Neonatal Jaundice for Infants 35 Weeks Gestational Age v.3
|
|
|
- Joel Daniels
- 9 years ago
- Views:
Transcription

1 Neonatal Jaundice for Infants 35 Weeks Gestational Age v.3 Approval & Citation Explanation of Evidence Ratings Summary of Version Changes Inclusion Criteria Previously healthy Age 14 days Born at 35 wks gestational age Exclusion Criteria Direct hyperbilirubinemia Meets NICU Direct Admit Criteria TSB > 5mg/dL above exchange transfusion threshold Signs of acute bilirubin encephalopathy Suspected sepsis or ill-appearing PHASE I (E.D.) Initial Assessment Clinical History / Physical Exam Blood Glucose only if symptomatic v Total Serum Bilirubin with conjugated fraction (use Heelstick sample) Initiate ED Hyperbilirubinemia (Neonatal) Orders Start phototherapy while awaiting results if clinically indicated Determine exchange transfusion threshold using AAP nomogram Determine phototherapy threshold using BiliTool or AAP nomogram Web Link to BiliTool Place PIV only if patient meets NICU Admission Criteria or NICU Consult Criteria v Pathophysiology Risk for Kernicterus v! IV Fluids NOT routinely indicated Automatic NICU Admission Criteria Evaluate for Discharge Evaluate for NICU Consult Criteria Evaluate for Inpatient Admission Signs of acute bilirubin encephalopathy TSB > 5 mg/dl above exchange transfusion threshold Include NICU attending on calls for patients that meet NICU direct admit criteria. TSB below phototherapy threshold Follow-up appointment arranged for next day Feeding adequately No concern for significant hemolysis TSB within 2mg/dL of exchange transfusion threshold Age < 24 hours High suspicion for or lab evidence of hemolysis (e.g. DAT positive) TSB above phototherapy threshold but not within 2mg/dL of exchange transfusion threshold (e.g. at 72 hours of age, exchange transfusion threshold 24 and TSB 21) Admit to NICU Meets discharge criteria Admit on phototherapy NICU (Off Pathway) Discharge Inpatient Admission TSB rising or meeting NICU admission criteria ED Management Give effective phototherapy Encourage feeding. The infant should not be removed from bili lights for > 20 mins in any 3 hour period. Use bottle if needed. DO NOT interrupt phototherapy for patients nearing exchange transfusion threshold or with rapidly rising TSB Use maternal EBM for supplemental feeds, when available Give 20 ml/kg NS bolus then maintenance IV fluids for patients that meet NICU consult criteria Consider additional labs For questions concerning this pathway, contact:[email protected] 2016, Seattle Children s Hospital, all rights reserved, Medical Disclaimer TSB stable or falling and otherwise clinically well Last Updated: May 2016 Next Expected Review: May 2017

2 Neonatal Jaundice for Infants 35 Weeks Gestational Age v.3 Approval & Citation Explanation of Evidence Ratings PHASE II (INPATIENT) Summary of Version Changes Inclusion Criteria Previously healthy Age 14 days Born at 35 wks gestational age! Supplemental IV Fluids NOT routinely indicated Exclusion Criteria Direct hyperbilirubinemia Meets NICU Direct Admit Criteria TSB > 5mg/dL above exchange transfusion threshold Signs of acute bilirubin encephalopathy Suspected sepsis or ill-appearing! Rebound TSB NOT routinely indicated prior to discharge Inpatient Management Initiate Hyperbilirubinemia (Neonatal) Admit Orders If direct admit, obtain baseline total serum bilirubin (TSB) Continue effective phototherapy until TSB at least 3 mg/dl below phototherapy threshold Encourage feeding. The infant should not be removed from bili lights for > 20 mins in any 3 hour period. Use bottle if needed. If patient unable to maintain normal temperature in an open crib, place in isolette per Isolette Use Policy & Procedure Consider additional labs for patients meeting NICU consult criteria Run maintenance IV fluids for patients within 2 mg/dl of exchange transfusion threshold or with rapidly rising TSB. Stop IVF once TSB has fallen to at least 2 mg/dl below exchange transfusion threshold and feeding well (e.g. at 72 hours of age, exchange transfusion threshold 24 and TSB less than 22) TSB within 2 mg/dl of exchange transfusion threshold, age <72 hours, or known/suspected hemolysis? No Yes Subsequent Labs TSB every 4 hours until TSB falling G6PD (for unexplained hemolysis) No Subsequent Labs TSB approximately 12 hours after starting phototherapy (or with routine AM labs) Subsequent checks as clinically indicated Meets Discharge Criteria Patient off phototherapy and otherwise well Follow-up appointment arranged for next day No concern for significant ongoing hemolysis Yes Discharge For questions concerning this pathway, contact:[email protected] 2016, Seattle Children s Hospital, all rights reserved, Medical Disclaimer Last Updated: May 2016 Next Expected Review: May 2017

