What Do We Know About Health Care Access and Quality in Medicare Advantage Versus the Traditional Medicare Program?
|
|
|
- Damon Campbell
- 8 years ago
- Views:
Transcription
1 REPORT What Do We Know About Health Care Access and Quality in Medicare Advantage Versus the Traditional Medicare Program? November 2014 Prepared by: Marsha Gold, Sc.D. Senior Fellow Emeritus, Mathematica Policy Research, and Consultant and Giselle Casillas Kaiser Family Foundation

2

3 Executive Summary... i Introduction... 1 Methods... 2 Findings... 4 Overview of Published Studies... 4 Characteristics and Relevance of Core Studies... 5 Study Findings by Type of Metric HEDIS Quality Metrics for Effective Care CAHPS and Similar Beneficiary-Reported Metrics Appropriateness and Outcomes of Medicare Hospitalizations Other Utilization Metrics Health Care Outcomes and Mortality Summary of Findings and Conclusions Works Cited Appendix. Care for Seniors in Medicare Advantage versus the Veterans Health Administration... 47

4 While the majority of Medicare beneficiaries still receive their benefits through the traditional Medicare program, 30 percent now obtain them through private health plans participating in Medicare Advantage. As the number of Medicare Advantage enrollees continues to climb, there is growing interest in understanding how the care provided to Medicare beneficiaries in Medicare Advantage plans differs from the care received by beneficiaries in traditional Medicare. Despite the interest, the last comprehensive review of research evidence on health care access and quality in Medicare Advantage and traditional Medicare is more than 10 years old and did not focus exclusively on Medicare (Miller and Luft 2002). That study found that health maintenance organizations (HMOs) provide care that is roughly comparable in quality to the care provided by non-hmos (mainly traditional indemnity insurance), and that quality varied across health plans. It also found that HMOs used somewhat fewer hospital and other expensive resources in delivering care, with enrollees rating them worse on many measures of access and satisfaction. However, the market has changed substantially over the last decade, making it important that policymakers have available more current analysis, particularly on Medicare health plans. This literature review synthesizes the findings of studies that focus specifically on Medicare and have been published between the year 2000 and early Forty-five studies met the criteria for selection, including 40 that made direct comparisons between Medicare health plans and traditional Medicare. An additional five studies are included, even though they have no traditional Medicare comparison group, because they include a comparison of health care access and quality in different types of Medicare Advantage plans. A full list of the studies included in this analysis is found in the Works Cited. The review of the literature comparing quality and access provided under traditional Medicare and Medicare Advantage plans suggests the following: Medicare Advantage, on average, scores more highly than traditional Medicare on subsets of Medicare HEDIS indicators primarily those pertaining to use of preventive care services. Two studies found Medicare preferred provider organizations (PPOs) outperformed traditional Medicare on some metrics (particularly mammography rates), though HMOs nevertheless performed better than PPOs. All of these studies were conducted prior to changes made by the Affordable Care Act (ACA) to improve coverage of preventive services under traditional Medicare. Medicare beneficiaries generally rated Medicare Advantage lower than traditional Medicare on questions about health care access and quality, especially if beneficiaries had a chronic illness or were sick; however, the difference in ratings between traditional Medicare and Medicare Advantage narrowed on some metrics by 2009 (e.g., overall care ratings). Keenan et al. (2009) found that sick beneficiaries in Medicare Advantage rated their plans substantially lower than beneficiaries of similar health status in traditional Medicare, and Elliott et al. (2011) found significantly lower CAHPS ratings (and greater disparities between Medicare Advantage and traditional Medicare) among vulnerable subgroups of beneficiaries in Medicare Advantage. Little is known about how CAHPS scores vary

5 by type of Medicare Advantage plan since most studies are based on HMOs or periods in which HMOs were the main plan type. Based on six studies involving beneficiaries in a limited number of states and/or plans represented by the Alliance of Community Health Plans (ACHP), Medicare beneficiaries in HMOs are less likely to be hospitalized for a potentially avoidable admission than beneficiaries in traditional Medicare. Four of these studies rely on data prior to 2006, and reflect HMO experiences in mature markets. While a number of studies examine whether readmission rates differ among beneficiaries in Medicare Advantage and traditional Medicare, the evidence from these studies is inconclusive because findings differ across the studies and many studies lack adjustments for important potentially confounding factors. There is some evidence that good coverage, as defined by relatively low cost-sharing (whether through Medicare HMOs or through Medicare with supplemental coverage), may result in earlier diagnoses of some cancers compared to traditional Medicare alone. Treatment patterns for some cancers also may differ between Medicare HMOs and traditional Medicare, but studies do not show that this affects patient outcomes. However, the age of the studies, the gaps in controls for selection, and the evolving nature of guidelines for appropriate care limit the conclusions that can be drawn. Medicare HMOs appear to provide a less resource-intensive style of practice than traditional Medicare, as measured in studies examining end-of-life care, use of certain procedures, and overall utilization rate in HMOs, especially for hospital services. However, most of these studies provide little direct evidence of whether less intensive care is better or worse or how the appropriateness of care differs between Medicare Advantage and traditional Medicare. On a variety of metrics, performance among Medicare Advantage plans varies substantially across plans, even among plans of the same plan type. The variations by market in more established HMOs with integrated delivery systems tend to be more represented in existing research, and to perform better. Performance on quality and access metrics varies across geographic areas, and the variations in Medicare Advantage and traditional Medicare ratings are not necessarily the same. To make a definitive comparison of both quality and access in traditional Medicare and Medicare Advantage plans, one would ideally draw from studies with relatively recent data that is nationally representative in terms of both the characteristics of health plans participating in Medicare Advantage and the characteristics of beneficiaries covered by the Medicare program. Performance measures would capture a broad range of metrics assessing both quality of care and access to care, and would include enrollees assessments, process measures, and outcome measures. The comparisons would adjust for factors that might explain differences in performance between Medicare Advantage and traditional Medicare, such as variations in medical practice by geographical location and patient health status. In an ideal world, studies would provide information to help clarify if differences vary by plan type, and how quality and access indicators compare for the typical Medicare beneficiary, as well as beneficiaries who are in relatively poor health with significant medical needs.

6 Unfortunately, while available evidence provides some insights, it falls short on many desirable dimensions. The most serious shortfalls are in the lack of timely data, the primary focus on HMOs rather than the full range of Medicare Advantage plans, and study populations that exclude important subgroups of beneficiaries (such as the under-65 disabled) and lack information on the experience of vulnerable subgroups of beneficiaries, such as those in poor health or with significant needs. In addition, available metrics are limited in their ability to capture performance across the full continuum of care and care for the total patient, particularly on a national basis. Our review of the literature comparing quality and access measures between traditional Medicare and Medicare Advantage finds: With one limited exception involving hospice care, none of the 40 studies comparing Medicare Advantage to traditional Medicare rely on data from 2010 or later. Thus, it is not yet possible to assess the performance of Medicare Advantage relative to traditional Medicare that reflects plan performance after the implementation of the Medicare Advantage payment changes included in the ACA (payment reductions, coupled with quality bonus payments). Fourteen of the 40 studies report only on experience in the 1990s or earlier, and of the 27 others covering the period, 16 provide estimates between 2006 and 2009, after the introduction of the Medicare prescription drug benefit. Almost all of the literature applies to the experience of beneficiaries in HMOs, rather than in the full range of plans that are currently available. In 2014, for example, one-third of all Medicare Advantage enrollees are in plans other than HMOs, mainly PPOs. Only three of the 40 studies that compared traditional Medicare to Medicare Advantage (and two of the five that compared Medicare Advantage plans only) included findings that were specific to Medicare PPOs. Others either are limited to HMOs, apply to a period when HMOs were the overwhelming plan type, or do not analyze data by plan type. As a result, the results are not generalizable to the Medicare Advantage program as a whole as contrasted with the experience of its older HMO component. Few of the existing studies provide insight on how Medicare Advantage and traditional Medicare perform on quality and access metrics for beneficiaries whose health characteristics suggest that they could have more complex needs. Only four studies, all based on beneficiary survey data, focused explicitly on subgroups of the Medicare population defined by the authors as high-need based on health or functional status (Keenan et al. 2009, Elliott et al. 2011, Pourat et al. 2001, and Beatty and Dhont 2001). One study (Elliott et al. 2011) also examined disparities in care for vulnerable subgroups defined by various socioeconomic indicators, along with health status. The inability to reflect the experiences of beneficiaries with significant health needs is a major limitation in the literature.. While several studies are national in scope (plans and beneficiaries), the metrics they include are limited by available data. Of the 17 national studies comparing Medicare Advantage to traditional Medicare (of 40 in total), 10 rely exclusively on CAHPS or other national population surveys, and seven use HEDIS data compared to claims data for traditional Medicare. Vital statistics data dealing with mortality were used in two of the studies as well. Studies on many metrics relevant to quality either do not exist (like intermediate outcomes for beneficiaries with multiple chronic

7 conditions or the personal experience with care of these patients) or, like studies of potentially avoidable admissions and readmissions, depend on data from a limited set of states or locales. Despite great interest in comparisons between traditional Medicare and Medicare Advantage, studies comparing overall quality and access to care between Medicare Advantage plans and traditional Medicare tend to be based on relatively old data, and a limited set of measures. On the one hand, the evidence indicates that Medicare HMOs tend to perform better than traditional Medicare in providing preventive services and using resources more conservatively, at least through These are metrics where HMOs have historically been strong. On the other hand, beneficiaries continue to rate traditional Medicare more favorably than Medicare Advantage plans in terms of quality and access, such as overall care and plan rating, though one study suggests that the difference may be narrowing between traditional Medicare and Medicare Advantage for the average beneficiary. Among beneficiaries who are sick, the differential between traditional Medicare and Medicare Advantage is particularly large (relative to those who are healthy), favoring traditional Medicare. Very few studies include evidence based on all types of Medicare Advantage plans, including analysis of performance for newer models, such as local and regional PPOs whose enrollment is growing. As the beneficiary population ages, better evidence is needed on how Medicare Advantage plans perform relative to traditional Medicare for patients with significant medical needs that make them particularly vulnerable to poorer care. The ability to assess quality and access for such subgroups is limited because many data sources do not allow subgroups to be identified or have too small a sample size to support estimates. Also, in many cases, metrics employed may not be specific to the particular needs or the way a patient s overall health and functional status or other comorbid conditions influence the care they receive. At a time when enrollment in Medicare Advantage is growing, it is disappointing that better information is not available to inform policymaking. Our findings highlight the gaps in available evidence and reinforce the potential value of strengthening available data and other support for tracking and monitoring performance across Medicare Advantage plans and traditional Medicare as each sector evolves.

