LOW GRADE GLIOMAS. Joe Waller, MD, MPH OHSU Dept. of Radiation Medicine PGY2 3/17/2010
|
|
|
- Tracey Sharp
- 7 years ago
- Views:
Transcription
1 LOW GRADE GLIOMAS Joe Waller, MD, MPH OHSU Dept. of Radiation Medicine PGY2 3/17/2010
2 Objectives Learn the specific histologies Learn basic epidemiology Learn common presenting s/s Learn EBM for treatments Understand the controversy of RT Appreciate the toxicities of radiation Briefly identify future directions for treatment
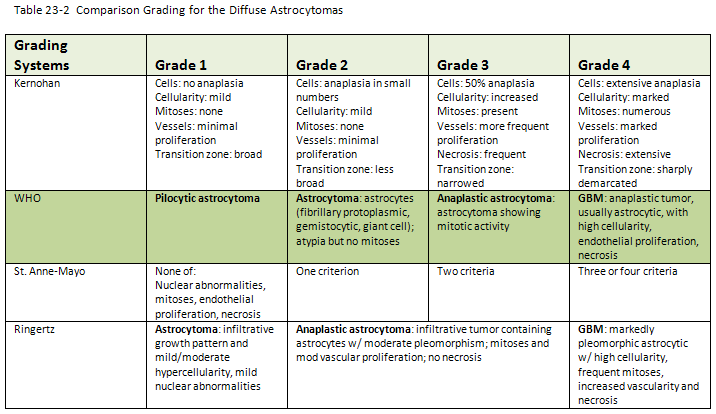
3 Histology
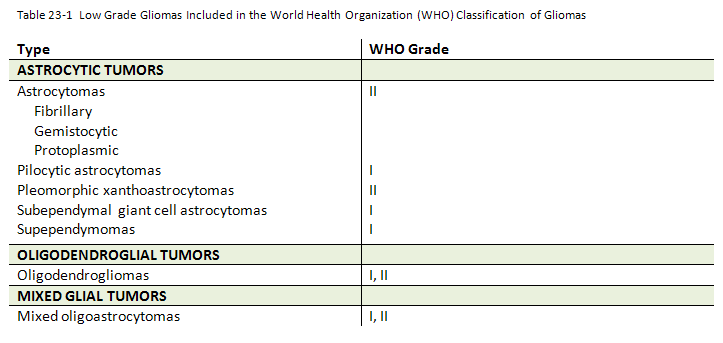
4 Histology
5 Histology Pilocytic astrocytomas (I) ~30% of astrocytomas More common cerebellum of children (JPA) Better circumscribed, often w/ cystic component Rarely transform Diffuse astrocytomas: Fibrillary, gemistocytic, protoplasmic (II) Represent 70% of low grade astrocytomas Poorly circumscribed 50-72% incidence of anaplastic transformation
6 Epidemiology Incidence: 1/100, : 18,820 CNS tumors 16,400 CNS primary ~10% CNS primary 8,200 gliomas» 2,000 low grade ~20-25% GBM 30% Meningioma 15% Pituitary 10% AA 10% LG astrocytomas 10% Schwannoma 5-10% Oligodendroglioma < 5%
7 Epidemiology Age: mean age 37 yrs range 7mos 78 yrs JPA yrs, Grade II yrs More common in males 1.4:1 Etiology: largely unknown NF-1 and NF-2 and astrocytomas NF1: NF2: optic glioma acoustic glioma subependymal giant cell astrocytoma Tuberous sclerosis:
8 Biology DNA 2:1 ratio of diploid to aneuploid Tumor proliferation Ki-67 marker (MIB-I) Montine 1994 study Ki-67 index +/- 3% expression prognostically important Ki-67 more related to OS than grade Other studies have not confirmed Cytogenic/molecular 30-35% have 17p alterations p53 p53 mutations poor prognostic factor 1p and 19q deletions more common in oligodendrogliomas and Grade III/IV
9 Biology MGMT O 6 -Methylguanine-DNA methyltransferase DNA repair enzyme Repairs damage induced by alkylating agents such as Temodar Therefore, active MGMT poorer outcomes Established in HGG LGG? VEGF Abdulrauf study: median survival 11.2 yrs v 5.3 yrs for VEGF +/- No such association w/ other growth factors: FGF, EGF Two precursor cell lines: Type I, protoplasmic astrocytes, reside in cortex INDOLENT Type II, fibrillary astrocytes, found in white matter AGGRESSIVE
10 Presentation - Sxs Seizure 67% Focal most common Generalized tonic-clonic 43% Simple partial 23% Complex partial 34% Headaches, weakness 33% Remainder < 15% Visual change/loss Personality change Focal sx NOS Sx onset to dx: 6-17mos Language dysfunction Altered sensation n/v AMS Altered consciousness Cranial neuropathy
11 Presentation - Signs 50% neurologically intact Sensory or motor deficit 42% AMS 23% Papilledema 22% Aphasia/dysphasia 20% Decreased memory 20% Focal deficit 15% Altered consciousness 8% Motor deficit 8% Take home: Normal/mild neuro dysfx 65% Moderate neuro dysfx 25% Severe neuro dysfx 10%
12 + Prognostic Factors Oligo component KPS prior to surgery Age < 40 most powerful predictor > 40 v 40+ mean survival of 10.7 v 8.1 yrs respectively ~90% 10 yr survival in children Seizure 5 yr survival: 64% w/ vs 14% w/o Long sx to dx interval > 6 mos 1p/19q deletion Ki-67 index MGMT ( methylation) One sided Radical/complete resection T stage (< 6cm) Previously untreated Median survival 9.7 mos 2 yr OS 29% EORTC 22844/22845 data < 3: low risk 3+: high risk
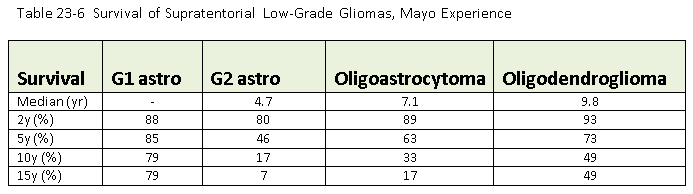
13 Prognosis
14 Staging None T parameter proposed by EORTC T1a diameter <=3 cm, confined to one side T1b diameter <=5 cm, unilaterally or small centrally T2 Diameter >5 cm but < 10 cm but not crossing midline T3 Any size encroaching on ventricles but not crossing midline T4 Any massive tumor not conforming to T3, crossing the midline or tentorium
15 Treatment Observation? Surgery + observation? Surgery + RT? Surgery + chemo? Surgery + chemort?
 < GTR 60%")
16 Surgery Extent resection 39% GTR or major subtotal 23% STR 38% minor subtotal or bx General 5 yr Survival GTR 87% (82-100%) < GTR 60% (24-64%)
17 Adjuvant Treatment Observe? Favorable natural history of LGG Survival benefit from surgery-rt has not yet been supported by prospective clinical trials Can always treat when see progression of disease Potential comorbidities of treatment Treat? Natural history worse than age and sex matched control population including pilocytic astrocytoma Retrospective studies have shown survival benefit for surgery or RT

18 Observe RTOG 98-02, Shaw (unpublished) 111 pts Low risk: < 40 y/o, GTR Oligo and oligo dominant-oa and < 4 cm 2 and 5 yr PFS 93% and 78% respectively Diffuse astro and astro dominant-oa and > 4 cm 2 and 5 yr PFS 67% and 34% respectively Shaw, J Neurosurg 1989 First study comparing observation vs RT Retrospective study Survival benefit 5/10 yr OS Surgery alone 30/10% Surgery + < 53 Gy 50/20% Surgery + > 53 Gy 67/40%
19 BELIEVERS & NONBELIEVERS
 7.4 vs 7.2 yrs (p=0.")
20 EORTC Non-believers Trial immediate vs delayed RT Karim, IJROBP, 2002 Van den Bent, Lancet, 2005 Included astro, O, OA, no JPA Median f/u: 7.8 yrs Median PFS: Median OS: Observation 5.3 vs 3.4 yrs (p<0.001) 7.4 vs 7.2 yrs (p=0.872) 311 pts Randomized post-op 54 Gy over 30 fractions
21 EORTC Findings Significant improvement in 5 yr PFS No improvement in 5 yr OS likely 2/2 effectiveness of salvage RT 2/3 pts in observation arm received RT at progression 2 yr progression free for both groups had similar cognitive deficits, KPS, headache Improved seizure control (25 v 41%) at 1 yr with RT arm No QOL data
22 EORTC Believers Trial radiation works, but at what dose? Karim, IJROBP, 1996 Included astro, O, OA, no JPA Median f/u: 74 mos Equivalent 5 yr OS Low dose: High dose: Equivalent 5 yr PFS Low dose: High dose: 58% 59% 47% 59% EORTC Median OS 7.4 yrs Median PFS 5.3 yrs 45 Gy over 25 fractions 343 pts Randomized post-op 59.4 Gy over 33 fractions
23 EORTC QOL analysis included Kiebert, European Journal of Cancer, item questionnaire Physical Psychological Social Symptom
24 EORTC QOL
25 EORTC QOL
26 EORTC Findings No dose response above 45 Gy T parameter important prognostic factor (p<0.0001)
27 EORTC Worse QOL above 45 Gy High dose: lower functioning and higher sx burden Higher fatigue/malaise and insomnia Reduced leisure time and emotional functioning
28 INTERGROUP/NCCTG Also looked at efficacy and dose-response Shaw, JCO pts 203 pts, post op Similar inclusion criteria to Randomized post-op Equivalent 5 yr OS Low dose: 72% High dose: 64% 50.4 Gy over 28 fractions 64.8 Gy over 36 fractions
29 Believers vs Nonbelievers Pro-RT LGG respond to RT Reduced tumor volume Less probability of dedifferentiation Debatable if RT alters transformation Imaging/RT methods improved less toxic Surgeons poor judge of extent removal Improved seizure control Con-RT No OS benefit Sequelae of RT Delayed RT equally effective
30 Radiotherapy 180 cgy x fractions to Gy Focal radiation recommended over WBRT with 2-3 cm margin outside of T2/FLAIR borders NCCTG % failures occurred within field 3% within 2 cm of treatment field 5% > 2 cm outside treatment field SRS? Gy in 1-2 fractions Max 4 cm diameter No evidence for outcomes although morbidity appears minimal in small studies to date
31 Radiotherapy Toxicities Taphoorn, Annals of Neurology 1994 Analyzed subset of pts from EORTC 22844/22845 Mean f/u 3.5 years Three arms: surgery, surgery+rt, control (heme malignancy w/o neuro involvement) Neuropsych tests similar for LGG arms, better than control group disease is underlying cause for cognitive dysfunction L hemispheric tumors had better scores w/ RT than w/o LGG regardless of RT higher frequency of: Fatigue Memory/concentration/speech difficulties Depression Tension Impediment of ADLs RT had no negative impact on neurological, functional, cognitive, and affective status
32 Radiotherapy Toxicities (cont) Klein, Lancet 2002 Update to Taphoorn LGG pts, regardless of RT, lower ability in all cognitive domains Poor cognitive function w/ daily RT fractions > 200 cgy The tumor itself has the most deleterious effect on cognitive dysfunction and that RT mainly results in additional long-term cognitive disability when high fraction doses are used. *Consistent w/ EORTC QOL study
33 Radiotherapy Toxicities (cont) Kleinberg, IJROBP 1993 Localized RT vs WBRT KPS decline Localized: 0/14 WBRT: 3/16 (19%) Employment 1 yr post RT Localized: 80% WBRT: 38-46% Moderate-severe memory deficits Localized: 6% WBRT: 43%
34 Radiotherapy Toxicities (cont) INTERGROUP / NCCTG study Subset of pts in both 50.4 Gy and 64.8 Gy arm Psychometric testing before and up to 5 yrs post RT No significant loss in: General intellect New learning Memory Mean scores higher post RT on all (non significant) Mild decline seen in 4 pts from 64.8 arm 2 yr incidence of severe/life threatening/fatal radionecrosis: 50.4 Gy: 1% 64.8 Gy: 5%
35 Radiotherapy Toxicities (cont) SUMMARY: The weight of evidence indicates a low incidence of neurocognitive difficulties after focal conventionally fractionated ( cgy) RT using modern techniques to deliver moderate dose in adults This is for adults only!
36 Radiotherapy Toxicities: Klein, Lancet 2002 Update to Taphoorn LGG pts, regardless of RT, lower ability in all cognitive domains Poor cognitive function w/ daily RT fractions > 200 cgy The tumor itself has the most deleterious effect on cognitive dysfunction and that RT mainly results in additional long-term cognitive disability when high fraction doses are used. *Consistent w/ EORTC QOL study
37 Radiotherapy Toxicities Update to Klein/Taphoorn Douw, Lancet 2009 Followed out to 12 yrs Long term survivors w/o RT had stable cognitive fx Long term survivors w/ RT Progressive decline in attentional and executive functioning Deficits noted in 5/18 neuropsych test parameters» 17 (53%) in RT arm vs 4 (27%) who were RT naive Even for < 2 Gy Associated with radiographic findings» Doses were Gy» Tx started in 70 s better in RT techniques» Non randomized worse tumors received RT
38 Radiotherapy Pediatric toxicity North, Cancer 1990 Assessed IQ < 70, special education, and other major neuro sequelae (require supervision, hospitalization, nursing care) Surgery alone: 40% Surgery + RT: 54%
39 Chemotherapy PCV therapy and oligo dominant tumors Response rates up to 90% w/ PCV Up to 47% w/ Temodar 1p/19q deletion? Part of RTOG 9802 trial
40 Treatment Summary JPA/piloctyic astrocytoma (G1) OPERATE Complete resection >90% cure rates No adjuvant therapies recommended Partial resection Survival rates 70-80% at 10 yrs Close f/u is standard Adjuvant RT» Gy; Gy/fraction
41 Treatment Summary Diffuse astrocytomas, O, OA OPERATE Complete resection Rarely achieved Observe; no adjuvant currently recommended Subtotal resection Adjuvant RT» Immediate: high risk, older, symptomatic, astro dominant» Delayed: low risk, young, asx, oligo dominant Chemotherapy for 1p/19q deletions? SRS/SBRT?
42 Treatment Summary Path Proven LGG Pediatrics Adult GTR STR/Bx GTR STR/Bx Observe Asx Sx JPA A, OA, O Asx Sx Observe Prepubertal Purbertal Observe Observe or RT Observe or RT RT Chemo or RT RT or chemo
43 Recurrence Poor prognosis in general Majority likely with high-grade transformation Median survival 9.7 mos 2 yr OS 29% Depends on histology Leighton J Clin Onc 1997 Median survival: 39 mos Recurrent diffuse astrocytomas: Recurrent oligodendrogliomas: 16 mos 60 mos Is it recurrence or it is radiation necrosis? Forsythe J neurosurg 1995 Suspected recurrence bx 59 % tumor, median survival 10 mos 33% tumor + necrosis, median survival 22 mos 6% radionecrosis only; no deaths
 for older and < GTR RTOG 0424 is assessing the role of concurrent/adjuvant Temodar w/ radiation for high-risk LGG SRS, SBRT, IORT,")
44 Future directions RTOG 9802 results pending Observe < 40 y/o and GTR Assess adjuvant RT alone vs chemort w/ PCV (procarbazine, lomustine, and vincristine) for older and < GTR RTOG 0424 is assessing the role of concurrent/adjuvant Temodar w/ radiation for high-risk LGG SRS, SBRT, IORT, brachytherapy
45 Thank You!
Management of low grade glioma s: update on recent trials
 Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
PRIMARY GLIOMA (oligodendroglioma, astrocytoma, oligodendroglioma, oligoastrocytoma, including anaplastic, gliosarcoma and glioblastoma multiforme)
") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PRIMARY GLIOMA (oligodendroglioma, astrocytoma, oligodendroglioma, oligoastrocytoma, including
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PRIMARY GLIOMA (oligodendroglioma, astrocytoma, oligodendroglioma, oligoastrocytoma, including
ARRO Case: Low Grade Glioma (LGG)
") ARRO Case: Low Grade Glioma (LGG) Stephanie Rice, BS (MSIV) Abigail T. Berman, MD Michelle Alonso-Basanta, MD, PhD University of Pennsylvania October 25, 2013 44 F, h/o hypothyroidism Presentation: Case
ARRO Case: Low Grade Glioma (LGG) Stephanie Rice, BS (MSIV) Abigail T. Berman, MD Michelle Alonso-Basanta, MD, PhD University of Pennsylvania October 25, 2013 44 F, h/o hypothyroidism Presentation: Case
Radioterapia panencefalica. Umberto Ricardi
 Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
How To Predict Prognosis From An Eortc Gb
 1 di 5 15/10/2011 9.22 Radiation Oncology/CNS/High grade glioma/overview Front Page: Radiation Oncology RTOG Trials Randomized Trials Glioblastoma and High Grade Gliomas Overview Pathology University of
1 di 5 15/10/2011 9.22 Radiation Oncology/CNS/High grade glioma/overview Front Page: Radiation Oncology RTOG Trials Randomized Trials Glioblastoma and High Grade Gliomas Overview Pathology University of
Supportive Care For Patients With High-Grade Glioma (primary brain tumours) Dr Susan Catt & Professor Lesley Fallowfield
 Dr Susan Catt & Professor Lesley Fallowfield") Supportive Care For Patients With High-Grade Glioma (primary brain tumours) Dr Susan Catt & Professor Lesley Fallowfield Partners Mr Giles Critchley Consultant Neurosurgeon Hurstwood Park Neurological
Supportive Care For Patients With High-Grade Glioma (primary brain tumours) Dr Susan Catt & Professor Lesley Fallowfield Partners Mr Giles Critchley Consultant Neurosurgeon Hurstwood Park Neurological
Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121
 Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2007. All rights reserved.
Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2007. All rights reserved.
Stomach (Gastric) Cancer. Prof. M K Mahajan ACDT & RC Bathinda
 Cancer. Prof. M K Mahajan ACDT & RC Bathinda") Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs. Case Study. Surgery. Lumpectomy and Radiation
 Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases
 I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
High Grade Gliomas: Update in Treatment and Care Ryan T. Merrell, M.D. Clinical Assistant Professor of Neurology NorthShore University HealthSystem
 High Grade Gliomas: Update in Treatment and Care Ryan T. Merrell, M.D. Clinical Assistant Professor of Neurology NorthShore University HealthSystem rmerrell@northshore.org Objectives Provide updates on
High Grade Gliomas: Update in Treatment and Care Ryan T. Merrell, M.D. Clinical Assistant Professor of Neurology NorthShore University HealthSystem rmerrell@northshore.org Objectives Provide updates on
THE SECRETS OF OUR SUCCESS
 THE SECRETS OF OUR SUCCESS QUALITY OF LIFE STUDIES OF THE NCIC Andrea Bezjak, MDCM, MSc,, FRCPC Chair, NCIC CTG QOL Committee Outline of the Presentation Can we consider NCIC CTG QOL activities a success?
THE SECRETS OF OUR SUCCESS QUALITY OF LIFE STUDIES OF THE NCIC Andrea Bezjak, MDCM, MSc,, FRCPC Chair, NCIC CTG QOL Committee Outline of the Presentation Can we consider NCIC CTG QOL activities a success?
How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer
 How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer Jeffrey S Tobias, Jayant S Vaidya, Frederik Wenz and Michael Baum, University College Hospital, London, UK - on behalf
How TARGIT Intra-operative Radiotherapy can help Older Patients with Breast cancer Jeffrey S Tobias, Jayant S Vaidya, Frederik Wenz and Michael Baum, University College Hospital, London, UK - on behalf
Carcinoma of the Cervix. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Management of stage III A-B of NSCLC. Hamed ALHusaini Medical Oncologist
 Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group
 Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Brain Tumor 101. Shanna Armstrong, RN Neuro Oncology Nurse Clinician UC Brain Tumor Center
 Brain Tumor 101 Shanna Armstrong, RN Neuro Oncology Nurse Clinician UC Brain Tumor Center Objectives Identify the different parts of the brain Describe how each part of the brain works Connect each part
Brain Tumor 101 Shanna Armstrong, RN Neuro Oncology Nurse Clinician UC Brain Tumor Center Objectives Identify the different parts of the brain Describe how each part of the brain works Connect each part
Radiotherapy in Plasmacytoma and Myeloma. David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015
 Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
Radiotherapy in locally advanced & metastatic NSC lung cancer
 Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Lung Cancer Treatment Guidelines
 Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Authors & Year. Prognostic Effect 1990-1995 1996-2000 2000-2006. Kowalczuk et al. 1997
 Figure 1: Low- and High-Grade Glioma Studies Selected For Review Authors & Year Prognostic Effect 1990-1995 1996-2000 2000-2006 Statistics Favor More Extensive Resections Vecht et 1990 Shibamoto et 1990
Figure 1: Low- and High-Grade Glioma Studies Selected For Review Authors & Year Prognostic Effect 1990-1995 1996-2000 2000-2006 Statistics Favor More Extensive Resections Vecht et 1990 Shibamoto et 1990
What is Glioblastoma? How is GBM classified according to the WHO Grading System? What risk factors pertain to GBM?
 GBM (English) What is Glioblastoma? Glioblastoma or glioblastoma multiforme is one of the most common brain tumors accounting for approximately 12 to 15 percent of all brain tumors. The name of the tumor
GBM (English) What is Glioblastoma? Glioblastoma or glioblastoma multiforme is one of the most common brain tumors accounting for approximately 12 to 15 percent of all brain tumors. The name of the tumor
the standard of care 2009 5/1/2009 Mesothelioma: The standard of care take home messages PILC 2006 Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009
 Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma
 Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Histopathologic results
 Self evaluation 1 Clinical Case 55-year-old woman Bilateral enlargement of cervical, axillary and inguinal lymph nodes, largest diameter > 6 cm Hepatosplenomegaly. Enlargement of retroperitoneal, mesenteric
Self evaluation 1 Clinical Case 55-year-old woman Bilateral enlargement of cervical, axillary and inguinal lymph nodes, largest diameter > 6 cm Hepatosplenomegaly. Enlargement of retroperitoneal, mesenteric
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives. Dominique ELIAS
 from colorectal cancers: New Perspectives. Dominique ELIAS") Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Prostatectomy, pelvic lymphadenect. Med age 63 years Mean followup 53 months No other cancer related therapy before recurrence. Negative.
 Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Pancreatic Cancer: FDA Approved Treatments and Clinical Trials
 Pancreatic Cancer: FDA Approved Treatments and Clinical Trials Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat 2 Pancreatic cancer:
Pancreatic Cancer: FDA Approved Treatments and Clinical Trials Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat 2 Pancreatic cancer:
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
Malignant Mesothelioma State of the Art
 Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Seton Medical Center Hepatocellular Carcinoma Patterns of Care Study Rate of Treatment with Chemoembolization 2007 2012 N = 50
 General Data Seton Medical Center Hepatocellular Carcinoma Patterns of Care Study Rate of Treatment with Chemoembolization 2007 2012 N = 50 The vast majority of the patients in this study were diagnosed
General Data Seton Medical Center Hepatocellular Carcinoma Patterns of Care Study Rate of Treatment with Chemoembolization 2007 2012 N = 50 The vast majority of the patients in this study were diagnosed
Radiation Therapy for Prostate Cancer: Treatment options and future directions
 Radiation Therapy for Prostate Cancer: Treatment options and future directions David Weksberg, M.D., Ph.D. PinnacleHealth Cancer Institute September 12, 2015 Radiation Therapy for Prostate Cancer: Treatment
Radiation Therapy for Prostate Cancer: Treatment options and future directions David Weksberg, M.D., Ph.D. PinnacleHealth Cancer Institute September 12, 2015 Radiation Therapy for Prostate Cancer: Treatment
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015. 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV
 CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
Clinical Trials of Lapatinib in Patients with Brain Metastases. Nancy U Lin, MD Dana Farber Cancer Institute March 1, 2009
 Clinical Trials of Lapatinib in Patients with Brain Metastases from HER2+ Breast Cancer Nancy U Lin, MD Dana Farber Cancer Institute March 1, 2009 Background ~1/3 of women with HER2+ MBC develop brain
Clinical Trials of Lapatinib in Patients with Brain Metastases from HER2+ Breast Cancer Nancy U Lin, MD Dana Farber Cancer Institute March 1, 2009 Background ~1/3 of women with HER2+ MBC develop brain
Ching-Yao Yang, Yu-Wen Tien
 Ching-Yao Yang, Yu-Wen Tien Division of General Surgery, Department of Surgery, National Taiwan University Hospital Oct-30-2010 Pancreatic NET have poorer prognosis when presence of liver metastases at
Ching-Yao Yang, Yu-Wen Tien Division of General Surgery, Department of Surgery, National Taiwan University Hospital Oct-30-2010 Pancreatic NET have poorer prognosis when presence of liver metastases at
Analysis of Prostate Cancer at Easter Connecticut Health Network Using Cancer Registry Data
 The 2014 Cancer Program Annual Public Reporting of Outcomes/Annual Site Analysis Statistical Data from 2013 More than 70 percent of all newly diagnosed cancer patients are treated in the more than 1,500
The 2014 Cancer Program Annual Public Reporting of Outcomes/Annual Site Analysis Statistical Data from 2013 More than 70 percent of all newly diagnosed cancer patients are treated in the more than 1,500
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases
 Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate e P rofessor Professor Radiation Oncology
 Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Clinical Trial Design. Sponsored by Center for Cancer Research National Cancer Institute
 Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Chemobrain. Halle C.F. Moore, MD The Cleveland Clinic October 3, 2015
 Chemobrain Halle C.F. Moore, MD The Cleveland Clinic October 3, 2015 Terminology Chemotherapy-associated cognitive dysfunction Post-chemotherapy cognitive impairment Cancer treatment-associated cognitive
Chemobrain Halle C.F. Moore, MD The Cleveland Clinic October 3, 2015 Terminology Chemotherapy-associated cognitive dysfunction Post-chemotherapy cognitive impairment Cancer treatment-associated cognitive
Management of spinal cord compression
 Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Prostate Cancer 2014
 Prostate Cancer 2014 Eric A. Klein, M.D. Chairman Glickman Urological and Kidney Institute Professor of Surgery Cleveland Clinic Lerner College of Medicine Incidence rates, US Men Mortality Rates, US Men
Prostate Cancer 2014 Eric A. Klein, M.D. Chairman Glickman Urological and Kidney Institute Professor of Surgery Cleveland Clinic Lerner College of Medicine Incidence rates, US Men Mortality Rates, US Men
A new score predicting the survival of patients with spinal cord compression from myeloma
 A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER. Walter Stadler, MD University of Chicago
 CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER Walter Stadler, MD University of Chicago Chemotherapy Doctor Terms Drugs used to treat cancer Will attack cancer no matter where it is located
CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER Walter Stadler, MD University of Chicago Chemotherapy Doctor Terms Drugs used to treat cancer Will attack cancer no matter where it is located
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES
 NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
Historical Basis for Concern
 Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Glioblastoma (cancer affecting the brain) A guide for journalists on glioblastoma and its treatment
 A guide for journalists on glioblastoma and its treatment") Glioblastoma (cancer affecting the brain) A guide for journalists on glioblastoma and its treatment Section 1 Glioblastoma Section 2 Epidemiology and prognosis Section 3 Treatment Contents Contents 2 3
Glioblastoma (cancer affecting the brain) A guide for journalists on glioblastoma and its treatment Section 1 Glioblastoma Section 2 Epidemiology and prognosis Section 3 Treatment Contents Contents 2 3
Frequency of NHL Subtypes in Adults
 Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer
 Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
Rectal Cancer. To Radiate or not to radiate? Q: Should rectal cancer RT/CRT decisions be based solely on stage? 11/09/2014
 Rectal Cancer To Radiate or not to radiate?? Dr. Corinne Doll Radiation Oncologist Tom Baker Cancer Centre Calgary, Alberta Q: Should rectal cancer RT/CRT decisions be based solely on stage? 1 Q: Can RT/CRT
Rectal Cancer To Radiate or not to radiate?? Dr. Corinne Doll Radiation Oncologist Tom Baker Cancer Centre Calgary, Alberta Q: Should rectal cancer RT/CRT decisions be based solely on stage? 1 Q: Can RT/CRT
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent. Disclosure
 Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
These rare variants often act aggressively and may respond differently to therapy than the more common prostate adenocarcinoma.
 Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer
 Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer Ryan J. Burri; Nancy Y. Lee Published: 03/23/2009 Abstract and Introduction Abstract Head and neck cancer is best managed in a multidisciplinary
Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer Ryan J. Burri; Nancy Y. Lee Published: 03/23/2009 Abstract and Introduction Abstract Head and neck cancer is best managed in a multidisciplinary
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
ROLE OF RADIATION THERAPY FOR RESECTABLE LUNG CANCER
 AFA 08958 From Bench to Bedside From KK DT1 10/27/2015 12:04 PM 01 ROLE OF RADIATION THERAPY FOR RESECTABLE LUNG CANCER Hak Choy, MD University of Texas Southwestern Medical Center Dallas, Texas, USA Orchestrating
AFA 08958 From Bench to Bedside From KK DT1 10/27/2015 12:04 PM 01 ROLE OF RADIATION THERAPY FOR RESECTABLE LUNG CANCER Hak Choy, MD University of Texas Southwestern Medical Center Dallas, Texas, USA Orchestrating
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof.
 Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
8 th Annual W/C Spine Summit. Ted A. Lennard, MD Feb. 12, 2015
 8 th Annual W/C Spine Summit Ted A. Lennard, MD Feb. 12, 2015 Case Study 45 y.o. male Truck Accident on 1/15/12 Slid on ice and crossed median. Case Study Taken by ambulance to ER in Texas +Loss of consciousness
8 th Annual W/C Spine Summit Ted A. Lennard, MD Feb. 12, 2015 Case Study 45 y.o. male Truck Accident on 1/15/12 Slid on ice and crossed median. Case Study Taken by ambulance to ER in Texas +Loss of consciousness
REPORT ASCO 2002 ORLANDO : LUNG CANCER Johan F. Vansteenkiste, MD, PhD, Univ. Hospital and Leuven Lung Cancer Group
 REPORT ASCO 2002 ORLANDO : LUNG CANCER Johan F. Vansteenkiste, MD, PhD, Univ. Hospital and Leuven Lung Cancer Group In the 2002 edition of the ASCO meeting, a total of 315 abstracts in the field of respiratory
REPORT ASCO 2002 ORLANDO : LUNG CANCER Johan F. Vansteenkiste, MD, PhD, Univ. Hospital and Leuven Lung Cancer Group In the 2002 edition of the ASCO meeting, a total of 315 abstracts in the field of respiratory
Overview: 1. Epidemiology of childhood cancer survivorship 2. Late effects 3. Palliative care of survivors 4. Examples
 Childhood Cancer Survivorship Jacqueline Casillas, M.D., M.S.H.S. Associate Program Director of the UCLA-LIVESTRONG LIVESTRONGTM TM Center of Excellence for Survivorship Care Overview: 1. Epidemiology
Childhood Cancer Survivorship Jacqueline Casillas, M.D., M.S.H.S. Associate Program Director of the UCLA-LIVESTRONG LIVESTRONGTM TM Center of Excellence for Survivorship Care Overview: 1. Epidemiology
CHILDHOOD CANCER SURVIVOR STUDY Analysis Concept Proposal
 CHILDHOOD CANCER SURVIVOR STUDY Analysis Concept Proposal 1. STUDY TITLE: Longitudinal Assessment of Chronic Health Conditions: The Aging of Childhood Cancer Survivors 2. WORKING GROUP AND INVESTIGATORS:
CHILDHOOD CANCER SURVIVOR STUDY Analysis Concept Proposal 1. STUDY TITLE: Longitudinal Assessment of Chronic Health Conditions: The Aging of Childhood Cancer Survivors 2. WORKING GROUP AND INVESTIGATORS:
Hodgkin Lymphoma Disease Specific Biology and Treatment Options. John Kuruvilla
 Hodgkin Lymphoma Disease Specific Biology and Treatment Options John Kuruvilla My Disclaimer This is where I work Objectives Pathobiology what makes HL different Diagnosis Staging Treatment Philosophy
Hodgkin Lymphoma Disease Specific Biology and Treatment Options John Kuruvilla My Disclaimer This is where I work Objectives Pathobiology what makes HL different Diagnosis Staging Treatment Philosophy
Proton Therapy for Pediatric Cancers
 Proton Therapy for Pediatric Cancers Christine Hill- Kayser, MD Editor- in- Chief, OncoLink Assistant Professor of Radiation Oncology, Pediatrics Service, University of Pennsylvania Melanie Eisenhower,
Proton Therapy for Pediatric Cancers Christine Hill- Kayser, MD Editor- in- Chief, OncoLink Assistant Professor of Radiation Oncology, Pediatrics Service, University of Pennsylvania Melanie Eisenhower,
CYBERKNIFE RADIOSURGERY FOR EARLY PROSTATE CANCER Rationale and Results. Alan Katz MD JD Flushing, NY USA
 CYBERKNIFE RADIOSURGERY FOR EARLY PROSTATE CANCER Rationale and Results Alan Katz MD JD Flushing, NY USA Prostate Ablative Therapy Over the last 10 years our therapy has improved bned rates for LDR/HDR
CYBERKNIFE RADIOSURGERY FOR EARLY PROSTATE CANCER Rationale and Results Alan Katz MD JD Flushing, NY USA Prostate Ablative Therapy Over the last 10 years our therapy has improved bned rates for LDR/HDR
Radiation Therapy for Pediatric Brain Tumors
 Radiation Therapy for Pediatric Brain Tumors David B. Mansur, M.D. Associate Professor of Radiation Oncology and Pediatrics Vice Chair and Director Proton Therapy Center Case Western Reserve University
Radiation Therapy for Pediatric Brain Tumors David B. Mansur, M.D. Associate Professor of Radiation Oncology and Pediatrics Vice Chair and Director Proton Therapy Center Case Western Reserve University
Protocol Abstract and Schema. A Phase 1 and Phase II Study of AZD6244 for Recurrent or Refractory Pediatric Low Grade Glioma
 Protocol Abstract and Schema A Phase 1 and Phase II Study of AZD6244 for Recurrent or Refractory Pediatric Low Grade Glioma Description and Rationale: Low grade gliomas are among the most common primary
Protocol Abstract and Schema A Phase 1 and Phase II Study of AZD6244 for Recurrent or Refractory Pediatric Low Grade Glioma Description and Rationale: Low grade gliomas are among the most common primary
The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality. Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006
 The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006 Overview Pancreatic ductal adenocarcinoma Pancreaticoduodenectomy
The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006 Overview Pancreatic ductal adenocarcinoma Pancreaticoduodenectomy
The Brain and Spine CenTer
 The Br ain and Spine Center Choosing the right treatment partner is important for patients facing tumors involving the brain, spine or skull base. The Brain and Spine Center at The University of Texas
The Br ain and Spine Center Choosing the right treatment partner is important for patients facing tumors involving the brain, spine or skull base. The Brain and Spine Center at The University of Texas
A new score predicting the survival of patients with spinal cord compression from myeloma
 A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
Adjuvant Therapy Non Small Cell Lung Cancer. Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015
 Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Transformation of low grade glioma and correlation with outcome: an NCCTG database analysis
 DOI 10.1007/s11060-010-0476-2 CLINICAL STUDY - PATIENT STUDY Transformation of low grade glioma and correlation with outcome: an NCCTG database analysis K. A. Jaeckle P. A. Decker K. V. Ballman P. J. Flynn
DOI 10.1007/s11060-010-0476-2 CLINICAL STUDY - PATIENT STUDY Transformation of low grade glioma and correlation with outcome: an NCCTG database analysis K. A. Jaeckle P. A. Decker K. V. Ballman P. J. Flynn
AMERICAN BRAIN TUMOR ASSOCIATION. Ependymoma
 AMERICAN BRAIN TUMOR ASSOCIATION Ependymoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization
AMERICAN BRAIN TUMOR ASSOCIATION Ependymoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization
Clinical Trials and Radiation Treatment. Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto
 Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
The evolution of rectal cancer therapy. Objectives
 The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical
 Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Global Objectives. Use of the NIH Stroke Scale (NIHSS) in Emergency Department Patients with Acute Stroke. Why Do This Exercise? Session Objectives
 in Emergency Department Patients with Acute Stroke. Why Do This Exercise? Session Objectives") 1 Use of the NIH Scale (NIHSS) in Emergency Department Patients with Acute Professor Department of Emergency Medicine University of Illinois College of Medicine Chicago, IL Global Objectives Improve pt
1 Use of the NIH Scale (NIHSS) in Emergency Department Patients with Acute Professor Department of Emergency Medicine University of Illinois College of Medicine Chicago, IL Global Objectives Improve pt
SBRT (Elekta), 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.
, 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.") Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Glioblastoma: Is Survival Possible? By Ben A. Williams Copyright, 2014
 Glioblastoma: Is Survival Possible? By Ben A. Williams Copyright, 2014 Glioblastoma multiforme are among the most deadly neoplasms and continue to be regarded as incurable and universally fatal. This reputation
Glioblastoma: Is Survival Possible? By Ben A. Williams Copyright, 2014 Glioblastoma multiforme are among the most deadly neoplasms and continue to be regarded as incurable and universally fatal. This reputation
How To Treat A Cancer With A Radical
 Management of mesothelioma Jan.vanmeerbeeck@ugent.be Amsterdam, March 6, 2010 1 management Palliation Symptomatic care Pain Breathlessness Radiotherapy Chemotherapy Surgery Radical (intention to cure)
Management of mesothelioma Jan.vanmeerbeeck@ugent.be Amsterdam, March 6, 2010 1 management Palliation Symptomatic care Pain Breathlessness Radiotherapy Chemotherapy Surgery Radical (intention to cure)
cancer cancer Hessamfar-Bonarek M et al. Int. J. Epidemiol. 2010;39:135-146
 Hematopoietic Stem Cell Transplant in HIV- related lymphoma Song Zhao, MD PhD Hematology-Oncology Program University of Washington/FHCRC Underlying Causes of Death in HIV-infected Adults 2000 2005 cancer
Hematopoietic Stem Cell Transplant in HIV- related lymphoma Song Zhao, MD PhD Hematology-Oncology Program University of Washington/FHCRC Underlying Causes of Death in HIV-infected Adults 2000 2005 cancer
Pediatric Medulloblastoma
 Pediatric Medulloblastoma Jeff Burkeen, MSIV (Texas A&M) Shalini Moningi, MSIV Amanda Walker, MD Stephanie Terezakis, MD Johns Hopkins Hospital Case Presentation 9 yo presented to the ED with 3 month history
Pediatric Medulloblastoma Jeff Burkeen, MSIV (Texas A&M) Shalini Moningi, MSIV Amanda Walker, MD Stephanie Terezakis, MD Johns Hopkins Hospital Case Presentation 9 yo presented to the ED with 3 month history
Robert Bristow MD PhD FRCPC
 Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Malignant pleural mesothelioma P/D vs. EPP
 3 rd International Thoracic Oncology Congress Dresden, September 13 15, 2012 Malignant pleural mesothelioma P/D vs. EPP Walter Weder, MD Professor of Surgery Dokumentenname Datum Seite 1 Extrapleural Pneumonectomy
3 rd International Thoracic Oncology Congress Dresden, September 13 15, 2012 Malignant pleural mesothelioma P/D vs. EPP Walter Weder, MD Professor of Surgery Dokumentenname Datum Seite 1 Extrapleural Pneumonectomy
Health-related quality of life in high-grade glioma patients
 Chinese Journal of Cancer Review Linda Dirven 1, Neil K. Aaronson 2, Jan J. Heimans 1 and Martin J.B. Taphoorn 1,3 Abstract Gliomas are malignant primary brain tumors and yet incurable. Palliation and
Chinese Journal of Cancer Review Linda Dirven 1, Neil K. Aaronson 2, Jan J. Heimans 1 and Martin J.B. Taphoorn 1,3 Abstract Gliomas are malignant primary brain tumors and yet incurable. Palliation and
The role of chemotherapy in the treatment of low-grade glioma A review of the literature
 Acta neurol. belg., 2005, 105, 137-143 The role of chemotherapy in the treatment of low-grade glioma A review of the literature Bart NEYNS 1, Jan SADONES 1, Cristo CHASKIS 2, Mark DE RIDDER 3, Marleen
Acta neurol. belg., 2005, 105, 137-143 The role of chemotherapy in the treatment of low-grade glioma A review of the literature Bart NEYNS 1, Jan SADONES 1, Cristo CHASKIS 2, Mark DE RIDDER 3, Marleen
Extrapleural Pneumonectomy for Malignant Mesothelioma: Pro. Joon H. Lee 9/17/2012
 Extrapleural Pneumonectomy for Malignant Mesothelioma: Pro Joon H. Lee 9/17/2012 Malignant Pleural Mesothelioma (Epidemiology) Incidence: 7/mil (Japan) to 40/mil (Australia) Attributed secondary to asbestos
Extrapleural Pneumonectomy for Malignant Mesothelioma: Pro Joon H. Lee 9/17/2012 Malignant Pleural Mesothelioma (Epidemiology) Incidence: 7/mil (Japan) to 40/mil (Australia) Attributed secondary to asbestos
High-grade glioma in a patient with breast cancer
 Asian Journal of Surgery (2014) 37, 162e166 Available online at www.sciencedirect.com journal homepage: www.e-asianjournalsurgery.com CASE REPORT High-grade glioma in a patient with breast cancer Che-Chao
Asian Journal of Surgery (2014) 37, 162e166 Available online at www.sciencedirect.com journal homepage: www.e-asianjournalsurgery.com CASE REPORT High-grade glioma in a patient with breast cancer Che-Chao
Kanıt: Klinik çalışmalarda ZYTIGA
 mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
La personalizzazione terapeutica: quanto influisce l età
 La personalizzazione terapeutica: quanto influisce l età PierFranco Conte University of Padova Department of Surgery, Oncology and Gastroenterology IOV Istituto Oncologico Veneto I.R.C.C.S. Breast Cancer
La personalizzazione terapeutica: quanto influisce l età PierFranco Conte University of Padova Department of Surgery, Oncology and Gastroenterology IOV Istituto Oncologico Veneto I.R.C.C.S. Breast Cancer
SAKK Lung Cancer Group. Current activities and future projects
 SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
Recommendations on Disease Management for Patients with Advanced HER2-Positive Breast Cancer and Brain Metastases
 Recommendations on Disease Management for Patients with Advanced HER2-Positive Breast Cancer and Brain Metastases Clinical Practice Guideline www.asco.org/guidelines/her2brainmets American Society of Clinical
Recommendations on Disease Management for Patients with Advanced HER2-Positive Breast Cancer and Brain Metastases Clinical Practice Guideline www.asco.org/guidelines/her2brainmets American Society of Clinical
Prognostic and Predictive Factors in Oncology. Mustafa Benekli, M.D.
 Prognostic and Predictive Factors in Oncology Mustafa Benekli, M.D. NCI Definitions ESMO Course -Essentials of Medical Oncology -Istanbul 2 Prognostic factor: NCI Definition A situation or condition, or
Prognostic and Predictive Factors in Oncology Mustafa Benekli, M.D. NCI Definitions ESMO Course -Essentials of Medical Oncology -Istanbul 2 Prognostic factor: NCI Definition A situation or condition, or
L Lang-Lazdunski, A Bille, S Marshall, R Lal, D Landau, J Spicer
 Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC)
") Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Hepatocellular Carcinoma Treatment Decision Tree
 Treatment Decision Tree Derek DuBay, MD Assistant Professor of Surgery Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery 1 UAB Liver Tumor Clinic Referrals: 205 996 5970 (phone) 205
Treatment Decision Tree Derek DuBay, MD Assistant Professor of Surgery Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery 1 UAB Liver Tumor Clinic Referrals: 205 996 5970 (phone) 205
Lung Cancer. Public Outcomes Report. Submitted by Omar A. Majid, MD
 Public Outcomes Report Lung Cancer Submitted by Omar A. Majid, MD Lung cancer is the most common cancer-related cause of death among men and women. It has been estimated that there will be 226,1 new cases
Public Outcomes Report Lung Cancer Submitted by Omar A. Majid, MD Lung cancer is the most common cancer-related cause of death among men and women. It has been estimated that there will be 226,1 new cases
Subcutaneous Testosterone-Anastrozole Therapy in Breast Cancer Survivors. 2010 ASCO Breast Cancer Symposium Abstract 221 Rebecca L. Glaser M.D.
 Subcutaneous Testosterone-Anastrozole Therapy in Breast Cancer Survivors 2010 ASCO Breast Cancer Symposium Abstract 221 Rebecca L. Glaser M.D., FACS Learning Objectives After reading and reviewing this
Subcutaneous Testosterone-Anastrozole Therapy in Breast Cancer Survivors 2010 ASCO Breast Cancer Symposium Abstract 221 Rebecca L. Glaser M.D., FACS Learning Objectives After reading and reviewing this
Mesothelioma. 1. Introduction. 1.1 General Information and Aetiology
 Mesothelioma 1. Introduction 1.1 General Information and Aetiology Mesotheliomas are tumours that arise from the mesothelial cells of the pleura, peritoneum, pericardium or tunica vaginalis [1]. Most are
Mesothelioma 1. Introduction 1.1 General Information and Aetiology Mesotheliomas are tumours that arise from the mesothelial cells of the pleura, peritoneum, pericardium or tunica vaginalis [1]. Most are
Malcolm Mattes, MD Ajay Tejwani, MD, MPH New York Methodist Hospital
 Malcolm Mattes, MD Ajay Tejwani, MD, MPH New York Methodist Hospital 39 year old female patient who felt a mass in the right gluteal area. Slowly growing over the course of 2 3 months. The mass is associated
Malcolm Mattes, MD Ajay Tejwani, MD, MPH New York Methodist Hospital 39 year old female patient who felt a mass in the right gluteal area. Slowly growing over the course of 2 3 months. The mass is associated
U.S. Food and Drug Administration
 U.S. Food and Drug Administration Notice: Archived Document The content in this document is provided on the FDA s website for reference purposes only. It was current when produced, but is no longer maintained
U.S. Food and Drug Administration Notice: Archived Document The content in this document is provided on the FDA s website for reference purposes only. It was current when produced, but is no longer maintained
Loco-regional Recurrence
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer AGO AGO e. e. V. V. Loco-regional Recurrence Loco-regional Recurrence Version 2002: Brunnert / Simon Versions 2003 2012: Audretsch
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer AGO AGO e. e. V. V. Loco-regional Recurrence Loco-regional Recurrence Version 2002: Brunnert / Simon Versions 2003 2012: Audretsch