A Comprehensive Review of Development and Testing for National Implementation of Hospital Core Measures
|
|
|
- Letitia Amice Elliott
- 7 years ago
- Views:
Transcription
1 A Comprehensive Review of Development and Testing for National Implementation of Hospital Core Measures This overview is intended to summarize the challenges and decisions that impacted the development and testing of acute myocardial infarction (AMI) heart failure (HF) and community acquired pneumonia (CAP) hospital core measures, as well as to provide the clinical rationale that supported the measures that were originally contained within the Joint Commission on Accreditation of Healthcare Organization s (Joint Commission) initial core measure sets for hospitals. Table of Contents Background 2 The Hospital Core Measure Pilot Project 3 National Comparison Group Data from the Core Measure Pilot Project 9 History of Core Measure Set Development and Revisions 20 Overview of the Acute Myocardial Infarction Core Measure Set 21 Overview of the Heart Failure Core Measure Set 26 Overview of the Community Acquired Pneumonia Core Measure Set 29 Overview of the Pregnancy and Related Conditions Core Measure Set 36 References 40 1

2 Background The Joint Commission began development of performance measures with the inception of the Agenda for Change in Eventually these activities were subsumed into what became called the ORYX initiative. The initial phase of the ORYX initiative offered health care organizations significant flexibility. Organizations could meet accreditation requirements by selecting from among literally hundreds of performance measurement systems and thousands of performance measures that best served their strategic measurement goals. The flexibility made available through the initial phases of the ORYX initiative also presented certain challenges. Most notable was the inability to compare health care organization data across systems and between disparate measures. The next phase of the ORYX initiative was intended to address this challenge through the use of standardized, evidence based measures. In 1999, the Joint Commission sought input from a variety of stakeholders including clinical professionals, hospitals, consumers, state hospital associations and medical societies about potential focus areas for an initial set of hospital core measures. Once focus areas were identified, advisory panels were convened to identify measures that, when viewed together, permitted a robust assessment of the care provided in a given focus area. The Attributes of Core Performance Measures and Associated Evaluation Criteria were used to evaluate candidate measures for potential use as core measures. Stakeholder engagement was actively sought by posting the potential core measures on the Joint Commission web site. A variety of stakeholders, including clinical professionals, health care provider organizations, health care consumers and performance measurement experts provided over 1,600 comments. These comments helped to mold and shape the specifications for the initial core measure sets prior to pilot testing. They also contributed to the postponement of implementation for the Surgical Procedures and Complications core measure set. Stakeholder comments and additional research indicated that consensus among the major professional organizations and stakeholder groups in this area was lacking in this area. Therefore, development of the Surgical Procedures and Complications core measure set was delayed until consensus could be reached. 2

3 The Hospital Core Measure Pilot Project Once the initial specifications for the first sets of core measure were developed, the Joint Commission initiated a pilot project to test the feasibility, usefulness, and costs associated with the implementation of core measures. Participants were drawn from eleven state hospital associations that expressed an interest in participating in a pilot project. Five were randomly selected to participate (Connecticut, Michigan, Missouri, Georgia and Rhode Island). Each hospital association then identified a single performance measurement system and 7-28 participant hospitals. The resulting project was a collaborative effort among the Joint Commission, five state hospitals associations, 5 listed measurement systems, and 83 hospitals in nine states (Connecticut, Michigan, Missouri, Georgia, Rhode Island, Texas, Virginia, California and South Carolina). The Joint Commission solicited ongoing feedback from participating systems and hospitals to modify core measure specifications throughout the project. Joint Commission staff also visited a random sample of 16 participating hospitals to assess the reliability of core measure data elements. Participant demographics are presented below: 3
.")
4 4

5 Objectives of the Pilot Project 1. Gain an early base of experience in implementing a limited number of core measures derived largely from the CMS PRO 6th Scope of Work quality indicators as adapted by the Joint Commission; 2. Assess the technical aspects of embedding core measures into disparate listed performance measurement systems, including the use of standardized technical specifications and calculation algorithms, the time required for systems to embed the measures, and the Joint Commission's ability to verify that the measures were embedded by the systems correctly; 3. Evaluate the training, staffing, and time required for data collection both at the system and health care organization level; Assess issues related to data quality (accuracy and completeness), data sources, data 4. elements, data definitions (e.g., problematic, difficult to collect data elements) and costs of data collection/abstraction; track trends and patterns in missing data to observe and understand potential variation across participating systems; 5. Assess whether all required data elements can be transmitted to the Joint Commission from the system on a timely basis; 6. Assess the level of Joint Commission support that is necessary for performance measurement systems implementing core measures; 7. Assess the Joint Commission's ability to handle missing and aberrant data. 8. Assess the Joint Commission's ability to produce control and comparison charts for core measure data; and 5

6 9. Study the use of core measures in hospital performance improvement efforts. Data Collection Effort: Each month, hospitals participating in the core measure pilot project submitted an activity log created by the Joint Commission that summarized the hospital's core measure activity during the previous month. Each activity log identified the type of activity (e.g., case identification, case abstraction), profession of the person(s) engaged in that activity, and the number of hours spent during the month. This initial analysis includes data from January December The graphs presented below display a breakdown of the average time spent on core measure data collection effort by participating hospitals. Figure 1illustrates the median (50 th percentile) amount of time participating hospitals spent on core measure activities. Since case volume tends to be the most significant predictor of activity time, the graph includes a break down by hospital bed size (small hospitals or fewer beds, and larger hospitals greater than 100 beds). Figure 2 illustrates the average (mean) amount of time participating hospitals spent on core measure activities. Note that hospitals collecting more than two measure sets have been removed from the data set, since the Joint Commission only requires data collection for two core measure sets. This graph also includes a breakdown by hospital bed size (small hospitals or fewer beds, and larger hospitals greater than 100 beds). 6

7 Figure 3 illustrates the differences in the average amount of time participating hospitals spent on core measure activities depending upon the measure sets they selected (including hospitals that selected all three core measure sets). Note that the increases in activity hours for the hospitals collecting three core measure sets are likely due to additional data collection activities that were not a requirement of the core measure pilot project (i.e., retrospectively collecting multiple months of data during the specified time period). 7
.")
8 Estimating Core Measure Activity Time: In an independent study of the data collection effort, one of the participating measurement systems (the Qualidigm Quality Partnership) measured actual time spent abstracting data per case for the 10 Rhode Island hospitals participating with their system. Each hospital collected data for the three core measure sets (AMI, HF, and CAP) for a period of 12 months, beginning in October To measure activity time per record, Qualidigm used a modified version of the CMS MedQuest data collection tool, which records the actual time spent abstracting each chart. Median time per hospital, per measure set, per chart was then calculated: AMI = 15.6 minutes (0.26 hours/case) HF = 12 minutes (0.20 hours/case) CAP = 12.6 minutes (0.21 hours/case) Qualidigm also experimented with adjusting the "actual" time to provide a better estimate of total time and money per core measure set selected. The actual times were adjusted to account for time spent identifying records (i.e., locating and gathering records for data abstraction) and for productivity limitations (i.e., confounding activities that preclude absolutely efficient data abstraction). Therefore, 0.1 hours were added to the median to account for time spent identifying and retrieving charts. This new figure was then divided by 0.80 (as an estimate of actual productivity). The results, as adjusted, were: AMI = 27 minutes (0.45 hours/case) HF = 22.2 minutes (0.37 hours/case) CAP = 23.4 minutes (0.39 hours/case) Using these figures, it is possible to achieve a rough estimate of the resources required per measure set for a given time period. To estimate core measure activity time, simply multiply the median abstraction time per case (i.e., 0.45 hours for AMI, 0.37 hours for HF) by the hospital's expected case volume for a given time period (i.e., 28 AMI cases per month, 40 HF cases per month). For example: AMI: 0.45 * 28 = 12.6 hours per month HF: 0.37 * 40 = 14.8 hours per month Total = 27.4 hours per month 8

9 Note: Although these calculations were also supported by the Joint Commission's activity log data, individual results will vary significantly depending upon the skill of the abstractor, the quality of documentation in the medical record, the efficiency of the data collection tool, and a number of related factors. These figures should therefore be considered estimates, and the results should be interpreted with caution. National Comparison Group Data from the Core Measure Pilot Project The following graphs are based on the national comparison group data gathered during the course of the pilot project. Where possible, a comparison to the CMS 6 th Scope of Work results is provided. 1 9

10 10

11 11

12 12

13 13

14 14

15 15

16 16
17 17

18 18

19 19

20 History of Core Measure Set Development and Revisions Throughout 2001, the Joint Commission received feedback from the participating state hospital associations, measurement systems, and hospitals. This feedback, the analysis of on-site reliability data, and the Joint Commission's ongoing discussions with CMS, directed toward alignment of similar measures, led to an number of improvements and modifications to the original core measures, prior to their release on November 21, Major Revisions: Initially surgical procedures and complications were identified by key Joint Commission stakeholders as one of the initial priority areas for hospital core measure development. However, CMS is currently developing quality indicators related to surgical infection prevention (SIP) including selection and timing of prophylactic antibiotics. The Joint Commission is a member of the SIP Project Panel. Therefore, the Joint Commission will delay implementing the surgical core measure set to allow the opportunity to continue to work with CMS. Discussions with CMS centered on measures shared between CMS and the Joint Commission and led to the development of common data element definitions and allowable values, and common measure population inclusions and exclusions. During the pilot, data were collected for 2 measures, both of which addressed the use of angiotensin converting enzyme inhibitors (ACEI), in order to determine which of these similar measures should be implemented nationally. One measure removed the contraindications from the numerator while the other measure removed the contraindications from the denominator. Due to the complexity in the design we needed to remove the contraindications from the numerator, the cardiovascular advisory panel recommended deleting this measure in favor of the measure that was implemented nationally. The measure pertaining to warfarin prescribed at discharge was deferred for national implementation. The measure was deferred because contraindications to warfarin are difficult and time consuming to abstract and the measure population for this indicator includes some patients not eligible for any other measures in the HF core set making it difficult to identify patients eligible for the measure. The AMI, HF and CAP measure set all contain a measure focused on adult smoking cessation advice/counseling. The measures specifications are identical with the exception of the measure population (denominator). A more in depth description of the development and modifications made to each measure -- and the rationale behind those decisions -- is included within the measure set specific sections that follow: 20

21 Overview of the Acute Myocardial Infarction (AMI) Core Measure Set (3/22/2002) Acute myocardial infarction (AMI) was identified by key Joint Commission stakeholders as one of the initial priority focus areas for hospital core measure development. The literature supports the importance of measuring the processes and outcomes of care for patients with AMI based primarily on disease prevalence. Currently, cardiovascular disease, including AMI, is the leading cause of death in the United States and is the primary disease category for hospital patient discharges. 2 Each year 900,000 people in the United States are diagnosed with AMI; of these, approximately 225,000 cases result in death and, it is estimated that an additional 125,000 patients die before obtaining medical care. 3 The Joint Commission's cardiovascular advisory panel articulated the clinical logic that provided the framework for identifying inter-related, evidence-based measures that, when used together, can more fully assess the overall quality of care provided for AMI patients. The scope of the AMI core measure set was limited to patients 18 years of age and older because the clinical treatment of younger patients is substantially different. Hospital AMI Core Measures Initial Release The following nine measures comprise the initial set of hospital AMI Core Measures and will be implemented on July 1, AMI-1 Aspirin at arrival AMI-2 Aspirin prescribed at discharge AMI-3 ACEI for LVSD AMI-4 Adult smoking cessation advice/counseling AMI-5 Beta blocker prescribed at discharge AMI-6 Beta blocker at arrival AMI-7 Time to thrombolysis AMI-8 Time to PTCA AMI-9 Inpatient mortality Hospital AMI Core Measures Recommended for Future Core Measure Set Completion The following measures were identified for potential future implementation. The specific date for implementation has not yet been determined. They are not included in the initial set because no specific measures have been identified for implementation at this time. 21
22 Lipid profile drawn within 24 hours of patient arrival for AMI Patients with abnormal lipid profile results with documented plan for lipid management (e.g., diet and/or drug therapy) AMI mortality within 30 days post AMI Individual Measure Descriptions: The following describes the rationale and related considerations underlying each of the measures currently included in the AMI Core Measure Set. AMI-1 Aspirin at arrival AMI-2 Aspirin prescribed at discharge Aspirin is estimated to prevent subsequent AMI in 3.5 to 4% of patients previously treated for AMI. Current guidelines recommend that a patient with suspected AMI, upon arrival to the emergency department (ED), should immediately receive aspirin.4 This indicator addresses aspirin administration anytime over the 24 hours prior to arrival and 24 hours after arrival at the hospital. The accommodation to 24 hours prior to arrival was believed important because of the increased public awareness about the benefits of immediate aspirin use (i.e., many patients are taking aspirin at home and/or emergency medical services are administering aspirin during transport). Preliminary data gathered during the Joint Commission's pilot project shows a mean measure rate of 94% for the aspirin at admission measure, and a rate of 95% for the asprin at discharge measure. Equating aspirin equivalents (e.g., clopidogrel) with aspirin was considered for these measures, but was rejected at this time for two reasons: Measure construct should not precede published guidelines. Doing so may focus attention on potentially controversial issues rather than on quality improvement. Patients with contraindications to aspirin (e.g., active bleeding) are excluded from the measure population. Thus, patients receiving aspirin equivalents would also already have been eliminated. Finally, during the pilot test, antiplatelet drugs and non-steroidal anti-inflammatory drugs (NSAIDs) were exclusions from the measure population (i.e., they were included on the contraindication list). Updated guidelines, however, do not include NSAIDs and antiplatelet drugs as contraindications for aspirin therapy; therefore, these medications were removed from the list of contraindications for aspirin at discharge. AMI-3 ACEI for LVSD 22
23 Clinical trials have established that the use of angiotensin converting enzyme inhibitor (ACEI) begun after a patient has recovered from an AMI improves long-term survival; patients with anterior infarctions or a left ventricular ejection fraction (LVEF) level <40% have the greatest benefit from this treatment. This measure assesses whether ACEI were prescribed at discharge for patients with left ventricular systolic dysfunction (LVSD) who have the potential to receive the intended benefit. Preliminary data from the pilot project shows a mean measure rate of 83% indicating an opportunity for improvement. During the pilot project, this measure excluded patients from the denominator admitted on angiotensin receptor blocker (ARB) drugs. Since this time, however, the Heart Failure Society of America (HFSA) guidelines, which reflect the latest clinical trial results, were modified and recommend that ACEIs and ARBs should not be considered equivalent. The HFSA guidelines recommend ARBs as second-line drugs to be used only when there are contraindications to ACEI. Therefore, ARBs were eliminated as a contraindication to prescribing ACEI. In the pilot project, bilateral renal artery stenosis was among the contraindications to ACEI at discharge. According to the CMS National Heart Failure Project baseline data, this was a rare event, present in only approximately 0.3 % of cases. Thus, to reduce data collection effort, bilateral renal artery stenosis was also eliminated as a contraindication to prescribing ACEI in the final measure specifications for national implementation. Finally, chronic renal dialysis was a contraindication for prescribing ACEI during the pilot project. Currently most nephrologists and cardiologists consider ACEI an appropriate medication for patients with LVSD undergoing chronic renal dialysis. Therefore, chronic renal dialysis was removed from the list of categorical contraindications. AMI-4 Adult smoking cessation advice/counseling Each year, more than 430,000 deaths in the United States are attributed to a smoking related illness. 5 Smoking triggers coronary spasm, reduces the anti-ischemic effects of beta blockers, and increases mortality after AMI. Evidence indicates that within one year of quitting smoking, a patient's risk of acute myocardial reinfarction and AMI mortality is reduced. Because between one third and one half of AMI patients begin smoking again within 6 to 12 months of their diagnosis, the patient population for this measure includes those who have a history of smoking within one year of admission. 6 Preliminary data from the pilot project indicate that 65% of AMI patients with a history of smoking within the past year received smoking cessation advice or counseling. For 23
24 further discussion on smoking cessation measures, refer to material in the Overview of the Community Acquired Pneumonia Core Measure Set for Hospitals. AMI-5 Beta blocker prescribed at discharge AMI-6 Beta blocker at arrival Evidence indicates that beta blocker therapy reduces both the degree of infarction and incidence of complications in patients not receiving concomitant thrombolytic therapy, and the incidence of reinfarction in patients who receive thrombolytic therapy. In addition, several placebo-controlled trials have shown that long-term beta blocker therapy decreases mortality by reducing the incidence of sudden and nonsudden cardiac death. 7 Preliminary pilot test data on these measures reveal a mean rate of 90% for the beta blocker prescribed at discharge measure, and 85% for the beta blocker at arrival measure. These beta blocker measures were originally adapted from the CMS PRO 6 th Scope of Work (SOW) National AMI Project. The following contraindications to beta blockers were included initially in the measures: second and third degree heart block; bifasicular block; and PR interval >0.24 sec. interval. For ease of abstraction, and to reflect current treatment guidelines, the only categorical exclusions for prescribing beta blockers in the final measure specifications is the presence of second or third degree heart block. Bifasicular block and PR interval >0.24 sec. interval are acceptable contraindications only if so documented by a physician, nurse practitioner, or physician assistant as a reason for not prescribing a beta blocker. Shock on day of admission, documented by a physician, was added as a contraindication for the beta blocker on admission measure. AMI-7 Time to thrombolysis AMI-8 Time to PTCA Evidence indicates that the timing of reperfusion is critical to the effective management of AMI patients and the earlier therapy is initiated, the better the outcome. Patients presenting with AMI and ST segment elevation or left bundle branch block (LBBB) are at a relatively high risk of death. This risk may be reduced by thrombolytic therapy or PTCA, but only if administered/performed in a timely manner. The greatest benefits of thrombolytic therapy are evident in the first 3 hours after the onset of symptoms, but there is proven benefit for up to 12 hours after the onset of symptoms. 8 PTCA is associated with a 1-year survival rate of 90% to 96%. The timeliness of reperfusion is of great importance and interest to the public (it is one of the AMI 24