8 Figure 1: Total Medicare Advantage Enrollment by Plan Type, Table 1: Overview of Reviewed Studies Table 2: Overview of Studies Comparing Medicare Advantage to Traditional Medicare by Category of Metric Table 3: Overview of Studies of Medicare Advantage Plans (no comparison with traditional Medicare) Table 4: Summary of Studies Comparing Medicare HEDIS Effectiveness of Care Metrics Table 5: Summary of Studies Comparing Medicare Beneficiary-Reported Metrics Table 6: Summary of Studies Comparing Appropriateness and Outcomes of Medicare Hospitalizations Table 7: Summary of Studies Comparing Utilization Table 8: Summary of Studies Comparing Health Care Outcomes and Mortality Appendix Table A.1: Summary of Studies Comparing Quality of Care for Seniors in Medicare Advantage versus the Veterans Health Administration

9 Medicare is critical to the well-being of the nation s seniors and people with disabilities, many of whom have low to moderate incomes, complex health care needs, and other characteristics that leave them disproportionately vulnerable. 1 While the majority of Medicare beneficiaries still receive their benefits through the traditional Medicare program, 30 percent now obtain their benefits through private health plans participating in Medicare Advantage. 2 As the number of enrollees in Medicare Advantage continues to climb, there is growing interest in understanding how care provided to Medicare beneficiaries in traditional Medicare and Medicare Advantage differs. Despite the considerable interest in this topic, solid analysis summarizing existing research comparing Medicare Advantage to traditional Medicare on various quality and access metrics is relatively limited. Historical reviews of performance differences across health plans have generally focused on comparisons of organizational structures (like health maintenance organizations or HMOs) rather than focusing on particular payers, like Medicare. The most widely cited reviews available have been conducted over the years by Miller and Luft, with the most recent review covering work through mid It concluded that the quality of care provided by HMOs was roughly comparable to traditional insurance, though it varied across health plans; HMOs used somewhat fewer hospital and other expensive resources to deliver care compared to traditional insurance, and had lower ratings by enrollees on many measures of access and satisfaction. An earlier study in the series (Miller and Luft 1997) noted that Medicare beneficiaries with chronic conditions had worse outcomes in HMOs. 4 Since these reviews were published, the environment has changed considerably. The historical base of HMOs in nonprofit staff and group model plans has shifted considerably, with new growth in for-profit plans that use more decentralized provider networks that tend to be less integrated. 5 Further, since the mid-2000s, the number and share of Medicare beneficiaries enrolled in private plans, now called Medicare Advantage, has increased dramatically, and while most enrollees are in HMOs, a growing number are enrolled in other types Figure Exhibit 1. 2 of plans, such as local and regional PPOs (Figure 1). Total Medicare Advantage Enrollment, by Plan Type, In millions: Other plan types HMOs % of Medicare Beneficiaries The policy environment and incentives facing providers in the Medicare program also have changed in ways that put increasing emphasis on payments that take into account performance on quality and efficiency metrics. For Medicare Advantage, the Affordable Care Act of 2010 (federal health reform law) enacted changes in payments to plans that are now being phased in, slowing the increase in Medicare Advantage payments and % 22% 23% 24% 25% 27% 28% 30% NOTE: Includes MSAs, cost plans and demonstrations. Includes Special Needs Plans as well as other Medicare Advantage plans. SOURCE: Analysis by the Kaiser Family Foundation of publicly-available CMS Medicare Advantage enrollment files,

10 linking them more closely with performance on quality and other performance metrics. 6 Medicare Advantage plans that score four or more out of five stars are provided bonus payments and those that score the highest (so-called five star plans ) gain other advantages, particularly the ability to continuously enroll beneficiaries throughout the year. 7 Payment to hospitals, physicians, and other providers in the traditional Medicare program also are increasingly tied to quality metrics as a result of changes in the ACA and other legislation. The ACA also improved coverage of preventive services under traditional Medicare, which has been a metric in which managed care plans have historically performed better. Such changes increase the interest within the policy community in current information comparing the quality of care provided to beneficiaries in Medicare Advantage plans and traditional Medicare. Proponents of the insurance industry argue that quality under Medicare Advantage has improved and is better than under the traditional program - an accomplishment, they argue, that could be undermined by ongoing reductions in payments as required under the federal health reform law. 8 In a recent review, Newhouse and McGuire (2013) summarized three studies they coauthored that compared Medicare Advantage to traditional Medicare, and concluded that the findings from those studies favored Medicare Advantage. 9 The review has gotten considerable attention. 10 Lost in the discussion, however, is the fact that the main thrust of the article focused on efficiency and selection within Medicare Advantage, with the authors acknowledging that research comparing the quality of care in Medicare Advantage versus traditional Medicare is limited. This study seeks to fill the gap in available information on current evidence comparing quality and access in Medicare Advantage plans and traditional Medicare. Unlike earlier literature reviews, the focus of this paper is on Medicare, and limited to studies that are relatively current; that is, published between 2000 and early We identified the initial list of studies using a Google Scholar search for articles on Medicare Advantage/Medicare HMOs published since We reviewed titles and abstracts to identify studies focusing on access/quality metrics and including a design that had some comparison group typically traditional Medicare, or what some still refer to as Medicare fee-for-service (FFS). Because Google Scholar does not index the most recent year s publications and is a less established search source, we also contracted with a trained health research librarian to conduct a formal Medline search covering the period That search used the terms Medicare health plans, Medicare HMO, Medicare Advantage, and Medicare Advantage PPO in comparison to FFS Medicare, Medicare, and traditional Medicare, with the keywords quality of care, access, and outcomes. 12 To ensure coverage of studies that may be relevant to the policy debate but are not found in the academic literature, we also reviewed the sources cited in industry briefs and the most recent Medicare Payment Advisory Commission (MedPAC) report to Congress on Medicare Advantage. 13 In addition, we checked citations in those studies identified for any other relevant studies not already identified. 14 To be included in the review, studies had to include (1) a written description of methods and data sources, (2) a formal comparison group, and (3) outcome measures relevant to access or quality. Although we did not

11 otherwise exclude studies based on the quality of their methods, we reviewed articles for how they handled such potentially confounding factors as geographic location, enrollee mix, and health and risk factors associated with selection. Because our analysis focused on Medicare health plans available for general enrollment, we excluded studies focused on specialized plans particularly social HMOs, PACE, and Special Needs Plans (SNPs). Health care quality problems can arise though underuse, overuse, and misuse of services. 15 Some of these domains are better captured in existing quality metrics than others. 16 Because the review was focused on access and quality of health care received by beneficiaries in different types of insurance arrangements, rather than insurance per se, studies focused primarily on benefits or the factors that influence health plan selection were not considered. Five categories of metrics are considered in this paper. HEDIS measures, which Medicare health plans report to the Centers for Medicare and Medicaid Services (CMS), are central to oversight in Medicare Advantage. In 2014, Medicare Advantage plans were required to submit audited data consistent with National Committee for Quality Assurance (NCQA) specifications for 25 metrics on health care effectiveness and another three on access and availability of services, among other metrics. 17 HEDIS effectiveness indicators focus on the processes of care or intermediate outcomes rather than ultimate outcomes; metrics relevant to those with chronic illness are limited, though efforts are underway to broaden the measure set. Patient-level data used to support these metrics come from claims, encounter data, and for some metrics, medical records. A subset of these metrics is used to support calculation of Medicare Advantage plan star quality ratings, the basis for bonus payments to plans. Increasing efforts have been made to align reporting requirements across Medicare Advantage plans of different types, but data historically have been most available for HMOs and least available for private FFS plans and regional PPOs. 18 HEDIS metrics are not routinely calculated for traditional Medicare. MedPAC is considering better ways to align requirements and metrics across programs, taking into account the differences in data sources used in each sector. 19 CAHPS is a health plan member survey that provides patient reports of care experiences with their plan, including ratings of access to care and satisfaction with the plan and its providers. 20 To support its use, CMS conducted a related survey of beneficiaries in traditional Medicare residing in those same geographical areas (in 2011, it replaced this survey with a requirement that freestanding prescription drug plans collect CAHPS data). Using its contractors, CMS has developed a number of composite measures of reported care and use of preventive services, as well as global health ratings. Some of the same items are included in standard national surveys, such as the Medicare Current Beneficiary Survey (MCBS) and the National Health Interview Survey (NHIS). Because they provide insight into how beneficiaries view care, beneficiary surveys long have been a central component of most efforts to examine access and quality of care in Medicare. From a quality and value perspective, metrics that provide information on the appropriateness and quality of hospital care are of growing interest. Key metrics in this area focus on the appropriateness of hospital admissions that potentially could be avoided by more timely and appropriate primary care, the appropriateness and quality of facilities and professional services used, and

12 the ability to structure discharges in ways that avoid personally and financially costly complications and hospital readmissions. CMS now captures data on case-mix adjusted Medicare rehospitalization rates as part of HEDIS reporting from health plans. In the absence of national data, most research on this topic has used data available through all-payer discharge data sets available in selected states and from the Agency for Healthcare Research and Quality's (AHRQ s) databases. Only some of these files have appropriate identifiers to distinguish enrollment in Medicare health plans, and the timeliness of information often lags. While adjusting for case mix and severity is important in all comparisons of quality, it is particularly important in studies of hospital appropriateness or outcomes, when poor outcomes may be small in number and highly sensitive to the mix of enrollees. Given the limitations in available data that directly measure access and quality of health services for beneficiaries in Medicare Advantage and traditional Medicare, researchers have included various other measures of utilization as a proxy for direct measures of these aspects of care. Like the hospital utilization measures, some of these metrics target specific kinds of utilization that have been used as markers for overuse, underuse, or misuse of services, including emergency department (ED) visits, patterns of care at the end of life, procedure use for urgent versus non-urgent conditions, or high-cost procedures versus others. Medicare Advantage plans report on some of these metrics in the Utilization and Relative Resource Use section of the HEDIS performance monitoring submission form. Utilization-based measures can be difficult to interpret as quality metrics when norms defining appropriateness are lacking or in dispute, and when it is unclear what constitutes overuse or underuse and whether overuse or underuse are markers for better or worse care. Such measures also require careful risk adjustment for selection. Studies that use aggregate measures of utilization probably are better interpreted as indications of resource use rather than quality of care. Ultimately, the goal of medical care is to improve patient outcomes and quality of life. Data sets available for studies of this type are limited and those that exist do not always include good information on health insurance type or adequate data to link with other sources containing such data. There are also methodological challenges in adjusting for patient selection and mix adequately. Cancer studies are supported by cancer registry data maintained by states and the National Cancer Institute s Surveillance and Epidemiology and End Results (SEER) data, among others. A total of 45 unique studies were identified using the methods and criteria discussed (Table 1), of which 40 involved comparisons between Medicare Advantage plans and traditional Medicare. The other five studies made comparisons among Medicare HMOs or between HMOs and PPOs, but did not compare Medicare Advantage plans to traditional Medicare. A complete list of all the studies that are included in our review is found at the end of this document. An additional six studies compared the care received in Medicare health plans to care in the Veterans Health Administration (VHA) system; since they involve a highly specialized comparison, they are not included in the core analysis and text but their findings are summarized in the Appendix.
 databases. Only some of these files have appropriate identifiers to distinguish enrollment in Medicare health plans, and the timeliness of information often lags.")
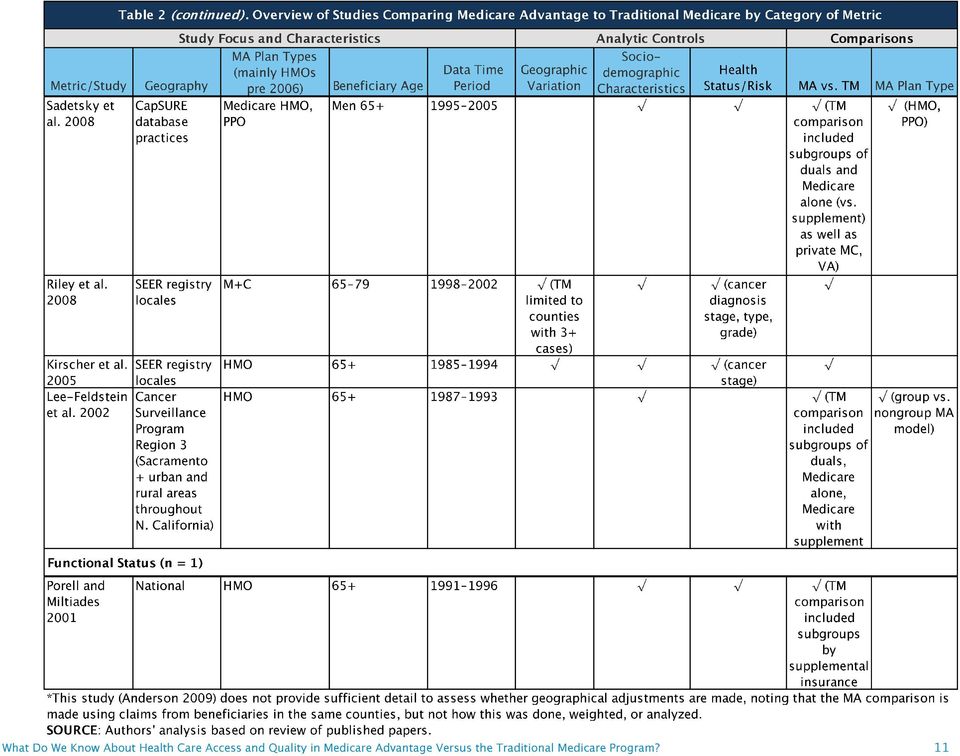
13 Table 2 summarizes the 40 studies that make comparisons between Medicare Advantage (or predecessor program health plans) and traditional Medicare. Studies (the rows) are grouped by type of quality or access metric, 1 with columns providing detail on the main focus and characteristics of individual studies and the types of study controls and comparisons made. Table 3 provides the same information for the five studies involving comparisons solely within Medicare Advantage. Ideally, one would want studies with current data, across a wide variety of health plans nationally, using diverse outcome measures, with good controls for other factors that could explain differences in performance between Medicare Advantage and traditional Medicare. Unfortunately, the studies identified fall short in many of these areas. Almost all studies focused only on a single type of metric because of the data sources they employed. (Ayanian 2013a is an exception). Where more than one source is used, we classify the study based on its predominant method but discuss findings wherever they are relevant.

14 While this review aims to assess current Medicare Advantage practice, the studies available to support such an assessment are very limited. With one limited exception an analysis of hospice use none of the studies comparing Medicare Advantage to traditional Medicare include data from 2010 or later, which means none cover the experience of beneficiaries after the changes enacted in the ACA. Fourteen of the 40 studies use data from the 1990s or earlier. Of the 27 other studies covering the period, 16 provide estimates for 2006 or later after the Medicare Advantage changes introduced in the Medicare Modernization Act of 2003 began to drive the market with the introduction of the Medicare prescription drug benefit in While Medicare health plans have become increasingly diverse, and more beneficiaries are enrolling in Medicare PPOs, the research to date comparing the traditional Medicare program to Medicare Advantage plans still mainly reflects the HMO experience. Only three of the 40 studies that compared traditional Medicare to Medicare Advantage (and two of the five that compared Medicare Advantage plans only) included findings that were specific to Medicare PPOs. Most studies use data for a time period in which HMOs were the main Medicare health plan option. Some of the more recent studies are limited to HMOs to address data constraints or create more homogeneous comparisons. Other studies are not limited to HMOs but do not provide evidence that distinguishes findings by plan type or other plan characteristics. For example, among studies that involved comparisons to traditional Medicare, only two studies analyzed Medicare Advantage plan performance by plan maturity (years of Medicare Advantage experience) and three (two without a traditional Medicare comparison) analyzed the relationship between performance and plan tax status (for profit/nonprofit). Few of the existing studies provide insight into how Medicare Advantage and traditional Medicare perform on quality and access metrics for beneficiaries whose health characteristics suggest that they could have more complex or specialized needs. Only four studies, all based on beneficiary survey data, focused explicitly on subgroups of the Medicare population defined by the authors as high need based on health, functional status, age, and/or income (Elliott et al. 2011, Keenan et al. 2009, Pourat et al. 2006, and Beatty and Dhont 2001). In the first two, using CAHPS data for and 2009 respectively, Keenan et al compared findings for beneficiaries based on self-reported health status, and Elliot et al examined disparities for seven vulnerable subgroups (by socioeconomic status and perceived health status). Using older data from the Medicare Current Beneficiary Survey (1996 and 1994 respectively), Pourat (2006) looked at chronically ill Medicare beneficiaries and Beatty and Dhont (2001) looked at under-65 disabled beneficiaries and elderly beneficiaries with one or more disabilities. Several other studies included health status and health indicators as covariates in their analysis, but did not focus on these subgroups for comparisons of quality and access between traditional Medicare and Medicare Advantage. Almost all studies were either limited to beneficiaries 65 and older (versus younger beneficiaries qualifying by virtue of disability) or did not analyze the experience of under-65 disabled in Medicare Advantage versus traditional Medicare. While some of this reflects the exclusion in this review of studies on specialized health plans, such as Special Needs Plans, research shows that meaningful numbers of beneficiaries who are disabled and under-65 have long been enrolled in Medicare Advantage plans open for general enrollment. 22 The inability to target findings to subgroups with more extensive needs is a major limitation since the studies that exist tend to show that such individuals, at least in survey data, are more likely to report more negatively

15 on their care, regardless of the system they are in, and some studies show this more in Medicare Advantage than traditional Medicare (see Table 5). Available studies include some that are national in scope, comparing Medicare health plans to traditional Medicare; 17 of the 40 studies that have traditional Medicare comparisons fall in this category. Such studies are feasible because CMS has supported the development of data that better support such analysis. In particular, CAHPS data support such comparisons and HEDIS data collection associated with Medicare Advantage provide nationally-representative data that on some metrics can be compared to estimates from claims generated in traditional Medicare. However, the data available to support comparisons on other types of metrics are limited nationally, which means that many analyses are feasible only for subgroups of states or communities that participate in various data collection efforts. For example, diagnostic specific studies involving hospitalizations are only feasible in some states with all payer hospitalization data sets since encounter data that equal claims data have not been collected historically for Medicare Advantage. Further, studies that link care for particular patients across settings or conditions tend not to be feasible in the absence of clinical data that allow for stronger comparisons between Medicare Advantage and traditional Medicare. In general, the lack of clinical data that link patient care across different settings has created a major barrier to developing more robust and meaningful quality measures, as many have noted. For example, the National Quality Forum has identified care coordination, patient centered care and outcomes, and care for patients with Alzheimer s disease and related dementia as three of the top five priorities in terms of future development of measures that matter. 23 Because Medicare Advantage enrollment is voluntary, it is important to control for characteristics of Medicare beneficiaries that may influence their choice of health plan and also the outcomes of their medical care. Roughly speaking, such variables include socio-demographic characteristics (for example, age, sex, race, and ethnicity) and specific health metrics that relate both to overall health status and the severity of comorbidities associated with particular conditions under study. Because practice patterns and socio-demographic characteristics of beneficiaries enrolled in Medicare Advantage may vary geographically, MedPAC also has recommended that comparisons between Medicare Advantage and traditional Medicare be based on beneficiaries in the same geographical payment areas. 24 Such adjustments reflect both the considerable variation in Medicare Advantage enrollment rates across the country and also the differences in individual markets that are likely to influence care both in Medicare Advantage and in traditional Medicare. In Table 2, the 40 studies that compare traditional Medicare to Medicare Advantage are described in terms of their use of locality, socio-demographic, and health status/risk controls, though more detail in the actual techniques used in individual studies are covered in later tables. The aggregate analysis suggests that most studies make some effort to control for confounding sources of variation, such as geography, population and health status, but do so to varying degrees. In many cases, the data available to support such adjustments are limited.

16 ᵟ ᵟ

17 Readmission Rate (n = 3)

18

19
20 ᵟ ᵟ

Medicare Advantage special needs plans
 C h a p t e r14 Medicare Advantage special needs plans R E C O M M E N D A T I O N S 14-1 The Congress should permanently reauthorize institutional special needs plans. COMMISSIONER VOTES: YES 16 NO 0
C h a p t e r14 Medicare Advantage special needs plans R E C O M M E N D A T I O N S 14-1 The Congress should permanently reauthorize institutional special needs plans. COMMISSIONER VOTES: YES 16 NO 0
EQR PROTOCOL 4 VALIDATION OF ENCOUNTER DATA REPORTED BY THE MCO
 OMB Approval No. 0938-0786 EQR PROTOCOL 4 VALIDATION OF ENCOUNTER DATA REPORTED BY THE MCO A Voluntary Protocol for External Quality Review (EQR) Protocol 1: Assessment of Compliance with Medicaid Managed
OMB Approval No. 0938-0786 EQR PROTOCOL 4 VALIDATION OF ENCOUNTER DATA REPORTED BY THE MCO A Voluntary Protocol for External Quality Review (EQR) Protocol 1: Assessment of Compliance with Medicaid Managed
The Promise of Regional Data Aggregation
 The Promise of Regional Data Aggregation Lessons Learned by the Robert Wood Johnson Foundation s National Program Office for Aligning Forces for Quality 1 Background Measuring and reporting the quality
The Promise of Regional Data Aggregation Lessons Learned by the Robert Wood Johnson Foundation s National Program Office for Aligning Forces for Quality 1 Background Measuring and reporting the quality
Medicare Advantage special needs plans
 O n l i n e A p p e n d i x e s14 Medicare Advantage special needs plans 14-A O n l i n e A p p e n d i x Additional data on Medicare Advantage special needs plans and information on quality TABLE 14 A1
O n l i n e A p p e n d i x e s14 Medicare Advantage special needs plans 14-A O n l i n e A p p e n d i x Additional data on Medicare Advantage special needs plans and information on quality TABLE 14 A1
Report to Congress. Improving the Identification of Health Care Disparities in. Medicaid and CHIP
 Report to Congress Improving the Identification of Health Care Disparities in Medicaid and CHIP Sylvia Mathews Burwell Secretary of the Department of Health and Human Services November 2014 TABLE OF CONTENTS
Report to Congress Improving the Identification of Health Care Disparities in Medicaid and CHIP Sylvia Mathews Burwell Secretary of the Department of Health and Human Services November 2014 TABLE OF CONTENTS
Synchronizing Medicare policy across payment models
 Synchronizing Medicare policy across payment models C h a p t e r1 C H A P T E R 1 Synchronizing Medicare policy across payment models Chapter summary In this chapter Historically, Medicare has had two
Synchronizing Medicare policy across payment models C h a p t e r1 C H A P T E R 1 Synchronizing Medicare policy across payment models Chapter summary In this chapter Historically, Medicare has had two
National Findings on Access to Health Care and Service Use for Non-elderly Adults Enrolled in Medicaid
 National Findings on Access to Health Care and Service Use for Non-elderly Adults Enrolled in Medicaid By Sharon K. Long Karen Stockley Elaine Grimm Christine Coyer Urban Institute MACPAC Contractor Report
National Findings on Access to Health Care and Service Use for Non-elderly Adults Enrolled in Medicaid By Sharon K. Long Karen Stockley Elaine Grimm Christine Coyer Urban Institute MACPAC Contractor Report
7/31/2014. Medicare Advantage: Time to Re-examine Your Engagement Strategy. Avalere Health. Eric Hammelman, CFA. Overview
 Medicare Advantage: Time to Re-examine Your Engagement Strategy July 2014 avalerehealth.net Avalere Health Avalere Health delivers research, analysis, insight & strategy to leaders in healthcare policy
Medicare Advantage: Time to Re-examine Your Engagement Strategy July 2014 avalerehealth.net Avalere Health Avalere Health delivers research, analysis, insight & strategy to leaders in healthcare policy
Health Care Reform Update January 2012 MG76120 0212 LILLY USA, LLC. ALL RIGHTS RESERVED
 Health Care Reform Update January 2012 Disclaimer This presentation is for educational purposes only. It is not a complete analysis of the material contained herein. Before taking any action on the issues
Health Care Reform Update January 2012 Disclaimer This presentation is for educational purposes only. It is not a complete analysis of the material contained herein. Before taking any action on the issues
Report on comparing quality among Medicare Advantage plans and between Medicare Advantage and fee-for-service Medicare
 O N L I N E A P P E N D I X E S 6 Report on comparing quality among Medicare Advantage plans and between Medicare Advantage and fee-for-service Medicare 6-A O N L I N E A P P E N D I X Current quality
O N L I N E A P P E N D I X E S 6 Report on comparing quality among Medicare Advantage plans and between Medicare Advantage and fee-for-service Medicare 6-A O N L I N E A P P E N D I X Current quality
Strategies for Success in the CMS Medicare Advantage Star Quality Ratings
 Strategies for Success in the CMS Medicare Advantage Star Quality Ratings The National Pay for Performance Summit February 20, 2013, San Francisco, CA Theresa C. Carnegie Mintz, Levin, Cohn, Ferris, Glovsky
Strategies for Success in the CMS Medicare Advantage Star Quality Ratings The National Pay for Performance Summit February 20, 2013, San Francisco, CA Theresa C. Carnegie Mintz, Levin, Cohn, Ferris, Glovsky
GAO MEDICARE ADVANTAGE. Relationship between Benefit Package Designs and Plans Average Beneficiary Health Status. Report to Congressional Requesters
 GAO United States Government Accountability Office Report to Congressional Requesters April 2010 MEDICARE ADVANTAGE Relationship between Benefit Package Designs and Plans Average Beneficiary Health Status
GAO United States Government Accountability Office Report to Congressional Requesters April 2010 MEDICARE ADVANTAGE Relationship between Benefit Package Designs and Plans Average Beneficiary Health Status
Quality Ratings of Medicare Advantage Plans, 2011
 Issue Brief Quality Ratings of Medicare Advantage Plans, 2011 February 2011 This information was reprinted with permission from the Henry J. Kaiser Family Foundation. The Kaiser Family Foundation is a
Issue Brief Quality Ratings of Medicare Advantage Plans, 2011 February 2011 This information was reprinted with permission from the Henry J. Kaiser Family Foundation. The Kaiser Family Foundation is a
How To Testify On The Medicare Advantage Program
 The Medicare Advantage Program and the Role of Private Health Plans in Serving Medicare Beneficiaries by Karen Ignagni President and CEO America s Health Insurance Plans for the House Ways and Means Committee
The Medicare Advantage Program and the Role of Private Health Plans in Serving Medicare Beneficiaries by Karen Ignagni President and CEO America s Health Insurance Plans for the House Ways and Means Committee
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics
 Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
December 23, 2010. Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services
 December 23, 2010 Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services RE: Prioritized measurement concepts Dear Dr. Blumenthal: Thank you
December 23, 2010 Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services RE: Prioritized measurement concepts Dear Dr. Blumenthal: Thank you
Health Disparities in H.R. 3590 (Merged Senate Bill)
") Health Disparities in H.R. 3590 (Merged Senate Bill) Definitions: Health disparity population is defined in the bill as defined in Section 485E (Sec. 931) Current Law: a population is a health disparity
Health Disparities in H.R. 3590 (Merged Senate Bill) Definitions: Health disparity population is defined in the bill as defined in Section 485E (Sec. 931) Current Law: a population is a health disparity
FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements Proposed Rule
 June 24, 2015 Andrew Slavitt Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Attention: CMS- 1629-P, Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850
June 24, 2015 Andrew Slavitt Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Attention: CMS- 1629-P, Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850
Quality Incentives for Medicare+Choice Plans
 No. 11, August 2002 Quality Incentives for Medicare+Choice Plans Lynn Etheredge Robert Berenson Jack Ebeler 2131 K Street, NW + Suite 500 + Washington, DC 20037 + 202/872-4036 + Fax 202/785-4749 Abstract:
No. 11, August 2002 Quality Incentives for Medicare+Choice Plans Lynn Etheredge Robert Berenson Jack Ebeler 2131 K Street, NW + Suite 500 + Washington, DC 20037 + 202/872-4036 + Fax 202/785-4749 Abstract:
Medicare Advantage 2014 Spotlight: Plan Availability And Premiums
 December 2013 Issue Brief Medicare Advantage 2014 Spotlight: Plan Availability And Premiums Marsha Gold, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Under the current Medicare program, beneficiaries
December 2013 Issue Brief Medicare Advantage 2014 Spotlight: Plan Availability And Premiums Marsha Gold, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Under the current Medicare program, beneficiaries
Assessing the 2015 MA Star ratings
 Intelligence Brief On October 10, 2014, CMS released the Medicare Advantage (MA) Star ratings for 2015. We analyzed CMS s data covering 691 MA plan contracts across the 50 states to determine which types
Intelligence Brief On October 10, 2014, CMS released the Medicare Advantage (MA) Star ratings for 2015. We analyzed CMS s data covering 691 MA plan contracts across the 50 states to determine which types
Medicare Advantage Stars: Are the Grades Fair?
 Douglas Holtz-Eakin Conor Ryan July 16, 2015 Medicare Advantage Stars: Are the Grades Fair? Executive Summary Medicare Advantage (MA) offers seniors a one-stop option for hospital care, outpatient physician
Douglas Holtz-Eakin Conor Ryan July 16, 2015 Medicare Advantage Stars: Are the Grades Fair? Executive Summary Medicare Advantage (MA) offers seniors a one-stop option for hospital care, outpatient physician
Insurance Trends for the Medicare Population, 1991-1999
 Insurance Trends for the Medicare Population, 1991-1999 Lauren A. Murray and Franklin J. Eppig INTRODUCTION The 1990s saw the emergence of managed care into the Medicare marketplace. In the beginning of
Insurance Trends for the Medicare Population, 1991-1999 Lauren A. Murray and Franklin J. Eppig INTRODUCTION The 1990s saw the emergence of managed care into the Medicare marketplace. In the beginning of
How To Understand And Understand The Health Care System In California
 Understanding Accountable Care Organizations (ACOs): What s Worked and What Hasn t in California s 30 Year ACO Experience ACOs are like unicorns mythical creatures. We know what they look like, but no
Understanding Accountable Care Organizations (ACOs): What s Worked and What Hasn t in California s 30 Year ACO Experience ACOs are like unicorns mythical creatures. We know what they look like, but no
Medi-Growth Medicaid, Medicare Poised to Expand
 C H A P T E R 7 Medi-Growth Medicaid, Medicare Poised to Expand More than 100 million Americans rely upon Medicaid and Medicare for insurance coverage. Medicaid, the government s insurance program for
C H A P T E R 7 Medi-Growth Medicaid, Medicare Poised to Expand More than 100 million Americans rely upon Medicaid and Medicare for insurance coverage. Medicaid, the government s insurance program for
Medicare Advantage Star Ratings: Detaching Pay from Performance Douglas Holtz- Eakin, Robert A. Book, & Michael Ramlet May 2012
 Medicare Advantage Star Ratings: Detaching Pay from Performance Douglas Holtz- Eakin, Robert A. Book, & Michael Ramlet May 2012 EXECUTIVE SUMMARY Rewarding quality health plans is an admirable goal for
Medicare Advantage Star Ratings: Detaching Pay from Performance Douglas Holtz- Eakin, Robert A. Book, & Michael Ramlet May 2012 EXECUTIVE SUMMARY Rewarding quality health plans is an admirable goal for
INTRODUCTION. 7 DISCUSSION AND ONGOING RESEARCH.. 29 ACKNOWLEDGEMENTS... 30 ENDNOTES.. 31
 May 2010 Working Paper: Using State Hospital Discharge Data to Compare Readmission Rates in Medicare Advantage and Medicare s Traditional Fee-for-Service Program TABLE OF CONTENTS SUMMARY 1 INTRODUCTION.
May 2010 Working Paper: Using State Hospital Discharge Data to Compare Readmission Rates in Medicare Advantage and Medicare s Traditional Fee-for-Service Program TABLE OF CONTENTS SUMMARY 1 INTRODUCTION.
STAR CROSSED: WHY DOCS TRUMP HEALTH PLANS IN CMS STAR SCORES
 Health and Life Sciences POINT OF VIEW STAR CROSSED: WHY DOCS TRUMP HEALTH PLANS IN CMS STAR SCORES AUTHORS Andrea Jensen, Senior Consultant Martin Graf, Partner An analysis of Medicare Advantage data
Health and Life Sciences POINT OF VIEW STAR CROSSED: WHY DOCS TRUMP HEALTH PLANS IN CMS STAR SCORES AUTHORS Andrea Jensen, Senior Consultant Martin Graf, Partner An analysis of Medicare Advantage data
PROPOSED US MEDICARE RULING FOR USE OF DRUG CLAIMS INFORMATION FOR OUTCOMES RESEARCH, PROGRAM ANALYSIS & REPORTING AND PUBLIC FUNCTIONS
 PROPOSED US MEDICARE RULING FOR USE OF DRUG CLAIMS INFORMATION FOR OUTCOMES RESEARCH, PROGRAM ANALYSIS & REPORTING AND PUBLIC FUNCTIONS The information listed below is Sections B of the proposed ruling
PROPOSED US MEDICARE RULING FOR USE OF DRUG CLAIMS INFORMATION FOR OUTCOMES RESEARCH, PROGRAM ANALYSIS & REPORTING AND PUBLIC FUNCTIONS The information listed below is Sections B of the proposed ruling
Submitted Electronically RE: CMS-1609-P: ISSUE # 1: Solicitation of Comments on Definitions of Terminal Illness and Related Conditions :
 June 20, 2014 Submitted Electronically Ms. Marilyn B. Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services 200 Independence Avenue, SW Washington, DC
June 20, 2014 Submitted Electronically Ms. Marilyn B. Tavenner Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services 200 Independence Avenue, SW Washington, DC
HDE FREE WEBINAR SERIES: BIDDING, RISK ADJUSTMENT, AND STARS. May 3, 2012
 HDE FREE WEBINAR SERIES: BIDDING, RISK ADJUSTMENT, AND STARS May 3, 2012 AGENDA Impact of Star Ratings on 2013 Part C bid Looking ahead: 2014 & beyond How risk scores & QBPs work hand-in-hand to maximize
HDE FREE WEBINAR SERIES: BIDDING, RISK ADJUSTMENT, AND STARS May 3, 2012 AGENDA Impact of Star Ratings on 2013 Part C bid Looking ahead: 2014 & beyond How risk scores & QBPs work hand-in-hand to maximize
October 15, 2010. Re: National Health Care Quality Strategy and Plan. Dear Dr. Wilson,
 October 15, 2010 Dr. Nancy Wilson, R.N., M.D., M.P.H. Senior Advisor to the Director Agency for Healthcare Research and Quality (AHRQ) 540 Gaither Road Room 3216 Rockville, MD 20850 Re: National Health
October 15, 2010 Dr. Nancy Wilson, R.N., M.D., M.P.H. Senior Advisor to the Director Agency for Healthcare Research and Quality (AHRQ) 540 Gaither Road Room 3216 Rockville, MD 20850 Re: National Health
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT
 ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries
 A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries Munevar D 1, Drozd E 1, & Ostrovsky A 2 1 Avalere Health, Inc.
A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries Munevar D 1, Drozd E 1, & Ostrovsky A 2 1 Avalere Health, Inc.
Quality Accountable Care Population Health: The Journey Continues
 Quality Accountable Care Population Health: The Journey Continues Health Insights April 10, 2014 Doug Hastings 2001 Institute of Medicine 2 An Agenda For Crossing The Chasm Between the health care we have
Quality Accountable Care Population Health: The Journey Continues Health Insights April 10, 2014 Doug Hastings 2001 Institute of Medicine 2 An Agenda For Crossing The Chasm Between the health care we have
MEDICARE ADVANTAGE ENROLLMENT AND QUALITY: IMPACT ON PAYMENT REFORM
 MEDICARE ADVANTAGE ENROLLMENT AND QUALITY: IMPACT ON PAYMENT REFORM Timothy D. McBride Leah Kemper Abigail Barker Keith Mueller July 2013 International Health Economics Association Sydney, Australia Washington
MEDICARE ADVANTAGE ENROLLMENT AND QUALITY: IMPACT ON PAYMENT REFORM Timothy D. McBride Leah Kemper Abigail Barker Keith Mueller July 2013 International Health Economics Association Sydney, Australia Washington
Panorama Rooms Thursday 5 March, 2015 14:00. Mr David Abernethy. Health Policy & Government Relations Consultant, Washington, DC
 Panorama Rooms Thursday 5 March, 2015 14:00 Mr David Abernethy Health Policy & Government Relations Consultant, Washington, DC U.S. Private Insurance Solutions in the US Social Insurance System for the
Panorama Rooms Thursday 5 March, 2015 14:00 Mr David Abernethy Health Policy & Government Relations Consultant, Washington, DC U.S. Private Insurance Solutions in the US Social Insurance System for the
Quality Assurance For Medicaid Managed Care. Lessons from a quality-improvement demonstration in three states.
 Outcome Report 248 Quality Assurance For Medicaid Managed Care Lessons from a quality-improvement demonstration in three states. b y Suzanne Fe lt-l is k a nd R ob er t St. P ete r The Quality A ssurance
Outcome Report 248 Quality Assurance For Medicaid Managed Care Lessons from a quality-improvement demonstration in three states. b y Suzanne Fe lt-l is k a nd R ob er t St. P ete r The Quality A ssurance
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
The Medicare Advantage program: Status report
 C h a p t e r13 The Medicare Advantage program: Status report R E C O M M E N D A T I O N S (The Commission reiterates its March 2014 recommendations on improving the bidding rules in the Medicare Advantage
C h a p t e r13 The Medicare Advantage program: Status report R E C O M M E N D A T I O N S (The Commission reiterates its March 2014 recommendations on improving the bidding rules in the Medicare Advantage
Medical Billing Analysis of Medicare
 Analysis of the Variation in Efficiency of Medicare Advantage Plans April 24, 2013 Marsha Gold Maria Cupples Hudson ABSTRACT This paper presents findings from an analysis of public data from 2009 on the
Analysis of the Variation in Efficiency of Medicare Advantage Plans April 24, 2013 Marsha Gold Maria Cupples Hudson ABSTRACT This paper presents findings from an analysis of public data from 2009 on the
Introduction and Invitation for Public Comment
 2 of 22 Introduction and Invitation for Public Comment The Patient-Centered Outcomes Research Institute (PCORI) is an independent, non-profit health research organization. Its mission is to fund research
2 of 22 Introduction and Invitation for Public Comment The Patient-Centered Outcomes Research Institute (PCORI) is an independent, non-profit health research organization. Its mission is to fund research
Profile of Rural Health Insurance Coverage
 Profile of Rural Health Insurance Coverage A Chartbook R H R C Rural Health Research & Policy Centers Funded by the Federal Office of Rural Health Policy www.ruralhealthresearch.org UNIVERSITY OF SOUTHERN
Profile of Rural Health Insurance Coverage A Chartbook R H R C Rural Health Research & Policy Centers Funded by the Federal Office of Rural Health Policy www.ruralhealthresearch.org UNIVERSITY OF SOUTHERN
INSIGHT on the Issues
 INSIGHT on the Issues AARP Public Policy Institute Medicare Beneficiaries Out-of-Pocket for Health Care Claire Noel-Miller, PhD AARP Public Policy Institute Medicare beneficiaries spent a median of $3,138
INSIGHT on the Issues AARP Public Policy Institute Medicare Beneficiaries Out-of-Pocket for Health Care Claire Noel-Miller, PhD AARP Public Policy Institute Medicare beneficiaries spent a median of $3,138
Response to Serving the Medi Cal SPD Population in Alameda County
 Expanding Health Coverage and Increasing Access to High Quality Care Response to Serving the Medi Cal SPD Population in Alameda County As the State has acknowledged in the 1115 waiver concept paper, the
Expanding Health Coverage and Increasing Access to High Quality Care Response to Serving the Medi Cal SPD Population in Alameda County As the State has acknowledged in the 1115 waiver concept paper, the
MEDICARE SUPPLEMENTAL COVERAGE. Medigap and Other Factors Are Associated with Higher Estimated Health Care Expenditures
 United States Government Accountability Office Report to the Ranking Member, Committee on Finance, U.S. Senate September 2013 MEDICARE SUPPLEMENTAL COVERAGE Medigap and Other Factors Are Associated with
United States Government Accountability Office Report to the Ranking Member, Committee on Finance, U.S. Senate September 2013 MEDICARE SUPPLEMENTAL COVERAGE Medigap and Other Factors Are Associated with
Racial and ethnic health disparities continue
 From Families USA Minority Health Initiatives May 2010 Moving toward Health Equity: Health Reform Creates a Foundation for Eliminating Disparities Racial and ethnic health disparities continue to persist
From Families USA Minority Health Initiatives May 2010 Moving toward Health Equity: Health Reform Creates a Foundation for Eliminating Disparities Racial and ethnic health disparities continue to persist
Medicare Premium Support: Lessons from Medicare Plans and Plan Competition Marsha Gold, ScD, Senior Fellow
 Medicare Premium Support: Lessons from Medicare Plans and Plan Competition Marsha Gold, ScD, Senior Fellow Presentation to the Annual Research Meeting, AcademyHealth, Orlando Florida, June 26, 2012 Review
Medicare Premium Support: Lessons from Medicare Plans and Plan Competition Marsha Gold, ScD, Senior Fellow Presentation to the Annual Research Meeting, AcademyHealth, Orlando Florida, June 26, 2012 Review
SYNOPSIS OF HEALTH CARE QUALITY MANAGEMENT SYSTEMS
 SYNOPSIS OF HEALTH CARE QUALITY MANAGEMENT SYSTEMS Administration for Community Living CBO Learning Collaborative Webinar Presenter: Sharon R. Williams, Health Care Consultant April 2, 2014 2 QUALITY ASSURANCE:
SYNOPSIS OF HEALTH CARE QUALITY MANAGEMENT SYSTEMS Administration for Community Living CBO Learning Collaborative Webinar Presenter: Sharon R. Williams, Health Care Consultant April 2, 2014 2 QUALITY ASSURANCE:
Historical Trends in Medicare s Private Plans
 Historical Trends in Medicare s Private Plans By: Marsha Gold, Sc.D. Senior Fellow April 28, 2005 For presentation to the National Health Policy Forum Session on Understanding Medicare Advantage Bidding
Historical Trends in Medicare s Private Plans By: Marsha Gold, Sc.D. Senior Fellow April 28, 2005 For presentation to the National Health Policy Forum Session on Understanding Medicare Advantage Bidding
Health Care Financing: ACC/ ACO s, beyond the hype hope. Brian Seppi, MD, President, Washington State Medical Assn.
 : ACC/ ACO s, beyond the hype hope Brian Seppi, MD, President, Washington State Medical Assn. Washington State Medical Association Health Care Financing Our vision Make Washington the best place to practice
: ACC/ ACO s, beyond the hype hope Brian Seppi, MD, President, Washington State Medical Assn. Washington State Medical Association Health Care Financing Our vision Make Washington the best place to practice
CURBING MEDICARE ADVANTAGE OVERPAYMENTS COULD BENEFIT MILLIONS OF LOW-INCOME AND MINORITY AMERICANS by January Angeles and Edwin Park
 820 First Street NE, Suite 510 Washington, DC 20002 Tel: 202-408-1080 Fax: 202-408-1056 center@cbpp.org www.cbpp.org February 19, 2009 CURBING MEDICARE ADVANTAGE OVERPAYMENTS COULD BENEFIT MILLIONS OF
820 First Street NE, Suite 510 Washington, DC 20002 Tel: 202-408-1080 Fax: 202-408-1056 center@cbpp.org www.cbpp.org February 19, 2009 CURBING MEDICARE ADVANTAGE OVERPAYMENTS COULD BENEFIT MILLIONS OF
Health Care Utilization and Costs of Full-Pay and Subsidized Enrollees in the Florida KidCare Program: MediKids
 Health Care Utilization and Costs of Full-Pay and Subsidized Enrollees in the Florida KidCare Program: MediKids Prepared for the Florida Healthy Kids Corporation Prepared by Jill Boylston Herndon, Ph.D.
Health Care Utilization and Costs of Full-Pay and Subsidized Enrollees in the Florida KidCare Program: MediKids Prepared for the Florida Healthy Kids Corporation Prepared by Jill Boylston Herndon, Ph.D.
Chartpack. August 2008
 Chartpack Examining Sources of Coverage Among Medicare Beneficiaries: Supplemental Insurance, Medicare Advantage, and Prescription Drug Coverage Findings from the Medicare Current Beneficiary Survey, 2006
Chartpack Examining Sources of Coverage Among Medicare Beneficiaries: Supplemental Insurance, Medicare Advantage, and Prescription Drug Coverage Findings from the Medicare Current Beneficiary Survey, 2006
Committee on Ways and Means Subcommittee on Health U.S. House of Representatives. Hearing on Examining Traditional Medicare s Benefit Design
 Committee on Ways and Means Subcommittee on Health U.S. House of Representatives Hearing on Examining Traditional Medicare s Benefit Design February 26, 2013 Statement of Cori E. Uccello, MAAA, FSA, MPP
Committee on Ways and Means Subcommittee on Health U.S. House of Representatives Hearing on Examining Traditional Medicare s Benefit Design February 26, 2013 Statement of Cori E. Uccello, MAAA, FSA, MPP
Supreme Court upholds the Affordable Care Act in its entirety:
 Supreme Court upholds the Affordable Care Act in its entirety: What does this mean for Seniors? The Supreme Court s decision to uphold the Affordable Care Act (ACA) in its entirety is a huge victory for
Supreme Court upholds the Affordable Care Act in its entirety: What does this mean for Seniors? The Supreme Court s decision to uphold the Affordable Care Act (ACA) in its entirety is a huge victory for
Although the Medicare+Choice legislation
 MONITORING MEDICARE+CHOICE OPERATIONALInsights October 2003, Number 12 Medicare s Experience with PPOs and Private Fee-for-Service Plans Although the Medicare+Choice legislation calls for a variety of
MONITORING MEDICARE+CHOICE OPERATIONALInsights October 2003, Number 12 Medicare s Experience with PPOs and Private Fee-for-Service Plans Although the Medicare+Choice legislation calls for a variety of
HEDIS/CAHPS 101. August 13, 2012 Minnesota Measurement and Reporting Workgroup
 HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
2014: Volume 4, Number 1. A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics
 2014: Volume 4, Number 1 A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics Medicare Post-Acute Care Episodes and Payment Bundling Melissa Morley,¹
2014: Volume 4, Number 1 A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics Medicare Post-Acute Care Episodes and Payment Bundling Melissa Morley,¹
Analysis of Care Coordination Outcomes /
 Analysis of Care Coordination Outcomes / A Comparison of the Mercy Care Plan Population to Nationwide Dual-Eligible Medicare Beneficiaries July 2012 Prepared by: Varnee Murugan Ed Drozd Kevin Dietz Aetna
Analysis of Care Coordination Outcomes / A Comparison of the Mercy Care Plan Population to Nationwide Dual-Eligible Medicare Beneficiaries July 2012 Prepared by: Varnee Murugan Ed Drozd Kevin Dietz Aetna
PRESCRIPTION DRUG COSTS FOR MEDICARE BENEFICIARIES: COVERAGE AND HEALTH STATUS MATTER
 PRESCRIPTION DRUG COSTS FOR MEDICARE BENEFICIARIES: COVERAGE AND HEALTH STATUS MATTER Bruce Stuart, Dennis Shea, and Becky Briesacher January 2000 ISSUE BRIEF How many Medicare beneficiaries lack prescription
PRESCRIPTION DRUG COSTS FOR MEDICARE BENEFICIARIES: COVERAGE AND HEALTH STATUS MATTER Bruce Stuart, Dennis Shea, and Becky Briesacher January 2000 ISSUE BRIEF How many Medicare beneficiaries lack prescription
All Payer Claims Databases: Options for Consideration Feasibility Study Final Report Presentation to the Alaska Health Care Commission March 7, 2013
 All Payer Claims Databases: Options for Consideration Feasibility Study Final Report Presentation to the Alaska Health Care Commission March 7, 2013 Overview of the Presentation Project summary Health
All Payer Claims Databases: Options for Consideration Feasibility Study Final Report Presentation to the Alaska Health Care Commission March 7, 2013 Overview of the Presentation Project summary Health
Measuring and Assigning Accountability for Healthcare Spending
 Measuring and Assigning Accountability for Healthcare Spending Fair and Effective Ways to Analyze the Drivers of Healthcare Costs and Transition to Value-Based Payment Harold D. Miller CONTENTS EXECUTIVE
Measuring and Assigning Accountability for Healthcare Spending Fair and Effective Ways to Analyze the Drivers of Healthcare Costs and Transition to Value-Based Payment Harold D. Miller CONTENTS EXECUTIVE
Healthcare Facilities Accreditation Program
 1 Healthcare Facilities 2 Moving Accreditation from Standards to Quality and Safety Based Lessons from the Healthcare Facilities Richard Snow DO, MPH Healthcare Facilities Advisory Board Medical Director
1 Healthcare Facilities 2 Moving Accreditation from Standards to Quality and Safety Based Lessons from the Healthcare Facilities Richard Snow DO, MPH Healthcare Facilities Advisory Board Medical Director
Performance Evaluation Report Kaiser Prepaid Health Plan (KP Cal, LLC) Marin and Sonoma Counties July 1, 2009 June 30, 2010
 Marin and Sonoma Counties July 1, 2009 June 30, 2010") Performance Evaluation Report Kaiser Prepaid Health Plan (KP Cal, LLC) Marin and Sonoma Counties July 1, 2009 June 30, 2010 Medi-Cal Managed Care Division California Department of Health Care Services
Performance Evaluation Report Kaiser Prepaid Health Plan (KP Cal, LLC) Marin and Sonoma Counties July 1, 2009 June 30, 2010 Medi-Cal Managed Care Division California Department of Health Care Services
STARs Tutorial Medicare Advantage Plan Star Ratings and Bonus Payments in 2012 A Tutorial for Utilizing SETMA s Deployment of the STARS MA Program
 STARs Tutorial Medicare Advantage Plan Star Ratings and Bonus Payments in 2012 A Tutorial for Utilizing SETMA s Deployment of the STARS MA Program Increasingly, health plans and particularly Federal programs
STARs Tutorial Medicare Advantage Plan Star Ratings and Bonus Payments in 2012 A Tutorial for Utilizing SETMA s Deployment of the STARS MA Program Increasingly, health plans and particularly Federal programs
While Congress is focusing on health insurance for low-income children, this survey highlights the vulnerability of low-income adults as well.
 Insurance Matters For Low-Income Adults: Results From A Five-State Survey While Congress is focusing on health insurance for low-income children, this survey highlights the vulnerability of low-income
Insurance Matters For Low-Income Adults: Results From A Five-State Survey While Congress is focusing on health insurance for low-income children, this survey highlights the vulnerability of low-income
Health Plan Quality Monitoring
 Health Plan Quality Monitoring Andrew L. Naugle, MBA Patty Jones, RN MBA BACKGROUND Section 1311(b) of the Patient Protection and Affordable Care Act of 2010 (ACA) detailed the intent of the federal government
Health Plan Quality Monitoring Andrew L. Naugle, MBA Patty Jones, RN MBA BACKGROUND Section 1311(b) of the Patient Protection and Affordable Care Act of 2010 (ACA) detailed the intent of the federal government
EARLY INDICATIONS OF CHANGES TO 2014 MAO PAYMENT METHODOLOGY
 Early indications of changes to the 2015 medicare advantage payment methodology and the potential effect on medicare advantage organizations and beneficiaries February 6, 2014 GLENN GIESE FSA, MAAA KELLY
Early indications of changes to the 2015 medicare advantage payment methodology and the potential effect on medicare advantage organizations and beneficiaries February 6, 2014 GLENN GIESE FSA, MAAA KELLY
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Colorado Choice Health Plans
 Quality Overview Colorado Choice Health Plans Accreditation Exchange Product Accrediting Organization: Accreditation Status: URAC Health Plan Accreditation (Marketplace HMO) Provisional Accreditation Commercial
Quality Overview Colorado Choice Health Plans Accreditation Exchange Product Accrediting Organization: Accreditation Status: URAC Health Plan Accreditation (Marketplace HMO) Provisional Accreditation Commercial
Medicare- Medicaid Enrollee State Profile
 Medicare- Medicaid Enrollee State Profile North Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6 Spending...
Medicare- Medicaid Enrollee State Profile North Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6 Spending...
Disclaimer HEALTHCARE REFORM 8/18/2015. CS EYE - Compliance Specialists, Inc. Compliance, Medicare Advantage and Accountable Care Organizations
 HEALTHCARE REFORM Compliance, Medicare Advantage and Accountable Care Organizations Jon Weeding President CS EYE CS EYE - Compliance Specialists, Inc. Outsource compliance and medical billing Assisted
HEALTHCARE REFORM Compliance, Medicare Advantage and Accountable Care Organizations Jon Weeding President CS EYE CS EYE - Compliance Specialists, Inc. Outsource compliance and medical billing Assisted
Introduction. What is Transparency in Health Care?
 Introduction Transparency is a vital component of an efficient and effective health care system. As concerns about the cost and quality of health care in the United States continue to grow and large employers
Introduction Transparency is a vital component of an efficient and effective health care system. As concerns about the cost and quality of health care in the United States continue to grow and large employers
Affordable Care Act at 3: Strengthening Medicare
 Affordable Care Act at 3: Strengthening Medicare ISSUE BRIEF Fifth in a series May 22, 2013 Kyle Brown Senior Health Policy Analyst 789 Sherman St. Suite 300 Denver, CO 80203 www.cclponline.org 303-573-5669
Affordable Care Act at 3: Strengthening Medicare ISSUE BRIEF Fifth in a series May 22, 2013 Kyle Brown Senior Health Policy Analyst 789 Sherman St. Suite 300 Denver, CO 80203 www.cclponline.org 303-573-5669
Data Shows Reduction in Medicare Hospital Readmission Rates During 2012
 Medicare & Medicaid Research Review 2013: Volume 3, Number 2 A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics Data Shows Reduction in Medicare
Medicare & Medicaid Research Review 2013: Volume 3, Number 2 A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics Data Shows Reduction in Medicare
Care needs for dual-eligible beneficiaries
 C h a p t e r6 Care needs for dual-eligible beneficiaries C H A P T E R 6 Care needs for dual-eligible beneficiaries Chapter summary In this chapter Dual-eligible beneficiaries are eligible for both Medicare
C h a p t e r6 Care needs for dual-eligible beneficiaries C H A P T E R 6 Care needs for dual-eligible beneficiaries Chapter summary In this chapter Dual-eligible beneficiaries are eligible for both Medicare
The U.S. Congress created the Medicare+Choice (M+C) program
 program") April 2002 Issue Brief Medicare Managed Care: Medicare+Choice at Five Years Colleen L. Barry* and Janet Kline** The Commonwealth Fund is a private foundation supporting independent research on health and
April 2002 Issue Brief Medicare Managed Care: Medicare+Choice at Five Years Colleen L. Barry* and Janet Kline** The Commonwealth Fund is a private foundation supporting independent research on health and
An Update on Medicare Parts C & D Performance Measures
 An Update on Medicare Parts C & D Performance Measures CMS Spring Conference April 12 & 13, 2011 Liz Goldstein, Ph.D. Director, Division of Consumer Assessment & Plan Performance Vikki Oates, M.A.S Director,
An Update on Medicare Parts C & D Performance Measures CMS Spring Conference April 12 & 13, 2011 Liz Goldstein, Ph.D. Director, Division of Consumer Assessment & Plan Performance Vikki Oates, M.A.S Director,
HOSPITAL VALUE- BASED PURCHASING. Initial Results Show Modest Effects on Medicare Payments and No Apparent Change in Quality-of- Care Trends
 United States Government Accountability Office Report to Congressional Committees October 2015 HOSPITAL VALUE- BASED PURCHASING Initial Results Show Modest Effects on Medicare Payments and No Apparent
United States Government Accountability Office Report to Congressional Committees October 2015 HOSPITAL VALUE- BASED PURCHASING Initial Results Show Modest Effects on Medicare Payments and No Apparent
2019 Healthcare That Works for All
 2019 Healthcare That Works for All This paper is one of a series describing what a decade of successful change in healthcare could look like in 2019. Each paper focuses on one aspect of healthcare. To
2019 Healthcare That Works for All This paper is one of a series describing what a decade of successful change in healthcare could look like in 2019. Each paper focuses on one aspect of healthcare. To
Accountable Care Organizations: An old idea with new potential. Stephen E. Whitney, MD, MBA Testimony to Senate State Affairs September 22, 2010
 Accountable Care Organizations: An old idea with new potential Stephen E. Whitney, MD, MBA Testimony to Senate State Affairs September 22, 2010 Impetus for ACO Formation Increased health care cost From
Accountable Care Organizations: An old idea with new potential Stephen E. Whitney, MD, MBA Testimony to Senate State Affairs September 22, 2010 Impetus for ACO Formation Increased health care cost From
What Providers Need To Know Before Adopting Bundling Payments
 What Providers Need To Know Before Adopting Bundling Payments Dan Mirakhor Master of Health Administration University of Southern California Dan Mirakhor is a Master of Health Administration student at
What Providers Need To Know Before Adopting Bundling Payments Dan Mirakhor Master of Health Administration University of Southern California Dan Mirakhor is a Master of Health Administration student at
Data Concerns in Out-of-Pocket Spending Comparisons between Medicare and Private Insurance. Cristina Boccuti and Marilyn Moon
 Data Concerns in Out-of-Pocket Spending Comparisons between Medicare and Private Insurance Cristina Boccuti and Marilyn Moon As Medicare beneficiaries double over the next 30 years, controlling per enrollee
Data Concerns in Out-of-Pocket Spending Comparisons between Medicare and Private Insurance Cristina Boccuti and Marilyn Moon As Medicare beneficiaries double over the next 30 years, controlling per enrollee
2015 HEDIS/CAHPS Effectiveness of Care Report for 2014 Service Measures Oregon, Idaho and Montana Commercial Business
 2015 HEDIS/CAHPS Effectiveness of Care Report for 2014 Service Measures Oregon, Idaho and Montana Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely
2015 HEDIS/CAHPS Effectiveness of Care Report for 2014 Service Measures Oregon, Idaho and Montana Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely
On the Road to Meaningful Use of EHRs:
 On the Road to Meaningful Use of EHRs: A Survey of California Physicians June 2012 On the Road to Meaningful Use of EHRs: A Survey of California Physicians Prepared for California HealthCare Foundation
On the Road to Meaningful Use of EHRs: A Survey of California Physicians June 2012 On the Road to Meaningful Use of EHRs: A Survey of California Physicians Prepared for California HealthCare Foundation
Sharp HealthCare ACO. Pioneer Introduction to the FSSB November 8, 2012
 Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
A Home Health Co-Payment: Affected Beneficiaries and Potential Implications
 A Home Health Co-Payment: Affected Beneficiaries and Potential Implications May 2, 203 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Executive Summary 38
A Home Health Co-Payment: Affected Beneficiaries and Potential Implications May 2, 203 Avalere Health LLC Avalere Health LLC The intersection of business strategy and public policy Executive Summary 38
Policy Forum. Understanding the Effects of Medicare Prescription Drug Insurance. About the Authors. By Robert Kaestner and Kelsey McCoy
 Policy Forum Volume 23, Issue 1 October 2010 Understanding the Effects of Medicare Prescription Drug Insurance By Robert Kaestner and Kelsey McCoy The Medicare Modernization The size and potential significance
Policy Forum Volume 23, Issue 1 October 2010 Understanding the Effects of Medicare Prescription Drug Insurance By Robert Kaestner and Kelsey McCoy The Medicare Modernization The size and potential significance
Premier ACO Collaboratives Driving to a Patient-Centered Health System
 Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
November 22, 2010. RE: File code CMS-1345-NC. Dear Dr. Berwick:
 601 New Jersey Avenue, N.W. Suite 9000 Washington, DC 20001 202-220-3700 Fax: 202-220-3759 www.medpac.gov. Glenn M. Hackbarth, J.D., Chairman Robert A. Berenson, M.D., F.A.C.P., Vice Chairman Mark E. Miller,
601 New Jersey Avenue, N.W. Suite 9000 Washington, DC 20001 202-220-3700 Fax: 202-220-3759 www.medpac.gov. Glenn M. Hackbarth, J.D., Chairman Robert A. Berenson, M.D., F.A.C.P., Vice Chairman Mark E. Miller,
HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT
 HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT CONTENTS A BACKGROUND AND PURPOSE OF THE MID-YEAR QUALITY AND RESOURCE USE REPORTS... 1 B EXHIBITS INCLUDED IN THE MID-YEAR QUALITY AND RESOURCE USE
HOW TO UNDERSTAND YOUR QUALITY AND RESOURCE USE REPORT CONTENTS A BACKGROUND AND PURPOSE OF THE MID-YEAR QUALITY AND RESOURCE USE REPORTS... 1 B EXHIBITS INCLUDED IN THE MID-YEAR QUALITY AND RESOURCE USE
1 Kaiser Commission on Medicaid and the Uninsured, Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2012 and 2013, October
 Managed Care in Oregon This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program start
Managed Care in Oregon This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program start
Managed Medical Care for Persons with Disabilities and Behavioral Health Needs
 January 2015 RDA Report 6.56 Olympia, Washington Managed Medical Care for Persons with Disabilities and Behavioral Health Needs Preliminary Findings from Washington State David Mancuso, PhD and Barbara
January 2015 RDA Report 6.56 Olympia, Washington Managed Medical Care for Persons with Disabilities and Behavioral Health Needs Preliminary Findings from Washington State David Mancuso, PhD and Barbara
Value Based Care and Healthcare Reform
 Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Medicare- Medicaid Enrollee State Profile
 Medicare- Medicaid Enrollee State Profile Montana Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6
Medicare- Medicaid Enrollee State Profile Montana Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6
Medicare Advantage: The Basics
 : The Basics Gretchen Jacobson, Ph.D. Associate Director, Program on Policy Kaiser Family Foundation Monday, June 10, 2013 Exhibit 1 More than one quarter of beneficiaries are enrolled in a private plan
: The Basics Gretchen Jacobson, Ph.D. Associate Director, Program on Policy Kaiser Family Foundation Monday, June 10, 2013 Exhibit 1 More than one quarter of beneficiaries are enrolled in a private plan
Medicare Advantage Payment Refresher
 Medicare Advantage Payment Refresher PRESENTING: Adam Zavadil, Director of Market Strategy & Analysis Stephen Cox, Manager of Business Improvement Programs May 13, 2015 1 Agenda Medicare Advantage (MA),
Medicare Advantage Payment Refresher PRESENTING: Adam Zavadil, Director of Market Strategy & Analysis Stephen Cox, Manager of Business Improvement Programs May 13, 2015 1 Agenda Medicare Advantage (MA),
Qualified Health Plan: Selection Process and Contracting Plan Management Advisory Group Discussion. February 19, 2013
 Qualified Health Plan: Selection Process and Contracting Plan Management Advisory Group Discussion February 19, 2013 HMO and PPO Options / Number and Type of Plans Geographic Coverage by Health Plan: Stimulating
Qualified Health Plan: Selection Process and Contracting Plan Management Advisory Group Discussion February 19, 2013 HMO and PPO Options / Number and Type of Plans Geographic Coverage by Health Plan: Stimulating
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare