Improving Transitions of Care Project BOOST and more
|
|
|
- Arlene Flowers
- 7 years ago
- Views:
Transcription

1 Improving Transitions of Care Project BOOST and more Greg Maynard MD, MSc Clinical Professor of Medicine Director, Center for Innovation and Improvement Science University of California, San Diego CMO, Society of Hospital Medicine NSW Ministry of Health Master Class Thursday, November 14 th, 2013
2 Transforming the Health Care System, Why?
3 Every system is perfectly designed to get the results it gets. - Dr. Paul Batalden

4 Why Patients Get Readmitted: A Adapted from Chris Kim, MD RCA On Admission: Poor communication with prior providers Redundant testing Inadequate medication information Limited efforts to identify risks and barriers to successful transition During Hospitalization: Poor communication among members of care team, including outpatient Delays in initiating interventions to improve transitions Insufficient involvement of patient/caregiver in discharge education/plan Failures to clarify goals of care Post-Discharge: Little/Late/No contact with patient post-discharge (hospital/pcp or other caregiver) Patients/caregivers unaware of how to manage acute problems LIFE HAPPENS (social, financial, logistical, clinical barriers) At Discharge: Appointments made when patient/caregiver cannot attend Discharge instructions cumbersome Inadequate information handoffs Error prone med rec Rushed education
5 Discharge Care Transitions ER visits Information loss Patient dissatisfaction Clinical deterioration Insufficient services Adverse drug events Inability to access care Inappropriate site of care Readmissions Lack of engagement
6 Traditional Care Transitions Poor communication Nonstandardized care Patient issues System failures Patients Hard work Adverse events Smart caregivers Good intentions Invested patients Modified from Reason, J. BMJ 2000
7 A Brief Primer on BOOST 2006 to SHM from the John A. Hartford Foundation. Better Outcomes for Older Adults Through Safe Transitions Identifies risk factors for failed discharge care transitions, standardizes interventions, improves patient preparation for discharge, and ensures access to appropriate and timely aftercare. Mentored implementation Initial 6 sites enrolled 2008 Now over 200 sites Partnerships with Beacon, BC/BS, QIOs Better Outcomes by Optimizing Safe Transitions
8 Key Components of BOOST Toolkit Standardized Risk Assessment: Tool for Identification of High Risk Patients (8Ps) Patient-centered Preparation for Discharge Checklists- GAP, Universal Patient Checklist Use of Teachback Technique Medication Reconciliation Patient-friendly discharge forms Principal Care Provider identification Who to contact with questions/concerns Warning signs/symptoms and how to respond Outpatient appointments Pending tests Standardized PCP communication 72 hour follow-up call for high risk patients Mentored Implementation
9
10 What It Means to Be BOOST! Official BOOST Sites get: Kickoff training (2-day) Access to free and firewalled resources months of mentorship Longitudinal 1:1 coaching, access Group webinars Robust community Data and Reporting Center A site visit
11 BOOST Tools/Resources Tools Risk assessment tool Discharge preparedness assessment Patient-centered discharge education tools Teach Back Resources Workbook Data collection tools Webinars Listserv access Online community Web-based resources ROI calculator Newsletters Teach Back Curriculum Mentors
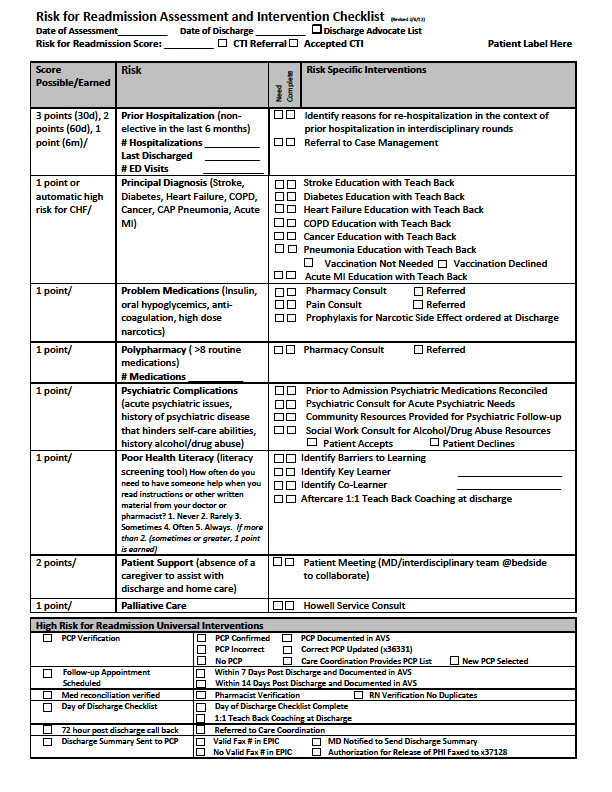
12 8P Risk Assessment Prior hospitalization Problem medications Psychological Principal diagnosis Polypharmacy Poor health literacy Patient support Palliative Care IDENTIFY MITIGATE COMMUNICATE
13
14 Interventions to mitigate risk GENERAL Early follow up, making appointment in conjunction with patient Follow up phone call within 24 hours Teach back RISK-SPECIFIC Pharmacy / medication management consultation for polypharmacy of problem medications Triggering pre-existing protocols (eg, make sure CHF discharge module is utilized)
15 NEW CONCEPT: Health information, advice, instructions, or change in management The Teach Back Method Assess patient comprehension / Ask patient to demonstrate Explain new concept / Demonstrate new skill Patient recalls and comprehends / Demonstrates skill mastery Clarify and tailor explanation Adherence / Error reduction Re-assess recall and comprehension / Ask patient to demonstrate Modified from Schillinger, D. et al. Arch Intern Med 2003;163:83-90
16 The General Assessment of Preparedness: The GAP Caregivers and social support circle for patient Functional status evaluation completed Cognitive status assessed Abuse/neglect Substance abuse Advanced care planning addressed and documented On Admission Functional status Cognitive status Access to meds Responsible party for ensuring med adherence prepared Home preparation for patient s arrival Financial resources for care needs Transportation home Access (e.g. keys) to home Nearing Discharge Understanding of dx, treatment, prognosis, followup and postdischarge warning S/S (using Teach Back) Transportation to initial follow-up At Discharge
17 Patient-friendly Discharge Document Form, plus a patient-centered med list, goes home with the patient Use as guide for discharge teaching Includes several key components: Hospital Diagnosis Warning signs F/u information Who to contact with issues
18
19 BOOST tools are not intended to worn right off the rack. They are to be tailored to your own institutional needs and resources.
20 Does it work? Volunteer sample of 11 out of 30 hospitals Vary in geography, size and academic affiliation Pre-post changes in same hospital readmission rates BOOST vs Control Units BOOST unit readmission rate: 14.7% to 12.7% in 12 months Relative reduction of 13.6% No change in control units (14.0 vs 14.1%) Hansen et al, JHM 2013

21 Readmission Rate (Illinois Cohort) * 7 th hospital s control unit had less than 10 monthly discharges and not included in the analysis. All units included in analysis had 60 or more monthly discharges. Preliminary

22 Readmission Rate (Illinois Cohort) 25% Decrease * 7 th hospital s control unit had less than 10 monthly discharges and not included in the analysis. All units included in analysis had 60 or more monthly discharges. Preliminary
23 Who We Are UC San Diego Health System The only academic health system in San Diego 2 campuses, totaling 600 beds Level I Trauma Center Certified Stroke Center Magnet Hospital Named one of the nation s Most Wired for the sixth consecutive year in 2011 Employees 850 physicians 2500 nurses Fiscal 2011 year key statistics 61,446 ED visits 25,742 discharges 54,013 total outpatient visits Project BOOST
24 UC San Diego Transitions of Care Efforts BOOST Framework PLUS CTI (Care Transitions Intervention) CCTP (Community Based Care Transitions Program) Medication Management
25 Building a BOOST Team C-suite, PO/PHO, ambulatory care leadership, hospital/board QI committee Project Leader & Mgr, QI/PI, RN, CM, SW, PharmD, IT/data, Doctor (inpt & outpt), Advanced Practice Provider Advisory Board Core BOOST Team Ad Hoc Members Schedulers, pt education, unit secretary, VNA, financial, patient and caregiver, hospice, SNF Subgroup Subgroup Subgroup Subgroup
26 Arch Intern Med 2006 Elderly patients transitioning to SNF/home Randomized: Intervention group paired with Transition Coach (TC) vs. standard care Empowerment and education: 4 pillars Facilitate self management/adherence Maintain a personal health record Timely follow-up Knowledge and management of complications Education during hospitalization including meds and med reconciliation Phone calls and personal visits by TC post discharge N=750
27 Copyright restrictions may apply. Coleman, E. A. et al. Arch Intern Med 2006

28 The Care Transition Coach Key Attributes of a CTI Coach Model & Facilitate New Behaviors & Skills Promote Patient Self-Activation Competent in Medication Review & Reconciliation Bridge between Staff and the Patient and/or Family
29 Key Elements of the Care Transitions Intervention (CTI) Referral Process Hospital Visit Phone call to patient after discharge from hospital Home visit within 2 days after discharge Phone calls to patient 7 days and 14 days after the home visit Enhanced CTI will provide additional services to a subset of patients
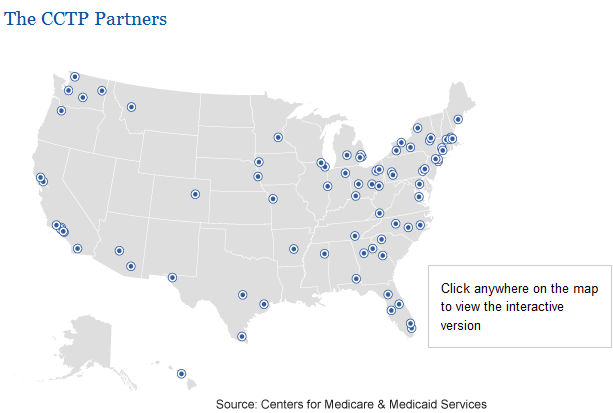
30 Community-based Care Transitions Partnership (CCTP) Mandated from the Affordable Care Act Part of larger Partnerships for Patients initiative Goals- improve patient care, reduce cost, reduce readmissions by 20% Target population - High Risk Medicare FFS inpatients $500 million in funding from Community Based Organizations (CBO) partner with hospitals and others in community Competitive process to obtain funding Currently 82 groups funded after four rounds
31
32 County AIS, Scripps, Sharp, Palomar, UCSD 11 hospitals targeting over 21,000 high risk patients UCSD interventions Phone call, medication management, Transition Nurse Specialist AIS Interventions Care Transitions Intervention (CTI), Enhanced CTI
33 Transitions Nurse Specialist (TNS) Blended role: nurse educator, case manager, community health nurse Bridge patients from inpatient to outpatient Available to patients for up to 30 days post discharge Manages high risk patient populations Average daily caseload of 8 patients
34 Transitions Nurse Specialist Daily Workflow Receives list of patients who are high risk (captured in PADB and Epic report) Uses Project BOOST 8 P s as a tool: In-depth patient/family interview, assessment Develops patient-centered discharge plan Uses teach back for patient/family education Communicates discharge plans and patient education needs with physician and multidisciplinary team Arranges post-discharge follow up appointment with primary care physician Communicates important updates with patient s primary care provider Reviews discharge instructions with patients Requests additional interventions, as appropriate: Pharmacy CTI Coach
35 Patient Follow Up Post Discharge Completes follow up phone call within 72 hours on a subset of patients Reviews Discharge Summary with patients: Reason for admission, medications, follow up appointments, and red flags that would require follow up Provides number to call should patient have questions/concerns Refers any questions or concerns to patient s primary care provider, as appropriate
36 Additional Interventions: CTI Transition Coach (provided by community partner) On identified subset of patients Hospital visit Personal Health Record Home visit Follow up phone calls CTI Advanced intervention Homemaker, personal care attendants, transportation Communicates any concerns or problems to UC San Diego Transition Nurse Specialist (TNS)
37 Pharmacist Interventions Pharmacist-performed medication reconciliation and patient education in the inpatient setting: Decreases errors Improves patient drug knowledge Reduces readmission rates Pharmacist interventions in the outpatient setting: Reduce readmissions Reduce mortality Increase adherence Increase medication knowledge Source: Al-Rashed et al. J Clin Pharmacol Murphy et al. Am J Health-Syst Pharm Ponniah et al. Journal of Clinical Pharmacy and Therapeutics Anderson et al. CHF

38 Transitional Care Pharmacist Model Admission/Inpatient Medication reconciliation Interdisciplinary rounds Address adherence/compliance to medications Discharge Medication reconciliation Medication education with patient friendly tools Coordination of medication acquisition Post Discharge 48 hour telephone follow-up 7-day clinic visit

39 Transitions of Care: Medication Management Program Medication Reconciliation Admission Discharge Discharge counseling with MedAction Plan Post discharge follow up hour phone call +/- 7 day clinic visit

40 Pilot results: Point of Pharmacist Intervention Follow Up Visit 7% Other 1% Admission: 38% Discharge Counseling 5% Follow Up Phone Call 17% Admission Med Rec 38% Discharge: 37% Post Discharge: 25% Discharge Med Rec 32% N=131
41 UCSD Hillcrest 6-East/6-West (BOOST Pilot Unit) 30-day Readmission Rates
42 UC San Diego Cardiology Services 30 day readmission rates Baseline Heart Failure Readmission Rate 36.1% (May 2010 April 2011) Current Heart Failure Readmission Rate 17.9%
43 UCSD Hospital Medicine Services 7 day readmission rates
44 DC Summaries Hospital Medicine UC San Diego Hospital Medicine Service Lines 100.0% Discharge Summaries Signed within 48 hours of Discharge September August % 80.0% 70.0% 60.0% 50.0% DY9 (FY13-14) Target is 90%. DY9 YTD 93.1% 40.0% 30.0% 20.0% September '12 October '12 November '12 December '12 January '13 February '13 March '13 April '13 May '13 June '13 July '13 August '13 FY YTD Total DC Summaries Hospital Medicine Dc Summaries win 48 hrs Percent 89.5% 94.9% 93.4% 92.9% 96.7% 94.2% 94.0% 94.9% 93.1% 95.0% 94.7% 91.1% 93.1% * Baseline data - 7/1/2011-6/30/2012
45 Lessons Learned Transitions in Care are not medical events Responsibility for the patient does not disappear when the patient disappears The entire continuum of care needs to be committed to improving transitions of care Focus on the patient not the disease Executive Support
46 Keep the patient at the center Vision Provide best quality service to all patients, regardless of payer Go outside of boundaries to accommodate our patients CCTP / CTI give us payment mechanism and opportunities to collaborate If you aren t part of the solution.. Identify, mitigate, communicate
47 BOOST Future State Adapted from Chris Kim, MD On Admission: Readmission risk factor screen Discharge needs analysis General assessment of preparedness Medication reconciliation Input from outpatient caregivers Readmit RCA (if needed) During Hospitalization: Interprofessional rounds to develop patient-centered, safe transition plan Initiate readmission risk reduction interventions Educate patient & caregiver using Teach Back Clarify goals of care Post-Discharge: Post-discharge call Follow-up appointment Transmit accurate discharge summary Family/caregiver support Appropriate services Transitional support At Discharge: Schedule post-discharge appointment Patient friendly discharge instructions Handoffs (hospital to aftercare) Medication reconciliation Reinforce education
