Fluids and Electrolytes. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
|
|
|
- Lester O’Neal’
- 7 years ago
- Views:
Transcription
1 Fluids and Electrolytes Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
2 Body Fluid Compartments
3 Total Body Water Approximates 60% of total body weight Composed of the intracellular and extracellular compartments The intracellular compartment or intracellular volume (ICV) constitutes 40% of total body weight Extracellular volume (ECV) makes up the remaining 20%
4 ECV Composed of interstitial fluid (IF) and the intravascular or plasma volume (PV) The PV constitutes 25% of ECV (5% of total body weight) remainder is IF Red cell volume, approximately 2 to 3% of TBW, is part of the ICV Total blood volume is approximately 7 to 8% of total body weight
5 Requirements Sufficient water is required to replace obligatory GU losses of approximately 1L/day and GI losses of ml/day Insensible water losses must also be considered in estimating maintenance fluid - Amount to 8 to 12ml/kg/day - Equally divided into respiratory and cutaneous water loss - Cutaneous losses increase by 10% for each degree of temperature greater than 37 C
6 Electrolytes Daily sodium intake approaches 100 to 250mEq/day Balanced by sodium losses in sweat, stool, and urine Renal conservation of sodium is extraordinary In cases of profound volume depletion, urinary losses of sodium may be less than 1mEq/day
7 Electrolytes In the perioperative period, adequate maintenance of sodium may be achieved with an intake of 1 to 2mEq/kg/day Normal potassium intake is approximately 40 to 120mEq/day 10-15% is excreted as normal urinary losses With normal renal function, body potassium stores can be maintained with an intake of approximately 0.5 to 1.0mEq/kg/day

8

9
10 Perioperative Fluid Requirements
11 Perioperative Appropriate management of fluids and electrolytes in the perioperative period requires a flexible yet systematic approach Ensures that fluid administration is appropriately tailored to the patient's changing requirements
12 Perioperative The amount of fluids administered in the immediate post-op period must take into account the existing deficit, maintenance requirements, and any ongoing losses Estimation of the existing deficit must incorporate an approximation of intra-op blood loss as well as fluid losses from evaporative and third-space fluid sequestration
13 Losses Extravascular fluid sequestration represents an important source of intra-op fluid loss Extensive dissection at the operative site induces a localized capillary leak, resulting in extravasation of intravascular fluid into the interstitium with edema formation The loss of intravascular volume via this route depends on the extent of exposure and degree of dissection
14 Losses For example, estimated intravascular fluid losses associated with IHR are 4ml/kg/h, while losses during AAA repair may be as high as 8ml/kg/h This capillary leak may persist as long as 24h into the post-op period and should be considered as part of ongoing losses in the immediate post-op period
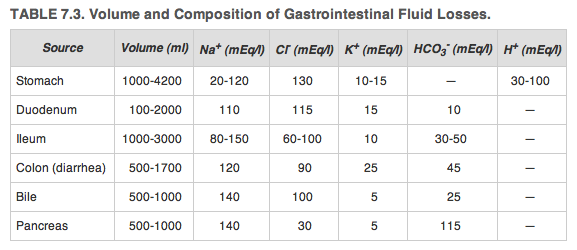
15 Losses GI losses (stomas, tubes/drains, or fistulae) comprise ongoing fluid losses These losses may be accurately estimated by closely following recorded hourly outputs The electrolyte composition of the output depends on the source of effluent Replacement fluids should be chosen to best approximate the composition of the ongoing losses
16
17 Post-op Post-op fluid orders should take into account the overall fluid balance in the OR as an estimate of the existing deficit along with maintenance fluid requirements and any ongoing losses The preferred approach is to reassess the patient frequently to determine volume status
18 Post-op Evaluation of heart rate, blood pressure, and most importantly, hourly urine output provides an excellent measure of intravascular volume status Orders for IVF should be rewritten frequently to maintain a normal heart rate, a urine output of approximately 1ml/kg/h, and adequate blood pressure
19 Disorders of Sodium Homeostasis
20 Sodium Maintenance of a normal serum [sodium] is intimately associated with control of plasma osmolarity P osm = 2 Plasma [Na + ] + [Gluc]/20 + [BUN]/3 Plasma [Na + ] alone provides no information about the total content of sodium in the body but simply provides an estimate of the relative amounts of free water and sodium
21 Osmolarity Maintenance of the plasma osmolarity within normal limits depends on the ability of the kidneys to excrete water, thus preventing hypoosmolarity, and on a normal thirst mechanism with access to water to prevent hypernatremia The ability to excrete maximally dilute urine (<100mOsm/kg) allows the kidneys to excrete in excess of 18L of water per day
22 Osmolarity In the presence of normal renal perfusion and intact renal function, ADH is the principal regulator of serum osmolarity 1-2% reduction in P osm maximally inhibits ADH release maximally dilute urine 1-2% increase in P osm or a 5-10% decrease in blood volume or pressure stimulates ADH With both a low P osm and blood volume or pressure, the latter effect will dominate
23 Hyponatremia Begins with an assessment of the serum osmolarity if serum osmolarity is high, then it is important to consider the possibility of other effective plasma osmoles Hyperglycemia shifts H 2 O from cells, leading to dilutional hyponatremia f or every 100mg/dl rise in glucose the [Na + ] falls by 1.3mEq/l
24 Pseudohyponatremia In rare cases, the serum osmolarity may be normal This phenomenon is referred to as pseudohyponatremia and is caused by hyperlipidemia or hyperproteinemia It is an artifact of the laboratory assay
25 Hyponatremia More frequently, a low [Na + ] will be associated with reduced plasma osmolarity The etiology and treatment of hypoosmolar hyponatremia may be classified into 3 groups depending on the ECV status of the patient
26 Hypovolemic Hyponatremia Most common causes are Na + loss A reduction in ECV leads to an increase in ADH secretion, impairing the kidney's ability to excrete free water Either administration of Na + -free solutions or the ingestion of free water induced by thirst aggravates the resulting hyponatremia
27 Hypovolemic Hyponatremia Typically, perioperative isotonic losses (plasma, gastric losses) are replaced with hypotonic solutions in the face of mild hypovolemia Treatment involves replenishing the extravascular volume with isotonic fluids in concert with restriction of free water
28 Hypervolemic Hyponatremia Hyponatremia in the presence of an increased extravascular volume Represents the next most common scenario in the perioperative period Edematous states in which there is a reduction in the effective circulating volume Low CO states, cirrhosis, and other hypoalbuminemic states are the more common etiologies
29 Hypervolemic Hyponatremia Both water restriction and Na + restriction are necessary Depending on the severity of the hyponatremia, a loop diuretic may be required to increase both Na + and water loss In most cases, this induces an excess of urinary water loss over Na + loss and should correct the hyponatremia
30 Euvolemic Hyponatremia Patients with a normal ECV status and hypoosmolar hyponatremia SIADH Nausea, pain, and narcotics, all of which are common in the post-op period, may result in SIADH and contribute to post-op hyponatremia
31 SIADH Diagnosis is confirmed by demonstrating a low plasma osmolarity, a less than maximally dilute urine (U osm. > 100mOsm/l), and renal salt wasting (U Na. > 20mEq/l) Treatment includes management of the underlying cause and water restriction Isotonic (0.9%) saline should not be administered to patients with SIADH as it may cause the plasma [Na + ] to fall
32 Treatment The presence of Sx depends on the rate at which hyponatremia occurred Sx of increased ICP from cerebral edema are the most prominent features and may be present at plasma [Na + ] < 125mEq/l if the development of hyponatremia was rapid If the reduction in [Na + ] occurs slowly, then symptoms may not be evident until plasma [Na + ] drops to as low as 110mEq/l
33 Treatment Too rapid correction may result in CPM If the patient is asx or mildly symptomatic, then the goal should be to raise the [Na + ] by approximately 0.5mEq/h If the patient is Sx with coma or convulsions, then more rapid correction is necessary Goal is to administer sufficient Na + until either the symptoms have improved or the plasma [Na + ] has increased by 5mEq/l
34 Treatment The following formula may be used to estimate the amount of Na + required to raise the [Na + ] to a safe level (approximately 120mEq/l) - Na + deficit = 0.60 Lean body weight (kg) (120 - Measured plasma Na + )
35 Hypernatremia Far less common than is hyponatremia Cellular shrinkage caused by fluid shifts from the intracellular space to the extracellular compartment may cause confusion, coma, and intracranial hemorrhage Symptoms are usually not evident below a plasma [Na + ] of 160mEq/l
36 Hypernatremia Occurs as a result of excessive free HOH loss Frequently associated with hypovolemia Excessive insensible losses caused by fever, hyperventilation, and burns or hypotonic fluid losses due to perspiration or severe diarrhea are the principal causes
37 Treatment If hypovolemia is sufficiently severe that tissue perfusion is compromised, then initial therapy should be isotonic saline until tissue perfusion is restored If perfusion is adequate, then 0.5 NS or D5W is sufficient to return plasma [Na + ] to normal
38 Treatment Rapid correction of severe hypernatremia may cause irreversible neurological deficits - Should not be corrected at a rate faster than 0.5 to 1.0mEq/l per hour In the presence of Sx, free water should be administered either to return the plasma [Na] to that documented before the Sx or to reduce the [Na] by about 6mmol/l - Water deficit = TBW {(Plasma [Na] Desired plasma [Na]) - 1}
39 Disorders of Potassium Homeostasis
40 Potassium The major intracellular cation Only 2% is located in the extracellular fluid Slight alterations in plasma [K + ] may have dramatic effects on muscle contraction and nerve conduction as the [gradient] across the plasma membrane is the main determinant of membrane excitability Abnormalities in plasma [K + ] should be treated expeditiously
41 Hypokalemia Usually from GI, kidney or skin losses Cardiac arrhythmias exacerbated with metabolic alkalosis, dig or hypercalcemia ECG = T-wave flattening or inversion and depressed ST segments, followed by U waves and a prolonged QT interval Replacement should be geared toward rapid correction of plasma [K + ], followed by slower repletion of the total body K + deficit
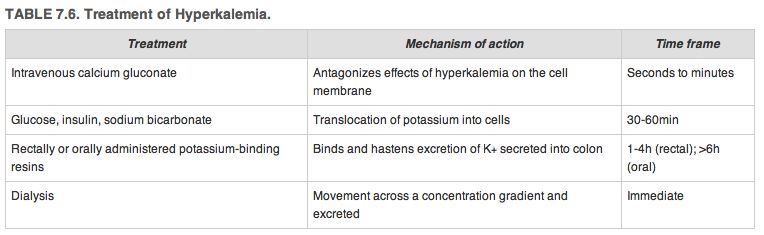
42 Hyperkalemia Main risks are weakness and myocardial irritability ECG = increase in T-wave amplitude, leading to a narrow, peaked symmetrical T wave, followed by reduced P-waves and widening of the QRS If untreated, may eventually cause a sinusoidal ECG complex and ultimately ventricular fibrillation
43
44 Disorders of Mineral Homeostasis
45 Calcium Total body stores are approximately 1000g Almost 99% is in bone The remainder is located within the ECF Either free (40%) or bound to albumin (50%) or other anions such as citrate, lactate, and sulfate Only the free or ionized component is biologically active
46 Calcium Acid-base alterations affect the binding of calcium to albumin Similarly, changes in serum protein levels affect total serum calcium The ionized calcium level can be estimated using the following formula - Ionized calcium (mg/dl) = Total serum calcium (mg/dl) Serum albumin (mg/dl)
47 Hypocalcemia Most frequent cause = low serum albumin In this case, the ionized fraction remains normal, and no treatment is indicated Other causes include acute pancreatitis, massive soft tissue infection, small-bowel fistulae, hypoparathyroidism and massive blood transfusion
48 Hypocalcemia Earliest Sx include numbness or tingling in the circumoral region or at the tips of the fingers Tetany or seizures may arise at more profound levels A positive Trousseau's sign or Chvostek's sign may be suggestive of it Alters myocardial repolarization and results in a prolonged QT interval
49 Hypercalcemia Primary hyperparathyroidism and malignant disease account for 90% of cases Sx include confusion, lethargy, coma, muscle weakness, anorexia, nausea, vomiting, pancreatitis, constipation, renal stones, nephrogenic DI and polyuria ECG = shortened QT interval
50 Magnesium The principal intracellular divalent cation Approximately 50% of total body magnesium is found in bone and is not readily exchangeable Absorption occurs throughout the small intestine and is reabsorbed effectively in the renal tubules
51 Hypomagnesemia May occur because of poor nutritional intake, malabsorption, or increased renal excretion Characterized by neuromuscular and CNS irritability Low serum magnesium levels appear to impair PTH excretion and may induce hypocalcemia refractory to calcium supplementation unless corrected
52 Phosphate The most abundant intracellular anion Only 0.1% of total body phosphorus is in the extracellular fluid compartment As a result, circulating plasma levels do not reflect total body stores
53 Hypophosphatemia May occur as the result of impaired intestinal absorption or increased renal excretion Hyperparathyroidism may induce a drop in serum phosphate levels through an increase in renal excretion Careful monitoring of phosphate should also occur with the administration of parenteral nutrition after prolonged starvation because profound hypophosphatemia may result
54 Hyperphosphatemia Most commonly seen in the setting of impaired renal phosphate excretion In this scenario is frequently associated with hypocalcemia. Similarly, hypoparathyroidism reduces renal phosphate excretion, leading to an increase in serum phosphate levels
55 Acid-Base Abnormalities
56 Metabolic Acidosis Arises as a result of retention (or administration) of fixed acids or the loss of bicarbonate Categorized by the presence or absence of an anion gap (AG) - Addition of fixed acids results in an AG metabolic acidosis - Bicarbonate loss results in a nonag metabolic acidosis

57
58 Metabolic Alkalosis Characterized by an elevated plasma [HCO 3- ] May occur as a result of one of three mechanisms - Loss of acid from the GI tract or urine - Administration of HCO 3- or a precursor, such as citrate (as occurs following massive blood transfusions) - Loss of fluid with a high chloride/bicarb ratio
59 Classification Either chloride sensitive or chloride resistant to the extent that they are reversed by the administration of NS Treatment should be directed toward the underlying cause
60 Summary Surgical patients undergo acute alterations in the volume and composition of fluids in the intracellular and extracellular spaces To a great extent, these changes occur as a result of the patient's underlying disease These alterations are not limited to patients requiring urgent operative intervention
61 Summary Elective surgery may result in dramatic fluid shifts without significant blood loss In addition to changes in fluid volume, surgical patients may develop potentially dangerous fluctuations in concentrations and total body content of important lytes Precise peri-op management of fluids and electrolytes is required to minimize peri-op morbidity and mortality
Interpretation of Laboratory Values
 Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
ACID- BASE and ELECTROLYTE BALANCE. MGHS School of EMT-Paramedic Program 2011
 ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
Dehydration & Overhydration. Waseem Jerjes
 Dehydration & Overhydration Waseem Jerjes Dehydration 3 Major Types Isotonic - Fluid has the same osmolarity as plasma Hypotonic -Fluid has fewer solutes than plasma Hypertonic-Fluid has more solutes than
Dehydration & Overhydration Waseem Jerjes Dehydration 3 Major Types Isotonic - Fluid has the same osmolarity as plasma Hypotonic -Fluid has fewer solutes than plasma Hypertonic-Fluid has more solutes than
Clinical Aspects of Hyponatremia & Hypernatremia
 Clinical Aspects of Hyponatremia & Hypernatremia Case Presentation: History 62 y/o male is admitted to the hospital with a 3 month history of excessive urination (polyuria) and excess water intake up to
Clinical Aspects of Hyponatremia & Hypernatremia Case Presentation: History 62 y/o male is admitted to the hospital with a 3 month history of excessive urination (polyuria) and excess water intake up to
Fluid, Electrolyte, and Acid-Base Balance
 Distribution of Body Fluids Fluid, Electrolyte, and Acid-Base Balance Total body fluids=60% of body weight Extracellular Fluid Comp 20% of Total body wt. Interstitial= 15% of total body wt. Intravascular=5%
Distribution of Body Fluids Fluid, Electrolyte, and Acid-Base Balance Total body fluids=60% of body weight Extracellular Fluid Comp 20% of Total body wt. Interstitial= 15% of total body wt. Intravascular=5%
Adult CCRN/CCRN E/CCRN K Certification Review Course: Endocrine 12/2015. Endocrine 1. Disclosures. Nothing to disclose
 Adult CCRN/CCRN E/CCRN K Certification Review Course: Carol Rauen RN BC, MS, PCCN, CCRN, CEN Disclosures Nothing to disclose 1 Body Harmony disorders and emergencies Body Harmony (cont) Introduction Disorders
Adult CCRN/CCRN E/CCRN K Certification Review Course: Carol Rauen RN BC, MS, PCCN, CCRN, CEN Disclosures Nothing to disclose 1 Body Harmony disorders and emergencies Body Harmony (cont) Introduction Disorders
Disorders of Fluid & Electrolyte Balance. Class 6 Objectives. Starling s Law of the Capillary
 Disorders of Fluid & Electrolyte Balance University of San Francisco Dr. M. Maag 2003 Margaret Maag 1 Class 6 Objectives Upon completion of this lesson, the student will be able to describe the outcomes
Disorders of Fluid & Electrolyte Balance University of San Francisco Dr. M. Maag 2003 Margaret Maag 1 Class 6 Objectives Upon completion of this lesson, the student will be able to describe the outcomes
ELECTROLYTE SOLUTIONS (Continued)
") ELECTROLYTE SOLUTIONS (Continued) Osmolarity Osmotic pressure is an important biologic parameter which involves diffusion of solutes or the transfer of fluids through semi permeable membranes. Per US Pharmacopeia,
ELECTROLYTE SOLUTIONS (Continued) Osmolarity Osmotic pressure is an important biologic parameter which involves diffusion of solutes or the transfer of fluids through semi permeable membranes. Per US Pharmacopeia,
Acid/Base Homeostasis (Part 4)
") Acid/Base Homeostasis (Part 4) Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) 5. The newly formed bicarbonate moves into the plasma.
Acid/Base Homeostasis (Part 4) Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) 5. The newly formed bicarbonate moves into the plasma.
Acid-Base Balance and the Anion Gap
 Acid-Base Balance and the Anion Gap 1. The body strives for electrical neutrality. a. Cations = Anions b. One of the cations is very special, H +, and its concentration is monitored and regulated very
Acid-Base Balance and the Anion Gap 1. The body strives for electrical neutrality. a. Cations = Anions b. One of the cations is very special, H +, and its concentration is monitored and regulated very
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Week 30. Water Balance and Minerals
 Week 30 Water Balance and Minerals Water: more vital to life than food involved in almost every body function is not stored--excreted daily largest single constituent of the human body, averaging 60% of
Week 30 Water Balance and Minerals Water: more vital to life than food involved in almost every body function is not stored--excreted daily largest single constituent of the human body, averaging 60% of
Intravenous Fluids: Composition & Uses. Srinidhi Jayaram, PGY1
 Intravenous Fluids: Composition & Uses Srinidhi Jayaram, PGY1 Body Fluid Compartments Total Body Water (TBW): 50-70% of total body wt. Avg. is greater for males. Decreases with age. Highest in newborn,
Intravenous Fluids: Composition & Uses Srinidhi Jayaram, PGY1 Body Fluid Compartments Total Body Water (TBW): 50-70% of total body wt. Avg. is greater for males. Decreases with age. Highest in newborn,
Problem 24. Pathophysiology of the diabetes insipidus
 Problem 24. Pathophysiology of the diabetes insipidus In order to workout this problem, study pages 240 6, 249 51, 318 9, 532 3 and 886 7 of the Pathophysiology, 5 th Edition. (This problem was based on
Problem 24. Pathophysiology of the diabetes insipidus In order to workout this problem, study pages 240 6, 249 51, 318 9, 532 3 and 886 7 of the Pathophysiology, 5 th Edition. (This problem was based on
Select the one that is the best answer:
 MQ Kidney 1 Select the one that is the best answer: 1) n increase in the concentration of plasma potassium causes increase in: a) release of renin b) secretion of aldosterone c) secretion of H d) release
MQ Kidney 1 Select the one that is the best answer: 1) n increase in the concentration of plasma potassium causes increase in: a) release of renin b) secretion of aldosterone c) secretion of H d) release
Mind the Gap: Navigating the Underground World of DKA. Objectives. Back That Train Up! 9/26/2014
 Mind the Gap: Navigating the Underground World of DKA Christina Canfield, MSN, RN, ACNS-BC, CCRN Clinical Nurse Specialist Cleveland Clinic Respiratory Institute Objectives Upon completion of this activity
Mind the Gap: Navigating the Underground World of DKA Christina Canfield, MSN, RN, ACNS-BC, CCRN Clinical Nurse Specialist Cleveland Clinic Respiratory Institute Objectives Upon completion of this activity
Chapter 23. Composition and Properties of Urine
 Chapter 23 Composition and Properties of Urine Composition and Properties of Urine urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless to deep
Chapter 23 Composition and Properties of Urine Composition and Properties of Urine urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless to deep
INTRAVENOUS FLUIDS. Acknowledgement. Background. Starship Children s Health Clinical Guideline
 Acknowledgements Background Well child with normal hydration Unwell children (+/- abnormal hydration Maintenance Deficit Ongoing losses (e.g. from drains) Which fluid? Monitoring Special Fluids Post-operative
Acknowledgements Background Well child with normal hydration Unwell children (+/- abnormal hydration Maintenance Deficit Ongoing losses (e.g. from drains) Which fluid? Monitoring Special Fluids Post-operative
Quiz Urinary System. 1. The kidneys help regulate blood volume. help control blood pressure. help control ph. All of the above are correct.
 Quiz Urinary System 1. The kidneys help regulate blood volume. help control blood pressure. help control ph. All of the above are correct. 2. The location of the kidneys in relationship to the peritoneal
Quiz Urinary System 1. The kidneys help regulate blood volume. help control blood pressure. help control ph. All of the above are correct. 2. The location of the kidneys in relationship to the peritoneal
Fluid, Electrolyte & ph Balance
 , Electrolyte & ph Balance / Electrolyte / AcidBase Balance Body s: Cell function depends not only on continuous nutrient supply / waste removal, but also on the physical / chemical homeostasis of surrounding
, Electrolyte & ph Balance / Electrolyte / AcidBase Balance Body s: Cell function depends not only on continuous nutrient supply / waste removal, but also on the physical / chemical homeostasis of surrounding
23.4% Sodium Chloride Injection, USP (4 meq/ml) Glass Fliptop Vials Rx only Pharmacy Bulk Package Not for Direct Infusion
 Glass Fliptop Vials Rx only Pharmacy Bulk Package Not for Direct Infusion") CONCENTRATE CAUTION: MUST BE DILUTED FOR I.V. USE. 23.4% Sodium Chloride Injection, USP (4 meq/ml) Glass Fliptop Vials Rx only Pharmacy Bulk Package Not for Direct Infusion DESCRIPTION 23.4% Sodium Chloride
CONCENTRATE CAUTION: MUST BE DILUTED FOR I.V. USE. 23.4% Sodium Chloride Injection, USP (4 meq/ml) Glass Fliptop Vials Rx only Pharmacy Bulk Package Not for Direct Infusion DESCRIPTION 23.4% Sodium Chloride
PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement)
") 1 PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement) PHOSPHATE-SANDOZ PHOSPHATE-SANDOZ Tablets are a high dose phosphate supplement containing sodium phosphate monobasic. The CAS registry number
1 PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement) PHOSPHATE-SANDOZ PHOSPHATE-SANDOZ Tablets are a high dose phosphate supplement containing sodium phosphate monobasic. The CAS registry number
Water Homeostasis. Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.
 Water Homeostasis Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) 1. Water Homeostasis The body maintains a balance of water intake
Water Homeostasis Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) 1. Water Homeostasis The body maintains a balance of water intake
ACID-BASE BALANCE AND ACID-BASE DISORDERS. I. Concept of Balance A. Determination of Acid-Base status 1. Specimens used - what they represent
 ACID-BASE BALANCE AND ACID-BASE DISORDERS I. Concept of Balance A. Determination of Acid-Base status 1. Specimens used - what they represent II. Electrolyte Composition of Body Fluids A. Extracellular
ACID-BASE BALANCE AND ACID-BASE DISORDERS I. Concept of Balance A. Determination of Acid-Base status 1. Specimens used - what they represent II. Electrolyte Composition of Body Fluids A. Extracellular
April 18, 2008 Dr. Alan H. Stephenson Pharmacological and Physiological Science
 Renal Mechanisms for Regulating Urine Concentration April 18, 2008 Dr. Alan H. Stephenson Pharmacological and Physiological Science Amount Filtered Reabsorption is selective Examples of substances that
Renal Mechanisms for Regulating Urine Concentration April 18, 2008 Dr. Alan H. Stephenson Pharmacological and Physiological Science Amount Filtered Reabsorption is selective Examples of substances that
Electrolyte Imbalances
 Imbalance Risk Factors Signs and Symptoms Interventions Electrolyte Imbalances Hypomagne- Malnutrition Tremors Treat underlying causes as semia Alcoholism Cramps prescribed (
Imbalance Risk Factors Signs and Symptoms Interventions Electrolyte Imbalances Hypomagne- Malnutrition Tremors Treat underlying causes as semia Alcoholism Cramps prescribed (
Electrolyte Physiology. Something in the way she moves
 Electrolyte Physiology Something in the way she moves me Electrolyte Movement CONCENTRATION GRADIENT ELECTRICAL GRADIENT DRIVING FORCE NERNST NUMBER (E-ion) CONDUCTANCE (G-ion) PERMEABILITY CHANNELS: small
Electrolyte Physiology Something in the way she moves me Electrolyte Movement CONCENTRATION GRADIENT ELECTRICAL GRADIENT DRIVING FORCE NERNST NUMBER (E-ion) CONDUCTANCE (G-ion) PERMEABILITY CHANNELS: small
Acid-Base Disorders. Jai Radhakrishnan, MD, MS
 Acid-Base Disorders Jai Radhakrishnan, MD, MS 1 Diagnostic Considerations Data points required: ABG: ph, pco 2, HCO 3 Chem-7 panel: anion gap Step 1: Acidemia/alkalemia (Primary disorder) Step 2: Compensation
Acid-Base Disorders Jai Radhakrishnan, MD, MS 1 Diagnostic Considerations Data points required: ABG: ph, pco 2, HCO 3 Chem-7 panel: anion gap Step 1: Acidemia/alkalemia (Primary disorder) Step 2: Compensation
Acid-Base Disorders. Jai Radhakrishnan, MD, MS. Objectives. Diagnostic Considerations. Step 1: Primary Disorder. Formulae. Step 2: Compensation
 Objectives Diagnostic approach to acid base disorders Common clinical examples of acidoses and alkaloses Acid-Base Disorders Jai Radhakrishnan 1 2 Diagnostic Considerations Data points required: ABG: ph,
Objectives Diagnostic approach to acid base disorders Common clinical examples of acidoses and alkaloses Acid-Base Disorders Jai Radhakrishnan 1 2 Diagnostic Considerations Data points required: ABG: ph,
Metabolic alkalosis. ICU Fellowship Training Radboudumc
 Metabolic alkalosis ICU Fellowship Training Radboudumc Case History 28-year-old male Discovered by roommate at home in bewildering state During transport by EMS possible tonicclonic seizure Arrival in
Metabolic alkalosis ICU Fellowship Training Radboudumc Case History 28-year-old male Discovered by roommate at home in bewildering state During transport by EMS possible tonicclonic seizure Arrival in
Management of Ileostomy and other GI Fluid Losses. Morbidity and Mortality Conference April 29, 2005 Kings County Hospital Sajani Shah MD
 Management of Ileostomy and other GI Fluid Losses Morbidity and Mortality Conference April 29, 2005 Kings County Hospital Sajani Shah MD Management of Ileostomy and other GI Fluid Losses Anatomy of Body
Management of Ileostomy and other GI Fluid Losses Morbidity and Mortality Conference April 29, 2005 Kings County Hospital Sajani Shah MD Management of Ileostomy and other GI Fluid Losses Anatomy of Body
Intravenous Fluid Selection
 BENNMC03_0131186116.qxd 3/9/05 18:24 Page 20 seema Seema-3:Desktop Folder:PQ731: CHAPTER 3 Intravenous Fluid Selection LEARNING OBJECTIVES By the end of this chapter, you should be able to: Describe and
BENNMC03_0131186116.qxd 3/9/05 18:24 Page 20 seema Seema-3:Desktop Folder:PQ731: CHAPTER 3 Intravenous Fluid Selection LEARNING OBJECTIVES By the end of this chapter, you should be able to: Describe and
RENAL WATER REGULATION page 1
 page 1 INTRODUCTION TO WATER EXCRETION A. Role of the Kidney: to adjust urine formation rate and urine concentration to maintain 1. body fluid osmolar concentration 2. body fluid volume 3. intravascular
page 1 INTRODUCTION TO WATER EXCRETION A. Role of the Kidney: to adjust urine formation rate and urine concentration to maintain 1. body fluid osmolar concentration 2. body fluid volume 3. intravascular
LECTURE 1 RENAL FUNCTION
 LECTURE 1 RENAL FUNCTION Components of the Urinary System 2 Kidneys 2 Ureters Bladder Urethra Refer to Renal System Vocabulary in your notes Figure 2-1,page10 Kidney Composition Cortex Outer region Contains
LECTURE 1 RENAL FUNCTION Components of the Urinary System 2 Kidneys 2 Ureters Bladder Urethra Refer to Renal System Vocabulary in your notes Figure 2-1,page10 Kidney Composition Cortex Outer region Contains
Essentials of Human Anatomy & Physiology. Chapter 15. The Urinary System. Slides 15.1 15.20. Lecture Slides in PowerPoint by Jerry L.
 Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 15 The Urinary System Slides 15.1 15.20 Lecture Slides in PowerPoint by Jerry L. Cook Functions of the Urinary System Elimination
Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 15 The Urinary System Slides 15.1 15.20 Lecture Slides in PowerPoint by Jerry L. Cook Functions of the Urinary System Elimination
Calcium (serum, plasma, blood)
") Calcium (serum, plasma, blood) 1 Name and description of analyte 1.1 Name of analyte Calcium (total in serum, plasma, ionised in blood (see 2.1 (2)). 1.2 Alternative names None 1.3 NMLC code 1.4 Description
Calcium (serum, plasma, blood) 1 Name and description of analyte 1.1 Name of analyte Calcium (total in serum, plasma, ionised in blood (see 2.1 (2)). 1.2 Alternative names None 1.3 NMLC code 1.4 Description
Learning Objectives. Hyperkalemia Hypomagnesemia Hpermagmesemia
 Fluids and Electrolytes Learning Objectives Total Body Fluid Intravascular Volume Depletion Fluid resuscitation vs. Maintenance IV Fluid Osmolarity of IV Fluids Hyponatremia Hypernatremia Hypokalemia Hyperkalemia
Fluids and Electrolytes Learning Objectives Total Body Fluid Intravascular Volume Depletion Fluid resuscitation vs. Maintenance IV Fluid Osmolarity of IV Fluids Hyponatremia Hypernatremia Hypokalemia Hyperkalemia
Fluid management. The use of intravenous therapy. IV therapy focus CONTINUING PROFESSIONAL DEVELOPMENT
 IV therapy focus CONTINUING PROFESSIONAL DEVELOPMENT By reading this article and writing a practice profile, you can gain ten continuing education points (CEPs). You have up to a year to send in your practice
IV therapy focus CONTINUING PROFESSIONAL DEVELOPMENT By reading this article and writing a practice profile, you can gain ten continuing education points (CEPs). You have up to a year to send in your practice
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
NICE guideline Published: 9 December 2015 nice.org.uk/guidance/ng29
 Intravenous fluid therapy in children and young people in hospital NICE guideline Published: 9 December 2015 nice.org.uk/guidance/ng29 NICE 2015. All rights reserved. Contents Key priorities for implementation...
Intravenous fluid therapy in children and young people in hospital NICE guideline Published: 9 December 2015 nice.org.uk/guidance/ng29 NICE 2015. All rights reserved. Contents Key priorities for implementation...
Isotonic, Hypertonic, Hypotonic or Water Which sports drink is the best for athletes? Fluid Facts for Winners
 Isotonic, Hypertonic, Hypotonic or Water Which sports drink is the best for athletes? Fluid Facts for Winners Why is fluid intake so important for runners? Fluid is a vital part of any athlete s diet for
Isotonic, Hypertonic, Hypotonic or Water Which sports drink is the best for athletes? Fluid Facts for Winners Why is fluid intake so important for runners? Fluid is a vital part of any athlete s diet for
Chapter 16: Disorders of Serum Sodium Concentration in the Elderly Patient
 Chapter 16: Disorders of Serum Sodium Concentration in the Elderly Patient Michael F. Michelis Division of Nephrology, Lenox Hill Hospital, New York, New York HYPONATREMIA Disorders of serum sodium concentration
Chapter 16: Disorders of Serum Sodium Concentration in the Elderly Patient Michael F. Michelis Division of Nephrology, Lenox Hill Hospital, New York, New York HYPONATREMIA Disorders of serum sodium concentration
Lothian Diabetes Handbook MANAGEMENT OF DIABETIC KETOACIDOSIS
 MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
3% Sodium Chloride Injection, USP 5% Sodium Chloride Injection, USP
 PRESCRIBING INFORMATION 3% Sodium Chloride Injection, USP 5% Sodium Chloride Injection, USP IV Fluid and Electrolyte Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision:
PRESCRIBING INFORMATION 3% Sodium Chloride Injection, USP 5% Sodium Chloride Injection, USP IV Fluid and Electrolyte Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision:
How To Treat A Diabetic Coma With Tpn
 GUIDELINES FOR TOTAL PARENTERAL NUTRITION (TPN) IN ADULT BONE MARROW TRANSPLANT PATIENTS TPN Indications TPN is indicated for any patient who is not expected to eat sufficiently for 3-5 days in severe
GUIDELINES FOR TOTAL PARENTERAL NUTRITION (TPN) IN ADULT BONE MARROW TRANSPLANT PATIENTS TPN Indications TPN is indicated for any patient who is not expected to eat sufficiently for 3-5 days in severe
Diabetic Emergencies. David Hill, D.O.
 Diabetic Emergencies David Hill, D.O. Class Outline Diabetic emergency/glucometer training Identify the different signs of insulin shock Diabetic coma, and HHNK Participants will understand the treatment
Diabetic Emergencies David Hill, D.O. Class Outline Diabetic emergency/glucometer training Identify the different signs of insulin shock Diabetic coma, and HHNK Participants will understand the treatment
Paediatric fluids 13/06/05
 Dr Catharine Wilson Consultant Paediatric Anaesthetist Sheffield Children s Hospital. UK Paediatric fluids 13/06/05 Self assessment: Complete these questions before reading the tutorial. Discuss the answers
Dr Catharine Wilson Consultant Paediatric Anaesthetist Sheffield Children s Hospital. UK Paediatric fluids 13/06/05 Self assessment: Complete these questions before reading the tutorial. Discuss the answers
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 Diabetic ketoacidosis in children and young people bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They
Diabetic ketoacidosis in children and young people bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They
Open the Flood Gates Urinary Obstruction and Kidney Stones. Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke
 Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
Body Fluids. Physiology of Fluid. Body Fluids, Kidneys & Renal Physiology
 Pc Remember arterioles have more smooth muscle So SNS effects are greater on arterioles than on venules Net effects: SNS P c (vasoconstriction > venoconstriction) SNS P c (vasodilation > venodilation)
Pc Remember arterioles have more smooth muscle So SNS effects are greater on arterioles than on venules Net effects: SNS P c (vasoconstriction > venoconstriction) SNS P c (vasodilation > venodilation)
Disability Evaluation Under Social Security
 Disability Evaluation Under Social Security Revised Medical Criteria for Evaluating Endocrine Disorders Effective June 7, 2011 Why a Revision? Social Security revisions reflect: SSA s adjudicative experience.
Disability Evaluation Under Social Security Revised Medical Criteria for Evaluating Endocrine Disorders Effective June 7, 2011 Why a Revision? Social Security revisions reflect: SSA s adjudicative experience.
NUTRITION IN LIVER DISEASES
 NUTRITION IN LIVER DISEASES 1. HEPATITIS: Definition: - Viral inflammation of liver cells. Types: a. HAV& HEV, transmitted by fecal-oral route. b. HBV & HCV, transmitted by blood and body fluids. c. HDV
NUTRITION IN LIVER DISEASES 1. HEPATITIS: Definition: - Viral inflammation of liver cells. Types: a. HAV& HEV, transmitted by fecal-oral route. b. HBV & HCV, transmitted by blood and body fluids. c. HDV
FLUID, ELECTROLYTES, ACID-BASE AND SHOCK
 FLUID, ELECTROLYTES, ACID-BASE AND SHOCK Objectives: 1. Discuss the importance of fluids, electrolytes and acid-base elements in ensuring/maintaining proper body function. 2. Describe the movement of fluids,
FLUID, ELECTROLYTES, ACID-BASE AND SHOCK Objectives: 1. Discuss the importance of fluids, electrolytes and acid-base elements in ensuring/maintaining proper body function. 2. Describe the movement of fluids,
Hypocalcaemia. Shaila Sukthankar
 Hypocalcaemia Shaila Sukthankar Ca Daily Requirements Age/ sex Ca (mg) 1-3 350 4-6 450 7-10 550 11-18 M 1000 11-18 F 800 19 + 700 Ca Dietary Sources (NDC) Milk 100 ml =120mg Cheese 15gm = 110mg Yoghurt
Hypocalcaemia Shaila Sukthankar Ca Daily Requirements Age/ sex Ca (mg) 1-3 350 4-6 450 7-10 550 11-18 M 1000 11-18 F 800 19 + 700 Ca Dietary Sources (NDC) Milk 100 ml =120mg Cheese 15gm = 110mg Yoghurt
FLUID & ELECTROLYTE THERAPY Lyon Lee DVM PhD DACVA
 FLUID & ELECTROLYTE THERAPY Lyon Lee DVM PhD DACVA Purposes of fluid administration during the perianesthetic period Replace insensible fluid losses (evaporation, diffusion) during the anesthetic period
FLUID & ELECTROLYTE THERAPY Lyon Lee DVM PhD DACVA Purposes of fluid administration during the perianesthetic period Replace insensible fluid losses (evaporation, diffusion) during the anesthetic period
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
The early symptoms of acute salicylism are the triad of gastrointestinal distress, tinnitus or altered hearing, and hyperventilation.
 POISONING SALICYLATES (ASPIRIN) Management Guidelines Emergency Department Princess Margaret Hospital for Children Perth, Western Australia Last reviewed: January 2007 Page 1 of 5 Dr Gary Geelhoed Dr Frank
POISONING SALICYLATES (ASPIRIN) Management Guidelines Emergency Department Princess Margaret Hospital for Children Perth, Western Australia Last reviewed: January 2007 Page 1 of 5 Dr Gary Geelhoed Dr Frank
American College of Sports Medicine Position Stand: Exercise and Fluid Replacement Summary
 American College of Sports Medicine Position Stand: Exercise and Fluid Replacement Summary American College of Sports Medicine. Position Stand on Exercise and Fluid Replacement. Med. Sci. Sports Exerc.,
American College of Sports Medicine Position Stand: Exercise and Fluid Replacement Summary American College of Sports Medicine. Position Stand on Exercise and Fluid Replacement. Med. Sci. Sports Exerc.,
STAGES OF SHOCK. IRREVERSIBLE SHOCK Heart deteriorates until it can no longer pump and death occurs.
 STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 One Children s Plaza Dayton, OH 45404-1815 www.childrensdayton.org DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended
One Children s Plaza Dayton, OH 45404-1815 www.childrensdayton.org DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended
Nutritional Support of the Burn Patient
 Nutritional Support of the Burn Patient Objectives To understand the principles of normal nutrient utilization and the abnormalities caused by burn injury To be able to assess nutrient needs To be able
Nutritional Support of the Burn Patient Objectives To understand the principles of normal nutrient utilization and the abnormalities caused by burn injury To be able to assess nutrient needs To be able
Advanced Practice Provider Academy
 (+)Corey M. Slovis, MD, FACEP Professor, Emergency Medicine and Medicine; Chairman, Department of Emergency Medicine, Vanderbilt University Medical Center, Nashville, Tennessee; Medical Director, Metro
(+)Corey M. Slovis, MD, FACEP Professor, Emergency Medicine and Medicine; Chairman, Department of Emergency Medicine, Vanderbilt University Medical Center, Nashville, Tennessee; Medical Director, Metro
Absorption of Drugs. Transport of a drug from the GI tract
 Absorption of Drugs Absorption is the transfer of a drug from its site of administration to the bloodstream. The rate and efficiency of absorption depend on the route of administration. For IV delivery,
Absorption of Drugs Absorption is the transfer of a drug from its site of administration to the bloodstream. The rate and efficiency of absorption depend on the route of administration. For IV delivery,
Case Study. Objectives
 Case Study One in a series of case studies developed to stimulate enhancement of problem-solving techniques for physicians and nurses and paramedical personnel when challenged by patients who present with
Case Study One in a series of case studies developed to stimulate enhancement of problem-solving techniques for physicians and nurses and paramedical personnel when challenged by patients who present with
Continuous Renal Replacement Therapy. Jai Radhakrishnan, MD, MS
 Continuous Renal Replacement Therapy Jai Radhakrishnan, MD, MS History of the CRRT program 1988 Open heart program Active transplant program Deep dissatisfaction with peritoneal dialysis in hemodynamically
Continuous Renal Replacement Therapy Jai Radhakrishnan, MD, MS History of the CRRT program 1988 Open heart program Active transplant program Deep dissatisfaction with peritoneal dialysis in hemodynamically
Electrolytes, their physiological action and interaction: A review
 Electrolytes, their physiological action and interaction: A review MATTILOU CATCHPOLE, CRNA, MS Springfield, Illinois Knowledge concerning the physiological action and interaction of electrolytes has greatly
Electrolytes, their physiological action and interaction: A review MATTILOU CATCHPOLE, CRNA, MS Springfield, Illinois Knowledge concerning the physiological action and interaction of electrolytes has greatly
References below to Guyton and Hall, Textbook of Medical Physiology, 9th Edition, 1996 are denoted as G&H.
 Osmolarity References below to Guyton and Hall, Textbook of Medical Physiology, 9th Edition, 1996 are denoted as G&H. The osmolarity of body fluids is an important part of many physiological responses.
Osmolarity References below to Guyton and Hall, Textbook of Medical Physiology, 9th Edition, 1996 are denoted as G&H. The osmolarity of body fluids is an important part of many physiological responses.
Those patients most "at risk" for developing Refeeding Syndrome are: Cats with hepatic lipidosis-the more severe the more "at risk"
 Refeeding Syndrome: When Good Food Goes Bad Atlantic Coast Veterinary Conference 2011 Ann Wortinger, BIS, LVT, VTS (ECC, SAIM) Sanford-Brown College, Dearborn, MI, USA 282320 Introduction A phenomenon
Refeeding Syndrome: When Good Food Goes Bad Atlantic Coast Veterinary Conference 2011 Ann Wortinger, BIS, LVT, VTS (ECC, SAIM) Sanford-Brown College, Dearborn, MI, USA 282320 Introduction A phenomenon
LAB 12 ENDOCRINE II. Due next lab: Lab Exam 3 covers labs 11 and 12, endocrine chart and endocrine case studies (1-4 and 7).
.") 111 LAB 12 ENDOCRINE II Assignments: Quiz : Endocrine Chart pages 112-114 Due next lab: Lab Exam 3 covers labs 11 and 12, endocrine chart and endocrine case studies (1-4 and 7). Objectives: Review the
111 LAB 12 ENDOCRINE II Assignments: Quiz : Endocrine Chart pages 112-114 Due next lab: Lab Exam 3 covers labs 11 and 12, endocrine chart and endocrine case studies (1-4 and 7). Objectives: Review the
ACID-BASE DISORDER. Presenter: NURUL ATIQAH AWANG LAH Preceptor: PN. KHAIRUL BARIAH JOHAN
 ACID-BASE DISORDER Presenter: NURUL ATIQAH AWANG LAH Preceptor: PN. KHAIRUL BARIAH JOHAN OBJECTIVES OF PRESENTATION 1. To refresh knowledge of acid-base disorders 2. To evaluate acid-base disorders using
ACID-BASE DISORDER Presenter: NURUL ATIQAH AWANG LAH Preceptor: PN. KHAIRUL BARIAH JOHAN OBJECTIVES OF PRESENTATION 1. To refresh knowledge of acid-base disorders 2. To evaluate acid-base disorders using
2. Understand the structure of the kidney, and how this structure facilitates its function
 Objectives 1. Understand the roles of the kidney 2. Understand the structure of the kidney, and how this structure facilitates its function 3. Begin to appreciate the inter-dependence of regulatory mechanisms
Objectives 1. Understand the roles of the kidney 2. Understand the structure of the kidney, and how this structure facilitates its function 3. Begin to appreciate the inter-dependence of regulatory mechanisms
Acid/Base Homeostasis (Part 3)
") Acid/Base Homeostasis (Part 3) Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) 27. Effect of Hypoventilation Now let's look at how the
Acid/Base Homeostasis (Part 3) Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) 27. Effect of Hypoventilation Now let's look at how the
Approach to the Patient with Acid-Base Problems. Maintenance of Normal ph. Henderson - Hasselbach Equation. normal ph = 7.40 --> [H + ] = 40 neq / L
![Approach to the Patient with Acid-Base Problems. Maintenance of Normal ph. Henderson - Hasselbach Equation. normal ph = 7.40 --> [H + ] = 40 neq / L](/thumbs/26/8280150.jpg "Approach to the Patient with Acid-Base Problems. Maintenance of Normal ph. Henderson - Hasselbach Equation. normal ph = 7.40 --> [H + ] = 40 neq / L") Approach to the Patient with Acid-Base Problems Maintenance of Normal ph normal ph = 7.40 --> [H + ] = 40 neq / L H 2 O + CO 2 H 2 CO 3 H + + HCO 3 - dietary breakdown of protein (about 80 meq
Approach to the Patient with Acid-Base Problems Maintenance of Normal ph normal ph = 7.40 --> [H + ] = 40 neq / L H 2 O + CO 2 H 2 CO 3 H + + HCO 3 - dietary breakdown of protein (about 80 meq
Diabetic Ketoacidosis
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Diabetic Ketoacidosis Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Diabetic Ketoacidosis Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Arterial Blood Gas Case Questions and Answers
 Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Practical Approach To Patients With Electrolyte Disorders
 Focus on CME at Université de Montréal Practical Approach To Patients With Electrolyte Disorders When dealing with hospitalized patients, electrolyte disorders, such as hypernatremia, hyponatremia, hyperkalemia
Focus on CME at Université de Montréal Practical Approach To Patients With Electrolyte Disorders When dealing with hospitalized patients, electrolyte disorders, such as hypernatremia, hyponatremia, hyperkalemia
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
 ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)
 SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)") Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Magnesium (serum, plasma)
") Magnesium (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Magnesium 1.2 Alternative names None 1.3 NMLC code To follow 1.4 Description of analyte Magnesium is the fourth most abundant
Magnesium (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Magnesium 1.2 Alternative names None 1.3 NMLC code To follow 1.4 Description of analyte Magnesium is the fourth most abundant
FLUID AND BLOOD THERAPY
 FLUID AND BLOOD THERAPY PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain fluid and blood therapy in the interfacility transfer environment
FLUID AND BLOOD THERAPY PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain fluid and blood therapy in the interfacility transfer environment
Albumin (serum, plasma)
") Albumin (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Albumin (plasma or serum) 1.2 Alternative names None (note that albumen is a protein found in avian eggs) 1.3 NLMC code 1.4
Albumin (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Albumin (plasma or serum) 1.2 Alternative names None (note that albumen is a protein found in avian eggs) 1.3 NLMC code 1.4
BLOOD GAS VARIATIONS. Respiratory Values PCO2 35-45 mmhg Normal range. PCO2 ( > 45) ph ( < 7.35) Respiratory Acidosis
 ph ( < 7.35) Respiratory Acidosis") BLOOD GAS VARIATIONS 1 BLOOD ph Normal range 7.35 7.45 Think of 7.40 as your new 0 or neutral If the reading is below 7.4 it is acid. Below 7.35 it is acid out of range or Acidosis If the reading is above
BLOOD GAS VARIATIONS 1 BLOOD ph Normal range 7.35 7.45 Think of 7.40 as your new 0 or neutral If the reading is below 7.4 it is acid. Below 7.35 it is acid out of range or Acidosis If the reading is above
3 Which fluid and why?
 3 Which fluid and why? Key points Blood products, colloids and crystalloids are the three main fluid types used in veterinary practice Blood transfusion requires a suitable donor and checks for compatibility
3 Which fluid and why? Key points Blood products, colloids and crystalloids are the three main fluid types used in veterinary practice Blood transfusion requires a suitable donor and checks for compatibility
LAGUARDIA COMMUNITY COLLEGE CITY UNIVERSITY OF NEW YORK PRACTICAL NURSING PROGRAM. Acute Renal Failure. by Marie Jimenez, SPN
 LAGUARDIA COMMUNITY COLLEGE CITY UNIVERSITY OF NEW YORK PRACTICAL NURSING PROGRAM Acute Renal Failure by Marie Jimenez, SPN SCL 115: Maternity Nursing Fall 2007 Session I Clinical Professor: Prof. Wilkes
LAGUARDIA COMMUNITY COLLEGE CITY UNIVERSITY OF NEW YORK PRACTICAL NURSING PROGRAM Acute Renal Failure by Marie Jimenez, SPN SCL 115: Maternity Nursing Fall 2007 Session I Clinical Professor: Prof. Wilkes
The digestive system eliminated waste from the digestive tract. But we also need a way to eliminate waste from the rest of the body.
 Outline Urinary System Urinary System and Excretion Bio105 Lecture 20 Chapter 16 I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system 1
Outline Urinary System Urinary System and Excretion Bio105 Lecture 20 Chapter 16 I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system 1
GUIDANCE FOR INTRAVENOUS FLUID AND ELECTROLYTE PRESCRIPTION IN ADULTS
 NHS NHS Lothian GUIDANCE FOR INTRAVENOUS FLUID AND ELECTROLYTE PRESCRIPTION IN ADULTS Fluid prescriptions are very important. Prescribing the wrong type or amount of fluid can do serious harm. Assessment
NHS NHS Lothian GUIDANCE FOR INTRAVENOUS FLUID AND ELECTROLYTE PRESCRIPTION IN ADULTS Fluid prescriptions are very important. Prescribing the wrong type or amount of fluid can do serious harm. Assessment
Syndrome of Inappropriate Antidiuretic Hormone and Cerebral Salt Wasting in Critically Ill Patients
 AACN Advanced Critical Care Volume 23, Number 3, pp.233 239 2012, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Syndrome of Inappropriate Antidiuretic Hormone
AACN Advanced Critical Care Volume 23, Number 3, pp.233 239 2012, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Syndrome of Inappropriate Antidiuretic Hormone
ASN Dialysis Advisory Group ASN DIALYSIS CURRICULUM
 ASN Dialysis Advisory Group ASN DIALYSIS CURRICULUM 0 ASN Dialysis Curriculum Dialysis Circuit Review Bessie A. Young, MD, MPH, FACP Associate Professor, University of Washington Director Home Dialysis,
ASN Dialysis Advisory Group ASN DIALYSIS CURRICULUM 0 ASN Dialysis Curriculum Dialysis Circuit Review Bessie A. Young, MD, MPH, FACP Associate Professor, University of Washington Director Home Dialysis,
Chapter 8. Calcium Homeostasis
 Chapter 8 Calcium Homeostasis Introduction Calcium has a number of critical roles in physiology. It is required for muscle contraction, as an enzyme co-factor, and as a second messenger. In order for these
Chapter 8 Calcium Homeostasis Introduction Calcium has a number of critical roles in physiology. It is required for muscle contraction, as an enzyme co-factor, and as a second messenger. In order for these
Phosphate (serum, plasma, urine)
") Phosphate (serum, plasma, urine) 1 Name and description of analyte 1.1 Name of analyte Phosphate 1.2 Alternative names Phosphorus, inorganic phosphorus (Pi), PO 4. 1.3 NMLC number 1.4 Description of analyte
Phosphate (serum, plasma, urine) 1 Name and description of analyte 1.1 Name of analyte Phosphate 1.2 Alternative names Phosphorus, inorganic phosphorus (Pi), PO 4. 1.3 NMLC number 1.4 Description of analyte
Paramedic Program Anatomy and Physiology Study Guide
 Paramedic Program Anatomy and Physiology Study Guide Define the terms anatomy and physiology. List and discuss in order of increasing complexity, the body from the cell to the whole organism. Define the
Paramedic Program Anatomy and Physiology Study Guide Define the terms anatomy and physiology. List and discuss in order of increasing complexity, the body from the cell to the whole organism. Define the
EFFIMET 1000 XR Metformin Hydrochloride extended release tablet
 BRAND NAME: Effimet XR. THERAPEUTIC CATEGORY: Anti-Diabetic PHARMACOLOGIC CLASS: Biguanides EFFIMET 1000 XR Metformin Hydrochloride extended release tablet COMPOSITION AND PRESENTATION Composition Each
BRAND NAME: Effimet XR. THERAPEUTIC CATEGORY: Anti-Diabetic PHARMACOLOGIC CLASS: Biguanides EFFIMET 1000 XR Metformin Hydrochloride extended release tablet COMPOSITION AND PRESENTATION Composition Each
Acquired, Drug-Induced Long QT Syndrome
 Acquired, Drug-Induced Long QT Syndrome A Guide for Patients and Health Care Providers Sudden Arrhythmia Death Syndromes (SADS) Foundation 508 E. South Temple, Suite 202 Salt Lake City, Utah 84102 800-STOP
Acquired, Drug-Induced Long QT Syndrome A Guide for Patients and Health Care Providers Sudden Arrhythmia Death Syndromes (SADS) Foundation 508 E. South Temple, Suite 202 Salt Lake City, Utah 84102 800-STOP
OSMITROL - mannitol injection, solution Baxter Healthcare Corporation
 OSMITROL - mannitol injection, solution Baxter Healthcare Corporation DESCRIPTION OSMITROL Injection (Mannitol Injection, USP) is a sterile, nonpyrogenic solution of Mannitol, USP in a single dose container
OSMITROL - mannitol injection, solution Baxter Healthcare Corporation DESCRIPTION OSMITROL Injection (Mannitol Injection, USP) is a sterile, nonpyrogenic solution of Mannitol, USP in a single dose container
Blood Pressure Regulation
 Blood Pressure Regulation Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) Page 1. Introduction There are two basic mechanisms for regulating
Blood Pressure Regulation Graphics are used with permission of: Pearson Education Inc., publishing as Benjamin Cummings (http://www.aw-bc.com) Page 1. Introduction There are two basic mechanisms for regulating
Fluid and electrolyte management in term and preterm neonates
 Fluid and electrolyte management in term and preterm neonates Rajiv Aggarwal, Ashok Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari
Fluid and electrolyte management in term and preterm neonates Rajiv Aggarwal, Ashok Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari
Acute Pancreatitis. Questionnaire. if yes: amount (cigarettes/day): since when (year): Drug consumption: yes / no if yes: type of drug:. amount:.
: since when (year): Drug consumption: yes / no if yes: type of drug:. amount:.") The physical examination has to be done AT ADMISSION! The blood for laboratory parameters has to be drawn AT ADMISSION! This form has to be filled AT ADMISSION! Questionnaire Country: 1. Patient personal
The physical examination has to be done AT ADMISSION! The blood for laboratory parameters has to be drawn AT ADMISSION! This form has to be filled AT ADMISSION! Questionnaire Country: 1. Patient personal
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2016 2/2017 2/2016 Description of Procedure or Service Vitamin D,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2016 2/2017 2/2016 Description of Procedure or Service Vitamin D,
Emergency Fluid Therapy in Companion Animals
 Emergency Fluid Therapy in Companion Animals Paul Pitney BVSc paul.pitney@tafensw.edu.au The administration of appropriate types and quantities of intravenous fluids is the cornerstone of emergency therapy
Emergency Fluid Therapy in Companion Animals Paul Pitney BVSc paul.pitney@tafensw.edu.au The administration of appropriate types and quantities of intravenous fluids is the cornerstone of emergency therapy
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE
 STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to