Prescribing and Administration of Emergency Oxygen in Adults Policy
|
|
|
- Letitia Mosley
- 7 years ago
- Views:
Transcription

1 This is an official Northern Trust policy and should not be edited in any way Prescribing and Administration of Emergency Oxygen in Adults Policy Reference Number: NHSCT/12/542 Target audience: Medical, Nursing, Physiotherapy staff and Pharmacy staff Sources of advice in relation to this document: Dr Eoin Murtagh, Consultant Physician Dr Peter Flanagan, Director of Medical & Governance Services Replaces (if appropriate): N/A Type of Document: Trust Wide Approved by: Policy, Standards and Guidelines Committee Date Approved: 31 May 2012 Date Issued by Policy Unit: 6 June 2012 NHSCT Mission Statement To provide for all the quality of services we would expect for our families and ourselves

2 Prescribing and Administration of Emergency Oxygen in Adults Policy May 2012

3 Contents 1. Introduction 2. Aim 3. Prescribing, administering and monitoring oxygen and emergency situations 4. Exclusions 5. Specialist areas 6. Indications 7. Contra indications 8. Cautions 9. Transfer and transportation of patients receiving oxygen therapy 10. Peri-operatively and immediately post operatively 11. Nebulised therapy and oxygen 12. Normal oxygen saturation ranges 13. Administration protocol 14. Humidification 15. Implementation 16. Health and Safety 17. Equality, Human Rights and DDA 18. Sources of advice in relation to this document 19. Alternative formats 20. References 21. Appendices a) Table 1 Critical illnesses requiring high levels of supplemental oxygen b) Table 2 Serious illnesses requiring moderate levels of supplemental oxygen if the patient is hypoxaemic c) Table 3 COPD and other conditions requiring controlled or low-dose oxygen therapy d) Table 4 Conditions for which patients should be monitored closely but oxygen therapy is not required unless the patient is hypoxaemic e) Figure 1 Oxygen prescription for acutely hypoxaemic patients in hospital f) Oxygen prescription within the hospital prescription chart g) Administering acute oxygen therapy h) Equipment used in the delivery of oxygen i) Flow Chart for oxygen administration on general wards in hospital j) Personnel who may administer oxygen k) Bedside observation chart (PEWS) and codes for oxygen delivery l) Monitoring of patients m) PEWS Scoring System and Action Protocol n) Humidification o) Health and safety 1

4 Prescribing and Administration of Emergency Oxygen in Adults Policy Target Audience Medical, Nursing, Physiotherapy staff and Pharmacy staff. 1.0 Introduction The administration of supplemental oxygen is an essential element of appropriate management for a wide range of clinical conditions; however oxygen is a drug and therefore requires prescribing in all but emergency situations. Failure to administer oxygen appropriately can result in serious harm to the patient. The safe implementation of oxygen therapy with appropriate monitoring is an integral component of the Healthcare Professional s role. Guidelines on the emergency use of oxygen in adult patients were originally produced by a working group of the British Thoracic Society and have been adapted by the Medical Gas Committee of the Northern Trust to form this policy. 2.0 Aim The aim of this policy is to ensure that: All patients who require supplementary oxygen therapy receive therapy that is appropriate to their clinical condition and in line with national guidance (BTS Guideline; Thorax, 2008). Oxygen will be prescribed according to a target saturation range. The system of prescribing target saturation aims to achieve a specified outcome, rather than specifying the oxygen delivery method alone. Those who administer oxygen therapy will monitor the patient and keep within the target saturation range. 3.0 Prescribing, administering and monitoring oxygen 3.1 Identifying appropriate target saturations Guidance on identifying appropriate saturations for patients is provided for the medical staff and other prescribers in Appendices a-e (table 1-4 and figure 1 in the guideline). In summary oxygen should be prescribed to achieve a target saturation of 94-98% for most acutely unwell patients or 88-92% for those at risk of hypercapnic respiratory failure. 3.2 Prescribing oxygen on the drug kardex An oxygen section on the drug kardex has been designed to assist prescription and administration. Oxygen should be prescribed in the designated section of the kardex (Appendix f) and the appropriate target saturation should be recorded on the chart (or if target saturations are not indicated the relevant box should be ticked). 3.3 Administering oxygen Once the target saturation has been identified and prescribed, guidance regarding the most appropriate delivery system to reach and maintain the prescribed saturation is provided for those administering oxygen in Appendix (g), (h) and (i). Personnel who may administer oxygen is shown in Appendix (j). 2

5 3.4 Monitoring and recording oxygen The patient's oxygen saturation and oxygen delivery system should be recorded on the bedside observation chart (PEWS Observation & Scoring Chart) alongside other physiological variables as shown in Appendix (k). This appendix also specifies the codes for oxygen delivery devices to be recorded on the observation chart. The flow rate (FR) and device (D) should be recorded at each drug round on the Oxygen Prescription Chart within the Medicine kardex. Patients should thus be monitored as specified in Appendix (l). All patients on oxygen therapy should have regular pulse oximetry measurements. The frequency of oximetry measurements will depend on the condition being treated and the stability of the patient. Critically ill patients should have their oxygen saturations monitored continuously and recorded every few minutes whereas patients with mild breathlessness due to a stable condition will need less frequent monitoring. Oxygen therapy should be increased if the saturation is below the desired range and decreased if the saturation is above the desired range (and eventually discontinued as the patient recovers). See section 13 and Appendix (i) for more details Any sudden fall in oxygen saturation should lead to clinical evaluation of the patient and in most cases, measurement of blood gases. Patients should be monitored accurately for signs of improvement or deterioration. Nurses should also monitor skin colour for peripheral cyanosis and respiratory rate. Oxygen saturations of less than 90%, with or without oxygen, noisy or laboured breathing or respiratory rate of less than 8 or more than 25 should be reported immediately to the medical team, according to the Action Protocol for the PEWS system Appendix (m). 3.5 Emergency situations In the emergency situation an oxygen prescription is not required. Oxygen should be given to the patient immediately without a formal prescription or drug order but documented later in the patient s record. All peri-arrest and critically ill patients should be given 100% oxygen (15 l/m reservoir mask) whilst awaiting immediate medical review. Patients with COPD and other risk factors for hypercapnia who develop critical illness should have the same initial target saturations as other critically ill patients pending the results of urgent blood gas results after which these patients may need controlled oxygen therapy or supported ventilation if there is severe hypoxaemia and/or hypercapnia with respiratory acidosis. All patients who have had a cardiac or respiratory arrest should have 100% Oxygen provided along with basic/advanced life support. A subsequent written record must be made of what oxygen therapy has been given to every patient alongside the recording of all other emergency treatment. Any qualified nurse/ health professional can commence oxygen therapy in an emergency situation. 3

6 4.0 Exclusions Patients admitted to specialist areas with a specialised oxygen prescribing policy (see section 5 of this policy document) Patients receiving oxygen as part of palliative care or patients on the end of life care pathway (in which case, the prescriber should tick the box target saturations not indicated on the drug chart). Patients admitted for Long Term Oxygen Therapy assessment. 5.0 Specialist Areas This policy is for general use within general wards and departments. Where specific clinical guidelines are required for oxygen administration within specialist areas, they must be approved via the appropriate clinical governance forum. They should reflect wherever possible the principles within this policy. Patients transferring from specialist areas must be transferred with a prescription for their oxygen therapy utilising target saturation, if the clinical indication is ongoing. If a patient transfers from an area not utilising the target saturation system, their oxygen should be administered as per the transferring area s prescription until the patient is reviewed and transferred over to the target saturation scheme, which should occur as soon as possible. 6.0 Indications The rationale for oxygen therapy is prevention of cellular hypoxia, caused by hypoxaemia (low PaO2), and thus prevention of potentially irreversible damage to vital organs. Therefore the most common reasons for oxygen therapy to be initiated are: Acute hypoxaemia (for example pneumonia, shock, asthma, heart failure, pulmonary embolus) Ischaemia (for example myocardial infarction, but only if associated with hypoxaemia (abnormally high levels may be harmful to patients with ischaemic heart disease and stroke). Abnormalities in quality or type of haemoglobin (for example acute GI blood loss or carbon monoxide poisoning). Other indications include: Pneumothorax Oxygen may increase the rate of resolution of pneumothorax. Post operative state (general anaesthesia can lead to decrease in functional residual capacity with in the lungs (especially following thoracic or abdominal surgery) resulting in hypoxaemia (Ferguson 1999). There is some evidence to suggest a decreased incidence of post operative wound infections with shortterm oxygen therapy following bowel surgery. 7.0 Contra-indications There are no absolute contraindications to oxygen therapy if indications are judged to be present. The goal of oxygen therapy is to achieve adequate tissue oxygenation using the lowest possible FiO 2. Supplemental O2 should be administered with caution in patients suffering from paraquat poisoning (BNF 2005) and with acid inhalation or previous bleomycin lung injury. 4

