Putting the Puzzle Pieces Together for Effective Care Transitions the people, the metrics, the technology, the processes, and the patients
|
|
|
- Cleopatra Bell
- 8 years ago
- Views:
Transcription
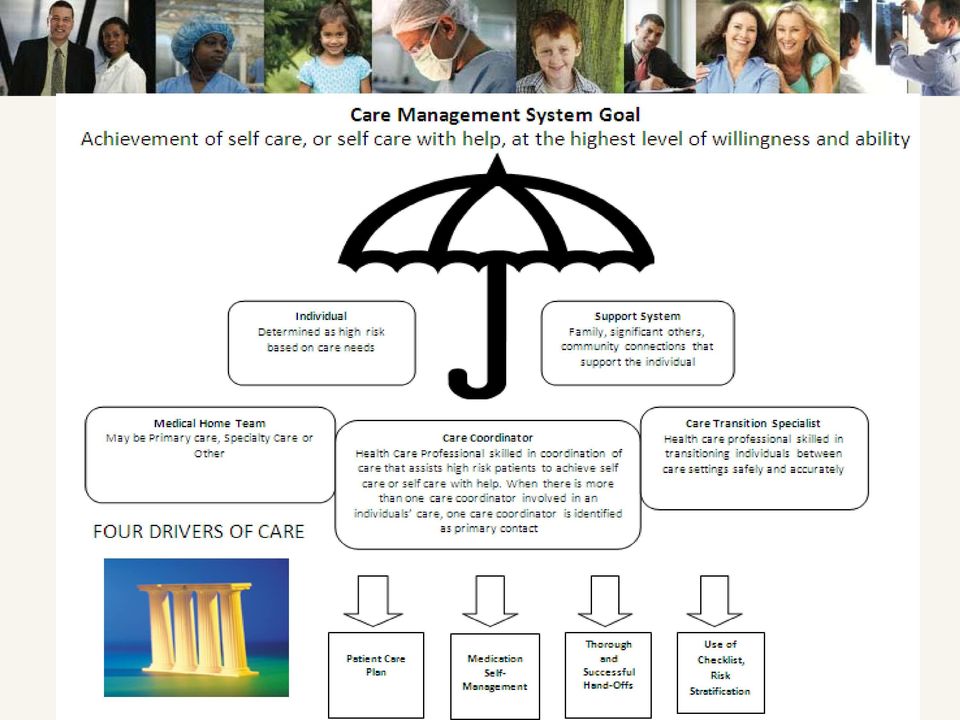
1 Putting the Puzzle Pieces Together for Effective Care Transitions the people, the metrics, the technology, the processes, and the patients April 2012 Vicki Weber & Beverly Christie Fairview Health Services

2 Addressing Three Problems 1. There are inconsistent hand offs between care settings with variation in information. 2. Multiple care coordinators are confusing to the patient and the broader team. 3. Care Transitions is a complicated process with increasing probability of error in some care settings due to volume, patient complexity and number of persons on the care team 1

3 Care Transition Movement of Patient From One Setting to Another Transition Transition Fall at Home Medical Home May be Primary Care or Specialty ED Fractured Hip Uncontrolled CHF Repair Hip Control CHF Hospital Post Acute Rehab TCU FV Acute Rehab TCU FV & Community Self Care with support for CHF Home Transition Transition In the space, or transition, between care environments, there is risk. 2

4 Our Objectives Design an integrated, coordinated, safe, effective care transition process Connect to care coordination models in clinics and in the community Address our core problems (handoffs, complexity, multiple care coordinators) Reduction in preventable events (e.g. admissions, readmissions, ED visits) 3
 Reduction in preventable events (e.g.")
