Grand Rounds: Can progesterone prevent preterm birth?
|
|
|
- Ruth Watson
- 7 years ago
- Views:
Transcription
1 Grand Rounds: Can progesterone prevent preterm birth? The research says that the drug can benefit women at risk, but how exactly should these data be applied in clinical practice? Two experts offer some valuable insights. Oct 1, 2005 By:Joanne Armstrong, MD, MPH, Michael Nageotte, MD Contemporary OB/GYN No one has to remind ob/gyns that preterm birth (PTB) takes a heavy toll both medically and financially on the American public. Unfortunately, in recent decades clinicians have had little success is reining in this problem, which is no doubt why so much attention has been given to recent research on the preventative effects of 17-alpha-hydroxyprogesterone caproate (17P). But in order to achieve the most benefit from this therapy, several educational and logistical barriers need to be addressed, and both physicians and patients need to understand more about the appropriate use of the medication and compliance support with the therapy. With appropriate planning, overcoming these obstacles is possible within an organized education and support network. (1 of 13)10/11/ :48:17 p.m.

2 Appreciating the scope of the problem Preterm birth, birth prior to 37 completed weeks of pregnancy, complicates 12.3% of all births in the United States annually. 1 In 2002, that translated into an estimated 480,000 preterm infants. Although advances in neonatal care have improved survival for these newborns, the rate of prematurity has steadily increased over the past three decades. 1,2 The incidence of delivery before 37 weeks' gestation increased from 9.4% of live births in 1981 to 11.0% in 1994 and 12.3% in ,2 These increases are attributed to increases in the multiple birth rate, although PTB is also increasing among singleton deliveries. 1 The rate of PTB in black women is nearly double the rate in white women. 1 National statistics indicate that PTB is the leading cause of perinatal mortality and morbidity in infants without birth defects. Prematurity causes an estimated 70% of all neonatal deaths of nonanomalous infants in the US. 3 Mortality is directly correlated with gestational age at delivery. The mortality rate for infants born at less than 32 weeks is almost 70 times the rate of a term infant (2.6 per 1,000 live births). 4 And for infants born less than 37 weeks it's 15 times the term infant rate. Of course, morbidity is also a major concern, especially for infants born at less than 32 weeks' gestation. Complications include respiratory distress syndrome, intraventricular hemorrhage, sepsis, necrotizing enterocolitis, and cerebral palsy. Preterm infants are also at risk for associated medical conditions extending into childhood and adulthood. One prospective study found that 25% of very premature infants have significant long-term neuro-developmental impairments not improved by educational intervention. 5 The extent of cognitive impairment extending into childhood for infants born at less than 26 weeks' gestation has been underestimated. New estimates suggest that 41% of these extremely preterm infants have serious cognitive deficits at 6 years of age. 6,7 In addition to the devastating toll on infant mortality and morbidity, prematurity exacts a heavy financial cost on the US health-care system. In 2001 alone, charges for hospital stays for infants with any diagnosis of prematurity were approximately $13.6 billion or about 50% of all birth-related spending. 8 Researchers have estimated that prematurity and low birthweight combined accounted for 35% of all direct infant care expenditures in the US. 9 Aetna, a national health benefits company serving 13.7 million Americans and covering over 140,000 deliveries a year, estimates that the cost of care through the first year of life for infants born at less than 37 weeks' gestation is $34,000 and for infants born at less than 32 weeks' gestation is $119, This excludes the associated maternal care costs. By comparison, the average cost of care through the first year of life for a term birth is $1,373. The financial cost of prematurity for the Medicaid population is no doubt greater because the proportion of births that are preterm is greater. Understanding risk factors for spontaneous preterm birth (2 of 13)10/11/ :48:17 p.m.

3 Preterm births are generally considered to be either "spontaneous" or "indicated." Spontaneous PTBs are initiated by spontaneous preterm labor with intact fetal membranes or preterm premature rupture of membranes (PPROM). Indicated PTBs result from either induction of labor or cesarean delivery without labor, most commonly in response to maternal complications of pregnancy such as hypertensive disorders or diabetes or fetal complications such as growth restriction or placental bleeding. Of all PTBs, about 20% are indicated while 80% are unanticipated or spontaneous. 11 As spontaneous and indicated PTB have different clinical presentations and probably different underlying causes as well, interventions to prevent one may not prevent the other. While many demographic characteristics are associated with PTB, traditional risk scoring systems do not predict PTB very accurately. 12 In fact, over 50% of women who have a spontaneous PTB don't have any identifiable risk factors. 13 The risk factor most consistently shown to predict PTB is history of a prior PTB. The estimated risk of having a subsequent PTB if a prior birth was preterm ranges from 15% to 80%, depending on the presence of other risk factors. The number of prior PTBs influences the risk of subsequent PTB. For example, women with one prior PTB are four times more likely to deliver another preterm infant and women with two prior PTBs have a sixfold increased risk of delivering preterm compared to multiparous women with no prior PTBs. 14 For African-American women, a two- to fourfold increased risk results in rates of 35% to 70% of recurrent PTB. 15 Additionally, the lower the gestational age of a prior spontaneous PTB, the greater the likelihood of subsequent PTB. For example, women who had a PTB at 23 to 27 weeks' gestation in the past had a 27.1% chance of delivering at less than 37 weeks in the current pregnancy. The corresponding probabilities when the prior delivery was at 28 to 34 weeks and 35 to 36 weeks were 24.0% and 20.9%. In comparison, women whose prior births occurred only at term had an 8.8% probability of delivering preterm in the current pregnancy. 16 How do you prevent preterm births? Efforts to avert a PTB can be categorized as primary, secondary, and tertiary prevention. 17 Primary prevention aims to provide prenatal care to the general population with the goal of preventing disease. Secondary prevention provides health services to high-risk patients who have not yet presented with signs or symptoms 17P would fall into this category. Tertiary prevention offers health services to patients after a disease is diagnosed with the intended goal of avoiding complication of the disease. While tertiary interventions such as antepartum corticosteroid therapy, and maternal and neonatal transport are effective, others are less clearly beneficial. For example, antibiotics have been shown to have benefits in the setting of PPROM 18,19 but not in women in preterm labor with intact membranes. 20 Tocolytics are effective at prolonging pregnancy for at least 48 hours, but their impact on neonatal morbidity and mortality appears minimal (3 of 13)10/11/ :48:17 p.m.

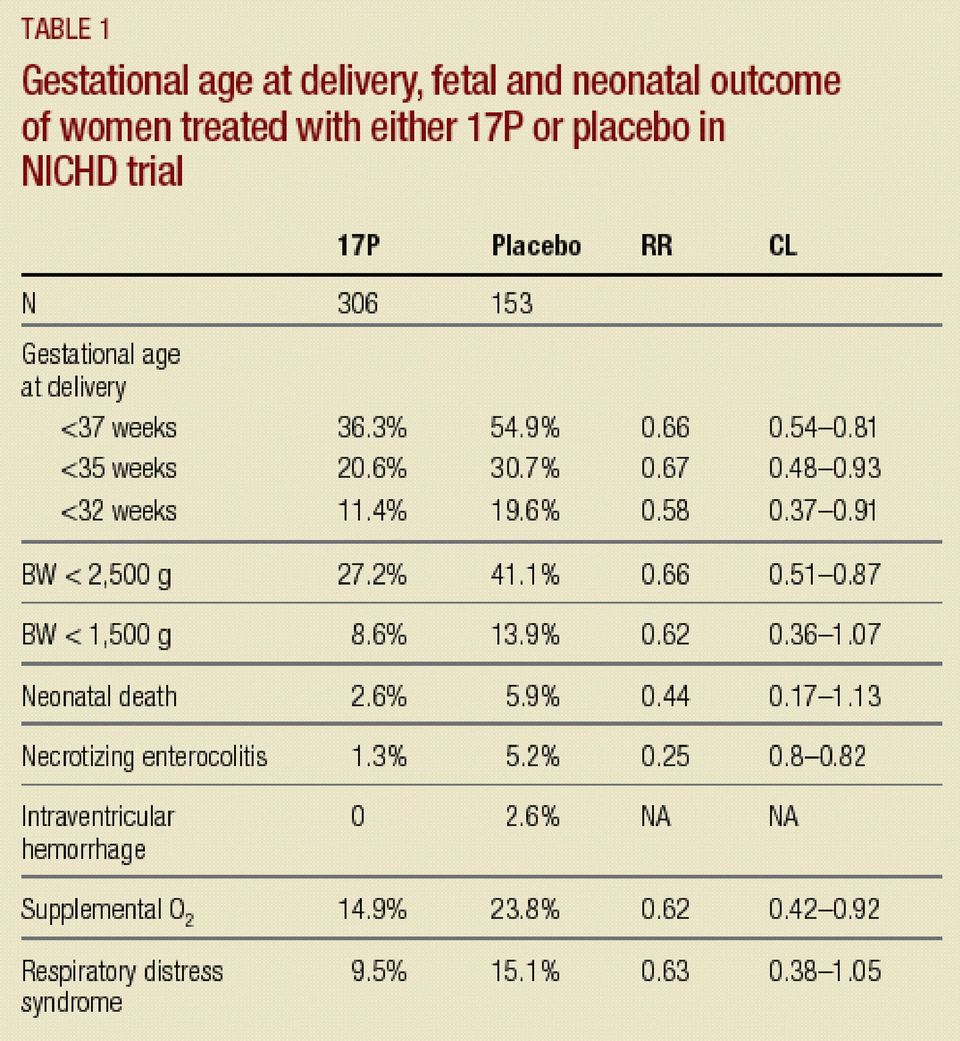
4 There are few primary or secondary treatments known to be effective for PTB, but several that have proven disappointing, including the provision of enhanced prenatal care, 21,22 psychosocial support, 23 nutritional supplementation, 17 ambulatory tocodynamometry, 24 prophylactic bed rest in twin pregnancy, 25 and screening and treatment of genital tract infections in asymptomatic women. 26 Using 17P to reduce the risk of recurrent PTB, on the other hand, is the first approach to secondary prevention that has proven effective in a randomized placebo-controlled trial. Reviewing the research on 17-alpha-hydroxyprogesterone 17P is a naturally occurring metabolite of progesterone. Both are produced in large amounts in human pregnancy; neither has androgenic activity. As long ago as 1964, progesterone's ability to prevent "prematurity" was described in several small clinical trials. A meta-analysis published in 1989 of 15 randomized controlled trials (RCTs) conducted between 1953 and 1985 involving 819 women treated with several different progestins found no significant reduction in the rate of PTB. 27 However, a subsequent meta-analysis of seven double-blind RCTs of women at high risk of PTB found a significant reduction in PTB in pregnancies that were treated specifically with 17P. 28 In 1998, the National Institute of Child Health and Human Development (NICHD), Maternal Fetal Medicine Units (MFMU) Network conducted an RCT to test the hypothesis that weekly intramuscular administration of 250 mg of 17P started at 15 to 20 completed weeks' gestation and continued through 36 completed weeks of pregnancy would reduce the risk of preterm birth in women who have previously experienced a spontaneous singleton preterm delivery. 29 Women eligible for the trial included those with a prior singleton spontaneous PTB between 20 and 37 weeks' gestation, singleton gestation in current pregnancy, and enrolled from 15 to 20 weeks of pregnancy. Women with anomalous fetuses, multiple gestations, planned or current cervical cerclage, and women on heparin or progesterone in the current pregnancy were excluded. There were 1,039 women eligible to participate in the trial, of whom 463 (44%) enrolled; 59% were African-American. Women randomized to progesterone had a significantly lower rate of recurrent PTB at less than 37 weeks, less than 35 weeks, and less than 32 weeks of gestation than women treated with placebo (see Table 1). The benefit was seen for all racial groups. Additionally the infants of women treated with 17P had significantly fewer complications, including necrotizing enterocolitis, and the need for supplemental oxygen. A sub-analysis of the NICHD data found that 17P prolonged pregnancy regardless of gestational age of the qualifying birth. The greatest benefit was seen in women with a prior spontaneous PTB at early gestational ages (less than 34 completed weeks). 30 Table 1. Gestational age at delivery, fetal and neonatal outcome of women treated with either 17P or placebo in (4 of 13)10/11/ :48:17 p.m.

5 Intramuscular progesterone was generally well-tolerated in the NICHD NICHD trial trial. Over 92% of women who started on the drug completed the trial. Although 50% reported some side effects, all were mild including local injection site reactions, soreness, swelling, or bruising. Adverse fetal effects did not differ significantly between 17P and placebo groups and no predominant defect was observed. A second, smaller RCT by da Fonseca and associates in 2003 reported on the efficacy of progesterone vaginal suppositories in high-risk women treated between 24 and 34 weeks' gestation, and found that PTBs were significantly reduced, from 28.5% to 13.8% for births before 37 weeks, and from 18.6% to 2.8% for births before 34 weeks in the placebo versus the progesterone groups, respectively. 31 This trial was complicated by a heterogeneous patient population (including women with a history of spontaneous prior PTB, uterine malformations, and prophylactic cervical cerclage placement in the current pregnancy); the relatively small number of participants (72 assigned to progesterone and 70 to placebo); and a relatively high rate of women who were lost to follow-up or dropped out of the study. Applying the research 'in the trenches' While the NICHD research represents a potential breakthrough, let's take a closer look at how it might apply in day-to-day practice. First, only 44% of eligible women consented to participate in the study. Those who did agree to enroll had a particularly high risk for recurrent PTB, as evidenced by the 55% rate of PTB in the placebo group. Although that rate is not surprising given their mean gestational age at first PTB (31 weeks) and the large percentage of enrollees with two or more prior PTBs (32%), these women may not have been representative of the population with prior PTB as a whole. Also bear in mind that the investigators did not have permission to collect information on those who declined to participate. [Paul Meis, personal communication January 4, 2005.] Second, the rate of PTB in the intervention group was still high (36%), which means that 17P doesn't provide complete protection. Nonetheless, the authors estimated that in this very highrisk population, only 12 women with prior PTB would need to be treated to prevent one PTB at less than 32 weeks and 5 to 6 women treated to prevent one PTB at less than 37 weeks. A recent estimate of the impact of 17P on the national prematurity rate predicted that 10,000 PTBs could be prevented with a resultant decrease in the national prematurity rate by 2%. 32 Although the reduction in the PTB rate is modest in absolute terms, the impact per case affected is significant. Following publication of the NICHD trial, the ACOG Committee on Obstetric Practice published an opinion stating that 17P offers "apparent benefits in a high-risk population" and recommended that women who had had a previous preterm delivery be considered for treatment. But ACOG also said that the ideal formulation, optimal route of delivery, and longterm safety are still unknown (5 of 13)10/11/ :48:17 p.m.

6 What's the mechanism of action? We still don't understand the mechanism of action by which 17P prevents PTB. It's possible that the drug works by relaxing uterine muscle; it may have anti-inflammatory effects; or it may affect the maternal-fetal pituitary/adrenal axis. Since the mechanism of action is not known, it is best to use only 17-alpha-hydroxyprogesterone, and to use it only in women for whom its benefit has been demonstrated (i.e., women with a prior spontaneous PTB). 17P has been studied in several animal species without evidence of teratogenicity. Likewise an extensive review of 17P in humans has failed to find teratogenic effects. 34 A meta-analysis of 186 articles by Raman-Wilms and colleagues showed no association between first-trimester exposure to sex hormones and genital malformations. 35 And studies with an average of 11.5 years of follow-up also found no anomalies. 36 The MFMU Network is currently conducting a follow-up study of the children born in the trial of 17P to prevent recurrent preterm delivery to evaluate their health status in the preschool years. Is the drug being fully utilized? Despite the encouraging news for recent RCTs, few ob/gyns seem to be using 17P. A survey of board-certified maternal-fetal medicine (MFM) specialists in the US conducted 6 months after the publication of the NICHD trial, for instance, found that only 38% of respondents were using the drug. Among those who were not, 25% said they were concerned with drug efficacy, 12% were concerned with safety, 12% were concerned with liability, and 81% were awaiting more data. 37 A follow-up survey of the SMFM membership to determine adoption trends is planned. The limited use of 17P indicated in this survey has also been observed in broad practice settings. Aetna, for example, initiated coverage of 17P for this indication in November 2003, following the publication of the NICHD trial and the ACOG Committee Opinion. Aetna's data monitoring systems revealed, however, that fewer than one prescription per month for the medication was written for Aetna members in the subsequent 6 months. A subsequent analysis was conducted by interviewing participating physicians, members of professional organizations, pharmacy partners, and others. In addition to those cited by the survey, other identified obstacles to expanded use included the lack of patient and physician awareness of the literature and eligibility criteria; lack of availability of a consistent and reliable supply of medication; lack of reimbursement by commercial health plans and Medicaid, and concern about patient adherence and support required for weekly injections. Patient and provider education. Little patient and provider information has been disseminated on the potential value of 17P. A news release was published on the ACOG Web site in October 2003 describing the study findings. 34 Electronic searches of content in news media outlets also reveal relatively few "hits" when searched for key words progesterone, 17 (6 of 13)10/11/ :48:17 p.m.

7 progesterone, and preterm birth. 38 We don't fully understand why so little attention has been given to this subject but the barriers discussed further on in this article may be contributing factors. Drug production and distribution. In the US, manufactured medications are regulated by the FDA in accordance with Good Manufacturing Practice (GMP) standards. By contrast, sterile compounded preparations like 17P (which are the combination of two of more finished dosage medications by a pharmacy rather than a manufacturer) are produced in accordance with requirements of the Federal Food, Drug and Cosmetic Act, not GMP standards. Oversight and regulation is the responsibility of State Boards of Pharmacy. Quality issues related to preparation, storage, and dispensing of compounded medications as a class are welldocumented and have resulted in product recalls, patient injury, and even death. 39 A 2002 national survey by the American Society for Health-System Pharmacists indicated that few pharmacies are equipped with the controlled compounding environments needed for dispensing sterile preparations. The survey also documented that many pharmacists are not performing critical quality assurance checks, such as end-product testing to ensure accuracy and consistency of product. 40 Efforts to improve the quality of pharmacy-prepared sterile preparations have been on-going. The first official and enforceable sterile preparation compounding requirements in the US, outlined in the US Pharmacopeias (USP) chapter 797, was made enforceable on January 1, The guidelines now set standards for sterile product compounding. The guidelines apply to all practice settings in which sterile preparations are compounded, including specialty pharmacies, hospitals, physician offices, or ambulatory care clinics. The USP guidelines may be adopted and enforced by state boards of pharmacy and surveyable by accreditation organizations such as the Joint Commission Accreditation of Healthcare Organizations (JCAHO). Some states, such as Missouri, have now adopted standards that are more stringent than the USP. Some health plans, such as Aetna, require compounding pharmacies to comply with the new USP guidelines. Pharmacies, unlike drug manufacturing organizations, are permitted to prepare a supply of compounded medications to meet the specific demands of their patients. They are prohibited from compounding a quantity that could be used by another pharmacy for their patients or for sale to physicians to dispense to their patients. Additionally, patient-specific compounded products prepared by a pharmacy may be shipped across state lines only if the pharmacy has an "out of state" license to sell pharmaceuticals in that state. At the present time, there are only a limited number of pharmacies that meet these requirements. (The drug is available from Freedom Drug, 12 Kent Way, Bayfield, MA 01922, Phone: ) Reimbursement by commercial health plans and Medicaid. A few commercial health plans are providing coverage for 17P as well as the administration of the medication. Aetna, for example, initiated coverage for 17P shortly after the NICHD trial and the ACOG Committee Opinion were published. Government plans like Medicaid, however, generally do not cover the (7 of 13)10/11/ :48:17 p.m.