3

4


5 Go to Pathophysiology Pg 2 Return to ED Management


6 Go to Pathophysiology Pg 3 Return to ED Management


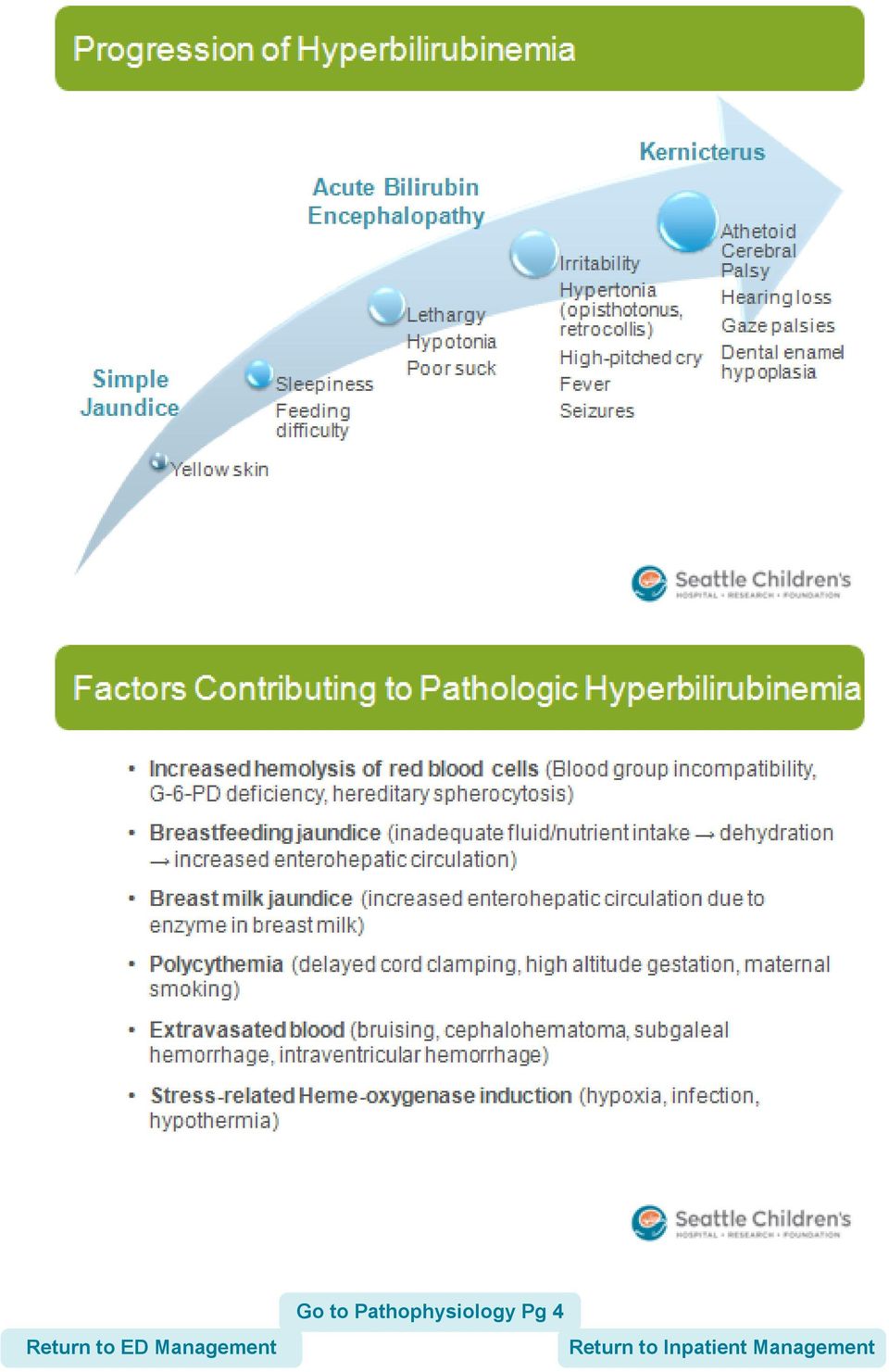
7 Go to Pathophysiology Pg 4

8

9
10 Pathophysiology of ABO Incompatibility Almost exclusively O mothers with A or B fetus A, B mothers make IgM antibodies O mothers make IgG antibodies IgM does not cross the placenta; IgG does Less severe than Rh disease Distraction (A & B antigens are widely expressed in various tissues so RBCs are not the only target) Low A & B surface Ag expression on fetal RBCs = fewer reactive sites Return to ED Management
 Low A & B surface Ag expression on fetal RBCs = fewer reactive sites Return to ED")
11

12


13

] AAP.")
14 Guidelines for Initiation of Phototherapy In Hospitalized Infants of 35 or More Weeks Gestation These levels are approximations representing a consensus based on limited evidence. [LOE: E (AAP 2004)] AAP. Pediatrics 2004;114(1): by American Academy of Pediatrics Return to ED Management
![consensus based on limited evidence. [LOE: E (AAP 2004)] AAP.](/docs-images/46/21493396/images/page_14.jpg "Pediatrics 2004;114(1):297-316 2004 by American Academy of Pediatrics")
15 Guidelines for Exchange Transfusion In Infants 35 or More Weeks Gestation These levels are approximations representing a consensus based largely on the goal of keeping TSB levels below those at which kernicterus has been reported. [LOE: E (AAP 2004)] AAP. Pediatrics 2004;114(1): by American Academy of Pediatrics Return to ED Management
![levels below those at which kernicterus has been reported. [LOE: E (AAP 2004)] AAP.](/docs-images/46/21493396/images/page_15.jpg "Pediatrics 2004;114(1):297-316 2004 by American Academy of Pediatrics Return to ED")


16


17

18


19

20


21
22 Feeding Encourage feeding. The infant should not be removed from bili lights for > 20 mins in any 3 hour period. Use bottle while remaining under bili lights if needed Use maternal expressed breast milk for supplemental feeds, when available Lactation consultation if mom desires to breast feed Rationale: Formula feeds and breastfeeding are equally effective at reducing serum bilirubin during phototherapy. [LOE: moderate quality (NICE 2010)] Return to ED Management

