Thank you for choosing JPS and we look forward to providing quality healthcare to you and your family. FINAL CHECK LIST
|
|
|
- Clifford Walton
- 7 years ago
- Views:
Transcription
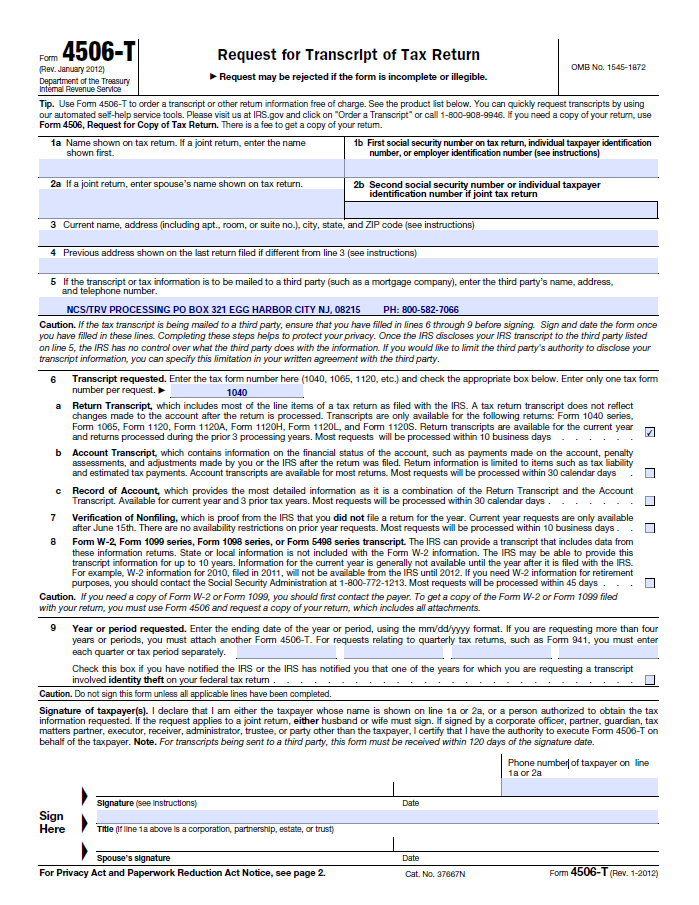
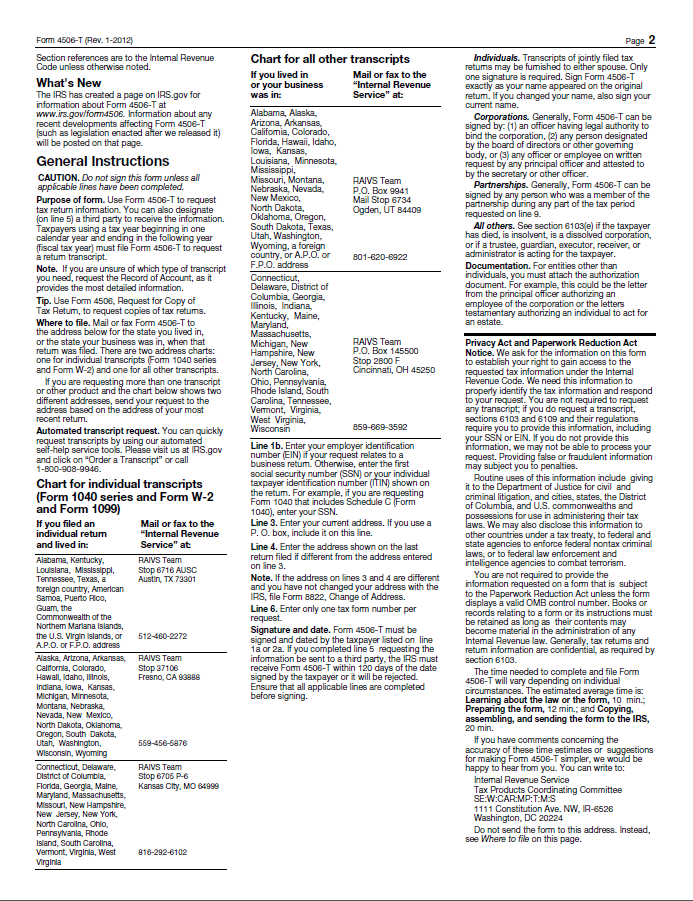
1 Welcome to JPS Health Network. We look forward to providing affordable health care to you and your family. The purpose of the JPS Connection program is to create a healthier community by providing discount health services to Tarrant County residents. Connection cardholders have the benefit of a medical home meaning you have a physician or nurse practitioner assigned to you and your family. You get access to preventative care such as physicals and screenings that will help keep you healthy and out of the emergency room. Inside this packet you will find the application and the documentation requirements for our JPS Connection program. All items on the application must be completed. If not applicable, place either a 0 or N/A in each box. Bring the completed application and required documentation per the final checklist below with you to any of the financial screening locations throughout Tarrant County between the hours of 8:00 a.m. and 4:00 p.m. You may call our Eligibility Center at (817) should you need assistance. Our staff members are happy to answer any questions you may have. Applications can also be faxed to or ed to Enroll@JPSHealth.org. Thank you for choosing JPS and we look forward to providing quality healthcare to you and your family. Regards, Kade Rutherford Executive Director, Revenue Cycle Picture ID (Government Issued or School ID) FINAL CHECK LIST Immigration Documentation (Resident Alien Cards, Passports, Certificate of Naturalization, I-94) Birth Certificates for child dependents Shelter /Approved Agency Residence Letter or Valid Homeless Scan Card Agency award letters (Food Stamps, TANF, Housing, CHIP/Medicaid) Completed Application (Incomplete applications will not be accepted) Application signed and dated by applicant and spouse (even if spouse is not applying) Complete and sign form 4506T Review, initial, and sign the Membership Responsibility Form Homeowners, self-employed, or clients receiving Social Security must provide current 30 day bank statement for all accounts, current asset documentation (401K, 403B, IRA, CD, Stocks, Mutual Funds, etc.) Full time students applying with parents must provide a copy of their school schedule **More information may be requested at time of interview** Revised 9/25/14
2 JPS Health Network Application for JPS Connection Program 11/19/13 Name: Maiden Name: (Last) (First) (MI) Live w/ someone Rent Home #: Address: Own Cell#: (Street) (Apt. #) (City) (State) (Zip) (County) Please check primary contact phone Address: Homeless / Scan Card Primary Language: English Spanish Vietnamese Other Marital Status: Single Separated Divorced Widowed Married (If married, spouse s signature also is required) Ethnicity: Caucasian African-American Hispanic Asian Native American Other List the names of each person living in household (attach additional sheets as necessary) Must provide copies of identification documents such as a state issued driver s license/id, birth certificates (for children under 18) & Immigration cards. Full Name of Household Members: Relationship to applicant: Self Spouse Child Child Child Sex: Date of Birth Place of Birth Check one: Social Security # Is this person applying for coverage? (Circle One) First time applying? Is this person pregnant? (Circle One) Does this person currently have medical coverage? (Check box) None None None None None Is this person a Veteran? (Circle One) Does person receive Food Stamps, TANF or Housing assistance**? (Circle one) **Must provide a copy of current award letters if, a member of your household receives TANF, Food Stamps and/or Housing assistance. 1 of 3
3 List the names of each person living in household (attach additional sheets as necessary) Do not leave blank spaces if it does not apply put a -0- or N/A Application will be returned if boxes are left unanswered. Full Name of Household Members: Relationship to applicant: Self Spouse Child Child Child If you and/or a member of the household work for yourself, do odd jobs or work for someone but do not have taxes withheld from your wages then you or that household member are self-employed. Is this person Self Employed? (Circle one) Monthly Income After Deductions from Self Employment $ $ $ $ $ Do you and/or a member of the household work: Is this person Employed? (Circle one) Name: Street Address: State, City, Zip: Phone: Monthly Income before deductions from Employment $ $ $ $ $ List additional work information here: 2 nd Name: 2 nd Street Address: 2 nd State, City, Zip: 2 nd Phone: Monthly Income before deductions from Employment $ $ $ $ $ Other Monthly Income and/or Financial Aid: Unemployment $ $ $ $ $ Workers Compensation $ $ $ $ $ Child Support/Alimony $ $ $ $ $ Pensions/Retirement $ $ $ $ $ Social Security (SSI)/(RSDI) $ $ $ $ $ VA Benefits $ $ $ $ $ Oil/Royalties $ $ $ $ $ School financial aid $ $ $ $ $ Money received from family and friends $ $ $ $ $ The last year an Income Tax Return was filed Year Year Year Year Year 2 of 3
4 List all assets owned by members of your household (attach additional sheets if necessary) Assets and Bank Accounts: Bank name Bank account type: (Circle All that Apply) Balance for all bank accounts $ Bank name Bank account type: (Circle All that Apply) Balance for all bank accounts $ Retirement Accounts: Bank or Company Name Account type: (Circle All that Apply) Current Cash Value for all accounts $ CD and Investment Accounts: Bank or Company Name Account type: (Circle All that Apply) Current Cash Value for all accounts $ Checking Savings Business Accounts Checking Savings Business Accounts IRA 401(k) 403(b) Other: CD Stocks Mutual Funds Other: "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under federal law and/or state law. Everything on this application is the truth as best I know it." If at any time false information is discovered, penalties will include, but are not limited to, loss of household benefits and the inability to reapply for the JPS Connection Program for no less than a period of ninety (90) days. I authorize JPS Health Network to obtain electronic records for the purpose of making a determination of whether I meet the eligibility requirements for the JPS Connection Program. I also understand that any approval will be conditional based on the information reviewed in my records. Signature of Applicant: Date: Signature of Co-Applicant/Spouse: Date: Spouse s signature is required to complete screening even if spouse is not requesting assistance at this time. For Office Use Only: This application is good for 30 days from the date above. If someone helped you to complete this form, please give his or her name. Name (please print): Telephone number: 3 of 3
5 JPS Health Network Verification of Assistance and Residency for JPS Connection Program This form only needs to be completed if the applicant is being assisted by another individual. I, verify that Name of person providing assistance Applicant(s) full name Patient s MR# and/or Social Security # lives at Applicant(s) Address City/Zip Code Financial Assistance: I provide financial assistance to the applicant. Yes No This individual is claimed as a dependent on my most recent filed income tax return. Yes No Does the applicant have a job? If yes, provide employer name Does the applicant have another income source? If yes, how much I provide applicant with the following: Food Personal items Transportation Cash/Check $ per Week or Month Other Do you pay rent or other bills for this applicant? If yes, how much and how often? Residency Assistance (check all that apply): The applicant(s) resides at my Tarrant County residence. The applicant(s) does not pay rent to me. The applicant(s) pays to help toward the rent and utilities. How long has the applicant(s) resided at your address? Does the applicant(s) have another residence? If yes, where Relationship of Person Providing the Assistance to the Applicant(s): I certify that the above information is true and correct. "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under federal law and/or state law. Everything on this application is the truth as best I know it. Signature of the Person Providing the Assistance: Address, City, State, Zip: Phone Number: Date signed:
6 JPS Health Network Membership Responsibilities for JPS Connection Indigent Healthcare Program I understand that the JPS Connection does not cover all of the services provided at JPS Health Network including, but not limited to, dental, podiatry, cosmetic procedures, assisted reproductive technology and transplants. JPS Connection is a tax-supported medical program offered to eligible Tarrant County residents. JPS Connection offers low cost medical care available only through JPS Health Network facilities. I understand that JPS Connection is not an insurance company or an insurance plan. At this time, I am not covered under any third party commercial insurance, Medicaid and/or parts A&B of Medicare. I understand that if I am deemed eligible for state, federal or pharmaceutical assistance programs, I must comply with seeking that assistance. Failure to do so will make me ineligible for JPS Connection. Documentation provided to JPS Health Network will be used to apply for any coverage for which I may be potentially eligible. I am aware that when JPS Connection is used secondary to another payor, I am responsible for all physician/professional fees, co-payments and any deductibles related to professional services rendered. This includes, but not limited to, NTMAG, UNT, Sheridan, RadCare, EmCare or any other professional group you may receive bills from. As a JPS Connection member, I understand that I have an obligation to notify the Financial Screening department of JPS Health Network of any changes. I agree to inform the Financial Screening department of the JPS Health Network immediately of any changes in my Tarrant County residence, household income, family size and insurance coverage. I understand that the JPS Connection membership privileges are on a limited time basis. In order to continue receiving a discount on medical services, through the JPS Connection program, it will be necessary to complete another financial screening at the end of my enrollment period. You will be expected to pay all charges incurred after eligibility has expired. I acknowledge that should the JPS Health Network receive returned mail, from the mailing address I provided, that my JPS Connection membership privileges will be suspended pending further review. I understand that I am responsible for providing true and accurate documentation. If at any time false information is discovered penalties may include, but not limited to, loss of my membership benefits and the inability to reapply for the JPS Connection Indigent Healthcare Program for no less than a period of ninety (90) days. "I understand that anyone who knowingly lies or misrepresents the truth or arranges for someone to knowingly lie or misrepresent the truth in the completion of this application is committing a crime which can be punished under Federal law, State law, or both. Everything on this application is the truth as best I know it." Signature of Applicant: Date: Signature of Co-Applicant: Date:
7
8
Application for Mississippi Medicaid Aged, Blind and Disabled Medicaid Programs
 Application for Mississippi Medicaid Aged, Blind and Disabled Medicaid Programs This application is used for an individual, couple or child to apply for Medicaid due to age or disability. Please read each
Application for Mississippi Medicaid Aged, Blind and Disabled Medicaid Programs This application is used for an individual, couple or child to apply for Medicaid due to age or disability. Please read each
Application for Legal Assistance
 Application for Legal Assistance 1. What kind of problem do you need help with? Divorce Child Custody Guardianship Bankruptcy Tax Landlord/Tenant Will / Estate Planning Other 2. Applicant Information Your
Application for Legal Assistance 1. What kind of problem do you need help with? Divorce Child Custody Guardianship Bankruptcy Tax Landlord/Tenant Will / Estate Planning Other 2. Applicant Information Your
Brook Haven 7781 Crystal Brook Circle * Brooksville, FL 34601 Office (352) 397-4340 Fax (813) 925-4287 RENTAL APPLICATION
 397-4340 Fax (813) 925-4287 RENTAL APPLICATION") Brook Haven 7781 Crystal Brook Circle * Brooksville, FL 34601 Office (352) 397-4340 Fax (813) 925-4287 RENTAL APPLICATION Desired Community Name Desired Move-in Date / /20 Desired Apartment Size (check
Brook Haven 7781 Crystal Brook Circle * Brooksville, FL 34601 Office (352) 397-4340 Fax (813) 925-4287 RENTAL APPLICATION Desired Community Name Desired Move-in Date / /20 Desired Apartment Size (check
MEDICAL ASSISTANCE (MA)/MCHP APPLICATION FOR FAMILIES, PREGNANT WOMEN, AND CHILDREN
/MCHP APPLICATION FOR FAMILIES, PREGNANT WOMEN, AND CHILDREN") Si necesita ayuda para llenar el formulario favor de llamar al 1-800-456-8900 Please PRINT in blue or black ink. MEDICAL ASSISTANCE (MA)/MCHP APPLICATION FOR FAMILIES, PREGNANT WOMEN, AND CHILDREN Date
Si necesita ayuda para llenar el formulario favor de llamar al 1-800-456-8900 Please PRINT in blue or black ink. MEDICAL ASSISTANCE (MA)/MCHP APPLICATION FOR FAMILIES, PREGNANT WOMEN, AND CHILDREN Date
Health Benefits for Workers with Disabilities Application
 Illinois Department of Public Aid Health Benefits for Workers with Disabilities Application Note: This is NOT an application for cash assistance, food stamps or enrollment in the Medicaid spenddown program.