25 treatment issues addressed in Healthy People 2010), is very amenable to quality improvement efforts, and is the one indicator that requires that quality improvement activities be closely integrated across hospital departments. The data elements comprising these two measures, particularly the time-related variables, are challenging to collect. This is primarily due to imprecise medical record documentation of time of patient arrival (found present in the medical record in 75% of the cases during the pilot test) and PTCA time (found present in the medical record in 70% of the cases). The data element assessing ST segment elevation is also problematic because ST segment elevation is often not stated explicitly in the ECG documentation. This lack of explicit documentation can result in cases being incorrectly eliminated from the population. However, the importance of these measures for monitoring AMI patient care transcends concerns raised by the data element related issues. Preliminary data from the pilot test show an average median rate of minutes for time to thrombolysis and an average median rate of minutes (5.2 hours) for time to PTCA. Therefore both of these measure rates would indicate an opportunity for improvement, as current guidelines recommend 30 minutes to thrombolysis and 90 minutes to PTCA. AMI-9 Inpatient mortality Mortality of patients with AMI represents a significantly deleterious outcome that is potentially related to the quality of care. This rate-based indicator identifies an undesirable outcome of care, and measures only intrahospital inpatient mortality. Preliminary data from the pilot test show a mean measure rate of.09%. Future Directions for the AMI Core Measure Set The Joint Commission has chosen to measure time to thrombolysis and time to PTCA as a continuous variable for multiple reasons relating to both the spirit of the continuous quality improvement (CQI) cycle, and the opportunities for robust statistical analyses afforded by the use of X-bar and S control charts with respect to trending performance data overtime. Both the Joint Commission measure and the CMS measure are identical at the data element level; therefore, data collection is not affected by the difference in data reporting. However, the Joint Commission and CMS realize that both rates are important for quality improvement purposes; therefore, both organizations will report rates for this measure as a proportion and a continuous variable. The Joint Commission will prepare specifications for the proportion measures in 2002, with release expected later in the year. 25
26 Overview of the Heart Failure (HF) Core Measure Set (3/22/2002) Heart failure (HF) was identified by key Joint Commission stakeholders as one of the initial priority focus areas for hospital core measure development. The literature supports the importance of measuring the processes and outcomes of care for patients with HF primarily based on disease prevalence. Nearly 5 million patients in the U.S. have HF, and approximately 500,000 to 900,000 new cases are diagnosed each year. Heart failure is the most common Medicare diagnosis-related group, and more Medicare dollars are spent for the diagnosis and treatment of HF than for any other diagnosis. 9 The Joint Commission's cardiovascular advisory panel articulated the clinical logic that provided the framework for identifying inter-related, evidence-based measures that, when used together, can more fully assess the overall quality of care provided for HF patients. The scope of the HF core measure set is limited to patients 18 years of age and older because the clinical treatment of younger patients is handled substantially differently. Hospital HF Core Measures Initial Release The following four measures comprise the initial set of hospital HF Core Measures and will be implemented on July 1, HF-1 Discharge instructions HF-2 LVF assessment HF-3 ACEI for LVSD HF-4 Adult smoking cessation advice/counseling Individual Measure Descriptions: The following describes the rationale and related considerations underlying each of the measures currently included in the HF Core Measure Set. HF-1 Discharge instructions Educating patients with heart failure and their families is critical. Patient non-compliance with physician's instructions is often a cause of re-hospitalization. It is thus important that health care professionals ensure that patients and their families understand the prognosis of heart failure, the rationale for pharmacotherapy and prescribed medication regimen, dietary restrictions, and activity recommendations, and the signs and symptoms of 26
27 deteriorating condition. Additionally, patients discharged from the hospital after an exacerbation of heart failure should have follow-up to ensure clinical stability. It is necessary that all six discharge instructions (see measure specifications) be given to the patient in order to qualify as a numerator event for this measure. For quality improvement efforts, the Joint Commission has provided algorithms to performance measurement systems that will assist health care organizations in identifying the individual discharge instructions that are problematic. During the Joint Commission pilot project, several participants believed this measure afforded them the greatest opportunity for quality improvement initiatives within their institution. This is substantiated by the overall pilot project data-the mean rate for this measure was 28%. HF-2 LVF assessment Measurement of left ventricular performance is a critical step in the evaluation and management of almost all patients with suspected or clinically evident heart failure. The combined use of history, physical examination, chest x-ray, and electrocardiography cannot reliably distinguish between the major categories of HF: left ventricular systolic dysfunction, left ventricular diastolic dysfunction, or a non-cardiac etiology. If measurement of ventricular performance is not obtained in patients presenting with heart failure, appropriate treatment may be withheld. Specifically, patients with left ventricular systolic dysfunction will not be identified and, therefore, will not be treated with agents known to prolong life. Preliminary data from the pilot test demonstrate an opportunity for improvement with a mean rate of 79%. This measure only addressed HF patients not admitted on angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) during the Joint Commission pilot project. It has been modified for national implementation in accord with recent updated guideline recommendations related to LVF assessment for patient with HF. 10 HF-3 ACEI for LVSD Clinical trials have established that the using ACEI for patients diagnosed with HF can alleviate symptoms, improve clinical status, enhance overall sense of well-being, and can reduce the risk of death and hospitalization. 11 This measure assesses whether ACEI were appropriately prescribed at discharge for patients with left ventricular systolic dysfunction (LVSD) who have the potential to receive the intended benefit. Preliminary data from the pilot project shows a mean measure rate of 86% indicating some opportunity for improvement. 27
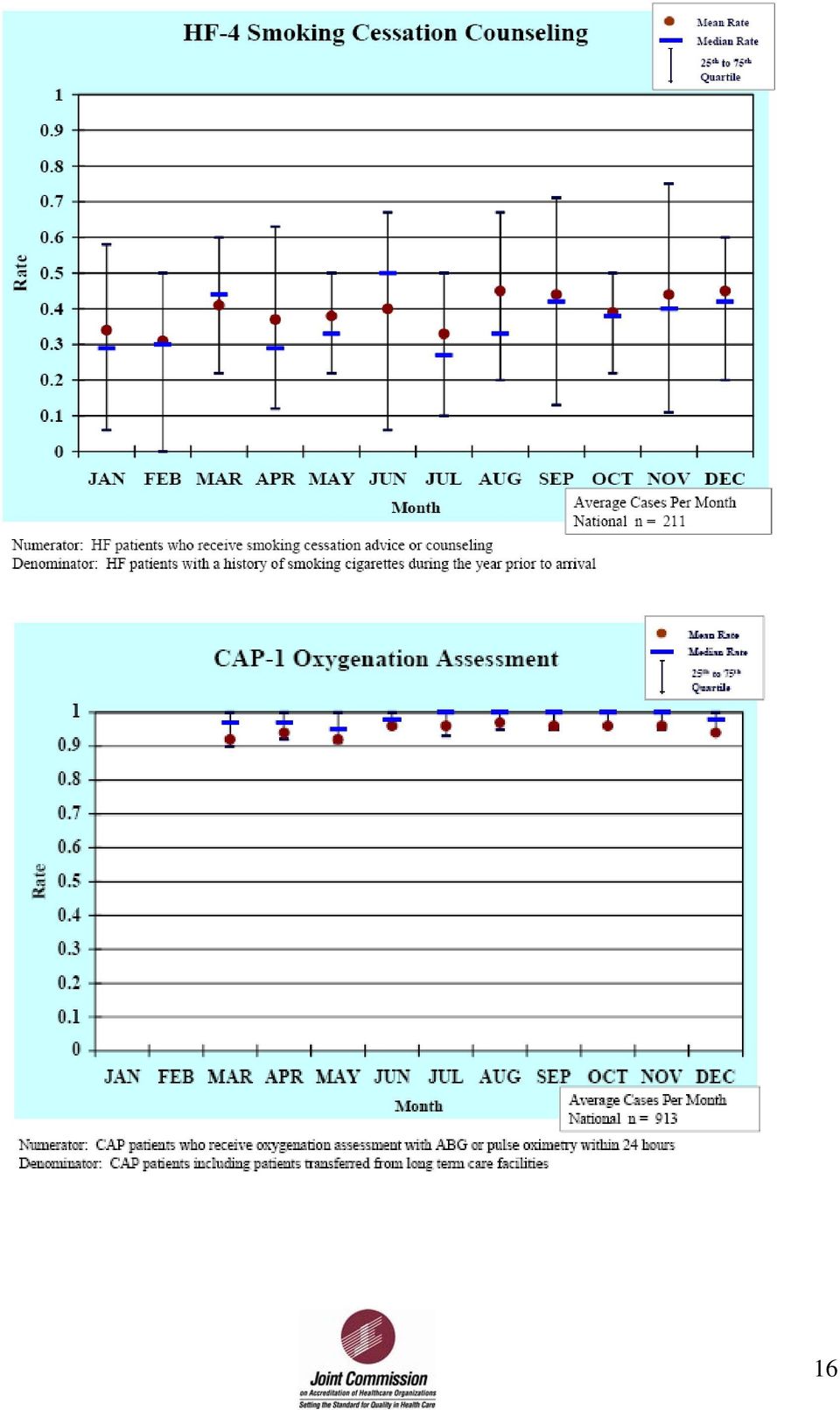
28 During the pilot project, this measure excluded patients from the denominator admitted on ARB drugs. Since this time, however, the Heart Failure Society of America (HFSA) guidelines, which reflect the latest clinical trial results, were modified and recommend that ACEIs and ARBs should not be considered equivalent. The HFSA guidelines recommend that ARBs as second-line drugs to be used only when there are contraindications to ACEI. 12 Therefore, ARBs were eliminated as a contraindication to prescribing ACEI. In the pilot project, bilateral renal artery stenosis was among the contraindications to ACEI at discharge. According to the CMS National Heart Failure Project baseline data, this was a rare event, present in only approximately 0.3 percent of cases. Thus, to reduce data collection effort, bilateral renal artery stenosis was also eliminated as a contraindication to prescribing ACEI in the final measure specifications for national implementation. Chronic renal dialysis was also identified as a contraindication to ACEI during the pilot project. Currently, however, most nephrologists and cardiologists consider ACEI to be an appropriate medication for patients with LVSD undergoing chronic renal dialysis. Therefore, chronic renal dialysis was removed from the list of categorical contraindications. HF-4 Adult smoking cessation advice/counseling Each year more than 430,000 deaths in the United States are attributed to a smoking related illness. 13 Because one third to one half of cardiovascular patients begin smoking again within 6 to 12 months of their diagnosis, the patient population for this measure includes those who have a history of smoking within one year of admission. 14 Preliminary data from the pilot project indicates that 39% of HF patients with a history of smoking within the past year received smoking cessation advice or counseling. For further discussion on smoking cessation measures, refer to material in the Overview of the Community Acquired Pneumonia Core. 28
29 Overview of the Community Acquired Pneumonia (CAP) Core Measure Set (3/22/2002) Community acquired pneumonia was one of the initial priority focus areas for hospital core measure development identified by key Joint Commission stakeholders. The importance of measuring the processes and outcomes of care for patients with pneumonia is further supported by the literature highlighting disease prevalence, increasing antibiotic resistance, and healthcare costs. In the United States, pneumonia is the sixth most common cause of death. From , the overall rates for death due to pneumonia and influenza increased by 59%. Much of the increase is due to a greater population of persons aged 65 years or older, and a changing epidemiology of pneumonia, including a greater proportion of the population with underlying medical conditions at increased risk of respiratory infection. Annually, 2-3 million cases of community acquired pneumonia (CAP) result in 10 million physician visits; 500,000 hospitalizations; and 45,000 deaths. 15 The Joint Commission s Pneumonia Advisory Panel articulated the clinical logic that provided the framework for identifying inter-related evidence-based measures that when used together, can assess the overall quality of care provided for patients with pneumonia. The scope of the pneumonia core measure set is limited to CAP. Nosocomial pneumonia was excluded for the following reasons: A limited number of well tested, evidence based measures are currently available; Case identification is difficult and not always accurate; Definitions are problematic; The literature has not clearly addressed how to decrease the incidence, suggestions available but lack scientific evidence; Therapy is difficult to standardize; Mortality and incidence may be due to comorbidities; and The linkage between best practices and outcomes has yet to be established Of the four initial hospital core measure sets, only the CAP core measure set contains measures applicable to the pediatric population. Four of the six measures in the CAP core measure set are applicable to pediatrics with populations that include patients 29 days of age and older. These measures include CAP 1, CAP 3, CAP 4b, and CAP 5 and are described in the Individual Measure Descriptions below. Hospital CAP Core Measures Initial Release 29
30 The following six measures comprise the initial set of hospital CAP Core Measures and will be implemented on July 1, CAP-1 Oxygenation assessment CAP-2 Pneumococcal screening and/or vaccination CAP-3 Blood cultures CAP-4a Adult smoking cessation advice/counseling CAP-4b Pediatric smoking cessation advice/counseling CAP-5 Antibiotic timing Hospital CAP Core Measures Delayed Implementation The implementation of the following two measures was delayed because 1999/2000 guideline revisions differed on antibiotic selection for CAP patients. Implementation will be delayed until consensus can be reached among specialty organizations. It is anticipated that the measures will be implemented in late CAP-6 Initial antibiotic selection consistent with current recommendation Intensive Care Unit (ICU) patients CAP-7 Initial antibiotic selection consistent with current recommendations non- Intensive Care Unit (ICU) patients Hospital CAP Core Measures Recommended for Future Core Measure Set Completion The following measures were identified for potential future implementation. The specific date for implementation has not yet been determined. Appropriate timing of IV to oral antibiotic switch Excessive antibiotic use Discharge within 24 hours of IV to oral antibiotic switch Intra-hospital risk adjusted pneumonia mortality rate Inpatients 65 years of age or older who are screened for or given influenza vaccine High risk inpatients less than 65 years of age who are screened for or given influenza vaccine Individual Measure Descriptions: 30
31 The following describes the rational and related considerations underlying each of the measures currently in the Community Acquired Core Measure Set CAP-1 Oxygenation assessment within 24 hours of hospital arrival This measure allows for an oxygenation assessment using either pulse oximetry or arterial blood gas as the diagnostic tool. Questions arose during the pilot test as to whether or not a capillary gas for infants could be used as a substitute for arterial blood gas. The decision, based on pediatric panel member input, was that the capillary gas is not a good measure of oxygenation. Pulse oximetry is a much better measurement and is as good a reflector of oxygenation in infants and children as it is in adults in the vast majority of cases. Data gathered from field studies indicated the initial test most often used was the pulse oximetry. This is usually done in the ED upon arrival and is quick and easy to perform, non-invasive, and cost-effective. Initial data from the pilot test show a mean measure rate of 95%. CAP-2 Inpatients screened for, and/or given pneumococcal vaccination Pneumococcal screening and vaccination is a very important national health issue that transcends the pneumonia diagnosis and measure set. Streptococcus pneumoniae is among the leading infectious causes of illness and death worldwide for young children, persons who have underlying chronic systemic conditions, and in the elderly. It accounts for two-thirds of over 7,000 cases in which an etiologic diagnosis was made, and for twothirds of the cases of lethal pneumonia. It is estimated that 125,000 cases of pneumococcal pneumonia necessitate hospitalization each year. 16 According to guidelines of the Advisory Council on Immunization Practices of the Centers for Disease Control and Prevention (CDC), the major preventive measures for CAP are use of influenza and pneumococcal vaccines. 17 Some stakeholder input suggested that this measure might be better utilized in the outpatient environment; however, many felt strongly that hospitalization was an under-utilized opportunity to provide the vaccine. This measure is limited to patients 65 years of age and older. In the near future, the Joint Commission will seek to provide a pneumonia core measure that focuses on a younger population with risk factors. The current measure first identifies that the patient was screened for pneumococcal vaccination, and if a candidate for the vaccine, the patient must receive it in order to meet the intent of the indicator. The CMS 7 th Scope of Work and Joint Commission measure are identical. 31
32 Preliminary data from the pilot test show a mean measure rate of 29%. Information from onsite pilot test field reviews indicate documentation of screening and vaccination are often missing from the medical record. As a result, data collection has been difficult and time consuming. Many pilot test hospitals have set up processes for screening and created new forms for documentation, thereby making data collection more efficient by locating measure documentation in one place in the medical record. CAP-3 Blood cultures obtained prior to first antibiotic administration The requirement for blood cultures for all hospitalized CAP patients remains a controversial issue. Although there is consensus that blood cultures prior to antibiotics is good practice, there was not sufficiently compelling evidence to infer, through the use of a core measure, that all CAP patients have a blood culture obtained. A guiding principle in the selection of the Joint Commission core measures is that the measures be evidencebased. While there is now emerging evidence in the literature to support blood cultures for all hospitalized CAP patients, the Joint Commission has taken a conservative approach in the selection of a blood culture core measure in order to promote cost effective care and reduce the data collection burden. This measure was selected in October 1999 over other blood culture measures, because the denominator consists of CAP patients who have had a blood culture, as opposed to all CAP patients. Many questions arose during the pilot test relative to patients who had antibiotics given prior to hospital arrival and were then cultured during the hospital stay. In the original version of the measure, such patients were excluded from the population. Early tests also identified that a large number of patients are treated with antibiotics prior to hospital arrival. Often the patients are hospitalized for failure to respond to treatment. Based on further input, it was determined that these patients should be included in the measure population. A new data element antibiotic received was added with allowable values that capture this type of patient. Preliminary data from the pilot test show a mean measure rate of 79%. Information gained from the onsite reliability test indicates initial antibiotic time/date and initial blood culture time/date are well documented and easy to find. CAP-4a Adult CAP smoking cessation counseling CAP-4b Pediatric CAP smoking cessation counseling As with the measure for pneumococcal screening and vaccination, input suggested that tobacco use was an important national health issue that transcends the pneumonia diagnosis and measure set. More than 430,000 deaths each year are attributed to a 32
33 smoking related illness; 18 included in these deaths are roughly 4,000 infants. 19 Furthermore, a high percentage of all smokers (at least 70%) have expressed a desire to quit smoking. 20 Recent studies indicate patients that receive brief smoking-cessation advice from their physicians are more likely to quit than those who receive no counseling at all. The smoking cessation counseling measure selected for the Pneumonia core measure set was adapted from the CMS PRO 6 th Scope of Work (SOW) National AMI Project, and addressed the adult population. The denominator was changed to address CAP patients. Input strongly suggested that pediatric caregivers should also be counseled about the effects of second hand smoke; thus, a second measure was added to address the primary pediatric caregiver, and younger children who smoke. Stakeholder comment acknowledged the positive impact on patient and national health, and the Advisory Panel believed that hospitalization was an excellent opportunity to initiate coordinated interventions that could lead to successful tobacco dependence treatment strategies. However, stakeholder input also indicated a perceived data collection burden. Some indicated that the measures would be more suitable to the ambulatory setting. Preliminary data from the pilot test show a mean measure rate of 35% for the adult smoking measure, and 18% for the pediatric measure, indicating significant room for improvement. Information from onsite pilot test field reviews indicate that documentation of smoking history, and especially smoking counseling, is often missing from the medical record. Some pilot test hospitals created new forms for documentation, or added a category for smoking assessment and counseling to already existing forms, making data collection more efficient. CAP-5 Time from initial hospital arrival to first dose of antibiotic Data strongly support the timing of antibiotics as an important factor in reducing mortality in CAP. The data further suggests that positive effects were seen with administration of antibiotics as early as 4 to 8 hours after admission. Recent studies completed by the Centers for Medicare and Medicaid Services on a data set indicate administration of antibiotics to Medicare patients with pneumonia within 4 hours of hospital arrival is associated with improved in-hospital and 30-day mortality. This has prompted CMS to change their proportion measure to identify patients who received their initial antibiotic within 4 hours of hospital arrival instead of the previous measure that looked at 8 hours. The Joint Commission has chosen to measure antibiotic timing as a continuous variable for multiple reasons relating to both the spirit of the continuous 33
34 quality improvement (CQI) cycle, and the opportunities for robust statistical analyses afforded by the X-bar and S control chart with regard to trending performance data overtime. Both the Joint Commission measure and the Centers for Medicare and Medicaid Services measure are identical at the data element level; therefore data collection is not affected by the difference in data reporting. However, the Joint Commission and CMS realize that both rates are important for quality improvement purposes; therefore, both organizations will report rates for this measure as a proportion and a continuous variable. Throughout the pilot test, questions arose about the measure population exclusion for patients who receive their initial antibiotic greater than 36 hours from the time of hospital arrival. The Joint Commission measure was adapted from the CMS 6 th Scope of Work (SOW) measure where the exclusion existed. CMS excluded these patients since it was assumed that if a physician waits longer than 36 hours to start a patient on an antibiotic, there must be a good reason that the abstraction process may not have identified. For example, the physician may have had a discussion with family members regarding aggressiveness of treatment (patient receiving comfort measures only) that was either not documented or not found. Preliminary data from the pilot test show an average median rate of minutes (3.2 hours). CAP Core Measures Delayed Implementation Increasing antibiotic resistance is an important public health issue underscoring the need to include measures addressing appropriate antibiotic selection for the treatment of CAP. Implementation of the following CAP core measures was delayed when revisions to guidelines from specialty organizations were published last year. Each specialty organization differed in their recommendations for antibiotic selection. Thus, these measures were held until consensus could be reached: CAP-6 Initial antibiotic selection consistent with current recommendations (ICU patients), and CAP-7 Initial antibiotic selection consistent with current recommendations (Non- ICU patients). During the past year, CMS has coordinated efforts among specialty organizations (American Thoracic Society, the Infectious Diseases Society of America, the Center for Disease Control and Prevention, and the Canadian Infectious Disease Society) to achieve a consensus statement thereby providing a simple, comprehensive antibiotic selection performance measure. The work was reviewed by the Joint Commission Pneumonia 34
35 Advisory Panel and, with minor revisions, a table of antibiotics was prepared for the two measures that will be shared by CMS and the Joint Commission. Technical specifications are now being developed and implementation of CAP-6 and CAP-7 for the Joint Commission Pneumonia Core Measure Set is planned for late Future Directions for the CAP Core Measure Set The following areas have been highlighted for future measure evaluation and possible inclusion into the core measure set. Antibiotic Switch Therapy (IV to oral). The panel was impressed with current research in the area of switch therapy and thought it an important area for measurement related to cost-effective care. Existing measures have been identified, and if submitted by the developer(s), will be evaluated for possible inclusion into the set in the future. Measures for influenza screening and vaccination were recommended for inclusion into the pneumonia core measure set following initial panel meetings. One measure was adapted from the CMS PRO 6 th SOW (Inpatients 65 years of age or older who are screened for or given influenza vaccine), and an additional measure was recommended to address high risk CAP patients less than 65 years of age. The implementation of both measures was delayed due to the need to identify salutary mechanisms for accommodating monthly data points and subsequent reporting. In the interim, the Joint Commission encourages health care organizations to utilize hospitalization as an opportunity to screen and vaccinate patients for influenza, as this is one of the major preventive measures for the prevention of CAP. The Pneumonia Advisory Panel recently recommended expanding the measure population of CAP-2 (Pneumococcal screening and vaccination) as identified in current guidelines, to include high risk patients less than 65 years of age, as immunization is one of the major preventive measures for CAP. The recommendation will require the addition of another measure to the pneumonia core measure set. Technical specifications for the measure are being developed and are expected to be released some time next year. A risk adjusted mortality measure to address outcome of care, and a measure for excessive antibiotic use to address increasing antibiotic resistance, were recommended to complete the pneumonia core measure set. The Joint Commission is still in the process of identifying appropriate measures that can be evaluated for inclusion into the set. As mentioned earlier in this section, the Joint Commission and CMS will both report the antibiotic timing measure (CAP-5) as a continuous variable and a 35
36 proportion as the individual measurements yield slightly different information which is thought to be necessary for quality improvement purposes. The Joint Commission will prepare specifications for the proportion measure in early 2002, with release expected later in the year. 36
37 Overview of the Pregnancy and Related Conditions (PR) Core Measure Set (3/22/2002) Pregnancy and related conditions was one of the initial priority focus areas for hospital core measure development identified by key Joint Commission stakeholders. Maternal mortality and morbidity as well as fetal and infant deaths are of continuing concern, along with associated conditions such as preterm births and birth defects. 21 The Joint Commission s pregnancy advisory panel articulated the clinical logic that provided the framework for identifying inter-related, evidence-based measures that, when used together, can more fully assess the overall quality of care provided for pregnancy related patients. All three measures in the Pregnancy and Related Conditions Core Measure Set can be primarily derived from administrative data and have been field tested in conjunction with the National Perinatal Information Center (NPIC) using its trend database to analyze the measures. This testing permitted refinement respecting the measures and provided information pertinent to risk adjustment models. Hospital PR Core Measures Initial Release The following three measures comprise the initial set of hospital Pregnancy and Related Conditions and will be implemented on July 1, PR-1 VBAC PR-2 Inpatient neonatal mortality PR-3 Third or fourth degree laceration Hospital PR Core Measures Recommended for Future Core Measure Set Completion The following measures were identified for potential future implementation. The specific date for implementation has not yet been determined. They have not been included in the initial set because no sufficiently evaluated measures have been identified for implementation at this time. Presence of prenatal record at time of admission Episiotomy rate Indications and/or rate of elective labor induction Primary cesarean section rate Attempted (unsuccessful) vaginal birth after cesarean section Neonatal transfer to perinatal center 37
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014
 CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
International Hospital Inpatient Quality Measures
 I-Acute Myocardial Infarction (I-AMI) I-AMI-1 Aspirin at Arrival Aspirin received within 24 hours of arrival to the hospital for patients having an acute myocardial infarction (AMI). I-AMI-2 Aspirin Prescribed
I-Acute Myocardial Infarction (I-AMI) I-AMI-1 Aspirin at Arrival Aspirin received within 24 hours of arrival to the hospital for patients having an acute myocardial infarction (AMI). I-AMI-2 Aspirin Prescribed
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Hospital Quality Initiative Overview CENTERS FOR MEDICARE & MEDICAID SERVICES December 2005
 Hospital Quality Initiative Overview CENTERS FOR MEDICARE & MEDICAID SERVICES December 2005 Background Quality health care is a high priority for the Bush administration, the Department of Health and Human
Hospital Quality Initiative Overview CENTERS FOR MEDICARE & MEDICAID SERVICES December 2005 Background Quality health care is a high priority for the Bush administration, the Department of Health and Human
Mar. 31, 2011 (202) 690-6145. Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 690-6145. Improving Quality of Care for Medicare Patients: Accountable Care Organizations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology
 Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
OBJECTIVES AGING POPULATION AGING POPULATION AGING IMPACT ON MEDICARE AGING POPULATION
 OBJECTIVES Kimberly S. Hodge, PhDc, MSN, RN, ACNS-BC, CCRN- K Director, ACO Care Management & Clinical Nurse Specialist Franciscan ACO, Inc. Central Indiana Region Indianapolis, IN By the end of this session
OBJECTIVES Kimberly S. Hodge, PhDc, MSN, RN, ACNS-BC, CCRN- K Director, ACO Care Management & Clinical Nurse Specialist Franciscan ACO, Inc. Central Indiana Region Indianapolis, IN By the end of this session
Office of Rural Health Policy MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT
 Office of Rural Health Policy MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT Paul Moore, DPh Senior Health Policy Advisor Office of Rural Health Policy Health Resources and Services Administration Department
Office of Rural Health Policy MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT Paul Moore, DPh Senior Health Policy Advisor Office of Rural Health Policy Health Resources and Services Administration Department
Aligning Incentives for Quality: Pharmacy's Role in Achieving Hospital and National Goals. Objectives. National Organizations: Key Linkages
 Aligning Incentives for Quality: Pharmacy's Role in Achieving Hospital and National Goals Kasey K. Thompson, Pharm.D. Director, Practice Standards and Quality Division Director, Patient Safety American
Aligning Incentives for Quality: Pharmacy's Role in Achieving Hospital and National Goals Kasey K. Thompson, Pharm.D. Director, Practice Standards and Quality Division Director, Patient Safety American
Radiology Business Management Association Technology Task Force. Sample Request for Proposal
 Technology Task Force Sample Request for Proposal This document has been created by the RBMA s Technology Task Force as a guideline for use by RBMA members working with potential suppliers of Electronic
Technology Task Force Sample Request for Proposal This document has been created by the RBMA s Technology Task Force as a guideline for use by RBMA members working with potential suppliers of Electronic
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Medicare Patients: Overview The Centers for Medicare & Medicaid Services (), an agency within the Department
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Medicare Patients: Overview The Centers for Medicare & Medicaid Services (), an agency within the Department
Congestive Heart Failure Management Program
 Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
MEASURING CARE QUALITY
 MEASURING CARE QUALITY Region November 2015 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
MEASURING CARE QUALITY Region November 2015 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
Clinical Quality Measure Crosswalk: HEDIS, Meaningful Use, PQRS, PCMH, Beacon, 10 SOW
 Clinical Crosswalk: HEDIS, Meaningful Use, PQRS, PCMH, Beacon, 10 SOW NQF 0105 PQRS 9 NQF 0002 PQRS 66 Antidepressant Medication Management Appropriate Testing for Children with Pharyngitis (2-18 years)
Clinical Crosswalk: HEDIS, Meaningful Use, PQRS, PCMH, Beacon, 10 SOW NQF 0105 PQRS 9 NQF 0002 PQRS 66 Antidepressant Medication Management Appropriate Testing for Children with Pharyngitis (2-18 years)
Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary. http://www.cms.gov/ehrincentiveprograms/
 Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary 2010 What are the Requirements of Stage 1 Meaningful Use? Basic Overview of Stage 1 Meaningful Use: Reporting period
Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary 2010 What are the Requirements of Stage 1 Meaningful Use? Basic Overview of Stage 1 Meaningful Use: Reporting period
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #317: Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented National Quality Strategy Domain: Community / Population Health 2016 PQRS OPTIONS F INDIVIDUAL MEASURES:
Measure #317: Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented National Quality Strategy Domain: Community / Population Health 2016 PQRS OPTIONS F INDIVIDUAL MEASURES:
11/2/2015 Domain: Care Coordination / Patient Safety
 11/2/2015 Domain: Care Coordination / Patient Safety 2014 CT Commercial Medicaid Compared to 2012 all LOB Medicaid Quality Compass Benchmarks 2 3 4 5 6 7 8 9 10 Documentation of Current Medications in
11/2/2015 Domain: Care Coordination / Patient Safety 2014 CT Commercial Medicaid Compared to 2012 all LOB Medicaid Quality Compass Benchmarks 2 3 4 5 6 7 8 9 10 Documentation of Current Medications in
Healthcare Data: Secondary Use through Interoperability
 Healthcare Data: Secondary Use through Interoperability Floyd Eisenberg MD MPH July 18, 2007 NCVHS Agenda Policies, Enablers, Restrictions Date Re-Use Landscape Sources of Data for Quality Measurement,
Healthcare Data: Secondary Use through Interoperability Floyd Eisenberg MD MPH July 18, 2007 NCVHS Agenda Policies, Enablers, Restrictions Date Re-Use Landscape Sources of Data for Quality Measurement,
Relevant Quality Measures for Critical Access Hospitals
 Policy Brief #5 January 0 Relevant Quality Measures for Critical Access Hospitals Michelle Casey MS, Ira Moscovice PhD, Jill Klingner RN, PhD, Shailendra Prasad MD, MPH University of Minnesota Rural Health
Policy Brief #5 January 0 Relevant Quality Measures for Critical Access Hospitals Michelle Casey MS, Ira Moscovice PhD, Jill Klingner RN, PhD, Shailendra Prasad MD, MPH University of Minnesota Rural Health
Chapter Three Accountable Care Organizations
 Chapter Three Accountable Care Organizations One of the most talked-about changes in health care delivery in recent decades is Accountable Care Organizations, or ACOs. Having gained the attention of both
Chapter Three Accountable Care Organizations One of the most talked-about changes in health care delivery in recent decades is Accountable Care Organizations, or ACOs. Having gained the attention of both
Psychiatrists and Reporting on Meaningful Use Stage 1. August 6, 2012
 Psychiatrists and Reporting on Meaningful Use Stage 1 August 6, 2012 Quick Overview Functional Measures Providers (tracked by NPI) must report on 15 core objectives and associated measures and 5 objectives
Psychiatrists and Reporting on Meaningful Use Stage 1 August 6, 2012 Quick Overview Functional Measures Providers (tracked by NPI) must report on 15 core objectives and associated measures and 5 objectives
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Improving America s Hospitals
 Improving America s Hospitals The Joint Commission s Annual Report on Quality and Safety 2010 Improving America s Hospitals: The Joint Commission s Annual Report on Quality and Safety 2010 Table of Contents
Improving America s Hospitals The Joint Commission s Annual Report on Quality and Safety 2010 Improving America s Hospitals: The Joint Commission s Annual Report on Quality and Safety 2010 Table of Contents
Acute Coronary Syndrome
 Acute Coronary Syndrome Quality Measures Length of Stay RCC Costs per Case Critical Event(s) Evaluation /Acute Phase ECG ASA on arrival (unless documented contraindication) Troponin STAT, repeat once in
Acute Coronary Syndrome Quality Measures Length of Stay RCC Costs per Case Critical Event(s) Evaluation /Acute Phase ECG ASA on arrival (unless documented contraindication) Troponin STAT, repeat once in
Stage 1 Meaningful Use for Specialists. NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene
 Stage 1 Meaningful Use for Specialists NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene 1 Today s Agenda Meaningful Use Overview Meaningful Use Measures Resources Primary
Stage 1 Meaningful Use for Specialists NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene 1 Today s Agenda Meaningful Use Overview Meaningful Use Measures Resources Primary
Rural Health Information Technology Cooperative. Clinician Survey on Quality Improvement, Best Practice Guidelines, and Information Technology
 Rural Health Information Technology Cooperative Clinician Survey on Quality Improvement, Best Practice Guidelines, and Information Technology Conducted for: The Rural Healthcare Quality Network Conducted
Rural Health Information Technology Cooperative Clinician Survey on Quality Improvement, Best Practice Guidelines, and Information Technology Conducted for: The Rural Healthcare Quality Network Conducted
America s Hospitals: Improving Quality and Safety
 America s Hospitals: Improving Quality and Safety The Joint Commission s Annual Report 2014 Top Performer on Key Quality Measures America s Hospitals: Improving Quality and Safety The Joint Commission
America s Hospitals: Improving Quality and Safety The Joint Commission s Annual Report 2014 Top Performer on Key Quality Measures America s Hospitals: Improving Quality and Safety The Joint Commission
Manitoba EMR Data Extract Specifications
 MANITOBA HEALTH Manitoba Data Specifications Version 1 Updated: August 14, 2013 1 Introduction The purpose of this document 1 is to describe the data to be included in the Manitoba Data, including the
MANITOBA HEALTH Manitoba Data Specifications Version 1 Updated: August 14, 2013 1 Introduction The purpose of this document 1 is to describe the data to be included in the Manitoba Data, including the
REACHING ZERO DEFECTS IN CORE MEASURES. Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC,
 REACHING ZERO DEFECTS IN CORE MEASURES Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC, 165 Lake Linden Dr., Bluffton SC 29910, 843-364-3408, marybrady6@gmail.com Primary
REACHING ZERO DEFECTS IN CORE MEASURES Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC, 165 Lake Linden Dr., Bluffton SC 29910, 843-364-3408, marybrady6@gmail.com Primary
ACO Program: Quality Reporting Requirements. Jennifer Faerberg Mary Wheatley April 28, 2011
 ACO Program: Quality Reporting Requirements Jennifer Faerberg Mary Wheatley April 28, 2011 Agenda for Today s Call Overview Quality Reporting Requirements Benchmarks/Thresholds Scoring Model Scoring Methodology
ACO Program: Quality Reporting Requirements Jennifer Faerberg Mary Wheatley April 28, 2011 Agenda for Today s Call Overview Quality Reporting Requirements Benchmarks/Thresholds Scoring Model Scoring Methodology
Mission: Lifeline Recommendations for Criteria for STEMI Systems of Care
 Mission: Lifeline Recommendations for Criteria for STEMI Systems of Care The Mission: Lifeline Certification Program will acknowledge STEMI Systems, EMS, Non-PCI/STEMI Referral Centers and PCI/STEMI Receiving
Mission: Lifeline Recommendations for Criteria for STEMI Systems of Care The Mission: Lifeline Certification Program will acknowledge STEMI Systems, EMS, Non-PCI/STEMI Referral Centers and PCI/STEMI Receiving
NHS outcomes framework and CCG outcomes indicators: Data availability table
 NHS outcomes framework and CCG outcomes indicators: Data availability table December 2012 NHS OF objectives Preventing people from dying prematurely DOMAIN 1: preventing people from dying prematurely Potential
NHS outcomes framework and CCG outcomes indicators: Data availability table December 2012 NHS OF objectives Preventing people from dying prematurely DOMAIN 1: preventing people from dying prematurely Potential
Value-Based Purchasing
 Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Summary Evaluation of the Medicare Lifestyle Modification Program Demonstration and the Medicare Cardiac Rehabilitation Benefit
 The Centers for Medicare & Medicaid Services' Office of Research, Development, and Information (ORDI) strives to make information available to all. Nevertheless, portions of our files including charts,
The Centers for Medicare & Medicaid Services' Office of Research, Development, and Information (ORDI) strives to make information available to all. Nevertheless, portions of our files including charts,
CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM
 For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
Introduction. The History of CMS/JCAHO Measure Alignment
 Release Notes: Introduction - Version 2.2 Introduction The History of CMS/JCAHO Measure Alignment In early 1999, the Joint Commission solicited input from a wide variety of stakeholders (e.g., clinical
Release Notes: Introduction - Version 2.2 Introduction The History of CMS/JCAHO Measure Alignment In early 1999, the Joint Commission solicited input from a wide variety of stakeholders (e.g., clinical
Improving Hospital Performance
 Improving Hospital Performance Background AHA View Putting patients first ensuring their care is centered on the individual, rooted in best practices and utilizes the latest evidence-based medicine is
Improving Hospital Performance Background AHA View Putting patients first ensuring their care is centered on the individual, rooted in best practices and utilizes the latest evidence-based medicine is
6. MEASURING EFFECTS OVERVIEW CHOOSE APPROPRIATE METRICS
 45 6. MEASURING EFFECTS OVERVIEW In Section 4, we provided an overview of how to select metrics for monitoring implementation progress. This section provides additional detail on metric selection and offers
45 6. MEASURING EFFECTS OVERVIEW In Section 4, we provided an overview of how to select metrics for monitoring implementation progress. This section provides additional detail on metric selection and offers
CYSTIC FIBROSIS CLINICS AS A MODEL OF INTERPROFESSIONAL CARE
 CYSTIC FIBROSIS CLINICS AS A MODEL OF INTERPROFESSIONAL CARE 1. Cystic fibrosis introduction 2. CF Foundation centers 3. Care disciplines: physician specialists (pulmonary, GI, endocrine, genetics, palliative
CYSTIC FIBROSIS CLINICS AS A MODEL OF INTERPROFESSIONAL CARE 1. Cystic fibrosis introduction 2. CF Foundation centers 3. Care disciplines: physician specialists (pulmonary, GI, endocrine, genetics, palliative
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION
 LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
New Jersey Delivery System Reform Incentive Program
 New Jersey Delivery System Reform Incentive Program The New Jersey Delivery System Reform Incentive Program (DSRIP) is part of New Jersey s Comprehensive Medicaid Waiver. The program provides incentive
New Jersey Delivery System Reform Incentive Program The New Jersey Delivery System Reform Incentive Program (DSRIP) is part of New Jersey s Comprehensive Medicaid Waiver. The program provides incentive
Objectives. Preoperative Cardiac Risk Stratification for Noncardiac Surgery. History
 Preoperative Cardiac Risk Stratification for Noncardiac Surgery Kimberly Boddicker, MD FACC Essentia Health Heart and Vascular Center 27 th Heart and Vascular Conference May 13, 2011 Objectives Summarize
Preoperative Cardiac Risk Stratification for Noncardiac Surgery Kimberly Boddicker, MD FACC Essentia Health Heart and Vascular Center 27 th Heart and Vascular Conference May 13, 2011 Objectives Summarize
Population Health Management Program
 Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
Re: CMS-1345-P; Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations; Proposed Rule
 Department of Health and Human Services Attention: CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re: CMS-1345-P; Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations;
Department of Health and Human Services Attention: CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re: CMS-1345-P; Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations;
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
Advanced Heart Failure & Transplantation Fellowship Program
 Advanced Heart Failure & Transplantation Fellowship Program Curriculum I. Patient Care When on the inpatient Heart Failure and Transplant Cardiology service, the cardiology fellow will hold primary responsibility
Advanced Heart Failure & Transplantation Fellowship Program Curriculum I. Patient Care When on the inpatient Heart Failure and Transplant Cardiology service, the cardiology fellow will hold primary responsibility
HOSPITAL VALUE- BASED PURCHASING. Initial Results Show Modest Effects on Medicare Payments and No Apparent Change in Quality-of- Care Trends
 United States Government Accountability Office Report to Congressional Committees October 2015 HOSPITAL VALUE- BASED PURCHASING Initial Results Show Modest Effects on Medicare Payments and No Apparent
United States Government Accountability Office Report to Congressional Committees October 2015 HOSPITAL VALUE- BASED PURCHASING Initial Results Show Modest Effects on Medicare Payments and No Apparent
CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE. Las Vegas, Nevada Bellagio March 4 6, 2016. Participating Faculty
 CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE Las Vegas, Nevada Bellagio March 4 6, 2016 Participating Faculty Friday, March 4th: 7:30 am - 8:00 am Registration and Hot Breakfast 8:00 am - 9:00 am Pulmonary
CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE Las Vegas, Nevada Bellagio March 4 6, 2016 Participating Faculty Friday, March 4th: 7:30 am - 8:00 am Registration and Hot Breakfast 8:00 am - 9:00 am Pulmonary
Educational Goals & Objectives
 Educational Goals & Objectives The Cardiology rotation will provide the resident with an understanding of cardiovascular physiology and its broad systemic manifestations. The resident will have the opportunity
Educational Goals & Objectives The Cardiology rotation will provide the resident with an understanding of cardiovascular physiology and its broad systemic manifestations. The resident will have the opportunity
Chapter 6 Case Ascertainment Methods
 Chapter 6 Case Ascertainment Methods Table of Contents 6.1 Introduction...6-1 6.2 Terminology...6-2 6.3 General Surveillance Development...6-4 6.3.1 Plan and Document... 6-4 6.3.2 Identify Data Sources...
Chapter 6 Case Ascertainment Methods Table of Contents 6.1 Introduction...6-1 6.2 Terminology...6-2 6.3 General Surveillance Development...6-4 6.3.1 Plan and Document... 6-4 6.3.2 Identify Data Sources...
ECG may be indicated for patients with cardiovascular risk factors
 eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
GAO HOSPITAL QUALITY DATA. HHS Should Specify Steps and Time Frame for Using Information Technology to Collect and Submit Data
 GAO United States Government Accountability Office Report to the Committee on Finance, U.S. Senate April 2007 HOSPITAL QUALITY DATA HHS Should Specify Steps and Time Frame for Using Information Technology
GAO United States Government Accountability Office Report to the Committee on Finance, U.S. Senate April 2007 HOSPITAL QUALITY DATA HHS Should Specify Steps and Time Frame for Using Information Technology
Telehealth and the Homebound Heart Failure Patient
 Telehealth and the Homebound Heart Failure Patient By Karen Malin Garfield, RN, BSN 104 HEART 2010 The Official Guide to a Strong Heart and Healthy Lifestyle PTS Article Heart2010_Suncrest.indd 1 Health
Telehealth and the Homebound Heart Failure Patient By Karen Malin Garfield, RN, BSN 104 HEART 2010 The Official Guide to a Strong Heart and Healthy Lifestyle PTS Article Heart2010_Suncrest.indd 1 Health
Renovascular Hypertension
 Renovascular Hypertension Philip Stockwell, MD Assistant Professor of Medicine (Clinical) Warren Alpert School of Medicine Cardiology for the Primary Care Provider September 28, 201 Renovascular Hypertension
Renovascular Hypertension Philip Stockwell, MD Assistant Professor of Medicine (Clinical) Warren Alpert School of Medicine Cardiology for the Primary Care Provider September 28, 201 Renovascular Hypertension
Immunization Infrastructure: The Role of Section 317
 Immunization Infrastructure: The Role of Section 317 Immunization plays a vital role in the control and prevention of infectious disease. Current immunization recommendations target 17 vaccine-preventable
Immunization Infrastructure: The Role of Section 317 Immunization plays a vital role in the control and prevention of infectious disease. Current immunization recommendations target 17 vaccine-preventable
AnMed Health Disparities Dashboard
 AnMed Health Quick Facts 588 Bed Acute Care System Level II Trauma Center Emergency Department visits: 112,329 Admissions: 23,489 Active Medical Staff: 455 Employees: 3,511 Source : CY2013 Setting the
AnMed Health Quick Facts 588 Bed Acute Care System Level II Trauma Center Emergency Department visits: 112,329 Admissions: 23,489 Active Medical Staff: 455 Employees: 3,511 Source : CY2013 Setting the
3/2/2010 Post CABG R h e bili a i tat on Ahmed Elkerdany Professor o f oof C ardiac Cardiac Surgery Ain Shams University 1
 Post CABG Rehabilitation i Ahmed Elkerdany Professor of Cardiac Surgery Ain Shams University 1 Definition Cardiac rehabilitation services are comprehensive, long-term programs involving : medical evaluation.
Post CABG Rehabilitation i Ahmed Elkerdany Professor of Cardiac Surgery Ain Shams University 1 Definition Cardiac rehabilitation services are comprehensive, long-term programs involving : medical evaluation.
ACCOUNTABLE CARE ORGANIZATION QUICK-REFERENCE SETUP GUIDE
 ACCOUNTABLE CARE ORGANIZATION QUICK-REFERENCE SETUP GUIDE V 9.0 eclinicalworks, 2013. All rights reserved Contents CONTENTS ACO SETUP 3 Demographics 3 ACO 12 4 ACO 13 6 ACO 14 7 ACO 15 8 ACO 16 9 ACO 17
ACCOUNTABLE CARE ORGANIZATION QUICK-REFERENCE SETUP GUIDE V 9.0 eclinicalworks, 2013. All rights reserved Contents CONTENTS ACO SETUP 3 Demographics 3 ACO 12 4 ACO 13 6 ACO 14 7 ACO 15 8 ACO 16 9 ACO 17
Community health care services Alternatives to acute admission & Facilitated discharge options. Directory
 Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Goal 1; Objective B: Improve health care quality and patient safety: Performance measure
 TRUST FOR AMERICA S HEALTH COMMENTS ON THE DEPARTMENT OF HEALTH AND HUMAN SERVICES (HHS) DRAFT STRATEGIC PLAN 2010 2015 Goal 1; Objective B: Improve health care quality and patient safety: Performance
TRUST FOR AMERICA S HEALTH COMMENTS ON THE DEPARTMENT OF HEALTH AND HUMAN SERVICES (HHS) DRAFT STRATEGIC PLAN 2010 2015 Goal 1; Objective B: Improve health care quality and patient safety: Performance
HEDIS/CAHPS 101. August 13, 2012 Minnesota Measurement and Reporting Workgroup
 HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
Guidelines for the management of hypertension in patients with diabetes mellitus
 Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
ABELMed EHR-EMR/PM version 12, an ONC HIT 2014 Edition Complete EHR, has been certified for the following 42 clinical quality measures (CQMs).
.") ABELMed EHR-EMR/PM version 12, an ONC HIT 2014 Edition Complete EHR, has been certified for the following 42 clinical quality measures (CQMs). The information contained in this document is also available
ABELMed EHR-EMR/PM version 12, an ONC HIT 2014 Edition Complete EHR, has been certified for the following 42 clinical quality measures (CQMs). The information contained in this document is also available
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
2012 Physician Quality Reporting System:
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Official CMS Information for Medicare Fee-For-Service Providers 2012 Physician Quality : Medicare Electronic Health Record
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Official CMS Information for Medicare Fee-For-Service Providers 2012 Physician Quality : Medicare Electronic Health Record
EMR Tutorial Acute Coronary Syndrome
 EMR Tutorial Acute Coronary Syndrome How to find the Acute Coronary Syndrome AAA Home Page 1 of 26 Master Tool Bar Icon When the Template button is clicked you will be presented with the preference list.
EMR Tutorial Acute Coronary Syndrome How to find the Acute Coronary Syndrome AAA Home Page 1 of 26 Master Tool Bar Icon When the Template button is clicked you will be presented with the preference list.
Medicaid Health Plans: Adding Value for Beneficiaries and States
 Medicaid Health Plans: Adding Value for Beneficiaries and States Medicaid is a program with numerous challenges, both for its beneficiaries and the state and federal government. In comparison to the general
Medicaid Health Plans: Adding Value for Beneficiaries and States Medicaid is a program with numerous challenges, both for its beneficiaries and the state and federal government. In comparison to the general
Critical Care Billing and Coding. Date: February 2015 Presented by: Part B Provider Outreach & Education (POE)
") Critical Care Billing and Coding Date: February 2015 Presented by: Part B Provider Outreach & Education (POE) Workshop Protocol Cannot register with WebEx using mobile device Must use desktop or laptop
Critical Care Billing and Coding Date: February 2015 Presented by: Part B Provider Outreach & Education (POE) Workshop Protocol Cannot register with WebEx using mobile device Must use desktop or laptop
. 4 " ~ f.".2 DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL. December 19,2003. Our Reference: Report Number A-O2-03-01016
 . 4 " ~..+.-"..i"..,. f.".2 '" '" ~ DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL Office of Audit Services Region II Jacob K. Javits Federal Building New York, New York 10278 (212)
. 4 " ~..+.-"..i"..,. f.".2 '" '" ~ DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL Office of Audit Services Region II Jacob K. Javits Federal Building New York, New York 10278 (212)
Overview of Clinical Quality Measures Reporting in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use
 Final Rule on Meaningful Use") Overview of Clinical Quality Measures Reporting in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use Clinical Quality Measures Clinical quality measures have been defined
Overview of Clinical Quality Measures Reporting in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use Clinical Quality Measures Clinical quality measures have been defined
Chapter Seven Value-based Purchasing
 Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Quality standard Published: 11 June 2015 nice.org.uk/guidance/qs89
 Pressure ulcers Quality standard Published: 11 June 2015 nice.org.uk/guidance/qs89 NICE 2015. All rights reserved. Contents Introduction... 6 Why this quality standard is needed... 6 How this quality standard
Pressure ulcers Quality standard Published: 11 June 2015 nice.org.uk/guidance/qs89 NICE 2015. All rights reserved. Contents Introduction... 6 Why this quality standard is needed... 6 How this quality standard
on a daily basis. On the whole, however, those with heart disease are more limited in their activities, including work.
 Heart Disease A disabling yet preventable condition Number 3 January 2 NATIONAL ACADEMY ON AN AGING SOCIETY Almost 18 million people 7 percent of all Americans have heart disease. More than half of the
Heart Disease A disabling yet preventable condition Number 3 January 2 NATIONAL ACADEMY ON AN AGING SOCIETY Almost 18 million people 7 percent of all Americans have heart disease. More than half of the
ACTION Registry - GWTG: Defect Free Care for Acute Myocardial Infarction Specifications and Testing Overview
 Measure Purpose Numerator To provide defect free AMI care to all patients. Meaning all of the ACC/AHA endorsed performance measures are followed for eligible patients. Count of Care patients that received
Measure Purpose Numerator To provide defect free AMI care to all patients. Meaning all of the ACC/AHA endorsed performance measures are followed for eligible patients. Count of Care patients that received
The Flex Program MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT
 Office of Rural Health Policy 2012 Rural Health Information Technology Network Development Grantee Meeting The Flex Program MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT Paul Moore, DPh Senior Health
Office of Rural Health Policy 2012 Rural Health Information Technology Network Development Grantee Meeting The Flex Program MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT Paul Moore, DPh Senior Health
Clinical Audit in Hospital Authority. Dr Betty Young Convenor for Clinical Audit, Hospital Authority
 Clinical Audit in Hospital Authority Dr Betty Young Convenor for Clinical Audit, Hospital Authority Background 1990 1992 1996 1998 2005 Establishment of the Hospital Authority Quality Assurance Subcommittee
Clinical Audit in Hospital Authority Dr Betty Young Convenor for Clinical Audit, Hospital Authority Background 1990 1992 1996 1998 2005 Establishment of the Hospital Authority Quality Assurance Subcommittee
Provider Manual. Section 18.0 - Case Management and Disease Management
 Section 18.0 - Case Management and Disease Management 18.1.1 Introduction 18.2.1 Scope 18.3.1 Objectives 18.4.1 Procedures Case Management 18.4.1-A. Referrals 18.4.1-B. Case Management Mercy Maricopa Acute
Section 18.0 - Case Management and Disease Management 18.1.1 Introduction 18.2.1 Scope 18.3.1 Objectives 18.4.1 Procedures Case Management 18.4.1-A. Referrals 18.4.1-B. Case Management Mercy Maricopa Acute
TO: FROM: DATE: RE: Mid-Year Updates Note: NCQA Benchmarks & Thresholds 2014
 TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: July 25, 2014 RE: 2014 Accreditation Benchmarks and Thresholds Mid-Year Update This document reports national benchmarks
TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: July 25, 2014 RE: 2014 Accreditation Benchmarks and Thresholds Mid-Year Update This document reports national benchmarks
Service delivery interventions
 Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Measure #236 (NQF 0018): Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care
: Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care") Measure #236 (NQF 0018): Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients
Measure #236 (NQF 0018): Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients
National Provider Call: Hospital Value-Based Purchasing (VBP) Program
 Program") National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
Facts about Diabetes in Massachusetts
 Facts about Diabetes in Massachusetts Diabetes is a disease in which the body does not produce or properly use insulin (a hormone used to convert sugar, starches, and other food into the energy needed
Facts about Diabetes in Massachusetts Diabetes is a disease in which the body does not produce or properly use insulin (a hormone used to convert sugar, starches, and other food into the energy needed
2014 Medicare Physician Fee Schedule Proposed Rule Quality Provisions
 2014 Medicare Physician Fee Schedule Proposed Rule Quality Provisions The 2014 Medicare Physician Fee Schedule (MPFS) Notice of Proposed Rulemaking (NPRM) was published in the Federal Register on July
2014 Medicare Physician Fee Schedule Proposed Rule Quality Provisions The 2014 Medicare Physician Fee Schedule (MPFS) Notice of Proposed Rulemaking (NPRM) was published in the Federal Register on July
6/5/2014. Objectives. Acute Coronary Syndromes. Epidemiology. Epidemiology. Epidemiology and Health Care Impact Pathophysiology
 Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Key Performance Measures for School-Based Health Centers
 Key Performance Measures for School-Based Health Centers As health care reform continues to take shape and additional provisions of the Affordable Care Act are implemented, there is an increasing demand
Key Performance Measures for School-Based Health Centers As health care reform continues to take shape and additional provisions of the Affordable Care Act are implemented, there is an increasing demand
Time for a Cool Change Measure and Compare
 Time for a Cool Change Measure and BRENDA BARTKOWSKI, CMA, CCA, BS HPA M ANAGER, C LINICAL D ATA A BSTRACTION About Amphion Dedicated core measure staff Experienced leadership in healthcare technology
Time for a Cool Change Measure and BRENDA BARTKOWSKI, CMA, CCA, BS HPA M ANAGER, C LINICAL D ATA A BSTRACTION About Amphion Dedicated core measure staff Experienced leadership in healthcare technology
Hospital Performance Comparisons, 2006
 Hospital Performance Comparisons, 2006 A REPORT ON QUALITY OF CARE IN CONNECTICUT HOSPITALS Joan Foland, M.Phil, M.H.S. Lloyd Mueller, Ph.D. State of Connecticut Department of Public Health Planning Branch
Hospital Performance Comparisons, 2006 A REPORT ON QUALITY OF CARE IN CONNECTICUT HOSPITALS Joan Foland, M.Phil, M.H.S. Lloyd Mueller, Ph.D. State of Connecticut Department of Public Health Planning Branch
Data, Outcomes and Population Health Management. CPPEG January 2016
 Data, Outcomes and Population Health Management CPPEG January 216 NHS Outcomes Framework There are national outcome measures which the CCG is held to account on. In conjunction to monitoring these the
Data, Outcomes and Population Health Management CPPEG January 216 NHS Outcomes Framework There are national outcome measures which the CCG is held to account on. In conjunction to monitoring these the
Ohio Health Homes Learning Community Meeting. Overview of Health Homes Measures
 Ohio Health Homes Learning Community Meeting Overview of Health Homes Measures Tuesday, March 5, 2013 Presenter: Amber Saldivar, MHSM Associate Director, Informatics Analysis Health Services Advisory Group,
Ohio Health Homes Learning Community Meeting Overview of Health Homes Measures Tuesday, March 5, 2013 Presenter: Amber Saldivar, MHSM Associate Director, Informatics Analysis Health Services Advisory Group,
Medical Management Program
 Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Medicare EHR Incentive Program - Meaningful Use
 EHR Incentive Programs A program administered by the Centers for Medicare & Medicaid Services (CMS) An Introduction to the Medicare EHR Incentive Program for Eligible Professionals cms.gov/ehrincentiveprograms
EHR Incentive Programs A program administered by the Centers for Medicare & Medicaid Services (CMS) An Introduction to the Medicare EHR Incentive Program for Eligible Professionals cms.gov/ehrincentiveprograms
May 7, 2012. Submitted electronically via www.regulations.gov. Re: CMS 0044 P. Dear Administrator Tavenner:
 Marilyn Tavenner Administrator Centers for Medicare and Medicaid Services (CMS) Department of Health and Human Services P.O. Box 8013 Baltimore MD 21244 8013 Submitted electronically via www.regulations.gov
Marilyn Tavenner Administrator Centers for Medicare and Medicaid Services (CMS) Department of Health and Human Services P.O. Box 8013 Baltimore MD 21244 8013 Submitted electronically via www.regulations.gov
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
2013 MEDICARE FEE-FOR-SERVICE QUALITY AND RESOURCE USE REPORT
 2013 MEDICARE FEE-FOR-SERVICE QUALITY AND RESOURCE USE REPORT Sample Medical Practice Last Four Digits of Your Taxpayer Identification Number (TIN): 1530 ABOUT THIS REPORT FROM MEDICARE WHAT This Quality
2013 MEDICARE FEE-FOR-SERVICE QUALITY AND RESOURCE USE REPORT Sample Medical Practice Last Four Digits of Your Taxpayer Identification Number (TIN): 1530 ABOUT THIS REPORT FROM MEDICARE WHAT This Quality