Intestinal Obstruction. Mr Ali Al-Sarira
|
|
|
- Toby Lambert
- 7 years ago
- Views:
Transcription
1 Mr Ali Al-Sarira
2 Common medical problem accounts for large percentage of surgical admissions It develops when air and secretions are prevented from passing aborally as a result from either extrinsic or intrinsic compression (i.e. Mechanical Obstruction) or gastrointestinal paralysis (i.e. Nonmechanical Obstruction in the form of ileus or pseudo-obstruction(
3 Classification Dynamic peristalsis working against a mechanical obstruction Adynamic peristalsis may be absent (e.g. paralytic ileus) or it may be present in none propulsive form (e.g. mesenteric vascular occlusion or pseudo-obstruction). In both types mechanical element is absent
4 Epidemiology Small intestinal ileus is the most common form of intestinal obstruction Occurs after most abdominal operations In response to acute extra-abdominal medical conditions and intra-abdominal inflammatory conditions
5 Table 1 - Causes of Ileus Intra-abdominal causes Intraperitoneal problems Peritonitis or abscess Inflammatory condition Mechanical: operation, foreign body Chemical: gastric juice, bile, blood Autoimmune: serositis, vasculitis Intestinal ischemia: arterial or venous, sickle-cell disease Retroperitoneal problems Pancreatitis Retroperitoneal hematoma Spine fracture Aortic operation Renal colic Pyelonephritis Metastasis
6 Causes of Ileus (continue) Extra-abdominal causes Thoracic problems Myocardial infarction Pneumonia Congestive heart failure Rib fractures Metabolic abnormalities Electrolyte imbalance (e.g., hypokalemia) Sepsis Lead poisoning Porphyria Hypothyroidism Hypoparathyroidism Uremia Medicines Drugs: Anticholinergics, Alpha agonists, Antihistamines, Catecholamines, Opiates Spinal cord injury or operations Head, thoracic, or retroperitoneal trauma Chemotherapy, radiation therapy
7 Mechanical small bowel obstruction is somewhat less common Obstruction secondary to adhesions, hernias, or cancer is about 90% of cases Mechanical colonic obstruction accounts for only 10% to 15% of all cases of mechanical obstruction and most often develops in response to obstructing carcinoma, diverticulitis or volvulus
8 Table 2 - Causes of Small Bowel Obstruction in Adults Extrinsic causes Adhesions* Hernias (external, internal [paraduodenal], incisional)* Metastatic cancer* Volvulus Intra-abdominal abscess Intra-abdominal hematoma Pancreatic pseudocyst Intra-abdominal drains Tight fascial opening at stoma Intraluminal causes Tumors* Gallstones Foreign body Worms Bezoars Intramural abnormalities Tumors Strictures Hematoma Intussusception Regional enteritis Radiation enteritis * Approximately 85% of all small bowel obstructions are secondary to adhesions, hernias, or tumors.
9 Table 3 - Causes of Colonic Obstruction Common causes Cancer (primary, anastomotic, metastatic) Volvulus Diverticulitis Pseudo-obstruction Hernia Anastomotic stricture Unusual causes Intussusception Fecal impaction Strictures (from one of the following) Inflammatory bowel disease Endometriosis Radiation therapy Ischemia Foreign body Extrinsic compression by a mass Pancreatic pseudocyst Hematoma Metastasis Primary tumors
10 Methods of classifying Mechanical Intestinal Obstruction (Things to be considered when dealing with patient with mechanical intestinal obstruction) - Acute vs Chronic - Partial vs Complete - Simple vs Closed loop - None Gangrenous (simple) vs Gangrenous (complicated / strangulated) WHY?
11 Natural history of the condition Response to treatment Associated Morbidity and Mortality All vary according to type of obstruction present
12 Partial vs Complete When chyme and gas can traverse the point of obstruction, obstruction is partial only (i.e. portion of the intestinal lumen is occluded)
13 Simple vs Closed loop Simple obstruction results from occlusion of bowel at a single point along the intestinal tract leading to intestinal dilatation, hyper-secretion, and bacterial overgrowth proximal to obstruction and decompression distal to obstruction Closed loop obstruction occurs when segment of bowel is occluded at two points along its course (at both proximal & distal points), while occlusion of segment of bowel at two points along its course by single constrictive lesion that occludes both proximal and distal end of the intestinal loop as well as traps the bowel mesentery called Volvulus
14 None Gangrenous (simple) vs Gangrenous (Complicated / strangulated) When blood supply to closed loop segment of bowel becomes compromised, leading to ischemia and eventually to bowel wall necrosis and perforation, strangulation is present
15 Pathophysiology Irrespective to etiology, in dynamic (mechanical obstruction) Proximal bowel dilates and develops altered motility Distal to obstruction, the bowel exhibits normal peristalsis and absorption until it becomes empty at which point it contracts and becomes immobile Initially proximal peristalsis is increased to overcome obstruction, if obstruction is not relieved, the bowel begins to dilate causing reduction in peristaltic strength ultimately resulting in flaccidity and paralysis
16 Pathophysiology (continue) Distension proximal to obstruction is produced by (1)Gas - Swallowed - Bacterial overgrowth (both aerobic & anaerobic organisms) (2)Fluid - Digestive juices (obstruction simulates intestinal epithelial water secretion and retard absorption) - Swallowed liquids
17 Pathophysiology (continue) Strangulation bowel obstruction When ongoing gas and fluid accumulation, the bowel distends and the intraluminal pressures rise. If pressure becomes high enough, microvascular perfusion to the intestine is impaired, leading to intestinal ischemia, and ultimately necrosis The venous return is impaired before the arterial supply, once arterial supply is impaired, hemorrhagic infarction occurs As viability of the bowel is compromised there is marked translocation and systemic exposure to anaerobic organisms and associated toxins. The morbidity from intraperitoneal strangulation is far greater than with an external hernia, which has a smaller absorptive surface
18 Clinical Features / Dynamic Obstruction Classic Quartet ( Cardinal Clinical Features) of: - Pain - Distension - Vomiting - Constipation The nature of presentation influenced by (1) Level (location) of obstruction - small bowel obstruction (high or low) - large bowel obstruction
19 Clinical Features / Dynamic Obstruction (2) Age of obstruction - Acute usually occurs in small bowel obstruction, with sudden onset of severe colicky central abdominal pain - Chronic usually seen in large bowel obstruction, with lower abdominal colic and absolute constipation - Acute on chronic short history of distension and vomiting against background of pain and constipation - Sub-acute implies an incomplete obstruction
20 Clinical Features / Dynamic Obstruction (3) Underlying pathology (4) Presence or absence of intestinal ischemia - Constant pain - Tenderness and rigidity - Shock
21 Clinical Features / Dynamic Obstruction History Cardinal quartet Previous episodes of bowel obstruction Previous abdominal or pelvic operations Hx of abdominal cancer / radiation Hx of intra-abdominal inflammations Medications e.g. anti- coagulant
22 Clinical Features / Dynamic Obstruction Physical Examination & Resuscitation Assessment of vital signs, hydration status & cardiopulmonary system N/G tube, Foley's catheter & I.V. line insertion Check volume and character of gastric aspirate - Clear gastric outlet obstruction - bilious, none feculent medial to proximal small bowel obstruction - Feculent distal small bowel obstruction
23 Clinical Features / Dynamic Obstruction Physical Examination & Resuscitation Fever? Abscess Abdominal examination Examine for inguinal, femoral, umbilical, and incisional hernias Rectal examination for masses, fecal impaction, and occult blood
24 Laboratory Tests Serum Electrolytes Serum Creatinine Hematocrit Platelet count WBC count Coagulation profile Ileus check electrolytes including Ca, Mg Urine for hematuria
25 Imaging When evaluating Abdominal radiographs Are there abnormally dilated loops of bowel, signs of small bowel dilatation, or air-fluid levels? Are air-fluid levels and bowel loops in the same place on supine and upright films? Is there gas throughout the entire length of the colon (suggestive of ileus or partial mechanical obstruction)?
