Advances in Pediatric Asthma
|
|
|
- Caitlin Gaines
- 7 years ago
- Views:
Transcription
1 Advances in Pediatric Asthma Stacy L Bichl APN, CPNP, AE-C Advocate Children s Outpatient Pediatrics Kim Watts, MD, MS Advocate Children s Pediatric Pulmonology
2 Objectives Describe the basic pathophysiology of asthma and diagnostic considerations when evaluating a child for asthma Restate the utility of the four components of asthma management as delineated in the NHLBI National Asthma Education and Prevention Program Explain the different purposes of rescue and controller asthma medications, their correct administration. Identify barriers to asthma control Describe health outcome disparities in children with asthma
3 The Burden of Pediatric Asthma
4 The Scope of Asthma Most common chronic disease of childhood Affects more than 7 million children in the United States Approximately 9% of all US children have asthma This rate has increased more than 160% in children under 5 in the last 20 years The annual economic cost of asthma is $19.7 billion Direct costs such as medications and indirect costs such as loss of productivity 13 million school days are missed each year
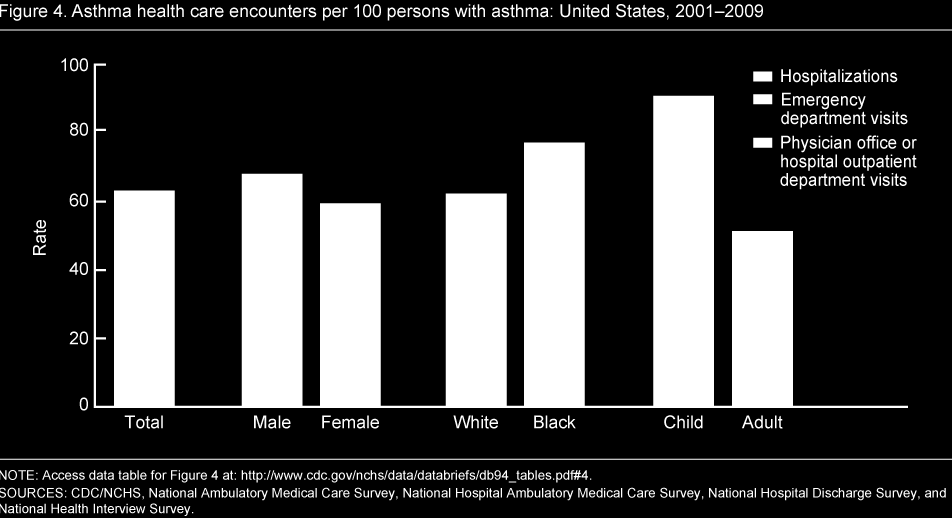
5 Healthcare Utilization
6 Rising Prevalence of Asthma Increase in asthma prevalence from 1980 to 1996 is greater than 50 % Estimated current asthma prevalence in general increased between Largest increase in patients younger than 18 years old
7 Why the increasing numbers? Improved hygiene Less exposure to pathogens disrupting innate immunity Increased indoor air pollution Caused by increase in energy efficient building Increased incidence of early onset viral infections Increase in host susceptibility Small lungs due to prematurity or maternal smoking Increased recognition and awareness
8 Pathophysiology
9 Pathophysiology of Asthma in a nutshell Asthma is a complex, chronic disorder with three main components. Bronchoconstriction bronchial smooth muscle contraction that quickly narrows the airways in response to exposure to a variety of stimuli, including allergens or irritants. Airway hyper-responsiveness an exaggerated bronchoconstrictor response to stimuli. (allergens, pollutants, histamine, viruses, cold air) Airway edema persistent airway inflammation which left untreated becomes progressive with airway edema, mucus hypersecretion and mucous plugs that create additional obstruction. 9
10 Asthma Pathophysiology Overview
11 Diagnosis
12 The diagnosis of asthma is a clinical diagnosis: Classic symptoms Recurrent wheezing not always presenting symptom. Cough Chest tightness Dyspnea Exacerbating factors Cough or wheezing more prominent with exercise Viral infections Inhaled allergens (pollen, dust, mold) Irritants (tobacco smoke exposure, perfumes) Stress, emotion (crying, laughing) Symptoms worsen at night/towards early morning Response to therapy Improves with asthma therapy. 12
13 Cough Most common cause of cough in children over 3 years Persistent in nature-lasting more than 3 weeks at a time Night time to early morning cough Cough to specific exposures, more prominent with activity The Wet-dry asthma cough Can be dry and hacking- reflective of airway edema Can be productive with clear to white sputum- from cellular infiltration, (with eosinophils, neutrophil and increased airway secretions Wheeze Polyphonic, musical, squeaky Generally expiratory but sometimes inspiratory
14 Symptom Patterns Intermittent exacerbations but asymptomatic when well. Or chronic symptoms that worsen with exacerbations Morning dipping Worsening of symptoms in the early morning corresponding to the physiologic dip in pulmonary function September epidemics Viral infections, mycoplasma pneumoniae or Chlamydia pneumoniae infection
15 Diagnostic tools - Spirometry Even children with moderate asthma can have normal spirometry! NAEPP recommends spirometry to be performed in patients older than 5 years: FEV 1 < 80% predicted is abnormal Reversibility (improvement in airflow of 12%) after albuterol is abnormal. However, even in children with normal FEV 1, more subtle changes in the small airways (FEF ) correlate with reversible airflow obstruction.
16 Spirometry loops
17 Diagnosis Peak Flow More variable and effort dependent Wide variability in published predicted peak expiratory flow reference values Can alter brand to brand Predicted target changes quickly with linear growth Peak flows should not be used to diagnose asthma Limited usefulness in monitoring acute changes in those with known diagnosis.
18 Other Diagnostic Modalities Impulse Oscillometry Passive cooperation Evaluates resistance pre and post bronchodilator Bronchoprovocation Testing Methylcholine, histamine, cold air, exercise If patient fails empiric trial of asthma medsications Chest x-ray Hyperinflation, increased perihilar markings, nonspecific signs of asthma
19 Risk Factors: The Asthma Predictive Index Risk factors in children <3 years that predict asthma symptoms at school age. The predictive index is positive when there is episodic wheezing during the preceding year AND One of 3 major criteria: Physician diagnosed atopic dermatitis Physician diagnosed parental asthma Evidence of sensitization to aeroallergens OR 2 of the following minor criteria: Peripheral blood eosinophilia 4% Wheezing apart from colds Evidence of sensitization to food allergens More than 75% of children with a positive index had symptoms of asthma between 6 and 13 years of age. 19
20 Other risk factors? Parental History: Odds of a child with asthma 25-30% greater with one asthmatic parent About 50% greater with two asthmatic parents Obesity ( as measured by BMI, higher fasting triglyceride levels, rate of acanthosis nigricans) Other Atopy the allergic triad Asthma Atopic Dermatitis Allergic Rhinitis Food Allergies (also a risk factor for intubation with exposure) Low fetal growth Recent/early Acetaminophen exposure 20
21 Other diagnostic considerations in infants Infection (post viral inflammation) Dysphagia with Aspiration GERD Sequelae of BPD Laryngotracheomalacia Interstitial Lung Disease Primary Ciliary Dyskinesia Cystic Fibrosis Congenital Heart Disease with L -> R shunt Immune Deficiency Vascular malformations/rings/slings Cystic Pulmonary Lesions (Congenital Lobar emphysema, CCAM) Tracheo-esophageal fistula 21
22 Other diagnostic considerations in children Allergic Rhinitis Chronic/acute sinusitis Foreign Body Aspiration Cystic Fibrosis Habit cough Vocal Cord Dysfunction Deconditioning +/- obesity Anemia GERD 22
23 Making a Diagnosis: Key Points Normal PFTs do not exclude a diagnosis of asthma The presence of wheezing is not a sure diagnostic sign nor does the absence of wheezing preclude a diagnosis of asthma. Reactive airways is a symptom, not a diagnosis and is given the same ICD-9 code as asthma. There are identifiable risk factors that should raise suspicion for a diagnosis of asthma Transient intermittent wheezing should be treated as asthma unless another underlying cause is identified. Take a step outside the asthma box- consider the age appropriate differential list. 23
24 Components of asthma management NAEPP 2007 GUIDELINES 1. Assessment Initially = severity Ongoing = control 2. Treatment (medication) Initiate treatment based on severity Adjust treatment based on control 3. Education 4. Reduction of environmental and co-morbid influences
25 Assessment:
26 Assessment: Dual domains to consider Impairment = impact on functioning: Daily symptoms Exercise intolerance Poor sleep quality Missed school/work Rescue medication use Risk= likelihood of the following: asthma exacerbation loss of lung function Impaired lung growth Impairment today Risk for adverse medication effects Risk tomorrow


27
28 Assessment: Who should get controller therapy? 0 to 4 years old Greater than 4 episodes of wheezing Parental history of asthma Patient with atopic dermatitis or allergies Food allergies with eosinophilia or wheezing without colds Require albuterol more than two days per week Experiences severe illness < 6 weeks apart 2 rounds of steroids in 6 months Intermittent disease with severe exacerbation
29 Assessment: Who should get controller therapy? 5 Years and older: For any persistent asthma Any symptoms > 2 days a week Night time symptoms greater than 2 times a month Albuterol more than 2 days a week Any interference with normal activity Requires oral steroids more than once a year Severity and interval of exacerbations
30 Treatment: Maintenance Therapy

31 Choosing controller therapy? Intermittent - - > Step 1 Mild - - -> Step 2 Moderate - - -> Step 3 Severe - - -> Step 3 or 4
32 Inhaled Corticosteroids Inhibiting steps in the inflammatory cascade Associated with reduction in Symptoms Irreversible decline in lung function Asthma exacerbations Functional limitations Side effects from other medications Reduction in parameters better than with leukotriene antagonist First line control therapy for persistent asthma
33 Key points in the inhaled steroid debate New literature in adults suggest possibility of ICS use episodically with symptoms for mild persistent asthma or titrated low dose ICS during time of symptoms in mild- moderate asthma these recommendations remain outside the NHLBI guidelines for children. Research showed initial slowing in height velocity in prepubertal children using ICS for > 2 years persisted as a reduction in adult height, although the average decrease was 1.2 cm and neither progressive or cumulative. One oral steroid BURST for a single asthma exacerbation The usual dose of an oral steroid burst is 40mg for 5 days =200mg or 200,000ug almost all of which is bioavailable. This is equal to: 400 days of Pulmicort 0.25 mg BID 625 days of QVAR 160ug BID 1,136 days of Flovent 88ug BID of which only 1-6% is bioavailable. Contemporary Pediatrics Contemporary Pediatrics
34 Leukotriene Receptor Agonists Cysteinyl leukotrienes found in BAL in asthmatic patients Inhibit production at various points in the cascade Adjuvant therapy to ICS in patients > 1 year old No evidence to support use as first line controller agent or as intermittent therapy Can be used to step down therapy from ICS or in mild patient who cannot tolerate ICS
35 Montelukast VS. Placebo 2-5 years olds Intermittent asthma associated with viral symptoms Better than placebo with a reduced rate of exacerbations and decreased use of ICS Vs. ICS Meta-analysis in mild to moderate persistent asthma children ICS had better pulmonary function and better asthma control ICS more cost effective
36 Long Acting Beta Agonists Used as an adjuvant to ICS Should not be used for acute exacerbations Once control is obtained, effort should be made to go to a single agent ICS Reserved for patients who fail medium dose ICS Black box warning May increase the chance of severe asthma episodes and asthma related deaths
37 Chronic Oral Steroids Severe persistent asthma Long term effects Adrenal suppression Weight gain Diabetes Hypertension Cataracts Delayed growth Immune suppression Osteoporosis Behavioral effects Lowest possible dose, every other day administration, trying all other modalities is preferable
38 Anti IgE ( Omalizumab) Monoclonal anti IgE Moderate to severe asthma Not controlled on ICS Elevated IgE levels Approved if > 12 year old in US IgE levels Positive allergy testing
39 Other Therapies Cromolyn Systemic review found no clear therapeutic effect vs. placebo No evidence to sport the concurrent use of cromolyn with ICS Theophylline Use limited secondary to potentially serious short term side effects ( arrhythmia, seizures and death) Needs frequent serum monitoring as well as monitoring with drug interactions
40 Treatment: Exacerbation Management
41 Asthma Exacerbations: Who is the child at risk for death? Previous severe exacerbations (intubation, ICU admit) > 2 hospitalizations or > 3 ED visits in the last year Use of > 2 canisters of rescue meds per month Dysfunctional family units, low SES, inner city residence Poor perception of airway obstruction Concurrent food allergies Illicit drug use Co-morbidities- GERD, OSA, sinusitis, chronic rhinitis, obesity, ABPA, Stress/anxiety/Depression Always respect a child s complaint of breathing difficulty Even a child with mild asthma can have a fatal exacerbation
42 Short Acting Beta Agonists Act to relax smooth muscles around the airways Overuse or regular use is associated with poor control Theoretical concern regarding down regulation of beta receptors with chronic use Can impact medication needed for urgent care
43 Short acting medications Albuterol MDI with spacer or nebulizer No role for oral albuterol given side effects Levalbuterol R- enantiomer active isomer only Approved MDI > 4 years old and neb > 6years old Comparable, no evidence for superiority
44 Ipratropium Bromide Anti-cholinergic Bronchodilator through smooth muscle relaxation Adjuvant for albuterol in emergency settings Reduce hospital admissions Improve lung function in severe asthma Also can use as an alternative agent to albuterol Tracheomalacia MDI not administered to soy or peanut allergy patients as it contains soy lecithin
45 Steroids INHALED STEROIDS 2007 NAEPP expert panel does NOT recommend increasing dosing of inhaled steroids for treatment of acute exacerbations Not found effective in reducing severity or progression of exacerbation Higher dose ( > 2 times the normal dose) may be an alternative to oral steroids in mild exacerbations if patient does not tolerate oral steroids- limited data. Short course of oral steroids in addition to short acting beta agonists should be mainstay of treatment for acute exacerbations
46 Delivery Considerations for Inhaled Medications Inhaled medications have equal delivery and efficacy when given properly by nebulizer or MDI/spacer/mask techniques. Blow-by nebulized therapies are ineffective!! Dry powder inhalers require a higher inspiratory flow rate for appropriate deposition (generally for children > 5 yrs) Appropriate spacer device should ALWAYS be used for MDI delivery. combination with a correctly facemask in young children) (in sized
47 Medication administration: MDI with spacers Every MDI needs a spacer No matter the age/medication!
48 Medication administration: Diskus
49 Medication administration: Nebulizers
50 Medication administration: Turbohalers/Twisthalers Budesonide = Controller (Pirbuterol) = Resuce med
51 Key points in medication management Have clear agreed upon goals of therapy Always consider risk of taking medication vs not taking medication. Know your medications ICS dose response curve is relatively flat. Leukotriene inhibitors can also treat Allergic rhinitis and EIA LABA should be reserved for difficult to treat situations and risks should be discussed before prescribing. Consider seasonal treatment for those with asthma symptoms only in relation to certain times of year 51
52 Maintaining Asthma Control Patient follow up at 1-6 month intervals Reassess Impairment and Risk at all visits Incorporate self- assessment (Asthma Control test) Monitor height at every visit Consider stepping up if exacerbation requires oral steroids/ed Consider stepping down therapy when asthma has been well controlled for at least 6 months: Make sure the changes are made gradually. This is necessary to identify minimum therapy associated with good control Closely monitor after changing any therapy to assure sustained control of asthma 52
53 Education & Environmental Prevention Strategies:
54 Asthma Education Basic facts of asthma Normal airways vs. asthma airways What happens to airways in exacerbations Medications Long acting controller meds Short- acting rescue meds Patient skills Medication administration techniques reviewed at every visit. Knowing triggers/ reducing environmental factors Self monitoring- recognizing exacerbations Accessing medical care appropriately Understanding of an asthma action plan Reviewed and provided in writing
55 Management Components: The asthma action plan Reviewed at each visit One for each household In the right language One for school Check literacy Convenient for clinicians Accessible in the EMR
56 Environmental/ Prevention Strategies Animal dander Pollen, outdoor molds, grasses Tobacco smoke Dust mites Live plants, christmas trees Cockroaches Smoke, strong odors, cleaning sprays Bedroom environment Limit stuffed animals Allergy covers on pillows NO pets in bed/bedroom
57 Barriers to Care
58 Unequal burden of asthma About 1 in 6 or (17%) of non-hispanic black children had asthma in 2009 In the greatest rise in asthma rates was among black children with an almost 50 % increase About 40% of uninsured people with asthma reported not being able to afford their medications About 11% of insured people can not afford their asthma medications

59 Asthma Prevalence in the US Affects of Poverty and Race on Pediatric Asthma Prevalence Definitions of poor, near poor and non-poor are based on federal poverty levels that take into account annual/ monthly income and family size Prevalence data MMRW, Jan. 14, 2011
60 Differences in Prevalence African American = 12.7 % Puerto Ricans = 25.7 % Mexican Americans = 6.6% Whites = 8.8% Higher among children Living below the poverty threshold Living in an urban setting Northeastern portion of the US
61 Signals of Poor Asthma Control Utilization of ER Frequency of hospitalizations Repeated use of oral glucocorticoids School absenteeism Inability to participate in physical activity
62 Co-morbidities affecting Asthma control Gastroesophageal reflux (GERD) Obesity Obstructive Sleep Apnea Seasonal or Allergic Rhinitis Sinusitis Allergic bronchopulmonary Aspergillosis (ABPA) Vitamin D Deficiency Stress Depression
63 Considerations for Poor Asthma Control Environmental Exposures ETS, mice, cockroaches Inadequate inhaler technique, broken or missing equipment Ineffective drug dose or dosing interval Other complicating medical problems Substitution of inappropriate treatment Response variability to certain medications Non-adherence
64 Factors affecting adherence Family disagreement about diagnosis Peer rejection Concern about adverse side effects of controllers Financial consequences Disruption of family routines Fear of inability to obtain health insurance with a pre-existing condition Limitations of social interactions because of triggers
65
66 Goals of asthma therapy Reduce Current Impairment Prevent symptoms Infrequent need (<2 days a week) for relief medications (not including prevention of exerciseinduced bronchospasm) Maintain normal, or near normal pulmonary function. Maintain normal activity levels (including exercise and other physical activity and attendance at school). Meet patients and families expectations of and satisfaction with asthma care.
67 Goals of asthma therapy Reduce Risk Prevent recurrent exacerbations of asthma Minimize the need for ED visits or hospitalizations. Prevent loss of lung function; for children, prevent reduced lung growth. Provide optimal pharmacotherapy with minimal or no adverse effects of therapy lowest effective dose.
68 When is a Referral to an Asthma Specialist Needed? Difficulty achieving or maintaining asthma control Patient requires > 2 bursts of systemic steroids in 1 year Exacerbation that requires hospitalization Step 4 or higher care is required (Step 3 or higher for children 0-4 years of age) Immunotherapy or Monoclonal therapy is considered When additional testing is indicated When parent or provider is concerned with symptoms, response to treatment or long term prognosis
69 Thank you Stacy Bichl, APN CPNP
An Overview of Asthma - Diagnosis and Treatment
 An Overview of Asthma - Diagnosis and Treatment Asthma is a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness,
An Overview of Asthma - Diagnosis and Treatment Asthma is a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness,
COPD and Asthma Differential Diagnosis
 COPD and Asthma Differential Diagnosis Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in America. Learning Objectives Use tools to effectively diagnose chronic obstructive
COPD and Asthma Differential Diagnosis Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in America. Learning Objectives Use tools to effectively diagnose chronic obstructive
Information for Behavioral Health Providers in Primary Care. Asthma
 What is Asthma? Information for Behavioral Health Providers in Primary Care Asthma Asthma (AZ-ma) is a chronic (long-term) lung disease that inflames and narrows the airways. Asthma causes recurring periods
What is Asthma? Information for Behavioral Health Providers in Primary Care Asthma Asthma (AZ-ma) is a chronic (long-term) lung disease that inflames and narrows the airways. Asthma causes recurring periods
ASTHMA IN INFANTS AND YOUNG CHILDREN
 ASTHMA IN INFANTS AND YOUNG CHILDREN What is Asthma? Asthma is a chronic inflammatory disease of the airways. Symptoms of asthma are variable. That means that they can be mild to severe, intermittent to
ASTHMA IN INFANTS AND YOUNG CHILDREN What is Asthma? Asthma is a chronic inflammatory disease of the airways. Symptoms of asthma are variable. That means that they can be mild to severe, intermittent to
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
YOU VE BEEN REFERRED TO AN ASTHMA SPECIALIST...
 YOU VE BEEN REFERRED TO AN ASTHMA SPECIALIST... ...HERE S WHAT TO EXPECT You have been referred to an allergist because you have or may have asthma. The health professional who referred you wants you to
YOU VE BEEN REFERRED TO AN ASTHMA SPECIALIST... ...HERE S WHAT TO EXPECT You have been referred to an allergist because you have or may have asthma. The health professional who referred you wants you to
Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis, and asthma
 Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Strategies for Improving Patient Outcomes in Pediatric Asthma Through Education. Pediatric Asthma. Epidemiology. Epidemiology
 Strategies for Improving Patient Outcomes in Pediatric Asthma Through Education Chris Orelup, MS3 Max Project 3/1/01 Pediatric Asthma The leading cause of illness in childhood 10, 000, 000 school absences
Strategies for Improving Patient Outcomes in Pediatric Asthma Through Education Chris Orelup, MS3 Max Project 3/1/01 Pediatric Asthma The leading cause of illness in childhood 10, 000, 000 school absences
Pre-Operative Services Teaching Rounds 2 Jan 2011
 Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Asthma in Infancy, Childhood and Adolescence. Presented by Frederick Lloyd, MD Palo Alto Medical Foundation Palo Alto, California
 Asthma in Infancy, Childhood and Adolescence Presented by Frederick Lloyd, MD Palo Alto Medical Foundation Palo Alto, California Major Health Problem in Childhood Afflicts 2.7 million children in the USA
Asthma in Infancy, Childhood and Adolescence Presented by Frederick Lloyd, MD Palo Alto Medical Foundation Palo Alto, California Major Health Problem in Childhood Afflicts 2.7 million children in the USA
Treatment of Asthma. Talk to your doctor about the various medications available to treat asthma.
 Please call 911 if you think you have a medical emergency. Treatment of Asthma The goals of asthma therapy are to prevent your child from having chronic and troublesome symptoms, to maintain your child's
Please call 911 if you think you have a medical emergency. Treatment of Asthma The goals of asthma therapy are to prevent your child from having chronic and troublesome symptoms, to maintain your child's
Background information
 Background information Asthma Asthma is a complex disease affecting the lungs that can be managed but cannot be cured. 1 Asthma can be controlled well in most people most of the time, although some people
Background information Asthma Asthma is a complex disease affecting the lungs that can be managed but cannot be cured. 1 Asthma can be controlled well in most people most of the time, although some people
PTE Pediatric Asthma Metrics Reporting Updated January 2015
 PTE Pediatric Asthma Metrics Reporting Updated January 20 Introduction: The Maine Health Management Coalition s (MHMC) Pathways to Excellence (PTE) Program is preparing for its next round of PTE Pediatric
PTE Pediatric Asthma Metrics Reporting Updated January 20 Introduction: The Maine Health Management Coalition s (MHMC) Pathways to Excellence (PTE) Program is preparing for its next round of PTE Pediatric
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age
 Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Medicines Use Review Supporting Information for Asthma Patients
 Medicines Use Review Supporting Information for Asthma Patients What is asthma? Asthma is a chronic inflammatory disorder of the airways. The inflammation causes an associated increase in airway hyper-responsiveness,
Medicines Use Review Supporting Information for Asthma Patients What is asthma? Asthma is a chronic inflammatory disorder of the airways. The inflammation causes an associated increase in airway hyper-responsiveness,
The Annual Direct Care of Asthma
 The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
Asthma Intervention. An Independent Licensee of the Blue Cross and Blue Shield Association.
 Asthma Intervention 1. Primary disease education Member will have an increased understanding of asthma and the classification by severity, the risks and the complications. Define asthma Explain how lungs
Asthma Intervention 1. Primary disease education Member will have an increased understanding of asthma and the classification by severity, the risks and the complications. Define asthma Explain how lungs
understanding the professional guidelines
 SEVERE ASTHMA understanding the professional guidelines This guide includes information on what the European Respiratory Society (ERS) and the American Thoracic Society (ATS) have said about severe asthma.
SEVERE ASTHMA understanding the professional guidelines This guide includes information on what the European Respiratory Society (ERS) and the American Thoracic Society (ATS) have said about severe asthma.
Tests. Pulmonary Functions
 Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
5. Treatment of Asthma in Children
 Treatment of sthma in hildren 5. Treatment of sthma in hildren 5.1 Maintenance Treatment 5.1.1 rugs Inhaled Glucocorticoids. Persistent wheezing in children under the age of three can be controlled with
Treatment of sthma in hildren 5. Treatment of sthma in hildren 5.1 Maintenance Treatment 5.1.1 rugs Inhaled Glucocorticoids. Persistent wheezing in children under the age of three can be controlled with
Pediatric. Updated 2008
 A S T H M A P R O V I D E R M A N U A L Pediatric Updated 2008 Asthma 2 Causes of Asthma 3 Utah Prevalence 3 Diagnosis 7 Managing Asthma 9 Education for Partnership in Care 11 Control of Environmental
A S T H M A P R O V I D E R M A N U A L Pediatric Updated 2008 Asthma 2 Causes of Asthma 3 Utah Prevalence 3 Diagnosis 7 Managing Asthma 9 Education for Partnership in Care 11 Control of Environmental
GCE AS/A level 1661/01A APPLIED SCIENCE UNIT 1. Pre-release Article for Examination in January 2010 JD*(A09-1661-01A)
") GCE AS/A level 1661/01A APPLIED SCIENCE UNIT 1 Pre-release Article for Examination in January 2010 JD*(A09-1661-01A) 2 BLANK PAGE 3 Information for Teachers The attached article on asthma is based on some
GCE AS/A level 1661/01A APPLIED SCIENCE UNIT 1 Pre-release Article for Examination in January 2010 JD*(A09-1661-01A) 2 BLANK PAGE 3 Information for Teachers The attached article on asthma is based on some
Respiratory Concerns in Children with Down Syndrome
 Respiratory Concerns in Children with Down Syndrome Paul E. Moore, M.D. Associate Professor of Pediatrics and Pharmacology Director, Pediatric Allergy, Immunology, and Pulmonary Medicine Vanderbilt University
Respiratory Concerns in Children with Down Syndrome Paul E. Moore, M.D. Associate Professor of Pediatrics and Pharmacology Director, Pediatric Allergy, Immunology, and Pulmonary Medicine Vanderbilt University
Management of Asthma
 Federal Bureau of Prisons Clinical Practice Guidelines May 2013 Clinical guidelines are made available to the public for informational purposes only. The Federal Bureau of Prisons (BOP) does not warrant
Federal Bureau of Prisons Clinical Practice Guidelines May 2013 Clinical guidelines are made available to the public for informational purposes only. The Federal Bureau of Prisons (BOP) does not warrant
Asthma Definition. Relationship of Airway Inflammation and Lung Function
 Asthma Guidelines Goals of Medical Care for Adults and Children with Asthma Source: National Institutes of Health, National Heart Lung, and Blood Institute, National Asthma Education and Prevention Program
Asthma Guidelines Goals of Medical Care for Adults and Children with Asthma Source: National Institutes of Health, National Heart Lung, and Blood Institute, National Asthma Education and Prevention Program
Breathe Easy: Asthma and FMLA
 This article was published in the FMLA Policy, Practice, and Legal Update newsletter, by Business & Legal Reports, Inc. (BLR). BLR is a nationally recognized publisher of regulatory and legal compliance
This article was published in the FMLA Policy, Practice, and Legal Update newsletter, by Business & Legal Reports, Inc. (BLR). BLR is a nationally recognized publisher of regulatory and legal compliance
Script Notes: Good (morning, afternoon, evening), my name is, and I will present Asthma Basics for Schools. My goal today is to help you learn more
, my name is, and I will present Asthma Basics for Schools. My goal today is to help you learn more") Script Notes: Good (morning, afternoon, evening), my name is, and I will present Asthma Basics for Schools. My goal today is to help you learn more about asthma and the school age child, as well as the
Script Notes: Good (morning, afternoon, evening), my name is, and I will present Asthma Basics for Schools. My goal today is to help you learn more about asthma and the school age child, as well as the
Asthma. Micah Long, MD
 Asthma Micah Long, MD Goals Define the two components of asthma. Describe the method of action and uses for: Steroids (inhaled and IV) Quick Beta Agonists (Nebs and MDIs) The "Others" Magnesium, Epi IM,
Asthma Micah Long, MD Goals Define the two components of asthma. Describe the method of action and uses for: Steroids (inhaled and IV) Quick Beta Agonists (Nebs and MDIs) The "Others" Magnesium, Epi IM,
ASTHMA< Observation about treatment and education of patients in San Pablo Clinic, Heredia Costa Rica
 ASTHMA< Observation about treatment and education of patients in San Pablo Clinic, Heredia Costa Rica Rachel Borovina, MSIV Lisa Troeger, MSIV University of California San Francisco IHCAI FOUNDATION 2001
ASTHMA< Observation about treatment and education of patients in San Pablo Clinic, Heredia Costa Rica Rachel Borovina, MSIV Lisa Troeger, MSIV University of California San Francisco IHCAI FOUNDATION 2001
Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus
 Asthma Pocket Guide for Primary Care Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus POSITION STATEMENT Despite advances in therapy, asthma remains a disease
Asthma Pocket Guide for Primary Care Annotated from the NAEPP/NHLBI Updated Asthma Guidelines and Developed Through Expert Consensus POSITION STATEMENT Despite advances in therapy, asthma remains a disease
II. ASTHMA BASICS. Overview of Asthma. Why do I need to know about asthma?
 II. ASTHMA BASICS Overview of Asthma Why do I need to know about asthma? In the United States, asthma is the most common chronic childhood illness. Asthma affects an estimated 4.8 million children nationally,
II. ASTHMA BASICS Overview of Asthma Why do I need to know about asthma? In the United States, asthma is the most common chronic childhood illness. Asthma affects an estimated 4.8 million children nationally,
Logistics. Registration for free continuing education (CE) hours or certificate of attendance through TRAIN at: https://tx.train.
 hours or certificate of attendance through TRAIN at: https://tx.train.") . DSHS Grand Rounds Logistics Registration for free continuing education (CE) hours or certificate of attendance through TRAIN at: https://tx.train.org Streamlined registration for individuals not requesting
. DSHS Grand Rounds Logistics Registration for free continuing education (CE) hours or certificate of attendance through TRAIN at: https://tx.train.org Streamlined registration for individuals not requesting
What You Should Know About ASTHMA
 What You Should Know About ASTHMA 200 Hospital Drive Galax, VA 24333 (276) 236-8181 www.tcrh.org WHAT IS ASTHMA? It s a lung condition that makes breathing difficult. The cause of asthma is not known.
What You Should Know About ASTHMA 200 Hospital Drive Galax, VA 24333 (276) 236-8181 www.tcrh.org WHAT IS ASTHMA? It s a lung condition that makes breathing difficult. The cause of asthma is not known.
Severe asthma Definition, epidemiology and risk factors. Mina Gaga Athens Chest Hospital
 Severe asthma Definition, epidemiology and risk factors Mina Gaga Athens Chest Hospital Difficult asthma Defined as asthma, poorly controlled in terms of chronic symptoms, with episodic exacerbations,
Severe asthma Definition, epidemiology and risk factors Mina Gaga Athens Chest Hospital Difficult asthma Defined as asthma, poorly controlled in terms of chronic symptoms, with episodic exacerbations,
Asthma (With a little SCID to start) Disclosures Outline Starting with the Immune System The Innate Immune System The Adaptive Immune System
 Disclosures Outline Starting with the Immune System The Innate Immune System The Adaptive Immune System") 1 2 3 4 5 6 7 8 9 Asthma (With a little SCID to start) Lauren Smith, MD CHKD Pediatric Allergy/Immunology Disclosures None Will be discussing some medications that are not yet FDA approved Outline SCID
1 2 3 4 5 6 7 8 9 Asthma (With a little SCID to start) Lauren Smith, MD CHKD Pediatric Allergy/Immunology Disclosures None Will be discussing some medications that are not yet FDA approved Outline SCID
The Right Medicines Can Help You Get Control of Asthma. BlueCare SM TennCareSelect
 The Right Medicines Can Help You Get Control of Asthma BlueCare SM TennCareSelect WHEEZING. COUGHING. SHORTNESS OF BREATH. CHEST TIGHTNESS. If you or a family member has asthma, you know these symptoms
The Right Medicines Can Help You Get Control of Asthma BlueCare SM TennCareSelect WHEEZING. COUGHING. SHORTNESS OF BREATH. CHEST TIGHTNESS. If you or a family member has asthma, you know these symptoms
Virginia Tech Departmental Policy 27 Sports Medicine Key Function:
 Virginia Tech Departmental Policy 27 Sports Medicine Key Function: Review: Yearly Director of Athletic Training Title: Management of Asthma in Athletes Section: Treatment S-A Safety POLICY STATEMENT: This
Virginia Tech Departmental Policy 27 Sports Medicine Key Function: Review: Yearly Director of Athletic Training Title: Management of Asthma in Athletes Section: Treatment S-A Safety POLICY STATEMENT: This
Dear Provider: Sincerely,
 Asthma Toolkit Dear Provider: L.A. Care is pleased to present this updated asthma toolkit. Our goal is to promote the highest level of asthma care, based on the 2007 National Asthma Education and Prevention
Asthma Toolkit Dear Provider: L.A. Care is pleased to present this updated asthma toolkit. Our goal is to promote the highest level of asthma care, based on the 2007 National Asthma Education and Prevention
Guide to Asthma. Children s of Alabama. P2: Asthma Basics. P4: Asthma Medicines. P6: Spacers. P9: Asthma Triggers. P10: Well-Controlled Asthma
 Children s of Alabama Guide to Asthma 1600 7th Avenue South Birmingham, Alabama 35233 205.638.9100 www.childrensal.org/asthma Patient Health and Safety Information P2: Asthma Basics P4: Asthma Medicines
Children s of Alabama Guide to Asthma 1600 7th Avenue South Birmingham, Alabama 35233 205.638.9100 www.childrensal.org/asthma Patient Health and Safety Information P2: Asthma Basics P4: Asthma Medicines
"Respiratory Problems in Swimmers: How to keep Swimmers Afloat" and in the Pool!
 "Respiratory Problems in Swimmers: How to keep Swimmers Afloat" and in the Pool! Charles Siegel, MD Associate Clinical Professor University of Missouri @ Kansas City School of Medicine USA Swimming does
"Respiratory Problems in Swimmers: How to keep Swimmers Afloat" and in the Pool! Charles Siegel, MD Associate Clinical Professor University of Missouri @ Kansas City School of Medicine USA Swimming does
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
inability to take a deep breath)
") Algorithm for the diagnosis and management of asthma: a practice parameter update These parameters were developed by the Joint Task Force on Practice Parameters, representing the American Academy of Allergy,
Algorithm for the diagnosis and management of asthma: a practice parameter update These parameters were developed by the Joint Task Force on Practice Parameters, representing the American Academy of Allergy,
Breathe With Ease. Asthma Disease Management Program
 Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
ASTHMA FACTS. Prevalence is increasing in many countries, especially in children.
 ASTHMA FACTS Asthma is one of the most common chronic diseases worldwide. It is the most common chronic illness in childhood. Unlike most other chronic diseases, asthma often appears early in life and
ASTHMA FACTS Asthma is one of the most common chronic diseases worldwide. It is the most common chronic illness in childhood. Unlike most other chronic diseases, asthma often appears early in life and
Your Go-to COPD Guide
 Your Go-to COPD Guide Learning how to live with chronic obstructive pulmonary disease (COPD) Inside, you ll learn: COPD facts COPD symptoms and triggers How to talk with your doctor Different treatment
Your Go-to COPD Guide Learning how to live with chronic obstructive pulmonary disease (COPD) Inside, you ll learn: COPD facts COPD symptoms and triggers How to talk with your doctor Different treatment
Asthma Glossary. Allergen
 Action plan Acute Adverse Allergen Allergic asthma Allergic rhinitis Allergist Allergy Allergy shots Alveoli Anaphylaxis Antibiotic Antibodies Antihistamine Asthma Asthma Attack Breath sounds Bronchi (singular,
Action plan Acute Adverse Allergen Allergic asthma Allergic rhinitis Allergist Allergy Allergy shots Alveoli Anaphylaxis Antibiotic Antibodies Antihistamine Asthma Asthma Attack Breath sounds Bronchi (singular,
Pathway for Diagnosing COPD
 Pathway for Diagnosing Visit 1 Registry Clients at Risk Patient presents with symptoms suggestive of Exertional breathlessness Chronic cough Regular sputum production Frequent bronchitis ; wheeze Occupational
Pathway for Diagnosing Visit 1 Registry Clients at Risk Patient presents with symptoms suggestive of Exertional breathlessness Chronic cough Regular sputum production Frequent bronchitis ; wheeze Occupational
COPD PROTOCOL CELLO. Leiden
 COPD PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives and medication of COPD. The Cello way of working can be viewed on
COPD PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives and medication of COPD. The Cello way of working can be viewed on
Childhood Asthma / Wheeze
 Childhood Asthma / Wheeze Symptoms Asthma causes a range of breathing problems. These include wheezing, feeling of tightness in the lungs/chest and a cough (often in the night or early morning). The most
Childhood Asthma / Wheeze Symptoms Asthma causes a range of breathing problems. These include wheezing, feeling of tightness in the lungs/chest and a cough (often in the night or early morning). The most
Objectives COPD. Chronic Obstructive Pulmonary Disease (COPD) 4/19/2011
 4/19/2011") Objectives Discuss assessment findings and treatment for: Chronic Obstructive Pulmonary Disease Bronchitis Emphysema Asthma Anaphylaxis Other respiratory issues Provide some definitions Chronic Obstructive
Objectives Discuss assessment findings and treatment for: Chronic Obstructive Pulmonary Disease Bronchitis Emphysema Asthma Anaphylaxis Other respiratory issues Provide some definitions Chronic Obstructive
EVIDENCE-BASED BEST PRACTICES FOR THE MANAGEMENT OF ASTHMA IN PEDIATRIC PRIMARY CARE IN SOUTH CAROLINA
 EVIDENCE-BASED BEST PRACTICES FOR THE MANAGEMENT OF ASTHMA IN PEDIATRIC PRIMARY CARE IN SOUTH CAROLINA Sarah Ball, PharmD Mike Bowman, MD Sandra Garner, PharmD Nancy Hahn, PharmD Sophie Robert, PharmD
EVIDENCE-BASED BEST PRACTICES FOR THE MANAGEMENT OF ASTHMA IN PEDIATRIC PRIMARY CARE IN SOUTH CAROLINA Sarah Ball, PharmD Mike Bowman, MD Sandra Garner, PharmD Nancy Hahn, PharmD Sophie Robert, PharmD
Guidance to support the stepwise review of combination inhaled corticosteroid therapy for adults ( 18yrs) in asthma
 in asthma") Guidance to support the stepwise review of combination inhaled corticosteroid therapy for adults ( 18yrs) in asthma Important Complete asthma control needs to be achieved for at least 12 weeks before attempting
Guidance to support the stepwise review of combination inhaled corticosteroid therapy for adults ( 18yrs) in asthma Important Complete asthma control needs to be achieved for at least 12 weeks before attempting
Chronic obstructive pulmonary disease (COPD)
") Chronic obstructive pulmonary disease (COPD) Chronic obstructive pulmonary disease (COPD) is the name for a group of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways
Chronic obstructive pulmonary disease (COPD) Chronic obstructive pulmonary disease (COPD) is the name for a group of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways
Prevention of Acute COPD exacerbations
 December 3, 2015 Prevention of Acute COPD exacerbations George Pyrgos MD 1 Disclosures No funding received for this presentation I have previously conducted clinical trials with Boehringer Ingelheim. Principal
December 3, 2015 Prevention of Acute COPD exacerbations George Pyrgos MD 1 Disclosures No funding received for this presentation I have previously conducted clinical trials with Boehringer Ingelheim. Principal
A PRACTICAL APPROACH TO CHRONIC COUGH IN CHILDREN
 A PRACTICAL APPROACH TO CHRONIC COUGH IN CHILDREN Chng Seo Yi Chronic cough is defined as a persistent cough of more than three weeks duration which is not getting better. It is a common symptom in childhood.
A PRACTICAL APPROACH TO CHRONIC COUGH IN CHILDREN Chng Seo Yi Chronic cough is defined as a persistent cough of more than three weeks duration which is not getting better. It is a common symptom in childhood.
Recurrent or Persistent Pneumonia
 Recurrent or Persistent Pneumonia Lower Respiratory Tract Dr T Avenant Recurrent or Persistent Pneumonia Definitions Recurrent pneumonia more than two episodes of pneumonia in 18 months Persistent pneumonia
Recurrent or Persistent Pneumonia Lower Respiratory Tract Dr T Avenant Recurrent or Persistent Pneumonia Definitions Recurrent pneumonia more than two episodes of pneumonia in 18 months Persistent pneumonia
Training Manual & Speaker s Guide
 Training Manual & Speaker s Guide Based on National Asthma Education and Prevention Program (NAEPP) Guidelines including the NAEPP s Guidelines Implementation Panel (GIP) Priority Messages. Funded in part
Training Manual & Speaker s Guide Based on National Asthma Education and Prevention Program (NAEPP) Guidelines including the NAEPP s Guidelines Implementation Panel (GIP) Priority Messages. Funded in part
MILITARY (ACTIVE DUTY)-SPECIFIC ISSUES
-SPECIFIC ISSUES") RECOMMENDATIONS MILITARY (ACTIVE DUTY)-SPECIFIC ISSUES Evaluation for possible asthma 1. Active duty service members should be diagnosed with asthma or exerciseinduced bronchospasm on the basis of the
RECOMMENDATIONS MILITARY (ACTIVE DUTY)-SPECIFIC ISSUES Evaluation for possible asthma 1. Active duty service members should be diagnosed with asthma or exerciseinduced bronchospasm on the basis of the
The Link Between Viruses and Asthma Catherine Kier, M.D.
 The Link Between Viruses and Asthma Catherine Kier, M.D. Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary Director, Cystic Fibrosis Center No disclosures Objectives: At the end of this
The Link Between Viruses and Asthma Catherine Kier, M.D. Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary Director, Cystic Fibrosis Center No disclosures Objectives: At the end of this
Spirometry Workshop for Primary Care Nurse Practitioners
 Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Visiting Assistant
Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Visiting Assistant
medicineupdate to find out more about this medicine
 medicineupdate Asking the right questions about new medicines Seretide for chronic obstructive pulmonary disease What this medicine is 1 What this medicine treats 2 Other medicines available for this condition
medicineupdate Asking the right questions about new medicines Seretide for chronic obstructive pulmonary disease What this medicine is 1 What this medicine treats 2 Other medicines available for this condition
Get Your Head In The Game. Matthew Voorman, MD Hutchinson Clinic March 21, 2016
 Get Your Head In The Game Matthew Voorman, MD Hutchinson Clinic March 21, 2016 About Me Otolaryngology Head & Neck Surgery Geisinger Medical Center General Surgery University of California San Francisco
Get Your Head In The Game Matthew Voorman, MD Hutchinson Clinic March 21, 2016 About Me Otolaryngology Head & Neck Surgery Geisinger Medical Center General Surgery University of California San Francisco
Frequent co-morbid conditions with asthma. Nelson Rosário MD, PhD, FAAAAI, FACAAI
 Frequent co-morbid conditions with asthma Nelson Rosário MD, PhD, FAAAAI, FACAAI Comorbidities in childhood asthma Knowledge is sparse. Further studies are needed: to identify the prevalence the effects
Frequent co-morbid conditions with asthma Nelson Rosário MD, PhD, FAAAAI, FACAAI Comorbidities in childhood asthma Knowledge is sparse. Further studies are needed: to identify the prevalence the effects
The Proper Treatment Of Asthma
 The Proper Treatment Of Asthma Southwest Allergy & Asthma Foundation Page 1 of 10 INTRODUCTION The purpose of this pamphlet is to supply information which will give patients suffering with asthma, an intelligent
The Proper Treatment Of Asthma Southwest Allergy & Asthma Foundation Page 1 of 10 INTRODUCTION The purpose of this pamphlet is to supply information which will give patients suffering with asthma, an intelligent
Seasonal Allergies. 1995-2012 The Patient Education Institute, Inc. www.x-plain.com im010101 Last reviewed: 05/30/2012 1
 Seasonal Allergies Introduction Seasonal allergies are allergies that develop during certain times of the year. Seasonal allergies are usually a response to pollen from trees, grasses, and weeds. Constant
Seasonal Allergies Introduction Seasonal allergies are allergies that develop during certain times of the year. Seasonal allergies are usually a response to pollen from trees, grasses, and weeds. Constant
COPD It Can Take Your Breath Away www.patientedu.org
 written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are 2 major diseases included in COPD:
written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are 2 major diseases included in COPD:
Making a Difference in the Management of Asthma: A Guide for Respiratory Therapists
 Making a Difference in the Management of Asthma: A Guide for Respiratory Therapists U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Heart, Lung, and Blood Institute
Making a Difference in the Management of Asthma: A Guide for Respiratory Therapists U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Heart, Lung, and Blood Institute
Arizona Comprehensive Asthma Control Plan...
 Arizona Comprehensive Asthma Control Plan... The Arizona Department of Health Services sponsored the development of this plan with the intent to set priorities and suggest strategies to address asthma
Arizona Comprehensive Asthma Control Plan... The Arizona Department of Health Services sponsored the development of this plan with the intent to set priorities and suggest strategies to address asthma
Pharmacology of the Respiratory Tract: COPD and Steroids
 Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
In the last few decades, asthma has become epidemic. As the most common
 Licensed School Nurse/ Public Health Nurse/ Registered Nurse In the last few decades, asthma has become epidemic. As the most common chronic childhood disease, asthma affects more than six million children
Licensed School Nurse/ Public Health Nurse/ Registered Nurse In the last few decades, asthma has become epidemic. As the most common chronic childhood disease, asthma affects more than six million children
Epidemiological Studies on Environmental Stressors from Tobacco to Pesticides
 Epidemiological Studies on Environmental Stressors from Tobacco to Pesticides W. Susan Cheng, PhD, MPH Rebecca Carlstrom, MPH Sukaina Hussain, MPH Healthy Lawn Symposium Oct 31, 2014 Two Presentations
Epidemiological Studies on Environmental Stressors from Tobacco to Pesticides W. Susan Cheng, PhD, MPH Rebecca Carlstrom, MPH Sukaina Hussain, MPH Healthy Lawn Symposium Oct 31, 2014 Two Presentations
The asthmatic patient and sedation
 The asthmatic patient and sedation Introduction The sedation practitioner is often faced with difficult questions to answer before the administration of sedation. Our guidelines say clearly that we are
The asthmatic patient and sedation Introduction The sedation practitioner is often faced with difficult questions to answer before the administration of sedation. Our guidelines say clearly that we are
So You Have Asthma NIH Publication No. 07-5248 March 2007
 So You HaveAsthma So You HaveAsthma NIH Publication No. 07-5248 March 2007 Contents Introduction.......................................................1 Asthma Some Basics..............................................3
So You HaveAsthma So You HaveAsthma NIH Publication No. 07-5248 March 2007 Contents Introduction.......................................................1 Asthma Some Basics..............................................3
How to Manage Asthma in Children
 Clinical Guideline for the Diagnosis, Evaluation and Management of Adults and Children with Asthma Color Key n Four Components of Asthma Care n Classifying Asthma Severity, Assessing Asthma Control and
Clinical Guideline for the Diagnosis, Evaluation and Management of Adults and Children with Asthma Color Key n Four Components of Asthma Care n Classifying Asthma Severity, Assessing Asthma Control and
COPD MANAGEMENT PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines f the collabative management of patients with a diagnosis of chronic obstructive pulmonary disease (COPD) who are not adequately controlled and to define the roles and
I. PURPOSE To establish guidelines f the collabative management of patients with a diagnosis of chronic obstructive pulmonary disease (COPD) who are not adequately controlled and to define the roles and
Understanding COPD. Carolinas Healthcare System
 Understanding COPD Carolinas Healthcare System 2013 This self-directed learning module contains information about the pathophysiology, diagnosis, and treatment of COPD. Target Audience: All RNs and LPNs
Understanding COPD Carolinas Healthcare System 2013 This self-directed learning module contains information about the pathophysiology, diagnosis, and treatment of COPD. Target Audience: All RNs and LPNs
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Afrezza Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
Afrezza Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
Drug therapy SHORT-ACTING BETA AGONISTS SHORT-ACTING ANTICHOLINERGICS LONG-ACTING BETA AGONISTS LONG-ACTING ANTICHOLINERGICS
 Drug therapy 6 6.1 What is the role of bronchodilators in COPD? 52 SHORT-ACTING BETA AGONISTS 6.2 How do short-acting beta agonists work? 52 6.3 What are the indications for their use? 52 6.4 What is the
Drug therapy 6 6.1 What is the role of bronchodilators in COPD? 52 SHORT-ACTING BETA AGONISTS 6.2 How do short-acting beta agonists work? 52 6.3 What are the indications for their use? 52 6.4 What is the
DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A TERTIARY CARE HOSPITAL
 International Journal of Pharmaceutical Applications ISSN 0976-2639, Online ISSN 2278 6023 Vol 3, Issue 2, 2012, pp 297-305 http://www.bipublication.com DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A
International Journal of Pharmaceutical Applications ISSN 0976-2639, Online ISSN 2278 6023 Vol 3, Issue 2, 2012, pp 297-305 http://www.bipublication.com DRUG UTILISATION STUDY IN BRONCHIAL ASTHMA IN A
PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE
 PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE The content of this booklet was developed by Allergy UK. MSD reviewed this booklet to comment
PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE The content of this booklet was developed by Allergy UK. MSD reviewed this booklet to comment
Subject ID: Subject Initials Date completed Interviewer. Person answering questions. 1 yes 2 no
 COAST III Childhood Origins of ASThma Asthma Allergy Symptoms COAST 3 year visit Subject ID Subject ID: Subject Initials Date completed Interviewer Person answering questions 99. This form was completed
COAST III Childhood Origins of ASThma Asthma Allergy Symptoms COAST 3 year visit Subject ID Subject ID: Subject Initials Date completed Interviewer Person answering questions 99. This form was completed
SIGN 141 British guideline on the management of asthma. A national clinical guideline. Evidence
 SIGN 141 British guideline on the management of asthma A national clinical guideline October 2014 Evidence KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality
SIGN 141 British guideline on the management of asthma A national clinical guideline October 2014 Evidence KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality
Allergy Testing Test Request and Result Interpretation. Learning Objectives
 Allergy Testing Test Request and Result Interpretation Dr. Kareena Schnabl, MSc, PhD, FCACB Clinical Biochemist, Genetic Laboratory Services University of Alberta Hospital Newborn Screening & Biochemical
Allergy Testing Test Request and Result Interpretation Dr. Kareena Schnabl, MSc, PhD, FCACB Clinical Biochemist, Genetic Laboratory Services University of Alberta Hospital Newborn Screening & Biochemical
British Guideline on the Management of Asthma
 101 British Guideline on the Management of Asthma A national clinical guideline May 2008 Revised January 2012 KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality
101 British Guideline on the Management of Asthma A national clinical guideline May 2008 Revised January 2012 KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality
Better Breathing with COPD
 Better Breathing with COPD People with Chronic Obstructive Pulmonary Disease (COPD) often benefit from learning different breathing techniques. Pursed Lip Breathing Pursed Lip Breathing (PLB) can be very
Better Breathing with COPD People with Chronic Obstructive Pulmonary Disease (COPD) often benefit from learning different breathing techniques. Pursed Lip Breathing Pursed Lip Breathing (PLB) can be very
RSPT 2317 Non-steroidal anti-asthma agents
 RSPT 2317 Non-steroidal Anti-asthma Agents Mechanisms of Inflammation in Asthma Mechanisms of Inflammation in Asthma Asthma is a chronic inflammatory disorder of the airways It is divided into extrinsic
RSPT 2317 Non-steroidal Anti-asthma Agents Mechanisms of Inflammation in Asthma Mechanisms of Inflammation in Asthma Asthma is a chronic inflammatory disorder of the airways It is divided into extrinsic
Interpretation of Pulmonary Function Tests
 Interpretation of Pulmonary Function Tests Dr. Sally Osborne Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp building 604 822-3421 sally.osborne@ubc.ca www.sallyosborne.com
Interpretation of Pulmonary Function Tests Dr. Sally Osborne Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp building 604 822-3421 sally.osborne@ubc.ca www.sallyosborne.com
ACTIVITY #3: LUNG HEALTH ASTHMA AND ALLERGIES
 ACTIVITY #3: LUNG HEALTH ASTHMA AND ALLERGIES TIME 50 minutes, computer lab REQUIRED RESOURCES Activity Computer lab with internet access for student research Notepaper and pencil for research Poster board
ACTIVITY #3: LUNG HEALTH ASTHMA AND ALLERGIES TIME 50 minutes, computer lab REQUIRED RESOURCES Activity Computer lab with internet access for student research Notepaper and pencil for research Poster board
Understanding and Controlling Asthma Attacks. Information for parents
 Understanding and Controlling Asthma Attacks Information for parents Your child was recently seen by a doctor for asthma. This guide will help you gain a better understanding about your child's recent
Understanding and Controlling Asthma Attacks Information for parents Your child was recently seen by a doctor for asthma. This guide will help you gain a better understanding about your child's recent
RELAPSE MANAGEMENT. Pauline Shaw MS Nurse Specialist 25 th June 2010
 RELAPSE MANAGEMENT Pauline Shaw MS Nurse Specialist 25 th June 2010 AIMS OF SESSION Relapsing/Remitting MS Definition of relapse/relapse rate Relapse Management NICE Guidelines Regional Clinical Guidelines
RELAPSE MANAGEMENT Pauline Shaw MS Nurse Specialist 25 th June 2010 AIMS OF SESSION Relapsing/Remitting MS Definition of relapse/relapse rate Relapse Management NICE Guidelines Regional Clinical Guidelines
Clinical Research Pediatric Pulmonary Division
 Clinical Research Pediatric Pulmonary Division Hengameh H. Raissy, PharmD Research Associate Professor, Pediatric Pulmonary UNM HSC Director of Clinical Trials Presented at Envision NM Asthma / Pulmonary
Clinical Research Pediatric Pulmonary Division Hengameh H. Raissy, PharmD Research Associate Professor, Pediatric Pulmonary UNM HSC Director of Clinical Trials Presented at Envision NM Asthma / Pulmonary
written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org/copd
 written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org/copd What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are two major diseases included in
written by Harvard Medical School COPD It Can Take Your Breath Away www.patientedu.org/copd What Is COPD? COPD stands for chronic obstructive pulmonary disease. There are two major diseases included in
Department of Surgery
 What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
PULMONARY FUNCTION TESTS A Workshop on Simple Spirometry & Flow Volume Loops
 PULMONARY FUNCTION TESTS A Workshop on Simple Spirometry & Flow Volume Loops YOU SHOULD READ THE FOLLOWING MATERIAL BEFORE Tuesday March 30 Interpretation of PFTs Learning Objectives 1. Specify the indications
PULMONARY FUNCTION TESTS A Workshop on Simple Spirometry & Flow Volume Loops YOU SHOULD READ THE FOLLOWING MATERIAL BEFORE Tuesday March 30 Interpretation of PFTs Learning Objectives 1. Specify the indications
British Guideline on the Management of Asthma
 101 British Guideline on the Management of Asthma A national clinical guideline May 2008 revised May 2011 KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality meta-analyses,
101 British Guideline on the Management of Asthma A national clinical guideline May 2008 revised May 2011 KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality meta-analyses,
Population Health Management Program
 Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Stanley J. Szefler, MD National Jewish Medical and Research Center
 New Asthma Guidelines: Special Attention to Infant Wheezers Stanley J. Szefler, MD Helen Wohlberg & Herman Lambert Chair in Pharmacokinetics, & Professor of Pediatrics and Pharmacology, University of Colorado
New Asthma Guidelines: Special Attention to Infant Wheezers Stanley J. Szefler, MD Helen Wohlberg & Herman Lambert Chair in Pharmacokinetics, & Professor of Pediatrics and Pharmacology, University of Colorado
Understanding Cough, Wheezing and Noisy Breathing in Children. Introduction
 Understanding Cough, Wheezing and Noisy Breathing in Children Introduction Symptoms such as cough, wheezing or noisy breathing can be caused by a number of conditions. When these occur, it is natural for
Understanding Cough, Wheezing and Noisy Breathing in Children Introduction Symptoms such as cough, wheezing or noisy breathing can be caused by a number of conditions. When these occur, it is natural for
Asthma Care. Of course, your coach is there to answer any questions you have about your asthma, such as:
 Asthma Care All Health Coaches in the Asthma Care Management program are registered or certified respiratory therapists. Your coach will listen to your story of living with asthma. This will help your
Asthma Care All Health Coaches in the Asthma Care Management program are registered or certified respiratory therapists. Your coach will listen to your story of living with asthma. This will help your
Objectives. Asthma Management
 Objectives Asthma Management BREATHE Conference Allergy and Asthma Specialists PC Christine Malloy MD March 22, 2013 Review the role of inflammation in asthma Discuss the components of the EPR-3 management
Objectives Asthma Management BREATHE Conference Allergy and Asthma Specialists PC Christine Malloy MD March 22, 2013 Review the role of inflammation in asthma Discuss the components of the EPR-3 management