EPILEPSY AND SYNCOPE. Ivo Bekavac, MD, PhD
|
|
|
- Marcia Morton
- 7 years ago
- Views:
Transcription
1 EPILEPSY AND SYNCOPE Ivo Bekavac, MD, PhD
2 SEIZURE Sudden change in behavior that is the consequence of brain dysfunction. Epileptic seizures result from electrical hypersynchronization of neuronal networks in the cerebral cortex. Epilepsy recurrent epileptic seizures due to genetically determines or acquired brain disorder % of the population Provoked seizures due to metabolic disturbance, drug or alcohol withdrawal, acute neurologic disorders such as stroke or encephalitis Nonepileptic seizures sudden changes in behavior that resemble epileptic seizures but are not associated with the typical neurophysiological changes that characterize epileptic seizures.
3 Syncope Loss of consciousness due to hypoperfusion/absent perfusion to the cerebral hemispheres or brainstem (hypotension, cardiac dysrhythmia, VBI)

4

5

6
7
8 Cerebrovascular Syncope Vertebrobasilar insufficiency (VBI) Migraine (basilar migraine) Takayasu disease Carotid sinus syncope
9 Etiology of Seizures Less than 50% have an identifiable cause Post-traumatic seizures (head trauma) Brain tumors Stroke Intracranial infection Cerebral degeneration Congenital brain malformations Inborn errors of metabolism
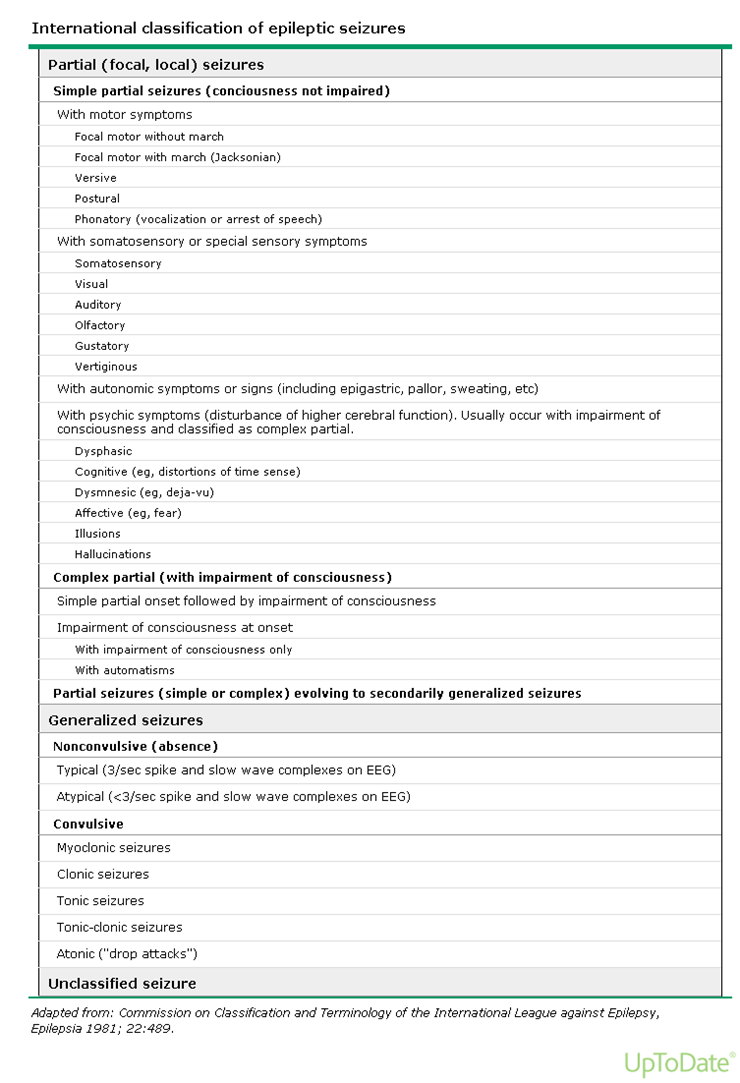
10 Classification Simple partial Complex partial Generalized tonic-clonic Less common varieties oabsence omyoclonic o Psychogenic
11
12 Acute symptomatic seizures
13
14
15
16 Clinical features History Prior seizures (including febrile seizures) Seizures precipitants or triggers (photic) Seizure symptoms and signs (aura, CPS, GTC) Postictal state (postictal paresis, confusion, suppressed alertness) Other aspects of the patient history (past medical history, medications, family history) Physical and neurologic examination
17
18

19
20

21
22
23
24
25
26 Diagnostic studies Laboratory screening Causative metabolic abnormalities Prolactin (low sensitivity) Other seizure biomarkers (CPK, cortisol, WBC, LDH, PCO2, NH3, NSE) Electrocardiogram Lumbar puncture Electroencephalography Neuroimaging
27
28
29
30
31
32
33
34
35
36

37
38
39 ANTIEPILEPTIC DRUG THERAPY When to start AED therapy Choosing an AED Combination therapy Side effects of therapy Specific adverse reactions Generic substitution Alcohol intake Nonadherence with AED therapy
40 Drug-resistant epilepsy Surgical treatment Temporal lobectomy Extratemporal cortical resection Hemispherectomy Corpus callosotomy Ketogenic diet Vagus nerve stimulation therapy
41 Special populations Women of childbearing age 1. Effect of AED on the fetus 2. Folic acid supplementation (4mg/day for VPA/CBZ 1-3 months prior to conception, mg/day other AED) 3. Contraception 4. Fertility Post-stroke seizures (when to treat?) Older patients
42 Complications of epilepsy Mortality Personal injury MVA (driving restrictions) Psychosocial issues Depression and psychiatric disease Cognitive impairment Medical comorbidities
43
44

45
46
47 STATUS EPILEPTICUS
48 Introduction A single unremitting seizure with a duration longer than 5-10 minutes, or frequent clinical seizures without an interictal return to the baseline clinical state
49 Epidemiology 100, ,000 episodes of SE/year in the USA Refractory SE (ongoing seizures after 1 st and 2 nd line AED):30-43% Encephalitis Subtherapeutic level = nonrefractory Nonconvulsive >GTC SE = refractory
50 Etiology predisposing factors AED noncompliance or discontinuation Withdrawal syndromes (EtOH, barbiturates, baclofen, benzodiapines-alprazolam) Acute structural injury (tumor, stroke, TBI, SAH, cerebral anoxia/hypoxia, infection Remote or longstanding structural injury (prior head injury, CP, prior NSG, AVM) Metabolic abnormalities (hypoglycemia, hepatic encephalopathy, uremia, pyridoxine deficiency, hyponatremia, hyperglycemia, hypocalcemia, hypomagnesemia) Use or overdose drugs that lower the seizure threshold (theophylline, imipenem, penicillin G, metronidazole, isoniazid, tricyclics, bupropion, Li, clozapine, flumazenil, cyclosporine, lidocaine, bupivacaine) NORSE (new onset refractory SE), unclear etiology, high mortality
51 Complications and outcome Mortality- 20% (1 st episode of SE) 69-81% after anoxia Etiology, older age, medical comorbidity, > initial APACHE-II score) Metabolic stress, rhabdomyolysis, lactic acidosis Aspiration pneumonitis Neurogenic pulmonary edema Cardiac injury Neuronal death (after min)
52 Diagnosis Neurologic examination Electroencephalogram Single photon emission computed tomography MRI
53 Neurologic examination Nonconvulsive SE Level of consciousness Observation for automatic movements or myoclonus Asymmetric features on examination Motor responses
54 Electroencephalogram Extremely valuable tool Continuous seizure activity
55
56
57
58
59 Single photon emission computed tomography Increased perfusion during status May persist for weeks after SE
60
61
62 Magnetic resonance imaging The best tool to reveal the structural lesions that may trigger SE Abnormalities during SE (cell edema)- may persist for days-weeks
63
64 Benzodiazepines Diazepam mg/kg, IV effect in seconds, t max/2 in in CSF in 3 min, lasts <20 min. Stops seizure in 50-80%, 50% recurrence if no 2 nd agent introduced. Rectal gel. Lorazepam 0.1 mg/kg IV effect in two minutes. Midazolam 0.2 mg/kg bolus, continuous infusion mcg/kg min
