Management of the Emergent Airway
|
|
|
- Walter Bond
- 7 years ago
- Views:
Transcription
1 Management of the Emergent Airway Benjamin Walton, M.D. Faculty Advisor: Michael Underbrink, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation March 31, 2011

2 Table of Contents I. The Difficult Airway Evaluation II. Non-surgical Options III. Surgical Options IV. Controversies V. Management of the Pediatric Patient

3 The Difficult Airway Problematic ventilation using a face mask Inability to deliver necessary tidal volume via face mask utilizing nasal or oral airway Incomplete laryngoscopic visualization Cormack and Lehane grade 3 or 4 Difficult Intubation with standard airway equipment Requiring external laryngeal manipulation Greater than 3 attempts at intubation Requiring nonstandard equipment

4 Evaluation of the Airway Elective Versus Urgent Adult Versus Pediatric Patient Status

5 Predictors of Significantly Difficult or Impossible Intubation in Adults Interincisor distance 3 cm or less Thyro-mental distance 6 cm or less Maxillary dentition interfering with jaw thrust Mallampati classification Neck in fixed flexion Extreme head and neck radiation changes, scarring, or large masses

6 Airway Management Team Anesthesiologist Otolaryngologist Emergency Physician Respiratory Therapist

7 OR vs. Emergency Room: Difficult Intubations Incidence of difficult intubation in OR: 1.15% to 3.80% Failed attempts occur in 0.05% to 0.35% Incidence of difficult intubations in ED: 3.0% to 5.3% Failure rates ranging from 0.5% to 1.1%

8 The difficult airway in the emergency department. Wong et al Prospective Observational Study from 1 January 2000 to 31 December ,343 patients who underwent advanced airway management, 93 (4.0%) were deemed difficult Difficult airway defined as difficulty with mask ventilation or at least 3 attempts at orotracheal intubation or failed intubation or cricothyroidotomy was difficult Failed airway defined as tracheal intubation cannot be achieved after multiple attempts by orotracheal, nasotracheal or transtracheal (cricothyroidotomy or tracheostomy) route, or if intubation abandoned

9 Diagnoses Encountered

10 Reasons for difficult intubation
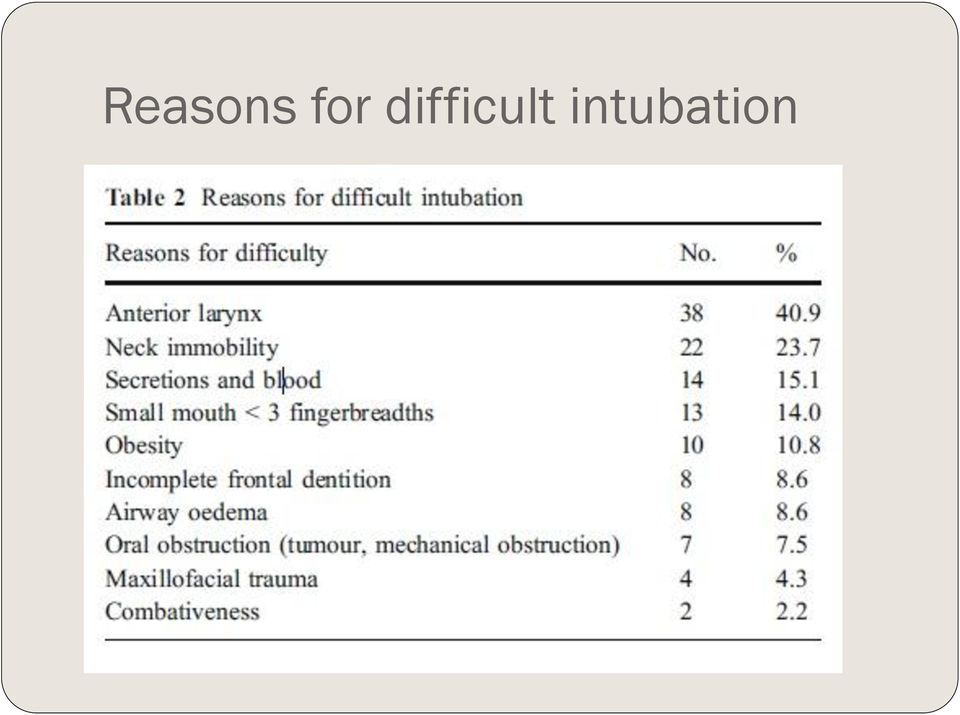
11 Results (continued) Mean number of attempts at intubation for difficult airway group was 3.6 compared to 1.2 for all patients Surgical airway rate was 0.3% Difficult intubation rate: 4% Failed intubation rate: 0.7%

12 Causes of a Difficult Airway Trauma Midface Mandible Neck Bleeding into airway Caustic ingestion Thermal burns

13 Causes of a Difficult Airway Disease Obstructive Sleep Apnea Malignancy, mucosal Oral Pharyngeal Laryngotracheal

14 Causes of a Difficult Airway Malignancy, extrinsic Thyroid Lymphoma Esophageal

15 Causes of a Difficult Airway Foreign Body Degenerative cervical spine disease Infection Deep Neck Space Abscess Ludwig s angina Trismus Anaphylaxis Angioedema Previous head and neck surgery Vocal cord paralysis

16 Causes of a Difficult Airway Anatomic/congenital factors Retrognathia Thick/Short neck Macroglossia Small mouth opening Kyphosis

17 Evaluation of the Airway Mallampati Classification: used to estimate ease of viewing patient s glottis

18 Cormack Lehane scale Visualization of glottis with Macintosh blade

19 Questions I Need to Ask Myself Can I perform effective mask ventilation? Incidence of difficult mask ventilation in adult patients in OR is 1.4-5% Defined as inability to maintain O2 sat >90% with 100% inspired O2 or to prevent or reverse signs of hypoventilation with positive-pressure mask ventilation Can I safely intubate this patient? Although tracheal intubation is the ultimate goal in airway management, the ability to provide effective mask-ventilation is life-saving (1)

