Hospital Based Transitions of Care Program. Dr Jeffery Liles, MD FHM. Providence Health Care
|
|
|
- Peregrine Gordon
- 8 years ago
- Views:
Transcription
1 Outcomes and Applications of a Hospital Based Transitions of Care Program. Dr Jeffery Liles, MD FHM Medical Director Care Management Providence Health Care

2 -Importance of D/C planning and transitions of care in current medical environment. -Difference between D/C Planning and Transitions of Care. -Current D/C Planning and Transitions of Care Projects at PSHMC. -Future State of Change.

3 -Changing face of medicine in last 20 years. -Tighter financial margins with focus less on production and more on pay for performance.

4 My role models during medical school.

5 My role models during residency.

6 Earliest medical show I remember ( )

7 Your patients ideal physician. ( )

8 Changing face of medicine nationwide and locally.

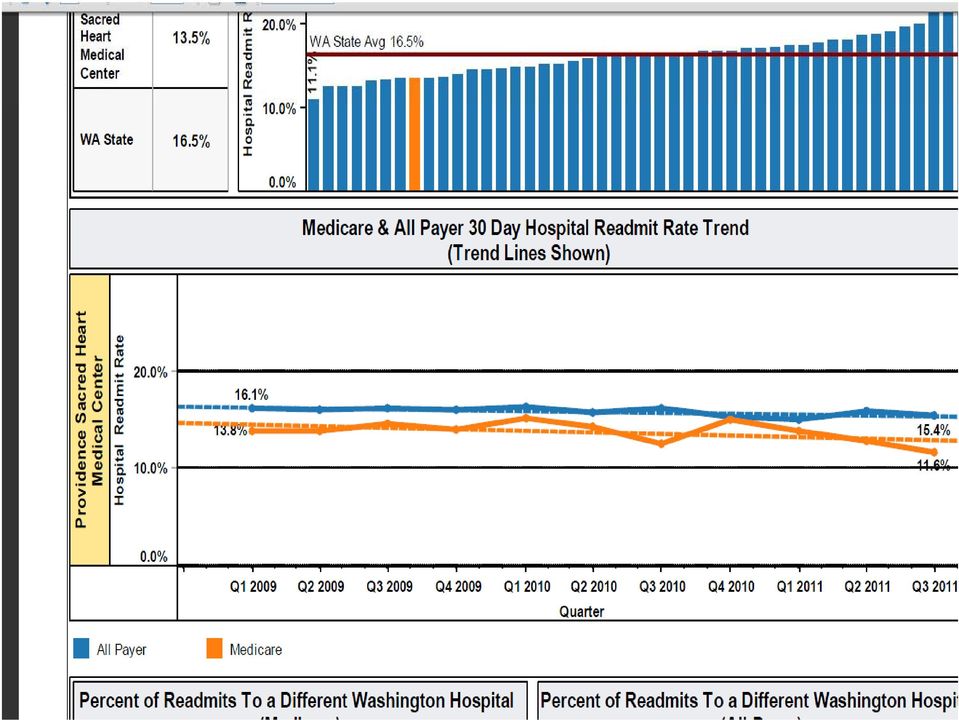
9 D/C Planning at SHMC 2006

10 Changing Payment Systems Penalties for readmission. 300 Million, 2200 hospitals will have money withheld from CMS. 1% % % 2015 Value Based Purchasing. Starts at 1% of DRG payment, up to 2% by 2017.

11 D/C Planning VS Transitions of Care Focus is on efficiently managing the patients stay in the hospital. Proactive process that starts on admission. Helps aligns patients t disposition iti needs with post acute services and providers. Is the set up for a good transition. Hospital focused. Metric Multiple transitions of care Home to hospital Hospital to home Hospital to ECF/Rehab Etc. Focus is to guide the patient through each transition. Patient and Provider focused. Metric LOS Patient Satisfaction Readmission i Rate Patient Satisfaction D/C Planning Transitions of Care

12 Home Homeless Rural Relationship between D/C planning and Transitions of Care. Transfer Center Home no services Home with services Homeless ECF Hospice Emergency Hospital Home Health Facility Hospital Room (D/C Planning) ECF/Rehab Hospice Hospice/ ECF/Rehab Transitions of Care Palliative care GIH Hospice House Home/ECF

13 Providence D/C planning Project Project Vision A Providence owned proactive discharge planning process that considers the comprehensive financial, social, spiritual and medical needs of patients, meeting those needs to provide a seam-less transition through the continuum of care Know Me, Care for Me, Ease my Way

14 Providence D/C planning Project Upon Admission Ease my way Form is filled out by patient/family. Daily D/C meeting between: Charge Nurse Social Worker Case Management Clinical information from provider to one of the above. Outcome of meeting: ADOD Discharge Pathway(Blue, Yellow, Green, Red) Barriers to D/C

15 Patient Name Sticker Here We care about you and your needs. You and your family are part of our health care team and it is important for you to have a say in decisions affecting you. This will help us plan your discharge better. Please read the following, check the boxes that apply to you, and give this to your nurse. Medications Transportation I may need help: Paying for my prescriptions I need somebody to drive me to a pharmacy so I can pick up my prescriptions I would like to use the pharmacy at Sacred Heart /7-6 weekdays/9-5 weekends New prescriptions ready in approximately 2 hours I don t understand how to take my medicine at home I may need information on available resources to help me pay for: My hospital stay My housing, electricity, food My equipment, oxygen, assistance at home Equipment I may need help obtaining: Equipment Walker or cane Wheelchair h Bed Bathroom aids Oxygen or other breathing equipment Safety equipment changing your home to meet your medical needs Imay need help getting: a ride home upon discharge a ride to my doctor appointments a ride to my other medical visits or therapy Financial Home I may need help with: Stairs, location of bed and bathroom access Ability to move around, walk, move from bed to chair, to bathroom Personal help for bathroom, bathing, dressing, personal care Cooking meals Getting groceries Housekeeping Pets Who will help you or provide care at home? Home Health Care Agency: How much help/care can family or friends provide? # of Hours per Day: # of Hours per Week: Know Me, Care for Me, Ease My Way

16 Transitional Care Projects D/C transitional care project. ARNP Hospitalist at SJCC. SLRI Hospitalist Pharmocotherapy Clinic. Homeless Respite. Single Joint Replacement prospective transitions of care. Admit Call Transfer Center. Telemedicine (Tele-Stroke/hospitalist)

17 D/C transitional care project Based on work by Dr Eric Coleman High risk patients were identified on admission and given enhanced services prior to D/C and after D/C. Allowed for submission of 3026 funding from CMS (awaiting outcome) Selected by WSHA for participation in Partnerships for Patients' (PfP) Care Transitions Demonstration Pilot Project
 Care Transitions Demonstration Pilot")
18 Results of D/C Transitional Care Project Growth Charts Data reveals a 30% relative risk reduction in 30 day ED visits and a 9% relative risk reduction in 30 day readmission rates when high risk patients enrolled in the Transitional Care Program are compared to the population of high risk patients % 30 Day Acute Care Use (03/11 06/11) 6.00% 4.00% 3M Patients (n=303) 2.00% 0.00% 30% Relative Risk Reduction ED Visits 9% Relative Risk Reduction Readmission TC Patients (n=272)
 2.00% 0.")
19
20 ARNP Hospitalist at SJCC SJCC 160 bed ECF, 40 beds are for TCU. ARNP on site 5 days a week, with hospitalist back up by phone at nights and on weekends. Priority of duties See acute issues as they arise at ECF. Perform H&P on new patients. Review D/C meds prior to D/C

