Clinical Manifestations and Treatment of HIV
|
|
|
- Alisha Shields
- 7 years ago
- Views:
Transcription
1 Clinical Manifestations and Treatment of HIV Ronald Mitsuyasu, MD Professor of Medicine Director, UCLA Center for Clinical AIDS Research and Education (CARE Center)

2 The Natural History of HIV Infection Pantaleo G, et al. N Engl J Med 1993;328;327.

3 Clinical Manifestations of HIV Early signs and symptoms Oral manifestations Malignancies Opportunistic Infections Neuro-psychiatric illnesses Women and HIV = Not in today s presentation,

4 Signs and Symptoms

5 CDC Stage of HIV Disease Stage I Acute HIV infection Stage II Asymptomatic HIV Stage III Early Symptomatic HIV Stage IV Late Symptomatic HIV A Constitutional Disease B Neurological Disease C Secondary Infections C1 AIDS defining C2 Other infections D Secondary Cancers E Other Conditions

6 Acute Retroviral Syndrome Fever 96% Lymphadenopathy 74% Pharyngitis 70% Rash 70% Myalgia/Arthraligia 54% Diarrhea 32% Headaches 32% Nausea/Vomiting 27% Hepatomegaly 14% Weight Loss 13% Neurologic symptoms 12%

7
8
9

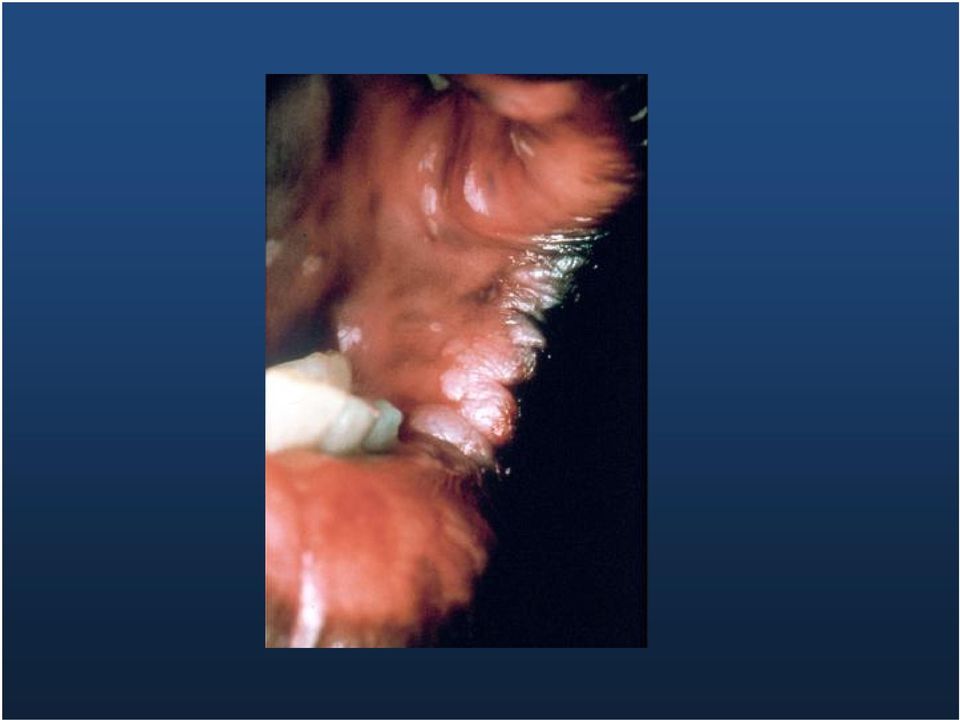
10 Oral Manifestations of HIV

11 WHO Clinical Staging of Oral Manifestations of HIV Stage 1 2 Adults and Adolescents (>15 yo) No disease Angular cheilitis Recurrent oral ulceration Children < 15 yo No disease Angular Cheilitis Linear gingival erythema, extensive warts Recurrent oral ulcerations, parotid enlarge 3 Persistent oral candidiasis Oral hairy leukoplakia Acute necrotizing ulcerative stomatitis, gingivitis, periodontitis Persistent oral candidiasis (after 8ws) Oral hairy leukoplakia Acute necrotizing ulcerative gingivitis or periodontitis 4 Chronic (>1 mo) orolabial HSV Kaposi s sarcoma Non-Hodgkin s lymphoma Chronic (>1 mo) orolabial HSV Kaposi s sarcoma Non-Hodgkin s lymphoma WHO, Classification of HIV, int/hiv/pub/guidelines/hivstaging pdf
 orolabial HSV Kaposi s sarcoma Non-Hodgkin s lymphoma WHO, Classification of HIV, 2007 http://www.who.")
12 HIV-related Oral Lesions Infections Fungal, Viral, Bacterial Neoplasms Kaposi s Sarcoma, Non-Hodgkin s Lymphoma Other Aphthous-like Ulcers, Lichenoid or Drug Reactions, Salivary Gland Disease

13 Oral Candidiasis Clinical Types Erythematous Pseudomembranous Angular Cheilitis DHS/HIV/PP

14 Hairy Leukoplakia Treatment and Management: Generally does not require treatment Antiviral treatment and topical podophyllum resin have been used to treat -- the result is temporary May wax and wane without treatment

15

16 Oral Ulcers Herpes simplex infection Cytomegalovirus infection Aphthous ulcers Histoplasmosis HPV lesions Lymphoma Necrotizing ulcerative gingivitis (NUG) Necrotizing ulcerative periodontitis (NUP) Necrotizing stomatitis (NS)
 Necrotizing")
17 Aphthous Lesions Clinical Types Minor (Lip) Minor (Tongue) Major DHS/ HIV/PP
 Major")
18 Oral Aphthous Lesions Treatment Options Topical Therapy - Topical Corticosteroids Intralesional - Triamcinolone: 40 mg /ml (0.5 ml-1.0 ml injected bid) Systemic Therapy - Prednisone: mg/kg qd x 7-10d, then taper - Thalidomide: 200 mg PO qd DHS/HIV/PP

19 Lesions Caused By Human Papilloma Virus (HPV) Appearance: exophytic, papillary, oral mucosal lesions Several different types of HPV have been reported to cause lesions May be multiple Often difficult to treat due to a high risk of recurrence

20
21 Kaposi s Sarcoma Appearance: Oral lesions appear as reddish purple, raised or flat Size ranges from small to extensive Behavior is unpredictable Definitive diagnosis: biopsy and histologic examination No curative therapy--antiretroviral therapy, radiation treatment, chemotherapy and sclerosing agents have been, used to control oral lesions
22
23
24 Cancers in HIV
25 Number of people living with AIDS, AIDS-defining cancers, non-aids-defining Cancer Incidences cancers, and in all HIV cancers in in USA the USA during Shiels M S et al. J Natl Cancer Inst 2011;103:
26 Categorizing Cancers in PWHA AIDS Defining Cancer KS (decreasing) NHL (BL, CNS, DLCBL) Cervical Cancer ( added in 1993) Elevated risk but rare Merkel Carcinoma Leiomyosarcoma Salivary gland LEC Non AIDS defining Cancers (increasing) Anal Cancer Lung Cancer Hodgkin Lymphoma Liver Cancer Unchanged risk Breast Colorectal Prostate Follicular lymphoma
27 Cancers in HIV Disease AIDS-Defining Defining Kaposi s s Sarcoma Non-Hodgkin Hodgkin s s Lymphoma (systemic and CNS) Invasive Cervical Carcinoma Non-AIDS Defining Anal Cancer Hodgkin s s Disease Leiomyosarcoma (pediatric) Squamous Carcinoma (oral) Merkel cell Carcinoma Hepatoma Virus HHV-8 EBV, HHV-8 HPV HPV EBV EBV HPV MCV HBV, HCV
28 Breakdown of causes of death: France 2005 AIDS Cancer Hepatitis C CVD Suicide Non-AIDS infection Accident Hepatitis B Liver disease OD / drug abuse neurologic renal pulmonary digestive iatrogenic metabolic psychiatric other unknown Percent Hessamfar-Bonarek Int. J. Epid 2010;39: N = 937 deaths Lewden JAIDS 2008, 48:590-9
29 Non-AIDS Defining Cancers NADC
30 Non AIDS-defining Cancers Emerging Epidemiologic Features Proportion of Cancers in HIV NADC 31% 58% Standardized Incidence Ratio HIV:non-HIV Lung Hodgkin lymphoma Larynx Anus Liver Engels EA, Int J Cancer. 2008;123:
31 Factors Contributing to the Increase in Cancer cases in HIV 4-fold increase in HIV/AIDS Population Greater and earlier start to smoking in HIV Rising proportion of HIV pts > 50 yo Cancer incidence increases with age Increase in some CA incidence rate among HIV Lung (3X), anal (29X), liver (3X), HL (11X) Suggests may be additional risk from HIV
32 NADC Incidence and Mortality Retrospective survey of Kaiser Permanente, N. and S. California; 22,081 HIV+, 230,069 HIV- matched by age, sex, clinic and initial yr of F/U 5-yr survival for incident prostate, anal, lung, colorectal cancers or Hodgkin lymphoma. All cause mortality rates and mortality hazard ratios Earlier mean age at dx in HIV+ for anal, lung and colorectal, but not for prostate or HL HIV+ dx at higher stage for lung and HL HIV+ reduced survival for HL, lung and prostate, but not for anal and colorectal Silverberg M et al. 19 th CROI, Seattle, 2012, abs 903.
33 NADC Mortality HIV+ vs HIV- Hodgkin Lymphoma HR 3.0 ( ) Lung 1.7 ( ) Prostate 2.2 ( ) Anal 1.7 ( ) Colorectal 1.6 ( ) Silverberg M et al. 19 th CROI, Seattle, 2012, abs 903.
34 Pathogenesis of Cancer in HIV Many are virally-induced induced cancers, but not all Immune activation, inflammation and decreased immune surveillance HIV may activate cellular genes or proto-oncogenes oncogenes or inhibit tumor suppressor genes HIV induces genetic instability (e.g( 6 fold higher number of MA in HIV lung CA over non-hiv) 1 Increase susceptibility to effects of carcinogens Endothelial abnormalities may allow for cancer development Population differences based on genetics and exposure to carcinogens Wistuba Il, Pathogenesis of NADC: a review. AIDS Pt Care 1999;13:415-26
35 Lymphomas
36 Pathology of AIDS-Related Non-Hodgkin Hodgkin s s Lymphoma Slide #36 Small noncleaved-cell cell lymphoma Burkitt s lymphoma and Burkitt-like lymphoma Immunoblastic lymphoma (primary CNS) Diffuse large-cell lymphoma (90% CD20+) Large noncleaved-cell cell lymphoma CD30+ anaplastic large B-cell B lymphoma Plasmablastic lymphoma Advanced stage (>75% III or IV) Extranodal involvement Central nervous system, liver, bone marrow, gastrointestinal Tirelli U, et al. AIDS. 2000;14:
37 AIDS-related Lymphoma Experience Suggests Cancer Treatment Outcome Can be Equivalent to General Population Percent Survival AMC 034 EPOCH CD4>100 NCI EPOCH : HAART Era : Pre-HAART NCI DLBCL non-aids Months Besson et al. Blood. 2001; 98: Little et al Blood. 2003; 101: Sparano et al. Blood, 2010;115:
38 Cancer Screening in HIV
39 ACS, NCI and USPSTF Cancer Screening Guidelines Cervical CA begin within 3 yrs of 1 st intercourse or 21 yo and q 1-2 yrs. If and 3 normal Paps q3 yrs Prostate CA discuss with MD at 50. DRE yearly and individualized PSA testing Breast CA clinical breast exam q 3 yr 20-30, yearly at 40, yearly mammogram start age 50 Colon CA flex sig q 5yrs or colon q 10 yrs and FOBT yearly Others periodic health exams after age 20, with health counseling and oral, skin, lymph nodes, testes, ovaries and thyroid exam Other tests based on family history, other known cancer risk exposures or known risk factors
40 HIV Patient Screening Routine screening for HIV patients seems to be done LESS frequently than age-appropriate SOC screening for breast (67% vs 79%) and colon (56% vs 77.8%) and prostate biopsies Preston-Martin. Prev Med 2002;34: Reinhold JP. Am J Gastroenterol 2005;100: Hsiao W, Science World J 2009;9:102-8 Concerns about higher false positive rate in HIV (eg, NLST found reduction in lung cancer mortality (20%) in older cigarette smokers with CT) but also high false positive rates, which may be true in HIV as well
41 Why is anogenital cancer important? Cervical cancer is the most common cancer in women worldwide and anal cancer is as common in MSM (75/100,000) as cervical cancer in unscreened populations of women (50-150/100,000 person-yr) Anal cancer particularly common in HIV+ MSM Anal cancer occurs in women as well Anal cancer is one of several cancers whose incidence in the HAART era is increasing, not decreasing
42 Screening for cervical and anal dysplasia No USA national or international guideline for anal screening other than NYS DOH anal Pap screening guidelines. Many HIV groups recommend yearly cervical and anal PAP, with colposcopy and/or HRA and biopsy of any suspicious lesions and q 6m F/U for those with abnormalities noted Many cervical cancer screen and treat program now operating in resource-limited settings Chiao EY et al. Clin Infect Dis 2006;43: Goldie SJ et al. JAMA 1999;282:1822-9
43 Cancer Prevention Smoking Cessation Highest priority Varenicline not hepatic met and no ART drug interaction expected Hepatitis B and HPV vaccination Treat active Hepatitis C Yearly cervical and anal Paps Gyn and HRA Advise sun screen and avoid overexposure Maintain high index of suspicion for cancer Complete family history for malignancies Breast, prostate and colon screening as per guidelines for general population CT Lung and liver ultrasound controversial Treat all HIV patients with HAART
44 Summary As HIV population ages with persistent immune abnormalities, cancers will increase in number The risk of NADC is high with lung, anal, liver and HL accounting for most of this increase. The risk of colon, breast and prostate cancers not elevated in HIV. HL occurs at older age, but may reflect lack of younger age peak, as all cases in HIV are EBV+ As a minimum, we should conduct age/gender appropriate screening for cancer. Counsel patients on ways to reduce cancer risks Only through prospective clinical trials research can prevention strategies and new treatments be effectively evaluated
45 Thank You For information on AMC clinical trials see: For information on NCI programs in HIV cancer see: To refer for AMC clinical trials in LA, call UCLA CARE Center ask for Maricela Gonzalez or page/ Dr. Mitsuyasu,
46 Use of Antiretroviral Therapy
47 Overview Benefits and limitations of HAART When to start What to start with Simplified drug regimens and treatment adherence When to change therapy Second line therapies
48 Benefits of ART Prevention of mother to child transmission Post exposure prophylaxis (PEP) Secondary prevention of HIV transmission Primary prevention (PrEP) Clinical management of patients with HIV Reduces HIV replication Increase or maintain CD4 numbers Maintain less fit mutated HIV
49 Current antiretroviral targets Entry Inhibitors CCR5, MRV Reverse transcriptase Inhibitors ZDV, ddi, ddc, d4t, 3TC, ABC, TDF, FTC DLV, NVP, EFV, ETV RPV RT Fusion Inhibitor Enfuvirtide RNA RNA DNA RT DNA DNA RNA RNA Provirus Proteins Viral protease Inhibitors Integrase Raltegravir Elvitegravir SQV RTV IDV NFV APV LPV FOS ATZ TPV DRV
50 Nucleoside analogues zidovudine (AZT, ZDV) didanosine (ddi) zalcitabine (ddc) stavudine (d4t) lamivudine (3TC) abacavir (ABC) emtricitabine (FTC) Nucleotide analogue tenofovir (TFV) Non-nucleoside analogues nevirapine (NVP) delavirdine (DLV) efavirenz (EFV) etravirine (ETV) rilpivirine (RPV) Antiretroviral Drugs 2013 Reverse Transcriptase Inhibitors(13) Protease Inhibitors (10) saquinavir (SQV) ritonavir (RTV) indinavir (IDV) nelfinavir (NFV) amprenavir (APV) lopinavir/r (LPV/r) Integrase Inhibitor (2) fosamprenavir (FPV) raltegravir (RAL) atazanavir (ATV) elvitegravir (ELV) tipranavir (TPV) Fusion Inhibitor darunavir (DRV) fuzeon (T20) dolutegravir (DTG) Entry Inhibitor (CCR5) maraviroc (MVC)
51 Overview Benefits and limitations of HAART When to start What to start with Simplified drug regimens and treatment adherence When to change therapy Second line therapies
52 Case 47 yo Black Male Diagnosed on routine insurance examination PMHx remarkable for HTN, diet controlled No AIDS associated diseases or symptoms No medications Understands treatment issues and wants to begin therapy if you think it is appropriate Has insurance that can pay for his meds
53 If his viral load is 30,000 c/ml, at which CD4 count would you recommend starting therapy? 1. Would treat at any CD4 count cells / ul cells / ul cells / ul cells / ul 6. < 200 cells /ul 7. < 50 cells /ul 8. Would not recommend ART
54 When to Start Therapy: Balance Tipping in Favor of Earlier Initiation Drug toxicity Preservation of limited Rx options Cost Potency, durability, simplicity and safety of current regimens Improved formulations and PK New classes of drugs Excess morbidity/mortality at higher CD4 Delayed CD4 Earlier
55 Reasons to Start Early The Biology Association of Inflammation and Disease Better Tolerated/Easier to Take Medications Randomized Controlled Trial Data Cohort Data Irreversible Damage Public Health
56 Latently Infected CD4+ Lymphocytes HIV Infected Cells HIV virions Antiretroviral Rx Uninfected Activated CD4+ Lymphocytes M Saag, UAB Uninfected Resting CD4+ Lymphocytes
57 Opportunistic Infections Occur at Higher CD4+ Cell Count Strata Incidence per 1000 PYFU (95%CI) CMV / MAC / TOXO PCP /EC TB 174 < >=500 < >=500 Latest CD4 count N events < >=500 Podlekareva et al. J Infect Dis 2006;194:633
58 When to start?: ART Cohort Collaboration Modeled data 10,855 patients included, with >61,000 personyears of F/U (median 2.7 yrs) 934 progressed to AIDS or died IDUs excluded from model Cumulative Probability of AIDS/Death by CD4 Count at Initiation of ART Probability of AIDS or Death cells/mm cells/mm cells/mm Years Since Initiation of HAART Antiretroviral Therapy (ART) Cohort Collaboration, AIDS 2007;21:
59 Variable Delayed Initiation of ART and Increased Risk of Death CD4+ count cells/ml Relative Risk ART deferral 1.6 ( ) Female sex 1.9 ( ) Older age (10yr) 1.9 ( Baseline CD4+ (100 cell increment) Baseline HIV RNA (log 10 increment) 0.7 ( ) 1.1 ( ) CD4+ count >500 cells/ml P Relative Risk Value ( ) ( ) < ( ) ( ) ( ) Kitahata et al, New Eng J Med 2009;360:1815 (adapted) P Value <
60 Cumulative Mortality Estimates Calculated Using Extended Kaplan-Meier Survival Estimates CD4 > 500 & Defer HAART (N=6,539) Years after 1996 CD4 > 500 & Initiate HAART (N= 2,616) Kitahata MM, et al. CROI Abstract 71.
61 Most New Infections Transmitted by Persons who Do Not Know Their Status ~25% Unaware of Infection ~75% Aware of Infection account for ~54% New Infections ~46% of New Infections Source: G. Marks et al. AIDS 2006
62 HPTN HIV discordant couples (HIV+ partner CD ) 886 immediate HAART 877 delayed HAART (CD4 250) All receiving HIV prevention services Cohen MS, N Engl J Med. 2011: transmission* & 3 cases of extrapulmonary TB 27 transmissions* & 17 cases of extrapulmonary TB *96% reduction in HIV transmission to HIV-negative partner median follow-up 2 years
63 Reasons to Start Early The Biology Association of Inflammation and Disease Better Tolerated Medications Today Randomized Controlled Trial Data Cohort Data Public Health Common Sense!
64 Relative Time on Treatment 40 years on Rx CD4 650/ul 5 years HARM? 35 years on Rx CD4 500/ul AGE (years)
65 So.what is the harm? Destruction of Lymphoid Tissue Inflammation Increased Cardiovascular Events Increased incidence of certain malignancies Accelerated Aging Accelerated Cognitive Decline
66 Conclusions Balance of data support starting Rx in ~ all individuals regardless of CD4+ T cell counts Understanding of HIV pathogenesis Cohort data Public health implications No randomized clinical trial data for higher CD4 counts > 500 yet (START study is enrolling) Waiting until RCT data could well lead to harm that likely will not be reversible
67 When to Start Treatment Clinical Category AIDS-defining illness or severe symptoms CD4 Count (cells/mm 3 ) HIV RNA (copies/ml) 2/13/13 DHHS Guidelines Any value Any value Treat 2012 IAS-USA Guidelines Asymptomatic <500 Any value Treat >500 Any value Treat Pregnant women Any value Any value Treat HIV-associated nephropathy HIV/HBV coinfection when HBV treatment is indicated Any value Any value Treat Any value Any value Treat *Unless elite controller (HIV RNA <50 copies/ml) or has stable CD4 cell count and low-level viremia in absence of therapy. The IAS-USA guidelines also recommends initiating antiretroviral therapy in HIV-infected patients with active hepatitis C virus infection, active or high risk for cardiovascular disease, and symptomatic primary HIV infection. DHHS. Available at: Revision February 2013; Thompson MA, et al. JAMA. 2012;308:
68 When To Start Treatment: Summary of Current Guidelines Guideline CD4 < 350 CD CD4 >500 British HIVA September, 2012 treat Consider unless: HBV or HCV, High CV risk, HIVAN, pregnantthen treat Unknown European ACS November, 2012 treat Consider unless: HCV, HIVAN, HBV needing Tx; CD4 decline >50-100/yr, pregnant Treat Unknown IAS-USA: treat treat July, 2012 DHHS: treat treat February, 2013
69 When to Start Therapy: Balance Tipping in Favor of Earlier Initiation Drug toxicity Preservation of limited Rx options Cost Potency, durability, simplicity and safety of current regimens Improved formulations and PK Enhanced adherence Diminished emergence of resistance New classes of drugs Excess morbidity/mortality at higher CD4 < 350 CD4 Everyone?
70 Overview Changing epidemiology of AIDS in the United States Benefits and limitations of HAART When to start What to start with Simplified drug regimens and treatment adherence Second line therapy
71 Factors to consider in choosing first-line therapy Patient s willingness to commit to therapy Baseline resistance Efficacy data Tolerability Convenience Comorbid conditions Consequences of failure (resistance) Since the introduction of potent ARV therapy preferred regimens all include NRTIs + third drug
72 DHHS Guidelines for Adolescents/Adults: What to Start Preferred Regimens Alternative Regimens Acceptable Regimens EFV/TDF/FTC ATV/r + TDF/FTC DRV/r (once daily) + TDF/FTC RAL + TDF/FTC [Pregnant Women Only: LPV/r (twice daily) + ZDV/3TC] EFV + ABC/3TC RPV + (TDF or ABC)/(FTC or 3TC) ATV/r or DRV/r + ABC/3TC FPV/r or LPV/r (qd or bid) ABC/3TC or TDF/FTC RAL + ABC/3TC EVG/COBI/TDF/FTC (9/18/12) EFV or RPV + ZDV/3TC NVP + TDF/FTC or ZDV/3TC or ABC/3TC ATV + (ABC or ZDV)/3TC ATV/r, DRV/r, LPV/r, FPV/r, RAL + ZDV/3TC MVC + ZDV or ABC/3TC SQV/r + TDF/FTC or ABC/3TC or ZDV/3TC (with caution) DHHS Guidelines. Available at: Revision Feb, 2013.
73 Boosted-Protease Inhibitors KLEAN 1 (ITT E, TLOVR) 48 weeks ARTEMIS 2 (ITT, TLOVR) 96 weeks CASTLE 3 (ITT, NC=F) 96 weeks n=434 LPV/r 400/100 BID N=444 FPV/r 700/100 BID 0 n=346 LPV/r QD or BID n=343 DRV/r 800/100 QD LPV/r 400/100 BID ATV/r 300/100 QD Adapted from: 1. Eron J, et al. Lancet 2006; 368: ; 2. Mills A, et al. AIDS May 29, Molina J-M, et al. 48 th ICAAC/46 th IDSA, Washington, DC, Abst. H-1250d 0 n=443 n=440
74 Daar ES, et al. Ann Intern Med 2011; 154: ATV/r vs. EFV Primary Endpoint
75 Pooled* ECHO and THRIVE W48 analysis: VL <50 copies/ml over 48 weeks (ITT-TLOVR) Virologic responders (%, 95% CI) RPV 25mg qd (N=686) EFV 600mg qd (N=682) Time (weeks) 84.3% 82.3% Each of the trials reached their primary objective of noninferiority of RPV to EFV in confirmed virologic response CI = confidence interval; *Pooled analyses were preplanned Difference (95% CI) in response rates estimated by logistic regression adjusted for stratification factors: 1.6 ( 2.2, 5.3) Cohen JAIDS 2012
76 STARTMRK: RAL vs. EFV ITT, NC=F Percentage of Patients with HIV RNA Levels <50 Copies/mL CD4 Change: RAL +374 vs. EFV Weeks Number of Contributing Patients Raltegravir 400 mg BID Efavirenz 770 mg QHS Rockstroh J, et al, 19th IAC; Washington, DC; July 22-27, 2012; Abst. LBPE19.
77 Elvitegravir/Cobicistat/FTC/TDF (Quad) vs. EFV/FTC/TDF (Study ) n=350 Treatment-Naïve Any CD4 count Randomized 1:1 Stratification by HIV-1 RNA (>100,000 c/ml) Quad QD EFV/FTC/TDF QHS Placebo n=350 EFV/FTC/TDF QHS Quad Placebo QD Week 48 Week 192 Primary Endpoint: Proportion with HIV-1 RNA < 50 copies/ml at Week 48 FDA snapshot analysis (ITT), 12% non-inferiority margin Sax P, et al. 19th CROI; Seattle, WA; March 5-8, Abst. 101.
78 Study : Primary Endpoint: HIV-1 RNA < 50 copies/ml +3.6%, 95% CI 3.6 (-1.6% to +8.8%) CD4+ change: Quad +239 vs. EFV +206 c/mm 3 (p=0.009) Sax P, et al. 19th CROI; Seattle, WA; March 5-8, Abst. 101.
79 Elvitegravir/Cobicistat/FTC/TDF (Quad) vs. ATV/r + FTC/TDF (Study ) Multicenter, international, randomized, blinded 192-week study ART-naïve subjects HIV RNA >5,000 c/ml egfr > 70ml/min (N = 708) Stratification by HIV RNA (> or 100,000 c/ml) Quad QD ATV/r + FTC/TDF Placebo QD Baseline: HIV RNA >100,000 c/ml 40-43% CD4 Count cells/mm 3 ATV/r + FTC/TDF QD Quad Placebo QD Week 48 Week 192 Primary Endpoint: Proportion with HIV-1 RNA < 50 c/ml at Week 48 FDA snapshot analysis, 12% non-inferiority margin DeJesus E, et al. 19th CROI; Seattle, WA; March 5-8, Abst. 627.
80 Study : HIV-1 RNA < 50 c/ml Through Week 48 Percent with HIV RNA <50 c/ml (ITT, M=F) QUAD ATV/r Diff: 3.5% (95% CI: -1.0 to 8.0) BL Week 92% 88% HIV RNA <50 c/ml Snapshot Analysis: Quad 90% vs. ATV/r/FTC/TDF 87% (P=NS) Changes in CD4+ count: Quad +207 vs. ATV/r +211 cells/mm 3 (p=0.61) DeJesus E, et al. 19th CROI; Seattle, WA; March 5-8, Abst. 627.
81 Comparisons of First Line Regimens Anchor Drug Anchor Drug Result Efavirenz Lopinavir/r Superior Efavirenz ATV/r Tied Efavirenz RAL Tied Efavirenz Rilpivirine Tied Efavirenz Maraviroc Superior Efavirenz Elvitegravir/cobisistat Tied
82 Slide 82 of 77 A5202: Study Design HIV-1 RNA 1000 c/ml Any CD4+ count > 16 years of age ART-naïve 1857 N=1858 enrolled Arm A B TDF/FTC QD ABC/3TC Placebo QD ABC/3TC QD TDF/FTC Placebo QD EFV QD EFV QD Randomized 1:1:1:1 C TDF/FTC QD ABC/3TC Placebo QD ATV/r QD Stratified by screening HIV-1 RNA (< or 100,000 c/ml) Enrolled Followed through Sept 2009, 96 wks after last pt enrolled D ABC/3TC QD TDF/FTC Placebo QD ATV/r QD
83 Slide 83 of 77 A5202: Time to Virologic Failure in Patients with HIV RNA >100,000 c/ml Probability of No Virologic Failure (%) Probability of No Virologic Failure TDF FTC (26 events) ABC 3TC (57 events) P<0.001, log rank test Hazard ratio, 2.33 (95% CI, ) Weeks since Randomization No. at Risk ABC-3TC TDF-FTC Sax PE, et al. NEJM 2009;361:
84 ABC/3TC vs. TDF/FTC Low Viral Load Stratum Slide 84 of 77 Sax PE, et al. JID 2011: 204:
85 Concerns regarding NRTIs Slide 85 of 77 For individuals with higher viral loads (e.g. >100,000 c/ml) TDF/FTC superior to ABC/3TC) Conflicting results regarding relationship between ABC and CV events TDF associated with greater decline in bone mineral density TDF associated with variable decline in renal function Given rise to preferred regimens of TDF/FTC with ABC/3TC as alternative
86 What Not to Use Guidelines: IAS-USA 1, WHO 2, DHHS 3 Any mono- or dual-therapy combo AZT + 3TC + ABV + FTC (first line) Nelfinavir (first line) ddi + TDF ddi + d4t AZT + d4t ATZ + IDV SQV or DRV or TPV unboosted RIT (full dose therapy) EFV in pregnancy Nevirapine in naïve women CD4>250 or men >400 Etravirine with unboosted PI or with ATZ/r, FOS/r, TPV/r 1 Thompson, et al. JAMA 2010;304:32; 2 Available at: 3 Available at: Revision March 27, 2012.
87 Side Effects and Toxicities
88 Patients Don t Like Surprises: Short-Term Side Effects to Discuss Before Starting Therapy NNRTIs Efavirenz: neuropsychiatric side effects, rash Nevirapine: hepatotoxicity, rash PIs Gastrointestinal toxicity Atazanavir: jaundice and scleral icterus NRTIs Zidovudine: nausea, anemia, fatigue Didanosine: gastrointestinal toxicity, neuropathy, pancreatitis Stavudine: neuropathy, pancreatitis
89 HAART: Long-Term Complications Dyslipidemia/CHD Abnormalities of Body Composition Hepatotoxicity
90 Overview Changing epidemiology of AIDS in the United States Benefits and limitations of HAART When to start What to start with Simplified drug regimens and treatment adherence When to change therapy Second line therapies
91 The Move Toward Simpler 3-Drug Regimens 1996 Didanosine + stavudine + saquinavir 24 pills/dose, 5 doses Saquinavir: 6 q8h with fatty food Didanosine: 2 bid ½ hour ac or 2 hours pc Stavudine: 1 pill bid 2006 Emtricitabine/tenofovir DF + efavirenz (Atripla) 1 pills qd No food restrictions
92 One pill, once a day ART EFV + TDF + FTC (Atripla) RPV +TDF + FTC (Complera) EVG +TDF + FTC + COBI (Stribild) NVP + d4t + 3TC (not available in west)
93 Overview Changing epidemiology of AIDS in United States Benefits and limitations of HAART When to start What to start with Simplified drug regimens and treatment adherence When to change therapy Second line therapies
94 When to Change Therapy? Virologic failure < log reduction in HIV RNA by 4 weeks or <1.0 log reduction by 8 weeks Failure to suppress HIV RNA BLD by 3 months Repeated detection of HIV RNA after suppression BLD Immunologic failure Persistently declining CD 4 cell counts Clinical failure Clinical deterioration or disease progression
95 Why Do Treatment Fail Patients? Poor adherence Baseline resistance or cross-resistance Use of less potent antiretroviral regimens Sequential mono- or dual-therapy Drug levels and drug interactions Tissue reservoir penetration Other, unknown reasons
96 Long-Term Risk of Developing Drug Resistance Risk of developing antiretroviral drug resistance from UK CHIC Study (n=4306) Longitudinal cohort from 6 clinics in London Started antiretroviral therapy with 2 NRTIs plus a third agent Overall risk of treatment failure 38% over 6 years Risk of accumulating resistance mutations to any drug 27% overall Resistance (% patients) Time to Multiclass Resistance classes 3 classes 2 Years 4 Years 6 Years Philips A, et al. Lancet 2007; 370:
97 Overview Changing Epidemiology of AIDS in the United States Benefits and limitations of HAART When to start What to start with Simplified drug regimens and treatment adherence When to change therapy Second line therapies
98 Strategic Therapy Considerations for the Treatment-Experienced Patient HIV drug resistance testing Optimize available treatment options Pharmacokinetic enhancement PK-boosting regimens (ritonavir or cobicistat) Availability of new drugs (and drug classes) Combine as many new drugs as possible Utilize new agents with favorable resistance profiles Maintenance of reduced viral fitness (less critical now) Example: adding lamivudine/emtricitabine or abacavir to maintain M184V mutation
99 Treatment Goals and Challenges Treatment Experienced Patient All patients Zero tolerance for virologic failure ( > 2 VL detectable) At least 2 fully active agents Do we always need 3 fully active agents A boosted PI plus TDF/FTC enough if no TDF resistance There is a balance between complexity of the second regimen with including 3 fully active agents High bar for safety in treatment experienced patients
100 Drug Resistance Testing: Caveats Resistance tests are most accurate in assessing resistance to the current regimen Absence of resistance to a previously used drug does not rule out archived resistant virus that might emerge after reinitiation of that drug Reduced potency should be expected from recycled drugs
101 New Paradigm in Therapy Complete suppression of plasma HIV-1 RNA should be the goal in all patients with HIV given the availability of new drugs Maximize virus suppression while minimizing drug toxicity For those who do not tolerate new agents, goal should be to maintain CD4 count as high as possible Second line therapy should be chosen on the basis of resistance testing, treatment history, tolerability
102 Think Strategically Long-term strategic anti-hiv therapy is similar to a chess game against a vastly superior opponent, in which the objective is to avoid checkmate and remain on the board after 20 years DD Richman, Science 1993
103
104 Clinical Manifestations and Treatment of HIV Questions Ronald Mitsuyasu, MD Professor of Medicine Director, UCLA Center for Clinical AIDS Research University of California, Los Angeles
Combination Anti-Retroviral Therapy (CART) - Rationale and Recommendation. M Dinaker. Fig.1: Effect of CART on CD4 and viral load
 - Rationale and Recommendation. M Dinaker. Fig.1: Effect of CART on CD4 and viral load") Combination Anti-Retroviral Therapy (CART) - Rationale and Recommendation M Dinaker INTRODUCTION The wide availability of effective, safe and mostly well tolerated combined anti-retroviral therapy (CART)
Combination Anti-Retroviral Therapy (CART) - Rationale and Recommendation M Dinaker INTRODUCTION The wide availability of effective, safe and mostly well tolerated combined anti-retroviral therapy (CART)
HIV Update: Epidemiology and Pathophysiology
 HIV Update: Epidemiology and Pathophysiology MATEC Michigan AIDS Research and Education Center Wayne State University School of Medicine (313) 962-2000 matecmichigan.org 1 Epidemiology of the Epidemic:
HIV Update: Epidemiology and Pathophysiology MATEC Michigan AIDS Research and Education Center Wayne State University School of Medicine (313) 962-2000 matecmichigan.org 1 Epidemiology of the Epidemic:
1/26/2015. Epidemiology of the Epidemic: World. Epidemiology of the Epidemic: United States. HIV Update: Epidemiology and Pathophysiology
 HIV Update: Epidemiology and Pathophysiology MATEC Michigan AIDS Research and Education Center Wayne State University School of Medicine (313) 962-2000 matecmichigan.org Epidemiology of the Epidemic: World
HIV Update: Epidemiology and Pathophysiology MATEC Michigan AIDS Research and Education Center Wayne State University School of Medicine (313) 962-2000 matecmichigan.org Epidemiology of the Epidemic: World
Antiretroviral therapy for HIV infection in infants and children: Towards universal access
 Antiretroviral therapy for HIV infection in infants and children: Towards universal access Executive summary of recommendations Preliminary version for program planning 2010 Executive summary Tremendous
Antiretroviral therapy for HIV infection in infants and children: Towards universal access Executive summary of recommendations Preliminary version for program planning 2010 Executive summary Tremendous
The Role of the Primary Care Clinician in HIV Care
 The Role of the Primary Care Clinician in HIV Care Jeffrey Kwong, DNP, ANP-BC, AAHIVS, ACRN, FAANP Columbia University School of Nursing New York, NY New York Nurse Practitioner Association Annual Meeting
The Role of the Primary Care Clinician in HIV Care Jeffrey Kwong, DNP, ANP-BC, AAHIVS, ACRN, FAANP Columbia University School of Nursing New York, NY New York Nurse Practitioner Association Annual Meeting
EACS 2013. Dominique Braun Universitätsspital Zürich
 EACS 2013 Switch data Rilpivirine: Swing-trial Elvitegravir: Flamingo-trial Simplification Dual-Therapy: LPV/r + 3TC in the Gardel-trial Mono-Therapy: Darunavir/r mono in clinical setting Boceprevir/Telaprevir
EACS 2013 Switch data Rilpivirine: Swing-trial Elvitegravir: Flamingo-trial Simplification Dual-Therapy: LPV/r + 3TC in the Gardel-trial Mono-Therapy: Darunavir/r mono in clinical setting Boceprevir/Telaprevir
Generic antiretrovirals in Europe: a blessing or a curse?
 Generic antiretrovirals in Europe: a blessing or a curse? Ricardo Jorge Camacho 1 Molecular Biology Laboratory, Centro Hospitalar de Lisboa Ocidental 2 Instituto de Higiene e Medicina Tropical, Universidade
Generic antiretrovirals in Europe: a blessing or a curse? Ricardo Jorge Camacho 1 Molecular Biology Laboratory, Centro Hospitalar de Lisboa Ocidental 2 Instituto de Higiene e Medicina Tropical, Universidade
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet 02300699 1 tablet daily. Complera 200/25/300 mg tablet 02374129 1 tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ emtricitabine/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ emtricitabine/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ emtricitabine/
Switch to Dolutegravir plus Rilpivirine dual therapy in cart-experienced Subjects: an Italian cohort
 Switch to Dolutegravir plus Rilpivirine dual therapy in cart-experienced Subjects: an Italian cohort Gaetana Sterrantino Azienda Ospedaliero-Universitaria Careggi Infectious diseases, Florence, Italy Background
Switch to Dolutegravir plus Rilpivirine dual therapy in cart-experienced Subjects: an Italian cohort Gaetana Sterrantino Azienda Ospedaliero-Universitaria Careggi Infectious diseases, Florence, Italy Background
Chapter 36. Media Directory. Characteristics of Viruses. Primitive Structure of Viruses. Therapy for Viral Infections. Drugs for Viral Infections
 Chapter 36 Media Directory Drugs for Viral Infections Slide 23 Slide 27 Slide 29 Zidovudine Animation Saquinavir Mesylate Animation Acyclovir Animation Upper Saddle River, New Jersey 07458 All rights reserved.
Chapter 36 Media Directory Drugs for Viral Infections Slide 23 Slide 27 Slide 29 Zidovudine Animation Saquinavir Mesylate Animation Acyclovir Animation Upper Saddle River, New Jersey 07458 All rights reserved.
FARMACI, INNOVAZIONE e INFEZIONE DA HIV / AIDS
 FARMACI, INNOVAZIONE e INFEZIONE DA HIV / AIDS Stefano Vella Dipartimento del Farmaco Istituto Superiore di Sanità - Roma Stages of HIV-1 Life Cycle Targeted by Anti-HIV Drugs In: Gulick RM, Topics HIV
FARMACI, INNOVAZIONE e INFEZIONE DA HIV / AIDS Stefano Vella Dipartimento del Farmaco Istituto Superiore di Sanità - Roma Stages of HIV-1 Life Cycle Targeted by Anti-HIV Drugs In: Gulick RM, Topics HIV
HIV Drug resistanceimplications
 HIV Drug resistanceimplications for therapy Deenan Pillay Africa Centre for Health and Population Studies, UKZN University College London Potential implications of HAART without virological monitoring:
HIV Drug resistanceimplications for therapy Deenan Pillay Africa Centre for Health and Population Studies, UKZN University College London Potential implications of HAART without virological monitoring:
Antiretroviral Drugs in the Treatment and Prevention of HIV Infection
 Antiretroviral Drugs in the Treatment and Prevention of HIV Infection Noga Shalev, MD Uses of Antiretroviral Agents Treatment of chronic HIV infection Prevention of mother-to-child transmission [PMTCT]
Antiretroviral Drugs in the Treatment and Prevention of HIV Infection Noga Shalev, MD Uses of Antiretroviral Agents Treatment of chronic HIV infection Prevention of mother-to-child transmission [PMTCT]
Comprehensive Case Management Reassessment
 Comprehensive Case Management Reassessment Reassessment Date: Date of previous Assessment/Reassessment: Name: Client ID # Address: If Reassessment early or late explain: Current HIV Status: Asymptomatic
Comprehensive Case Management Reassessment Reassessment Date: Date of previous Assessment/Reassessment: Name: Client ID # Address: If Reassessment early or late explain: Current HIV Status: Asymptomatic
Pediatric HIV - The World At It's Best
 VIH/SIDA en Pediatría: Epidemiología Mundial, Transmisión Perinatal, Manejo Integral. Juan Carlos Salazar, M.D. Universidad de Connecticut, EE.UU. End-1998 global estimates Children (
VIH/SIDA en Pediatría: Epidemiología Mundial, Transmisión Perinatal, Manejo Integral. Juan Carlos Salazar, M.D. Universidad de Connecticut, EE.UU. End-1998 global estimates Children (
Theonest Ndyetabura KILIMANJARO CHRISTIAN MEDICAL CENTRE / KILIMANJARO CLINICAL RESERCH
 TREATMENT FAILURE AND PATTERNS OF GENOTYPIC DRUG RESISTANCE MUTATIONS AMONG HAART EXPERIENCED HIV-1 PATIENTS AT KCMC Theonest Ndyetabura KILIMANJARO CHRISTIAN MEDICAL CENTRE / KILIMANJARO CLINICAL RESERCH
TREATMENT FAILURE AND PATTERNS OF GENOTYPIC DRUG RESISTANCE MUTATIONS AMONG HAART EXPERIENCED HIV-1 PATIENTS AT KCMC Theonest Ndyetabura KILIMANJARO CHRISTIAN MEDICAL CENTRE / KILIMANJARO CLINICAL RESERCH
HIV Guidelines. New Strategies.
 HIV Guidelines. New Strategies. Santiago Moreno Hospital Universitario Ramón y Cajal Madrid HIV Guidelines. New Strategies. Outline HIV Guidelines What is new? New strategies Treatment as Prevention HIV
HIV Guidelines. New Strategies. Santiago Moreno Hospital Universitario Ramón y Cajal Madrid HIV Guidelines. New Strategies. Outline HIV Guidelines What is new? New strategies Treatment as Prevention HIV
Chapter 3 South African guidelines and introduction to clinical cases
 Chapter 3 South African guidelines and introduction to clinical cases 3.1. South African national antiretroviral guidelines When this book was published in 2012 the current national antiretroviral treatment
Chapter 3 South African guidelines and introduction to clinical cases 3.1. South African national antiretroviral guidelines When this book was published in 2012 the current national antiretroviral treatment
London Therapeutic Tender Implementation: Guidance for Clinical Use. 4 th June 2014 FINAL
 London Therapeutic Tender Implementation: Guidance for Clinical Use 4 th June 2014 FINAL Contents 3. General principles 4. Financial impact of therapeutic tendering for branded ARVs 5. London ARV algorithm:
London Therapeutic Tender Implementation: Guidance for Clinical Use 4 th June 2014 FINAL Contents 3. General principles 4. Financial impact of therapeutic tendering for branded ARVs 5. London ARV algorithm:
HIV 1. A reference guide for prescription HIV-1 medications
 HIV 1 A reference guide for prescription HIV-1 medications Several different kinds of antiretroviral drugs are currently used to treat HIV-1 infection. These medicines are the ones most commonly used in
HIV 1 A reference guide for prescription HIV-1 medications Several different kinds of antiretroviral drugs are currently used to treat HIV-1 infection. These medicines are the ones most commonly used in
Clinical rationale for viral load testing
 Clinical rationale for viral load testing Francois Venter Wits Reproductive Health & HIV Institute Caveats I m a believer in VLs My talk looks at resource poor environments Why do we need a rationale???
Clinical rationale for viral load testing Francois Venter Wits Reproductive Health & HIV Institute Caveats I m a believer in VLs My talk looks at resource poor environments Why do we need a rationale???
British HIV Association (BHIVA) guidelines for the treatment of HIV-infected adults with antiretroviral therapy (2006)
 guidelines for the treatment of HIV-infected adults with antiretroviral therapy (2006)") r 2006 British HIV Association HIV Medicine (2006), 7, 487 503 British HIV Association (BHIVA) guidelines for the treatment of HIV-infected adults with antiretroviral therapy (2006) B Gazzard on behalf
r 2006 British HIV Association HIV Medicine (2006), 7, 487 503 British HIV Association (BHIVA) guidelines for the treatment of HIV-infected adults with antiretroviral therapy (2006) B Gazzard on behalf
ARV treatment Update 2012. Avondseminarie 18 december 2012 Eric Florence ITG, Antwerpen
 ARV treatment Update 2012 Avondseminarie 18 december 2012 Eric Florence ITG, Antwerpen Three big conferences in 2012 http://retroconference.org/2012/ http://www.aids2012.org/ http://www.hiv11.com/ Current
ARV treatment Update 2012 Avondseminarie 18 december 2012 Eric Florence ITG, Antwerpen Three big conferences in 2012 http://retroconference.org/2012/ http://www.aids2012.org/ http://www.hiv11.com/ Current
Decision Analysis Example
 Options for Doing Cost-Effectiveness Analysis Decision Analysis Example after Occupational Exposure to Clinical trial Mathematical modeling Clinical Trial Incremental Cost-Effectiveness Ratio Conduct a
Options for Doing Cost-Effectiveness Analysis Decision Analysis Example after Occupational Exposure to Clinical trial Mathematical modeling Clinical Trial Incremental Cost-Effectiveness Ratio Conduct a
Treatment Information Service 1 800 HIV 0440 HIV/AIDS. HIV and Its Treatment What You Should Know. 2nd edition
 HIV/AIDS Treatment Information Service 1 800 HIV 0440 HIV and Its Treatment What You Should Know 2nd edition HIV/AIDS TREATMENT INFORMATION SERVICE 2nd Edition HIV and Its Treatment: What You Should Know
HIV/AIDS Treatment Information Service 1 800 HIV 0440 HIV and Its Treatment What You Should Know 2nd edition HIV/AIDS TREATMENT INFORMATION SERVICE 2nd Edition HIV and Its Treatment: What You Should Know
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Treatment 2.0 as a catalyst for Tasp through Drug / Treatment Optimization
 Treatment 2.0 as a catalyst for Tasp through Drug / Treatment Optimization STEFANO VELLA MD ISTITUTO SUPERIORE DI SANITÀ ROME - ITALY DDF 6 WAFAA EL SADR, CROI 2012 The problem is in how to efficiently
Treatment 2.0 as a catalyst for Tasp through Drug / Treatment Optimization STEFANO VELLA MD ISTITUTO SUPERIORE DI SANITÀ ROME - ITALY DDF 6 WAFAA EL SADR, CROI 2012 The problem is in how to efficiently
Management of HIV and TB Co-infection in South Africa
 Management of HIV and TB Co-infection in South Africa Halima Dawood Department of Medicine Case Report 39 yr old female Referred to clinic on 14/06/2006 for consideration to commence antiretroviral therapy
Management of HIV and TB Co-infection in South Africa Halima Dawood Department of Medicine Case Report 39 yr old female Referred to clinic on 14/06/2006 for consideration to commence antiretroviral therapy
HIV and Hepatitis Co-infection. Martin Fisher Brighton and Sussex University Hospitals, UK
 HIV and Hepatitis Co-infection Martin Fisher Brighton and Sussex University Hospitals, UK Useful References British HIV Association 2010 http://www.bhiva.org/documents/guidelines/hepbc/2010/ hiv_781.pdf
HIV and Hepatitis Co-infection Martin Fisher Brighton and Sussex University Hospitals, UK Useful References British HIV Association 2010 http://www.bhiva.org/documents/guidelines/hepbc/2010/ hiv_781.pdf
Safety and Efficacy of DAA + PR in HCV/HIV co-infected patients. Mark Sulkowski, MD Johns Hopkins University Baltimore Maryland USA
 Safety and Efficacy of DAA + PR in HCV/HIV co-infected patients Mark Sulkowski, MD Johns Hopkins University Baltimore Maryland USA Liver disease is the second leading cause of death amongst HIV-positive
Safety and Efficacy of DAA + PR in HCV/HIV co-infected patients Mark Sulkowski, MD Johns Hopkins University Baltimore Maryland USA Liver disease is the second leading cause of death amongst HIV-positive
UPDATE IN HIV POST-EXPOSURE PROPHYLAXIS. Weerawat Manosuthi
 UPDATE IN HIV POST-EXPOSURE PROPHYLAXIS Weerawat Manosuthi Outline Case scenario of postexposure prophylaxis Risks of and how to manage postexposure prophylaxis Current PEP guideline US PHS 2013 New York
UPDATE IN HIV POST-EXPOSURE PROPHYLAXIS Weerawat Manosuthi Outline Case scenario of postexposure prophylaxis Risks of and how to manage postexposure prophylaxis Current PEP guideline US PHS 2013 New York
HBV screening and management in HIV-infected children and adolescents
 HBV screening and management in HIV-infected children and adolescents Linda Aurpibul M.D. Research Institute for Health Sciences, Chiang Mai University 8% HIV and Hepatitis B Co-infection Among Perinatally
HBV screening and management in HIV-infected children and adolescents Linda Aurpibul M.D. Research Institute for Health Sciences, Chiang Mai University 8% HIV and Hepatitis B Co-infection Among Perinatally
What is HIV? What is AIDS? The HIV pandemic HIV transmission Window period Stages of HIV infection
 Module 1 Overview of HIV Infection Purpose Pre-requisite Modules Learning Objectives To provide you with the basic terms and concepts related to HIV infection. None At the end of this module, you will
Module 1 Overview of HIV Infection Purpose Pre-requisite Modules Learning Objectives To provide you with the basic terms and concepts related to HIV infection. None At the end of this module, you will
Routine HIV Monitoring
 Routine HIV Monitoring Guideline of the HIV/AIDS Division at San Francisco General Hospital Statement of Guideline: Patients will be routinely evaluated and monitored for HIV parameters, antiretroviral
Routine HIV Monitoring Guideline of the HIV/AIDS Division at San Francisco General Hospital Statement of Guideline: Patients will be routinely evaluated and monitored for HIV parameters, antiretroviral
Paediatric HIV treatment update
 Paediatric HIV treatment update James Nuttall Red Cross War Memorial Children s Hospital & University of Cape Town ART Resistance & New Treatment Options 6 th FIDSSA Conference, 5-7 November 2015 ART Eligibility
Paediatric HIV treatment update James Nuttall Red Cross War Memorial Children s Hospital & University of Cape Town ART Resistance & New Treatment Options 6 th FIDSSA Conference, 5-7 November 2015 ART Eligibility
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS FOR SEXUAL ASSAULT SURVIVORS. Carl LeBuhn, MD
 NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS FOR SEXUAL ASSAULT SURVIVORS Carl LeBuhn, MD Post-Exposure Prophylaxis (PEP) The use of therapeutic agents to prevent infection following exposure to a pathogen
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS FOR SEXUAL ASSAULT SURVIVORS Carl LeBuhn, MD Post-Exposure Prophylaxis (PEP) The use of therapeutic agents to prevent infection following exposure to a pathogen
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Appendix E-- The CDC s Current and Proposed Classification System for HIV Infection
 Appendix E-- The CDC s Current and Proposed Classification System for HIV Infection The Centers for Disease Control (CDC) has developed a classification system for human immunodeficiency virus (HIV) infection
Appendix E-- The CDC s Current and Proposed Classification System for HIV Infection The Centers for Disease Control (CDC) has developed a classification system for human immunodeficiency virus (HIV) infection
CDC occupation Codes used to code ( map ) facility locations
 facility locations") CDC occupation Codes used to code ( map ) facility locations CDC (occupation) Code BLS SOC (2000)* CDC (occupation) Code BLS SOC (2000)* ATT-Attendant/orderly 31-1012 CLA-Clerical/administrative CNA-Nurse
CDC occupation Codes used to code ( map ) facility locations CDC (occupation) Code BLS SOC (2000)* CDC (occupation) Code BLS SOC (2000)* ATT-Attendant/orderly 31-1012 CLA-Clerical/administrative CNA-Nurse
Consolidated guidelines on the use of antiretroviral drugs for treating
 TB conference, 10-13 June 2014, Durban, South Africa Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection Dr Augustin Ntilivamunda Objectives of 2013 WHO
TB conference, 10-13 June 2014, Durban, South Africa Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection Dr Augustin Ntilivamunda Objectives of 2013 WHO
Estimated New Cases of Leukemia, Lymphoma, Myeloma 2014
 ABOUT BLOOD CANCERS Leukemia, Hodgkin lymphoma (HL), non-hodgkin lymphoma (NHL), myeloma, myelodysplastic syndromes (MDS) and myeloproliferative neoplasms (MPNs) are types of cancer that can affect the
ABOUT BLOOD CANCERS Leukemia, Hodgkin lymphoma (HL), non-hodgkin lymphoma (NHL), myeloma, myelodysplastic syndromes (MDS) and myeloproliferative neoplasms (MPNs) are types of cancer that can affect the
July 3, 2015. III. VA policy:
 Antiretroviral Postexposure Prophylaxis After Sexual, Injection- Drug Use, or Other Nonoccupational Exposure to HIV (nonoccupational post- exposure prophylaxis [npep]) VA Greater Los Angeles Healthcare
Antiretroviral Postexposure Prophylaxis After Sexual, Injection- Drug Use, or Other Nonoccupational Exposure to HIV (nonoccupational post- exposure prophylaxis [npep]) VA Greater Los Angeles Healthcare
Long-term Results of Pegylated Interferon alfa-2a and Tenofovir for Hepatitis B
 Long-term Results of Pegylated Interferon alfa-2a and Tenofovir for Hepatitis B Patrick Marcellin Viral Hepatitis Research Center Hôpital Beaujon, University of Paris France OBJECTIVES OF THERAPY IN CHRONIC
Long-term Results of Pegylated Interferon alfa-2a and Tenofovir for Hepatitis B Patrick Marcellin Viral Hepatitis Research Center Hôpital Beaujon, University of Paris France OBJECTIVES OF THERAPY IN CHRONIC
Antiretroviral Therapy for HIV Infection: When to Initiate Therapy, Which Regimen to Use, and How to Monitor Patients on Therapy
 Perspective Antiretroviral Therapy for HIV Infection: When to Initiate Therapy, Which Regimen to Use, and How to Monitor Patients on Therapy Antiretroviral therapy is recommended for all patients with
Perspective Antiretroviral Therapy for HIV Infection: When to Initiate Therapy, Which Regimen to Use, and How to Monitor Patients on Therapy Antiretroviral therapy is recommended for all patients with
Preferred Regimens as recommended by DHHS guidelines (listed by class) strength of evidence = A1
 strength of evidence = A1") Recommendations for Use of Antiretroviral Regimens in HIV-infected Treatment-naïve Veterans March 2013 VHA Pharmacy Benefits Management Services, the Medical Advisory Panel, VISN Pharmacist Executives,
Recommendations for Use of Antiretroviral Regimens in HIV-infected Treatment-naïve Veterans March 2013 VHA Pharmacy Benefits Management Services, the Medical Advisory Panel, VISN Pharmacist Executives,
Management of HIV/HCV Co-infected Patients
 Management of HIV/HCV Co-infected Patients David Wyles, MD Associate Professor of Medicine Division of Infectious Diseases University of California, San Diego San Diego, California Disclosures Grants/Research
Management of HIV/HCV Co-infected Patients David Wyles, MD Associate Professor of Medicine Division of Infectious Diseases University of California, San Diego San Diego, California Disclosures Grants/Research
Presented by: Canadian Working Group on HIV and Rehabilitation
 Rehabilitation in the Context of HIV: An Interprofessional Course for Occupational Therapists, Physiotherapists, Speech-Language Pathologists and Audiologists Presented by: Canadian Working Group on HIV
Rehabilitation in the Context of HIV: An Interprofessional Course for Occupational Therapists, Physiotherapists, Speech-Language Pathologists and Audiologists Presented by: Canadian Working Group on HIV
The treatment of HIV is currently focused on drug
 Vol 1 October 2009 Clinical Pharmacist 393 Since the advent of combination antiretroviral therapy in the mid-1990s HIV-infected individuals are now living longer with improved quality of life. Medication
Vol 1 October 2009 Clinical Pharmacist 393 Since the advent of combination antiretroviral therapy in the mid-1990s HIV-infected individuals are now living longer with improved quality of life. Medication
Highlights in HIV Medicine for Internists
 Highlights in HIV Medicine for Internists Charurut Somboonwit,MD,FACP Associate Professor Division of Infectious Diseases and International Mdii Medicine Morsani College of Medicine Disclosure Speaker
Highlights in HIV Medicine for Internists Charurut Somboonwit,MD,FACP Associate Professor Division of Infectious Diseases and International Mdii Medicine Morsani College of Medicine Disclosure Speaker
In Tanzania, ARVs were introduced free-of-charge by the government in 2004 and, by July 2008, almost 170,000 people were receiving the drugs.
 ANTIRETROVIRAL TREATMENT What is ART and ARV? ART is a short form for Antiretroviral Therapy (or Treatment). Antiretroviral therapy is a treatment consisting of a combination of drugs which work against
ANTIRETROVIRAL TREATMENT What is ART and ARV? ART is a short form for Antiretroviral Therapy (or Treatment). Antiretroviral therapy is a treatment consisting of a combination of drugs which work against
Reference: NHS England B06/P/a
 Clinical Commissioning Policy: Dolutegravir for treatment of HIV- 1 in adults and adolescents Reference: NHS England B06/P/a 1 NHS England Clinical Commissioning Policy: Dolutegravir for treatment of HIV-1
Clinical Commissioning Policy: Dolutegravir for treatment of HIV- 1 in adults and adolescents Reference: NHS England B06/P/a 1 NHS England Clinical Commissioning Policy: Dolutegravir for treatment of HIV-1
Antiretroviral Treatment
 Antiretroviral Treatment Michael A. Tolle, MD, MPH Heidi Schwarzwald, MD, MPH Nancy R. Calles, MSN, PNP, ACRN, MPH Objectives 1. Discuss the goals of treatment for human immunodeficiency virus (HIV) infection.
Antiretroviral Treatment Michael A. Tolle, MD, MPH Heidi Schwarzwald, MD, MPH Nancy R. Calles, MSN, PNP, ACRN, MPH Objectives 1. Discuss the goals of treatment for human immunodeficiency virus (HIV) infection.
Diagnosis and Treatment of Common Oral Lesions Causing Pain
 Diagnosis and Treatment of Common Oral Lesions Causing Pain John D. McDowell, DDS, MS University of Colorado School of Dentistry Chair, Oral Diagnosis, Medicine and Radiology Director, Oral Medicine and
Diagnosis and Treatment of Common Oral Lesions Causing Pain John D. McDowell, DDS, MS University of Colorado School of Dentistry Chair, Oral Diagnosis, Medicine and Radiology Director, Oral Medicine and
HIV/AIDS. HIV- Human Immunodeficiency Virus. AIDS immume system severely damaged
 HIV/AIDS HIV- Human Immunodeficiency Virus Person is infected with virus. May have no s/s (but may transmit virus) More common to have brief flu-like illness 2-6 wks after becoming infected (swollen lymph
HIV/AIDS HIV- Human Immunodeficiency Virus Person is infected with virus. May have no s/s (but may transmit virus) More common to have brief flu-like illness 2-6 wks after becoming infected (swollen lymph
HIV and Hepatitis B CoInfection
 HIV and Hepatitis B CoInfection Douglas G. Fish, MD June 3, 2014 44 yo male with AIDS who had fallen out of care and returned in October 2013 Last seen in November 2012 CD4 at that time 340 cells/cmm HIV
HIV and Hepatitis B CoInfection Douglas G. Fish, MD June 3, 2014 44 yo male with AIDS who had fallen out of care and returned in October 2013 Last seen in November 2012 CD4 at that time 340 cells/cmm HIV
Hepatitis B and C Co-infection. Mark Hull MHSc, FRCPC Clinical Assistant Professor Division of AIDS
 Hepatitis B and C Co-infection Mark Hull MHSc, FRCPC Clinical Assistant Professor Division of AIDS Objectives Review natural history of hepatitis coinfection Brief overview of treatment indications for
Hepatitis B and C Co-infection Mark Hull MHSc, FRCPC Clinical Assistant Professor Division of AIDS Objectives Review natural history of hepatitis coinfection Brief overview of treatment indications for
Understanding Pharmacokinetic Variability and Managing Drug Interactions
 Understanding Pharmacokinetic Variability and Managing Drug Interactions Courtney V. Fletcher, Pharm.D. Dean, College of Pharmacy Professor, Department of Pharmacy Practice and Division of Infectious Diseases
Understanding Pharmacokinetic Variability and Managing Drug Interactions Courtney V. Fletcher, Pharm.D. Dean, College of Pharmacy Professor, Department of Pharmacy Practice and Division of Infectious Diseases
Core Competencies: HIV/AIDS: HIV Basics HIV/AIDS JEOPARDY* Overview. To change category names: Instructions. 2. Introduce session.
 Core Competencies: HIV/AIDS: HIV Basics HIV/AIDS JEOPARDY* ABOUT THIS ACTIVITY Time: 60 minutes Objectives: By the end of this session, participants will be able to: Reviewed their knowledge of HIV/AIDS
Core Competencies: HIV/AIDS: HIV Basics HIV/AIDS JEOPARDY* ABOUT THIS ACTIVITY Time: 60 minutes Objectives: By the end of this session, participants will be able to: Reviewed their knowledge of HIV/AIDS
Hepatitis Update. Study 110: SVR at post-treatment week 24 (SVR24) Jürgen Rockstroh, MD. No ART EFV/TDF/FTC ART/r/TDF/FTC Total
 Jürgen Rockstroh, MD. No ART EFV/TDF/FTC ART/r/TDF/FTC Total") Hepatitis Update Jürgen Rockstroh, MD Study 11: SVR at post-treatment week 24 (SVR24) Patients with Undetectable HCV RNA (Percentage) 8 7 6 5 4 3 2 1 71 No ART EFV/TDF/FTC ART/r/TDF/FTC Total 69 8 74 n/n
Hepatitis Update Jürgen Rockstroh, MD Study 11: SVR at post-treatment week 24 (SVR24) Patients with Undetectable HCV RNA (Percentage) 8 7 6 5 4 3 2 1 71 No ART EFV/TDF/FTC ART/r/TDF/FTC Total 69 8 74 n/n
Protease Inhibitor Resistance at 2nd-line HIV Treatment Failure in Sub-Saharan Africa
 Protease Inhibitor Resistance at 2nd-line HIV Treatment Failure in Sub-Saharan Africa T. Sonia Boender; Raph L. Hamers; Pascale Ondoa; Maureen Wellington; Cleophas Chimbetete; Margaret Siwale; Eman E F
Protease Inhibitor Resistance at 2nd-line HIV Treatment Failure in Sub-Saharan Africa T. Sonia Boender; Raph L. Hamers; Pascale Ondoa; Maureen Wellington; Cleophas Chimbetete; Margaret Siwale; Eman E F
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2013
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2013 VERSION 14 March 2013 Contents Acronym glossary... 2 1. Goals of the programme... 3 2. Objectives... 3 3. Specific Objectives... 3 4. Adults and
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2013 VERSION 14 March 2013 Contents Acronym glossary... 2 1. Goals of the programme... 3 2. Objectives... 3 3. Specific Objectives... 3 4. Adults and
Meeting Report 15 th PK Workshop, Washington, 2014 Produced by www.hiv-druginteractions.org
 Page 1 of 7 HIV Interaction Studies presented at the 15 th International Workshop on Clinical Pharmacology of HIV and HCV Therapy, Washington, April 2014. This report summarises interaction studies relating
Page 1 of 7 HIV Interaction Studies presented at the 15 th International Workshop on Clinical Pharmacology of HIV and HCV Therapy, Washington, April 2014. This report summarises interaction studies relating
Frequently Asked Questions: Pre-Exposure Prophylaxis (PrEP) for HIV Infection Massachusetts Department of Public Health Updated July 2013
 for HIV Infection Massachusetts Department of Public Health Updated July 2013") Frequently Asked Questions: Pre-Exposure Prophylaxis (PrEP) for HIV Infection Massachusetts Department of Public Health Updated July 2013 On July 16, 2012, the Food and Drug Administration (FDA) approved
Frequently Asked Questions: Pre-Exposure Prophylaxis (PrEP) for HIV Infection Massachusetts Department of Public Health Updated July 2013 On July 16, 2012, the Food and Drug Administration (FDA) approved
The question and answer session is not available after the live webinar.
 1 Read verbatim. 2 The Infectious Diseases Society of America (IDSA) Hepatitis C Knowledge Network offers monthly, 1 hour webinars to educate IDSA members on current recommended practices and treatments
1 Read verbatim. 2 The Infectious Diseases Society of America (IDSA) Hepatitis C Knowledge Network offers monthly, 1 hour webinars to educate IDSA members on current recommended practices and treatments
The Basics of Drug Resistance:
 CONTACT: Lisa Rossi +1-412-641-8940 +1-412- 916-3315 (mobile) rossil@upmc.edu The Basics of Drug Resistance: QUESTIONS AND ANSWERS HIV Drug Resistance and ARV-Based Prevention 1. What is drug resistance?
CONTACT: Lisa Rossi +1-412-641-8940 +1-412- 916-3315 (mobile) rossil@upmc.edu The Basics of Drug Resistance: QUESTIONS AND ANSWERS HIV Drug Resistance and ARV-Based Prevention 1. What is drug resistance?
Pharmacoprevention. HIV-drugs for prevention. Instituut Tropische Geneeskunde, Antwerpen
 Pharmacoprevention HIV-drugs for prevention Instituut Tropische Geneeskunde, Antwerpen Introduction Afkortingskunde: What s in a name/ abbreviation? PEP PrEP TASP PMTCT Introduction PEP: Post-Exposure
Pharmacoprevention HIV-drugs for prevention Instituut Tropische Geneeskunde, Antwerpen Introduction Afkortingskunde: What s in a name/ abbreviation? PEP PrEP TASP PMTCT Introduction PEP: Post-Exposure
Cancer Screening. Robert L. Robinson, MD, MS. Ambulatory Conference SIU School of Medicine Department of Internal Medicine.
 Cancer Screening Robert L. Robinson, MD, MS Ambulatory Conference SIU School of Medicine Department of Internal Medicine March 13, 2003 Why screen for cancer? Early diagnosis often has a favorable prognosis
Cancer Screening Robert L. Robinson, MD, MS Ambulatory Conference SIU School of Medicine Department of Internal Medicine March 13, 2003 Why screen for cancer? Early diagnosis often has a favorable prognosis
B.C. HIV/AIDS Drug Treatment Program
 B.C. HIV/AIDS Drug Treatment Program Monthly Report January 215 215 BC Centre for Excellence in HIV/AIDS DISCLAIMER: This document is published by the British Columbia Centre for Excellence in HIV/AIDS
B.C. HIV/AIDS Drug Treatment Program Monthly Report January 215 215 BC Centre for Excellence in HIV/AIDS DISCLAIMER: This document is published by the British Columbia Centre for Excellence in HIV/AIDS
GENERAL INSTRUCTIONS FOR COMPLETING THE HIV TEST FORM
 GENERA INSTRUCTIONS FOR COMPETING THE This form is designed to be read by an Optical Character Recognition (OCR) scanner. The legibility of this form depends on the quality of the a hand written and selected
GENERA INSTRUCTIONS FOR COMPETING THE This form is designed to be read by an Optical Character Recognition (OCR) scanner. The legibility of this form depends on the quality of the a hand written and selected
HIV/AIDS: Controversies 2008-10
 HIV/AIDS: Controversies 2008-10 1. Prevention 2. Treatment Josep M Gatell Hospital Clinic. Barcelona. gatell0@attglobal.net AIDS: year 2008-10 AIDS is a STD and a world wide epidemy (sub-saharan Africa,
HIV/AIDS: Controversies 2008-10 1. Prevention 2. Treatment Josep M Gatell Hospital Clinic. Barcelona. gatell0@attglobal.net AIDS: year 2008-10 AIDS is a STD and a world wide epidemy (sub-saharan Africa,
Frequently Asked Questions (FAQs)
") Frequently Asked Questions (FAQs) Research Rationale 1. What does PrEP stand for? There is scientific evidence that antiretroviral (anti-hiv) medications may be able to play an important role in reducing
Frequently Asked Questions (FAQs) Research Rationale 1. What does PrEP stand for? There is scientific evidence that antiretroviral (anti-hiv) medications may be able to play an important role in reducing
Covered California s 2016 Formularies
 Covered California s 2016 Formularies An analysis of the drugs per tier in all 12 health plans that are available for treating and preventing HIV (pp 1 24) and for treating hepatitis B (pp 26 37) and hepatitis
Covered California s 2016 Formularies An analysis of the drugs per tier in all 12 health plans that are available for treating and preventing HIV (pp 1 24) and for treating hepatitis B (pp 26 37) and hepatitis
Die Toronto Konferenz. K. Arasteh Auguste-Viktoria-Klinikum
 Die Toronto Konferenz K. Arasteh Auguste-Viktoria-Klinikum Subjektive Schwerpunkte Medizinische Prävention Monotherapie CD4 guided treatment interuption (CD4-TI) HIV Prävention (Gita Ramjee) Rationale
Die Toronto Konferenz K. Arasteh Auguste-Viktoria-Klinikum Subjektive Schwerpunkte Medizinische Prävention Monotherapie CD4 guided treatment interuption (CD4-TI) HIV Prävention (Gita Ramjee) Rationale
Drug Treatment Program Update
 Drug Treatment Program Update As of May 211 Drug Treatment Program Update A key component of the Centre s mandate is to monitor the impact of HIV/AIDS on British Columbia. The Centre provides essential
Drug Treatment Program Update As of May 211 Drug Treatment Program Update A key component of the Centre s mandate is to monitor the impact of HIV/AIDS on British Columbia. The Centre provides essential
POSTEXPOSURE PROPHYLAXIS
 POSTEXPOSURE PROPHYLAXIS Bloodborne viruses Hepatitis B Hepatitis C HIV Hepatitis B Risk of seroconversion HBeAg negative 2% HBeAg positive 20-40% If seroconvert most recover completely and develop immunity
POSTEXPOSURE PROPHYLAXIS Bloodborne viruses Hepatitis B Hepatitis C HIV Hepatitis B Risk of seroconversion HBeAg negative 2% HBeAg positive 20-40% If seroconvert most recover completely and develop immunity
Guideline. Treatment of tuberculosis in patients with HIV co-infection. Version 3.0
 Guideline Treatment of tuberculosis in patients with HIV co-infection Version 3.0 Key critical points Co-infection with Tuberculosis (TB) and HIV is common in many parts of the world, especially sub-saharan
Guideline Treatment of tuberculosis in patients with HIV co-infection Version 3.0 Key critical points Co-infection with Tuberculosis (TB) and HIV is common in many parts of the world, especially sub-saharan
HIV/Hepatitis C co-infection. Update on treatment Eoin Feeney
 HIV/Hepatitis C co-infection Update on treatment Eoin Feeney HIV/Hepatitis C coinfection Where we are now Current treatment regimens and outcomes What s coming soon Direct acting antivirals (DAAs) What
HIV/Hepatitis C co-infection Update on treatment Eoin Feeney HIV/Hepatitis C coinfection Where we are now Current treatment regimens and outcomes What s coming soon Direct acting antivirals (DAAs) What
Clinical Indicator Ages 19-29 Ages 30-39 Ages 40-49 Ages 50-64 Ages 65+ Frequency of visit as recommended by PCP
 SCREENING EXAMINATION & COUNSELING UPMC Health Plan Clinical Indicator Ages 19-29 Ages 30-39 Ages 40-49 Ages 50-64 Ages 65+ Annually Physical Exam and Counseling 1 Blood Pressure 2 At each visit. At least
SCREENING EXAMINATION & COUNSELING UPMC Health Plan Clinical Indicator Ages 19-29 Ages 30-39 Ages 40-49 Ages 50-64 Ages 65+ Annually Physical Exam and Counseling 1 Blood Pressure 2 At each visit. At least
Mutations: 2 general ways to alter DNA. Mutations. What is a mutation? Mutations are rare. Changes in a single DNA base. Change a single DNA base
 Mutations Mutations: 2 general ways to alter DNA Change a single DNA base Or entire sections of DNA can move from one place to another What is a mutation? Any change in the nucleotide sequence of DNA Here
Mutations Mutations: 2 general ways to alter DNA Change a single DNA base Or entire sections of DNA can move from one place to another What is a mutation? Any change in the nucleotide sequence of DNA Here
DOI: 10.1111/hiv.12119 2014 British HIV Association HIV Medicine (2014), 15 (Suppl. 1), 1 85
, 15 (Suppl. 1), 1 85") DOI: 10.1111/hiv.12119 British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2012 (Updated November 2013. All changed text is cast in yellow highlight.)
DOI: 10.1111/hiv.12119 British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2012 (Updated November 2013. All changed text is cast in yellow highlight.)
PSA Testing 101. Stanley H. Weiss, MD. Professor, UMDNJ-New Jersey Medical School. Director & PI, Essex County Cancer Coalition. weiss@umdnj.
 PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2015
 2015 British HIV Association British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2015 NHS Evidence has accredited the process used by the British HIV
2015 British HIV Association British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2015 NHS Evidence has accredited the process used by the British HIV
Case Finding for Hepatitis B and Hepatitis C
 Case Finding for Hepatitis B and Hepatitis C John W. Ward, M.D. Division of Viral Hepatitis Centers for Disease Control and Prevention Atlanta, Georgia, USA Division of Viral Hepatitis National Center
Case Finding for Hepatitis B and Hepatitis C John W. Ward, M.D. Division of Viral Hepatitis Centers for Disease Control and Prevention Atlanta, Georgia, USA Division of Viral Hepatitis National Center
OUTLINE POST EXPOSURE PROPHYLAXIS (PEP) OCCUPATIONAL RISK OF VIRAL TRANSMISSION WITH SHARP INJURY FROM INFECTED SOURCE:
 OCCUPATIONAL RISK OF VIRAL TRANSMISSION WITH SHARP INJURY FROM INFECTED SOURCE:") Professional needle stick accidents should be dealt with within 48 hours. An ARC (Aids Reference Centre) or an emergency department must be contacted as soon as possible. OUTLINE POST EXPOSURE PROPHYLAXIS
Professional needle stick accidents should be dealt with within 48 hours. An ARC (Aids Reference Centre) or an emergency department must be contacted as soon as possible. OUTLINE POST EXPOSURE PROPHYLAXIS
HIV/AIDS Care: The Diagnosis Code Series 2. Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer
 HIV/AIDS Care: The Diagnosis Code Series 2 Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer Learning Outcomes Identify and explain the difference between ICD-9-CM
HIV/AIDS Care: The Diagnosis Code Series 2 Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer Learning Outcomes Identify and explain the difference between ICD-9-CM
Prevalenza HIV/HCV in Italia
 Prevalence of HIV/HCV co-infection by region, 2013 WHO global systematic review of prevalence of HIV/HCV Ab co-infection based on prevalence studies in HIV+ persons stratified by risk group (where available)
Prevalence of HIV/HCV co-infection by region, 2013 WHO global systematic review of prevalence of HIV/HCV Ab co-infection based on prevalence studies in HIV+ persons stratified by risk group (where available)
CIBMTR Infection Data and the New Infection Inserts.
 CIBMTR Infection Data and the New Infection Inserts. Marcie Tomblyn, MD, MS Scientific Director, CIBMTR Infection and Immune Reconstitution Working Committee Overview Indication for expanded data collection
CIBMTR Infection Data and the New Infection Inserts. Marcie Tomblyn, MD, MS Scientific Director, CIBMTR Infection and Immune Reconstitution Working Committee Overview Indication for expanded data collection
Cytoreductive Therapy for Autologous Cell Therapy in HIV
 Cytoreductive Therapy for Autologous Cell Therapy in HIV Ronald Mitsuyasu, MD Professor of Medicine UCLA Center for Clinical AIDS Research and Education (CARE Center) HSC Transfer from CCR5-delta 32 Donor
Cytoreductive Therapy for Autologous Cell Therapy in HIV Ronald Mitsuyasu, MD Professor of Medicine UCLA Center for Clinical AIDS Research and Education (CARE Center) HSC Transfer from CCR5-delta 32 Donor
William Atkinson, MD, MPH Hepatitis B Vaccine Issues June 16, 2016
 William Atkinson, MD, MPH Hepatitis B Vaccine Issues June 16, 2016 Advisory Committee on Immunization Practices (ACIP) The recommendations to be discussed are primarily those of the ACIP composed of 15
William Atkinson, MD, MPH Hepatitis B Vaccine Issues June 16, 2016 Advisory Committee on Immunization Practices (ACIP) The recommendations to be discussed are primarily those of the ACIP composed of 15
HEPATITIS WEB STUDY Acute Hepatitis C Virus Infection: Epidemiology, Clinical Features, and Diagnosis
 HEPATITIS WEB STUDY Acute C Virus Infection: Epidemiology, Clinical Features, and Diagnosis H. Nina Kim, MD Assistant Professor of Medicine Division of Infectious Diseases University of Washington School
HEPATITIS WEB STUDY Acute C Virus Infection: Epidemiology, Clinical Features, and Diagnosis H. Nina Kim, MD Assistant Professor of Medicine Division of Infectious Diseases University of Washington School
Screening for Cancer in Light of New Guidelines and Controversies. Christopher Celio, MD St. Jude Heritage Medical Group
 Screening for Cancer in Light of New Guidelines and Controversies Christopher Celio, MD St. Jude Heritage Medical Group Screening Tests The 2 major objectives of a good screening program are: (1) detection
Screening for Cancer in Light of New Guidelines and Controversies Christopher Celio, MD St. Jude Heritage Medical Group Screening Tests The 2 major objectives of a good screening program are: (1) detection
Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64
 Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64 1. BMI - Documented in patients medical record on an annual basis. Screen for obesity and offer intensive counseling and behavioral
Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64 1. BMI - Documented in patients medical record on an annual basis. Screen for obesity and offer intensive counseling and behavioral
HIV/HCV Co-Infection
 HIV/HCV Co-Infection 2015 Kentucky Conference on Viral Hepatitis Matt Cave, M.D. Associate Professor Department of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of Pharmacology
HIV/HCV Co-Infection 2015 Kentucky Conference on Viral Hepatitis Matt Cave, M.D. Associate Professor Department of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of Pharmacology
cancer cancer Hessamfar-Bonarek M et al. Int. J. Epidemiol. 2010;39:135-146
 Hematopoietic Stem Cell Transplant in HIV- related lymphoma Song Zhao, MD PhD Hematology-Oncology Program University of Washington/FHCRC Underlying Causes of Death in HIV-infected Adults 2000 2005 cancer
Hematopoietic Stem Cell Transplant in HIV- related lymphoma Song Zhao, MD PhD Hematology-Oncology Program University of Washington/FHCRC Underlying Causes of Death in HIV-infected Adults 2000 2005 cancer
Clinical Commissioning Policy: Stribild for the treatment of HIV-1 infection in adults
 Clinical Commissioning Policy: Stribild for the treatment of HIV-1 infection in adults Reference: NHS England B06/P/x 1 Clinical Commissioning Policy: Stribild for the treatment of HIV-1 infection in adults
Clinical Commissioning Policy: Stribild for the treatment of HIV-1 infection in adults Reference: NHS England B06/P/x 1 Clinical Commissioning Policy: Stribild for the treatment of HIV-1 infection in adults
Aktuell HIV-forskning 2014-05-06
 Aktuell HIV-forskning 2014-05-06 Alexey Kashpersky Aktuell HIV-forskning Bot Smittsamhet Nya läkemedel HIV och åldrande Etc HPTN 052 Prevention Conclusion Early ART that suppresses viral replication led
Aktuell HIV-forskning 2014-05-06 Alexey Kashpersky Aktuell HIV-forskning Bot Smittsamhet Nya läkemedel HIV och åldrande Etc HPTN 052 Prevention Conclusion Early ART that suppresses viral replication led
HIV Case Conference: HIV Associated Lymphoma
 F/C AETC Faculty General HIV Tuesday, July 22, 2014 12:30 1:30pm (EDT) Facilitator Todd S. Wills, MD University of South Florida Didactic Presenter Jose Castro, MD University of Miami Case Discussant(s)
F/C AETC Faculty General HIV Tuesday, July 22, 2014 12:30 1:30pm (EDT) Facilitator Todd S. Wills, MD University of South Florida Didactic Presenter Jose Castro, MD University of Miami Case Discussant(s)
HEPATITIS COINFECTIONS
 HEPATITIS COINFECTIONS Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Disclosures (Activity w/i 12 months)
HEPATITIS COINFECTIONS Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Disclosures (Activity w/i 12 months)
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 TB in the HIV Patient Lisa Armitige, MD, PhD November 13, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas November 11 14, 2014 TB in the HIV Patient Lisa Armitige, MD, PhD November 13, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
HIV Post Exposure Prophylaxis Update
 HIV Post Exposure Prophylaxis Update Mary Goodspeed, RN, BS 716-898-4713 Coordinator, HIV Clinical Education Initiative Erie County Medical Center, Buffalo, NY PEP Hotline 1-888-448-4911 www.aidscenterecmc.org
HIV Post Exposure Prophylaxis Update Mary Goodspeed, RN, BS 716-898-4713 Coordinator, HIV Clinical Education Initiative Erie County Medical Center, Buffalo, NY PEP Hotline 1-888-448-4911 www.aidscenterecmc.org