20 Prediction and Outcomes of Impossible Mask Ventilation Kheterpal et al. reviewed 50,000 patients undergoing airway management in the operating room Impossible mask ventilation in 0.15% of cases Predictors included previous neck radiation, male sex, OSA, Mallampati class III or IV, and presence of a beard 25% (19/77) of patients with impossible mask ventilation were difficult to intubate. 2 of those patients required surgical airways
 of patients with impossible mask ventilation were difficult to intubate.")
21 Pre-oxygenation Healthy adults breathing room air will develop oxygen desaturation (Sp02 <90%) with 2 minutes of apnea Preoxygenation with 100% oxygen can maintain oxygen saturation above 90% for more than 6 minutes 4 vital-capacity breaths in 30 seconds or 8 vital capacity breaths in 60 seconds provide adequate pre-oxygenation
22 Monitoring During Anesthesia American Society of Anesthesiology Standards for Basic Anesthetic Monitoring released in 1986 Continual monitoring of oxygen, ventilation, circulation, temperature Intermittent (no less frequent than every 5 minutes) measurement of arterial blood pressure and heart rate
23 Anesthetic Pharmacology
24 Induction Agents IV induction agents have quick onset, produce unconsciousness within 1-2 minutes Thiopental and Propofol: negative inotropic effect and produces apnea along with unconsciousness Etomidate: less effects on hemodynamics, potential adrenal suppression and myoclonic activity Ketamine: does not produce apnea with administration, can give IM, can cause tachycardia and hypertension along with exaggerated secretions
25 Volatile Anesthetic Agents Used for maintenance in most instances Halothane- nonflammable, alkane, lacks bronchoirritant effects, highly soluble in blood and fatty tissues, negative inotropic effects on cardiac muscles Enflurane and Isoflurane: nonflammable, pungent odor, produce more intrinsic respiratory depression, less cardiac effects (Enflurane now rarely used due to risk of renal toxicity and seizure) Sevoflurane and Desflurane: low lipid solubility, cause little myocardial depression, Desflurane has bronchoirritative properties
26 Nitrous Oxide Not potent enough as single agent, Used in conjunction with volatile agents to decrease the requirements Can support combustion with oxygen Quickly diffuses into closed, air-filled body cavities Avoid in obstructive ileus, pulmonary bullae, unrelieved pneumothorax Useful in PE tube placement but not during tympanoplasty
27 Neuromuscular Blocking Drugs Competitive Inhibitors Pancuronium Metabolized in the Liver, Excreted by Kidneys CV Effects: Tachycardia Onset: < 3 min Duration: min Vecuronium Metabolized in Liver, Excreted by Kidneys CV Effects: None Onset: < 3 min Duration: min Rocuronium Metabolized in Liver, Excreted by Kidneys CV effects: None Onset: < 1 min Duration: min Non-competitive Inhibitors Succinylcholine Metabolized by plasma cholinesterase, Excreted by Kidneys CV Effects: Bradycardia in children or in repetitive bolus to adults Onset: < 1 min Duration: < 10 minutes
28 Rapid Sequence Intubation Most common approach to securing airway in ER, ICU, and OR with concerns for aspiration Pre-oxygenation, administration of induction agent with muscle relaxant in rapid succession, Wait s without mask ventilation then intubation with cricoid pressure Controversy over cricoid pressure: Studies show it lies over the hypopharynx that can only be compressed 35% in diameter, Smith et al used MRI to demonstrate greater than 50% of patients have esophagus displaced laterally with cricoid pressure and is not compressible
29 Adult Evaluation Evaluate for: Facial or Neck Masses Deformities, scars, quality of dentition, Maxillary and Mandibular position, pharyngeal structures, and Neck Mobility Flexible fiber-optic endoscopy is the most important factor in determining the status of the upper airway and cause of impairment; however, when do we have the time? Controversy whether increased age, male sex, OSA, high BMI, Pretracheal soft tissue increase challenge
30 Pediatric Evaluation Noisy breathing during exercise, at rest or when feeding Previous surgeries or Intubations Neck pain, fever, recent upper respiratory infections Birth Trauma Congenital Anomalies
31 Difficult Airway Algorithm Accepted by the American Society of Anesthesiologists 4 main steps in the process of developing the strategy for acquiring control of the airway (1) Assess the likelihood and clinical impact of basic management problems Difficult ventilation Difficult intubation Difficulty with Patient Cooperation or Consent Difficult Tracheostomy
32 Algorithm continued (2) Actively pursue opportunities to deliver supplemental oxygen throughout the process of difficult airway management (3) Consider the relative merits and feasibility of basic management choices Awake intubation vs. Intubation Attempts After Induction of General Anesthesia Non-invasive Technique for Initial Approach to Intubation vs. Invasive Technique for Initial Approach to Intubation Preservation of Spontaneous Ventilation vs. Ablation of Spontaneous Ventilation (4) Develop primary and alternative strategies
33 Scenario 1 You decide that the best approach is an awake intubation Decision is between approaching the airway by non-invasive intubation or invasive airway access (tracheostomy vs. cricothyroidotomy)
34 You succeed!!! Hooray, you have confirmed ventilation, tracheal intubation, or LMA placement with exhaled CO2
35 Or -- You Have Failed (1) Consider cancelling the case (2) Consider feasibility of other options: face mask or LMA, local anesthesia infiltration or regional nerve block (not really an option for many of our cases) (3) Invasive Airway Access
36 Scenario 2 Intubation Attempts After Induction of General Anesthesia Major decision tree based on ability to adequately ventilate through face mask
37 Tube is in the trachea Congrats, you are done. Go on your coffee break then 20 minutes later, go on your lunch break, then read the paper for 30 minutes while various beeps go off. Take out a syringe and then push some saline into the IV. Complain for a while about the length of the OR case and why you wish your stocks were doing better. Flirt with the scrub nurse.
38 Initial Intubation Attempt Unsuccessful From here on out consider: Calling for Help, Return to Spontaneous Ventilation, Awakening the Patient Attempt Face Mask Ventilation If adequate, head toward non-emergent pathway
39 Alternative Approaches to Intubation Using different laryngoscope blades LMA as an intubation conduit (with or without fiberoptic guidance) Fiberoptic Intubation Intubating stylet or tube changer Light wand Retrograde Intubation Blind oral or nasal intubation
40 Failing after Multiple Attempts Invasive Airway Access Consider other options Awaken the patient
41 If Face Mask Ventilation Not Adequate First Consider or Attempt to place LMA If the LMA is adequate then you can attempt alternative approaches to intubation If LMA is not adequate or not feasible: Call for Help Emergency Non-Invasive Airway Ventilation Rigid Bronchoscopy Esophageal-Tracheal Combitube Transtracheal jet ventilation
42 Laryngeal Mask Courtesy Cummings
43 Esophageal Combitube Courtesy Cummings
44 Rigid Bronchoscope
45 If Emergency Non-invasive Ventilation is Successful Consider invasive airway access Consider feasibility of other options as discussed before Awaken the Patient
46 If Emergency Non-Invasive Ventilation is Unsuccessful Emergency Invasive Airway Access That would be us.
47 ASA Difficult Airway Algorithm
48 Or, if you d like to see a little bigger picture, try turning it SIDEWAYS
49 Non-surgical Options Face Mask Ventilation Endotracheal Intubation LMA Combitube Fiberoptic Nasotracheal Intubation
50 Face Mask Ventilation Essential element to airway management Used during induction and as a rescue technique during failed attempts More difficult in bearded patients Using a nasal trumpet or oral airway may assist in ventilation
51 Anesthesiologist establishing mask ventilation Courtesy Cummings
52 Endotracheal Intubation First accounts of orotracheal intubation in 1000 AD by Avicenna * *Avicenna was middle eastern physician and philosopher.
53 Oroendotracheal intubation Utilizes either Macintosh or Miller Blade Macintosh is a curved laryngoscope that slides under the vallecula and lifts the entire larynx anteriorly or ventrally to expose the glottis Miller is a straight laryngoscope and is placed under the epiglottis where it sits in the petiole of the epiglottis lifting the larynx anteriorly to view the glottis If not successful on initial attempt, 3 maneuvers are helpful Place patient in modified Jackson s position Apply external laryngeal pressure Maneuver Laryngoscope After 3 failed attempts, proceed with alternative procedures
54
55 Incidence of Endotracheal Intubation Complications
56 LMA Initially introduced in the U.S in early 1990s First utilized for elective face mask cases requiring general anesthesia Has revolutionized the algorithm for difficult airway management Is fast and easy to place, even by inexperience personnel Does not offer full protection of airway from aspiration Can intubate patient through LMA
57 Inserting the LMA Miller: Miller s Anesthesia. 7 th ed.
58 Combitube Widely used in prehospital care Closed distal end designed for passage into esophagus with inflatable cuff providing seal Proximal seal achieved with facemask or oropharyngeal cuff Holes in tube between proximal seal and distal cuff deliver gases to laryngopharynx Has second open-ended tube that can function as tracheal tube if inserted into trachea