23

24

25
26
27
28 Value Analysis: Blood Glucose VALUE ANALYSIS TOOL DIMENSION CARE OPTION A CARE OPTION B PREFERRED OPTION ASSUMPTIONS MADE DESCRIPTION OF CARE TREATMENT OPTION Obtain serum blood glucose on all patients admitted with neonatal jaundice Do not routinely obtain blood glucose levels on patients unless symptomatic OPERATIONAL FACTORS Percent adherence to care (goal 80%) Neutral Neutral NEUTRAL Care delivery team effects Preferred OPTION B BENEFITS / HARMS (QUALITY/OUTCOME) Degree of recovery at discharge Neutral Neutral NEUTRAL Effects on natural history of the disease over equivalent time Neutral Neutral NEUTRAL Potential to cause harm Neutral Neutral NEUTRAL Palatability to patient/family Preferred OPTION B Population-related benefits Neutral Neutral NEUTRAL Threshold for population-related benefits reached COST (Arising from Options A or B) - express as cost per day ROOM RATE ($ or time to recovery) Neutral Neutral NEUTRAL Dx/Rx costs ($) Preferred OPTION B SAVINGS: $1,333/yr COST (Complications/adverse effects arising from Options A or B)- express as cost per day ROOM RATE ($ or time to recovery) Neutral Neutral NEUTRAL Dx/Rx costs ($) Neutral Neutral NEUTRAL VALUE ANALYSIS GRID BENEFIT (QUALITY & OUTCOMES) COST A > B A = B A < B Unclear A costs more than B Make value judgement B B Do B and PDSA in 1 year A and B costs are the same A A or B, operational factors may influence choice B A or B, operational factors may influence choice, PDSA in 1 year B costs more than A A A Make value judgement Do A and PDSA in 1 year VALUE STATEMENT FINAL CSW VALUE STATEMENT Blood glucose should not be ordered routinely for patients with neonatal jaundice, levels should be obtained only if symptomatic. This recommendation is based on a review of local data, 1 out of 194 blood glucose values was <40mg/dl, this patient was asymptomatic and did not require intravenous glucose. Estimated yearly cost savings is $1,333. Return to ED Management
29 Value Analysis: PIVs and IV Fluids VALUE ANALYSIS TOOL DIMENSION CARE OPTION A CARE OPTION B PREFERRED OPTION ASSUMPTIONS MADE DESCRIPTION OF CARE TREATMENT OPTION Obtain peripheral IV (PIV) upon admission and give IVFs. Obtain peripheral IV and give IVFs only if patient meets NICU admission or consult criteria. OPERATIONAL FACTORS Percent adherence to care (goal 80%) Neutral Neutral NEUTRAL Care delivery team effects Preferred OPTION B BENEFITS / HARMS (QUALITY/OUTCOME) Degree of recovery at discharge Neutral Neutral OPTION B Effects on natural history of the disease over equivalent time Neutral Neutral NEUTRAL Potential to cause harm Preferred OPTION B Palatability to patient/family Preferred OPTION B Population-related benefits Neutral Neutral NEUTRAL COST (Arising from Options A or B) - express as cost per day ROOM RATE ($ or time to recovery) Neutral Neutral NEUTRAL Dx/Rx costs ($) Preferred OPTION B SAVINGS: $ 4,623/yr COST (Complications/adverse effects arising from Options A or B)- express as cost per day ROOM RATE ($ or time to recovery) Neutral Neutral NEUTRAL Dx/Rx costs ($) Neutral Neutral VALUE ANALYSIS GRID BENEFIT (QUALITY & OUTCOMES) COST A > B A = B A < B Unclear A costs more than B Make value judgement B B Do B and PDSA in 1 year A and B costs are the same A A or B, operational factors may influence choice B A or B, operational factors may influence choice, PDSA in 1 year B costs more than A A A Make value judgement Do A and PDSA in 1 year VALUE STATEMENT FINAL CSW VALUE STATEMENT Peripheral IVs and IVFs should only be utilized if the patient meets NICU admission or consult criteria. This option is preferred due to lower cost, increased palatability and decreased risk for harm while providing safe and appropriate care. Estimated yearly cost savings is $4,633 Return to ED Management
30 Neonatal Jaundice Approval & Citation Approved by the CSW Neonatal Jaundice for 5/31/2012 go live CSW Neonatal Jaundice Team: Hospital Medicine, Owner Emergency Dept Owner Emergency Dept, CNS Emergency Dept, CNS Intensive Care Unit, RN Medical Unit, CNS Neonatology, Stakeholder Janie Hallstrand, MD Ron Kaplan, MD Sara Fenstermacher, CNS Elaine Beardsley, RN Karen Kelly, RN Coral Ringer, CNS Linda Wallen, MD Clinical Effectiveness Team: Consultant: Project Manager: CE Analyst: CIS Informatician: CIS Analyst: Librarian: Program Coordinator: Darren Migita, MD Jennifer Magin, MBA James Johnson Michael Leu, MD, MS, MHS Heather Marshall Jackie Morton, MLIS Asa Herrman Executive Approval: Sr. VP, Chief Medical Officer Sr. VP, Chief Nursing Officer Surgeon-in-Chief Mark Del Beccaro, MD Madlyn Murrey, BSN, MN Bob Sawin, MD Retrieval Website: Please cite as: Hallstrand, J., Fenstermacher, S., Kaplan, R., Kelly K., Migita, D., Ringer, C., 2012 October. Neonatal Jaundice Pathway. Available from: Return to Home
31 Evidence Ratings We used the GRADE method of rating evidence quality. Evidence is first assessed as to whether it is from randomized trial, or observational studies. The rating is then adjusted in the following manner: Quality ratings are downgraded if studies: Have serious limitations Have inconsistent results If evidence does not directly address clinical questions If estimates are imprecise OR If it is felt that there is substantial publication bias Quality ratings can be upgraded if it is felt that: The effect size is large If studies are designed in a way that confounding would likely underreport the magnitude of the effect OR If a dose-response gradient is evident Quality of Evidence: High quality Moderate quality Low quality Very low quality Expert Opinion (E) Reference: Guyatt G et al. J Clin Epi 2011: To Bibliography Return to ED Management
32 Summary of Version Changes Version 1 (5/31/2012): Go live Version 2 (4/2/2013): Added recommendation for ED to notify NICU attending if patient meets NICU admission criteria; established recommendations for removal from phototherapy for feeding. Version 3: (5/10/2016): Added Value Analysis #1 (Glucose Testing) Return to ED Management
33 Medical Disclaimer Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor Seattle Children s Healthcare System nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such information. Readers should confirm the information contained herein with other sources and are encouraged to consult with their health care provider before making any health care decision. Return to ED Management For questions concerning this pathway, contact: [email protected] Last Updated: xx/xx/xxxx Valid until: xx/xx/xxxx
34 Bibliography Identification 52 records identified through database searching 0 additional records identified through other sources Screening 48 records after duplicates removed 48 records screened 21 records excluded Elgibility 27 full-text articles assessed for eligibility 22 full-text articles excluded, 16 did not answer clinical question 6 did not meet quality threshold Included 6 studies included in pathway Flow diagram adapted from Moher D et al. BMJ 2009;339:bmj.b2535 To Bibliography Return to ED Management