7 8.0 Cautions 8.1. Oxygen administration and carbon dioxide retention In patients with chronic carbon dioxide retention, oxygen administration may cause further increases in carbon dioxide and respiratory acidosis. This may occur in patients with COPD, neuromuscular disorders, morbid obesity or musculoskeletal disorders. There are several factors which lead to the rise in CO 2 with oxygen therapy in patients with hypercapnic respiratory failure and details are in the BTS guideline Other precautions/ Hazards/ Complications of oxygen therapy Drying of nasal and pharyngeal mucosa Oxygen toxicity Absorption atelectasis Skin irritation Fire hazard Potentially inadequate flow resulting in lower FiO 2 than intended due to high inspiratory demand or inappropriate oxygen delivery device or equipment faults 9.0 Transfer and transportation of patients receiving oxygen Patients who are transferred from one area to another must have clear documentation of their ongoing oxygen requirements and documentation of their oxygen saturation. If a patient transfers from an area not utilising the target saturation system (see specialist areas above) their oxygen should be administered as per the transferring areas prescription until the patient is reviewed and transferred over to the target saturation scheme, which should occur as soon as possible. Patients requiring oxygen therapy whilst being transferred from one area to another should be accompanied by a trained member of the nursing staff wherever possible. If this does not occur, clear instructions must be provided for personnel involved in the transfer of the patient, which must include delivery device and flow rate Peri-operative and immediately post operatively The usual procedure for prescribing oxygen therapy in these areas should be adhered to, utilising the target saturation. If a patient is transferred back to the ward on oxygen therapy and is not on the target saturation system, the need for ongoing oxygen therapy should be reviewed as soon as possible. If oxygen therapy is to be continued, it should be prescribed using the target saturation scheme unless there is an alternative time-limited instruction which is part of the Trust s Post- Operative care policy for selected patients Nebulised therapy and oxygen When nebulised therapy is administered to patients at risk of hypercapnic respiratory failure (see section 8.1), it should be driven by compressed air. If necessary, supplementary oxygen should be given concurrently by nasal prongs at 1-4 litres per minute to maintain an oxygen saturation of 88-92% or other specified target range. All patients requiring 35% or greater oxygen therapy should have their nebulised therapy by oxygen at a flow rate of >6 litres/minute. 5

8 12.0 Normal Oxygen saturations In adults less than 70 years of age at rest at sea level 96% - 98% when awake. Aged 70 and above at rest at sea level greater than 94% when awake. Patients of all ages may have transient dips of saturation to 84% during sleep Summary Oxygen Administration protocol (and weaning protocol) ACTION All patients requiring oxygen therapy will have a prescription for oxygen therapy recorded on the patients drug prescription chart. N.B exceptions- see emergency situations The prescription will incorporate a target saturation that will be identified by the clinician prescribing the oxygen in accordance with the Trust's oxygen guideline The prescription will incorporate an initial starting dose (i.e. delivery device and flow rate) The drug chart should be signed at every drug round Once oxygen is in situ the nurse will monitor observations in line with trust policy. All patients should have their oxygen saturation observed for at least five minutes after starting oxygen therapy. If a patient is receiving intermittent therapy they may be monitored at least 8 hourly. The oxygen delivery device and oxygen flow rate should be recorded together with the oxygen saturation on the bedside observation chart. Oxygen saturations must always be interpreted alongside the patients clinical status incorporating the early warning score. If the patient falls outside of the target saturation range, the oxygen therapy will be adjusted accordingly The saturation should be monitored continuously for at least 5 minutes after any increase or decrease in oxygen dose to ensure that the patient acheives the desired saturation range. RATIONALE Oxygen should be regarded as a drug and should be prescribed. BTS National guidelines (2008). British National Formulary 61 (2011). Certain groups of patients require different target ranges for their oxygen saturation, see Tables 1-4. Certain groups of patients are at risk of hyperoxaemia, particularly patients with COPD. To provide the nurses with guidance for the appropriate starting point for the oxygen delivery system and flow rate To ensure that the patient is receiving oxygen if prescribed and to consider weaning and discontinuation To identify if oxygen therapy is maintaining the target saturation or if an increase or decrease in oxygen therapy is required To provide an accurate record and allow trends in oxygen therapy and saturation levels to be identified. To identify early signs of clinical deterioration, e.g. elevated respiratory rate To maintain the saturation in the desired range. 6

9 Saturation higher than target specified or >98% for an extended period of time. Step down oxygen therapy as per guidance for delivery Consider discontinuation of oxygen therapy Saturation lower than target specified Check all elements of oxygen delivery system for faults or errors. Step up oxygen therapy as per protocols in appendix (i). Any sudden fall in oxygen saturation should lead to clinical evaluation and in most cases measurement of blood gases Monitor Early Warning Score (PEWS) and respiratory rate for further clinical signs of deterioration Saturation within target specified Continue with oxygen therapy, and monitor patient to identify appropriate time for stepping down therapy, once clinical condition allows A change in delivery device (without an increase in O2 therapy) does not require review by the medical team. Oxygen delivery methods The Trusts recommended delivery devices will be utilised to ensure a standardised approach to oxygen delivery, see Appendix (h) The patient will require weaning down from current oxygen delivery system. See Appendix (i) The patients clinical condition may have improved negating the need for supplementary oxygen In most instances a fall in oxygen saturation is due to deterioration of the patient however equipment faults should be checked for. To assess the patients response to oxygen increase, and ensure that PaCO2 has not risen to an unacceptable level, or Ph dropped to an unacceptable level and to screen for the cause of deteriorating oxygen level (e.g. pneumonia, heart failure etc) Patient safety (The change may be made in stable patients due to patient preference or comfort). Previous audits have demonstrated wide variations in delivery devices across clinical areas, potentially increasing the risk of adverse incidents 14. Humidification Humidification may be required for some patient groups, especially neck-breathing patients or those who have difficulty in clearing airway secretions or mucus. See Appendix (n). 15. Implementation All nurses, midwives, nursing assistants and other healthcare professionals involved in prescribing or administrating oxygen should be taught on the oxygen policy. Teaching aides are available on 7
 and respiratory rate for further clinical signs")
10 All doctors should be taught about the oxygen policy. Teaching aids are available on the BTS website. Audits should be performed in all clinical areas. Audit proformas are available on the BTS website. The Trust will participate in the national audits organised by the BTS Health and Safety issues are covered in Appendix (p) Equality, Human Rights and DDA The policy is purely clinical/technical in nature and will have no bearing in terms of its likely impact on equality of opportunity or good relations for people within the equality and good relations categories Sources of advice in relation to this document Policy author: Dr Eoin Murtagh, Consultant Physician, on behalf of Trust Medical Gas Committee. Fiona Gallagher, Ward Pharmacist A4, Antrim Hospital Pat Scullion, Respiratory Nurse Specialist, Antrim Hospital Jenny Wilson, Respiratory Nurse Specialist, Antrim Hospital Dr Peter Flanagan, Director of Medical Services 19.0 Alternative formats This document can be made available on request on disc, larger font, Braille, audio-cassette and in other minority languages to meet the needs of those who are not fluent in English References O Driscoll B R, Howard L S, Davison A G. BTS guideline for emergency oxygen use in adult patients. Thorax 2008; 63: Supplement VI. Summary guideline for prescribing oxygen emergency oxygen in hospital. Available on BTS website: Summary of prescription, administration and discontinuation of oxygen therapy. Available on BTS website: 8