59 Semi-rigid Gum Elastic Bougie Anterior Commissure laryngoscope used to view larynx Semi-rigid gum elastic bougie introduced under direct visualization then endotracheal tube may be inserted The Difficult Airway
60 Hollinger Laryngoscope with Eschmann stylet and endotracheal tube
61 Nasotracheal Intubation Fiberoptic flexible bronchoscope is passed transnasally after passing through endotracheal tube Endoscope introduced into the subglottic trachea then endotracheal tube passed over the endoscope Contraindications include history or possible basal skull fracture Can cause damage to nasal mucosa creating epistaxis and can tear mucosa of posterior nasopharynx passing submucosally
62 Retrograde Intubation Percutaneously passing narrow flexible guide into the trachea from site below the vocal cords, advancing guide out of mouth or nose Endotracheal tube then passed over the guide into the upper part of the trachea Can perform either oral or nasal intubation
63 Retrograde Intubation (continued) Diagram on left shows stylet passed through CTM while diagram on right shows stylet from below CTM
64 Retrograde Intubation Invasive and takes time Complications: Minor bleeding Subcutaneous emphysema Pneumomediastinum Infection Contraindications: Coagulopathy Inability to identify landmarks Laryngeal disease Local infection
65 Surgical Management of the Difficult Airway Awake Tracheostomy Emergency Cricothyroidotomy Transtracheal Needle Ventilation Emergency Tracheostomy
66 Awake Tracheostomy When intubation is deemed impractical Best performed in a controlled environment Requires clear communication among surgeon, anesthesiologist, nurses, and technicians Place patient where anesthesia can have ready access to airway and to improve primary and accessory respiratory muscle function Under local anesthesia with minimal sedation to keep patient comfortable
67 Emergency Cricothyroidotomy Relatively simple, fast and with lower perioperative complication rate Cricothyroid Membrane only separated from skin by subcutaneous fat, anterior cervical fascia and strap muscles laterally Vocal cords are approximately 1 cm above Cricothyroid membrane
68 Contraindications to Cricothyroidotomy Age less than 10 years of age Severe neck trauma with inability to palpate landmarks Expanding neck hematoma Preexisting laryngeal disease with subglottic extension Planned urgent awake tracheostomy preferred
69 Procedure Palpate the landmarks Stabilize upper airway with nondominant hand is single most important factor in successful outcome Perform midline vertical skin incision Palpate membrane through incision and enter with a horizontal incision at lower edge of membrane Dilate with a hemostat or Kelly clamp Place small (5.0) endotracheal tube or tracheostomy tube
70
71
72
73
74
75
76 Transtracheal Needle Ventilation Equipment: 100% oxygen at 50 psi Large-bore needle and cannula (14 G) Luer-lok connector Puncture either trachea or Cricothyroid Membrane with saline-filled syringe in midline at 30-degree caudal direction Patient can be oxygenated for 30 minutes to 2 hours
77 Emergency Tracheostomy Slash Trach Since anoxia causes death in 4-5 minutes, so must perform within 2 or 3 minutes Perform through a vertical incision Stabilize the larynx with non-dominant hand Vertical incision through skin, platysma and subcutaneous tissue and thyroid isthmus Use index finger of non-dominant finger to help palpate and dissect Make vertical incision at second or third tracheal ring If available, use reinforced endotracheal tube
78 Outcomes of Emergency Surgical Airway Procedures in a Hospital-Wide Setting Gillespie et al. Records of 35 adult patients receiving emergency tracheotomy or cricothyroidotomy From January 1, 1993 to December 31, 1998 Patients with spontaneous ventilation and underwent urgent surgical airway access excluded Need for Emergent surgical airway: Cardiac or pulmonary arrest in 13 patients (37%) Head and neck cancer in 12 patients (34%) Trauma in 10 patients (29%)
79 Outcomes (continued) Patients unable to be treated with mask ventilation or intubation: Upper airway edema in 14 patients (40%) Difficult anatomy with inability to visualize vocal cords in 8 patients (23%) Obstructing lesion in oropharynx or larynx in 7 patients (20%) Maxillofacial or neck trauma in 6 patients (17%)
80 Outcomes (continued) Surgical airway established in 34 patients in 37 attempts (92% success) Cricothyroidotomy established in 20 of 23 attempts (87%) Tracheostomy established in 14 patients (100%)
81 Complications
82 Complications (continued) Less known about role of tracheotomy in emergency situation In study, effective 100% of attempts Emergency cricothyroidotomy associated with 13% to 40% complication rate Elective Tracheostomy has complication rate of 15%, complication rate of emergent tracheostomy thought to be 2 to 5 times higher In present study, equivalent complication rates between both procedures
83 Controversy in Cricothyroidotomy Principal long-term morbidity is subglottic stenosis Intense debate since publication of Chevalier Jackson s article on tracheostomy in 1921 discouraging the use of elective cricothyroidotomy due to high rate of subglottic stenosis High rate in study secondary to use of metal tracheostomy tubes in pediatric patients with chronic inflammatory disease of laryngotracheal framework Elective cricothyroidotomy shown to have low rate of subglottic stenosis (<1%); Avoid in patients treated with intubation for more than 7 days True incidence of subglottic and tracheal stenosis is difficult to determine as many patients lost to follow-up
84 Converting from Cricothyroidotomy to Tracheostomy Controversy surrounds whether to expeditiously convert emergency cricothyroidotomy to tracheostomy Conversion advocated by many authors to decrease incidence of subglottic stenosis DeLaurier et al questioned need to convert, 0 of 11 patients they studied who underwent cricothyroidotomy developed stenosis 2 of the 9 patients who underwent conversion developed tracheal granulation tissue secondary to tracheostomy tube Conversion did not prevent the only case of cricothyroidotomy-related subglottic stenosis Trauma patients decannulated after average of 3 days and had lower rate of complication than patients undergoing conversion to tracheostomy
85 When to consider conversion Patients requiring operative exploration for hemorrhage or other complications including suspected laryngeal cartilage injury Patients requiring long-term airway maintenance or mechanical ventilation
86 Management of the Pediatric Patient Anatomic Considerations Larynx closer to level of C3 leads to higher level of tongue and appearance of anterior larynx Proportionally larger tongues Larger, stiffer epiglottis Angle of thyroid cartilage is broader Narrowest part of airway is at level of cricoid (not true vocal cords as in adults) Large occiput makes positioning more challenging
87 Anatomic Differences
88 Anatomic Differences A: Adult Larynx, B: Pediatric Larynx
89 General Considerations in Pediatric Airway Management Resistance to flow is inversely proportional to radius of the lumen to the fourth power, makes similar changes in edema more substantial in pediatrics Estimate endotracheal tubes using formula (Age + 16)/4 = ETT size Pre-operative medications should be given that have minimal respiratory depressant effects, such as Midazolam
90 Laryngeal Mask Airway Can be easily placed and removed while inflated in children Correct size is based on patient s weight
91 Light Wand Rigid fiber optic stylet with light at its tip Blind Technique for intubation Does not depend on good mouth opening or extension of the neck Can be simpler and quicker than fiberoptic intubation, can succeed even with bleeding in airway Requires room lights dimmed Difficult to use when anatomy is distorted and laryngeal structures not midline
92 Light Wand Light wand correctly positioned in trachea. Note the tear drop appearance as light tracks to sternum
93 Flexible Fiberoptic Bronchoscope Allows operator to see around corners Advantageous in patients with poor mouth opening, limited neck movement or other conditions that make direct laryngoscopy difficult Bleeding and secretions cane make it difficult to use Keep child anesthetized but breathing spontaneously at 100% oxygen LMA is good adjunct in difficult intubation
94 Craniofacial Dysmorphologies Pierre-Robin Sequence Treacher-Collins Syndrome (mandibulofacial dysostosis) Goldenhar Syndrome (oculoauriculovertebral dysplasia) Hallerman-Streiff Syndrome (oculomanidbulodyscephaly) Mobius Syndrome Cornelia de Lange Syndrome Macroglossia with glycogen storage disease Cystic Hygroma of the tongue Fetal Alcohol Syndrome Cherubism (familial osseous dysplasia) Carpenter Syndrome Crouzon disease Freeman-Sheldon Syndrome
95 Treacher-Collins Syndrome Patients have maxillary, mandibular, and zygomatic hypoplasia Mask ventilation and tracheal intubation are difficult, impossible if there are TMJ abnormalities Sedated fiberoptic intubation or laryngeal mask placement is helpful Generally intubation improves as patients grow older Many patients require surgical airway
