Sensational Sensors Real Time Continuous Glucose Sensors. Marcia Miller RN, MSN ARNP
|
|
|
- Rolf Harris
- 7 years ago
- Views:
Transcription


1 Sensational Sensors Real Time Continuous Glucose Sensors Marcia Miller RN, MSN ARNP
2 Objectives Identify models of professional and personal CGMS with and without pump tx Discuss evidence based guidelines for use of CGMS in pediatrics and adults. Describe basic functions of CGMS for acceptance and accuracy of sensors. Review software for analysis of BS levels for improved pt outcomes

3 All CGMS Measures levels of glucose in interstitial fluid every 3-5 minutes ISF proven reasonably assessable ISF reflects concentrations in the brain Lag time between serum BS and ISF Cell s Cell s Cell s Cell s Cell s Interstitial fluid Cell s
4 How does the. glucose sensor work? Glucose + O 2 The sensor soaks up fluid from ISF. The fluid contains oxygen and glucose During the initial wetting period (5 minutes), the fluid (glucose and oxygen) diffuses through the membrane and reacts with the glucose oxidase Gluconic Acid + H 2 O 2 Electrode Membrane Glucose Oxidase 2e - H 2 O 2H + + O e Sensor - signal End of the reaction, the electrode produces a current that is measured as the sensor signal (ISIG). This energy signal is turned into a glucose number ISIG = the signal
5 Site Differences in Glucose Testing Sensor Interstitial versus Capillary Sensor and SMBG are testing at different sites Interstitial Space Sensor mirrors its reading to match SMBG, a process called calibration Skin Cells Capillary Sensor reading and Meter readings should be 20% of each other.
6 Glucose Concentration (mg/dl) A1C versus Glycemic Variability Patients with average A1C of < 7% (ADA goal) 400 Mean A1C 6.7% AM 4AM 8AM 12PM 4PM 8PM 12AM A normal or low A1C may be the result of hypoglycemic events Amylin internal date (Medtronic Diabetes obtained permission to use)
7


8 ipro Models of CGMS Professional Model Blinded so pt cannot see results Pt wears sensor for >48 hrs with easy set up Pt journals food, activity and meds for 3 + days Later downloaded and reviewed with HCP and pt Great visual Detect problems with pt current behavior Ipro with Medtronic and DexCom set to blinded
9 I Professional Blinded CGMS Alternative for pt who cannot take advantage of real time CGMS Easy to put on and use Great visual *Help pt awareness of effects of current regimen Pts with nocturnal hypoglycemia Pts changing to new insulin regimen
10 MDI: Glargine HS and RA at Meals Lab 6.7% A1C
11 Candidates for Professional CGM? Patients with discrepancies between A1C and SMBG Unable to achieve goal with SMBG Patients who are pregnant Insulin requiring patients Type 2 patients with increased CV risk Patients with repeated hypoglycemia Pts not ready for RT-CGMS
12 Professional CGM Service Reimbursement Code Purpose Providers Description Payment Level ($) Professional CGM: CGM technical Training Any HCPs Patient training, hookup, removal, download Can be billed more than once based on payor coverage Medicare: ~ $145* Private: ~ $165** Professional CGM: CGM professional interpretation MD/DO NP/PA Data interpretation Can be used for non face-to-face time Can be billed more than once based on payor coverage Medicare: ~ $38* Private: ~ $40**. Individual coverage depends on insurance plan and clinical situation * PMIC Medical Fees in the U.S **All payment levels are estimated average based on Medtronic internal EOB data (October 2008)
13 Real Time CGMS Stand alone Dex Com Seven Plus Guardian RT(Medtronic) FreeStyle Navigator (Abbott DC d in USused internationally) Integrated with pump Animas Vibe with Dexcom in future Medtronic Paradigm Pump (522/722 series and Revel= 523/723 series)
14
15
16
17
18 All RT- CGMS show. BS level Trends of BS levels Rate of change 1 arrow changing 2-3 mg/min (20mg hour) 2 arrows 4-5 mg/min (30-40 mg hr) Alarms for low and high set points
19
20
21 Patient Perspective from U-Tube
22
23 Pump and Sensor Advantages Transmitter is pump Same adv as all CGMS HCP can see everything.. carbs, insulin, BS,Trends Area under/over the curve Predictive alerts Disadvantage Wearing too much?? Information overload Nuisance alarms
24 Many Trails RT-CGMS 1. Eurthicmics Trial (2009 European Ass.) 1. SAP vs MDI/BSM decreased A1C 1.1 % Achieved A1C <7 in 34.1 % pts 2. Real Trend (Diabetes Care 2009) 2. SAP vs Pump/BSM decreased A1C by.96% in pts wearing CGMS >70% time (1/2 children)
25 3.JDRF CGM Study Group CGMS and Intensive Treatment of Type 1 n engl j med 359;14, october 2, 2008 Pump/ MDI + CGMCGM Medtronic, DexCom & Abbott Pump or MDI with SBGM Hypoglycemia didn t differ in tx groups Consistent use of CGMS predicts A1C reduction AGE 6mo A1c CGMS 6mo A1c SBSM %Time Worn
26 Diabetes Care Jan Short and Long Term Effects of RT-CGMS with Type 2 diabetes 12 wks of RT-CGM vs SBGM on Type 2 pts NOT on prandial insulin receiving care from PCP. Improved A1C at 12 wks and sustained at 24 wks 40 wk FU. (without CGMS) No change in any meds just awareness of what effects BS levels
27 AACE CGM Task Force Authors AACE members and CGM thought-leaders Thomas C. Blevins, MD, FACE Bruce W. Bode, MD, FACE Satish K. Garg, MD George Grunberger, MD, FACP, FACE Irl B. Hirsch, MD Lois Jovanovic, MD, MACE Elizabeth Nardacci, FNP, CDE, BC-ADM Eric A. Orzeck, MD, FACP, FACE Victor L. Roberts, MD, MBA, FACP, FACE Objective of Consensus Statement: Provide a credible source of opinions and recommendations on how to best use and succeed with CGM therapy William V. Tamborlane, MD
28 Continuous glucose monitoring (CGM) technology is not only novel, but it can improve the lives of patients who incorporate it into a comprehensive diabetes management plan. -- AACE Consensus Statement on CGM
29 AACE Reviews Clinical Evidence on CGM Professional Can identify undetected hyperglycemia in pregnant women Professional CGM identified minutes/day of undetected hyperglycemia in studies 1,2,3 Effective in improving maternal glycemic control, infant birth weight, and macrosomia risk in women with type 1 or type 2 diabetes 4,5
30 AACE -Ideal Candidates for Professional CGM 1. Pts with type 1 or type 2 diabetes who: are not at their A1C target. have recurrent hypoglycemia or hypo unawareness. 2. All pregnant women with type 1 diabetes. 3. May increase tx adherence for women with type 2 diabetes or insulin-requiring gestational diabetes 4. Intermittent use may be useful for youth with type 1 diabetes who are changing their diabetes regimen or are experiencing nocturnal hypo, dawn phenomenon, hypo unawareness, or post-prandial hyperglycemia. 5. Recommended to use Professional CGM on an episodic basis.
31 AACE CLINIC REVIEWS PERSONAL Can reduce A1C in adult and pediatric patients with type 1 diabetes and A1C > 7.0%, without increasing hypoglycemia in adult and pediatric patients 6,7 In adults and adolescents, more consistent use predicts successful A1C reductions 7 Can reduce hypoglycemia in well-controlled adult and youth patients (A1C<7.0%) with type 1 diabetes, without increasing A1C 8
32 AACE Ideal Candidates for Personal CGM Patients with type 1 diabetes with: Hypoglycemia unawareness or frequent hypoglycemia. A1C above target or with excess glucose variability. Requires lowering A1C without increased hypoglycemia. During preconception and pregnancy. Children and adolescents who have met A1C targets (<7.0%) and who may be highly motivated. Youth with A1C levels 7.0% and are able to use the device on a neardaily basis. Maybe good candidates and trial period of 2-4 weeks is recommended: Youth who frequently monitor their blood glucose levels. Committed families of children (younger than 8 years) especially if the patient is having problems with hypoglycemia.
33 2011 Endocrine Society CGMS Practice Guidelines Children/Adolescents with T1DM > 7yo Use when A1C <7% to help maintain A1C without increased hypoglycemia. Use with children and adolescents with T1DM with A1C >7% who are able to use on daily basis.
34 2011 Practice Guidelines (Continued) Use intermittent personal /professional CGMS when concerned with: Nocturnal hypoglycemia Dawn phenomenon Hypoglycemic unawareness PP hyperglycemia Changes in insulin therapy
35 Practice Guidelines Continued No recommendations for or against with children less 7 yo Adult recommendations the same as pediatrics Not recommended for inpt ICU or Surgical settings due to accuracy concerns, co-morbidities and hypoglycemic risks
36 Setting the Right Expectations For Patients CGM is not a fingerstick replacement - fingersticks are needed to: Calibrate the system Before making a treatment decisions Sensor glucose (SG) and blood glucose (BG) meter values will rarely be identical, however, SG readings are clinically accurate Studies show more improvement in A1C the more frequently you wear it and look at the receiver (Don t put it on and forget about it)
37 Secrets to make Sensors Sensational..Not Frustrating 1. Calibration 2. SG BG with Lag Time 3. Focus on Trends not BS 4. Insertion/ Comfort 5. Wetting 6. Alerts and Alarms 7. Software for interpretation
38 #1 Calibration Pairing of fingerstick (FS) value to ISF space value Teaches sensor to recognize glucose value to responds to electrical current Reference of sensor mathematical algorithm to calculate BS levels of sensors Essential for optimal outcomes/performance of sensor.