5 Measures of Success Delivering greater value (Triple Aim) for at risk, attributed population Improve Quality: Reduce readmissions Reduce preventable admissions Reduce complications (e.g. medication errors) Improve experience Decrease Total Cost of Care Improved Processes: Completion of the Risk Stratification and Care Transitions Checklists Up to date Health Care Home Patient Care Plan Medication reconciliation at every transition Post-event primary care visit with care coordinator intervention 4

6 The People the development team Representation from vast areas across the organization Hospital Home Care PATIENT Hospice Specialty Care Rehab Services Transitional Care Units Senior Care Primary Care Behavioral Services 5

7 6
8 Care Transitions Specialists RN / SW Newly defined role in hospital settings Position Summary Provides comprehensive care transition management of patients Assesses the patient s needs, evaluates progress, facilitates decisionmaking and collaborates with the health care team during the patient s episode of care. Responsibilities include the identification of resources, facilitation of options for movement along the care continuum, and identification of transition of care needs. The intensity of care transition services is situational and appropriate based on patient need. Accountable for the quality of clinical services delivered by both them and others, and identifies/resolves barriers which may hinder effective patient care. 7

9 Technology Care Transitions Checklist Items on the checklist include: Triggering event (e.g. hospitalization, home care needed) Face to face meeting with patient Complete patient profile Care plan initiated/updated Risk assessment completed/updated Post-event needs identified/initiated (e.g. DME, MTM) Visit summary initiated/completed Handoff initiated/communicated to appropriate person(s) (e.g. PCP, care coordinator) Documentation sent to appropriate person(s) 8

10 At Risk: Definition 9

11 Pilot Implemented April 16 th Early Successes and Learnings Early Successes 1) Identification of high risk and moderate-high risk patients needing intervention 2) Improved communication between all transition points 3) Better understanding of the Patient s Story 4) Improved patient engagement via Health Care Home Patient Care Plan Early Learnings 1) Difficult to understand literacy level of patient and/or caregiver 2) Risk levels can change between transitions 3) Community transitions can be challenging due to lack of care transition support 4) Medication reconciliation needs to occur multiple times 10
 Community transitions can be challenging due to lack of care transition support 4) Medication reconciliation needs to occur")
12 Summary Challenges and Strategies Attention to cultural differences Socializing concepts takes time Competing organizational priorities Communication and transparency is key Stakeholder input/consensus final decision Forming structures/processes with no increased resources Measurement what, who, how, frequency Creating and changing functions can be messy Patience and when needed, executive champion involvement 11

13 12 Questions

Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT
 HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT #607 Friday, October 30, 2015 MARY NEWBERRY, MSN RN, DIRECTOR, HOME BASED & TRANSITIONAL CARE DEBORAH BRADLEY, MSN RN, MANAGER HOME HEALTH CARE BETH
HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT #607 Friday, October 30, 2015 MARY NEWBERRY, MSN RN, DIRECTOR, HOME BASED & TRANSITIONAL CARE DEBORAH BRADLEY, MSN RN, MANAGER HOME HEALTH CARE BETH
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Care Transitions: Success Stories and Lessons Learned
 Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE. Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center
 CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
HealthEast Care Naviga0on Strategy February 17, 2011
 HealthEast Care Naviga0on Strategy February 17, 2011 Rahul Koranne, MD, MBA, FACP Series Objec+ves At the conclusion of this learning activity, participants will be able to: 1. Identify key changes and
HealthEast Care Naviga0on Strategy February 17, 2011 Rahul Koranne, MD, MBA, FACP Series Objec+ves At the conclusion of this learning activity, participants will be able to: 1. Identify key changes and
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents
 Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management 10.0 Care Management
Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management 10.0 Care Management
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Five Myths Surrounding the Business of Population Health Management
 Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Our Patient-Centered Medical Home a Process, not a Click
 Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care
 Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Integrated Comprehensive Care Bundled Care
 Integrated Comprehensive Care Bundled Care Health Council of Canada National Symposium on Integrated Care Oct 10, 2012 C. Gosse, K. Ciavarella St. Joseph s Health System SJHS is one of Canada s largest
Integrated Comprehensive Care Bundled Care Health Council of Canada National Symposium on Integrated Care Oct 10, 2012 C. Gosse, K. Ciavarella St. Joseph s Health System SJHS is one of Canada s largest
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
New Models of Care and Approaches to Payment
 New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
ACO Operational Innovations Featuring the Winners of NAACOS Call for Innovation
 ACO Operational Innovations Featuring the Winners of NAACOS Call for Innovation January 14, 2014 Brian Silverstein, MD Managing Partner HC Wisdom briansilverstein@hcwisdom.com April 24,2014 AGENDA INNOVATION
ACO Operational Innovations Featuring the Winners of NAACOS Call for Innovation January 14, 2014 Brian Silverstein, MD Managing Partner HC Wisdom briansilverstein@hcwisdom.com April 24,2014 AGENDA INNOVATION
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT
 ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
We CAN Keep Our Patients at Home! The Home Health Therapist's Role. Care Transitions and Preventing Rehospitalizations. Objectives 11/5/2013
 We CAN Keep Our Patients at Home! The Home Health Therapist's Role in Care Transitions and Preventing Rehospitalizations Theresa Gates, PT Beyond Home Health Care Services, CEO/Owner Objectives Demonstrate
We CAN Keep Our Patients at Home! The Home Health Therapist's Role in Care Transitions and Preventing Rehospitalizations Theresa Gates, PT Beyond Home Health Care Services, CEO/Owner Objectives Demonstrate
Objectives. Clinical Impact of An Inpatient Diabetes Care Model. Impact of Diabetes on Hospitals. The Nebraska Medical Center Stats 6/5/2014
 Objectives Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE Andjela Drincic, MD 1. Examine the development of the role of the diabetes case manager model in the inpatient setting
Objectives Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE Andjela Drincic, MD 1. Examine the development of the role of the diabetes case manager model in the inpatient setting
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Hand-Off Communications Targeted Solutions Tool (TST ) Implementation Guide for Health Care Organizations
 Implementation Guide for Health Care Organizations") Hand-Off Communications Targeted Solutions Tool (TST ) Implementation Guide for Health Care Organizations Key Features of TST Hand-Off Communications Module Facilitates the examination of the current hand-off
Hand-Off Communications Targeted Solutions Tool (TST ) Implementation Guide for Health Care Organizations Key Features of TST Hand-Off Communications Module Facilitates the examination of the current hand-off
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM?
 BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
Second Forum on Health Care Management & Policy November 28 30, 2012. Discussion Report. Care Management
 Second Forum on Health Care Management & Policy November 28 30, 2012 Discussion Report Care Management Thomas G. Rundall Henry J. Kaiser Emeritus Professor of Organized Health Systems School of Public
Second Forum on Health Care Management & Policy November 28 30, 2012 Discussion Report Care Management Thomas G. Rundall Henry J. Kaiser Emeritus Professor of Organized Health Systems School of Public
Clinical Impact of An Inpatient Diabetes Care Model. Objectives
 Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE June 4, 2014 Objectives 1. Examine the development of the role of the diabetes case manager model in the inpatient setting 2.
Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE June 4, 2014 Objectives 1. Examine the development of the role of the diabetes case manager model in the inpatient setting 2.
How to Prepare for CMS Bundled Payments
 How to Prepare for CMS Bundled Payments Mandatory bundled payments for joint replacement will serve as many hospitals first pilot program for value-based reimbursement in 2016. Combined with the five-star
How to Prepare for CMS Bundled Payments Mandatory bundled payments for joint replacement will serve as many hospitals first pilot program for value-based reimbursement in 2016. Combined with the five-star
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement
 Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement") Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
The Trinity Pioneer Story ACO SETTLERS THE PIONEER JOURNEY TO THE TRIPLE AIM. Sue Thompson Chief Executive Officer
 The Trinity Pioneer Story ACO SETTLERS THE PIONEER JOURNEY TO THE TRIPLE AIM Sue Thompson Chief Executive Officer 2 UnityPoint Health: Organizational Profile 3 4 UnityPoint Health Fort Dodge: Organizational
The Trinity Pioneer Story ACO SETTLERS THE PIONEER JOURNEY TO THE TRIPLE AIM Sue Thompson Chief Executive Officer 2 UnityPoint Health: Organizational Profile 3 4 UnityPoint Health Fort Dodge: Organizational
URAC PATIENT CENTERED HEALTH CARE HOME PROGRAMS
 URAC PATIENT CENTERED HEALTH CARE HOME PROGRAMS Today s Speaker Christine G. Leyden, RN, MSN SVP & GM Client Services, Chief Accreditation Officer 7/27/2011 2011 URAC 2 Learning Objectives for Today s
URAC PATIENT CENTERED HEALTH CARE HOME PROGRAMS Today s Speaker Christine G. Leyden, RN, MSN SVP & GM Client Services, Chief Accreditation Officer 7/27/2011 2011 URAC 2 Learning Objectives for Today s
Melissa Edmister, RN, BSN Clinical Manager Surgical Acute Unit Providence St. Peter Hospital
 Melissa Edmister, RN, BSN Clinical Manager Surgical Acute Unit Providence St. Peter Hospital Why do some organizations do well with safety initiatives while others do poorly or fail? The most important
Melissa Edmister, RN, BSN Clinical Manager Surgical Acute Unit Providence St. Peter Hospital Why do some organizations do well with safety initiatives while others do poorly or fail? The most important
The Evolution of Managed Care as the Foundation for Health Reform ACO s as the Vehicle for Integration and Coordination of Care for All Patients
 The Evolution of Managed Care as the Foundation for Health Reform ACO s as the Vehicle for Integration and Coordination of Care for All Patients Stuart Levine MD MHA Corporate/ Regional Medical Dir., Asst.
The Evolution of Managed Care as the Foundation for Health Reform ACO s as the Vehicle for Integration and Coordination of Care for All Patients Stuart Levine MD MHA Corporate/ Regional Medical Dir., Asst.
Transitional Care Codes New Codes, New Requirements
 Transitional Care Codes New Codes, New Requirements Karen W. Foster, MSA, RN Project Facilitator New Jersey Academy of Family Physicians 2014. NJAFP This presentation and content shared during this session
Transitional Care Codes New Codes, New Requirements Karen W. Foster, MSA, RN Project Facilitator New Jersey Academy of Family Physicians 2014. NJAFP This presentation and content shared during this session
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
Accountable Care Organizations
 Accountable Care Organizations Myth, Reality, Facts Why =System Failure Low Quality - IOM report High Cost Quality Cost disconnect Low Value Problems Disconnect between Quality and Cost Care is fragmented
Accountable Care Organizations Myth, Reality, Facts Why =System Failure Low Quality - IOM report High Cost Quality Cost disconnect Low Value Problems Disconnect between Quality and Cost Care is fragmented
Post-Acute Opportunities in Population Health Management
 Post-Acute Opportunities in Population Health Management Opening Questions Types of facilities Roles Parts of a Pioneer, Medicare Shared Savings Program (MSSP) or Commercial ACO network In a bundled payment
Post-Acute Opportunities in Population Health Management Opening Questions Types of facilities Roles Parts of a Pioneer, Medicare Shared Savings Program (MSSP) or Commercial ACO network In a bundled payment
The Value Quadrant of Healthcare Reform. 2008 Pharos Innovations, LLC. All Rights Reserved.
 The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
Medication Reconciliation
 Medication Reconciliation Jackie Rice, RN EMR Team Supervisor Frederick Memorial Hospital Frederick, Maryland Scope of the Project Implement an automated medication reconciliation tool Meet the 2006 JCAHO
Medication Reconciliation Jackie Rice, RN EMR Team Supervisor Frederick Memorial Hospital Frederick, Maryland Scope of the Project Implement an automated medication reconciliation tool Meet the 2006 JCAHO
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Relative patient benefits of a hospital-pcmh collaboration within an ACO to improve care transitions:
 Relative patient benefits of a hospital-pcmh collaboration within an ACO to improve care transitions: Lessons learned from the PCORI grant application experience Jeffrey L. Schnipper, MD, MPH, FHM Director
Relative patient benefits of a hospital-pcmh collaboration within an ACO to improve care transitions: Lessons learned from the PCORI grant application experience Jeffrey L. Schnipper, MD, MPH, FHM Director
An Accountable Care Organization Pilot: Lessons Learned
 An Accountable Care Organization Pilot: Lessons Learned blueshieldca.com Overview In 2008, an IPA (Hill Physicians Medical Group), a hospital system (Catholic Healthcare West, now Dignity Health) and a
An Accountable Care Organization Pilot: Lessons Learned blueshieldca.com Overview In 2008, an IPA (Hill Physicians Medical Group), a hospital system (Catholic Healthcare West, now Dignity Health) and a
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Crucial Complications: Preventing Harm and Promoting Health
 Crucial Complications: Preventing Harm and Promoting Health MARCI RUEDIGER, PT, MS Agenda What puts patients at risk after acute care? How are these risks managed in rehab? How has the ACA changed the
Crucial Complications: Preventing Harm and Promoting Health MARCI RUEDIGER, PT, MS Agenda What puts patients at risk after acute care? How are these risks managed in rehab? How has the ACA changed the
Qualis Health Alaska Medicaid Case Management Overview
 Qualis Health Alaska Medicaid Case Management Overview Deon Westmorland, RN, BSN, CCM Director, Alaska and Idaho Medicaid & Private Services Advancing Healthcare Improving Health One of the nation s leading
Qualis Health Alaska Medicaid Case Management Overview Deon Westmorland, RN, BSN, CCM Director, Alaska and Idaho Medicaid & Private Services Advancing Healthcare Improving Health One of the nation s leading
AGS REHABILITATION/ POST-HOSPITAL CARE OF THE GERIATRIC FRACTURE PATIENT. Egan Allen, MD University of Rochester
 AGS REHABILITATION/ POST-HOSPITAL CARE OF THE GERIATRIC FRACTURE PATIENT Egan Allen, MD University of Rochester THE AMERICAN GERIATRICS SOCIETY Geriatrics Health Professionals. Leading change. Improving
AGS REHABILITATION/ POST-HOSPITAL CARE OF THE GERIATRIC FRACTURE PATIENT Egan Allen, MD University of Rochester THE AMERICAN GERIATRICS SOCIETY Geriatrics Health Professionals. Leading change. Improving
Southern California Patient Safety Collaborative
 Southern California Patient Safety Collaborative Track II: Care Transitions March 6 th, 2012 Markus Mettler, NHA, PT : REDUCING SNF TO ACUTE RE-HOSPITALIZATIONS Markus Mettler, NHA, PT 20 years in Healthcare
Southern California Patient Safety Collaborative Track II: Care Transitions March 6 th, 2012 Markus Mettler, NHA, PT : REDUCING SNF TO ACUTE RE-HOSPITALIZATIONS Markus Mettler, NHA, PT 20 years in Healthcare
IssueBrief. Case managers strengthen health care s weakest link: Improving care transitions
 IssueBrief VOLUME 4, ISSUE 3 Case managers strengthen health care s weakest link: Improving care transitions Don t dare call them handoffs. Guiding patients to the care they need, when they need it, lies
IssueBrief VOLUME 4, ISSUE 3 Case managers strengthen health care s weakest link: Improving care transitions Don t dare call them handoffs. Guiding patients to the care they need, when they need it, lies
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care
 NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Care Transition Bundle Seven Essential Intervention Categories
 Seven 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family
Seven 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
Care Transition Bundle Seven Essential Intervention Categories. Examples of Transition of Care Interventions
 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family education
1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family education
Premier ACO Collaboratives Driving to a Patient-Centered Health System
 Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Technology and Analytics Roadmap Positioning for the Future
 Technology and Analytics Roadmap Positioning for the Future ASU Summer Institute July 15, 2015 Suzanne Rabideau, Rabideau Consulting Brian Jung, MSS Technologies www.msstech.com Introductions Background
Technology and Analytics Roadmap Positioning for the Future ASU Summer Institute July 15, 2015 Suzanne Rabideau, Rabideau Consulting Brian Jung, MSS Technologies www.msstech.com Introductions Background
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
Note: This is an authorized excerpt from 57 Population Health Management Metrics. To download the entire report, go to
 Note: This is an authorized excerpt from 57 Population Health Management Metrics. To download the entire report, go to http://store.hin.com/product.asp?itemid=4817 or call 888-446-3530. 57 Population Health
Note: This is an authorized excerpt from 57 Population Health Management Metrics. To download the entire report, go to http://store.hin.com/product.asp?itemid=4817 or call 888-446-3530. 57 Population Health
DATA DRIVEN HEALTH CARE TRANSFORMATION
 DATA DRIVEN HEALTH CARE TRANSFORMATION Population Health Analytics as the Foundation for Primary Care Redesign Sylvia Meltzer, MD, LSSGBC Laura Spurr, MPS, PMP Learning Objectives Organization description
DATA DRIVEN HEALTH CARE TRANSFORMATION Population Health Analytics as the Foundation for Primary Care Redesign Sylvia Meltzer, MD, LSSGBC Laura Spurr, MPS, PMP Learning Objectives Organization description
Integrated Community Assessment and Referral Team (ICART) A proactive approach to communitybased services for high-risk seniors
 A proactive approach to communitybased services for high-risk seniors") June 2014, OACCAC Annual Conference Integrated Community Assessment and Referral Team (ICART) A proactive approach to communitybased services for high-risk seniors Joanne Billing, South East CCAC Benedict
June 2014, OACCAC Annual Conference Integrated Community Assessment and Referral Team (ICART) A proactive approach to communitybased services for high-risk seniors Joanne Billing, South East CCAC Benedict
Accountable Care Organizations Understanding What They Are and How to Structure Them
 Accountable Care Organizations Understanding What They Are and How to Structure Them Maria T. Currier HOLLAND & KNIGHT LLP Miami Chamber of Commerce Healthcare Subcommittee December 7, 2010 Copyright 2010
Accountable Care Organizations Understanding What They Are and How to Structure Them Maria T. Currier HOLLAND & KNIGHT LLP Miami Chamber of Commerce Healthcare Subcommittee December 7, 2010 Copyright 2010
STAAR Issue Brief: Reducing Barriers to Care Across the Continuum - Engaging Physicians
 STAAR Issue Brief: Reducing Barriers to Care Across the Continuum - Engaging Physicians Amy Boutwell, MD, MPP, Vanessa Calderon, MD, MPP, and Ali Khan, MD, MPP Overview: Reducing Avoidable Rehospitalizations
STAAR Issue Brief: Reducing Barriers to Care Across the Continuum - Engaging Physicians Amy Boutwell, MD, MPP, Vanessa Calderon, MD, MPP, and Ali Khan, MD, MPP Overview: Reducing Avoidable Rehospitalizations
Readmission Webinar: Palliative Care. April 2, 2013 12:00 to 1:00 pm CST
 Readmission Webinar: Palliative Care April 2, 2013 12:00 to 1:00 pm CST Welcome and Overview Welcome, thank you for joining us today! Housekeeping This webinar is being recorded and will be archived. You
Readmission Webinar: Palliative Care April 2, 2013 12:00 to 1:00 pm CST Welcome and Overview Welcome, thank you for joining us today! Housekeeping This webinar is being recorded and will be archived. You
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Analytic-Driven Quality Keys Success in Risk-Based Contracts. Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst
 Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Stacy McLaughlin, RN, MSN. Director of Quality & Performance Improvement
 Stacy McLaughlin, RN, MSN Director of Quality & Performance Improvement 25-bed CAH 21 beds: acute / observation / swingbed 4 bed ICU ED volumes: 14,400 encounters/year 5 Clinics: Rural Health / Primary
Stacy McLaughlin, RN, MSN Director of Quality & Performance Improvement 25-bed CAH 21 beds: acute / observation / swingbed 4 bed ICU ED volumes: 14,400 encounters/year 5 Clinics: Rural Health / Primary
Emerging g Trends in Home Care
 Emerging g Trends in Home Care Dana Sheer, ACNP, MSN Susan Beausoliel, BSN, MS, DNP 1 The Triple Aim Goals Quality Improve Patient Outcomes Goal Readmissions Cost Reduce costs/penalties associated w/ readmissions
Emerging g Trends in Home Care Dana Sheer, ACNP, MSN Susan Beausoliel, BSN, MS, DNP 1 The Triple Aim Goals Quality Improve Patient Outcomes Goal Readmissions Cost Reduce costs/penalties associated w/ readmissions
UCare provides case management for all UCare members not affiliated with one of the above listed care systems. 2011 UCare for Seniors
 Case Requirements Updated 3/16/2011 According to the Case Society of America (CMSA), Case Model Act of 2009, Case management is a collaborative process of assessment, planning, facilitation, care coordination,
Case Requirements Updated 3/16/2011 According to the Case Society of America (CMSA), Case Model Act of 2009, Case management is a collaborative process of assessment, planning, facilitation, care coordination,
Realizing ACO Success with ICW Solutions
 Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
Financial and Population Analytics for Accountable Care Organizations SEPTEMBER 20, 2012
 Financial and Population Analytics for Accountable Care Organizations Valence Biographies Lori Fox Ward is Senior Vice President of Clinical Integration for Valence Health where her primary role involves
Financial and Population Analytics for Accountable Care Organizations Valence Biographies Lori Fox Ward is Senior Vice President of Clinical Integration for Valence Health where her primary role involves
E. Christopher Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences
 Accountable Care Organizations and You E. Christopher Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State University
Accountable Care Organizations and You E. Christopher Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State University
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
Building a Post Acute Network: Care Management and ACOs
 Building a Post Acute Network: Care Management and ACOs A high level summary of proposed rules for ACOs and the shared savings program most relevant to post acute providers. Prepared By: Kathleen M. Griffin,
Building a Post Acute Network: Care Management and ACOs A high level summary of proposed rules for ACOs and the shared savings program most relevant to post acute providers. Prepared By: Kathleen M. Griffin,
The Transformational Role of Case Management in Community Health Care. Caroline Brereton, RN, MBA Chief Executive Officer Mississauga Halton CCAC
 The Transformational Role of Case Management in Community Health Care Caroline Brereton, RN, MBA Chief Executive Officer Mississauga Halton CCAC September 26-27, 2013 Agenda During this session we will:
The Transformational Role of Case Management in Community Health Care Caroline Brereton, RN, MBA Chief Executive Officer Mississauga Halton CCAC September 26-27, 2013 Agenda During this session we will:
NetworkCares (PPO SNP) 2016 Model of Care Training. H5215_360r1_092714 NHIC 12/2015 m-cnm-ncprovpres-1215
 2016 Model of Care Training. H5215_360r1_092714 NHIC 12/2015 m-cnm-ncprovpres-1215") NetworkCares (PPO SNP) 2016 Model of Care Training H5215_360r1_092714 NHIC 12/2015 m-cnm-ncprovpres-1215 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training
NetworkCares (PPO SNP) 2016 Model of Care Training H5215_360r1_092714 NHIC 12/2015 m-cnm-ncprovpres-1215 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training
Proven Population Health Management. Faster.
 Proven Population Health Management. Faster. At Medecision, our quest to liberate healthcare means tackling the big obstacles by connecting more data from more care teams than other population health management
Proven Population Health Management. Faster. At Medecision, our quest to liberate healthcare means tackling the big obstacles by connecting more data from more care teams than other population health management
Procedure and Transportation Codes Billing Limitations
 Procedure and Billing Limitations Treatment Services That Can Not be Billed on Same Day Procedure 90832 Psychotherapy, 30 minutes with patient and/or family member 90833 Psychotherapy, 30 minutes with
Procedure and Billing Limitations Treatment Services That Can Not be Billed on Same Day Procedure 90832 Psychotherapy, 30 minutes with patient and/or family member 90833 Psychotherapy, 30 minutes with
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed?
 Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Signature Leadership Series. Metrics for the Second Curve of Health Care
 Signature Leadership Series Metrics for the Second Curve of Health Care April 2013 Metrics for the Second Curve of Health Care Resources: For information related to health care delivery transformation,
Signature Leadership Series Metrics for the Second Curve of Health Care April 2013 Metrics for the Second Curve of Health Care Resources: For information related to health care delivery transformation,
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
APPENDIX I. Best Practices: Ten design Principles for Performance Management 1 1) Reflect your company's performance values.
 Reflect your company's performance values.") APPENDIX I Best Practices: Ten design Principles for Performance Management 1 1) Reflect your company's performance values. Identify the underlying priorities that should guide decisions about performance.
APPENDIX I Best Practices: Ten design Principles for Performance Management 1 1) Reflect your company's performance values. Identify the underlying priorities that should guide decisions about performance.
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I
 DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
Delivery System Innovation
 Healthcare Transformation Concepts and Definitions Our healthcare transformation process is invigorated by many stakeholders with differing backgrounds. To help them with new terms and all of us to use
Healthcare Transformation Concepts and Definitions Our healthcare transformation process is invigorated by many stakeholders with differing backgrounds. To help them with new terms and all of us to use
Testimony of Amy Whitcomb Slemmer, Esq. Executive Director Health Care For All
 Testimony of Amy Whitcomb Slemmer, Esq. Executive Director Health Care For All Health Care Cost Trends Hearing Massachusetts Health Policy Commission October 7, 2014 Chairman Altman, Secretaries Shor and
Testimony of Amy Whitcomb Slemmer, Esq. Executive Director Health Care For All Health Care Cost Trends Hearing Massachusetts Health Policy Commission October 7, 2014 Chairman Altman, Secretaries Shor and
Kaiser Permanente: Transition Care Performance and Strategies
 Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS carbarne@gmail.com April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS carbarne@gmail.com April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda