How Common is Cervical Cancer?
|
|
|
- Rolf Allison
- 7 years ago
- Views:
Transcription
1 Cervix Cancer 101 Lois M Ramondetta M.D. Professor Gynecologic Oncology MD Anderson Cancer Center Chief, Division of Gynecologic Oncology Lyndon Baines Johnson Hospital Houston Texas

2
3 How Common is Cervical Cancer? The number of new cervical cancer cases per year increased from 378,000 in 1980 to 454,000 in By age 50, at least 80% of women will have acquired HPV 9K-12K new cervical cancers diagnosed in the U.S. per year Yearly Over 3,500 preventable deaths from cervical cancer in the U.S. & 200,000 world wide Source: Texas department of State Health Services, Texas Cancer Registry October 2010 Forouzanfar MH, Lancet. September 15, 2011.

4 Cervical Cancer Facts Cervical cancer is a sexually transmitted disease. HPV DNA is present in virtually all cases of cervical cancer and precursors. More than 75% of sexually active women exposed to HPV Little understanding of why small subset are affected by HPV. In most cases HPV goes away Only women with persistent HPV are at risk for cervical cancer

5 HPV-associated Cancer Rates and County Poverty Level in the US,

6 Incidence by Race

7 In the 50 years following the introduction of pap, US cervical cancer rates decreased by 75% and mortality by 74% Despite this success: Imperfect sensitivity of testing: 30% of all cancers Error in follow-up of abnormal results: another 10% Now we enter a new era the Co Testing ERA Cytology + HPV DNA

8 High Grade lesions : 65% HPV 16, 18, 45, and 31. Low grade lesions: 50% HPV 16, 18, 45, 31; 12% HPV 6 and 11 Up to 40 % of patients are infected with more than one HPV type. HPV 16 and HPV 18 are associated with 50% and 20 % of cancers The first peak of oncogenic HPV infection occurs between the ages of 15 to 25 years, with a secondary peak in the sixth decade of life.

9 Kreimer Cancer Epidemiol Biomarkers Prev 2005; von Krogh Eur J Dermatol 2001 HPV vaccine types association with diseases HPV HPV 16/18 Cervical cancer >99% 70-75% Anal cancer Vaginal cancer Vulvar cancer Penile cancer* Head & Neck cancer Oropharyngeal cancer Oral cavity cancer 84% 70% 40% 47% 36% 23% > 80% 80-90% > 90% > 80% > 95% > 95% In addition, 90% of genital warts are caused by HPV 6 and 11 and almost all cases of recurrent respiratory papillomatosis (RRP) DE Vuyst Eur J Cancer 2009; De Vuyst Int J Cancer 2009; Miralles-Guri J Clin Pathol 2009;
 DE Vuyst Eur J Cancer 2009; De Vuyst Int J Cancer 2009; Miralles-Guri J")
10
11 Placing risk in perspective in making management decisions Using risk of CIN3+ to make guidelines that incorporate HPV testing Guidelines-recommend co testing 90% HPV-and PAP- so 3-5 yrs 10% HPV+ or PAP + so how do we manage this

12 Too Much vs Too Little both can do harm

13 CIN 3 - Carcinoma in situ

14 Cumulative Risk of Cervical cancer in treated or untreated CIN3 <1% vs. 50% Lancet Oncol 2008; 9:

15

16 Cervix Cancer Age Mean 52.2 yrs Bimodal distribution - peaks yrs and yrs Screening 50% of women diagnosed with cervix have never had a PAP 10% of women diagnosed with cervix cancer have not had a PAP in 5 years

17 Cervical Cancer: Symptoms Often no symptoms Post coital bleeding Foul vaginal discharge Abnormal bleeding Pelvic pain Unilateral leg swelling or pain Pelvic mass/gross cervical lesion

18 Cervical cancer: What is the chance of survival? FIGO Stage 5-Year Survival Stage I 81-96% Stage II 65-87% Stage III 35-50% Stage IVA 15-20%

19 Clinical staging of cervical cancer Source: FIGO Annual Report on The Results of Treatment in Gynaecological Cancer Journal of Epidemiology and Biostatistics, (2001) vol. 6 no. 1, page 14. *Mutch D. The new FIGO 2009 staging system for cancers of the vulva, cervix, endometrium and sarcomas Gynecologic Oncology, (2009) vol. 115, no. 3, pgs

20 FIGO 2009 Going Backwards or Forwards? Updates Still clinically staged EUA, cystoscopy, proctoscopy, IVP optional CT, MRI, PET don t change clinical stage Clinical Staging doesn t take into account LND EUA incorrect in 25% Stage I & 50% Stage II

21 Staging Options: FIGO-Basic vs FIGO-Enhanced Any imaging (PET/MRI/CT) allowed but biopsy/surgery conformation required Stage IA IA1-unchanged IA2-based on final pathology P+/P- Stage IB P+/P- Stage IIA/IIB P+/P- PA+/PA- PA+/PA- Stage IIIA/Stage IIIB P+/P- Stage IVA P+/P- PA+/PA- PA+/PA- Stage IVB-unchanged
22 Staging Workup Examination under anesthesia +/-Cystoscopy / proctoscopy Chest radiograph CT or MRI and PET Other tests can be performed for treatment planning but won t change the stage
23 Treatment Stage IA1 Simple Hysterectomy (Extrafascial) Conization Intracavitary radiation
24 Treatment Microinvasive CA Implies minimal risk of nodal involvement 3 mm or less invasion and NO LVSI Simple hysterectomy Cone biopsy
25 Radical hysterectomy Used to treat cervical cancers with invasion > 3mm but confined to the cervix and vagina < 4 cm (Stage IA2 IB1) Removal of parametrium and upper vagina
26 When is RT or Chemo/RT Indicated After Radical Hysterectomy? Radiation if two of the following: deep invasion, large tumor or vascular invasion GOG 92 (Sedlis A Gyn Onc 73: , 1999) Chemo-RT if one of the following: Positive margin, parametrial extension, positive node GOG 109 (Peters WA J Clinic Oncol 18: , 2000)
27 Treatment Options Stages IA2- IIA Radical Hysterectomy and node dissection Patients with two or more risk factors are candidates for post-op radiation: greater than 1/3 stromal invasion, lymph-vascular space invasion, clinical tumor size >4cm Fertility sparing surgery Trachelectomy / cryopreservation Chemo-Radiation Therapy Number and Level of positive nodes?
28 Radical Trachelectomy Candidates: Desire to retain fertility Stage IA2 or IB1 Lesion < cm No evidence of lymph node or distant metastases Absence of high risk histologies (e.g. neuroendocrine tumors)
29 Protocol Prospective, multi-center, international study Objective: To evaluate the safety and feasibility of performing conservative surgery in women with early stage cervical cancer with favorable pathologic characteristics Inclusion Criteria: Stage IA2 or IB1 cervical cancer Tumor diameter < 2 cm No LVSI Squamous cell histology (any grade) or adenocarcinoma (grade 1 or 2 only) Cone margins and ECC negative for malignancy or AIS (one repeat cone/ecc permitted)
30 Radiation Early stage disease Equally effective Side effect profile less desirable Longer treatment duration Obliterates ovarian function Decline in sexual function?
31 Advanced Cervical Cancer Advanced disease (Stage IIB-IV) Chemo-radiation Treatment: Radiotherapy to known volume of disease 25 outpatient treatments Chemotherapy, sensitizers given along with radiation to improve response Brachytherapy/high dose rate inplants Rarely: Surgery Ultra-radical (exenterative) surgery limited to cases of locally invasive disease Problem: Distant metastatic failure occurs in 66% of patients in this group
32 Global Standard Stage IB2 -IVA External beam pelvic radiation (40-60 Gy) Brachytherapy (80-85 Gy to Point A) I.V. Cisplatin chemotherapy Cisplatin 40mg/m 2 (Max 70mg) IV q wk during RT (6wks) GOG 120 (Rose PG et al. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. NEJM 340(15):1144, 1999 Reduces risk of pelvic recurrence by 50% Extends OS by 5-20% c/w XRT alone Monk et al J Clin Oncol 25:
33 Chemoradiation: Risk of Death Decreased by 30-50%
34 Side effect profile Surgery vs. ChemoXRT Surgery-related risk Bladder atony 4% 1-3% fistula rate, half heal spontaneously Mortality <1% 14% risk of major complications (bowel, bladder) Stage (5-10 vs 15%) Dose Early > late 26% severe urinary sx
35 New considerations MIS? Lymphatic mapping Retroperitoneal lymphadenectomy Additional chemotherapy New radiation sensitizers/imrt
36 A Phase III Randomized Clinical Trial of Laparoscopic or Robotic Radical Hysterectomy versus Abdominal Radical Hysterectomy in Patients with Early Stage Cervical Cancer Primary Objective To compare disease-free survival amongst patients who undergo a Minimally Invasive Radical Hysterectomy (TLRH,TRRH) versus Abdominal Radical Hysterectomy (TARH)
37 Patterns of Spread
38 Sentinel node, Right side: Lymphatic Mapping Lymphazurin Ombel. artery
39 New considerations MIS? Lymphatic mapping Retroperitoneal lymphadenectomy Additional chemotherapy New radiation sensitizers/imrt
40 Surgical Staging Options Complication rates: Transperitoneal laparotomy 10-16% Extraperitoneal laparotomy 5-10% Laparoscopy extraperitoneal 1-3% Survival advantage: Surgical vs Radiogr. 4yr PFS 49 vs 36% N=555/130 GOG studies HR 1.46 ( ) Gold MA et al Cancer 2008; 112: Surgical vs Clinical 29 vs 19 months N=274 Stage IIB-IVA Holcomb et al. Eur J Gynecol Oncol 1999;20:90-3 *p=0.01
41 Laparoscopic RPLND in locally advanced cervical cancer Of the 26 patients with negative pelvic and para-aortic nodes on PET/CT 3 (12%) had histopathologically positive para-aortic nodes. Of the 27 patients with positive pelvic but negative para-aortic nodes on PET/CT, 6 (22%) had histopathologically positive para-aortic nodes. Eleven (18.3%) patients had a treatment modification based on surgical findings. Cancer May 1;117(9):
42 New considerations MIS? Lymphatic mapping Retroperitoneal lymphadenectomy Additional chemotherapy New radiation sensitizers/imrt
43 C-xrt followed by Chemo Meta analysis showed increased OS of 19% at 5 yrs Included early trials but did not include GOG 120 or RTOG which set standard for C-xrt Lorvidhaya 4 arm trial Increased OS in C-xrt but no further increase in C-xrt and adj chemo Klopp Curr Oncol Rep DOI Nov 2010 Lorvidhaya Radiat Oncol Biol Phys 2003
44 RTOG-0724 (GOG): Early stage cervical cancer s/p RH Stage IA2-IB2: Positive nodes parametrial extension positive margins after radical hysterectomy Patients had positive nodes or parametrial involvement and disposition to C-XRT Randomized to adjuvant T/C or none
45 THE OUTBACK TRIAL: Phase III trial of adjuvant chemo following chemoradiation for locally advanced cervical cancer VS chemoradiation Stage IB 2 -IVa Cervical cancer: Stratify for - FIGO stage - Pelvic nodal involvement - Uterine +ve on MRI Standard chemoxrt Standard chemoxrt 4 cycles Carboplatin + Paclitaxel
46 New considerations MIS? Lymphatic mapping Retroperitoneal lymphadenectomy Additional chemotherapy New radiation sensitizers/imrt
47 GOG Phase I Trials of CRT GOG 9803 CDDP-Paclitaxel-Pelvic RT (PALN-neg) MTD = CDDP 40 mg/m2 (maximum 70 mg) and paclitaxel 40 mg/m2 weekly x 6 cycles 1 GOG 9804 CDDP-Paclitaxel-EFRT (PALN-pos) MTD = CDDP 40 mg/m2 (maximum 70 mg) and paclitaxel 40 mg/m2 weekly x 6 cycles GOG 9912 CDDP-Gemcitabine-RT (PALN-neg) Closed due to toxicty GOG 9918 CDDP-Cetuximab-RT (PALN-any) Active for accrual GOG 9913 CDDP-Topo (weekly)-rt (PALN-neg) Active for accrual DiSilvestro PA, Walker JL et al Gynecol Oncol 103: , 2006
