Improving Surgical Wound Classification in the Operating Room April 26, 2011
|
|
|
- Roy Wilcox
- 7 years ago
- Views:
Transcription
1 Improving Surgical Wound Classification in the Operating Room April 26, 2011 Aline Van RN, NSQIP SCNR Kaiser Permanente, Modesto Hemant Keny, M.D Christina Solis RN, NSQIP SCNR Kaiser Permanente, San Jose

2 What is NSQIP National Surgical Quality Improvement Program Report risk adjusted surgical outcomes Provides benchmark for hospitals to compare surgical outcomes data Provides us an opportunity to assess and evaluate how well we are providing surgical care Identify area for improvement in care practices and systems

3 Importance of Wound Class SB A required part of the risk adjustment score for selected Colon, Orthopedic and Cardiac procedures with s/p deep & organ space surgical site infections. Evaluate surgical infection risk Accurate documentation NSQIP uses to risk adjusted outcomes

4 Wound Class & Risks Class 1- Clean wound has a 1% to 5% of developing SSI or deep tissue infection. Class 2- Clean/Contaminated has 4%-10% risk. Class 3- Contaminated has > 10% risk of getting infection even w/ prophylactic antibiotics. Class 4- Dirty cases increase to 27% risk of SSI. Devaney, Lynn, et al. Improving Surgical Wound Classification-Why it Matters, AORN. (August 2004). 80,(2) pg

5 Test your Wound Classification Knowledge Let s take a quiz-see (Test questions taken from The American College of Surgeons) 1.
 1.")
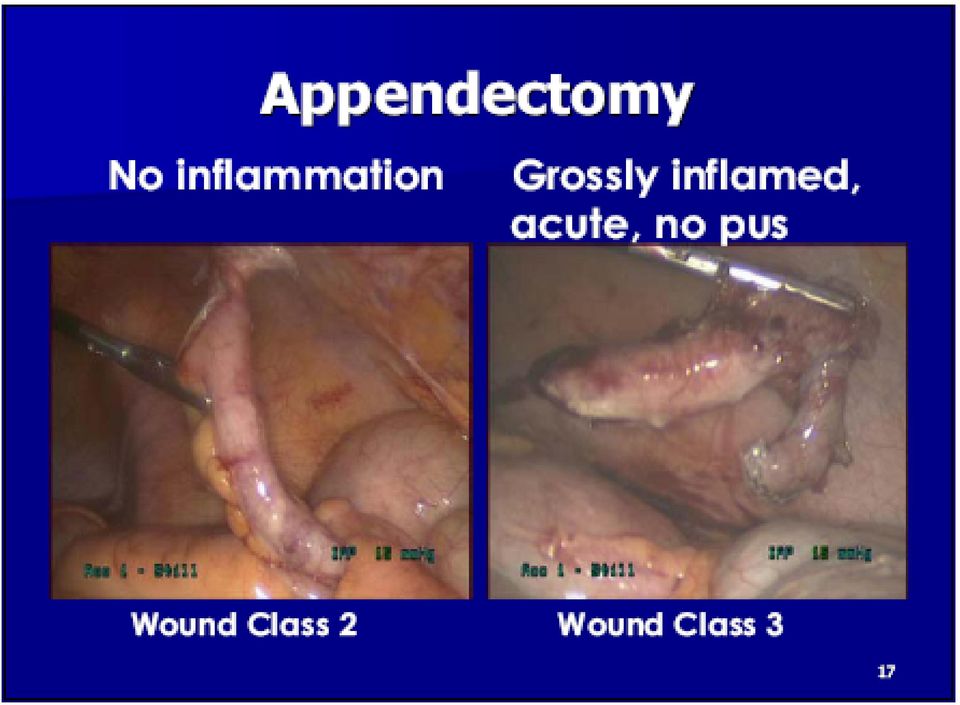
6 General Surgery Case A patient underwent a laparoscopic appendectomy. The preoperative CT scan reported the appendix contained a fecalith. There was no mention of infection, rupture, or inflammation in the operative report. What wound classification should be reported? 1. Clean 2. Clean/Contaminated 3. Contaminated 4. Dirty/Infected

7 Quiz Answer B-wound class 2 There was no documentation of rupture, inflammation, or purulence, a wound class 2 would be assigned. Appy s are always a wound 2 as a baseline.

8 I am not sure of the correct wound class Voice of the Customer Staff s Perspective I ve never been trained Why does it even matter? We rarely do the debriefingtoo much to do We never talk about the wound class-never have

9 Wound Classification 1- Clean: Uninfected wound, no inflammation, closed, and if necessary, w/ closed drainage. Non-penetrating (blunt) trauma. 2- Clean/Contaminated: Respiratory, alimentary, genital, or urinary tract ENTERING ORGANS w/o Major break in technique 3- Contaminated: Open, acute wounds, breaks in technique or gross spillage, necrotic w/o drainage. Key words: ACUTE WOUND & INFLAMMATION, NONPURULENT 4- Dirty/Infected: Old traumatic wound w/ retained devitalized tissue, and existing infection wounds. Wet gangrene. Key words: PERFORATED, ABSCESS, RUPTURE,INFECTED, PURULENT, SUPPURATIVE

10 What are we trying to Improve? Baseline Performance 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% GOAL 90% SURGICAL WOUND CLASSIFICATION KAISER SAN JOSE MEDICAL CENTER 2009 AVERAGE 69% DATE RANGE

11 80/20 Rule 100 Pareto's Chart- Misclassified Wound Class Modesto: May June 2009 Misclassified Wound Class (%) General Surgery Orthopedics GYN Urology Vascular HNS Misclassified % Cummulative %

12 Baseline- General Surgery General Surgery Wound Classification Modesto 40 Misclassified % Acute Lap. Chole Acute Appendectomy Hernias Colon Misclassified %

13 Most Common Misused Class 2- Clean/Contaminated Specifically used when ENTERING ORGANS ENTERING & INVOLVING TRACTS only IS NOT: A default wound class when there s uncertainty A gray area between class 1 and class 3 wound

14
15 Goal/ AIM Statement To achieve 90% or higher in correct wound classification by (You pick your target date).

16 PI Strategy Pareto s Rule (80/20) 3S : Simple + System = Sustainable Efficiency Leverage technology Lean Process: people steps = variations involved Staff Motivation & Engagement Where can I start that will make the most impact in our performance?