21 Pharmocotherapy Clinic Pharmacist run clinic specifically for medication reconciliation and medication counseling. Patients can access clinic pre or post discharge. Works with physicians offices to clarify and rectify any discrepancies. Worked as integral part of Transitional Care D/C project.
22 What does the future hold? Dammit Jim I m Doctor, Not a Magician
23 Patient Satisfaction
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
How To Plan For A Hospital Discharge
 Family Caregiver Guide Rehab-to-Home Discharge Guide In Rehab: Planning for Discharge The best time to start planning for discharge is just after your family member is admitted. While it may seem too soon
Family Caregiver Guide Rehab-to-Home Discharge Guide In Rehab: Planning for Discharge The best time to start planning for discharge is just after your family member is admitted. While it may seem too soon
HOSPITAL TO HOME. Plan for a Smooth Transition
 HOSPITAL TO HOME Plan for a Smooth Transition R et urning home from a hospital stay can result in unexpected challenges for many seniors. Finding themselves back at home after a hospital stay, many older
HOSPITAL TO HOME Plan for a Smooth Transition R et urning home from a hospital stay can result in unexpected challenges for many seniors. Finding themselves back at home after a hospital stay, many older
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
EndLink: An Internet-based End of Life Care Education Program www.endlink.rhlurie.northwestern.edu ABOUT HOSPICE CARE
 EndLink: An Internet-based End of Life Care Education Program www.endlink.rhlurie.northwestern.edu ABOUT HOSPICE CARE What is hospice? Hospice care focuses on improving the quality of life for persons
EndLink: An Internet-based End of Life Care Education Program www.endlink.rhlurie.northwestern.edu ABOUT HOSPICE CARE What is hospice? Hospice care focuses on improving the quality of life for persons
Acute Care for Elders (ACE)
") Acute Care for Elders (ACE) Providing Excellence in Care for Older Patients/Families Vancouver General Hospital 899 West 12th Avenue Vancouver BC V5Z 1M9 Tel: 604-875-4111 Our Purpose The Phyllis Howard
Acute Care for Elders (ACE) Providing Excellence in Care for Older Patients/Families Vancouver General Hospital 899 West 12th Avenue Vancouver BC V5Z 1M9 Tel: 604-875-4111 Our Purpose The Phyllis Howard
CAREGIVER GUIDE. A doctor. He or she authorizes (approves) the rehab discharge.
 the rehab discharge.") Guide for Discharge to Home From Inpatient Rehab Who Is on the Discharge Team? Many people help plan a rehab discharge, and they are often referred to as a team. The team members include: A doctor. He
Guide for Discharge to Home From Inpatient Rehab Who Is on the Discharge Team? Many people help plan a rehab discharge, and they are often referred to as a team. The team members include: A doctor. He
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
Hospice and Palliative Care: Help Throughout Life s Journey. John P. Langlois MD CarePartners Hospice and Palliative Care
 Hospice and Palliative Care: Help Throughout Life s Journey John P. Langlois MD CarePartners Hospice and Palliative Care Goals Define Palliative Care and Hospice. Describe and clarify the differences and
Hospice and Palliative Care: Help Throughout Life s Journey John P. Langlois MD CarePartners Hospice and Palliative Care Goals Define Palliative Care and Hospice. Describe and clarify the differences and
ENHANCED TRANSITIONAL CARE MODEL:
 ENHANCED TRANSITIONAL CARE MODEL: A HOSPITAL TO HOME 30 DAY PILOT PROGRAM BROUGHT TO YOU BY INTRODUCTION One in five Medicare recipients discharged from the hospital today is reportedly readmitted within
ENHANCED TRANSITIONAL CARE MODEL: A HOSPITAL TO HOME 30 DAY PILOT PROGRAM BROUGHT TO YOU BY INTRODUCTION One in five Medicare recipients discharged from the hospital today is reportedly readmitted within
How To Help A Nursing Home And Hospital Collaborate
 Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
HealthEast Hospitals Policies Manual Nursing Service Administration Page 1 of 5
 Nursing Service Administration Page 1 of 5 Owners/Group: Care Management Services HealthEast Nurse Practice Committee Policy No. HE Administrative Policy: 100.C-6 HENSA Policy T-7 POLICY TITLE: Discharge/Transfer/Care
Nursing Service Administration Page 1 of 5 Owners/Group: Care Management Services HealthEast Nurse Practice Committee Policy No. HE Administrative Policy: 100.C-6 HENSA Policy T-7 POLICY TITLE: Discharge/Transfer/Care
Hospital-to-Home Discharge Guide
 Family Caregiver Guide Hospital-to-Home Discharge Guide In the Hospital: Planning for Discharge The best time to start planning for discharge is just after your family member is admitted. While it may
Family Caregiver Guide Hospital-to-Home Discharge Guide In the Hospital: Planning for Discharge The best time to start planning for discharge is just after your family member is admitted. While it may
Running head: COMMUNICATION DEFICITS 1. Communication Deficits Among the Bedside Nurse and Palliative Care Team. Linn L. Groom
 Running head: COMMUNICATION DEFICITS 1 Communication Deficits Among the Bedside Nurse and Palliative Care Team Linn L. Groom California State University, Stanislaus COMMUNICATION DEFICITS 2 Communication
Running head: COMMUNICATION DEFICITS 1 Communication Deficits Among the Bedside Nurse and Palliative Care Team Linn L. Groom California State University, Stanislaus COMMUNICATION DEFICITS 2 Communication
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Reconciling the Differences. Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit
 Reconciling the Differences Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit Objectives 1. Review the medication discharge counselling process in the renal dialysis program 2.
Reconciling the Differences Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit Objectives 1. Review the medication discharge counselling process in the renal dialysis program 2.
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Cedars Sinai Medical Center (CSMC) Learning Objectives. Why Medication Reconciliation?
 Learning Objectives. Why Medication Reconciliation?") Management Case Study: Transitions Trifecta Calibrating the Severity of Drug Related Problems, dherence, and Literacy in a High Risk Population Tuesday, December 10, 2013 2:00 p.m. 2:30 p.m. Management
Management Case Study: Transitions Trifecta Calibrating the Severity of Drug Related Problems, dherence, and Literacy in a High Risk Population Tuesday, December 10, 2013 2:00 p.m. 2:30 p.m. Management
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Types of Home Health Care Services You Need
 Types of Home Health Care Services You Need You may receive one type or many depending on your needs. Care may be provided by one source or by several sources. Work with your physician, clinic staff, or
Types of Home Health Care Services You Need You may receive one type or many depending on your needs. Care may be provided by one source or by several sources. Work with your physician, clinic staff, or
Medical Rehabilitation. Rehabilitation Unit
 Medical Rehabilitation Rehabilitation Unit Medical Rehabilitation The purpose of this handout is to give you information about University Hospital s Rehabilitation Unit (2 North or 2N). It will explain:
Medical Rehabilitation Rehabilitation Unit Medical Rehabilitation The purpose of this handout is to give you information about University Hospital s Rehabilitation Unit (2 North or 2N). It will explain:
Going Home after Rehab: A Family Caregiver s Guide
 Family Caregiver Guide Going Home after Rehab: A Family Caregiver s Guide Discharge from a rehabilitation (rehab) facility to home can be hard for all involved. Your family member may still need a lot
Family Caregiver Guide Going Home after Rehab: A Family Caregiver s Guide Discharge from a rehabilitation (rehab) facility to home can be hard for all involved. Your family member may still need a lot
Medication Reconciliation
 Medication Reconciliation Jackie Rice, RN EMR Team Supervisor Frederick Memorial Hospital Frederick, Maryland Scope of the Project Implement an automated medication reconciliation tool Meet the 2006 JCAHO
Medication Reconciliation Jackie Rice, RN EMR Team Supervisor Frederick Memorial Hospital Frederick, Maryland Scope of the Project Implement an automated medication reconciliation tool Meet the 2006 JCAHO
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services. Discharge Planning
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
Be Careful What You Ask For A Predictive Model That Really Works
 Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
How to choose the right health care agency for your loved one
 1 CONSUMER AWARENESS GUIDE How to choose the right health care agency for your loved one HOSPICE (Page 2) HOME HEALTH CARE (Page 9) PERSONAL CARE (Page 12) There are hundreds of home health agencies in
1 CONSUMER AWARENESS GUIDE How to choose the right health care agency for your loved one HOSPICE (Page 2) HOME HEALTH CARE (Page 9) PERSONAL CARE (Page 12) There are hundreds of home health agencies in
Sanford Improvement Making Lean Work in Healthcare
 Sanford Improvement Making Lean Work in Healthcare David Peterson Enterprise Director of Continuous Improvement Outline/Agenda Office of Continuous Improvement Who are we and what do we do? History/Journey
Sanford Improvement Making Lean Work in Healthcare David Peterson Enterprise Director of Continuous Improvement Outline/Agenda Office of Continuous Improvement Who are we and what do we do? History/Journey
Home and Community Care. A Guide to Your Care
 Home and Community Care A Guide to Your Care August 2007 For information on any of these services, contact the home and community care program at the local health authority. For contact information on
Home and Community Care A Guide to Your Care August 2007 For information on any of these services, contact the home and community care program at the local health authority. For contact information on
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Clarification of Patient Discharge Status Codes and Hospital Transfer Policies
 The Acute Inpatient Prospective Payment System Fact Sheet (revised November 2007), which provides general information about the Acute Inpatient Prospective Payment System (IPPS) and how IPPS rates are
The Acute Inpatient Prospective Payment System Fact Sheet (revised November 2007), which provides general information about the Acute Inpatient Prospective Payment System (IPPS) and how IPPS rates are
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15
 Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
A Guide to Patient Services. Cedars-Sinai Health Associates
 A Guide to Patient Services Cedars-Sinai Health Associates Welcome Welcome to Cedars-Sinai Health Associates. We appreciate the trust you have placed in us by joining our dedicated network of independent-practice
A Guide to Patient Services Cedars-Sinai Health Associates Welcome Welcome to Cedars-Sinai Health Associates. We appreciate the trust you have placed in us by joining our dedicated network of independent-practice
