to the
Lung Cancer Screening with Low-dose CT Imaging Edgar Fearnow, M.D. Section Chief, Computed Tomography, Lancaster General Hospital Despite recent declines in the incidence of lung cancer related to the
Secondary Cancer and Relapse Rates Following Radical Prostatectomy for Prostate-Confined Cancer
 Copyright E 2007 Journal of Insurance Medicine J Insur Med 2007;39:242 250 MORTALITY Secondary Cancer and Relapse Rates Following Radical Prostatectomy for Prostate-Confined Cancer David Wesley, MD; Hugh
Copyright E 2007 Journal of Insurance Medicine J Insur Med 2007;39:242 250 MORTALITY Secondary Cancer and Relapse Rates Following Radical Prostatectomy for Prostate-Confined Cancer David Wesley, MD; Hugh
Polyps. Hyperplasias. CAP 2011: Course AP104. The High Risk Benign Endometrium. Mutter and Nucci 1
 Course AP104 Endometrial Hyperplasia A morphologic Definition Hyperplasias Hormonal Effect or Precancer? George L. Mutter, MD Harvard Medical School and Brigham and Women s Hospital Boston, MA Endometrial
Course AP104 Endometrial Hyperplasia A morphologic Definition Hyperplasias Hormonal Effect or Precancer? George L. Mutter, MD Harvard Medical School and Brigham and Women s Hospital Boston, MA Endometrial
Prostate Cancer In-Depth
 Prostate Cancer In-Depth Introduction Prostate cancer is the most common visceral malignancy among American men. In the year 2003, there are expected to be 220,000 new cases and nearly 29,000 deaths in
Prostate Cancer In-Depth Introduction Prostate cancer is the most common visceral malignancy among American men. In the year 2003, there are expected to be 220,000 new cases and nearly 29,000 deaths in
Update on Mesothelioma
 November 8, 2012 Update on Mesothelioma Intro incidence and nomenclature Update on Classification Diagnostic specimens Morphologic features Epithelioid Histology Biphasic Histology Immunohistochemical
November 8, 2012 Update on Mesothelioma Intro incidence and nomenclature Update on Classification Diagnostic specimens Morphologic features Epithelioid Histology Biphasic Histology Immunohistochemical
Brachytherapy for prostate cancer
 Brachytherapy for prostate cancer Findings by SBU Alert Published Jun 7, 2000 Version 1 Brachytherapy is not widely used in Sweden to treat localized prostate cancer. This treatment method has been available
Brachytherapy for prostate cancer Findings by SBU Alert Published Jun 7, 2000 Version 1 Brachytherapy is not widely used in Sweden to treat localized prostate cancer. This treatment method has been available
Prostate cancer is the most common cause of death from cancer in men over age 75. Prostate cancer is rarely found in men younger than 40.
 A.D.A.M. Medical Encyclopedia. Prostate cancer Cancer - prostate; Biopsy - prostate; Prostate biopsy; Gleason score Last reviewed: October 2, 2013. Prostate cancer is cancer that starts in the prostate
A.D.A.M. Medical Encyclopedia. Prostate cancer Cancer - prostate; Biopsy - prostate; Prostate biopsy; Gleason score Last reviewed: October 2, 2013. Prostate cancer is cancer that starts in the prostate