26 Imaging When evaluating Abdominal radiographs (continue) Is there a paucity of distal colonic gas or an abrupt cutoff of colonic gas with proximal colonic distention and air-fluid levels (suggestive of complete or near-complete colonic obstruction)? Is there evidence of strangulation (e.g., thickened small bowel loops, mucosal thumb printing, pneumatosis cystoides intestinalis, or free peritoneal air)? Is there massive distention of the colon, especially of the cecum or sigmoid (suggestive of either volvulus or pseudo-obstruction)? Are there any biliary or renal calculi, and is there any air in the biliary tree (suggestive of gallstone ileus or a renal stone that could be causing ileus)?
27
28
29
30 Adjunct Tests for Equivocal Situations Sigmoidoscopy / Colonoscopy Water-soluble contrast study / enema Ultrasonography / Computed Tomography Abdominal radiographs can be entirely normal in patients with complete, closed loop, or strangulation obstruction, therefore, other imaging studies has to be done e.g. U/S or CT scan
31 Adjunct Tests for Equivocal Situations U/S Simultaneous observation of distended and collapsed bowel segments Free peritoneal fluid Inspissated intestinal content Paradoxical pendulating peristalsis Highly reflective fluid within bowel lumen Bowel wall edema
32 Adjunct Tests for Equivocal Situations CT scan Ascertain the level of obstruction Assess the severity of obstruction and determine the cause of obstruction Detect closed loop obstruction and early strangulation Detect inflammatory processes Detect small amounts of pneumatosis cystoides intestinalis
33
34
35 CT scan: early closed-loop small bowel obstruction
36 Treatment of Acute Mechanical Intestinal Obstruction Gastrointestinal Drainage Resuscitation / Fluid and Electrolytes replacement THEN
37 Treatment of Acute Mechanical Intestinal Obstruction (continue) Consider Relief of Obstruction and Surgical Treatment (if needed)
38 Treatment of Acute Mechanical Intestinal Obstruction Immediate Operation Urgent Operation Delayed Operation No Operation
39 Situations necessitating emergent operation Incarcerated, strangulated hernias Peritonitis Pneumatosis cystoides intestinalis Pneumoperitoneum Suspected or proven intestinal strangulation Closed-loop obstruction Nonsigmoid colonic volvulus Sigmoid volvulus associated with toxicity or peritoneal signs Complete bowel obstruction
40 Situations necessitating urgent operation Progressive bowel obstruction at any time after nonoperative measures are started Failure to improve with conservative therapy within hr Early postoperative technical complications
41 Situations in which delayed operation is usually safe Immediate postoperative obstruction Sigmoid volvulus successfully decompressed by sigmoidoscopy Acute exacerbation of Crohn disease, diverticulitis, or radiation enteritis Chronic, recurrent partial obstruction Paraduodenal hernia Gastric outlet obstruction Postoperative adhesions Resolved partial colonic obstruction
42 No operation Partial Obstruction secondary to intraabdominal adhesions Immediate postoperative period Inflammatory conditions (IBD, Radiation enteritis, diverticulitis)
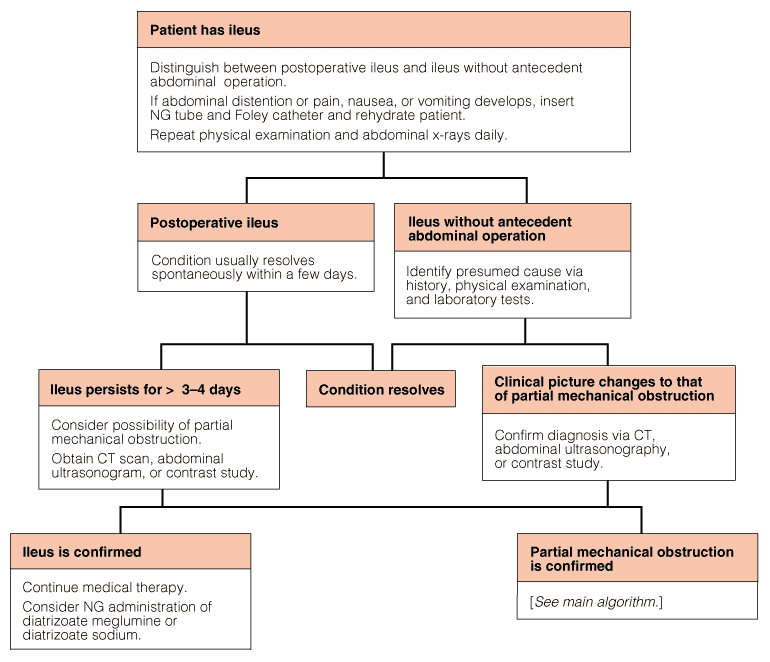
43 Nonmechanical Obstruction Ileus: failure of transmission of peristaltic waves secondary to neuromuscular failure Varieties - Postoperative: usually self limiting hours, prolonged if associated with hypoproteinemia or metabolic abnormality - Infection: intra-abdominal sepsis - Reflex: fractures spine, retroperitoneal hematoma - Metabolic: uremia and hypokalemia
44 Nonmechanical Obstruction Ileus Management - N/G tube gastrointestinal decompression - Restrict oral intake - Maintain electrolyte balance - Remove underlying cause - If prolonged consider laparotomy to exclude hidden cause and facilitate bowel decompression
45
46 Nonmechanical Obstruction Pseudo-obstruction Usually of colon Acute (Ogilvie s syndrome( or chronic Radiograph show evidence of colonic obstruction Caecal distension is common feature Caecal perforation well known complication
47 Nonmechanical Obstruction Pseudo-obstruction Confirm by colonoscopy, water soluble contrast enema or CT scan Treatment Decompression with colonoscopy / flatus tube Tube caecostomy Subtotal colectomy

48
Acute abdominal conditions Key Points
 7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
The Acute Abdomen. Dr. Ed Snyder Dr. Melanie Walker Huntington Memorial Hospital
 The Acute Abdomen Dr. Ed Snyder Dr. Melanie Walker Huntington Memorial Hospital Causes of the Acute Abdomen Hemorrhage in the GI tract Blood vessel GU tract Perforation of the GI tract Ulcer Infection
The Acute Abdomen Dr. Ed Snyder Dr. Melanie Walker Huntington Memorial Hospital Causes of the Acute Abdomen Hemorrhage in the GI tract Blood vessel GU tract Perforation of the GI tract Ulcer Infection
Diseases of peritoneum Lect. Al Qassim University, Faculty of Medicine Phase II Year III, CMD 332 Pathology Department 31-32
 Diseases of peritoneum Lect Al Qassim University, Faculty of Medicine Phase II Year III, CMD 332 Pathology Department 31-32 Describe the etiology, pathogenesis and types of peritonitis Define ascites and
Diseases of peritoneum Lect Al Qassim University, Faculty of Medicine Phase II Year III, CMD 332 Pathology Department 31-32 Describe the etiology, pathogenesis and types of peritonitis Define ascites and
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Colocutaneous Fistula. Disclosures
 Colocutaneous Fistula Madhulika G. Varma MD Associate Professor Chief, Colorectal Surgery University of California, San Francisco Honoraria Applied Medical Covidien Disclosures 1 Colocutaneous Fistula
Colocutaneous Fistula Madhulika G. Varma MD Associate Professor Chief, Colorectal Surgery University of California, San Francisco Honoraria Applied Medical Covidien Disclosures 1 Colocutaneous Fistula
Learning Objectives. Introduction to Medical Careers. Vocabulary: Chapter 16 FACTS. Functions. Organs. Digestive System Chapter 16
 Learning Objectives Introduction to Medical Careers Digestive System Chapter 16 Define at least 10 terms relating to the digestive Describe the four functions of the digestive Identify different structures
Learning Objectives Introduction to Medical Careers Digestive System Chapter 16 Define at least 10 terms relating to the digestive Describe the four functions of the digestive Identify different structures
Bowel Obstruction and Hernia
 Bowel Obstruction and Hernia Geoffrey E. Hayden, MD a, *, Kevin L. Sprouse, DO b KEYWORDS Obstruction Ileus Hernia BOWEL OBSTRUCTION Bowel obstruction accounts for more than 15% of admissions from the
Bowel Obstruction and Hernia Geoffrey E. Hayden, MD a, *, Kevin L. Sprouse, DO b KEYWORDS Obstruction Ileus Hernia BOWEL OBSTRUCTION Bowel obstruction accounts for more than 15% of admissions from the
Acute Abdominal Pain: Other causes
 Acute Abdominal Pain: Other causes Vishal Gupta, MCh Associate Professor Deptt Surg. Gastroenterology KGMU Definition Acute abdominal pain: Presentation of previously undiagnosed abdominal pain Lasting
Acute Abdominal Pain: Other causes Vishal Gupta, MCh Associate Professor Deptt Surg. Gastroenterology KGMU Definition Acute abdominal pain: Presentation of previously undiagnosed abdominal pain Lasting
Abdominal CT scan findings in Acute Appendicitis
 Abdominal CT scan findings in Acute Appendicitis Pathophysiology of acute appendicitis. Acute appendicitis occurs when the lumen is obstructed, leading to fluid accumulation, luminal distention, inflammation
Abdominal CT scan findings in Acute Appendicitis Pathophysiology of acute appendicitis. Acute appendicitis occurs when the lumen is obstructed, leading to fluid accumulation, luminal distention, inflammation
Open the Flood Gates Urinary Obstruction and Kidney Stones. Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke
 Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
Emergencies in Post- Bariatric Surgery Patients
 Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Introduction. Physiology of the Abdomen. Anatomy & Physiology. Abdominal Pain Introduction (2 of 2) Gastrointestional and Urologic Emergencies
 Gastrointestional and Urologic Emergencies") Gastrointestional and Urologic Emergencies Introduction Abdominal pain is a common complaint. Cause of abdominal pain is often difficult to determine. As an EMT: You do not need to determine exact cause.
Gastrointestional and Urologic Emergencies Introduction Abdominal pain is a common complaint. Cause of abdominal pain is often difficult to determine. As an EMT: You do not need to determine exact cause.
Early Colonoscopy in Patients with Acute Diverticulitis Simon Bar-Meir, M.D.
 Early Colonoscopy in Patients with Acute Diverticulitis Simon Bar-Meir, M.D. Professor of Medicine Germanis Kaufman Chair of Gastroenterology Director, Dept. of Gastroenterology Chaim Sheba Medical Center,
Early Colonoscopy in Patients with Acute Diverticulitis Simon Bar-Meir, M.D. Professor of Medicine Germanis Kaufman Chair of Gastroenterology Director, Dept. of Gastroenterology Chaim Sheba Medical Center,
Abdominal Pain. Charles Henley, DO, MPH Department of Family Medicine. OSU College of Osteopathic Medicine (Revised 9/2002)
") Abdominal Pain Charles Henley, DO, MPH Department of Family Medicine OSU College of Osteopathic Medicine (Revised 9/2002) Common Causes of Abdominal Pain Infants - colic, gastroenteritis, constipation,
Abdominal Pain Charles Henley, DO, MPH Department of Family Medicine OSU College of Osteopathic Medicine (Revised 9/2002) Common Causes of Abdominal Pain Infants - colic, gastroenteritis, constipation,
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
Pediatric Upper GI Series New Patient
 Pediatric Upper GI Series New Patient Upper GI Series Thought to be malrotation, no evidence of midgut volvulus Needed to repeat UGI Series WHY? Repeat UGI Series Repeat UGI Series Repeat UGI Series No
Pediatric Upper GI Series New Patient Upper GI Series Thought to be malrotation, no evidence of midgut volvulus Needed to repeat UGI Series WHY? Repeat UGI Series Repeat UGI Series Repeat UGI Series No
Bile Duct Diseases and Problems
 Bile Duct Diseases and Problems Introduction A bile duct is a tube that carries bile between the liver and gallbladder and the intestine. Bile is a substance made by the liver that helps with digestion.
Bile Duct Diseases and Problems Introduction A bile duct is a tube that carries bile between the liver and gallbladder and the intestine. Bile is a substance made by the liver that helps with digestion.
PREPARING FOR YOUR STOMA REVERSAL
 PREPARING FOR YOUR STOMA REVERSAL Information Leaflet Your Health. Our Priority. Page 2 of 6 Introduction- What you need to know As part of your bowel operation you may have had a temporary stoma formed.
PREPARING FOR YOUR STOMA REVERSAL Information Leaflet Your Health. Our Priority. Page 2 of 6 Introduction- What you need to know As part of your bowel operation you may have had a temporary stoma formed.
Intra-abdominal conditions causing colic: How they alter normal physiology and why they result in pain
 Intra-abdominal conditions causing colic: How they alter normal physiology and why they result in pain Nathaniel A. White DVM MS DACVS Author s address: Marion dupont Scott Equine Medical Center, VMRCVM-Virginia
Intra-abdominal conditions causing colic: How they alter normal physiology and why they result in pain Nathaniel A. White DVM MS DACVS Author s address: Marion dupont Scott Equine Medical Center, VMRCVM-Virginia
Open Ventral Hernia Repair
 Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Understanding Laparoscopic Colorectal Surgery
 Understanding Laparoscopic Colorectal Surgery University Colon & Rectal Surgery A Problem with Your Colon Your doctor has told you that you have a colon problem. Now you ve learned that surgery is needed
Understanding Laparoscopic Colorectal Surgery University Colon & Rectal Surgery A Problem with Your Colon Your doctor has told you that you have a colon problem. Now you ve learned that surgery is needed
Colic is one of the most dreaded conditions horse owners and trainers encounter with
 Impaction Colic and Hydration Michele Frazer, DVM, DACVIM, DACVECC Impaction Colic Colic is one of the most dreaded conditions horse owners and trainers encounter with their horses. The term colic, however,
Impaction Colic and Hydration Michele Frazer, DVM, DACVIM, DACVECC Impaction Colic Colic is one of the most dreaded conditions horse owners and trainers encounter with their horses. The term colic, however,
Differential diagnosis of abdominal pain. Lakatos Péter László
 Differential diagnosis of abdominal pain Lakatos Péter László Precise anamnesis Physical examination are prognosticated to the cause of the pain Anamnesis Sudden pain Perforation Mesenteric infarction
Differential diagnosis of abdominal pain Lakatos Péter László Precise anamnesis Physical examination are prognosticated to the cause of the pain Anamnesis Sudden pain Perforation Mesenteric infarction
Cardiovascular diseases. pathology
 Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Guide to Abdominal or Gastroenterological Surgery Claims
 What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
A Left Paraduodenal Hernia Causing Recurrent Small Bowel Obstruction : A Case Report
 Article ID: WMC001308 2046-1690 A Left Paraduodenal Hernia Causing Recurrent Small Bowel Obstruction : A Case Report Corresponding Author: Dr. Prashanth Shetty, Associate Professor, Kasturba Medical College,
Article ID: WMC001308 2046-1690 A Left Paraduodenal Hernia Causing Recurrent Small Bowel Obstruction : A Case Report Corresponding Author: Dr. Prashanth Shetty, Associate Professor, Kasturba Medical College,
Preoperative Laboratory and Diagnostic Studies
 Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Influenza (Flu) Influenza is a viral infection that may affect both the upper and lower respiratory tracts. There are three types of flu virus:
 Influenza is a viral infection that may affect both the upper and lower respiratory tracts. There are three types of flu virus:") Respiratory Disorders Bio 375 Pathophysiology General Manifestations of Respiratory Disease Sneezing is a reflex response to irritation in the upper respiratory tract and is associated with inflammation
Respiratory Disorders Bio 375 Pathophysiology General Manifestations of Respiratory Disease Sneezing is a reflex response to irritation in the upper respiratory tract and is associated with inflammation
GI Bleeding. Thomas S.Foster,Pharm.D. PHR 961 Integrated Therapeutics
 GI Bleeding Thomas S.Foster,Pharm.D. PHR 961 Integrated Therapeutics Overview Because GI bleeding is internal, it is possible for a person to have GI bleeding without symptoms. Important to recognize
GI Bleeding Thomas S.Foster,Pharm.D. PHR 961 Integrated Therapeutics Overview Because GI bleeding is internal, it is possible for a person to have GI bleeding without symptoms. Important to recognize
Chapter 6 Gastrointestinal Impairment
 Chapter 6 Gastrointestinal This chapter consists of 2 parts: Part 6.1 Diseases of the digestive system Part 6.2 Abdominal wall hernias and obesity PART 6.1: DISEASES OF THE DIGESTIVE SYSTEM Diseases of
Chapter 6 Gastrointestinal This chapter consists of 2 parts: Part 6.1 Diseases of the digestive system Part 6.2 Abdominal wall hernias and obesity PART 6.1: DISEASES OF THE DIGESTIVE SYSTEM Diseases of
Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions
 A Simple Guide to Help Answer Your Questions") Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions What are the Colon and Rectum? The colon and rectum together make up the large intestine. After
Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions What are the Colon and Rectum? The colon and rectum together make up the large intestine. After
Constipation in Adults. Abdominal Pain, Acute
 1 Constipation in Adults Abdominal Pain, Acute Abdominal pain is common and often inconsequential. Acute and severe abdominal pain, however, is almost always a symptom of intraabdominal disease. It may
1 Constipation in Adults Abdominal Pain, Acute Abdominal pain is common and often inconsequential. Acute and severe abdominal pain, however, is almost always a symptom of intraabdominal disease. It may
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy. Case Series
 ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
Marginal Ulcers. Marginal Ulcers. Gastric Remnant Ulcers. Double Balloon Enteroscopy. Marginal Ulcer. Gastrojejunal Stricture.
 Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16
 Effective Date: 1/1/2012 Last Update Effective: 4/16") Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
11/10/2014. I have nothing to Disclose. Covered Stents discussed are NOT FDA approved for the indications covered in my presentation
 I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
Advanced Practice Provider Academy
 (+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
(+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
Sonography of Hernias
 Sonography of Hernias Cindy Rapp BS, RDMS, FAIUM, FSDMS Sr. Clinical Marketing Manager Toshiba America Medical Systems Tustin, California What is a hernia? A hernia is a protrusion of an organ or tissue
Sonography of Hernias Cindy Rapp BS, RDMS, FAIUM, FSDMS Sr. Clinical Marketing Manager Toshiba America Medical Systems Tustin, California What is a hernia? A hernia is a protrusion of an organ or tissue
Gallstone Ileus. Audrey C. Durrant,, M.D. SUNY Downstate Medical Center May 20, 2005
 Gallstone Ileus Audrey C. Durrant,, M.D. SUNY Downstate Medical Center May 20, 2005 Gallstone Ileus Diagnosis and Management Background Misnomer coined by Bartolin in 1654 Not a true ileus True mechanical
Gallstone Ileus Audrey C. Durrant,, M.D. SUNY Downstate Medical Center May 20, 2005 Gallstone Ileus Diagnosis and Management Background Misnomer coined by Bartolin in 1654 Not a true ileus True mechanical
Clostridium Difficile Colitis: Treatments, Guidelines, and Challenges
 Clostridium Difficile Colitis: Treatments, Guidelines, and Challenges Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma and Acute Care Surgery
Clostridium Difficile Colitis: Treatments, Guidelines, and Challenges Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma and Acute Care Surgery
Types of Bariatric Procedures. Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012
 Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
KEYHOLE HERNIA SURGERY
 Disclaimer This movie is an educational resource only and should not be used to manage a hernia or abdominal pain. All decisions about the management of a hernia must be made in conjunction with your Physician
Disclaimer This movie is an educational resource only and should not be used to manage a hernia or abdominal pain. All decisions about the management of a hernia must be made in conjunction with your Physician
Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma
 Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma Chapter 50 Abdominal Trauma 1 Describe the epidemiology, including morbidity, mortality rates, and prevention strategies,
Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma Chapter 50 Abdominal Trauma 1 Describe the epidemiology, including morbidity, mortality rates, and prevention strategies,
Lenox Hill Hospital Department of Surgery General Surgery Goals and Objectives
 Lenox Hill Hospital Department of Surgery General Surgery Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate knowledge and application of the pathophysiology and epidemiology
Lenox Hill Hospital Department of Surgery General Surgery Goals and Objectives Medical Knowledge and Patient Care: Residents must demonstrate knowledge and application of the pathophysiology and epidemiology
Gastrointestinal Bleeding
 Gastrointestinal Bleeding Introduction Gastrointestinal bleeding is a symptom of many diseases rather than a disease itself. A number of different conditions can cause gastrointestinal bleeding. Some causes
Gastrointestinal Bleeding Introduction Gastrointestinal bleeding is a symptom of many diseases rather than a disease itself. A number of different conditions can cause gastrointestinal bleeding. Some causes
Urinary tract and perineum
 9 Urinary tract and perineum Key Points 9.1 9.1 THE URINARY BLADDER URINARY RETENTION Acute retention of urine is an indication for emergency drainage of the bladder The common causes of acute retention
9 Urinary tract and perineum Key Points 9.1 9.1 THE URINARY BLADDER URINARY RETENTION Acute retention of urine is an indication for emergency drainage of the bladder The common causes of acute retention
Sample Learning Objectives for a Medical School Radiology Curriculum: Listed by Subjects
 Sample Learning Objectives for a Medical School Radiology Curriculum: Listed by Subjects This document lists sample learning objectives by subject matter The numerical ranking in parenthesis following
Sample Learning Objectives for a Medical School Radiology Curriculum: Listed by Subjects This document lists sample learning objectives by subject matter The numerical ranking in parenthesis following
Management of high output stomas (HOS) Marian Martyn Clinical Nurse Specialist
 Marian Martyn Clinical Nurse Specialist") Management of high output stomas (HOS) Marian Martyn Clinical Nurse Specialist Case History Mr C 50 year old male diagnosed with rectal cancer. He presented to GP with 5 month history of altered bowel
Management of high output stomas (HOS) Marian Martyn Clinical Nurse Specialist Case History Mr C 50 year old male diagnosed with rectal cancer. He presented to GP with 5 month history of altered bowel
CT scans and IV contrast (radiographic iodinated contrast) utilization in adults
 utilization in adults") CT scans and IV contrast (radiographic iodinated contrast) utilization in adults At United Radiology Group, a majority of CT exams are performed either with IV contrast or without while just a few exams
CT scans and IV contrast (radiographic iodinated contrast) utilization in adults At United Radiology Group, a majority of CT exams are performed either with IV contrast or without while just a few exams
DISEASES OF THE DIGESTIVE SYSTEM
 DISEASES OF THE DIGESTIVE SYSTEM DISEASES OF ORAL CAVITY, SALIVARY GLANDS AND JAWS (520-529.9) 520 DISORDERS OF TOOTH DEVELOPMENT AND ERUPTION 520.0 ANODONTIA 520.1 SUPERNUMERARY TEETH 520.2 ABNORMALITIES
DISEASES OF THE DIGESTIVE SYSTEM DISEASES OF ORAL CAVITY, SALIVARY GLANDS AND JAWS (520-529.9) 520 DISORDERS OF TOOTH DEVELOPMENT AND ERUPTION 520.0 ANODONTIA 520.1 SUPERNUMERARY TEETH 520.2 ABNORMALITIES
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
ICD-9-CM coding for patients with Spinal Cord Injury*
 ICD-9-CM coding for patients with Spinal Cord Injury* indicates intervening codes have been left out of this list. OTHER DISORDERS OF THE CENTRAL NERVOUS SYSTEM (340-349) 344 Other paralytic syndromes
ICD-9-CM coding for patients with Spinal Cord Injury* indicates intervening codes have been left out of this list. OTHER DISORDERS OF THE CENTRAL NERVOUS SYSTEM (340-349) 344 Other paralytic syndromes
AORTOENTERIC FISTULA. Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005
 AORTOENTERIC FISTULA Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA diagnosis and management Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA Aortoenteric
AORTOENTERIC FISTULA Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA diagnosis and management Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA Aortoenteric
CT Scheduling Guidelines
 March 2015 1250 S. Cedar Crest Blvd., Suite 100, Allentown, PA 18103 Phone: 610-435-1600; Fax: 610-435-8330 NPI: 1164400131 250 Cetronia Road, Suite 101, Allentown, PA 18104 Phone: 610-674-4940; Fax: 610-674-4944
March 2015 1250 S. Cedar Crest Blvd., Suite 100, Allentown, PA 18103 Phone: 610-435-1600; Fax: 610-435-8330 NPI: 1164400131 250 Cetronia Road, Suite 101, Allentown, PA 18104 Phone: 610-674-4940; Fax: 610-674-4944
Amylase and Lipase Tests
 Amylase and Lipase Tests Also known as: Amy Formal name: Amylase Related tests: Lipase The Test The blood amylase test is ordered, often along with a lipase test, to help diagnose and monitor acute or
Amylase and Lipase Tests Also known as: Amy Formal name: Amylase Related tests: Lipase The Test The blood amylase test is ordered, often along with a lipase test, to help diagnose and monitor acute or
Dept. of Medical Imaging University of Ottawa
 ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
Mikael Petrosyan, Joaquin J. Estrada, Stefano Giuliani, Monica Williams, Heather Rosen, and Rodney J. Mason
 Case Reports in Medicine Volume 2009, Article ID 426162, 4 pages doi:10.1155/2009/426162 Case Report Gastric Perforation and Pancreatitis Manifesting after an Inadvertent Nissen Fundoplication in a Patient
Case Reports in Medicine Volume 2009, Article ID 426162, 4 pages doi:10.1155/2009/426162 Case Report Gastric Perforation and Pancreatitis Manifesting after an Inadvertent Nissen Fundoplication in a Patient
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Ischemia and Infarction
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Hemorrhagic Infarction of the Small Intestine due to Transmesenteric Hernia in an Adolescent: A Case Report
 Korean J Leg Med 2012;36:102-106 Available online at http://www.kjlm.or.kr Case Report http://dx.doi.org/10.7580/koreanjlegmed.2012.36.1.102 Hemorrhagic Infarction of the Small Intestine due to Transmesenteric
Korean J Leg Med 2012;36:102-106 Available online at http://www.kjlm.or.kr Case Report http://dx.doi.org/10.7580/koreanjlegmed.2012.36.1.102 Hemorrhagic Infarction of the Small Intestine due to Transmesenteric
Laparoscopic Repair of Hernias. A simple guide to help answer your questions
 Laparoscopic Repair of Hernias A simple guide to help answer your questions What is a hernia? A hernia is defined as a hole or defect in the abdominal (belly) wall. A hernia can either be congenital (a
Laparoscopic Repair of Hernias A simple guide to help answer your questions What is a hernia? A hernia is defined as a hole or defect in the abdominal (belly) wall. A hernia can either be congenital (a
10 Common Questions Answers SBO
 10 Common Questions Answers SBO 1 What is Small Bowel Obstruction (SBO)? After food passes through our stomach, it soon arrives in our intestines, starting at the small bowel. This tube-like organ meanders
10 Common Questions Answers SBO 1 What is Small Bowel Obstruction (SBO)? After food passes through our stomach, it soon arrives in our intestines, starting at the small bowel. This tube-like organ meanders
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop
 Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers SURGERY
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers SURGERY
Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins.
 Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins.") Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins. LMP of child-bearing age female patients should be checked. 1. Acute abdomen
Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins. LMP of child-bearing age female patients should be checked. 1. Acute abdomen
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Luis D. Carcorze Soto, MD PGY-3
 Luis D. Carcorze Soto, MD PGY-3 Peritoneal Surface Malignancies Peritoneum Patient Selection Operative Technique HIPEC EPIC Primary: Primary Peritoneal Carcinoma Malignant Peritoneal Mesothelioma Metastatic:
Luis D. Carcorze Soto, MD PGY-3 Peritoneal Surface Malignancies Peritoneum Patient Selection Operative Technique HIPEC EPIC Primary: Primary Peritoneal Carcinoma Malignant Peritoneal Mesothelioma Metastatic:
Digestive System AKA. GI System. Overview. GI Process Process Includes. G-I Tract Alimentary Canal
 Digestive System AKA G-I Tract Alimentary Canal Overview GI System Consists of Mouth, pharynx, esophagus, stomach, small intestine, large intestine, anus About 30 in length Accessory Organs Teeth, tongue,
Digestive System AKA G-I Tract Alimentary Canal Overview GI System Consists of Mouth, pharynx, esophagus, stomach, small intestine, large intestine, anus About 30 in length Accessory Organs Teeth, tongue,
Colon Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with COLON CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with COLON CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Consent for Treatment/Procedure Laparoscopic Sleeve Gastrectomy
 Patient's Name: Today's Date: / / The purpose of this document is to confirm, in the presence of witnesses, your informed request to have Surgery for obesity. You are asked to read the following document
Patient's Name: Today's Date: / / The purpose of this document is to confirm, in the presence of witnesses, your informed request to have Surgery for obesity. You are asked to read the following document
Abdominal Pain in the Elderly
 CHAPTER 30 Abdominal Pain in the Elderly S. S. Mehta Abdominal pain is a common presentation in the elderly population. Roughly 5% to 10% of all emergency department visits are for abdominal pain, and
CHAPTER 30 Abdominal Pain in the Elderly S. S. Mehta Abdominal pain is a common presentation in the elderly population. Roughly 5% to 10% of all emergency department visits are for abdominal pain, and
X-ray (Radiography), Lower GI Tract
, Lower GI Tract") Scan for mobile link. X-ray (Radiography), Lower GI Tract What is Lower GI Tract X-ray Radiography (Barium Enema)? Lower gastrointestinal (GI) tract radiography, also called a lower GI or barium enema,
Scan for mobile link. X-ray (Radiography), Lower GI Tract What is Lower GI Tract X-ray Radiography (Barium Enema)? Lower gastrointestinal (GI) tract radiography, also called a lower GI or barium enema,
Inflammation and Healing. Review of Normal Defenses. Review of Normal Capillary Exchange. BIO 375 Pathophysiology
 Inflammation and Healing BIO 375 Pathophysiology Review of Normal Defenses Review of Normal Capillary Exchange 1 Inflammation Inflammation is a biochemical and cellular process that occurs in vascularized
Inflammation and Healing BIO 375 Pathophysiology Review of Normal Defenses Review of Normal Capillary Exchange 1 Inflammation Inflammation is a biochemical and cellular process that occurs in vascularized
GI Bleed. Steven Lichtenstein, D.O. Chief, Division of Gastroenterology Mercy Health System. Director, Endoscopy/GI Lab Mercy Fitzgerald Hospital
 October 3, 2015 GI Bleed Steven Lichtenstein, D.O. Chief, Division of Gastroenterology Mercy Health System Director, Endoscopy/GI Lab Mercy Fitzgerald Hospital Clinical Associate Professor of Medicine
October 3, 2015 GI Bleed Steven Lichtenstein, D.O. Chief, Division of Gastroenterology Mercy Health System Director, Endoscopy/GI Lab Mercy Fitzgerald Hospital Clinical Associate Professor of Medicine
Evaluation of Acute Abdominal Pain in Adults
 Evaluation of Acute Abdominal Pain in Adults Sarah L. Cartwright, MD, and Mark P. Knudson, MD, MSPH Wake Forest University School of Medicine, Winston-Salem, North Carolina Acute abdominal pain can represent
Evaluation of Acute Abdominal Pain in Adults Sarah L. Cartwright, MD, and Mark P. Knudson, MD, MSPH Wake Forest University School of Medicine, Winston-Salem, North Carolina Acute abdominal pain can represent
Simple appendicitis: Complicated appendicitis: Sympathetic nervous system Vague abdominal pain
 Appendicitis: When simple becomes not so simple Appendicitis: When simple becomes not so simple Elizabeth H. Ey, MD Associate Clinical Professor of Pediatrics Department of Medical Imaging Dayton Children
Appendicitis: When simple becomes not so simple Appendicitis: When simple becomes not so simple Elizabeth H. Ey, MD Associate Clinical Professor of Pediatrics Department of Medical Imaging Dayton Children
Abdominal Pain. Learning Objectives:
 Abdominal Pain Learning Objectives: Knowledge At the end of the subinternship, the subinterns should be able to: Describe the common causes of abdominal pain in hospitalized patient including o Intestinal
Abdominal Pain Learning Objectives: Knowledge At the end of the subinternship, the subinterns should be able to: Describe the common causes of abdominal pain in hospitalized patient including o Intestinal
Chronic abdominal pain of childhood
 Chronic abdominal pain of childhood Sandra I. Escalera, M.D. ProHealth Physicians Associate Clinical Professor Department of Pediatrics Yale University School of Medicine Objectives Brief overview of approach
Chronic abdominal pain of childhood Sandra I. Escalera, M.D. ProHealth Physicians Associate Clinical Professor Department of Pediatrics Yale University School of Medicine Objectives Brief overview of approach
Adynamic Ileus and Acute Colonic Pseudo-obstruction Occurring After Cesarean Section in Patients With Massive Peripartum Hemorrhage
 CASE REPORT Adynamic Ileus and Acute Colonic Pseudo-obstruction Occurring After Cesarean Section in Patients With Massive Peripartum Hemorrhage Fu-Nan Cho*, Cheng-Bin Liu, Ju-Yueh Li, San-Nung Chen, Ken-Jen
CASE REPORT Adynamic Ileus and Acute Colonic Pseudo-obstruction Occurring After Cesarean Section in Patients With Massive Peripartum Hemorrhage Fu-Nan Cho*, Cheng-Bin Liu, Ju-Yueh Li, San-Nung Chen, Ken-Jen
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Spinal Cord and Bladder Management Male: Intermittent Catheter
 Spinal Cord and Bladder Management Male: Intermittent Catheter The 5 parts of the urinary system work together to get rid of waste and make urine. Urine is made in your kidneys and travels down 2 thin
Spinal Cord and Bladder Management Male: Intermittent Catheter The 5 parts of the urinary system work together to get rid of waste and make urine. Urine is made in your kidneys and travels down 2 thin
What to Expect from Intestinal Ultrasonography
 261) What to Expect from Intestinal Ultrasonography Červenková J., Steyerová P. Charles University in Prague, First Faculty of Medicine and General Teaching Hospital, Department of Radiology, Prague, Czech
261) What to Expect from Intestinal Ultrasonography Červenková J., Steyerová P. Charles University in Prague, First Faculty of Medicine and General Teaching Hospital, Department of Radiology, Prague, Czech
Gastrointestinal bleeding
 Gastrointestinal bleeding..is the reason in 2 % of all admissions to hospital 85.000 cases/year in the US. The incidence of urgent upper GI bleeding: 145/100.000 inhabitant/year in Hungary ( Nagy Gy. MBA
Gastrointestinal bleeding..is the reason in 2 % of all admissions to hospital 85.000 cases/year in the US. The incidence of urgent upper GI bleeding: 145/100.000 inhabitant/year in Hungary ( Nagy Gy. MBA
What Is Clostridium Difficile (C. Diff)? CLOSTRIDIUM DIFFICILE (C. DIFF)
? CLOSTRIDIUM DIFFICILE (C. DIFF)") What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium, or bug, that can grow in your intestines and cause bad GI symptoms. The main risk
What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium, or bug, that can grow in your intestines and cause bad GI symptoms. The main risk
Intra-abdominal abdominal Infections
 Intra-abdominal abdominal Infections Marnie Peterson, Pharm.D., BCPS Dept. of Pediatric Infectious Diseases Medical School University of Minnesota Intra-abdominal abdominal Infections Intra-abdominal abdominal
Intra-abdominal abdominal Infections Marnie Peterson, Pharm.D., BCPS Dept. of Pediatric Infectious Diseases Medical School University of Minnesota Intra-abdominal abdominal Infections Intra-abdominal abdominal
Gallbladder Diseases and Problems
 Gallbladder Diseases and Problems Introduction Your gallbladder is a pear-shaped organ under your liver. It stores bile, a fluid made by your liver to digest fat. There are many diseases and problems that
Gallbladder Diseases and Problems Introduction Your gallbladder is a pear-shaped organ under your liver. It stores bile, a fluid made by your liver to digest fat. There are many diseases and problems that
MR Imaging of Peritoneal Malignancy Russell N. Low, MD
 MR Imaging of Peritoneal Malignancy Russell N. Low, MD From: Sharp and Children's MRI Center and Sharp HealthCare, 7901 Frost Street, San Diego, California, 92123. Phone: (858) 939-3600. Email: rlow@ucsd.edu
MR Imaging of Peritoneal Malignancy Russell N. Low, MD From: Sharp and Children's MRI Center and Sharp HealthCare, 7901 Frost Street, San Diego, California, 92123. Phone: (858) 939-3600. Email: rlow@ucsd.edu
Patient information regarding care and surgery associated with ULCERATIVE COLITIS
 Patient information regarding care and surgery associated with ULCERATIVE COLITIS by: Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou, M.D. location: Michigan Heart & Vascular Institute,
Patient information regarding care and surgery associated with ULCERATIVE COLITIS by: Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou, M.D. location: Michigan Heart & Vascular Institute,
Substandard Underwriting Structured Settlements
 Substandard Underwriting Structured Settlements Structures 101-Back to Basics February 20-22, 2013 Las Vegas, Nevada Rosemary Brindamour BSN CSSC Chief Medical Underwriter Structured Settlement Underwriting
Substandard Underwriting Structured Settlements Structures 101-Back to Basics February 20-22, 2013 Las Vegas, Nevada Rosemary Brindamour BSN CSSC Chief Medical Underwriter Structured Settlement Underwriting
By Anne C. Travis, M.D., M.Sc. and John R. Saltzman, M.D., FACG Brigham and Women's Hospital Harvard Medical School Boston, MA
 SMALL BOWEL BLEEDING: CAUSES, DIAGNOSIS AND TREATMENT By Anne C. Travis, M.D., M.Sc. and John R. Saltzman, M.D., FACG Brigham and Women's Hospital Harvard Medical School Boston, MA 1. What is the small
SMALL BOWEL BLEEDING: CAUSES, DIAGNOSIS AND TREATMENT By Anne C. Travis, M.D., M.Sc. and John R. Saltzman, M.D., FACG Brigham and Women's Hospital Harvard Medical School Boston, MA 1. What is the small
ABDOMINAL PAIN CHAPTER 14. John T. Boyle, MD ACUTE ABDOMINAL PAIN
 CHAPTER 14 ABDOMINAL PAIN John T. Boyle, MD ACUTE ABDOMINAL PAIN Acute abdominal pain is a popular descriptor that has evolved from the seminal definition by Sir Zachary Cope of abdominal pain of recent
CHAPTER 14 ABDOMINAL PAIN John T. Boyle, MD ACUTE ABDOMINAL PAIN Acute abdominal pain is a popular descriptor that has evolved from the seminal definition by Sir Zachary Cope of abdominal pain of recent
Overview of Bariatric Surgery
 Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Interpretation of Laboratory Values
 Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Common Pathology Diagnoses: ICD-9 to ICD-10 Mapping
 PERFORMANCE THAT MATTERS NUMBER OF CODES 14,000 69,000 ICD-9 DIAGNOSIS CODES ICD-10 DIAGNOSIS CODES CODE STRUCTURE ICD-9-CM CODE FORMAT ICD-10-CM CODE FORMAT X X X X X X X X X X X X CATEGORY ETIOLOGY,
PERFORMANCE THAT MATTERS NUMBER OF CODES 14,000 69,000 ICD-9 DIAGNOSIS CODES ICD-10 DIAGNOSIS CODES CODE STRUCTURE ICD-9-CM CODE FORMAT ICD-10-CM CODE FORMAT X X X X X X X X X X X X CATEGORY ETIOLOGY,
WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS
 WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS This is a patient information booklet providing specific practical information about gall bladder polyps in brief. Its aim is to provide the patient
WHAT S WRONG WITH MY GALL BLADDER? GALL BLADDER POLYPS This is a patient information booklet providing specific practical information about gall bladder polyps in brief. Its aim is to provide the patient
TPN/ Enteral nutrition. Salsabil HADIRE Dietitian in Oncology Hematology Center of University Hospital Mohammed VI Marrakech-
 TPN/ Enteral nutrition Salsabil HADIRE Dietitian in Oncology Hematology Center of University Hospital Mohammed VI Marrakech- Work plan Part 1: Total Parenteral Nutrition (TPN) Part 2: Enteral Nutrition
TPN/ Enteral nutrition Salsabil HADIRE Dietitian in Oncology Hematology Center of University Hospital Mohammed VI Marrakech- Work plan Part 1: Total Parenteral Nutrition (TPN) Part 2: Enteral Nutrition
Home Health Care ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Home Health Care and Top 20 codes
 Home Health Care ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Home Health Care and Top 20 codes Chapter 4: Endocrine, Nutritional and Metabolic Diseases (E00-E99) ICD-10-CM diabetes mellitus
Home Health Care ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Home Health Care and Top 20 codes Chapter 4: Endocrine, Nutritional and Metabolic Diseases (E00-E99) ICD-10-CM diabetes mellitus
2016 Quick Reference Coding Chart
 43197 Trans nasal esophagoscopy 43198 Biospy Trans Nasal Esophagoscopy Esophagoscopy 43200 Esophagoscopy Includes collection of specimen(s) by brushing or washing, when performed. 43201 Submucosal injection
43197 Trans nasal esophagoscopy 43198 Biospy Trans Nasal Esophagoscopy Esophagoscopy 43200 Esophagoscopy Includes collection of specimen(s) by brushing or washing, when performed. 43201 Submucosal injection