Z Take this folder with you to your
 my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Utilizing Pharmacy Technicians for Medication Reconciliation. Kristy Malacos, MS, CPhT Magruder Hospital Port Clinton, OH Pharmacy Systems, Inc.
 Utilizing Pharmacy Technicians for Medication Reconciliation Kristy Malacos, MS, CPhT Magruder Hospital Port Clinton, OH Pharmacy Systems, Inc. Magruder Hospital Located on the shores of Lake Erie in Port
Utilizing Pharmacy Technicians for Medication Reconciliation Kristy Malacos, MS, CPhT Magruder Hospital Port Clinton, OH Pharmacy Systems, Inc. Magruder Hospital Located on the shores of Lake Erie in Port
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
Discharge Planning. Home Care 1. Objectives. Where are they Going?
 Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
RED, BOOST, and You: Improving the Discharge Transition of Care
 RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
my personal joint profile Your own personal profile of how rheumatoid arthritis is affecting your joints.
 my personal joint profile Your own personal profile of how rheumatoid arthritis is affecting your joints. What you and your rheumatologist can learn from your joint profile. It seems like a simple question:
my personal joint profile Your own personal profile of how rheumatoid arthritis is affecting your joints. What you and your rheumatologist can learn from your joint profile. It seems like a simple question:
*Explain strategies that support utilization management in a health care setting.
 Deborah Cutts, Chief Quality Officer 1 Chris Rovinski-Wagner, Coach Captain Discuss utilization management in the context of variation in health care delivery. Explain strategies that support utilization
Deborah Cutts, Chief Quality Officer 1 Chris Rovinski-Wagner, Coach Captain Discuss utilization management in the context of variation in health care delivery. Explain strategies that support utilization
General Practitioner
 Palliative Care/End of Life Related Fees Service Type Fee code When to use General Practitioner Palliative Care Planning 14063 Once a patient living in the community (own or family home or assisted living;
Palliative Care/End of Life Related Fees Service Type Fee code When to use General Practitioner Palliative Care Planning 14063 Once a patient living in the community (own or family home or assisted living;
Rehabilitation Unit 4C
 If you have any questions please do not hesitate to ask any team member for assistance Your Room Phone Number is: Rehabilitation Unit 4C Rehab 4C Trillium - Mississauga 100 Queensway West Mississauga,
If you have any questions please do not hesitate to ask any team member for assistance Your Room Phone Number is: Rehabilitation Unit 4C Rehab 4C Trillium - Mississauga 100 Queensway West Mississauga,
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
A Family Caregiver s Guide to Care Coordination
 Family Caregiver Guide A Family Caregiver s Guide to Care Coordination You have many responsibilities as a family caregiver for someone with a serious chronic illness or disability. You may do personal
Family Caregiver Guide A Family Caregiver s Guide to Care Coordination You have many responsibilities as a family caregiver for someone with a serious chronic illness or disability. You may do personal
Lydia Klinger Director, Ryan White & HIV Clinical Service Programs Virginia Commonwealth University. Mark Loafman MD, MPH
 Lydia Klinger Director, Ryan White & HIV Clinical Service Programs Virginia Commonwealth University Mark Loafman MD, MPH Chair, Family and Community Medicine, Cook County Health and Hospitals System Lead,
Lydia Klinger Director, Ryan White & HIV Clinical Service Programs Virginia Commonwealth University Mark Loafman MD, MPH Chair, Family and Community Medicine, Cook County Health and Hospitals System Lead,
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Inpatient Rehabilitation Patient Handbook
 Inpatient Rehabilitation Patient Handbook Welcome to the Acute Inpatient Rehabilitation Program! The Acute Inpatient Rehabilitation Program welcomes you and your family. We look forward to the opportunity
Inpatient Rehabilitation Patient Handbook Welcome to the Acute Inpatient Rehabilitation Program! The Acute Inpatient Rehabilitation Program welcomes you and your family. We look forward to the opportunity
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
GOING HOME AFTER YOUR TAVR PROCEDURE
 GOING HOME AFTER YOUR TAVR PROCEDURE HENRY FORD HOSPITAL CENTER FOR STRUCTURAL HEART DISEASE GOING HOME After your TAVR procedure, you will need help when you go home. It is hard to predict how much help
GOING HOME AFTER YOUR TAVR PROCEDURE HENRY FORD HOSPITAL CENTER FOR STRUCTURAL HEART DISEASE GOING HOME After your TAVR procedure, you will need help when you go home. It is hard to predict how much help
CCNC Care Management Standardized Plan
 Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
Aging & Disability Resource Centers of Wisconsin Considering a Move? The Cost Calculator Can Help
 Aging & Disability Resource Centers of Wisconsin Considering a Move? The Cost Calculator Can Help Content Introduction... 2 Helpful Services... 3 Long Form... 5 Short Form... 7 My Choice... 9 Next Steps...
Aging & Disability Resource Centers of Wisconsin Considering a Move? The Cost Calculator Can Help Content Introduction... 2 Helpful Services... 3 Long Form... 5 Short Form... 7 My Choice... 9 Next Steps...
Medicare and Home Health Care
 CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare and Home Health Care This is the official U.S. government booklet about Medicare home health care benefits for people with Original Medicare. This booklet
CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare and Home Health Care This is the official U.S. government booklet about Medicare home health care benefits for people with Original Medicare. This booklet
4/26/2013. Premier Health. Premier Health Pharmacy Services. Expanding Role of CPhT in a Five Hospital System. Objective
 Expanding Role of CPhT in a Five Hospital System Nathan Simmons, PharmD, MBA Director of Pharmacy, GSH Pam Fair, CPhT GSH Jessica Brock, CPhT GSH Allyson Ashford, CPhT -UVMC 1 2 Objective All truth passes
Expanding Role of CPhT in a Five Hospital System Nathan Simmons, PharmD, MBA Director of Pharmacy, GSH Pam Fair, CPhT GSH Jessica Brock, CPhT GSH Allyson Ashford, CPhT -UVMC 1 2 Objective All truth passes
Chapter 7: Inpatient & Outpatient Hospital Care
 7 Inpatient & Outpatient Hospital Care ACUTE INPATIENT ADMISSIONS All elective and emergent admissions require prior authorization and/or notification for all Health Choice Generations Members admissions.
7 Inpatient & Outpatient Hospital Care ACUTE INPATIENT ADMISSIONS All elective and emergent admissions require prior authorization and/or notification for all Health Choice Generations Members admissions.
Caregivers Social Workers Nurse Case Managers. Where the Needs of Others Come First! Caring Consistent Dependable 1-800-777-4750
 Caregivers Social Workers Nurse Case Managers Where the Needs of Others Come First! Caring Consistent Dependable 1-800-777-4750 Personal assistance does not limit someone s independence it enhances it!
Caregivers Social Workers Nurse Case Managers Where the Needs of Others Come First! Caring Consistent Dependable 1-800-777-4750 Personal assistance does not limit someone s independence it enhances it!
Care Transitions: Success Stories and Lessons Learned
 Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
HOSPITALIST PROGRAMS: START SMALL & BE CREATIVE
 HOSPITALIST PROGRAMS: START SMALL & BE CREATIVE HOSPITALIST PROGRAMS: START SMALL & BE CREATIVE 1. GROWTH OF HOSPITALIST MEDICINE 2. BIG PICTURE HOSPITAL IMPACT/BENEFIT 3. KEY QUESTIONS 4. STAFFING MODELS
HOSPITALIST PROGRAMS: START SMALL & BE CREATIVE HOSPITALIST PROGRAMS: START SMALL & BE CREATIVE 1. GROWTH OF HOSPITALIST MEDICINE 2. BIG PICTURE HOSPITAL IMPACT/BENEFIT 3. KEY QUESTIONS 4. STAFFING MODELS
Family Caregiver s Guide to Hospice and Palliative Care
 Family Caregiver Guide Family Caregiver s Guide to Hospice and Palliative Care Even though you have been through transitions before, this one may be harder. If you have been a family caregiver for a while,
Family Caregiver Guide Family Caregiver s Guide to Hospice and Palliative Care Even though you have been through transitions before, this one may be harder. If you have been a family caregiver for a while,
The Path to Excellence: How One Facility Received and Maintained a CMS 5 Star Rating
 The Path to Excellence: How One Facility Received and Maintained a CMS 5 Star Rating South Mountain Healthcare and Rehabilitation Center 2385 Springfield Avenue Vauxhall, NJ 07088 Author: Antonio Onday,
The Path to Excellence: How One Facility Received and Maintained a CMS 5 Star Rating South Mountain Healthcare and Rehabilitation Center 2385 Springfield Avenue Vauxhall, NJ 07088 Author: Antonio Onday,
UW MEDICINE PATIENT EDUCATION. Your Care Team. Helpful information
 UW MEDICINE PATIENT EDUCATION Your Care Team Helpful information In this section: You: The Patient Medical Staff Nursing Staff Allied Health Professionals Support Staff Peer Mentors for People with Spinal
UW MEDICINE PATIENT EDUCATION Your Care Team Helpful information In this section: You: The Patient Medical Staff Nursing Staff Allied Health Professionals Support Staff Peer Mentors for People with Spinal
the California Home Care guide How to navigate your home care options to find care for your loved ones Created for our clients by the team at:
 the California Home Care guide How to navigate your home care options to find care for your loved ones Created for our clients by the team at: Orange County Home Care Guide:: How to find care for your
the California Home Care guide How to navigate your home care options to find care for your loved ones Created for our clients by the team at: Orange County Home Care Guide:: How to find care for your
Parkview Health s Population Health Journey
 Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Integration of Home Health, Hospice, and Personal Service Agencies into Indiana s District Preparedness Planning Process
 Integration of Home Health, Hospice, and Personal Service Agencies into Indiana s District Preparedness Planning Process Indiana Association for Home & Hospice Care Emergency Preparedness Information for
Integration of Home Health, Hospice, and Personal Service Agencies into Indiana s District Preparedness Planning Process Indiana Association for Home & Hospice Care Emergency Preparedness Information for
This information is provided by SRC for Medicare Information. (The costs that are used in these examples are from 2006.)
") Medicare Information Source This information is provided by SRC for Medicare Information. (The costs that are used in these examples are from 2006.) The Senior Resource Center for Medicare Information
Medicare Information Source This information is provided by SRC for Medicare Information. (The costs that are used in these examples are from 2006.) The Senior Resource Center for Medicare Information
Implementing an Evidence Based Hospital Discharge Process
 Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Sentara Healthcare EMR: Our Journey. Bert Reese, CIO and Senior Vice President
 Sentara Healthcare EMR: Our Journey Bert Reese, CIO and Senior Vice President Sentara Healthcare 123-year not-for-profit mission 10 hospitals; 2,349 beds; 3,700 physicians on staff 10 long term care/assisted
Sentara Healthcare EMR: Our Journey Bert Reese, CIO and Senior Vice President Sentara Healthcare 123-year not-for-profit mission 10 hospitals; 2,349 beds; 3,700 physicians on staff 10 long term care/assisted
Inpatient Rehabilitation
 Inpatient Rehabilitation Patient Handbook 2601 Electric Avenue, Port Huron, MI 48060 810-985-1500 mymercy.us SJMPH 12-12 300 My Rehabilitation Team Physician Nurse Case Manager Physical Therapist Occupational
Inpatient Rehabilitation Patient Handbook 2601 Electric Avenue, Port Huron, MI 48060 810-985-1500 mymercy.us SJMPH 12-12 300 My Rehabilitation Team Physician Nurse Case Manager Physical Therapist Occupational
Easing the Transition: Moving Your Relative to a Nursing Home
 Easing the Transition: Moving Your Relative to a Nursing Home Alzheimer s Association, New York City Chapter 360 Lexington Avenue, 4th Floor New York, NY 10017 24-hour Helpline 1-800-272-3900 www.alz.org/nyc
Easing the Transition: Moving Your Relative to a Nursing Home Alzheimer s Association, New York City Chapter 360 Lexington Avenue, 4th Floor New York, NY 10017 24-hour Helpline 1-800-272-3900 www.alz.org/nyc
Medicare and Home Health Care
 Medicare and Home Health Care This is the official government booklet that explains... How to find and compare home health agencies. The Medicare home health benefit and who is eligible. What is covered
Medicare and Home Health Care This is the official government booklet that explains... How to find and compare home health agencies. The Medicare home health benefit and who is eligible. What is covered
MEMO. Questions and Answers Related to the New Hospice Conditions of Participation {Effective 12/2/08}
 MEMO Questions and Answers Related to the New Hospice Conditions of Participation {Effective 12/2/08} PATIENT RIGHTS 1) Is there any problem with agencies incorporating their agency grievance procedures
MEMO Questions and Answers Related to the New Hospice Conditions of Participation {Effective 12/2/08} PATIENT RIGHTS 1) Is there any problem with agencies incorporating their agency grievance procedures
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM?
 BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Empowering Case Managers In The Emergency Department A STRATEGIC ROLE BENEFITS PATIENTS, CARE TEAMS, AND PROVIDERS
 Empowering Case Managers In The Emergency Department A STRATEGIC ROLE BENEFITS PATIENTS, CARE TEAMS, AND PROVIDERS Empowering Case Managers In The Emergency Department A STRATEGIC ROLE BENEFITS PATIENTS,
Empowering Case Managers In The Emergency Department A STRATEGIC ROLE BENEFITS PATIENTS, CARE TEAMS, AND PROVIDERS Empowering Case Managers In The Emergency Department A STRATEGIC ROLE BENEFITS PATIENTS,
Let s Keep You Home. Sleep in your own bed. have a nap in your favourite chair. eat at your own table
 Let s Keep You Home Sleep in your own bed have a nap in your favourite chair eat at your own table Fraser Health Home Health knows that home is the best place to be. With a bit of help, even with a chronic
Let s Keep You Home Sleep in your own bed have a nap in your favourite chair eat at your own table Fraser Health Home Health knows that home is the best place to be. With a bit of help, even with a chronic
Jon S. Howell, LNHA President & CEO Georgia Health Care Association November 18, 2013
 Jon S. Howell, LNHA President & CEO Georgia Health Care Association November 18, 2013 GEORGIA HEALTH CARE ASSOCIATION Represents 336 skilled nursing facilities 13 SOURCE agencies 15 assisted living communities
Jon S. Howell, LNHA President & CEO Georgia Health Care Association November 18, 2013 GEORGIA HEALTH CARE ASSOCIATION Represents 336 skilled nursing facilities 13 SOURCE agencies 15 assisted living communities
Enhancing Behavioral Health Crisis Response
 Enhancing Behavioral Health Response July 2010 Michael Flaum, MD ?? Family / Natural Supports Law Enforcement CMHC Emergency Room Center MECCA Psychiatric Hospitalization Homeless Shelter ? Family / Natural
Enhancing Behavioral Health Response July 2010 Michael Flaum, MD ?? Family / Natural Supports Law Enforcement CMHC Emergency Room Center MECCA Psychiatric Hospitalization Homeless Shelter ? Family / Natural
Rhode Island Hospital Inpatient Rehab Unit (IRU)
") Rhode Island Hospital Inpatient Rehab Unit (IRU) We are located on the 7 th floor of the Main Building. The unit phone number is (401) 444-2217 Within this packet, you will find answers to some commonly
Rhode Island Hospital Inpatient Rehab Unit (IRU) We are located on the 7 th floor of the Main Building. The unit phone number is (401) 444-2217 Within this packet, you will find answers to some commonly
ST. LUKE S ACUTE REHABILITATION CENTER PATIENT/FAMILY GUIDELINES
 ST. LUKE S ACUTE REHABILITATION CENTER PATIENT/FAMILY GUIDELINES St. Luke s Hospital Acute Rehabilitation Center considers you the patient, and your family or caregiver to be very important partners of
ST. LUKE S ACUTE REHABILITATION CENTER PATIENT/FAMILY GUIDELINES St. Luke s Hospital Acute Rehabilitation Center considers you the patient, and your family or caregiver to be very important partners of
David Eubanks, RN, MSN Billie Papasifakis, RN-BC, MSN, AACC. Describe model of care most appropriate
 THE BRIDGE PROGRAM David Eubanks, RN, MSN Billie Papasifakis, RN-BC, MSN, AACC Pamela Teenier, RN, MBA, COC-C, C HCS-D HCSD 1 Objectives Describe model of care most appropriate for a Bridge program from
THE BRIDGE PROGRAM David Eubanks, RN, MSN Billie Papasifakis, RN-BC, MSN, AACC Pamela Teenier, RN, MBA, COC-C, C HCS-D HCSD 1 Objectives Describe model of care most appropriate for a Bridge program from
Heart Failure Clinical Pathway
 Patient & Family Guide 2016 Heart Failure Clinical Pathway www.nshealth.ca Heart Failure Clinical Pathway Your hospital stay will follow a written care plan called a Clinical Pathway. The pathway is a
Patient & Family Guide 2016 Heart Failure Clinical Pathway www.nshealth.ca Heart Failure Clinical Pathway Your hospital stay will follow a written care plan called a Clinical Pathway. The pathway is a
Issues in Health Care Delivery
 BOARD of GOVERNORS Health Initiatives Committee Issues in Health Care Delivery Alma B. Littles, M.D. Special Advisor, STEM/Health Initiatives September 17, 2014 www.flbog.edu www.flbog.edu BOARD of GOVERNORS
BOARD of GOVERNORS Health Initiatives Committee Issues in Health Care Delivery Alma B. Littles, M.D. Special Advisor, STEM/Health Initiatives September 17, 2014 www.flbog.edu www.flbog.edu BOARD of GOVERNORS
Medication Error. Medication Errors. Transitions in Care: Optimizing Intern Resources
 Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Inpatient Rehabilitation Guidebook
 Inpatient Rehabilitation Guidebook Welcome to Alta Bates Summit Medical Center s Regional Rehabilitation Program Our experienced and caring team will provide you with outstanding care as you begin your
Inpatient Rehabilitation Guidebook Welcome to Alta Bates Summit Medical Center s Regional Rehabilitation Program Our experienced and caring team will provide you with outstanding care as you begin your
Discharge Information Information for patients This leaflet is intended to help you, your carer, relatives and friends understand and prepare for
 Discharge Information Information for patients This leaflet is intended to help you, your carer, relatives and friends understand and prepare for your discharge or transfer from hospital. Healthcare professionals
Discharge Information Information for patients This leaflet is intended to help you, your carer, relatives and friends understand and prepare for your discharge or transfer from hospital. Healthcare professionals
Choosing a Nursing Home: What to Look For, What to Ask.
 Choosing a Nursing Home: What to Look For, What to Ask. When considering moving Mom into a nursing home, you should determine Mom s specific needs and your specific family situation as well as what aspects
Choosing a Nursing Home: What to Look For, What to Ask. When considering moving Mom into a nursing home, you should determine Mom s specific needs and your specific family situation as well as what aspects
INNOVATION TITLE: HOSPITAL: Innovation Category: select all that apply
 *DO NOT fill out this form in your browser. Save the form to your computer and then open to complete. Emergency Care Innovation of the Year Award Submission Form email completed submission forms to urgentmatters@gwu.edu
*DO NOT fill out this form in your browser. Save the form to your computer and then open to complete. Emergency Care Innovation of the Year Award Submission Form email completed submission forms to urgentmatters@gwu.edu
How To Know If A Patient Is Happy With Palliative Care
 Quality Metrics in Palliative Care R. Sean Morrison, MD Director, National Palliative Care Research Center Director, Hertzberg Palliative Care Institute Hermann Merkin Professor of Palliative Care Professor,
Quality Metrics in Palliative Care R. Sean Morrison, MD Director, National Palliative Care Research Center Director, Hertzberg Palliative Care Institute Hermann Merkin Professor of Palliative Care Professor,
Transforming Patient Flow, Improving Patient Care
 Transforming Patient Flow, Improving Patient Care Transformation by Design (TbyD) Dr. Peter Nord, VP, CMO, Chief of Staff Thelma Horwitz, Director, Quality and Process Improvement Heidi Hunter, Quality
Transforming Patient Flow, Improving Patient Care Transformation by Design (TbyD) Dr. Peter Nord, VP, CMO, Chief of Staff Thelma Horwitz, Director, Quality and Process Improvement Heidi Hunter, Quality
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Patient Flow and Care Transitions Strategy 2013-2018. Updated September 2014
 Patient Flow and Care Transitions Strategy 2013-2018 Updated Introduction Island Health s Patient Flow and Care Transitions 2013-2018 Strategy builds on the existing work within the organization to address
Patient Flow and Care Transitions Strategy 2013-2018 Updated Introduction Island Health s Patient Flow and Care Transitions 2013-2018 Strategy builds on the existing work within the organization to address
David Glendenning Presentation Title
 David Glendenning Presentation Title Education Coordinator Emergency Medical Services New Hanover Regional Medical Center New Hanover Regional Medical Center Emergency Medical Services Our EMS Reality
David Glendenning Presentation Title Education Coordinator Emergency Medical Services New Hanover Regional Medical Center New Hanover Regional Medical Center Emergency Medical Services Our EMS Reality
Equipment and Supplies
 Equipment and Supplies Bridge to Independence: This study was supported by grant R40 MC 08960 from the Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration,
Equipment and Supplies Bridge to Independence: This study was supported by grant R40 MC 08960 from the Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration,