IMAGING OF BENIGN RENAL MASSES. Dr. Darragh Halpenny NYU Langone Medical Center New York
|
|
|
- Allan Nichols
- 7 years ago
- Views:
Transcription
1 IMAGING OF BENIGN RENAL MASSES Dr. Darragh Halpenny NYU Langone Medical Center New York
2 Dr. Andrew Rosenkrantz Dr. Mark Page
3 Overview of the common benign renal masses and their imaging features Briefly discuss some rarer benign renal masses Discuss common mimics of renal mass lesions and potential pitfalls in renal mass imaging
4 Role of the radiologist in the management of small renal masses Attention on the incidental renal mass
5 Over riding clinical questions: Can we make a definitive diagnosis? Could we to follow it up? Does the lesion need intervention?
6 Prasad et al. AJR 2008; 190:
7 BENIGN RENAL MASS Solid mass Cystic mass With fat Angiomyolipoma Without fat Oncocytoma Lipid poor AML Leiomyoma Haemangioma Reninoma Renal cyst Cystic nephroma Lymphangioma Mixed epithelial and stromal tumor
8 ONCOCYTOMA
9 ONCOCYTOMA 5% of solid renal lesions 13% of resected renal lesions are benign almost all are oncocytoma or AML Peak age of incidence is in the seventh decade Men > women
10 ONCOCYTOMA If bilateral or multicentric consider hereditary syndromes Renal oncocytosis Birt-Hogg-Dubé syndrome Main clinical issues Indistinguishable from renal cell carcinomas on imaging alone May be associated with RCCs either as hybrid tumors or as collision tumors
11 ONCOCYTOMA Renal cortical tumors Solitary Well-demarcated Unencapsulated (pseudocapsule - rim of compressed normal renal parenchyma)
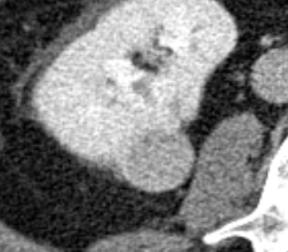
12 ONCOCYTOMA - CT Non contrast < 3 cm - homogenous attenuation > 3 cm - heterogenous attenuation Post contrast Small tumors may enhance homogeneously Larger masses heterogenous enhancement
13 ONCOCYTOMA Characteristic central stellate fibrotic scar Seen in 1/3rd More often with large tumors Hemorrhage in up to 20% of cases
14 ONCOCYTOMA - MRI Relative to the renal cortex T1-weighted most are hypointense T2-weighted most are hyperintense
15 ONCOCYTOMA - MRI Central scar (when present) Low signal intensity on T1 Variable signal intensity on T2 May show delayed enhancement

16 Oncocytoma CT Chromophobe T1 T2 Gd +
17 ONCOCYTOMA DWI Lassel EA et al Eur Radiol 2014 Meta-analysis based on 17 studies with 764 patients Significant difference between ADC values of renal cell carcinomas and oncocytomas
18 Managed surgically
19 ANGIOMYOLIPOMA
20 BACKGROUND Angiomyolipoma is the most common benign renal tumor Variable amounts of muscle, fat and vascular tissue 80% sporadic Remainder associated with tuberous sclerosis
21 BACKGROUND Most commonly an incidental finding Over 4cm: Symptoms develop in up to 80% Most commonly haemorrhage


22

 which do not contain")
23 CT Classical finding is a fat containing mass RCCs containing macroscopic fat extremely rare Small subset (<5%) which do not contain macroscopic fat
24 CT Differentiate AML from the very rare retroperitoneal liposarcoma AML Renal origin Defect in the renal parenchyma Liposarcoma Smooth interface Displace and compress kidney Yeh et al J Computed Assist Tomography 2008
25 Yeh et al J Computed Assist Tomography 2008
26 MRI For classic AML

27 T1 with and without fat suppression
28 India ink artifact
29 MINIMAL FAT AML Account for 6% of surgically excised small renal masses No macroscopic fat 3% 10% of fat at histology
30 MINIMAL FAT AML IMAGING FEATURES Non contrast homogenously hyper-attenuating Enhance mild - moderately Quite different to Clear Cell RCC But very similar to papillary RCC T2 Hypointense Kim J et al. Radiology 2009 Aug;252(2):441-8
31 MANAGEMENT Macroscopic fat < 4 cm Observe Consider US every 12 months Consider intervention if > 4cm Symptomatic Large aneurysms Surgery or embolization If no macroscopic fat - diagnostic dilemma - surgery
32 ADDITIONAL BENIGN RENAL MASSES Very rare Most are asymptomatic Most managed surgically as they are indistinguishable from RCC Most common symptoms flank pain abdominal mass hematuria
33 METANEPHRIC ADENOMA Peak incidence in the sixth decade Well-defined solid mass CT Non-contrast Hyper-attenuating Post contrast Minimal enhancement


34 METANEPHRIC ADENOMA MRI Hypointense/Isointense on T1 Heterogenous on T2 Hypovascular
35 LEIOMYOMA Smooth muscle of the capsule - peripheral Buckling of the cortex CT Non- contrast hyperattenuating solid mass MR T1 and T2 hypointense Mild homogenous enhancement
36 PAPILLARY ADENOMA Most common renal epithelial neoplasm Approximately 40% of patients >70 years Common in patients with acquired renal cystic disease long-term hemodialysis patients Extremely small (< 5 mm) Cannot be distinguished from other tumors on imaging
37 RENAL HEMANGIOMA Rare mesenchymal neoplasm 1 in 2000 to 1 in 30,000 individuals Young adults Can be associated with Sturge-Weber and Klippel-Trénaunay
38 RENAL HEMANGIOMA 90% arise from the renal pyramids or the pelvis CT Noncontrast lobulated isoattenuating mass phleboliths uncommon Post contrast early, intense persistent enhancement Venkata S. RadioGraphics 2010, 30,
39 RENAL HEMANGIOMA MRI T1 hypointense T2 hyperintense Can mimic a complex cyst with enhancing solid components Venkata S. RadioGraphics 2010, 30,
40
41 CYSTIC NEPHROMA Cystic lesion Predominantly perimenopausal women Benign but sarcomatous degeneration has been described
42 CYSTIC NEPHROMA CT Well-demarcated, multilocular cystic lesion with thin septations Enhancing septations Usually without solid components
43 CYSTIC NEPHROMA MRI T2 T1 Gd+ Capsule and septa are hypointense Cystic locules hyperintense Cystic locules may have varying appearance (presence proteins/blood) Septations enhance
44 CYSTIC NEPHROMA Fall under Bosniack category 3 cyst Mimics cystic renal cell carcinoma Managed surgically in the majority of cases
45 CYSTIC NEPHROMA V MIXED EPITHELIAL AND STROMAL TUMOR Very similar clinical and radiological appearance MEST may have more solid components
46 LYMPHANGIOMA Multilocular cystic mass Perinephric or renal sinus region typical Involvement of both kidneys not uncommon Dilated retroperitoneal lymphatics Prasad et al. AJR.2008
47 LYMPHANGIOMA MR T1 hypointense T2 hyperintense Signal intensity of the intracystic fluid may be variable, depending on the presence of hemorrhage/debris/protein Venkata S. RadioGraphics 2010, 30,
48 RENINOMA Juxtaglomerular cell neoplasm Secretes renin Young adults Triad of poorly controlled hypertension hypokalemia high plasma renin activity Typically well-circumscribed cortical tumor Hypovascular on arterial phase - possibly because of renin-induced vasoconstriction
49 MANAGEMENT OF INCIDENTAL MASS
50 INCIDENTAL MASS Establish that the lesion is indeed a mass Mass should demonstrate Tissue with HU > 20 Enhance >20 HU between non contrast and post contrast (beware pseudo-enhancement) >15 HU is equivocal HU measurement can be unreliable
51 INCIDENTAL MASS If difficulty demonstrating enhancement on CT, consider MRI Image subtraction is a useful tool
52 MIMICS OF A NEOPLASM
53
54
55
56
57
58
59
60
61
62
63
64 Fever Leukcytosis Flank pain
65 Other potential mimics include Renal trauma Renal infarction
66 INCIDENTAL RENAL MASS One you have established a true mass is present..
67 INCIDENTAL RENAL MASS Characterize the lesion Identify features that predict benignity
68 INCIDENTAL SOLID RENAL MASS Aside from fat, no single feature predicts benignity Some features should be looked for, but are not specific E.G. Small, hyper-attenuating, homogeneously enhancing, T2 hypointense mass Kim J et al. Radiology 2009 Aug;252(2):441-8
69 INCIDENTAL RENAL MASS Consider management options Do nothing Observe Percutaneous biopsy Surgery/Ablation
70 IMPORTANT CONSIDERATIONS If there is a history of primary extra-renal neoplasm 50% 85% of solitary renal masses are metastatic If multiple solid masses consider multifocal renal cell carcinoma Consider biopsy multiple oncocytomas Can be syndromic lymphoma (but rarely presents only in the kidney)
71 Remainder of the approach to a solid renal mass is largely based on size Most important predictor of aggressive behavior
72 SIZE 13% of all resected solid renal masses are benign However < 3cm 25% benign < 2 cm 30% benign < 1 cm 44% benign Is there an alternative strategy for small solid renal lesions?
73 Incidental solid mass on CT <1 cm 1 3 cm > 3 cm Follow up at months - 12 months - Then yearly If becomes >1cm Hyper-attenuating, homogeneously enhancing Surgery Surgery Consider MRI or biopsy J Am Coll Radiol 2010;7:
74 INCIDENTAL CYSTIC MASS Follows Bosniak categorization In general, size is not a factor
75 Bosniak I + II Bosniak IIF Bosniak III + IV
76 Incidental cystic mass on CT Bosniak I + II Bosniak IIF Bosniak III + IV Benign No follow-up CT/MRI at 6 months 12 months 5 Years Surgery No change = benign Morphologic change Surgery
77 ACTIVE SURVEILLANCE Initially observe selected patients Intervene when specified size or growth rate criteria met When solid lesions undergo active surveillance, approximately 1% will develop metastases Vast majority in lesions which show interval growth Only 1 reported case of 2.4-cm mass progressing to metastases with no increase in tumor size
78 Evidence for active surveillance? Retrospective example Patel et al. BJU 2012 mainly retrospective Delayed Intervention and Surveillance for Small Renal Masses (DISSRM) Register 202 patients with T1a lesions 46 months patients 71 active surveillance 131 surgery 101 active surveillance 226 surgery Median follow-up of 34 months No difference in overall or cancer-specific survival 4 deaths 0 RCC related 4 deaths 1 RCC related Average growth rate = 1mm/year
79 ACTIVE SURVEILLANCE Rate of malignancy in lesions with zero growth is similar to the rate in growing lesions Benign lesions can grow at similar rates to malignant lesions Very rare for lesions without interval growth to metastasize Emerging as an alternate strategy for select patients
80 CONCLUSION Discussed Imaging characteristics of the common benign renal masses Features that can help make a pre operative diagnosis of benignity Mimics of renal mass Management and follow-up of incidentally discovered small renal masses, many of which are benign
81 THANK YOU
Kidney Cancer OVERVIEW
 Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Characterization of small renal lesions: Problem solving with MRI Gary Israel, MD
 Characterization of small renal lesions: Problem solving with MRI Gary Israel, MD With the widespread use of cross-sectional imaging, many renal masses are incidentally found. These need to be accurately
Characterization of small renal lesions: Problem solving with MRI Gary Israel, MD With the widespread use of cross-sectional imaging, many renal masses are incidentally found. These need to be accurately
Renal Cysts What should I do now?
 Renal Cysts What should I do now? Dr Edmund Chiong Asst. Professor & Consultant Department of Urology National University Hospital What are renal cysts? Fluid-filled structures in the kidney that are not
Renal Cysts What should I do now? Dr Edmund Chiong Asst. Professor & Consultant Department of Urology National University Hospital What are renal cysts? Fluid-filled structures in the kidney that are not
Benign Liver Tumors. Cameron Schlegel PGY-1 3/6/2013
 Benign Liver Tumors Cameron Schlegel PGY-1 3/6/2013 Outline Benign Liver Tumors are, in general. Asymptomatic Diagnosed: imaging Treatment: Do no harm Unless Malignant potential Causing symptoms Differential
Benign Liver Tumors Cameron Schlegel PGY-1 3/6/2013 Outline Benign Liver Tumors are, in general. Asymptomatic Diagnosed: imaging Treatment: Do no harm Unless Malignant potential Causing symptoms Differential
CT and MRI features of the Pathologic Subtypes of Papillary Renal Cell Carcinoma. Melissa Price, MD Aoife Kilcoyne, MD Mukesh G.
 CT and MRI features of the Pathologic Subtypes of Papillary Renal Cell Carcinoma Melissa Price, MD Aoife Kilcoyne, MD Mukesh G. Harisinghani, MD Disclosures Neither I nor my immediate family members have
CT and MRI features of the Pathologic Subtypes of Papillary Renal Cell Carcinoma Melissa Price, MD Aoife Kilcoyne, MD Mukesh G. Harisinghani, MD Disclosures Neither I nor my immediate family members have
Something Old, Something New.
