LAWRENCE DOTT, CHIEF EXECUTIVE OFFICER, MCKENZIE INSTITUTE INTERNATIONAL
|
|
|
- Branden Summers
- 7 years ago
- Views:
Transcription
1 The McKenzie Institute International 2014 Vol. 3, No. 3 Feature Commentary 13 TH INTERNATIONAL CONFERENCE ENCE IN MECHANICAL DIAGNOSIS AND THERAPY COPENHAGEN, DENMARK ~ SEPTEMBER 2015 LAWRENCE DOTT, CHIEF EXECUTIVE OFFICER, MCKENZIE INSTITUTE INTERNATIONAL They say time flies and, as such, September 2015 will be with us sooner than we all realise. I have been very fortunate to have visited Copenhagen and believe this is a wonderful city in which to present our next International Conference. The capital city of Denmark is full of history and beauty, and has attractions and sights to suit every taste and interest. Three of the most famous attractions in the city are the more than 100 year old amusement park Tivoli Gardens, the statue of The Little Mermaid, and the freetown of Christiania. The Conference theme is With the Tide MDT into the Future, and is a tribute to Robin McKenzie. The theme will reflect the changes that have transpired as a result of Robin s influence, not only in regards to the development and dissemination of Mechanical Diagnosis and Therapy, but also in the much wider context of conservative care. Robin s legacy will continue to impact the way musculoskeletal conditions are managed, and most importantly, will continue to benefit patients throughout the world, long into the future. As has been our custom in the past for our International Conferences, we have assembled, for your further education and enlightenment, an array of world renowned keynote speakers and researchers who will provide you with their views. The conference programme is structured in a manner where the speakers will challenge our beliefs, our methods, and make us think again. However, I believe they will, at the same time, be most controversial and very entertaining. The delegates will enjoy presentations of research, panel debates, patient assessments, diagnosis, and treatment, discussions and poster presentations. We have also secured a beautiful venue for the Conference Gala Event on the Saturday evening at Moltke s Palace. The Palace was originally built in 1702 and has served a myriad of purposes over its time-honoured history; a home for nobles, merchants, a dowager queen, a Danish prime minister and an array of upper class personages. Today, the palace has been lovingly and thoroughly restored. Our evening will commence with a canal ride from the Tivoli Hotel to Nyhavn while enjoying a pre-dinner drink. Then a short walk from Nyhavn to the Palace, to enjoy a great evening with superb cuisine and good wine. We are expecting we will have delegates from over 34 countries attending. The Institute currently has 28 branches worldwide, and is in the process of establishing new branches in Spain and South Africa. We also present MDT Education in an additional nine countries. MDT is clearly very effective and continuing to grow worldwide. Copenhagen 2015 will further prove this. Full details on our conference - the programme, hotel accommodation, gala dinner, together with the pre-conference workshop MDT and the Athlete, including registration - are available by clicking the banner below, or by visiting the Institute s website, I encourage you to register early, and look forward to greeting you in Copenhagen during 4 6 September Best Regards, Lawrence Dott Chief Executive Officer McKenzie Institute International Inside This Issue: Feature Commentary Branch Spotlight A Clinician s Perspective Literature Reviews Business & Marketing Corner

2 The McKenzie Institute International 2014 Vol. 3, No. 3 BRANCH SPOTLIGHT McKenzie Institute Japan Yoshihiro Iwasada, PT, MS, Dip. MDT Greetings Konnichiwa (Hello) from the country of The Rising Sun! The island nation of Japan can be found in East Asia. Its territory is a little smaller than the US state of Montana and slightly larger than the country of Norway. About three quarters of the land is not suitable for living, yet over 100,000,000 people call this island home. Japan is one of the most densely populated nations in the world. Medical and Healthcare Providers Registered medical and healthcare providers for musculoskeletal medicine in Japan are Medical Doctors (MD), Physical Therapists (PT), Occupational Therapists (OT), Judo Therapists, Acupuncturists and Massage Therapists. Chiropractors and Osteopathologists are not registered providers in our country calculations show that there are about 93,000 Physical Therapists in Japan. PTs working under our national medical insurance system are not entitled to run PT clinics and need doctors prescriptions to perform treatments. Development of the Japanese Branch The Japanese Branch was established in 2002 and was designated the 25 th branch of The McKenzie Institute. The branch is a registered not-for-profit organization (NPO) consisting of six members. Our board is unique, as it is comprised of multi-disciplinary professions. I serve as our Chairman and am a PT, while our Vice-Chairman is an Orthopaedic Surgeon. The remaining four board members are comprised of two PTs, one other Orthopaedic Surgeon and one Judo Therapist. This multi-profession composition indicates how MDT in Japan opens its doors to any medical or healthcare professionals who have a passion to learn MDT. Courses Our official inaugural McKenzie course was held in March 2000, where we were very honored to learn from Robin McKenzie, himself, as well as MIUSA Diplomate and Faculty member, Robert Medcalf. In the first few years, we held only a few courses each year, but in the last few years we have finally come to have more than 10 courses a year. In 2013, we hosted 12 courses from Parts A-D, one Physician Seminar, two brush-up seminars for Certified MDT clinicians and one Branch Conference. PTs, OTs, Judo Therapists, Acupuncturists, Chiropractors, Dentists and many other medical and healthcare professionals are eligible to attend our courses. In Japan there is no discrimination or barrier among medical and healthcare providers when they learn MDT. Human Assets (Dip. MDT and Cert. MDT) As of August 2014, the Japanese Branch has three Diplomaed McKenzie Clinicians and 212 Credentialed McKenzie Clinicians. All three of our Diplomates are closely involved in the teaching of our courses. I, myself, am a Senior Instructor, Hana Sano is an Instructor and Takenori Maekawa is Probationary Faculty. In many cases, the three of us work together on patient demonstrations, answering questions from course participants and teaching techniques. The teaching style seems
, Physical Therapists (PT), Occupational Therapists (OT),")
3 well received by course participants and is likely to encourage many of them to proceed to the next course. In Japan, Cert. MDTs are invited to retake Part A-D for free to brush up on their MDT knowledge and techniques. Looking at this privilege from the standpoint of an Instructor, it is beneficial because those Cert. MDTs become valuable assistants, especially during practical sessions. I cannot overemphasize how important the McKenzie Institute International Instructors were, are and will continue to be for MDT in Japan. Starting with Robin and Robert in 2000, we are very lucky to have had first-rate instructors, such as Scott Herbowy, Colin Davies, Kevin Turner, Helen Clare, Stephen May, Grant Watson and Greg Lynch, working with us over the last 13 years. They are all wonderful instructors, and we are fascinated not only with their clinical skills, but also their strong belief and commitment to MDT. Although Japanese instructors are now entitled to teach all Japanese courses, we would like to keep learning from such first rate international instructors. Agenda Among various levels of agenda, the following two goals are what the Japanese Branch is now most focused on targeting: 1. More publications of MDT research: We have to admit that MDT evidence is mostly produced outside of Japan. It is our strong intention to publish valuable evidence that will be cited by our international MDT colleagues. Since 2013, we have started hosting an annual branch conference. This conference is purely for research presentations and one of its purposes is to encourage Japanese MDT clinicians to commit themselves to more research projects. Fortunately, Hiroshi Takasaki, PT, PhD, Cert. MDT, who has already published some important literature in English, returned from the University of Queensland, Australia after attaining PhD this year. He has suggested a few interesting research projects regarding MDT. I hope that he will become one of the key persons in this field. 2. Maintenance of the Certified MDT competence: This must be a universal agenda. Expectations from the Japanese public on MDT clinicians have grown steadily over the last few years. We are seriously concerned with whether or not Certified MDT practitioners are competent to live up to this expectation. We offer Certified MDT clinicians two educational opportunities: One is a Brush-Up Seminar and the other is, as described above, the opportunity to retake Parts A-D free of charge. The Brush-Up Seminar in Japan is very clinically oriented. Participants are separated into a few groups and each group assesses and manages a volunteer patient in front of the other groups. This is really exciting and an effective learning experience for both participants and instructors.

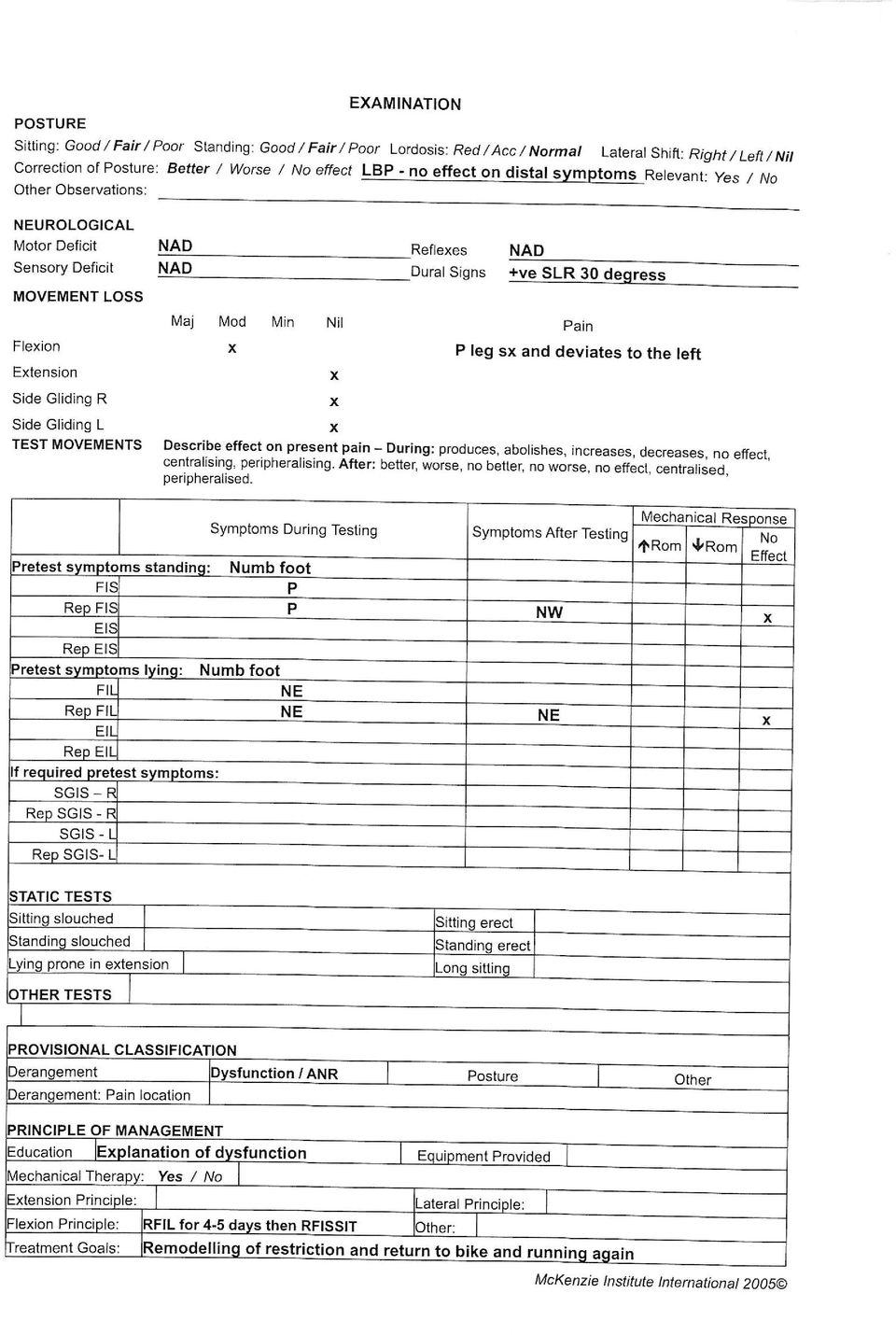
4 The McKenzie Institute International 2014 Vol. 3, No. 3 CASE REVIEW: A CLINICIAN S PERSPECTIVE Case Review: 35-Year-Old Male with History of Low Back Pain Brian Østergaard Sørensen, PT, Dip.MDT Introduction Non-specific low back pain is the most common musculoskeletal problem. A wide range of tests and treatments have been suggested, however, most are not well-validated (Deyo et al. 2009) and have poor reliability (May et al. 2006) and very low success rates when it comes to effective treatment (Delitto et al. 2012). According to Delitto et al. (2012), subgroup classification has the potential to improve outcomes. The patient in this case report has been subgroup classified using the classification system proposed by McKenzie (McKenzie and May 2003). On the initial visit, the patient presented with characteristics that required further testing and clinical reasoning prior to classification. This process included intervention and a six month follow-up and is presented in the following review. Patient Presentation The patient, a 35-year-old male, presents with a nine month history of low back and leg pain which has been unchanged for five months. Symptoms commenced for no apparent reason, however exacerbation of symptoms during a game of bumperz made him visit his GP where he was given advice according to the guidelines for acute low back pain (Cost B13, 2004). The patient s back, thigh (posterior) and calf symptoms are intermittent, but his foot (mainly lateral) symptoms are constant and without much variation in intensity. He described symptoms consistent with S1 nerve root pathology. He displayed the following neurological signs: positive SLR at 30 degrees. The patient reports more symptoms with activities involving flexion, both with and without rotation, including standing up riding his bike. If he rides his bike, runs more than one kilometer or sits for prolonged periods of time, both back and leg pain are produced, but his symptoms return to normal within a few minutes of the conclusion of those activities. At times, the patient s back pain and soreness is present for longer, but always returns to normal again by the next morning. His sitting tolerance improves with lumbar support. He reports less pain when standing, walking and lying with no preference to a specific position. Based on what gives him the most relief from pain, he has changed working position from sitting to standing; although, at the end of the day, he feels that he benefits from sitting due to a tired and sore back. He states that except for running, which produces his leg symptoms to a very unpleasant level of pain, he still tries to do his leisure activities, though they have been greatly reduced in length of time and intensity since these activities provoke symptoms in the back and leg. He states that he believes that exercise will help him recover. Earlier in the process, he received care from a chiropractor, a massage therapist and a physiotherapist. The latter of these three therapists prescribed extension in lying, which reduced back pain slightly between visits one and three, but without any further improvement. Clinical Reasoning The patient presents with no red flags and no indications of maladaptive behaviour in regard to fear avoidance. Based on his history, symptom location, timeframe and symptomatic behaviour, the working diagnoses are either a reducible derangement, an irreducible derangement (McKenzie & May 2003), an adherent nerve root (ANR) or an entrapment (Petersen 2003; Ido & Urushidani 2001). Constant symptoms in the foot and intermittent back pain (which he describes as sore and not painful) have been unchanged for the last five months and, thus, the constant foot symptoms are inconsistent with a classical ANR diagnosis. However, his description of intermittent symptoms in a narrow band as a result of bending (NW afterwards), does fit the pattern of a restrictive lesion, such as an ANR. The constant symptoms in his foot would be more consistent with a MDT defined entrapment, however, the literature doesn t seem to agree on how to define an entrapment (Ido & Urushidani 2001; Porter et al. 1984).
, subgroup classification has the potential to improve outcomes.")
5 Both ANR and entrapment are rarely encountered (Petersen 2003). Further differentiation between these would require flexion-based testing showing that the entrapment would have a brief increase in ROM that would subside again within minutes. The ANR flexion motion would remain unchanged. Furthermore, the entrapment would have motion loss in extension and a likely loss of lateral movement toward the symptomatic side. This patient displays good extension and lateral motion. His reporting of aggravation of symptoms in sitting is likely to occur in both reducible and irreducible derangements, as well as entrapment, but not in an ANR. The indication of a reducible posterior derangement with a directional preference for extension is that symptoms in the back and thigh decrease or abolish when lordosis is maintained in sitting, standing, walking and lying prone and remain better afterwards. In this case, prolonged sitting consistently produced lingering symptoms and extension exercises provided only temporary relief to his back pain as he performed them. Lateral techniques had no effect on symptoms. He didn t respond with either symptomatic or mechanical changes when tested with repeated movements or sustained positions, as would be encountered in a derangement (McKenzie & May 2003). The irreducible derangement often reports worse leg pain than back pain. Based on anecdotal experience, this statement is often related to the early phases of the phenomenon. His constant foot symptoms did not appear to be relevant to his current condition. These long standing sensory disturbances are commonly seen in patients who have experienced disc prolapse, as most of their symptoms have subsided and functional levels have returned towards normalization due to the generally favourable prognosis (Jensen et al. 2006). This hypothesis was confirmed by a MRI. Objective Examination During the history taking, his back starts to turn sore and correction of posture results in a slight decrease, however it has no effect on distal symptoms. His neurological exam was negative except for a positive SLR. ROM testing presents a moderate loss of flexion, deviation to the symptomatic side, and a production of familiar thigh symptoms. There is nil loss or symptom production in extension or SGIS in either direction. A provocative strategy with repeated flexion in standing presents a consistent response with thigh and leg symptom production on each repetition that is no worse afterwards. Repeated flexion in lying has no effect on symptoms during or after testing. Clinical Reasoning and Management The core of the mechanical and symptomatic pattern is that he has been unchanged for five months and unable to produce a lasting response with mechanical loading. The lesion behaviour closely resembles an ANR based on the following objective findings: positive SLR, no loss of lumbar extension or SGIS, response to repeated flexion in standing (Prod NW), the lack of production of symptoms during repeated unloaded flexion, and no change in the mechanical baseline (including deviation to the symptomatic side). The management of this diagnosis was aimed at remodelling the restrictive lesion (McKenzie & May 2003) and functional rehabilitation involving bike rides and running based on the patient s preferences for these activities (Kool et al. 2007). The patient was prescribed an exercise program consisting of four days of 4-5 times RFIL to test the integrity of the lesion. Next step was to progress to 5-6 times repeated flexion in sitting with gradually straightening the leg, and then finally to 5-6 times flexion in standing as it became tolerable, always followed by a few extensions. Familiar pain should be produced, but be no worse afterward and no further obstruction to movement should appear. The patient was told that prognosis is difficult to predict with this diagnosis and that he must have patience. Evidence for this approach is limited and only supported in case reports (Melbye 2010; Gallegos et al. 2008) and on ligaments (Benani 2008). It is important to note that the actual mechanisms responsible for these positive changes have not yet been discovered. It is relevant to mention that six days after the patient s first visit, while at his second visit, he presented unchanged on all baselines. Following the second visit, the patient was managed by phone and . At his six month phone follow-up, the patient reported returning to his previous functional level as before his symptoms started. The soreness in his back was almost never present and thigh and leg pain was gone, however, his foot symptoms were only reduced slightly. This patient presents with a rather grey pattern of signs and symptoms and therefore doesn t perfectly match a sub-classification, however, he was showing characteristics of an inactive and restricted lesion, as compared to an active lesion, which determined the path to follow for recovery.

6 References Benani, A. et al. (2008). How a daily and moderate exercise improves ligament healing. IRBM; 29(4): Cost B13. (2004). European Guidelines for the Management of Acute Nonspecific Low Back Pain in Primary Care. European Commission Research Directorate General. Web. 19 Nov Delitto, A. et al. (2012). Clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. Journal of Orthopaedic & Sports Physical Therapy; 42(4): A1-A57. Gallegos et al. (2008). Mechanical Diagnosis and Therapy of an Adherent Lumbar Nerve Root. Athletic Therapy Today; 13(4): Ido, K. & Urushidani, H. (2001). Fibrous adhesive entrapment of lumbosacral nerve roots as a cause of sciatica. Spinal Cord; 39: Jensen, T. S. et al., Natural Course of Disc Morphology in Patients with Sciatica. Spine; 31(14): Kool, J. et al. (2007). Function-Centered Rehabilitation Increases Work Days in Patients With Nonacute Nonspecific Low Back Pain: 1-Year Results From a Randomized Controlled Trial. Archives of Physical Medicine and Rehabilitation; 88: McKenzie, R. and May, S. The Lumbar Spine: Mechanical Diagnosis & Therapy; Waikanae, New Zealand: Spinal Publications New Zealand LTD nd ed. Print. Melbye, M. (2010). An adherent nerve root - Classification and exercise therapy in a patient diagnosed with lumbar disc prolapse. Manual Therapy; 15: Petersen, T. Non-specific Low Back Pain: Classification and Treatment. Sweden: Studentlitteratur AB, Print. Porter, et al. (1984). The Natural History of Root Entrapment Syndrome. Spine; 9(4): Suri, P. et al. (2010). The accuracy of the physical examination for the diagnosis of midlumbar and low lumbar nerve root impingement. Spine; 36(1): 63-73

7

8
9 The McKenzie Institute International 2014 Vol. 3, No..3 LITERATURE REVIEWS Summary and Perspective of Recent Literature Stephen May, PhD, MA, FCSP, Dip. MDT, MSc (UK) Henry SM, van Dillen L, Oulette-Morton RH, Hitt JR, Lomond KV, DeSamo MJ, Bunn JY. (2014). Outcomes are not different for patient-matched versus non-matched treatment in subjects with chronic, recurrent low back pain: a randomized clinical trial. Spine J; doi: Background Classification systems are meant to improve treatment outcomes. Two commonly used classification systems in the USA are the Treatment Based Classification System, advocated by Fritz et al., and the Movement Impairment System, advocated by Sarhmann et al. Purpose To assess if providing matched treatment based on patient clinical features provided superior outcomes to unmatched treatment for patients with chronic low back pain. Study Design A randomized controlled trial. Patients In total, 1,022 patients were screened and 898 were excluded according to pre-ordained exclusion criteria. Following a sample size calculation, patients with low back pain of at least 12 months (N = 124) were examined and then stratified into two groups: those who were eligible for stabilization exercises according to the Treatment Based Classification System or the Movement Impairment System and those who were ineligible. Outcome Measures Oswestry Disability Index (ODI) and Numeric Pain Rating Scale were the primary outcome measures. Secondary outcome measures were gathered at baseline, after the seventh week of treatment, and at 12 months. Successful treatment was determined by at least an 8% point reduction on the ODI. Interventions 124 back pain patients were assessed for eligibility for the Treatment Based Classification System or the Movement Impairment System and then randomized to matched or unmatched treatments. 76 received a matched treatment and 25 an unmatched treatment. Results Both groups improved significantly, but there was no significant difference in primary outcomes between the groups at seven weeks and 12 months. The matched group did not show superior outcomes at any point, except on one secondary measure, the disability scale, at seven weeks (p=0.01) and 12 months (p=<0.0001). Approximately 45% of the matched group and 48% of the unmatched group achieved treatment success of at least 8% reduction in ODI score. Conclusion Providing a treatment matched to the criteria for either the Treatment Based Classification System or the Movement Impairment System did not improve treatment outcomes compared to treatment that was unmatched, except on one secondary outcome measure. Comment This article is in line with previous work that has stated that matching patient sub-groups to specific treatments on the lines of the clinical prediction rules does not result in better outcomes (Haskins et al. 2012; Patel et al. 2013). Such a conclusion is counter-intuitive, but, unfortunately, supported by the evidence. What is not clear is if the lack of effect is because matching sub-groups to specific treatment is not helpful or if it is the Treatment Based Classification System that is of no value in optimising treatment. References Haskins R, Rivett DA, Osmotherly PG. (2012). Clinical prediction rules in the physiotherapy management of

10 low back pain: a systematic review. Manual Therapy; 17:9-21. Patel S, Friede T, Froud R, Evans DW, Underwood M. (2013). Systematic review of randomized controlled trials of clinical prediction rules for physical therapy in low back pain. Spine; 38: Miller-Spoto M, Gombatta SP. (2014). Diagnostic labels assigned to patients with orthopaedic conditions and the influences of the label on selection of interventions: a qualitative study of orthopaedic clinical specialists (OCS). Physical Therapy; 94: Background A variety of diagnostic classification systems are used by physical therapists, but what systems are used is not known, nor how these systems affect treatment decisions. Purposes 1. To examine the diagnostic labels used. 2. To determine how the label affects treatment. Study design A cross-sectional survey, using two case studies, developed for the study; one with low back pain and the other with shoulder pain. Participants Over a six week period, the case studies and the survey were ed via SurveyMonkey to 877 physical therapists who were Orthopaedic Certified Specialists in the USA. 135 responded, of which 107 (12%) were completed thoroughly enough to use for data analysis. The low response rate may have limited the generalisability of the results. The majority (72%) had been in practice more than 15 years, 91% worked in outpatients, and 55% were male. Outcome measures The type of classification system or diagnostic label they would have used for case studies. Results The most common labels used for the back case study were combination (49%) and pathology (33%). For the shoulder case study, the most common labels were pathology (57%) and combination (35%). For the low back case study, 47% would have used the McKenzie Method, 18% a patho-anatomic label, 9% the Treatment -Based Classification System, 1% the Movement Impairment System, 6.5% APTA practice patterns, and 19% other. For the shoulder case study, 58% would have used a patho-anatomic label, 17% APTA practice patterns, 4% Movement Impairment System, 3% McKenzie Method, and 19% other. The classification systems used did not impact the interventions used, with similar treatment patterns for combination and pathology-based labels. Treatments were most commonly some form of exercise or mobilisation of joints or soft tissues. Over 75% reported they would use mobilisation, functional training, neuromuscular re-education, and stretching. Over 50% reported soft tissue mobilization. About 30% reported balance training. Over 15% reported modalities. The treatment interventions were very similar for both case studies. Conclusion There is little consistency in how therapists assign diagnostic labels, and the label does not seem to influence the selection of interventions. Comment Amongst the responding therapists, clearly the McKenzie Method was commonly used for spinal patients, but not for extremity patients. Counter-intuitively, the classification system did not appear to influence the treatments that they would have provided. This rather begs the question: Why bother to use a classification system at all?
.")
11 Cakir S, Hepguler S, Ozturk C, Korkmaz M, Isleten B, Atamaz FC. (2014). Efficacy of therapeutic ultrasound for the management of knee osteoarthritis. A randomized, controlled, and double-blind study. Am J Phys Med & Rehab; 93: Background Thermal and electro-therapy modalities continue to be used for the treatment of patients with osteoarthritis of the knee, despite limited evidence for its efficacy. Purpose To compare the effectiveness of pulsed and continuous ultrasound against sham ultrasound in patients with osteoarthritis of the knee. Study design A randomized controlled trial. Patients 60 patients with osteoarthritis of the knee, according to American College of Rheumatology criteria, randomized into one of three groups: continuous ultrasound, pulsed ultrasound or sham ultrasound. Interventions Continuous ultrasound, pulsed ultrasound or sham ultrasound; all five times a week, for two weeks. All groups also received a home exercise programme, comprised of strengthening and stretching exercises, to be completed at least three times per week. Outcomes WOMAC index for pain and function at baseline, the end of treatment and at six months. Results All groups showed significant improvement at both follow-up times, but there were no significant differences between groups. Conclusion The results suggest that therapeutic ultrasound proved no additional benefit to improve pain and function when used in addition to exercise training. 60 patients with knee osteoarthritis were randomised to continuous, pulsed or sham ultrasound in addition to being prescribed a home exercise strengthening programme. All groups showed significant improvements in pain and function, with no significant differences between groups, at six months. This trial adds further evidence about the value of exercise in knee osteoarthritis. It also provides further evidence about the lack of value in ultrasounds. Proponents for the use of ultrasound could argue that different intensity levels of ultrasound could have been more effective. A frequency of 1 MHz with intensity of 1W/cm 2 was used for continuous and pulsed at the same frequency on 1:4 pulse ratio, which was derived from previous studies. However, this ignores the fact that several applications were tried and these were compared to a placebo application with the machine switched off, where both the patients and the treatment providers were blinded to the status of the machine. A sample size was conducted so the number of patients, though apparently quite small, was sufficient to have detected a difference, if one really existed. The patients were allowed to take NSAIDs and paracetamol, and usage was higher in the sham group.

12 The McKenzie Institute International 2014 Vol. 3, No. 3 BUSINESS & MARKETING CORNER Are MDT Practitioners Ready to Consult Patients Online? Yoav Suprun, PT, DPT, Dip. MDT, CSCS To start, let s look at a couple of questions you may want to ask yourself: 1. Are you comfortable doing an initial evaluation while seeing your patient remotely in a secure way? (see Google Helpouts below) 2. Can you provide Skype, Google Helpouts or any other web based tool for follow-ups with your traveling patients? 3. What about a patients who you discharged, who wants you to see them three or six months down the road to make sure they are doing their exercises correctly? 4. What are the legal implications of online patient consultation in your State and/or Country? Telemedicine is growing at a fast pace. The latest predictions by world-renowned firm, Deloitte, state that Almost one in six doctor visits will be virtual this year (Mearian, L. 2014). To read the full report by Deloitte, click here. Regulations regarding online help and advice by healthcare professionals are still in the works worldwide. Google Helpouts, for example, is an online collaboration service from Google that launched in November 2013 and allows users to share their expertise through live video and provide real-time help from their computers or mobile devices. Practitioners, referred to as Providers, offering help through Google Helpouts range from large, medium, or small companies to individuals. Providers must speak English as a first language and be residents of either the United States, Canada, Ireland, the United Kingdom, Australia or New Zealand. Providers create and maintain listings that explain what they offer, their qualifications, their prices, and their schedules. Every listing has a link to the provider s Helpouts calendar. Providers must pass Google's screening process to qualify. To read more on this unique, new service by Google, feel free to visit helpouts.google.com/home. Let s start a dialogue on this topic! Do you feel it is time for us to make MDT a leading online service provider? Do we have the tools necessary to observe movement loss and question our patients on their symptom response to repeated movement testing via a computer or mobile device? International MDT clinicians: What trends do you see shaping up in your respective countries in terms of online live video support? Please share your experiences with the MDT World Press Editorial Team. Let s have an open discussion that will hopefully lead us to share stories on how MDT is successfully utilized to provide care online. me at yoav@sobespine.com to share your opinion. If you would rather remain anonymous - just let me know and your name will not be shared. I look forward to hearing from all of you! References: Mearian, L. (8 August 2014). Almost one in six doctor visits will be virtual this year.

Clinical Reasoning The patient presents with no red flags and no indications of maladaptive behaviour in regard to fear avoidance.
 The McKenzie Institute International 2014 Vol. 3, No. 3 CASE REVIEW: A CLINICIAN S PERSPECTIVE Case Review: 35-Year-Old Male with History of Low Back Pain Brian Østergaard Sørensen, PT, Dip.MDT Introduction
The McKenzie Institute International 2014 Vol. 3, No. 3 CASE REVIEW: A CLINICIAN S PERSPECTIVE Case Review: 35-Year-Old Male with History of Low Back Pain Brian Østergaard Sørensen, PT, Dip.MDT Introduction
Mechanical Diagnosis And Therapy of the Cervical Spine. The McKenzie Method. Allan Besselink, PT, Dip.MDT Smart Sport International Austin, Texas
 Mechanical Diagnosis And Therapy of the Cervical Spine The McKenzie Method Allan Besselink, PT, Dip.MDT Smart Sport International Austin, Texas Background Physical Therapist Queen s s University 1988 McKenzie
Mechanical Diagnosis And Therapy of the Cervical Spine The McKenzie Method Allan Besselink, PT, Dip.MDT Smart Sport International Austin, Texas Background Physical Therapist Queen s s University 1988 McKenzie
McKenzie Method. Physical Therapy Treatment for lower back pain by Amy Romano
 McKenzie Method Physical Therapy Treatment for lower back pain by Amy Romano What is the McKenzie Method? The McKenzie method (also known as MDT = Mechanical Diagnosis and Therapy) is a comprehensive method
McKenzie Method Physical Therapy Treatment for lower back pain by Amy Romano What is the McKenzie Method? The McKenzie method (also known as MDT = Mechanical Diagnosis and Therapy) is a comprehensive method
Design System review of Medline, CINAHL, AMED, PEDro, and Cochrane databases till August 2010.
 The McKenzie Institute International 2013 Vol. 2, No. 2 LITERATURE REVIEWS Summary and Perspective of Recent Literature Stephen May, PhD, MA, FCSP, Dip. MDT, MSc (UK) May S, Comer C. Is surgery more effective
The McKenzie Institute International 2013 Vol. 2, No. 2 LITERATURE REVIEWS Summary and Perspective of Recent Literature Stephen May, PhD, MA, FCSP, Dip. MDT, MSc (UK) May S, Comer C. Is surgery more effective
Lumbar Disc Herniation/Bulge Protocol
 Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
RNOH Physiotherapy Department (020 8909 5820) Rehabilitation guidelines for patients undergoing spinal surgery
 Rehabilitation guidelines for patients undergoing spinal surgery") RNOH Physiotherapy Department (020 8909 5820) Rehabilitation guidelines for patients undergoing spinal surgery As a specialist orthopaedic hospital we recognise that our broad and often complex patient
RNOH Physiotherapy Department (020 8909 5820) Rehabilitation guidelines for patients undergoing spinal surgery As a specialist orthopaedic hospital we recognise that our broad and often complex patient
Annie O'Connor MSPT, OCS, Cert. MDT
 Annie O'Connor MSPT, OCS, Cert. MDT 541 N. Elmwood #2, Oak Park, IL. 60302 Mobile: 708-921-3352 / Fax: 708-427-3651 aoconnor@ric.org Education / Certifications: 1993 (9 week) Orthopedic Physical Therapy
Annie O'Connor MSPT, OCS, Cert. MDT 541 N. Elmwood #2, Oak Park, IL. 60302 Mobile: 708-921-3352 / Fax: 708-427-3651 aoconnor@ric.org Education / Certifications: 1993 (9 week) Orthopedic Physical Therapy
Alberta s chiropractors: Spine care experts Patient satisfaction and research synopsis
 www.albertachiro.com 11203 70 Street NW Edmonton, AB T5B 1T1 Telephone: 780.420.0932 Fax: 780.425.6583 Alberta s chiropractors: Spine care experts Patient satisfaction and research synopsis Chiropractic
www.albertachiro.com 11203 70 Street NW Edmonton, AB T5B 1T1 Telephone: 780.420.0932 Fax: 780.425.6583 Alberta s chiropractors: Spine care experts Patient satisfaction and research synopsis Chiropractic
OVERALL PROGRAM GOALS AND OBJECTIVES
 The McKenzie Institute is credentialed by the American Physical Therapy Association as a post-professional clinical fellowship program for physical therapists in Mechanical Diagnosis and Therapy (MDT)
The McKenzie Institute is credentialed by the American Physical Therapy Association as a post-professional clinical fellowship program for physical therapists in Mechanical Diagnosis and Therapy (MDT)
A chiropractic approach to managing migraine
 A chiropractic approach to managing migraine What is chiropractic? Chiropractic is a primary healthcare profession that specialises in the diagnosis, treatment and overall management of conditions that
A chiropractic approach to managing migraine What is chiropractic? Chiropractic is a primary healthcare profession that specialises in the diagnosis, treatment and overall management of conditions that
RNOH Physiotherapy Department (020 8909 5820) Rehabilitation guidelines for patients undergoing spinal surgery
 Rehabilitation guidelines for patients undergoing spinal surgery") RNOH Physiotherapy Department (020 8909 5820) Rehabilitation guidelines for patients undergoing spinal surgery As a specialist orthopaedic hospital, we recognise that our broad and often complex patient
RNOH Physiotherapy Department (020 8909 5820) Rehabilitation guidelines for patients undergoing spinal surgery As a specialist orthopaedic hospital, we recognise that our broad and often complex patient
.org. Herniated Disk in the Lower Back. Anatomy. Description
 Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
First Year. PT7040- Clinical Skills and Examination II
 First Year Summer PT7010 Anatomical Dissection for Physical Therapists This is a dissection-based, radiographic anatomical study of the spine, lower extremity, and upper extremity as related to physical
First Year Summer PT7010 Anatomical Dissection for Physical Therapists This is a dissection-based, radiographic anatomical study of the spine, lower extremity, and upper extremity as related to physical
Back & Neck Pain Survival Guide
 Back & Neck Pain Survival Guide www.kleinpeterpt.com Zachary - 225-658-7751 Baton Rouge - 225-768-7676 Kleinpeter Physical Therapy - Spine Care Program Finally! A Proven Assessment & Treatment Program
Back & Neck Pain Survival Guide www.kleinpeterpt.com Zachary - 225-658-7751 Baton Rouge - 225-768-7676 Kleinpeter Physical Therapy - Spine Care Program Finally! A Proven Assessment & Treatment Program
WorkCover s physiotherapy forms: Purpose beyond paperwork?
 WorkCover s physiotherapy forms: Purpose beyond paperwork? Eva Schonstein, Dianna T Kenny and Christopher G Maher The University of Sydney We retrospectively analysed 219 consecutive treatment plans submitted
WorkCover s physiotherapy forms: Purpose beyond paperwork? Eva Schonstein, Dianna T Kenny and Christopher G Maher The University of Sydney We retrospectively analysed 219 consecutive treatment plans submitted
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional
 Cox Technic Email Case Report 72, June 2009, James Schantz DC 1 The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional James E. Schantz, D.C. Leading
Cox Technic Email Case Report 72, June 2009, James Schantz DC 1 The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional James E. Schantz, D.C. Leading
Appointment Types First outpatient. Clinic Types CATS Spine CATS Hip and Knee CATS General Orthopaedic Injection Clinic Podiatry/Foot and Ankle
 Clinic Types CATS Spine CATS Hip and Knee CATS General Orthopaedic Injection Clinic Podiatry/Foot and Ankle Conditions Treated Ankle & foot pain & stiffness Back pain & stiffness Carpal Tunnel/ Nerve impingement/entrapment
Clinic Types CATS Spine CATS Hip and Knee CATS General Orthopaedic Injection Clinic Podiatry/Foot and Ankle Conditions Treated Ankle & foot pain & stiffness Back pain & stiffness Carpal Tunnel/ Nerve impingement/entrapment
Degenerative Lumbar Scoliosis with Stenosis Successfully Treated with Cox Distraction Manipulation
 Cox Technic Case Report #92 (sent February 2011 2/8/11 ) 1 Degenerative Lumbar Scoliosis with Stenosis Successfully Treated with Cox Distraction Manipulation Presented By Robert E. Patterson Jr., D.C.
Cox Technic Case Report #92 (sent February 2011 2/8/11 ) 1 Degenerative Lumbar Scoliosis with Stenosis Successfully Treated with Cox Distraction Manipulation Presented By Robert E. Patterson Jr., D.C.
OUTPATIENT PHYSICAL AND OCCUPATIONAL THERAPY PROTOCOL GUIDELINES
 OUTPATIENT PHYSICAL AND OCCUPATIONAL THERAPY PROTOCOL GUIDELINES General Therapy Guidelines 1. Therapy evaluations must be provided by licensed physical and/or occupational therapists. Therapy evaluations
OUTPATIENT PHYSICAL AND OCCUPATIONAL THERAPY PROTOCOL GUIDELINES General Therapy Guidelines 1. Therapy evaluations must be provided by licensed physical and/or occupational therapists. Therapy evaluations
The McKenzie Institute USA Orthopaedic Manual Physical Therapy Fellowship Program Page 1 of 6
 The McKenzie Institute USA Orthopaedic Manual Physical Therapy Fellowship Program is accredited by the American Physical Therapy Association as a post-professional fellowship program for physical therapists
The McKenzie Institute USA Orthopaedic Manual Physical Therapy Fellowship Program is accredited by the American Physical Therapy Association as a post-professional fellowship program for physical therapists
Archived PHYSIOTHERAPY
 PHYSIOTHERAPY Occupations covered on this sheet are Physiotherapy Assistant, Technical Instructor, Assistant Practitioner, Physiotherapist and Senior Physiotherapist BACKGROUND INFORMATION Physiotherapy
PHYSIOTHERAPY Occupations covered on this sheet are Physiotherapy Assistant, Technical Instructor, Assistant Practitioner, Physiotherapist and Senior Physiotherapist BACKGROUND INFORMATION Physiotherapy
What are Core Muscles?... 2. A Healthy Lumbar Spine...3. What is Low Back Pain?...4. Rehabilitation...6. Stages of Rehabilitation...
 Table of Contents What are Core Muscles?... 2 A Healthy Lumbar Spine...3 What is Low Back Pain?...4 Rehabilitation...6 Stages of Rehabilitation...7 Pain Management....................... 8 Heat/Ice What
Table of Contents What are Core Muscles?... 2 A Healthy Lumbar Spine...3 What is Low Back Pain?...4 Rehabilitation...6 Stages of Rehabilitation...7 Pain Management....................... 8 Heat/Ice What
Low Back Pain Protocols
 Low Back Pain Protocols Introduction: Diagnostic Triage And 1. Patient Group Adults aged 18 years and over with routine low back problems. Patients who have had recent surgery should be referred directly
Low Back Pain Protocols Introduction: Diagnostic Triage And 1. Patient Group Adults aged 18 years and over with routine low back problems. Patients who have had recent surgery should be referred directly
Real Time Ultrasound (RTUS) imaging of the stabilizing muscles of the spine and torso is now available at Marda Loop Sport Physiotherapy.
 imaging of the stabilizing muscles of the spine and torso is now available at Marda Loop Sport Physiotherapy.") Real Time Ultrasound (RTUS) imaging of the stabilizing muscles of the spine and torso is now available at Marda Loop Sport Physiotherapy. Stabilizing Muscles of the Spine & Torso Core muscles that are
Real Time Ultrasound (RTUS) imaging of the stabilizing muscles of the spine and torso is now available at Marda Loop Sport Physiotherapy. Stabilizing Muscles of the Spine & Torso Core muscles that are
Sciatica Yuliya Mutsa PTA 236
 Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
Doctor of Science in Physical Therapy
 Doctor of Science in Physical Therapy The mission for the Doctor of Science (Sc.D.) Program in Physical Therapy is to provide advanced post-professional education to practicing physical therapists in Texas
Doctor of Science in Physical Therapy The mission for the Doctor of Science (Sc.D.) Program in Physical Therapy is to provide advanced post-professional education to practicing physical therapists in Texas
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
Pain-Relief Exercise: The Lower Back
 Pain-Relief Exercise: The Lower Back by Marc Heller, DC Specific exercises are a powerful tool for acute pain relief. These exercises are specific for sciatica or discogenic low back pain, and can help
Pain-Relief Exercise: The Lower Back by Marc Heller, DC Specific exercises are a powerful tool for acute pain relief. These exercises are specific for sciatica or discogenic low back pain, and can help
Introduction: Anatomy of the spine and lower back:
 Castleknock GAA club member and Chartered Physiotherapist, James Sherry MISCP, has prepared an informative article on the common causes of back pain and how best it can be treated. To book a physiotherapy
Castleknock GAA club member and Chartered Physiotherapist, James Sherry MISCP, has prepared an informative article on the common causes of back pain and how best it can be treated. To book a physiotherapy
Rehabilitation Where You Recover. Inpatient Rehabilitation Services at Albany Medical Center
 Rehabilitation Where You Recover Inpatient Rehabilitation Services at Albany Medical Center You're Here and So Are We As the region s only academic medical center, Albany Medical Center offers a number
Rehabilitation Where You Recover Inpatient Rehabilitation Services at Albany Medical Center You're Here and So Are We As the region s only academic medical center, Albany Medical Center offers a number
33 % of whiplash patients develop. headaches originating from the upper. cervical spine
 33 % of whiplash patients develop headaches originating from the upper cervical spine - Dr Nikolai Bogduk Spine, 1995 1 Physical Treatments for Headache: A Structured Review Headache: The Journal of Head
33 % of whiplash patients develop headaches originating from the upper cervical spine - Dr Nikolai Bogduk Spine, 1995 1 Physical Treatments for Headache: A Structured Review Headache: The Journal of Head
Physiotherapy fees and utilization guidelines for auto insurance accident claimants
 No. A-12/97 Property & Casualty ) Auto Physiotherapy fees and utilization guidelines for auto insurance accident claimants To the attention of all insurance companies licensed to transact automobile insurance
No. A-12/97 Property & Casualty ) Auto Physiotherapy fees and utilization guidelines for auto insurance accident claimants To the attention of all insurance companies licensed to transact automobile insurance
SUBMISSION TO THE MEDICARE BENEFITS SCHEDULE REVIEW TASKFORCE
 SUBMISSION November 2015 SUBMISSION TO THE MEDICARE BENEFITS SCHEDULE REVIEW TASKFORCE Submission by the Chiropractors Association of Australia Page 1 of 10 About the Chiropractors Association of Australia
SUBMISSION November 2015 SUBMISSION TO THE MEDICARE BENEFITS SCHEDULE REVIEW TASKFORCE Submission by the Chiropractors Association of Australia Page 1 of 10 About the Chiropractors Association of Australia
Notice of Independent Review Decision DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE:
 Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Live a life with fewer limits Orthopaedic Services
 Live a life with fewer limits Orthopaedic Services Crittenton Orthopaedic Services Repair. Restore. Return. A full range of services for full motion living. From the strains and sprains children experience
Live a life with fewer limits Orthopaedic Services Crittenton Orthopaedic Services Repair. Restore. Return. A full range of services for full motion living. From the strains and sprains children experience
Recovering from a Mild Traumatic Brain Injury (MTBI)
") Recovering from a Mild Traumatic Brain Injury (MTBI) What happened? You have a Mild Traumatic Brain Injury (MTBI), which is a very common injury. Some common ways people acquire this type of injury are
Recovering from a Mild Traumatic Brain Injury (MTBI) What happened? You have a Mild Traumatic Brain Injury (MTBI), which is a very common injury. Some common ways people acquire this type of injury are
Is manual physical therapy more effective than other physical therapy approaches in reducing pain and disability in adults post whiplash injury?
 Is manual physical therapy more effective than other physical therapy approaches in reducing pain and disability in adults post whiplash injury? Clinical Bottom Line Manual therapy may have a role in the
Is manual physical therapy more effective than other physical therapy approaches in reducing pain and disability in adults post whiplash injury? Clinical Bottom Line Manual therapy may have a role in the
Medical Report Prepared for The Court on
 Medical Report Prepared for The Court on Mr Sample Report Claimant's Address Claimant's Date of Birth Instructing Party Instructing Party Address Instructing Party Ref Solicitors Ref Corex Ref 1 The Lane
Medical Report Prepared for The Court on Mr Sample Report Claimant's Address Claimant's Date of Birth Instructing Party Instructing Party Address Instructing Party Ref Solicitors Ref Corex Ref 1 The Lane
Our mission is to help you experience the greatest benefits possible. Our physicians and care staff are dedicated to your needs.
 What to Expect Our mission is to help you experience the greatest benefits possible. Our physicians and care staff are dedicated to your needs. You will most likely require 20-30 procedure sessions to
What to Expect Our mission is to help you experience the greatest benefits possible. Our physicians and care staff are dedicated to your needs. You will most likely require 20-30 procedure sessions to
Studies tell us the pain will be gone or improved significantly in ¾ of patients in 4 weeks and 9/10ths of patients in 6 weeks.
 Back pain is common and ranges from mild to severe pain. Most episodes soon ease within 4 weeks and are not due to serious illness. Keeping active is the most important message along with painkillers if
Back pain is common and ranges from mild to severe pain. Most episodes soon ease within 4 weeks and are not due to serious illness. Keeping active is the most important message along with painkillers if
MANAGING BACK PAIN GETTING YOU BACK INTO ACTION MANAGING BACK PAIN. www.healthcare-rm.com
 H E A L T H R I S K M A N A G E M E N T MANAGING BACK PAIN MANAGING BACK PAIN GETTING YOU BACK INTO ACTION GETTING YOU BACK INTO ACTION www.healthcare-rm.com Who is this for? CONTENTS Introduction about
H E A L T H R I S K M A N A G E M E N T MANAGING BACK PAIN MANAGING BACK PAIN GETTING YOU BACK INTO ACTION GETTING YOU BACK INTO ACTION www.healthcare-rm.com Who is this for? CONTENTS Introduction about
Document Author: Frances Hunt Date 03/03/2008. 1. Purpose of this document To standardise the treatment of whiplash associated disorder.
 Guideline Title: WHIPLASH ASSOCIATED DISORDER Document Author: Frances Hunt Date 03/03/2008 Ratified by: Frances Hunt, Head of Physiotherapy Date: 16.09.15 Review date: 16.09.17 Links to policies: All
Guideline Title: WHIPLASH ASSOCIATED DISORDER Document Author: Frances Hunt Date 03/03/2008 Ratified by: Frances Hunt, Head of Physiotherapy Date: 16.09.15 Review date: 16.09.17 Links to policies: All
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Information on the Chiropractic Care of Lower Back Pain
 Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
Care and Prevention of Sedentary Workplace Injuries. By: Colin Beattie, BKIN, mpt, cafci Registered physical therapist & medical acupuncturist
 Care and Prevention of Sedentary Workplace Injuries By: Colin Beattie, BKIN, mpt, cafci Registered physical therapist & medical acupuncturist Learning Objectives By the end of this presentation you should
Care and Prevention of Sedentary Workplace Injuries By: Colin Beattie, BKIN, mpt, cafci Registered physical therapist & medical acupuncturist Learning Objectives By the end of this presentation you should
Welcome to your LOW BACK PAIN treatment guide
 Welcome to your LOW BACK PAIN treatment guide You are receiving this guide because you have recently experienced low back pain. Back pain is one of the most common musculoskeletal problems treated in medicine
Welcome to your LOW BACK PAIN treatment guide You are receiving this guide because you have recently experienced low back pain. Back pain is one of the most common musculoskeletal problems treated in medicine
Neck Pain & Cervicogenic Headache Integrating Research into Practice: San Luis Sports Therapy s Approach to Evidence-Based Practice
 Neck Pain & Cervicogenic Headache Integrating Research into Practice: San Luis Sports Therapy s Approach to Evidence-Based Practice PROBLEM: Neck Pain and Cervicogenic Headache 66% Proportion of individuals
Neck Pain & Cervicogenic Headache Integrating Research into Practice: San Luis Sports Therapy s Approach to Evidence-Based Practice PROBLEM: Neck Pain and Cervicogenic Headache 66% Proportion of individuals
Range of Motion Exercises
 Range of Motion Exercises Range of motion (ROM) exercises are done to preserve flexibility and mobility of the joints on which they are performed. These exercises reduce stiffness and will prevent or at
Range of Motion Exercises Range of motion (ROM) exercises are done to preserve flexibility and mobility of the joints on which they are performed. These exercises reduce stiffness and will prevent or at
Interpreting Physical Therapy Notes
 Interpreting Physical Therapy Notes Sending a patient to physical therapy does not always guarantee that they are going to receive the same treatment. In fact, the same patient with the same diagnosis
Interpreting Physical Therapy Notes Sending a patient to physical therapy does not always guarantee that they are going to receive the same treatment. In fact, the same patient with the same diagnosis
LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014
 LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014 GUIDE Acknowledgements Acknowledgements The WSIB would like to acknowledge the significant contributions of the following regulated Health
LOW BACK INJURIES PROGRAM OF CARE PROGRAM OF CARE 4TH EDITION 2014 GUIDE Acknowledgements Acknowledgements The WSIB would like to acknowledge the significant contributions of the following regulated Health
This booklet can also be provided in large print on request. Please call 01865 738126. Spinal Stenosis. The Oxford Spine Unit
 This booklet can also be provided in large print on request. Please call 01865 738126 Nuffield Orthopaedic Centre NHS Trust NHS Spinal Team Nuffield Orthopaedic Centre Windmill Road Headington Oxford OX3
This booklet can also be provided in large print on request. Please call 01865 738126 Nuffield Orthopaedic Centre NHS Trust NHS Spinal Team Nuffield Orthopaedic Centre Windmill Road Headington Oxford OX3
PATELLOFEMORAL TRACKING AND MCCONNELL TAPING. Minni Titicula
 PATELLOFEMORAL TRACKING AND MCCONNELL TAPING Minni Titicula PF tracking disorder PF tracking disorder occurs when patella shifts out of the femoral groove during joint motion. most common in the US. affects
PATELLOFEMORAL TRACKING AND MCCONNELL TAPING Minni Titicula PF tracking disorder PF tracking disorder occurs when patella shifts out of the femoral groove during joint motion. most common in the US. affects
Cervical Spondylosis (Arthritis of the Neck)
") Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis North American Spine Society Public Education Series What Is Lumbar Spinal Stenosis? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
Lumbar Spinal Stenosis North American Spine Society Public Education Series What Is Lumbar Spinal Stenosis? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
Case Studies Updated 10.24.11
 S O L U T I O N S Case Studies Updated 10.24.11 Hill DT Solutions Cervical Decompression Case Study An 18-year-old male involved in a motor vehicle accident in which his SUV was totaled suffering from
S O L U T I O N S Case Studies Updated 10.24.11 Hill DT Solutions Cervical Decompression Case Study An 18-year-old male involved in a motor vehicle accident in which his SUV was totaled suffering from
Standard of Care: Cervical Radiculopathy
 Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
WORKERS COMPENSATION APPEAL TRIBUNAL [PERSONAL INFORMATION] CASE ID #[PERSONAL INFORMATION] WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND
![WORKERS COMPENSATION APPEAL TRIBUNAL [PERSONAL INFORMATION] CASE ID #[PERSONAL INFORMATION] WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND](/thumbs/27/10826215.jpg "WORKERS COMPENSATION APPEAL TRIBUNAL [PERSONAL INFORMATION] CASE ID #[PERSONAL INFORMATION] WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND") WORKERS COMPENSATION APPEAL TRIBUNAL BETWEEN: [PERSONAL INFORMATION] CASE ID #[PERSONAL INFORMATION] APPELLANT AND: WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND RESPONDENT DECISION #194 Appellant
WORKERS COMPENSATION APPEAL TRIBUNAL BETWEEN: [PERSONAL INFORMATION] CASE ID #[PERSONAL INFORMATION] APPELLANT AND: WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND RESPONDENT DECISION #194 Appellant
International Postprofessional Doctoral of Physical Therapy (DPT) in Musculoskeletal Management Program (non US/Canada) Curriculum
 in Musculoskeletal Management Program (non US/Canada) Curriculum") International Postprofessional Doctoral of Physical Therapy (DPT) in Musculoskeletal Management Program (non US/Canada) Curriculum Effective: July 2015 INTERNATIONAL POSTPROFESSIONAL DOCTORAL OF PHYSICAL
International Postprofessional Doctoral of Physical Therapy (DPT) in Musculoskeletal Management Program (non US/Canada) Curriculum Effective: July 2015 INTERNATIONAL POSTPROFESSIONAL DOCTORAL OF PHYSICAL
UTILIZING STRAPPING AND TAPING CODES FOR HEALTH CARE REIMBURSEMENT:
 UTILIZING STRAPPING AND TAPING CODES FOR HEALTH CARE REIMBURSEMENT: A GUIDE TO BILLING FOR SPIDERTECH PRE-CUT APPLICATIONS AND TAPE Billing and coding taping and strapping services can be a complex issue.
UTILIZING STRAPPING AND TAPING CODES FOR HEALTH CARE REIMBURSEMENT: A GUIDE TO BILLING FOR SPIDERTECH PRE-CUT APPLICATIONS AND TAPE Billing and coding taping and strapping services can be a complex issue.
Dr. Khaled E. Ayad Alrehab City, Cairo Egypt Cell phone: 002 0100 617 3954 khaled-ayad@hotmail.com
 Dr. Khaled E. Ayad Alrehab City, Cairo Egypt Cell phone: 002 0100 617 3954 khaled-ayad@hotmail.com Education Doctor of Philosophy (physical therapy) Cairo University Cairo, Egypt, Jan 2006 Title of Ph.D.
Dr. Khaled E. Ayad Alrehab City, Cairo Egypt Cell phone: 002 0100 617 3954 khaled-ayad@hotmail.com Education Doctor of Philosophy (physical therapy) Cairo University Cairo, Egypt, Jan 2006 Title of Ph.D.
Physical Therapy. Physical Therapy Payment Policy Policy number M.RTH.02.120301 effective 10/01/2015. Page 1
 Physical Therapy I. Policy University Health Alliance (UHA) will reimburse for physical therapy when it is determined to be medically necessary and when it meets the medical criteria guidelines (subject
Physical Therapy I. Policy University Health Alliance (UHA) will reimburse for physical therapy when it is determined to be medically necessary and when it meets the medical criteria guidelines (subject
2015 EDUCATIONAL PROGRAMMING Mechanical Diagnosis and Therapy : McKenzie Method
 The Robin McKenzie Institute Canada 72 Pinehurst Drive, Dorchester ON N0L 1G2 PH: 1-800-463-8568 Email: mckenziecanada@bellnet.ca 2015 EDUCATIONAL PROGRAMMING Mechanical Diagnosis and Therapy : McKenzie
The Robin McKenzie Institute Canada 72 Pinehurst Drive, Dorchester ON N0L 1G2 PH: 1-800-463-8568 Email: mckenziecanada@bellnet.ca 2015 EDUCATIONAL PROGRAMMING Mechanical Diagnosis and Therapy : McKenzie
Passive Range of Motion Exercises
 Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
What is a Sports Physician?
 What is a Sports Physician? Dr Mike Bundy MBBS MRCGP Dip Sports Med FFSEM Consultant in Sport and Exercise Medicine Medical Director at Pure Sports Medicine Ex-England Rugby senior team Doctor www.puresportsmed.com
What is a Sports Physician? Dr Mike Bundy MBBS MRCGP Dip Sports Med FFSEM Consultant in Sport and Exercise Medicine Medical Director at Pure Sports Medicine Ex-England Rugby senior team Doctor www.puresportsmed.com
Treating Bulging Discs & Sciatica. Alexander Ching, MD
 Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
Treating Bulging Discs & Sciatica Alexander Ching, MD Disclosures Depuy Spine Teaching and courses K2 Spine Complex Spine Study Group Disclosures Take 2 I am a spine surgeon I like spine surgery I believe
FACULTY BIOS HonorHealth Orthopedic Physical Therapy Residency Program
 FACULTY BIOS HonorHealth Orthopedic Physical Therapy Residency Program Jason Tjeerdsma, PT, DPT, OCS, CIDN Dr. Tjeerdsma graduated from the University of South Dakota in 2011 with his Doctorate in Physical
FACULTY BIOS HonorHealth Orthopedic Physical Therapy Residency Program Jason Tjeerdsma, PT, DPT, OCS, CIDN Dr. Tjeerdsma graduated from the University of South Dakota in 2011 with his Doctorate in Physical
SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS?
 SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS? The spinal canal is best imagined as a bony tube through which nerve fibres pass. The tube is interrupted between each pair of adjacent
SPINAL STENOSIS Information for Patients WHAT IS SPINAL STENOSIS? The spinal canal is best imagined as a bony tube through which nerve fibres pass. The tube is interrupted between each pair of adjacent
New York State Workers' Comp Board. Mid and Lower Back Treatment Guidelines. Summary From 1st Edition, June 30, 2010. Effective December 1, 2010
 New York State Workers' Comp Board Mid and Lower Back Treatment Guidelines Summary From 1st Edition, June 30, 2010 Effective December 1, 2010 General Principles Treatment should be focused on restoring
New York State Workers' Comp Board Mid and Lower Back Treatment Guidelines Summary From 1st Edition, June 30, 2010 Effective December 1, 2010 General Principles Treatment should be focused on restoring
Clinical Medical Policy Outpatient Rehab Therapies (PT & OT) for Members With Special Needs
 for Members With Special Needs") Benefit Coverage Rehabilitative services, (PT, OT,) are covered for members with neurodevelopmental disorders when recommended by a medical provider to address a specific condition, deficit, or dysfunction,
Benefit Coverage Rehabilitative services, (PT, OT,) are covered for members with neurodevelopmental disorders when recommended by a medical provider to address a specific condition, deficit, or dysfunction,
Expectancy Effects of Performance Enhancing Supplements on Motivation to Exercise. Chris Dawson and Alfonso Ribero.
 Running Head: EXPECTANCY EFFECTS ON MOTIVATION Expectancy Effects of Performance Enhancing Supplements on Motivation to Exercise Chris Dawson and Alfonso Ribero Hanover College Expectancy Effects 2 Abstract
Running Head: EXPECTANCY EFFECTS ON MOTIVATION Expectancy Effects of Performance Enhancing Supplements on Motivation to Exercise Chris Dawson and Alfonso Ribero Hanover College Expectancy Effects 2 Abstract
Low back pain. Quick reference guide. Issue date: May 2009. Early management of persistent non-specific low back pain
 Issue date: May 2009 Low back pain Early management of persistent non-specific low back pain Developed by the National Collaborating Centre for Primary Care About this booklet This is a quick reference
Issue date: May 2009 Low back pain Early management of persistent non-specific low back pain Developed by the National Collaborating Centre for Primary Care About this booklet This is a quick reference
How To Cover Occupational Therapy
 Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
Guidelines for Medical Necessity Determination for Occupational Therapy These Guidelines for Medical Necessity Determination (Guidelines) identify the clinical information MassHealth needs to determine
15 things you might not know about back pain
 15 things you might not know about back pain Mary O Keeffe (University of Limerick), Dr Kieran O Sullivan (University of Limerick), Dr Derek Griffin (Tralee Physiotherapy Clinic) Managing back pain costs
15 things you might not know about back pain Mary O Keeffe (University of Limerick), Dr Kieran O Sullivan (University of Limerick), Dr Derek Griffin (Tralee Physiotherapy Clinic) Managing back pain costs
Spinal Discectomy & Decompression Surgery
 1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Pre-Operative... 3 7.2 Post-Operative...
1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Pre-Operative... 3 7.2 Post-Operative...
NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES Version 2015-1 Page 1 of 11 Table of Contents SECTION I REQUIREMENTS FOR PARTICIPATION IN MEDICAID 3 QUALIFIED PRACTITIONERS. 3
NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES Version 2015-1 Page 1 of 11 Table of Contents SECTION I REQUIREMENTS FOR PARTICIPATION IN MEDICAID 3 QUALIFIED PRACTITIONERS. 3
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2115/14
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2115/14 BEFORE: C. M. MacAdam : Vice-Chair S. T. Sahay : Member Representative of Employers K. Hoskin : Member Representative of Workers HEARING:
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2115/14 BEFORE: C. M. MacAdam : Vice-Chair S. T. Sahay : Member Representative of Employers K. Hoskin : Member Representative of Workers HEARING:
Fact Sheet. Queensland Spinal Cord Injuries Service. Pain Management Following Spinal Cord Injury for Health Professionals
 Pain Management Following Injury for Health Professionals and Introduction Pain is a common problem following SCI. In the case where a person with SCI does have pain, there are treatments available that
Pain Management Following Injury for Health Professionals and Introduction Pain is a common problem following SCI. In the case where a person with SCI does have pain, there are treatments available that
Nerve Root Pain. Your back pain diagnosis. Contact Details. Spinal Triage Nuffield Orthopaedic Centre Windmill Road Headington Oxford OX3 7LD
 Nerve Root Pain Contact Details Spinal Triage Nuffield Orthopaedic Centre Windmill Road Headington Oxford OX3 7LD Phone: 01865 738051 Fax: 01865 738027 Web Site www.noc.nhs.uk Nerve Pain Patient Information
Nerve Root Pain Contact Details Spinal Triage Nuffield Orthopaedic Centre Windmill Road Headington Oxford OX3 7LD Phone: 01865 738051 Fax: 01865 738027 Web Site www.noc.nhs.uk Nerve Pain Patient Information
Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario
 Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Physiotherapist referral to specialist medical practitioners. 2014 15 pre-budget submission
 Physiotherapist referral to specialist medical practitioners 2014 15 pre-budget submission 1 2014 15 Pre-budget Submission Letter from Marcus Dripps APA President The Australian primary healthcare system
Physiotherapist referral to specialist medical practitioners 2014 15 pre-budget submission 1 2014 15 Pre-budget Submission Letter from Marcus Dripps APA President The Australian primary healthcare system
Hip Arthroscopy Post-operative Rehabilitation Protocol
 Hip Arthroscopy Post-operative Rehabilitation Protocol Introduction Since the early 20 th century, when hip arthroscopy was regarded as being almost impossible to undertake, the procedure has developed
Hip Arthroscopy Post-operative Rehabilitation Protocol Introduction Since the early 20 th century, when hip arthroscopy was regarded as being almost impossible to undertake, the procedure has developed
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN
 CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
Online Course Descriptions (degree seeking):
:") Online Course Descriptions (degree seeking): BSC 6001 Foundations of Clinical Orthopaedics This is an online self study course discussing the foundations of orthopaedics and manipulative therapy. The history
Online Course Descriptions (degree seeking): BSC 6001 Foundations of Clinical Orthopaedics This is an online self study course discussing the foundations of orthopaedics and manipulative therapy. The history
.org. Plantar Fasciitis and Bone Spurs. Anatomy. Cause
 Plantar Fasciitis and Bone Spurs Page ( 1 ) Plantar fasciitis (fashee-eye-tiss) is the most common cause of pain on the bottom of the heel. Approximately 2 million patients are treated for this condition
Plantar Fasciitis and Bone Spurs Page ( 1 ) Plantar fasciitis (fashee-eye-tiss) is the most common cause of pain on the bottom of the heel. Approximately 2 million patients are treated for this condition
NAVIGATING THE MEDICARE MAZE OF REHABILITATIVE SERVICES
 NAVIGATING THE MEDICARE MAZE OF REHABILITATIVE SERVICES NAVIGATING THE COMPLEXITY OF INSURANCE COVERAGE. Fox Rehabilitation is a private practice of physical, occupational, and speech therapists who specialize
NAVIGATING THE MEDICARE MAZE OF REHABILITATIVE SERVICES NAVIGATING THE COMPLEXITY OF INSURANCE COVERAGE. Fox Rehabilitation is a private practice of physical, occupational, and speech therapists who specialize
Updates into Therapeutic Exercise Programs for Patients with LBP. Maximizing Patient Motivation and Outcomes Alice M.
 Updates into Therapeutic Exercise Programs for Patients with LBP Maximizing Patient Motivation and Outcomes Alice M. Davis, PT, DPT Objectives Review Statistics on LBP Discuss current research findings
Updates into Therapeutic Exercise Programs for Patients with LBP Maximizing Patient Motivation and Outcomes Alice M. Davis, PT, DPT Objectives Review Statistics on LBP Discuss current research findings
Rehabilitation after shoulder dislocation
 Physiotherapy Department Rehabilitation after shoulder dislocation Information for patients This information leaflet gives you advice on rehabilitation after your shoulder dislocation. It is not a substitute
Physiotherapy Department Rehabilitation after shoulder dislocation Information for patients This information leaflet gives you advice on rehabilitation after your shoulder dislocation. It is not a substitute
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1708/15
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1708/15 BEFORE: E. Kosmidis : Vice-Chair E. Tracey : Member Representative of Employers C. Salama : Member Representative of Workers HEARING:
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1708/15 BEFORE: E. Kosmidis : Vice-Chair E. Tracey : Member Representative of Employers C. Salama : Member Representative of Workers HEARING:
CANBI. Work Injury Rehabilitation. Canadian Back Institute. The Basics. Canadian vs Hong Kong Experience. www.cbi.ca
 Work Injury Rehabilitation Canadian vs Hong Kong Experience Canadian Back Institute www.cbi.ca Specialists in the prevention and treatment of back and neck pain Founded in 1974 as an education facility
Work Injury Rehabilitation Canadian vs Hong Kong Experience Canadian Back Institute www.cbi.ca Specialists in the prevention and treatment of back and neck pain Founded in 1974 as an education facility
This is my information booklet: Introduction
 Hip arthroscopy is a relatively new procedure which allows the surgeon to diagnose and treat hip disorders by providing a clear view of the inside of the hip with very small incisions. This is a more complicated
Hip arthroscopy is a relatively new procedure which allows the surgeon to diagnose and treat hip disorders by providing a clear view of the inside of the hip with very small incisions. This is a more complicated
CURRICULUM VITAE. 2004-2006 Doctor of Physical Therapy, Temple University, Philadelphia, PA
 CURRICULUM VITAE Jeffrey A. Thompson, PT, DPT, OCS, Cert. MDT Assistant Professor Department of Physical Therapy School of Allied Health Professions LSU Health Science Center 1900 Gavier Street New Orleans,
CURRICULUM VITAE Jeffrey A. Thompson, PT, DPT, OCS, Cert. MDT Assistant Professor Department of Physical Therapy School of Allied Health Professions LSU Health Science Center 1900 Gavier Street New Orleans,
Diagnosis and Management for Chronic Back Pain: Critical for your Recovery
 Diagnosis and Management for Chronic Back Pain: Critical for your Recovery Dr. Connie D Astolfo, DC, PhD (candidate) In past articles I have stressed that the causes of back pain can be very complex. This
Diagnosis and Management for Chronic Back Pain: Critical for your Recovery Dr. Connie D Astolfo, DC, PhD (candidate) In past articles I have stressed that the causes of back pain can be very complex. This
Butler Chiropractic and Wellness "WHAT... "You Should Know and Ask" before going to the Chiropractor"
 Butler Chiropractic and Wellness "WHAT... "You Should Know and Ask" before going to the Chiropractor" 1. What is chiropractic care? There's nothing mysterious about chiropractic. It's a natural method
Butler Chiropractic and Wellness "WHAT... "You Should Know and Ask" before going to the Chiropractor" 1. What is chiropractic care? There's nothing mysterious about chiropractic. It's a natural method
Exercise is Medicine Australia Education evaluation summary
 Exercise is Medicine Australia Education evaluation summary Exercise is Medicine Australia (EIM Australia) seeks to support health care providers to become consistently effective in counselling and referring
Exercise is Medicine Australia Education evaluation summary Exercise is Medicine Australia (EIM Australia) seeks to support health care providers to become consistently effective in counselling and referring
INTERPROFESSIONAL WOUND MANAGEMENT COURSE:
 INTERPROFESSIONAL WOUND MANAGEMENT COURSE: Part A Wound Management Principles and Wound Assessment. Part A: Sat. & Sun January 6&7, 2007 + Part B - Adjunctive Therapies including Electrical Stimulation
INTERPROFESSIONAL WOUND MANAGEMENT COURSE: Part A Wound Management Principles and Wound Assessment. Part A: Sat. & Sun January 6&7, 2007 + Part B - Adjunctive Therapies including Electrical Stimulation
Selkäkipu ajoissa hallintaan kliiniset testit terapian perustana
 Selkäkipu ajoissa hallintaan kliiniset testit terapian perustana Markku Paatelma Auron OMT Keskus Helsinki, Finland What is a clinical reasoning? With the expanding roles of physiotherapists and greater
Selkäkipu ajoissa hallintaan kliiniset testit terapian perustana Markku Paatelma Auron OMT Keskus Helsinki, Finland What is a clinical reasoning? With the expanding roles of physiotherapists and greater
Spine Vol. 30 No. 16; August 15, 2005, pp 1799-1807
 A Randomized Controlled Trial of an Educational Intervention to Prevent the Chronic Pain of Whiplash Associated Disorders Following Rear-End Motor Vehicle Collisions 1 Spine Vol. 30 No. 16; August 15,
A Randomized Controlled Trial of an Educational Intervention to Prevent the Chronic Pain of Whiplash Associated Disorders Following Rear-End Motor Vehicle Collisions 1 Spine Vol. 30 No. 16; August 15,
Is electrotherapy more effective than other physical therapy approaches in reducing pain and disability in adults with supraspinatus tendonitis?
 Is electrotherapy more effective than other physical therapy approaches in reducing pain and disability in adults with supraspinatus tendonitis? Is one modality of electrotherapy more effective than another?
Is electrotherapy more effective than other physical therapy approaches in reducing pain and disability in adults with supraspinatus tendonitis? Is one modality of electrotherapy more effective than another?