8 medication for their insured members. One third of all live births in the US are reimbursed through Medicaid. This population probably has a higher rate of prematurity and extreme prematurity than the general population (due to the higher rate of risk factors for prematurity among Medicaid recipients including the African-American race, poverty, cigarette smoking, young maternal age, and unmarried status) and are likely to benefit the most from the medication. Although most Medicaid plans do not currently cover the cost of this therapy, the relatively low cost of approximately $100 for an entire treatment course may prompt more plans to cover it in the future. Patient adherence and challenge to self-administration. 17P is administered weekly as an IM injection. In the NICHD trial, patients generally made weekly clinic visits. A requirement for weekly visits may be a barrier to administration of treatment. Liability issues. Some clinicians are not using 17P because they're concerned about liability. Although 60% of non-user MFM specialists in the above survey were "not or minimally concerned" with the 17P safety, 12% of non-users indicated liability concerns as a barrier to use. 37 ACOG has specifically advised "... further studies are needed to evaluate the use of progesterone in patients with other high-risk obstetric factors, such as multiple gestations, short cervical length, or positive test results for cervicovaginal fetal fibronectin. When progesterone is used, it is important to restrict its use to only women with a documented history of a previous spontaneous birth at less than 37 weeks' gestation because unresolved issues remain, such as optimal route of drug delivery and long-term safety of the drug..." 33 Despite this recommendation, the survey indicated 20% of current 17P prescribers said they use 17P for indications not described in the NICHD trial, including women with a short cervix or symptomatic women. Conversely, there may also be a liability concern associated with not offering 17P to eligible women. The hassle factor. When you combine the lack of information and education about the research findings with an uncertain or inconsistent supply of medication, lack of coverage or inconsistency of coverage by private and public payers, the logistics of administering the medication, and the compliance factor, it's understandable that many physicians don't want to deal with the hassle. Unfortunately, these obstacles mean many eligible patients won't benefit from the drug. A system-wide approach to overcoming obstacles NIH and ACOG have the opportunity to educate caregivers and patients regarding the potential benefits of and indications for effective new treatments. They can work with industry to encourage the widespread availability of an adequate supply of medication, and can support the needed long-term evaluations of safety and efficacy of such treatments. (8 of 13)10/11/ :48:17 p.m.

9 Health-care organizations also have an opportunity to take an active role in promoting effective treatment for appropriate candidates. Aetna, for example, through a dedicated Women's Health unit, has developed a comprehensive initiative to: (1) increase member and physician awareness of the published literature and potential value of the therapy; (2) ensure access to a reliable and consistent supply of the medication for Aetna members; and (3) develop a case management program for women eligible for 17P therapy in accordance with the NICHD evidence. The insurer's experience in implementing this program may be useful for other companies contemplating this issue. As a first step, Aetna surveyed compounding pharmacies within its pharmacy network to identify one that documented compliance with the USP guidelines and worked with that vendor to ensure that members who needed it would have an adequate supply of 17P. They also developed a tracking mechanism to monitor progesterone usage. A comprehensive educational outreach program was then developed for obstetrical care providers and neonatologists, to educate them about the research findings, indications for 17P therapy, and the process to obtain the medication. Women who elect 17P are offered a single home nurse visit to teach the woman or a family member how to administer the medication. Additionally, women are offered compliance support services by obstetrical case managers throughout their pregnancies. Case management also includes the coordination of services for preterm labor education or specialty care. Through May 2005, 82 of 263 identified eligible women received 17P through this Aetna program. The most common reason for not using 17P was uncertainty by physicians and their patients about the indications for and availability of the drug. While enrollment in the Aetna program is too small to draw statistically significant conclusions, the anecdotal information is instructive. To date, patient and physician feedback has been overwhelmingly positive. Preliminary experience with this program indicates that physicians and patients generally have been unaware of the literature, potential benefits, and eligibility criteria, and are uncertain about how to obtain the medication. In addition, physicians have used 17P in ways not supported by the literature including as treatment for active preterm labor, or for multiple gestations, history of spontaneous abortions without prior PTBs, or uterine abnormalities. Most members participating in this program have been able to administer the medication at home with the assistance of a family member and the aid of a single home nurse visit. It may be more difficult, however, for women with less support, such as young Medicaid patients, to self-administer medication, although this has not been formally evaluated. Despite these positive developments, we remain uncertain about a number of issues. The NICHD trial didn't include women with multifetal gestation, short cervical length, and other women at known risk for PTB, so 17P is not currently recommended for them. A NICHD trial evaluating the drug in multifetal pregnancy is ongoing. It is also not known whether other progestins or less invasive forms of administration of the drug are equally effective. (9 of 13)10/11/ :48:17 p.m.

10 We now know that 17P can prevent a significant number of PTBs in women who have had a prior spontaneous PTB. While promising, much is still unanswered about the mechanism of action and other population groups that may benefit. With these data in hand, it's important for physicians to be educated about the appropriate applications of the medication and it's important that they discuss it with women who may benefit. Of course, clinicians need to exercise caution in clinical settings not covered by the research. And finally, access to the medication and coordination of services necessary to support compliance is essential to overcoming the logistical barriers to its use. With appropriate planning, such obstacles can often be overcome. ACKNOWLEDGMENT The authors would like to thank Mark Klebanoff, MD, MPH, at the National Institute of Child Health and Human Development for his thoughtful contributions and review of the manuscript. REFERENCES 1. Hamilton BE, Martin JA, Sutton PD, et al. Births: preliminary data for Natl Vital Stat Rep. 2004;53(9): Ventura SJ, Martin JA, Mathews TJ, et al. Advance report of final natality statistics, Monthly Vital Statistics Report. 1996;44(11 Suppl). Hyattsville, Maryland: National Center for Health Statistics, Guyer B, Martin JA, MacDorman MF, et al. Annual summary of vital statistics Pediatrics. 1997;100: March of Dimes Birth Defects Foundation. Available at: Accessed July 11, Hack M, Flannery DJ, Schluchter M, et al. Outcomes in young adulthood for very-low-birthweight infants. N Engl J Med. 2002;346: Wood NS, Marlow N, Costeloe K, et al. Neurologic and developmental disability after extremely preterm birth. N Engl J Med. 2000;343: Marlow N, Wolke D, Bracewell MA, et al. Neurologic and developmental disability at six years of age after extremely preterm birth. N Engl J Med. 2005;352: Peristats. March of Dimes Birth Defects Foundation Website. Available at: marchofdimes.com/peristats. Accessed July 11, (10 of 13)10/11/ :48:17 p.m.

11 9. Lewit EM, Baker LS, Corman H, et al. The direct cost of low birth weight. Future Child. 1995;5: Aetna, Integrated Informatics, Meis PJ, Michielutte R, Peters TJ, et al. Factors associated with preterm birth in Cardiff, Wales. II. Indicated and spontaneous preterm birth. Am J Obstet Gynecol. 1995;173: Shiono PH, Klebanoff MA. A review of risk scoring for preterm birth. Clin Perinatol. 1993;20: Mercer BM, Goldenberg RL, Das A, et al. The preterm prediction study: a clinical risk assessment system. Am J Obstet Gynecol. 1996;174: Bakketeig LS, Hoffman HJ. Epidemiology of preterm birth: results from a longitudinal study of births in Norway. In: Elder MG, Hendricks CH, eds. Preterm Labor. London; Boston: Butterworths; 1981: Adams MM, Elam-Evans LD, Wilson HG, et al. Rates of and factors associated with recurrence of preterm delivery. JAMA. 2000;283: Mercer BM, Goldenberg RL, Moawad AH, et al. The preterm prediction study: effect of gestational age and cause of preterm birth on subsequent obstetric outcome. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol. 1999;181(5 Pt 1): Goldenberg RL, Rouse DJ. Prevention of premature birth. N Engl J Med. 1998;339: Mercer BM, Miodovnik M, Thurnau GR, et al. Antibiotic therapy for reduction of infant morbidity after preterm premature rupture of the membranes. A randomized, controlled trial. National Institute of Child Health and Human Development Maternal-Fetal medicine Units Network. JAMA. 1997;278: Kenyon SL, Taylor DJ, Tarnow-Mordi W, et al. Broad-spectrum antibiotics for preterm, prelabour rupture of fetal membranes: the ORACLE I randomised trial. ORACLE Collaborative Group. Lancet. 2001;357: Kenyon SL, Taylor DJ, Tarnow-Mordi W, et al. Broad-spectrum antibiotics for spontaneous preterm labour: the ORACLE II randomised trial. ORACLE Collaborative Group. Lancet. 2001;357: Multicenter randomized, controlled trial of a preterm birth prevention program. Collaborative (11 of 13)10/11/ :48:17 p.m.

12 Group on Preterm Birth Prevention. Am J Obstet Gynecol. 1993;169: Main DM, Gabbe SG, Richardson D, et al. Can preterm deliveries be prevented? Am J Obstet Gynecol. 1985;151: Villar J, Farnot U, Barros F, et al. A randomized trial of psychosocial support during highrisk pregnancies. The Latin American Network for Perinatal and Reproductive Research. N Engl J Med. 1992;327: Dyson DC, Danbe KH, Bamber JA, et al. Monitoring women at risk for preterm labor. N Engl J Med. 1998;338: Crowther CA, Verkuyl DA, Neilson JP, et al. The effects of hospitalization for rest on fetal growth, neonatal morbidity and length of gestation in twin pregnancy. Br J Obstet Gynaecol. 1990;97: Riggs MA, Klebanoff MA. Treatment of vaginal infections to prevent preterm birth: a metaanalysis. Clin Obstet Gynecol. 2004;47: Goldstein P, Berrier J, Rosen S, et al. A meta-analysis of randomized control trials of progestational agents in pregnancy. Br J Obstet Gynaecol. 1989;96: Keirse MJ. Progestogen administration in pregnancy may prevent preterm delivery. Br J Obstet Gynaecol. 1990;97: Meis PJ, Klebanoff M, Thom E, et al. Prevention of recurrent preterm delivery by 17 alphahydroxyprogesterone caproate. N Engl J Med. 2003;348: Spong CY. Progesterone for prevention of recurrent preterm birth: impact of gestational age at prior delivery. Am J Obstet Gynecol. 2004;191:S da Fonseca EB, Bittar RE, Carvalho MH, et al. Prophylactic administration of progesterone by vaginal suppository to reduce the incidence of spontaneous preterm birth in women at increased risk: a randomized placebo-controlled double-blind study. Am J Obstet Gynecol. 2003;188: Petrini JR, Callaghan WM, Klebanoff M, et al. Estimated effect of 17 alphahydroxyprogesterone caproate on preterm birth in the United States. Obstet Gynecol. 2005;105: American College of Obstetricians and Gynecologists. Use of progesterone to reduce preterm birth. ACOG Committee Opinion No. 291, November (12 of 13)10/11/ :48:17 p.m.

13 34. Schardein JL. Congenital abnormalities and hormones during pregnancy: a clinical review. Teratology. 1980;22(3): Raman-Wilms L, Tseng AL, Wighardt S, et al. Fetal genital effects of first-trimester sex hormone exposure: a meta-analysis. Obstet Gynecol. 1995;85: Resseguie LJ, Hick JF, Bruen JA, et al. Congenital malformations among offspring exposed in utero to progestins, Olmsted County, Minnesota, Fertil Steril. 1985;43: Ness A, Baxter J, Hyslop T, et al. Progesterone use among board-certified maternal-fetal specialists in the United States. J Repro Medicine. 2005; in press. 38. Factiva search, January 9, The ASHP Discussion guide for compounding sterile preparations. Summary and implementation of USP Chapter <797>. American Society for Health-System Pharmacists. Available at: Accessed July 11, Myers CE. Needed: serious attention to sterile products. Am J Health Syst Pharm. 1996;53: (13 of 13)10/11/ :48:17 p.m.

14
In This Issue: Summer 2012. Tell Us What You Think... 1
 Summer 2012 Important information from UnitedHealthcare Community Plan for physicians and other health care professionals and facilities serving New Jersey FamilyCare/Medicaid members Physician Satisfaction
Summer 2012 Important information from UnitedHealthcare Community Plan for physicians and other health care professionals and facilities serving New Jersey FamilyCare/Medicaid members Physician Satisfaction
Clinical Policy Title: Home uterine activity monitoring
 Clinical Policy Title: Home uterine activity monitoring Clinical Policy Number: 12.01.01 Effective Date: August 19, 2015 Initial Review Date: July 17, 2013 Most Recent Review Date: July 15, 2015 Next Review
Clinical Policy Title: Home uterine activity monitoring Clinical Policy Number: 12.01.01 Effective Date: August 19, 2015 Initial Review Date: July 17, 2013 Most Recent Review Date: July 15, 2015 Next Review
Strategies for the Prevention of Prematurity Progesterone. Cervical Screening, Cerclage, and Pessaries
 Strategies for the Prevention of Prematurity Progesterone. Cervical Screening, Cerclage, and Pessaries Thomas J. Garite, M.D. Professor Emeritus, University of CA Irvine Editor Emeritus, American Journal
Strategies for the Prevention of Prematurity Progesterone. Cervical Screening, Cerclage, and Pessaries Thomas J. Garite, M.D. Professor Emeritus, University of CA Irvine Editor Emeritus, American Journal
Rural Health Advisory Committee s Rural Obstetric Services Work Group
 Rural Health Advisory Committee s Rural Obstetric Services Work Group March 15 th webinar topic: Rural Obstetric Patient and Community Issues Audio: 888-742-5095, conference code 6054760826 Rural Obstetric
Rural Health Advisory Committee s Rural Obstetric Services Work Group March 15 th webinar topic: Rural Obstetric Patient and Community Issues Audio: 888-742-5095, conference code 6054760826 Rural Obstetric
North Carolina Medicaid Special Bulletin
 North Carolina Medicaid Special Bulletin An Information Service of the Division of Medical Assistance Visit DMA on the web at http://www.ncdhhs.gov/dma Number 1 (Revised 8/23/11) July 2011 Pregnancy Medical
North Carolina Medicaid Special Bulletin An Information Service of the Division of Medical Assistance Visit DMA on the web at http://www.ncdhhs.gov/dma Number 1 (Revised 8/23/11) July 2011 Pregnancy Medical
Preterm Labor, the Cervix, and Progesterone. The Cervix. The Cervix. Disclosure of Conflict of Interest. 2nd Trimester Cervical Length
 Disclosure of Conflict of Interest Preterm Labor, the Cervix, and Progesterone John C. Hobbins, M.D. Professor of Obstetrics and Gynecology University of Colorado Health Sciences Center Denver, CO Dr.
Disclosure of Conflict of Interest Preterm Labor, the Cervix, and Progesterone John C. Hobbins, M.D. Professor of Obstetrics and Gynecology University of Colorado Health Sciences Center Denver, CO Dr.
Epidemiology 521. Epidemiology of Maternal and Child Health Problems. Winter / Spring, 2010
 Extended MPH Degree Program School of Public Health Department of Epidemiology University of Washington Epidemiology 521 Epidemiology of Maternal and Child Health Problems Winter / Spring, 2010 Instructor:
Extended MPH Degree Program School of Public Health Department of Epidemiology University of Washington Epidemiology 521 Epidemiology of Maternal and Child Health Problems Winter / Spring, 2010 Instructor:
Innovative use of Neonatal Nurse Practitioners in Rural Hawaii
 Innovative use of Neonatal Nurse Practitioners in Rural Hawaii Petri Pate Pieron, MSN, MPH, APRN Rx, CPNP, NNP Presentation was supported by NIH 1 R25 RR019321 Clinical Research Education and Career Development
Innovative use of Neonatal Nurse Practitioners in Rural Hawaii Petri Pate Pieron, MSN, MPH, APRN Rx, CPNP, NNP Presentation was supported by NIH 1 R25 RR019321 Clinical Research Education and Career Development
Provider Notification Obstetrical Billing
 Provider Notification Obstetrical Billing Date of Notification September 1, 20 Revision Date September 17, 2015 Plans Affected Mercy Care Plan and Mercy Care Long Term Care Plan Referrals As outlined in
Provider Notification Obstetrical Billing Date of Notification September 1, 20 Revision Date September 17, 2015 Plans Affected Mercy Care Plan and Mercy Care Long Term Care Plan Referrals As outlined in
AUSTRALIA AND NEW ZEALAND FACTSHEET
 AUSTRALIA AND NEW ZEALAND FACTSHEET What is Stillbirth? In Australia and New Zealand, stillbirth is the death of a baby before or during birth, from the 20 th week of pregnancy onwards, or 400 grams birthweight.
AUSTRALIA AND NEW ZEALAND FACTSHEET What is Stillbirth? In Australia and New Zealand, stillbirth is the death of a baby before or during birth, from the 20 th week of pregnancy onwards, or 400 grams birthweight.
Chapter 3: Healthy Start Risk Screening
 Introduction Healthy Start legislation requires that all pregnant women and infants be offered screening for risk factors that may affect their pregnancy, health, or development. The prenatal and infant
Introduction Healthy Start legislation requires that all pregnant women and infants be offered screening for risk factors that may affect their pregnancy, health, or development. The prenatal and infant
Why is prematurity a concern?
 Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Certified Professional Midwives Caring for Mothers and Babies in Virginia
 Certified Professional Midwives Caring for Mothers and Babies in Virginia Commonwealth Midwives Alliance Certified Professional Midwives in VA Licensed by the BOM since January 2006 5 member Midwifery
Certified Professional Midwives Caring for Mothers and Babies in Virginia Commonwealth Midwives Alliance Certified Professional Midwives in VA Licensed by the BOM since January 2006 5 member Midwifery
ABSTRACT LABOR AND DELIVERY
 ABSTRACT POLICY Prior to fetal viability, intentionally undertaking delivery of a fetus is the equivalent of abortion and is not permissible. After fetal viability has been reached, intentionally undertaking
ABSTRACT POLICY Prior to fetal viability, intentionally undertaking delivery of a fetus is the equivalent of abortion and is not permissible. After fetal viability has been reached, intentionally undertaking
The Minnesota Chlamydia Strategy: Action Plan to Reduce and Prevent Chlamydia in Minnesota Minnesota Chlamydia Partnership, April 2011
 The Minnesota Chlamydia Strategy: Action Plan to Reduce and Prevent Chlamydia in Minnesota Minnesota Chlamydia Partnership, April 2011 Section 5: Screening, Treating and Reporting Chlamydia While the information
The Minnesota Chlamydia Strategy: Action Plan to Reduce and Prevent Chlamydia in Minnesota Minnesota Chlamydia Partnership, April 2011 Section 5: Screening, Treating and Reporting Chlamydia While the information
OBGYN Orientation & Billing Guide 9/22/2014
 OBGYN Orientation & Billing Guide 2014 Welcome to Magnolia Health! We thank you for being part of or considering Magnolia s network of participating providers, hospitals, and other healthcare professionals.
OBGYN Orientation & Billing Guide 2014 Welcome to Magnolia Health! We thank you for being part of or considering Magnolia s network of participating providers, hospitals, and other healthcare professionals.
in children less than one year old. It is commonly divided into two categories, neonatal
 INTRODUCTION Infant Mortality Rate is one of the most important indicators of the general level of health or well being of a given community. It is a measure of the yearly rate of deaths in children less
INTRODUCTION Infant Mortality Rate is one of the most important indicators of the general level of health or well being of a given community. It is a measure of the yearly rate of deaths in children less
On behalf of the Association of Maternal and Child Health Programs (AMCHP), I am
, I am") Christopher Kus, M.D., M.P.H. Association of Maternal and Child Health Programs, Public Witness Testimony House Labor, Health and Human Services and Education Appropriations Subcommittee March 13, 2013
Christopher Kus, M.D., M.P.H. Association of Maternal and Child Health Programs, Public Witness Testimony House Labor, Health and Human Services and Education Appropriations Subcommittee March 13, 2013
49. INFANT MORTALITY RATE. Infant mortality rate is defined as the death of an infant before his or her first birthday.
 49. INFANT MORTALITY RATE Wing Tam (Alice) Jennifer Cheng Stat 157 course project More Risk in Everyday Life Risk Meter LIKELIHOOD of exposure to hazardous levels Low Medium High Consequences: Severity,
49. INFANT MORTALITY RATE Wing Tam (Alice) Jennifer Cheng Stat 157 course project More Risk in Everyday Life Risk Meter LIKELIHOOD of exposure to hazardous levels Low Medium High Consequences: Severity,
Denver County Births and Deaths 2013
 Denver County Births and Deaths 2013 Selected birth characteristics: County residents, 2013... 2 Selected birth characteristics by age group of mother: County residents, 2013... 3 Selected birth characteristics
Denver County Births and Deaths 2013 Selected birth characteristics: County residents, 2013... 2 Selected birth characteristics by age group of mother: County residents, 2013... 3 Selected birth characteristics
Crohn's disease and pregnancy.
 Gut, 1984, 25, 52-56 Crohn's disease and pregnancy. R KHOSLA, C P WILLOUGHBY, AND D P JEWELL From the Gastroenterology Unit, Radcliffe Infirmary, Oxford SUMMARY Infertility and the outcome of pregnancy
Gut, 1984, 25, 52-56 Crohn's disease and pregnancy. R KHOSLA, C P WILLOUGHBY, AND D P JEWELL From the Gastroenterology Unit, Radcliffe Infirmary, Oxford SUMMARY Infertility and the outcome of pregnancy
Wendy Martinez, MPH, CPH County of San Diego, Maternal, Child & Adolescent Health
 Wendy Martinez, MPH, CPH County of San Diego, Maternal, Child & Adolescent Health Describe local trends in birth Identify 3 perinatal health problems Identify 3 leading causes of infant death Age Class
Wendy Martinez, MPH, CPH County of San Diego, Maternal, Child & Adolescent Health Describe local trends in birth Identify 3 perinatal health problems Identify 3 leading causes of infant death Age Class
The Clinical Content of Preconception Care: Alcohol, Tobacco, and Illicit Drug Exposures
 The Clinical Content of Preconception Care: Alcohol, Tobacco, and Illicit Drug Exposures by R. Louise Floyd, DSN, RN; Brian W. Jack, MD; Robert Cefalo, MD, PhD; Hani Atrash, MD, MPH; Jeanne Mahoney, BSN,
The Clinical Content of Preconception Care: Alcohol, Tobacco, and Illicit Drug Exposures by R. Louise Floyd, DSN, RN; Brian W. Jack, MD; Robert Cefalo, MD, PhD; Hani Atrash, MD, MPH; Jeanne Mahoney, BSN,
OBSTETRICAL POLICY. Page
 OBSTETRICAL POLICY REIMBURSEMENT POLICY Policy Number: ADMINISTRATIVE 200.14 T0 Effective Date: April 1, 2016 Table of Contents APPLICABLE LINES OF BUSINESS/PRODUCTS... APPLICATION... OVERVIEW... REIMBURSEMENT
OBSTETRICAL POLICY REIMBURSEMENT POLICY Policy Number: ADMINISTRATIVE 200.14 T0 Effective Date: April 1, 2016 Table of Contents APPLICABLE LINES OF BUSINESS/PRODUCTS... APPLICATION... OVERVIEW... REIMBURSEMENT
Chapter 10. When Abortion Fails
 Chapter 10 When Abortion Fails Occasionally abortion fails, especially when it is drug induced. When this happens, either a second D&C or a more serious surgery may be attempted. The other alternative
Chapter 10 When Abortion Fails Occasionally abortion fails, especially when it is drug induced. When this happens, either a second D&C or a more serious surgery may be attempted. The other alternative
A8b. Resuscitation of a Term Infant with Meconium Staining. Session Summary. Session Objectives. References
 A8b Resuscitation of a Term Infant with Meconium Staining Karen Wright, PhD, NNP-BC Assistant Professor and Coordinator, Neonatal Nurse Practitioner Program Dept. of Women, Children, and Family Nursing,
A8b Resuscitation of a Term Infant with Meconium Staining Karen Wright, PhD, NNP-BC Assistant Professor and Coordinator, Neonatal Nurse Practitioner Program Dept. of Women, Children, and Family Nursing,
Quality of Birth Certificate Data. Daniela Nitcheva, PhD Division of Biostatistics PHSIS
 Quality of Birth Certificate Data Daniela Nitcheva, PhD Division of Biostatistics PHSIS Data Quality SC State Law requires that you file the birth certificate within 5 days of a child s birth. Data needs
Quality of Birth Certificate Data Daniela Nitcheva, PhD Division of Biostatistics PHSIS Data Quality SC State Law requires that you file the birth certificate within 5 days of a child s birth. Data needs
No. 125 April 2001. Enhanced Surveillance of Maternal Mortality in North Carolina
 CHIS Studies North Carolina Public Health A Special Report Series by the 1908 Mail Service Center, Raleigh, N.C. 27699-1908 www.schs.state.nc.us/schs/ No. 125 April 2001 Enhanced Surveillance of Maternal
CHIS Studies North Carolina Public Health A Special Report Series by the 1908 Mail Service Center, Raleigh, N.C. 27699-1908 www.schs.state.nc.us/schs/ No. 125 April 2001 Enhanced Surveillance of Maternal
Breastfeeding. Nursing Education
 Breastfeeding AWHONN supports breastfeeding as the optimal method of infant nutrition. AWHONN believes that women should be encouraged to breastfeed and receive instruction and support from the entire
Breastfeeding AWHONN supports breastfeeding as the optimal method of infant nutrition. AWHONN believes that women should be encouraged to breastfeed and receive instruction and support from the entire
Guidelines for States on Maternity Care In the Essential Health Benefits Package
 Guidelines for States on Maternity Care In the Essential Health Benefits Package Section 2707(a) of the Patient Protection and Affordable Care Act (ACA) requires that all new health insurance plans in
Guidelines for States on Maternity Care In the Essential Health Benefits Package Section 2707(a) of the Patient Protection and Affordable Care Act (ACA) requires that all new health insurance plans in
March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]
![March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]](/thumbs/27/11703693.jpg "March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. <http://www.marchofdimes.com/14332_1169.asp>. [accessed February 2010]") March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. . [accessed February 2010] After delivery, babies who were exposed to amphetamines before birth
March of Dimes. FAQ on Drug Use and Pregnancy. November 2006. . [accessed February 2010] After delivery, babies who were exposed to amphetamines before birth
Caesarean section and quality of obstetric care
 Caesarean section and quality of obstetric care Gjennombruddsprosjekt for keisersnitt September 2014 Michael Robson The National Maternity Hospital Dublin, Ireland Mrobson@nmh.ie Gjennombruddsprosjekt
Caesarean section and quality of obstetric care Gjennombruddsprosjekt for keisersnitt September 2014 Michael Robson The National Maternity Hospital Dublin, Ireland Mrobson@nmh.ie Gjennombruddsprosjekt
Pregnant and Parenting Youth in Foster Care in Washington State: Comparison to Other Teens and Young Women who Gave Birth
 January 2014 RDA Report 11.202 Olympia, Washington Pregnant and Parenting in Care in Washington State: Comparison to Other and Women who Gave Birth Laurie Cawthon, MD, MPH Barbara Lucenko, PhD Peter Woodcox,
January 2014 RDA Report 11.202 Olympia, Washington Pregnant and Parenting in Care in Washington State: Comparison to Other and Women who Gave Birth Laurie Cawthon, MD, MPH Barbara Lucenko, PhD Peter Woodcox,
Populations of Color in Minnesota
 Populations of Color in Minnesota Health Status Report Update Summary Spring 2009 Center for Health Statistics Minnesota Department of Health TABLE OF CONTENTS BACKGROUND... 1 PART I: BIRTH-RELATED HEALTH
Populations of Color in Minnesota Health Status Report Update Summary Spring 2009 Center for Health Statistics Minnesota Department of Health TABLE OF CONTENTS BACKGROUND... 1 PART I: BIRTH-RELATED HEALTH
Methodology for Safety Surveillance of Adverse Events Following Vaccination During Pregnancy
 Methodology for Safety Surveillance of Adverse Events Following Vaccination During Pregnancy C. Jouquelet-Royer September 2012 Fondation Merieux NAME OF PRESENTATION 1 Presentation Outline Background Company
Methodology for Safety Surveillance of Adverse Events Following Vaccination During Pregnancy C. Jouquelet-Royer September 2012 Fondation Merieux NAME OF PRESENTATION 1 Presentation Outline Background Company
Cerebral Palsy. www.teachinngei.org p. 1
 Cerebral Palsy What is cerebral palsy? Cerebral palsy (CP) is a motor disability caused by a static, non-progressive lesion (encephalopathy) in the brain that occurs in early childhood, usually before
Cerebral Palsy What is cerebral palsy? Cerebral palsy (CP) is a motor disability caused by a static, non-progressive lesion (encephalopathy) in the brain that occurs in early childhood, usually before
ST Segment Analysis (STAN) as an Adjunct to Electronic Fetal Monitoring, Part II: Clinical Studies and Future Directions
 as an Adjunct to Electronic Fetal Monitoring, Part II: Clinical Studies and Future Directions") ST Segment Analysis (STAN) as an Adjunct to Electronic Fetal Monitoring, Part II: Clinical Studies and Future Directions Michael A. Belfort, MBBCH, MD, PhD*, George R. Saade, MD KEYWORDS ST segment analysis
ST Segment Analysis (STAN) as an Adjunct to Electronic Fetal Monitoring, Part II: Clinical Studies and Future Directions Michael A. Belfort, MBBCH, MD, PhD*, George R. Saade, MD KEYWORDS ST segment analysis
Overcoming Barriers to Discharge for Home Infusion
 VOLUME 19 CORAM S CONTINUING EDUCATION PROGRAM Overcoming Barriers to Discharge for Home Infusion Successful home infusion therapy relies on timely and effective transitions to home. Early identification
VOLUME 19 CORAM S CONTINUING EDUCATION PROGRAM Overcoming Barriers to Discharge for Home Infusion Successful home infusion therapy relies on timely and effective transitions to home. Early identification
Evaluation and Assessment and Eligibility Regulations 2011
 303.10 Developmental delay. As used in this part, developmental delay, when used with respect to an individual residing in a State, has the meaning given to that term under 303.300. 303.10 Developmental
303.10 Developmental delay. As used in this part, developmental delay, when used with respect to an individual residing in a State, has the meaning given to that term under 303.300. 303.10 Developmental
By Dr. Mindy Aisen CEO and Director United Cerebral Palsy Research and Educational Foundation www.ucpresearch.org CEREBRAL PALSY RESEARCH
 By Dr. Mindy Aisen CEO and Director United Cerebral Palsy Research and Educational Foundation www.ucpresearch.org CEREBRAL PALSY RESEARCH Main Sources of Federal Funding for Cerebral Palsy and Disability
By Dr. Mindy Aisen CEO and Director United Cerebral Palsy Research and Educational Foundation www.ucpresearch.org CEREBRAL PALSY RESEARCH Main Sources of Federal Funding for Cerebral Palsy and Disability
Prognosis of Very Large First-Trimester Hematomas
 Case Series Prognosis of Very Large First-Trimester Hematomas Juliana Leite, MD, Pamela Ross, RDMS, RDCS, A. Cristina Rossi, MD, Philippe Jeanty, MD, PhD Objective. The aim of this study was to evaluate
Case Series Prognosis of Very Large First-Trimester Hematomas Juliana Leite, MD, Pamela Ross, RDMS, RDCS, A. Cristina Rossi, MD, Philippe Jeanty, MD, PhD Objective. The aim of this study was to evaluate
35-40% of GBS disease occurs in the elderly or in adults with chronic medical conditions.