11 APPENDICES Appendix (a) 9

12 Appendix (b) 10

13 Appendix (c) 11

14 Appendix (d) 12

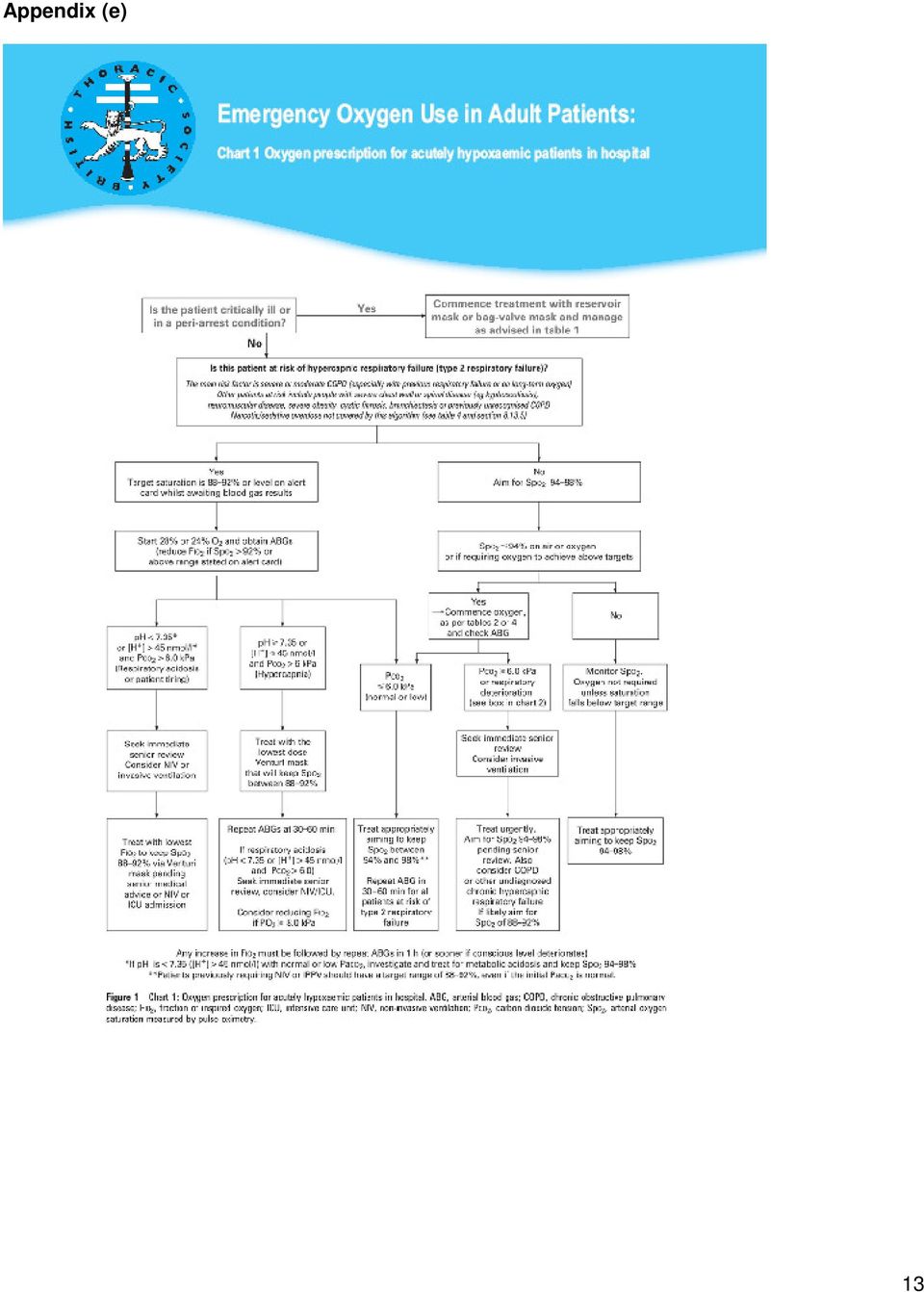
15 Appendix (e) 13
16 Appendix (f) Oxygen prescription chart for use in adult patients (16 years and over) The doctor must prescribe the initial flow rate and device. The method and rate of oxygen delivery should be altered by nurses or other healthcare professionals in order to achieve the prescribed saturation range. NB: The initial prescription does NOT need to be rewritten if the device or flow rate is changed by the nurse or physiotherapist. Remember, rapid changes in clinical condition require medical review. WRITE IN CAPITAL LETTERS or use addressograph Surname: First names: Hospital No: DOB: Doctor: For most chronic conditions, oxygen should be prescribed to achieve a target saturation of 94-98% (or 88-92% for those at risk of hypercapnic respiratory failure i.e. C0 2 retainers). Is the patient a known CO 2 retainer? Yes No Nursing Staff: Sign this chart on each drug round. Record flow rate and device (FR/D) at each drug round using the codes below* Year: Day & month: Circle times or enter variable times and circle Continuous oxygen therapy When required (PRN) oxygen therapy FR/D Target oxygen saturation 88-92% 94-98% Other saturation range Starting device and flow rate: FR/D FR/D Tick here if saturation NOT indicated and state reason (e.g. end of life care) Start date Stop date Signature FR/D FR/D Signature Print name Pharmacy FR/D Bleep Year: Day & month: Circle times or enter variable times and circle Continuous oxygen therapy When required (PRN) oxygen therapy FR/D Target oxygen saturation 88-92% 94-98% Other saturation range Starting device and flow rate: FR/D FR/D Tick here if saturation NOT indicated and state reason (e.g. end of life care) Start date Stop date Signature FR/D FR/D Signature Print name Pharmacy Bleep FR/D 14

17 * Codes for recording oxygen flow rate & delivery device on PEWS Observation Chart: A Air (not requiring oxygen or weaning or on PRN oxygen) RM Reservoir mask N Nasal cannula TM Tracheostomy mask SM Simple mask CP Patient on CPAP system V24 Venturi 24% (change figure as appropriate for % in use) NIV Patient on NIV system H28 Humidified oxygen at 28% (change figure as appropriate or % in use) OTH Other device (specify). Flow Rate (FRI) Always record flow rate in L/min (e.g. 4 = 4 L/min or 2 = 2 L/min) 15
 OTH Other device (specify). Flow Rate (FRI) Always record flow rate in L/min (e.g.")
18 Appendix (g) ADMINISTERING ACUTE OXYGEN THERAPY ACTION RATIONALE 1. Ensure patency of airway To promote effective oxygenation 2. The type of delivery system used will To provide accurate oxygen delivery depend on the needs and comfort of It to the patient. Most stable patients prefer the patient. It is the nurses role to assess nasal cannulae to masks. the patient and use the prescribed system. 3. Ensure oxygen is prescribed on To ensure a complete record is prescription chart. maintained and expedite patient In some situations a protocol may be in treatment. place to allow designated nurses to The exception to this action would be administer oxygen. during an emergency situation where In these cases the doctor must review the resuscitation guideline should be the patients condition within the stated followed. time and prescribe oxygen accordingly. 4. Ensure that the oxygen dose is clearly In accordance with the administration of indicated. If nasal cannula medicines policy. or reservoir masks are being used check that the flow rate is clearly indicated. 5. Inform patient and or relative/ carer of Oxygen supports combustion therefore the combustibility of oxygen there is always a danger of fire when oxygen is being used. 6. Show and explain the oxygen delivery To obtain consent and cooperation. system to the patient. Give the patient the information sheet about oxygen. 7. Assemble the oxygen delivery system To ensure oxygen is given as prescribed. carefully as shown in Appendix (h). 8. Attach oxygen delivery system to To ensure oxygen supply is ready oxygen source. 9. Attach oxygen delivery system to patient For oxygen to be administered to according to manufacturers instructions. patient. 10. Turn on oxygen flow in accordance To administer correct % of oxygen. with prescription and manufacturers instruction. 11. Ensure patient has either a drink or To prevent drying or the oral mucosa. a mouthwash within reach. 12. Clean oxygen mask as required with To minimise risk of infection general purpose detergent and dry thoroughly needed. Discard systems (Single patient device) after use. 16

; A) Nasal cannula DEVICE DESCRIPTION PURPOSE Nasal Cannulae Nasal cannulae consist of pair of tubes about 2cm long, each")

19 Appendix (h) EQUIPMENT USED IN THE DELIVERY OF OXYGEN (Choose the appropriate delivery device) 1. Oxygen source (piped or cylinder) 2. Flow meter 3. Saturation monitor 4. Oxygen Delivery system - (see appendix j for advice on use of each device); A) Nasal cannula DEVICE DESCRIPTION PURPOSE Nasal Cannulae Nasal cannulae consist of pair of tubes about 2cm long, each projecting into the nostril and stemming from a tube which passes over the ears and which is thus selfretaining. Uncontrolled oxygen therapy Cannulae are preferred to masks by most patients. They have the advantage of not interfering with feeding and are not as inconvenient as masks during coughing and sneezing. It is not advisable to assume what percent oxygen (FI02) the patient is receiving according to the Litres delivered but this is not important if the patient is in the correct target range. ACTION RATIONALE 1. (When using nasal cannula). Position the tips of the cannula in the patient s nose so that the tips do not extend more than 1.5cm into the nose. Overlong tubing is uncomfortable, which may make the patient reject the procedure. Sore nasal mucosa can result from pressure or friction of tubing that is too long. 2. Place tubing over the ears and under the chin as shown above. Educate patient re prevention of pressure areas on the back of the ear. 3. Adjust flow rate, usually 2-4 l/min but may vary from 1-6 l/min in some circumstances. To allow optimum comfort for the patient. To prevent pressure sores. Set the flow rate to achieve the desired target oxygen saturation. 17

20 B) Fixed performance mask (Venturi mask and valve) DEVICE DESCRIPTION PURPOSE Venturi mask ACTION A mask incorporating a device to enable a fixed concentration of oxygen to be delivered independent of patient factors or fit to the face or flow rate. Oxygen is forced out through a small hole causing a Venturi effect which enables air to mix with oxygen. Controlled oxygen therapy RATIONALE This is a high performance oxygen mask designed to deliver a specified oxygen concentration regardless of breathing rate or tidal volume. Venturi devices come in different colours for % Blue = 24% White = 28% Yellow = 35% Red = 40% Green = 60% 1. (When using Venturi mask) Connect the mask to the appropriate Venturi barrel attached firmly into the mask inlet. To ensure that patient receives the correct concentration of oxygen 2.Fasten oxygen tubing securely. Correctly secured tubing is comfortable and prevents displacement of mask/cannulae. 3.Assess the patient s condition and functioning of equipment at regular intervals according to care plan. 4. Adjust flow rate. The minimum flow rate is indicated on the mask or packet. The flow should be doubled if the patient has a respiratory rate above 30 per minute. To ensure patient s safety and that oxygen is being administered as prescribed. Higher flows are required for patients with rapid respiration and high inspiratory flow rates. This does not affect the concentration of oxygen but allows the gas flow rate to match the patient s breathing pattern. 18