17 Small Test of Change Goal: To achieve 90% or higher in correct wound classification Jan A P S D Cycle 4: Dec- Jan - concurrent audit and real time education Wound class decision tree implementation Cycle 3: Nov.- Dec. Re-enforce education to General Surgeons in staff meeting and via & meetings to all other subspecialty. Change Concept: Utilize NSQIP and CDC Wound Classification Guidelines 17 A P S D Cycle 2: Sept.- Oct.: spread education to all OR nurses of guidelines and encouraged RN to confirm w/ Surgeon of correct wound class during debriefing process. Physicians teaching Cycle 1: July-Aug Weeks 1-4: Tracking wound classification documentation from RN champion after education of guidelines. Audits were done from surgical logs by SCNR for compliance

18 PDSA in 2010 Goal: To achieve 90% or higher in correct wound classification by January Cycle 8: Spread improvement to Manteca A P S D Cycle 7: Sustainable Plan: Auditing Education Spread improvement Change Concept: Utilize NSQIP and CDC Wound Classification Guidelines A P S D Cycle 6: Cycle 5: Update performance, data definition teaching/re-enforcing. Start Using crystal reports for audit. RN Champion does 100% auditing Celebrate! Treat staff for lunch. Goal reached! 18

19 PDSA Action Plan Annotated Run Chart WOUND CLASSIFICATION GENERAL AND VASCULAR SURGERY SUSTAINABILITY PHASE 2010 PERCENTAGE CORRECT 100% 90% 80% 70% 60% 50% Wound class added to Debriefing 1/25-2/1 Education to Gen/Vas Surgeons 2/2-2/9 2/10-2/17 OR/ASU Managers discussed with Staff 2/18-2/25 2/26-3/5 Wound Class Posters/decsion trees up in OR and ASU rooms 3/6-3/13 3/14-3/21 3/22-3/29 Education to all OR Nurses 3/30-4/6 4/7-4/14 Education to Gen/Vas surgeons 4/15-4/22 Spread to all Surgical Services 4/23-4/30 Newsletter 5/1-5/8 Wound Debriefing Audits 5/9-5/16 5/17-5/24

20 Process Change in the OR Efficiency in Process

21 How will we reach our goal? Goal To achieve 90% or higher in correct wound classification by Jan Modesto OR. Drivers Communication Education Previous Process New Process Previous State Goal Wound class is assigned based on : conversations during surgery. Requested equipment Dx. On consent or HC surgery case/log info. Validation of wound class during debriefing. Practice based on past experience & knowledge. Inconsistent knowledge of wound class definition To utilize standardized wound class definition. To have continuous support and feedback to surgeons and OR staff No communication Between RN & surgeons
22 Modesto Performance
23 Manteca Performance
24 Tools Created Wound Class Poster Wound Class Decision Tree Wound Class added to Debriefing Wound Class Newsletter Wound Class Quiz and Educational ppt Wound Class/Debriefing Audit Tool
25 Wound Classification 1- Clean: Uninfected wound, no inflammation, closed, and if necessary, w/ closed drainage. Non-penetrating (blunt) trauma. 2- Clean/Contaminated: Respiratory, alimentary, genital, or urinary tract ENTERING ORGANS w/o Major break in technique 3- Contaminated: Open, acute wounds, breaks in technique or gross spillage, necrotic w/o drainage. Key words: ACUTE WOUND & INFLAMMATION, NONPURULENT 4- Dirty/Infected: Old traumatic wound w/ retained devitalized tissue, and existing infection wounds. Wet gangrene. Key words: PERFORATED, ABSCESS, RUPTURE,INFECTED, PURULENT, SUPPURATIVE
26 Things that does not change wound classification: Chronic inflammation Closed Drains Cyst drainage Colostomy ** Document the highest wound class if there are multiple operating sites involved w/ multiple wound classes. Document Class 2- Clean/ Contaminated No Yes Major breaks in sterile field? Acute, Nonpurulent inflammation? Open wound? GI spillage? Yes WOUND CLASSIFICATION DECISION TREE CVA NSQIP Does the procedure involving the GI tract, Respiratory tract, Urinary tract, or Genital tract? No Does operating site has old wound w/ dead tissue? Gangrene? Active Infection? Yes No Major breaks in sterile field? Acute, Nonpurulent inflammation? Open wound? GI spillage? No Yes - Pus/purulence? - Abscess? - Peritonitis? - Perforated Viscera? - Retained devitalized tissue? (active infection) Document: Class 3 Contaminated No - Pus/purulence? - Abscess? - Peritonitis? - Perforated Viscera? - Retained devitalized tissue? (active infection) No Document Class 4 Dirty/Infected Document Class 3 Contaminated Yes Yes Document Class 1- Clean Document Class 4 Dirty/Infected Document Class 4 Dirty/Infected CVA NSQIP - Aline Van, SCNR
27 Circulator Following final count: Is the team ready to debrief? Surgeon Verify Procedure, Diagnosis Wound Class Specimen (s) review (Path Sheet & Labels including history) Identify equipment issues Circulator Scrub Anesthesia With the Surgeon review (Path Sheet & Labels including history) With the Scrub indicate final count correct (sharp, sponge & instrument) With the RN Circulator indicate final count correct (sharp, sponge & instrument) VTE prophylaxis Return to Room Time Anesthesia/RN HRST SAFETY DEBRIEFING- HRST Approved
28 Team Communication
29 Tracking Performance Leverage on electronic surgical reports Audit team communication Was the Debriefing discussed? Was wound class discussed as part of the debriefing?
30 Sustainability Process Annual Staff competency training Orientation process Concurrent daily audits and real-time education Continuous physician teaching and re-enforce validation during debriefing process.
31 PI Overview Collect baseline data & identify areas of improvement (start small). Recruit RN and Surgeon Champion Educate OR nurses and surgeons on CDC wound class definitions. Incorporate wound class validation as part of team debriefing process. Monitor data for improvement and evaluate PDSA cycles. Develop sustainability plan
32 San Jose Kaiser Team
33 Thank You Modesto/Manteca Team!
34 REFERENCES Devaney, Lynn, et al. Improving Surgical Wound Classification-Why it Matters, AORN. (August 2004). 80,(2) pg Howard, J.M. Ultraviolet Radiation in the Operating Room: A Historical Review Annals of Surgery 160(August 1964). Pg Culver, D., et al. Surgical Wound Infection Rates by wound class, operative procedure, and patient risk index American Journal of Medicine. (September 1991).
35 Questions & Feedback
Improving Surgical Wound Classification in the Operating Room May 11, 2012
 Improving Surgical Wound Classification in the Operating Room May 11, 2012 Christina Solis RN,BSN, IA, NSQIP SCNR Kaiser Permanente, San Jose Bruce Ryon RN, MS, PhD, NSQIP SCNR Kaiser Permanente, San Francisco
Improving Surgical Wound Classification in the Operating Room May 11, 2012 Christina Solis RN,BSN, IA, NSQIP SCNR Kaiser Permanente, San Jose Bruce Ryon RN, MS, PhD, NSQIP SCNR Kaiser Permanente, San Francisco
State of Kuwait Ministry of Health Infection Control Directorate. Guidelines for Prevention of Surgical Site Infection (SSI)
") State of Kuwait Ministry of Health Infection Control Directorate Guidelines for Prevention of Surgical Site Infection (SSI) September 1999 Updated 2007 Surgical Wound: According to 1998 Kuwait National
State of Kuwait Ministry of Health Infection Control Directorate Guidelines for Prevention of Surgical Site Infection (SSI) September 1999 Updated 2007 Surgical Wound: According to 1998 Kuwait National
Cheryl Richardson, RN, BSN, CIC
 NHSN Surgical Definitions Cheryl Richardson, RN, BSN, CIC Conflict of Interest and Disclosure of Financial Relationships I m an employee of CareFusion. No financial or in-kind contributions have been given
NHSN Surgical Definitions Cheryl Richardson, RN, BSN, CIC Conflict of Interest and Disclosure of Financial Relationships I m an employee of CareFusion. No financial or in-kind contributions have been given
Long-term urinary catheters: prevention and control of healthcare-associated infections in primary and community care
 Long-term urinary catheters: prevention and control of healthcare-associated infections in primary and community care A NICE pathway brings together all NICE guidance, quality standards and materials to
Long-term urinary catheters: prevention and control of healthcare-associated infections in primary and community care A NICE pathway brings together all NICE guidance, quality standards and materials to
Surgical Site Infection (SSI) Prevention. Basics of Infection Prevention 2-Day Mini-Course 2013
 Prevention. Basics of Infection Prevention 2-Day Mini-Course 2013") 1 Surgical Site Infection (SSI) Prevention Basics of Infection Prevention 2-Day Mini-Course 2013 2 Objectives Review the epidemiology of SSI Explore causes and mechanisms of SSI Describe evidence-based
1 Surgical Site Infection (SSI) Prevention Basics of Infection Prevention 2-Day Mini-Course 2013 2 Objectives Review the epidemiology of SSI Explore causes and mechanisms of SSI Describe evidence-based
Missouri Healthcare-Associated Infection Reporting System (MHIRS)
") Missouri Healthcare-Associated Infection Reporting System (MHIRS) Surgical Site Infection (SSI) Reporting A. INTRODUCTION An estimated 27 million surgical procedures are performed each year in the US.
Missouri Healthcare-Associated Infection Reporting System (MHIRS) Surgical Site Infection (SSI) Reporting A. INTRODUCTION An estimated 27 million surgical procedures are performed each year in the US.
Assuring Data Quality
 Assuring Data Quality Jennie Wilson Programme Leader SSI Surveillance Dept. of Healthcare-Associated Infection & Antimicrobial Resistance, Health Protection Agency SSI cumulative incidence (%) 8.0% 7.0%
Assuring Data Quality Jennie Wilson Programme Leader SSI Surveillance Dept. of Healthcare-Associated Infection & Antimicrobial Resistance, Health Protection Agency SSI cumulative incidence (%) 8.0% 7.0%
Using the COLO and HYST Surgical Site Infection (SSI) Medical Record Abstraction Tools
 Medical Record Abstraction Tools") Using the COLO and HYST Surgical Site Infection (SSI) Medical Record Abstraction Tools Janet Brooks RN, BSN, CIC Nurse Consultant State HAI Grantee Meeting November 14, 2013 National Center for Emerging
Using the COLO and HYST Surgical Site Infection (SSI) Medical Record Abstraction Tools Janet Brooks RN, BSN, CIC Nurse Consultant State HAI Grantee Meeting November 14, 2013 National Center for Emerging
SURGICAL ANTIBIOTIC PROPHYLAXIS. Steve Johnson, PharmD, BCPS Prime Therapeutics, Inc
 SURGICAL ANTIBIOTIC PROPHYLAXIS Steve Johnson, PharmD, BCPS Prime Therapeutics, Inc OBJECTIVES Discuss antibiotic use as prophylaxis vs presumptive therapy vs treatment of infections. Discuss risk factors
SURGICAL ANTIBIOTIC PROPHYLAXIS Steve Johnson, PharmD, BCPS Prime Therapeutics, Inc OBJECTIVES Discuss antibiotic use as prophylaxis vs presumptive therapy vs treatment of infections. Discuss risk factors
Antimicrobial Prophylaxis for Transrectal Prostate Biopsy: Organizational Recommendations. J. Stuart Wolf, Jr., M.D.
 Antimicrobial Prophylaxis for Transrectal Prostate Biopsy: Organizational Recommendations J. Stuart Wolf, Jr., M.D. Department of Urology University of Michigan Ann Arbor, MI Official Recommendations for
Antimicrobial Prophylaxis for Transrectal Prostate Biopsy: Organizational Recommendations J. Stuart Wolf, Jr., M.D. Department of Urology University of Michigan Ann Arbor, MI Official Recommendations for
Deborah Young, RN, BSN, CNOR Green Belt Charleston Area Medical Center
 Deborah Young, RN, BSN, CNOR Green Belt Charleston Area Medical Center Charleston Area Medical Center Charleston, West Virginia 5,818 Employees 913 Licensed Beds 392 General Hospital 375 Memorial Hospital
Deborah Young, RN, BSN, CNOR Green Belt Charleston Area Medical Center Charleston Area Medical Center Charleston, West Virginia 5,818 Employees 913 Licensed Beds 392 General Hospital 375 Memorial Hospital
Surgical Site Infection. Kings County Hospital Center Audrey C. Durrant 6/10/2005
 Surgical Site Infection Kings County Hospital Center Audrey C. Durrant 6/10/2005 Case Presentation HPI patient xx year old presented with approximately xx days periumbillical pain 10/10 on pain scale,
Surgical Site Infection Kings County Hospital Center Audrey C. Durrant 6/10/2005 Case Presentation HPI patient xx year old presented with approximately xx days periumbillical pain 10/10 on pain scale,
Errors in the Operating Room. Patrick E. Voight RN BSN MSA CNOR President Association of perioperative Registered Nurses (AORN)
") Errors in the Operating Room Patrick E. Voight RN BSN MSA CNOR President Association of perioperative Registered Nurses (AORN) What What We All We Strive All Strive For: For: Patient Patient Safety Safety
Errors in the Operating Room Patrick E. Voight RN BSN MSA CNOR President Association of perioperative Registered Nurses (AORN) What What We All We Strive All Strive For: For: Patient Patient Safety Safety
Implementation Manual for the Colorado Surgical Site Checklist
 Implementation Manual for the Colorado Surgical Site Checklist Additional Information or Questions: Crystal Berumen, MSPH Director of Patient Safety Initiatives Colorado Hospital Association 7335 E. Orchard
Implementation Manual for the Colorado Surgical Site Checklist Additional Information or Questions: Crystal Berumen, MSPH Director of Patient Safety Initiatives Colorado Hospital Association 7335 E. Orchard
Surgical Site Infection Prevention
 Surgical Site Infection Prevention 1 Objectives 1. Discuss risk factors for SSI 2. Describe evidence-based best practices for SSI prevention 3. State principles of antibiotic prophylaxis 4. Discuss novel
Surgical Site Infection Prevention 1 Objectives 1. Discuss risk factors for SSI 2. Describe evidence-based best practices for SSI prevention 3. State principles of antibiotic prophylaxis 4. Discuss novel
Appendicitis National Digestive Diseases Information Clearinghouse
 Appendicitis National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH The appendix is a small, tube-like structure
Appendicitis National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH The appendix is a small, tube-like structure
Please answer each question by filling in the blank or by marking the box to the left of your answer.
 SAFE SURGERY 5: SOUTH CAROLINA Tool 1: Checklist Implementation Leader Survey This questionnaire requests information about the hospital in which you work, the surgical service or services in which the
SAFE SURGERY 5: SOUTH CAROLINA Tool 1: Checklist Implementation Leader Survey This questionnaire requests information about the hospital in which you work, the surgical service or services in which the
Surgical Safety Checklists and Briefings Clinician s User Guidelines
 Surgical Safety Checklists and Briefings Clinician s User Guidelines 3/15/2009 Surrey Memorial Hospital Author: Keith Martinsen Before Induction Checklist Surgeon s Team Briefing Before Skin Incision Checklist
Surgical Safety Checklists and Briefings Clinician s User Guidelines 3/15/2009 Surrey Memorial Hospital Author: Keith Martinsen Before Induction Checklist Surgeon s Team Briefing Before Skin Incision Checklist
PREDICTIVE ANALYTICS AT THE BEDSIDE: The 5 W s. John W. Cromwell, MD
 PREDICTIVE ANALYTICS AT THE BEDSIDE: The 5 W s John W. Cromwell, MD Disclosures Entac Medical, Inc. - Chief Medical Officer Apervita, Inc. - Consultant Dell, Inc. - Consultant Cromwell Lab Analytics 2009
PREDICTIVE ANALYTICS AT THE BEDSIDE: The 5 W s John W. Cromwell, MD Disclosures Entac Medical, Inc. - Chief Medical Officer Apervita, Inc. - Consultant Dell, Inc. - Consultant Cromwell Lab Analytics 2009
Guide to Abdominal or Gastroenterological Surgery Claims
 What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
What are the steps towards abdominal surgery? Investigation and Diagnosis It is very important that all necessary tests are undertaken to investigate the patient s symptoms appropriately and an accurate
Safety FIRST: Infection Prevention Tips
 Reading Hospital Safety FIRST: Infection Prevention Tips Reading Hospital is committed to providing high quality care to our patients. Your healthcare team does many things to help prevent infections.
Reading Hospital Safety FIRST: Infection Prevention Tips Reading Hospital is committed to providing high quality care to our patients. Your healthcare team does many things to help prevent infections.
OU Medical System Safe Procedural and Surgical Verification
 OU Medical System Safe Procedural and Surgical Verification I hereby attest that I am aware of OUMS Safe Procedural and Surgical Verification process. I have received a copy of the OUMS Policy on Safe
OU Medical System Safe Procedural and Surgical Verification I hereby attest that I am aware of OUMS Safe Procedural and Surgical Verification process. I have received a copy of the OUMS Policy on Safe
Acute abdominal conditions Key Points
 7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
Clinical Nurse Specialist Practice Across the Continuum
 Clinical Nurse Specialist Practice Across the Continuum Angela Rowe, MSN, APRN, PCNS-BC Pediatric Clinical Nurse Specialist Arkansas Children s Hospital Presentation ID: CD3 Disclosure Today s presenters
Clinical Nurse Specialist Practice Across the Continuum Angela Rowe, MSN, APRN, PCNS-BC Pediatric Clinical Nurse Specialist Arkansas Children s Hospital Presentation ID: CD3 Disclosure Today s presenters
CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM
 For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
Nursing Quality: Measurement and Improvement
 Nursing Quality: Measurement and Improvement This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Target Audience: CMC and
Nursing Quality: Measurement and Improvement This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Target Audience: CMC and
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy. Case Series
 ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
Vanderbilt Perioperative Nurse Internship Syllabus
 Vanderbilt Perioperative Nurse Internship Syllabus Director of Perioperative Education and Research: Audrey H. Kuntz, EdD, RN Pager: 835-1513, Office: 322-7387 Audrey.Kuntz@vanderbilt.edu Nurse Educators:
Vanderbilt Perioperative Nurse Internship Syllabus Director of Perioperative Education and Research: Audrey H. Kuntz, EdD, RN Pager: 835-1513, Office: 322-7387 Audrey.Kuntz@vanderbilt.edu Nurse Educators:
AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Verificatoin Criterea EFFECTIVE JANUARY 1, 2015. Criterion. Level (1 or 2) Number
 Number") Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
2015-2018. Patient Safety and Quality Improvement Plan. Patient Safety and Quality Improvement Plan
 Patient Safety and Quality Improvement Plan Patient Safety and Quality Improvement Plan 2015-2018 Muskoka Algonquin Healthcare is a community of providers dedicated to delivering best patient outcomes
Patient Safety and Quality Improvement Plan Patient Safety and Quality Improvement Plan 2015-2018 Muskoka Algonquin Healthcare is a community of providers dedicated to delivering best patient outcomes
AORTOENTERIC FISTULA. Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005
 AORTOENTERIC FISTULA Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA diagnosis and management Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA Aortoenteric
AORTOENTERIC FISTULA Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA diagnosis and management Mark H. Tseng MD Brooklyn VA Hospital February 11, 2005 AORTOENTERIC FISTULA Aortoenteric
The facility must have methods in place to ensure staff are managed effectively to support the care, treatment and services it provides.
 HUMAN RESOURCES The facility must have methods in place to ensure staff are managed effectively to support the care, treatment and services it provides. This standard addresses human resource planning,
HUMAN RESOURCES The facility must have methods in place to ensure staff are managed effectively to support the care, treatment and services it provides. This standard addresses human resource planning,
SECTION 12.1 URINARY CATHETERS
 SECTION 12.1 URINARY CATHETERS Introduction Summary of Recommendations taken from Guidelines for the Prevention of Catheter-associated Urinary Tract Infection, Published on behalf of SARI by HSE Health
SECTION 12.1 URINARY CATHETERS Introduction Summary of Recommendations taken from Guidelines for the Prevention of Catheter-associated Urinary Tract Infection, Published on behalf of SARI by HSE Health
Open Ventral Hernia Repair
 Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Stacy McLaughlin, RN, MSN. Director of Quality & Performance Improvement
 Stacy McLaughlin, RN, MSN Director of Quality & Performance Improvement 25-bed CAH 21 beds: acute / observation / swingbed 4 bed ICU ED volumes: 14,400 encounters/year 5 Clinics: Rural Health / Primary
Stacy McLaughlin, RN, MSN Director of Quality & Performance Improvement 25-bed CAH 21 beds: acute / observation / swingbed 4 bed ICU ED volumes: 14,400 encounters/year 5 Clinics: Rural Health / Primary
ACS NSQIP The Role of Clinical Support. June 21, 2012 Ava Griffin, RN, CNOR Clinical Support Specialist
 ACS NSQIP The Role of Clinical Support June 21, 2012 Ava Griffin, RN, CNOR Clinical Support Specialist Mission of the Clinical Support Team Members of the Clinical Support Team SCR Training and Ongoing
ACS NSQIP The Role of Clinical Support June 21, 2012 Ava Griffin, RN, CNOR Clinical Support Specialist Mission of the Clinical Support Team Members of the Clinical Support Team SCR Training and Ongoing
Laparoscopic Gallbladder Removal (Cholecystectomy) Patient Information from SAGES
 Patient Information from SAGES") Laparoscopic Gallbladder Removal (Cholecystectomy) Patient Information from SAGES Gallbladder removal is one of the most commonly performed surgical procedures. Gallbladder removal surgery is usually performed
Laparoscopic Gallbladder Removal (Cholecystectomy) Patient Information from SAGES Gallbladder removal is one of the most commonly performed surgical procedures. Gallbladder removal surgery is usually performed
Infection Surveillance Program
 Building an ASC Surgical Site Infection Surveillance Program Lori Groven, MSPHN, RN, CIC Mary Haugen, RN, MA Lori Groven, MSPHN, RN, CIC Mary Haugen, RN, MA Objectives 1. Describe the process of starting
Building an ASC Surgical Site Infection Surveillance Program Lori Groven, MSPHN, RN, CIC Mary Haugen, RN, MA Lori Groven, MSPHN, RN, CIC Mary Haugen, RN, MA Objectives 1. Describe the process of starting
A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page
 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IX0200: Prevention & Control of Catheter Associated
A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IX0200: Prevention & Control of Catheter Associated
Value-Based Purchasing Program Overview. Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012
 Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
How To Become A Surgical Technologist
 JOB DESCRIPTION: SURGICAL TECHNOLOGIST. The Standards and Guidelines for the Accreditation of Educational Programs in Surgical Technology have been approved by the Association of Surgical Technologists
JOB DESCRIPTION: SURGICAL TECHNOLOGIST. The Standards and Guidelines for the Accreditation of Educational Programs in Surgical Technology have been approved by the Association of Surgical Technologists
Red Flags. Whether you handle malpractice. in General Surgical Malpractice Cases
 10 Red Flags in General Surgical Malpractice Cases Whether you handle malpractice cases regularly or you have a general personal injury practice, at some point you likely will need to evaluate a general
10 Red Flags in General Surgical Malpractice Cases Whether you handle malpractice cases regularly or you have a general personal injury practice, at some point you likely will need to evaluate a general
PREVENTION OF CATHETER ASSOCIATED URINARY TRACT INFECTIONS. (CAUTIs)
") PREVENTION OF CATHETER ASSOCIATED URINARY TRACT INFECTIONS (CAUTIs) CAUTIs A UTI where an indwelling urinary catheter was in place for >2 calendar days on the date of event. OR If an indwelling urinary
PREVENTION OF CATHETER ASSOCIATED URINARY TRACT INFECTIONS (CAUTIs) CAUTIs A UTI where an indwelling urinary catheter was in place for >2 calendar days on the date of event. OR If an indwelling urinary
Introduction to Perioperative Nursing
 Jones & Bartlett Learning, LLC. NOT FOR SALE OR DISTRIBUTION C H A P T E R 1 Introduction to Perioperative Nursing Learner Objectives 1. Define the three phases of the surgical experience. 2. Describe
Jones & Bartlett Learning, LLC. NOT FOR SALE OR DISTRIBUTION C H A P T E R 1 Introduction to Perioperative Nursing Learner Objectives 1. Define the three phases of the surgical experience. 2. Describe
The Clinical Nurse Leader Role: A Pilot Evaluation By An Early Adopter
 The Clinical Nurse Leader Role: A Pilot Evaluation By An Early Adopter James L. Harris, DSN, RN, APRN-BC, MBA Sandra E. Walters, MSN, RN Charlene Quinn, PhD, RN Joan Stanley, PhD, RN, APRN-BC, FAAN Kathy
The Clinical Nurse Leader Role: A Pilot Evaluation By An Early Adopter James L. Harris, DSN, RN, APRN-BC, MBA Sandra E. Walters, MSN, RN Charlene Quinn, PhD, RN Joan Stanley, PhD, RN, APRN-BC, FAAN Kathy
Policy for Screening Patients for MRSA Colonisation
 Policy for Screening Patients for MRSA Colonisation To whom this document applies: All staff in Colchester Hospital University Foundation Trust screening Patients for MRSA Procedural Documents Approval
Policy for Screening Patients for MRSA Colonisation To whom this document applies: All staff in Colchester Hospital University Foundation Trust screening Patients for MRSA Procedural Documents Approval
ROLES OF THE PERIOPERATIVE NURSE
 Roles of the This manuscript version is a rendition of the author s post review copy. The official version of record is available at the Perioperative Nursing Clinics site. Perioperative Nurse and Informaticist
Roles of the This manuscript version is a rendition of the author s post review copy. The official version of record is available at the Perioperative Nursing Clinics site. Perioperative Nurse and Informaticist
OUR NEW INPATIENT ORTHOPEDIC AND SPINE UNIT BRINGS THE BEST OF BOSTON TO YOU.
 www.brighamandwomensfaulkner.org OUR NEW INPATIENT ORTHOPEDIC AND SPINE UNIT BRINGS THE BEST OF BOSTON TO YOU. Following orthopedic or spine surgery, your inpatient therapy is a vital first step to your
www.brighamandwomensfaulkner.org OUR NEW INPATIENT ORTHOPEDIC AND SPINE UNIT BRINGS THE BEST OF BOSTON TO YOU. Following orthopedic or spine surgery, your inpatient therapy is a vital first step to your
Kaiser Oakland Urology
 Kaiser Oakland Urology The Main Purpose of Bladder Catheterization Complete Bladder Emptying! Help maintain a healthy bladder Help maintain healthy kidneys Reduce the chances of significant urinary tract
Kaiser Oakland Urology The Main Purpose of Bladder Catheterization Complete Bladder Emptying! Help maintain a healthy bladder Help maintain healthy kidneys Reduce the chances of significant urinary tract
Specific Standards of Accreditation for Residency Programs in General Surgery
 Specific Standards of Accreditation for Residency Programs in General Surgery 2010 INTRODUCTION The purpose of this document is to provide program directors and surveyors with an interpretation of the
Specific Standards of Accreditation for Residency Programs in General Surgery 2010 INTRODUCTION The purpose of this document is to provide program directors and surveyors with an interpretation of the
BERGEN COMMUNITY COLLEGE DIVISION OF HEALTH PROFESSIONS SURGICAL TECHNOLOGY PROGRAM
 SUR 201 COURSE SYLLABUSES CREDITS: 6 BERGEN COMMUNITY COLLEGE DIVISION OF HEALTH PROFESSIONS SURGICAL TECHNOLOGY PROGRAM INSTRUCTORS: CAROLAN SHERMAN CST, RN, BSN, MSN MARY CHMIELEWSKI CST E-MAIL: CSHERMAN@BERGEN.EDU
SUR 201 COURSE SYLLABUSES CREDITS: 6 BERGEN COMMUNITY COLLEGE DIVISION OF HEALTH PROFESSIONS SURGICAL TECHNOLOGY PROGRAM INSTRUCTORS: CAROLAN SHERMAN CST, RN, BSN, MSN MARY CHMIELEWSKI CST E-MAIL: CSHERMAN@BERGEN.EDU
41 Assisting with Minor Surgery
 Learning Outcomes 41.1 Define the medical assistant s role in minor surgical procedures. 41-2 CHAPTER 41 Assisting with Minor Surgery 41.2 Describe types of wounds and explain how they heal. 41.3 Describe
Learning Outcomes 41.1 Define the medical assistant s role in minor surgical procedures. 41-2 CHAPTER 41 Assisting with Minor Surgery 41.2 Describe types of wounds and explain how they heal. 41.3 Describe
Health-Care Associated Infection Rates among Adult Patients in Bahrain Military Hospital: A Cross Sectional Survey
 Bahrain Medical Bulletin, Vol. 32, No. 1, March 2010 Health-Care Associated Infection Rates among Adult Patients in Bahrain Military Hospital: A Cross Sectional Survey Kelechi Austin Ofurum, M.Sc, B.Sc*,
Bahrain Medical Bulletin, Vol. 32, No. 1, March 2010 Health-Care Associated Infection Rates among Adult Patients in Bahrain Military Hospital: A Cross Sectional Survey Kelechi Austin Ofurum, M.Sc, B.Sc*,
Mosby s Nursing Skills Perioperative Skills and Procedures
 Mosby s Nursing Skills Perioperative Skills and Procedures Surgical Gown: Applying Gown and Maintaining Sterility Surgical Field: Maintaining Sterility Surgical Packs: Maintaining Sterility Surgical Packs:
Mosby s Nursing Skills Perioperative Skills and Procedures Surgical Gown: Applying Gown and Maintaining Sterility Surgical Field: Maintaining Sterility Surgical Packs: Maintaining Sterility Surgical Packs:
Partnership for Healthcare Payment Reform Total Knee Replacement Pilot Quality Report Quarter 1 Quarter 4, 2013
 Partnership for Healthcare Payment Reform Total Knee Replacement Pilot Quality Report Quarter 1 Quarter 4, 2013 Introduction This report outlines the total knee replacement pilot quality results for care
Partnership for Healthcare Payment Reform Total Knee Replacement Pilot Quality Report Quarter 1 Quarter 4, 2013 Introduction This report outlines the total knee replacement pilot quality results for care
Surgical Scrub Tech Population and Age Specific Competencies (3/2011 jyc) Name: Completion Year:
 Name: Completion Year:") Surgical Scrub Tech Population and Age Specific Competencies (3/2011 jyc) Name: Completion Year: Directions: Upon completing the selected skill for the selected age group, the evaluator will place their
Surgical Scrub Tech Population and Age Specific Competencies (3/2011 jyc) Name: Completion Year: Directions: Upon completing the selected skill for the selected age group, the evaluator will place their
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop
 Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
YALE UNIVERSITY SCHOOL OF MEDICINE: SECTION OF OTOLARYNGOLOGY PATIENT INFORMATION FUNCTIONAL ENDOSCOPIC SINUS SURGERY
 YALE UNIVERSITY SCHOOL OF MEDICINE: SECTION OF OTOLARYNGOLOGY PATIENT INFORMATION FUNCTIONAL ENDOSCOPIC SINUS SURGERY What is functional endoscopic sinus surgery (FESS)? Functional endoscopic sinus surgery
YALE UNIVERSITY SCHOOL OF MEDICINE: SECTION OF OTOLARYNGOLOGY PATIENT INFORMATION FUNCTIONAL ENDOSCOPIC SINUS SURGERY What is functional endoscopic sinus surgery (FESS)? Functional endoscopic sinus surgery
Clock Hours I Anatomy and Physiology 1-9 180. II Basic Science 10-18 180. III Surgical Technology 19-27 180. IV Surgical Procedures 28-36 180
 SURGICAL TECHNOLOGY (ST) 1500 clock hours/ 70 weeks (Total time to complete the program may vary based on school holidays and breaks) 45 weeks Theory/Lab (20 hours per week) + 25 weeks externship (24 hours
SURGICAL TECHNOLOGY (ST) 1500 clock hours/ 70 weeks (Total time to complete the program may vary based on school holidays and breaks) 45 weeks Theory/Lab (20 hours per week) + 25 weeks externship (24 hours
Surgical Technology. Washburn Institute of Technology. Program Number 51.0909. Target Population. Description. Entry Requirements.
 Surgical Technology Organization Washburn Institute of Technology Program Number 51.0909 Instructional Level Certificate Target Population Post-secondary Description This program provides an opportunity
Surgical Technology Organization Washburn Institute of Technology Program Number 51.0909 Instructional Level Certificate Target Population Post-secondary Description This program provides an opportunity
Introduction to CPT. Current Procedural Terminology. Laura Sullivan, CPC Coordinator Corporate Compliance Auditing & Education
 Introduction to CPT Current Procedural Terminology Laura Sullivan, CPC Coordinator Corporate Compliance Auditing & Education 1 Legal Stuff The information provided here is personal opinion only and should
Introduction to CPT Current Procedural Terminology Laura Sullivan, CPC Coordinator Corporate Compliance Auditing & Education 1 Legal Stuff The information provided here is personal opinion only and should
Dermatology Associates of KY, PSC Job Description
 Dermatology Associates of KY, PSC Job Description Job Title: Perioperative R.N. Department: Ambulatory Surgery Center Reports To: ASC Manager FLSA Status: Non-Exempt;Hourly; Full-Time Summary Responsible
Dermatology Associates of KY, PSC Job Description Job Title: Perioperative R.N. Department: Ambulatory Surgery Center Reports To: ASC Manager FLSA Status: Non-Exempt;Hourly; Full-Time Summary Responsible
Urinary tract and perineum
 9 Urinary tract and perineum Key Points 9.1 9.1 THE URINARY BLADDER URINARY RETENTION Acute retention of urine is an indication for emergency drainage of the bladder The common causes of acute retention
9 Urinary tract and perineum Key Points 9.1 9.1 THE URINARY BLADDER URINARY RETENTION Acute retention of urine is an indication for emergency drainage of the bladder The common causes of acute retention
REGISTERED NURSE AS CIRCULATOR FOR ASC Last updated 5/16/2012
 REGISTERED NURSE AS CIRCULATOR FOR ASC Last updated 5/16/2012 STATE CITATION STATUTORY / REGULATORY LANGUAGE Alabama ALABAMA ADMINISTRATIVE 420-5-2-.02 Administration (3) Personnel... (b) Director of Nursing
REGISTERED NURSE AS CIRCULATOR FOR ASC Last updated 5/16/2012 STATE CITATION STATUTORY / REGULATORY LANGUAGE Alabama ALABAMA ADMINISTRATIVE 420-5-2-.02 Administration (3) Personnel... (b) Director of Nursing
Wound management can be exciting and
 P r o c e d u r e s P r o Peer Reviewed S U R G E R Y / W O U N D M A N A G E M E N T Karen M. Tobias, DVM, MS, DACVS, & John Ayers, DVM University of Tennessee THE ESSENTIAL WOUND CARE SERIES Wound Management
P r o c e d u r e s P r o Peer Reviewed S U R G E R Y / W O U N D M A N A G E M E N T Karen M. Tobias, DVM, MS, DACVS, & John Ayers, DVM University of Tennessee THE ESSENTIAL WOUND CARE SERIES Wound Management
Vascular Training Paradigms: Integrated vs. Independent?
 Vascular Training Paradigms: Integrated vs. Independent? Murray L. Shames, MD, FACS, RPVI Professor of Surgery and Radiology Program Director Vascular Surgery Vascular Annual Meeting San Francisco May
Vascular Training Paradigms: Integrated vs. Independent? Murray L. Shames, MD, FACS, RPVI Professor of Surgery and Radiology Program Director Vascular Surgery Vascular Annual Meeting San Francisco May
BOWEL CANCER. The doctor has explained that you have a growth or tumour, in your bowel or rectum and could be cancer.
 Patient and Carer Information BOWEL CANCER Please read this leaflet carefully. It is important that you take note of any instructions or advice given. If you have any questions or problems that are not
Patient and Carer Information BOWEL CANCER Please read this leaflet carefully. It is important that you take note of any instructions or advice given. If you have any questions or problems that are not
Wound and Skin Assessment. Mary Carvalho RN, BSN, MBA Clinical Coordinator Johnson Creek Wound and Edema Center
 Wound and Skin Assessment Mary Carvalho RN, BSN, MBA Clinical Coordinator Johnson Creek Wound and Edema Center Skin The largest Organ Weighs between 6 and 8 pounds Covers over 20 square feet Thickness
Wound and Skin Assessment Mary Carvalho RN, BSN, MBA Clinical Coordinator Johnson Creek Wound and Edema Center Skin The largest Organ Weighs between 6 and 8 pounds Covers over 20 square feet Thickness
POST-OPERATIVE WOUND INFECTION
 POST-OPERATIVE WOUND INFECTION IN AMBULATORY SURGERY: IMPACT, BURDEN, AND STRATEGIES FOR IMPROVEMENT Nicholas Costanzo MS3 OVERVIEW Definitions Epidemiology Cost Guidelines Pre-op Factors Immediate Peri-operative
POST-OPERATIVE WOUND INFECTION IN AMBULATORY SURGERY: IMPACT, BURDEN, AND STRATEGIES FOR IMPROVEMENT Nicholas Costanzo MS3 OVERVIEW Definitions Epidemiology Cost Guidelines Pre-op Factors Immediate Peri-operative
ORTHOPAEDIC INFECTION PREVENTION AND CONTROL: AN EMERGING NEW PARADIGM
 ORTHOPAEDIC INFECTION PREVENTION AND CONTROL: AN EMERGING NEW PARADIGM AMERICAN ACADEMY OF ORTHOPAEDIC SURGEONS 77th Annual Meeting March 9-12, 2010 New Orleans, Louisiana COMMITTEE ON PATIENT SAFETY PREPARED
ORTHOPAEDIC INFECTION PREVENTION AND CONTROL: AN EMERGING NEW PARADIGM AMERICAN ACADEMY OF ORTHOPAEDIC SURGEONS 77th Annual Meeting March 9-12, 2010 New Orleans, Louisiana COMMITTEE ON PATIENT SAFETY PREPARED
Hospital Value-based Purchasing Specifications 2016 Updated August 2015
 Description Methodology Measurement Period Allowable Exclusions Total Performance Score Individual measures CMS incentive program for PPS hospitals. The purpose is to achieve value by tying payment to
Description Methodology Measurement Period Allowable Exclusions Total Performance Score Individual measures CMS incentive program for PPS hospitals. The purpose is to achieve value by tying payment to
Biodesign. Ventral Hernia Repair Best Outcomes. Procedural Guide
 Biodesign Ventral Hernia Repair Best Outcomes Procedural Guide Achieve best outcomes using Biodesign for ventral hernia repair. Achieving complete and permanent closure of the abdomen following ventral
Biodesign Ventral Hernia Repair Best Outcomes Procedural Guide Achieve best outcomes using Biodesign for ventral hernia repair. Achieving complete and permanent closure of the abdomen following ventral
NYSARC TRC QUALITY INITIATIVE. Reducing ER Admissions
 NYSARC TRC QUALITY INITIATIVE Reducing ER Admissions QUALITY IMPROVEMENT PROJECT- REDUCING ER ADMISSIONS Identification of a High Risk Concern: Complaint from one of the local hospitals that TRC had a
NYSARC TRC QUALITY INITIATIVE Reducing ER Admissions QUALITY IMPROVEMENT PROJECT- REDUCING ER ADMISSIONS Identification of a High Risk Concern: Complaint from one of the local hospitals that TRC had a
Not Just Another Checklist: Using Technology to Implement the Time- Out in the Non-OR Setting
 Not Just Another Checklist: Using Technology to Implement the Time- Out in the Non-OR Setting Ross Ehrmantraut, RN, CCRN Patient Safety Officer Liz McNamara, RN, MN Clinical Operations Manager for Infection
Not Just Another Checklist: Using Technology to Implement the Time- Out in the Non-OR Setting Ross Ehrmantraut, RN, CCRN Patient Safety Officer Liz McNamara, RN, MN Clinical Operations Manager for Infection
3M Steri-Strip S Surgical Skin Closure. Commonly Asked Questions
 3M Steri-Strip S Surgical Skin Closure Commonly Asked Questions What are the indications for use of 3M Steri-Strip S Surgical Skin Closure? Steri-Strip S Surgical Skin Closures are indicated as a primary
3M Steri-Strip S Surgical Skin Closure Commonly Asked Questions What are the indications for use of 3M Steri-Strip S Surgical Skin Closure? Steri-Strip S Surgical Skin Closures are indicated as a primary
Nursing Infection Prevention Leaders Academy Brown Bag Session Surgical Site Infections April 22, 2014 Alisa Trout, RN, BSN Surgical Site Infection
 Nursing Infection Prevention Leaders Academy Brown Bag Session Surgical Site Infections April 22, 2014 Alisa Trout, RN, BSN Surgical Site Infection Prevention Coordinator Infection Prevention Department
Nursing Infection Prevention Leaders Academy Brown Bag Session Surgical Site Infections April 22, 2014 Alisa Trout, RN, BSN Surgical Site Infection Prevention Coordinator Infection Prevention Department
CDR Matt Armentano, PT, DPT, OCS FMC Lexington
 CDR Matt Armentano, PT, DPT, OCS FMC Lexington Define standard acceptable rates of surgical site infections in lower extremity total joint procedures Describe risk factors for surgical site infections
CDR Matt Armentano, PT, DPT, OCS FMC Lexington Define standard acceptable rates of surgical site infections in lower extremity total joint procedures Describe risk factors for surgical site infections
Joint Surgery/Thoracic Surgery Program Review Committees for Surgery and Thoracic Surgery
 I. Introduction Joint Surgery/Thoracic Surgery Program Review Committees for Surgery and Thoracic Surgery The Joint Surgery/Thoracic Surgery program is approved by both the American Board of Surgery (ABS)
I. Introduction Joint Surgery/Thoracic Surgery Program Review Committees for Surgery and Thoracic Surgery The Joint Surgery/Thoracic Surgery program is approved by both the American Board of Surgery (ABS)
How a Hospital Rapidly Smoothed Out Patient Flow and Spurred Cultural Change
 How a Hospital Rapidly Smoothed Out Patient Flow and Spurred Cultural Change In mid-2008, Heartland Regional Medical Center (HRMC) in St. Joseph, Mo., was like almost every other hospital in the United
How a Hospital Rapidly Smoothed Out Patient Flow and Spurred Cultural Change In mid-2008, Heartland Regional Medical Center (HRMC) in St. Joseph, Mo., was like almost every other hospital in the United
Introduction. Advantages of minimally invasive surgery (MIS) in pediatric trauma:
 in pediatric trauma:") Introduction Purpose of Study: To validate the use of laparoscopic and thoracoscopic surgery for diagnostic and therapeutic modalities in the treatment of pediatric trauma Advantages of minimally invasive
Introduction Purpose of Study: To validate the use of laparoscopic and thoracoscopic surgery for diagnostic and therapeutic modalities in the treatment of pediatric trauma Advantages of minimally invasive
Accountable Care Organization
 Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Continuous Quality Improvement using Centricity EMR
 Continuous Quality Improvement using Centricity EMR Jamie Howard, MD David A. Nelsen, Jr, MD, MS Associate Professors, UAMS Family & Preventive Medicine Sept 22-25, 2004 CLINICAL INFORMATION SYSTEMS 1
Continuous Quality Improvement using Centricity EMR Jamie Howard, MD David A. Nelsen, Jr, MD, MS Associate Professors, UAMS Family & Preventive Medicine Sept 22-25, 2004 CLINICAL INFORMATION SYSTEMS 1
Defining the Core Clinical Documentation Set
 Defining the Core Clinical Documentation Set for Coding Compliance Quality Healthcare Through Quality Information It is time to examine coding compliance policy and test it against the upcoming challenges
Defining the Core Clinical Documentation Set for Coding Compliance Quality Healthcare Through Quality Information It is time to examine coding compliance policy and test it against the upcoming challenges
MRSA, Hand Hygiene and Contact Precautions
 MRSA, Hand Hygiene and Contact Precautions Wesley Medical Center Department of Education May 2007 Authors: Lois Rahal, RN, BSN, CIC Brandy Jackson, RN, BSN Hope Helferich, RNC, BSN 1 Objectives Upon completion
MRSA, Hand Hygiene and Contact Precautions Wesley Medical Center Department of Education May 2007 Authors: Lois Rahal, RN, BSN, CIC Brandy Jackson, RN, BSN Hope Helferich, RNC, BSN 1 Objectives Upon completion
Acute Care Episode (ACE) Demonstration
 Demonstration") Acute Care Episode (ACE) Demonstration Gary L. Whittington CFO, Region Services Baptist Health System San Antonio, Texas Daniel Hurry VP, Supply Chain & Purchased Services Baptist Health System San Antonio,
Acute Care Episode (ACE) Demonstration Gary L. Whittington CFO, Region Services Baptist Health System San Antonio, Texas Daniel Hurry VP, Supply Chain & Purchased Services Baptist Health System San Antonio,
INTRAPERITONEAL HYPERTHERMIC CHEMOTHERAPY (IPHC) FOR PERITONEAL CARCINOMATOSIS AND MALIGNANT ASCITES. INFORMATION FOR PATIENTS AND FAMILY MEMBERS
 FOR PERITONEAL CARCINOMATOSIS AND MALIGNANT ASCITES. INFORMATION FOR PATIENTS AND FAMILY MEMBERS") INTRAPERITONEAL HYPERTHERMIC CHEMOTHERAPY (IPHC) FOR PERITONEAL CARCINOMATOSIS AND MALIGNANT ASCITES. INFORMATION FOR PATIENTS AND FAMILY MEMBERS Description of Treatment A major difficulty in treating
INTRAPERITONEAL HYPERTHERMIC CHEMOTHERAPY (IPHC) FOR PERITONEAL CARCINOMATOSIS AND MALIGNANT ASCITES. INFORMATION FOR PATIENTS AND FAMILY MEMBERS Description of Treatment A major difficulty in treating
Safe Surgery Process Steps (including the Minnesota Time Out) to Prevent Wrong Surgery
 to Prevent Wrong Surgery") Safe Surgery Process Steps (including the Minnesota Time Out) to Prevent Wrong Surgery Kathleen A. Harder, PhD Center for Design in Health University of Minnesota The Safe Surgery Process including the
Safe Surgery Process Steps (including the Minnesota Time Out) to Prevent Wrong Surgery Kathleen A. Harder, PhD Center for Design in Health University of Minnesota The Safe Surgery Process including the
STANDARD OPERATING PROCEDURE #201 RODENT SURGERY
 STANDARD OPERATING PROCEDURE #201 RODENT SURGERY 1. PURPOSE The intent of this Standard Operating Procedure (SOP) is to describe procedures for survival rodent surgery. 2. RESPONSIBILITY Principal investigators
STANDARD OPERATING PROCEDURE #201 RODENT SURGERY 1. PURPOSE The intent of this Standard Operating Procedure (SOP) is to describe procedures for survival rodent surgery. 2. RESPONSIBILITY Principal investigators
TUTORIAL: How to Code an Emergency Department (ED) Record
 Record") TUTORIAL: How to Code an Emergency Department (ED) Record Welcome! Assigning ICD-10-CM codes to diagnoses and CPT/HCPCS Level II codes to procedures/services for emergency department office records can
TUTORIAL: How to Code an Emergency Department (ED) Record Welcome! Assigning ICD-10-CM codes to diagnoses and CPT/HCPCS Level II codes to procedures/services for emergency department office records can
Ellen F. Robinson, PT ATC Clinical Quality Specialist Seattle, WA
 Ellen F. Robinson, PT ATC Clinical Quality Specialist Seattle, WA Mission and Priority of care Confidential: Quality Improvement 2 July 2009 Oh I wish I had a toolkit July 2010 AHRQ Toolkit Project July
Ellen F. Robinson, PT ATC Clinical Quality Specialist Seattle, WA Mission and Priority of care Confidential: Quality Improvement 2 July 2009 Oh I wish I had a toolkit July 2010 AHRQ Toolkit Project July
Hernia- Open Inguinal Hernia Repair PROCEDURAL CONSENT FORM. A. Interpreter / cultural needs. B. Condition and treatment
 DO NOT WRITE IN THIS BINDING MARGIN v5.00-04/2011 SW9317 Hernia- Open Inguinal Hernia Repair Facility: A. Interpreter / cultural needs An Interpreter Service is required? Yes No If Yes, is a qualified
DO NOT WRITE IN THIS BINDING MARGIN v5.00-04/2011 SW9317 Hernia- Open Inguinal Hernia Repair Facility: A. Interpreter / cultural needs An Interpreter Service is required? Yes No If Yes, is a qualified
JOB DESCRIPTION FORM. Location: FHP
 JOB DESCRIPTION FORM Job Title: Medical Assistant Location: FHP Job Summary: Reports directly to the Senior Specialty Services Manager and interviews patients to obtain medical information and measures
JOB DESCRIPTION FORM Job Title: Medical Assistant Location: FHP Job Summary: Reports directly to the Senior Specialty Services Manager and interviews patients to obtain medical information and measures
CLABSI Experience Saint Louis University Hospital
 CLABSI Experience Saint Louis University Hospital Thursday, September, 01 Our Story Academic medical center Owned by Tenet Healthcare affiliated with Saint Louis University (SLU) and a closed medical staff
CLABSI Experience Saint Louis University Hospital Thursday, September, 01 Our Story Academic medical center Owned by Tenet Healthcare affiliated with Saint Louis University (SLU) and a closed medical staff
Prevention and Recognition of Obstetric Fistula Training Package. Module 8: Pre-repair Care and Referral for Women with Obstetric Fistula
 Prevention and Recognition of Obstetric Fistula Training Package Module 8: Pre-repair Care and Referral for Women with Obstetric Fistula Early detection and treatment If a woman has recently survived a
Prevention and Recognition of Obstetric Fistula Training Package Module 8: Pre-repair Care and Referral for Women with Obstetric Fistula Early detection and treatment If a woman has recently survived a
Hot Topics In Infection Control!
 2015 SASKPIC Fall Conference Hot Topics In Infection Control! According to the Provincial ICCs that is Objectives Provide context for UTI prevention in Continuing Care settings Recommendations and tools
2015 SASKPIC Fall Conference Hot Topics In Infection Control! According to the Provincial ICCs that is Objectives Provide context for UTI prevention in Continuing Care settings Recommendations and tools
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
James T. Dwyer DO, FACOI
 Antibiotics in the Surgical Patient James T. Dwyer DO, FACOI Objectives Define current prophylactic recommendations for the use of antibiotics in the surgical patient List current antibiotics available
Antibiotics in the Surgical Patient James T. Dwyer DO, FACOI Objectives Define current prophylactic recommendations for the use of antibiotics in the surgical patient List current antibiotics available
Lymph Node Dissection for Penile Cancer
 Lymph Node Dissection for Penile Cancer Exceptional healthcare, personally delivered Removal of Lymph Nodes Why are the Lymph Nodes so important when I have penile cancer? Lymph nodes are small bean shaped
Lymph Node Dissection for Penile Cancer Exceptional healthcare, personally delivered Removal of Lymph Nodes Why are the Lymph Nodes so important when I have penile cancer? Lymph nodes are small bean shaped
4/5/2013. Dee Webber RN BSN Staff Nurse EMMC CCU. Health care-associated infections are one of the most common complications of hospital care.
 Dee Webber RN BSN Staff Nurse EMMC CCU Critical Care Staff Nurse Leaders Sara Sabal ADN, RN Dee Webber BSN, RN Critical Care Leadership Joyce Hill BSN, RN Tina Closson BSN,RN, CCRN, CSC Cynthia Downs MSN,
Dee Webber RN BSN Staff Nurse EMMC CCU Critical Care Staff Nurse Leaders Sara Sabal ADN, RN Dee Webber BSN, RN Critical Care Leadership Joyce Hill BSN, RN Tina Closson BSN,RN, CCRN, CSC Cynthia Downs MSN,