 What is Group B Strep (GBS)? Group B Streptococcus (GBS) is a type of bacteria that is found in the lower intestine of 10-35% of all healthy adults and in the vagina and/or lower intestine of 10-35% of
What is Group B Strep (GBS)? Group B Streptococcus (GBS) is a type of bacteria that is found in the lower intestine of 10-35% of all healthy adults and in the vagina and/or lower intestine of 10-35% of
Public Health Services
 Public Health Services FUNCTION The functions of the Public Health Services programs are to protect and promote the health and safety of County residents. This is accomplished by monitoring health status
Public Health Services FUNCTION The functions of the Public Health Services programs are to protect and promote the health and safety of County residents. This is accomplished by monitoring health status
Delayed Cord Clamping
 ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
MANA Home Birth Data 2004-2009: Consumer Considerations
 MANA Home Birth Data 2004-2009: Consumer Considerations By: Lauren Korfine, PhD U.S. maternity care costs continue to rise without evidence of improving outcomes for women or babies. The cesarean section
MANA Home Birth Data 2004-2009: Consumer Considerations By: Lauren Korfine, PhD U.S. maternity care costs continue to rise without evidence of improving outcomes for women or babies. The cesarean section
METHODOLOGICAL ISSUES IN THE MEASURES OF MATERNAL MORBIDITY MORTALITY (MM 1 MM 2 ) Dr. AKO Simon
 Dr. AKO Simon") (1) METHODOLOGICAL ISSUES IN THE MEASURES OF MATERNAL MORBIDITY MORTALITY (MM 1 MM 2 ) Dr. AKO Simon Postgraduate Research Training in Reproductive Health 2004 Faculty of Medicine, University of Yaounde
(1) METHODOLOGICAL ISSUES IN THE MEASURES OF MATERNAL MORBIDITY MORTALITY (MM 1 MM 2 ) Dr. AKO Simon Postgraduate Research Training in Reproductive Health 2004 Faculty of Medicine, University of Yaounde
Preterm Labor Assessment Toolkit. Kenneth E. Brown, MD, MBA, FACOG
 Preterm Labor Assessment Toolkit Kenneth E. Brown, MD, MBA, FACOG Chief Medical Director Woman s Hospital Baton Rouge, LA Associate Clinical Professor Louisiana State University Lafayette, LA Disclosures
Preterm Labor Assessment Toolkit Kenneth E. Brown, MD, MBA, FACOG Chief Medical Director Woman s Hospital Baton Rouge, LA Associate Clinical Professor Louisiana State University Lafayette, LA Disclosures
Statement for the Record. Mr. Chairman and Members of the Committee:
 The Need For National Cerebral Palsy Surveillance - Testimony before the House Subcommittee on Labor, Health and Human Services, Education, and Related Agencies - Committee on Appropriations Dr. Janice
The Need For National Cerebral Palsy Surveillance - Testimony before the House Subcommittee on Labor, Health and Human Services, Education, and Related Agencies - Committee on Appropriations Dr. Janice
Institute for Safe Medication Practices
 Institute for Safe Medication Practices 1800 Byberry Road, Suite 810 Huntingdon Valley, PA 19006 FOR MORE INFORMATION, CONTACT : Michael A. Donio, MPA Marketing & Consumer Affairs 215-947-7797 Mdonio@ismp.org
Institute for Safe Medication Practices 1800 Byberry Road, Suite 810 Huntingdon Valley, PA 19006 FOR MORE INFORMATION, CONTACT : Michael A. Donio, MPA Marketing & Consumer Affairs 215-947-7797 Mdonio@ismp.org
Pregnancy and Substance Abuse
 Pregnancy and Substance Abuse Introduction When you are pregnant, you are not just "eating for two." You also breathe and drink for two, so it is important to carefully consider what you put into your
Pregnancy and Substance Abuse Introduction When you are pregnant, you are not just "eating for two." You also breathe and drink for two, so it is important to carefully consider what you put into your
A single center experience with 1000 consecutive cases of multifetal pregnancy reduction
 A single center experience with 1000 consecutive cases of multifetal pregnancy reduction Joanne Stone, MD, Keith Eddleman, MD, Lauren Lynch, MD, and Richard L. Berkowitz, MD New York, NY, and San Juan,
A single center experience with 1000 consecutive cases of multifetal pregnancy reduction Joanne Stone, MD, Keith Eddleman, MD, Lauren Lynch, MD, and Richard L. Berkowitz, MD New York, NY, and San Juan,
Registered Midwife Clinical Privileges REAPPOINTMENT 2015-2016 Effective from July 1, 2015 to June 30, 2016
 Name: Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the governing body, effective: 04/Jun/2013. Applicant:
Name: Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the governing body, effective: 04/Jun/2013. Applicant:
Appendices. 2006 Bexar County Community Health Assessment Appendices Appendix A 125
 Appendices Appendix A Recent reports suggest that the number of mothers seeking dropped precipitously between 2004 and 2005. Tables 1A and 1B, below, shows information since 1990. The trend has been that
Appendices Appendix A Recent reports suggest that the number of mothers seeking dropped precipitously between 2004 and 2005. Tables 1A and 1B, below, shows information since 1990. The trend has been that
Ana M. Viamonte Ros, M.D., M.P.H. State Surgeon General
 Florida Department of Health Division of Disease Control Bureau of Epidemiology Chronic Disease Epidemiology Section Charlie Crist Governor Ana M. Viamonte Ros, M.D., M.P.H. State Surgeon General Florida
Florida Department of Health Division of Disease Control Bureau of Epidemiology Chronic Disease Epidemiology Section Charlie Crist Governor Ana M. Viamonte Ros, M.D., M.P.H. State Surgeon General Florida
An Overview of Abortion in the United States. Guttmacher Institute January 2014
 An Overview of Abortion in the United States Guttmacher Institute January 2014 Objectives Provide an overview of unintended pregnancy and abortion in the United States. Review the incidence of pregnancy
An Overview of Abortion in the United States Guttmacher Institute January 2014 Objectives Provide an overview of unintended pregnancy and abortion in the United States. Review the incidence of pregnancy
Developing Human Fetus
 Period Date LAB. DEVELOPMENT OF A HUMAN FETUS After a human egg is fertilized with human sperm, the most amazing changes happen that allow a baby to develop. This amazing process, called development, normally
Period Date LAB. DEVELOPMENT OF A HUMAN FETUS After a human egg is fertilized with human sperm, the most amazing changes happen that allow a baby to develop. This amazing process, called development, normally
March of Dimes 2016 Chapter Community Grants Program
 March of Dimes 2016 Chapter Community Grants Program Community Award Application March of Dimes Maryland National Capital Area Chapter 175 West Ostend St., Suite C-2 Baltimore, MD 21230 Marchofdimes.org/marylandmetrodc
March of Dimes 2016 Chapter Community Grants Program Community Award Application March of Dimes Maryland National Capital Area Chapter 175 West Ostend St., Suite C-2 Baltimore, MD 21230 Marchofdimes.org/marylandmetrodc
Testimony of the American College of Nurse-Midwives. at a Hearing of the House Committee on Energy and Commerce Subcommittee on Health.
 Testimony of the American College of Nurse-Midwives at a Hearing of the House Committee on Energy and Commerce Subcommittee on Health on the Improving Access to Maternity Care Act (H.R.1209) Wednesday,
Testimony of the American College of Nurse-Midwives at a Hearing of the House Committee on Energy and Commerce Subcommittee on Health on the Improving Access to Maternity Care Act (H.R.1209) Wednesday,
4/30/2013 HPV VACCINE AND NORTH DAKOTA HPV IMMUNIZATION RATES HUMAN PAPILLOMAVIRUS (HPV) HUMAN PAPILLOMAVIRUS HPV CONTINUED
 HUMAN PAPILLOMAVIRUS HPV CONTINUED") HPV VACCINE AND NORTH DAKOTA HPV IMMUNIZATION RATES HUMAN PAPILLOMAVIRUS (HPV) HUMAN PAPILLOMAVIRUS What is human papillomavirus (HPV)? HPV is the most common sexually transmitted infection. There are
HPV VACCINE AND NORTH DAKOTA HPV IMMUNIZATION RATES HUMAN PAPILLOMAVIRUS (HPV) HUMAN PAPILLOMAVIRUS What is human papillomavirus (HPV)? HPV is the most common sexually transmitted infection. There are
Cerebral palsy can be classified according to the type of abnormal muscle tone or movement, and the distribution of these motor impairments.