48 Modified from Reason, J. BMJ 2000;320 Improved Care Transitions Effective communication Standardized care Patient-centered care System support Patients Hard work Adverse events Smart caregivers Good intensions Invested patients
49 The Future is Coming


50 Greg Maynard MD, MSc, SFHM

51 Thank you
RED, BOOST, and You: Improving the Discharge Transition of Care
 RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
Risk Assessment Model
 Transitions of Care and Readmissions Focus on Risk Assessment (and what to do with results) Greg Maynard MD, MSc Clinical Professor of Medicine, Division of Hospital Medicine Director, UCSD Center for
Transitions of Care and Readmissions Focus on Risk Assessment (and what to do with results) Greg Maynard MD, MSc Clinical Professor of Medicine, Division of Hospital Medicine Director, UCSD Center for
March 19, 2008 Team San Diego GMU Module 1 Draft 2
 2 March 19, 2008 Team San Diego GMU Module 1 Draft 2 2 THE LEVEL OF COMPETITION THE LEVEL OF COOPERATION White Space (No Network) Love-Fest Rumble in the Jungle Co-opetition (San Diego County) Community-based
2 March 19, 2008 Team San Diego GMU Module 1 Draft 2 2 THE LEVEL OF COMPETITION THE LEVEL OF COOPERATION White Space (No Network) Love-Fest Rumble in the Jungle Co-opetition (San Diego County) Community-based
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Implementing an Evidence Based Hospital Discharge Process
 Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP
 THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP Transforming Care Across the Continuum Julianne R. Howell, Ph.D. Senior Health Policy Advisor County of San Diego Health and Human Services Agency SAN DIEGO COUNTY
THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP Transforming Care Across the Continuum Julianne R. Howell, Ph.D. Senior Health Policy Advisor County of San Diego Health and Human Services Agency SAN DIEGO COUNTY
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Relative patient benefits of a hospital-pcmh collaboration within an ACO to improve care transitions:
 Relative patient benefits of a hospital-pcmh collaboration within an ACO to improve care transitions: Lessons learned from the PCORI grant application experience Jeffrey L. Schnipper, MD, MPH, FHM Director
Relative patient benefits of a hospital-pcmh collaboration within an ACO to improve care transitions: Lessons learned from the PCORI grant application experience Jeffrey L. Schnipper, MD, MPH, FHM Director
Using Root Cause Analysis to Determine Why Readmissions are High. Presentation Objectives. Background Information 11/30/2011
 Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
A I S. San Diego s ADRC CARE TRANSITIONS INTERVENTION (CTI) 9/19/2011
 9/19/2011") CARE TRANSITIONS INTERVENTION (CTI) Brenda Schmitthenner, MPA Aging Program Administrator (858) 495 5853 brenda.schmitthenner@sdcounty.ca.gov A I S RSVP Veterans Health Promotion Info & Assistance Outreach
CARE TRANSITIONS INTERVENTION (CTI) Brenda Schmitthenner, MPA Aging Program Administrator (858) 495 5853 brenda.schmitthenner@sdcounty.ca.gov A I S RSVP Veterans Health Promotion Info & Assistance Outreach
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
CCNC Care Management Standardized Plan
 Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Transitional Care at Mount Sinai The PACT Program
 Transitional Care at Mount Sinai The PACT Program Maria Basso Lipani, LCSW Program Director, PACT Mount Sinai Hospital Mount Sinai Medical Center Founded in 1852 1,171-bed tertiary-care teaching and research
Transitional Care at Mount Sinai The PACT Program Maria Basso Lipani, LCSW Program Director, PACT Mount Sinai Hospital Mount Sinai Medical Center Founded in 1852 1,171-bed tertiary-care teaching and research
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
Kaiser Permanente: Transition Care Performance and Strategies
 Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS carbarne@gmail.com April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS carbarne@gmail.com April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Care Transition Bundle Seven Essential Intervention Categories
 Seven 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family
Seven 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Care Transition Bundle Seven Essential Intervention Categories. Examples of Transition of Care Interventions
 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family education
1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family education
Cheryl Schraeder, RN, PhD, FAAN. The demographic landscape of America is changing at an accelerated pace
 Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Root Cause Analysis (RCA) Getting to the Root of the Problem
 Getting to the Root of the Problem") Root Cause Analysis (RCA) Getting to the Root of the Problem DRIVING IMPROVEMENT The focus is on three critical aims to make care better for everyone: Better patient care Better population health Lower
Root Cause Analysis (RCA) Getting to the Root of the Problem DRIVING IMPROVEMENT The focus is on three critical aims to make care better for everyone: Better patient care Better population health Lower
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
How To Help A Nursing Home And Hospital Collaborate
 Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit
 Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit Presented By: Dr. Micah Beachy, Rickelle Collins and Nicole Turille Context As part of healthcare reform, hospitals are being challenged
Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit Presented By: Dr. Micah Beachy, Rickelle Collins and Nicole Turille Context As part of healthcare reform, hospitals are being challenged
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care
 NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Care Transitions: Success Stories and Lessons Learned
 Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Community Care of North Carolina
 Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Community Care of North Carolina. Statewide program for managing Carolina Access recipients
 Community Care of North Carolina Statewide program for managing Carolina Access recipients Key Goals Improve access to, quality of, and coordination of care for Carolina Access Medicaid patients. By doing
Community Care of North Carolina Statewide program for managing Carolina Access recipients Key Goals Improve access to, quality of, and coordination of care for Carolina Access Medicaid patients. By doing
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David
 Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Transitions of Care: The need for a more effective approach to continuing patient care
 H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Using Root Cause Analysis to Reduce All-Cause Readmissions. Howard Dubin, MD
 Using Root Cause Analysis to Reduce All-Cause Readmissions Howard Dubin, MD Test Your Problem Solving Skills If you had two U.S. coins totaling 55 cents and one of the coins was NOT a nickel, what are
Using Root Cause Analysis to Reduce All-Cause Readmissions Howard Dubin, MD Test Your Problem Solving Skills If you had two U.S. coins totaling 55 cents and one of the coins was NOT a nickel, what are
Service delivery interventions
 Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Assessing Risk of Readmission. NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013
 Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
Care Management Approach for People Who Are at High Risk
 Care Management Approach for People Who Are at High Risk Presented by: Ann Larsen RN, CDE Care Manger - Herefordshire Clinic/Trainer Care Management Plus June 11, 2013 Welcome! Type questions into the
Care Management Approach for People Who Are at High Risk Presented by: Ann Larsen RN, CDE Care Manger - Herefordshire Clinic/Trainer Care Management Plus June 11, 2013 Welcome! Type questions into the
ST JOHN S LUTHERAN MINISTRIES. Kent Burgess President & CEO
 ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
Overcoming Barriers to Discharge for Home Infusion
 VOLUME 19 CORAM S CONTINUING EDUCATION PROGRAM Overcoming Barriers to Discharge for Home Infusion Successful home infusion therapy relies on timely and effective transitions to home. Early identification
VOLUME 19 CORAM S CONTINUING EDUCATION PROGRAM Overcoming Barriers to Discharge for Home Infusion Successful home infusion therapy relies on timely and effective transitions to home. Early identification
Care Transitions. Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model. Share This
 Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Learning Collaborative
 Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Kaiser Permanente of Ohio
 Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Combined Assessment Program Summary Report. Evaluation of Pressure Ulcer Prevention and Management at Veterans Health Administration Facilities
 Department of Veterans Affairs Office of Inspector General Report No. 14-05132-90 Office of Healthcare Inspections Combined Assessment Program Summary Report Evaluation of Pressure Ulcer Prevention and
Department of Veterans Affairs Office of Inspector General Report No. 14-05132-90 Office of Healthcare Inspections Combined Assessment Program Summary Report Evaluation of Pressure Ulcer Prevention and
What Do We Know? Does the Current Evidence Support Business as Usual? Eric A. Coleman, MD, MPH
 Listen to Your Patients They Are Telling You How to Improve the Quality of their Transitional Care Eric A. Coleman, MD, MPH, AGSF, FACP Professor of Medicine Director, Care Transitions Program University
Listen to Your Patients They Are Telling You How to Improve the Quality of their Transitional Care Eric A. Coleman, MD, MPH, AGSF, FACP Professor of Medicine Director, Care Transitions Program University
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions
 and its impact in COPD 30-day readmissions") From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: cristiane.fukuda@northside.com Office: 404-851-6914
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: cristiane.fukuda@northside.com Office: 404-851-6914
HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT
 HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT #607 Friday, October 30, 2015 MARY NEWBERRY, MSN RN, DIRECTOR, HOME BASED & TRANSITIONAL CARE DEBORAH BRADLEY, MSN RN, MANAGER HOME HEALTH CARE BETH
HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT #607 Friday, October 30, 2015 MARY NEWBERRY, MSN RN, DIRECTOR, HOME BASED & TRANSITIONAL CARE DEBORAH BRADLEY, MSN RN, MANAGER HOME HEALTH CARE BETH
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
Care Coordination and Aging
 Care Coordination and Aging September 3, 2014 Robyn Golden, LCSW Director of Health and Aging Rush University Medical Center Robyn_L_Golden@rush.edu Our nation faces significant challenges when it comes
Care Coordination and Aging September 3, 2014 Robyn Golden, LCSW Director of Health and Aging Rush University Medical Center Robyn_L_Golden@rush.edu Our nation faces significant challenges when it comes
Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents
 Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management 10.0 Care Management
Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management 10.0 Care Management
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
Leveraging EHR to Improve Patient Safety: A Davies Story
 Leveraging EHR to Improve Patient Safety: A Davies Story Claudia Colgan, Vice President of Quality Initiatives Bruce Darrow, MD, PhD, Interim Chief Medical Information Officer Jill Kalman, MD, Director
Leveraging EHR to Improve Patient Safety: A Davies Story Claudia Colgan, Vice President of Quality Initiatives Bruce Darrow, MD, PhD, Interim Chief Medical Information Officer Jill Kalman, MD, Director
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
APPENDIX F TRANSITIONS OF CARE SUBCOMMITTEE
 APPENDIX F TRANSITIONS OF CARE SUBCOMMITTEE INTRODUCTION Effectively managing patient transitions between settings of care (eg, from hospital to primary care, or from community to nursing home) is one
APPENDIX F TRANSITIONS OF CARE SUBCOMMITTEE INTRODUCTION Effectively managing patient transitions between settings of care (eg, from hospital to primary care, or from community to nursing home) is one
Cedars Sinai Medical Center (CSMC) Learning Objectives. Why Medication Reconciliation?
 Learning Objectives. Why Medication Reconciliation?") Management Case Study: Transitions Trifecta Calibrating the Severity of Drug Related Problems, dherence, and Literacy in a High Risk Population Tuesday, December 10, 2013 2:00 p.m. 2:30 p.m. Management
Management Case Study: Transitions Trifecta Calibrating the Severity of Drug Related Problems, dherence, and Literacy in a High Risk Population Tuesday, December 10, 2013 2:00 p.m. 2:30 p.m. Management
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Care Coordination and Transitions in Behavioral Health
 Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
What is Palliative Care
 What is Palliative Care Maine Quality Counts Portland Regional Forum Isabella N. Stumpf, DO Division Director, Palliative Medicine, Maine Medical Center Medical Director, Palliative Care, MaineHealth Disclosure
What is Palliative Care Maine Quality Counts Portland Regional Forum Isabella N. Stumpf, DO Division Director, Palliative Medicine, Maine Medical Center Medical Director, Palliative Care, MaineHealth Disclosure
Discharge Planning. Home Care 1. Objectives. Where are they Going?
 Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Our Patient-Centered Medical Home a Process, not a Click
 Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
hospital readmission rate reduction: building better interfaces within the community.
 hospital readmission rate reduction: building better interfaces within the community. Whitepaper By Ken Taverner, M.Sc. the issue of hospital readmission rates Leaving the hospital after being admitted
hospital readmission rate reduction: building better interfaces within the community. Whitepaper By Ken Taverner, M.Sc. the issue of hospital readmission rates Leaving the hospital after being admitted
Technician Learning Objectives 3/25/2014. Pharmacy Practice Changes in ACA Accountable Care Organizations
 Pharmacy Practice Changes in ACA Accountable Care Organizations Avani S. Desai, PharmD & Emory S. Martin PharmD Sunday, April 12, 2014 9:05 10:05 am Pharmacist Learning Objectives At the conclusion of
Pharmacy Practice Changes in ACA Accountable Care Organizations Avani S. Desai, PharmD & Emory S. Martin PharmD Sunday, April 12, 2014 9:05 10:05 am Pharmacist Learning Objectives At the conclusion of
COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA
 COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA USA COPD Data 24 Million Americans under the age of 65 with COPD Almost 20% readmit
COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA USA COPD Data 24 Million Americans under the age of 65 with COPD Almost 20% readmit
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE. Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center
 CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Improving Hospital Performance
 Improving Hospital Performance Background AHA View Putting patients first ensuring their care is centered on the individual, rooted in best practices and utilizes the latest evidence-based medicine is
Improving Hospital Performance Background AHA View Putting patients first ensuring their care is centered on the individual, rooted in best practices and utilizes the latest evidence-based medicine is
AMERICAN MEDICAL DIRECTORS ASSOCIATION WHITE PAPER RESOLUTION C09
 AMERICAN MEDICAL DIRECTORS ASSOCIATION WHITE PAPER RESOLUTION C09 SUBJECT: IMPROVING CARE TRANSITIONS FROM THE NURSING FACILITY TO A COMMUNITY-BASED SETTING INTRODUCED BY: AMDA PUBLIC POLICY COMMITTEE
AMERICAN MEDICAL DIRECTORS ASSOCIATION WHITE PAPER RESOLUTION C09 SUBJECT: IMPROVING CARE TRANSITIONS FROM THE NURSING FACILITY TO A COMMUNITY-BASED SETTING INTRODUCED BY: AMDA PUBLIC POLICY COMMITTEE
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Risk Tools in Predicting Rehospitalization from Home Care. VNAA Best Practice for Home Health
 Risk Tools in Predicting Rehospitalization from Home Care VNAA Best Practice for Home Health Learning objectives The participant will be able to: Discuss the need for risk assessment for home health patients
Risk Tools in Predicting Rehospitalization from Home Care VNAA Best Practice for Home Health Learning objectives The participant will be able to: Discuss the need for risk assessment for home health patients
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Locking the Revolving Door of Readmissions
 Locking the Revolving Door of Readmissions The Pharmacist s Role in Keeping Patients Healthy, Happy and At Home Steve Riddle, BS Pharm, BCPS, FASHP VP of Clinical Affairs, Pharmacy OneSource Objectives
Locking the Revolving Door of Readmissions The Pharmacist s Role in Keeping Patients Healthy, Happy and At Home Steve Riddle, BS Pharm, BCPS, FASHP VP of Clinical Affairs, Pharmacy OneSource Objectives
Driving The Ultimate Patient Experience Patient Discharge
 Driving The Ultimate Patient Experience Patient Discharge Date: January 12 th, 2012 Hendricks Regional Health BOH-HFAP Joint Webcast Agenda for today s discussion: About Hendricks Regional Health HFAP
Driving The Ultimate Patient Experience Patient Discharge Date: January 12 th, 2012 Hendricks Regional Health BOH-HFAP Joint Webcast Agenda for today s discussion: About Hendricks Regional Health HFAP
Preventing Avoidable Re-Hospitalizations: Where Do You Fit in the Quality Care Puzzle?
 Speaker Disclosures Care Transitions Interventions: The Sussex County Transitional Care Program Dr. Wang has disclosed that he has no relevant financial relationship(s). George C. Wang, MD, PhD Medical
Speaker Disclosures Care Transitions Interventions: The Sussex County Transitional Care Program Dr. Wang has disclosed that he has no relevant financial relationship(s). George C. Wang, MD, PhD Medical
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
How To Plan A Rehabilitation Program
 Project Plan to Rehabilitation Service Connecting and Collaborating in the Continuity of Care in Rehabilitation Presented By: Arlene Whitehead, May 31, 2011 Rehabilitation Collaborative Overview OUTLINE
Project Plan to Rehabilitation Service Connecting and Collaborating in the Continuity of Care in Rehabilitation Presented By: Arlene Whitehead, May 31, 2011 Rehabilitation Collaborative Overview OUTLINE
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Improving Care Transitions using PDSA Methodology
 Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
THE CARE INTERVENTION: IMPROVING TRANSITIONS ACROSS SITES OF CARE
 THE CARE TRANSITIONS INTERVENTION: IMPROVING TRANSITIONS ACROSS SITES OF CARE FUNDING PROVIDED BY THE JOHN A. HARTFORD FOUNDATION AND THE ROBERT WOOD JOHNSON FOUNDATION RECOMMENDED CITATION: USERS MANUAL:
THE CARE TRANSITIONS INTERVENTION: IMPROVING TRANSITIONS ACROSS SITES OF CARE FUNDING PROVIDED BY THE JOHN A. HARTFORD FOUNDATION AND THE ROBERT WOOD JOHNSON FOUNDATION RECOMMENDED CITATION: USERS MANUAL:
The Children s Readmissions Collaborative Kick-Off Conference April 28, 2014 Project Tools
 The Children s Readmissions Collaborative Kick-Off Conference April 28, 2014 Project Tools Kate M. Sherman Manager, Readmissions Quality Collaborative New York State Psychiatric Institute/ State Office
The Children s Readmissions Collaborative Kick-Off Conference April 28, 2014 Project Tools Kate M. Sherman Manager, Readmissions Quality Collaborative New York State Psychiatric Institute/ State Office
Coaching Patients to Improve Care Transitions in Pennsylvania. May 26, 2010
 Coaching Patients to Improve Care Transitions in Pennsylvania Naomi Hauser, RN, MPA, CLNC Director Care Transitions Quality Insights of Pennsylvania Dr. Eric Coleman, MPH Professor of Medicine University
Coaching Patients to Improve Care Transitions in Pennsylvania Naomi Hauser, RN, MPA, CLNC Director Care Transitions Quality Insights of Pennsylvania Dr. Eric Coleman, MPH Professor of Medicine University
RE: CMS-3819-P; Medicare and Medicaid Programs; Conditions of Participation for Home Health Agencies
 January 6, 2015 Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445 G Attention: CMS-3819-P Hubert H. Humphrey Building, 200 Independence
January 6, 2015 Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445 G Attention: CMS-3819-P Hubert H. Humphrey Building, 200 Independence
Atlanta Care Transitions Initiative. Atlanta Regional Commission Area Agency on Aging
 Atlanta Care Transitions Initiative Atlanta Regional Commission Area Agency on Aging Atlanta Regional Commission Atlanta Region Area Agency on Aging Regional Planning Commission 1 of 12 AAAs in Georgia
Atlanta Care Transitions Initiative Atlanta Regional Commission Area Agency on Aging Atlanta Regional Commission Atlanta Region Area Agency on Aging Regional Planning Commission 1 of 12 AAAs in Georgia
Eddy VNA Care Transitions Program
 Eddy VNA Care Transitions Program Patrick Archambeault RN, MS, CRNI Director of Clinical Specialties About Eddy VNA Large not for profit home care agency based in upstate New York CHHA, LTHHCP, Licensed
Eddy VNA Care Transitions Program Patrick Archambeault RN, MS, CRNI Director of Clinical Specialties About Eddy VNA Large not for profit home care agency based in upstate New York CHHA, LTHHCP, Licensed
7/25/2015. Disclosure(s) Prescription for the Future: Pharmacists Influencing Positive Health Outcomes. Clinical Practice.
 Prescription for the Future: Pharmacists Influencing Positive Health Outcomes. Clinical Practice.") 49th Annual Meeting Prescription for the Future: Pharmacists Influencing Positive Health Outcomes Daniel E. Buffington, PharmD, MBA, FAPhA Clinical Pharmacology Services, Inc Tampa, FL Disclosure(s) Daniel
49th Annual Meeting Prescription for the Future: Pharmacists Influencing Positive Health Outcomes Daniel E. Buffington, PharmD, MBA, FAPhA Clinical Pharmacology Services, Inc Tampa, FL Disclosure(s) Daniel