 Something Old, Something New. Michelle A. Fajardo, D.O. Loma Linda University Medical Center Clinical Presentation 6 year old boy, presented with hematuria Renal mass demonstrated by ultrasound & CT scan
Something Old, Something New. Michelle A. Fajardo, D.O. Loma Linda University Medical Center Clinical Presentation 6 year old boy, presented with hematuria Renal mass demonstrated by ultrasound & CT scan
CASE OF THE MONTH AUGUST-2015 DR. GURUDUTT GUPTA HEAD HISTOPATHOLOGY
 CASE OF THE MONTH AUGUST-2015 DR. GURUDUTT GUPTA HEAD HISTOPATHOLOGY CASE HISTORY 52Y MALE RIGHT RADICAL NEPHERECTOMY Case of right renal mass with IVC thrombus. History of surgery and RT for right occipital
CASE OF THE MONTH AUGUST-2015 DR. GURUDUTT GUPTA HEAD HISTOPATHOLOGY CASE HISTORY 52Y MALE RIGHT RADICAL NEPHERECTOMY Case of right renal mass with IVC thrombus. History of surgery and RT for right occipital
SEMESTER VI 3 RD YEAR PATHOLOGY KIDNEY TUMORS
 SEMESTER VI 3 RD YEAR PATHOLOGY KIDNEY TUMORS LEARNING OBJECTIVES At the end of the lecture, students should be able to: Know the pathology of renal tumors. RENAL TUMORS RENAL PAPILLARY ADENOMA Common
SEMESTER VI 3 RD YEAR PATHOLOGY KIDNEY TUMORS LEARNING OBJECTIVES At the end of the lecture, students should be able to: Know the pathology of renal tumors. RENAL TUMORS RENAL PAPILLARY ADENOMA Common
Radiologic Evaluation of Renal Cysts
 Eugene K. Cha, HMS III November 2004 Radiologic Evaluation of Renal Cysts Eugene K. Cha, Harvard Medical School III Renal Anatomy Netter FH. Atlas of Human Anatomy, Second Edition. 2001, p 313. 2 HPI:
Eugene K. Cha, HMS III November 2004 Radiologic Evaluation of Renal Cysts Eugene K. Cha, Harvard Medical School III Renal Anatomy Netter FH. Atlas of Human Anatomy, Second Edition. 2001, p 313. 2 HPI:
CONTEMPORARY MANAGEMENT OF RENAL ANGIOMYOLIPOMA
 CONTEMPORARY MANAGEMENT OF RENAL ANGIOMYOLIPOMA Stephen A. Boorjian, MD Professor of Urology Vice Chair of Research Director, Urologic Oncology Fellowship Department of Urology Mayo Clinic, Rochester,
CONTEMPORARY MANAGEMENT OF RENAL ANGIOMYOLIPOMA Stephen A. Boorjian, MD Professor of Urology Vice Chair of Research Director, Urologic Oncology Fellowship Department of Urology Mayo Clinic, Rochester,
Medullary Renal Cell Carcinoma Case Report
 Bahrain Medical Bulletin, Vol. 27, No. 4, December 2005 Medullary Renal Cell Carcinoma Case Report Mohammed Abdulla Al-Tantawi MBBCH, CABS* Abdul Amir Issa MBBCH, CABS*** Mohammed Abdulla MBBCH, CABS**
Bahrain Medical Bulletin, Vol. 27, No. 4, December 2005 Medullary Renal Cell Carcinoma Case Report Mohammed Abdulla Al-Tantawi MBBCH, CABS* Abdul Amir Issa MBBCH, CABS*** Mohammed Abdulla MBBCH, CABS**
Benign Ovarian Masses
 Benign Ovarian Masses Anthony Hanbidge Learning Objectives Describe technique for assessment of ovarian masses Explain importance of transvaginal scan List the common benign masses Specify distinguishing
Benign Ovarian Masses Anthony Hanbidge Learning Objectives Describe technique for assessment of ovarian masses Explain importance of transvaginal scan List the common benign masses Specify distinguishing
Epithelial Tumors of the Kidney Diagnostic Problems and Recently Described Entities
 Pathology of Renal Neoplasia Epithelial Tumors of the Kidney Diagnostic Problems and Recently Described Entities Wael A Sakr, MD Wayne State University School of Medicine CURRENT CLASSIFICATION = EPITHELIAL
Pathology of Renal Neoplasia Epithelial Tumors of the Kidney Diagnostic Problems and Recently Described Entities Wael A Sakr, MD Wayne State University School of Medicine CURRENT CLASSIFICATION = EPITHELIAL
Measure #405: Appropriate Follow-up Imaging for Incidental Abdominal Lesions National Quality Strategy Domain: Effective Clinical Care
 Measure #405: Appropriate Follow-up Imaging for Incidental Abdominal Lesions National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Measure #405: Appropriate Follow-up Imaging for Incidental Abdominal Lesions National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Cystic Neoplasms of the Pancreas: A multidisciplinary approach to the prevention and early detection of invasive pancreatic cancer.
 This lecture is drawn from the continuing medical education program Finding Hope: Prevention, Early Detection and Treatment of Pancreatic Cancer, Nov, 2011. Robert P. Jury, MD Cystic Neoplasms of the Pancreas:
This lecture is drawn from the continuing medical education program Finding Hope: Prevention, Early Detection and Treatment of Pancreatic Cancer, Nov, 2011. Robert P. Jury, MD Cystic Neoplasms of the Pancreas:
MRI of Benign Liver Lesions and Metastatic Disease Characterization with. Gadoxetate Disodium
 MRI of Benign Liver Lesions and Metastatic Disease Characterization with Gadoxetate Disodium Rocky C. Saenz, D.O. Department of Diagnostic Radiology, Botsford Hospital, Farmington Hills, MI Introduction
MRI of Benign Liver Lesions and Metastatic Disease Characterization with Gadoxetate Disodium Rocky C. Saenz, D.O. Department of Diagnostic Radiology, Botsford Hospital, Farmington Hills, MI Introduction
Four Important Facts about Kidney Cancer
 Volume Article.13-11 Publish Date: 24th June 2013 Author(s): MPUH - CRS Team Four Important Facts about Kidney Cancer ARTICLE hhh Muljibhai Patel Urological Hospital (MPUH) Centre For Robotic Surgery (CRS)
Volume Article.13-11 Publish Date: 24th June 2013 Author(s): MPUH - CRS Team Four Important Facts about Kidney Cancer ARTICLE hhh Muljibhai Patel Urological Hospital (MPUH) Centre For Robotic Surgery (CRS)
Renal Pathology Update. Sundus Hussein MD, FRCPC
 Renal Pathology Update Sundus Hussein MD, FRCPC Case History A 45 year old male with incidentally discovered a 3.5 x 3.9 x 2.7 cm renal mass Handling partial nephrectomy Handling partial nephrectomy
Renal Pathology Update Sundus Hussein MD, FRCPC Case History A 45 year old male with incidentally discovered a 3.5 x 3.9 x 2.7 cm renal mass Handling partial nephrectomy Handling partial nephrectomy
Cardiac Masses and Tumors
 Cardiac Masses and Tumors Question: What is the diagnosis? A. Aortic valve myxoma B. Papillary fibroelastoma C. Vegetation from Infective endocarditis D. Thrombus in transit E. None of the above Answer:
Cardiac Masses and Tumors Question: What is the diagnosis? A. Aortic valve myxoma B. Papillary fibroelastoma C. Vegetation from Infective endocarditis D. Thrombus in transit E. None of the above Answer:
RENAL CELL CARCINOMA EPIDEMIOLOGY
 RENAL CELL CARCINOMA: THE 2012 ISUP VANCOUVER CLASSIFICATION David Grignon MD, Indiana University, Indianapolis, IN RENAL CELL CARCINOMA EPIDEMIOLOGY Siegel et al. CaA Cancer J Clin 63:11-30, 2013 1 EPITHELIAL
RENAL CELL CARCINOMA: THE 2012 ISUP VANCOUVER CLASSIFICATION David Grignon MD, Indiana University, Indianapolis, IN RENAL CELL CARCINOMA EPIDEMIOLOGY Siegel et al. CaA Cancer J Clin 63:11-30, 2013 1 EPITHELIAL
Renal Tumors with Eosinophilic Cytoplasm: 2013 Classification. Jesse K. McKenney, MD Associate Head, Surgical Pathology
 Renal Tumors with Eosinophilic Cytoplasm: 2013 Classification Jesse K. McKenney, MD Associate Head, Surgical Pathology Renal Epithelial Neoplasia History 1981: WHO Classification of Renal Neoplasms 1.
Renal Tumors with Eosinophilic Cytoplasm: 2013 Classification Jesse K. McKenney, MD Associate Head, Surgical Pathology Renal Epithelial Neoplasia History 1981: WHO Classification of Renal Neoplasms 1.
THYROID CANCER. I. Introduction
 THYROID CANCER I. Introduction There are over 11,000 new cases of thyroid cancer each year in the US. Females are more likely to have thyroid cancer than men by a ratio of 3:1, and it is more common in
THYROID CANCER I. Introduction There are over 11,000 new cases of thyroid cancer each year in the US. Females are more likely to have thyroid cancer than men by a ratio of 3:1, and it is more common in
Managing Incidental Findings on Abdominal CT: White Paper of the ACR Incidental Findings Committee
 Managing Incidental Findings on Abdominal CT: White Paper of the ACR Incidental Findings Committee Lincoln L. Berland, MD a, Stuart G. Silverman, MD b, Richard M. Gore, MD c, William W. Mayo-Smith, MD
Managing Incidental Findings on Abdominal CT: White Paper of the ACR Incidental Findings Committee Lincoln L. Berland, MD a, Stuart G. Silverman, MD b, Richard M. Gore, MD c, William W. Mayo-Smith, MD
RENAL CANCER PATHOLOGY WHAT REALLY MATTERS? STEWART FLEMING UNIVERSITY OF DUNDEE
 RENAL CANCER PATHOLOGY WHAT REALLY MATTERS? STEWART FLEMING UNIVERSITY OF DUNDEE MAJOR PARADIGM SHIFT IN EARLY 1990S IN UNDERSTANDING RENAL CANCER Molecular differential pathology of renal cell tumours
RENAL CANCER PATHOLOGY WHAT REALLY MATTERS? STEWART FLEMING UNIVERSITY OF DUNDEE MAJOR PARADIGM SHIFT IN EARLY 1990S IN UNDERSTANDING RENAL CANCER Molecular differential pathology of renal cell tumours
Guideline for the Imaging of Patients Presenting with Breast Symptoms incorporating the guideline for the use of MRI in breast cancer
 Guideline for the Imaging of Patients Presenting with Breast Symptoms incorporating the guideline for the use of MRI in breast cancer Version History Version Date Summary of Change/Process 0.1 09.01.11
Guideline for the Imaging of Patients Presenting with Breast Symptoms incorporating the guideline for the use of MRI in breast cancer Version History Version Date Summary of Change/Process 0.1 09.01.11
Angiomyolipoma, Oncocytoma, Translocation Carcinoma, Sarcomatoid RCC. Goh Cheng Hood
 Angiomyolipoma, Oncocytoma, Translocation Carcinoma, Sarcomatoid RCC Goh Cheng Hood Angiomyolipoma Benign renal tumour compose of blood vessels, smooth muscle and adipose tissue. Angio- blood vessel, Myo-
Angiomyolipoma, Oncocytoma, Translocation Carcinoma, Sarcomatoid RCC Goh Cheng Hood Angiomyolipoma Benign renal tumour compose of blood vessels, smooth muscle and adipose tissue. Angio- blood vessel, Myo-
Renal Cell Carcinoma. Background 1. General information. Pathophysiology 1. Pathology of disease. Diagnostics 1. History
 Renal Cell Carcinoma Background 1. General information o Accounts for 2-3 % of all malignancies o 5 variants 75-85% clear cell tumors 12-14% chromophilic 4-6% chromophobic 2-4% oncocytic 1% collecting
Renal Cell Carcinoma Background 1. General information o Accounts for 2-3 % of all malignancies o 5 variants 75-85% clear cell tumors 12-14% chromophilic 4-6% chromophobic 2-4% oncocytic 1% collecting
Cystic renal cell carcinoma rare clinical finding Radiographic variations of tumor/cyst appearance and further diagnostic work-up
 96 Bratisl Lek Listy 2006; 107 (3): 96 100 CASE REPORT Cystic renal cell carcinoma rare clinical finding Radiographic variations of tumor/cyst appearance and further diagnostic work-up Weibl P, Lutter
96 Bratisl Lek Listy 2006; 107 (3): 96 100 CASE REPORT Cystic renal cell carcinoma rare clinical finding Radiographic variations of tumor/cyst appearance and further diagnostic work-up Weibl P, Lutter
Metastatic Renal Cell Carcinoma: Staging and Prognosis of Three Separate Cases.
 Metastatic Renal Cell Carcinoma: Staging and Prognosis of Three Separate Cases. Abstract This paper describes the staging, imaging, treatment, and prognosis of renal cell carcinoma. Three case studies
Metastatic Renal Cell Carcinoma: Staging and Prognosis of Three Separate Cases. Abstract This paper describes the staging, imaging, treatment, and prognosis of renal cell carcinoma. Three case studies
Condi&ons Associated with Macroscopic Fat in the Genitourinary System: A Review From Top to Bo>om
 Condi&ons Associated with Macroscopic Fat in the Genitourinary System: A Review From Top to Bo>om Katryana Hanley- Knutson, MD, Christopher Brady, MD and Ray Dyer, MD Department of Radiology, Wake Forest
Condi&ons Associated with Macroscopic Fat in the Genitourinary System: A Review From Top to Bo>om Katryana Hanley- Knutson, MD, Christopher Brady, MD and Ray Dyer, MD Department of Radiology, Wake Forest
NEOPLASMS OF KIDNEY (RENAL CELL CARCINOMA) And RENAL PELVIS (TRANSITIONAL CELL CARCINOMA)
 And RENAL PELVIS (TRANSITIONAL CELL CARCINOMA)") NEOPLASMS OF KIDNEY (RENAL CELL CARCINOMA) And RENAL PELVIS (TRANSITIONAL CELL CARCINOMA) Merat Esfahani, MD Medical Oncologist, Hematologist Cancer Liaison Physician SwedishAmerican Regional Cancer Center
NEOPLASMS OF KIDNEY (RENAL CELL CARCINOMA) And RENAL PELVIS (TRANSITIONAL CELL CARCINOMA) Merat Esfahani, MD Medical Oncologist, Hematologist Cancer Liaison Physician SwedishAmerican Regional Cancer Center
Radiologic Diagnosis of Spinal Metastases
 September 2002 Radiologic Diagnosis of Spinal Metastases Natalie J. M. Dailey, Harvard Medical Student Year III Our Patient s Presenting Story 70 year old male Presents to the hospital for laparascopic
September 2002 Radiologic Diagnosis of Spinal Metastases Natalie J. M. Dailey, Harvard Medical Student Year III Our Patient s Presenting Story 70 year old male Presents to the hospital for laparascopic
Emerging Subtypes in Renal Cancer. Donna E. Hansel, MD PhD Professor of Pathology, UC San Diego Division Chief, Anatomic Pathology dhansel@ucsd.
 Emerging Subtypes in Renal Cancer Donna E. Hansel, MD PhD Professor of Pathology, UC San Diego Division Chief, Anatomic Pathology dhansel@ucsd.edu Some General Comments Fuhrman nuclear grading clear cell
Emerging Subtypes in Renal Cancer Donna E. Hansel, MD PhD Professor of Pathology, UC San Diego Division Chief, Anatomic Pathology dhansel@ucsd.edu Some General Comments Fuhrman nuclear grading clear cell
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD
 SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
Translocation Renal Cell Carcinomas
 Translocation Renal Cell Carcinomas Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Kidney cancer is not a single disease Clear cell (75%)
Translocation Renal Cell Carcinomas Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Kidney cancer is not a single disease Clear cell (75%)
Radiologic Imaging of Renal Masses
 Radiologic Imaging of Renal Masses Vincent G. Bird and Victoria Y. Bird University of Florida, College of Medicine, Department of Urology and Veteran s Administration Medical Center, Gainesville, Florida
Radiologic Imaging of Renal Masses Vincent G. Bird and Victoria Y. Bird University of Florida, College of Medicine, Department of Urology and Veteran s Administration Medical Center, Gainesville, Florida
Gladwyn Leiman, MCCCh, FIAC, FRCPath Scott Anderson, MD
 Cytology Works shop #5 Gladwyn Leiman, MCCCh, FIAC, FRCPath Scott Anderson, MD Disclosur re information The speakers have no relationship that represents a possible conflict of interest with respect to
Cytology Works shop #5 Gladwyn Leiman, MCCCh, FIAC, FRCPath Scott Anderson, MD Disclosur re information The speakers have no relationship that represents a possible conflict of interest with respect to
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Breast cancer Faculty of Clinical Radiology www.rcr.ac.uk Contents Breast cancer 2 Clinical background 2 Who
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Breast cancer Faculty of Clinical Radiology www.rcr.ac.uk Contents Breast cancer 2 Clinical background 2 Who
MAJOR PARADIGM SHIFT IN EARLY 1990S IN UNDERSTANDING RENAL CANCER
 Renal tumours WHO 4 MAJOR PARADIGM SHIFT IN EARLY 1990S IN UNDERSTANDING RENAL CANCER Molecular differential pathology of renal cell tumours G. KOVACS A CLASSIFICATION BASED ON UNDERSTANDING THE GENETIC
Renal tumours WHO 4 MAJOR PARADIGM SHIFT IN EARLY 1990S IN UNDERSTANDING RENAL CANCER Molecular differential pathology of renal cell tumours G. KOVACS A CLASSIFICATION BASED ON UNDERSTANDING THE GENETIC
POSTMENOPAUSAL ASSESS AND WHAT TO DO
 POSTMENOPAUSAL OVARIAN CYSTS:HOW TO ASSESS AND WHAT TO DO Steven R. Goldstein, MD Professor of Obstetrics and Gynecology Director of Gynecologic Ultrasound Co-Director, Bone Densitometry New York University
POSTMENOPAUSAL OVARIAN CYSTS:HOW TO ASSESS AND WHAT TO DO Steven R. Goldstein, MD Professor of Obstetrics and Gynecology Director of Gynecologic Ultrasound Co-Director, Bone Densitometry New York University
Hepatocellular Carcinoma: A Guide to Screening and Diagnosis
 February 2012 Hepatocellular Carcinoma: A Guide to Screening and Diagnosis Reid Merryman, Harvard Medical School Year III Agenda Hepatocellular carcinoma (HCC) introduction Index patient: clinical presentation
February 2012 Hepatocellular Carcinoma: A Guide to Screening and Diagnosis Reid Merryman, Harvard Medical School Year III Agenda Hepatocellular carcinoma (HCC) introduction Index patient: clinical presentation
Nicole Kounalakis, MD
 Breast Disease: Diagnosis and Management Nicole Kounalakis, MD Assistant Professor of Surgery Goal of Breast Evaluation The goal of breast evaluation is to classify findings as: normal physiologic variations
Breast Disease: Diagnosis and Management Nicole Kounalakis, MD Assistant Professor of Surgery Goal of Breast Evaluation The goal of breast evaluation is to classify findings as: normal physiologic variations
WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS
 WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS This is a patient information booklet providing specific practical information about gall bladder polyps in brief. Its aim is to provide the patient
WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS This is a patient information booklet providing specific practical information about gall bladder polyps in brief. Its aim is to provide the patient
A912: Kidney, Renal cell carcinoma
 A912: Kidney, Renal cell carcinoma General facts of kidney cancer Renal cell carcinoma, a form of kidney cancer that involves cancerous changes in the cells of the renal tubule, is the most common type
A912: Kidney, Renal cell carcinoma General facts of kidney cancer Renal cell carcinoma, a form of kidney cancer that involves cancerous changes in the cells of the renal tubule, is the most common type
Ovarian cysts Diagnosis and Management
 Ovarian cysts Diagnosis and Management Mr P K Athanasias MRCOG Consultant Gynaecologist St Anthony s Hospital pathanasias@gmail.com Introduction ovary is an ovum-producing reproductive organ located in
Ovarian cysts Diagnosis and Management Mr P K Athanasias MRCOG Consultant Gynaecologist St Anthony s Hospital pathanasias@gmail.com Introduction ovary is an ovum-producing reproductive organ located in
Multiple Primary and Histology Site Specific Coding Rules KIDNEY. FLORIDA CANCER DATA SYSTEM MPH Kidney Site Specific Coding Rules
 Multiple Primary and Histology Site Specific Coding Rules KIDNEY 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways to view the Multiple l Primary/Histology
Multiple Primary and Histology Site Specific Coding Rules KIDNEY 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways to view the Multiple l Primary/Histology
Corso di Oncologia Medica, AA 2009-2010 RENAL CELL CARCINOMA
 Corso di Oncologia Medica, AA 2009-2010 RENAL CELL CARCINOMA RENAL CELL CARCINOMA (RCC) 90-95% of malignant renal neoplasms; notable features include: - refractoriness to cytotoxic agents; - infrequent
Corso di Oncologia Medica, AA 2009-2010 RENAL CELL CARCINOMA RENAL CELL CARCINOMA (RCC) 90-95% of malignant renal neoplasms; notable features include: - refractoriness to cytotoxic agents; - infrequent
MANAGEMENT OF BENIGN BONE TUMORS
 MANAGEMENT OF BENIGN BONE TUMORS HISTORY AND EXAMINATION An adequate history and physical examination are the first and most important steps in evaluating a patient with a musculoskeletal tumor PRESENTING
MANAGEMENT OF BENIGN BONE TUMORS HISTORY AND EXAMINATION An adequate history and physical examination are the first and most important steps in evaluating a patient with a musculoskeletal tumor PRESENTING
Frequently Asked Questions About Ovarian Cancer
 Media Contact: Gerri Gomez Howard Cell: 303-748-3933 gerri@gomezhowardgroup.com Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Media Contact: Gerri Gomez Howard Cell: 303-748-3933 gerri@gomezhowardgroup.com Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014
 Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014 Prof. Dr. Chris Verslype, Leuven Prof. Dr. Aurel Perren, Bern Menue Challenges: 1. Gastric NET 2. Appendiceal NET 3. Rectal NET SEER,
Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014 Prof. Dr. Chris Verslype, Leuven Prof. Dr. Aurel Perren, Bern Menue Challenges: 1. Gastric NET 2. Appendiceal NET 3. Rectal NET SEER,
Ovarian Torsion: Sonographic Evaluation
 J Clin Ultrasound 17:327-332, June 1989 Ovarian Torsion: Sonographic Evaluation Mark A. Helvie, MD,* and Terry M. Silver, MDI Abstract: The sonographic and clinical findings of 13 patients with surgically
J Clin Ultrasound 17:327-332, June 1989 Ovarian Torsion: Sonographic Evaluation Mark A. Helvie, MD,* and Terry M. Silver, MDI Abstract: The sonographic and clinical findings of 13 patients with surgically
Clinical Management Guideline Management of locally advanced or recurrent Renal cell carcinoma. Protocol for Planning and Treatment
 Protocol for Planning and Treatment The process to be followed in the management of: LOCALLY ADVANCED OR METASTATIC RENAL CELL CARCINOMA Patient information given at each stage following agreed information
Protocol for Planning and Treatment The process to be followed in the management of: LOCALLY ADVANCED OR METASTATIC RENAL CELL CARCINOMA Patient information given at each stage following agreed information
Sternotomy and removal of the tumor
 Sternotomy and removal of the tumor All thymomas originate from epithelial thymic cells 4% of them consist of a pure population of epithelial cells Most have mixed populations of lymphoid cells to a
Sternotomy and removal of the tumor All thymomas originate from epithelial thymic cells 4% of them consist of a pure population of epithelial cells Most have mixed populations of lymphoid cells to a
DIFFERENTIATION OF RENAL CELL CARCINOMA SUBTYPES BY MULTISLICE COMPUTERIZED TOMOGRAPHY
 0022-5347/05/1742-0451/0 Vol. 174, 451 455, August 2005 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000165341.08396.a9 DIFFERENTIATION
0022-5347/05/1742-0451/0 Vol. 174, 451 455, August 2005 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000165341.08396.a9 DIFFERENTIATION
KIDNEY FUNCTION RELATION TO SIZE OF THE TUMOR IN RENAL CELL CANCINOMA
 KIDNEY FUNCTION RELATION TO SIZE OF THE TUMOR IN RENAL CELL CANCINOMA O.E. Stakhvoskyi, E.O. Stakhovsky, Y.V. Vitruk, O.A. Voylenko, P.S. Vukalovich, V.A. Kotov, O.M. Gavriluk National Canсer Institute,
KIDNEY FUNCTION RELATION TO SIZE OF THE TUMOR IN RENAL CELL CANCINOMA O.E. Stakhvoskyi, E.O. Stakhovsky, Y.V. Vitruk, O.A. Voylenko, P.S. Vukalovich, V.A. Kotov, O.M. Gavriluk National Canсer Institute,
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER
 GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
Renal Cell Carcinoma The New Frontier (To boldly go... ) Sean A. Pierre, MD, RCPSC (Urology)
 Sean A. Pierre, MD, RCPSC (Urology)") The New Frontier (To boldly go... ) Sean A. Pierre, MD, RCPSC (Urology) QUEENSWAY CARLETON HOSPITAL DIVISION OF UROLOGY NEPEAN, ON, CANADA Disclosures None Objectives Advances in the field of Renal Cell
The New Frontier (To boldly go... ) Sean A. Pierre, MD, RCPSC (Urology) QUEENSWAY CARLETON HOSPITAL DIVISION OF UROLOGY NEPEAN, ON, CANADA Disclosures None Objectives Advances in the field of Renal Cell
Comparison of CT analyses of primary renal cell carcinoma and of metastatic neoplasms of the kidney
 Comparison of CT analyses of primary renal cell carcinoma and of metastatic neoplasms of the kidney Ingrid Prkačin, Slavica Naumovski-Mihalić, Nives Dabo, Iva Palčić, Svetozar Vujanić, Zdravko Babić Department
Comparison of CT analyses of primary renal cell carcinoma and of metastatic neoplasms of the kidney Ingrid Prkačin, Slavica Naumovski-Mihalić, Nives Dabo, Iva Palčić, Svetozar Vujanić, Zdravko Babić Department
OBJECTIVES By the end of this segment, the community participant will be able to:
 Cancer 101: Cancer Diagnosis and Staging Linda U. Krebs, RN, PhD, AOCN, FAAN OCEAN Native Navigators and the Cancer Continuum (NNACC) (NCMHD R24MD002811) Cancer 101: Diagnosis & Staging (Watanabe-Galloway
Cancer 101: Cancer Diagnosis and Staging Linda U. Krebs, RN, PhD, AOCN, FAAN OCEAN Native Navigators and the Cancer Continuum (NNACC) (NCMHD R24MD002811) Cancer 101: Diagnosis & Staging (Watanabe-Galloway
The Lewin Group undertook the following steps to identify the guidelines relevant to the 11 targeted procedures:
 Guidelines The following is a list of proposed medical specialty guidelines that have been found for the 11 targeted procedures to be included in the Medicare Imaging Demonstration. The list includes only
Guidelines The following is a list of proposed medical specialty guidelines that have been found for the 11 targeted procedures to be included in the Medicare Imaging Demonstration. The list includes only
Spleen. Anatomy. (Effective February 2007) (1%-5%) Normal. Related Anatomy Anterior to spleen. Medial border. Posteriorly
 (1%-5%) Normal. Related Anatomy Anterior to spleen. Medial border. Posteriorly") Spleen (Effective February 2007) (1%-5%) Anatomy Normal Intraperitoneal, except hilum Left hypochondrium Left hemidiaphragm superior generally considered to be ovoid, with a convex superior and a concave
Spleen (Effective February 2007) (1%-5%) Anatomy Normal Intraperitoneal, except hilum Left hypochondrium Left hemidiaphragm superior generally considered to be ovoid, with a convex superior and a concave
Frozen Section Diagnosis
 Frozen Section Diagnosis Dr Catherine M Corbishley Honorary Consultant Histopathologist St George s Healthcare NHS Trust and lead examiner final FRCPath Practical 2008-2011 Frozen Section Diagnosis The
Frozen Section Diagnosis Dr Catherine M Corbishley Honorary Consultant Histopathologist St George s Healthcare NHS Trust and lead examiner final FRCPath Practical 2008-2011 Frozen Section Diagnosis The
Histologic Subtypes of Renal Cell Carcinoma
 Histologic Subtypes of Renal Cell Carcinoma M. Scott Lucia, MD Associate Professor Chief of Genitourinary and Renal Pathology Director, Prostate Diagnostic Laboratory Dept. of Pathology University of Colorado
Histologic Subtypes of Renal Cell Carcinoma M. Scott Lucia, MD Associate Professor Chief of Genitourinary and Renal Pathology Director, Prostate Diagnostic Laboratory Dept. of Pathology University of Colorado
Study of minor abnormalities. Minor adrenal abnormalities. Example. Example. Pseudoadrenal mass. Teaching point. Minor thickening or nodularity of
 Pitfalls in Genitourinary Imaging Objectives Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Review sources of error in GU imaging
Pitfalls in Genitourinary Imaging Objectives Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Review sources of error in GU imaging
CHARACTERSTIC RADIOGRAPHIC APPEARANCE
 OSTEOLYTIC LESIONS APPROACH AGE Metastatic Neuroblastoma in infant and young child. Metastases and multiple myeloma in middle aged and elderly. Ewing s sarcoma and simple bone cyst in children and teens.
OSTEOLYTIC LESIONS APPROACH AGE Metastatic Neuroblastoma in infant and young child. Metastases and multiple myeloma in middle aged and elderly. Ewing s sarcoma and simple bone cyst in children and teens.
How I Do It: Evaluating Renal Masses 1
 HowIDoIt Radiology Gary M. Israel, MD Morton A. Bosniak, MD Published online 10.1148/radiol.2362040218 Radiology 2005; 236:441 450 Abbreviations: ROI region of interest 3D three-dimensional 1 From the
HowIDoIt Radiology Gary M. Israel, MD Morton A. Bosniak, MD Published online 10.1148/radiol.2362040218 Radiology 2005; 236:441 450 Abbreviations: ROI region of interest 3D three-dimensional 1 From the
OVARIAN CYSTS. Types of Ovarian Cysts There are many types of ovarian cysts and these can be categorized into functional and nonfunctional
 OVARIAN CYSTS Follicular Cyst Ovarian cysts are fluid-filled sacs that form within or on the ovary. The majority of these cysts are functional meaning they usually form during a normal menstrual cycle.
OVARIAN CYSTS Follicular Cyst Ovarian cysts are fluid-filled sacs that form within or on the ovary. The majority of these cysts are functional meaning they usually form during a normal menstrual cycle.
Radiologic Evaluation of Renal Cell Carcinoma
 Radiologic Evaluation of Renal Cell Carcinoma Teresa Kim, Harvard Medical School Year III Objectives Our patient: Initial presentation Differential diagnosis: Solid renal mass Background: Renal cell carcinoma
Radiologic Evaluation of Renal Cell Carcinoma Teresa Kim, Harvard Medical School Year III Objectives Our patient: Initial presentation Differential diagnosis: Solid renal mass Background: Renal cell carcinoma
RENAL ANGIOMYOLIPOMA EMBOLIZATION
 RENAL ANGIOMYOLIPOMA EMBOLIZATION The information about renal angiomyolipomas on the next several pages includes questions commonly asked about the embolization procedure. Please take a few moments to
RENAL ANGIOMYOLIPOMA EMBOLIZATION The information about renal angiomyolipomas on the next several pages includes questions commonly asked about the embolization procedure. Please take a few moments to
LIVER CANCER AND TUMOURS
 LIVER CANCER AND TUMOURS LIVER CANCER AND TUMOURS Healthy Liver Cirrhotic Liver Tumour What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood
LIVER CANCER AND TUMOURS LIVER CANCER AND TUMOURS Healthy Liver Cirrhotic Liver Tumour What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood
Case Report. Central Neurocytoma. Fotis Souslian, MD; Dino Terzic, MD; Ramachandra Tummala, MD. Department of Neurosurgery, University of Minnesota
 1 Case Report Central Neurocytoma Fotis, MD; Dino Terzic, MD; Ramachandra Tummala, MD Department of Neurosurgery, University of Minnesota Case This is a previously healthy 20 year old female, with 3 months
1 Case Report Central Neurocytoma Fotis, MD; Dino Terzic, MD; Ramachandra Tummala, MD Department of Neurosurgery, University of Minnesota Case This is a previously healthy 20 year old female, with 3 months
Breast Cancer: from bedside and grossing room to diagnoses and beyond. Adriana Corben, M.D.
 Breast Cancer: from bedside and grossing room to diagnoses and beyond Adriana Corben, M.D. About breast anatomy Breasts are special organs that develop in women during puberty when female hormones are
Breast Cancer: from bedside and grossing room to diagnoses and beyond Adriana Corben, M.D. About breast anatomy Breasts are special organs that develop in women during puberty when female hormones are
Ovarian Cysts Made Simple Michael East. Oxford Clinic
 Ovarian Cysts Made Simple Michael East Oxford Clinic Objectives of this talk To understand risk of malignancy and thus not fear it Practical advice for follow up of asymptomatic cysts Practical advice
Ovarian Cysts Made Simple Michael East Oxford Clinic Objectives of this talk To understand risk of malignancy and thus not fear it Practical advice for follow up of asymptomatic cysts Practical advice
Your Guide to Express Critical Illness Insurance Definitions
 Your Guide to Express Critical Illness Insurance Definitions Your Guide to EXPRESS Critical Illness Insurance Definitions This guide to critical illness definitions will help you understand the illnesses
Your Guide to Express Critical Illness Insurance Definitions Your Guide to EXPRESS Critical Illness Insurance Definitions This guide to critical illness definitions will help you understand the illnesses
Evaluation and Management of the Breast Mass. Gary Dunnington,, M.D. Department of Surgery Internal Medicine Ambulatory Conference December 4, 2003
 Evaluation and Management of the Breast Mass Gary Dunnington,, M.D. Department of Surgery Internal Medicine Ambulatory Conference December 4, 2003 Common Presentations of Breast Disease Breast Mass Abnormal
Evaluation and Management of the Breast Mass Gary Dunnington,, M.D. Department of Surgery Internal Medicine Ambulatory Conference December 4, 2003 Common Presentations of Breast Disease Breast Mass Abnormal
Primary -Benign - Malignant Secondary
 TUMOURS OF THE LUNG Primary -Benign - Malignant Secondary The incidence of lung cancer has been increasing almost logarithmically and is now reaching epidemic levels. The overall cure rate is very low
TUMOURS OF THE LUNG Primary -Benign - Malignant Secondary The incidence of lung cancer has been increasing almost logarithmically and is now reaching epidemic levels. The overall cure rate is very low
The TV Series. www.healthybodyhealthymind.com INFORMATION TELEVISION NETWORK
 The TV Series www.healthybodyhealthymind.com Produced By: INFORMATION TELEVISION NETWORK ONE PARK PLACE 621 NW 53RD ST BOCA RATON, FL 33428 1-800-INFO-ITV www.itvisus.com 2005 Information Television Network.
The TV Series www.healthybodyhealthymind.com Produced By: INFORMATION TELEVISION NETWORK ONE PARK PLACE 621 NW 53RD ST BOCA RATON, FL 33428 1-800-INFO-ITV www.itvisus.com 2005 Information Television Network.
The WHO Classification of Renal Tumors and Common Issues in TNM Staging for Renal Cell Carcinoma
 The WHO Classification of Renal Tumors and Common Issues in TNM Staging for Renal Cell Carcinoma Steven Shen, M.D.,Ph.D. Staff Pathologist and Assistant Member The Methodsit Hospital and Research Institute
The WHO Classification of Renal Tumors and Common Issues in TNM Staging for Renal Cell Carcinoma Steven Shen, M.D.,Ph.D. Staff Pathologist and Assistant Member The Methodsit Hospital and Research Institute
MRI of the Uterus BENIGN. Jeffrey C. Weinreb, M.D. FACR jeffrey.weinreb@yale.edu Yale University School of Medicine
 MRI of the Uterus BENIGN Jeffrey C. Weinreb, M.D. FACR jeffrey.weinreb@yale.edu Yale University School of Medicine Normal Anatomy M Junctional JZ Zone EE Junctional Zone is the inner layer or the myometrium
MRI of the Uterus BENIGN Jeffrey C. Weinreb, M.D. FACR jeffrey.weinreb@yale.edu Yale University School of Medicine Normal Anatomy M Junctional JZ Zone EE Junctional Zone is the inner layer or the myometrium
Objectives. Mylene T. Truong, MD. Malignant Pleural Mesothelioma Background
 Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Term Critical Illness Insurance
 Term Critical Illness Insurance PRODUCT GUIDE 5368-01A-JUL14 ASSUMPTION LIFE This document is a summary of the various features of Assumption Life's products. It is neither a contract nor an insurance
Term Critical Illness Insurance PRODUCT GUIDE 5368-01A-JUL14 ASSUMPTION LIFE This document is a summary of the various features of Assumption Life's products. It is neither a contract nor an insurance
Catheter Embolization and YOU
 Catheter Embolization and YOU What is catheter embolization? Embolization therapy is a minimally invasive (non-surgical) treatment that occludes or blocks one or more blood vessels or vascular channels
Catheter Embolization and YOU What is catheter embolization? Embolization therapy is a minimally invasive (non-surgical) treatment that occludes or blocks one or more blood vessels or vascular channels
Introduction: Tumor Swelling / new growth / mass. Two types of growth disorders: Non-Neoplastic. Secondary / adaptation due to other cause.
 Disorders of Growth Introduction: Tumor Swelling / new growth / mass Two types of growth disorders: Non-Neoplastic Secondary / adaptation due to other cause. Neoplastic. Primary growth abnormality. Non-Neoplastic
Disorders of Growth Introduction: Tumor Swelling / new growth / mass Two types of growth disorders: Non-Neoplastic Secondary / adaptation due to other cause. Neoplastic. Primary growth abnormality. Non-Neoplastic
Breast Ultrasound: Benign vs. Malignant Lesions
 October 25-November 19, 2004 Breast Ultrasound: Benign vs. Malignant Lesions Jill Steinkeler,, Tufts University School of Medicine IV Breast Anatomy Case Presentation-Patient 1 62 year old woman with a
October 25-November 19, 2004 Breast Ultrasound: Benign vs. Malignant Lesions Jill Steinkeler,, Tufts University School of Medicine IV Breast Anatomy Case Presentation-Patient 1 62 year old woman with a
Metastatic Prostate Cancer Causing Complete Obstruction of the IVC
 Department of Radiology Henry Ford Health System Detroit, Michigan Metastatic Prostate Cancer Causing Complete Obstruction of the IVC Jennifer Johnston MSIII, Wayne State Medical School Stage 4 Metastatic
Department of Radiology Henry Ford Health System Detroit, Michigan Metastatic Prostate Cancer Causing Complete Obstruction of the IVC Jennifer Johnston MSIII, Wayne State Medical School Stage 4 Metastatic
Cervical Cancer The Importance of Cervical Screening and Vaccination
 Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
ProSono Copyright 2006. Ovarian Pathology
 Ovarian Pathology Physiologic cysts: Functional cysts Pathology: A simple cyst is a sac containing fluid or semi-solid material. Physiologic cysts are generic types of hormonally active cysts that result
Ovarian Pathology Physiologic cysts: Functional cysts Pathology: A simple cyst is a sac containing fluid or semi-solid material. Physiologic cysts are generic types of hormonally active cysts that result
Pancreatic masses: What is there besides cancer
 Pancreatic masses: What is there besides cancer Poster No.: C-0201 Congress: ECR 2010 Type: Educational Exhibit Topic: Abdominal Viscera (Solid Organs) Authors: M. A. Portilha, C. Ruivo, I. Santiago, M.
Pancreatic masses: What is there besides cancer Poster No.: C-0201 Congress: ECR 2010 Type: Educational Exhibit Topic: Abdominal Viscera (Solid Organs) Authors: M. A. Portilha, C. Ruivo, I. Santiago, M.
Cystic Lung Diseases. Melissa Price Gillian Lieberman, MD Advanced Radiology Clerkship Beth Israel Deaconess Medical Center November, 2008
 Cystic Lung Diseases Melissa Price Gillian Lieberman, MD Advanced Radiology Clerkship Beth Israel Deaconess Medical Center November, 2008 How do we define a cyst of the lung? Hansell DM, Bankier AA, MacMahon
Cystic Lung Diseases Melissa Price Gillian Lieberman, MD Advanced Radiology Clerkship Beth Israel Deaconess Medical Center November, 2008 How do we define a cyst of the lung? Hansell DM, Bankier AA, MacMahon
.org. Osteochondroma. Solitary Osteochondroma
 Osteochondroma Page ( 1 ) An osteochondroma is a benign (noncancerous) tumor that develops during childhood or adolescence. It is an abnormal growth that forms on the surface of a bone near the growth
Osteochondroma Page ( 1 ) An osteochondroma is a benign (noncancerous) tumor that develops during childhood or adolescence. It is an abnormal growth that forms on the surface of a bone near the growth
Mammography Education, Inc.
 Mammography Education, Inc. 2011 LÁSZLÓ TABÁR, M.D.,F.A.C.R (Hon) 3D image of a milk duct MULTIMODALITY DETECTION and DIAGNOSIS of BREAST DISEASES PRAGUE, Czech Republic Crown Plaza, Prague June 29 - July
Mammography Education, Inc. 2011 LÁSZLÓ TABÁR, M.D.,F.A.C.R (Hon) 3D image of a milk duct MULTIMODALITY DETECTION and DIAGNOSIS of BREAST DISEASES PRAGUE, Czech Republic Crown Plaza, Prague June 29 - July
MRI of Bone Marrow Radiologic-Pathologic Correlation
 MRI of Bone Marrow Radiologic-Pathologic Correlation Marilyn J. Siegel, M.D. Mallinckrodt Institute of Radiology Washington University School of Medicine St. Louis, MO and Visiting Scientist, AFIP, Washington,
MRI of Bone Marrow Radiologic-Pathologic Correlation Marilyn J. Siegel, M.D. Mallinckrodt Institute of Radiology Washington University School of Medicine St. Louis, MO and Visiting Scientist, AFIP, Washington,
Kidney Cancer (Adult) - Renal Cell Carcinoma What is cancer?
 - Renal Cell Carcinoma What is cancer?") Kidney Cancer (Adult) - Renal Cell Carcinoma What is cancer? The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early
Kidney Cancer (Adult) - Renal Cell Carcinoma What is cancer? The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early
Accurate Differentiation of Focal Nodular Hyperplasia from Hepatic Adenoma at Gadobenate Dimeglumine enhanced MR Imaging: Prospective Study 1
 Luigi Grazioli, MD Giovanni Morana, MD Miles A. Kirchin, PhD Günther Schneider, MD Published online before print 10.1148/radiol.2361040338 Radiology 2005; 236:166 177 Abbreviations: BOPTA benzyloxypropionictetraacetate
Luigi Grazioli, MD Giovanni Morana, MD Miles A. Kirchin, PhD Günther Schneider, MD Published online before print 10.1148/radiol.2361040338 Radiology 2005; 236:166 177 Abbreviations: BOPTA benzyloxypropionictetraacetate
Malignant Pleural Diseases Advances Clinicians Should Know F Gleeson
 Malignant Pleural Diseases Advances Clinicians Should Know F Gleeson The following relevant disclosures, conflicts of interest and/ or financial relationships exist related to this presentation: Consultant
Malignant Pleural Diseases Advances Clinicians Should Know F Gleeson The following relevant disclosures, conflicts of interest and/ or financial relationships exist related to this presentation: Consultant
Male. Female. Death rates from lung cancer in USA
 Male Female Death rates from lung cancer in USA Smoking represents an interesting combination of an entrenched industry and a clearly drug-induced cancer Tobacco Use in the US, 1900-2000 5000 100 Per Capita
Male Female Death rates from lung cancer in USA Smoking represents an interesting combination of an entrenched industry and a clearly drug-induced cancer Tobacco Use in the US, 1900-2000 5000 100 Per Capita
Hepatocellular Carcinoma (HCC)
") Abhishek Vadalia Introduction Chemoembolization is being used with increasing frequency in the treatment of solid hepatic tumors such as Hepatocellular Carinoma (HCC) & rare Cholangiocellular Carcinoma
Abhishek Vadalia Introduction Chemoembolization is being used with increasing frequency in the treatment of solid hepatic tumors such as Hepatocellular Carinoma (HCC) & rare Cholangiocellular Carcinoma
The evolving pathology of solitary fibrous tumours. Luciane Dreher Irion MREH / CMFT / NSOPS
 The evolving pathology of solitary fibrous tumours Luciane Dreher Irion MREH / CMFT / NSOPS Historical review Haemangiopericytoma (HPC) first described primarily as a soft tissue vascular tumour of pericytic
The evolving pathology of solitary fibrous tumours Luciane Dreher Irion MREH / CMFT / NSOPS Historical review Haemangiopericytoma (HPC) first described primarily as a soft tissue vascular tumour of pericytic
D. FREQUENTLY ASKED QUESTIONS
 ACR BI-RADS ATLAS D. FREQUENTLY ASKED QUESTIONS 1. Under MQSA, is it necessary to include a numeric assessment code (i.e., 0, 1, 2, 3, 4, 5, or 6) in addition to the assessment category in all mammography
ACR BI-RADS ATLAS D. FREQUENTLY ASKED QUESTIONS 1. Under MQSA, is it necessary to include a numeric assessment code (i.e., 0, 1, 2, 3, 4, 5, or 6) in addition to the assessment category in all mammography