35 Bibliography American Academy of Pediatrics, Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks gestation. Pediatrics. 2004;114(1): American Academy of Pediatrics, Subcommittee on Hyperbilirubinemia. Phototherapy to prevent severe neonatal hyperbilirubinemia in the newborn infant 35 or more weeks gestation. Pediatrics. 2011;128(4):e1046-e1052 Atkinson LR, et al. Phototherapy use in jaundiced newborns in a large managed care organization: do clinicians adhere to the guideline? Pediatrics.2003;111:e555 Barak M, et al. When should phototherapy be stopped? A pilot study comparing two targets of serum bilirubin concentration. Acta Paediatrica. 2009; 98:(2) Bhutani VK, et al. A systems approach for neonatal hyperbilirubinemia in term and near-term newborns. J Obstet Gynecol Neonatal Nurs. 2006;35: Chavez GF, et al. Epidemiology of Rh hemolytic disease of the newborn in the United States. JAMA. Jun ;265(24): Eggert LD, et al. The effect of instituting a prehospital-discharge newborn bilirubin screening program in an 18- hospital health system. Pediatrics. 2006;117:e855-e862 Harris M, et al. Developmental follow-up of breastfed term and near-term infants with marked hyperbilirubinemia. Pediatrics. 2001;107: Kaplan M, et al. Post-phototherapy neonatal bilirubin rebound: a potential cause of significant hyperbilirubinaemia. Archives of Disease in Childhood. 2006; 91:(1)31-34 Maisels MJ, Kring E. Bilirubin rebound following intensive phototherapy. Arch Pediatr Adolesc Med. 2002;156(7): Maisels MJ, Kring EA. Length of stay, jaundice, and hospital readmission. Pediatrics. 1998;101: Murray NA, Roberts IA. Haemolytic disease of the newborn. Arch Dis Child Fetal Neonatal Ed. Mar 2007;92(2):F83-8 National Institute for Health and Clinical Excellence. Neonatal jaundice. (Clinical guideline 98.) Newman TB, et al. Frequency of neonatal bilirubin testing and hyperbilirubinemia in a large health maintenance organization. Pediatrics. 1999;104: Spencer J. Common problems of breastfeeding and weaning. UpToDate. March Tan KL. The nature of the dose-response relationship of phototherapy for neonatal hyperbilirubinemia. J Pediatr. 1977;90(3): Tan KL. The pattern of bilirubin response to phototherapy for neonatal hyperbilirubinemia. Pediatr Res. 1982;16(8): Wagle S, Rosenkrantz T (ed.). Hemolytic Disease of Newborn. Medscape Reference. May Return to ED Management
Depressive Disorders Inpatient Management v.1.1
 Depressive Disorders Inpatient Management v.1.1 Executive Summary Citation Information Explanation of Evidence Ratings Summary of Version Changes Intake Admission interview, physical exam, and review of
Depressive Disorders Inpatient Management v.1.1 Executive Summary Citation Information Explanation of Evidence Ratings Summary of Version Changes Intake Admission interview, physical exam, and review of
MANAGEMENT OF DIRECT ANTIGLOBULIN TEST (DAT) POSITIVE INFANTS NEONATAL CLINICAL GUIDELINE
 POSITIVE INFANTS NEONATAL CLINICAL GUIDELINE") MANAGEMENT OF DIRECT ANTIGLOBULIN TEST (DAT) POSITIVE INFANTS NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1. To provide monitoring and treatment guidance for medical and nursing staff
MANAGEMENT OF DIRECT ANTIGLOBULIN TEST (DAT) POSITIVE INFANTS NEONATAL CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1. To provide monitoring and treatment guidance for medical and nursing staff
Hyperbilirubinemia in the Newborn Infant 35 Weeks Gestation: An Update With Clarifications
 COMMENTARY Hyperbilirubinemia in the Newborn Infant 35 Weeks Gestation: An Update With Clarifications AUTHORS: M. Jeffrey Maisels, MB, BCh, DSc, a Vinod K. Bhutani, MD, b Debra Bogen, MD, c Thomas B. Newman,
COMMENTARY Hyperbilirubinemia in the Newborn Infant 35 Weeks Gestation: An Update With Clarifications AUTHORS: M. Jeffrey Maisels, MB, BCh, DSc, a Vinod K. Bhutani, MD, b Debra Bogen, MD, c Thomas B. Newman,
Haemolytic disease of the newborn. 09.06.2016 Burak Salgin
 Haemolytic disease of the newborn 09.06.2016 Burak Salgin Innovation and excellence in health and care Addenbrooke s Hospital I Rosie Hospital Haemolytic disease of the newborn......used to be synonymous
Haemolytic disease of the newborn 09.06.2016 Burak Salgin Innovation and excellence in health and care Addenbrooke s Hospital I Rosie Hospital Haemolytic disease of the newborn......used to be synonymous
Why is prematurity a concern?
 Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Clinical guideline Published: 19 May 2010 nice.org.uk/guidance/cg98
 Jaundice in newborn babies under 28 days Clinical guideline Published: 19 May 2010 nice.org.uk/guidance/cg98 NICE 2010. All rights reserved. Last updated May 2016 Your responsibility The recommendations
Jaundice in newborn babies under 28 days Clinical guideline Published: 19 May 2010 nice.org.uk/guidance/cg98 NICE 2010. All rights reserved. Last updated May 2016 Your responsibility The recommendations
Quality-Based Procedures Clinical Handbook for Hyperbilirubinemia in Term and Late Pre-Term Infants ( 35 weeks)
") Quality-Based Procedures Clinical Handbook for Hyperbilirubinemia in Term and Late Pre-Term Infants ( 35 weeks) Provincial Council for Maternal & Child Health & Ministry of Health and Long-Term Care September
Quality-Based Procedures Clinical Handbook for Hyperbilirubinemia in Term and Late Pre-Term Infants ( 35 weeks) Provincial Council for Maternal & Child Health & Ministry of Health and Long-Term Care September
Yale- New Haven Hospital- Quality Improvement Project Well Newborn Team. Kate Manuel, APRN, IBCLC Lactation Program Manager Yale- New Haven Hospital
 Yale- New Haven Hospital- Quality Improvement Project Well Newborn Team Kate Manuel, APRN, IBCLC Lactation Program Manager Yale- New Haven Hospital Our Team Kate Manuel, APRN, IBCLC Jaspreet Loyal, MD
Yale- New Haven Hospital- Quality Improvement Project Well Newborn Team Kate Manuel, APRN, IBCLC Lactation Program Manager Yale- New Haven Hospital Our Team Kate Manuel, APRN, IBCLC Jaspreet Loyal, MD
NICU Level of Care Criteria
 Introduction The NICU Criteria were developed to assist in the authorization for various levels of Neonatal Intensive Care Unit (NICU), as well as assistance in determining the appropriate level of care.
Introduction The NICU Criteria were developed to assist in the authorization for various levels of Neonatal Intensive Care Unit (NICU), as well as assistance in determining the appropriate level of care.
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE CENTRE FOR CLINICAL PRACTICE QUALITY STANDARDS PROGRAMME
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE CENTRE FOR CLINICAL PRACTICE QUALITY STANDARDS PROGRAMME standard topic: Specialist neonatal care Output: standard advice to the Secretary of State
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE CENTRE FOR CLINICAL PRACTICE QUALITY STANDARDS PROGRAMME standard topic: Specialist neonatal care Output: standard advice to the Secretary of State
Prediction of the development of neonatal hyperbilirubinemia by increased umbilical cord blood bilirubin
 Prediction of the development of neonatal hyperbilirubinemia by increased umbilical cord blood bilirubin Author(s): Amar Taksande, Krishna Vilhekar, Manish Jain, Preeti Zade, Suchita Atkari, Sherin Verkey
Prediction of the development of neonatal hyperbilirubinemia by increased umbilical cord blood bilirubin Author(s): Amar Taksande, Krishna Vilhekar, Manish Jain, Preeti Zade, Suchita Atkari, Sherin Verkey
Jaundice in the Newborns
 Jaundice in the Newborns Satish Mishra, Ramesh Agarwal, Ashok K Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari Nagar, New Delhi 110029
Jaundice in the Newborns Satish Mishra, Ramesh Agarwal, Ashok K Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari Nagar, New Delhi 110029
HOSPITAL GRADE ELECTRIC BREAST PUMP Corporate Medical Policy
 HOSPITAL GRADE ELECTRIC BREAST PUMP Corporate Medical Policy File name: Hospital Grade Electric Breast Pump File code: UM.DME.06 Origination: 04/2005 Last Review: 09/2015 Next Review: 09/2016 Effective
HOSPITAL GRADE ELECTRIC BREAST PUMP Corporate Medical Policy File name: Hospital Grade Electric Breast Pump File code: UM.DME.06 Origination: 04/2005 Last Review: 09/2015 Next Review: 09/2016 Effective
D-94164-2013. Gentle for the newborn, efficient for you. DRÄGER JAUNDICE METER JM-105
 D-94164-2013 Gentle for the newborn, efficient for you. DRÄGER JAUNDICE METER JM-105 2 Assessing jaundice risk without the trauma D-94313-2013 D-7346-2009 While neonatal jaundice or hyperbilirubinemia
D-94164-2013 Gentle for the newborn, efficient for you. DRÄGER JAUNDICE METER JM-105 2 Assessing jaundice risk without the trauma D-94313-2013 D-7346-2009 While neonatal jaundice or hyperbilirubinemia
Sample Usage Protocol Jaundice Meter JM-105
 D-94164-2013 Sample Usage Protocol Jaundice Meter JM-105 This Sample Usage Protocol is provided as a template for creating a facility or department-specific protocol for using the Dräger Jaundice Meter
D-94164-2013 Sample Usage Protocol Jaundice Meter JM-105 This Sample Usage Protocol is provided as a template for creating a facility or department-specific protocol for using the Dräger Jaundice Meter
Supporting Breastfeeding and Lactation: The Primary Care Pediatrician s Guide to Getting Paid
 Supporting Breastfeeding and Lactation: The Primary Care Pediatrician s Guide to Getting Paid Breastfeeding support can often be quite time-intensive initially but pays off in a healthier patient population.
Supporting Breastfeeding and Lactation: The Primary Care Pediatrician s Guide to Getting Paid Breastfeeding support can often be quite time-intensive initially but pays off in a healthier patient population.
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Routine Screening of Neonates Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Routine Screening of Neonates Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6
Breastfeeding. Clinical Case Studies. Residency Curriculum
 Teaching Tool Clinical Case Studies These clinical cases highlight common breastfeeding issues and concerns that your residents will encounter. You can use them during grand rounds, noon lecture, journal
Teaching Tool Clinical Case Studies These clinical cases highlight common breastfeeding issues and concerns that your residents will encounter. You can use them during grand rounds, noon lecture, journal
CDC National Survey of Maternity Practices in Infant Nutrition and Care (mpinc)
") OMB #0920-0743 EXP. DATE: 10/31/2010 CDC National Survey of Maternity Practices in Infant Nutrition and Care (mpinc) Hospital Survey Conducted for Centers for Disease Control and Prevention National Center
OMB #0920-0743 EXP. DATE: 10/31/2010 CDC National Survey of Maternity Practices in Infant Nutrition and Care (mpinc) Hospital Survey Conducted for Centers for Disease Control and Prevention National Center
SOUTHERN WEST MIDLANDS NEWBORN NETWORK
 SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Title Person Responsible for Review Delayed Umbilical Cord Clamping Dr Andrew Gallagher Date Guideline Agreed:
SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Title Person Responsible for Review Delayed Umbilical Cord Clamping Dr Andrew Gallagher Date Guideline Agreed:
Milliman Guidelines NICU Levels*
 Milliman Guidelines NICU Levels* Neonatal Intensive Care Unit Level IV If the following conditions/procedures exist, in addition to the fulfillment of Level III Criteria, the approved inpatient days should
Milliman Guidelines NICU Levels* Neonatal Intensive Care Unit Level IV If the following conditions/procedures exist, in addition to the fulfillment of Level III Criteria, the approved inpatient days should
Parvovirus B19 Infection in Pregnancy
 Parvovirus B19 Infection in Pregnancy Information Pack Parvovirus B19 Infection in Pregnancy Information Booklet CONTENTS: THE VIRUS page 3 CLINICAL MANIFESTATIONS page 6 DIAGNOSIS page 8 PATIENT MANAGEMENT
Parvovirus B19 Infection in Pregnancy Information Pack Parvovirus B19 Infection in Pregnancy Information Booklet CONTENTS: THE VIRUS page 3 CLINICAL MANIFESTATIONS page 6 DIAGNOSIS page 8 PATIENT MANAGEMENT
Dr.U.Venkataramana Rao DNB Resident, Neonatology Unit, Southern Railway HQ Hospital.
 NEONATAL DENGUE Dr.N.Kannan Prof and HOD, Dpt of Pediatrics & Child Health, Southern Railway HQ Hospital, Ayanavaram. Dr.U.Venkataramana Rao DNB Resident, Neonatology Unit, Southern Railway HQ Hospital.
NEONATAL DENGUE Dr.N.Kannan Prof and HOD, Dpt of Pediatrics & Child Health, Southern Railway HQ Hospital, Ayanavaram. Dr.U.Venkataramana Rao DNB Resident, Neonatology Unit, Southern Railway HQ Hospital.
Breastfeeding. Cultural Case Studies. Residency Curriculum
 Teaching Tool Cultural Case Studies These cultural cases are designed to help the residents understand cultural effectiveness as it relates to breastfeeding. You can use them during grand rounds, noon
Teaching Tool Cultural Case Studies These cultural cases are designed to help the residents understand cultural effectiveness as it relates to breastfeeding. You can use them during grand rounds, noon
Delayed Cord Clamping
 ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
Validation of Umbilical Cord Blood Sampling to Reduce Phlebotomy Losses in Newborns at Risk for IVH
 Validation of Umbilical Cord Blood Sampling to Reduce Phlebotomy Losses in Newborns at Risk for IVH Julianne Cramer APRN, NNP, Thomas George MD, Marla Mills DNP, PNP, Kim Popp RN, BSN, MA, Raghavendra
Validation of Umbilical Cord Blood Sampling to Reduce Phlebotomy Losses in Newborns at Risk for IVH Julianne Cramer APRN, NNP, Thomas George MD, Marla Mills DNP, PNP, Kim Popp RN, BSN, MA, Raghavendra
BLOOD GROUP ANTIGENS AND ANTIBODIES
 BLOOD GROUP ANTIGENS AND ANTIBODIES Over 20 blood group systems having approximately 400 blood group antigens are currently recognised. The ABO and Rhesus (Rh) blood group systems are of major clinical
BLOOD GROUP ANTIGENS AND ANTIBODIES Over 20 blood group systems having approximately 400 blood group antigens are currently recognised. The ABO and Rhesus (Rh) blood group systems are of major clinical
Perinatal Symposium--2012
 Perinatal Symposium--2012 Neonatal Jaundice: When Do the Light Bulbs Go On? Theodore R. Thompson, MD Professor of Pediatrics Division of Neonatology University of Minnesota Medical School I have no financial
Perinatal Symposium--2012 Neonatal Jaundice: When Do the Light Bulbs Go On? Theodore R. Thompson, MD Professor of Pediatrics Division of Neonatology University of Minnesota Medical School I have no financial
2016 CODING FOR FETAL ALCOHOL SPECTRUM DISORDERS
 2016 CODING FOR FETAL ALCOHOL SPECTRUM DISORDERS Listed below are the most commonly used codes applicable to FASD patient care. Code Description ICD-10-CM Primary Diagnosis P04.3 Newborn (suspected to
2016 CODING FOR FETAL ALCOHOL SPECTRUM DISORDERS Listed below are the most commonly used codes applicable to FASD patient care. Code Description ICD-10-CM Primary Diagnosis P04.3 Newborn (suspected to
Premature Infant Care
 Premature Infant Care Introduction A premature baby is born before the 37th week of pregnancy. Premature babies are also called preemies. Premature babies may have health problems because their organs
Premature Infant Care Introduction A premature baby is born before the 37th week of pregnancy. Premature babies are also called preemies. Premature babies may have health problems because their organs
The sensitive marker for glomerular filtration rate (GFR) Estimation of GFR from Serum Cystatin C:
 Estimation of GFR from Serum Cystatin C:") The sensitive marker for glomerular filtration rate (GFR) Estimation of GFR from Serum Cystatin C: The good correlation allows close estimation of GFR Cystatin C GFR GFR in serum estimated* measured* n
The sensitive marker for glomerular filtration rate (GFR) Estimation of GFR from Serum Cystatin C: The good correlation allows close estimation of GFR Cystatin C GFR GFR in serum estimated* measured* n
Direct Antiglobulin Test (DAT)
") Exercise 8 Exercise 9 Direct Antiglobulin Test (DAT) Elution Study Task Aim Introduction To perform the DAT and elution procedure with correct interpretation of results. To perform with 100% accuracy the
Exercise 8 Exercise 9 Direct Antiglobulin Test (DAT) Elution Study Task Aim Introduction To perform the DAT and elution procedure with correct interpretation of results. To perform with 100% accuracy the
Direct Antiglobulin Test (DAT)
") Exercise 8 Direct Antiglobulin Test (DAT) Objectives: 1. State the purpose for performing the DAT. 2. State what a positive DAT indicates. 3. List the reagents which are used for performing the DAT. 4.
Exercise 8 Direct Antiglobulin Test (DAT) Objectives: 1. State the purpose for performing the DAT. 2. State what a positive DAT indicates. 3. List the reagents which are used for performing the DAT. 4.
William Atkinson, MD, MPH Hepatitis B Vaccine Issues June 16, 2016
 William Atkinson, MD, MPH Hepatitis B Vaccine Issues June 16, 2016 Advisory Committee on Immunization Practices (ACIP) The recommendations to be discussed are primarily those of the ACIP composed of 15
William Atkinson, MD, MPH Hepatitis B Vaccine Issues June 16, 2016 Advisory Committee on Immunization Practices (ACIP) The recommendations to be discussed are primarily those of the ACIP composed of 15
Institutional Handbook of Operating Procedures Policy 9.1.10
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 9.1.10 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 9.1.10 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Krystal Revai, MD, FAAP. Written Testimony. Breastfeeding as Primary Obesity Prevention. Obesity Prevention Initiative Act Public Hearings