65 Phenytoin 50 mg/min, total 20 mg/kg Risk of hypotension and cardiac arrhythmias Fosphenytoin Pro-drug of phenytoin Up to 150 mg/min, IV/IM Intensify seizures caused by cocaine, other local anesthetics
66 Barbiturates Phenobarbital- 20 mg/kg infused at a rate mg/min (t/2 100 h) Pentobarbital loading dose of 10 mg/kg, up to 100 mg/min, continuous infusion 1-4 mg/kg/h)
67 Propofol Hypotension, respiratory depression, metabolic acidosis, cardiac dysfunction
68 Valproic acid Slow infusion, up to 20 mg/min Safe up to 10 mg/kg/min
69 Newer AED Topiramate Levetiracetam Lacosamide
70 Assessment and support Rapid neurologic examination Rapid general evaluation IV catheter placement Electrolytes, ABG, cardiac
71 Initial pharmacologic therapy for patients in an ER or hospital setting Lorazepam (0.02 to 0.03 mg/kg) cumulative dose of 0.1 mg/kg, max 2 mg/min) Diazepam (0.1 mg/kg IV) Midazolam (0.05 mg/kg IV) If no IV access midazolam 10 mg IM (>40 kg), 5 mg (13-40 kg) Phenytoin (but not fosphenytoin) and any of benzodiazepines are incompatible (precipitation) if infused through the same IV line. Phenytoin (20 mg/kg) mg/min (100 PE/min for fosphenytoin) 30 min
72 Treatment of refractory seizures SE refractory to 1 st line of AED NICU management Another 10 mg/kg phenytoin Phenobarbital Pentobarbital Midazolam Propofol
73 Hemodynamically stable patients High dose barbiturates Phenobarbital 20 mg/kg, max 100 mg/min Pentobarbital 100 mg/kg EEG monitoring, clinical & subclinical seizures, burst suppression If seizures terminated with pentobarbital 1-4 mg/kg/hr X 24 hrs, then tape off over following 24 hrs Vasopressor support (phenylephrine or dopamine)
74 Patients at high risk for respiratory failure Propofol (severe COPD, severe debilitation, cancer) to minimize the duration of sedation. Start 1-2 mg/kg/hr, titrated over next min up to mg/kg/h, <18-48 hours If not successful midazolam or barbiturates
75 Malignant SE 20% of refractory SE
76 Out-of-hospital/prehospital treatment Safe and effective
77
Status Epilepticus and Epilepsy
 Status Epilepticus and Epilepsy Chapter 25 Status Epilepticus and Epilepsy Status Epilepticus Defined as protracted or recurrent seizures causing prolonged changes in sensorium and other neurological impairment
Status Epilepticus and Epilepsy Chapter 25 Status Epilepticus and Epilepsy Status Epilepticus Defined as protracted or recurrent seizures causing prolonged changes in sensorium and other neurological impairment
The Clinical Evaluation of the Comatose Patient in the Emergency Department
 The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
MANAGEMENT OF STATUS EPILEPTICUS. Elizabeth Macri, MS, MD
 MANAGEMENT OF STATUS EPILEPTICUS Elizabeth Macri, MS, MD Definition Continuous or repeat seizure activity persisting for at least 30 minutes without full recovery between attacks. Very few single seizures
MANAGEMENT OF STATUS EPILEPTICUS Elizabeth Macri, MS, MD Definition Continuous or repeat seizure activity persisting for at least 30 minutes without full recovery between attacks. Very few single seizures
Seizures (Convulsions, Status Epilepticus) in Dogs
 in Dogs") Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Seizures (Convulsions, Status Epilepticus) in Dogs Basics OVERVIEW Seizures are
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Seizures (Convulsions, Status Epilepticus) in Dogs Basics OVERVIEW Seizures are
Guidelines for the Evaluation and Management of Status Epilepticus
 DOI 10.1007/s12028-012-9695-z REVIEW Guidelines for the Evaluation and Management of Status Epilepticus Gretchen M. Brophy Rodney Bell Jan Claassen Brian Alldredge Thomas P. Bleck Tracy Glauser Suzette
DOI 10.1007/s12028-012-9695-z REVIEW Guidelines for the Evaluation and Management of Status Epilepticus Gretchen M. Brophy Rodney Bell Jan Claassen Brian Alldredge Thomas P. Bleck Tracy Glauser Suzette
Alcohol Withdrawal. Introduction. Blood Alcohol Concentration. DSM-IV Criteria/Alcohol Abuse. Pharmacologic Effects of Alcohol
 Pharmacologic Effects of Alcohol Alcohol Withdrawal Kristi Theobald, Pharm.D., BCPS Therapeutics III Fall 2003 Inhibits glutamate receptor function (NMDA receptor) Inhibits excitatory neurotransmission
Pharmacologic Effects of Alcohol Alcohol Withdrawal Kristi Theobald, Pharm.D., BCPS Therapeutics III Fall 2003 Inhibits glutamate receptor function (NMDA receptor) Inhibits excitatory neurotransmission
Gloucestershire Hospitals
 Gloucestershire Hospitals NHS Foundation Trust TRUST GUIDELINE EPILEPSY AND STATUS EPILEPTICUS MANAGEMENT 1. INTRODUCTION The aim of this guideline is to ensure safe management of Status Epilepticus in
Gloucestershire Hospitals NHS Foundation Trust TRUST GUIDELINE EPILEPSY AND STATUS EPILEPTICUS MANAGEMENT 1. INTRODUCTION The aim of this guideline is to ensure safe management of Status Epilepticus in
Review Article Treatment of Refractory Status Epilepticus: Literature Review and a Proposed Protocol
 Review Article Treatment of Refractory Status Epilepticus: Literature Review and a Proposed Protocol Nicholas S. Abend, MD* and Dennis J. Dlugos, MD, MSCE* Refractory status epilepticus describes continuing
Review Article Treatment of Refractory Status Epilepticus: Literature Review and a Proposed Protocol Nicholas S. Abend, MD* and Dennis J. Dlugos, MD, MSCE* Refractory status epilepticus describes continuing
EMS Branch / Office of the Medical Director. Active Seziures (d) Yes Yes Yes Yes. Yes Yes No No. Agitation (f) No Yes Yes No.
