Management of secondary headaches WCN 2013
|
|
|
- Antonia Miller
- 7 years ago
- Views:
Transcription
1 Management of secondary headaches WCN 2013 Rigmor Højland Jensen Danish Headache Centre, Department of Neurology, Glostrup Hospital, University of Copenhagen, Denmark Disclosures: Lectures for Pfizer, Berlin-Chemie, Allergan, Merck Member of advisory boards in: ATI, Medotech, Neurocore, and Linde Gas ltd. Director in LTB, EHMTIC and President in EHF

2 Headache Care: Organization of Headache Service Level 3: Specialized headache centres - Both inpatient and outpatient treatment - Multidisciplinary treatment - Education - Research - Organisation of networks with levels 1 and 2 Level 2: Special Interest Headache Care Secondary care or primary care with special interest in headache disorders - Completion of special training - Fulfills national guidelines and requirements for special headache/pain therapy Kommentare H. Göbel Level 1: General Primary Care Primary care without special interest in headache disorders -Following treatment guidelines -Selecting patients for higher levels (gate-keeper function) -Long-term care after discharge from levels 2 and 3

3 International Headache Classification, (ICHD- III beta 2013) IHCD-II 14 subgroups Group 1-4 Primary headaches Group 5 12 Secondary headaches Group Cranial neuralgias, etc Migraine Tension-type headache, Cluster headache? Medication Trauma, stroke, Neoplastic and systemic disorders Trigeminal neuralgia, Other cranial neuralgia and Facial pain disorders

4 WHAT IS A SECONDARY HEADACHE? Etiology based, not symptom based as the primary headaches Standard Secondary Headache Diagnostic Criteria in ICHD III A. Any headache fulfilling criterion C B. Another disorder scientifically documented to be able to cause headache has been diagnosed C. Evidence of causation demonstrated by at least two of the following: 1. headache has developed in temporal relation to the onset of the presumed causative disorder 2. one or both of the following: a. headache has significantly worsened in parallel with worsening of the presumed causative disorder b. headache has significantly improved in parallel with improvement of the presumed causative disorder 3. headache has characteristics typical for the causative disorder 4. other evidence exists of causation D. Not better accounted for by another ICHD-III diagnosis.

5 Edition (ICHD III) Basic Organization Part 1: Primary headaches, chapters 1-4 (no other causative disorder) 1. Migraine 2. Tension-type Headache 3. Trigeminal Autonomic Cephalalgias 4. Other primary headaches Part 2: Secondary headaches 5. Posttraumatic 6. Vascular disease 7. Other intracranial pathology 8. Substances 9. CNS infection 10. Homeostatic disorders 11. Cranium, Neck, Eyes, ENT, Sinuses, Mouth, Teeth, TMJ 12. Psychiatric Part 3: Cranial Neuralgias and other facial pain 13. Neuralgias and neuropathy Appendix

6 5. Headache attributed to head trauma DANISH HEADACHE CENTER

7 5.2.2 Persistent post-traumatic headache attributed to mild head injury Headache of any type, fulfilling criteria C and D Head trauma with all of the following: Either no loss of consciousness, or loss of consciousness of <30 minutes duration Glasgow Coma Scale (GCS)?<13 Post-traumatic amnesia2? 24 hours in duration Alteration in consciousness?c24 hours in duration - Symptoms and/or signs diagnostic of mild traumatic brain injury, manifest by?õ1 of the following immediately following the head injury: > Transient confusion, disorientation, or impaired consciousness > Loss of memory for events immediately before or after injury > Other neurologic deficits Evidence of causation shown by: Headache develops within 7 days after head trauma Headache persists for >3 months after head trauma Headache is not better accounted for by another headache diagnosis

8 Management of Posttraumatic headache Mild Moderate Severe?? Persistent TTH-like headache with photo-and phonophobia associated with cognitive symptoms No known mechanisms and pharmacological RCT s Clinical practise: Acute attacks: Limited effect of analgesics and MOH-risk Preventives most relevant: Amitriptyline start low and go slow Migraine Preventives (betablockers, antiepileptics) Psychological counseling: Cognitive Behavioural Treatment, Relaxation and Biofeedback Reassuring
 Psychological")
9
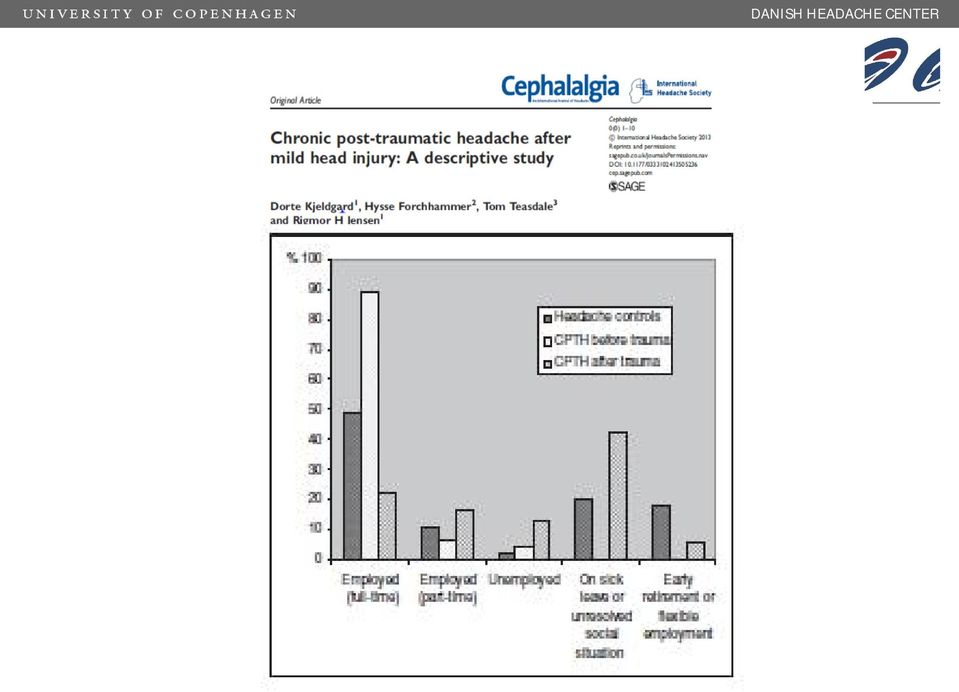
10 Quality of Life and Functioning in posttraumatic headache (Kjeldgaard et al 2013)

11 Conclusion: Posttraumatic headache Symptomatic treatment with unspecific migraine preventives Low dose amitriptyline has a positive effect on headache and sleep but RCT s are lacking Psychological support, CBT and relaxation may be beneficial but evidence is scarce Mechanisms based treatment and new drugs targets are needed

12 DANISH HEADACHE CENTER Idiopathic Intracranial Hypertension ICHD-III Classification Criteria 1. Alert patient with neurological examination that is normal or demonstrates any of the following abnormalities: a) papilledema b) enlarged blind spot c) visual field defect (progressive if untreated) d) sixth nerve palsy 2. Increased CSF pressure (>250 mm H2O) measured by lumbar puncture or by epidural or intraventricular pressure monitoring 3. Normal CSF chemistry (low CSF protein is acceptable) and cellularity 4. Intracranial diseases ruled out by appropriate investigations 5. No metabolic, toxic or hormonal cause of intracranial hypertension Glostrup Hospital, the Capital Region of Denmark
 and cellularity 4. Intracranial diseases ruled out by appropriate investigations 5.")
13 Background and signs of IIH progressive permanent visual loss obese?o headache papilledema

14 MR findings 25 IIH-patients and 25 controls Most sensitive findings: Empty sella and nerve sheat distension = most reliable signs. Posterior globe flattening: specific but not sensitive. No changes in lateral ventricles (+VBM) and no relation to clinical presentations. Jan Hoffmann et al Cephalalgia 2013
 and no relation to clinical")
15 OPTICAL COHERENCE TOMOGRAPHY
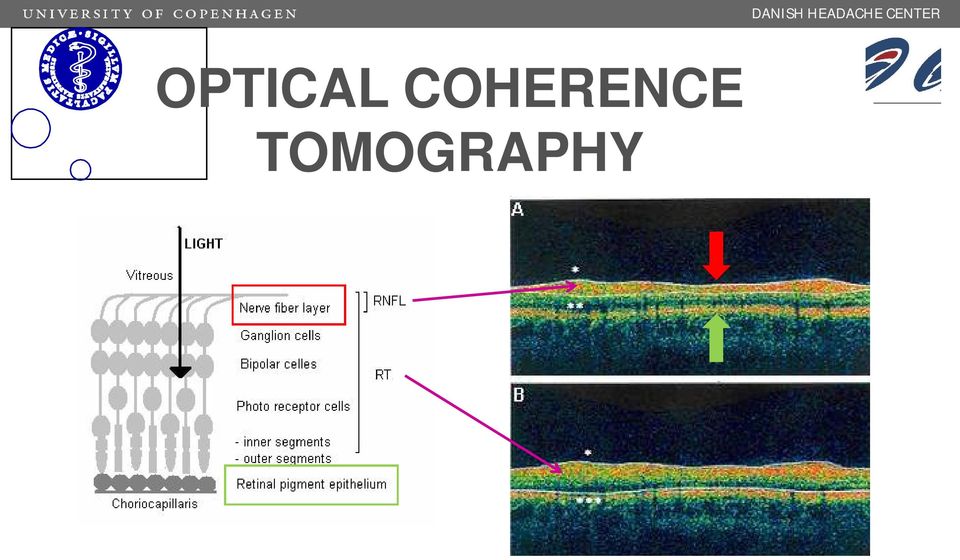
16 Onset 3 months

17 D A N I S H H E A D A C H E C E N T E R Scatter plots of ICP and RT (n=37) and RNFL (n=35) in all IIH subjects (N-/LH-/LL-IIH). Interocular means unadjusted for age and BMI. Correlations: N-IIH LH-IIH ICP vs RNFL r = 0.5, p = 0.01 ICP vs RT r = 0.5, p = 0.03 ICP vs RNFL r = 0.7, p = 0.02 ICP vs RT r = 0.6, p = 0.07 Glostrup Hospital, the Capital Region of Denmark Skau et al 2010

18 D A N I S H H E A D A C H E C E N T E R Proportional change in BMI vs ICP Linear regression analysis: slope: 5.2 cmh 2 0*m 2 )/kg p = N = 13 Median ICP (cmh 2 O) baseline 31.0 (23.4->50) final 24.0 ( ) p < 0.02 Mean BMI (kg/m 2 ) baseline 33.4 ( ) final 31.1 ( ) p < Skau et al 2010 Glostrup Hospital, the Capital Region of Denmark
 final 31.1 (23.5-44.1) p < 0.")
19 Idiopathic Intracranial Hypertension is not always Idiopathic Sinus venous trombosis Infections Inflammation - Sarcoidosis Endokrinological - parathyroid, thyroid, growth hormone, corticosteroid Neoplastic Uremia Toxic: - Tetracycline, steroids, vitamin A

20 Treatment strategy of IIH Mild Intact visual fields/ no papiledema Mild-moderate defects in visual fields Severe or malignant visual impairment Diamox mg/døgn Diamox mg/døgn (+ Topimax/Furix) Acute intervention and V-P shunting Dietary counselleling and weight reduction Frequent follow-up in headache center and neuroopthalmologists for at least 1 year DHC standard and Ball et al J Neurol 2011

21 Conclusions IIH The incidence of IIH is rapidly increasing in the wake of the obesity epidemics Exciting model of ICP regulation and headache? IIH (former benign intracranial hypertension) is not benign and not always idiopathic Active treatment with high doses of azetazolamid an weight loss are requiered Close follow up visits are needed to prevent relapse
22 Medication-Overuse Headache ICHD-III beta a system whereby medication overuse headache became a default diagnosis in all patients with medication overuse would encourage doctors all over the world to do the right thing, namely, to take patients off medication overuse as the first step in a treatment plan. A. Headache present on?ï15 days/month B. Regular overuse for >3 months of one or more acute/symptomatic treatment drugs as defined under sub form Ergotamine, triptans, opioids or combination analgesic medications on?^10 days/month on a regular basis for >3 months 2. Simple analgesics or any combination of ergotamine, triptans, analgesics, opioids on?d10 days/ month on a regular basis for > 3 months without overuse of any single class alone C. Not better accounted for by another ICHD-3 diagnosis (Headache has developed or markedly worsened during medication overuse)
23 Most important chronifying factor: medication overuse Chronic migraine Transformed migraine Chronic daily headache Chronic mixed headache Tension-type headache Post traumatic headache Post craniotomy headache
24 Clinical features (MOH) Daily or almost daily headaches Medication overuse Dull diffuse headache Mild to moderate Holocranial Medication intake Without associated symptoms Mon Tue Wed Thur Wake up with headache Superimposed migraine like attacks
25 Headache Care: What does the patients want? MOH-Patient Expectations to treatment A multicenter study. 100% 80% 60% 40% 20% 0% A cure for headache Frequency reduction Intensity reduction Fast working treatment Effective prevention Education on headache prevention Information on MOH Munksgaard et al JHHP 2011
26 Medication overuse headache (MOH) 1 2% of the general population 20-30% in European Headache Centres % in US Headache centers Favourable outcome by detoxifications in up to 60% BUT To detox or not to detox? In-patient or out-patient basis? Little research on patients with treatment-resistant MOH Initial or delayed start of prophylaxis? 1) Stovner et al ) Zeeberg et al ) Hagen et al ) Evers, Jensen EFNS Guidelines 2011
27 Strategy for detoxification? MOH Mild to moderate Simple analgesics Advice and information Moderate Triptans and analgesics Headache schools Outpatient basis Severe, Relapse or Comorbidity Opioids or Combinations Inpatient
28 MOH in the general population Screening for MOH and chronic headache (1-2%) Simple verbal and written advice by neurologist N=109 patients Average duration of chronic headache 15.5 yrs Follow-up after 1.5 years: Headache frequency: 22 days/mth Grande et al Eur J Neurol 2011
29 Medication and headache days Mean follow-up-time was 1½ years Mean medication days Headache days per month Cured from MO: 76% baseline (open bars) and follow-up (filled bars) Reversed to episodic headache: 42% Frequency reduction: 22 to 6 days pr mth Grande et al. Eur J Neurol 2011
30 Headache in the clinical population (frequency before and after detoxification and preventives in MOH (N= 651)) Headache days /month Highly significant effect on: Use of medication Pain intensity and duration Costs of health care Quality of life Depression and anxiety 78% reverted to episodic headache Tassorelli et ComoEstas study group 2013
31 Effect of detoxification in a headache center 30 *** p< Days/month *** *** Visit 1 Final visit 5 0 Tension-type headache Migraine Zeeberg et al 2005
32 Topiramate in chronic migraine without detox Diener et al Cephalalgia 2007;27: topiramate and 13 placebo completers, 78% MOH. Difference between active and placebo 20% Silberstein et al Headache 2007;47: and 2009;49: Same material. 92 topiramate and 90 placebo completers i.e. 55% completers. Effect size 10%. Medication use unchanged 3 months follow up
33 Effect of prophylaxis without and with detox Days/month Without detox (Silberstein 2007) With detox (Zeeberg 2005)
34 Treatment 98 patients MOH during 5 years Unsuccessfully treated by neurologists Aims Test 2 treatment regimens on: outcome use of medication, relapse, quality of life and cost-effectiveness A Individual based Prophylactics from Day 1 Symptomatic medication 2 days/week 1-year follow-up B Group-based, multidisciplinary Prophylactics after 2 months if needed No symptomatic medication for 2 months 1-year follow-up
35 Results in total 90% completed 2 months withdrawal 83% remained cured of MOH after 12 months 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Lost to follow-up between month 2 and 12 Cured of medication overuse Episodic headache More than 50% reduction in headache frequency Munksgaard et al. Headache 2012
36 Results-in total 39% reduction in headache frequency (p<0.001) 63% reduction in medication use (p<0.001) Headache frequency, days/4 weeks Frequency of medication intake, days/4 weeks Baseline 2 months 12 months Baseline 2 months 12 months Munksgaard et al. Headache 2012
37 Results pressure pain pain thresholds: MOH < healthy (p<0.05) suprathreshold pain (Pain scores 100 mm VAS): no difference extracephalic localisations cephalic locations: MOH patients > healthy (p<0,05) baseline > 6 months and 12 months (p<0,05) Controls MOH baseline MOH 2 months MOH 6 months MOH 12 months
38 12 months follow-up after detoxification with or without prophylaxis from start Munksgaard et al Cephalalgia 2012 Similar headache frequency, duration, intensity and relapse rate in group A and B Group B: Higher quality of life (MIDAS) Group B: Reduced use of analgesics (p=0.02) days/ 4 wks Group B: Reduced use of prophylaxis (p=0.01) 80% 57% Group A: High use of health care service and higher number of visits in the headache centre (p<0.01)
39 Conclusions Very important to identify and treat secondary headaches IIH is not benign and the incidence is rapidly increasing Detoxification is rewarding and very effective in MOH MOH prevention is crucial Specific treatment for most sec. headaches and RCT s are lacking
40
41
Tension-type headache Non-pharmacological and pharmacological treatment
 Danish Headache Center Tension-type headache Non-pharmacological and pharmacological treatment Lars Bendtsen Associate professor, MD, PhD, Dr Med Sci Danish Headache Center, Department of Neurology Glostrup
Danish Headache Center Tension-type headache Non-pharmacological and pharmacological treatment Lars Bendtsen Associate professor, MD, PhD, Dr Med Sci Danish Headache Center, Department of Neurology Glostrup
Tension-type headache Non-pharmacological and pharmacological treatment
 Danish Headache Center Tension-type headache Non-pharmacological and pharmacological treatment Lars Bendtsen Associate professor, MD, PhD, Dr Med Sci Danish Headache Center, Department of Neurology Glostrup
Danish Headache Center Tension-type headache Non-pharmacological and pharmacological treatment Lars Bendtsen Associate professor, MD, PhD, Dr Med Sci Danish Headache Center, Department of Neurology Glostrup
HEADACHE. as. MUDr. Rudolf Černý, CSc. doc. MUDr. Petr Marusič, Ph.D.
 HEADACHE as. MUDr. Rudolf Černý, CSc. doc. MUDr. Petr Marusič, Ph.D. Dpt. of Neurology Charles University in Prague, 2nd Faculty of Medicine Motol University Hospital History of headache 1200 years B.C.
HEADACHE as. MUDr. Rudolf Černý, CSc. doc. MUDr. Petr Marusič, Ph.D. Dpt. of Neurology Charles University in Prague, 2nd Faculty of Medicine Motol University Hospital History of headache 1200 years B.C.
New appendix criteria open for a broader concept of chronic migraine
 Blackwell Publishing LtdOxford, UKCHACephalalgia0333-1024Blackwell Science, 20062006266742746Original ArticleA broader concept of chronic migrainej Olesen et al. BRIEF REPORT New appendix criteria open
Blackwell Publishing LtdOxford, UKCHACephalalgia0333-1024Blackwell Science, 20062006266742746Original ArticleA broader concept of chronic migrainej Olesen et al. BRIEF REPORT New appendix criteria open
The ICHD III Secondary Headaches
 The ICHD III Secondary Headaches ICHD II Morris Levin, MD Professor of Neurology Professor of Psychiatry Dartmouth Medical School Co-Director, Dartmouth Headache Center Hanover, New Hampshire, USA ICHD
The ICHD III Secondary Headaches ICHD II Morris Levin, MD Professor of Neurology Professor of Psychiatry Dartmouth Medical School Co-Director, Dartmouth Headache Center Hanover, New Hampshire, USA ICHD
Headaches + Facial pain
 Headaches + Facial pain Introduction: Each of us experienced sporadically/ chronically headache 40% worldwide population suffers with severe, disabling headache at least annually Common ailment Presenting
Headaches + Facial pain Introduction: Each of us experienced sporadically/ chronically headache 40% worldwide population suffers with severe, disabling headache at least annually Common ailment Presenting
Classification of Chronic Headache
 Chronic Headache Classification of Chronic Headache JMAJ 47(3): 112 117, 2004 Mitsunori MORIMATSU Professor, Department of Neurology and Clinical Neuroscience, Yamaguchi University School of Medicine Abstract:
Chronic Headache Classification of Chronic Headache JMAJ 47(3): 112 117, 2004 Mitsunori MORIMATSU Professor, Department of Neurology and Clinical Neuroscience, Yamaguchi University School of Medicine Abstract:
Differential Diagnosis of Craniofacial Pain
 1. Differential Diagnosis of Craniofacial Pain 2. Headache Page - 1 3. International Headache Society International Classification... 4. The Primary Headaches (1-4) Page - 2 5. The Secondary Headaches
1. Differential Diagnosis of Craniofacial Pain 2. Headache Page - 1 3. International Headache Society International Classification... 4. The Primary Headaches (1-4) Page - 2 5. The Secondary Headaches
Frequent headache is defined as headaches 15 days/month and daily. Course of Frequent/Daily Headache in the General Population and in Medical Practice
 DISEASE STATE REVIEW Course of Frequent/Daily Headache in the General Population and in Medical Practice Egilius L.H. Spierings, MD, PhD, Willem K.P. Mutsaerts, MSc Department of Neurology, Brigham and
DISEASE STATE REVIEW Course of Frequent/Daily Headache in the General Population and in Medical Practice Egilius L.H. Spierings, MD, PhD, Willem K.P. Mutsaerts, MSc Department of Neurology, Brigham and
None related to the presentation Grants to conduct clinical trials from:
 Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Headaches in Children How to Manage Difficult Headaches
 Headaches in Children How to Manage Difficult Headaches Peter Procopis Childhood headaches Differential diagnosis Migraine Psychological Raised Pressure Childhood headaches Other causes: Constitutional
Headaches in Children How to Manage Difficult Headaches Peter Procopis Childhood headaches Differential diagnosis Migraine Psychological Raised Pressure Childhood headaches Other causes: Constitutional
UBC Pain Medicine Residency Program: CanMEDS Goals and Objectives of the UBC Headache Clinic Rotation
 UBC Pain Medicine Residency Program: CanMEDS Goals and Objectives of the UBC Headache Clinic Rotation Overview: The UBC Headache Clinic is located in located in rm. 267, on the 2nd floor of UBC Hospital.
UBC Pain Medicine Residency Program: CanMEDS Goals and Objectives of the UBC Headache Clinic Rotation Overview: The UBC Headache Clinic is located in located in rm. 267, on the 2nd floor of UBC Hospital.
Adult with headache. Problem-specific video guides to diagnosing patients and helping them with management and prevention
 Adult with headache Problem-specific video guides to diagnosing patients and helping them with management and prevention London Strategic Clinical Networks London Neuroscience Strategic Clinical Network
Adult with headache Problem-specific video guides to diagnosing patients and helping them with management and prevention London Strategic Clinical Networks London Neuroscience Strategic Clinical Network
Post Traumatic and other Headache Syndromes. Danielle L. Erb, MD Brain Rehabilitation Medicine, LLC Brain Injury Rehab Center, PRA
 Post Traumatic and other Headache Syndromes Danielle L. Erb, MD Brain Rehabilitation Medicine, LLC Brain Injury Rehab Center, PRA Over 45 million Americans have chronic, recurring headaches 62% of these
Post Traumatic and other Headache Syndromes Danielle L. Erb, MD Brain Rehabilitation Medicine, LLC Brain Injury Rehab Center, PRA Over 45 million Americans have chronic, recurring headaches 62% of these
HEADACHES IN CHILDREN AND ADOLESCENTS. Brian D. Ryals, M.D.
 HEADACHES IN CHILDREN AND ADOLESCENTS Brian D. Ryals, M.D. Frequency and Type of Headaches in Schoolchildren 8993 children age 7-15 in Sweden Migraine in 4% Frequent Nonmigrainous in 7% Infrequent Nonmigrainous
HEADACHES IN CHILDREN AND ADOLESCENTS Brian D. Ryals, M.D. Frequency and Type of Headaches in Schoolchildren 8993 children age 7-15 in Sweden Migraine in 4% Frequent Nonmigrainous in 7% Infrequent Nonmigrainous
HEADACHES IN CHILDREN : A CLINICAL APPROACH
 HEADACHES IN CHILDREN : A CLINICAL APPROACH Chong Shang Chee A physician is commonly faced with a child presenting with headaches. The assessment of a child s headache is challenging, but an accurate assessment
HEADACHES IN CHILDREN : A CLINICAL APPROACH Chong Shang Chee A physician is commonly faced with a child presenting with headaches. The assessment of a child s headache is challenging, but an accurate assessment
Neuroimaging of Headache. Kenneth D. Williams, MD
 Neuroimaging of Headache Kenneth D. Williams, MD Disclosures Financial: None Off Label Usage: None Key Points Headache is an extremely common symptom. Structural abnormalities (Primary HA) are rare. Clinical
Neuroimaging of Headache Kenneth D. Williams, MD Disclosures Financial: None Off Label Usage: None Key Points Headache is an extremely common symptom. Structural abnormalities (Primary HA) are rare. Clinical
Evaluation of Headache Syndromes and Migraine
 Evaluation of Headache Syndromes and Migraine Sonja Potrebic MD PhD Department of Neurology Los Angeles Kaiser Objectives 1) Identify the diagnostic features of migraine Differentiate from sinusitis 2)
Evaluation of Headache Syndromes and Migraine Sonja Potrebic MD PhD Department of Neurology Los Angeles Kaiser Objectives 1) Identify the diagnostic features of migraine Differentiate from sinusitis 2)
9/2/2010. Debbie Zajac has no conflict of interest to disclose.
 Management of Chronic Headaches: An Interdisciplinary Approach September 25, 2010 Deborah C. Zajac RN-BC Clinical Coordinator / IMATCH Program Debbie Zajac has no conflict of interest to disclose. Identify
Management of Chronic Headaches: An Interdisciplinary Approach September 25, 2010 Deborah C. Zajac RN-BC Clinical Coordinator / IMATCH Program Debbie Zajac has no conflict of interest to disclose. Identify
Headaches and Kids. Jennifer Bickel, MD Assistant Professor of Neurology Co-Director of Headache Clinic Children s Mercy Hospital
 Headaches and Kids Jennifer Bickel, MD Assistant Professor of Neurology Co-Director of Headache Clinic Children s Mercy Hospital Overview Headache classifications and diagnosis Address common headache
Headaches and Kids Jennifer Bickel, MD Assistant Professor of Neurology Co-Director of Headache Clinic Children s Mercy Hospital Overview Headache classifications and diagnosis Address common headache
Headaches in Children
 Children s s Hospital Headaches in Children Manikum Moodley, MD, FRCP Section of Pediatric Neurology The Cleveland Clinic Foundation Introduction Headaches are common in children Most headaches are benign
Children s s Hospital Headaches in Children Manikum Moodley, MD, FRCP Section of Pediatric Neurology The Cleveland Clinic Foundation Introduction Headaches are common in children Most headaches are benign
Akuter Kopfschmerz. Till Sprenger, MD Neurologie USB
 Akuter Kopfschmerz Till Sprenger, MD Neurologie USB Disclosure I have consulted for Biogen Idec, Novartis, Mitsubishi Pharmaceuticals, Eli Lilly, Genzyme and Allergan. I have received compensation for
Akuter Kopfschmerz Till Sprenger, MD Neurologie USB Disclosure I have consulted for Biogen Idec, Novartis, Mitsubishi Pharmaceuticals, Eli Lilly, Genzyme and Allergan. I have received compensation for
SIGN. Diagnosis and management of headache in adults. Quick Reference Guide. Scottish Intercollegiate Guidelines Network
 SIGN Scottish Intercollegiate Guidelines Network 107 iagnosis and management of headache in adults Quick Reference Guide November 2008 opies of all SIGN guidelines are available online at www.sign.ac.uk
SIGN Scottish Intercollegiate Guidelines Network 107 iagnosis and management of headache in adults Quick Reference Guide November 2008 opies of all SIGN guidelines are available online at www.sign.ac.uk
Chronic migraine and medication overuse headache: clarifying the current International Headache Society classification criteria
 Chronic migraine and medication overuse headache: clarifying the current International Headache Society classification criteria doi:10.1111/j.1468-2982.2008.01753.x C Sun-Edelstein 1, ME Bigal 2 & AM Rapoport
Chronic migraine and medication overuse headache: clarifying the current International Headache Society classification criteria doi:10.1111/j.1468-2982.2008.01753.x C Sun-Edelstein 1, ME Bigal 2 & AM Rapoport
Introduction. Jean-Christophe Cuvellier 1 Frédéric Couttenier 2 Stéphane Auvin 1 Louis Vallée 1 ORIGINAL RESEARCH
 ORIGINAL RESEARCH The classifi cation of chronic daily headache in French children and adolescents: A comparison between the second edition of the International Classifi cation of Headache Disorders and
ORIGINAL RESEARCH The classifi cation of chronic daily headache in French children and adolescents: A comparison between the second edition of the International Classifi cation of Headache Disorders and
Sinus Headache vs. Migraine
 Sinus Headache vs. Migraine John M. DelGaudio, MD, FACS Professor and Vice Chair Chief of Rhinology and Sinus Surgery Department of Otolaryngology Emory University School of Medicine 1 Sinus Headache Problems
Sinus Headache vs. Migraine John M. DelGaudio, MD, FACS Professor and Vice Chair Chief of Rhinology and Sinus Surgery Department of Otolaryngology Emory University School of Medicine 1 Sinus Headache Problems
Tension Type Headaches
 Tension Type Headaches Research Review by : Dr. Ian MacIntyre Physiotherapy for tension-type Headache: A Controlled Study P. Torelli, R. Jenson, J. Olsen: Cephalalgia, 2004, 24, 29-36 Tension-type headache
Tension Type Headaches Research Review by : Dr. Ian MacIntyre Physiotherapy for tension-type Headache: A Controlled Study P. Torelli, R. Jenson, J. Olsen: Cephalalgia, 2004, 24, 29-36 Tension-type headache
Headaches when to worry is a scan always needed? Regan Solomons
 Headaches when to worry is a scan always needed? Regan Solomons Introduction o Headache is a common problem in childhood o Up to 25% of school children suffer from chronic recurrent headaches o Primary
Headaches when to worry is a scan always needed? Regan Solomons Introduction o Headache is a common problem in childhood o Up to 25% of school children suffer from chronic recurrent headaches o Primary
Chronic daily headache with analgesic overuse Epidemiology and impact on quality of life. NEUROLOGY April, 2004;62:1338 1342
 Chronic daily headache with analgesic overuse Epidemiology and impact on quality of life 1 NEUROLOGY April, 2004;62:1338 1342 R. Colás, MD; P. Muñoz, MD; R. Temprano, MD; C. Gómez, SW; and J. Pascual,
Chronic daily headache with analgesic overuse Epidemiology and impact on quality of life 1 NEUROLOGY April, 2004;62:1338 1342 R. Colás, MD; P. Muñoz, MD; R. Temprano, MD; C. Gómez, SW; and J. Pascual,
sound or ringing in the ears.
 (Idiopathic Intracranial Hypertension) Sashank Prasad, MD www.brighamandwomens.org/neuro-ophthalmology A Patient s Guide Symptoms Diagnosis Treatment Prognosis Symptoms The symptoms of include: Headaches
(Idiopathic Intracranial Hypertension) Sashank Prasad, MD www.brighamandwomens.org/neuro-ophthalmology A Patient s Guide Symptoms Diagnosis Treatment Prognosis Symptoms The symptoms of include: Headaches
Headache - What is Your Migraine Size?
 Headache The Pharmacist s Role in Assessment & Peter Loewen, B.Sc.(Pharm), Pharm.D. Vancouver Hospital & Health Sciences Centre University of British Columbia ETC, Headache. Nan Quintin www.vhpharmsci.com
Headache The Pharmacist s Role in Assessment & Peter Loewen, B.Sc.(Pharm), Pharm.D. Vancouver Hospital & Health Sciences Centre University of British Columbia ETC, Headache. Nan Quintin www.vhpharmsci.com
Guidance for Industry Migraine: Developing Drugs for Acute Treatment
 Guidance for Industry Migraine: Developing Drugs for Acute Treatment DRAFT GUIDANCE This guidance document is being distributed for comment purposes only. Comments and suggestions regarding this draft
Guidance for Industry Migraine: Developing Drugs for Acute Treatment DRAFT GUIDANCE This guidance document is being distributed for comment purposes only. Comments and suggestions regarding this draft
The Clinical Evaluation of the Comatose Patient in the Emergency Department
 The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
HEADACHE: CLINICAL SYNDROMES, PATHOPHYSIOLOGY AND MANAGEMENT Joanna G Katzman, M.D., MSPH Assistant Professor UNM Pain Center and ECHO Pain
 HEADACHE: CLINICAL SYNDROMES, PATHOPHYSIOLOGY AND MANAGEMENT Joanna G Katzman, M.D., MSPH Assistant Professor UNM Pain Center and ECHO Pain University of New Mexico Health Sciences Center 11/14/13 After
HEADACHE: CLINICAL SYNDROMES, PATHOPHYSIOLOGY AND MANAGEMENT Joanna G Katzman, M.D., MSPH Assistant Professor UNM Pain Center and ECHO Pain University of New Mexico Health Sciences Center 11/14/13 After
Headache: Differential diagnosis and Evaluation. Raymond Rios PGY-1 Pediatrics
 Headache: Differential diagnosis and Evaluation Raymond Rios PGY-1 Pediatrics You are evaluating a 9 year old male patient at the ED brought by his mother, who says that her son has had a fever, cough,
Headache: Differential diagnosis and Evaluation Raymond Rios PGY-1 Pediatrics You are evaluating a 9 year old male patient at the ED brought by his mother, who says that her son has had a fever, cough,
When the Pain Won t Stop: Managing Chronic Daily Headache
 When the Pain Won t Stop: Managing Chronic Daily Headache Arnolda Eloff, MB, ChB, Mmed Presented at the University of Calgary s Wednesday Evening Course Program, Calgary, Alberta. Copyright Chronic daily
When the Pain Won t Stop: Managing Chronic Daily Headache Arnolda Eloff, MB, ChB, Mmed Presented at the University of Calgary s Wednesday Evening Course Program, Calgary, Alberta. Copyright Chronic daily
Neurovascular Orofacial Pain. Orofacial pain of potential neurovascular origin may mimic odontogenic pain to the extent that
 Neurovascular Orofacial Pain Introduction Orofacial pain of potential neurovascular origin may mimic odontogenic pain to the extent that a large population of patients with migraine and trigeminal autonomic
Neurovascular Orofacial Pain Introduction Orofacial pain of potential neurovascular origin may mimic odontogenic pain to the extent that a large population of patients with migraine and trigeminal autonomic
Prednisone for the treatment of withdrawal headache in patients with medication overuse headache: A randomized, double-blind, placebo-controlled study
 Brief Report Prednisone for the treatment of withdrawal headache in patients with medication overuse headache: A randomized, double-blind, placebo-controlled study Cephalalgia 33(3) 202 207! International
Brief Report Prednisone for the treatment of withdrawal headache in patients with medication overuse headache: A randomized, double-blind, placebo-controlled study Cephalalgia 33(3) 202 207! International
See also www.thiswayup.org.au/clinic for an online treatment course.
 Depression What is depression? Depression is one of the common human emotional states. It is common to experience feelings of sadness and tiredness in response to life events, such as losses or disappointments.
Depression What is depression? Depression is one of the common human emotional states. It is common to experience feelings of sadness and tiredness in response to life events, such as losses or disappointments.
33 % of whiplash patients develop. headaches originating from the upper. cervical spine
 33 % of whiplash patients develop headaches originating from the upper cervical spine - Dr Nikolai Bogduk Spine, 1995 1 Physical Treatments for Headache: A Structured Review Headache: The Journal of Head
33 % of whiplash patients develop headaches originating from the upper cervical spine - Dr Nikolai Bogduk Spine, 1995 1 Physical Treatments for Headache: A Structured Review Headache: The Journal of Head
New daily persistent headache in the paediatric population
 doi:10.1111/j.1468-2982.2008.01647.x New daily persistent headache in the paediatric population E Kung 1, SJ Tepper 2, AM Rapoport 3, FD Sheftell 4 & ME Bigal 1,5 1 Department of Neurology, Albert Einstein
doi:10.1111/j.1468-2982.2008.01647.x New daily persistent headache in the paediatric population E Kung 1, SJ Tepper 2, AM Rapoport 3, FD Sheftell 4 & ME Bigal 1,5 1 Department of Neurology, Albert Einstein
DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource
 E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
BOTOX Treatment. for Chronic Migraine. Information for patients and their families. Botulinum Toxin Type A
 BOTOX Treatment Botulinum Toxin Type A for Chronic Migraine Information for patients and their families. Is Chronic Migraine the same as Migraine? Chronic Migraine is similar to migraine as sufferers experience
BOTOX Treatment Botulinum Toxin Type A for Chronic Migraine Information for patients and their families. Is Chronic Migraine the same as Migraine? Chronic Migraine is similar to migraine as sufferers experience
PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain
 P a g e 1 PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain Clinical Phase 4 Study Centers Study Period 25 U.S. sites identified and reviewed by the Steering Committee and Contract
P a g e 1 PROTOCOL SYNOPSIS Evaluation of long-term opioid efficacy for chronic pain Clinical Phase 4 Study Centers Study Period 25 U.S. sites identified and reviewed by the Steering Committee and Contract
TYPE OF INJURY and CURRENT SABS Paraplegia/ Tetraplegia
 Paraplegia/ Tetraplegia (a) paraplegia or quadriplegia; (a) paraplegia or tetraplegia that meets the following criteria i and ii, and either iii or iv: i. ii. iii i. The Insured Person is currently participating
Paraplegia/ Tetraplegia (a) paraplegia or quadriplegia; (a) paraplegia or tetraplegia that meets the following criteria i and ii, and either iii or iv: i. ii. iii i. The Insured Person is currently participating
6.0 Management of Head Injuries for Maxillofacial SHOs
 6.0 Management of Head Injuries for Maxillofacial SHOs As a Maxillofacial SHO you are not required to manage established head injury, however an awareness of the process is essential when dealing with
6.0 Management of Head Injuries for Maxillofacial SHOs As a Maxillofacial SHO you are not required to manage established head injury, however an awareness of the process is essential when dealing with
Idiopathic Intracranial Hypertension Investigation and Treatment
 Idiopathic Intracranial Hypertension Investigation and Treatment Dr CP White Consultant Paediatric Neurologist Abertawe Bro Morgannwg UHB January 2011 Definition a condition of increased intracranial pressure
Idiopathic Intracranial Hypertension Investigation and Treatment Dr CP White Consultant Paediatric Neurologist Abertawe Bro Morgannwg UHB January 2011 Definition a condition of increased intracranial pressure
Authors and Disclosures
 Authors and Disclosures www.medscape.com Marco Trucco, MD, Piero Meineri, MD, Luigi Ruiz, MD, Maurizio Gionco, MD, on behalf of the "Gruppo Neurologico Ospedaliero Interregionale per lo Studio delle Cefalee"
Authors and Disclosures www.medscape.com Marco Trucco, MD, Piero Meineri, MD, Luigi Ruiz, MD, Maurizio Gionco, MD, on behalf of the "Gruppo Neurologico Ospedaliero Interregionale per lo Studio delle Cefalee"
Migraine, Tension-type Headache, and Transformed Migraine
 Migraine, Tension-type Headache, and Transformed Migraine Mario F. P. Peres, MD, PhD, Andre Leite Gonçalves, MD, and Abouch Krymchantowski, MD, MSc, PhD Corresponding author Mario F. P. Peres, MD, PhD
Migraine, Tension-type Headache, and Transformed Migraine Mario F. P. Peres, MD, PhD, Andre Leite Gonçalves, MD, and Abouch Krymchantowski, MD, MSc, PhD Corresponding author Mario F. P. Peres, MD, PhD
REHABILITATION MEDICINE by PROFESSOR ANTHONY WARD
 REHABILITATION MEDICINE by PROFESSOR ANTHONY WARD What is Rehabilitation Medicine? Rehabilitation Medicine (RM) is the medical specialty with rehabilitation as its primary strategy. It provides services
REHABILITATION MEDICINE by PROFESSOR ANTHONY WARD What is Rehabilitation Medicine? Rehabilitation Medicine (RM) is the medical specialty with rehabilitation as its primary strategy. It provides services
Updated guidelines on headache management for use by the pharmacist
 M I P C A MIGRAINE IN PRIMARY CARE ADVISORS Updated guidelines on headache management for use by the pharmacist Introduction N U M B E R 2 1, O C T O B E R 2 0 1 2 Headache is a major public health problem,
M I P C A MIGRAINE IN PRIMARY CARE ADVISORS Updated guidelines on headache management for use by the pharmacist Introduction N U M B E R 2 1, O C T O B E R 2 0 1 2 Headache is a major public health problem,
Medical Tourism - Complicated MOH Patients on the Rise
 Rossi et al. The Journal of Headache and Pain 2013, 14:10 RESEARCH ARTICLE Open Access Advice alone versus structured detoxification programmes for complicated medication overuse headache (MOH): a prospective,
Rossi et al. The Journal of Headache and Pain 2013, 14:10 RESEARCH ARTICLE Open Access Advice alone versus structured detoxification programmes for complicated medication overuse headache (MOH): a prospective,
Addiction Medicine for FP / GP. Dr. Francisco Ward, DABPMR/PM SetonPainRehab.com setonpr@gmail.com
 Addiction Medicine for FP / GP Dr. Francisco Ward, DABPMR/PM SetonPainRehab.com setonpr@gmail.com S Disease of Chemical Addiction Short Definition of Addiction (ASAM): Addiction is a primary, chronic disease
Addiction Medicine for FP / GP Dr. Francisco Ward, DABPMR/PM SetonPainRehab.com setonpr@gmail.com S Disease of Chemical Addiction Short Definition of Addiction (ASAM): Addiction is a primary, chronic disease
`çããçå=jéåí~ä= aáëçêçéêëw=^åñáéíó=~åç= aééêéëëáçå. aêk=`=f=lâçåü~ jéçáå~ä=aáêéåíçê lñäé~ë=kep=cçìåç~íáçå=qêìëí=
 `çããçå=jéåí~ä= aáëçêçéêëw=^åñáéíó=~åç= aééêéëëáçå aêk=`=f=lâçåü~ jéçáå~ä=aáêéåíçê lñäé~ë=kep=cçìåç~íáçå=qêìëí= Overview: Common Mental What are they? Disorders Why are they important? How do they affect
`çããçå=jéåí~ä= aáëçêçéêëw=^åñáéíó=~åç= aééêéëëáçå aêk=`=f=lâçåü~ jéçáå~ä=aáêéåíçê lñäé~ë=kep=cçìåç~íáçå=qêìëí= Overview: Common Mental What are they? Disorders Why are they important? How do they affect
July 2012 Target Population. Adult patients 18 years or older in primary care settings.
 Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
Chronic Daily Headache in a Patient With Nasopharyngeal Carcinoma
 CASE REPORT Chronic Daily Headache in a Patient With Nasopharyngeal Carcinoma Jiann-Jy Chen 1,2,3, Dem-Lion Chen 4 * 1 Department of Otorhinolaryngology, Taoyuan Hospital, Department of Health, Executive
CASE REPORT Chronic Daily Headache in a Patient With Nasopharyngeal Carcinoma Jiann-Jy Chen 1,2,3, Dem-Lion Chen 4 * 1 Department of Otorhinolaryngology, Taoyuan Hospital, Department of Health, Executive
THE COMMONWEALTH OF MASSACHUSETTS Department of Industrial Accidents
 THE COMMONWEALTH OF MASSACHUSETTS Department of Industrial Accidents 1 Congress Street, Suite 100 Boston, Massachusetts 02114-2017 DEVAL L. PATRICK Governor PHILIP L. HILLMAN Director TIMOTHY P. MURRAY
THE COMMONWEALTH OF MASSACHUSETTS Department of Industrial Accidents 1 Congress Street, Suite 100 Boston, Massachusetts 02114-2017 DEVAL L. PATRICK Governor PHILIP L. HILLMAN Director TIMOTHY P. MURRAY
Emergency and inpatient treatment of migraine: An American Headache Society
 Emergency and inpatient treatment of migraine: An American Headache Society survey. The objective of this study was to determine the practice preferences of AHS members for acute migraine treatment in
Emergency and inpatient treatment of migraine: An American Headache Society survey. The objective of this study was to determine the practice preferences of AHS members for acute migraine treatment in
Welcome to the program!
 Calgary Headache Assessment & Management Program (CHAMP) EDUCATION SESSION Welcome to the program! Why is this Session Mandatory? Provide headache management information and orientation to the Champ program
Calgary Headache Assessment & Management Program (CHAMP) EDUCATION SESSION Welcome to the program! Why is this Session Mandatory? Provide headache management information and orientation to the Champ program
Attention, memory and learning and acquired brain injury. Vicki Anderson. Jamie M. Attention & learning: an information processing model
 Attention, memory and learning and acquired brain injury Vicki Anderson Jamie M. Childhood acquired amnesia Attention & learning: an information processing model MANAGEMENT Organising, problem solving
Attention, memory and learning and acquired brain injury Vicki Anderson Jamie M. Childhood acquired amnesia Attention & learning: an information processing model MANAGEMENT Organising, problem solving
How To Treat An Elderly Patient
 1. Introduction/ Getting to know our Seniors a. Identify common concepts and key terms used when discussing geriatrics b. Distinguish between different venues of senior residence c. Advocate the necessity
1. Introduction/ Getting to know our Seniors a. Identify common concepts and key terms used when discussing geriatrics b. Distinguish between different venues of senior residence c. Advocate the necessity
Diagnosing and treating episodic migraine
 D A N I S H H E A D A C H E C E N T E R Danish Headache Center Disclosures Diagnosing and treating episodic migraine M.A. is a consultant or scientific adviser for Allergan, Alder, Amgen, ATI, Bayer and
D A N I S H H E A D A C H E C E N T E R Danish Headache Center Disclosures Diagnosing and treating episodic migraine M.A. is a consultant or scientific adviser for Allergan, Alder, Amgen, ATI, Bayer and
Evidence review group report: Botulinum toxin type A for the prophylaxis of headaches in adults with chronic migraine
 Evidence review group report: Botulinum toxin type A for the prophylaxis of headaches in adults with chronic migraine Produced by Warwick Evidence Authors: Dr Pamela Royle, senior research fellow Dr Ewen
Evidence review group report: Botulinum toxin type A for the prophylaxis of headaches in adults with chronic migraine Produced by Warwick Evidence Authors: Dr Pamela Royle, senior research fellow Dr Ewen
Mellen Center for Multiple Sclerosis
 Mellen Center Cleveland Clinic Marie Namey, RN, MSN, MSCN Mellen Center Cleveland Clinic Cleveland, OH Home of. Mellen Center for Multiple Sclerosis Mellen Center Mission The Mellen Center remains committed
Mellen Center Cleveland Clinic Marie Namey, RN, MSN, MSCN Mellen Center Cleveland Clinic Cleveland, OH Home of. Mellen Center for Multiple Sclerosis Mellen Center Mission The Mellen Center remains committed
The essentials of a good headache history
 The essentials of a good headache history Shuu?Jiun Wang, MD The Neurological Institute, Taipei Veterans General Hospital National Yang?øMing University School of Medicine Taipei, Taiwan September 21,
The essentials of a good headache history Shuu?Jiun Wang, MD The Neurological Institute, Taipei Veterans General Hospital National Yang?øMing University School of Medicine Taipei, Taiwan September 21,
Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults
 doi:10.1111/j.1468-2982.2008.01555.x REVIEW Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults S Silberstein 1 (Chairman, USA), P Tfelt-Hansen 2 (Co-Chairman, Denmark),
doi:10.1111/j.1468-2982.2008.01555.x REVIEW Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults S Silberstein 1 (Chairman, USA), P Tfelt-Hansen 2 (Co-Chairman, Denmark),
MIGRAINE. Denise Cambier M.D. Delaware Neurology, Ohio Health March 2013
 MIGRAINE Denise Cambier M.D. Delaware Neurology, Ohio Health March 2013 HISTORY: Graham and Wolff 1938: decreased amplitude of arterial pulsations coincided with reduction of headache with IV ergotamine.
MIGRAINE Denise Cambier M.D. Delaware Neurology, Ohio Health March 2013 HISTORY: Graham and Wolff 1938: decreased amplitude of arterial pulsations coincided with reduction of headache with IV ergotamine.
DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE
 1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache
 Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache Douglas C. McCrory, MD, MHSc Donald B. Penzien, PhD Vic Hasselblad, PhD Rebecca N. Gray, DPhil Duke University
Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache Douglas C. McCrory, MD, MHSc Donald B. Penzien, PhD Vic Hasselblad, PhD Rebecca N. Gray, DPhil Duke University
National Hospital for Neurology and Neurosurgery. Migraine associated dizziness Department of Neuro-otology
 National Hospital for Neurology and Neurosurgery Migraine associated dizziness Department of Neuro-otology If you would like this document in another language or format or if you require the services of
National Hospital for Neurology and Neurosurgery Migraine associated dizziness Department of Neuro-otology If you would like this document in another language or format or if you require the services of
Traumatic brain injury (TBI)
") Traumatic brain injury (TBI) A topic in the Alzheimer s Association series on understanding dementia. About dementia Dementia is a condition in which a person has significant difficulty with daily functioning
Traumatic brain injury (TBI) A topic in the Alzheimer s Association series on understanding dementia. About dementia Dementia is a condition in which a person has significant difficulty with daily functioning
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
Headache Medicine Core Curriculum
 Headache Medicine Core Curriculum Adopted by the United Council for Neurologic Subspecialties (UCNS) Board of Directors December 2005 2005 Table of Contents 1. Traditional Curriculum Components 3 A. Definition
Headache Medicine Core Curriculum Adopted by the United Council for Neurologic Subspecialties (UCNS) Board of Directors December 2005 2005 Table of Contents 1. Traditional Curriculum Components 3 A. Definition
Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas
 Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Headaches. This chapter will discuss:
 C H A P T E R Headaches 1 1 Almost everyone gets an occasional headache at some time or another. Some people get frequent headaches. Most people do not worry about headaches and learn to live with them
C H A P T E R Headaches 1 1 Almost everyone gets an occasional headache at some time or another. Some people get frequent headaches. Most people do not worry about headaches and learn to live with them
Return to Work after Brain Injury
 Return to Work after Brain Injury This section talks about return to work after head injury and what kind of difficulties people experience. It moves onto talking about what kind of help and support is
Return to Work after Brain Injury This section talks about return to work after head injury and what kind of difficulties people experience. It moves onto talking about what kind of help and support is
Attention & Memory Deficits in TBI Patients. An Overview
 Attention & Memory Deficits in TBI Patients An Overview References Chan, R., et.al.. (2003). Are there sub-types of attentional deficits in patients with persisting post- concussive symptoms? A cluster
Attention & Memory Deficits in TBI Patients An Overview References Chan, R., et.al.. (2003). Are there sub-types of attentional deficits in patients with persisting post- concussive symptoms? A cluster
APPENDIX A NEUROLOGIST S GUIDE TO USING ICD-9-CM CODES FOR CEREBROVASCULAR DISEASES INTRODUCTION
 APPENDIX A NEUROLOGIST S GUIDE TO USING ICD-9-CM CODES FOR CEREBROVASCULAR DISEASES INTRODUCTION ICD-9-CM codes for cerebrovascular diseases is not user friendly. This presentation is designed to assist
APPENDIX A NEUROLOGIST S GUIDE TO USING ICD-9-CM CODES FOR CEREBROVASCULAR DISEASES INTRODUCTION ICD-9-CM codes for cerebrovascular diseases is not user friendly. This presentation is designed to assist
Treatment of opioid use disorders
 Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Differential Diagnosis of Chronic Headache
 Chronic Headache Differential Diagnosis of Chronic Headache JMAJ 47(3): 118 123, 2004 Koichi HIRATA Professor, Department of Neurology, Dokkyo University School of Medicine Abstract: Headache is one of
Chronic Headache Differential Diagnosis of Chronic Headache JMAJ 47(3): 118 123, 2004 Koichi HIRATA Professor, Department of Neurology, Dokkyo University School of Medicine Abstract: Headache is one of
A chiropractic approach to managing migraine
 A chiropractic approach to managing migraine What is chiropractic? Chiropractic is a primary healthcare profession that specialises in the diagnosis, treatment and overall management of conditions that
A chiropractic approach to managing migraine What is chiropractic? Chiropractic is a primary healthcare profession that specialises in the diagnosis, treatment and overall management of conditions that
Toothaches of Non-dental Origin
 Toothaches of Non-dental Origin This brochure is produced by the American Academy of Orofacial Pain The American Academy of Orofacial Pain is an organization of health care professionals dedicated to alleviating
Toothaches of Non-dental Origin This brochure is produced by the American Academy of Orofacial Pain The American Academy of Orofacial Pain is an organization of health care professionals dedicated to alleviating
Health Care Service System in Thailand for Patients with Alcohol Use Disorder
 Health Care Service System in Thailand for Patients with Alcohol Use Disorder Health Care Service System In Thailand Screening for alcohol use disorder and withdrawal syndrome AUDIT MAST CAGE CIWA or AWS
Health Care Service System in Thailand for Patients with Alcohol Use Disorder Health Care Service System In Thailand Screening for alcohol use disorder and withdrawal syndrome AUDIT MAST CAGE CIWA or AWS
Migraine The Problem: Common Symptoms:
 Migraine The Problem: A combination of genetic and environmental factors alter pain mechanisms in your brain Transient changes in brain chemicals such as serotonin and neuropeptides affect the membranes
Migraine The Problem: A combination of genetic and environmental factors alter pain mechanisms in your brain Transient changes in brain chemicals such as serotonin and neuropeptides affect the membranes
Traumatic Brain Injury and Incarceration. Objectives. Traumatic Brain Injury. Which came first, the injury or the behavior?
 Traumatic Brain Injury and Incarceration Which came first, the injury or the behavior? Barbara Burchell Curtis RN, MSN Objectives Upon completion of discussion, participants should be able to Describe
Traumatic Brain Injury and Incarceration Which came first, the injury or the behavior? Barbara Burchell Curtis RN, MSN Objectives Upon completion of discussion, participants should be able to Describe
May 3, 2015 Sunday. 17.00-17.30 Opening (H. Bolay, A. Rapoport) 17.30-19.30 Pain disorders in Africa (Chair: A. Rapoport)
 17.30-19.30 Pain disorders in Africa (Chair: A. Rapoport)") May 3, 2015 Sunday 17.00-17.30 Opening (H. Bolay, A. Rapoport) 17.30-19.30 Pain disorders in Africa (Chair: A. Rapoport) 20.00-22.00 Dinner Burden of headache in Africa and emerging challenges (Y. Woldeamanuel-25
May 3, 2015 Sunday 17.00-17.30 Opening (H. Bolay, A. Rapoport) 17.30-19.30 Pain disorders in Africa (Chair: A. Rapoport) 20.00-22.00 Dinner Burden of headache in Africa and emerging challenges (Y. Woldeamanuel-25
Conjoint Professor Brian Draper
 Chronic Serious Mental Illness and Dementia Optimising Quality Care Psychiatry Conjoint Professor Brian Draper Academic Dept. for Old Age Psychiatry, Prince of Wales Hospital, Randwick Cognitive Course
Chronic Serious Mental Illness and Dementia Optimising Quality Care Psychiatry Conjoint Professor Brian Draper Academic Dept. for Old Age Psychiatry, Prince of Wales Hospital, Randwick Cognitive Course
The Burden of Pain Among Adults in the United States
 P F I Z E R F A C T S The Burden of Pain Among Adults in the United States Findings from the National Health and Nutrition Examination Survey, the National Health Care Surveys, and the National Health
P F I Z E R F A C T S The Burden of Pain Among Adults in the United States Findings from the National Health and Nutrition Examination Survey, the National Health Care Surveys, and the National Health
Step 4: Complex and severe depression in adults
 Step 4: Complex and severe depression in adults A NICE pathway brings together all NICE guidance, quality standards and materials to support implementation on a specific topic area. The pathways are interactive
Step 4: Complex and severe depression in adults A NICE pathway brings together all NICE guidance, quality standards and materials to support implementation on a specific topic area. The pathways are interactive
Wellness for People with MS: What do we know about Diet, Exercise and Mood And what do we still need to learn? March 2015
 Wellness for People with MS: What do we know about Diet, Exercise and Mood And what do we still need to learn? March 2015 Introduction Wellness and the strategies needed to achieve it is a high priority
Wellness for People with MS: What do we know about Diet, Exercise and Mood And what do we still need to learn? March 2015 Introduction Wellness and the strategies needed to achieve it is a high priority
These changes are prominent in individuals with severe disorders, but also occur at the mild or moderate level.
 Substance-Related Disorders DSM-V Many people use words like alcoholism, drug dependence and addiction as general descriptive terms without a clear understanding of their meaning. What does it really mean
Substance-Related Disorders DSM-V Many people use words like alcoholism, drug dependence and addiction as general descriptive terms without a clear understanding of their meaning. What does it really mean
The Child With Headache in a Pediatric Emergency Department
 Headache 2008 the Authors Journal compilation 2008 American Headache Society ISSN 0017-8748 doi: 10.1111/j.1526-4610.2007.01052.x Published by Wiley Periodicals, Inc. Research Submission The Child With
Headache 2008 the Authors Journal compilation 2008 American Headache Society ISSN 0017-8748 doi: 10.1111/j.1526-4610.2007.01052.x Published by Wiley Periodicals, Inc. Research Submission The Child With
Careful Coding: Headaches
 Dynamic Chiropractic March 26, 2012, Vol. 30, Issue 07 Careful Coding: Headaches By K. Jeffrey Miller, DC, DABCO and Ray Tuck, DC Because s are among the most common reasons for seeking chiropractic care,
Dynamic Chiropractic March 26, 2012, Vol. 30, Issue 07 Careful Coding: Headaches By K. Jeffrey Miller, DC, DABCO and Ray Tuck, DC Because s are among the most common reasons for seeking chiropractic care,
Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease.
 Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease. Memory loss and changes in mood and behavior are some signs that you or a family member may have Alzheimer s disease. If you have
Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease. Memory loss and changes in mood and behavior are some signs that you or a family member may have Alzheimer s disease. If you have
TBI TRAUMATIC BRAIN INJURY WITHIN THE MILITARY/VETERAN POPULATION
 TBI TRAUMATIC BRAIN INJURY WITHIN THE MILITARY/VETERAN POPULATION What is TBI? An external force that disrupts the normal function of the brain. Not all blows or jolts to the head result in a TBI. The
TBI TRAUMATIC BRAIN INJURY WITHIN THE MILITARY/VETERAN POPULATION What is TBI? An external force that disrupts the normal function of the brain. Not all blows or jolts to the head result in a TBI. The
Chronic daily headache
 Chronic daily headache Chronic daily headache (CDH) is defined as any headache syndrome affecting more than half of the month, i.e. a headache on more than 15 days per month. It is also known as daily
Chronic daily headache Chronic daily headache (CDH) is defined as any headache syndrome affecting more than half of the month, i.e. a headache on more than 15 days per month. It is also known as daily
What is chronic daily headache? Information for patients Neurology
 What is chronic daily headache? Information for patients Neurology What is chronic daily headache (CDH)? Chronic daily headache (CDH) is the term used when a person has a headache on 15 days a month or
What is chronic daily headache? Information for patients Neurology What is chronic daily headache (CDH)? Chronic daily headache (CDH) is the term used when a person has a headache on 15 days a month or
Sponsor Novartis. Generic Drug Name Secukinumab. Therapeutic Area of Trial Psoriasis. Approved Indication investigational
 Clinical Trial Results Database Page 2 Sponsor Novartis Generic Drug Name Secukinumab Therapeutic Area of Trial Psoriasis Approved Indication investigational Clinical Trial Results Database Page 3 Study
Clinical Trial Results Database Page 2 Sponsor Novartis Generic Drug Name Secukinumab Therapeutic Area of Trial Psoriasis Approved Indication investigational Clinical Trial Results Database Page 3 Study
HEPATIC ENCEPHALOPATHY
 HEPATIC ENCEPHALOPATHY Jan Albrecht Department of Neurotoxicology, Medical Research Centre, Polish Academy of Sciences, Warsaw, Poland Brussels, July 14, 2009 DEFINITIONS: - HEPATIC ENCEPHALOPATHY (HE)
HEPATIC ENCEPHALOPATHY Jan Albrecht Department of Neurotoxicology, Medical Research Centre, Polish Academy of Sciences, Warsaw, Poland Brussels, July 14, 2009 DEFINITIONS: - HEPATIC ENCEPHALOPATHY (HE)