 Written Testimony Breastfeeding as Primary Obesity Prevention Obesity Prevention Initiative Act Public Hearings on behalf of the ILLINOIS CHAPTER, AMERICAN ACADEMY OF PEDIATRICS Submitted March 15, 2010
Written Testimony Breastfeeding as Primary Obesity Prevention Obesity Prevention Initiative Act Public Hearings on behalf of the ILLINOIS CHAPTER, AMERICAN ACADEMY OF PEDIATRICS Submitted March 15, 2010
Neonatal Intensive Care Unit A photographic tour
 Patient Education : A photographic tour Neonatal Intensive Care Unit A photographic tour This booklet was created by mothers who gave birth to premature babies at University of Washington Medical Center
Patient Education : A photographic tour Neonatal Intensive Care Unit A photographic tour This booklet was created by mothers who gave birth to premature babies at University of Washington Medical Center
SUPPORT OF BREASTFEEDING FAMILIES IN NICU THE WOMEN S HOSPITAL AT JACKSON MEMORIAL
 SUPPORT OF BREASTFEEDING FAMILIES IN NICU THE WOMEN S HOSPITAL AT JACKSON MEMORIAL OBJECTIVES To verbalize the benefits of breast milk for preterm and critical ill infants To recognize how to assist mother
SUPPORT OF BREASTFEEDING FAMILIES IN NICU THE WOMEN S HOSPITAL AT JACKSON MEMORIAL OBJECTIVES To verbalize the benefits of breast milk for preterm and critical ill infants To recognize how to assist mother
CHAPTER 10 BLOOD GROUPS: ABO AND Rh
 CHAPTER 10 BLOOD GROUPS: ABO AND Rh The success of human blood transfusions requires compatibility for the two major blood group antigen systems, namely ABO and Rh. The ABO system is defined by two red
CHAPTER 10 BLOOD GROUPS: ABO AND Rh The success of human blood transfusions requires compatibility for the two major blood group antigen systems, namely ABO and Rh. The ABO system is defined by two red
Breastfeeding Friendly Physician Offices
 Breastfeeding Friendly Physician Offices Jennifer Stewart, R.D., M.B.A., CLS Loving Support Breastfeeding Program, Riverside County Department of Public Health Susanna Sibilsky, Regional Breastfeeding
Breastfeeding Friendly Physician Offices Jennifer Stewart, R.D., M.B.A., CLS Loving Support Breastfeeding Program, Riverside County Department of Public Health Susanna Sibilsky, Regional Breastfeeding
A8b. Resuscitation of a Term Infant with Meconium Staining. Session Summary. Session Objectives. References
 A8b Resuscitation of a Term Infant with Meconium Staining Karen Wright, PhD, NNP-BC Assistant Professor and Coordinator, Neonatal Nurse Practitioner Program Dept. of Women, Children, and Family Nursing,
A8b Resuscitation of a Term Infant with Meconium Staining Karen Wright, PhD, NNP-BC Assistant Professor and Coordinator, Neonatal Nurse Practitioner Program Dept. of Women, Children, and Family Nursing,
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Sepsis Core Measures Bundle Requirements
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Sepsis Core Measures Bundle Requirements
New York State Ten Steps to a Breastfeeding Friendly Practice Implementation Guide June 2014
 Ten Steps to a Breastfeeding Friendly Practice 1. Develop and maintain a written breastfeeding friendly office policy. 2. Train all staff to promote, support and protect breastfeeding and breastfeeding
Ten Steps to a Breastfeeding Friendly Practice 1. Develop and maintain a written breastfeeding friendly office policy. 2. Train all staff to promote, support and protect breastfeeding and breastfeeding
Lyme Disease in Pregnancy. Dr Sarah Chissell Consultant Obstetrician William Harvey Hospital, Kent
 Lyme Disease in Pregnancy Dr Sarah Chissell Consultant Obstetrician William Harvey Hospital, Kent Conflict of interest My son has chronic Lyme disease Infections in pregnancy Transplacental infection Perinatal
Lyme Disease in Pregnancy Dr Sarah Chissell Consultant Obstetrician William Harvey Hospital, Kent Conflict of interest My son has chronic Lyme disease Infections in pregnancy Transplacental infection Perinatal
American Academy of Pediatrics Section on Breastfeeding. Ten Steps to Support Parents Choice to Breastfeed Their Baby
 American Academy of Pediatrics Section on Breastfeeding 1 2 3 4 5 6 7 8 9 10 Ten Steps to Support Parents Choice to Breastfeed Their Baby This practice enthusiastically supports parents plans to breastfeed
American Academy of Pediatrics Section on Breastfeeding 1 2 3 4 5 6 7 8 9 10 Ten Steps to Support Parents Choice to Breastfeed Their Baby This practice enthusiastically supports parents plans to breastfeed
Caring for your baby in the NICU: feeding
 C1 At birth, all newborns need a great deal of energy and nutrients from food to help their bodies grow, and to adjust to life outside the womb. Babies who are born early (premature) and/or with a very
C1 At birth, all newborns need a great deal of energy and nutrients from food to help their bodies grow, and to adjust to life outside the womb. Babies who are born early (premature) and/or with a very
Effect of White Plastic Cover around the Phototherapy Unit on Hyperbilirubinemia in Full Term Neonates
 Original Article Iran J Pediatr Apr 213; Vol 23 (No 2), Pp: 143148 Effect of White Plastic Cover around the Phototherapy Unit on Hyperbilirubinemia in Full Term Neonates Homa Babaei* 1, MD; AliAsghar Alipour
Original Article Iran J Pediatr Apr 213; Vol 23 (No 2), Pp: 143148 Effect of White Plastic Cover around the Phototherapy Unit on Hyperbilirubinemia in Full Term Neonates Homa Babaei* 1, MD; AliAsghar Alipour
Magee-Womens Hospital
 Magee-Womens Hospital Magee Pregnancy Recovery Program: History Pregnancy Recovery Center A Medical Home Model Approach to Strengthen Families Bawn Maguire, MSN, RN Programmatic Nurse Specialist Stephanie
Magee-Womens Hospital Magee Pregnancy Recovery Program: History Pregnancy Recovery Center A Medical Home Model Approach to Strengthen Families Bawn Maguire, MSN, RN Programmatic Nurse Specialist Stephanie
Suggested BiliChek Usage Protocol
 Suggested BiliChek Usage Protocol I. Subject: BiliChek Non-Invasive Bilirubin Analyzer II. Purpose: To outline and define the use of the BiliChek Non-Invasive Bilirubin Analyzer in the hospital setting
Suggested BiliChek Usage Protocol I. Subject: BiliChek Non-Invasive Bilirubin Analyzer II. Purpose: To outline and define the use of the BiliChek Non-Invasive Bilirubin Analyzer in the hospital setting
Mother s blood test to check her unborn baby s blood group
 Mother s blood test to check her unborn baby s blood group This leaflet explains why it is important to have a blood test to check the baby s blood group, so that only those who need it, receive anti-d
Mother s blood test to check her unborn baby s blood group This leaflet explains why it is important to have a blood test to check the baby s blood group, so that only those who need it, receive anti-d
DMBA Student Health Plan
 2 1 6 3 1 DMBA Student Health Plan Maternity Benefits for the Non-Student Dependents FIRST: Find a CONTRACTED PROVIDER by going to www.dmba.com. Find a Provider (under QuickLinks) Find a Deseret Mutual
2 1 6 3 1 DMBA Student Health Plan Maternity Benefits for the Non-Student Dependents FIRST: Find a CONTRACTED PROVIDER by going to www.dmba.com. Find a Provider (under QuickLinks) Find a Deseret Mutual
EPIDEMIOLOGY OF HEPATITIS B IN IRELAND
 EPIDEMIOLOGY OF HEPATITIS B IN IRELAND Table of Contents Acknowledgements 3 Summary 4 Introduction 5 Case Definitions 6 Materials and Methods 7 Results 8 Discussion 11 References 12 Epidemiology of Hepatitis
EPIDEMIOLOGY OF HEPATITIS B IN IRELAND Table of Contents Acknowledgements 3 Summary 4 Introduction 5 Case Definitions 6 Materials and Methods 7 Results 8 Discussion 11 References 12 Epidemiology of Hepatitis
DMBA Student Health Plan
 622 661 156 703 141 DMBA Student Health Plan FIRST: Find a CONTRACTED PROVIDER by going to www.dmba.com. Find a Provider (under QuickLinks) Find a Deseret Mutual Contracted provider in Utah Select # 2;
622 661 156 703 141 DMBA Student Health Plan FIRST: Find a CONTRACTED PROVIDER by going to www.dmba.com. Find a Provider (under QuickLinks) Find a Deseret Mutual Contracted provider in Utah Select # 2;
Priya Rajan, MD Northwestern University September 13, 2013
 Priya Rajan, MD Northwestern University September 13, 2013 o Study Finds Benefits in Delaying Severing of Umbilical Cord nytimes.com, 7/10/13 o Delay cord clamping for baby health, say experts bbc.com.uk,
Priya Rajan, MD Northwestern University September 13, 2013 o Study Finds Benefits in Delaying Severing of Umbilical Cord nytimes.com, 7/10/13 o Delay cord clamping for baby health, say experts bbc.com.uk,
Regions Hospital Delineation of Privileges Nurse Practitioner
 Regions Hospital Delineation of Privileges Nurse Practitioner Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Regions Hospital Delineation of Privileges Nurse Practitioner Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Copyright 2015 Maureen Shogan. Not to be reproduced without permission in writing from above. [email protected]
 Nourishing the Neonate Phoenix, AZ 10/8/15 Meeting 2016 TJC Perinatal Core Measure for Exclusive Breastfeeding Perinatal Core Measure PC 05 ANY Percentage of US children breastfeed Exclusive Neonatal Clinical
Nourishing the Neonate Phoenix, AZ 10/8/15 Meeting 2016 TJC Perinatal Core Measure for Exclusive Breastfeeding Perinatal Core Measure PC 05 ANY Percentage of US children breastfeed Exclusive Neonatal Clinical
CORD BLOOD EVALUATION
 CORD BLOOD EVALUATION Principle: When there is incompatibility between a mother s antibodies and an infant s red blood cell antigens, the infant is at risk of developing Hemolytic Disease of the Fetus
CORD BLOOD EVALUATION Principle: When there is incompatibility between a mother s antibodies and an infant s red blood cell antigens, the infant is at risk of developing Hemolytic Disease of the Fetus
Breastfeeding. Nursing Education
 Breastfeeding AWHONN supports breastfeeding as the optimal method of infant nutrition. AWHONN believes that women should be encouraged to breastfeed and receive instruction and support from the entire
Breastfeeding AWHONN supports breastfeeding as the optimal method of infant nutrition. AWHONN believes that women should be encouraged to breastfeed and receive instruction and support from the entire
Zika Virus. Fred A. Lopez, MD, MACP Richard Vial Professor Department of Medicine Section of Infectious Diseases
 Zika Virus Fred A. Lopez, MD, MACP Richard Vial Professor Department of Medicine Section of Infectious Diseases What is the incubation period for Zika virus infection? Unknown but likely to be several
Zika Virus Fred A. Lopez, MD, MACP Richard Vial Professor Department of Medicine Section of Infectious Diseases What is the incubation period for Zika virus infection? Unknown but likely to be several
Evaluation and Treatment of Neonatal Hyperbilirubinemia
 Evaluation and Treatment of Neonatal Hyperbilirubinemia KAREN E. MUCHOWSKI, MD, Naval Hospital Camp Pendleton Family Medicine Residency Program, Camp Pendleton, California Although neonatal jaundice is
Evaluation and Treatment of Neonatal Hyperbilirubinemia KAREN E. MUCHOWSKI, MD, Naval Hospital Camp Pendleton Family Medicine Residency Program, Camp Pendleton, California Although neonatal jaundice is
Prevention of Pertussis Among Pregnant & Post Partum Women and Their Infants. Marilyn Michels RN MSN CIC Kathleen Curtis MS RN
 Prevention of Pertussis Among Pregnant & Post Partum Women and Their Infants Marilyn Michels RN MSN CIC Kathleen Curtis MS RN Pertussis and Adults Pertussis (whooping cough) a poorly controlled vaccine-preventable
Prevention of Pertussis Among Pregnant & Post Partum Women and Their Infants Marilyn Michels RN MSN CIC Kathleen Curtis MS RN Pertussis and Adults Pertussis (whooping cough) a poorly controlled vaccine-preventable
Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over
 Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over 1. BMI - Documented in patients medical record on an annual basis up to age 74. Screen for obesity and offer counseling to encourage
Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over 1. BMI - Documented in patients medical record on an annual basis up to age 74. Screen for obesity and offer counseling to encourage
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor. No disclosures
 Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
4/15/2013. Maribeth Inturrisi RN MS CNS CDE Perinatal Diabetes Educator [email protected]
 Maribeth Inturrisi RN MS CNS CDE Perinatal Diabetes Educator [email protected] List the potential complications associated with diabetes during labor. Identify the 2 most important interventions essential
Maribeth Inturrisi RN MS CNS CDE Perinatal Diabetes Educator [email protected] List the potential complications associated with diabetes during labor. Identify the 2 most important interventions essential
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
ESCMID Online Lecture Library. by author
 Do statins improve outcomes of patients with sepsis and pneumonia? Jordi Carratalà Department of Infectious Diseases Statins for sepsis & community-acquired pneumonia Sepsis and CAP are major healthcare
Do statins improve outcomes of patients with sepsis and pneumonia? Jordi Carratalà Department of Infectious Diseases Statins for sepsis & community-acquired pneumonia Sepsis and CAP are major healthcare
Chapter 18. Blood Types
 Chapter 18 Blood Types Blood Types blood types and transfusion compatibility are a matter of interactions between plasma proteins and erythrocytes Karl Landsteiner discovered blood types A, B and O in
Chapter 18 Blood Types Blood Types blood types and transfusion compatibility are a matter of interactions between plasma proteins and erythrocytes Karl Landsteiner discovered blood types A, B and O in
 GUIDELINES FOR HOSPITALS WITH NEONATAL INTENSIVE CARE SERVICE : REGULATION 4 OF THE PRIVATE HOSPITALS AND MEDICAL CLINICS REGULATIONS [CAP 248, Rg 1] I Introduction 1. These Guidelines serve as a guide
GUIDELINES FOR HOSPITALS WITH NEONATAL INTENSIVE CARE SERVICE : REGULATION 4 OF THE PRIVATE HOSPITALS AND MEDICAL CLINICS REGULATIONS [CAP 248, Rg 1] I Introduction 1. These Guidelines serve as a guide
Hypoglycemia in the Newborn
 Hypoglycemia in the Newborn Shankar Narayan, Rajiv Aggarwal, Ashok K Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari Nagar, New Delhi
Hypoglycemia in the Newborn Shankar Narayan, Rajiv Aggarwal, Ashok K Deorari, Vinod K Paul Division of Neonatology, Department of Pediatrics All India Institute of Medical Sciences Ansari Nagar, New Delhi
ASSESSMENT AND MANAGEMENT OF NEONATAL JAUNDICE IN THE FIRST TWO WEEKS OF LIFE NEONATAL CLINICAL GUIDELINE
 ASSESSMENT AND MANAGEMENT OF NEONATAL JAUNDICE IN THE FIRST TWO WEEKS OF LIFE NEONATAL CLINICAL GUIDELINE Contents 2.1. Background 2.2. Communication and Consent 2.3. Recognition of significant Jaundice
ASSESSMENT AND MANAGEMENT OF NEONATAL JAUNDICE IN THE FIRST TWO WEEKS OF LIFE NEONATAL CLINICAL GUIDELINE Contents 2.1. Background 2.2. Communication and Consent 2.3. Recognition of significant Jaundice
Normal Pregnancy and Pain Management Case Study
 Normal Pregnancy and Pain Management Case Study Time: 1845 Heather Morris, RN, has just arrived to work her evening shift in Labor & Delivery. This is her 5th year as an RN in the unit. While waiting for
Normal Pregnancy and Pain Management Case Study Time: 1845 Heather Morris, RN, has just arrived to work her evening shift in Labor & Delivery. This is her 5th year as an RN in the unit. While waiting for
Guideline for staff involvement and responsibility with cord blood collection for stem cells (GL811)
") Guideline for staff involvement and responsibility with cord blood collection for stem cells (GL811) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical
Guideline for staff involvement and responsibility with cord blood collection for stem cells (GL811) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical
Reporting Adverse Events and Concerns at Stroger Hospital
 Reporting Adverse Events and Concerns at Stroger Hospital Case Pt on coumadin comes in for community acquired pneumonia and is started on levaquin After several days, you note a lot of bruising.. You realize