39 When Should I Calibrate? 1. *Must be done when BS not changing for Medtronic. Changing BS OK with DexCom. 2. Must be done 2 hrs after insertion, within 6 hrs later and then q 12hrs. 3. Calibrating before bedtime will help you avoid a METER BG NOW during sleep. 4. Can insert sensor and leave for 2+ hours (HS) and turn sensor on later ( in AM). Sensor will ask you to calibrate with in 5 minutes when BS stable.
40 #2. Lag Time Physiologic lag times 5-10 min. & more with rapid change in BS CGMS show relative difference is 10-20% for different BS ranges Only 60-80% in Clarks A- Zone (lower than SBGM) Maybe due to calibrating in home setting.
41 Differences Between Sensor & Meter Glucose Values Why don t they match exactly? Physiologic lag time Technological lag time Sensor glucose values are updated on the pump every 5 minutes Blood glucose (BG) meter Inaccurate meter readings (related to the meter/strip maintenance, poor hand washing and variability in meter technology) Human Error Not calibrating properly (time of BG change, late BG entries, rounding) Not enough calibrations Too many calibrations
42 #3 CGM Trends Take the focus AWAY from the number!
43


44 #5: Insertion 45-60º Introducer needle should be pulled out at the same angle it is inserted Hold gently Do not twist or wiggle the needle when removing
45 Key to Success #4: Insertion 90º
46 #5. Insertion Sites Best sites: Abdominal area or hip area Chose a site that is at least 2 inches away from your naval, 2 inches away from your insulin pump site or 3 inches away from any manual injection site Chose a site that is not restricted by clothing Rotate sites Position glucose sensor 5-6 feet from the insulin pump/monitor (to avoid lost sensor)
47 Superhero
48 #5: Wetting Wait minutes for sensor to wet before connecting transmitter. Avoid inserting sensor into areas that have become thick or hardened Lost Sensor and Sensor Error alarms during the 2 hour initialization time are common if the sensor is not properly wetted.
49 # 6. Alerts/Alarms Common Alerts METER BG NOW SENSR END WEAK SIGNAL Instructions Meter fingerstick is needed to update glucose sensor and continue receiving sensor glucose information Glucose sensor is at the end of its 3 day use and needs to be replaced Insulin pump has not received data for a period of time: Move insulin pump closer to transmitter and check connection
50 Alerts /Alarms CAL ERROR BAD SENSOR SENSOR ERROR Make sure glucose is not changing rapidly then recalibrate If during or shortly after start-up then clear it and continue with or redo start-up: Otherwise replace the glucose sensor Out of range reading is detected by transmitter: Clear the alarm If this alarm occurs repeatedly: Change the glucose sensor

51 #6. Alerts/Alarms ALERTS must be managed and personalized. Some are initiating sensor with high sensor glucose alerts OFF.

52
53 CGM Considerations for CGMS Start -Dr. Fran Kaufman Predictive Alarm High Initial Setting OFF or 15 min. Hypo Unaware Low OFF or 20 min 30 min. Rate of Change Alarm Rise OFF or > 4.0mg/dl/min Fall OFF or > 4.0mg/dl/min < 4.0 mg/dl/min High Alert OFF or 250 Low Alert 70mg/dl 100mg/dl
54
55
56
57
58
59
60
61
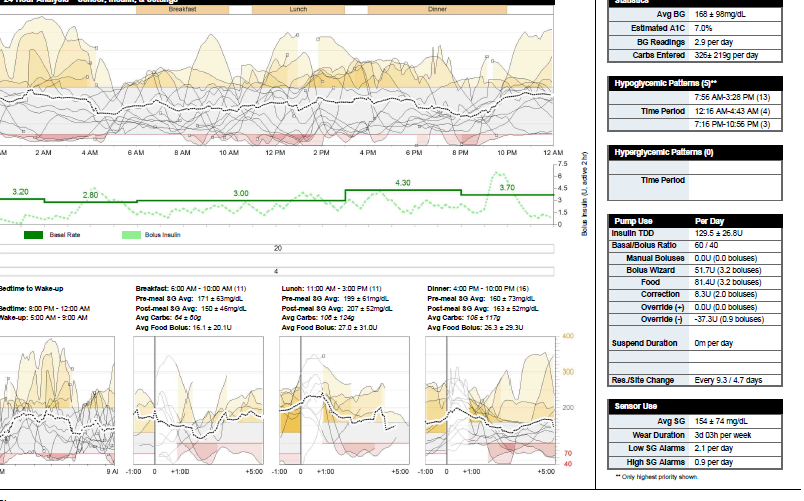
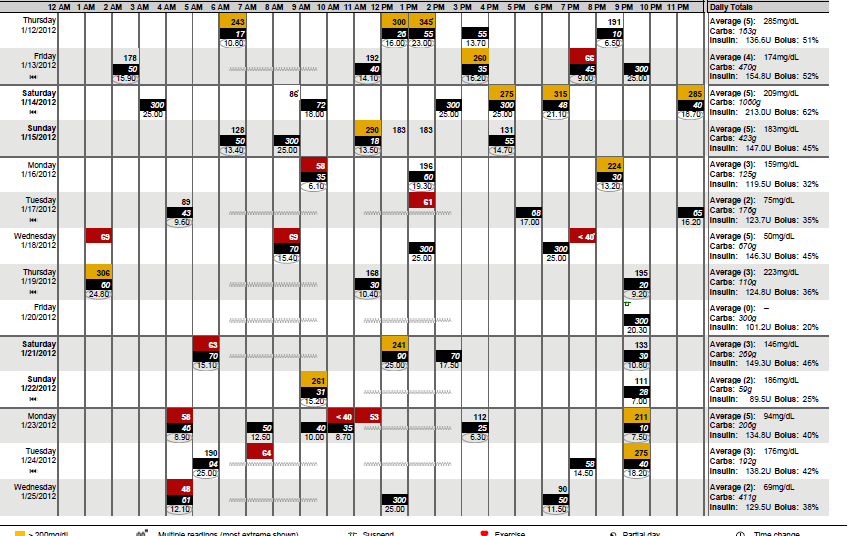
62 Begin with two reports Daily Summary Sensor Daily Overlay Medtronic Carelink Personal and Pro Daily Summary shows information about the number of sensor alerts each day, amount of insulin taken, and carbohydrates eaten.
63 Sensor Overlay Gold: Above Target Gap in Sensor Data Red: Below Target Avg. Sensor Glucose


64 Overnight and Meal Sensor Overlays This graph combines the sensor glucose tracing recorded between bedtime and wake-up. These graphs combine the pre-meal and post-meal sensor glucose tracings. Time food was entered in the Bolus Wizard
65 Therapy Management Dashboard Overview Snapshot of the key patient information on one page Allows HCPs to see sensor glucose, insulin delivery, and key settings in a visual format Specific hypo- and hyperglycemia pattern identification New pump and sensor statistics such as override data and Estimated A1C To generate the Therapy Management Dashboard and Episode Summary, 5 days of sensor and pump data are needed.
66 Statistics Table Avg. BG: Average of all BG meter readings obtained and the standard deviation. Estimated A1C: Calculated using sensor data over the selected reporting period. Estimated A1C = (Avg. SG )/28.7* BG Readings: Average number of BG meter readings obtained per day. Carbs Entered: Average daily carbohydrate intake and the standard deviation. * Nathan, David M., et al. Translating the A1C Assay Into Estimated Average Glucose Values. Diabetes Care. 31(2008).
67 Hyperglycemic Patterns Table Number of Patterns Time of Pattern Notes: The top 3 hyper patterns are listed based on the magnitude of AUC. If two asterisks appear in the title bar, this indicates that there are >3 patterns and refers to a note at the bottom of the page that states Only highest priority shown.
68 Pump Use Table Insulin TDD: Average total daily dose of insulin and the standard deviation. Basal/Bolus Ratio: The ratio of basal to bolus insulin delivered (% of total for each). Manual Boluses: Avg. daily amount of insulin delivered using manual boluses, and the avg. number of manual boluses delivered per day.
69 Pump Use Table (Continued) Bolus Wizard: Avg. daily amount of insulin delivered using the BW, and the avg. number of boluses delivered for food each day. Food: Avg. daily amount of insulin recommended for food, and the avg. number of boluses delivered for food each day. Correction: Avg. daily amount of insulin recommended for correction, and the avg. # of correction boluses delivered each day. Override (+): Avg. daily amount of insulin increased over the recommended amount, and the avg. # of positive overrides each day. Override (-): Avg. daily amount of insulin reduced over the recommended amount, and the avg. # of negative overrides each day.
70 Pump Use Table (Continued) Suspend Duration: Avg. daily time in minutes spent with insulin delivery suspended manually by the user. Res./Site Change: Avg. time in days between reservoir changes based upon manual prime (tubing fill) events, and the avg. time between infusion set changes based upon fixed prime (cannula fill) events.

71 Pump and Sensor Settings
 esp.")
72 Sensor Alerts Predictive Alert is same as Rate of Change but alarms at rate set ( mg/min) esp. helpful if not looking at pump Area under the curve (AUC)- another new measurement!
73 Area Under the Curve (AUC) Provides insight to how long (duration) glucose is high or low and the severity (magnitude) of the excursion Only available with CGM AUC High and Low Limits are set independently AUC= Area under or over set target limits Total number date points
74 AUC Expect small change in an AUC Low value to be more significant than the same change in an AUC High value ZERO: The closer an AUC value is to zero, the closer you are to your target limit APPLES TO APPLES: Identical AUC Set Limits must be used to compare AUC values USAGE: AUC CANNOT be used alone to make specific treatment changes CALCULATING AUC does NOT mean averaging high or low glucose values
75 Sensor Use Table Avg SG: Avg. of all sensor glucose values obtained and the standard deviation. Wear Duration: Avg. amount of time per week with sensor glucose data. Low SG Alarms: Avg. number of low sensor glucose threshold and predictive alerts per day. High SG Alarms: Avg. number of high sensor glucose threshold and predictive alerts per day.
76 Episode Summary Overview Provides a summary of the hypo- and hyperglycemic episodes and events preceding those episodes Offers therapy considerations based on the most common events observed for hypo- and hyperglycemic episodes Offers therapy considerations for other behaviors related to pump, CGM, and BG meter usage
77 Hypo- and Hyperglycemic Episode Bar Charts Total Number of Episodes Threshold Most events occur within 3 hours prior to the episode Preceding Event Number of Episodes Preceded by the Event

78 Event Pie Charts Total Event Occurrences Percentage of Occurrences that Preceded an Episode
79 Event Description Tables Event Percentage of time event preceded total number of episodes Therapy Consideration
80 Other Observations Table Observation Therapy Consideration(s)
81
82
83
84
85
86
87
88
89
90 Case Studies Lets Practice!
91 Case Studies 1. I PRO 62 yo F T2DM on metformin and TID u500 insulin. A1C Dex Com 3.Medtronic 722& CGMS 56 yo F on MDI Levimer 13 units AM, 12 units PM ;Novolog 1/20 g CHO & correct 1/50 >150 & Symlin 60 mcg AC A1C 5.8% 35 yo male on 722 Medtronic pump for 3 years and CGMS for 6 months p seizure A1C 7.2%
92
93
94
95
96
97
98
99
100
101
102 Case #1 Suggestions?
103 Case #2
104
105
106
107
108
109
110
111 Case #2 Suggestions?

112 Case #3
113 #3 SAP

114

115
116
117
118 1/23-25
119 Suggestions for Case #3
120 CGMS Conclusions Use of CGM require a steep learning curve, so HCP and payers are slow to accept. CGMS is not perfect and can cause frustration for pts and clinicians. Concerns with limited reimbursement for technology itself and HCP time and resources. More Research needed on use in hospital setting.
121 Honoring the past while reaching the Future Compare past to urine testing in the 80 s and acceptance of BSM High amount of education on proper technique for accuracy Need to work with MD s, Patients and Payers and Companies for acceptance CGMS is so similar to moving forward with CGMS.
Basal and Bolus Insulin 7/16/2014. Jackie Aday RN, BSN, CDE Jeni Neighbors RN, BSN, CDE. BASAL: Small amount of insulin infused every few minutes
 Jackie Aday RN, BSN, CDE Jeni Neighbors RN, BSN, CDE Insulin Pump Therapy Open looped system in which a small amount of insulin is continuously infused through a cannula or needle (basal rate) Larger doses
Jackie Aday RN, BSN, CDE Jeni Neighbors RN, BSN, CDE Insulin Pump Therapy Open looped system in which a small amount of insulin is continuously infused through a cannula or needle (basal rate) Larger doses
Insulin Pump Management and Continuous Glucose Monitoring Systems (CGMS)
") Insulin Pump Management and Continuous Glucose Monitoring Systems (CGMS) Faith Daily, RN, BSN, CDE, CPT Certified Diabetes Educator/Insulin Pump Trainer August 16, 2014 Why Pump Therapy? Mimics normal
Insulin Pump Management and Continuous Glucose Monitoring Systems (CGMS) Faith Daily, RN, BSN, CDE, CPT Certified Diabetes Educator/Insulin Pump Trainer August 16, 2014 Why Pump Therapy? Mimics normal
Alternative method for delivering insulin using continuous subcutaneous insulin infusion (CSII) open loop system
 open loop system") ISHP Spring CE Conference April 12, 2015 St. Luke s Medical Center Randi Lynn Griffiths, PharmD Clinical outpatient pharmacist Boise VA Medical Center Boise, Idaho Alternative method for delivering insulin
ISHP Spring CE Conference April 12, 2015 St. Luke s Medical Center Randi Lynn Griffiths, PharmD Clinical outpatient pharmacist Boise VA Medical Center Boise, Idaho Alternative method for delivering insulin
AACE Consensus Statement
 AACE Consensus Statement Thomas C. Blevins, MD, FACE; Bruce W. Bode, MD, FACE; Satish K. Garg, MD; George Grunberger, MD, FACP, FACE; Irl B. Hirsch, MD; Lois Jovanovič, MD, MACE; Elizabeth Nardacci, FNP,
AACE Consensus Statement Thomas C. Blevins, MD, FACE; Bruce W. Bode, MD, FACE; Satish K. Garg, MD; George Grunberger, MD, FACP, FACE; Irl B. Hirsch, MD; Lois Jovanovič, MD, MACE; Elizabeth Nardacci, FNP,
Medical Benefit Effective Date: 04/01/11 Next Review Date: 01/13 Preauthorization* Yes Review Dates: 07/07, 07/08, 07/09, 01/10, 01/11, 01/12
 Continuous or Intermittent Monitoring of Glucose in Interstitial (10120) Medical Benefit Effective Date: 04/01/11 Next Review Date: 01/13 Preauthorization* Yes Review Dates: 07/07, 07/08, 07/09, 01/10,
Continuous or Intermittent Monitoring of Glucose in Interstitial (10120) Medical Benefit Effective Date: 04/01/11 Next Review Date: 01/13 Preauthorization* Yes Review Dates: 07/07, 07/08, 07/09, 01/10,
The Quantified Self on Steroids: Innovation in Devices, Pumps and Monitors
 The Quantified Self on Steroids: Innovation in Devices, Pumps and Monitors Howard A. Wolpert, MD 1 Diabetes is different to many other conditions Patient/Self Managed 2 To achieve the therapeutic goals
The Quantified Self on Steroids: Innovation in Devices, Pumps and Monitors Howard A. Wolpert, MD 1 Diabetes is different to many other conditions Patient/Self Managed 2 To achieve the therapeutic goals
Insulin Pump Therapy and Continuous Glucose Sensor Use in the Management of Diabetes Mellitus
 Insulin Pump Therapy and Continuous Glucose Sensor Use in the Management of Diabetes Mellitus Louis Haenel, IV, DO, FACOI, FACE Endocrinology Roper Hospital Charleston, SC Dr. Louis Haenel IV has disclosed
Insulin Pump Therapy and Continuous Glucose Sensor Use in the Management of Diabetes Mellitus Louis Haenel, IV, DO, FACOI, FACE Endocrinology Roper Hospital Charleston, SC Dr. Louis Haenel IV has disclosed
Medical Coverage Policy Glucose Monitoring Systems sad
 Medical Coverage Policy Glucose Monitoring Systems sad EFFECTIVE DATE: 03 03 2009 POLICY LAST UPDATED: 01 17 2012 OVERVIEW This policy addresses several methods of monitoring blood glucose: the glucometer,
Medical Coverage Policy Glucose Monitoring Systems sad EFFECTIVE DATE: 03 03 2009 POLICY LAST UPDATED: 01 17 2012 OVERVIEW This policy addresses several methods of monitoring blood glucose: the glucometer,
Challenges in Glycemic Control in Adult and Geriatric Patients. Denyse Gallagher, APRN-BC, CDE Endocrinology Nurse Practitioner
 Challenges in Glycemic Control in Adult and Geriatric Patients Denyse Gallagher, APRN-BC, CDE Endocrinology Nurse Practitioner Provide an overview of diabetes prevalence; discuss challenges and barriers
Challenges in Glycemic Control in Adult and Geriatric Patients Denyse Gallagher, APRN-BC, CDE Endocrinology Nurse Practitioner Provide an overview of diabetes prevalence; discuss challenges and barriers
4/7/2015 CONFLICT OF INTEREST DISCLOSURE OBJECTIVES. Conflicts of Interest None Heather Rush. Heather M. Rush, APRN, CDE Louisville, KY
 Heather M. Rush, APRN, CDE Louisville, KY CONFLICT OF INTEREST DISCLOSURE Conflicts of Interest None Heather Rush A conflict of interest exists when an individual is in a position to profit directly or
Heather M. Rush, APRN, CDE Louisville, KY CONFLICT OF INTEREST DISCLOSURE Conflicts of Interest None Heather Rush A conflict of interest exists when an individual is in a position to profit directly or
Smart Pumping with Insulin Pumps
 Smart Pumping with Insulin Pumps Rita Ketay RN, CDE, Ed.M, BC-ADM Dartmouth Hitchcock Medical Center During this discussion we will: * Review the DCCT recommendations; * Define smart pumping ; * Discuss