21 C) Simple face mask (variable flow) DEVICE DESCRIPTION Mask has a soft plastic face piece, vent holes are provided to allow air to escape. Maximum 50%-60% at 15ltrs/minute flow. PURPOSE This is a variable performance device. The oxygen concentration delivered will be influenced by: a. the oxygen flow rate( litres per minute) used, leakage between the mask and face; Simple face mask Variable Percentage (Delivers unpredictable concentrations that vary with flow rate) Nasal cannulae should be used for most patients who require medium dose oxygen but a simple face mask may be used due to patient preference or if the nose is blocked ACTION Uncontrolled Oxygen therapy b. the patient s tidal volume and breathing rate. NOT to be used for CO 2 retaining patients. RATIONALE (If using simple face mask) Gently place mask over the patient s face, position the strap behind the head or the loops over the ears then carefully pull both ends through the front of the mask until secure. Ensure a comfortable fit and delivery of prescribed oxygen is maintained. Check that strap is not across ears and if necessary insert padding between the strap and head. Adjust the oxygen flow rate. Must never be below 5L/min To prevent irritation. Flows below 5L/m do not give enough oxygen and may cause increased resistance to breathing and may also cause CO2 rebreathing due to the small mask size. 19
22 D) Reservoir mask (non re-breathe mask) DEVICE DESCRIPTION PURPOSE Reservoir Mask (Non-rebreathe Mask) Mask has a soft plastic face piece with flap-valve exhalation ports which may be removed for emergency air-intake. There is also a one-way valve between the face mask and reservoir bag. In non re-breathing systems the oxygen may be stored in the reservoir bag during exhalation by means of a one-way valve. High concentrations of oxygen 80-90% can be achieved at relatively low flow rates. Uncontrolled oxygen therapy NOT to be used for C02 retaining patients except in lifethreatening emergencies such as cardiac arrest or major trauma. ACTION 1. (Non Rebreathe Reservoir Mask) Ensure the reservoir bag is inflated before placing mask on patient, this can be maintained by using litres of oxygen per min. 2. Adjust the oxygen flow to the prescribed rate. RATIONALE To ensure the optimal flow of oxygen to the patient. Inadequate flow rates may result in administration of inadequate oxygen concentration to the patient. In disposable reservoir, oxygen flows directly into the mask during inspiration and into the reservoir bag during exhalation. All exhaled air is vented through a port in the mask and a one-way valve between the bag and mask, which prevents re-breathing. E) Tracheostomy mask for patients with tracheostomy or laryngectomy DEVICE DESCRIPTION Mask designed for neck breathing patients. Fits comfortably over tracheostomy or tracheotomy. Exhalation port on front of mask. PURPOSE This is a variable performance device for patients with tracheostomy or tracheotomy. The oxygen concentration delivered will be influenced by: a. the oxygen flow rate( litres per minute) used. b. the patient s tidal volume and breathing rate. Tracheostomy mask Variable Percentage (Delivers unpredictable concentrations that vary with flow rate) Uncontrolled Oxygen therapy Use cautiously at low flow rates in CO2 retaining patients as there may be no alternative. 20
23 ACTION RATIONALE Gently place mask over the patient s airway, position the strap behind the head then carefully pull both ends through the front of the mask until secure. Ensure a comfortable fit and delivery of prescribed oxygen is maintained. Adjust the oxygen flow rate to achieve the desired target saturation range. Start at 4 l/min and adjust the flow up or down as necessary to achieve the desired oxygen saturation range. To ensure that the correct amount of oxygen is given to keep the patient in the target range. F) Oxygen Flow Meter DEVICE DESCRIPTION Device to allow the patient to receive an accurate flow of oxygen, usually between 2 and 15 litres per minute. May be wall-mounted or on a cylinder. Take special care if your Trust uses a twin oxygen outlets or if there are air outlets which may be mistaken for oxygen outlets. PURPOSE To ensure that the patient receives the correct amount of oxygen Correct Setting for 2 l/min Oxygen flow meter Delivers oxygen to the patient. ACTION RATIONALE Attach the oxygen tubing to the nozzle on the flow meter. To ensure that the patient receives the correct amount of oxygen. Turn the finger-valve to obtain the desired flow rate. The CENTRE of the ball shows the correct flow rate. The diagrams shows the correct setting to deliver 2 l/min. 21
24 Appendix (i) Flow chart for oxygen administration on general wards in hospitals 22
25 Appendix (j) PERSONNEL WHO MAY ADMINISTER OXYGEN Any registered nurse/midwife, doctor, RSCN, RN or physiotherapist. In accordance with policy for administration of medicines. 23
26 Appendix (k) 24
27 Appendix (l) MONITORING OF PATIENTS (See PEWS Observation and Scoring chart, appendix k) 1. Observe the following; In order to accurately monitor the patient for signs of improvement or deterioration. a. Monitor arterial oxygen saturation levels according to Trust 0xygen policy. b. Visual observations of skin colour for central cyanosis (blue lips). c. Respiratory rate. d. Any sign of respiratory distress should be reported immediately. 2. If the arterial oxygen saturation is above or below the target saturation the observer (often a Health Care Assistant) must inform the personnel who are qualified to administer oxygen (usually a Nurse see appendix g). 3. Check the patients mouth and nose and To identify signs of infection and behind the ears. pressure sores as soon as possible. 4. Record all observations on appropriate To ensure adequate record keeping. Chart 4 hourly if on continuous oxygen 8 hourly if on intermittent oxygen 25
28 Appendix (m) 26
29 Appendix (n) HUMIDIFICATION This should only be used if specifically requested by the doctor or physiotherapist in the following circumstances. 1. If the flow rate exceeds 4 litres per minute for several days 2. Tracheotomy or tracheostomy patients ( neck-breathing patients) 3. Cystic Fibrosis patients 4. Bronchiectasis patients 5. Patients with a chest infection retaining secretions Can be given by warm or cold humidifier systems (warm humidifier systems are mainly used in critical care areas) Appendix (o) HEALTH AND SAFETY 1. Inform patients and carers about the combustibility of oxygen Oxygen supports combustion, there.is always a danger of fire when oxygen is being used. 2. Oxygen should be stored in an area designated as no smoking. 3. Electrical appliances should be kept at least five feet away from the source of oxygen. Oxygen can be potentially dangerous when in contact with sources of ignition and flammable material. 4. Avoid grease or oil coming into contact with apparatus. 5. Store unused cylinders in a dry well ventilated place. 27
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Prescription and Administration of Emergency Oxygen in Adults in Hospital. Charlie Turner, Senior Nurse Patient Safety
 Policy: Prescription and Administration of Emergency Oxygen in Adults in Hospital Executive or Associate Director lead Policy author/ lead Feedback on implementation to Karen Tomlinson, Executive/Chief
Policy: Prescription and Administration of Emergency Oxygen in Adults in Hospital Executive or Associate Director lead Policy author/ lead Feedback on implementation to Karen Tomlinson, Executive/Chief
GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY
 SOUTH DURHAM HEALTH CARE NHS TRUST GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY AIM To supplement oxygen intake using the appropriate equipment in order to correct hypoxia and relieve breathlessness.
SOUTH DURHAM HEALTH CARE NHS TRUST GUIDELINES FOR THE MANAGEMENT OF OXYGEN THERAPY AIM To supplement oxygen intake using the appropriate equipment in order to correct hypoxia and relieve breathlessness.
Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow
 Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow Author: Dr Louise Thomson, Paediatric Respiratory Consultant Lynda Peacock, Complex Respiratory
Guideline for the prescription and administration of oxygen in children. Royal Hospital for Sick Children, Glasgow Author: Dr Louise Thomson, Paediatric Respiratory Consultant Lynda Peacock, Complex Respiratory
Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities
 Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities August 2013 Page 1 of 32 Policy Title Policy for the Prescription and Administration of Oxygen to Adults in Inpatient
Policy for the Prescription and Administration of Oxygen to Adults in Inpatient Facilities August 2013 Page 1 of 32 Policy Title Policy for the Prescription and Administration of Oxygen to Adults in Inpatient
Respiratory failure and Oxygen Therapy
 Respiratory failure and Oxygen Therapy A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention
Respiratory failure and Oxygen Therapy A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD
 Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Peninsula Community Health. Policy for the Prescription, Administration. monitoring of Oxygen and Emergency Oxygen in Adults
 Peninsula Community Health Policy for the Prescription, Administration and monitoring of Oxygen and Emergency Oxygen in Adults Title: Policy for the Prescription, Administration and monitoring of Emergency
Peninsula Community Health Policy for the Prescription, Administration and monitoring of Oxygen and Emergency Oxygen in Adults Title: Policy for the Prescription, Administration and monitoring of Emergency
Applicant Information Sheet for MASS 45 Adult Oxygen: Initial Application and 4 Month Review
 , Queensland Health Applicant Information Sheet for Applicants should retain this section for their records Eligibility Administrative eligibility is dependent upon the applicant being a permanent Queensland
, Queensland Health Applicant Information Sheet for Applicants should retain this section for their records Eligibility Administrative eligibility is dependent upon the applicant being a permanent Queensland
GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS
 GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS Key Points 1. No patient should be denied oxygen therapy in an emergency. Patients in cardiac and/or respiratory arrest should be managed
GUIDELINES FOR ACUTE OXYGEN THERAPY FOR WESTERN AUSTRALIAN HOSPITALS Key Points 1. No patient should be denied oxygen therapy in an emergency. Patients in cardiac and/or respiratory arrest should be managed
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Oxygen Therapy. A guide for the patient. Please bring to any outpatient appointments. Patients name. Exceptional healthcare, personally delivered
 A guide for the patient Please bring to any outpatient appointments Patients name Exceptional healthcare, personally delivered Introduction This leaflet has been written for patients starting, or who have
A guide for the patient Please bring to any outpatient appointments Patients name Exceptional healthcare, personally delivered Introduction This leaflet has been written for patients starting, or who have
ADMINISTERING EMERGENCY OXYGEN
 FACT SHEET ADMINISTERING EMERGENCY OXYGEN Emergency oxygen can be given for many breathing and cardiac emergencies. It can help improve hypoxia (insufficient oxygen reaching the cells) and reduce pain
FACT SHEET ADMINISTERING EMERGENCY OXYGEN Emergency oxygen can be given for many breathing and cardiac emergencies. It can help improve hypoxia (insufficient oxygen reaching the cells) and reduce pain
Oxygenation and Oxygen Therapy Michael Billow, D.O.
 Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
POLICIES & PROCEDURES. ID Number: 1115
 POLICIES & PROCEDURES Title: OXYGEN ADMINISTRATION ID Number: 1115 Authorization [X] SHR Nursing Practice Committee Source: Nursing, Respiratory Therapy, Physiotherapy Date Revised: March 2015 Date of
POLICIES & PROCEDURES Title: OXYGEN ADMINISTRATION ID Number: 1115 Authorization [X] SHR Nursing Practice Committee Source: Nursing, Respiratory Therapy, Physiotherapy Date Revised: March 2015 Date of
How To Treat A Patient With A Lung Condition
 NHS FORTH VALLEY BIPAP Guideline Date of First Issue 27 / 10 / 2010 Approved 27 / 10 / 2010 Current Issue Date 27 / 10 / 2010 Review Date 27 / 10 / 2012 Version Version 1.00 EQIA Yes 27 / 10 / 2010 Author
NHS FORTH VALLEY BIPAP Guideline Date of First Issue 27 / 10 / 2010 Approved 27 / 10 / 2010 Current Issue Date 27 / 10 / 2010 Review Date 27 / 10 / 2012 Version Version 1.00 EQIA Yes 27 / 10 / 2010 Author
PROCEDURE FOR USING A NASAL CANNULA
 FOR USING A NASAL CANNULA A nasal cannula is used to deliver a low to moderate concentration of oxygen. It can be used as long as nasal passages are open. A deviated septum, swelling of the nasal passages,
FOR USING A NASAL CANNULA A nasal cannula is used to deliver a low to moderate concentration of oxygen. It can be used as long as nasal passages are open. A deviated septum, swelling of the nasal passages,
PROCEDURE FOR USING A NASAL CANNULA
 PROCEDURE FOR USING A NASAL CANNULA A nasal cannula is used to deliver a low to moderate concentration of oxygen. It can be used as long as nasal passages are open. A deviated septum, swelling of the nasal
PROCEDURE FOR USING A NASAL CANNULA A nasal cannula is used to deliver a low to moderate concentration of oxygen. It can be used as long as nasal passages are open. A deviated septum, swelling of the nasal
Oxygen for Symptom Relief (Palliative Oxygen)
") Oxygen for Symptom Relief (Palliative Oxygen) Exceptional healthcare, personally delivered This leaflet has been written for patients starting, or who have just started, oxygen therapy and answers any
Oxygen for Symptom Relief (Palliative Oxygen) Exceptional healthcare, personally delivered This leaflet has been written for patients starting, or who have just started, oxygen therapy and answers any
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
MECHINICAL VENTILATION S. Kache, MD
 MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care
 Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Management of exacerbations in chronic obstructive pulmonary disease in Primary Care Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with significant morbidity and mortality.
Keeping your lungs healthy
 Keeping your lungs healthy A guide for you after spinal cord injury and other neurological conditions Regional Rehabilitation Program This booklet has been written by the health care providers who provide
Keeping your lungs healthy A guide for you after spinal cord injury and other neurological conditions Regional Rehabilitation Program This booklet has been written by the health care providers who provide
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log
 and Emergency Medical Responder (EMR) Progress Log") First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
GRADE 11F: Biology 3. UNIT 11FB.3 9 hours. Human gas exchange system and health. Resources. About this unit. Previous learning.
 GRADE 11F: Biology 3 Human gas exchange system and health UNIT 11FB.3 9 hours About this unit This unit is the third of six units on biology for Grade 11 foundation. The unit is designed to guide your
GRADE 11F: Biology 3 Human gas exchange system and health UNIT 11FB.3 9 hours About this unit This unit is the third of six units on biology for Grade 11 foundation. The unit is designed to guide your
SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE POSITIVE PRESSURE (NPPV) VENTILATION (CPAP/BIPAP) Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Director, Respiratory
PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE POSITIVE PRESSURE (NPPV) VENTILATION (CPAP/BIPAP) Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Director, Respiratory
How To Get On A Jet Plane
 Nature of disability Hospital Details TEL : +91 22 6711 6618 / 09 l FAX : +91 22 26156290 +91 11 49637953 +91 44 22568009 +91 33 25111359 Information Sheet for Guest Requiring Medical Clearance (to be
Nature of disability Hospital Details TEL : +91 22 6711 6618 / 09 l FAX : +91 22 26156290 +91 11 49637953 +91 44 22568009 +91 33 25111359 Information Sheet for Guest Requiring Medical Clearance (to be
Oxygen Policy and Procedure
 Approved by: Date of approval: Oxygen Policy and Originator: Medical Director AIM AND SCOPE OF PROCEDURE Oxygen therapy requires the use of oxygen cylinders, oxygen concentrators, or oxygen piped from
Approved by: Date of approval: Oxygen Policy and Originator: Medical Director AIM AND SCOPE OF PROCEDURE Oxygen therapy requires the use of oxygen cylinders, oxygen concentrators, or oxygen piped from
Understanding Anesthetic Delivery Systems Dean Knoll, CVT, VTS (Anes.) Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003
 Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003") Understanding Anesthetic Delivery Systems Dean Knoll, CVT, VTS (Anes.) Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003 Knowing the functions of the anesthetic delivery system
Understanding Anesthetic Delivery Systems Dean Knoll, CVT, VTS (Anes.) Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003 Knowing the functions of the anesthetic delivery system
NURSING SERVICES DEPARTMENT
 NURSING SERVICES DEPARTMENT TITLE: Mechanical Ventilation PATIENT CARE PLAN DIAGNOSIS: DISCHARGE CRITERIA: 1 The patient will: Maintain adequate mechanics of PERTINENT INFORMATION:. ventilation as demonstrated
NURSING SERVICES DEPARTMENT TITLE: Mechanical Ventilation PATIENT CARE PLAN DIAGNOSIS: DISCHARGE CRITERIA: 1 The patient will: Maintain adequate mechanics of PERTINENT INFORMATION:. ventilation as demonstrated
Emergency Medical Services Advanced Level Competency Checklist
 Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
Community health care services Alternatives to acute admission & Facilitated discharge options. Directory
 Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Medical Section. Email : acmedical@aircanada.ca. Fax : 1 888 334-7717 (toll-free) or 514 828-0027
 or 514 828-0027") Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 828-0027 Telephone : 1 800 667-4732
Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 828-0027 Telephone : 1 800 667-4732
Medicines reconciliation on admission and discharge from hospital policy April 2013. WHSCT medicines reconciliation policy 1
 Medicines reconciliation on admission and discharge from hospital policy April 2013 WHSCT medicines reconciliation policy 1 Policy Title Policy Reference Number Medicines reconciliation on admission and
Medicines reconciliation on admission and discharge from hospital policy April 2013 WHSCT medicines reconciliation policy 1 Policy Title Policy Reference Number Medicines reconciliation on admission and
Suturing Policy for Nurses in Emergency Departments
 This is an official Northern Trust policy and should not be edited in any way Suturing Policy for Nurses in Emergency Departments Reference Number: NHSCT/12/545 Target audience: Registered Nurses Sources
This is an official Northern Trust policy and should not be edited in any way Suturing Policy for Nurses in Emergency Departments Reference Number: NHSCT/12/545 Target audience: Registered Nurses Sources
Children s Nursing Hearing Aid
 This is an official Northern Trust policy and should not be edited in any way Reference Number: Children s Nursing Hearing Aid NHSCT/10/369 Target audience: Registered nursing staff within the paediatric
This is an official Northern Trust policy and should not be edited in any way Reference Number: Children s Nursing Hearing Aid NHSCT/10/369 Target audience: Registered nursing staff within the paediatric
Adult Home Oxygen Therapy. Purpose To provide guidance on the requirements for and procedures relating to domiciliary oxygen therapy.
 Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Ventilation Perfusion Relationships
 Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
TRACHEOSTOMY TUBE PARTS
 Page1 NR 33 TRACHEOSTOMY CARE AND SUCTIONING Review ATI Basic skills videos: Tracheostomy care and Endotracheal suction using a closed suction set. TRACHEOSTOMY TUBE PARTS Match the numbers on the diagram
Page1 NR 33 TRACHEOSTOMY CARE AND SUCTIONING Review ATI Basic skills videos: Tracheostomy care and Endotracheal suction using a closed suction set. TRACHEOSTOMY TUBE PARTS Match the numbers on the diagram
Critical Care Therapy and Respiratory Care Section
 Category: Section: Title: Critical Care Therapy and Respiratory Care Section Policy #: 03 Revised: 5/02 1.0 DESCRIPTION Clinical Ventilator Management Invasive and Noninvasive Positive Pressure Ventilation
Category: Section: Title: Critical Care Therapy and Respiratory Care Section Policy #: 03 Revised: 5/02 1.0 DESCRIPTION Clinical Ventilator Management Invasive and Noninvasive Positive Pressure Ventilation
VA SAN DIEGO HEALTHCARE SYSTEM MEMORANDUM 118-28 SAN DIEGO, CA
 GUIDELINES FOR PATIENT-CONTROLLED ANALGESIA (PCA) AND PATIENT- CONTROLLED EPIDURAL ANALGESIA (PCEA) FOR ACUTE PAIN MANAGEMENT 1. PURPOSE: To assure the safe and effective use of patient controlled analgesia
GUIDELINES FOR PATIENT-CONTROLLED ANALGESIA (PCA) AND PATIENT- CONTROLLED EPIDURAL ANALGESIA (PCEA) FOR ACUTE PAIN MANAGEMENT 1. PURPOSE: To assure the safe and effective use of patient controlled analgesia
Seven steps to patient safety The full reference guide. Second print August 2004
 Seven steps to patient safety The full reference guide Second print August 2004 National Patient Safety Agency Seven steps to patient safety 113 Appendix Four F Examples of events according to severity
Seven steps to patient safety The full reference guide Second print August 2004 National Patient Safety Agency Seven steps to patient safety 113 Appendix Four F Examples of events according to severity
Mirage FX NASAL MASK. User Guide
 Mirage FX NASAL MASK User Guide Mirage FX NASAL MASK Fitting// 1 2 3 4 5 6 Mirage FX i Removal// 1 2 Disassembly// 1 2 3 ii Reassembly// 1 2 3 4 iii Mirage FX A 2 3 1 4 7 6 5 B iv Mask components// Item/
Mirage FX NASAL MASK User Guide Mirage FX NASAL MASK Fitting// 1 2 3 4 5 6 Mirage FX i Removal// 1 2 Disassembly// 1 2 3 ii Reassembly// 1 2 3 4 iii Mirage FX A 2 3 1 4 7 6 5 B iv Mask components// Item/
Intro Who should read this document 2 Key Messages 2 Background 2
 Classification: Policy Lead Author: Nathan Griffiths, Consultant Nurse Paediatric Emergency Medicine Additional author(s): N/A Authors Division: Salford Healthcare Unique ID: DDCPan04(14) Issue number:
Classification: Policy Lead Author: Nathan Griffiths, Consultant Nurse Paediatric Emergency Medicine Additional author(s): N/A Authors Division: Salford Healthcare Unique ID: DDCPan04(14) Issue number:
National Hospital for Neurology and Neurosurgery. Continuous positive airway pressure (CPAP) Sleep Respiratory Unit
 Sleep Respiratory Unit") National Hospital for Neurology and Neurosurgery Continuous positive airway pressure (CPAP) Sleep Respiratory Unit If you would like this document in another language or format or if you require the services
National Hospital for Neurology and Neurosurgery Continuous positive airway pressure (CPAP) Sleep Respiratory Unit If you would like this document in another language or format or if you require the services
Care Pathway for the Administration of Intravenous Iron Sucrose (Venofer )
") Departments of Haematology, Nephrology and Pharmacy Care Pathway for the Administration of Intravenous Iron Sucrose (Venofer ) [Care Pathway Review Date] Guidance for use This Care Pathway is intended
Departments of Haematology, Nephrology and Pharmacy Care Pathway for the Administration of Intravenous Iron Sucrose (Venofer ) [Care Pathway Review Date] Guidance for use This Care Pathway is intended
Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when
 Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Common Ventilator Management Issues
 Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Artificial Ventilation Theory into practice
 Artificial Ventilation Theory into practice Keith Simpson BVSc MRCVS MIET(Electronics) www.vetronic.co.uk ksimpson@vetronic.co.uk June 13 th 2014 Today we will discuss the administration of IPPV to anaesthetised
Artificial Ventilation Theory into practice Keith Simpson BVSc MRCVS MIET(Electronics) www.vetronic.co.uk ksimpson@vetronic.co.uk June 13 th 2014 Today we will discuss the administration of IPPV to anaesthetised
Oxygen AND COPD. This fact sheet talks about home oxygen, prescribed as a medicine for some people with COPD.
 Oxygen AND COPD This fact sheet talks about home oxygen, prescribed as a medicine for some people with COPD. For more information on COPD, phone 1-866-717-COPD (2673) or visit us online at www.lung.ca/copd
Oxygen AND COPD This fact sheet talks about home oxygen, prescribed as a medicine for some people with COPD. For more information on COPD, phone 1-866-717-COPD (2673) or visit us online at www.lung.ca/copd
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Guideline for the use of Non-Invasive Ventilation (NIV) TCP 180
 TCP 180") Guideline for the use of Non-Invasive Ventilation (NIV) CROSS REFERENCE Progress/date of approval This Strategy/ Policy should be read in conjunction with: Mental Capacity Act Policy -TCP 199 June 2009
Guideline for the use of Non-Invasive Ventilation (NIV) CROSS REFERENCE Progress/date of approval This Strategy/ Policy should be read in conjunction with: Mental Capacity Act Policy -TCP 199 June 2009
Oxford Centre for Respiratory Medicine Bronchial-Artery Embolisation Information for patients
 Oxford Centre for Respiratory Medicine Bronchial-Artery Embolisation Information for patients This leaflet tells you about the bronchial-artery embolisation procedure. It explains what is involved and
Oxford Centre for Respiratory Medicine Bronchial-Artery Embolisation Information for patients This leaflet tells you about the bronchial-artery embolisation procedure. It explains what is involved and
HLTEN609B Practise in the respiratory nursing environment
 HLTEN609B Practise in the respiratory nursing environment Release: 1 HLTEN609B Practise in the respiratory nursing environment Modification History Not Applicable Unit Descriptor Descriptor This unit addresses
HLTEN609B Practise in the respiratory nursing environment Release: 1 HLTEN609B Practise in the respiratory nursing environment Modification History Not Applicable Unit Descriptor Descriptor This unit addresses
Pneumonia. Pneumonia is an infection that makes the tiny air sacs in your lungs inflamed (swollen and sore). They then fill with liquid.
. They then fill with liquid.") Pneumonia Pneumonia is an infection that makes the tiny air sacs in your lungs inflamed (swollen and sore). They then fill with liquid. People with mild (not so bad) pneumonia can usually be treated at
Pneumonia Pneumonia is an infection that makes the tiny air sacs in your lungs inflamed (swollen and sore). They then fill with liquid. People with mild (not so bad) pneumonia can usually be treated at
Airway Pressure Release Ventilation
 Page: 1 Policy #: 25.01.153 Issued: 4-1-2006 Reviewed/ Revised: Section: 10-11-2006 Respiratory Care Airway Pressure Release Ventilation Description/Definition Airway Pressure Release Ventilation (APRV)
Page: 1 Policy #: 25.01.153 Issued: 4-1-2006 Reviewed/ Revised: Section: 10-11-2006 Respiratory Care Airway Pressure Release Ventilation Description/Definition Airway Pressure Release Ventilation (APRV)
Staff Skin Care Policy
 This is an official Northern Trust policy and should not be edited in any way Staff Skin Care Policy Reference Number: NHSCT/10/350 Target audience: All Trust staff and in particular those involved in
This is an official Northern Trust policy and should not be edited in any way Staff Skin Care Policy Reference Number: NHSCT/10/350 Target audience: All Trust staff and in particular those involved in
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Your Lungs and COPD. Patient Education Pulmonary Rehabilitation. A guide to how your lungs work and how COPD affects your lungs
 Patient Education Your Lungs and COPD A guide to how your lungs work and how COPD affects your lungs Your lungs are organs that process every breath you take. They provide oxygen (O 2 ) to the blood and
Patient Education Your Lungs and COPD A guide to how your lungs work and how COPD affects your lungs Your lungs are organs that process every breath you take. They provide oxygen (O 2 ) to the blood and
COPD. Information brochure for chronic obstructive pulmonary disease.
 COPD Information brochure for chronic obstructive pulmonary disease. CONTENTS What does COPD mean?...04 What are the symptoms of COPD?...06 What causes COPD?...09 Treating COPD...10 Valve therapy in COPD...12
COPD Information brochure for chronic obstructive pulmonary disease. CONTENTS What does COPD mean?...04 What are the symptoms of COPD?...06 What causes COPD?...09 Treating COPD...10 Valve therapy in COPD...12
RES Non-Invasive Positive Pressure Ventilation Guideline Page 1 of 9
 Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Name of procedure: Laparoscopic (key-hole) ovarian surgery. Left/ Right unilateral salpingo-oophorectomy* (removal of one fallopian tube and ovary)
 ovarian surgery. Left/ Right unilateral salpingo-oophorectomy* (removal of one fallopian tube and ovary)") For staff use only: Patient Details: Surname: First names: Date of birth: Hospital no: Female: (Use hospital identification label) Gynaecology Patient agreement to treatment Name of procedure: Laparoscopic
For staff use only: Patient Details: Surname: First names: Date of birth: Hospital no: Female: (Use hospital identification label) Gynaecology Patient agreement to treatment Name of procedure: Laparoscopic
Respiratory Care. A Life and Breath Career for You!
 Respiratory Care A Life and Breath Career for You! Respiratory Care Makes a Difference At 9:32 am, Lori Moreno brought a newborn baby struggling to breathe back to life What have you accomplished today?
Respiratory Care A Life and Breath Career for You! Respiratory Care Makes a Difference At 9:32 am, Lori Moreno brought a newborn baby struggling to breathe back to life What have you accomplished today?
3100B Clinical Training Program. 3100B HFOV VIASYS Healthcare
 3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
Idiopathic Pulmonary Fibrosis
 Idiopathic Pulmonary Fibrosis What is Idiopathic Pulmonary Fibrosis? Idiopathic pulmonary fibrosis (IPF) is a condition that causes persistent and progressive scarring of the tiny air sacs (alveoli) in
Idiopathic Pulmonary Fibrosis What is Idiopathic Pulmonary Fibrosis? Idiopathic pulmonary fibrosis (IPF) is a condition that causes persistent and progressive scarring of the tiny air sacs (alveoli) in
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
MODULE. POSITIVE AIRWAY PRESSURE (PAP) Titrations
 Titrations") MODULE POSITIVE AIRWAY PRESSURE (PAP) Titrations POSITIVE AIRWAY PRESSURE (PAP) TITRATIONS OBJECTIVES At the end of this module the student must be able to: Identify the standards of practice for administering
MODULE POSITIVE AIRWAY PRESSURE (PAP) Titrations POSITIVE AIRWAY PRESSURE (PAP) TITRATIONS OBJECTIVES At the end of this module the student must be able to: Identify the standards of practice for administering
Mirage FX. User Guide. English NASAL MASK
 Mirage FX NASAL MASK User Guide English Did you know? Replacing your mask and supplies is one of the most important steps in maintaining effective therapy. Replace when... The cushion is no longer clear
Mirage FX NASAL MASK User Guide English Did you know? Replacing your mask and supplies is one of the most important steps in maintaining effective therapy. Replace when... The cushion is no longer clear
OXYGEN THERAPY. DR :Gehan Ali. Lecturer of chest Ds Menoufia university
 OXYGEN THERAPY DR :Gehan Ali Lecturer of chest Ds Menoufia university O 2 Therapy : Indications Documented hypoxemia as evidenced by PaO 2 < 60 mmhg or SaO 2 < 90% on room air PaO 2 or SaO 2 below desirable
OXYGEN THERAPY DR :Gehan Ali Lecturer of chest Ds Menoufia university O 2 Therapy : Indications Documented hypoxemia as evidenced by PaO 2 < 60 mmhg or SaO 2 < 90% on room air PaO 2 or SaO 2 below desirable
Using home NIV for the management of hypercapnic COPD
 Home NIV Program for COPD Using home NIV for the management of hypercapnic COPD This program offers COPD treatment guidelines to physicians to help appropriately target and qualify patients for noninvasive
Home NIV Program for COPD Using home NIV for the management of hypercapnic COPD This program offers COPD treatment guidelines to physicians to help appropriately target and qualify patients for noninvasive
Lesson 7: Respiratory and Skeletal Systems and Tuberculosis
 Glossary 1. asthma: when the airways of the lungs narrow, making breathing difficult 2. bacteria: tiny living creatures that can only be seen with a microscope; some bacteria help the human body, and other
Glossary 1. asthma: when the airways of the lungs narrow, making breathing difficult 2. bacteria: tiny living creatures that can only be seen with a microscope; some bacteria help the human body, and other
CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT
 CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT The 'DR ABCDE' approach to assessing an acutely unwell patient should be at the front of every junior doctor's mind whenever they get bleeped or asked to see
CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT The 'DR ABCDE' approach to assessing an acutely unwell patient should be at the front of every junior doctor's mind whenever they get bleeped or asked to see
Southern Stone County Fire Protection District Emergency Medical Protocols
 TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
1.40 Prevention of Nosocomial Pneumonia
 1.40 Purpose Audience Policy Statement: The guideline is designed to reduce the incidence of pneumonia and other acute lower respiratory tract infections. All UTMB healthcare workers and contract healthcare
1.40 Purpose Audience Policy Statement: The guideline is designed to reduce the incidence of pneumonia and other acute lower respiratory tract infections. All UTMB healthcare workers and contract healthcare
Department of Surgery
 What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
Asthma and COPD Awareness
 Asthma and COPD Awareness Molina Breathe with Ease sm and Chronic Obstructive Pulmonary Disease Molina Healthcare of Michigan Fall 2012 Importance of Controller Medicines Asthma is a disease that causes
Asthma and COPD Awareness Molina Breathe with Ease sm and Chronic Obstructive Pulmonary Disease Molina Healthcare of Michigan Fall 2012 Importance of Controller Medicines Asthma is a disease that causes
New 7/1/2015 MCFRS 1
 New 7/1/2015 MCFRS 1 The providers will summarize the need for this change from an epinephrine auto injector The provider will define the proper dosage of epinephrine for the adult and pediatric patient
New 7/1/2015 MCFRS 1 The providers will summarize the need for this change from an epinephrine auto injector The provider will define the proper dosage of epinephrine for the adult and pediatric patient
American Heart Association
 American Heart Association Basic Life Support for Healthcare Providers Pretest April 2006 This examination to be used only as a PRECOURSE TEST For BLS for Healthcare Providers Courses 2006 American Heart
American Heart Association Basic Life Support for Healthcare Providers Pretest April 2006 This examination to be used only as a PRECOURSE TEST For BLS for Healthcare Providers Courses 2006 American Heart
Having a PEG tube inserted?
 Having a PEG tube inserted? Information for Patients and Carers Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Having a PEG tube inserted? Information for Patients and Carers Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
READ THIS LEAFLET VERY CAREFULLY, AND KEEP IT IN A SAFE PLACE. FLU IS SPREADING IN IRELAND, AND THIS INFORMATION IS IMPORTANT FOR YOU AND YOUR FAMILY.
 READ THIS LEAFLET VERY CAREFULLY, AND KEEP IT IN A SAFE PLACE. FLU IS SPREADING IN IRELAND, AND THIS INFORMATION IS IMPORTANT FOR YOU AND YOUR FAMILY. Information and medical advice for the public on Pandemic
READ THIS LEAFLET VERY CAREFULLY, AND KEEP IT IN A SAFE PLACE. FLU IS SPREADING IN IRELAND, AND THIS INFORMATION IS IMPORTANT FOR YOU AND YOUR FAMILY. Information and medical advice for the public on Pandemic
CH CONSCIOUS SEDATION
 Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Working together to prevent pressure ulcers (prevention and pressure-relieving devices)
") Working together to prevent pressure ulcers (prevention and pressure-relieving devices) Understanding NICE guidance information for people at risk of pressure ulcers, their carers, and the public Draft
Working together to prevent pressure ulcers (prevention and pressure-relieving devices) Understanding NICE guidance information for people at risk of pressure ulcers, their carers, and the public Draft
Summary of EWS Policy for NHSP Staff
 Summary of EWS Policy for NHSP Staff For full version see CMFT Intranet Contact Sister Donna Egan outreach coordinator bleep 8742 Tel: 0161 276 8742 Introduction The close monitoring of patients physiological
Summary of EWS Policy for NHSP Staff For full version see CMFT Intranet Contact Sister Donna Egan outreach coordinator bleep 8742 Tel: 0161 276 8742 Introduction The close monitoring of patients physiological
HANDBOOK FOR HOME OXYGEN THERAPY - 2013
 HANDBOOK FOR HOME OXYGEN THERAPY - 2013 Medical Aids Subsidy Scheme Supporting Independence at Home Your prescription Table of Contents 2 What is oxygen therapy? 3 What is the aim? 3 What are the benefits?
HANDBOOK FOR HOME OXYGEN THERAPY - 2013 Medical Aids Subsidy Scheme Supporting Independence at Home Your prescription Table of Contents 2 What is oxygen therapy? 3 What is the aim? 3 What are the benefits?
Coordinating Committee in Occupational Therapy, Hospital Authority
 Home Oxygen Therapy (Pulmonary Rehabilitation Educational Booklet) Contents Home Oxygen Therapy - Right Patient Aim of Home Oxygen Therapy Operation of Oxygen Concentrator (Flowmeter Ball Type) Operation
Home Oxygen Therapy (Pulmonary Rehabilitation Educational Booklet) Contents Home Oxygen Therapy - Right Patient Aim of Home Oxygen Therapy Operation of Oxygen Concentrator (Flowmeter Ball Type) Operation
CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES
 CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES This document has been prepared by members of the British Thoracic Society (BTS) Working Group on Home Oxygen Services, which is a Sub-Committee
CLINICAL COMPONENT FOR THE HOME OXYGEN SERVICE IN ENGLAND AND WALES This document has been prepared by members of the British Thoracic Society (BTS) Working Group on Home Oxygen Services, which is a Sub-Committee
THERAPEUTIC USE OF HEAT AND COLD
 THERAPEUTIC USE OF HEAT AND COLD INTRODUCTION Heat and cold are simple and very effective therapeutic tools. They can be used locally or over the whole body, and the proper application of heat and cold
THERAPEUTIC USE OF HEAT AND COLD INTRODUCTION Heat and cold are simple and very effective therapeutic tools. They can be used locally or over the whole body, and the proper application of heat and cold
Elective Laparoscopic Cholecystectomy
 General Surgery Elective Laparoscopic Cholecystectomy This information aims to explain what will happen before, during and after your surgery to remove your gallbladder. It includes information about the
General Surgery Elective Laparoscopic Cholecystectomy This information aims to explain what will happen before, during and after your surgery to remove your gallbladder. It includes information about the
Epidural Management. Policy/Purpose. Scope
 Fluid & Medications Management Policy/Purpose... 1 Scope... 1 Associated documents... 2 General... 2 Epidural Indications... 2 Contra-indications:... 2 Educational requirements... 3 Procedural Considerations...
Fluid & Medications Management Policy/Purpose... 1 Scope... 1 Associated documents... 2 General... 2 Epidural Indications... 2 Contra-indications:... 2 Educational requirements... 3 Procedural Considerations...
U S E R M A N U A L. (CGA 870 Connection)
") U S E R M A N U A L 1900 Series (CGA 870 Connection) SAVE THESE INSTRUCTIONS CAUTION Federal (USA) law restricts this device to sale by or on the order of a physician. 300 Held Drive Tel: (+001) 610-262-6090
U S E R M A N U A L 1900 Series (CGA 870 Connection) SAVE THESE INSTRUCTIONS CAUTION Federal (USA) law restricts this device to sale by or on the order of a physician. 300 Held Drive Tel: (+001) 610-262-6090
EMPHYSEMA THERAPY. Information brochure for valve therapy in the treatment of emphysema.
 EMPHYSEMA THERAPY Information brochure for valve therapy in the treatment of emphysema. PATIENTS WITH EMPHYSEMA With every breath, lungs deliver oxygen to the rest of the body to perform essential life
EMPHYSEMA THERAPY Information brochure for valve therapy in the treatment of emphysema. PATIENTS WITH EMPHYSEMA With every breath, lungs deliver oxygen to the rest of the body to perform essential life
Understanding your Peripherally Inserted Central Catheter (PICC) Patient Information
 Patient Information") Understanding your Peripherally Inserted Central Catheter (PICC) Patient Information The Purpose of this Information Sheet This information sheet has been written by patients, members of the public and
Understanding your Peripherally Inserted Central Catheter (PICC) Patient Information The Purpose of this Information Sheet This information sheet has been written by patients, members of the public and
High Impact Intervention Care bundle to reduce ventilation-association pneumonia
 High Impact Intervention Care bundle to reduce ventilation-association pneumonia Aim To reduce the incidence of ventilation-associated pneumonia (VAP). Context The aim of the care bundle, as set out in
High Impact Intervention Care bundle to reduce ventilation-association pneumonia Aim To reduce the incidence of ventilation-associated pneumonia (VAP). Context The aim of the care bundle, as set out in
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPORT State Form 54407 (R / 5-13)
 PRACTICAL SKILLS EXAMINATION REPORT State Form 54407 (R / 5-13)") EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT State Form 54407 (R / 5-3) INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street,
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT State Form 54407 (R / 5-3) INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street,
The Annual Direct Care of Asthma
 The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
5/30/2014 OBJECTIVES THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM. Disclosure
 THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES