Essential Evidence Topics January North Dakota Academy of Family Physicians. Big Sky, Montana
|
|
|
- Rafe May
- 8 years ago
- Views:
Transcription
1 Essential Evidence Topics January 2015 North Dakota Academy of Family Physicians Big Sky, Montana Learning Objectives Discuss recent research critical to family physicians for updating their diagnostic and treatment approaches to selected issues in cardiovascular disease, hypertension, diabetes, behavioral health and sports medicine. Objectives for each presentation are listed at the beginning of each talk. Each talk is based on a literature review of recent research studies. Sources include PubMed, InfoPoems and Cochrane systematic reviews. Faculty John Hickner, MD, MSc. is Professor and Head of Family Medicine at the University of Illinois at Chicago and Editor in Chief of the Journal of Family Practice. His research centers on patient safety, especially testing safety and medication safety in primary care practice. After receiving his medical degree from Indiana University School of Medicine, Dr. Hickner completed his residency in family medicine at the Medical University of South Carolina and received a master s degree in Biostatistics and Research Design from the University of Michigan School of Public Health. Gary Ferenchick, MD, MS. is Division Chief, General Internal Medicine, and Professor of Medicine at Michigan State University College of Human Medicine. He earned his master s degree in human nutrition and medical degree from Michigan State University. He completed his residency training in internal medicine at Michigan State University College of Human Medicine. Dr. Ferenchick is a Past- President of the Clerkship Directors in Internal Medicine. His research interest is the interface between medical education and information technology. Both John and Gary have been teaching evidence based medicine for over 20 years. Speaker and Faculty Disclosures John Hickner, MD, MSc disclosed no relevant financial relationship or interest with a proprietary entity producing health care goods or services. Gary Ferenchick, MD disclosed no relevant financial relationship or interest with a proprietary entity producing health care goods or services. Essential Evidence and all content in this handout is copyright by John Wiley and Sons, Inc, This syllabus may not be reproduced without permission from the publisher. 1

2 Information Mastery and Searching for Evidence: Key Points (also see PowerPoint Slides for this presentation) Objectives 1. Learn the importance of patient oriented evidence for interpreting medical studies 2. Learn an efficient way to search PubMed for clinically relevant information Usefulness of medical information = (relevance x validity) / work Relevance is a continuum: Rat studies Surrogates Disease-specific All-cause mortality/qol Validity is a continuum: Case study Case-control Cohort RCT Systematic review Patient oriented evidence: anything that helps patients live a longer or better life. Disease oriented evidence: everything else; surrogate or physiologic markers POEM (Patient Oriented Evidence that Matters): a study that addresses a common or important condition, demonstrates improved patient oriented outcomes, and matters because it would change what we do. Evidence-based sources to explore: Essential Evidence: Clinical Evidence: Cochrane Library: DynaMed: TRIP Database: Bandolier: National Guidelines Clearinghouse: Search hints Use Clinical Queries at the PubMed site Select Narrow filter Use quotes to narrow search to only those words appearing next to each other, i.e. acute bronchitis eliminates acute exacerbation of chronic bronchitis Combination of drug and disease is useful: acute bronchitis azithromycin; infectious mononucleosis corticosteroid; influenza osletamivir Optionally, See all and then add additional limits (English, abstract, human) Use Not terms to exclude groups of articles Then, select Related articles once you have a good hit. 2

3 ANTICOAGULATION UPDATE: 2015 NEW AGENTS Gary Ferenchick MD Objective 1. Understand the evidence behind the FDA approved uses of newer oral anticoagulants (i.e. NOAs) including dabigatran and apixaban and rivaroxaban What is the role of newer anticoagulants in the prevention of thromboembolic disease? Some of the difference between the newer anticoagulants and the older anticoagulants, such as warfarin and heparin, is that the new agents target a single enzyme within the coagulation pathway (e.g. thrombin [aka activated factor IIa] or factor Xa); whereas warfarin inhibits the synthesis of factors II, VII, IX, and X, and heparin increases the activity of antithrombin (AT) which exerts an inhibitory effect on factor Xa, thrombin and other factors. Additionally the newer agents have a more rapid onset of action than warfarin, lack the need for bridging anticoagulation and have fewer dietary and drug restrictions and possess a predictable anticoagulant effect limiting the need for routine monitoring protocols. The development of thrombus is a fast process, taking < 5 minutes from the activation of the clotting cascade to the development of clot. Factor Xa is located at the convergence point of both the intrinsic and extrinsic pathways and has proven to be an effective target for anticoagulation. Note that one molecule of factor Xa catalyzes the formation of ~ 1000 molecules of thrombin. The oral direct Xa inhibitors, rivaroxaban, apixaban and edoxaban, inhibit both free and bound factor Xa, whereas the indirect factor Xa inhibitor is fondaparinux, which is given subcutaneously and acts by enhancing the activity of AT, only inhibits free factor Xa. Am J Emerg Med 2012;30:2046 The direct thrombin inhibitor dabigatran inhibits thrombin (thus preventing fibrin formation) and thrombin-mediated activation of several clotting factors (V, VIII and XI) along with inhibiting thrombin mediated platelet activation. Dabigatran was the first new oral anticoagulant to become available in 50 years and directly inhibits thrombin (see figure). In 2011 the American College of Cardiology and the American Heart Association published an update on the management of patients with atrial fibrillation with a focus on dabigatran. They issued a new recommendation that endorsed dabigatran (with a Class I recommendation, meaning the treatment should be administered) as a useful alternative "... to warfarin for the prevention of stroke and systemic thromboembolism in patients with paroxysmal to permanent AF and risk factors for stroke or systemic embolization who do not have a prosthetic heart valve or hemodynamically significant valve disease, severe renal failure (creatinine clearance <15 ml/min), or advanced liver disease (impaired baseline clotting function)." The recommendation also states that patients already taking warfarin with excellent INR control may have little to gain by switching to dabigatran. (Circulation 2011;123: ) Additionally, as of January of 2014 edoxaban, this directly inhibits factor Xa, is awaiting FDA approval for stroke prophylaxis in patients with atrial fibrillation among other indications. 3

4 As a general rule for patients with non-valvular atrial fibrillation, aspirin in doses mg decreases the combination of CVA, MI and vascular death by about 29% compared to placebo in primary prevention trials; and oral anticoagulants (warfarin) decreases the risk of stroke and other major vascular events by another 33% compared to aspirin, and by about 64% in those with atrial fibrillation and a history of a TIA. Drug Major studies supporting FDA approval FDA approved indications Rivaroxaban (Xarelto) ROCKET AF Treatment non valvular AF EINSTEIN DVT EINSTEIN PE RECORD1-4 Treatment of DVT, PE AND Reduction of the risk of recurrence of DVT and PE Prevention of DVT in patients undergoing knee or hip replacement surgery Apixiban (Eloquiis) ARISTOTLE, AVERROES Treatment of non-valvular atrial fib Dabigitran (Pradaxa) RE-LY Treatment of non valvular as Oct 2010 According to the FDA Specific antidotes or reversal agents for all of the above are not available Note also many other studies from the manufacturers are on-going in an attempt to expand indications for their drugs Note most of these newer anticoagulants have renal cautions; both in initiating the drugs and a caution to Periodically assess renal function Atrial Fibrillation #1: Dabigatran reduces risk of stroke and embolism in patients with AF (RE-LY) Clinical question: Is dabigatran more safe and effective than warfarin for the prevention of complications of atrial fibrillation? Study design: Randomized controlled trial (single-blinded) Setting: Outpatient (any) Synopsis: Dabigatran etexilate is an oral alternative to warfarin that directly inhibits thrombin. In this study, patients were randomized to receive dabigatran 110 mg twice daily, dabigatran 150 mg twice daily, or warfarin targeted to an INR between 2.0 and 3.0. Although patients and physicians were masked to the dose of dabigatran, they were not masked to the choice of dabigatran or warfarin. However, outcome assessors were masked to both, which is more important. The researchers enrolled 18,113 patients, with a mean age of 71 years. Groups were balanced at the start of the study, analysis was by intention to treat, and patients were followed up for a median of 2 years. Only 20 patients were lost to follow-up. In general, clinical outcomes were similar between the 110 mg dose of dabigatran and the warfarin. When compared with warfarin, the 150 mg dose of dabigatran was associated with a lower risk of stroke and death from vascular causes, but a slightly higher risk of myocardial infarction. Major bleeding was less common with the 110 mg dose than with warfarin (but not with the 150 mg dose). On balance, the net benefit was similar between the 2 doses of dabigatran; the lower risk of ischemia with the higher dose was balanced by a lower risk of bleeding with the higher dose. All-cause mortality was 3.75% in the 110 mg dose group, 3.64% in the 150 mg dose group, and 4.13% in the warfarin group. The comparison between dabigatran 150 mg and warfarin was of borderline statistical significance (P =.051, NNT = 200 for 2 years). Using the CHADS score as a measure of risk of stroke, only patients with a score of 3 or higher benefited from the lower dose, while all patients benefited from the higher dose. Bottom line: Dabigatran was slightly more effective than warfarin at preventing stroke and embolism, especially the dosage of 150 mg given twice daily, and may reduce all-cause mortality (number needed to treat [NNT] = 200 over 2 years). It will be important to balance efficacy with the higher cost but greater convenience of dabigatran when comparing it with standard warfarin therapy. Reference: Connolly SJ, Ezekowitz MD, Yusuf S, et al, for the RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361(12): #2: Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. (ROCKET AF) 4
 ROCKET AF Treatment non valvular AF EINSTEIN DVT EINSTEIN PE RECORD1-4 Treatment of DVT, PE AND Reduction of")
5 BACKGROUND: The use of warfarin reduces the rate of ischemic stroke in patients with atrial fibrillation but requires frequent monitoring and dose adjustment. Rivaroxaban, an oral factor Xa inhibitor, may provide more consistent and predictable anticoagulation than warfarin. METHODS: In a double-blind trial, we randomly assigned 14,264 patients with nonvalvular atrial fibrillation who were at increased risk for stroke to receive either rivaroxaban (at a daily dose of 20 mg) or dose-adjusted warfarin. The per-protocol, as-treated primary analysis was designed to determine whether rivaroxaban was noninferior to warfarin for the primary end point of stroke or systemic embolism. RESULTS: In the primary analysis, the primary end point occurred in 188 patients in the rivaroxaban group (1.7% per year) and in 241 in the warfarin group (2.2% per year) (hazard ratio in the rivaroxaban group, 0.79; 95% confidence interval [CI], 0.66 to 0.96; P<0.001 for noninferiority). In the intention-to-treat analysis, the primary end point occurred in 269 patients in the rivaroxaban group (2.1% per year) and in 306 patients in the warfarin group (2.4% per year) (hazard ratio, 0.88; 95% CI, 0.74 to 1.03; P<0.001 for noninferiority; P=0.12 for superiority). Major and nonmajor clinically relevant bleeding occurred in 1475 patients in the rivaroxaban group (14.9% per year) and in 1449 in the warfarin group (14.5% per year) (hazard ratio, 1.03; 95% CI, 0.96 to 1.11; P=0.44), with significant reductions in intracranial hemorrhage (0.5% vs. 0.7%, P=0.02) and fatal bleeding (0.2% vs. 0.5%, P=0.003) in the rivaroxaban group. CONCLUSIONS: In patients with atrial fibrillation, rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolism. There was no significant between-group difference in the risk of major bleeding, although intracranial and fatal bleeding occurred less frequently in the rivaroxaban group. (Funded by Johnson & Johnson and Bayer; ROCKET AF ClinicalTrials.gov.number, NCT ). Reference: Patel MR, Mahaffey KW, Garg J, Pan G, et al. ROCKET AF Investigators. N Engl J Med Sep 8;365(10): doi: /NEJMoa #3: Apixaban slightly more effective and safe than warfarin, but more expensive (ARISTOTLE) Clinical question: Is apixaban safer and more effective than warfarin for patients with atrial fibrillation? Study design: Randomized controlled trial (double-blinded). Funding source: Industry. Allocation: Concealed. Setting: Outpatient (any) Synopsis: This study of apixaban, an oral factor Xa inhibitor, included patients with atrial fibrillation or flutter and at least one risk factor for stroke (aged 75 years or older, previous stroke, transient ischemic attack, systemic embolism, heart failure, diabetes mellitus, or hypertension). Patients with recent stroke, mitral stenosis, prosthetic heart valve, need for aspirin, or renal insufficiency (serum creatinine > 2.5 mg/dl or 221 umol/l) were excluded. Patients (N = 18,201) were randomized with concealed allocation to receive apixaban 5 mg twice daily or matching placebo; patients older than 80 years, those who weighed less than 60 kg, and those with serum creatinine levels of less than 1.5 mg/dl (133 umol/l) received a dose of 2.5 mg twice daily. Patients also received warfarin adjusted to an INR of 2.0 to 3.0, or matching placebo with sham adjustments. Thus, half of patients got apixaban twice daily plus sham warfarin, while half got placebo twice daily plus real warfarin. The mean age of participants was 70 years, 35% were women, and 85% had persistent or permanent atrial fibrillation (as opposed to paroxysmal). Patients were followed up for a median of 1.8 years, which is somewhat short for a study of a chronic disease. The primary efficacy outcome was the rate of stroke (ischemic, hemorrhagic, or uncertain) or systemic embolism, which occurred in 1.3% of patients receiving apixaban and 1.6% receiving warfarin (absolute risk reduction = 0.3%; number needed to treat [NNT] = 333/year; P =.01). When you look at the individual end points, the only one that improved was hemorrhagic stroke (0.24% vs 0.47%; P <.001; NNT = 434/year). Death from any cause was marginally less likely with apixaban (3.52% vs 3.94%; P =.047; NNT = 238/year), and major bleeding was also slightly less likely with apixaban (2.13% vs 3.09%/year; P <.001; NNT = 105). There was no difference between groups regarding liver function or hepatic outcomes, and there was no difference regarding the likelihood of myocardial infarction, pulmonary embolism, or deep vein thrombosis. Bottom line: In low-risk patients with atrial fibrillation, apixaban (Eliquis) was associated with a slightly lower risk of stroke or venous thromboembolism, as well as a slighly lower risk of major bleeding. It is more convenient than warfarin (as an oral drug that does not require regular INR testing) but is more expensive. Although pricing has not been established, it is likely to be similar to that for Pradaxa: approximately $200 per month. Of course, this higher drug cost has to be balanced against the costs of monitoring for warfarin and the slightly higher risk of stroke and bleeding with warfarin; an objective cost-effectiveness analysis is needed to help sort this out. Reference: Granger CB, Alexander JH, McMurray JJ, et al, for the ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365(11): #4: Edoxaban noninferior to warfarin for atrial fibrillation BACKGROUND: Edoxaban is a direct oral factor Xa inhibitor with proven antithrombotic effects. The long-term efficacy and safety of edoxaban as compared with warfarin in patients with atrial fibrillation is not known. METHODS: We conducted a randomized, double-blind, double-dummy trial comparing two once-daily regimens of edoxaban with warfarin in 21,105 patients with moderate-to-high-risk atrial fibrillation (median follow-up, 2.8 years). The primary efficacy end point was stroke or systemic embolism. Each edoxaban regimen was tested for noninferiority to warfarin during the treatment period. The principal safety end point was major bleeding. RESULTS: The annualized rate of the primary end point during treatment was 1.50% with warfarin (median time in the therapeutic range, 68.4%), as compared with 1.18% with high-dose edoxaban (hazard ratio, 0.79; 97.5% confidence interval [CI], 0.63 to 0.99; P<0.001 for noninferiority) and 1.61% with low-dose edoxaban (hazard ratio, 1.07; 97.5% CI, 0.87 to 1.31; P=0.005 for noninferiority). In the intention-to-treat analysis, there was a trend favoring high-dose edoxaban versus warfarin (hazard ratio, 0.87; 97.5% CI, 0.73 to 1.04; P=0.08) and an unfavorable trend with low-dose edoxaban versus warfarin (hazard ratio, 1.13; 97.5% CI, 0.96 to 1.34; P=0.10). The annualized rate of major bleeding was 3.43% with warfarin versus 2.75% with high-dose edoxaban (hazard ratio, 0.80; 95% CI, 0.71 to 0.91; P<0.001) and 1.61% with low-dose edoxaban (hazard ratio, 0.47; 95% CI, 0.41 to 0.55; P<0.001). The corresponding annualized rates of death from cardiovascular causes were 3.17% versus 2.74% (hazard ratio, 0.86; 95% CI, 0.77 to 0.97; P=0.01), and 2.71% (hazard ratio, 0.85; 95% CI, 0.76 to 0.96; P=0.008), and the corresponding rates of the key secondary end point (a composite of stroke, systemic embolism, or death from cardiovascular 5
 or dose-adjusted warfarin.")
6 causes) were 4.43% versus 3.85% (hazard ratio, 0.87; 95% CI, 0.78 to 0.96; P=0.005), and 4.23% (hazard ratio, 0.95; 95% CI, 0.86 to 1.05; P=0.32). CONCLUSIONS: Both once-daily regimens of edoxaban were noninferior to warfarin with respect to the prevention of stroke or systemic embolism and were associated with significantly lower rates of bleeding and death from cardiovascular causes. (Funded by Daiichi Sankyo Pharma Development; ENGAGE AF-TIMI 48 ClinicalTrials.gov number, NCT ). REFERENCE: Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med Nov 28;369(22): #5: Apixaban versus warfarin in nonvalvular atrial fibrillation: warfarin naïve vs warfarin experienced patients BACKGROUND: Patients with atrial fibrillation who are vitamin K antagonist (VKA)-naive may have a higher risk of thrombosis and/or bleeding than VKA-experienced patients. METHODS AND RESULTS: Using data from ARISTOTLE, we assessed baseline characteristics and the treatment effect of apixaban versus warfarin in the VKA-naive and VKA-experienced cohorts. We compared rates of study drug discontinuation and time-intherapeutic range. Overall, 7,800 (43%) were VKA naive, and 10,401 were VKA experienced. At baseline, both groups were similar with respect to age and congestive heart failure, hypertension, age, diabetes, stroke score (CHADS2). Fewer VKA-naive patients had a history of prior stroke (18% vs 21%) or prior bleeding (10% vs 22%) and were more often female (39% vs 33%). The effect of apixaban on the primary efficacy and safety outcomes was similar in VKA-naive (stroke/systemic embolism: hazard ratio [HR] 0.86, 95% CI and major bleeding: HR 0.73, 95% CI ) and VKA-experienced populations (stroke/systemic embolism: HR 0.73, 95% CI , P value for interaction = 0.39 and major bleeding: HR 0.66, 95% CI , P value for interaction = 0.50). Permanent study drug discontinuation was numerically less likely in patients receiving apixaban whether they were VKA naive (HR for discontinuation: 0.87, 95% CI ) or VKA experienced (HR for discontinuation: 0.93, 95% CI ). Among patients receiving warfarin, the mean/median times in therapeutic range were lower in the VKA-naive group (VKA-naive: 57.5/61.4, VKAexperienced: 66.0/69.1, P <.001). CONCLUSION: The treatment effects of apixaban (vs warfarin) were not modified by VKA naivety. The rates of stroke/systemic embolism and major bleeding were numerically lower among the patients assigned to apixaban, irrespective of prior VKA use. REFERENCE: Garcia DA, Wallentin L, Lopes RD, et al. Apixaban versus warfarin in patients with atrial fibrillation according to prior warfarin use: results from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation trial. Am Heart J Sep;166(3): #6: Rivaroxaban versus warfarin in nonvalvular atrial fibrillation: warfarin naïve vs warfarin experienced patients BACKGROUND: In ROCKET AF (Rivaroxaban Once-Daily, Oral, Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation), a large randomized, clinical trial, rivaroxaban was noninferior to warfarin in preventing stroke or systemic embolism in patients with atrial fibrillation. OBJECTIVE: To determine the efficacy and safety of rivaroxaban compared with warfarin among vitamin K antagonist (VKA)-naive and VKA-experienced patients. DESIGN: Prespecified subgroup analysis. (ClinicalTrials.gov: NCT ). SETTING: Global. PATIENTS: 14,264 persons with atrial fibrillation. MEASUREMENTS: Interaction of the relative treatment effect of rivaroxaban and warfarin on stroke or systemic embolism among VKAnaive and VKA-experienced patients. RESULTS: Overall, 7897 (55.4%) patients were VKA-experienced and 6367 (44.6%) were VKA-naive. The effect of rivaroxaban versus warfarin on stroke or systemic embolism was consistent: Rates per 100 patient-years of follow-up were 2.32 versus 2.87 for VKA-naive patients (hazard ratio [HR], 0.81 [95% CI, 0.64 to 1.03]) and 1.98 versus 2.09 for VKA-experienced patients (HR, 0.94 [CI, 0.75 to 1.18]; interaction P = 0.36). During the first 7 days, rivaroxaban was associated with more bleeding than warfarin (HR in VKA-naive patients, 5.83 [CI, 3.25 to 10.44], and in VKA-experienced patients, 6.66 [CI, 3.83 to 11.58]; interaction P = 0.53). After 30 days, rivaroxaban was associated with less bleeding than warfarin in VKA-naive patients (HR, 0.84 [CI, 0.74 to 0.95]) and similar bleeding in VKAexperienced patients (HR, 1.06 [CI, 0.96 to 1.17]; interaction P = 0.003). LIMITATION: The trial was not designed to detect differences in these subgroups. CONCLUSION: The efficacy of rivaroxaban in VKA-experienced and VKA-naive patients was similar to that of the overall trial. There were more bleeding events within 7 days of study drug initiation with rivaroxaban, but after 30 days, rivaroxaban was associated with less bleeding in VKA-naive patients and similar bleeding in VKA-experienced patients. This information may be useful to clinicians considering a transition to rivaroxaban for patients receiving VKA therapy. PRIMARY FUNDING SOURCE: Johnson & Johnson and Bayer HealthCare. REFERENCE: Mahaffey KW, Wojdyla D, Hankey GJ, ET AL. Clinical outcomes with rivaroxaban in patients transitioned from vitamin K antagonist therapy: a subgroup analysis of a randomized trial. Ann Intern Med Jun 18;158(12):
:2093-104.")
7 VTE Treatment/Prophylaxis #7: Rivaroxaban effective for acute DVT (EINSTEIN DVT) Clinical question: Is rivaroxaban safe and effective for the treatment of acute deep vein thrombosis? Study design: Randomized controlled trial (single-blinded). Funding source: Industry. Allocation: Concealed. Setting: Outpatient (any). Synopsis: Rivaroxaban is a direct inhibitor of coagulation factor Xa, and is given orally either once or twice a day. In this industry-sponsored study, patients with acute proximal DVT and no evidence of pulmonary embolism were randomized (allocation concealed) to receive either rivaroxaban (15 mg twice daily for 3 weeks, then 20 mg once daily) or standard therapy (enoxaparin 1 mg/kg twice a day, followed by warfarin titrated to an international normalized ratio of between 2.0 and 3.0). The duration of therapy was based on a risk factor assessment and was determined by the treating physician. Analysis was by intention to treat, groups were balanced at the start of the study, and outcomes were adjudicated by a central committee masked to treatment assignment. The mean age of the 3449 participants was 56 years, and the intended duration of therapy was 6 months for 63%, 12 months for 25%, and 3 months for 12%. Outcomes favored rivaroxaban: recurrent venous thromboembolism occurred less often (2.1% vs 3.0%; P <.001; number needed to treat [NNT] = 111), largely due to fewer episodes of DVT (14 vs 28). There was no difference in episodes of major bleeding between groups (14 for rivaroxaban vs 20 for standard therapy) and no difference in all-cause mortality (38 vs 49). In a second phase of the trial, the researchers enrolled 1196 patients who were felt to be at equipoise for continued anticoagulation after 6 months to 12 months (ie, their physician believed it was a toss-up whether they needed continued anticoagulation). In this phase, the patients were randomized in double-blind fashion to receive continued rivaroxaban or placebo and were followed up for up to 1 year. During that time, the combined outcome of major bleeding or recurrent VTE occurred in 2.0% in the rivaroxaban group and 7.1% in the placebo group (P <.001; NNT = 20). There was no evidence of hepatic toxicity, which was seen with an earlier factor Xa inhibitor. Bottom line: Rivaroxaban provides an oral alternative to warfarin for patients with acute deep vein thrombosis (DVT). The risk of major bleeding during a 1-year follow-up was approximately 0.7%, which is similar to that seen in other studies of long-term anticoagulant use. Although rivaroxaban is more convenient than warfarin, the cost is certain to be much higher. Reference: The EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010;363(26): #8: Oral rivaroxaban as effective as standard therapy for treatment of acute PE. (EINSTEIN PE) Clinical question: Is rivaroxaban as effective as enoxaparin plus an adjusted-dose vitamin K antagonist for the treatment of symptomatic pulmonary embolism? Study design: Randomized controlled trial (nonblinded). Funding source: Industry. Allocation: Concealed. Setting: Inpatient (any location) with outpatient follow-up Synopsis: In this open-label study, rivaroxaban was compared with enoxaparin plus a vitamin K antagonist for the treatment of PE. Adult patients with acute symptomatic PE were enrolled. Those with clinically significant kidney disease or liver disease were excluded. In the rivaroxaban group (n = 2419), patients received oral rivaroxaban 15 mg twice daily for 3 weeks, followed by 20 mg once daily. In the standard therapy group (n = 2413), patients received enoxaparin at a dose of 1 mg per kg twice daily along with either warfarin or acenocoumarol. Enoxaparin was discontinued after at least 5 days or after a therapeutic international normalized ratio (INR) was achieved. Duration of anticoagulation of 3, 6, or 12 months was determined by the treating physician prior to randomization. Almost 90% of the included patients were hospitalized and the majority was diagnosed with an unprovoked PE. It is noted that the use of nonsteroidal anti-inflammatory drugs and antiplatelet agents was discouraged, and if used, doses were limited to 100 mg of aspirin and 75 mg of clopidogrel. However, no data regarding these characteristics amongst the study population was reported. The primary efficacy analysis was by intention to treat, while the safety analysis included patients who received at least one dose of the study drug. For the primary outcome of symptomatic recurrent venous thromboembolism, there was no difference between rivaroxaban and standard therapy (50 events vs 44 events). For the primary safety outcome, there was no significant difference in the rates of overall clinically relevant bleeding between the 2 groups (10.3% in the rivaroxaban group vs 11.4% in the standard therapy group). However, the rivaroxaban group did have a lower rate of major bleeding events (1.1% vs 2.2%; hazard ratio = 0.49; 95% CI, ; number needed to treat = 90). Bottom line: For patients with acute symptomatic pulmonary embolism (PE), oral rivaroxaban was shown to be noninferior to standard therapy (enoxaparin and a vitamin K antagonist) in preventing recurrent venous thromboembolism. Although there is no significant difference in overall clinically relevant bleeding rates between the 2 groups, the rivaroxaban group had fewer major bleeding events. We would have to treat 90 people with rivaroxaban instead of standard therapy to prevent 1 major bleed. Reference: EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012;366(14): #9: Apixaban for VTE Clinical question: Is apixaban safer and more effective than conventional anticoagulation for venous thromboembolism? Bottom line: Apixaban (Eliquis) is no more effective than conventional anticoagulation for the treatment of venous thromboembolism. There is a small benefit in terms of reducing major bleeds in critical sites (approximately 1 fewer for every 270 patients given apixaban), but it is not clear whether this benefit is cost-effective. If apixaban costs $100 more per month than conventional therapy, then the cost per prevented critical site bleed is well over $150,000 for 6 months. A full cost-effectiveness analysis could better clarify the balance of 7
 to receive either rivaroxaban (15 mg twice daily for 3")
8 benefits, harms, and costs. It is likely that this drug is a good choice for selected patients (those who may have difficulty complying with warfarin and international normalized ratio (INR) monitoring, or those who have higher bleeding risk), but is unlikely to be cost-effective for many others. (LOE = 1b) Study design: Randomized controlled trial (double-blinded) Funding source: Industry Allocation: Concealed Setting: Outpatient (any) Synopsis: Apixaban is an oral factor Xa inhibitor given twice daily. In this trial, 5395 adults with venous thromboembolism (n = 3532), pulmonary embolism (n = 1359), or both (n = 477) were randomized to receive apixaban or usual therapy with enoxaparin 1 mg per kg every 12 hours for at least 5 days, and then warfarin for 6 months at a target range INR of 2.0 to 3.0. Apixaban was given in a dosage of 10 mg twice daily for 7 days, followed by 5 mg twice daily for 6 months. The groups were balanced at the beginning of the study: mean age 57 years, 58% male, and a median of 5 days from onset of symptoms to randomization. Patients were followed up for 6 months by telephone or in the clinic, and outcomes were assessed by committee members masked to treatment assignment. The authors excluded patients with active bleeding, anemia, impaired renal function, or cancer, and those who were taking aspirin. They also excluded patients who had a clear cause for the clot that could be removed (for example, a postoperative or travel-related clot, which is often treated with only 3 months of anticoagulation). Major bleeding occurred more often in the conventional therapy group (1.8% vs 0.6%; P <.001; number needed to treat = 83). Critical site bleeds -- a subset of major bleeds that included intracranial, retroperitoneal, intrathoracic, intraocular, and intraarticular bleeds -- were also somewhat less common (4 vs 14), but a test of statistical significance is not provided. If we assume that it is significant, that is approximately 1 fewer critical site bleed for every 270 patients given apixaban instead of conventional therapy. There was no difference in the likelihood of death or recurrent venous thromboembolism. Approximately half of the recurrences and major bleeds occurred during the first month of therapy for both groups. Reference: Agnelli G, Buller HR, Cohen A, et al, for the AMPLIFY Investigators. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med 2013;369(9): #10: Dabigatran for prevention of VTE recurrence BACKGROUND: Dabigatran, which is administered in a fixed dose and does not require laboratory monitoring, may be suitable for extended treatment of venous thromboembolism. METHODS: In two double-blind, randomized trials, we compared dabigatran at a dose of 150 mg twice daily with warfarin (activecontrol study) or with placebo (placebo-control study) in patients with venous thromboembolism who had completed at least 3 initial months of therapy. RESULTS: In the active-control study, recurrent venous thromboembolism occurred in 26 of 1430 patients in the dabigatran group (1.8%) and 18 of 1426 patients in the warfarin group (1.3%) (hazard ratio with dabigatran, 1.44; 95% confidence interval [CI], 0.78 to 2.64; P=0.01 for noninferiority). Major bleeding occurred in 13 patients in the dabigatran group (0.9%) and 25 patients in the warfarin group (1.8%) (hazard ratio, 0.52; 95% CI, 0.27 to 1.02). Major or clinically relevant bleeding was less frequent with dabigatran (hazard ratio, 0.54; 95% CI, 0.41 to 0.71). Acute coronary syndromes occurred in 13 patients in the dabigatran group (0.9%) and 3 patients in the warfarin group (0.2%) (P=0.02). In the placebo-control study, recurrent venous thromboembolism occurred in 3 of 681 patients in the dabigatran group (0.4%) and 37 of 662 patients in the placebo group (5.6%) (hazard ratio, 0.08; 95% CI, 0.02 to 0.25; P<0.001). Major bleeding occurred in 2 patients in the dabigatran group (0.3%) and 0 patients in the placebo group. Major or clinically relevant bleeding occurred in 36 patients in the dabigatran group (5.3%) and 12 patients in the placebo group (1.8%) (hazard ratio, 2.92; 95% CI, 1.52 to 5.60). Acute coronary syndromes occurred in 1 patient each in the dabigatran and placebo groups. CONCLUSIONS: Dabigatran was effective in the extended treatment of venous thromboembolism and carried a lower risk of major or clinically relevant bleeding than warfarin but a higher risk than placebo. (Funded by Boehringer Ingelheim; RE-MEDY and RE-SONATE ClinicalTrials.gov numbers, NCT and NCT , respectively.). REFERENCE: Schulman S(1), Kearon C, Kakkar AK, et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med Feb 21;368(8): #11: Edoxaban for prevention of VTE recurrence BACKGROUND: Whether the oral factor Xa inhibitor edoxaban can be an alternative to warfarin in patients with venous thromboembolism is unclear. METHODS: In a randomized, double-blind, noninferiority study, we randomly assigned patients with acute venous thromboembolism, who had initially received heparin, to receive edoxaban at a dose of 60 mg once daily, or 30 mg once daily (e.g., in the case of patients with creatinine clearance of 30 to 50 ml per minute or a body weight below 60 kg), or to receive warfarin. Patients received the study drug for 3 to 12 months. The primary efficacy outcome was recurrent symptomatic venous thromboembolism. The principal safety outcome was major or clinically relevant nonmajor bleeding. RESULTS: A total of 4921 patients presented with deep-vein thrombosis, and 3319 with a pulmonary embolism. Among patients receiving warfarin, the time in the therapeutic range was 63.5%. Edoxaban was noninferior to warfarin with respect to the primary efficacy outcome, which occurred in 130 patients in the edoxaban group (3.2%) and 146 patients in the warfarin group (3.5%) (hazard ratio, 0.89; 95% confidence interval [CI], 0.70 to 1.13; P<0.001 for noninferiority). The safety outcome occurred in 349 patients (8.5%) in the edoxaban group and 423 patients (10.3%) in the warfarin group (hazard ratio, 0.81; 95% CI, 0.71 to 0.94; P=0.004 for superiority). The rates of other adverse events were similar in the two groups. A total of 938 patients with pulmonary embolism had right ventricular 8
 Study design: Randomized controlled trial (double-blinded) Funding source: Industry Allocation: Concealed Setting: Outpatient (any) Synopsis: Apixaban is an oral factor Xa inhibitor given")
9 dysfunction, as assessed by measurement of N-terminal pro-brain natriuretic peptide levels; the rate of recurrent venous Thromboembolism in this subgroup was 3.3% in the edoxaban group and 6.2% in the warfarin group (hazard ratio, 0.52;95% CI, 0.28 to 0.98). CONCLUSIONS: Edoxaban administered once daily after initial treatment with heparin was noninferior to high-quality standard therapy and caused significantly less bleeding in a broad spectrum of patients with venous thromboembolism, including those with severe pulmonary embolism. (Funded by Daiichi-Sankyo; Hokusai-VTE ClinicalTrials.gov number, NCT ). REFERENCE: Hokusai-VTE Investigators, Büller HR, Décousus H, ET AL. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med Oct 10;369(15): #12: Meta-analysis: Warfarin more effective but has higher bleeding risk vs newer agents in secondary VTE prevention OBJECTIVE: To summarise and compare the efficacy and safety of various oral anticoagulants (dabigatran, rivaroxaban, apixaban, and vitamin K antagonists) and antiplatelet agents (acetylsalicylic acid) for the secondary prevention of venous thromboembolism. DESIGN: Systematic review and network meta-analysis. DATA SOURCES: Literature search using Medline (1950 to present), Embase (1980 to present), and the Cochrane Register of Controlled Trials using the OVID interface. Publications from potentially relevant journals were also searched by hand. REVIEW METHODS: Randomised controlled trials of patients receiving anticoagulants, antiplatelet drugs, or placebo or observation for secondary prevention of venous thromboembolism. Selected outcomes were rates of recurrent venous thromboembolism and major bleeding. Two reviewers independently extracted data onto standardised forms. RESULTS: 12 articles met our inclusion criteria, with 11,999 patients evaluated for efficacy and 12,167 for safety. All treatments reduced the risk of recurrent venous thromboembolism. Compared with placebo or observation, vitamin K antagonists at a standard adjusted dose (target international normalised ratio ) showed the highest risk difference (odds ratio 0.07; 95% credible interval 0.03 to 0.15) and acetylsalicylic acid showed the lowest risk difference (0.65; 0.39 to 1.03). Risk of major bleeding was higher with a standard adjusted dose of vitamin K antagonists (5.24; 1.78 to 18.25) than with placebo or observation. Fatal recurrent venous thromboembolism and fatal bleeding were rare. Detailed subgroup and individual patient level data were not available. CONCLUSIONS: All oral anticoagulants and antiplatelet agents investigated in this analysis were associated with a reduced recurrence of venous thromboembolism compared with placebo or observation, although acetylsalicylic acid was associated with the lowest risk reduction. Vitamin K antagonists given at a standard adjusted dose was associated with the greatest risk reduction in recurrent venous thromboembolism, but also the greatest risk of major bleeding. REFERENCE: Castellucci LA, Cameron C, Le Gal G, et al. Efficacy and safety outcomes of oral anticoagulants and antiplatelet drugs in the secondary prevention of venous thromboembolism: systematic review and network meta-analysis. BMJ Aug 30;347 The following is one of the four RECORD trials on the use of rivaroxaban in THROMBOPROPHYLAXIS in THR and TKR patients. #13: Oral rivaroxaban for thromboprophylaxis in THR patients. (RECORD 1) BACKGROUND: This phase 3 trial compared the efficacy and safety of rivaroxaban, an oral direct inhibitor of factor Xa, with those of enoxaparin for extended thromboprophylaxis in patients undergoing total hip arthroplasty. METHODS: In this randomized, double-blind study, we assigned 4541 patients to receive either 10 mg of oral rivaroxaban once daily, beginning after surgery, or 40 mg of enoxaparin subcutaneously once daily, beginning the evening before surgery, plus a placebo tablet or injection. The primary efficacy outcome was the composite of deep-vein thrombosis (either symptomatic or detected by bilateral venography if the patient was asymptomatic), nonfatal pulmonary embolism, or death from any cause at 36 days (range, 30 to 42). The main secondary efficacy outcome was major venous thromboembolism (proximal deep-vein thrombosis, nonfatal pulmonary embolism, or death from venous thromboembolism). The primary safety outcome was major bleeding. RESULTS: A total of 3153 patients were included in the superiority analysis (after 1388 exclusions), and 4433 were included in the safety analysis (after 108 exclusions). The primary efficacy outcome occurred in 18 of 1595 patients (1.1%) in the rivaroxaban group and in 58 of 1558 patients (3.7%) in the enoxaparin group (absolute risk reduction, 2.6%; 95% confidence interval [CI], 1.5 to 3.7; P<0.001). Major venous thromboembolism occurred in 4 of 1686 patients (0.2%) in the rivaroxaban group and in 33 of 1678 patients (2.0%) in the enoxaparin group (absolute risk reduction, 1.7%; 95% CI, 1.0 to 2.5; P<0.001). Major bleeding occurred in 6 of 2209 patients (0.3%) in the rivaroxaban group and in 2 of 2224 patients (0.1%) in the enoxaparin group (P=0.18). CONCLUSIONS: A once-daily, 10-mg oral dose of rivaroxaban was significantly more effective for extended thromboprophylaxis than a once-daily, 40-mg subcutaneous dose of enoxaparin in patients undergoing elective total hip arthroplasty. The two drugs had similar safety profiles. REFERENCE: Eriksson BI, Borris LC, Friedman RJ, et al. RECORD1 Study Group. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med Jun 26;358(26): #14: Clinical benefits of newer agents for thromboprophylaxis are marginal 9
.")
10 BACKGROUND: Pharmacologic thromboprophylaxis reduces the risk for venous thromboembolism after total hip replacement (THR) or total knee replacement (TKR). New oral anticoagulants (NOACs), including direct thrombin inhibitors and factor Xa inhibitors, are emerging options for thromboprophylaxis after these procedures. PURPOSE: To compare the benefits and risks of NOACs versus standard thromboprophylaxis for adults having THR or TKR. DATA SOURCES: MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews from January 2009 through March STUDY SELECTION: English-language systematic reviews. DATA EXTRACTION: Two independent reviewers abstracted data and rated study quality and strength of evidence. DATA SYNTHESIS: Six good-quality systematic reviews compared NOACs with low-molecular-weight heparin (LMWH) for thromboprophylaxis after THR or TKR. Risk for symptomatic deep venous thrombosis, but not risk for death or nonfatal pulmonary embolism, was reduced with factor Xa inhibitors compared with LMWH (4 fewer events per 1000 patients). Conversely, the risk for major bleeding increased (2 more events per 1000 patients). Outcomes of dabigatran did not significantly differ from those of LMWH. Indirect evaluation of NOACs by common comparison with LMWH showed nonsignificantly reduced risks for venous thromboembolism with rivaroxaban compared with dabigatran (risk ratio [RR], 0.68 [95% CI, 0.21 to 2.23]) and apixaban (RR, 0.59 [CI, 0.26 to 1.33]) but increased major bleeding. New oral anticoagulants have not been compared with warfarin,aspirin, or unfractionated heparin. LIMITATIONS: Head-to-head comparisons among NOACs were not available. Efficacy is uncertain in routine clinical practice. CONCLUSION: New oral anticoagulants are effective for thromboprophylaxis after THR and TKR. Their clinical benefits over LMWH are marginal and offset by increased risk for major bleeding. REFERENCE: Adam SS, McDuffie JR, Lachiewicz PF, et al. Comparative effectiveness of new oral anticoagulants and standard thromboprophylaxis in patients having total hip or knee replacement: a systematic review. Ann Intern Med Aug 20;159(4): PRIMARY FUNDING SOURCE: U.S. Department of Veterans Affairs. Safety issues The following 3 abstracts remind us that if an anticoagulant is safe and effective for one indication, it does not follow that is safe to stretch the indications nor that the new drug is effective for non-approved indications. Therefore pay attention to FDA approved indications #15: Dabigatran is neither safe nor effective for anticoagulation with mechanical heart valves Clinical question: Is dabigatran a safe and effective anticoagulant for patients with mechanical heart valves? Bottom line: Warfarin is a safer and more effective alternative than dabigatran for anticoagulation of patients with a mechanical heart valve. (LOE = 1b) Study design: Randomized controlled trial (single-blinded) Funding source: Industry Allocation: Concealed Setting: Outpatient (specialty) Synopsis: The authors identified adults undergoing implantation of a mechanical valve for the aortic or mitral valve (or both), as well as patients who had received a mechanical valve at least 3 months previously. Patients were randomized with concealed allocation to receive either dabigatran or warfarin. Dabigatran was initially dosed in a range from 150 mg twice daily to 300 mg twice daily (depending on renal function), and the dose was adjusted to maintain a level of at least 50 ng/ml. Warfarin was dosed to maintain an international normalized ratio (INR) between 2.5 and 3.5 for those with a mechanical aortic valve and additional risk factors for thromboembolism and for those with a mitral valve; patients with an aortic valve and no risk factors were maintained at an INR range of 2.0 to 3.0. A total of 252 patients, with a mean age of 56 years, were randomized; 68% had a mechanical aortic valve, 28% a mitral valve, and 4% both. This was an open-label trial, but with masked outcome assessment and appropriate concealment of allocation. Patients were followed up for 12 weeks, and at that time could choose whether or not to continue to take the assigned study drug as part of an extension trial. A total of 168 patients participated in the extension trial (99 in the dabigatran group, 59 in the warfarin group), with a median duration of treatment between 136 days and 152 days, depending on the study drug and population. The study was terminated prematurely because of an excess of strokes (5% in the dabigatran group vs 0% in the warfarin group), major bleeding (4% vs 2%) and any bleeding (27% vs 12%). Although only the difference in any bleeds was statistically significant, the weight of the evidence led the researchers to discontinue the trial. The major bleeds were all pericardial. Reference: Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med 2013;369: #16: Dabigatran associated with increased risk of coronary events Clinical question: Does the use of dabigatran increase the risk of acute coronary events? Bottom line: The increased risk of myocardial infarction (MI) or acute coronary syndrome (ACS) associated with dabigatran is small, but statistically significant. You would have to treat 250 patients with dabigatran to cause one additional acute coronary event. Study design: Meta-analysis (randomized controlled trials) Funding source: Unknown/not stated Setting: Various (meta-analysis)synopsis The original RE-LY (Randomized Evaluation of Long-term Anticoagulant Therapy) study, comparing dabigatran with warfarin for stroke prophylaxis in atrial fibrillation, revealed a slightly higher risk of MI with dabigatran (Connolly et al; Daily POEM, 11/9/09). To investigate the association of dabigatran 10

11 and acute coronary events, these authors searched PubMed, Scopus, and the Web of Science and selected 7 randomized controlled trials (N = 30,514) that evaluated the efficacy of dabigatran for different indications, including stroke prophylaxis for atrial fibrillation, treatment of acute venous thrombembolism, and deep venous thrombosis prophylaxis in joint replacement patients. All of the included trials also reported on secondary outcomes of MI or ACS. One author independently extracted data, which was then reviewed by the second author. Study quality was assessed using the Jadad scale. Of note, the 7 included studies were all industry funded. Pooled together, the data showed that dabigatran is associated with a higher risk of MI or ACS than warfarin, enoxaparin, and placebo (1.19% vs 0.79%; odds ratio = 1.33; 95% CI, ; P =.03). The RE-LY study, which comprised 59% of the cohort for this meta-analysis, had the largest effect on the result. This risk remained high when using the revised data from RE-LY that added previously unreported events, including 4 clinical MIs and 28 silent MIs. Data from the 6 trials that reported on mortality showed that dabigatran was associated with a lower risk of death than the control group (4.83% vs 5.02%; P =.04). However, this was not the primary outcome studied in this meta-analysis. Furthermore, given the different disease processes represented, there was significant heterogeneity across studies in the measure of absolute risk reduction for mortality. Reference: Uchino K, Hernandez AV. Dabigatran association with higher risk of acute coronary events. Arch Intern Med 2012;172: #17 Apixaban increases bleeding with no benefit in high-risk patients with ACS Clinical question: Does the use of apixaban along with standard antiplatelet therapy decrease recurrent ischemic events following acute coronary syndrome? Bottom line: Apixaban added to standard antiplatelet therapy in high-risk patients with recent acute coronary syndrome (ACS) increases bleeding without significantly reducing recurrent ischemic events, such as stroke, myocardial infarction, or death. Study design: Randomized controlled trial (double-blinded). Funding source: Industry. Allocation: Concealed. Setting: Inpatient (any location) with outpatient follow-up. Synopsis: Apixaban, an oral direct factor Xa inhibitor, can be used to prevent venous thromboembolism in patients undergoing orthopedic surgery and thromboembolic events in patients with atrial fibrillation. This study examined the effect of apixaban in preventing ishcemic events in high-risk patients with ACS. Using concealed allocation, investigators randomized 7392 patients with ACS within the previous 7 days to receive apixaban 5 mg twice daily or placebo. Patients were also receiving standard treatment with aspirin alone or aspirin and clopidogrel. In addition, eligible patients had 2 or more high-risk factors, such as older age, diabetes, peripheral vascular disease, heart failure, history of stroke, renal dysfunction, or lack of revascularization after the index event. At baseline, patients in both groups were well matched with similar comorbidities. The authors performed both intention-to-treat and on-treatment analyses. Because of an excess of clinically significant bleeding events, the trial was stopped early. For the composite outcome of cardiovascular death, myocardial infarction, or ischemic stroke, there was no difference detected between the apixaban and the placebo groups. This was true in patients receiving aspirin alone and in patients receiving both aspirin and clopidogrel. Bleeding, however, was more prominent in the apixaban group; major bleeding, including fatal and intracranial bleeding, was found in 1.3% of patients taking apixaban compared with 0.5% of patients taking placebo (hazard ratio = 2.59; 95% CI, ; P =.001).Reference: Alexander JH, Lopes RD, James S, et al, for the the APPRAISE-2 Investigators. Apixaban with antiplatelet therapy after acute coronary syndrome. N Engl J Med 2011; Jul 24. #18: ICH risk with newer anticoagulants 0.6% vs 1.2% with warfarin/asa Clinical question: Are the newer anticoagulants less likely to cause intracranial hemorrhage than warfarin or aspirin? Bottom line: This meta-analysis of randomized trials comparing newer anticoagulants against warfarin or aspirin for patients with atrial fibrillation (AF) showed that patients in the treatment groups had fewer intracranial hemorrhages (ICHs) than those in the control groups. It remains to be seen if this result will hold up with longer duration of use in patients less selected than those enrolled in clinical trials. (LOE = 1a) Study design: Meta-analysis (randomized controlled trials) Funding source: Unknown/not stated Setting: Various (meta-analysis) Synopsis: The newer anticoagulants dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis) are marketed heavily as not needing frequent laboratory monitoring, and the manufacturers claim greater effectiveness than warfarin. Although anticoagulants can prevent ischemic stroke in patients with AF, they also cause ICH, a catastrophic event. These authors searched multiple databases, conference abstracts, references of included papers, and a clinical trials registry to identify randomized trials of newer anticoagulants against any comparison intervention in preventing stroke in patients with nonvalvular AF. Two authors independently determined study inclusion and assessed study quality. For these elements, they don't say how disagreements were handled. Additionally, 2 authors independently extracted the data and resolved any discrepancies through consensus. In addition to the usual statistical methods used in meta-analyses, these authors did a whole bunch of additional nerdy stuff (Bayesian analyses, Monte Carlo simulation, Gibbs sampling) to obfuscate their real intent. Ultimately, they included 6 studies with more than 57,000 patients. Five studies compared the new agent against warfarin (target INR = ) and one compared them against aspirin ( mg/day). Five studies went beyond 1 year and one was only 12 weeks duration. Needless to say, all the included studies were industry sponsored. The authors, however, reported no conflicts of interest. If you ignore all the nerdy stuff and just look at the raw data, the rate of ICH in each of the included studies was lower in the patients receiving the newer agents, although the confidence intervals were enormous in most studies and not statistically significant in 3 studies. When you pool the data, the rate of ICH in patients treated with newer agents was 0.6% compared with 1.2% in the comparison groups (number needed to treat to prevent 1 ICH = 154; 95% CI, ). So, this is a good example of how reducing by half the rate of a bad event can sound good until you realize the event rate is rare. Keep in mind that industry-sponsored studies, while having decent internal validity, are designed to weed out those patients who are unlikely to respond and who are among the healthiest. When we try to use these products in the real world, where we stretch the eligibility and give them to 11

12 our frailest patients, we often find that our patients don't have the same experiences as did those in the studies. Perhaps the only important outcome from all the other analyses was that, indirectly, no newer agent appeared any safer than the rest. Reference: Chatterjee S, Sardar P, Biondi-Zoccai G, Kumbhani DJ. New oral anticoagulants and the risk of intracranial hemorrhage: traditional and Bayesian meta-analysis and mixed treatment comparison of randomized trials of new oral anticoagulants in atrial fibrillation. JAMA Neurol 2013;70: Bottom Lines 1. The three newer oral anticoagulants (dabigatran and apixaban and rivaroxaban) have all been approved for the treatment of non-valvular atrial fibrillation. Whether these drugs should be used in place of warfarin for this indication is still undetermined. The NNTs for differences in clinical outcomes between these drugs and warfarin are between 100 and Rivaroxaban has also been FDA approved for the treatment of VTE and prophylaxis of VTE in patients undergoing THR and TKR. 3. Note which drugs have which indications, as extrapolating from one indication to another indication may be unsafe. 4. Newer drugs and studies on broader indications are in the pipeline so stay tuned! 12

13 Appendix: Data tables from the 3 major studies on the newer oral anticoagulants vs warfarin Table 1 Data from the RE-LY Study on dabigatran vs warfarin for atrial fibrillation. N Engl J Med 2009;361(12): Warfarin Dabigatran 150 bid * NNT All CVA or systemic emboli per year (%) Major bleeding per year (%) Intracerebral hemorrhages per year (%) % (p=.001) % (p=.31) % (p=.001) 357 Dyspepsia (% of patients) % (p=.001) 18 MI (% of patients) % (p=.048) 476 Mortality (%) all cause % (p=.051) 204 Mean follow up duration was 2 years No difference in mortality between groups Shaded = favoring dabigitran Not shaded = favoring warfarin Dabigatran 150 bid was superior to warfarin in primary outcome Note there is no specific antidote to dabigatran, its half-life is hours (major hemorrhage treatment is supportive, and transfusions and surgery if needed The FDA approved dabigatran in October of 2010 at a dose of 150 mg bid if the GFR is > 30, and 75 bid if the GFR is < 30 but > 15; there are no dosing recommendations for patients with a GFR < 15 or on dialysis The 110 mg dose was not approved 13

14 Table 2 Data from the Rocket AF. Rivaroxaban vs Warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365): Warfarin Rivaroxaban * NNT All CVA or systemic emboli per year (%) Major bleeding per year (%) Intracerebral hemorrhages per year (%) % (p=.001) % (p=.58) % (p=.02) 500 MI (% of patients) % (p=.12) 500 Mortality (%) all cause % (p=.15) 250 Mean follow up duration was ~ 2 years No difference in mortality between groups Shaded = favoring rivaroxaban Not shaded = favoring warfarin Rivaroxaban was non inferior to warfarin in primary outcome Note there is no specific antidote to rivaroxaban (major hemorrhage treatment is supportive, and transfusions and surgery if needed Table 3 Data from Aristotle. Apixiban vs Warfarin in patients with atrial fibrillation. N Engl J Med 2011;365): Warfarin Apixaban * NNT All CVA or systemic emboli per year (%) Major bleeding per year (%) Intracerebral hemorrhages per year (%) % (p=.01) % (p=.001) % (p=.001) 212 MI (% of patients) % (p=.37) 1111 Mortality (%) all cause % (p=.047) 238 Mean follow up duration was 1.8 years Shaded = favoring Apixaban Not shaded = favoring warfarin Apixaban was non inferior and superior to warfarin in primary outcome Note there is no specific antidote to apixiban (major hemorrhage treatment is supportive, and transfusions and surgery if needed 14
 250 Mean follow up duration was ~ 2 years No difference in mortality between groups Shaded = favoring rivaroxaban Not shaded = favoring warfarin Rivaroxaban was non inferior to warfarin in")
15 Table 4 Comparisons between warfarin and 4 NOAs for atrial fibrillation Table 5 Comparisons between warfarin and 4 NOAs for VTE 15

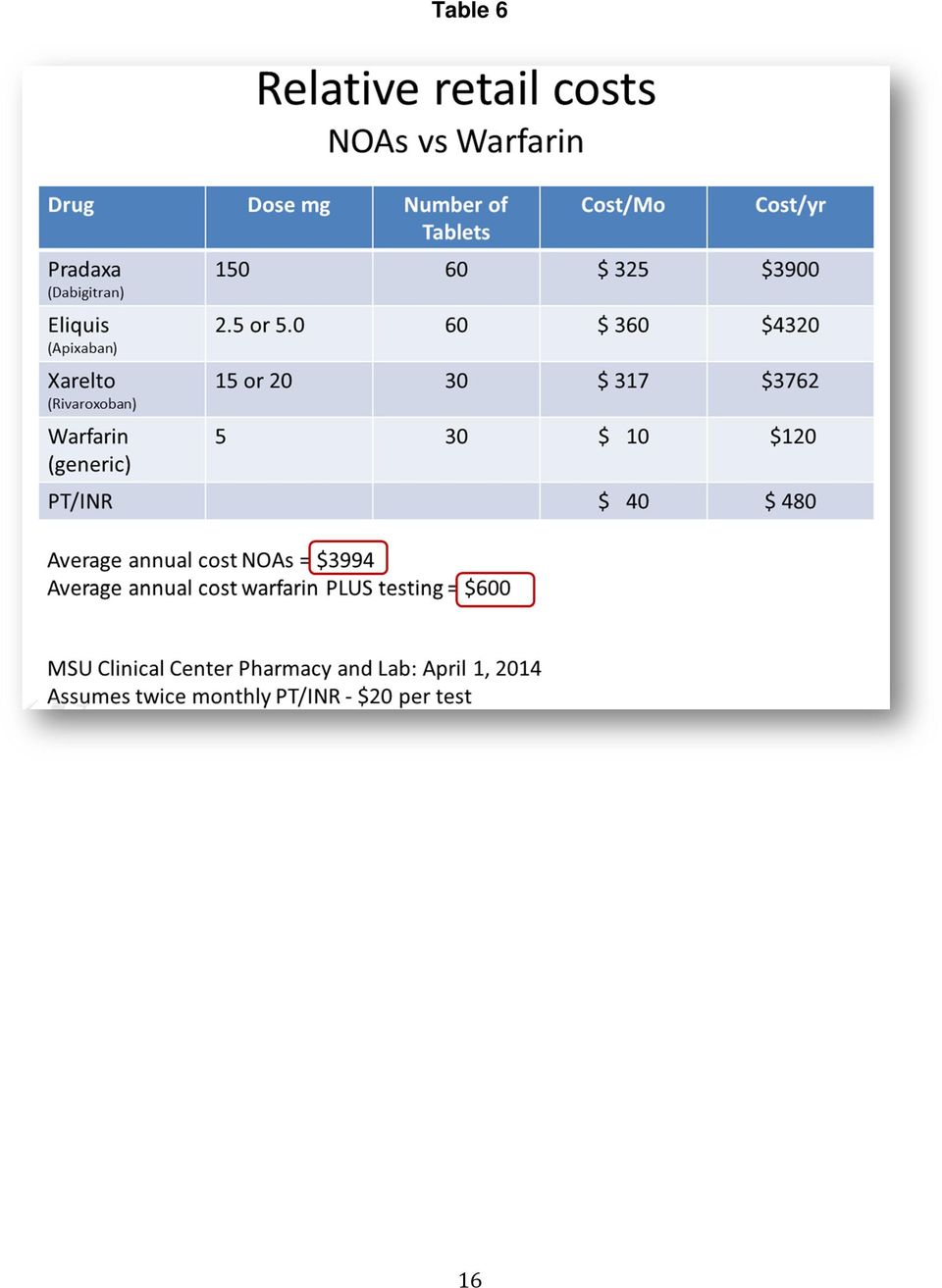
16 Table 6 16
17 Table 7 Drug (Trade Name) Mechanism FDA Approved Indication(s) General Dosing DDIs Apixaban (Eliquis) Factor Xa inhibitor Nonvalvular atrial fib mg bid itraconazole, clarithromycin among others Rivaroxaban (Xarelto) Factor Xa inhibitor Nonvalvular atrial fib Treatment of DVT and/or PE Prevent of recurrent DVT and PE following initial 6 months treatment for DVT and/or PE Dosing more complex: AF: mg with evening meal for AF (depending on creatinine clearance) (DDI major = amiodarone diltiazem, verapamil, felodipine, azithromycin among others) Prevention of DVT/PE in pts undergoing knee or hip replacement surgery Rx DVT/PE: 15 bid with food for 21 days, then 20 mg daily with food Prevent DVT/PE recurrence: 20 daily with food DVT prophylaxis with hip and knee surgery: 10 mg once daily for 12 (knee) or 35 (hip) days Edoxaban (Savaysa) Factor Xa inhibitor Seeking approval for Non-valvular atrial fibrillation (NVAF) The treatment of DVT/PE Dabigatran (Pradaxa) Direct thrombin inhibitor The prevention of recurrence of symptomatic venous thromboembolism Nonvalvular atrial fib mg bid depending on Cr Clearance 17
 Prevention of DVT/PE in pts undergoing knee or hip replacement surgery Rx DVT/PE: 15 bid with food for 21 days, then 20 mg daily with food Prevent DVT/PE recurrence: 20")
18 Behavioral Health Update John Hickner, MD, MSc Objectives 1. Evaluate alternative approaches to management of depression 2. Describe two effective approaches to post traumatic stress disorder 3. Summarize recent evidence regarding effective behavioral and medical approaches to a variety of conditions. Other than medications and psychotherapy, what treatments are effective (or not effective) for depression? Psychotropic drugs and psychotherapy are both somewhat effective for depression, though neither is a silver bullet. Other approaches include vitamin supplementation, exercise, computer games, telemedicine and repetitive transcranial magnetic brain stimulation. Following is some recent evidence to support or refute these integrative and novel approaches. #1: Vitamin D has no effect on depressive symptoms Clinical question: In patient with low vitamin D levels, does vitamin D supplementation improve symptoms of depression? Study design: Randomized controlled trial (double-blinded) Setting: Outpatient (primary care) Synopsis: This study was conducted in Norway, where researchers started by identifying patients with depressive symptoms and low vitamin D levels (< 22 ng/ml [< 55 nmol/l]). The authors excluded patients with severe depression (who were sent for treatment). The remaining 243 patients had a range of depression scores, though the percent with mild to moderate depression were not reported. These patients were randomized, using concealed allocation, to receive oral placebo or cholecalciferol 40,000 IU weekly. After 6 months, vitamin D levels increased to normal in 97.5% of treated patients but only in 1.6% of the placebo group. However, there were significant improvements in depression scores in both groups, including an increase in global seasonality score, a measure of seasonal affective disorder. Patients with higher depression scores (who met the definition of depressive disorder) at the start of the study may have had a greater improvement in depression scores with treatment than patients receiving placebo, though this result needs to be confirmed by other studies. Bottom line: Taken in aggregate, symptoms of depression do not improve in patients with low vitamin D levels when given vitamin D supplementation any more than when given placebo. There may be a benefit in patients with low vitamin D levels and mild to moderate depression. Kjærgaard M, Waterloo K, Wang CE, et al. Effect of vitamin D supplement on depression scores in people with low levels of serum 25- hydroxyvitamin D: nested case-control study and randomised clinical trial. Br J Psychiatry 2012;201(5): #2: Meta-analysis shows no effect of Vitamin D on depression symptoms Context: Randomized controlled trials (RCTs) investigating the efficacy of vitamin D (Vit D) in depression provided inconsistent results. Objective: We aim to summarize the evidence of RCTs to assess the efficacy of oral Vit D supplementation in depression compared to placebo. Data sources: Electronic databases, two conferences proceedings, and grey literature by contacting authors of included studies. Study selection: Parallel RCTs investigating the effect of oral Vit D supplementation compared with placebo on depression in adults at risk of depression, with depression symptoms or a primary diagnosis of depression. Data extraction: Two reviewers independently extracted data from relevant literature. Data synthesis: Classical and Bayesian randomeffects meta-analyses were used to pool relative risk (RR), odds ratio (OR) and standardized mean difference (SMD). Quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool. Results: Six RCTs were identified with 1,203 participants (72% for females) including 71 depressed patients, of which five studies involved adults at risk of depression and one trial used depressed patients. Results of the classical meta-analysis showed no significant effect of Vit D supplementation on post-intervention depression scores (SMD=-0.14, 95% CI: to 0.13, P=0.32; OR=0.93, 95% CI: 0.54 to 1.59, P=0.79). The quality of evidence was low. No significant differences were demonstrated in subgroup or sensitivity analyses. Similar results were found when Bayesian meta-analyses were applied. Conclusions: There is insufficient evidence to support the efficacy of Vit D supplementation in depression symptoms, and more RCTs using depressed patients are warranted. Li G, Mbuagbaw L, Samaan Z, Falavigna M, Zhang S, Adachi JD, Cheng J, Papaioannou A, Thabane L. Efficacy of vitamin D supplementation in depression in adults: a systematic review. J Clin Endocrinol Metab Dec 10:jc PMID:

19 #3: Exercise effective for depression in older people Clinical question: Is an exercise program effective in older patients with depressive symptoms? Study design: Meta-analysis (randomized controlled trials) Funding source: Unknown/not stated Setting: Various (meta-analysis) Synopsis: The authors searched many databases, including the Cochrane Central Register of Controlled Trials, and reference lists of relevant articles for unpublished and published randomized controlled trials of exercise programs in patients at least 60 years of age. Two authors independently selected articles for inclusion. One author abstracted the data, which was checked by a second author. The 9 studies enrolled a total of 667 patients and used a variety of exercise programs, including endurance and strength training, and tai chi and qi gong. Risk of bias was assessed independently by 2 authors and was low for most studies (except for the studies of tai chi and qi gong, which were excluded from the meta-analysis). Publication bias was not formally assessed. Four studies did not clearly analyze results by intention to treat, making it more difficult to extrapolate the results to everyday practice. Exercise programs lowered depression severity scores by a small to medium degree (standardized mean difference = -.34; 95% CI, -.52 to -.17); translated, this means that 13% of the patients in the exercise group did better than expected and had an approximately 20% reduction in the severity of their depression symptoms. Bottom line: An organized exercise program for older patients, which may include strength training or endurance training, or both, may be helpful for some patients with symptoms of depression. The results will not be striking, but exercise is an option for patients willing to participate. (LOE = 1a) Reference; Bridle C, Spanjers K, Patel S, Atherton NM, Lamb SE. Effect of exercise on depression severity in older people: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry 2012;201(3): #4: Exercise decreases depressive symptoms of chronic illness Clinical question: In patients with chronic illness complicated by depressive symptoms, is exercise effective in decreasing these symptoms? Study design: Meta-analysis (randomized controlled trials) Setting: Various (meta-analysis) Synopsis: The authors included English language studies of sedentary patients with a chronic illness -- cardiovascular disease, cancer, fibromyalgia, multiple sclerosis, and others -- with depression who were randomly assigned to exercise or a nonexercise treatment. The authors searched several databases, but not the Cochrane Library or any other evidence-based resource. Two authors independently assessed the studies for quality. There was heterogeneity among the studies, perhaps due to the type of patients enrolled. There was no evidence of publication bias. Surprisingly, the authors identified 90 articles evaluating 10,534 patients. They were able to find this many studies because depressive symptoms were often secondary outcomes in other studies. They were not looking for studies of chronically ill patients with major depressive disorder, though some patients undoubtedly could have met this diagnosis. Overall, exercise had a moderate effect on depressive symptoms, with greater effects seen in patients with higher baseline depression scores and in patients who did the exercises regularly. Bottom line: Getting chronically ill patients up on their feet and into exercise programs will decrease their depressive symptoms. The response is greater in patients with higher depression scores and in patients who exercise regularly. These results apply to patients with depressive symptoms in general, not just to patients with major depressive disorder. Herring MP, Puetz TW, O'Connor PJ, Dishman RK. Effect of exercise training on depressive symptoms among patients with a chronic illness. A systematic review and meta-analysis of randomized controlled trials. Arch Intern Med 2012;172(2): #5: Exercise is somewhat effective in relieving symptoms of depression BACKGROUND: Depression is a common and important cause of morbidity and mortality worldwide. Depression is commonly treated with antidepressants and/or psychological therapy, but some people may prefer alternative approaches such as exercise. There are a number of theoretical reasons why exercise may improve depression. This is an update of an earlier review first published in OBJECTIVES: To determine the effectiveness of exercise in the treatment of depression in adults compared with no treatment or a comparator intervention. SEARCH METHODS: We searched the Cochrane Depression, Anxiety and Neurosis Review Group's Controlled Trials Register (CCDANCTR) to 13 July This register includes relevant randomised controlled trials from the following bibliographic databases: The Cochrane Library (all years); MEDLINE (1950 to date); EMBASE (1974 to date) and PsycINFO (1967 to date). We also searched ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform. No date or language restrictions were applied to the search.we conducted an additional search of the CCDANCTR up to 1st March 2013 and any potentially eligible trials not already included are listed as 'awaiting classification.' SELECTION CRITERIA: Randomised controlled trials in which exercise (defined according to American College of Sports Medicine criteria) was compared to standard treatment, no treatment or a placebo treatment, pharmacological treatment, psychological treatment or other active treatment in adults (aged 18 and over) with depression, as defined by trial authors. We included cluster trials and those that randomised individuals. We excluded trials of postnatal depression. DATA COLLECTION AND ANALYSIS: Two review authors extracted data on primary and secondary outcomes at the end of the trial and end of follow-up (if available). We calculated effect sizes for each trial using Hedges' g method and a standardised mean difference (SMD) for the overall pooled effect, using a random-effects model risk ratio for dichotomous data. Where trials used a number of different tools to assess depression, we included the main outcome measureonly in the meta-analysis. Where trials provided several 'doses' of exercise, we used data from the biggest 'dose' of exercise, and performed sensitivity analyses using the lower 'dose'. We performed subgroup analyses to explore the influence of method of diagnosis of depression (diagnostic interview or cut-off point on 19

20 scale), intensity of exercise and the number of sessions of exercise on effect sizes. Two authors performed the 'Risk of bias' assessments. Our sensitivity analyses explored the influence of study quality on outcome. MAIN RESULTS: Thirty-nine trials (2326 participants) fulfilled our inclusion criteria, of which 37 provided data for meta-analyses. There were multiple sources of bias in many of the trials; randomisation was adequately concealed in 14 studies, 15 used intention-to-treat analyses and 12 used blinded outcome assessors. For the 35 trials (1356 participants) comparing exercise with no treatment or a control intervention, the pooled SMD for the primary outcome of depression at the end of treatment was (95% confidence interval (CI) to -0.42), indicating a moderate clinical effect. There was moderate heterogeneity (I² = 63%).When we included only the six trials (464 participants) with adequate allocation concealment, intention-to-treat analysis and blinded outcome assessment, the pooled SMD for this outcome was not statistically significant (-0.18, 95% CI to 0.11). Pooled data from the eight trials (377 participants) providing long-term follow-up data on mood found a small effect in favour of exercise (SMD , 95% CI to -0.03).Twenty-nine trials reported acceptability of treatment, three trials reported quality of life, none reported cost, and six reported adverse events. For acceptability of treatment (assessed by number of drop-outs during the intervention), the risk ratio was 1.00 (95% CI 0.97 to 1.04).Seven trials compared exercise with psychological therapy (189 participants), and found no significant difference (SMD -0.03, 95% CI to 0.26). Four trials (n = 300) compared exercise with pharmacological treatment and found no significant difference (SMD -0.11, -0.34, 0.12). One trial (n = 18) reported that exercise was more effective than bright light therapy (MD -6.40, 95% CI to -2.60).For each trial that was included, two authors independently assessed for sources of bias in accordance with the Cochrane Collaboration 'Risk of bias' tool. In exercise trials, there are inherent difficulties in blinding both those receiving the intervention and those delivering the intervention. Many trials used participant self-report rating scales as a method for post-intervention analysis, which also has the potential to bias findings. AUTHORS' CONCLUSIONS: Exercise is moderately more effective than a control intervention for reducing symptoms of depression, but analysis of methodologically robust trials only shows a smaller effect in favour of exercise. When compared to psychological or pharmacological therapies, exercise appears to be no more effective, though this conclusion is based on a few small trials. Cooney GM, Dwan K, Greig CA, Lawlor DA, Rimer J, Waugh FR, McMurdo M, Mead GE. Exercise for depression. Cochrane Database Syst Rev Sep 12;9:CD doi: / cd pub6. PMID: #6: Telemedicine collaborative care effective for depression Clinical question: Is telemedicine-based collaborative care for the treatment of depression more effective than practice-based collaborative care? Study design: Randomized controlled trial (nonblinded) Setting: Outpatient (primary care) Synopsis: This multicenter randomized controlled trial was conducted at 5 federally qualified health centers without on-site mental health providers. Patients (N = 364) were randomized to receive either practice-based management or telemedicine-based management of depression. Patients were included if they had a positive screening result for depression using the 9-item Patient Health Questionnaire (a score of at least 10) and completed the baseline telephone interview. Patients were excluded if they were cognitively impaired; did not speak English; did not have a phone; were pregnant; had schizophrenia or bipolar disorder, acute suicidal ideation, substance dependence, or a recent bereavement; or were currently in subspecialty mental health treatment. Patients and providers were not masked to treatment arm, but baseline and follow-up interviews at 6, 12 and 18 months for outcomes assessment were masked. Mean baseline depression severity was 1.9 as assessed with the 20-item Hopkins Symptom Checklist (HSCL). Patients also had a mean of 4.6 chronic physical health disorders. Nearly half (48%) were already receiving treatment for depression at enrollment. The article describes the protocol in detail, if you are wondering whether this would be feasible in your practice. There were no significant differences between groups for receiving antidepressant prescriptions, the number of prescribed antidepressants, dosing level, or adherence. The telemedicine group had significantly more encounters. Clinical outcomes were superior in the telemedicine group for treatment response (reduction in HSCL score by at least 50%) with an odds ratio of 7.7. Similarly remissions (reduction in HSCL score to less than 0.5) were greater in the telemedicine group with an odds ratio of The telemedicine group had higher patient satisfaction scores. The authors noted that the telemedicine group received care with more fidelity to the care-management protocol. Bottom line: Telemedicine-based collaborative care was more effective than site-based collaborative care for the treatment of depression. There was greater fidelity to evidence-based treatment guidelines in the telemedicine-based group. Although telemedicinebased care can be considered at least as effective as practice-based collaborative care, replication of this study is indicated before we can say that it is superior. Fortney JC, Pyne JM, Mouden SB, et al. Practice-based vs telemedicine-based collaborative care for depression in rural federally qualified health centers: A pragmatic randomized comparative effectiveness trial. Am J Psychiatry 2013;170(4): #7: Repetitive transcranial magnetic stimulation effective for treatment resistant depression Electroconvulsive therapy (ECT) is the most effective treatment of depression. During the last decades Repetitive Transcranial magnetic stimulation (rtms), an alternative method using electric stimulation of the brain, has revealed possible alternative to ECT in the treatment of depression. There are some clinical trials comparing their efficacies and safeties but without clear conclusions, mainly due to their small sample sizes. In the present study, a meta-analysis had been carried out to gain statistical power. Outcomes were response, remission, acceptability and cognitive effects in depression. Following a comprehensive literature search that included both English and Chinese language databases, we identified all randomized controlled trials that directly compared rtms and ECT for major depression. 10 articles (9 trials) with a total of 425 patients were identified. Methodological quality, heterogeneity, sensitivity and publication bias were systematically evaluated. ECT was superior to high frequency rtms in terms of response (64.4% vs. 48.7%, 20

Essential Evidence Topics 2014. NDAFP 59th Annual Meeting and Scientific Assembly
 Essential Evidence Topics 2014 NDAFP 59th Annual Meeting and Scientific Assembly Learning Objective Discuss recent research important to family physicians for updating their diagnostic and treatment approaches
Essential Evidence Topics 2014 NDAFP 59th Annual Meeting and Scientific Assembly Learning Objective Discuss recent research important to family physicians for updating their diagnostic and treatment approaches
Thrombosis and Hemostasis
 Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
4/9/2015. Risk Stratify Our Patients. Stroke Risk in AF: CHADS2 Scoring system JAMA 2001; 285: 2864-71
 Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
ABOUT XARELTO CLINICAL STUDIES
 ABOUT XARELTO CLINICAL STUDIES FAST FACTS Xarelto (rivaroxaban) is a novel, oral direct Factor Xa inhibitor. On September 30, 2008, the European Commission granted marketing approval for Xarelto for the
ABOUT XARELTO CLINICAL STUDIES FAST FACTS Xarelto (rivaroxaban) is a novel, oral direct Factor Xa inhibitor. On September 30, 2008, the European Commission granted marketing approval for Xarelto for the
Failure or significant adverse effects to all of the alternatives: Eliquis and Xarelto
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
Committee Approval Date: September 12, 2014 Next Review Date: September 2015
 Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Breadth of indications matters One drug for multiple indications
 Breadth of indications matters One drug for multiple indications Sylvia Haas, MD, PhD Formerly of the Technical University of Munich Munich, Germany Disclosures: Sylvia Haas 1 Novel oral anticoagulants:
Breadth of indications matters One drug for multiple indications Sylvia Haas, MD, PhD Formerly of the Technical University of Munich Munich, Germany Disclosures: Sylvia Haas 1 Novel oral anticoagulants:
Review of Non-VKA Oral AntiCoagulants (NOACs) and their use in Great Britain
 and their use in Great Britain") Review of Non-VKA Oral AntiCoagulants (NOACs) and their use in Great Britain Dr Alexander (Ander) Cohen Guy s and St Thomas Hospitals, King s College London, UK Pavia Spring Meeting 13 June 2014 Overview
Review of Non-VKA Oral AntiCoagulants (NOACs) and their use in Great Britain Dr Alexander (Ander) Cohen Guy s and St Thomas Hospitals, King s College London, UK Pavia Spring Meeting 13 June 2014 Overview
Cardiovascular Disease
 Cardiovascular Disease 1 Cardiovascular Disease 1. More target specific oral anticoagulants (TSOAC) 2. Vorapaxar (Zonivity) 3. Continued noise about a polypill 4. WATCHMAN 3 1 2 3 4 Left Atrial Appendage
Cardiovascular Disease 1 Cardiovascular Disease 1. More target specific oral anticoagulants (TSOAC) 2. Vorapaxar (Zonivity) 3. Continued noise about a polypill 4. WATCHMAN 3 1 2 3 4 Left Atrial Appendage
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM
 Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
STROKE PREVENTION IN ATRIAL FIBRILLATION. TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: ABBREVIATIONS: BACKGROUND:
 STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
Antiplatelet and Antithrombotics From clinical trials to guidelines
 Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation
 Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
Bios 6648: Design & conduct of clinical research
 Bios 6648: Design & conduct of clinical research Section 1 - Specifying the study setting and objectives 1. Specifying the study setting and objectives 1.0 Background Where will we end up?: (a) The treatment
Bios 6648: Design & conduct of clinical research Section 1 - Specifying the study setting and objectives 1. Specifying the study setting and objectives 1.0 Background Where will we end up?: (a) The treatment
Therapeutic Class Overview Oral Anticoagulants
 Therapeutic Class Overview Oral Anticoagulants Therapeutic Class Overview/Summary: The oral anticoagulants, dabigatran etexilate mesylate (Pradaxa ), rivaroxaban (Xarelto ), and warfarin (Coumadin, Jantoven
Therapeutic Class Overview Oral Anticoagulants Therapeutic Class Overview/Summary: The oral anticoagulants, dabigatran etexilate mesylate (Pradaxa ), rivaroxaban (Xarelto ), and warfarin (Coumadin, Jantoven
Prior Authorization Guideline
 Guideline Guideline Name Formulary Xarelto (rivaroxaban) UnitedHealthcare Community & State Approval Date 0/0/203 Revision Date 8//204 Technician Note: CPS Approval Date: /5/20; CPS Revision Date: 8/20/204
Guideline Guideline Name Formulary Xarelto (rivaroxaban) UnitedHealthcare Community & State Approval Date 0/0/203 Revision Date 8//204 Technician Note: CPS Approval Date: /5/20; CPS Revision Date: 8/20/204
The author has no disclosures
 Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013
 Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013 Family physician with Rivergrove Medical Clinic Practice in the north end since 1985 Medical Director of the Wellness
Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013 Family physician with Rivergrove Medical Clinic Practice in the north end since 1985 Medical Director of the Wellness
STROKE PREVENTION IN ATRIAL FIBRILLATION
 STROKE PREVENTION IN ATRIAL FIBRILLATION OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention of ischemic stroke and arterial thromboembolism in patients
STROKE PREVENTION IN ATRIAL FIBRILLATION OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention of ischemic stroke and arterial thromboembolism in patients
CDEC FINAL RECOMMENDATION
 CDEC FINAL RECOMMENDATION RIVAROXABAN (Xarelto Bayer Inc.) New Indication: Pulmonary Embolism Note: The Canadian Drug Expert Committee (CDEC) previously reviewed rivaroxaban for the treatment of deep vein
CDEC FINAL RECOMMENDATION RIVAROXABAN (Xarelto Bayer Inc.) New Indication: Pulmonary Embolism Note: The Canadian Drug Expert Committee (CDEC) previously reviewed rivaroxaban for the treatment of deep vein
Novel Anticoagulation Agents DISCLOSURES. Objectives ATRIAL FIBRILLATION TRIALS. NOAC Comparison 6/12/2015
 Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Rivaroxaban A new oral anti-thrombotic Dr. Hisham Aboul-Enein Professor of Cardiology Benha University 12/1/2012
 Rivaroxaban A new oral anti-thrombotic Dr. Hisham Aboul-Enein Professor of Cardiology Benha University 12/1/2012 Agenda Ideal anticoagulant. Drawbacks of warfarin. Rivaroxaban in clinical trails. Present
Rivaroxaban A new oral anti-thrombotic Dr. Hisham Aboul-Enein Professor of Cardiology Benha University 12/1/2012 Agenda Ideal anticoagulant. Drawbacks of warfarin. Rivaroxaban in clinical trails. Present
RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) 3.75
 P=0.051 (superiority) 3.75") ALL-CAUSE MORTALITY RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) Rate per year (%) 5.0 4.0 3.0 2.0 1.0 0 3.64 D150 mg BID 3.75 D110 mg BID RR 0.91 (95% CI: 0.80 1.03) P=0.13 (superiority) 4.13 Warfarin
ALL-CAUSE MORTALITY RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) Rate per year (%) 5.0 4.0 3.0 2.0 1.0 0 3.64 D150 mg BID 3.75 D110 mg BID RR 0.91 (95% CI: 0.80 1.03) P=0.13 (superiority) 4.13 Warfarin
Anticoagulation For Atrial Fibrillation
 Anticoagulation For Atrial Fibrillation New Agents In A New Era Arjun V Gururaj, MD Arrhythmia and Electrophysiology Nevada Heart and Vascular Center Disclosures Biotronik Speaker Clinical investigator
Anticoagulation For Atrial Fibrillation New Agents In A New Era Arjun V Gururaj, MD Arrhythmia and Electrophysiology Nevada Heart and Vascular Center Disclosures Biotronik Speaker Clinical investigator
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation. Joy Wahawisan, Pharm.D., BCPS April 25, 2012
 New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below
 RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below") Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008:
 have been licensed in Ireland since 2008:") Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
Randomized, double-blind, parallel-group, multicenter, doubledummy
 ABOUT RECORD STUDIES FAST FACTS RECORD is a global program of four trials in more than 12,500 patients, comparing Xarelto (rivaroxaban) and enoxaparin in the prevention of venous thromboembolism (VTE)
ABOUT RECORD STUDIES FAST FACTS RECORD is a global program of four trials in more than 12,500 patients, comparing Xarelto (rivaroxaban) and enoxaparin in the prevention of venous thromboembolism (VTE)
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical
 Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
Eliquis. Policy. covered: Eliquis is. indicated to. reduce the. therapy. Eliquis is. superior to. of 32 to. Eliquis is AMPLIFY. nonfatal. physicians.
 Eliquis (apixaban) Policy Number: 5.01.573 Origination: 06/2014 Last Review: 07/2015 Next Review: 07/2016 Policy BCBSKC will provide coverage for Eliquis when it is determined to be medically necessary
Eliquis (apixaban) Policy Number: 5.01.573 Origination: 06/2014 Last Review: 07/2015 Next Review: 07/2016 Policy BCBSKC will provide coverage for Eliquis when it is determined to be medically necessary
New Oral AntiCoagulants (NOAC) in 2015
 in 2015") New Oral AntiCoagulants (NOAC) in 2015 William R. Hiatt, MD Professor of Medicine and Cardiology University of Colorado School of Medicine President CPC Clinical Research Disclosures Received research
New Oral AntiCoagulants (NOAC) in 2015 William R. Hiatt, MD Professor of Medicine and Cardiology University of Colorado School of Medicine President CPC Clinical Research Disclosures Received research
Cardiology Update 2014
 Cardiology Update 2014 Update on the Novel Oral Anticoagulants (NOACS) Raymond Kawasaki, MD AMG Cardiology December 6, 2014 Disclosures I have no disclosures relevant to this presentation Contents I. The
Cardiology Update 2014 Update on the Novel Oral Anticoagulants (NOACS) Raymond Kawasaki, MD AMG Cardiology December 6, 2014 Disclosures I have no disclosures relevant to this presentation Contents I. The
xaban) Policy covered: Coverage of following criteria: the following those who meet the or Hip Xarelto is For those impacted by this policy.
 Policy covered: Coverage of following criteria: the following those who meet the or Hip Xarelto is For those impacted by this policy.") Xarelto (rivarox xaban) Policy Number: 5.01.575 Origination: 06/2014 Last Review: 07/2015 Next Review: 07/2016 Policy BCBSKC will provide coverage for Xarelto when it is determined to be medically necessary
Xarelto (rivarox xaban) Policy Number: 5.01.575 Origination: 06/2014 Last Review: 07/2015 Next Review: 07/2016 Policy BCBSKC will provide coverage for Xarelto when it is determined to be medically necessary
Investor News. Phase III J-ROCKET AF Study of Bayer s Xarelto (rivaroxaban) Meets Primary Endpoint. Not intended for U.S.
 Meets Primary Endpoint. Not intended for U.S.") Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Phase III J-ROCKET AF Study of Bayer s Xarelto (rivaroxaban) Meets Primary Endpoint
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Phase III J-ROCKET AF Study of Bayer s Xarelto (rivaroxaban) Meets Primary Endpoint
Cardiovascular Subcommittee of PTAC Meeting held 27 February 2014. (minutes for web publishing)
") Cardiovascular Subcommittee of PTAC Meeting held 27 February 2014 (minutes for web publishing) Cardiovascular Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Cardiovascular Subcommittee of PTAC Meeting held 27 February 2014 (minutes for web publishing) Cardiovascular Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Are there sufficient indications for switching to new anticoagulant agents
 Are there sufficient indications for switching to new anticoagulant agents Meyer Michel Samama et Gregoris Gerotziafas Groupe Hémostase-Thrombose Hôtel-Dieu, Hôpital Tenon, Paris & Biomnis Ivry/seine,
Are there sufficient indications for switching to new anticoagulant agents Meyer Michel Samama et Gregoris Gerotziafas Groupe Hémostase-Thrombose Hôtel-Dieu, Hôpital Tenon, Paris & Biomnis Ivry/seine,
AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation
 AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation A Statement for Healthcare Professionals from the American Heart Association/American Stroke
AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation A Statement for Healthcare Professionals from the American Heart Association/American Stroke
Anticoagulation in Atrial Fibrillation
 Anticoagulation in Atrial Fibrillation Parag P. Patel, MD FACC Disclosures Eliquis Speakers Bureau 1 Clinical Scenario Ms. L is a 76F admitted to the stroke service with a dense right sided hemiparesis
Anticoagulation in Atrial Fibrillation Parag P. Patel, MD FACC Disclosures Eliquis Speakers Bureau 1 Clinical Scenario Ms. L is a 76F admitted to the stroke service with a dense right sided hemiparesis
Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial
 Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial Camillo Autore Università di Roma Sapienza II Facoltà di Medicina e Chirurgia
Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial Camillo Autore Università di Roma Sapienza II Facoltà di Medicina e Chirurgia
3/25/14. To Clot or Not What s New In Anticoagulation? Clotting Cascade. Anticoagulant drug targets. Anita Ralstin, MS CNS CNP. Heparin.
 To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
Gruppo di lavoro: Malattie Tromboemboliche
 Gruppo di lavoro: Malattie Tromboemboliche 2381 Soluble Recombinant Thrombomodulin Ameliorates Hematological Malignancy-Induced Disseminated Intravascular Coagulation More Promptly Than Conventional Anticoagulant
Gruppo di lavoro: Malattie Tromboemboliche 2381 Soluble Recombinant Thrombomodulin Ameliorates Hematological Malignancy-Induced Disseminated Intravascular Coagulation More Promptly Than Conventional Anticoagulant
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
Medication Policy Manual. Topic: Eliquis, apixaban Date of Origin: July 12, 2013. Committee Approval Date: July 11, 2014 Next Review Date: July 2015
 Medication Policy Manual Policy No: dru313 Topic: Eliquis, apixaban Date of Origin: July 12, 2013 Committee Approval Date: July 11, 2014 Next Review Date: July 2015 Effective Date: August 1, 2014 IMPORTANT
Medication Policy Manual Policy No: dru313 Topic: Eliquis, apixaban Date of Origin: July 12, 2013 Committee Approval Date: July 11, 2014 Next Review Date: July 2015 Effective Date: August 1, 2014 IMPORTANT
rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (755/12) Bayer PLC
 SMC No. (755/12) Bayer PLC") rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (755/12) Bayer PLC 13 January 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (755/12) Bayer PLC 13 January 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
2. Background This indication of rivaroxaban had not previously been considered by the PBAC.
 PUBLIC SUMMARY DOCUMENT Product: Rivaroxaban, tablets, 15mg and 20mg, Xarelto Sponsor: Bayer Australia Ltd Date of PBAC Consideration: March 2013 1. Purpose of Application The application requested the
PUBLIC SUMMARY DOCUMENT Product: Rivaroxaban, tablets, 15mg and 20mg, Xarelto Sponsor: Bayer Australia Ltd Date of PBAC Consideration: March 2013 1. Purpose of Application The application requested the
Abbreviated Class Update: Anticoagulants. Month/Year of Review: July 2014 End date of literature search: June 2014
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
How To Treat Aneuricaagulation
 Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
2/17/2015 ANTICOAGULATION UPDATE OBJECTIVES BRIEF REVIEW: CLASSES OF ORAL ANTICOAGULANTS
 ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis
 New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis Holster IL, Valkhoff VE, Kuipers EJ, Tjwa ET Departments of Gastroenterology and Hepatology,
New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding - A Systematic Review and Meta-Analysis Holster IL, Valkhoff VE, Kuipers EJ, Tjwa ET Departments of Gastroenterology and Hepatology,
The Role of the Newer Anticoagulants
 The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
DATE: 06 May 2013 CONTEXT AND POLICY ISSUES
 TITLE: Low Molecular Weight Heparins versus New Oral Anticoagulants for Long-Term Thrombosis Prophylaxis and Long-Term Treatment of DVT and PE: A Review of the Clinical and Cost-Effectiveness DATE: 06
TITLE: Low Molecular Weight Heparins versus New Oral Anticoagulants for Long-Term Thrombosis Prophylaxis and Long-Term Treatment of DVT and PE: A Review of the Clinical and Cost-Effectiveness DATE: 06
FDA Approved Oral Anticoagulants
 FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (756/12) Bayer PLC
 SMC No. (756/12) Bayer PLC") rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (756/12) Bayer PLC 13 January 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (756/12) Bayer PLC 13 January 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
Bayer Initiates Rivaroxaban Phase III Study to Support Dose Selection According to Individual Benefit-Risk Profile in Long- Term VTE Prevention
 Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Long-term prevention of venous blood clots (VTE): Bayer Initiates Rivaroxaban
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Long-term prevention of venous blood clots (VTE): Bayer Initiates Rivaroxaban
rivaroxaban 15mg and 20mg film-coated tablets (Xarelto ) SMC No. (852/13) Bayer plc
 SMC No. (852/13) Bayer plc") rivaroxaban 15mg and 20mg film-coated tablets (Xarelto ) SMC No. (852/13) Bayer plc 08 February 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
rivaroxaban 15mg and 20mg film-coated tablets (Xarelto ) SMC No. (852/13) Bayer plc 08 February 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM
 NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
WOEST TRIAL- NO ASPIRIN IN STENTED PATIENTS REQUIRING ANTICOAGULATION. Van Crisco, MD, FACC, FSCAI First Coast
 WOEST TRIAL- NO ASPIRIN IN STENTED PATIENTS REQUIRING ANTICOAGULATION Van Crisco, MD, FACC, FSCAI First Coast Conflicts of Interest I have been a paid consultant and speaker for AstraZeneca, makers of
WOEST TRIAL- NO ASPIRIN IN STENTED PATIENTS REQUIRING ANTICOAGULATION Van Crisco, MD, FACC, FSCAI First Coast Conflicts of Interest I have been a paid consultant and speaker for AstraZeneca, makers of
Authors: Partha Sardar MDa; Saurav Chatterjee MDb; Joydeep Ghosh MDc; Debabrata Mukherjee MD, MS d, Gregory Y H Lip MD, FRCP, FACC, FESCe.
 Risk of Major Bleeding in Different Indications for New Oral Anticoagulants: Insights from a Meta- Analysis of Approved Dosages from 48 Randomized Trials Authors: Partha Sardar MDa; Saurav Chatterjee MDb;
Risk of Major Bleeding in Different Indications for New Oral Anticoagulants: Insights from a Meta- Analysis of Approved Dosages from 48 Randomized Trials Authors: Partha Sardar MDa; Saurav Chatterjee MDb;
THE BENEFITS OF RIVAROXABAN (XARELTO ) ACROSS MULTIPLE INDICATIONS AND THE RELEVANCE TO CARDIOLOGISTS
 ACROSS MULTIPLE INDICATIONS AND THE RELEVANCE TO CARDIOLOGISTS") THE BENEFITS OF RIVAROXABAN (XARELTO ) ACROSS MULTIPLE INDICATIONS AND THE RELEVANCE TO CARDIOLOGISTS Ingo Ahrens, Christoph Bode Cardiology and Angiology I, Heart Center Freiburg University, Freiburg,
THE BENEFITS OF RIVAROXABAN (XARELTO ) ACROSS MULTIPLE INDICATIONS AND THE RELEVANCE TO CARDIOLOGISTS Ingo Ahrens, Christoph Bode Cardiology and Angiology I, Heart Center Freiburg University, Freiburg,
Summary Review. Newer Oral Anticoagulant Drugs
 Summary Review Newer Oral Anticoagulant Drugs Final Original Report January 2013 The Agency for Healthcare Research and Quality has not yet seen or approved this report The purpose of reports is to make
Summary Review Newer Oral Anticoagulant Drugs Final Original Report January 2013 The Agency for Healthcare Research and Quality has not yet seen or approved this report The purpose of reports is to make
3/3/2015. Patrick Cobb, MD, FACP March 2015
 Patrick Cobb, MD, FACP March 2015 I, Patrick Cobb, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict
Patrick Cobb, MD, FACP March 2015 I, Patrick Cobb, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict
Antiplatelet and Antithrombotic Therapy. Dr Curry Grant Stroke Prevention Clinic Quinte Health Care
 Antiplatelet and Antithrombotic Therapy Dr Curry Grant Stroke Prevention Clinic Quinte Health Care Disclosure of Potential for Conflict of Interest Dr. F.C. Grant Atrial Fibrillation FINANCIAL DISCLOSURE:
Antiplatelet and Antithrombotic Therapy Dr Curry Grant Stroke Prevention Clinic Quinte Health Care Disclosure of Potential for Conflict of Interest Dr. F.C. Grant Atrial Fibrillation FINANCIAL DISCLOSURE:
1/7/2012. Objectives. Epidemiology of Atrial Fibrillation(AF) Stroke in AF. Stroke Risk Stratification in AF
 Stroke in AF. Stroke Risk Stratification in AF") Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
New Oral Anticoagulants: Topic Brief
 New Oral Anticoagulants: Topic Brief June 9, 2015 High-Level Research Question In patients with nonvalvular atrial fibrillation (AF) or venous thromboembolic disease, or who have undergone surgery for
New Oral Anticoagulants: Topic Brief June 9, 2015 High-Level Research Question In patients with nonvalvular atrial fibrillation (AF) or venous thromboembolic disease, or who have undergone surgery for
TA 256: Rivaroxaban for the prevention of stroke and systemic embolism in people with atrial fibrillation
 Service Notification in response to DHSSPS endorsed NICE Technology Appraisals TA 256: Rivaroxaban for the prevention of stroke and systemic embolism in people with atrial fibrillation 1 Name of Commissioning
Service Notification in response to DHSSPS endorsed NICE Technology Appraisals TA 256: Rivaroxaban for the prevention of stroke and systemic embolism in people with atrial fibrillation 1 Name of Commissioning
Anticoagulation Therapy Update
 Anticoagulation Therapy Update JUDY R. WALLING, FNP-BC ARRHYTHMIA MANAGEMENT MUSC CARDIOLOGY Outline Who do we anticoagulate? Review classes of Anticoagulants Review examples of Anticoagulants Review CHADS2
Anticoagulation Therapy Update JUDY R. WALLING, FNP-BC ARRHYTHMIA MANAGEMENT MUSC CARDIOLOGY Outline Who do we anticoagulate? Review classes of Anticoagulants Review examples of Anticoagulants Review CHADS2
Anticoagulants in Atrial Fibrillation
 Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
Rivaroxaban. Practical Experience in the Cardiology Setting. Bernhard Meier, Bern Bayer Satellite Symposium Cardiology Update Davos February 11, 2013
 Rivaroxaban Practical Experience in the Cardiology Setting Bernhard Meier, Bern Bayer Satellite Symposium Cardiology Update Davos February 11, 2013 Overview of phase III clinical trials of new oral anticoagulants
Rivaroxaban Practical Experience in the Cardiology Setting Bernhard Meier, Bern Bayer Satellite Symposium Cardiology Update Davos February 11, 2013 Overview of phase III clinical trials of new oral anticoagulants
Venous Thromboembolism: Long Term Anticoagulation. Dan Johnson, Pharm.D.
 Venous Thromboembolism: Long Term Anticoagulation Dan Johnson, Pharm.D. Disclosures No financial relationships with products discussed Off-label use of drug therapy always discussed Objectives Review clinical
Venous Thromboembolism: Long Term Anticoagulation Dan Johnson, Pharm.D. Disclosures No financial relationships with products discussed Off-label use of drug therapy always discussed Objectives Review clinical
Goals 6/6/2014. Stroke Prevention in Atrial Fibrillation: New Oral Anti-Coagulants No More INRs. Ashkan Babaie, MD
 Stroke Prevention in Atrial Fibrillation: New Oral Anti-Coagulants No More INRs Ashkan Babaie, MD Arrhythmia Service Providence Heart Clinic June 8 th, 2014 Goals Discuss the data behind approval of NOACs
Stroke Prevention in Atrial Fibrillation: New Oral Anti-Coagulants No More INRs Ashkan Babaie, MD Arrhythmia Service Providence Heart Clinic June 8 th, 2014 Goals Discuss the data behind approval of NOACs
Prevention of stroke in patients with atrial fibrillation
 www.sign.ac.uk Prevention of stroke in patients with atrial fibrillation A guide for primary care January 2014 Evidence Contents 1 Introduction... 1 2 Detection...2 3 Risk stratification... 3 4 Treatment
www.sign.ac.uk Prevention of stroke in patients with atrial fibrillation A guide for primary care January 2014 Evidence Contents 1 Introduction... 1 2 Detection...2 3 Risk stratification... 3 4 Treatment
Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation
 Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation Goal Statement Pharmacists and technicians will gain knowledge in the use of target specific oral anticoagulants
Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation Goal Statement Pharmacists and technicians will gain knowledge in the use of target specific oral anticoagulants
Management for Deep Vein Thrombosis and New Agents
 Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Xarelto (Rivaroxaban)
") Xarelto (Rivaroxaban) Hightly selective, reversible, direct oral FXa inhibitor Maxium concentratiion after 2 to 4 hrs High bioavailability(66%),increase with food ( suggest with food) 1/3 from renal excretion,
Xarelto (Rivaroxaban) Hightly selective, reversible, direct oral FXa inhibitor Maxium concentratiion after 2 to 4 hrs High bioavailability(66%),increase with food ( suggest with food) 1/3 from renal excretion,
Disclosure. New Agents for Treatment of DVT. Prevalence of DVT VTE. Normal Hemostasis 7/17/2015. Mark Oliver, MD, RVT, RPVI,FSVU
 New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
Time of Offset of Action The Trial
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Anticoagulation before and after cardioversion; which and for how long
 Anticoagulation before and after cardioversion; which and for how long Sameh Samir, MD Cardiovascular medicine dept. Tanta faculty of medicine Atrial fibrillation goals of management Identify and treat
Anticoagulation before and after cardioversion; which and for how long Sameh Samir, MD Cardiovascular medicine dept. Tanta faculty of medicine Atrial fibrillation goals of management Identify and treat
Xarelto (Rivaroxaban): Effective in a broad spectrum. Joep Hufman, MD Medical Scientific Liason
: Effective in a broad spectrum. Joep Hufman, MD Medical Scientific Liason") Xarelto (Rivaroxaban): Effective in a broad spectrum Joep Hufman, MD Medical Scientific Liason Xarelto : Effective in a broad spectrum Introduction Therapeutic areas SPAF VTE Prevention VTE treatment Practical
Xarelto (Rivaroxaban): Effective in a broad spectrum Joep Hufman, MD Medical Scientific Liason Xarelto : Effective in a broad spectrum Introduction Therapeutic areas SPAF VTE Prevention VTE treatment Practical
Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation (AF) with one or more risk factors
 with one or more risk factors") News Release For use outside the US and UK only Bayer Pharma AG 13342 Berlin Germany Tel. +49 30 468-1111 www.bayerpharma.com Bayer s Xarelto Approved in the EU for the Prevention of Stroke in Patients
News Release For use outside the US and UK only Bayer Pharma AG 13342 Berlin Germany Tel. +49 30 468-1111 www.bayerpharma.com Bayer s Xarelto Approved in the EU for the Prevention of Stroke in Patients
The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era. CCRN State of the Heart 2012 June 2, 2012
 The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era CCRN State of the Heart 2012 June 2, 2012 Disclosures I have I have been involved in trials of new anticoagulants and have received
The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era CCRN State of the Heart 2012 June 2, 2012 Disclosures I have I have been involved in trials of new anticoagulants and have received
Apixaban Plus Mono vs. Dual Antiplatelet Therapy in Acute Coronary Syndromes: Insights from the APPRAISE-2 Trial
 Apixaban Plus Mono vs. Dual Antiplatelet Therapy in Acute Coronary Syndromes: Insights from the APPRAISE-2 Trial Connie N. Hess, MD, MHS, Stefan James, MD, PhD, Renato D. Lopes, MD, PhD, Daniel M. Wojdyla,
Apixaban Plus Mono vs. Dual Antiplatelet Therapy in Acute Coronary Syndromes: Insights from the APPRAISE-2 Trial Connie N. Hess, MD, MHS, Stefan James, MD, PhD, Renato D. Lopes, MD, PhD, Daniel M. Wojdyla,
NnEeWw DdEeVvEeLlOoPpMmEeNnTtSs IiıNn OoRrAaLl AaNnTtIiıCcOoAaGgUuLlAaTtIiıOoNn AaNnDd RrEeVvEeRrSsAaLl
 NnEeWw DdEeVvEeLlOoPpMmEeNnTtSs IiıNn OoRrAaLl AaNnTtIiıCcOoAaGgUuLlAaTtIiıOoNn AaNnDd RrEeVvEeRrSsAaLl Mikele Wissing, RN June 2014 Introduction until recently, was the unrivaled medication for treatment
NnEeWw DdEeVvEeLlOoPpMmEeNnTtSs IiıNn OoRrAaLl AaNnTtIiıCcOoAaGgUuLlAaTtIiıOoNn AaNnDd RrEeVvEeRrSsAaLl Mikele Wissing, RN June 2014 Introduction until recently, was the unrivaled medication for treatment
New Oral Anticoagulants. How safe are they outside the trials?
 New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
The New Anticoagulants: Which one is for You?
 The New Anticoagulants: Which one is for You? by Hans R. Larsen Although there is no evidence that otherwise healthy lone afibbers have an increased risk of ischemic stroke, it is clear that atrial fibrillation
The New Anticoagulants: Which one is for You? by Hans R. Larsen Although there is no evidence that otherwise healthy lone afibbers have an increased risk of ischemic stroke, it is clear that atrial fibrillation
New Anticoagulants and GI bleeding
 New Anticoagulants and GI bleeding DR DANNY MYERS MD FRCP(C) CLINICAL ASSISTANT PROFESSOR OF MEDICINE, UBC Conflicts of Interest None I am unbiased in the use of NOAC s vs Warfarin based on risk benefit
New Anticoagulants and GI bleeding DR DANNY MYERS MD FRCP(C) CLINICAL ASSISTANT PROFESSOR OF MEDICINE, UBC Conflicts of Interest None I am unbiased in the use of NOAC s vs Warfarin based on risk benefit
New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis. Mark Crowther
 New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis Mark Crowther 1 Disclosures Advisory Boards in last 24 months Pfizer, Alexion, Bayer, CSL Behring,
New Anticoagulants for the Treatment of Thromboembolism With a little subplot on superficial thrombophlebitis Mark Crowther 1 Disclosures Advisory Boards in last 24 months Pfizer, Alexion, Bayer, CSL Behring,
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Rivaroxaban for acute coronary syndromes
 Northern Treatment Advisory Group Rivaroxaban for acute coronary syndromes Lead author: Nancy Kane Regional Drug & Therapeutics Centre (Newcastle) May 2014 2014 Summary Current long-term management following
Northern Treatment Advisory Group Rivaroxaban for acute coronary syndromes Lead author: Nancy Kane Regional Drug & Therapeutics Centre (Newcastle) May 2014 2014 Summary Current long-term management following
The New Kids on the Block: Oral Anticoagulants
 The New Kids on the Block: Oral Anticoagulants Lauren E. Odum, PharmD, BCPS Clinical Assistant Professor UMKC School of Pharmacy at MU April 11, 2014 Objectives Be able to Understand the major trials leading
The New Kids on the Block: Oral Anticoagulants Lauren E. Odum, PharmD, BCPS Clinical Assistant Professor UMKC School of Pharmacy at MU April 11, 2014 Objectives Be able to Understand the major trials leading
Traditional anticoagulants
 TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
Hot Line Session at European Society of Cardiology (ESC) Congress 2014:
 Congress 2014:") Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Hot Line Session at European Society of Cardiology (ESC) Congress 2014: Once-Daily
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Hot Line Session at European Society of Cardiology (ESC) Congress 2014: Once-Daily
New Anticoagulants: When and Why Should I Use Them? Disclosures
 Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Anticoagulation at the end of life. Rhona Maclean Rhona.maclean@sth.nhs.uk
 Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulant therapy
 Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Comparison between New Oral Anticoagulants and Warfarin
 Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
1 Introduction. Walter Ageno 1. demonstrate a broadly favorable benefit risk profile across multiple clinical indications.
 Drugs R D DOI 10.1007/s40268-015-0105-9 REVIEW ARTICLE Rivaroxaban: An Evaluation of its Cardiovascular Benefit Risk Profile Across Indications Based on Numbers Needed to Treat or Harm, and on Clinically
Drugs R D DOI 10.1007/s40268-015-0105-9 REVIEW ARTICLE Rivaroxaban: An Evaluation of its Cardiovascular Benefit Risk Profile Across Indications Based on Numbers Needed to Treat or Harm, and on Clinically
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM OPTIONAL CE ADVANCED LEVEL (EMTP, PHRN, ECRN) August 2013. Anticoagulants
 August 2013. Anticoagulants") MCHENRY WESTERN LAKE COUNTY EMS SYSTEM OPTIONAL CE ADVANCED LEVEL (EMTP, PHRN, ECRN) August 2013 Anticoagulants Anticoagulants are agents that prevent the formation of blood clots. Before we can talk about
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM OPTIONAL CE ADVANCED LEVEL (EMTP, PHRN, ECRN) August 2013 Anticoagulants Anticoagulants are agents that prevent the formation of blood clots. Before we can talk about