 Yes Yes Yes Yes. Yes Yes No No. Agitation (f) No Yes Yes No.") M07 Medications 2015-07-15 All ages EMS Branch / Office of the Medical Director Benzodiazepines Primary Intermediate Advanced Critical INDICATIONS Diazepam (c) Lorazepam (c) Midazolam (c) Intranasal Midazolam
M07 Medications 2015-07-15 All ages EMS Branch / Office of the Medical Director Benzodiazepines Primary Intermediate Advanced Critical INDICATIONS Diazepam (c) Lorazepam (c) Midazolam (c) Intranasal Midazolam
Practice Guideline. Neuropsychological Evaluations
 Practice Guideline Neuropsychological Evaluations Adapted from the practice guideline of the same name by the Arizona Department of Health Services Division of Behavioral Health Services Effective: 06/30/2006
Practice Guideline Neuropsychological Evaluations Adapted from the practice guideline of the same name by the Arizona Department of Health Services Division of Behavioral Health Services Effective: 06/30/2006
VAGUS NERVE STIMULATION FOR PATIENTS IN RESIDENTIAL TREATMENT FACILITIES
 VAGUS NERVE STIMULATION FOR PATIENTS IN RESIDENTIAL TREATMENT FACILITIES Michael Frost, MD Roger Huf, MD John Gates, MD This paper has been prepared specifically for: American Epilepsy Society Annual Meeting
VAGUS NERVE STIMULATION FOR PATIENTS IN RESIDENTIAL TREATMENT FACILITIES Michael Frost, MD Roger Huf, MD John Gates, MD This paper has been prepared specifically for: American Epilepsy Society Annual Meeting
Neurological System Best Practice Documentation
 Neurological System Best Practice Documentation Click on the desired Diagnoses link or press Enter to view all information. Diagnoses: Dementia Delirium/Encephalopathy Parkinson s Epilepsy /Seizure Migraines
Neurological System Best Practice Documentation Click on the desired Diagnoses link or press Enter to view all information. Diagnoses: Dementia Delirium/Encephalopathy Parkinson s Epilepsy /Seizure Migraines
Fit, (falls) and funny turns. Richard J Davenport Consultant Neurologist Edinburgh
 and funny turns. Richard J Davenport Consultant Neurologist Edinburgh") Fit, (falls) and funny turns Richard J Davenport Consultant Neurologist Edinburgh The plan Epilepsy nuggets 10 things I would like GPs to know This week s FS clinic What is epilepsy? Characterised by two
Fit, (falls) and funny turns Richard J Davenport Consultant Neurologist Edinburgh The plan Epilepsy nuggets 10 things I would like GPs to know This week s FS clinic What is epilepsy? Characterised by two
Multiple-Choice Questions
 CME Multiple-Choice Questions The Multiple-Choice Questions are an integral part of the issue. They are intended as a means of stimulating thought and helping participants assess general understanding
CME Multiple-Choice Questions The Multiple-Choice Questions are an integral part of the issue. They are intended as a means of stimulating thought and helping participants assess general understanding
Department of Clinical Pharmacy, University of Colorado, Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, CO 6
 American Epilepsy Society Guideline Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society Tracy
American Epilepsy Society Guideline Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society Tracy
Epilepsy 101: Getting Started
 American Epilepsy Society 1 Epilepsy 101 for nurses has been developed by the American Epilepsy Society to prepare professional nurses to understand the general issues, concerns and needs of people with
American Epilepsy Society 1 Epilepsy 101 for nurses has been developed by the American Epilepsy Society to prepare professional nurses to understand the general issues, concerns and needs of people with
Differential Diagnosis of the epileptic seizures Concerned: 6 year Medical students
 Differential Diagnosis of the epileptic seizures Concerned: 6 year Medical students Dr. Faustin YEPNJIO University of Dakar-Senegal 2nd IBRO-SfN-NAS Teaching Tools worshop in Africa, Fayoum, Egypt 2009
Differential Diagnosis of the epileptic seizures Concerned: 6 year Medical students Dr. Faustin YEPNJIO University of Dakar-Senegal 2nd IBRO-SfN-NAS Teaching Tools worshop in Africa, Fayoum, Egypt 2009
What is epilepsy? English
 What is epilepsy? English WHAT IS EPILEPSY? An epileptic seizure is the term used for a temporary brain dysfunction due to a sudden and uncontrolled disturbance of the brain s electrical activity. Epilepsy
What is epilepsy? English WHAT IS EPILEPSY? An epileptic seizure is the term used for a temporary brain dysfunction due to a sudden and uncontrolled disturbance of the brain s electrical activity. Epilepsy
APPROACH TO THE CHILD WITH A SEIZURE
 APPROACH TO THE CHILD WITH A SEIZURE 1. Background... 1 2. Questions to ask... 1 a) Pre-ictal... 2 b) Ictal... 2 c) Post-ictal... 2 d) Other questions to ask... 2 3. Diagnosis... 3 a) Clinical categories...
APPROACH TO THE CHILD WITH A SEIZURE 1. Background... 1 2. Questions to ask... 1 a) Pre-ictal... 2 b) Ictal... 2 c) Post-ictal... 2 d) Other questions to ask... 2 3. Diagnosis... 3 a) Clinical categories...
Headaches and Kids. Jennifer Bickel, MD Assistant Professor of Neurology Co-Director of Headache Clinic Children s Mercy Hospital
 Headaches and Kids Jennifer Bickel, MD Assistant Professor of Neurology Co-Director of Headache Clinic Children s Mercy Hospital Overview Headache classifications and diagnosis Address common headache
Headaches and Kids Jennifer Bickel, MD Assistant Professor of Neurology Co-Director of Headache Clinic Children s Mercy Hospital Overview Headache classifications and diagnosis Address common headache
Hepatic Encephalopathy, Hyperammonemia, and Current Treatment in ICU Room
 Hepatic Encephalopathy, Hyperammonemia, and Current Treatment in ICU Room Assoc.Prof. Chan Sovandy Chairman by : Prof.So Saphy and Assoc Prof, Kim chhoung Hepatic Encephalopathy Hepatic (portal systemic
Hepatic Encephalopathy, Hyperammonemia, and Current Treatment in ICU Room Assoc.Prof. Chan Sovandy Chairman by : Prof.So Saphy and Assoc Prof, Kim chhoung Hepatic Encephalopathy Hepatic (portal systemic
New Onset Seizure Clinic
 New Onset Seizure Clinic Timely Care from the Region s Experts The New Onset Seizure Clinic at UH Rainbow Babies & Children s Hospital provides expert diagnostic services, referrals, treatment and follow-up
New Onset Seizure Clinic Timely Care from the Region s Experts The New Onset Seizure Clinic at UH Rainbow Babies & Children s Hospital provides expert diagnostic services, referrals, treatment and follow-up
CHILDREN S NEUROSCIENCE CENTER
 CHILDREN S NEUROSCIENCE CENTER W hen families come to Children s Memorial Hermann Hospital, they expect to find the technological advances and healing expertise of a university-affiliated, academic hospital.
CHILDREN S NEUROSCIENCE CENTER W hen families come to Children s Memorial Hermann Hospital, they expect to find the technological advances and healing expertise of a university-affiliated, academic hospital.
Practice Protocol. Neuropsychological Evaluations
 Practice Protocol Neuropsychological Evaluations Jointly Developed by the Arizona Department of Health Services/Division of Behavioral Health Services and AHCCCS/Health Plans Effective June 30, 2006 Revised
Practice Protocol Neuropsychological Evaluations Jointly Developed by the Arizona Department of Health Services/Division of Behavioral Health Services and AHCCCS/Health Plans Effective June 30, 2006 Revised
Philip Moore DO, Toxicology Fellow, PinnacleHealth Toxicology Center Joanne Konick-McMahan RN MSRN, Staff RN, PinnacleHealth
 Philip Moore DO, Toxicology Fellow, PinnacleHealth Toxicology Center Joanne Konick-McMahan RN MSRN, Staff RN, PinnacleHealth I. II. Background A. AWS can occur in anyone who consumes alcohol B. Risk correlates
Philip Moore DO, Toxicology Fellow, PinnacleHealth Toxicology Center Joanne Konick-McMahan RN MSRN, Staff RN, PinnacleHealth I. II. Background A. AWS can occur in anyone who consumes alcohol B. Risk correlates
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE
 STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
Hospice Palliative Care Program Symptom Guidelines. Twitching/Myoclonus/ Seizures
 Hospice Palliative Care Program Symptom Guidelines Twitching/Myoclonus/ Seizures Twitching/Myoclonus/Seizures Rationale This guideline is adapted for inter-professional primary care providers working
Hospice Palliative Care Program Symptom Guidelines Twitching/Myoclonus/ Seizures Twitching/Myoclonus/Seizures Rationale This guideline is adapted for inter-professional primary care providers working
Clinical guideline Published: 11 January 2012 nice.org.uk/guidance/cg137
 Epilepsies: diagnosis and management Clinical guideline Published: 11 January 2012 nice.org.uk/guidance/cg137 NICE 2012. All rights reserved. Last updated February 2016 Your responsibility The recommendations
Epilepsies: diagnosis and management Clinical guideline Published: 11 January 2012 nice.org.uk/guidance/cg137 NICE 2012. All rights reserved. Last updated February 2016 Your responsibility The recommendations
Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease.
 Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease. Memory loss and changes in mood and behavior are some signs that you or a family member may have Alzheimer s disease. If you have
Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease. Memory loss and changes in mood and behavior are some signs that you or a family member may have Alzheimer s disease. If you have
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES
 APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
Disability Evaluation Under Social Security
 Disability Evaluation Under Social Security Revised Medical Criteria for Evaluating Endocrine Disorders Effective June 7, 2011 Why a Revision? Social Security revisions reflect: SSA s adjudicative experience.
Disability Evaluation Under Social Security Revised Medical Criteria for Evaluating Endocrine Disorders Effective June 7, 2011 Why a Revision? Social Security revisions reflect: SSA s adjudicative experience.
Seizure Acute Management: Emergency Department v.1.2
 Seizure Acute Management: Emergency Department v.1.2 Executive Summary Test Your Knowledge Inclusion Criteria Patient presenting with epileptic seizure Explanation of Evidence Ratings Summary of Version
Seizure Acute Management: Emergency Department v.1.2 Executive Summary Test Your Knowledge Inclusion Criteria Patient presenting with epileptic seizure Explanation of Evidence Ratings Summary of Version
Emergency Room Treatment of Psychosis
 OVERVIEW The term Lewy body dementias (LBD) represents two clinical entities dementia with Lewy bodies (DLB) and Parkinson s disease dementia (PDD). While the temporal sequence of symptoms is different
OVERVIEW The term Lewy body dementias (LBD) represents two clinical entities dementia with Lewy bodies (DLB) and Parkinson s disease dementia (PDD). While the temporal sequence of symptoms is different
Alcohol Withdrawal Syndromes
 Alcohol Withdrawal Syndromes Should You Treat This Patient s Alcohol Withdrawal With Benzodiazepines?! Meta-analysis of RCTs of benzodiazepines for the treatment of alcohol withdrawal! 11 RCTs identified,
Alcohol Withdrawal Syndromes Should You Treat This Patient s Alcohol Withdrawal With Benzodiazepines?! Meta-analysis of RCTs of benzodiazepines for the treatment of alcohol withdrawal! 11 RCTs identified,
Seizures and Epilepsy S. Nizam Ahmed, MD, FRCPC Associate Professor Neurology University of Alberta snahmed@ualberta.ca
 Seizures and Epilepsy S. Nizam Ahmed, MD, FRCPC Associate Professor Neurology University of Alberta snahmed@ualberta.ca What is an epileptic seizure? An epileptic seizure is a paroxysmal hyper synchronous
Seizures and Epilepsy S. Nizam Ahmed, MD, FRCPC Associate Professor Neurology University of Alberta snahmed@ualberta.ca What is an epileptic seizure? An epileptic seizure is a paroxysmal hyper synchronous
Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas
 Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Introduction. Differential Diagnosis of Epilepsy. 2016 Thai Epilepsy Teaching Course 8/20/2016. Tayard Desudchit, M.D Chulalongkorn U.