Smart Pumping with Insulin Pumps Rita Ketay RN, CDE, Ed.M, BC-ADM Dartmouth Hitchcock Medical Center During this discussion we will: * Review the DCCT recommendations; * Define smart pumping ; * Discuss
Corporate Medical Policy
 Corporate Medical Policy Continuous Monitoring of Glucose in the Interstitial Fluid File Name: Origination: Last CAP Review: Next CAP Review: Last Review: continuous_monitoring_of_glucose_in_the_interstitial_fluid
Corporate Medical Policy Continuous Monitoring of Glucose in the Interstitial Fluid File Name: Origination: Last CAP Review: Next CAP Review: Last Review: continuous_monitoring_of_glucose_in_the_interstitial_fluid
Blood Glucose Monitoring Basics
 Blood glucose (BG) monitoring is a critical aspect of diabetes management and, for patients using insulin, the purpose is robust. A patient s insulin dose design and adjustment are based on glycemic patterns
Blood glucose (BG) monitoring is a critical aspect of diabetes management and, for patients using insulin, the purpose is robust. A patient s insulin dose design and adjustment are based on glycemic patterns
Intensifying Insulin Therapy
 Intensifying Insulin Therapy Rick Hess, PharmD, CDE, BC-ADM Associate Professor Gatton College of Pharmacy, Department of Pharmacy Practice East Tennessee State University Johnson City, Tennessee Learning
Intensifying Insulin Therapy Rick Hess, PharmD, CDE, BC-ADM Associate Professor Gatton College of Pharmacy, Department of Pharmacy Practice East Tennessee State University Johnson City, Tennessee Learning
Insulin Dose Adjustment REAL-Time CGMS Guidelines for Subjects on Pump Therapy
 Insulin Dose Adjustment REAL-Time CGMS Guidelines for Subjects on Pump Therapy In addition to using the blood sugar logs to adjust your insulin doses every week, you should also use your continuous glucose
Insulin Dose Adjustment REAL-Time CGMS Guidelines for Subjects on Pump Therapy In addition to using the blood sugar logs to adjust your insulin doses every week, you should also use your continuous glucose
Insulin: Breaking Barriers Enhancing Therapies. Jerry Meece, RPh, FACA, CDE jmeece12@cooke.net
 Insulin: Breaking Barriers Enhancing Therapies Jerry Meece, RPh, FACA, CDE jmeece12@cooke.net Questions To Address Who are candidates for insulin? When do we start insulin? How do the different types of
Insulin: Breaking Barriers Enhancing Therapies Jerry Meece, RPh, FACA, CDE jmeece12@cooke.net Questions To Address Who are candidates for insulin? When do we start insulin? How do the different types of
Report reference guide. mmol/l. One. solution EMR. No fuss
 Report reference guide mmol/l One solution No fuss 0000000000 00 0 0000 00 0 0 0 0 0 0 000000000 0 0 00 0 0 0 00 00 0 0 0 0 0 0 00 00000000000000000000 00 EMR About. Plug Transmitter into your outlet is
Report reference guide mmol/l One solution No fuss 0000000000 00 0 0000 00 0 0 0 0 0 0 000000000 0 0 00 0 0 0 00 00 0 0 0 0 0 0 00 00000000000000000000 00 EMR About. Plug Transmitter into your outlet is
How To Manage Diabetes
 INSULIN PUMPS PHYSIOLOGIC INSULIN SECRETION Daniel L. Metzger, MD, FAAP, FRCPC INSULIN PUMP INFUSION SETS BOLUS BASAL Breakfast Bed Dinner Snack Lunch Breakfast BRANDS OF PUMPS ADVANTAGES I ANIMAS MINIMED
INSULIN PUMPS PHYSIOLOGIC INSULIN SECRETION Daniel L. Metzger, MD, FAAP, FRCPC INSULIN PUMP INFUSION SETS BOLUS BASAL Breakfast Bed Dinner Snack Lunch Breakfast BRANDS OF PUMPS ADVANTAGES I ANIMAS MINIMED
The Diabetes Self Management Insulin Pump Therapy Program
 The Diabetes Self Management Insulin Pump Therapy Program Is part of a Nationally recognized program taught by CPT s Offers classes during the daytime in a three part series: PRE-PUMP CLASS SALINE START
The Diabetes Self Management Insulin Pump Therapy Program Is part of a Nationally recognized program taught by CPT s Offers classes during the daytime in a three part series: PRE-PUMP CLASS SALINE START
Objectives PERINATAL INSULIN PUMPS: BASICS FOR NURSES. Historical Perspective. Insulin Pumps in Pregnancy. Insulin Pumps in the US
 Objectives PERINATAL INSULIN PUMPS: BASICS FOR NURSES Jo M. Kendrick, APN BC, CDE jkendric@utmck.edu Describe indications and contraindications for insulin pump use in hospitalized patients Differentiate
Objectives PERINATAL INSULIN PUMPS: BASICS FOR NURSES Jo M. Kendrick, APN BC, CDE jkendric@utmck.edu Describe indications and contraindications for insulin pump use in hospitalized patients Differentiate
A Reference Guide for School Nurses. with the Medtronic MiniMed Insulin Pump
 A Reference Guide for School Nurses with the Medtronic MiniMed Insulin Pump Table Of Contents I Table of Contents The Medtronic MiniMed Insulin Pump A Reference Guide for School Nurses For the 522, 722,
A Reference Guide for School Nurses with the Medtronic MiniMed Insulin Pump Table Of Contents I Table of Contents The Medtronic MiniMed Insulin Pump A Reference Guide for School Nurses For the 522, 722,
Insulin Pump Therapy in children & Adolescents. Dr. Abdulmoein Al-Agha, MBBS,DCH, FRCP(UK) Pediatric Endocrinologist
 Pediatric Endocrinologist") Insulin Pump Therapy in children & Adolescents Dr. Abdulmoein Al-Agha, MBBS,DCH, FRCP(UK) Pediatric Endocrinologist Insulin The most powerful agent we have to control glucose Banting and Best The Miracle
Insulin Pump Therapy in children & Adolescents Dr. Abdulmoein Al-Agha, MBBS,DCH, FRCP(UK) Pediatric Endocrinologist Insulin The most powerful agent we have to control glucose Banting and Best The Miracle
Pump Therapy Indications:
 Insulin Pumping Getting Started March 7, 2008 Clinical Pearls To understand the rational behind pump therapy To explore patient preferences for and against insulin pump therapy Realistic expectations for
Insulin Pumping Getting Started March 7, 2008 Clinical Pearls To understand the rational behind pump therapy To explore patient preferences for and against insulin pump therapy Realistic expectations for
Imagine a world... Believe in better control. MiniMed Veo Paradigm System Questions and Answers About Insulin Pumping
 Imagine a world... Believe in better control MiniMed Veo Paradigm System Questions and Answers About Insulin Pumping 1 Imagine a world... Where you can exercise whenever you want and not have to carb load
Imagine a world... Believe in better control MiniMed Veo Paradigm System Questions and Answers About Insulin Pumping 1 Imagine a world... Where you can exercise whenever you want and not have to carb load
Diabetes and Technology. Disclosures Certified Insulin Pump Trainer for: Animas Medtronic Diabetes Omnipod. Rebecca Ray, MSN, APRN, FNP-C
 Diabetes and Technology Rebecca Ray, MSN, APRN, FNP-C Insulin Pump Therapy and Continuous Glucose Monitoring In Patients with Type 2 Diabetes Page 1 Disclosures Certified Insulin Pump Trainer for: Animas
Diabetes and Technology Rebecca Ray, MSN, APRN, FNP-C Insulin Pump Therapy and Continuous Glucose Monitoring In Patients with Type 2 Diabetes Page 1 Disclosures Certified Insulin Pump Trainer for: Animas
Insulin Initiation and Intensification
 Insulin Initiation and Intensification ANDREW S. RHINEHART, MD, FACP, CDE MEDICAL DIRECTOR AND DIABETOLOGIST JOHNSTON MEMORIAL DIABETES CARE CENTER Objectives Understand the pharmacodynamics and pharmacokinetics
Insulin Initiation and Intensification ANDREW S. RHINEHART, MD, FACP, CDE MEDICAL DIRECTOR AND DIABETOLOGIST JOHNSTON MEMORIAL DIABETES CARE CENTER Objectives Understand the pharmacodynamics and pharmacokinetics
Introducing DEXCOM STUDIO INTUITIVE. FOCUSED. SIMPLIFIED. HELP TAKE the GUESSWORK OUT of GLUCOSE PATTERN MANAGEMENT
 Introducing DEXCOM STUDIO Continuous Glucose Monitoring Software INTUITIVE. FOCUSED. SIMPLIFIED. HELP TAKE the GUESSWORK OUT of GLUCOSE PATTERN MANAGEMENT Glucose Pattern Management A Guide to Interpreting
Introducing DEXCOM STUDIO Continuous Glucose Monitoring Software INTUITIVE. FOCUSED. SIMPLIFIED. HELP TAKE the GUESSWORK OUT of GLUCOSE PATTERN MANAGEMENT Glucose Pattern Management A Guide to Interpreting
Insulin/Diabetes Calculations
 Insulin/Diabetes Calculations Dr. Aipoalani St Lukes Endocrinology Goals Describe various calculations for insulin dosing Understand importance of the total daily dose (TDD) of insulin Be able to calculate
Insulin/Diabetes Calculations Dr. Aipoalani St Lukes Endocrinology Goals Describe various calculations for insulin dosing Understand importance of the total daily dose (TDD) of insulin Be able to calculate
Jane Jeffrie Seley DNP, MPH, GNP, CDE, BC-ADM, CDTC Diabetes Nurse Practitioner Division of Endocrinology NewYork-Presbyterian Hospital Weill Cornell
 Jane Jeffrie Seley DNP, MPH, GNP, CDE, BC-ADM, CDTC Diabetes Nurse Practitioner Division of Endocrinology NewYork-Presbyterian Hospital Weill Cornell Medical College Disclosures Advisory Board Member:
Jane Jeffrie Seley DNP, MPH, GNP, CDE, BC-ADM, CDTC Diabetes Nurse Practitioner Division of Endocrinology NewYork-Presbyterian Hospital Weill Cornell Medical College Disclosures Advisory Board Member:
QUESTION 3. HOW SHOULD THE DATA AND REPORTING BE INTERPRETED?