 The Face of Cerebral Palsy Segment I Discovering Patterns What is Cerebral Palsy? Cerebral palsy (CP) is an umbrella term for a group of non-progressive but often changing motor impairment syndromes, which
The Face of Cerebral Palsy Segment I Discovering Patterns What is Cerebral Palsy? Cerebral palsy (CP) is an umbrella term for a group of non-progressive but often changing motor impairment syndromes, which
Family Health Dataline
 October 1999 Vol 5, No 3 Corrected Feb. 2000 IN THIS ISSUE: In Alaska during 1996-97, 41% of live births were the result of unintended pregnancies. All racial, age, and education groups evaluated had high
October 1999 Vol 5, No 3 Corrected Feb. 2000 IN THIS ISSUE: In Alaska during 1996-97, 41% of live births were the result of unintended pregnancies. All racial, age, and education groups evaluated had high
Pregnancy Intendedness
 Pregnancy Intendedness What moms had to say: "Very excited! We wanted to be pregnant for 8 years!" "I felt too old." "I wanted to have a baby to get some support so I could be on my own; if didn't have
Pregnancy Intendedness What moms had to say: "Very excited! We wanted to be pregnant for 8 years!" "I felt too old." "I wanted to have a baby to get some support so I could be on my own; if didn't have
Maternity Care Primary C-Section Rate Specifications 2014 (07/01/2013 to 06/30/2014 Dates of Service)
") Summary of Changes Denominator Changes: Two additions were made to the denominator criteria. The denominator was changed to include patients who had: a vertex position delivery AND a term pregnancy of
Summary of Changes Denominator Changes: Two additions were made to the denominator criteria. The denominator was changed to include patients who had: a vertex position delivery AND a term pregnancy of
Who Is Involved in Your Care?
 Patient Education Page 3 Pregnancy and Giving Birth Who Is Involved in Your Care? Our goal is to surround you and your family with a safe environment for the birth of your baby. We look forward to providing
Patient Education Page 3 Pregnancy and Giving Birth Who Is Involved in Your Care? Our goal is to surround you and your family with a safe environment for the birth of your baby. We look forward to providing
Beyond Meaningful Use -- Multi- disciplinary Team Integration of Customized Smoking Cessation Patient Education Into EMR Clinical Decision Support
 Beyond Meaningful Use -- Multi- disciplinary Team Integration of Customized Smoking Cessation Patient Education Into EMR Clinical Decision Support Wendy Angelo, MD Capital Region Healthcare Learning Objectives
Beyond Meaningful Use -- Multi- disciplinary Team Integration of Customized Smoking Cessation Patient Education Into EMR Clinical Decision Support Wendy Angelo, MD Capital Region Healthcare Learning Objectives
Preconception Clinical Care for Women Medical Conditions
 Preconception Clinical Care for Women All women of reproductive age are candidates for preconception care; however, preconception care must be tailored to meet the needs of the individual. Given that preconception
Preconception Clinical Care for Women All women of reproductive age are candidates for preconception care; however, preconception care must be tailored to meet the needs of the individual. Given that preconception
GUIDELINES FOR TUBERCULOSIS PREVENTIVE THERAPY AMONG HIV INFECTED INDIVIDUALS IN SOUTH AFRICA
 GUIDELINES FOR TUBERCULOSIS PREVENTIVE THERAPY AMONG HIV INFECTED INDIVIDUALS IN SOUTH AFRICA 2010 1 TB prophylaxis GUIDELINES FOR TUBERCULOSIS PREVENTIVE THERAPY AMONG HIV INFECTED INDIVIDUALS Background
GUIDELINES FOR TUBERCULOSIS PREVENTIVE THERAPY AMONG HIV INFECTED INDIVIDUALS IN SOUTH AFRICA 2010 1 TB prophylaxis GUIDELINES FOR TUBERCULOSIS PREVENTIVE THERAPY AMONG HIV INFECTED INDIVIDUALS Background
Medical Care Advisory Committee. David Auzenne Department of State Health Services
 TO: Medical Care Advisory Committee DATE: November 8, 2013 FROM: David Auzenne Department of State Health Services Agenda Item No.: 9 SUBJECT: Amendments to Title 25. Health Services, Part 1. Department
TO: Medical Care Advisory Committee DATE: November 8, 2013 FROM: David Auzenne Department of State Health Services Agenda Item No.: 9 SUBJECT: Amendments to Title 25. Health Services, Part 1. Department
Medical Care Costs for Diabetes Associated with Health Disparities Among Adults Enrolled in Medicaid in North Carolina
 No. 160 August 2009 Among Adults Enrolled in Medicaid in North Carolina by Paul A. Buescher, Ph.D. J. Timothy Whitmire, Ph.D. Barbara Pullen-Smith, M.P.H. A Joint Report from the and the Office of Minority
No. 160 August 2009 Among Adults Enrolled in Medicaid in North Carolina by Paul A. Buescher, Ph.D. J. Timothy Whitmire, Ph.D. Barbara Pullen-Smith, M.P.H. A Joint Report from the and the Office of Minority
A Strategic Plan for Improving Preconception Health and Health Care: Recommendations from the CDC Select Panel on Preconception Care
 1 A Strategic Plan for Improving Preconception Health and Health Care: Recommendations from the CDC Select Panel on Preconception Care Presentation by Kay A. Johnson, MPH, EdM Research Assistant Professor,
1 A Strategic Plan for Improving Preconception Health and Health Care: Recommendations from the CDC Select Panel on Preconception Care Presentation by Kay A. Johnson, MPH, EdM Research Assistant Professor,
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.9 Case Management Services G.12 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.9 Case Management Services G.12 Special Needs Services
Epilepsy 101: Getting Started
 American Epilepsy Society 1 Epilepsy 101 for nurses has been developed by the American Epilepsy Society to prepare professional nurses to understand the general issues, concerns and needs of people with
American Epilepsy Society 1 Epilepsy 101 for nurses has been developed by the American Epilepsy Society to prepare professional nurses to understand the general issues, concerns and needs of people with
Critical care decisions in fetal and neonatal medicine: ethical issues
 Critical care decisions in fetal and neonatal medicine: ethical issues a guide to the Report Introduction Major improvements in medical care mean that extremely premature and very ill babies have better
Critical care decisions in fetal and neonatal medicine: ethical issues a guide to the Report Introduction Major improvements in medical care mean that extremely premature and very ill babies have better
Lyme Disease in Pregnancy. Dr Sarah Chissell Consultant Obstetrician William Harvey Hospital, Kent
 Lyme Disease in Pregnancy Dr Sarah Chissell Consultant Obstetrician William Harvey Hospital, Kent Conflict of interest My son has chronic Lyme disease Infections in pregnancy Transplacental infection Perinatal
Lyme Disease in Pregnancy Dr Sarah Chissell Consultant Obstetrician William Harvey Hospital, Kent Conflict of interest My son has chronic Lyme disease Infections in pregnancy Transplacental infection Perinatal
- 103-7. CIGARETTE USE COUNSELING Steven Asch, M.D., M.P.H.
 - 103-7. CIGARETTE USE COUNSELING Steven Asch, M.D., M.P.H. We relied on Chapter 48 of the Guide to Clinical Preventive Services published by the U.S. Preventive Services Task Force (USPSTF, 1989) to construct
- 103-7. CIGARETTE USE COUNSELING Steven Asch, M.D., M.P.H. We relied on Chapter 48 of the Guide to Clinical Preventive Services published by the U.S. Preventive Services Task Force (USPSTF, 1989) to construct
Respiratory Distress Syndrome of the Newborn
 19 Respiratory Distress Syndrome of the Newborn Respiratory distress syndrome (RDS) of the newborn, also known as hyaline membrane disease, is a breathing disorder of premature babies. In healthy infants,
19 Respiratory Distress Syndrome of the Newborn Respiratory distress syndrome (RDS) of the newborn, also known as hyaline membrane disease, is a breathing disorder of premature babies. In healthy infants,
ICD-10 OVERVIEW Coding Guidelines For OB/GYN
 ICD-10 OVERVIEW Coding Guidelines For OB/GYN ICD-10 Chapter 15 Pregnancy, Childbirth and the Puerperium (O00-O9A) Note: Codes from this chapter are for use only on maternal records, NEVER on newborn records.
ICD-10 OVERVIEW Coding Guidelines For OB/GYN ICD-10 Chapter 15 Pregnancy, Childbirth and the Puerperium (O00-O9A) Note: Codes from this chapter are for use only on maternal records, NEVER on newborn records.
Medication Assisted Treatment
 Medication Assisted Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority Bureau Of Prevention, Treatment, & Recovery State of Wisconsin Elizabeth Collier, MSW, CSAC, ICS, LCSW TANF Best Practice
Medication Assisted Treatment Tanya Hiser, MS, LPC State Opioid Treatment Authority Bureau Of Prevention, Treatment, & Recovery State of Wisconsin Elizabeth Collier, MSW, CSAC, ICS, LCSW TANF Best Practice
Guidance for Industry Diabetes Mellitus Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes
 Guidance for Industry Diabetes Mellitus Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes U.S. Department of Health and Human Services Food and Drug Administration Center
Guidance for Industry Diabetes Mellitus Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes U.S. Department of Health and Human Services Food and Drug Administration Center
Intervention and clinical epidemiological studies
 Intervention and clinical epidemiological studies Including slides from: Barrie M. Margetts Ian L. Rouse Mathew J. Reeves,PhD Dona Schneider Tage S. Kristensen Victor J. Schoenbach Experimental / intervention
Intervention and clinical epidemiological studies Including slides from: Barrie M. Margetts Ian L. Rouse Mathew J. Reeves,PhD Dona Schneider Tage S. Kristensen Victor J. Schoenbach Experimental / intervention
Chapter 14. Board of Certified Direct-Entry Midwives.
 Chapter 14. Board of Certified Direct-Entry Midwives. (Words in boldface and underlined indicate language being added; words [CAPITALIZED AND BRACKETED] indicate language being deleted. Complete new sections
Chapter 14. Board of Certified Direct-Entry Midwives. (Words in boldface and underlined indicate language being added; words [CAPITALIZED AND BRACKETED] indicate language being deleted. Complete new sections
Lecture 12a: Complications of Pregnancy
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Roles of the Nurse Practitioner. Abby Smith. Auburn University/Auburn Montgomery
 Running Head: ROLES OF THE NURSE PRACTITIONER Roles of the Nurse Practitioner Abby Smith Auburn University/Auburn Montgomery 2 Abstract Advanced practice nursing has many roles in health care today, with
Running Head: ROLES OF THE NURSE PRACTITIONER Roles of the Nurse Practitioner Abby Smith Auburn University/Auburn Montgomery 2 Abstract Advanced practice nursing has many roles in health care today, with
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2014 October 1 st, 2014
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2014 October 1 st, 2014 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2014 October 1 st, 2014 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Medicaid Health Plans: Adding Value for Beneficiaries and States
 Medicaid Health Plans: Adding Value for Beneficiaries and States Medicaid is a program with numerous challenges, both for its beneficiaries and the state and federal government. In comparison to the general
Medicaid Health Plans: Adding Value for Beneficiaries and States Medicaid is a program with numerous challenges, both for its beneficiaries and the state and federal government. In comparison to the general
The National Survey of Children s Health 2011-2012 The Child
 The National Survey of Children s 11-12 The Child The National Survey of Children s measures children s health status, their health care, and their activities in and outside of school. Taken together,
The National Survey of Children s 11-12 The Child The National Survey of Children s measures children s health status, their health care, and their activities in and outside of school. Taken together,
Prescription Drug Plan
 Prescription Drug Plan The prescription drug plan helps you pay for prescribed medications using either a retail pharmacy or the mail order program. For More Information Administrative details and procedures
Prescription Drug Plan The prescription drug plan helps you pay for prescribed medications using either a retail pharmacy or the mail order program. For More Information Administrative details and procedures
10/31/2014. Medication Adherence: Development of an EMR tool to monitor oral medication compliance. Conflict of Interest Disclosures.
 Medication Adherence: Development of an EMR tool to monitor oral medication compliance Donna Williams, RN PHN Carol Bell, NP MSN Andrea Linder, RN MS CCRC Clinical Research Nurses Stanford University SOM
Medication Adherence: Development of an EMR tool to monitor oral medication compliance Donna Williams, RN PHN Carol Bell, NP MSN Andrea Linder, RN MS CCRC Clinical Research Nurses Stanford University SOM
Screening Mammography for Breast Cancer: American College of Preventive Medicine Practice Policy Statement
 Screening Mammography for Breast Cancer: American College of Preventive Medicine Practice Policy Statement Rebecca Ferrini, MD, Elizabeth Mannino, MD, Edith Ramsdell, MD and Linda Hill, MD, MPH Burden
Screening Mammography for Breast Cancer: American College of Preventive Medicine Practice Policy Statement Rebecca Ferrini, MD, Elizabeth Mannino, MD, Edith Ramsdell, MD and Linda Hill, MD, MPH Burden
OET: Listening Part A: Influenza
 Listening Test Part B Time allowed: 23 minutes In this part, you will hear a talk on critical illnesses due to A/H1N1 influenza in pregnant and postpartum women, given by a medical researcher. You will
Listening Test Part B Time allowed: 23 minutes In this part, you will hear a talk on critical illnesses due to A/H1N1 influenza in pregnant and postpartum women, given by a medical researcher. You will
Evaluation and Follow-up of Fetal Hydronephrosis
 Evaluation and Follow-up of Fetal Hydronephrosis Deborah M. Feldman, MD, Marvalyn DeCambre, MD, Erin Kong, Adam Borgida, MD, Mujgan Jamil, MBBS, Patrick McKenna, MD, James F. X. Egan, MD Objective. To
Evaluation and Follow-up of Fetal Hydronephrosis Deborah M. Feldman, MD, Marvalyn DeCambre, MD, Erin Kong, Adam Borgida, MD, Mujgan Jamil, MBBS, Patrick McKenna, MD, James F. X. Egan, MD Objective. To
Oregon Birth Outcomes, by Planned Birth Place and Attendant Pursuant to: HB 2380 (2011)
") Oregon Birth Outcomes, by Birth Place and Attendant Pursuant to: HB 2380 (2011) In 2011, the Oregon Legislature passed House Bill 2380, which required the Oregon Public Health Division to add two questions
Oregon Birth Outcomes, by Birth Place and Attendant Pursuant to: HB 2380 (2011) In 2011, the Oregon Legislature passed House Bill 2380, which required the Oregon Public Health Division to add two questions
Article. Anthony O. Odibo, MD, Christopher Riddick, Emmanuelle Pare, MD, David M. Stamilio, MD, MSCE, George A. Macones, MD, MSCE
 Article Cerebroplacental Doppler Ratio and Adverse Perinatal Outcomes in Intrauterine Growth Restriction Evaluating the Impact of Using Gestational Age Specific Reference Values Anthony O. Odibo, MD, Christopher
Article Cerebroplacental Doppler Ratio and Adverse Perinatal Outcomes in Intrauterine Growth Restriction Evaluating the Impact of Using Gestational Age Specific Reference Values Anthony O. Odibo, MD, Christopher
Parvovirus B19 Infection in Pregnancy
 Parvovirus B19 Infection in Pregnancy Information Pack Parvovirus B19 Infection in Pregnancy Information Booklet CONTENTS: THE VIRUS page 3 CLINICAL MANIFESTATIONS page 6 DIAGNOSIS page 8 PATIENT MANAGEMENT
Parvovirus B19 Infection in Pregnancy Information Pack Parvovirus B19 Infection in Pregnancy Information Booklet CONTENTS: THE VIRUS page 3 CLINICAL MANIFESTATIONS page 6 DIAGNOSIS page 8 PATIENT MANAGEMENT
Neonatal Abstinence Syndrome
 Neonatal Abstinence Syndrome Effective Prevention Strategies Division of Prevention and Health Promotion Injury Prevention Program Objectives Characterize PDA as a public health problem Detail the impact
Neonatal Abstinence Syndrome Effective Prevention Strategies Division of Prevention and Health Promotion Injury Prevention Program Objectives Characterize PDA as a public health problem Detail the impact
Participating in Alzheimer s Disease Clinical Trials and Studies
 Participating in Alzheimer s Disease Clinical Trials and Studies FACT SHEET When Margaret was diagnosed with earlystage Alzheimer s disease at age 68, she wanted to do everything possible to combat the
Participating in Alzheimer s Disease Clinical Trials and Studies FACT SHEET When Margaret was diagnosed with earlystage Alzheimer s disease at age 68, she wanted to do everything possible to combat the
Fetal Therapy Center. Phone: 305-585-6636 Fax: 305-325-1282 www.uhealthobgyn.com www.jhsmiami.org AMNIOPATCH INFORMATION PACKET
 Fetal Therapy Center Phone: 305-585-6636 Fax: 305-325-1282 www.uhealthobgyn.com www.jhsmiami.org AMNIOPATCH INFORMATION PACKET 2 AMNIOPATCH FOR TREATMENT OF PREVIABLE PREMATURE RUPTURE OF MEMBRANES Premature
Fetal Therapy Center Phone: 305-585-6636 Fax: 305-325-1282 www.uhealthobgyn.com www.jhsmiami.org AMNIOPATCH INFORMATION PACKET 2 AMNIOPATCH FOR TREATMENT OF PREVIABLE PREMATURE RUPTURE OF MEMBRANES Premature
Baltimore, MD 21225 * The Corporation Trust Inc 351 West Camden Street * Baltimore, MD 21201. KATHLEEN WARD, M.D. 3001 South Hanover Street *
 JAYLAN NORFLEET, a minor, by and through his Parents and Next Friends, SHANTIAH MOORE-NORFLEET and IN THE JOEL NORFLEET 5337 4 th Street CIRCUIT COURT Brooklyn, MD 21225 BALTIMORE CITY SHANTIAH MOORE-NORFLEET,
JAYLAN NORFLEET, a minor, by and through his Parents and Next Friends, SHANTIAH MOORE-NORFLEET and IN THE JOEL NORFLEET 5337 4 th Street CIRCUIT COURT Brooklyn, MD 21225 BALTIMORE CITY SHANTIAH MOORE-NORFLEET,
Expedited Partner Therapy (EPT) for Sexually Transmitted Diseases Protocol for Health Care Providers in Oregon
 for Sexually Transmitted Diseases Protocol for Health Care Providers in Oregon") Expedited Partner Therapy (EPT) for Sexually Transmitted Diseases Protocol for Health Care Providers in Oregon Oregon Health Authority Center for Public Health Practice HIV/STD/TB Section Principles of
Expedited Partner Therapy (EPT) for Sexually Transmitted Diseases Protocol for Health Care Providers in Oregon Oregon Health Authority Center for Public Health Practice HIV/STD/TB Section Principles of
Why the INFANT Study
 The INFANT Study A multi-centre Randomised Controlled Trial (RCT) of an intelligent system to support decision making in the management of labour using the CTG Why the INFANT Study INFANT stands for INtelligent
The INFANT Study A multi-centre Randomised Controlled Trial (RCT) of an intelligent system to support decision making in the management of labour using the CTG Why the INFANT Study INFANT stands for INtelligent