 Introduction Differential Diagnosis of Epilepsy Tayard Desudchit, M.D Chulalongkorn U. A diagnosis of epilepsy carries with it many important psychosocial issues as well as therapy decisions. The consequence
Introduction Differential Diagnosis of Epilepsy Tayard Desudchit, M.D Chulalongkorn U. A diagnosis of epilepsy carries with it many important psychosocial issues as well as therapy decisions. The consequence
Diagnosis and Management of Epilepsy
 Diagnosis and Management of Epilepsy Imran I Ali MD Professor of Neurology Director, Comprehensive Epilepsy Program University of Toledo, College of Medicine Definition A seizure is a clinical event associated
Diagnosis and Management of Epilepsy Imran I Ali MD Professor of Neurology Director, Comprehensive Epilepsy Program University of Toledo, College of Medicine Definition A seizure is a clinical event associated
Alcohol Withdrawal Syndrome & CIWA Assessment
 Alcohol Withdrawal Syndrome & CIWA Assessment Alcohol Withdrawal Syndrome is a set of symptoms that can occur when an individual reduces or stops alcoholic consumption after long periods of use. Prolonged
Alcohol Withdrawal Syndrome & CIWA Assessment Alcohol Withdrawal Syndrome is a set of symptoms that can occur when an individual reduces or stops alcoholic consumption after long periods of use. Prolonged
in the Elderly Thomas Robinson, MD Surgery Grand Rounds March 10 th, 2008
 Post- Operative Delirium in the Elderly Thomas Robinson, MD Surgery Grand Rounds March 10 th, 2008 What is the most common post-operative complication in elderly patients? What is the most common post-operative
Post- Operative Delirium in the Elderly Thomas Robinson, MD Surgery Grand Rounds March 10 th, 2008 What is the most common post-operative complication in elderly patients? What is the most common post-operative
MOH CLINICAL PRACTICE GUIDELINES 2/2008 Prescribing of Benzodiazepines
 MOH CLINICL PRCTICE GUIELINES 2/2008 Prescribing of Benzodiazepines College of Family Physicians, Singapore cademy of Medicine, Singapore Executive summary of recommendations etails of recommendations
MOH CLINICL PRCTICE GUIELINES 2/2008 Prescribing of Benzodiazepines College of Family Physicians, Singapore cademy of Medicine, Singapore Executive summary of recommendations etails of recommendations
What s new, and why, in Neurology 4?
 What s new, and why, in Neurology 4? All topics in Neurology 4 have been extensively reviewed and updated by the expert writing group, to provide concise evidence-based advice for the busy practitioner.
What s new, and why, in Neurology 4? All topics in Neurology 4 have been extensively reviewed and updated by the expert writing group, to provide concise evidence-based advice for the busy practitioner.
Headaches in Children
 Children s s Hospital Headaches in Children Manikum Moodley, MD, FRCP Section of Pediatric Neurology The Cleveland Clinic Foundation Introduction Headaches are common in children Most headaches are benign
Children s s Hospital Headaches in Children Manikum Moodley, MD, FRCP Section of Pediatric Neurology The Cleveland Clinic Foundation Introduction Headaches are common in children Most headaches are benign
COMPREHENSIVE MANAGEMENT OF THE ELDERLY PATIENT WITH MANIA
 COMPREHENSIVE MANAGEMENT OF THE ELDERLY PATIENT WITH MANIA Manic depressive illness is a biological brain disorder that produces significant alterations of mood and psychosis. Mania in the elderly occurs
COMPREHENSIVE MANAGEMENT OF THE ELDERLY PATIENT WITH MANIA Manic depressive illness is a biological brain disorder that produces significant alterations of mood and psychosis. Mania in the elderly occurs
Below, this letter outlines [patient name] s medical history, prognosis, and treatment rationale.
![Below, this letter outlines [patient name] s medical history, prognosis, and treatment rationale.](/thumbs/25/5563775.jpg "Below, this letter outlines [patient name] s medical history, prognosis, and treatment rationale.") [Date] [Name of Contact] [Title] [Name of Health Insurance Company] [Address] [City, State, Zip Code] Insured: [Patient Name] Policy Number: [Number] Group Number: [Number] Diagnosis: [Diagnosis and ICD-9-CM
[Date] [Name of Contact] [Title] [Name of Health Insurance Company] [Address] [City, State, Zip Code] Insured: [Patient Name] Policy Number: [Number] Group Number: [Number] Diagnosis: [Diagnosis and ICD-9-CM
NATIONAL COMPETENCY SKILL STANDARDS FOR PERFORMING AN ELECTROENCEPHALOGRAM
 NATIONAL COMPETENCY SKILL STANDARDS FOR PERFORMING AN ELECTROENCEPHALOGRAM Electroencephalographic (EEG) providers practice in accordance with the facility policy and procedure manual which details every
NATIONAL COMPETENCY SKILL STANDARDS FOR PERFORMING AN ELECTROENCEPHALOGRAM Electroencephalographic (EEG) providers practice in accordance with the facility policy and procedure manual which details every
EPILEPSY AND SEIZURES
 EPILEPSY AND SEIZURES INTRODUCTION There are many different types of seizures disorders. Seizures can be caused by drugs or alcohol, or they can be caused by withdrawal from drugs or alcohol. They can
EPILEPSY AND SEIZURES INTRODUCTION There are many different types of seizures disorders. Seizures can be caused by drugs or alcohol, or they can be caused by withdrawal from drugs or alcohol. They can
Depression in Older Persons
 Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
Clinical Case Studies in Epilepsy
 NEUROLOGY BOARD REVIEW MANUAL STATEMENT OF EDITORIAL PURPOSE The Hospital Physician Neurology Board Review Manual is a peer-reviewed study guide for residents and practicing physicians preparing for board
NEUROLOGY BOARD REVIEW MANUAL STATEMENT OF EDITORIAL PURPOSE The Hospital Physician Neurology Board Review Manual is a peer-reviewed study guide for residents and practicing physicians preparing for board
Developmental delay and Cerebral palsy. Present the differential diagnosis of developmental delay.
 Developmental delay and Cerebral palsy objectives 1. developmental delay Define developmental delay Etiologies of developmental delay Present the differential diagnosis of developmental delay. 2. cerebral
Developmental delay and Cerebral palsy objectives 1. developmental delay Define developmental delay Etiologies of developmental delay Present the differential diagnosis of developmental delay. 2. cerebral
Paediatric Clinical Guidelines: Status Epilepticus
 Paediatric Clinical Guidelines: Status Epilepticus Consultant: Dr Alastair Sutcliffe, Dr Christina Petrololous, Dr Tom Bailey Pharmacist: Simon Keady/Neil Tickner To be reviewed: Autumn 2010 The following
Paediatric Clinical Guidelines: Status Epilepticus Consultant: Dr Alastair Sutcliffe, Dr Christina Petrololous, Dr Tom Bailey Pharmacist: Simon Keady/Neil Tickner To be reviewed: Autumn 2010 The following
How To Treat Alcohol Withdrawal In The Elderly
 ALCOHOL ABUSE AND WITHDRAWAL SYNDROME IN THE ELDERLY Colin Muscat Family Medicine Case 90 year old Female Lives with son on vacation Admitted for FTT Consult -? GARP Develops increasing confusion during
ALCOHOL ABUSE AND WITHDRAWAL SYNDROME IN THE ELDERLY Colin Muscat Family Medicine Case 90 year old Female Lives with son on vacation Admitted for FTT Consult -? GARP Develops increasing confusion during
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
 ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
Mental health issues in the elderly. January 28th 2008 Presented by Éric R. Thériault etheriau@lakeheadu.ca
 Mental health issues in the elderly January 28th 2008 Presented by Éric R. Thériault etheriau@lakeheadu.ca Cognitive Disorders Outline Dementia (294.xx) Dementia of the Alzheimer's Type (early and late
Mental health issues in the elderly January 28th 2008 Presented by Éric R. Thériault etheriau@lakeheadu.ca Cognitive Disorders Outline Dementia (294.xx) Dementia of the Alzheimer's Type (early and late
TCHP Behavioral Health Psychological/Neuropsychological Testing Child/Adolescent Guidelines
 TCHP Behavioral Health Psychological/Neuropsychological Testing Child/Adolescent Guidelines Psychological testing involves the culturally and linguistically competent administration and interpretation
TCHP Behavioral Health Psychological/Neuropsychological Testing Child/Adolescent Guidelines Psychological testing involves the culturally and linguistically competent administration and interpretation
About 2 to 5 percent of Americans
 Evaluation of a First Seizure STEPHEN M. ADAMS, MD, and PAUL D. KNOWLES, MD, University of Tennessee College of Medicine, Chattanooga Unit, Chattanooga, Tennessee Seizure is a common presentation in the
Evaluation of a First Seizure STEPHEN M. ADAMS, MD, and PAUL D. KNOWLES, MD, University of Tennessee College of Medicine, Chattanooga Unit, Chattanooga, Tennessee Seizure is a common presentation in the
The Nuts and Bolts of Multiple Sclerosis. Rebecca Milholland, M.D., Ph.D. Center for Neurosciences
 The Nuts and Bolts of Multiple Sclerosis Rebecca Milholland, M.D., Ph.D. Center for Neurosciences Objectives Discuss which patients are at risk for Multiple Sclerosis Discuss the diagnostic criteria for
The Nuts and Bolts of Multiple Sclerosis Rebecca Milholland, M.D., Ph.D. Center for Neurosciences Objectives Discuss which patients are at risk for Multiple Sclerosis Discuss the diagnostic criteria for
Behavioral Health Psychological/Neuropsychological Testing Guidelines
 Behavioral Health Psychological/Neuropsychological Testing Guidelines Psychological testing (procedural code 96101) and Neuropsychological Testing (procedural code 96118) involve the culturally and linguistically
Behavioral Health Psychological/Neuropsychological Testing Guidelines Psychological testing (procedural code 96101) and Neuropsychological Testing (procedural code 96118) involve the culturally and linguistically
Alcohol-Related Seizures
 Alcohol-Related Seizures David McMicken, MD*, Jonathan L. Liss, MD KEYWORDS Seizures Alcohol withdrawal Benzodiazepines Among the various medical problems related to alcohol abuse, the differential diagnosis
Alcohol-Related Seizures David McMicken, MD*, Jonathan L. Liss, MD KEYWORDS Seizures Alcohol withdrawal Benzodiazepines Among the various medical problems related to alcohol abuse, the differential diagnosis
Managing Epileptic Dogs By William B. Thomas, DVM,MS, University of Tennessee
 Managing Epileptic Dogs By William B. Thomas, DVM,MS, University of Tennessee KEY FACTS * Poor seizure control may result from inaccurate diagnosis of underlying disease, insufficient client education,
Managing Epileptic Dogs By William B. Thomas, DVM,MS, University of Tennessee KEY FACTS * Poor seizure control may result from inaccurate diagnosis of underlying disease, insufficient client education,
Introduction. What is syncope?
 Syncope Introduction What is syncope? Syncope (SING-kuh-pee) is a medical term for fainting. When you faint, your brain is not receiving enough blood and oxygen, so you lose consciousness temporarily.
Syncope Introduction What is syncope? Syncope (SING-kuh-pee) is a medical term for fainting. When you faint, your brain is not receiving enough blood and oxygen, so you lose consciousness temporarily.
1. According to recent US national estimates, which of the following substances is associated
 1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Acquired, Drug-Induced Long QT Syndrome
 Acquired, Drug-Induced Long QT Syndrome A Guide for Patients and Health Care Providers Sudden Arrhythmia Death Syndromes (SADS) Foundation 508 E. South Temple, Suite 202 Salt Lake City, Utah 84102 800-STOP
Acquired, Drug-Induced Long QT Syndrome A Guide for Patients and Health Care Providers Sudden Arrhythmia Death Syndromes (SADS) Foundation 508 E. South Temple, Suite 202 Salt Lake City, Utah 84102 800-STOP
Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) (APA, 2001) 10
 (APA, 2001) 10") 5. Diagnosis Questions to be answered: 5.1. What are the diagnostic criteria for ADHD in children and adolescents? 5.2. How is ADHD diagnosed in children and adolescents? Who must diagnose it? 5.3. Which
5. Diagnosis Questions to be answered: 5.1. What are the diagnostic criteria for ADHD in children and adolescents? 5.2. How is ADHD diagnosed in children and adolescents? Who must diagnose it? 5.3. Which
Naloxone: Effects and Side Effects
 Gregory W. Terman M.D., Ph.D. Professor Department of Anesthesiology and Pain Medicine and the Graduate Program in Neurobiology Mayday Pain and Society Fellow University of Washington Seattle, Washington
Gregory W. Terman M.D., Ph.D. Professor Department of Anesthesiology and Pain Medicine and the Graduate Program in Neurobiology Mayday Pain and Society Fellow University of Washington Seattle, Washington
Preconception Clinical Care for Women Medical Conditions
 Preconception Clinical Care for Women All women of reproductive age are candidates for preconception care; however, preconception care must be tailored to meet the needs of the individual. Given that preconception
Preconception Clinical Care for Women All women of reproductive age are candidates for preconception care; however, preconception care must be tailored to meet the needs of the individual. Given that preconception
Why study clinical neuropsychology?
 University Leiden, The Netherlands Master (MSc) in Clinical Neuropsychology H.A.M.Middelkoop@lumc.nl www.neuropsychologie.leidenuniv.nl Why study clinical neuropsychology? You are interested in: brain/behavior
University Leiden, The Netherlands Master (MSc) in Clinical Neuropsychology H.A.M.Middelkoop@lumc.nl www.neuropsychologie.leidenuniv.nl Why study clinical neuropsychology? You are interested in: brain/behavior
NeuroStar TMS Therapy Patient Guide for Treating Depression
 NeuroStar TMS Therapy Patient Guide for Treating Depression This NeuroStar TMS Therapy Patient Guide for Treating Depression provides important safety and use information for you to consider about treating
NeuroStar TMS Therapy Patient Guide for Treating Depression This NeuroStar TMS Therapy Patient Guide for Treating Depression provides important safety and use information for you to consider about treating
GUIDELINE FOR THE MANAGEMENT OF FIRST SEIZURE EMERGENCY DEPARTMENT IN THE. Stacy Turner; Jonathan Benger. December 2009
 GUIDELINE FOR THE MANAGEMENT OF FIRST SEIZURE IN THE EMERGENCY DEPARTMENT Stacy Turner; Jonathan Benger December 2009 For The College of Emergency Medicine CONTENTS 1. Executive Summary 3 2. Introduction
GUIDELINE FOR THE MANAGEMENT OF FIRST SEIZURE IN THE EMERGENCY DEPARTMENT Stacy Turner; Jonathan Benger December 2009 For The College of Emergency Medicine CONTENTS 1. Executive Summary 3 2. Introduction
Hair of the Dog. www.wellcon.net. Reference Information. Scope of the Problem. How To Avoid Being Bitten By Withdrawal Syndromes
 Hair of the Dog How To Avoid Being Bitten By Withdrawal Syndromes Reference Information Copies of slides and modified CIWA (Clinical Institute Withdrawal Assessment) scale available at: www.wellcon.net
Hair of the Dog How To Avoid Being Bitten By Withdrawal Syndromes Reference Information Copies of slides and modified CIWA (Clinical Institute Withdrawal Assessment) scale available at: www.wellcon.net
CLINICAL NEUROPHYSIOLOGY
 CLINICAL NEUROPHYSIOLOGY Barry S. Oken, MD, Carter D. Wray MD Objectives: 1. Know the role of EMG/NCS in evaluating nerve and muscle function 2. Recognize common EEG findings and their significance 3.
CLINICAL NEUROPHYSIOLOGY Barry S. Oken, MD, Carter D. Wray MD Objectives: 1. Know the role of EMG/NCS in evaluating nerve and muscle function 2. Recognize common EEG findings and their significance 3.
DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE
 1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
BIPOLAR DISORDER IN PRIMARY CARE
 E-Resource January, 2014 BIPOLAR DISORDER IN PRIMARY CARE Mood Disorder Questionnaire Common Comorbidities Evaluation of Patients with BPD Management of BPD in Primary Care Patient resource Patients with
E-Resource January, 2014 BIPOLAR DISORDER IN PRIMARY CARE Mood Disorder Questionnaire Common Comorbidities Evaluation of Patients with BPD Management of BPD in Primary Care Patient resource Patients with
Clinical Practice Guidelines: Attention Deficit/Hyperactivity Disorder
 Clinical Practice Guidelines: Attention Deficit/Hyperactivity Disorder AACAP Official Action: OUTLINE OF PRACTICE PARAMETERS FOR THE ASSESSMENT AND TREATMENT OF CHILDREN, ADOLESCENTS, AND ADULTS WITH ADHD
Clinical Practice Guidelines: Attention Deficit/Hyperactivity Disorder AACAP Official Action: OUTLINE OF PRACTICE PARAMETERS FOR THE ASSESSMENT AND TREATMENT OF CHILDREN, ADOLESCENTS, AND ADULTS WITH ADHD
Paxil/Paxil-CR (paroxetine)
") Generic name: Paroxetine Available strengths: 10 mg, 20 mg, 30 mg, 40 mg tablets; 10 mg/5 ml oral suspension; 12.5 mg, 25 mg, 37.5 mg controlled-release tablets (Paxil-CR) Available in generic: Yes, except
Generic name: Paroxetine Available strengths: 10 mg, 20 mg, 30 mg, 40 mg tablets; 10 mg/5 ml oral suspension; 12.5 mg, 25 mg, 37.5 mg controlled-release tablets (Paxil-CR) Available in generic: Yes, except
1. What are anti-epileptic drugs? Anti-epileptic drugs (AEDs) are prescribed to control seizures. They do not cure epilepsy.
 are prescribed to control seizures. They do not cure epilepsy.") 14 FREQUENTLY ASKED QUESTIONS ON ANTI- EPILEPTIC DRUGS 1. What are anti-epileptic drugs? Anti-epileptic drugs (AEDs) are prescribed to control seizures. They do not cure epilepsy. 2. When should treatment
14 FREQUENTLY ASKED QUESTIONS ON ANTI- EPILEPTIC DRUGS 1. What are anti-epileptic drugs? Anti-epileptic drugs (AEDs) are prescribed to control seizures. They do not cure epilepsy. 2. When should treatment
Assessment, diagnosis and specialist referral of adults (>16 years) with an episode of transient loss of consciousness (TLoC) or a blackout.
 with an episode of transient loss of consciousness (TLoC) or a blackout.") Assessment, diagnosis and specialist referral of adults (>16 years) with an episode of transient loss of consciousness (TLoC) or a blackout. TLoC is common huge variation in management range of clinicians
Assessment, diagnosis and specialist referral of adults (>16 years) with an episode of transient loss of consciousness (TLoC) or a blackout. TLoC is common huge variation in management range of clinicians
MOOD DISORDERS AND EPILEPSY
 MOOD DISORDERS AND EPILEPSY March 5 th, 2011 Michael Caucci, M.D. Vanderbilt University Department of Psychiatry and Obstetrics & Gynecology GOAL OF TALK Present different types of seizures Present different
MOOD DISORDERS AND EPILEPSY March 5 th, 2011 Michael Caucci, M.D. Vanderbilt University Department of Psychiatry and Obstetrics & Gynecology GOAL OF TALK Present different types of seizures Present different
trust clinical guideline
 CG23 VERSION 1.0 1/7 Guideline ID CG23 Version 1.0 Title Approved by Transient Loss of Consciousness Clinical Effectiveness Group Date Issued 01/01/2013 Review Date 31/12/2016 Directorate Authorised Staff
CG23 VERSION 1.0 1/7 Guideline ID CG23 Version 1.0 Title Approved by Transient Loss of Consciousness Clinical Effectiveness Group Date Issued 01/01/2013 Review Date 31/12/2016 Directorate Authorised Staff
FastTest. You ve read the book... ... now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
NEONATAL ABSTINENCE SYNDROME. Osama Naga, M.D. PGY2
 NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
NEONATAL ABSTINENCE SYNDROME Osama Naga, M.D. PGY2 Objective: Describe the common causes of NAS Clinical Presentation Diagnosis Identify the different scoring system for pharmacologic therapy Minimize
Usual total daily dosage *Indicates usual starting dose in mg/kg/day (mg of AED per kg of the child s weight per day) Drug (Generic Name)
 Drug (Generic Name)") Table of Anti Epileptic Drugs (AEDs) used in the treatment of Epilepsy in Children under 12. IMPORTANT All the tables below are guidelines only, giving average daily dose ranges. Treatment will generally
Table of Anti Epileptic Drugs (AEDs) used in the treatment of Epilepsy in Children under 12. IMPORTANT All the tables below are guidelines only, giving average daily dose ranges. Treatment will generally
Autonomic Dysfunction: Autonomic Non-Epileptic Seizures and the Autonomic Epilepsies
 Autonomic Dysfunction: Autonomic Non-Epileptic Seizures and the Autonomic Epilepsies James J. Riviello, Jr., MD Sergievsky Family Professor of Neurology and Pediatrics Director, Division of Child Neurology
Autonomic Dysfunction: Autonomic Non-Epileptic Seizures and the Autonomic Epilepsies James J. Riviello, Jr., MD Sergievsky Family Professor of Neurology and Pediatrics Director, Division of Child Neurology
Do I Have Epilepsy? Diagnosing Epilepsy and Seizures. Epilepsy & Seizures: Diagnosis
 Epilepsy & Seizures: Diagnosis Do I Have Epilepsy? Diagnosing Epilepsy and Seizures Artwork by Studio E participant Ashley N. (details on inside cover) About the Cover: Cover artwork was created by Ashley
Epilepsy & Seizures: Diagnosis Do I Have Epilepsy? Diagnosing Epilepsy and Seizures Artwork by Studio E participant Ashley N. (details on inside cover) About the Cover: Cover artwork was created by Ashley
The Adverse Health Effects of Cannabis
 The Adverse Health Effects of Cannabis Wayne Hall National Addiction Centre Kings College London and Centre for Youth Substance Abuse Research University of Queensland Assessing the Effects of Cannabis
The Adverse Health Effects of Cannabis Wayne Hall National Addiction Centre Kings College London and Centre for Youth Substance Abuse Research University of Queensland Assessing the Effects of Cannabis
Glasgow Assessment and Management of Alcohol
 Glasgow Assessment and Management of Alcohol If you would like further information or advice on the alcohol screening and withdrawal management guideline(gmaws) please contact your local acute addiction
Glasgow Assessment and Management of Alcohol If you would like further information or advice on the alcohol screening and withdrawal management guideline(gmaws) please contact your local acute addiction
PSYCHOLOGICAL AND NEUROPSYCHOLOGICAL TESTING
 Status Active Medical and Behavioral Health Policy Section: Behavioral Health Policy Number: X-45 Effective Date: 01/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
Status Active Medical and Behavioral Health Policy Section: Behavioral Health Policy Number: X-45 Effective Date: 01/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
EPIDEMIOLOGY OF OPIATE USE
 Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
FUNCTIONAL EEG ANALYZE IN AUTISM. Dr. Plamen Dimitrov
 FUNCTIONAL EEG ANALYZE IN AUTISM Dr. Plamen Dimitrov Preamble Autism or Autistic Spectrum Disorders (ASD) is a mental developmental disorder, manifested in the early childhood and is characterized by qualitative
FUNCTIONAL EEG ANALYZE IN AUTISM Dr. Plamen Dimitrov Preamble Autism or Autistic Spectrum Disorders (ASD) is a mental developmental disorder, manifested in the early childhood and is characterized by qualitative
Stroke Thrombolysis Awareness. Initial patient assessment. Using F.A.S.T., Rosier, & NIHSS Tools
 Stroke Thrombolysis Awareness Initial patient assessment Using F.A.S.T., Rosier, & NIHSS Tools Adapted from 5 Acute Trusts - 6 Primary Care Trusts Ambulance Trust 4 Local Authorities Aims Improve recognition
Stroke Thrombolysis Awareness Initial patient assessment Using F.A.S.T., Rosier, & NIHSS Tools Adapted from 5 Acute Trusts - 6 Primary Care Trusts Ambulance Trust 4 Local Authorities Aims Improve recognition
Guidelines for Clinical Neurophysiology
 Guidelines for Clinical Neurophysiology These Guidelines have been drawn up along the lines of those of the Department of Clinical Radiology to help referring clinicians make the best use of Clinical Neurophysiology.
Guidelines for Clinical Neurophysiology These Guidelines have been drawn up along the lines of those of the Department of Clinical Radiology to help referring clinicians make the best use of Clinical Neurophysiology.
Antipsychotic drug prescription for patients with dementia in long-term care. A practice guideline for physicians and caregivers
 SUPPLEMENT 1: (Supplementary Material for online publication) Antipsychotic drug prescription for patients with dementia in long-term care. A practice guideline for physicians and caregivers About this
SUPPLEMENT 1: (Supplementary Material for online publication) Antipsychotic drug prescription for patients with dementia in long-term care. A practice guideline for physicians and caregivers About this
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
GUIDELINES FOR COMMUNITY ALCOHOL DETOXIFICATION IN SHARED CARE
 GUIDELINES FOR COMMUNITY ALCOHOL DETOXIFICATION IN SHARED CARE Dr Millicent Chikoore MBBS MRCPsych Dr O Lagundoye MBBS MRCPsych Community based alcohol detoxification is a safe and effective option for
GUIDELINES FOR COMMUNITY ALCOHOL DETOXIFICATION IN SHARED CARE Dr Millicent Chikoore MBBS MRCPsych Dr O Lagundoye MBBS MRCPsych Community based alcohol detoxification is a safe and effective option for
Diabetic Emergencies. David Hill, D.O.
 Diabetic Emergencies David Hill, D.O. Class Outline Diabetic emergency/glucometer training Identify the different signs of insulin shock Diabetic coma, and HHNK Participants will understand the treatment
Diabetic Emergencies David Hill, D.O. Class Outline Diabetic emergency/glucometer training Identify the different signs of insulin shock Diabetic coma, and HHNK Participants will understand the treatment