 QUESTION 3. HOW SHOULD THE DATA AND REPORTING BE INTERPRETED? AACE/ACE CGM Consensus Conference: Medical, Scientific, Professional, and Educational Societies Question 3a. Are there standard metrics that
QUESTION 3. HOW SHOULD THE DATA AND REPORTING BE INTERPRETED? AACE/ACE CGM Consensus Conference: Medical, Scientific, Professional, and Educational Societies Question 3a. Are there standard metrics that
The Department of Vermont Health Access Medical Policy
 State of Vermont Department of Vermont Health Access 312 Hurricane Lane, Suite 201 [Phone] 802-879-5903 Williston, VT 05495-2807 [Fax] 802-879-5963 www.dvha.vermont.gov Agency of Human Services The Department
State of Vermont Department of Vermont Health Access 312 Hurricane Lane, Suite 201 [Phone] 802-879-5903 Williston, VT 05495-2807 [Fax] 802-879-5963 www.dvha.vermont.gov Agency of Human Services The Department
Insulin Pump Therapy. Jen Block, MSN, RN, CDE Stanford University Department of Pediatric Endocrinology
 Insulin Pump Therapy Jen Block, MSN, RN, CDE Stanford University Department of Pediatric Endocrinology Disclosures Member of Clinical Advisory Panel for Tandem Work on a variety of clinical trials funded
Insulin Pump Therapy Jen Block, MSN, RN, CDE Stanford University Department of Pediatric Endocrinology Disclosures Member of Clinical Advisory Panel for Tandem Work on a variety of clinical trials funded
Health Professional s. Guide to INSULIN PUMP THERAPY
 Health Professional s Guide to INSULIN PUMP THERAPY Table of Contents Introduction Presenting Insulin Pump Therapy to Your Patients When Your Patient Chooses the Pump Estimates for Starting Insulin Pump
Health Professional s Guide to INSULIN PUMP THERAPY Table of Contents Introduction Presenting Insulin Pump Therapy to Your Patients When Your Patient Chooses the Pump Estimates for Starting Insulin Pump
Emma Jenkins BSc, RD, CEDT Diabetes Specialist Dietitian Royal Bournemouth Hospital Dorset, UK. Pens & calculators at the ready?!...
 Emma Jenkins BSc, RD, CEDT Diabetes Specialist Dietitian Royal Bournemouth Hospital Dorset, UK Pens & calculators at the ready?!... Robert, age 42. Type 1 diabetes for 26yrs. HbA1c 76mmols/mol 2 recent
Emma Jenkins BSc, RD, CEDT Diabetes Specialist Dietitian Royal Bournemouth Hospital Dorset, UK Pens & calculators at the ready?!... Robert, age 42. Type 1 diabetes for 26yrs. HbA1c 76mmols/mol 2 recent
Why is Insulin so Important?
 Insulin Therapy Why is Insulin so Important? If the glucose stays in your blood it doesn t do your cells (body) any good The glucose has to get inside the cells for the body to use it What Does Insulin
Insulin Therapy Why is Insulin so Important? If the glucose stays in your blood it doesn t do your cells (body) any good The glucose has to get inside the cells for the body to use it What Does Insulin
INPATIENT DIABETES MANAGEMENT Robert J. Rushakoff, MD Professor of Medicine Director, Inpatient Diabetes University of California, San Francisco
 INPATIENT DIABETES MANAGEMENT Robert J. Rushakoff, MD Professor of Medicine Director, Inpatient Diabetes University of California, San Francisco CLINICAL RECOGNITION Background: Appropriate inpatient glycemic
INPATIENT DIABETES MANAGEMENT Robert J. Rushakoff, MD Professor of Medicine Director, Inpatient Diabetes University of California, San Francisco CLINICAL RECOGNITION Background: Appropriate inpatient glycemic
Desktop Guidelines for Insulin Adjustment
 Desktop Guidelines for Insulin Adjustment Disclaimer and terms of use: This document and workshop (the Material ) has been prepared for informational and training purposes for employees of the Endocrinology
Desktop Guidelines for Insulin Adjustment Disclaimer and terms of use: This document and workshop (the Material ) has been prepared for informational and training purposes for employees of the Endocrinology
Numerous studies have demonstrated that utilization
 DIABETES TECHNOLOGY & THERAPEUTICS Volume 18, Supplement 2, 2016 ª Mary Ann Liebert, Inc. DOI: 10.1089/dia.2015.0369 ORIGINAL ARTICLE Use of Glucose Rate of Change Arrows to Adjust Insulin Therapy Among
DIABETES TECHNOLOGY & THERAPEUTICS Volume 18, Supplement 2, 2016 ª Mary Ann Liebert, Inc. DOI: 10.1089/dia.2015.0369 ORIGINAL ARTICLE Use of Glucose Rate of Change Arrows to Adjust Insulin Therapy Among
MiniMed 640G System Intelligent for Better Control
 Getting Started with the MiniMed 640G System Intelligent for Better Control Table Of Contents Introduction I MiniMed Care Introducing the MiniMed 640G System MiniMed Care...3 Welcome...4 The Delivery of
Getting Started with the MiniMed 640G System Intelligent for Better Control Table Of Contents Introduction I MiniMed Care Introducing the MiniMed 640G System MiniMed Care...3 Welcome...4 The Delivery of
CONTINUOUS GLUCOSE MONITORING AND INSULIN DELIVERY FOR MANAGING DIABETES
 MEDICAL POLICY CONTINUOUS GLUCOSE MONITORING AND INSULIN DELIVERY FOR MANAGING DIABETES Policy Number: 2015T0347R Effective Date: April 22, 2015 Table of Contents BENEFIT CONSIDERATIONS COVERAGE RATIONALE
MEDICAL POLICY CONTINUOUS GLUCOSE MONITORING AND INSULIN DELIVERY FOR MANAGING DIABETES Policy Number: 2015T0347R Effective Date: April 22, 2015 Table of Contents BENEFIT CONSIDERATIONS COVERAGE RATIONALE
CONTINUOUS GLUCOSE MONITORING AND INSULIN DELIVERY FOR MANAGING DIABETES
 MEDICAL POLICY CONTINUOUS GLUCOSE MONITORING AND INSULIN DELIVERY FOR MANAGING DIABETES Policy Number: CS024.E Effective Date: April 1, 2016 Table of Contents COVERAGE RATIONALE APPLICABLE CODES.. DESCRIPTION
MEDICAL POLICY CONTINUOUS GLUCOSE MONITORING AND INSULIN DELIVERY FOR MANAGING DIABETES Policy Number: CS024.E Effective Date: April 1, 2016 Table of Contents COVERAGE RATIONALE APPLICABLE CODES.. DESCRIPTION
Algorithms for Glycemic Management of Type 2 Diabetes
 KENTUCKY DIABETES NETWORK, INC. Algorithms for Glycemic Management of Type 2 Diabetes The Diabetes Care Algorithms for Type 2 Diabetes included within this document are taken from the American Association
KENTUCKY DIABETES NETWORK, INC. Algorithms for Glycemic Management of Type 2 Diabetes The Diabetes Care Algorithms for Type 2 Diabetes included within this document are taken from the American Association
The MiniMed Paradigm Veo System
 The MiniMed Paradigm Veo System Live More, Worry Less First CGM-ready insulin pump with automatic insulin shut-off mechanism www.medtronic-diabetes.co.uk The freedom you deserve Round-the clock support
The MiniMed Paradigm Veo System Live More, Worry Less First CGM-ready insulin pump with automatic insulin shut-off mechanism www.medtronic-diabetes.co.uk The freedom you deserve Round-the clock support
Get Primed on Pumps: A beginners guide to Insulin Pump Therapy
 Get Primed on Pumps: A beginners guide to Insulin Pump Therapy Advantages of insulin pump therapy There are many advantages to using an insulin pump. Anyone can do it with the right training and support.
Get Primed on Pumps: A beginners guide to Insulin Pump Therapy Advantages of insulin pump therapy There are many advantages to using an insulin pump. Anyone can do it with the right training and support.
Imagine a world... Believe in better control. MiniMed Veo Paradigm System
 Imagine a world... Believe in better control MiniMed Veo Paradigm System 1 Imagine a world... Where you can exercise whenever you want and not have to carb load or worry about hypos. R Where you can eat
Imagine a world... Believe in better control MiniMed Veo Paradigm System 1 Imagine a world... Where you can exercise whenever you want and not have to carb load or worry about hypos. R Where you can eat
Implementing The Portland Protocol - Continuous Intravenous Insulin Infusion in your institution
 Implementing The Portland Protocol - Continuous Intravenous Insulin Infusion in your institution Anthony P. Furnary, MD St Vincent Medical Center Providence Health Systems Portland, OR Phased Implementation
Implementing The Portland Protocol - Continuous Intravenous Insulin Infusion in your institution Anthony P. Furnary, MD St Vincent Medical Center Providence Health Systems Portland, OR Phased Implementation
Pumping Protocol A Guide to Insulin Pump Therapy Initiation
 Pumping Protocol A Guide to Insulin Pump Therapy Initiation Includes an introduction to continuous glucose monitoring (CGM) and therapy management software Medical Education Academia Innovating for life.
Pumping Protocol A Guide to Insulin Pump Therapy Initiation Includes an introduction to continuous glucose monitoring (CGM) and therapy management software Medical Education Academia Innovating for life.
Intensifying Insulin In Type 2 Diabetes
 Intensifying Insulin In Type 2 Diabetes Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine University of North Dakota School of Medicine and Health Sciences Assistant
Intensifying Insulin In Type 2 Diabetes Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine University of North Dakota School of Medicine and Health Sciences Assistant
Diabetes Self Management Training Insulin Pump Follow Up
 701 East Marshall Street, West Chester, PA 19380 www.chestercountyhospital.org 610.431.5000 Diabetes Self Management Training Insulin Pump Follow Up Patient Name: Visit Date: Time: To prepare for your
701 East Marshall Street, West Chester, PA 19380 www.chestercountyhospital.org 610.431.5000 Diabetes Self Management Training Insulin Pump Follow Up Patient Name: Visit Date: Time: To prepare for your
Insulin Pump Therapy Education Protocol
 Insulin Pump Therapy Education Protocol Considerations for Developing Your Own Best Practices 9402474-011 1 Objective Provide an overview of the importance of developing an insulin pump therapy education
Insulin Pump Therapy Education Protocol Considerations for Developing Your Own Best Practices 9402474-011 1 Objective Provide an overview of the importance of developing an insulin pump therapy education
The What, Why, Who & How of Insulin Pumps. Bridget Lydon May 2014
 The What, Why, Who & How of Insulin Pumps Bridget Lydon May 2014 Topics WHAT is an insulin pump HOW a pump works WHY use a pump WHO should use a pump Pharmac criteria for funded pumps All began back in
The What, Why, Who & How of Insulin Pumps Bridget Lydon May 2014 Topics WHAT is an insulin pump HOW a pump works WHY use a pump WHO should use a pump Pharmac criteria for funded pumps All began back in
Medical Policy Insulin Pumps
 Medical Policy Insulin Pumps Document Number: 027 Authorization required Insulin Pumps & supplies Notification within 24 hours of service or next business day No Prior Authorization Not covered Pulsatile
Medical Policy Insulin Pumps Document Number: 027 Authorization required Insulin Pumps & supplies Notification within 24 hours of service or next business day No Prior Authorization Not covered Pulsatile
Anneli, Martina s daughter In better control with her pump since 2011 MY CHILD HAS TYPE 1 DIABETES
 Anneli, Martina s daughter In better control with her pump since 2011 MY CHILD HAS TYPE 1 DIABETES Many parents whose child is diagnosed with Type 1 diabetes wonder: Why is this happening to my child?
Anneli, Martina s daughter In better control with her pump since 2011 MY CHILD HAS TYPE 1 DIABETES Many parents whose child is diagnosed with Type 1 diabetes wonder: Why is this happening to my child?
Clinical Validity of Insulin Bolus Calculators
 Clinical Validity of Insulin Bolus Calculators Howard A. Wolpert, MD Senior Physician, Joslin Diabetes Center Associate Professor, Harvard Medical School Director, Joslin Institute for Technology Translation
Clinical Validity of Insulin Bolus Calculators Howard A. Wolpert, MD Senior Physician, Joslin Diabetes Center Associate Professor, Harvard Medical School Director, Joslin Institute for Technology Translation
MEDICAL COVERAGE POLICY. SERVICE: Insulin Pump and Continuous Glucose Monitoring. PRIOR AUTHORIZATION: Required. POLICY:
 Important note Even though this policy may indicate that a particular service or supply may be considered covered, this conclusion is not based upon the terms of your particular benefit plan. Each benefit
Important note Even though this policy may indicate that a particular service or supply may be considered covered, this conclusion is not based upon the terms of your particular benefit plan. Each benefit
Insulin therapy in various type 1 diabetes patients workshop
 Insulin therapy in various type 1 diabetes patients workshop Bruce H.R. Wolffenbuttel, MD PhD Dept of Endocrinology, UMC Groningen website: www.umcg.net & www.gmed.nl Twitter: @bhrw Case no. 1 Male of
Insulin therapy in various type 1 diabetes patients workshop Bruce H.R. Wolffenbuttel, MD PhD Dept of Endocrinology, UMC Groningen website: www.umcg.net & www.gmed.nl Twitter: @bhrw Case no. 1 Male of
Basal Rate Testing Blood sugar is affected at any time by 1) basal insulin 2) food (carbohydrate) intake 3) bolus insulin (meal time and correction)
 basal insulin 2) food (carbohydrate) intake 3) bolus insulin (meal time and correction)") Basal Rate Testing Blood sugar is affected at any time by 1) basal insulin 2) food (carbohydrate) intake 3) bolus insulin (meal time and correction) 4) activity and 5) other factors such as stress and
Basal Rate Testing Blood sugar is affected at any time by 1) basal insulin 2) food (carbohydrate) intake 3) bolus insulin (meal time and correction) 4) activity and 5) other factors such as stress and
I HAVE JUST BEEN DIAGNOSED WITH TYPE 1 DIABETES
 Dominika In better control with her pump since 2012 I HAVE JUST BEEN DIAGNOSED WITH TYPE 1 DIABETES The diagnosis of Type 1 diabetes may come as a shock and may lead to many questions, such as: Why is
Dominika In better control with her pump since 2012 I HAVE JUST BEEN DIAGNOSED WITH TYPE 1 DIABETES The diagnosis of Type 1 diabetes may come as a shock and may lead to many questions, such as: Why is
Glucose Monitoring in Interstitial Fluid Diabetes
 Medical Coverage Policy Subject: Continuous Glucose Monitoring in Interstitial Fluid Policy #: MED Current Effective Date: 11/10/14 Status: New Last Review Date: 11/10/14 Description/Scope Tight glucose
Medical Coverage Policy Subject: Continuous Glucose Monitoring in Interstitial Fluid Policy #: MED Current Effective Date: 11/10/14 Status: New Last Review Date: 11/10/14 Description/Scope Tight glucose
BASAL BOLUS INSULIN FOR MEDICAL- SURGICAL INPATIENTS
 BASAL BOLUS INSULIN FOR MEDICAL- SURGICAL INPATIENTS C O N T A C T D I A B E T E S S E R V I C E S F O R M O R E I N F O R M A T I O N 8 4 7-9 1 7-6 9 0 7 THIS SLIDE PRESENTATION WAS PREPARED BY SUE DROGOS,
BASAL BOLUS INSULIN FOR MEDICAL- SURGICAL INPATIENTS C O N T A C T D I A B E T E S S E R V I C E S F O R M O R E I N F O R M A T I O N 8 4 7-9 1 7-6 9 0 7 THIS SLIDE PRESENTATION WAS PREPARED BY SUE DROGOS,
Taking Insulin Pumps to School. Rachel Calendo, MS, RN, CPNP, CDE, Martha Cuevas, RN, BSN, CPT
 Taking Insulin Pumps to School Rachel Calendo, MS, RN, CPNP, CDE, Martha Cuevas, RN, BSN, CPT Insulin Pumps Today A micro-computer, about the size of a pager Programmed to deliver both a preset amount
Taking Insulin Pumps to School Rachel Calendo, MS, RN, CPNP, CDE, Martha Cuevas, RN, BSN, CPT Insulin Pumps Today A micro-computer, about the size of a pager Programmed to deliver both a preset amount
Insulin Algorithm for Type 2 Diabetes Mellitus in Children and Adults
 Insulin Algorithm for Type 2 Diabetes Mellitus in Children and Adults Stock # 45-11647 Revised 10/28/10 Glycemic Goals 1,2 Individualize goal based on patient risk factors A1c 6%
Insulin Algorithm for Type 2 Diabetes Mellitus in Children and Adults Stock # 45-11647 Revised 10/28/10 Glycemic Goals 1,2 Individualize goal based on patient risk factors A1c 6%
WHAT CAN I DO TO REDUCE MY RISK OF DEVELOPING THE COMPLICATIONS OF TYPE 1 DIABETES?
 Christian In better control with his pump since 2012 WHAT CAN I DO TO REDUCE MY RISK OF DEVELOPING THE COMPLICATIONS OF TYPE 1 DIABETES? Many people with Type 1 diabetes worry about potential long-term
Christian In better control with his pump since 2012 WHAT CAN I DO TO REDUCE MY RISK OF DEVELOPING THE COMPLICATIONS OF TYPE 1 DIABETES? Many people with Type 1 diabetes worry about potential long-term
Diabetes: When To Treat With Insulin and Treatment Goals
 Diabetes: When To Treat With Insulin and Treatment Goals Lanita. S. White, Pharm.D. Director, UAMS 12 th Street Health and Wellness Center Assistant Professor of Pharmacy Practice, UAMS College of Pharmacy
Diabetes: When To Treat With Insulin and Treatment Goals Lanita. S. White, Pharm.D. Director, UAMS 12 th Street Health and Wellness Center Assistant Professor of Pharmacy Practice, UAMS College of Pharmacy
SUBJECT: DIABETES MEDICATION MANAGEMENT PROTOCOLS
 SUBJECT: DIABETES MEDICATION MANAGEMENT PROTOCOLS PURPOSE To establish a process that will enable Certified Diabetes Educators (CDE) and/or staff with Board Certification in Advanced Diabetes Management
SUBJECT: DIABETES MEDICATION MANAGEMENT PROTOCOLS PURPOSE To establish a process that will enable Certified Diabetes Educators (CDE) and/or staff with Board Certification in Advanced Diabetes Management
Blood Sugar and How to Manage It
 PO Box 70735, SW Station Washington, DC 20024-0735 800-717-0060 office / 202-889-0502 fax Young Marines Diabetes Care Plan Child s Name: Date of Birth: Age: Unit: Event: (Drill, Encampment, SPACES, NDSP,
PO Box 70735, SW Station Washington, DC 20024-0735 800-717-0060 office / 202-889-0502 fax Young Marines Diabetes Care Plan Child s Name: Date of Birth: Age: Unit: Event: (Drill, Encampment, SPACES, NDSP,
Anneli, Martina s daughter In better control with her pump since 2011 MY CHILD HAS TYPE 1 DIABETES
 Anneli, Martina s daughter In better control with her pump since 2011 MY CHILD HAS TYPE 1 DIABETES Many parents whose child is diagnosed with Type 1 diabetes wonder: Why is this happening to my child?
Anneli, Martina s daughter In better control with her pump since 2011 MY CHILD HAS TYPE 1 DIABETES Many parents whose child is diagnosed with Type 1 diabetes wonder: Why is this happening to my child?
Inpatient Treatment of Diabetes
 Inpatient Treatment of Diabetes Alan J. Conrad, MD Medical Director Diabetes Services EVP, Physician Alignment Diabetes Symposium November 12, 2015 Objectives Explain Palomar Health goals for inpatient
Inpatient Treatment of Diabetes Alan J. Conrad, MD Medical Director Diabetes Services EVP, Physician Alignment Diabetes Symposium November 12, 2015 Objectives Explain Palomar Health goals for inpatient
Insulin Administration: What You Don t Know May Hurt Your Patient
 Insulin Administration: What You Don t Know May Hurt Your Patient Jaime A. Davidson, MD, FACP, MACE Clinical Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Jaime A. Davidson,
Insulin Administration: What You Don t Know May Hurt Your Patient Jaime A. Davidson, MD, FACP, MACE Clinical Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Jaime A. Davidson,
JDRF Type One Nation Research Summit Diabetes Technology: A Bridge to a Cure
 JDRF Type One Nation Research Summit Diabetes Technology: A Bridge to a Cure Kelly L. Close, president, Close Concerns editor-in-chief, diatribe March 1, 2014 closeconcerns.com diatribe.org @diatribenews
JDRF Type One Nation Research Summit Diabetes Technology: A Bridge to a Cure Kelly L. Close, president, Close Concerns editor-in-chief, diatribe March 1, 2014 closeconcerns.com diatribe.org @diatribenews
INSULIN TREATMENT FOR TYPE 2 DIABETES MANAGEMENT
 INSULIN TREATMENT FOR TYPE 2 DIABETES MANAGEMENT APIRADEE SRIWIJITKAMOL DIVISION OF ENDOCRINOLOGY AND METABOLISM DEPARTMENT OF MEDICINE FACULTY OF MEDICINE SIRIRAJ HOSPITOL QUESTION 1 1. ท านเคยเป นแพทย
INSULIN TREATMENT FOR TYPE 2 DIABETES MANAGEMENT APIRADEE SRIWIJITKAMOL DIVISION OF ENDOCRINOLOGY AND METABOLISM DEPARTMENT OF MEDICINE FACULTY OF MEDICINE SIRIRAJ HOSPITOL QUESTION 1 1. ท านเคยเป นแพทย
Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid
 Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Get to know the Animas Vibe insulin pump and CGM * system.
 Get to know the Animas Vibe insulin pump and CGM * system. * Continuous glucose monitoring with Animas Vibe is indicated for adult patients 18 years and older only. Hello. Get to know Animas. We make insulin
Get to know the Animas Vibe insulin pump and CGM * system. * Continuous glucose monitoring with Animas Vibe is indicated for adult patients 18 years and older only. Hello. Get to know Animas. We make insulin
A Prospective Evaluation of Insulin Dosing Recommendations in Patients with Type 1 Diabetes at Near Normal Glucose Control: Basal Dosing
 Journal of Diabetes Science and Technology Volume 1, Issue 1, January 2007 Diabetes Technology Society ORIGINAL ARTICLES A Prospective Evaluation of Insulin Dosing Recommendations in Patients Allen B.,
Journal of Diabetes Science and Technology Volume 1, Issue 1, January 2007 Diabetes Technology Society ORIGINAL ARTICLES A Prospective Evaluation of Insulin Dosing Recommendations in Patients Allen B.,
ALVIN INDEPENDENT SCHOOL DISTRICT Diabetes Medical Management Plan
 ALVIN INDEPENDENT SCHOOL DISTRICT Diabetes Medical Management Plan of Plan: School Year (must be current): This plan should be completed by the student s personal health care team and parents/guardian.
ALVIN INDEPENDENT SCHOOL DISTRICT Diabetes Medical Management Plan of Plan: School Year (must be current): This plan should be completed by the student s personal health care team and parents/guardian.
Glucose Management University of Colorado Hospital
 Glucose Management University of Colorado Hospital Bridget Everhart, MSN, NP, CDE Inpatient Diabetes Educator Bridget.Everhart@uch.edu M F Pager 303 266-7898 UCH Diabetes Program Michael McDermott MD Diabetes
Glucose Management University of Colorado Hospital Bridget Everhart, MSN, NP, CDE Inpatient Diabetes Educator Bridget.Everhart@uch.edu M F Pager 303 266-7898 UCH Diabetes Program Michael McDermott MD Diabetes
INSULIN ALGORITHM FOR TYPE 2 DIABETES MELLITUS IN CHILDREN 1 AND ADULTS
 Publication # 45-11647 Targets*
Publication # 45-11647 Targets*
A Prospective Evaluation of Insulin Dosing Recommendations in Patients with Type 1 Diabetes at Near Normal Glucose Control: Bolus Dosing
 Journal of Diabetes Science and Technology Volume 1, Issue 1, January 2007 Diabetes Technology Society ORIGINAL ARTICLES A Prospective Evaluation of Insulin Dosing Recommendations in Patients Allen B.,
Journal of Diabetes Science and Technology Volume 1, Issue 1, January 2007 Diabetes Technology Society ORIGINAL ARTICLES A Prospective Evaluation of Insulin Dosing Recommendations in Patients Allen B.,
BOLUS INSULIN DOSAGES H. Peter Chase, MD and Erin Cobry, BS
 CHAPTER 6: BOLUS INSULIN DOSAGES H. Peter Chase, MD and Erin Cobry, BS WHAT IS BOLUS INSULIN? Bolus insulin dosages refer to the quick bursts of insulin given to cover the carbohydrates in meals or snacks
CHAPTER 6: BOLUS INSULIN DOSAGES H. Peter Chase, MD and Erin Cobry, BS WHAT IS BOLUS INSULIN? Bolus insulin dosages refer to the quick bursts of insulin given to cover the carbohydrates in meals or snacks
by Rodney Lorenz, MD and Janet Silverstein, MD
 Managing Insulin Requirements at School by Rodney Lorenz, MD and Janet Silverstein, MD Introduction Multiple advances over the past decade have revolutionized treatment of diabetes in youth. Two fundamental
Managing Insulin Requirements at School by Rodney Lorenz, MD and Janet Silverstein, MD Introduction Multiple advances over the past decade have revolutionized treatment of diabetes in youth. Two fundamental
The MiniMed Paradigm Veo System A step-by-step guide
 The MiniMed Paradigm Veo System A step-by-step guide www.medtronic-diabetes.com.au Your HCPs Contact Details Staying in touch with your Healthcare Professionals (HCPs) Your Endocrinologist: Phone number:
The MiniMed Paradigm Veo System A step-by-step guide www.medtronic-diabetes.com.au Your HCPs Contact Details Staying in touch with your Healthcare Professionals (HCPs) Your Endocrinologist: Phone number:
Diabetes Management and Treatment Plan for School (For the insulin pump student)
") Lafayette School Corporation Health Services Diabetes Management and Treatment Plan for School (For the insulin pump student) Effective Dates: This plan should be complete by the student s personal health
Lafayette School Corporation Health Services Diabetes Management and Treatment Plan for School (For the insulin pump student) Effective Dates: This plan should be complete by the student s personal health
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Haidar A, Legault L, Matteau-Pelletier L, et
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Haidar A, Legault L, Matteau-Pelletier L, et
A Simplified Approach to Initiating Insulin. 4. Not meeting glycemic goals with oral hypoglycemic agents or
 A Simplified Approach to Initiating Insulin When to Start Insulin: 1. Fasting plasma glucose (FPG) levels >250 mg/dl or 2. Glycated hemoglobin (A1C) >10% or 3. Random plasma glucose consistently >300 mg/dl
A Simplified Approach to Initiating Insulin When to Start Insulin: 1. Fasting plasma glucose (FPG) levels >250 mg/dl or 2. Glycated hemoglobin (A1C) >10% or 3. Random plasma glucose consistently >300 mg/dl
Diabetes Medical Management Plan (DMMP)
") Diabetes Medical Management Plan (DMMP) This plan should be completed by the student s personal diabetes health care team, including the parents/guardian. It should be reviewed with relevant school staff
Diabetes Medical Management Plan (DMMP) This plan should be completed by the student s personal diabetes health care team, including the parents/guardian. It should be reviewed with relevant school staff
The Basics of Insulin Pump Therapy
 The Basics of Insulin Pump Therapy Table of Contents The Basics of Insulin Pump Therapy Introduction Welcome... 3 Chapter 1 Balancing Glucose and Insulin............................. 10 Section 1: Glucose,
The Basics of Insulin Pump Therapy Table of Contents The Basics of Insulin Pump Therapy Introduction Welcome... 3 Chapter 1 Balancing Glucose and Insulin............................. 10 Section 1: Glucose,
Diabetes Health Care Plan
 The Public Schools of Brookline School Health Services of Plan: Diabetes Health Care Plan To be completed by the student s health care team and parents/guardian. Plan will be kept with the school nurse
The Public Schools of Brookline School Health Services of Plan: Diabetes Health Care Plan To be completed by the student s health care team and parents/guardian. Plan will be kept with the school nurse
Most patients with T2DM will eventually require insulin therapy. ADA Glycemic Control Targets. What are some of the obstacles?
 ADA Glycemic Control Targets A1C < 7% Preprandial plasma glucose 70-130 mg/dl Postprandial plasma glucose (PPG)
ADA Glycemic Control Targets A1C < 7% Preprandial plasma glucose 70-130 mg/dl Postprandial plasma glucose (PPG)
INTERNAL MEDICINE RESIDENTS NOON CONFERENCE: INPATIENT GLYCEMIC CONTROL
 INTERNAL MEDICINE RESIDENTS NOON CONFERENCE: INPATIENT GLYCEMIC CONTROL Presented by: Leyda Callejas PGY5 Endocrinology, Diabetes and Metabolism Acknowledgements: Dr. P Orlander Dr. V Lavis Dr. N Shah
INTERNAL MEDICINE RESIDENTS NOON CONFERENCE: INPATIENT GLYCEMIC CONTROL Presented by: Leyda Callejas PGY5 Endocrinology, Diabetes and Metabolism Acknowledgements: Dr. P Orlander Dr. V Lavis Dr. N Shah
CLASS OBJECTIVES. Describe the history of insulin discovery List types of insulin Define indications and dosages Review case studies
 Insulins CLASS OBJECTIVES Describe the history of insulin discovery List types of insulin Define indications and dosages Review case studies INVENTION OF INSULIN 1921 The first stills used to make insulin
Insulins CLASS OBJECTIVES Describe the history of insulin discovery List types of insulin Define indications and dosages Review case studies INVENTION OF INSULIN 1921 The first stills used to make insulin
The Future of Diabetes Old and New Working Together
 The Future of Diabetes Old and New Working Together David L. Joffe, BSPharm, CDE, FACA Clinical Associate Professor Department of Pharmacotherapy & Translational Research, College of Pharmacy, University
The Future of Diabetes Old and New Working Together David L. Joffe, BSPharm, CDE, FACA Clinical Associate Professor Department of Pharmacotherapy & Translational Research, College of Pharmacy, University
OneTouch Reveal Web Application. User Manual for Patients Instructions for Use
 OneTouch Reveal Web Application User Manual for Patients Instructions for Use Contents 2 Contents Chapter 1: Introduction...3 Product Overview...3 Intended Use...3 System Requirements... 3 Technical Support...3
OneTouch Reveal Web Application User Manual for Patients Instructions for Use Contents 2 Contents Chapter 1: Introduction...3 Product Overview...3 Intended Use...3 System Requirements... 3 Technical Support...3
Insulin Pump Therapy
 Introduction The first insulin pumps, or continuous subcutaneous insulin infusion systems (CSII), were introduced in 1976. These early pumps were the size of a backpack and were unreliable. Since then,
Introduction The first insulin pumps, or continuous subcutaneous insulin infusion systems (CSII), were introduced in 1976. These early pumps were the size of a backpack and were unreliable. Since then,
Insulin therapy in type 2 diabetes When and how? Disclosures. Learning Objectives. None relevant to today s talk
 Insulin therapy in type 2 diabetes When and how? Cecilia C Low Wang, MD Univ Colorado AMC SOM Department of Medicine Division of Endocrinology, Metabolism, and Diabetes Disclosures None relevant to today
Insulin therapy in type 2 diabetes When and how? Cecilia C Low Wang, MD Univ Colorado AMC SOM Department of Medicine Division of Endocrinology, Metabolism, and Diabetes Disclosures None relevant to today
at The Valley Hospital (TVH) for Nursing Students/Nursing Instructors 2012
 for Nursing Students/Nursing Instructors 2012") at The Valley Hospital (TVH) for Nursing Students/Nursing Instructors 2012 Subject - Insulin Safety Background Insulin known to be high risk medication Can promote serious hypoglycemia if given incorrectly
at The Valley Hospital (TVH) for Nursing Students/Nursing Instructors 2012 Subject - Insulin Safety Background Insulin known to be high risk medication Can promote serious hypoglycemia if given incorrectly
Intensive Insulin Therapy in Diabetes Management
 Intensive Insulin Therapy in Diabetes Management Lillian F. Lien, MD Medical Director, Duke Inpatient Diabetes Management Assistant Professor of Medicine Division of Endocrinology, Metabolism, & Nutrition
Intensive Insulin Therapy in Diabetes Management Lillian F. Lien, MD Medical Director, Duke Inpatient Diabetes Management Assistant Professor of Medicine Division of Endocrinology, Metabolism, & Nutrition
FDA Perspective on Closed-Loop Studies
 FDA Perspective on Closed-Loop Studies Practical Ways to Achieve Targets in Diabetes Care July 19, 2014 Keystone, CO Courtney H. Lias, Ph.D. Office of In Vitro Diagnostic Device Evaluation and Safety Center
FDA Perspective on Closed-Loop Studies Practical Ways to Achieve Targets in Diabetes Care July 19, 2014 Keystone, CO Courtney H. Lias, Ph.D. Office of In Vitro Diagnostic Device Evaluation and Safety Center
Insulin Pump Therapy
 CHILDREN S SERVICES Insulin Pump Therapy These guidelines are not intended for starting a patient on an insulin pump. They are intended to give staff not part of the diabetic team information regarding
CHILDREN S SERVICES Insulin Pump Therapy These guidelines are not intended for starting a patient on an insulin pump. They are intended to give staff not part of the diabetic team information regarding
Continuous Subcutaneous Insulin Infusion (CSII)
") IMPORTANCE OF FOCUS CSII (Insulin pumps) have been used for more than 35 years. In the U.S. in 2005, the level of insulin pump penetration was estimated at 20 to 30% in patients with type 1 diabetes mellitus
IMPORTANCE OF FOCUS CSII (Insulin pumps) have been used for more than 35 years. In the U.S. in 2005, the level of insulin pump penetration was estimated at 20 to 30% in patients with type 1 diabetes mellitus
Insulin Delivery and Glucose Monitoring Methods: Future Research Needs
 Future Research Needs Paper Number 32 Insulin Delivery and Glucose Monitoring Methods: Future Research Needs Identification of Future Research Needs From Comparative Effectiveness Review No. 57 Prepared
Future Research Needs Paper Number 32 Insulin Delivery and Glucose Monitoring Methods: Future Research Needs Identification of Future Research Needs From Comparative Effectiveness Review No. 57 Prepared