Illinois Department of Public Aid Health Benefits for Workers with Disabilities Application Note: This is NOT an application for cash assistance, food stamps or enrollment in the Medicaid spenddown program.
FINANCIAL ASSISTANCE APPLICATION: COVER LETTER
 FINANCIAL ASSISTANCE APPLICATION: COVER LETTER Thank you for choosing Children s of Alabama to provide for the healthcare needs of your child. Please find attached the forms you must complete in order
FINANCIAL ASSISTANCE APPLICATION: COVER LETTER Thank you for choosing Children s of Alabama to provide for the healthcare needs of your child. Please find attached the forms you must complete in order
Please note: We are accepting applications for 1-4 bedroom apartments only.
 Page 1 Gardens at SouthBay Preliminary Application 6720 S. Louis Ave, Tampa, FL 33616 PLEASE RETURN APPLICATION MONDAY THURSDAY 9AM 6PM POR FAVOR DE REGRESAR LA APLICACIÓN DE LUNES A JUEVES DE 9AM A 6PM
Page 1 Gardens at SouthBay Preliminary Application 6720 S. Louis Ave, Tampa, FL 33616 PLEASE RETURN APPLICATION MONDAY THURSDAY 9AM 6PM POR FAVOR DE REGRESAR LA APLICACIÓN DE LUNES A JUEVES DE 9AM A 6PM
Application for Subsidized Child Care
 COMMONWEALTH OF PENNSYLVANIA Application for Subsidized Child Care This application may be used by families who want help in paying their child care costs. The Child Care Information Services (CCIS) agency
COMMONWEALTH OF PENNSYLVANIA Application for Subsidized Child Care This application may be used by families who want help in paying their child care costs. The Child Care Information Services (CCIS) agency
Criminal background and eviction will be check within the past 5 years.
 Housing Authority of the City of Fort Lauderdale (HACFL) Telephone: (954)556-4100 Submit your application to: HACFL- Affordable Housing Division 500 West Sunrise Boulevard Fort Lauderdale, FL 33311 The
Housing Authority of the City of Fort Lauderdale (HACFL) Telephone: (954)556-4100 Submit your application to: HACFL- Affordable Housing Division 500 West Sunrise Boulevard Fort Lauderdale, FL 33311 The
FREE CARE APPLICATION ATTACHMENT
 FREE CARE APPLICATION ATTACHMENT PLEASE REMEMBER THIS IS NOT AN INSURANCE PLAN IT IS A CHARITABLE CARE PROGRAM AND THERE IS NO ESTABLISHED FUND. THERE IS NO MONEY EXCHANGED FOR SERVICES BY ANY CMC PHYSICIAN/PRACTICE.
FREE CARE APPLICATION ATTACHMENT PLEASE REMEMBER THIS IS NOT AN INSURANCE PLAN IT IS A CHARITABLE CARE PROGRAM AND THERE IS NO ESTABLISHED FUND. THERE IS NO MONEY EXCHANGED FOR SERVICES BY ANY CMC PHYSICIAN/PRACTICE.
City of Odessa Community Development Home of Your Own/Homeownership Assistance Programs
 City of Odessa Community Development Home of Your Own/Homeownership Assistance Programs The following items must be submitted with your application before we can proceed with processing. All portions of
City of Odessa Community Development Home of Your Own/Homeownership Assistance Programs The following items must be submitted with your application before we can proceed with processing. All portions of
SECTION I. Answer the questions in Section I to determine if application needs to be completed for person needing help with medical bills.
 N.C. Department of Health and Human Services Division of Medical Assistance Breast and Cervical Cancer Medicaid Application SECTION I. Answer the questions in Section I to determine if application needs
N.C. Department of Health and Human Services Division of Medical Assistance Breast and Cervical Cancer Medicaid Application SECTION I. Answer the questions in Section I to determine if application needs
P E N N S Y L V A N I A
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
The Kaiser Permanente Bridge Program Application
 The Kaiser Permanente Bridge Program Application Kaiser Foundation Health Plan of Georgia, Inc. APP/CB-080500 11/08 Instructions ISTRUCTIOS: Please print clearly using a blue or black ink pen. If the question
The Kaiser Permanente Bridge Program Application Kaiser Foundation Health Plan of Georgia, Inc. APP/CB-080500 11/08 Instructions ISTRUCTIOS: Please print clearly using a blue or black ink pen. If the question
Medical Assistance Application for the Elderly and Persons with Disabilities
 Medical Assistance Application for the Elderly and Persons with Disabilities Who can use this application? Apply faster online This application is for the elderly and persons with disabilities applying
Medical Assistance Application for the Elderly and Persons with Disabilities Who can use this application? Apply faster online This application is for the elderly and persons with disabilities applying
APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS
 Capital Advantage Insurance Company Commonwealth of Pennsylvania Edward G. Rendell, Governor APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS Application Information The information
Capital Advantage Insurance Company Commonwealth of Pennsylvania Edward G. Rendell, Governor APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS Application Information The information
You will need to mail or fax us copies of items that apply to your case. See the next page for a list of these items.
 Getting started: Health care for children CHIP and Children s Medicaid These programs offer health-care benefits for newborns and children age 18 and younger who live in Texas. With these programs, your
Getting started: Health care for children CHIP and Children s Medicaid These programs offer health-care benefits for newborns and children age 18 and younger who live in Texas. With these programs, your
APPLICATION COVER LETTER
 APPLICATION COVER LETTER RE: 66 FLATBUSH APTS Dear Prospective Applicant: Enclosed is an application for the above-referenced building, which participates in a governmentally assisted affordable housing
APPLICATION COVER LETTER RE: 66 FLATBUSH APTS Dear Prospective Applicant: Enclosed is an application for the above-referenced building, which participates in a governmentally assisted affordable housing
SAMPLE ONLY. FACTS Grant & Aid Application For the School Year Beginning Fall 2015. Save Time Apply Online.
 10000028406 Save Time Apply Online. Apply online at online.factsmgt.com/aid w available in Spanish. Applying online allows your institution to view your application electronically within minutes of submission.
10000028406 Save Time Apply Online. Apply online at online.factsmgt.com/aid w available in Spanish. Applying online allows your institution to view your application electronically within minutes of submission.
ONLY. FACTS Grant & Aid Application For the School Year Beginning Fall 2014. Save Time Apply Online.
 10000028406 Save Time Apply Online. Apply online at online.factsmgt.com/aid w available in Spanish. Applying online allows your institution to view your application electronically within minutes of submission.
10000028406 Save Time Apply Online. Apply online at online.factsmgt.com/aid w available in Spanish. Applying online allows your institution to view your application electronically within minutes of submission.
TAX DEFERRAL INFORMATION AND INSTRUCTION SHEET
 CECIL COUNTY, MARYLAND OFFICE OF FINANCE 200 CHESAPEAKE BLVD, STE. 1100 ELKTON, MARYLAND 21921 TAX DEFERRAL INFORMATION AND INSTRUCTION SHEET The Annotated Code of Maryland, Tax-Property Article 10-204
CECIL COUNTY, MARYLAND OFFICE OF FINANCE 200 CHESAPEAKE BLVD, STE. 1100 ELKTON, MARYLAND 21921 TAX DEFERRAL INFORMATION AND INSTRUCTION SHEET The Annotated Code of Maryland, Tax-Property Article 10-204
Sample Only. Grant & Aid Application For the School Year Beginning Fall 2012. Save Time Apply Online. Information needed to complete your application:
 10000028406 Save Time Apply Online. Apply online at www.factstuitionaid.com - Applying online is the fastest and most direct method of submitting your application. It allows your institution to view your
10000028406 Save Time Apply Online. Apply online at www.factstuitionaid.com - Applying online is the fastest and most direct method of submitting your application. It allows your institution to view your
FOLLOW STEPS 1 6 TO COMPLETE the Sandy B. Muller Breast Cancer Foundation Application
 Application Directions and Checklist Please Read Carefully Please be sure to provide all the information requested here. An incomplete application will delay our ability to provide you with assistance.
Application Directions and Checklist Please Read Carefully Please be sure to provide all the information requested here. An incomplete application will delay our ability to provide you with assistance.
2015-2016 Dependent Verification
 V6- DEP FORM 2015-2016 Dependent Verification Your 2015-2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. Northern must compare information
V6- DEP FORM 2015-2016 Dependent Verification Your 2015-2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called verification. Northern must compare information
MARYLAND SENIOR PRESCRIPTION DRUG ASSISTANCE PROGRAM ENROLLMENT APPLICATION
 MARYLAND SENIOR PRESCRIPTION DRUG ASSISTANCE PROGRAM ENROLLMENT APPLICATION Dear Applicant: The Maryland Senior Prescription Drug Assistance Program (SPDAP) is pleased to provide you with the enclosed
MARYLAND SENIOR PRESCRIPTION DRUG ASSISTANCE PROGRAM ENROLLMENT APPLICATION Dear Applicant: The Maryland Senior Prescription Drug Assistance Program (SPDAP) is pleased to provide you with the enclosed
MEDICAL ASSISTANCE (MEDICAID) FINANCIAL ELIGIBILITY APPLICATION
 FINANCIAL ELIGIBILITY APPLICATION") COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE MEDICAL ASSISTANCE (MEDICAID) FINANCIAL ELIGIBILITY APPLICATION FOR LONG TERM CARE, SUPPORTS AND SERVICES You may also apply online at www.compass.state.pa.us
COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE MEDICAL ASSISTANCE (MEDICAID) FINANCIAL ELIGIBILITY APPLICATION FOR LONG TERM CARE, SUPPORTS AND SERVICES You may also apply online at www.compass.state.pa.us
How to Apply To complete your application, here s what you need to do:
 What is Kern Medical Center Health Plan (KMCHP)? KMCHP is a county and federally-funded program that provides medical care to some people living in Kern County. It s a new way for Kern residents who meet
What is Kern Medical Center Health Plan (KMCHP)? KMCHP is a county and federally-funded program that provides medical care to some people living in Kern County. It s a new way for Kern residents who meet
INSTRUCTIONS FOR COMPLETING THE APPLICATION FOR PARTICIPATION IN THE ADDP AND/OR HICP PROGRAM
 New Jersey Department of Health AIDS Drug Distribution Program (ADDP) and Health Insurance Continuation Program (HICP) PO Box 722 Trenton, NJ 08625-0722 INSTRUCTIONS FOR COMPLETING THE APPLICATION FOR
New Jersey Department of Health AIDS Drug Distribution Program (ADDP) and Health Insurance Continuation Program (HICP) PO Box 722 Trenton, NJ 08625-0722 INSTRUCTIONS FOR COMPLETING THE APPLICATION FOR
Application for Adults and Children with Long Term Care Needs
 State of Alaska Department of Health and Social Services Division of Public Assistance Application for Adults and Children with Long Term Care Needs Please check the services you need: Home and Community-Based
State of Alaska Department of Health and Social Services Division of Public Assistance Application for Adults and Children with Long Term Care Needs Please check the services you need: Home and Community-Based
Important! How the Affordable Care Program works
 Important! How the Affordable Care Program works What is the Affordable Care Program? The Program allows us to offer patients a sliding fee scale, depending on household income. You share the costs of
Important! How the Affordable Care Program works What is the Affordable Care Program? The Program allows us to offer patients a sliding fee scale, depending on household income. You share the costs of
South Carolina Medicaid Program Annual Review Form
 Date: BG #: HH #: Case Name: South Carolina Medicaid Program Annual Review Form This form is used to review your Medicaid coverage. You must return this form to us by: Return to: Healthy Connections, PO
Date: BG #: HH #: Case Name: South Carolina Medicaid Program Annual Review Form This form is used to review your Medicaid coverage. You must return this form to us by: Return to: Healthy Connections, PO
Individual Enrollment Request Form
 Individual Enrollment Request Form 3800 Kilroy Airport Way, Suite 100 Long Beach, CA 90806 Please contact VillageHealth if you need information in another language or format (Braille). To enroll in VillageHealth,
Individual Enrollment Request Form 3800 Kilroy Airport Way, Suite 100 Long Beach, CA 90806 Please contact VillageHealth if you need information in another language or format (Braille). To enroll in VillageHealth,
Application for Medical Assistance for Families with Children
 Application for Medical Assistance for Families with Children Who can use this application? Use this application to see what choices you have Apply faster online This application is for families, children,
Application for Medical Assistance for Families with Children Who can use this application? Use this application to see what choices you have Apply faster online This application is for families, children,
Massachusetts Application for Health and Dental Coverage and Help Paying Costs
 Massachusetts Application for Health and Dental Coverage and Help Paying Costs THINGS TO KNOW HOW TO APPLY Use this application to see what coverage choices you may qualify for. Who can use this application?
Massachusetts Application for Health and Dental Coverage and Help Paying Costs THINGS TO KNOW HOW TO APPLY Use this application to see what coverage choices you may qualify for. Who can use this application?
I have received a copy of the Notice of Privacy Practices True Health.
 Sign-in Time: I have received a copy of the Notice of Privacy Practices True Health. Signature of Patient/Patient Representative Relationship of Patient Representative to Patient 2400 State Road 415 11881-A
Sign-in Time: I have received a copy of the Notice of Privacy Practices True Health. Signature of Patient/Patient Representative Relationship of Patient Representative to Patient 2400 State Road 415 11881-A
450-458 Gouverneur Place Apartments WESTHAB, INC. (Property Management) 8 BASHFORD ST, YONKERS, N.Y. 10701 HOUSING APPLICATION
 8 BASHFORD ST, YONKERS, N.Y. 10701 HOUSING APPLICATION") Mail to: 450-458 Gouverneur Place Apartments WESTHAB, INC. (Property Management) 8 BASHFORD ST, YONKERS, N.Y. 10701 HOUSING APPLICATION Agency Use Only Date Received Application # Approved YES NO 1) LAST
Mail to: 450-458 Gouverneur Place Apartments WESTHAB, INC. (Property Management) 8 BASHFORD ST, YONKERS, N.Y. 10701 HOUSING APPLICATION Agency Use Only Date Received Application # Approved YES NO 1) LAST
Health Care Coverage APPLICATION FOR. Health Care in Pennsylvania. Easy, affordable protection for your family
 Important information about health care benefits. Ask someone to read this to you. APPLICATION FOR Health Care Coverage This application may be used by families with children or by pregnant women who apply
Important information about health care benefits. Ask someone to read this to you. APPLICATION FOR Health Care Coverage This application may be used by families with children or by pregnant women who apply
Health Insurance for Illinois Families. Rod R. Blagojevich, Governor
 Health Insurance for Illinois Families Rod R. Blagojevich, Governor KC 2378KC (R-3-04) IL478-2437 KidCare and FamilyCare Plans KidCare and FamilyCare are health insurance plans for Illinois residents.
Health Insurance for Illinois Families Rod R. Blagojevich, Governor KC 2378KC (R-3-04) IL478-2437 KidCare and FamilyCare Plans KidCare and FamilyCare are health insurance plans for Illinois residents.
Healthy Kids Annual Renewal Application
 Healthy Kids Annual Renewal Application Application Due By: It is time to renew your Healthy Kids health care coverage. If you would like it in another language, please call (415) 777-9992. It is time
Healthy Kids Annual Renewal Application Application Due By: It is time to renew your Healthy Kids health care coverage. If you would like it in another language, please call (415) 777-9992. It is time
Monday between 1:00 pm - 4:00pm
 Attention: Tempe and ountain Hills Residents UTILITY ASSISTANCE PROCESS Income eligible Tempe and ountain Hills residents can apply for financial help with electricity, including M-Power and gas bills.
Attention: Tempe and ountain Hills Residents UTILITY ASSISTANCE PROCESS Income eligible Tempe and ountain Hills residents can apply for financial help with electricity, including M-Power and gas bills.
Financial Assistance
 Financial Assistance Process & Application The Ochsner Health System ( OHS ) is committed to providing financial assistance for patients with a demonstrated financial need or hardship, who have received
Financial Assistance Process & Application The Ochsner Health System ( OHS ) is committed to providing financial assistance for patients with a demonstrated financial need or hardship, who have received
INSURANCE ASSISTANCE PROGRAM (IAP) Michigan Department of Human Services
 Michigan Department of Human Services") INSURANCE ASSISTANCE PROGRAM (IAP) Dear Applicant: Thank you for your interest in the Insurance Assistance Program (IAP). This program was developed to assist individuals to maintain and continue their
INSURANCE ASSISTANCE PROGRAM (IAP) Dear Applicant: Thank you for your interest in the Insurance Assistance Program (IAP). This program was developed to assist individuals to maintain and continue their
V6-Independent Student
 2015 2016 Household Resources Verification Worksheet V6-Independent Student Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called Verification. The
2015 2016 Household Resources Verification Worksheet V6-Independent Student Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called Verification. The
Instructions for Completing a Medicare Savings Program (MSP) Application
 Application") Instructions for Completing a Medicare Savings Program (MSP) Application The attached Department of Human Services (DHS) Health Services Application is used to apply for Medicare Savings Programs (MSP)
Instructions for Completing a Medicare Savings Program (MSP) Application The attached Department of Human Services (DHS) Health Services Application is used to apply for Medicare Savings Programs (MSP)
You may go to any medical provider who accepts payment from the Department of Public Aid.
 Illinois Department of Human Services Illinois Department of Public Aid Mail-In Application for Medical Benefits (Esta solicitud está disponible en español.) (This application is available in Spanish.)
Illinois Department of Human Services Illinois Department of Public Aid Mail-In Application for Medical Benefits (Esta solicitud está disponible en español.) (This application is available in Spanish.)
APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS
 APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS 1. Please read the enclosed brochure for important information. 2. You may use this application to apply for Special Care for adults
APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS 1. Please read the enclosed brochure for important information. 2. You may use this application to apply for Special Care for adults
Thank you for requesting an application for an apartment. Enclosed, please find an application package.
 Dear Applicant, Thank you for requesting an application for an apartment. Enclosed, please find an application package. Please read the application carefully, complete every section, and date where indicated.
Dear Applicant, Thank you for requesting an application for an apartment. Enclosed, please find an application package. Please read the application carefully, complete every section, and date where indicated.
One Affordable Homeownership Unit - Adaptable Unit with Accessible Features
 One Affordable Homeownership Unit - Adaptable Unit with Accessible Features Located at 100 Pacific Street near Central Square, this unit will be available, through the City s Inclusionary Housing Program,
One Affordable Homeownership Unit - Adaptable Unit with Accessible Features Located at 100 Pacific Street near Central Square, this unit will be available, through the City s Inclusionary Housing Program,
COLORADO HEALTH CARE COVERAGE
 COLORADO HEALTH CARE COVERAGE Colorado Department of Health Care Policy and Financing administers a variety of Medical Assistance Programs for qualifying persons who live in Colorado and meet eligibility
COLORADO HEALTH CARE COVERAGE Colorado Department of Health Care Policy and Financing administers a variety of Medical Assistance Programs for qualifying persons who live in Colorado and meet eligibility
Child Care Assistance Application Checklist
 State of Alaska Department of Health and Social Services Division of Public Assistance Child Care Program Office http://www.hss.state.ak.us/dpa/programs/ccare/ Child Care Assistance Application Checklist
State of Alaska Department of Health and Social Services Division of Public Assistance Child Care Program Office http://www.hss.state.ak.us/dpa/programs/ccare/ Child Care Assistance Application Checklist
Lee County Central Point of Coordination Application Return Application Requested By: HIPPA Yes NO. Date of Application: / / Phone: #( )- -
- -") Lee County Central Point of Coordination Application Return Application Requested By:_ HIPPA Yes NO Date of Application: / /Phone: #()-- Name of Applicant: Last First M.I. Current Address: City State Zip
Lee County Central Point of Coordination Application Return Application Requested By:_ HIPPA Yes NO Date of Application: / /Phone: #()-- Name of Applicant: Last First M.I. Current Address: City State Zip
ARIZONA DEPARTMENT OF ECONOMIC SECURITY Child Care Administration APPLICATION FOR CHILD CARE ASSISTANCE
 CC-001 (7-11) PAGE 1 ARIZONA DEPARTMENT OF ECONOMIC SECURITY Child Care Administration APPLICATION FOR CHILD CARE ASSISTANCE RECEIVED INITIAL APPLICATION AND REQUEST REAPPLICATION To apply for benefits,
CC-001 (7-11) PAGE 1 ARIZONA DEPARTMENT OF ECONOMIC SECURITY Child Care Administration APPLICATION FOR CHILD CARE ASSISTANCE RECEIVED INITIAL APPLICATION AND REQUEST REAPPLICATION To apply for benefits,
Individual HealthPartners Wisconsin Freedom Plan (Cost) Enrollment Form
 Enrollment Form") Individual HealthPartners Wisconsin Freedom Plan (Cost) Enrollment Form This is the enrollment application for your HealthPartners Wisconsin Freedom plan (Cost) medical and prescription drug options. Follow
Individual HealthPartners Wisconsin Freedom Plan (Cost) Enrollment Form This is the enrollment application for your HealthPartners Wisconsin Freedom plan (Cost) medical and prescription drug options. Follow
City of Victorville Mortgage Assistance Program Application (80% AMI)
") City of Victorville Mortgage Assistance Program Application (80% AMI) Congratulations on taking steps towards homeownership. The City of Victorville, through its Mortgage Assistance Program, offers up
City of Victorville Mortgage Assistance Program Application (80% AMI) Congratulations on taking steps towards homeownership. The City of Victorville, through its Mortgage Assistance Program, offers up
Housing & Human Services Department Community Acton Agency 400 South Varr Avenue Telephone: (321) 633-1951 Cocoa, Florida 32922 Fax: (321) 633-1958
 633-1951 Cocoa, Florida 32922 Fax: (321) 633-1958") Housing & Human Services Department Community Acton Agency 400 South Varr Avenue Telephone: (321) 633-1951 Cocoa, Florida 32922 Fax: (321) 633-1958 Thank you for your interest in the Brevard County Low
Housing & Human Services Department Community Acton Agency 400 South Varr Avenue Telephone: (321) 633-1951 Cocoa, Florida 32922 Fax: (321) 633-1958 Thank you for your interest in the Brevard County Low
STUDENT INFORMATION FAMILY INFORMATION
 Your 2015-2016 Free Application for Federal Student Aid (FAFSA) was selected by the U.S. Department of Education for a review process called Verification. In this process, we are required by federal regulations
Your 2015-2016 Free Application for Federal Student Aid (FAFSA) was selected by the U.S. Department of Education for a review process called Verification. In this process, we are required by federal regulations
Carroll College Matched Education Savings Account Application
 PERSONAL INFORMATION Name: Social Sec. No. (last four digits): Gender: Female Male Date of Birth: / / Ethnicity: African American Caucasian Latino or Hispanic Asian, Pacific Islander Native American Other
PERSONAL INFORMATION Name: Social Sec. No. (last four digits): Gender: Female Male Date of Birth: / / Ethnicity: African American Caucasian Latino or Hispanic Asian, Pacific Islander Native American Other
Application for Free Home Repairs
 Application for Free Home Repairs Name of Homeowner: Date of Birth: Gender Male Female Is this a female headed household? Is this a grandparent headed household? Street Address: City: County: Zip Marital
Application for Free Home Repairs Name of Homeowner: Date of Birth: Gender Male Female Is this a female headed household? Is this a grandparent headed household? Street Address: City: County: Zip Marital
2015-2016 Independent Verification
 V6- IND FORM 2015-2016 Independent Verification Your 2015-2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called Aggregate Verification. Northern is required
V6- IND FORM 2015-2016 Independent Verification Your 2015-2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called Aggregate Verification. Northern is required
Application & Renewal Form
 Section A: I want health insurance for: (Check ( ) the category or categories that match your situation.) Myself, my spouse (or other parent of my children) and our children under age 19 who live with
Section A: I want health insurance for: (Check ( ) the category or categories that match your situation.) Myself, my spouse (or other parent of my children) and our children under age 19 who live with
Renewal Form. www.upmchealthplan.com/upmcforkids
 Renewal Form www.upmchealthplan.com/upmcforkids There are three easy ways to renew CHIP coverage! To keep CHIP coverage, you can: 1. RENEW ONLINE USING COMPASS: (If you apply online, most of your information
Renewal Form www.upmchealthplan.com/upmcforkids There are three easy ways to renew CHIP coverage! To keep CHIP coverage, you can: 1. RENEW ONLINE USING COMPASS: (If you apply online, most of your information
It is our mission to provide excellence in quality and service
 It is our mission to provide excellence in quality and service Date: Patient Name: MRN: For your convenience, enclosed is a Financial Assistance Application. The application is for bills acquired for services
It is our mission to provide excellence in quality and service Date: Patient Name: MRN: For your convenience, enclosed is a Financial Assistance Application. The application is for bills acquired for services
Effective Date: 7/10/2015. Title: Financial Assistance Policy. Document Owner: Jonathan Binder Approver(s):Professional Advisory Group
:Professional Advisory Group") Title: Financial Assistance Policy Document Owner: Jonathan Binder Approver(s):Professional Advisory Group Effective Date: 7/10/2015 I. Policy: It is the policy of HomeCare Maryland (HCM) to adhere to
Title: Financial Assistance Policy Document Owner: Jonathan Binder Approver(s):Professional Advisory Group Effective Date: 7/10/2015 I. Policy: It is the policy of HomeCare Maryland (HCM) to adhere to
Memorial Hermann Advantage (HMO)
") Memorial Hermann Advantage (HMO) 2016 Enrollment Form Follow these easy steps to enroll in a Memorial Hermann Advantage Health Maintenance Organization (HMO). 1. Each applicant must fill out a separate
Memorial Hermann Advantage (HMO) 2016 Enrollment Form Follow these easy steps to enroll in a Memorial Hermann Advantage Health Maintenance Organization (HMO). 1. Each applicant must fill out a separate
MANUAL: TCH POLICY NO: GA303-01 SECTION: General and Administrative PROC. NO: GA303-01 TITLE: FINANCIAL ASSISTANCE/
 TEXAS CHILDREN S HOSPITAL POLICY & PROCEDURE MANUAL: TCH POLICY NO: GA303-01 SECTION: General and Administrative PROC. NO: GA303-01 TITLE: FINANCIAL ASSISTANCE/ ORIG. DATE: 01/05/89 CHARITY CARE POLICY
TEXAS CHILDREN S HOSPITAL POLICY & PROCEDURE MANUAL: TCH POLICY NO: GA303-01 SECTION: General and Administrative PROC. NO: GA303-01 TITLE: FINANCIAL ASSISTANCE/ ORIG. DATE: 01/05/89 CHARITY CARE POLICY
CHIP Health Insurance Renewal Form
 CHIP Health Insurance Renewal Form 1. Household Information. First: MI: Last: Suffix: Head of Household : Street: Apt #: Address: Phone: City: State: Zip: Email: Primary: Alternate: Best time to call:
CHIP Health Insurance Renewal Form 1. Household Information. First: MI: Last: Suffix: Head of Household : Street: Apt #: Address: Phone: City: State: Zip: Email: Primary: Alternate: Best time to call:
Start here Tear and separate pages along the perforated edge before completing
 Start here Tear and separate pages along the perforated edge before completing Medicare Plus (Cost) INDIVIDUAL ENROLLMENT REQUEST FORM INSTRUCTIONS Kaiser Foundation Health Plan of the Mid-Atlantic States,
Start here Tear and separate pages along the perforated edge before completing Medicare Plus (Cost) INDIVIDUAL ENROLLMENT REQUEST FORM INSTRUCTIONS Kaiser Foundation Health Plan of the Mid-Atlantic States,
MEMBER S NAME (LAST, FIRST, M.I.) MEMBER ID OR SSN PHONE NUMBER ( ) PHYSICAL ADDRESS (CANNOT BE A PO BOX) COUNTY OF RESIDENCE EMAIL ADDRESS
 MEMBER ID OR SSN PHONE NUMBER ( ) PHYSICAL ADDRESS (CANNOT BE A PO BOX) COUNTY OF RESIDENCE EMAIL ADDRESS") Department of Technology, Management & Budget Office of Retirement Services www.michigan.gov/ors (800) 381-5111 P.O. Box 30171 Lansing, MI 48909-7671 Insurance Enrollment/Change Request MEMBER S NAME (LAST,
Department of Technology, Management & Budget Office of Retirement Services www.michigan.gov/ors (800) 381-5111 P.O. Box 30171 Lansing, MI 48909-7671 Insurance Enrollment/Change Request MEMBER S NAME (LAST,
New York Lifeline Application
 New York Lifeline is a government program that provides a monthly discount on home or mobile telephone services. Only ONE Lifeline discount is allowed per household. Members of a household are not permitted
New York Lifeline is a government program that provides a monthly discount on home or mobile telephone services. Only ONE Lifeline discount is allowed per household. Members of a household are not permitted
Application for Health Coverage Assistance
 Application for Health Coverage Assistance Health Coverage Assistance The Health Coverage Assistance Program provides health coverage assistance according to individual needs. Eligible families may qualify
Application for Health Coverage Assistance Health Coverage Assistance The Health Coverage Assistance Program provides health coverage assistance according to individual needs. Eligible families may qualify
We Do Business in Accordance to the Federal Fair Housing Law
 PLEASE COMPLETE IN FULL Housing Authority of the City of Fort Myers Public Housing Application SOUTHWARD VILLAGE APTS. 3040 Franklin Street, Fort Myers, FL 33916 Telephone (239) 332-6635 Fax (239) 344-3273
PLEASE COMPLETE IN FULL Housing Authority of the City of Fort Myers Public Housing Application SOUTHWARD VILLAGE APTS. 3040 Franklin Street, Fort Myers, FL 33916 Telephone (239) 332-6635 Fax (239) 344-3273
HURRICANE IKE INTAKE APPLICATION
 HURRICANE IKE INTAKE APPLICATION INSTRUCTIONS FOR APPLICATION STEP 1: Read the instructions for this application and the Frequently Asked Questions (FAQ). They contain important information about documents
HURRICANE IKE INTAKE APPLICATION INSTRUCTIONS FOR APPLICATION STEP 1: Read the instructions for this application and the Frequently Asked Questions (FAQ). They contain important information about documents
APPLICATION COVER LETTER
 APPLICATION COVER LETTER RE: BAM SOUTH APTS Dear Prospective Applicant: Enclosed is an application for the above-referenced building, which participates in a governmentally assisted affordable housing
APPLICATION COVER LETTER RE: BAM SOUTH APTS Dear Prospective Applicant: Enclosed is an application for the above-referenced building, which participates in a governmentally assisted affordable housing
Williamson Medical Center Charitable Care, Prompt Payment, Uninsured/Underinsured Discount Policy
 Williamson Medical Center Charitable Care, Prompt Payment, Uninsured/Underinsured Discount Policy Effective January 1, 2013 1. Policy: Williamson Medical Center is committed to provide high quality patient
Williamson Medical Center Charitable Care, Prompt Payment, Uninsured/Underinsured Discount Policy Effective January 1, 2013 1. Policy: Williamson Medical Center is committed to provide high quality patient
NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM APPLICATION FOR PARTICIPATION
 NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM APPLICATION FOR PARTICIPATION Dear Applicants: To participate in the New Jersey Hospital Care Assistance program, you will need to fill out an application form
NEW JERSEY HOSPITAL CARE ASSISTANCE PROGRAM APPLICATION FOR PARTICIPATION Dear Applicants: To participate in the New Jersey Hospital Care Assistance program, you will need to fill out an application form
Patient Financial Assistance Program
 PO Box 1810, Burlington, Vermont 05402 802-847-8000, 800-639-2719 Fax: 802-847-7618 customerservice@uvmhealth.org Dear Applicant, Thank you for choosing The University of Vermont Medical Center as your
PO Box 1810, Burlington, Vermont 05402 802-847-8000, 800-639-2719 Fax: 802-847-7618 customerservice@uvmhealth.org Dear Applicant, Thank you for choosing The University of Vermont Medical Center as your
APPLICATION FOR APARTMENT
 APPLICATION FOR APARTMENT INSTRUCTIONS: 1. SUBMIT ONLY ONE APPLICATION PER HOUSEHOLD. Applications are selected randomly through a lottery. You will be disqualified if more than one application is received
APPLICATION FOR APARTMENT INSTRUCTIONS: 1. SUBMIT ONLY ONE APPLICATION PER HOUSEHOLD. Applications are selected randomly through a lottery. You will be disqualified if more than one application is received
Date Received: Time Received: Application taken by:
 Received: Time Received: Application taken by: APPLICATION FOR HOUSING Low-Income Housing Tax Credit Property This is an application for housing at: Whitney Young Manor, LP 358 Nepperhan Avenue, Management
Received: Time Received: Application taken by: APPLICATION FOR HOUSING Low-Income Housing Tax Credit Property This is an application for housing at: Whitney Young Manor, LP 358 Nepperhan Avenue, Management
Aquinas Institute of Rochester
 Aquinas Institute of Rochester 2015-2016 STUDENT FINANCIAL AID APPLICATION Information needed to complete your application: * Copies of your complete 2014 IRS Federal Form 1040, 1040A or 1040 EZ U.S. Individual
Aquinas Institute of Rochester 2015-2016 STUDENT FINANCIAL AID APPLICATION Information needed to complete your application: * Copies of your complete 2014 IRS Federal Form 1040, 1040A or 1040 EZ U.S. Individual
Application for Vocational Rehabilitation Services
 Strong Families Make a Strong Kansas Application for Vocational Rehabilitation Services Is Vocational Rehabilitation the right program for you? Some brief information about the Vocational Rehabilitation
Strong Families Make a Strong Kansas Application for Vocational Rehabilitation Services Is Vocational Rehabilitation the right program for you? Some brief information about the Vocational Rehabilitation
SUBJECT: CHARITY AND UNCOMPENSATED CARE 1 of 13 DEPARTMENT: BUSINESS OFFICE REVISED: 10/2012
 REFERENCE # SUBJECT: CHARITY AND UNCOMPENSATED CARE 1 of 13 DEPARTMENT: BUSINESS OFFICE REVISED: 10/2012 CHARITY AND UNCOMPENSATED CARE Purpose To provide definition of health care assistance to eligible
REFERENCE # SUBJECT: CHARITY AND UNCOMPENSATED CARE 1 of 13 DEPARTMENT: BUSINESS OFFICE REVISED: 10/2012 CHARITY AND UNCOMPENSATED CARE Purpose To provide definition of health care assistance to eligible
First-Time Homebuyers Training Assistance Program Application
 Dear Prospective First Time Home Buyer: Thank you for your recent inquiry regarding the City of Kenner Department of Community Development s First Time Home Buyers Training Assistance Program. The purpose
Dear Prospective First Time Home Buyer: Thank you for your recent inquiry regarding the City of Kenner Department of Community Development s First Time Home Buyers Training Assistance Program. The purpose
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services
 Financial Eligibility Application for Long Term Care, Supports and Services") Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
Medical Assistance (Medicaid) Financial Eligibility Application for Long Term Care, Supports and Services You may also apply online at www.compass.state.pa.us Check any that you are applying for: Care
Health Coverage & Help Paying Costs Application for One Person
 THINGS TO KNOW Health Coverage & Help Paying Costs Application for One Person Use this application to see what insurance choices you qualify for Free or low-cost insurance from Medicaid or the Kentucky
THINGS TO KNOW Health Coverage & Help Paying Costs Application for One Person Use this application to see what insurance choices you qualify for Free or low-cost insurance from Medicaid or the Kentucky
Hallandale Beach Community Redevelopment Agency First Time Homebuyers Program
 Hallandale Beach Community Redevelopment Agency First Time Homebuyers Program Program Overview Under the First Time Homebuyer Program, the Hallandale Beach CRA will provide up to $50,000 in assistance
Hallandale Beach Community Redevelopment Agency First Time Homebuyers Program Program Overview Under the First Time Homebuyer Program, the Hallandale Beach CRA will provide up to $50,000 in assistance
2015 2016 Household Resources Verification Worksheet. V6-Dependent Student
 2015 2016 Household Resources Verification Worksheet V6-Dependent Student Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called Verification. The Financial
2015 2016 Household Resources Verification Worksheet V6-Dependent Student Your 2015 2016 Free Application for Federal Student Aid (FAFSA) was selected for review in a process called Verification. The Financial
Pre-Application for Waiting List Section 8 Housing Choice Voucher (HCV) Program
 Program") Pre-Application for Waiting List Section 8 Housing Choice Voucher (HCV) Program Please designate which county you are applying for (can change county when pulled from the waiting list): Clatsop County
Pre-Application for Waiting List Section 8 Housing Choice Voucher (HCV) Program Please designate which county you are applying for (can change county when pulled from the waiting list): Clatsop County
Application for Request for a Tax Payment Plan and Your Responsibilities
 Application for Request for a Tax Plan and Your Responsibilities Attached you will find an application for requesting a Tax Plan from the New Durham Board of Selectmen. Please fully complete the application.
Application for Request for a Tax Plan and Your Responsibilities Attached you will find an application for requesting a Tax Plan from the New Durham Board of Selectmen. Please fully complete the application.
Bridge Closing Cost Assistance Loan Program Application
 Bridge Closing Cost Assistance Loan Program Application Congratulations on taking the steps towards Bridging" the Gap to Sustainable Homeownership. NPHS, through its partnership with the High Desert Association
Bridge Closing Cost Assistance Loan Program Application Congratulations on taking the steps towards Bridging" the Gap to Sustainable Homeownership. NPHS, through its partnership with the High Desert Association
ENROLLMENT APPLICATION. Vista Healthplan Of. Vista South Florida
 2009 ENROLLMENT APPLICATION Vista Healthplan Of South Florida, Inc. Vista South Florida Individual Enrollment Request Form To Enroll in Vista Healthplan of South Florida, Inc., Please Provide the Following
2009 ENROLLMENT APPLICATION Vista Healthplan Of South Florida, Inc. Vista South Florida Individual Enrollment Request Form To Enroll in Vista Healthplan of South Florida, Inc., Please Provide the Following
Please complete the 2010 Enrollment Form and return to:
 Please complete the 2010 Enrollment Form and return to: WellCare Health Plan P.O. Box 69339 Harrisburg, PA 17106-9339 If you have any questions, please contact Customer Service at 1-866-765-4385 (TTY users
Please complete the 2010 Enrollment Form and return to: WellCare Health Plan P.O. Box 69339 Harrisburg, PA 17106-9339 If you have any questions, please contact Customer Service at 1-866-765-4385 (TTY users
Who you are Where you live How you have been living How we can help you
 PUB-1301 Statewide (Rev. 1/05) PAGE 1 NEW YORK STATE HOW TO COMPLETE THE TEMPORARY ASSISTANCE (TA) - MEDICAL ASSISTANCE (MA) - MEDICARE SAVINGS PROGRAM (MSP) - FOOD STAMP BENEFITS (FS) - SERVICES (S),
PUB-1301 Statewide (Rev. 1/05) PAGE 1 NEW YORK STATE HOW TO COMPLETE THE TEMPORARY ASSISTANCE (TA) - MEDICAL ASSISTANCE (MA) - MEDICARE SAVINGS PROGRAM (MSP) - FOOD STAMP BENEFITS (FS) - SERVICES (S),
UPMC Financial Assistance Application Information
 UPMC Financial Assistance Application Information UPMC offers financial assistance for medical care provided by UPMC facilities and UPMC affiliated physicians to eligible individuals and families. Based
UPMC Financial Assistance Application Information UPMC offers financial assistance for medical care provided by UPMC facilities and UPMC affiliated physicians to eligible individuals and families. Based
Application for Medicaid
 Application for Medicaid N.C. Department of Health and Human Services This application is intended for medical assistance for the Aged, Blind and Disabled or those who want Family Planning services. A
Application for Medicaid N.C. Department of Health and Human Services This application is intended for medical assistance for the Aged, Blind and Disabled or those who want Family Planning services. A
Patient Financial Assistance Application Madison Valley Medical Center and Rural Health Clinic
 Patient Financial Assistance Application Madison Valley Medical Center and Rural Health Clinic Madison Valley Medical Center and Rural Health Clinic (MVMC) provides, within the limits of its resources,
Patient Financial Assistance Application Madison Valley Medical Center and Rural Health Clinic Madison Valley Medical Center and Rural Health Clinic (MVMC) provides, within the limits of its resources,
Please submit all of the above forms via one of the following options:
 Dear Applicant(s): Thank you for applying for a Home Equity Loan with Investors Bank. In order to begin the application process, please complete the paperwork within this Application Packet: 1. ECOA Notice
Dear Applicant(s): Thank you for applying for a Home Equity Loan with Investors Bank. In order to begin the application process, please complete the paperwork within this Application Packet: 1. ECOA Notice
Healthy Smiles Ontario Program Application Form A
 Ministry of Health and Long-Term Care Healthy Smiles Ontario Program Application Form A Program Information The Healthy Smiles Ontario Program is an Ontario government-funded basic dental program providing
Ministry of Health and Long-Term Care Healthy Smiles Ontario Program Application Form A Program Information The Healthy Smiles Ontario Program is an Ontario government-funded basic dental program providing
NOTICE OF DIRECT CERTIFICATION
 East Catholic School 2001 Ardmore Blvd. Pittsburgh, PA 15221 Phone: 412/351-5403 Fax: 412/273-9114 www.eastcatholicschool.org Dear Parent/Guardian: Children need healthy meals to learn. East Catholic School
East Catholic School 2001 Ardmore Blvd. Pittsburgh, PA 15221 Phone: 412/351-5403 Fax: 412/273-9114 www.eastcatholicschool.org Dear Parent/Guardian: Children need healthy meals to learn. East Catholic School
CHARITY CARE APPLICATION REQUIRED DOCUMENTATION CHECK LIST
 CHARITY CARE APPLICATION REQUIRED DOCUMENTATION CHECK LIST Please return the items below if they apply to your situation. Theses items are required to process your application for charity care assistance.
CHARITY CARE APPLICATION REQUIRED DOCUMENTATION CHECK LIST Please return the items below if they apply to your situation. Theses items are required to process your application for charity care assistance.
Rialto Housing Authority Mortgage Assistance Program Application
 Rialto Housing Authority Mortgage Assistance Program Application Congratulations on taking steps towards homeownership. The Rialto Housing Authority, through its Mortgage Assistance Program, offers up
Rialto Housing Authority Mortgage Assistance Program Application Congratulations on taking steps towards homeownership. The Rialto Housing Authority, through its Mortgage Assistance Program, offers up