48 Overall Survival Gem/cis/rad Cis/rad OS probability Log-rank p = Hazard ratio = % CI = Abbreviations: CI = confidence interval; cis = cisplatin; Gem = gemcitabine; OS = overall survival; Rad = radiation. PFS at 3 yrs: 74.4% Gem/cis/rad vs 65.0% Cis/rad (p=0.029) PFS and OS was statistically superior for Gem/cis/rad months OS at 3 years: 78.2% in Gem/cis/rad vs 69.1% Cis/rad Dueñas-González A et al J Clin Oncol 27:15s, 2009 (suppl; abstr 5507 )
49 RTOG 0417 Phase II Study of Bevacizumab with Radiotherapy and Cisplatin Chemotherapy in Locally Advanced Cervical Carcinoma N=57 Bulky IB-IIIB Weekly CDDP Avastin10mg/kg Schefter T
50 Case Presentation: Recurrent 41 y.o. G 3 P 2 - Principal Previous Stage IB 2 SCC Standard CDDP-XRT Complete response LLE swelling, pelvic ache, cough Exam: Pelvic mass Nodes Lung nodules Disease
51 Signs and Symptoms of Recurrent Disease Weight loss Leg edema Pelvic and/or thigh-buttock pain Serosanguinous vaginal discharge Progressive ureteral obstruction Supraclavicular adenopathy Cough Chest pain
52 What if it comes back? Bottom line: Bad news Isolated central pelvic recurrence: Total pelvic exenteration 50% cure Multiple metastases Chemotherapy limited success
53 Total Pelvic Exenteration Removal of gynecologic organs and vagina Removal of bladder and rectosigmoid Colostomy Urinary conduit Neovagina
54 Prognostic Variables Pathologic Subtype Tumor Size Depth of Invasion Lymphvascular Invasion Lymph Node Metastases Early stage negative nodes 86-92% 5 yr survival Early stage positive nodes 50-60% 5 yr survival
55 Predictors of Response to Chemotherapy in Recurrent Cervical Cancer Previous radio-sensitizing chemotherapy Platinum free interval Quality of life / Pain / Performance Status Site of recurrence Response more frequent in non-irradiated sites (70% v 23%, P =.008, GOG 76X, Rose PG et al J Clin Oncol 17:2676, 1999)
56 Recurrent Cervical Cancer: Current GOG Studies (Phase II) 76 series (limited access), untreated 127 series, prior therapy, squamous 227 biologic series 128 series, prior therapy, nonsquamous No further studies planned
57 Extrapelvic Non-Isolated and Pelvic Sidewall Recurrence following XRT Cisplatin + Taxol- 43% Cisplatin + Topotecan- 27% Cisplatin + Gemzar- 22% Cisplatin + Navelbine- 30% Cisplatin % Ifosfamide- 15% 5-FU- 18% Navelbine- 18% CPT-11-18% Bleomycin- 10% Vincristine- 18%
58 nab-paclitaxel in advanced cervix cancer 28.6% had a partial response 42.9% had stable disease Median progression-free and overall survival were 5.0 and 9.4 months, respectively
59 Treatment of Recurrence Phase III GOG 204 TP vs VP vs GP vs TP closed, unable to show superiority over TP GOG 169 CDDP vs CDDP/Taxol RR superior with combination JCO 22(15) Moore GOG 179 CDDP vs CDDP/Topo RR, OS, PFS superior with combination JCO 23(21) 4626, 2005 Long
60 Phase II n=6 median 3 priors 1CR, 1PR, 2 SD TTP 4 mos Wright eg al Gyn Onc 2006 GOG Phase II 227-C Bevacizumab 1-2 priors Bev 15mg/kg q 3 weeks 23.9% progression free >6 months 10.9% PR MRD 6.21 months (range, 2.83 to 8.28 months) Median PFS and OS: 3.40 mos and 7.29 mos respectively. J Clin Oncol Mar 1;27(7):
61 240-Randomized 4 arm study Non platinum doublets Topotecan/Paclitaxel or Platinum/Paclitaxel +/- Bevacizumab Results pending Non superiority of Topotecan/Paclitaxel over Platinum/Paclitaxel
62 Targeted Therapies for Recurrent Cervical Cancer Therapeutic HPV Vaccines Anti-EGFR Anti-angiogenesis Important in cervical cancer growth, invasion, and metastasis E6 mediated inactivation of wild-type p53 up-regulates VEGF Oncolytic viruses EGFR=Epidermal growth factor receptor VEGF=Vascular endothelial growth factor TSP-1=Thrombospondin-1
63 Cetuximab in Combination with Cisplatin in Advanced Carcinoma Of The Cervix 76-DD RR=11.6% PI John Farley
64 pemetrexed (Alimta, LY231514) as second line chemotherapy carcinoma of the cervix 15% had partial responses with a median response duration of 4.4 months The response rate for non-radiated or radiated disease sites was 25% and 7% respectively. 59% had stable disease and 26% patients had increasing disease. Median progression free survival (PFS) was 3.1 months and overall survival (OS) was 7.4 months.
65 A Phase II Trial of Erlotinib In Recurrent Carcinoma of The Cervix: A Gynecologic Oncology Group Study PO erlotinib 150 mg daily until progressive disease or adverse effects 28 enrolled 25 evaluable No objective responses 1 patient had a progression-free survival (PFS) 6 months (4%) Schilder RJ et al in press
66 Study VEG GSK FIGO Stage IVB or recurrent or persistent cervical cancer O Zero or one prior chemo regimens for advanced/recurrent disease Randomized Phase II Endpoint: PFS TR Analyses ERbB1, ERbB2, and the combined ERbB1/ERbB2 overexpressed and gene-amplified (FISH+) populations R A N D M I Z E Oral Lapatinib 1500mg qd Oral Pazopanib 800mg qd Oral Lapatinib 1000mg + Pazopanib 400mg qd Lapatinib: oral dual EGFR/HER2/neu TK inhibitor Pazopanib: oral TK inhibitor in VEGF pathway Monk BJ et al J Clin Oncol 27:15s, 2009 (suppl; abstr 5520)
67 Kaplan-Meier Curve OS Monk BJ et al J Clin Oncol 27:15s, 2009 (suppl; abstr 5520) Median OS (weeks) Lapatinib 39.1 Pazopanib 50.7 HR (90% CI) p-value 0.67 (0.46,0.99) p=0.045 ** The CI are 90% (alpha=10%) naïve CIs. *** Wald normal approximation is used to calculate the p-value * One-sided p-value due to study design. Two-sided would be p=.09. **** Stratified log-rank p-value and hazard ratio (Pike) adjusted only for one of the stratification factors prior chemotherapy.
68 GOG Protocol 227G A PHASE II EVALUATION OF BRIVANIB (BMS582664, IND#) IN THE TREATMENT OF PERSISTENT OR RECURRENT CARCINOMA OF THE CERVIX (BMS Study CA ) Two stage phase II The primary measures of efficacy will be objective response and whether the patient survived progression-free for at least 6 months Study Chair: J Chan
69 GOG 265 A PHASE II EVALUATION OF ADXS (NSC , IND#13,712) IN PERSISTENT OR RECURRENT CARCINOMA OF THE CERVIX 6 patient safety lead in Two stage phase II The primary measure of efficacy will be overall survival at 12 months. Study Chair: W Huh
70 Summary of Treatment for Recurrent Disease Only pelvic exenteration curative for central pelvic recurrences Palliative radiation of painful metastases Cisplatin doublets standard in treating metastatic disease Anti-vascular compounds emerging as new systemic agents for advanced and recurrent cancer Quality of life and honesty needs to be emphasized
71 Beta-adrenergic blockers, Stress, and QOL Clinical trial using beta blockade and stress reduction techniques Outcomes- 1-Overall Survival 2-Improved QOL Translational outcomes- biologic stress markers
72 2 nd Annual Houston Cervical Cancer Summit Convened by: Cervical Cancer-Free Texas, Cervical Comp Cancer Workgroup, Houston Community College Coleman College for Health Sciences and the Gynecologic Department at MD Anderson Cancer Center. SAVE THE DATE: Tuesday, January 29, :00 a.m. 4:00 p.m. United Way of Greater Houston 50 Waugh Drive Houston, Texas Registration opens in December. Registration Fee: $25 Cervical Cancer Survivors attend for FREE. Linda Leach at: or (713)
 Known cause HPV Belief barriers Screening test Pap smear (HPV test) Barriers to screening and follow up A preventative vaccine Barriers to access and acceptability Long preinvasive development")
73 omen s (extremely unnecessary) ough ight (!) Known cause HPV Belief barriers Screening test Pap smear (HPV test) Barriers to screening and follow up A preventative vaccine Barriers to access and acceptability Long preinvasive development stage 3-10 years Barriers to follow up Curable preinvasive stage leep, cone, hysterectomy Missed opportunities Curable early stage radical hysterectomy Missed opportunities
74 YO! Cervical Cancer Survivors!!! Unite! Have a voice! Be heard! Lobby for vaccination and education in schools Lobby for money Know sources for help Raise awareness and funding disease of the developing world its only 4000 women Are they serious????
Carcinoma of the Cervix. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Invasive Cervical Cancer. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Invasive Cervical Cancer Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Etiology Human Papilloma Virus (HPV): Detected in 99.7% of cervical cancers Cancer
Invasive Cervical Cancer Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Etiology Human Papilloma Virus (HPV): Detected in 99.7% of cervical cancers Cancer
How To Compare The Effects Of A Hysterectomy And A Hysterectomy
 A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
Carcinoma of the vagina is a relatively uncommon disease, affecting only about 2,000 women in
 EVERYONE S GUIDE FOR CANCER THERAPY Malin Dollinger, MD, Ernest H. Rosenbaum, MD, Margaret Tempero, MD, and Sean Mulvihill, MD 4 th Edition, 2001 Vagina Jeffrey L. Stern, MD Carcinoma of the vagina is
EVERYONE S GUIDE FOR CANCER THERAPY Malin Dollinger, MD, Ernest H. Rosenbaum, MD, Margaret Tempero, MD, and Sean Mulvihill, MD 4 th Edition, 2001 Vagina Jeffrey L. Stern, MD Carcinoma of the vagina is
How To Treat A Uterine Sarcoma
 EVERYONE S GUIDE FOR CANCER THERAPY Malin Dollinger, MD, Ernest H. Rosenbaum, MD, Margaret Tempero, MD, and Sean Mulvihill, MD 4 th Edition 2001 Uterus: Uterine Sarcomas Jeffrey L. Stern, MD Uterine sarcomas
EVERYONE S GUIDE FOR CANCER THERAPY Malin Dollinger, MD, Ernest H. Rosenbaum, MD, Margaret Tempero, MD, and Sean Mulvihill, MD 4 th Edition 2001 Uterus: Uterine Sarcomas Jeffrey L. Stern, MD Uterine sarcomas
SCAN Gynaecological Group. Clinical Management Protocols: Cancer of the Cervix. www.scan.scot.nhs.uk
 SE Scotland Cancer Network SCAN Gynaecological Group Clinical Management Protocols: Cancer of the Cervix www.scan.scot.nhs.uk Table of contents 3 Introduction 4 Diagnosis 5-6 Staging and spread of disease
SE Scotland Cancer Network SCAN Gynaecological Group Clinical Management Protocols: Cancer of the Cervix www.scan.scot.nhs.uk Table of contents 3 Introduction 4 Diagnosis 5-6 Staging and spread of disease
Overview of Gynaecologic Cancer
 Overview of Gynaecologic Cancer Stuart Salfinger Gynaecologic Oncologist St John of God Hospital King Edward Memorial Hospital Cervical Cancer Cervical Cancer Risk HPV Smoking?OCP Cervical Cancer Symptoms
Overview of Gynaecologic Cancer Stuart Salfinger Gynaecologic Oncologist St John of God Hospital King Edward Memorial Hospital Cervical Cancer Cervical Cancer Risk HPV Smoking?OCP Cervical Cancer Symptoms
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent. Disclosure
 Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Stomach (Gastric) Cancer. Prof. M K Mahajan ACDT & RC Bathinda
 Cancer. Prof. M K Mahajan ACDT & RC Bathinda") Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
PRIMARY TREATMENT CLINICAL PRESENTATION INITIAL EVALUATION. Conclude procedure with/without lymph node dissection
 INITIAL EVALUATION History and Physical CXR Pathology review 1 Labs Consider CA125, and pre-operative imaging of abdomen and pelvis Screen for Lynch Syndrome by family history or molecular testing CLINICAL
INITIAL EVALUATION History and Physical CXR Pathology review 1 Labs Consider CA125, and pre-operative imaging of abdomen and pelvis Screen for Lynch Syndrome by family history or molecular testing CLINICAL
Endometrial cancer-carcinoma of the lining of the uterus-is the most common gynecologic
 EVERYONE S GUIDE FOR CANCER THERAPY Malin Dollinger, MD, Ernest H. Rosenbaum, MD, Margaret Tempero, MD, and Sean Mulvihill, MD 4th Edition 2001 Uterus: Endometrial Carcinoma Jeffrey L. Stern, MD Endometrial
EVERYONE S GUIDE FOR CANCER THERAPY Malin Dollinger, MD, Ernest H. Rosenbaum, MD, Margaret Tempero, MD, and Sean Mulvihill, MD 4th Edition 2001 Uterus: Endometrial Carcinoma Jeffrey L. Stern, MD Endometrial
Maintenance therapy in in Metastatic NSCLC. Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai
 Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
The Role of Laparoscopy in Endometrial Cancer
 The Role of Laparoscopy in Endometrial Cancer Prof. Dr. Tugan BEŞE İstanbul University, Cerrahpaşa Medical Faculty Gynecologic Oncology Department Surgical staging in Endometrial Cancer Laparoscopic surgery
The Role of Laparoscopy in Endometrial Cancer Prof. Dr. Tugan BEŞE İstanbul University, Cerrahpaşa Medical Faculty Gynecologic Oncology Department Surgical staging in Endometrial Cancer Laparoscopic surgery
What is neuroendocrine cervical cancer?
 Key Points: 1. Neuroendocrine cancer of the uterine cervix is a rare and aggressive disease. 2. Treatment for neuroendocrine cervical cancer is usually more intensive than that for most other types of
Key Points: 1. Neuroendocrine cancer of the uterine cervix is a rare and aggressive disease. 2. Treatment for neuroendocrine cervical cancer is usually more intensive than that for most other types of
Sentinel Lymph Node Mapping for Endometrial Cancer. Locke Uppendahl, MD Grand Rounds
 Sentinel Lymph Node Mapping for Endometrial Cancer Locke Uppendahl, MD Grand Rounds Endometrial Cancer Most common gynecologic malignancy in US estimated 52,630 new cases in 2014 estimated 8,590 deaths
Sentinel Lymph Node Mapping for Endometrial Cancer Locke Uppendahl, MD Grand Rounds Endometrial Cancer Most common gynecologic malignancy in US estimated 52,630 new cases in 2014 estimated 8,590 deaths
Cancer of the Cervix
 Cancer of the Cervix WOMENCARE A Healthy Woman is a Powerful Woman (407) 898-1500 A woman's cervix (the opening of the uterus) is lined with cells. Cancer of the cervix occurs when those cells change,
Cancer of the Cervix WOMENCARE A Healthy Woman is a Powerful Woman (407) 898-1500 A woman's cervix (the opening of the uterus) is lined with cells. Cancer of the cervix occurs when those cells change,
Metastatic Cervical Cancer s/p Radiation Therapy, Radical Hysterectomy and Attempted Modified Internal Hemipelvectomy
 Metastatic Cervical Cancer s/p Radiation Therapy, Radical Hysterectomy and Attempted Modified Internal Hemipelvectomy Sarah Hutto,, MSIV Marc Underhill, M.D. January 27, 2009 Past History 45 yo female
Metastatic Cervical Cancer s/p Radiation Therapy, Radical Hysterectomy and Attempted Modified Internal Hemipelvectomy Sarah Hutto,, MSIV Marc Underhill, M.D. January 27, 2009 Past History 45 yo female
Cervical Cancer The Importance of Cervical Screening and Vaccination
 Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
U.S. Food and Drug Administration
 U.S. Food and Drug Administration Notice: Archived Document The content in this document is provided on the FDA s website for reference purposes only. It was current when produced, but is no longer maintained
U.S. Food and Drug Administration Notice: Archived Document The content in this document is provided on the FDA s website for reference purposes only. It was current when produced, but is no longer maintained
2015 RN.ORG, S.A., RN.ORG, LLC
 Cervical Cancer WWW.RN.ORG Reviewed September, 2015, Expires September, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A., RN.ORG,
Cervical Cancer WWW.RN.ORG Reviewed September, 2015, Expires September, 2017 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2015 RN.ORG, S.A., RN.ORG,
Cervical Cancer: Definitive Chemoradiation
 Cervical Cancer: Definitive Chemoradiation Huma Chaudhry Jordan Kharofa Faculty: Dr. Beth Erickson, MD Medical College of Wisconsin Department of Radiation Oncology July 14, 2013 Clinical Presentation
Cervical Cancer: Definitive Chemoradiation Huma Chaudhry Jordan Kharofa Faculty: Dr. Beth Erickson, MD Medical College of Wisconsin Department of Radiation Oncology July 14, 2013 Clinical Presentation
Cervical Carcinoma. Chris DeSimone, M.D. Assistant Professor Division of Gynecologic Oncology
 Cervical Carcinoma Chris DeSimone, M.D. Assistant Professor Division of Gynecologic Oncology Outline Cervical Carcinoma Epidemiology Clinical symptoms Risk factors Staging Cell types Prognostic factors
Cervical Carcinoma Chris DeSimone, M.D. Assistant Professor Division of Gynecologic Oncology Outline Cervical Carcinoma Epidemiology Clinical symptoms Risk factors Staging Cell types Prognostic factors
Pancreatic Cancer: FDA Approved Treatments and Clinical Trials
 Pancreatic Cancer: FDA Approved Treatments and Clinical Trials Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat 2 Pancreatic cancer:
Pancreatic Cancer: FDA Approved Treatments and Clinical Trials Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat 2 Pancreatic cancer:
Building Awareness of Cervical Cancer
 Building Awareness of Cervical Cancer Guest Expert: Peter, MD John Slade Ely Professor of Obstetrics, Gynecology & Reproductive Sciences www.wnpr.org www.yalecancercenter.org Welcome to Yale Cancer Center
Building Awareness of Cervical Cancer Guest Expert: Peter, MD John Slade Ely Professor of Obstetrics, Gynecology & Reproductive Sciences www.wnpr.org www.yalecancercenter.org Welcome to Yale Cancer Center
Adjuvant Therapy Non Small Cell Lung Cancer. Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015
 Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
Adjuvant Therapy Non Small Cell Lung Cancer Sunil Nagpal MD Director, Thoracic Oncology Jan 30, 2015 No Disclosures Number of studies Studies Per Month 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3
INTERVENTIONAL PROCEDURES PROGRAMME
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of radical laparoscopic hysterectomy for early stage cervical cancer Introduction This overview
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of radical laparoscopic hysterectomy for early stage cervical cancer Introduction This overview
New Trends & Current Research in the Treatment of Lung Cancer, Pt. II
 New Trends & Current esearch in the Treatment of Lung Cancer, Pt. II Howard (Jack) West, MD President & CEO, GACE Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA Cancer
New Trends & Current esearch in the Treatment of Lung Cancer, Pt. II Howard (Jack) West, MD President & CEO, GACE Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA Cancer
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER
 GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
GUIDELINES FOR THE MANAGEMENT OF LUNG CANCER BY Ali Shamseddine, MD (Coordinator); as04@aub.edu.lb Fady Geara, MD Bassem Shabb, MD Ghassan Jamaleddine, MD CLINICAL PRACTICE GUIDELINES FOR THE TREATMENT
Outcome of Early Cervical Carcinoma Treated by Wertheim Hysterectomy with Selective Postoperative Radiotherapy
 ORIGINAL ARTICLES 613 Outcome of Early Cervical Carcinoma Treated by Wertheim Hysterectomy with Selective Postoperative Radiotherapy S K Tay,*FAMS, MD, FRCOG, L K Tan,**MBBS, M Med (O & G), MRCOG Abstract
ORIGINAL ARTICLES 613 Outcome of Early Cervical Carcinoma Treated by Wertheim Hysterectomy with Selective Postoperative Radiotherapy S K Tay,*FAMS, MD, FRCOG, L K Tan,**MBBS, M Med (O & G), MRCOG Abstract
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Small Cell Lung Cancer
 Small Cell Lung Cancer Types of Lung Cancer Non-small cell carcinoma (NSCC) (87%) Adenocarcinoma (38%) Squamous cell (20%) Large cell (5%) Small cell carcinoma (13%) Small cell lung cancer is virtually
Small Cell Lung Cancer Types of Lung Cancer Non-small cell carcinoma (NSCC) (87%) Adenocarcinoma (38%) Squamous cell (20%) Large cell (5%) Small cell carcinoma (13%) Small cell lung cancer is virtually
Management of low grade glioma s: update on recent trials
 Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Examples of good screening tests include: mammography for breast cancer screening and Pap smears for cervical cancer screening.
 CANCER SCREENING Dr. Tracy Sexton (updated July 2010) What is screening? Screening is the identification of asymptomatic disease or risk factors by history taking, physical examination, laboratory tests
CANCER SCREENING Dr. Tracy Sexton (updated July 2010) What is screening? Screening is the identification of asymptomatic disease or risk factors by history taking, physical examination, laboratory tests
Nursing Care of the Patient Receiving Brachytherapy for Gynecologic Cancer
 Nursing Care of the Patient Receiving Brachytherapy for Gynecologic Cancer Una Randall, RN, BSN, OCN Dana Farber / Brigham and Women s Cancer Center Department of Radiation Oncology Una Randall is not
Nursing Care of the Patient Receiving Brachytherapy for Gynecologic Cancer Una Randall, RN, BSN, OCN Dana Farber / Brigham and Women s Cancer Center Department of Radiation Oncology Una Randall is not
Chemotherapy in Ovarian Cancer. Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group
 Chemotherapy in Ovarian Cancer Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group Adjuvant chemotherapy for early stage EOC Fewer than 30% women present with FIGO stage
Chemotherapy in Ovarian Cancer Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group Adjuvant chemotherapy for early stage EOC Fewer than 30% women present with FIGO stage
Surgical Staging of Endometrial Cancer
 Surgical Staging of Endometrial Cancer I. Endometrial Cancer Surgical Staging Overview Uterine cancer types: carcinomas type I and type II, sarcomas, carcinosarcomas Hysterectomy with BSO Surgical Staging
Surgical Staging of Endometrial Cancer I. Endometrial Cancer Surgical Staging Overview Uterine cancer types: carcinomas type I and type II, sarcomas, carcinosarcomas Hysterectomy with BSO Surgical Staging
Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases
 I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
Harmesh Naik, MD. Hope Cancer Clinic HOW DO I MANAGE STAGE 4 NSCLC IN 2012: STATE OF THE ART
 Harmesh Naik, MD. Hope Cancer Clinic HOW DO I MANAGE STAGE 4 NSCLC IN 2012: STATE OF THE ART Goals Discuss treatment options for stage 4 lung cancer: New and old Discuss new developments in personalized
Harmesh Naik, MD. Hope Cancer Clinic HOW DO I MANAGE STAGE 4 NSCLC IN 2012: STATE OF THE ART Goals Discuss treatment options for stage 4 lung cancer: New and old Discuss new developments in personalized
Cervical Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2015 NCCN.org. Continue
 Version 1.2015 NCCN.org. Continue") NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2015 NCCN.org Continue Version 1.2015, 08/07/14 National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCN
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2015 NCCN.org Continue Version 1.2015, 08/07/14 National Comprehensive Cancer Network, Inc. 2014, All rights reserved. The NCCN
SMALL CELL LUNG CANCER
 Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
Protocol for Planning and Treatment The process to be followed in the management of: SMALL CELL LUNG CANCER Patient information given at each stage following agreed information pathway 1. DIAGNOSIS New
SIGN. Management of cervical cancer. Scottish Intercollegiate Guidelines Network. A national clinical guideline
 SIGN Scottish Intercollegiate Guidelines Network Help us to improve SIGN guidelines - click here to complete our survey 99 Management of cervical cancer A national clinical guideline 1 Introduction 1 2
SIGN Scottish Intercollegiate Guidelines Network Help us to improve SIGN guidelines - click here to complete our survey 99 Management of cervical cancer A national clinical guideline 1 Introduction 1 2
Chapter 14 Cancer of the Cervix Uteri
 Carol L. Kosary Introduction Despite the existence of effective screening through the use of Pap smears since the 195 s, there were 9,71 estimated cases of invasive cervical cancer and 3,7 deaths in 26
Carol L. Kosary Introduction Despite the existence of effective screening through the use of Pap smears since the 195 s, there were 9,71 estimated cases of invasive cervical cancer and 3,7 deaths in 26
Treatment Paradigm in NSCLC Treatment
 Treatment Paradigm in NSCLC Treatment Era of Targeted Therapy Aumkhae Sookprasert, MD Medicine Department, KKU Which factors taken to be account in NSCLC treatment? 1. Staging 2. ECOG performance status
Treatment Paradigm in NSCLC Treatment Era of Targeted Therapy Aumkhae Sookprasert, MD Medicine Department, KKU Which factors taken to be account in NSCLC treatment? 1. Staging 2. ECOG performance status
Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer
 Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer Ryan J. Burri; Nancy Y. Lee Published: 03/23/2009 Abstract and Introduction Abstract Head and neck cancer is best managed in a multidisciplinary
Concurrent Chemotherapy and Radiotherapy for Head and Neck Cancer Ryan J. Burri; Nancy Y. Lee Published: 03/23/2009 Abstract and Introduction Abstract Head and neck cancer is best managed in a multidisciplinary
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery
 Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER. Walter Stadler, MD University of Chicago
 CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER Walter Stadler, MD University of Chicago Chemotherapy Doctor Terms Drugs used to treat cancer Will attack cancer no matter where it is located
CHEMOTHERAPY FOR ADVANCED UROTHELIAL CANCER OF THE BLADDER Walter Stadler, MD University of Chicago Chemotherapy Doctor Terms Drugs used to treat cancer Will attack cancer no matter where it is located
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs. Case Study. Surgery. Lumpectomy and Radiation
 Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
PRIMARY GLIOMA (oligodendroglioma, astrocytoma, oligodendroglioma, oligoastrocytoma, including anaplastic, gliosarcoma and glioblastoma multiforme)
") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PRIMARY GLIOMA (oligodendroglioma, astrocytoma, oligodendroglioma, oligoastrocytoma, including
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PRIMARY GLIOMA (oligodendroglioma, astrocytoma, oligodendroglioma, oligoastrocytoma, including
Myths & Facts. about cervical cancer. What you need to know
 Myths & Facts about cervical cancer What you need to know Clinical opinions expressed in this book are those of the authors and do not necessarily reflect the opinions of the supporter, editors, or the
Myths & Facts about cervical cancer What you need to know Clinical opinions expressed in this book are those of the authors and do not necessarily reflect the opinions of the supporter, editors, or the
Frequently Asked Questions About Ovarian Cancer
 Media Contact: Gerri Gomez Howard Cell: 303-748-3933 gerri@gomezhowardgroup.com Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Media Contact: Gerri Gomez Howard Cell: 303-748-3933 gerri@gomezhowardgroup.com Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Kanıt: Klinik çalışmalarda ZYTIGA
 mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
Radiotherapy in locally advanced & metastatic NSC lung cancer
 Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
COMMISSIONING. for ULTRA-RADICAL SURGERY ADVANCED OVARIAN CANCER
 COMMISSIONING for ULTRA-RADICAL SURGERY in ADVANCED OVARIAN CANCER WHY THIS MUST HAPPEN PERSPECTIVE COMMISSIONING FOR WHO, FOR WHAT? Biological Basis Surgical Basis International and national standards
COMMISSIONING for ULTRA-RADICAL SURGERY in ADVANCED OVARIAN CANCER WHY THIS MUST HAPPEN PERSPECTIVE COMMISSIONING FOR WHO, FOR WHAT? Biological Basis Surgical Basis International and national standards
Ovarian cancer. A guide for journalists on ovarian cancer and its treatment
 Ovarian cancer A guide for journalists on ovarian cancer and its treatment Contents Contents 2 3 Section 1: Ovarian Cancer 4 i. Types of ovarian cancer 4 ii. Causes and risk factors 5 iii. Symptoms and
Ovarian cancer A guide for journalists on ovarian cancer and its treatment Contents Contents 2 3 Section 1: Ovarian Cancer 4 i. Types of ovarian cancer 4 ii. Causes and risk factors 5 iii. Symptoms and
NCCN Non-Small Cell Lung Cancer V.1.2011 Update Meeting 07/09/10
 Guideline Page and Request NSCL-3 Stage IA, margins positive delete the recommendation for chemoradiation. Stage IB, IIA, margins positive delete the recommendation for chemoradiation + Stage IIA, Stage
Guideline Page and Request NSCL-3 Stage IA, margins positive delete the recommendation for chemoradiation. Stage IB, IIA, margins positive delete the recommendation for chemoradiation + Stage IIA, Stage
Background. t 1/2 of 3.7 4.7 days allows once-daily dosing (1.5 mg) with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4
 with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4") Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Thomas A. Kollmorgen, M.D. Oregon Urology Institute
 Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Understanding Your Diagnosis of Endometrial Cancer A STEP-BY-STEP GUIDE
 Understanding Your Diagnosis of Endometrial Cancer A STEP-BY-STEP GUIDE Introduction This guide is designed to help you clarify and understand the decisions that need to be made about your care for the
Understanding Your Diagnosis of Endometrial Cancer A STEP-BY-STEP GUIDE Introduction This guide is designed to help you clarify and understand the decisions that need to be made about your care for the
Management of stage III A-B of NSCLC. Hamed ALHusaini Medical Oncologist
 Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Management of stage III A-B of NSCLC Hamed ALHusaini Medical Oncologist Global incidence, CA cancer J Clin 2011;61:69-90 Stage III NSCLC Includes heterogeneous group of patients with differences in the
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group
 Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Prognostic and Predictive Factors in Oncology. Mustafa Benekli, M.D.
 Prognostic and Predictive Factors in Oncology Mustafa Benekli, M.D. NCI Definitions ESMO Course -Essentials of Medical Oncology -Istanbul 2 Prognostic factor: NCI Definition A situation or condition, or
Prognostic and Predictive Factors in Oncology Mustafa Benekli, M.D. NCI Definitions ESMO Course -Essentials of Medical Oncology -Istanbul 2 Prognostic factor: NCI Definition A situation or condition, or
Lung Cancer Treatment Guidelines
 Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
Updated June 2014 Derived and updated by consensus of members of the Providence Thoracic Oncology Program with the aid of evidence-based National Comprehensive Cancer Network (NCCN) national guidelines,
An introduction to invasive cancer of the uterine cervix
 An introduction to invasive cancer of the uterine cervix Preclinical invasive cancer refers to early cervical cancer, with minimal stromal invasion, often without any symptoms or clinical features. As
An introduction to invasive cancer of the uterine cervix Preclinical invasive cancer refers to early cervical cancer, with minimal stromal invasion, often without any symptoms or clinical features. As
Cervical Cancer. Cervical smear test. The cervix. Dysplasia. Cervical cancer. The female reproductive system
 INFORMATION SHEET Cervical Cancer This information sheet has been written to provide you with information about cervical cancer (cancer of the cervix). The sheet has information about the different types
INFORMATION SHEET Cervical Cancer This information sheet has been written to provide you with information about cervical cancer (cancer of the cervix). The sheet has information about the different types
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
GYNECOLOGIC CANCERS Facts to Help Patients Make an Informed Decision
 RADIATION THERAPY FOR GYNECOLOGIC CANCERS Facts to Help Patients Make an Informed Decision TARGETING CANCER CARE AMERICAN SOCIETY FOR RADIATION ONCOLOGY FACTS ABOUT GYNECOLOGIC CANCERS Gynecologic cancers
RADIATION THERAPY FOR GYNECOLOGIC CANCERS Facts to Help Patients Make an Informed Decision TARGETING CANCER CARE AMERICAN SOCIETY FOR RADIATION ONCOLOGY FACTS ABOUT GYNECOLOGIC CANCERS Gynecologic cancers
SAKK Lung Cancer Group. Current activities and future projects
 SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
SAKK Lung Cancer Group Current activities and future projects SAKK Lung Cancer Group Open group of physicians interested in lung cancer Mostly Medical Oncologists, but also Thoracic Surgeons Radiation
Avastin in breast cancer: Summary of clinical data
 Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015. 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV
 CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
CANCER PULMON: ESTADIOS INICIALES POSTMUNDIAL PULMON DENVER 2015 8-10-2015.Manuel Cobo Dols S. Oncología Médica HU Málaga Regional y VV Meta-analisis LACE: adyuvancia vs no adyuvancia Pignon JP, et al.
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives. Dominique ELIAS
 from colorectal cancers: New Perspectives. Dominique ELIAS") Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Treatment Guide Gynecologic Cancer
 Treatment Guide Gynecologic Cancer Cleveland Clinic experts tailor treatment to their patients needs, taking into account the type of cancer, the degree to which the cancer has spread, the age of the individual
Treatment Guide Gynecologic Cancer Cleveland Clinic experts tailor treatment to their patients needs, taking into account the type of cancer, the degree to which the cancer has spread, the age of the individual
Endometrial Cancer Treatment
 Endometrial Cancer Treatment January 2006 By Shelly Smits, RHIT, CCS, CTR mary by Ian Thompson, MD Data Source: Cancer registry information on uterine cancer diagnosed 1/1/2000 to 12/31/2004. Reason for
Endometrial Cancer Treatment January 2006 By Shelly Smits, RHIT, CCS, CTR mary by Ian Thompson, MD Data Source: Cancer registry information on uterine cancer diagnosed 1/1/2000 to 12/31/2004. Reason for
the standard of care 2009 5/1/2009 Mesothelioma: The standard of care take home messages PILC 2006 Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009
 Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Monthly palliative pelvic radiotherapy in advanced carcinoma of uterine cervix
 Original Article Free full text available from www.cancerjournal.net Monthly palliative pelvic radiotherapy in advanced carcinoma of uterine cervix Mishra Sanjib K, Laskar Siddhartha, Muckaden Mary Ann,
Original Article Free full text available from www.cancerjournal.net Monthly palliative pelvic radiotherapy in advanced carcinoma of uterine cervix Mishra Sanjib K, Laskar Siddhartha, Muckaden Mary Ann,
Objectives. Mylene T. Truong, MD. Malignant Pleural Mesothelioma Background
 Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Metastatic Breast Cancer 201. Carolyn B. Hendricks, MD October 29, 2011
 Metastatic Breast Cancer 201 Carolyn B. Hendricks, MD October 29, 2011 Overview Is rebiopsy necessary at the time of recurrence or progression of disease? How dose a very aggressive treatment upfront compare
Metastatic Breast Cancer 201 Carolyn B. Hendricks, MD October 29, 2011 Overview Is rebiopsy necessary at the time of recurrence or progression of disease? How dose a very aggressive treatment upfront compare
Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy
 Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy W. Fraser Symmans, M.D. Associate Professor of Pathology UT M.D. Anderson Cancer Center Pathologic Complete Response (pcr) Proof
Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy W. Fraser Symmans, M.D. Associate Professor of Pathology UT M.D. Anderson Cancer Center Pathologic Complete Response (pcr) Proof
Mesothelioma. Malignant Pleural Mesothelioma
 Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
Mesothelioma William G. Richards, PhD Brigham and Women s Hospital Malignant Pleural Mesothelioma 2,000-3,000 cases per year (USA) Increasing incidence Asbestos (50-80%, decreasing) 30-40 year latency
L Lang-Lazdunski, A Bille, S Marshall, R Lal, D Landau, J Spicer
 Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine and systemic chemotherapy in malignant pleural mesothelioma. A 10-year experience. L Lang-Lazdunski, A Bille, S Marshall, R Lal,
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer
 Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof.
 Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Corso Integrato di Clinica Medica ONCOLOGIA MEDICA AA 2010-2011 LUNG CANCER. VIII. THERAPY. V. SMALL CELL LUNG CANCER Prof. Alberto Riccardi SMALL CELL LUNG CARCINOMA Summary of treatment approach * limited
Cancer of the Cervix, Vagina, Vulva, and Trophoblastic Tumors
 Cancer of the Cervix, Vagina, Vulva, and Trophoblastic Tumors Daniel L. Clarke-Pearson, M.D. Robert A. Ross Distinguished Professor Chair, Department of Obstetrics and Gynecology University of North Carolina,
Cancer of the Cervix, Vagina, Vulva, and Trophoblastic Tumors Daniel L. Clarke-Pearson, M.D. Robert A. Ross Distinguished Professor Chair, Department of Obstetrics and Gynecology University of North Carolina,
Drug/Drug Combination: Bevacizumab in combination with chemotherapy
 AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
These rare variants often act aggressively and may respond differently to therapy than the more common prostate adenocarcinoma.
 Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Adjuvant Therapy for Breast Cancer: Questions and Answers
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Adjuvant Therapy for Breast
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Adjuvant Therapy for Breast
Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer John delcharco, MD (Statistics based on CVMC data 2009-2013) Statistics Lung cancer is the leading cause of cancer deaths in the United States. The American Cancer Society estimates
Non-Small Cell Lung Cancer John delcharco, MD (Statistics based on CVMC data 2009-2013) Statistics Lung cancer is the leading cause of cancer deaths in the United States. The American Cancer Society estimates
Kidney Cancer OVERVIEW
 Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Avastin in breast cancer: Summary of clinical data
 Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
Avastin in breast cancer: Summary of clinical data Worldwide, over one million people are diagnosed with breast cancer every year 1. It is the most frequently diagnosed cancer in women 1,2, and the leading
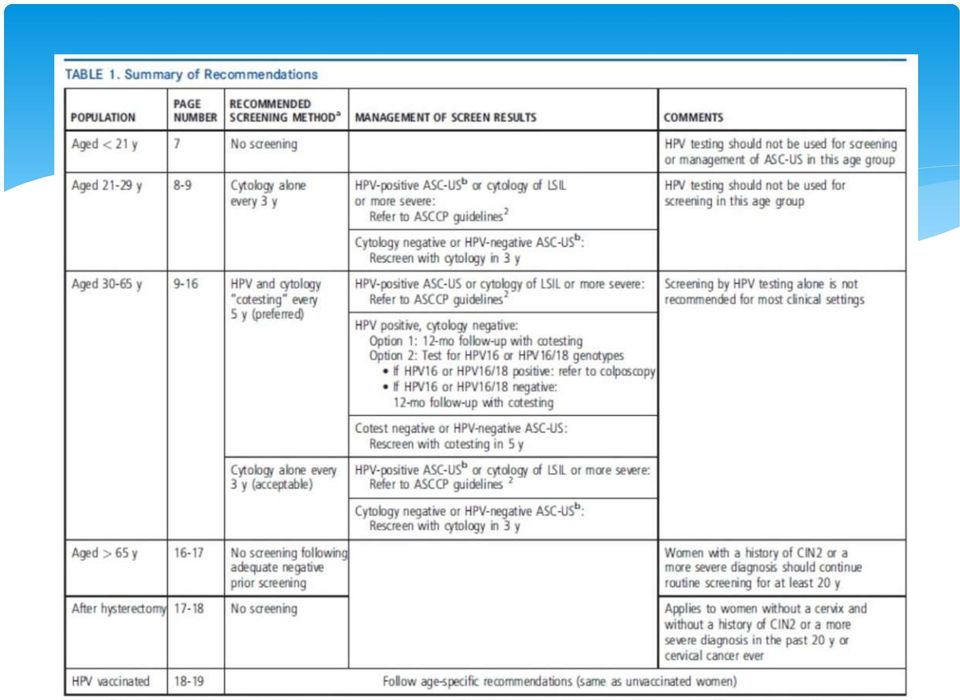
Cervical Cancer Screening and Management Guidelines: Changing Again, Huh?
 Cervical Cancer Screening and Management Guidelines: Changing Again, Huh? Summary of 2013 recommendations from ASC (American Cancer Society), ASCCP (American Society for Colposcopy and Cervical Pathology),
Cervical Cancer Screening and Management Guidelines: Changing Again, Huh? Summary of 2013 recommendations from ASC (American Cancer Society), ASCCP (American Society for Colposcopy and Cervical Pathology),
Avastin: Glossary of key terms
 Avastin: Glossary of key terms Adenocarcinoma Adenoma Adjuvant therapy Angiogenesis Anti-angiogenics Antibody Antigen Avastin (bevacizumab) Benign A form of carcinoma that originates in glandular tissue.
Avastin: Glossary of key terms Adenocarcinoma Adenoma Adjuvant therapy Angiogenesis Anti-angiogenics Antibody Antigen Avastin (bevacizumab) Benign A form of carcinoma that originates in glandular tissue.
How To Perform Da Vinci Surgery
 Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Radioterapia panencefalica. Umberto Ricardi
 Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Radioterapia panencefalica Umberto Ricardi Background Systemic disease to the brain is unfortunately a quite common event Radiotherapy, especially with the great technical development during the past decades,
Stage I, II Non Small Cell Lung Cancer
 Stage I, II Non Small Cell Lung Cancer Best Results T1 (less 3 cm) N0 80% 5 year survival No Role Adjuvant Chemotherapy Radiation Therapy Reduces Local Recurrence No Improvement in Survival 1 Staging Mediastinal
Stage I, II Non Small Cell Lung Cancer Best Results T1 (less 3 cm) N0 80% 5 year survival No Role Adjuvant Chemotherapy Radiation Therapy Reduces Local Recurrence No Improvement in Survival 1 Staging Mediastinal
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate e P rofessor Professor Radiation Oncology
 Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
What is cervical cancer?
 What is cervical cancer? Cervical cancer is a term used for a tumour that starts in the cervix where the uterus (womb) meets the vagina (birth canal). The cells of the cervix don t suddenly turn into cancer;
What is cervical cancer? Cervical cancer is a term used for a tumour that starts in the cervix where the uterus (womb) meets the vagina (birth canal). The cells of the cervix don t suddenly turn into cancer;
What is HPV? Low-risk HPV types. High-risk HPV types
 HPV and Cancer What is HPV? HPV is short for human papilloma (PAP-uh-LO-muh) virus. HPVs are a large group of related viruses. Each HPV virus in the group is given a number, which is called an HPV type.
HPV and Cancer What is HPV? HPV is short for human papilloma (PAP-uh-LO-muh) virus. HPVs are a large group of related viruses. Each HPV virus in the group is given a number, which is called an HPV type.
January 2013 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Summary. Contents
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
ALCHEMIST (Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials)
") ALCHEMIST (Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials) 3 Integrated Trials Testing Targeted Therapy in Early Stage Lung Cancer Part of NCI s Precision Medicine Effort in
ALCHEMIST (Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials) 3 Integrated Trials Testing Targeted Therapy in Early Stage Lung Cancer Part of NCI s Precision Medicine Effort in
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases
 Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Hodgkin Lymphoma Disease Specific Biology and Treatment Options. John Kuruvilla
 Hodgkin Lymphoma Disease Specific Biology and Treatment Options John Kuruvilla My Disclaimer This is where I work Objectives Pathobiology what makes HL different Diagnosis Staging Treatment Philosophy
Hodgkin Lymphoma Disease Specific Biology and Treatment Options John Kuruvilla My Disclaimer This is where I work Objectives Pathobiology what makes HL different Diagnosis Staging Treatment Philosophy