Reporting Adverse Events and Concerns at Stroger Hospital Case Pt on coumadin comes in for community acquired pneumonia and is started on levaquin After several days, you note a lot of bruising.. You realize
As you know, the CPT Editorial Panel developed two new codes to describe complex ACP services for CY 2015.
 December 30, 2014 SUBMITTED ELECTRONICALLY VIA http://www.regulations.gov Marilyn Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS
December 30, 2014 SUBMITTED ELECTRONICALLY VIA http://www.regulations.gov Marilyn Tavenner Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS
NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources
 NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources Key: DP = Documented Process N/D = Report numerator and denominator creating percent of use RPT = Report of data or information
NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources Key: DP = Documented Process N/D = Report numerator and denominator creating percent of use RPT = Report of data or information
Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64
 Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64 1. BMI - Documented in patients medical record on an annual basis. Screen for obesity and offer intensive counseling and behavioral
Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64 1. BMI - Documented in patients medical record on an annual basis. Screen for obesity and offer intensive counseling and behavioral
Assessment of Fetal Growth
 Assessment of Fetal Growth Unit / Trust: 1. INTRODUCTION The aim of this guideline template is to outline the methods used to assess fetal growth and the referral pathways utilising customised antenatal
Assessment of Fetal Growth Unit / Trust: 1. INTRODUCTION The aim of this guideline template is to outline the methods used to assess fetal growth and the referral pathways utilising customised antenatal
Detection of Newborns at Risk for Pathologic Hyperbilirubinemia: A Handheld End-Tidal CO Measurement Device For Quantification Of Hemolysis
 Detection of Newborns at Risk for Pathologic Hyperbilirubinemia: A Handheld End-Tidal CO Measurement Device For Quantification Of Hemolysis George F. Tidmarsh, MD, PhD Associate Professor, Pediatrics and
Detection of Newborns at Risk for Pathologic Hyperbilirubinemia: A Handheld End-Tidal CO Measurement Device For Quantification Of Hemolysis George F. Tidmarsh, MD, PhD Associate Professor, Pediatrics and
8/13/2014. Blood, Sweat (and Tears): Delayed Cord Clamping and Delivery Room Temperature. Delayed Cord Clamping
: Delayed Cord Clamping and Delivery Room Temperature. Delayed Cord Clamping") 8/13/2014 Blood, Sweat (and Tears): Delayed Cord Clamping and Delivery Room Temperature James F. Smith, Jr., MD Professor and Chair Obstetrics and Gynecology Creighton University School of Medicine The
8/13/2014 Blood, Sweat (and Tears): Delayed Cord Clamping and Delivery Room Temperature James F. Smith, Jr., MD Professor and Chair Obstetrics and Gynecology Creighton University School of Medicine The
Clinical Policy Title: Home uterine activity monitoring
 Clinical Policy Title: Home uterine activity monitoring Clinical Policy Number: 12.01.01 Effective Date: August 19, 2015 Initial Review Date: July 17, 2013 Most Recent Review Date: July 15, 2015 Next Review
Clinical Policy Title: Home uterine activity monitoring Clinical Policy Number: 12.01.01 Effective Date: August 19, 2015 Initial Review Date: July 17, 2013 Most Recent Review Date: July 15, 2015 Next Review
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NEONATAL INTENSIVE CARE UNIT: ADMISSION AND TRANSFER PROCEDURE AND ACUITY GUIDELINES Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE:
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NEONATAL INTENSIVE CARE UNIT: ADMISSION AND TRANSFER PROCEDURE AND ACUITY GUIDELINES Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE:
2) Anticipatory guidance for the breastfeeding infant and mother on the day of hospital discharge includes all of the following EXCEPT:
 Anticipatory guidance for the breastfeeding infant and mother on the day of hospital discharge includes all of the following EXCEPT:") Evaluation Tool Pre-test (with Answers) Section I: Knowledge 1) Hypoglycemia, both symptomatic and asymptomatic, is a common concern in healthy term breastfed neonates. While glucose monitoring should
Evaluation Tool Pre-test (with Answers) Section I: Knowledge 1) Hypoglycemia, both symptomatic and asymptomatic, is a common concern in healthy term breastfed neonates. While glucose monitoring should
Intro Who should read this document 2 Key Messages 2 Background 2
 Classification: Policy Lead Author: Nathan Griffiths, Consultant Nurse Paediatric Emergency Medicine Additional author(s): N/A Authors Division: Salford Healthcare Unique ID: DDCPan04(14) Issue number:
Classification: Policy Lead Author: Nathan Griffiths, Consultant Nurse Paediatric Emergency Medicine Additional author(s): N/A Authors Division: Salford Healthcare Unique ID: DDCPan04(14) Issue number:
Immunohematology. Immunohematology. Blood Group Antigens
 Immunohematology Immunohematology Jeffrey S. Jhang, MD Assistant Director, Transfusion Medicine Demonstration of red cell antigen-red cell antibody reactions is the key to immunohematology Combination
Immunohematology Immunohematology Jeffrey S. Jhang, MD Assistant Director, Transfusion Medicine Demonstration of red cell antigen-red cell antibody reactions is the key to immunohematology Combination
Feeding The Late Preterm Infant
 Feeding The Late Preterm Infant Richard J. Schanler, M.D. Neonatal-Perinatal Medicine, Schneider Children s Hospital at North Shore, Manhasset, NY and Albert Einstein College of Medicine, Bronx, NY October
Feeding The Late Preterm Infant Richard J. Schanler, M.D. Neonatal-Perinatal Medicine, Schneider Children s Hospital at North Shore, Manhasset, NY and Albert Einstein College of Medicine, Bronx, NY October
Quality of Birth Certificate Data. Daniela Nitcheva, PhD Division of Biostatistics PHSIS
 Quality of Birth Certificate Data Daniela Nitcheva, PhD Division of Biostatistics PHSIS Data Quality SC State Law requires that you file the birth certificate within 5 days of a child s birth. Data needs
Quality of Birth Certificate Data Daniela Nitcheva, PhD Division of Biostatistics PHSIS Data Quality SC State Law requires that you file the birth certificate within 5 days of a child s birth. Data needs
11.0 SERVICE DEPARTMENTS
 Horizon NJ Health is available to assist you in providing health care services to our members. This section describes each of the service departments by function. 11.1 Professional Contracting & Servicing
Horizon NJ Health is available to assist you in providing health care services to our members. This section describes each of the service departments by function. 11.1 Professional Contracting & Servicing
Your Baby s Care Team
 UW MEDICINE PATIENT EDUCATION Your Baby s Care Team For parents of NICU infants Parents and Family You and your baby are the center of the NICU care team. As parents, you will give input and take part
UW MEDICINE PATIENT EDUCATION Your Baby s Care Team For parents of NICU infants Parents and Family You and your baby are the center of the NICU care team. As parents, you will give input and take part
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
QUICK REFERENCE TO BLOOD BANK TESTING
 QUICK REFERENCE TO BLOOD BANK TESTING All Blood bank Tests are performed on demand 24 hours a day, 7 days a week. Feto/Maternal Bleed Quantitation estimates will be available within 4 hours of blood bank
QUICK REFERENCE TO BLOOD BANK TESTING All Blood bank Tests are performed on demand 24 hours a day, 7 days a week. Feto/Maternal Bleed Quantitation estimates will be available within 4 hours of blood bank
Quality standard Published: 11 June 2015 nice.org.uk/guidance/qs89
 Pressure ulcers Quality standard Published: 11 June 2015 nice.org.uk/guidance/qs89 NICE 2015. All rights reserved. Contents Introduction... 6 Why this quality standard is needed... 6 How this quality standard
Pressure ulcers Quality standard Published: 11 June 2015 nice.org.uk/guidance/qs89 NICE 2015. All rights reserved. Contents Introduction... 6 Why this quality standard is needed... 6 How this quality standard