Angela Coladonato, MSN, RN, NEA-BC Tina Maher, BSN, RN, NE-BC Kathy Zopf-Herling, MSN, RN-BC
|
|
|
- Lynne Charles
- 8 years ago
- Views:
Transcription
1 Leveraging IT to Support a Re-engineered engineered Discharge Process Angela Coladonato, MSN, RN, NEA-BC Tina Maher, BSN, RN, NE-BC Kathy Zopf-Herling, MSN, RN-BC All speakers have completed commercial bias disclosure forms and do not have any conflicts of interest. January 2013

2 Disclosures It is the policy of Corexcel and IMNE to ensure fair balance, independence, objectivity, and scientific rigor in all programming. In compliance with the American Nurses Credentialing Center (ANCC) and the Accreditation Council for Pharmacy Education (ACPE), it is the policy of Corexcel and IMNE that faculty disclose all financial relationships with commercial interests over the past 12 months. Corexcel s provider status through the ANCC and IMNE s provider status through the ACPE, are limited to educational activities. Corexcel, IMNE, ANCC and ANCC do not endorse commercial products. 1

3 Objectives Understand the current discharge process and its impact on readmissions Discuss three components of a re-engineered discharge process Articulate ways in which IT can support the discharge process Review the discharge process and how it is used in daily practice Describe the impacts of a re-engineered discharge process 2

4 Agenda Current state of discharge nation-wide. Project RED History and purpose at TCCH Soarian Re-Engineered Discharge Project Goals Multi-disciplinary inputs to the new Discharge Plan Outputs- My Discharge Plan (Patient and facility Version) Identification and management of high risk patients Outcomes so far Questions/Discussion 3
 Identification and management of high risk")
5 Discharge: the Perfect Storm" for Patient Safety The hospital discharge is non-standardized and frequently marked with poor quality. Loose Ends Communication Poor Quality Info Poor Preparation Fragmentation 20% of Medicare patients readmitted within 30 days Only half had a visit in the 30 days after discharge N Engl J Med ;360(14):

6 Other references: the last place patients want to end up after a hospital stay is right back in the hospital millions of patients are readmitted to hospitals each year, and many of those admissions could have been prevented on average, 8 minutes of conversation occurs about how to care for oneself at home, so it is no surprise that patients end up in trouble.. (AHRQ 2011) More than 1/3 of required appointments for follow up not completed (Moore et al. Archives of Internal Medicine. 2007;167: ) 41% of inpatients discharged with a pending test result 37% actionable and 13% urgent 2/3 of physicians unaware of results (Roy, et. al. Annals of Internal Medicine. 2005; 143(2):121-8.) Patients are not prepared at discharge: 37% able to state the purpose of their medications; 42% able to state their diagnosis (Mayo Clinic Proceedings. August 2005; 80(8):
 41% of inpatients discharged with a pending test result 37% actionable and 13% urgent 2/3 of physicians unaware of results (Roy, et. al. Annals of Internal Medicine.")
7 Our Story: Dr. B. Jack/AHRQ- the national RED Roll-Out Pilot Project TCCH asked to be one of 11 hospitals to participate nationally Answer the following questions: Does the Project RED 11 Element Checklist work in the real world? Can the Project RED 11 Element Checklist be used more efficiently? June 2011 site visit; Dr. Jack, Boston Implementation team, AHRQ CHF patients discharged to home from Telemetry = pilot population Pilot year: summer

8 Readmission Rate Data during pilot - FY11 vs. FY12 All Telemetry Patients with a Primary Diagnosis of CHF at Discharge 30 Day Readmissions 7

9 RED & HCAHPS : Enhancing Communication 8 8

10 RED Checklist Adopted by National Quality Forum as Safe Practice Make appointments for follow-up medical appointments and post discharge tests/labs. 2. Plan for the follow-up of results from lab tests or studies that are pending at discharge. 3. Organize post-discharge outpatient services and medical equipment. 4. Identify the correct medicines and a plan for the patient to obtain and take them. 5. Reconcile discharge plan with national guidelines. 6. Teach a written discharge plan (AHCP) the patient can understand. 7. Educate the patient about his/her diagnosis. 8. Assess the degree of the patient s understanding of this plan. 9. Review with the patient what to do if a problem arises. 10. Expedite transmission of the discharge summary to clinicians accepting care of the patient. 11. Provide telephone reinforcement of the Discharge Plan.
 the patient can understand. 7. Educate the patient about his/her diagnosis. 8. Assess the degree of the patient s understanding of this plan. 9.")
11 Our Story: Personalized Plan 10

12 List of Medicines: Why & How 11
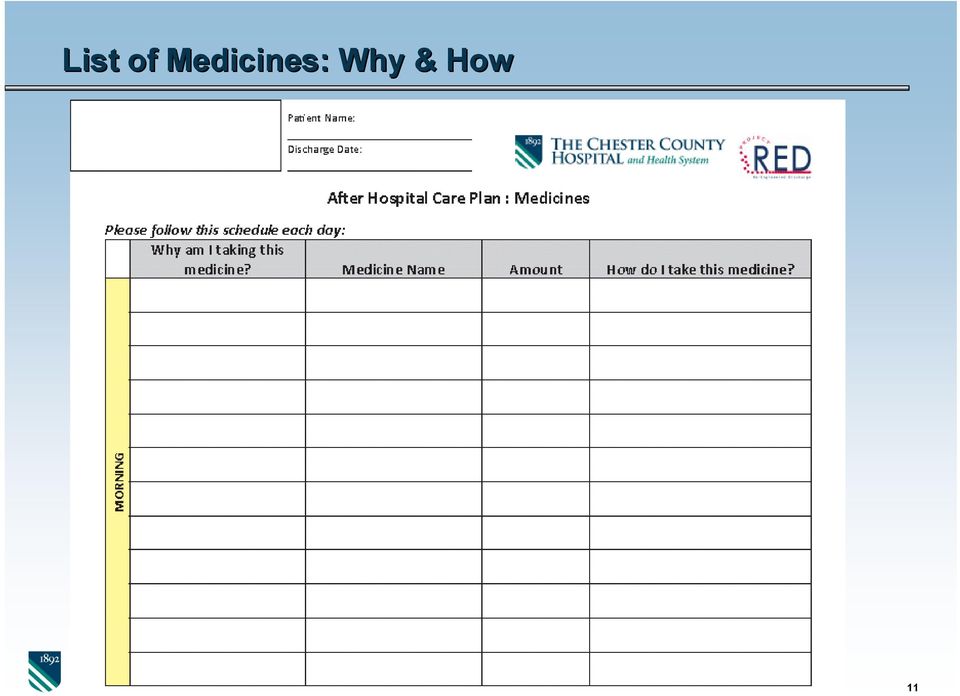
13 TCCH Clinical Pharmacists: Medication Teaching Tylenol Brand Name Ventolin, ProAir, Proventil pain, fever Why am I taking this med? breathing problems, asthma What do I need to look for? too much can cause liver damage (read OTC labels), higher doses for long periods can increase warfarin effects "rescue" inhaler, fast heart beat, chest pain/pressure Uroxatral Dizziness,HA, avoid grapefruit juice, alcohol, enlarged prostate, kidney stones changes in sex ability Zyloprim gout/high uric acid upset stomach, rash/skin irritation Xanax anxiety, "nerves" drowsiness, dry mouth Cordarone, Pacerone abnormal heart rhythm constipation, sensitivity to sunlight (wear sunscreen) Elavil mood, migraine, nerve pain sedation, dry mouth, avoid grapefruit juice 12
 Elavil mood, migraine, nerve pain sedation, dry mouth, avoid")
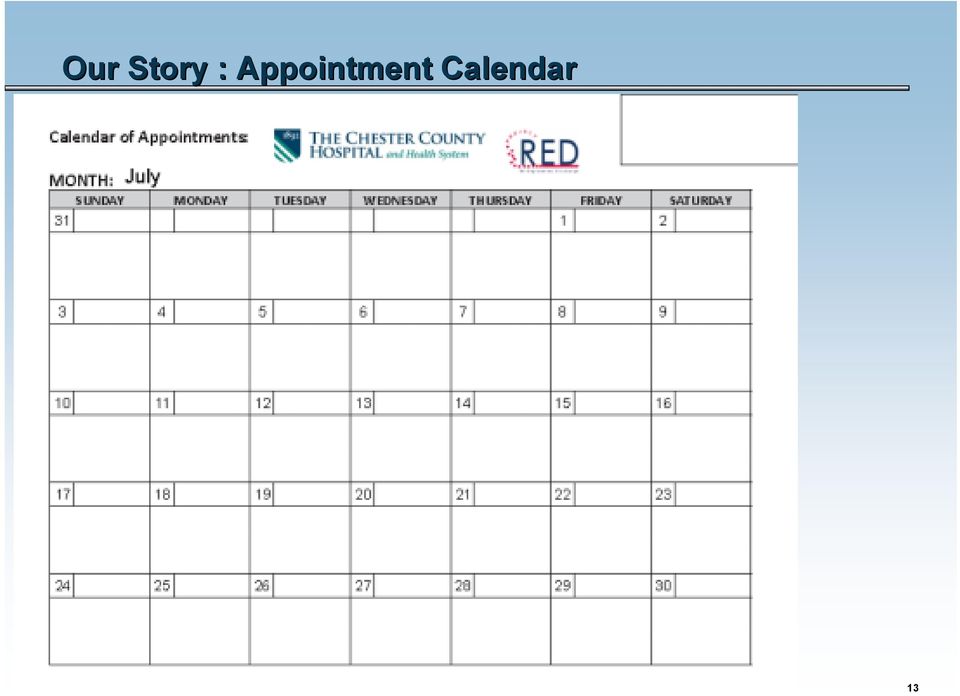
14 Our Story : Appointment Calendar 13
15 Re-Engineered Discharge: TCCH Expansion Pilot project was a success. Biggest challenge= biggest opportunity! Replication of the AHCP in Soarian; collaboration once more! RED 11 element Checklist worked; what is TCCH model? Re-Engineer the discharge experience for all; additional interventions for some TCCH Re-Engineered Discharge: 5 Core RED Principles Discharge planning begins Day 1 all TCCH patients My Discharge Plan all TCCH patients Teach-back methodology all TCCH patients Follow-up apts. High Risk patients Follow-up phone calls High Risk patients 14

16 Re-Engineered Discharge: TCCH Expansion Staff education on discharge and teach back methodology High Risk patients: F/Up Apts. Unit Coordinators own the process Patient/family interaction & the MD offices huge value! High Risk patients: F/Up phone calls Modified script from the Project RED pilot year; hours after D/C Access the medical record ; document the call CV Nurse Navigator, Paramedics and Clinical Pharmacists Content to date: medication clarification, transition support & compliments Volunteers & transport staff: discharge at curb-side Reinforce importance of My Discharge Plan as TCCH says good-bye 15 15

17 Goal of Soarian Re-engineered engineered Discharge Leverage our already existing electronic interdisciplinary documentation and processes to create patient friendly discharge instructions: Make the small RED pilot scalable to benefit all of our patients. No niche system No double documentation and re-work for staff/physicians Leverage Soarian work flow engine to identify high risk patients and help ensure that key activities occur, such as making appts and post discharge phone calls. 16

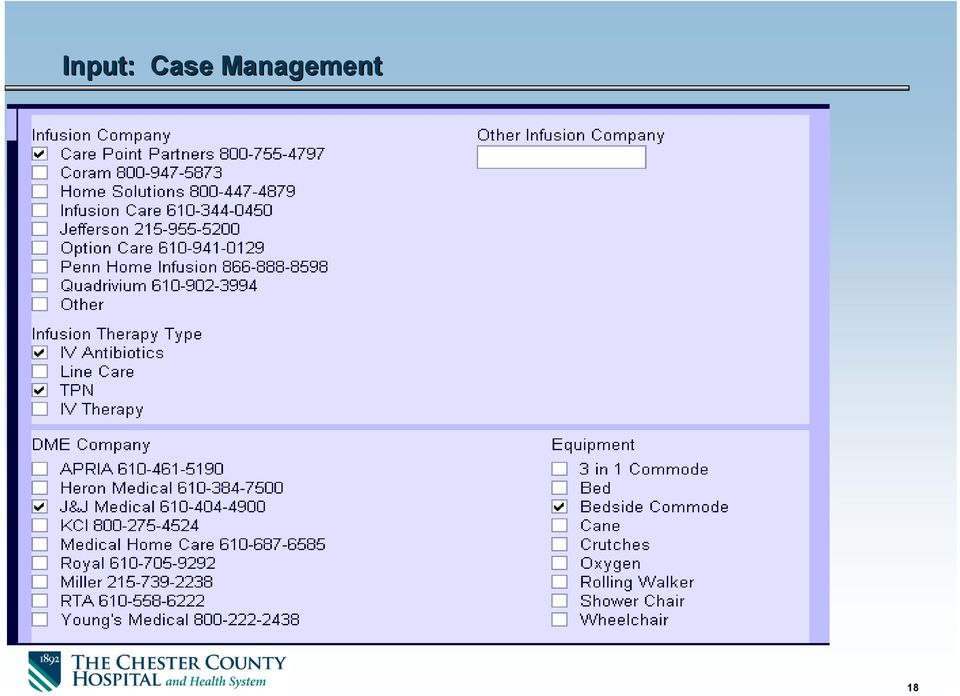
18 Goal 1: Patient friendly discharge instructions The discharge plan that the patient receives is created from electronic interdisciplinary documentation that is captured in the natural course of providing care: Uses ADT information- Demographics Uses CPOE orders Uses Case Management -facility plans, VNA, DME, etc. Uses Discharge Medication Reconciliation Uses Nursing Documentation- MAK, Discharge Instructions, Shift Assessments, ADLs, Vital Signs Unit Coordinators pull in follow-up contact information; make appts Discharge Instructions Library Nutritionists, Diabetes Nurse Educators, NPs, PAs, RT, PT/OT can add discharge instructions too! Facility/VNA version has additional clinical data 17

19 Input: Case Management 18
20 Input: Clinicians via discharge instruction order sets 19

21 Specialty addendums can easily be added 20
22 Unit Coordinator Role Unit Coordinators add follow-up appointment informationaddresses, phone numbers, time frame, and, for high risk patients, make these appointments in consultation with the patient and family. This made possible due to successful CPOE and MAK implementation that reduced amount of time spent in order transcription. We were able to insert links into the assessment form so that physician office locations and contact information could be readily found and inserted into the form (and eventually the report) 21
23 Patient Ed form- last chapter for discharge: nurse and others enter specific instructions/appts 22
24 Populating follow up physician contact information 23
25 Find the clinician, cut and paste! 24
26 Nurses and other disciplines add instructions- free text or templated information. 25
27 Text block library for templated last licks instructions 26
28 Nurses Role Nurses are responsible for patient education throughout the patient s hospitalization. They use teach back methodology and a variety of tools, such as Lexicomp, ExitCare, total joint booklet, etc. At discharge, they add final discharge instructions individualized for the patient- either free text or from a document library. These become part of the discharge plan given to the patient. Nurses coordinate discharge, so help to ensure that the discharge plan given to the patient is complete and accurate. Nurses also review the final discharge plan with the patient before discharge. 27
29 Physicians, Nurses, Pharmacists: Medication Section Clinicians complete discharge medication reconciliation in Soarian, which will inform the patient what medications they should continue at home. Nurses administer medications in MAK, which populate the last dose taken Pharmacists pre-built Commonly Used to for top 400 discharged medications. 28
30 Discharge Medication Reconciliation and MAK 29
31 Nurses contribute some Clinical Data from Shift Assessments 30
32 Creating the Report Specs for the Discharge Plan 31
33 Report Specs: Identifying the look back period 32
34 33
35 Discharge Plan Features Labels are in Patient Friendly language. For example, Physician enters discharge diagnosis in Soarian, but the label on the report is My main medical problem, according to Dr. Smith was: Visually designed to be easy on the eye and welcoming. Change from historically, where we gave patients very important information in a manner that was overwhelming. Large Font and Landscape orientation Lots of Page Breaks so that (for example) the medication chart starts on a new page 34
36 First page- vaccines and general info about hospital 35
37 Clinician Orders inserted into the document 36
38 Medication instructions- DMR with MAK last dose time and common use of medications 37
39 Yield and Stop signs for PRN and stopped meds. 38
40 Instructional material inserted into document or typed in free text. t 39
41 Case Management section 40
42 Appointments section 41
43 Calendar included if appts made. 42
44 Final product Final product For SNF/VNA all the patient stuff plus more! 43
45 First page- some added sections on Advance Directives, general patient information. 44
46 Added sections for the Nursing Home/VNA version 45
47 Last set (within 24 hours) of vitals signs, O2 46
48 Part 2: Management of High Risk Patients Automated work flow processes to identify patients at risk (modified Boost criteria). List updates with changes: Poly pharmacy Recent 30 day Readmission, all cause Certain diagnoses: Stroke, AMI, HF, COPD, TIA, Psych Lives alone On Warfarin or Aspirin/Clopidogrel SNF patients excluded Creates high risk for readmission order visible in chart 47
49 Part 2: Management of High Risk Patients Populates a report showing all high risk patients on the unit/hospital and reason for inclusion Populates a report for after discharge phone calls: 48
50 Lessons Learned Need robust DC instructions in the text block library. Engage physicians and staff early and include broader stakeholders (we started with heart failure because they were the pilot) Get a top notch report writer! Make sure report runs consistently and quickly. Plan to spend a lot of time on report specifications and testing. Tell nurses to preview the report to ensure completeness and accuracy. Nurses will sometimes have to sign DMR as complete if clinician forgot. Need to review report for accuracy Allow that nurses will spend more time with patient at discharge reviewing this discharge document. 49
51 Summary From an organizational perspective, this project has been a huge success, and has been well received by our patients: Minimized duplication and manual entry Refocused Unit Coordinator role on a value added patient activity. More robust, automated identification of patients at high risk for readmission. Legible, and complete discharge plan that is well received by patients, primary care physicians and receiving facilities. My Discharge Plan it s like getting an award for discharge (patient quote) Huge paradigm shift for most clinical staff - instead of the focus being on what they could enter into the electronic medical record, they saw their normal documentation actually used to produce something that would benefit the patients. 50
52 TCCH : HCAHPS Discharge Domain 51 51
53 RED & HCAHPS: Enhancing Communication New 2013 HCAHPS Care Transition Questions 4 point scale; from Strongly Disagree to Strongly Agree During this hospital stay, staff took my preferences & those of my family/caregiver into account in deciding what my health care needs would be when I left When I left the hospital, I had a good understanding of the things I was responsible for in managing my health When I left the hospital, I clearly understood the purpose for taking each of my medications 52
54 TCCH : HCAHPS Care Transitions 53 53
55 Lots of positive feedback from community agencies: I just wanted to let you know, how pleased we are with the ease of discharge from your hospital to our community. Mrs. E was followed by your SW, Linda. She communicated well with our SW. And the information that was sent upon discharge was terrific and will follow the resident home. We have commented among ourselves what a great discharge program you have in your IT dept, and how helpful all this info was. It was a pleasure working with you, hope we can do again sometime in the future. Thanks, Maggie 54
56 Future Plans Roll out to Maternal Child Health next week! Continue to improve the discharge instructions library Continue to improve the report (My discharge plan) Add past med/surg history at request of SNFs Move sections for maximum emphasis/readability Add eprescribe transactions including quantity and refill Try to find a way not to have to print and copy report (patient portal/hie/electronic patient signature and electronic annotations. Query review to make report run faster (completed) Review newly available metrics reports and see where that leads us 55
57 Questions?
58 Download the Free Chapter The Chester County Hospital and Health System: Using Technology to Re-Engineer Discharge Processes and Enhance Transitional Care Part of the new series, Technology in the New World of Healthcare, from Siemens Healthcare. techseries
59 Contact Hour Credits In order to receive contact hours for today s session: If you are eligible and would like to receive credit, please follow the instructions for completing the evaluation. The instructions will appear on your screen momentarily. Or you can click on the evaluation link located on the bottom of your viewing console. Once you have completed the evaluation, you will have the ability to print out your certificate for Continuing Nursing Education Credits of 1.0 contact hour offered by Corexcel. For those of you in a group setting: If you are viewing this webcast in a group setting and would like credits, you may do the following: If you are not already registered, please be sure to register to view the playback of this event. You can access the playback through the or through the follow-up that will be sent to all registrants. The playback will be available within a few days after the conclusion of the live event. Once you complete the evaluation and are eligible for credits, you may print your certificate. These instructions will also be included in the follow-up to all attendees. Copyright 2013 Siemens Medical Solutions USA, Inc. All rights reserved.
60 Upcoming Siemens Webcast Topics Contact Information: Gail E. Latimer, MSN, RN, FACHE, FAAN, Vice President, Chief Nursing Officer, Siemens Healthcare Upcoming Thought-Leadership Webcasts will be Announced Shortly. - Check Siemens Clinical Gateway for more information Missed a webcasts? To view previous webcasts or to learn more on how healthcare IT can help tackle the challenges clinicians face today visit Siemens Clinical Gateway at: Copyright 2013 Siemens Medical Solutions USA, Inc. All rights reserved.
Helen M. Simpson Rehabilitation Hospital Leveraging IT to Coordinate Care Transitions
 Helen M. Simpson Rehabilitation Hospital Leveraging IT to Coordinate Care Transitions All speakers have completed commercial bias disclosure forms and do not have any conflicts of interest Disclosures
Helen M. Simpson Rehabilitation Hospital Leveraging IT to Coordinate Care Transitions All speakers have completed commercial bias disclosure forms and do not have any conflicts of interest Disclosures
Learning Collaborative
 Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Implementing an Evidence Based Hospital Discharge Process
 Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
THE NEXT FRONTIER OF UNDERSTANDING NURSING TIME IN THE EMR
 THE NEXT FRONTIER OF UNDERSTANDING NURSING TIME IN THE EMR Presentation ID: 484 Nikki Polis PhD, RN SVP and CNE Methodist LeBonheur Healthcare Interim CNO LeBonheur Children's Hospital Memphis, TN Darinda
THE NEXT FRONTIER OF UNDERSTANDING NURSING TIME IN THE EMR Presentation ID: 484 Nikki Polis PhD, RN SVP and CNE Methodist LeBonheur Healthcare Interim CNO LeBonheur Children's Hospital Memphis, TN Darinda
The Children s Readmissions Collaborative Kick-Off Conference April 28, 2014 Project Tools
 The Children s Readmissions Collaborative Kick-Off Conference April 28, 2014 Project Tools Kate M. Sherman Manager, Readmissions Quality Collaborative New York State Psychiatric Institute/ State Office
The Children s Readmissions Collaborative Kick-Off Conference April 28, 2014 Project Tools Kate M. Sherman Manager, Readmissions Quality Collaborative New York State Psychiatric Institute/ State Office
Driving The Ultimate Patient Experience Patient Discharge
 Driving The Ultimate Patient Experience Patient Discharge Date: January 12 th, 2012 Hendricks Regional Health BOH-HFAP Joint Webcast Agenda for today s discussion: About Hendricks Regional Health HFAP
Driving The Ultimate Patient Experience Patient Discharge Date: January 12 th, 2012 Hendricks Regional Health BOH-HFAP Joint Webcast Agenda for today s discussion: About Hendricks Regional Health HFAP
Using Root Cause Analysis to Determine Why Readmissions are High. Presentation Objectives. Background Information 11/30/2011
 Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Kaiser Permanente: Transition Care Performance and Strategies
 Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS carbarne@gmail.com April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS carbarne@gmail.com April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
How To Help A Nursing Home And Hospital Collaborate
 Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
Continuum of Care Bridging the Gap between the Hospital and Nursing Home Scott Wells, RN MSN Tiffany Noller, RN MSN Objectives Name key members involved in hospital/nursing home collaborative Identify
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
Reducing Avoidable Readmissions by Improving Transitions in Care New Jersey Hospital Association, Princeton, NJ
 Reducing Avoidable Readmissions by Improving Transitions in Care New Jersey Hospital Association, Princeton, NJ Sept. 29, 2015 Registration: 7:45 a.m. Location: NJHA Conference and Event Center Program:
Reducing Avoidable Readmissions by Improving Transitions in Care New Jersey Hospital Association, Princeton, NJ Sept. 29, 2015 Registration: 7:45 a.m. Location: NJHA Conference and Event Center Program:
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
A Collaborative Initiative to Implement a New Patient Centered, Team Based Care Model Called Accountable Care Unit
 A Collaborative Initiative to Implement a New Patient Centered, Team Based Care Model Called Accountable Care Unit Carolyn Swinton, RN, MN, NEA-BC, FACHE Chief Nursing Officer, Palmetto Health Christina
A Collaborative Initiative to Implement a New Patient Centered, Team Based Care Model Called Accountable Care Unit Carolyn Swinton, RN, MN, NEA-BC, FACHE Chief Nursing Officer, Palmetto Health Christina
Assessing Risk of Readmission. NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013
 Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
Agenda. Topic Industry Today - Quality Measure Reporting Stage 1 Meaningful Use - Overview - Tenet Experience
 Achieving Meaningful Use Symposium Eligible Hospital Perspective Stage 1 Learnings, Stage 2 Preparation Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC, VP, Applied Clinical Informatics, Tenet Health DISCLAIMER:
Achieving Meaningful Use Symposium Eligible Hospital Perspective Stage 1 Learnings, Stage 2 Preparation Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC, VP, Applied Clinical Informatics, Tenet Health DISCLAIMER:
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Mastering emeasures - Charting a Course To Align Quality And Payment
 Mastering emeasures - Charting a Course To Align Quality And Payment a complimentary webinar from healthsystemcio.com, sponsored by Encore Health Resources Housekeeping To ensure you enjoy all the functionality
Mastering emeasures - Charting a Course To Align Quality And Payment a complimentary webinar from healthsystemcio.com, sponsored by Encore Health Resources Housekeeping To ensure you enjoy all the functionality
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
10/16/2013. Partnering with Skilled Nursing Facilities & Home Health Agencies to Prevent Hospital Readmissions. Cedars-Sinai Health System
 Partnering with Skilled Nursing Facilities & Home Health Agencies to Prevent Hospital Readmissions Kelley Hart, LVN, Katie Gurvitz, MHA, Michelle Hofhine, RN Turning on the High Beams October 10, 2013
Partnering with Skilled Nursing Facilities & Home Health Agencies to Prevent Hospital Readmissions Kelley Hart, LVN, Katie Gurvitz, MHA, Michelle Hofhine, RN Turning on the High Beams October 10, 2013
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Erlanger s Care Transitions. Working Together. UT Resident Orientation June 26, 2015
 Erlanger s Care Transitions Working Together UT Resident Orientation June 26, 2015 WHAT IS CARE TRANSITIONS? What is Care Transitions? A program that has been formed to meet and exceed CMS changes from
Erlanger s Care Transitions Working Together UT Resident Orientation June 26, 2015 WHAT IS CARE TRANSITIONS? What is Care Transitions? A program that has been formed to meet and exceed CMS changes from
MEDICAL MANAGEMENT PROGRAM LAKELAND REGIONAL MEDICAL CENTER
 MEDICAL MANAGEMENT PROGRAM LAKELAND REGIONAL MEDICAL CENTER Publication Year: 2013 Summary: The Medical Management Program provides individualized care plans for frequent visitors presenting to the Emergency
MEDICAL MANAGEMENT PROGRAM LAKELAND REGIONAL MEDICAL CENTER Publication Year: 2013 Summary: The Medical Management Program provides individualized care plans for frequent visitors presenting to the Emergency
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Soarian Gaining Momentum
 Soarian Gaining Momentum www.usa.siemens.com/healthcare What is Soarian? Soarian is the next generation healthcare information system (HIS) solution from Siemens. Siemens has engineered Soarian for efficiency.
Soarian Gaining Momentum www.usa.siemens.com/healthcare What is Soarian? Soarian is the next generation healthcare information system (HIS) solution from Siemens. Siemens has engineered Soarian for efficiency.
Expanding the team to the health care community. One practice s experience Holly Cleney, MD
 Expanding the team to the health care community One practice s experience Holly Cleney, MD Objectives Develop a strategy for coordinating care effectively for patients across hospital stays and through
Expanding the team to the health care community One practice s experience Holly Cleney, MD Objectives Develop a strategy for coordinating care effectively for patients across hospital stays and through
Risk Assessment Model
 Transitions of Care and Readmissions Focus on Risk Assessment (and what to do with results) Greg Maynard MD, MSc Clinical Professor of Medicine, Division of Hospital Medicine Director, UCSD Center for
Transitions of Care and Readmissions Focus on Risk Assessment (and what to do with results) Greg Maynard MD, MSc Clinical Professor of Medicine, Division of Hospital Medicine Director, UCSD Center for
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
Tips and Strategies on Handoffs
 Tips and Strategies on Handoffs In 2007, the Handoffs & Transitions Learning Network (H&T) was established to support the mid-atlantic healthcare community in tackling the complex problem of handoffs and
Tips and Strategies on Handoffs In 2007, the Handoffs & Transitions Learning Network (H&T) was established to support the mid-atlantic healthcare community in tackling the complex problem of handoffs and
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Patient Centered Medical Home (PCMH): Communication and Care Coordination
: Communication and Care Coordination") Patient Centered Medical Home (PCMH): Communication and Care Coordination Phillip Roemer, MD Assistant Professor of Medicine General Internal Medicine Feinberg School of Medicine Northwestern University
Patient Centered Medical Home (PCMH): Communication and Care Coordination Phillip Roemer, MD Assistant Professor of Medicine General Internal Medicine Feinberg School of Medicine Northwestern University
Medication Reconciliation
 Medication Reconciliation Jackie Rice, RN EMR Team Supervisor Frederick Memorial Hospital Frederick, Maryland Scope of the Project Implement an automated medication reconciliation tool Meet the 2006 JCAHO
Medication Reconciliation Jackie Rice, RN EMR Team Supervisor Frederick Memorial Hospital Frederick, Maryland Scope of the Project Implement an automated medication reconciliation tool Meet the 2006 JCAHO
Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit
 Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit Presented By: Dr. Micah Beachy, Rickelle Collins and Nicole Turille Context As part of healthcare reform, hospitals are being challenged
Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit Presented By: Dr. Micah Beachy, Rickelle Collins and Nicole Turille Context As part of healthcare reform, hospitals are being challenged
Dr. Peters has declared no conflicts of interest related to the content of his presentation.
 Dr. Peters has declared no conflicts of interest related to the content of his presentation. Steve G. Peters MD NAMDRC 2013 No financial conflicts No off-label usages If specific vendors are named, will
Dr. Peters has declared no conflicts of interest related to the content of his presentation. Steve G. Peters MD NAMDRC 2013 No financial conflicts No off-label usages If specific vendors are named, will
Value-Based Purchasing
 Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Meaningful Use. Medicare and Medicaid EHR Incentive Programs
 Meaningful Use Medicare and Medicaid Table of Contents What is Meaningful Use?... 1 Table 1: Patient Benefits... 2 What is an EP?... 4 How are Registration and Attestation Being Handled?... 5 What are
Meaningful Use Medicare and Medicaid Table of Contents What is Meaningful Use?... 1 Table 1: Patient Benefits... 2 What is an EP?... 4 How are Registration and Attestation Being Handled?... 5 What are
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care
 NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes
 Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
PHS-Connect Users Group Forum. November 7, 2013
 PHS-Connect Users Group Forum November 7, 2013 Agenda Introductions and Opening Remarks PHS-Connect Update Direction of PHS-Connect What can PHS-Connect Do for Me and My EMR Secure Messaging for MU2 and
PHS-Connect Users Group Forum November 7, 2013 Agenda Introductions and Opening Remarks PHS-Connect Update Direction of PHS-Connect What can PHS-Connect Do for Me and My EMR Secure Messaging for MU2 and
THE ACTIVELY CONNECTED PHYSICIAN
 THE ACTIVELY CONNECTED PHYSICIAN How Direct Messaging Leads to Improved Patient Care OVERVIEW Health care connectivity made great strides in 2014. As more health delivery networks, hospitals and physicians
THE ACTIVELY CONNECTED PHYSICIAN How Direct Messaging Leads to Improved Patient Care OVERVIEW Health care connectivity made great strides in 2014. As more health delivery networks, hospitals and physicians
MEDICAL CENTER POLICY NO. 0094. A. SUBJECT: Documentation of Patient Care (Electronic Medical Record)
") Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0094 A. SUBJECT: Documentation of Patient Care (Electronic Medical Record) B. EFFECTIVE DATE: April 1, 2012 (R) C. POLICY: The University of
Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0094 A. SUBJECT: Documentation of Patient Care (Electronic Medical Record) B. EFFECTIVE DATE: April 1, 2012 (R) C. POLICY: The University of
REACHING ZERO DEFECTS IN CORE MEASURES. Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC,
 REACHING ZERO DEFECTS IN CORE MEASURES Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC, 165 Lake Linden Dr., Bluffton SC 29910, 843-364-3408, marybrady6@gmail.com Primary
REACHING ZERO DEFECTS IN CORE MEASURES Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC, 165 Lake Linden Dr., Bluffton SC 29910, 843-364-3408, marybrady6@gmail.com Primary
Announcements. Upcoming Report Dates 3/12/2013. Best Practices to Improve Your Hospital Outpatient Quality Reporting.
 Best Practices to Improve Your Hospital Outpatient Quality Reporting March 20, 2013 Announcements This program has been approved for 1.0 continuing education unit (CEU) given by Continuing Education (CE)
Best Practices to Improve Your Hospital Outpatient Quality Reporting March 20, 2013 Announcements This program has been approved for 1.0 continuing education unit (CEU) given by Continuing Education (CE)
Clinical Outcomes and Home Infusion A Way Forward Connie Sullivan, RPh demand side strategy References: National Business Coalition on Health
 Clinical Outcomes and Home Infusion A Way Forward Connie Sullivan, RPh Senior Director Education and Data, NHIA Vice President of Research, NHIF Session Objectives Define value based purchasing, and describe
Clinical Outcomes and Home Infusion A Way Forward Connie Sullivan, RPh Senior Director Education and Data, NHIA Vice President of Research, NHIF Session Objectives Define value based purchasing, and describe
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Transitions of Care: The need for a more effective approach to continuing patient care
 H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
Population Health Management Infrastructure
 Population Health Management Infrastructure William Pagano MD, MPH SVP of Clinical Operations Doreen Colella RN, MSN AVP of Quality Interfaces The Azara reporting tool interfaces with multiple systems.
Population Health Management Infrastructure William Pagano MD, MPH SVP of Clinical Operations Doreen Colella RN, MSN AVP of Quality Interfaces The Azara reporting tool interfaces with multiple systems.
With New Models of Value-Based Care. September 1, 2015
 With New Models of Value-Based Care September 1, 2015 Using Community Care Coordination and Mobile Technology to Impact Health Outcomes and Reduce Avoidable Hospital Encounters Presenters: Chris Parsons,
With New Models of Value-Based Care September 1, 2015 Using Community Care Coordination and Mobile Technology to Impact Health Outcomes and Reduce Avoidable Hospital Encounters Presenters: Chris Parsons,
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
Introduction... 2. The Value of Certification... 3. Promote your ONC, ONP C, and OCNS C Credentials... 5. Serve as a Certification Leader...
 TABLE OF CONTENTS Introduction... 2 The Value of Certification... 3 Promote your ONC, ONP C, and OCNS C Credentials... 5 Serve as a Certification Leader... 6 Certification Resources... 9 Appendix A Sample
TABLE OF CONTENTS Introduction... 2 The Value of Certification... 3 Promote your ONC, ONP C, and OCNS C Credentials... 5 Serve as a Certification Leader... 6 Certification Resources... 9 Appendix A Sample
Medical Clinic Tasking Guidelines
 Medical Clinic Tasking Guidelines 2011 Our Mission The mission of Neighborcare Health is to provide comprehensive health care to families and individuals who have difficulty accessing care; respond with
Medical Clinic Tasking Guidelines 2011 Our Mission The mission of Neighborcare Health is to provide comprehensive health care to families and individuals who have difficulty accessing care; respond with
Eddy VNA Care Transitions Program
 Eddy VNA Care Transitions Program Patrick Archambeault RN, MS, CRNI Director of Clinical Specialties About Eddy VNA Large not for profit home care agency based in upstate New York CHHA, LTHHCP, Licensed
Eddy VNA Care Transitions Program Patrick Archambeault RN, MS, CRNI Director of Clinical Specialties About Eddy VNA Large not for profit home care agency based in upstate New York CHHA, LTHHCP, Licensed
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES. MICROMEDEX Patient Connect. Patient Education & Engagement
 TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES MICROMEDEX Patient Connect Patient Education & Engagement Trusted Patient Education for Better Outcomes All your training, experience, tools, and technology
TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES MICROMEDEX Patient Connect Patient Education & Engagement Trusted Patient Education for Better Outcomes All your training, experience, tools, and technology
Discharge Planning. Home Care 1. Objectives. Where are they Going?
 Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
New Models of Care and Approaches to Payment
 New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Contact: Barbara J Stout RN, BSC Implementation Specialist University of Kentucky Regional Extension Center 859-323-4895
 Contact: Barbara J Stout RN, BSC Implementation Specialist University of Kentucky Regional Extension Center 859-323-4895 $19.2B $17.2B Provider Incentives $2B HIT (HHS/ONC) Medicare & Medicaid Incentives
Contact: Barbara J Stout RN, BSC Implementation Specialist University of Kentucky Regional Extension Center 859-323-4895 $19.2B $17.2B Provider Incentives $2B HIT (HHS/ONC) Medicare & Medicaid Incentives
EMR DOCUMENTATION LYNX. Instructor Script
 EMR DOCUMENTATION LYNX Instructor Script Table of Contents TABLE OF CONTENTS INFORMATION SECURITY AND CONFIDENTIALITY... 4 OVERVIEW... 5 LEARNING OBJECTIVES... 5 TIPS AND TRICKS... 5 SOLUTION ICONS...
EMR DOCUMENTATION LYNX Instructor Script Table of Contents TABLE OF CONTENTS INFORMATION SECURITY AND CONFIDENTIALITY... 4 OVERVIEW... 5 LEARNING OBJECTIVES... 5 TIPS AND TRICKS... 5 SOLUTION ICONS...
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Care Transitions: Success Stories and Lessons Learned
 Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
Care Transitions: Success Stories and Lessons Learned Kim McCoy, Stratis Health Kris Garman, Redwood Area Hospital Joleen Johnson, Redwood Area Hospital June 29, 2015 Objectives Learn strategies for implementation
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Improving Care Transitions using PDSA Methodology
 Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
Medweb Telemedicine 667 Folsom Street, San Francisco, CA 94107 Phone: 415.541.9980 Fax: 415.541.9984 www.medweb.com
 Medweb Telemedicine 667 Folsom Street, San Francisco, CA 94107 Phone: 415.541.9980 Fax: 415.541.9984 www.medweb.com Meaningful Use On July 16 2009, the ONC Policy Committee unanimously approved a revised
Medweb Telemedicine 667 Folsom Street, San Francisco, CA 94107 Phone: 415.541.9980 Fax: 415.541.9984 www.medweb.com Meaningful Use On July 16 2009, the ONC Policy Committee unanimously approved a revised
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
Welcome to the New England QIN-QIO Medication Safety Webinar!
 Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line by calling: 888-285-0307
Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line by calling: 888-285-0307
OF MEANINGFUL USE THE HIDDEN REQUIREMENTS HOSPITAL QUALITY REPORTING: Introduction. Authors: Jane Metzger, Melissa Ames and Jared Rhoads
 HOSPITAL QUALITY REPORTING: THE HIDDEN REQUIREMENTS OF MEANINGFUL USE Authors: Jane Metzger, Melissa Ames and Jared Rhoads Hospitals must report on 15 required quality measures for Stage 1, using the certified
HOSPITAL QUALITY REPORTING: THE HIDDEN REQUIREMENTS OF MEANINGFUL USE Authors: Jane Metzger, Melissa Ames and Jared Rhoads Hospitals must report on 15 required quality measures for Stage 1, using the certified
How To Prepare For A Patient Care System
 Preparing for Online Communication with Your Patients A Guide for Providers This easy-to-use, time-saving guide is designed to help medical practices and community clinics prepare for communicating with
Preparing for Online Communication with Your Patients A Guide for Providers This easy-to-use, time-saving guide is designed to help medical practices and community clinics prepare for communicating with
Medication Error. Medication Errors. Transitions in Care: Optimizing Intern Resources
 Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/26/2015 This document is intended to provide health care s in Ontario with guidance as to how they can develop a Quality
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/26/2015 This document is intended to provide health care s in Ontario with guidance as to how they can develop a Quality
Community Care of North Carolina
 Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
UTILIZATION MANAGEMENT PROGRAM Introduction Health Care Services
 UTILIZATION MANAGEMENT PROGRAM Introduction Health Care Services Call us: 1-888-898-7969, Option 1, then Option 4 Fax us: 1-800-594-7404 Business hours: Monday Friday (excluding holidays), 8:30 a.m. to
UTILIZATION MANAGEMENT PROGRAM Introduction Health Care Services Call us: 1-888-898-7969, Option 1, then Option 4 Fax us: 1-800-594-7404 Business hours: Monday Friday (excluding holidays), 8:30 a.m. to
Overview of emar Electronic Medication Administration Record
 Overview of emar Electronic Medication Administration Record March 2006 WHAT IS emar? emar Electronic Medication Administration Record - Replaces the paper MAR MAK Medication Administration Check (Siemens)
Overview of emar Electronic Medication Administration Record March 2006 WHAT IS emar? emar Electronic Medication Administration Record - Replaces the paper MAR MAK Medication Administration Check (Siemens)
RED, BOOST, and You: Improving the Discharge Transition of Care
 RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Before and After Your Cardioversion
 2013 Before and After Your Cardioversion Before and After Your Cardioversion Preparing for your cardioversion Your doctor has recommended cardioversion to treat your heart rhythm problem. This booklet
2013 Before and After Your Cardioversion Before and After Your Cardioversion Preparing for your cardioversion Your doctor has recommended cardioversion to treat your heart rhythm problem. This booklet
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Reconciling the Differences. Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit
 Reconciling the Differences Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit Objectives 1. Review the medication discharge counselling process in the renal dialysis program 2.
Reconciling the Differences Karen Lippett B.Sc.Phm Humber River Regional Hospital Renal Dialysis Unit Objectives 1. Review the medication discharge counselling process in the renal dialysis program 2.
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
NICHE: Innovations and Nursing Practice
 NICHE: Innovations and Nursing Practice nicheprogram.org Linda Bub MSN, RN, GCNS-BC Director of Education and Program Development, NICHE Objectives Describe the NICHE program and the impact on nursing
NICHE: Innovations and Nursing Practice nicheprogram.org Linda Bub MSN, RN, GCNS-BC Director of Education and Program Development, NICHE Objectives Describe the NICHE program and the impact on nursing
Traditional and Emerging Roles of the Stroke Coordinator. Kathy Morrison, MSN, RN, CNRN, SCRN Jean Luciano, MSN, RN, CNRN, CRNP
 Traditional and Emerging Roles of the Stroke Coordinator Kathy Morrison, MSN, RN, CNRN, SCRN Jean Luciano, MSN, RN, CNRN, CRNP Disclosures: Kathy Morrison - I have no actual or potential conflict of interest
Traditional and Emerging Roles of the Stroke Coordinator Kathy Morrison, MSN, RN, CNRN, SCRN Jean Luciano, MSN, RN, CNRN, CRNP Disclosures: Kathy Morrison - I have no actual or potential conflict of interest
OPTIMIZING THE USE OF YOUR ELECTRONIC HEALTH RECORD. A collaborative training offered by Highmark and the Pittsburgh Regional Health Initiative
 OPTIMIZING THE USE OF YOUR ELECTRONIC HEALTH RECORD A collaborative training offered by Highmark and the Pittsburgh Regional Health Initiative Introductions Disclosures Successful completion of training
OPTIMIZING THE USE OF YOUR ELECTRONIC HEALTH RECORD A collaborative training offered by Highmark and the Pittsburgh Regional Health Initiative Introductions Disclosures Successful completion of training
MD-REPORTS. Comprehensive, specialty specific one stop solution for Office, Ambulatory and Hospital electronic document requirements
 MD-REPORTS COMPLETE SOFTWARE SOLUTION FOR OFFICE, SURGERY CENTER AND HOSPITAL Comprehensive, specialty specific one stop solution for Office, Ambulatory and Hospital electronic document requirements ONC-ATCB
MD-REPORTS COMPLETE SOFTWARE SOLUTION FOR OFFICE, SURGERY CENTER AND HOSPITAL Comprehensive, specialty specific one stop solution for Office, Ambulatory and Hospital electronic document requirements ONC-ATCB
Streamline Your Radiology Workflow. With Radiology Information Systems (RIS) and EHR
 and EHR") Streamline Your Radiology Workflow With Radiology Information Systems (RIS) and EHR 2 Practicing medicine effectively requires transferring large amounts of information quickly, accurately, and securely.
Streamline Your Radiology Workflow With Radiology Information Systems (RIS) and EHR 2 Practicing medicine effectively requires transferring large amounts of information quickly, accurately, and securely.
Title/Description: Discharge Medication Planning, Education, and Procurement
 University of Kentucky / UK HealthCare Policy and Procedure Policy # A02-030 Title/Description: Discharge Medication Planning, Education, and Procurement Purpose: To educate patients discharged from UK
University of Kentucky / UK HealthCare Policy and Procedure Policy # A02-030 Title/Description: Discharge Medication Planning, Education, and Procurement Purpose: To educate patients discharged from UK
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time