96 Cornelia de Lange Syndrome Courtesy Emedicine
97 Cornelia De Lange Syndrome Microcephaly Confluent eyebrows Underdeveloped orbital arches Long philtrum High arched palate and overt or submucous cleft palate Micrognathia
98 Hallerman-Streiff Syndrome Courtesy: microcephaly, malar hypoplasia, micrognathia, thin small pointed nose with hypoplasia of the cartilage (becoming parrot like), narrow and high arched palate, thin and light hair with hypotrichosis, especially of the eyebrows and eyelashes, and low set ears
99 Hallerman-Streif Syndrome Microcephaly, Malar hypoplasia, Micrognathia, Thin small pointed nose with hypoplasia of the cartilage (becoming parrot like), Narrow and high arched palate Thin and light hair with hypotrichosis, especially of the eyebrows and eyelashes Low set ears
100 Carpenter Syndrome Courtesy:
101 Carpenter Syndrome Autosomal Recessive Condition Craniosynostosis Many fusions of sutures Soft tissue syndactyly of hands and feet always present
102 Crouzon Disease Courtesy:
103 Crouzon Disease Craniosynostosis with midface hypoplasia, hypertelorism, and proptosis Patients are primarily mouth breathers Many have obstructive apnea Can have vertebral abnormalities causing limited neck mobility Can have tracheal abnormalities requiring smaller endotracheal tube Mask ventilation can be difficult
104 Freeman-Sheldon Syndrome
105 Freeman-Sheldon Syndrome Rare myopathic dysplasia Patients have mask-like facies with circumoral fibrosis and microstomia Inhalational agents are contraindicated in these patients due to increased risk of malignant hyperthermia
106 Inflexibility or Instability of Larynx Down Syndrome Juvenile Rheumatoid Arthritis Goldenhar Syndrome Klippel-Feil Syndrome
107 Laryngeal Anomalies Congenital Lesions Cricoid Ring Stenosis Subglottic Stenosis Laryngeal Webs Laryngeal Cysts Laryngoceles Subglottic Hemangiomas Bilateral True Vocal Cord Paralysis Infectious Disease Epiglottitis Respiratory Papillomatosis Croup Traumatic Injuries Foreign Bodies Chemical or Thermal Burns
108 Conclusions Very few difficult airway scenarios require a surgical airway It is best to have several back-up plans and then back-up plans for those back-up plans Know where your equipment is and how to use it The LMA has revolutionized airway management and can create time for more permanent solutions Pediatric patients have differing anatomy from adults that can be more challenging Otolaryngologists have many special skills and tools that are invaluable in the management of the difficult and emergent airway
109 References Tekin M, Bodurtha J. Cornelia De Lange Syndrome. Emedicine overview. Site visited 3/29/2011. Issaivanan M, Virdi V. Dyscephalia Mandibulo-Oculo-Facialis. Indian Pediatrics. 2001; 38: Carpenter Syndrome diseases_v2/gendis_detail_list.php?cat3=1785. Site visited on 3/29/2011 Kinsman SL, Johnston, MV. Craniosynostosis Kliegman: Nelson Textbook of Pediatrics, 18 th ed. 2007: Philadelphia, PA. Gudzenko V, Bittner EA, Schmidt UH. Emergency Airway Management. Respiratory Care. (2010) 55, Katos, MG, Goldenbery D. Emergency Cricothyrotomy. Operative Techniques in Otolaryngology. (2007) 18, Ondik MP, Kmatian S, Carr MM. Management of the difficult airway in the pediatric patient. Operative Techniques in Otolaryngology. (2007) 18, Gillespie MB, Eisele DW. Outcomes of Emergency Surgical Airway Procedures in a Hopsital-Wide Setting. Laryngoscope. (1999) 109, Infosino A. Pediatric upper airway and congenital anomalies. Anesthesiology Clin N Am. (2002) 20, Nargozian C. The airway in patients with craniofacial abnormalities. Pediatric Anesthesia. (2004) 14,
110 References Goldstein BJ, Goldenberg D. The difficult airway: Implications for the otolaryngologist-head and neck surgeon. Operative Techniques in Otolaryngology. (2007) 18, Wong E, Ng Y. The difficult airway in the emergency department. Int J Emerg Med. (2008) 1, Liess BD, Scheidt TD, Templer JW. The Difficult Airway. Otolaryngol Clin N Am. (2008) 41, Bruce IA, Rothera MP. Upper airway obstruction in children. Pediatric Anesthesia. (2009) 19, Sofferman RA, Greene CM. Complex Upper Airway Problems. Head & Neck Surgery Otolaryngology. Bailey BJ and Johnson JT, 2006; Philadelphia, PA. Weissler MC, Couch ME. Tracheotomy and Intubation. Head & Neck Surgery Otolaryngology. Bailey BJ and Johnson JT, 2006; Philadelphia, PA. Bhatti NI. Surgical Management of the Difficult Adult Airway.. Flint: Cummings Otolaryngology: Head & Neck Surgery, 5 th ed Mark L, Herzer K, Akst S, Michelson J. General Considerations of Anesthesia and Management of the Difficult Airway.. Flint: Cummings Otolaryngology: Head & Neck Surgery, 5 th ed Henderson J. Airway Management in Adults. Miller: Miller s Anesthesia, 7 th ed
AIRWAY MANAGEMENT. Angkana Lurngnateetape, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
The Difficult Airway. The Difficult Airway. Difficult Airway Algorithms: ASA. Ectopic Anesthesia. Cancel Case. Awaken. airway. Defining ng the problem
 The Difficult Airway The Difficult Airway Robert J. Vissers, MD FACEP Department of Emergency Medicine Legacy, Emanuel Hospital Defining ng the problem Defining ng the difficult d airway a Identifying
The Difficult Airway The Difficult Airway Robert J. Vissers, MD FACEP Department of Emergency Medicine Legacy, Emanuel Hospital Defining ng the problem Defining ng the difficult d airway a Identifying
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
TRACHEOSTOMY TUBE PARTS
 Page1 NR 33 TRACHEOSTOMY CARE AND SUCTIONING Review ATI Basic skills videos: Tracheostomy care and Endotracheal suction using a closed suction set. TRACHEOSTOMY TUBE PARTS Match the numbers on the diagram
Page1 NR 33 TRACHEOSTOMY CARE AND SUCTIONING Review ATI Basic skills videos: Tracheostomy care and Endotracheal suction using a closed suction set. TRACHEOSTOMY TUBE PARTS Match the numbers on the diagram
Airway assessment. Bran Retnasingham Andy McKechnie
 Airway assessment Bran Retnasingham Andy McKechnie The average Camberwell patient? Airway assessment There is one skill above all else that an anaesthetist is expected to exhibit and that is to
Airway assessment Bran Retnasingham Andy McKechnie The average Camberwell patient? Airway assessment There is one skill above all else that an anaesthetist is expected to exhibit and that is to
Neonatal Intubation. Purpose. Scope. Indications. Equipment Cardiorespiratory monitor SaO 2 monitor. Anatomic Considerations.
 Page 1 of 5 Purpose Scope Indications Neonatal Intubation To assure proper placement of endotracheal tubes for maximum ventilation using proper intubation procedures. The policy applies to all Respiratory
Page 1 of 5 Purpose Scope Indications Neonatal Intubation To assure proper placement of endotracheal tubes for maximum ventilation using proper intubation procedures. The policy applies to all Respiratory
AEROSPACE MEDICAL SERVICE SPECIALTY INDEPENDENT DUTY MEDICAL TECHNICIAN EMERGENCY MEDICINE PROCEDURES
 QTP4N0X1C-9 02 July 2015 AEROSPACE MEDICAL SERVICE SPECIALTY INDEPENDENT DUTY MEDICAL TECHNICIAN EMERGENCY MEDICINE PROCEDURES Volume 9 TOTAL FORCE, TOTAL CARE EVERYTIME, ANYWHERE 383d TRAINING SQUADRON/XUFB
QTP4N0X1C-9 02 July 2015 AEROSPACE MEDICAL SERVICE SPECIALTY INDEPENDENT DUTY MEDICAL TECHNICIAN EMERGENCY MEDICINE PROCEDURES Volume 9 TOTAL FORCE, TOTAL CARE EVERYTIME, ANYWHERE 383d TRAINING SQUADRON/XUFB
a guide to understanding pierre robin sequence
 a guide to understanding pierre robin sequence a publication of children s craniofacial association a guide to understanding pierre robin sequence this parent s guide to Pierre Robin Sequence is designed
a guide to understanding pierre robin sequence a publication of children s craniofacial association a guide to understanding pierre robin sequence this parent s guide to Pierre Robin Sequence is designed
X-Plain Trigeminal Neuralgia Reference Summary
 X-Plain Trigeminal Neuralgia Reference Summary Introduction Trigeminal neuralgia is a condition that affects about 40,000 patients in the US every year. Its treatment mostly involves the usage of oral
X-Plain Trigeminal Neuralgia Reference Summary Introduction Trigeminal neuralgia is a condition that affects about 40,000 patients in the US every year. Its treatment mostly involves the usage of oral
PRACTICE Guidelines are systematically developed
 Copyright by the American Society of Anesthesiologists. Unauthorized reproduction of this article is prohibited. Special Articles Practice Guidelines for Management
Copyright by the American Society of Anesthesiologists. Unauthorized reproduction of this article is prohibited. Special Articles Practice Guidelines for Management
Interscalene Block. Nancy A. Brown, MD
 Interscalene Block Nancy A. Brown, MD What is an Interscalene Block? An Interscalene block is a form of regional anesthesia used in conjunction with general anesthesia for surgeries of the shoulder and
Interscalene Block Nancy A. Brown, MD What is an Interscalene Block? An Interscalene block is a form of regional anesthesia used in conjunction with general anesthesia for surgeries of the shoulder and
Medical Coverage Policy Monitored Anesthesia Care (MAC)
") Medical Coverage Policy Monitored Anesthesia Care (MAC) Device/Equipment Drug Medical Surgery Test Other Effective Date: 9/1/2004 Policy Last Updated: 1/8/2013 Prospective review is recommended/required.
Medical Coverage Policy Monitored Anesthesia Care (MAC) Device/Equipment Drug Medical Surgery Test Other Effective Date: 9/1/2004 Policy Last Updated: 1/8/2013 Prospective review is recommended/required.
Laryngeal Mask Airways (LMA), Indications and Use for the Pre-Hospital Provider. www.umke.org
, Indications and Use for the Pre-Hospital Provider. www.umke.org") Laryngeal Mask Airways (LMA), Indications and Use for the Pre-Hospital Provider Objectives: Identify the indications, contraindications and side effects of LMA use. Identify the equipment necessary for
Laryngeal Mask Airways (LMA), Indications and Use for the Pre-Hospital Provider Objectives: Identify the indications, contraindications and side effects of LMA use. Identify the equipment necessary for
Perioperative Management of Patients with Obstructive Sleep Apnea. Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine
 Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
Continued on next page
 Resident Journal Review An Update on Airway Management in Emergency Medicine Authors: Michael Allison, MD; Michael Scott, MD; Kami Hu, MD; David Bostick, MD; Daniel Boutsikaris, MD Edited by: Michael C.
Resident Journal Review An Update on Airway Management in Emergency Medicine Authors: Michael Allison, MD; Michael Scott, MD; Kami Hu, MD; David Bostick, MD; Daniel Boutsikaris, MD Edited by: Michael C.
Virginia Office of Emergency Medical Services Scope of Practice - Procedures for EMS Personnel
 Specific tasks in this document shall refer to the Virginia Education Standards. AIRWAY TECHNIQUES Airway Adjuncts Airway Maneuvers Alternate Airway Devices Cricothyrotomy Obstructed Airway Clearance Intubation
Specific tasks in this document shall refer to the Virginia Education Standards. AIRWAY TECHNIQUES Airway Adjuncts Airway Maneuvers Alternate Airway Devices Cricothyrotomy Obstructed Airway Clearance Intubation
Airway and Breathing Skills Levels Interpretive Guidelines
 Office of Emergency Medical Services and Trauma INDEX EFFECTIVE LAST REVIEW PAGES VERSION R-P11A 7/1/2011 7/1/2011 5 2011 Scope of Practice for EMS Personnel Emergency Medical Personnel are permitted to
Office of Emergency Medical Services and Trauma INDEX EFFECTIVE LAST REVIEW PAGES VERSION R-P11A 7/1/2011 7/1/2011 5 2011 Scope of Practice for EMS Personnel Emergency Medical Personnel are permitted to
PHSW Procedural Sedation Post-Test Answer Key. For the following questions, circle the letter of the correct answer(s) or the word true or false.
 or the word true or false.") PHSW Procedural Sedation Post-Test Answer Key 1 1. Define Procedural (Conscious) Sedation: A medically controlled state of depressed consciousness where the patient retains the ability to continuously
PHSW Procedural Sedation Post-Test Answer Key 1 1. Define Procedural (Conscious) Sedation: A medically controlled state of depressed consciousness where the patient retains the ability to continuously
Procedure -8. Intraosseous Infusion Adult and Pediatric EZIO. Page 1 of 7 APPROVED:
 Page 1 of 7 Intraosseous Infusion Adult and Pediatric APPROVED: EMS Medical Director EMS Administrator 1. Goals/Introduction: 1.1 Intraosseous (IO) infusion provides an effective alternative means of providing
Page 1 of 7 Intraosseous Infusion Adult and Pediatric APPROVED: EMS Medical Director EMS Administrator 1. Goals/Introduction: 1.1 Intraosseous (IO) infusion provides an effective alternative means of providing
The American Society of Anesthesiologists (ASA) has defined MAC as:
 has defined MAC as:") Medical Coverage Policy Monitored Anesthesia Care (MAC) sad EFFECTIVE DATE: 09 01 2004 POLICY LAST UPDATED: 11 04 2014 OVERVIEW The intent of this policy is to address anesthesia services for diagnostic
Medical Coverage Policy Monitored Anesthesia Care (MAC) sad EFFECTIVE DATE: 09 01 2004 POLICY LAST UPDATED: 11 04 2014 OVERVIEW The intent of this policy is to address anesthesia services for diagnostic
One Lung Ventilation Module (OLV)
") 1 One Lung Ventilation Module (OLV) A Thoracic Surgery Directors Association (TSDA) Cardiothoracic Surgery Resident Boot Camp Syllabus The ability to isolate one of the lungs is an essential skill set
1 One Lung Ventilation Module (OLV) A Thoracic Surgery Directors Association (TSDA) Cardiothoracic Surgery Resident Boot Camp Syllabus The ability to isolate one of the lungs is an essential skill set
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
a guide to understanding moebius syndrome a publication of children s craniofacial association
 a guide to understanding moebius syndrome a publication of children s craniofacial association a guide to understanding moebius syndrome this parent s guide to Moebius syndrome is designed to answer questions
a guide to understanding moebius syndrome a publication of children s craniofacial association a guide to understanding moebius syndrome this parent s guide to Moebius syndrome is designed to answer questions
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings
 AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE
AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE
Coventry Airway Management course
 Airway workshops The workshops are based on DAS Guidelines for managing un-anticipated difficult intubation. In addition lung isolation techniques workshop is recently introduced to this course. The aim
Airway workshops The workshops are based on DAS Guidelines for managing un-anticipated difficult intubation. In addition lung isolation techniques workshop is recently introduced to this course. The aim
EYE, EAR, NOSE, and THROAT INJURIES
 T6 EYE, EAR, NOSE, and THROAT INJURIES Management of injuries of the eyes, ears, nose, and throat focuses on airway management and initial stabilization of the injury. Bilateral comparisons can assist
T6 EYE, EAR, NOSE, and THROAT INJURIES Management of injuries of the eyes, ears, nose, and throat focuses on airway management and initial stabilization of the injury. Bilateral comparisons can assist
Respiratory System. Chapter 21
 Respiratory System Chapter 21 Structural Anatomy Upper respiratory system Lower respiratory system throat windpipe voice box Function of Respiratory System Gas exchange Contains receptors for sense of
Respiratory System Chapter 21 Structural Anatomy Upper respiratory system Lower respiratory system throat windpipe voice box Function of Respiratory System Gas exchange Contains receptors for sense of
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
THE AIRWAY IN AEROMEDICAL EVACUATION. PBLD (Problem Based Learning Discussion)
") THE AIRWAY IN AEROMEDICAL EVACUATION PBLD (Problem Based Learning Discussion) D. John Doyle MD PhD 2012 Edition Image Credit: http://www.arabianaerospace.aero/media/images/stories/medevac%20services.jpg
THE AIRWAY IN AEROMEDICAL EVACUATION PBLD (Problem Based Learning Discussion) D. John Doyle MD PhD 2012 Edition Image Credit: http://www.arabianaerospace.aero/media/images/stories/medevac%20services.jpg
1.4.4 Oxyhemoglobin desaturation
 Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Clinical Monitoring Title: Monitoring of Patients Undergoing Conscious Sedation Policy #: 09 Revised: 05/00 1.0 DESCRIPTION
Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Clinical Monitoring Title: Monitoring of Patients Undergoing Conscious Sedation Policy #: 09 Revised: 05/00 1.0 DESCRIPTION
Respiratory Concerns in Children with Down Syndrome
 Respiratory Concerns in Children with Down Syndrome Paul E. Moore, M.D. Associate Professor of Pediatrics and Pharmacology Director, Pediatric Allergy, Immunology, and Pulmonary Medicine Vanderbilt University
Respiratory Concerns in Children with Down Syndrome Paul E. Moore, M.D. Associate Professor of Pediatrics and Pharmacology Director, Pediatric Allergy, Immunology, and Pulmonary Medicine Vanderbilt University
UC Davis Medical Center Emergency Medicine Airway Equipment: Contents, Cleaning and Stocking
 UC Davis Medical Center Emergency Medicine Airway Equipment: Contents, Cleaning and Stocking Introduction: Due to the large volume of critically ill patients who present for care at the U.C. Davis Emergency
UC Davis Medical Center Emergency Medicine Airway Equipment: Contents, Cleaning and Stocking Introduction: Due to the large volume of critically ill patients who present for care at the U.C. Davis Emergency
PROCEDURAL SEDATION/ANALGESIA NCBON Position Statement for RN Practice
 PROCEDURAL SEDATION/ANALGESIA NCBON Position Statement for RN Practice P.O. BOX 2129 Raleigh, NC 27602 (919) 782-3211 FAX (919) 781-9461 Nurse Aide II Registry (919) 782-7499 www.ncbon.com Issue: Administration
PROCEDURAL SEDATION/ANALGESIA NCBON Position Statement for RN Practice P.O. BOX 2129 Raleigh, NC 27602 (919) 782-3211 FAX (919) 781-9461 Nurse Aide II Registry (919) 782-7499 www.ncbon.com Issue: Administration
Feline Anesthesia Richard M. Bednarski, DVM, MSc The Ohio State University College of Veterinary Medicine Current Issues in Feline Anesthesia
 Feline Anesthesia Richard M. Bednarski, DVM, MSc The Ohio State University College of Veterinary Medicine Current Issues in Feline Anesthesia Chemical Restraint Protocols Trap, Neuter, Release Anesthetic
Feline Anesthesia Richard M. Bednarski, DVM, MSc The Ohio State University College of Veterinary Medicine Current Issues in Feline Anesthesia Chemical Restraint Protocols Trap, Neuter, Release Anesthetic
Goals and Objectives for the General Surgery Rotation Resident PGY1 Hamilton Health Sciences or St. Joseph Healthcare (2 four-week rotational blocks)
") Goals and Objectives for the General Surgery Rotation Resident PGY1 Hamilton Health Sciences or St. Joseph Healthcare (2 four-week rotational blocks) Overview During the first year of their residency training
Goals and Objectives for the General Surgery Rotation Resident PGY1 Hamilton Health Sciences or St. Joseph Healthcare (2 four-week rotational blocks) Overview During the first year of their residency training
Acute Respiratory Failure
 Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine mark.tieszen@sanfordhealth.org Acute Respiratory
Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine mark.tieszen@sanfordhealth.org Acute Respiratory
X-Plain Sinus Surgery Reference Summary
 X-Plain Sinus Surgery Reference Summary Introduction Sinus surgery is a very common and safe operation. Your doctor may recommend that you have sinus surgery. The decision whether or not to have sinus
X-Plain Sinus Surgery Reference Summary Introduction Sinus surgery is a very common and safe operation. Your doctor may recommend that you have sinus surgery. The decision whether or not to have sinus
Department of Surgery
 What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
What is emphysema? 2004 Regents of the University of Michigan Emphysema is a chronic disease of the lungs characterized by thinning and overexpansion of the lung-like blisters (bullae) in the lung tissue.
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
General Thoracic Surgery ICD9 to ICD10 Crosswalks. C34.11 Malignant neoplasm of upper lobe, right bronchus or lung
 ICD-9 Code ICD-9 Description ICD-10 Code ICD-10 Description 150.3 Malignant neoplasm of upper third of esophagus C15.3 Malignant neoplasm of upper third of esophagus 150.4 Malignant neoplasm of middle
ICD-9 Code ICD-9 Description ICD-10 Code ICD-10 Description 150.3 Malignant neoplasm of upper third of esophagus C15.3 Malignant neoplasm of upper third of esophagus 150.4 Malignant neoplasm of middle
2.06 Understand the functions and disorders of the respiratory system
 2.06 Understand the functions and disorders of the respiratory system 2.06 Understand the functions and disorders of the respiratory system Essential questions What are the functions of the respiratory
2.06 Understand the functions and disorders of the respiratory system 2.06 Understand the functions and disorders of the respiratory system Essential questions What are the functions of the respiratory
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
AWAKE FIBREOPTIC INTUBATION THE BASICS ANAESTHESIA TUTORIAL OF THE WEEK 201
 AWAKE FIBREOPTIC INTUBATION THE BASICS ANAESTHESIA TUTORIAL OF THE WEEK 201 18 TH OCTOBER 2010 Dr S Kritzinger Registrar in Anaesthetics Pinderfields General Hospital, Wakefield, UK Dr M van Greunen Consultant
AWAKE FIBREOPTIC INTUBATION THE BASICS ANAESTHESIA TUTORIAL OF THE WEEK 201 18 TH OCTOBER 2010 Dr S Kritzinger Registrar in Anaesthetics Pinderfields General Hospital, Wakefield, UK Dr M van Greunen Consultant
Treatment of Maxillary Sinusitis Using the SinuSys Vent-Os Sinus Dilation System
 White PAPer Treatment of Maxillary Sinusitis Using the SinuSys Vent-Os Sinus Dilation System Jerome Hester, MD Chief Medical Officer SinuSys Corporation Palo Alto, California USA introduction Establishment
White PAPer Treatment of Maxillary Sinusitis Using the SinuSys Vent-Os Sinus Dilation System Jerome Hester, MD Chief Medical Officer SinuSys Corporation Palo Alto, California USA introduction Establishment
Department of Veterans Affairs VHA DIRECTIVE 2012-032 Veterans Health Administration Washington, DC 20420 October 26, 2012
 Department of Veterans Affairs VHA DIRECTIVE 2012-032 Veterans Health Administration Washington, DC 20420 OUT OF OPERATING ROOM AIRWAY MANAGEMENT 1. PURPOSE: This Veterans Health Administration (VHA) Directive
Department of Veterans Affairs VHA DIRECTIVE 2012-032 Veterans Health Administration Washington, DC 20420 OUT OF OPERATING ROOM AIRWAY MANAGEMENT 1. PURPOSE: This Veterans Health Administration (VHA) Directive
Program Specification for Master Degree Anesthesia, ICU and Pain Management
 Cairo University Faculty of Medicine Program type: Single Program Specification for Master Degree Anesthesia, ICU and Pain Management Department offering program: Anesthesia, intensive care and pain management
Cairo University Faculty of Medicine Program type: Single Program Specification for Master Degree Anesthesia, ICU and Pain Management Department offering program: Anesthesia, intensive care and pain management
COMPLICATIONS OF SUSPENSION LARYNGOSCOPY
 Ann Otol Rhinol Laryngol 111:2002 Ann Otol Rhinol Laryngol 111:2002 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY November 2002 Volume 111 Number 11 COPYRIGHT 2002, ANNALS PUBLISHING COMPANY
Ann Otol Rhinol Laryngol 111:2002 Ann Otol Rhinol Laryngol 111:2002 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY November 2002 Volume 111 Number 11 COPYRIGHT 2002, ANNALS PUBLISHING COMPANY
Minimally Invasive Spine Surgery
 Chapter 1 Minimally Invasive Spine Surgery 1 H.M. Mayer Primum non nocere First do no harm In the long history of surgery it always has been a basic principle to restrict the iatrogenic trauma done to
Chapter 1 Minimally Invasive Spine Surgery 1 H.M. Mayer Primum non nocere First do no harm In the long history of surgery it always has been a basic principle to restrict the iatrogenic trauma done to
New 7/1/2015 MCFRS 1
 New 7/1/2015 MCFRS 1 The providers will summarize the need for this change from an epinephrine auto injector The provider will define the proper dosage of epinephrine for the adult and pediatric patient
New 7/1/2015 MCFRS 1 The providers will summarize the need for this change from an epinephrine auto injector The provider will define the proper dosage of epinephrine for the adult and pediatric patient
Why is prematurity a concern?
 Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Conundrums in Ambulatory Anesthesia I
 THE UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DALLAS Parkland Hospital, Dallas, Texas Conundrums in Ambulatory Anesthesia I Girish P. Joshi, MBBS, MD, FFARCSI Professor of Anesthesiology and Pain
THE UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DALLAS Parkland Hospital, Dallas, Texas Conundrums in Ambulatory Anesthesia I Girish P. Joshi, MBBS, MD, FFARCSI Professor of Anesthesiology and Pain
Corporate Medical Policy
 File Name: anesthesia_services Origination: 8/2007 Last CAP Review: 1/2016 Next CAP Review: 1/2017 Last Review: 1/2016 Corporate Medical Policy Description of Procedure or Service There are three main
File Name: anesthesia_services Origination: 8/2007 Last CAP Review: 1/2016 Next CAP Review: 1/2017 Last Review: 1/2016 Corporate Medical Policy Description of Procedure or Service There are three main
Integumentary System Individual Exercises
 Integumentary System Individual Exercises 1. A physician performs an incision and drainage of a subcutaneous abscess in his office for a particularly uncooperative established patient. How should this
Integumentary System Individual Exercises 1. A physician performs an incision and drainage of a subcutaneous abscess in his office for a particularly uncooperative established patient. How should this
Epidural Continuous Infusion. Patient information Leaflet
 Epidural Continuous Infusion Patient information Leaflet April 2015 Introduction You may already know that epidural s are often used to treat pain during childbirth. This same technique can also used as
Epidural Continuous Infusion Patient information Leaflet April 2015 Introduction You may already know that epidural s are often used to treat pain during childbirth. This same technique can also used as
ENT Emergencies. Injuries of the Neck. Registrar Dept Trauma and emergency Medicine Tygerberg Hospital
 ENT Emergencies Injuries of the Neck Registrar Dept Trauma and emergency Medicine Tygerberg Hospital Neck Injuries Blunt and Penetrating Trauma Blunt Injuries Blunt trauma direct/indirect Trauma to larynx
ENT Emergencies Injuries of the Neck Registrar Dept Trauma and emergency Medicine Tygerberg Hospital Neck Injuries Blunt and Penetrating Trauma Blunt Injuries Blunt trauma direct/indirect Trauma to larynx
Anatomy and Physiology: Understanding the Importance of CPR
 Anatomy and Physiology: Understanding the Importance of CPR Overview This document gives you more information about the body s structure (anatomy) and function (physiology). This information will help
Anatomy and Physiology: Understanding the Importance of CPR Overview This document gives you more information about the body s structure (anatomy) and function (physiology). This information will help
INTERNATIONAL MEDICAL COLLEGE
 INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Basic modules: List of individual modules Basic Module 1 Basic principles of general and dental medicine
INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Basic modules: List of individual modules Basic Module 1 Basic principles of general and dental medicine
The EMT Instructional Guidelines in this section include all the topics and material at the EMR level PLUS the following material:
 Airway Management, Respiration and Artificial Ventilation EMR Applies knowledge (fundamental depth, foundational breadth) of general anatomy and physiology to assure a patent airway, adequate mechanical
Airway Management, Respiration and Artificial Ventilation EMR Applies knowledge (fundamental depth, foundational breadth) of general anatomy and physiology to assure a patent airway, adequate mechanical
Patient Information. Posterior Cervical Surgery. Here to help. Respond Deliver & Enable
 Here to help Our Health Information Centre (HIC) provides advice and information on a wide range of health-related topics. We also offer: Services for people with disabilities. Information in large print,
Here to help Our Health Information Centre (HIC) provides advice and information on a wide range of health-related topics. We also offer: Services for people with disabilities. Information in large print,
Community Ambulance Service of Minot ALS Standing Orders Legend
 Legend Indicates General Information and Guidelines Indicates Procedures Indicates Medication Administration Indicates Referral to Other Protocol Indicates Referral to Online Medical Direction Pediatric
Legend Indicates General Information and Guidelines Indicates Procedures Indicates Medication Administration Indicates Referral to Other Protocol Indicates Referral to Online Medical Direction Pediatric
Liposuction GUIDELINE
 .goo NON HOSPITAL MEDICAL AND SURGICAL FACILITIES PROGRAM College of Physicians and Surgeons of British Columbia Liposuction GUIDELINE You may download, print or make a copy of this material for your noncommercial
.goo NON HOSPITAL MEDICAL AND SURGICAL FACILITIES PROGRAM College of Physicians and Surgeons of British Columbia Liposuction GUIDELINE You may download, print or make a copy of this material for your noncommercial
Difficult Pre-hospital Airway Management
 Difficult Pre-hospital Airway Management Frans L. Rutten, MD, FDSA Elisabeth Hospital Tilburg, The Netherlands In management of patients with an emergency, airway management and ventilatory care are the
Difficult Pre-hospital Airway Management Frans L. Rutten, MD, FDSA Elisabeth Hospital Tilburg, The Netherlands In management of patients with an emergency, airway management and ventilatory care are the
Posterior Cervical Decompression
 Posterior Cervical Decompression Spinal Unit Tel: 01473 702032 or 702097 Issue 2: January 2009 Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed with a
Posterior Cervical Decompression Spinal Unit Tel: 01473 702032 or 702097 Issue 2: January 2009 Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed with a
Medical Review Criteria Dental and Oral Surgery Services
 Medical Review Criteria Dental and Oral Surgery Services Effective Date: April 13, 2016 Subject: Dental and Oral Surgery Services Policy: HPHC covers medically necessary dental/oral surgery services included
Medical Review Criteria Dental and Oral Surgery Services Effective Date: April 13, 2016 Subject: Dental and Oral Surgery Services Policy: HPHC covers medically necessary dental/oral surgery services included
Airway Management. J. D Urbano. For the Respiratory Therapist. Because at the Head of Every Team is a Respiratory Therapist
 Airway Management For the Respiratory Therapist J. D Urbano Respiratory Therapists are highly trained and specialized members of the allied healthcare arsenal. They deal directly with patients who suffer
Airway Management For the Respiratory Therapist J. D Urbano Respiratory Therapists are highly trained and specialized members of the allied healthcare arsenal. They deal directly with patients who suffer
5/30/2014 OBJECTIVES THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM. Disclosure
 THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log
 and Emergency Medical Responder (EMR) Progress Log") First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
TRANSPORT OF CRITICALLY ILL PATIENTS
 TRANSPORT OF CRITICALLY ILL PATIENTS Introduction Inter-hospital and intra-hospital transport of critically ill patients places the patient at risk of adverse events and increased morbidity and mortality.
TRANSPORT OF CRITICALLY ILL PATIENTS Introduction Inter-hospital and intra-hospital transport of critically ill patients places the patient at risk of adverse events and increased morbidity and mortality.
SAMPLE. Anesthesia Services. An essential coding, billing, and reimbursement resource for anesthesiology and pain management ICD-10
 Coding and Payment Guide www.optumcoding.com Anesthesia Services An essential coding, billing, and reimbursement resource for anesthesiology and pain management 2017 a ICD10 A full suite of resources including
Coding and Payment Guide www.optumcoding.com Anesthesia Services An essential coding, billing, and reimbursement resource for anesthesiology and pain management 2017 a ICD10 A full suite of resources including
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center
 Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
a guide to understanding crouzon syndrome a publication of children s craniofacial association
 a guide to understanding crouzon syndrome a publication of children s craniofacial association a guide to understanding crouzon syndrome this parent s guide to Crouzon syndrome is designed to answer questions
a guide to understanding crouzon syndrome a publication of children s craniofacial association a guide to understanding crouzon syndrome this parent s guide to Crouzon syndrome is designed to answer questions
Canine Tactical Combat Casualty Care
 Canine Tactical Combat Casualty Care The following C-TCC guidelines are based on human C-TCCC guidelines and the limited data available on combat injuries and field treatment of working dogs. These guideline
Canine Tactical Combat Casualty Care The following C-TCC guidelines are based on human C-TCCC guidelines and the limited data available on combat injuries and field treatment of working dogs. These guideline
PLASTIC SURGERY RESIDENTS HANDBOOK
 PLASTIC SURGERY RESIDENTS HANDBOOK I. PLASTIC SURGERY REQUIREMENTS a. AACPS Post Interview Communication Guidelines b. General Competencies c. Plastic Surgery Goals & Objectives d. ACGME Required Index
PLASTIC SURGERY RESIDENTS HANDBOOK I. PLASTIC SURGERY REQUIREMENTS a. AACPS Post Interview Communication Guidelines b. General Competencies c. Plastic Surgery Goals & Objectives d. ACGME Required Index
What is Balloon Sinuplasty?
 What is Balloon Sinuplasty? The painful symptoms associated with chronic sinusitis can be overwhelming. If symptoms are difficult to control with medications alone, your primary doctor may refer you to
What is Balloon Sinuplasty? The painful symptoms associated with chronic sinusitis can be overwhelming. If symptoms are difficult to control with medications alone, your primary doctor may refer you to
Vascular Access. Chapter 3
 Vascular Access Chapter 3 Vascular Access Introduction Obtaining vascular access in infants and children can be difficult even under optimal conditions. Attempting emergent access in a hypotensive, struggling
Vascular Access Chapter 3 Vascular Access Introduction Obtaining vascular access in infants and children can be difficult even under optimal conditions. Attempting emergent access in a hypotensive, struggling
Enables MDA Medical Teams to categorize victims in mass casualty scenarios, in order to be able to triage and treat casualties
 MDA Disposable ALS + BLS Medical Ambulance Equipment Prices shown in CDN. Funds Items Description Picture Mass Casualty ID tag 1000 units = $350 Enables MDA Medical Teams to categorize victims in mass
MDA Disposable ALS + BLS Medical Ambulance Equipment Prices shown in CDN. Funds Items Description Picture Mass Casualty ID tag 1000 units = $350 Enables MDA Medical Teams to categorize victims in mass
First Responder: The National EMS Scope of Practice changes the name to Emergency Medical Responder.
 APPROVED SCOPE 2/8/08 BOARD MTG First Responder: The National EMS Scope of Practice changes the name to Emergency Medical Responder. Emergency Medical Responder (EMR) Description of the Profession The
APPROVED SCOPE 2/8/08 BOARD MTG First Responder: The National EMS Scope of Practice changes the name to Emergency Medical Responder. Emergency Medical Responder (EMR) Description of the Profession The
THE LUNGS IN MARFAN SYNDROME
 THE LUNGS IN MARFAN SYNDROME Many people with Marfan syndrome and some related disorders experience pulmonary complications, or problems with their lungs. If you have Marfan syndrome, it is important for
THE LUNGS IN MARFAN SYNDROME Many people with Marfan syndrome and some related disorders experience pulmonary complications, or problems with their lungs. If you have Marfan syndrome, it is important for
Chapter 2 - Anatomy & Physiology of the Respiratory System
 Chapter 2 - Anatomy & Physiology of the Respiratory System Written by - AH Kendrick & C Newall 2.1 Introduction 2.2 Gross Anatomy of the Lungs, 2.3 Anatomy of the Thorax, 2.4 Anatomy and Histology of the
Chapter 2 - Anatomy & Physiology of the Respiratory System Written by - AH Kendrick & C Newall 2.1 Introduction 2.2 Gross Anatomy of the Lungs, 2.3 Anatomy of the Thorax, 2.4 Anatomy and Histology of the
THYMECTOMY. Thymectomy. Common questions patients ask about thymectomies. www.myasthenia.org
 THYMECTOMY Thymectomy Common questions patients ask about thymectomies. www.myasthenia.org The following are some of the most common questions asked when a thymectomy is being considered for adult and
THYMECTOMY Thymectomy Common questions patients ask about thymectomies. www.myasthenia.org The following are some of the most common questions asked when a thymectomy is being considered for adult and
Plantar Fascia Release
 Plantar Fascia Release Introduction Plantar fasciitis is a common condition that causes pain around the heel. It may be severe enough to affect regular activities. If other treatments are unsuccessful,
Plantar Fascia Release Introduction Plantar fasciitis is a common condition that causes pain around the heel. It may be severe enough to affect regular activities. If other treatments are unsuccessful,
Ankle Block. Indications The ankle block is suitable for the following: Orthopedic and podiatry surgical procedures of the distal foot.
 Ankle Block The ankle block is a common peripheral nerve block. It is useful for procedures of the foot and toes, as long as a tourniquet is not required above the ankle. It is a safe and effective technique.
Ankle Block The ankle block is a common peripheral nerve block. It is useful for procedures of the foot and toes, as long as a tourniquet is not required above the ankle. It is a safe and effective technique.
UNMH Oral and Maxillofacial Surgery Clinical Privileges
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 09/26/2014 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 09/26/2014 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
Patient Care Services Policy & Procedure Title: No. 8720-0059
 Page: 1 of 8 I. SCOPE: This policy applies to Saint Francis Hospital, its employees, medical staff, contractors, patients and visitors regardless of service location or category of patient. This policy
Page: 1 of 8 I. SCOPE: This policy applies to Saint Francis Hospital, its employees, medical staff, contractors, patients and visitors regardless of service location or category of patient. This policy
Minimally Invasive Hip Replacement through the Direct Lateral Approach
 Surgical Technique INNOVATIONS IN MINIMALLY INVASIVE JOINT SURGERY Minimally Invasive Hip Replacement through the Direct Lateral Approach *smith&nephew Introduction Prosthetic replacement of the hip joint
Surgical Technique INNOVATIONS IN MINIMALLY INVASIVE JOINT SURGERY Minimally Invasive Hip Replacement through the Direct Lateral Approach *smith&nephew Introduction Prosthetic replacement of the hip joint
GENERAL OTOLARYNGOLOGY HEAD and NECK SURGICAL ONCOLOGY. MEE General ORL/Head and Neck Rotation - PGY 2,3,4,5 Longwood Rotation - PGY 2,3,4,5
 GENERAL OTOLARYNGOLOGY HEAD and NECK SURGICAL ONCOLOGY 1. BRIEF DESCRIPTION Training in general otolaryngology, upper aerodigestive tract endoscopy and head and neck oncologic surgery begins and continues
GENERAL OTOLARYNGOLOGY HEAD and NECK SURGICAL ONCOLOGY 1. BRIEF DESCRIPTION Training in general otolaryngology, upper aerodigestive tract endoscopy and head and neck oncologic surgery begins and continues
A. function: supplies body with oxygen and removes carbon dioxide. a. O2 diffuses from air into pulmonary capillary blood
 A. function: supplies body with oxygen and removes carbon dioxide 1. ventilation = movement of air into and out of lungs 2. diffusion: B. organization a. O2 diffuses from air into pulmonary capillary blood
A. function: supplies body with oxygen and removes carbon dioxide 1. ventilation = movement of air into and out of lungs 2. diffusion: B. organization a. O2 diffuses from air into pulmonary capillary blood
The Difficult Airway in Head and Neck Tumor Surgery. Niels F. Jensen, MD. Jonathan L. Benumof, MD
 1 The Difficult Airway in Head and Neck Tumor Surgery Niels F. Jensen, MD Jonathan L. Benumof, MD 1. Assistant Professor, Department of Anesthesiology, University of Iowa 2. Professor, Department of Anesthesiology,
1 The Difficult Airway in Head and Neck Tumor Surgery Niels F. Jensen, MD Jonathan L. Benumof, MD 1. Assistant Professor, Department of Anesthesiology, University of Iowa 2. Professor, Department of Anesthesiology,
Information for the Patient About Surgical
 Information for the Patient About Surgical Decompression and Stabilization of the Spine Aging and the Spine Daily wear and tear, along with disc degeneration due to aging and injury, are common causes
Information for the Patient About Surgical Decompression and Stabilization of the Spine Aging and the Spine Daily wear and tear, along with disc degeneration due to aging and injury, are common causes
What You Should Know About Cerebral Aneurysms
 What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Interventions Committee of the American Heart Association Cardiovascular Radiology Council Randall T. Higashida, M.D.,
What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Interventions Committee of the American Heart Association Cardiovascular Radiology Council Randall T. Higashida, M.D.,
RESPIRATORY VENTILATION Page 1
 Page 1 VENTILATION PARAMETERS A. Lung Volumes 1. Basic volumes: elements a. Tidal Volume (V T, TV): volume of gas exchanged each breath; can change as ventilation pattern changes b. Inspiratory Reserve
Page 1 VENTILATION PARAMETERS A. Lung Volumes 1. Basic volumes: elements a. Tidal Volume (V T, TV): volume of gas exchanged each breath; can change as ventilation pattern changes b. Inspiratory Reserve
LASER Safety in the Operating Room. Andrew Dick Resident Research Night February 20 th, 2008
 LASER Safety in the Operating Room Andrew Dick Resident Research Night February 20 th, 2008 LASER LASER is an Acronym Light Amplification by Stimulated Emission of Radiation Lasers work on several principles
LASER Safety in the Operating Room Andrew Dick Resident Research Night February 20 th, 2008 LASER LASER is an Acronym Light Amplification by Stimulated Emission of Radiation Lasers work on several principles
LESSON 4 ORAL, NASOPHARYNGEAL, AND NASOTRACHEAL SUCTIONING.
 LESSON 4 ORAL, NASOPHARYNGEAL, AND NASOTRACHEAL SUCTIONING. 4-1. SUCTIONING a. Suctioning is a common nursing activity performed for the purpose of removing accumulated secretions from the patient's nose,
LESSON 4 ORAL, NASOPHARYNGEAL, AND NASOTRACHEAL SUCTIONING. 4-1. SUCTIONING a. Suctioning is a common nursing activity performed for the purpose of removing accumulated secretions from the patient's nose,
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES
 APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
I) Rotation Goals. Teaching Methods
 Rotation Goals. Teaching Methods") I) Rotation Goals UNMC Anesthesia Rotation Rotation Goals and Objectives Pulmonary/Critical Care Medicine Fellowship Program University of Nebraska Medical Center Revised: 3/2016 A) To manage patients
I) Rotation Goals UNMC Anesthesia Rotation Rotation Goals and Objectives Pulmonary/Critical Care Medicine Fellowship Program University of Nebraska Medical Center Revised: 3/2016 A) To manage patients
INFORMED CONSENT DERMABRASION
 INFORMED CONSENT DERMABRASION INSTRUCTION This is an informed-consent document which has been prepared to help your plastic surgeon inform you about dermabrasion, its risks, and alternative treatments.
INFORMED CONSENT DERMABRASION INSTRUCTION This is an informed-consent document which has been prepared to help your plastic surgeon inform you about dermabrasion, its risks, and alternative treatments.
IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Level IA: Submental Group
 Level IA: Submental Group") IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Fig. 1 The level system is used for describing the location of lymph nodes in the neck: Level I, submental and submandibular group; Level II, upper jugular
IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Fig. 1 The level system is used for describing the location of lymph nodes in the neck: Level I, submental and submandibular group; Level II, upper jugular
Human Capital Development & Education Program Proposal
 Human Capital Development & Education Program Proposal Cardiology & Cardiovascular Surgery Emergency Medicine Respiratory Medicine Infection Control HMIS 1 (15 Courses) Module 1/2 1/15 Course Title : Management
Human Capital Development & Education Program Proposal Cardiology & Cardiovascular Surgery Emergency Medicine Respiratory Medicine Infection Control HMIS 1 (15 Courses) Module 1/2 1/15 Course Title : Management