Chronic Kidney Disease. Nervik Roy, D.O. Internal Medicine, PGY-3 Valley Hospital Medical Center
|
|
|
- Roberta Hudson
- 3 years ago
- Views:
Transcription
1 Chronic Kidney Disease Nervik Roy, D.O. Internal Medicine, PGY-3 Valley Hospital Medical Center 1
2 Disclosures No financial disclosures unfortunately 2
3 Introduction It is estimated that over 1 in 7 Americans (~15% of the population amassing ~37 million people) have CKD But, 9 in 10 American Adults who have CKD are not aware of their diagnosis. CKD is the most common cause of patients requiring Dialysis and Kidney Transplants. Patient s with CKD are at higher risk for early death than patient s with normal Kidney function. 3
4 Largest risk factors most adults are with Diabetes Mellitus and Hypertension children and adolescents younger than 18 years, polycystic kidney disease and glomerulonephritis (inflammation of the kidneys) are the main causes of CKD/ESRD. Certain agents (Over-the-counter pain medicines like ibuprofen and naproxen, Some antibiotics, and PPIs such as omeprazole and lansoprazole) can be considered nephrotoxic and large amounts over a long time can cause CKD or quicker progression to ESRD. Some other agents that can harm the kidney are contrast dyes. Kidney stones or Urinary outlet obstructions (BPH) can also lead to CKD. 4
5 The most definitive treatment to ESRD is Kidney transplant However, Transplant list is between 3-5 years and can last up to 8-10 years, depending on variety of factors. Any patient that has CKD should be followed by a Nephrologist 5
6 What is CKD? Chronic kidney disease (CKD) is defined as abnormal kidney structure or function present for >3 months. Structure Horseshoe kidney? Kidney Transplant? One singular kidney? PCKD? Function: CKD is stratified into stages 1 to 5 based on estimated glomerular filtration rate (egfr). 6
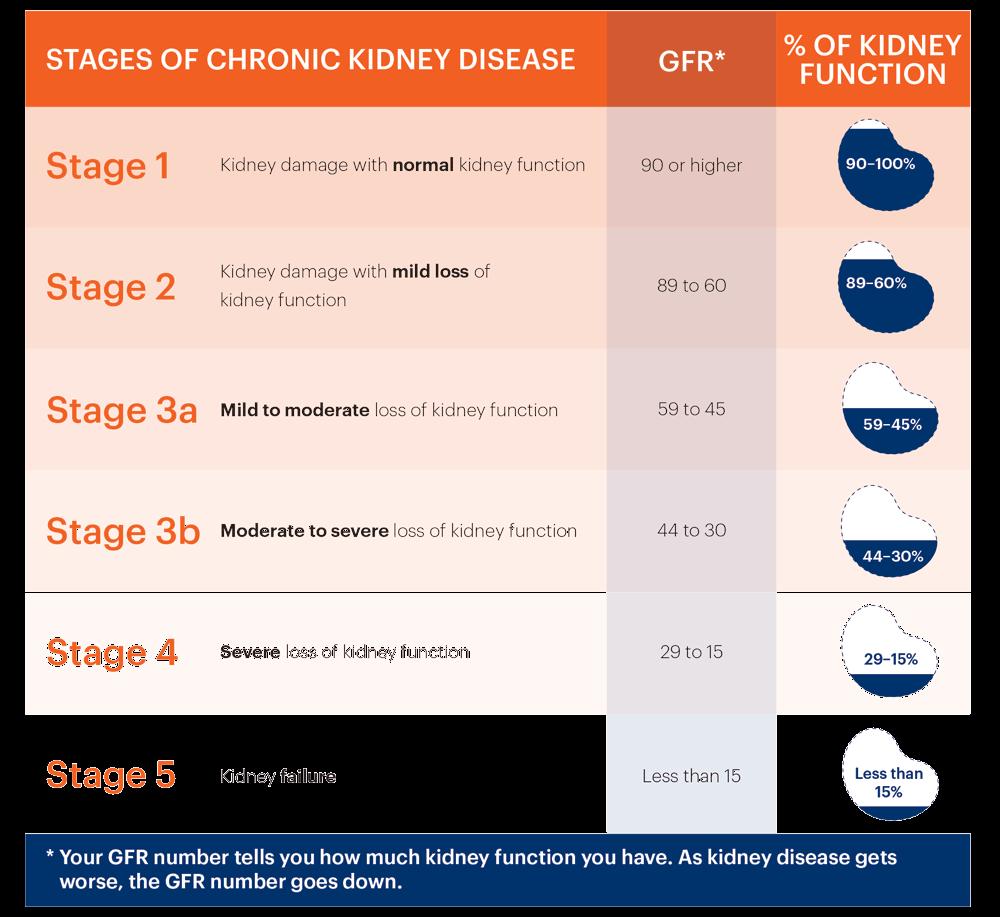
7 7
8 Stages G1 and G2 do not have reductions in egfr and therefore are defined by the presence of anatomical defects or markers of kidney damage such as albuminuria, hematuria, or electrolyte abnormalities. Because albuminuria is associated with increased renal and cardiovascular morbidity and mortality, the Kidney Disease: Improving Global Outcomes (KDIGO) group further subdivides the egfr-based kidney stages by degree of albuminuria. This dual egfr and albuminuria staging algorithm provides a means for predicting which patients are at highest risk for developing progressive CKD into end-stage renal disease (ESRD), defined as CKD stage G5 treated with chronic dialysis or kidney transplantation. 8
9 CKD, defined by either albuminuria or egfr <60 ml/min/1.73 m 2 The prevalence of CKD is heavily influenced by age and has increased severalfold in elderly persons over the past 20 years. In the United States, the prevalence of CKD stage G3 or worse is 0.3% in those aged 20 to 39 years 3.3% in those aged 40 to 59 years 22.6% in those aged 60 years. In contrast, the prevalence of albuminuria is less age dependent. 9
10 Approximately 6% of people aged 40 to 59 years have a urine albumin-creatinine ratio 30 mg/g, compared with 8.5% of those aged 60 years. Advanced CKD, defined by stages G4 or G5, is present in <1% of the population. 10
11 CKD results from various etiologies that cause chronic damage to the glomeruli, tubulointerstitium, or both. Glomerular damage is reflected by proteinuria or albuminuria. Although a large degree of tubulointerstitial damage (both chronic inflammation and fibrosis) can exist subclinically and thus go unnoticed, eventually the underlying structural abnormalities affect kidney function, and GFR falls below normal levels. Not all patients with CKD progress to ESKD. The most important predictors of progression are the baseline level of egfr and the degree of albuminuria/proteinuria. 11
12 egfr trajectory over time also adds prognostic value for ESKD and cardiovascular outcomes. Patients with diabetic CKD usually progress faster than those without diabetes. The rate of egfr decline ranges between -3 and -6 ml per year in patients who have type 2 diabetes with high albuminuria. Renal risk variants in the apolipoprotein L1 (APOL1) gene are prevalent in black persons and are associated with higher rates of ESKD and progression of CKD, regardless of diabetes status. 12
13 Risk Factors Largest risk factor populations are those with Diabetes Mellitus, Hypertension, any history of Glomerulonephritis These account for >75% of causes of CKD Having any combination of the three above dramatically increases the chances of CKD Other risk factors: CHF Smoking NSAIDs Urinary output obstruction High protein diets 13
14 Screening CKD is typically asymptomatic except in advanced stages (G4, G5). Controversy exists regarding screening patients for CKD. USPSTF and the American College of Physicians recommend against screening for CKD in asymptomatic adults with or without risk factors for CKD. In contrast, the American Society of Nephrology advises screening all adults for CKD, including, but not limited to, those with a family history of kidney disease or adults with risk factors for CKD (diabetes, hypertension, or cardiovascular disease) 14
15 CKD is typically asymptomatic except in advanced stages (G4, G5). When egfr falls below 30 ml/min/1.73 m 2, numerous alterations in metabolic pathways, including 1,25-dihydroxyvitamin D production and erythrocyte production, become altered due to the lack of nephron mass and loss of 1α-hydroxylase and erythropoietin synthesis. Moderate to severe CKD can also result in impaired ability to excrete salt and water, and may manifest as edema. CKD in a patient with nephrotic-range proteinuria may also result in edema or anasarca. 15
16 When CKD progresses to ESKD, several nonspecific ( uremic ) symptoms can occur. Uremia: Fatigue Nausea Loss of appetite Insomnia Irritability difficulty concentrating Confusion pruritus serositis, including pleuritis and pericarditis. uremic frost 16
17 Diagnosis CKD may be clinically suspected, or it may be incidentally detected on serum creatinine. Initial assessment of GFR includes establishing egfr based on serum creatinine using the Chronic Kidney Disease Epidemiology (CKD-EPI) Collaboration creatinine equation. If confirmation of GFR is required because of conditions that affect serum creatinine independent of GFR (such as extremes of muscle mass or diet), cystatin C should be measured to employ the CKD-EPI creatinine-cystatin equation, or GFR should be measured directly using a clearance procedure. 17
18 Initial assessment of albuminuria includes a random urine albumincreatinine ratio. If confirmation of albuminuria is required because of diurnal variation or conditions affecting creatinine excretion, the albumin excretion rate should be measured from a timed urine collection. Diagnosis of CKD requires a low egfr confirmed at least 3 months after initial assessment, or persistent proteinuria or albuminuria. Kidney biopsy is used to determine the etiology of CKD when a glomerulonephritis, unexplained tubulointerstitial disease, or severe proteinuria is likely based upon clinical history, urine sediment, and laboratory results and/or antibody tests 18
19 Occasionally, patients are noted to have medical Renal disease on imaging (such as US revealing hyperechoic kidneys). Urinalysis done for other nonspecific reasons may detect previously undiagnosed hematuria or proteinuria, which may suggest the presence of CKD and should prompt close observation or additional evaluation depending on the clinical scenario. Patients who experience acute kidney injury (AKI) can have slow recovery** sometimes mistaken for CKD*** 19
20 Diagnosis Quick Summary CMP/BMP/ Renal Function Panel Creatinine, BUN or electrolyte abnormalities UA Proteinuria Specific management Urine microalbumin, albumin, UPC Ultrasound 20
21 Predict Chronic Kidney Disease A kidney failure risk equation (KFRE) has been developed and validated. The KFRE uses four variables to predict 2-year and 5-year risk for ESKD in patients with CKD stages G3 to G5. age sex egfr Albuminuria*** The KFRE performs well across age, sex, race, and presence/absence of diabetes. The use of this equation is consistent with KDIGO guidelines, which recommend integration of risk prediction in the evaluation and management of CKD. eight-variable KFRE (previous four variables, plus serum calcium, phosphate, bicarbonate, and albumin); not as paramount as the 4 variable 21
22 Complications and Management According to KDIGO guidelines, referral to a nephrologist is indicated for evaluation and management of CKD in the presence of the following: AKI or an abrupt, sustained fall in GFR GFR <30 persistent albuminuria (>300 mg/g)**** progression of CKD erythrocyte casts >20 erythrocytes/hpf that is sustained and not readily explained hypertension refractory to treatment with four or more antihypertensive agents persistent abnormalities of serum potassium recurrent or extensive nephrolithiasis hereditary kidney disease 22
23 Reduction of all cause-mortality from CKD Lifestyle Modifications Diet Lower overall caloric intake decreased Potassium, Phosphorous Monitor Fluid intake as well as Sodium KidneyFund.org Exercise 30 min x day x 5 days/week Focus on large muscles and aerobic/cardio types of exercises Kidney.org 23
24 Cardiovascular Disease Cardiovascular disease is the leading cause of death among patients with CKD. **** The risk for cardiovascular-related death in patients with CKD stages G3 and G4 is 4 to 5 times higher than the risk for progression to ESKD. Mortality risk increases with decreasing egfr and increasing albuminuria. 24
25 HTN****** KDIGO and (ACC), (AHA), and nine other organizations recommend a blood pressure target of: <130/80 mm Hg in patients with CKD. An ACEi/ARB is preferred treatment of hypertension for patients with stage G3 CKD or higher or for those with stage G1 or G2 CKD with albuminuria These medications may also slow the progression of CKD in some patients. Thiazide diuretics are a cornerstone of hypertension treatment but may lose efficacy with severe CKD. 25
26 Loop diuretics therefore serve an important role in managing salt and water retention associated with proteinuria and CKD.***** Mechanism is inhibiting Loop of Henle and thus causing Salt and other electrolyte wasting, which thus causes overall water to decrease cornerstone of blood pressure management in patients with advanced chronic kidney disease. Torsemide, Furosemide, Bumetadine Dietary sodium chloride restriction is essential for blood pressure control in most forms of CKD, and KDIGO recommends restricting sodium intake to <2000 mg/d. 26
27 Dyslipidemia***** Elevated LDL cholesterol and triglyceride levels with low HDL cholesterol levels are common among patients with CKD. Statins have been shown to reduce cardiovascular and all-cause mortality in patients with CKD KDIGO recommends: statin in all patients aged 50 years with non-dialysis dependent CKD OR adults aged 18 to 49 years with non-dialysis dependent CKD and Ischemic risk factors Statins are also recommended for adult kidney transplant recipients. Dyslipidemia associated with the nephrotic syndrome helps maintain plasma oncotic pressure but, over time, may hasten the progression of glomerular injury. Dyslipidemia in the nephrotic syndrome requires aggressive treatment to prevent atherosclerotic disease, especially in patients with existing cardiovascular risk factors and in younger patients to prevent premature cardiovascular disease. 27
28 CAD There is a significantly increased prevalence of coronary artery disease (CAD) among patients with CKD compared with the general population. This is partly explained by the high prevalence of shared risk factors/comorbidities such as diabetes or hypertension. However, CKD is independently associated with CAD, and this association strengthens with declining egfr and rising albuminuria. Despite high cardiovascular mortality among patients with CKD, these patients may be less likely to undergo coronary revascularization procedures, possibly because of the increased risk for contrast-induced nephropathy. In patients with CKD, serum biomarkers for myocardial ischemia such as cardiac troponins may be chronically elevated due to decreased renal clearance. Serial troponin measurements and other markers such as creatine kinase-mb can help distinguish acute ischemia from stable elevations. 28
29 Ca and Phos homeostasis Three hormones are largely responsible for regulating calcium and phosphorus homeostasis: parathyroid hormone (PTH), vitamin D, and fibroblast growth factor 23 (FGF-23). PTH is the most important regulator of calcium and phosphorus concentrations. PTH has three separate mechanisms to increase serum calcium: It stimulates osteoclasts to resorb bone, stimulates hydroxylation of 25-hydroxyvitamin D in the kidneys, and stimulates tubular reabsorption of calcium Concurrently, PTH induces renal phosphorus excretion. FGF-23 is a peptide secreted by various types of bone cells. It acts on the kidney to induce phosphaturia and downregulates 1αhydroxylase to inhibit synthesis of 1,25 dihydroxyvitamin D. 29
30 As CKD progresses, increased FGF-23 and decreased nephron mass reduce the conversion of 25-hydroxyvitamin D to 1,25- dihydroxyvitamin D by renal tubular cells. 30
31 Secondary HyperPTH Increased plasma PTH as a result of CKD = secondary hyperparathyroidism. However, as CKD progresses, the kidney is unable to compensate for the increased release of phosphorus from bone, and phosphorus levels rise. This results in a vicious cycle as hyperphosphatemia stimulates PTH production. 31
32 Teritiary HyperPTH If secondary hyperparathyroidism cannot be adequately controlled, tertiary hyperparathyroidism can occur. Tertiary hyperparathyroidism is the result of the prolonged PTH stimulation needed to maintain eucalcemia. This prolonged stimulation results in increased calcium levels and severe hyperparathyroid hyperplasia with elevated PTH levels that are no longer responsive to the plasma calcium concentration. 32
33 Serum calcium and phosphorus levels typically remain in the normal range until the GFR drops below 20 to 30 (stages G4-G5) Ability of elevated FGF-23 and PTH levels to promote phosphorus excretion becomes overwhelmed, and hyperphosphatemia develops. Progressive decline in 1,25-d-vit D levels results in reduced intestinal calcium absorption, and hyperphosphatemia promotes precipitation of calcium and phosphorus in extra-skeletal tissues, leading to hypocalcemia. KDIGO recommends: egfr <60 (stage G3-G5) be evaluated for 25- hydroxyvitamin D deficiency and supplemented KDIGO guidelines: measure intact PTH levels in these patients to aid in the detection and management of secondary hyperparathyroidism and its complications. 33
34 Renal Osteodystrophy Renal osteodystrophy refers to alteration of bone morphology in patients with CKD KDIGO: recommends a bone biopsy if knowledge of the type of renal osteodystrophy will affect treatment decisions in patients with CKD stages G3a to G5. This recommendation is based on the growing experience with osteoporosis medications in patients with CKD, low bone mineral density, and a high risk of fracture. The lack of ability to perform a bone biopsy may not justify withholding antiresorptive therapy from patients at high risk of fracture. 34
35 Osteitis fibrosa cystica Osteitis fibrosa cystica is due to abnormally high bone turnover that can occur after prolonged exposure of bone to sustained high levels of PTH in secondary hyperparathyroidism. It is associated with an increased number and activity of osteoblasts and osteoclasts and expansion of osteoid surfaces, resulting in an increased risk for fracture. Patients can be asymptomatic or have bone pain. Classic skeletal changes on radiograph include subperiosteal resorption of bone, most prominently at the phalanges of the hands, and radiolucent bone cysts of the long bones. 35
36 Adynamic Bone Disease Adynamic bone disease occurs when there is a lack of bone cell activity and a markedly reduced rate of bone turnover. Histopathologic abnormalities include decreased osteoclast activity without an increase in osteoid due to decreased osteoblast activity, resulting in an increased risk for fracture. Patients have suppressed PTH levels (due to chronic illness or aggressive treatment with vitamin D analogues) or skeletal resistance to PTH from down-regulation of the bone PTH receptor due to high circulating PTH levels. PTH and Alk Phos levels are typically normal**** Patients may be asymptomatic or have bone pain. Adynamic bone disease should be excluded prior to bisphosphonate therapy because these drugs can cause and/or worsen the disease by inhibiting osteoclast activity. 36
37 Osteomalacia Osteomalacia is characterized by decreased mineralization of osteoid at sites of bone turnover, with increased risk of fracture. The most common symptoms include bone pain and tenderness. Although patients with CKD are at increased risk for osteomalacia, CKD does not cause osteomalacia per se; vitamin D deficiency caused by coexisting factors such as intestinal malabsorption due to gastrointestinal disorders or restricted access to sunlight is often present. 37
38 Osteoporosis Patients with CKD have many causes of reduced bone density. Current KDIGO guidelines indicate that in patients with CKD stages G3a to G5 with evidence of CKD-MBD and/or risk factors for osteoporosis, bone mineral density testing is suggested to assess fracture risk if results will affect treatment decisions. 38
39 Anemia Anemia in the setting of CKD is common, and its prevalence increases as CKD progresses into stages G4 and G5. Most often normocytic, anemia in CKD largely results from lack of erythropoietin production due to the decline in functional renal mass. Other contributors include erythropoietin resistance, neocytolysis (decreased survival time of erythrocytes), and iron deficiency. Although modest declines in hemoglobin are well tolerated, concern for inducing or contributing to the development of left ventricular hypertrophy has been the key driver in the belief that higher hemoglobin values are beneficial. 39
40 KDIGO recommendation: are to consider ESAs for patients with CKD who have hemoglobin concentrations <10. Goal Hgb concentration is between 9-12g/dL 40
41 All patients with CKD and anemia should have iron profiles assessed, including total iron-binding capacity and ferritin levels. KDIGO recommendation: 1. maintain t-saturation levels of >30% ****** 2. serum ferritin levels of >500 ng/ml using either oral or intravenous iron supplementation****** Inadequate iron stores will contribute to ESA hyporesponsiveness. Minimize the number of erythrocyte transfusions in patients with CKD and ESKD due to concerns for iron overload and sensitization to HLA antigens. 41
42 Management In patients with CKD stages G3a to G5 = serial assessments of phosphorus, calcium, and PTH levels. KDIGO recommend: that in patients with CKD stages G3a to G5, elevated phosphorus levels should be lowered toward the normal range, not into the normal range Thus, treatment should be aimed at overt hyperphosphatemia, and decisions to start phosphate-lowering treatment should be based solely on progressively or persistently elevated serum phosphorus levels.*** KDIGO recommend: avoid hypercalcemia. Mild and asymptomatic hypocalcemia can be tolerated to avoid inappropriate calcium loading. KDIGO recommends: restricting the dose of calcium-based phosphate binders (calcium carbonate and calcium acetate) in CKD stages G3a to G5, rather than restriction only in those with hypercalcemia. 42
43 For patients with CKD stages G3a to G5 who are not on dialysis, optimal PTH levels are not known. Previously, patients with PTH levels above the upper normal limit were targeted for management. KDIGO guidelines recommend against routine use of calcitriol and vitamin D analogues to lower PTH levels in patients with CKD stages G3a to G5 not on dialysis, because trials of these agents failed to demonstrate improvements in clinically relevant outcomes. Instead, these agents should be reserved for patients with CKD stages G4 to G5 with severe and progressive hyperparathyroidism. PTH goal for stage 4/5 In patients on dialysis, KDIGO guidelines recommend use of calcimimetics, calcitriol, or vitamin D analogues, or a combination of calcimimetics and calcitriol or vitamin D analogues, to lower PTH levels. Tertiary hyperparathyroidism does not respond to phosphate binders or calcitriol therapy, and patients often require parathyroidectomy for definitive treatment. 43
44 *** Metabolic acidosis frequently occurs in patients with CKD due to defective acid excretion, most commonly due to impaired ammoniagenesis. Untreated metabolic acidosis can lead to muscle loss (due to increased muscle proteolysis) and bone loss (due to increased bone resorption and impaired bone formation). In early CKD, metabolic acidosis is typically a normal anion gap hyperchloremic metabolic acidosis. As egfr declines, organic and inorganic anions are retained, and an increased anion gap metabolic acidosis develops. Alkali therapy, most commonly sodium bicarbonate or sodium citrate, can delay the progression of CKD. KDIGO: recommend alkali therapy when the serum bicarbonate is chronically <22 44
45 Nephrotoxins Two major issues exist regarding drug administration in patients with CKD: 1) Renally excreted drugs require dose adjustment to avoid accumulation and potential side effects 2) Reduced functional nephron mass increases the probability that a potentially nephrotoxic drug will cause nephrotoxicity. NSAIDS!!! STOP EM!!!! 45
46 Conceptually, compartmentalize nephrotoxic medications by their main site of action. including NSAIDs, calcineurin inhibitors, and ACE inhibitors/angiotensin receptor blockers, can have effects on glomerular blood flow. Patients with AKI who are on NSAIDs should have the medications immediately discontinued. For patients with CKD, the American Society of Nephrology recommends the avoidance of NSAIDs, including cyclooxygenase-2 inhibitors, due to the risk of worsening kidney function. ACE inhibitors or angiotensin receptor blockers are the cornerstone of treatment for patients with CKD; however, during episodes of acute illness and/or volume depletion, these drugs increase the risk for AKI due to their effects on intraglomerular pressure. Emerging literature suggests that proton pump inhibitors, in addition to their classic association with acute interstitial nephritis/aki, may contribute to the development and progression of CKD. These studies used careful comparators, including the use of H 2 blockers, and adjusted for numerous potential confounding variables, including chronic NSAID use. 46
47 Proteinuria***** The severity of proteinuria is strongly associated with adverse clinical outcomes, including progression of CKD to ESKD, cardiovascular morbidity, and mortality. It is unclear whether proteinuria is simply a marker of the underlying severity of kidney damage and disease, or if proteinuria itself activates inflammatory pathways and contributes to tubulointerstitial fibrosis. Although dual renin-angiotensin system blockade via combinations of ACE inhibitors, angiotensin receptor blockers, or direct renin inhibitors have been shown to decrease proteinuria, several clinical trials have revealed that use of combination renin-angiotensin system antagonism results in more adverse events (hyperkalemia, hypotension, AKI) without additional cardiovascular or renal benefits. insufficient evidence to recommend routine use of low protein diets to slow progression of CKD, high protein diets may precipitate or exacerbate symptoms of uremia in patients with stage G5 CKD 47
48 Considerations Imagining Intravenous iodinated contrast can cause contrast-induced nephropathy (CIN), and risk for CIN increases with increasing severity of CKD. Patients with CKD should receive IV hydration with isotonic saline or bicarbonate-containing solutions before and after receiving contrast unless there is evidence of frank pulmonary edema******** Gadolinium contrast used in MRI is associated with risk for nephrogenic systemic fibrosis (NSF) and must be avoided in patients with an egfr <30 In life-threatening situations in which benefit outweighs the risk for NSF, MRI is performed with low doses of stable gadolinium agents. Prior nephrology consult should be obtained to assess risks of gadolinium administration and guide the use of dialysis in advanced CKD and ESKD. In those with severe CKD who require gadolinium, daily dialysis for 3 days appears to be effective at clearing the gadolinium and reducing the risk for NSF. 48
49 Vaccinations Patients with CKD are at increased risk for infections that can be prevented by vaccination; however, these patients also have impaired immune responses to vaccines. The Centers for Disease Control and Prevention guidelines state that vaccinations in patients with CKD may be more effective when performed before the need for chronic dialysis or kidney transplantation. Patients with advanced CKD near dialysis dependence or those with ESKD on hemodialysis should be vaccinated against hepatitis B virus. Patients with CKD (stage not specified) or the nephrotic syndrome should receive the 23- and 13-valent pneumococcal vaccines, with revaccination with the 23- valent vaccine after a minimum of 5 years. Influenza vaccine should be administered annually to patients with CKD, but patients with ESRD should only receive the inactivated influenza vaccine due to risks associated with the live vaccines in immunocompromised patients. 49
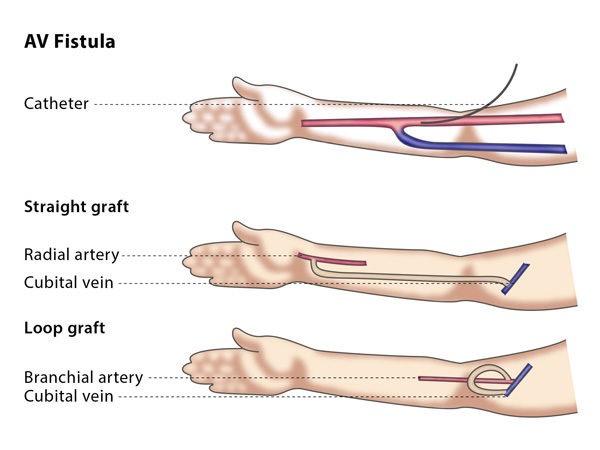
50 Vascular access Patients with advanced CKD may ultimately require renal replacement therapy; for those who choose hemodialysis, timely vascular access creation is essential. Referral to an experienced surgeon many months before dialysis is critical because arteriovenous fistula placement can be technically challenging and may require several months for full maturation. Arteriovenous fistulas have superior clinical outcomes compared with arteriovenous grafts and tunneled catheters. Protecting the nondominant arm veins is paramount and involves limiting phlebotomy and intravenous catheters in that arm. Peripherally inserted central venous catheters should be avoided in patients with an egfr <60. Avoidance of subclavian venous catheters helps to limit subclavian stenosis, which could impair the proper functioning of an arteriovenous fistula or arteriovenous graft used for dialysis. 50
51 51
52 Elderly CKD stages G1 through G3a in elderly patients without albuminuria is of minimal clinical importance; some may refer to this mild decrement in egfr as normal aging. For elderly persons with progressing or severe CKD necessitating discussions about renal replacement therapy and/or referral for evaluation for kidney transplantation, a patient-centered approach is preferred. Comorbid medical conditions, functional status, expected outcomes, and patient preferences regarding goals of care should be considered. For patients aged 80 years at the start of hemodialysis treatment, data demonstrate better survival among those who received pre-hemodialysis nephrology care that followed a planned management pathway, those who had a good nutritional status, and those with an arteriovenous fistula as vascular access for hemodialysis at the time of hemodialysis initiation. 52
53 Acquired cystic kidney disease Common among patients with severe CKD and ESRD. Cysts are usually detected during routine kidney ultrasonography or incidentally found on abdominal CT or MRI. These cysts are at increased risk for transformation into renal cell carcinoma, but routine screening is not recommended for most patients. A high index of suspicion is warranted for patients with new gross hematuria or unexplained flank pain. For cysts that are highly suspicious for malignancy, partial nephrectomy and nephron-sparing approaches are indicated for less severe stages of CKD. For patients with advanced CKD or ESRD, radical nephrectomy is the most prudent option. 53
54 Most important things to consider in Treatment Lifestyle, lifestyle, LIFESTYLE! BP control, consider ACEi/ARB DM control (SGLT-2i, metformin, insulin) Smoking cessation Use medications that do not target the kidney (Acetaminophen vs ibuprofen) Relieve UOP obstruction (stones, BPH) 54
55 References KDIGO Guidelines SPRINT trial NHANES survey MKSAPP 18 UpToDate Kidney.org KidneyFund.org 55
56 Center for Disease Control and Prevention. kidneyfailurerisk.com 56
57 Fin 57
Chronic Kidney Disease and the Electronic Health Record. Duaine Murphree, MD Sarah M. Thelen, MD
 Chronic Kidney Disease and the Electronic Health Record Duaine Murphree, MD Sarah M. Thelen, MD Definition of Chronic Kidney Disease (CKD) Defined by the National Kidney Foundation Either a decline in
Chronic Kidney Disease and the Electronic Health Record Duaine Murphree, MD Sarah M. Thelen, MD Definition of Chronic Kidney Disease (CKD) Defined by the National Kidney Foundation Either a decline in
Chronic Kidney Disease (CKD) Algorithm. Chronic Kidney Disease (CKD) Algorithm Page 1
 Algorithm. Chronic Kidney Disease (CKD) Algorithm Page 1") Chronic Kidney Disease (CKD) Algorithm Chronic Kidney Disease (CKD) Algorithm Page 1 Chronic Kidney Disease (CKD) Algorithm (See NICE Clinical Guideline CG73 1 and Quality Standards 2 ) Who should have
Chronic Kidney Disease (CKD) Algorithm Chronic Kidney Disease (CKD) Algorithm Page 1 Chronic Kidney Disease (CKD) Algorithm (See NICE Clinical Guideline CG73 1 and Quality Standards 2 ) Who should have
Diabetic Nephropathy
 Diabetic Nephropathy Kidney disease is common in people affected by diabetes mellitus Definition Urinary albumin excretion of more than 300mg in a 24 hour collection or macroalbuminuria Abnormal renal
Diabetic Nephropathy Kidney disease is common in people affected by diabetes mellitus Definition Urinary albumin excretion of more than 300mg in a 24 hour collection or macroalbuminuria Abnormal renal
HYPERTENSION ASSOCIATED WITH RENAL DISEASES
 RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria.
 Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Guideline for Microalbuminuria Screening
 East Lancashire Diabetes Network Guideline for Microalbuminuria Screening Produced by: Task and Finish Group, Clinical Standards Group Produced: August 2006 Approved by: East Lancashire Diabetes Network
East Lancashire Diabetes Network Guideline for Microalbuminuria Screening Produced by: Task and Finish Group, Clinical Standards Group Produced: August 2006 Approved by: East Lancashire Diabetes Network
Open the Flood Gates Urinary Obstruction and Kidney Stones. Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke
 Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
Open the Flood Gates Urinary Obstruction and Kidney Stones Dr. Jeffrey Rosenberg Dr. Emilio Lastarria Dr. Richard Kasulke Nephrology vs. Urology Nephrologist a physician who has been trained in the diagnosis
OUTPATIENT MANAGEMENT OF CHRONIC KIDNEY DISEASE. Jeanie Park, MD MS Assistant Professor Renal Division Emory University School of Medicine
 OUTPATIENT MANAGEMENT OF CHRONIC KIDNEY DISEASE Jeanie Park, MD MS Assistant Professor Renal Division Emory University School of Medicine Disclosures None Goals Background and staging Strategies to slow
OUTPATIENT MANAGEMENT OF CHRONIC KIDNEY DISEASE Jeanie Park, MD MS Assistant Professor Renal Division Emory University School of Medicine Disclosures None Goals Background and staging Strategies to slow
Chronic Kidney Disease
 Page 1 of 6 Chronic Kidney Disease Chronic kidney disease (CKD) means that your kidneys are not working as well as they once did. Various conditions can cause CKD. Severity can vary but most cases are:
Page 1 of 6 Chronic Kidney Disease Chronic kidney disease (CKD) means that your kidneys are not working as well as they once did. Various conditions can cause CKD. Severity can vary but most cases are:
GFR (Glomerular Filtration Rate) A Key to Understanding How Well Your Kidneys Are Working
 A Key to Understanding How Well Your Kidneys Are Working") GFR (Glomerular Filtration Rate) A Key to Understanding How Well Your Kidneys Are Working www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National
GFR (Glomerular Filtration Rate) A Key to Understanding How Well Your Kidneys Are Working www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2016 2/2017 2/2016 Description of Procedure or Service Vitamin D,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2016 2/2017 2/2016 Description of Procedure or Service Vitamin D,
William B. Schwartz Division of Nephrology Fellowship Training Program Curriculum
 William B. Schwartz Division of Nephrology Fellowship Training Program Curriculum Consult/Transplant Servic Patient Care Take medical history Perform physical examination Urinalysis and sediment eval Interpret
William B. Schwartz Division of Nephrology Fellowship Training Program Curriculum Consult/Transplant Servic Patient Care Take medical history Perform physical examination Urinalysis and sediment eval Interpret
Renal Disease in Type 2 Diabetes Mellitus
 Renal Disease in Type 2 Diabetes Mellitus 6th Collaborative DiGP/HSE/UCC Conference 25 th September 2013 Dr. Eoin O Sullivan Consultant Endocrinologist Bon Secours Hospital Cork Case 69 year old woman
Renal Disease in Type 2 Diabetes Mellitus 6th Collaborative DiGP/HSE/UCC Conference 25 th September 2013 Dr. Eoin O Sullivan Consultant Endocrinologist Bon Secours Hospital Cork Case 69 year old woman
Kidney Disease WHAT IS KIDNEY DISEASE? TESTS TO DETECT OR DIAGNOSE KIDNEY DISEASE TREATMENT STRATEGIES FOR KIDNEY DISEASE
 Kidney Disease WHAT IS KIDNEY DISEASE? Kidney disease is when your kidneys are damaged and not functioning as they should. When kidney disease is not going away it is called chronic kidney disease or CKD.
Kidney Disease WHAT IS KIDNEY DISEASE? Kidney disease is when your kidneys are damaged and not functioning as they should. When kidney disease is not going away it is called chronic kidney disease or CKD.
Diabetes and the Kidneys
 Diabetes and the Kidneys Aim(s) and objective(s) This guideline focuses on the detection, prevention, and management of kidney disease in people with diabetes. The management of end-stage renal disease
Diabetes and the Kidneys Aim(s) and objective(s) This guideline focuses on the detection, prevention, and management of kidney disease in people with diabetes. The management of end-stage renal disease
Treatment Recommendations for CKD in Cats (2015)
") All treatments for chronic kidney disease (CKD) need to be tailored to the individual patient. The following recommendations are useful starting points for the majority of cats at each stage. Serial monitoring
All treatments for chronic kidney disease (CKD) need to be tailored to the individual patient. The following recommendations are useful starting points for the majority of cats at each stage. Serial monitoring
Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results
 Principal Results") Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results Paul K. Whelton, MB, MD, MSc Chair, SPRINT Steering Committee Tulane University School of Public Health and Tropical Medicine, and
Systolic Blood Pressure Intervention Trial (SPRINT) Principal Results Paul K. Whelton, MB, MD, MSc Chair, SPRINT Steering Committee Tulane University School of Public Health and Tropical Medicine, and
UCSF Kidney Transplant Symposium 2012
 UCSF Kidney Transplant Symposium 2012 Nutrition Fitness in Kidney Transplant Mary Ellen DiPaola, RD, CDE UCSF Outpatient Dietitian Goal of Nutrition Fitness for Transplant Nutritional guidance of pre-
UCSF Kidney Transplant Symposium 2012 Nutrition Fitness in Kidney Transplant Mary Ellen DiPaola, RD, CDE UCSF Outpatient Dietitian Goal of Nutrition Fitness for Transplant Nutritional guidance of pre-
Guidelines for the management of hypertension in patients with diabetes mellitus
 Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
Guidelines for the management of hypertension in patients with diabetes mellitus Quick reference guide In the Eastern Mediterranean Region, there has been a rapid increase in the incidence of diabetes
Identifying and treating long-term kidney problems (chronic kidney disease)
") Understanding NICE guidance Information for people who use NHS services Identifying and treating long-term kidney problems (chronic kidney disease) NICE clinical guidelines advise the NHS on caring for
Understanding NICE guidance Information for people who use NHS services Identifying and treating long-term kidney problems (chronic kidney disease) NICE clinical guidelines advise the NHS on caring for
Renovascular Hypertension
 Renovascular Hypertension Philip Stockwell, MD Assistant Professor of Medicine (Clinical) Warren Alpert School of Medicine Cardiology for the Primary Care Provider September 28, 201 Renovascular Hypertension
Renovascular Hypertension Philip Stockwell, MD Assistant Professor of Medicine (Clinical) Warren Alpert School of Medicine Cardiology for the Primary Care Provider September 28, 201 Renovascular Hypertension
Your Kidneys: Master Chemists of the Body
 Your Kidneys: Master Chemists of the Body www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney Foundation's Kidney Disease Outcomes
Your Kidneys: Master Chemists of the Body www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney Foundation's Kidney Disease Outcomes
Chronic Kidney Disease and Diabetes
 Anyone with diabetes can get kidney disease. Diabetes and high blood pressure are the most common causes of kidney disease, and people often have both. Chronic (long term) kidney disease (CKD) caused by
Anyone with diabetes can get kidney disease. Diabetes and high blood pressure are the most common causes of kidney disease, and people often have both. Chronic (long term) kidney disease (CKD) caused by
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Definition, Prevalence, Pathophysiology and Complications of CKD. JM Krzesinski CHU Liège-ULg Core curriculum Nephrology September 28 th 2013
 Definition, Prevalence, Pathophysiology and Complications of CKD JM Krzesinski CHU Liège-ULg Core curriculum Nephrology September 28 th 2013 KI supplements January 2013 Objectives of the course on CKD:
Definition, Prevalence, Pathophysiology and Complications of CKD JM Krzesinski CHU Liège-ULg Core curriculum Nephrology September 28 th 2013 KI supplements January 2013 Objectives of the course on CKD:
InDependent Diabetes Trust
 InDependent Diabetes Trust Kidneys and Diabetes Updated July 2015 Registered Company Number 3148360 Registered Charity No 1058284 Contents Introduction Healthy Kidneys Kidney disease and diabetes The use
InDependent Diabetes Trust Kidneys and Diabetes Updated July 2015 Registered Company Number 3148360 Registered Charity No 1058284 Contents Introduction Healthy Kidneys Kidney disease and diabetes The use
CHRONIC KIDNEY DISEASE MANAGEMENT GUIDE
 CHRONIC KIDNEY DISEASE MANAGEMENT GUIDE Outline I. Introduction II. Identifying Members with Kidney Disease III. Clinical Guidelines for Kidney Disease A. Chronic Kidney Disease B. End Stage Renal Disease
CHRONIC KIDNEY DISEASE MANAGEMENT GUIDE Outline I. Introduction II. Identifying Members with Kidney Disease III. Clinical Guidelines for Kidney Disease A. Chronic Kidney Disease B. End Stage Renal Disease
High Blood pressure and chronic kidney disease
 High Blood pressure and chronic kidney disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
High Blood pressure and chronic kidney disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
High Blood Pressure and Chronic Kidney Disease. For People With CKD Stages 1 4
 High Blood Pressure and Chronic Kidney Disease For People With CKD Stages 1 4 National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation s Kidney
High Blood Pressure and Chronic Kidney Disease For People With CKD Stages 1 4 National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation s Kidney
Diabetes and Your Kidneys
 American Kidney Fund reaching out giving hope improving lives Diabetes and Your Kidneys reaching out giving hope improving lives Diabetes: The #1 Cause of Kidney Failure Your doctor told you that you have
American Kidney Fund reaching out giving hope improving lives Diabetes and Your Kidneys reaching out giving hope improving lives Diabetes: The #1 Cause of Kidney Failure Your doctor told you that you have
DISCLOSURES RISK ASSESSMENT. Stroke and Heart Disease -Is there a Link Beyond Risk Factors? Daniel Lackland, MD
 STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
Southern Derbyshire Shared Care Pathology Guidelines. AKI guidelines for primary care
 Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE...2 FLOW DIAGRAM: POST AKI MANAGEMENT
Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE...2 FLOW DIAGRAM: POST AKI MANAGEMENT
Chronic Kidney Disease (CKD) Guideline
 Guideline") Chronic Kidney Disease (CKD) These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They are not intended to replace
Chronic Kidney Disease (CKD) These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They are not intended to replace
MANAGING ANEMIA. When You Have Kidney Disease or Kidney Failure. www.kidney.org
 MANAGING ANEMIA When You Have Kidney Disease or Kidney Failure www.kidney.org About the Information in this Booklet Did you know that the National Kidney Foundation (NKF) offers guidelines and commentaries
MANAGING ANEMIA When You Have Kidney Disease or Kidney Failure www.kidney.org About the Information in this Booklet Did you know that the National Kidney Foundation (NKF) offers guidelines and commentaries
Objectives. Functions of the kidney. Renal failure. Categories of AKI. Acute Kidney Injury (AKI) RENAL FAILURE: AN UPDATE FOR HEALTHCARE PROFESSIONALS
 RENAL FAILURE: AN UPDATE FOR HEALTHCARE PROFESSIONALS") RENAL FAILURE: AN UPDATE FOR HEALTHCARE PROFESSIONALS Tamara Kear, PhD, RN Assistant Professor of Nursing Villanova University Objectives Review normal kidney function. Define the pathophysiology of acute
RENAL FAILURE: AN UPDATE FOR HEALTHCARE PROFESSIONALS Tamara Kear, PhD, RN Assistant Professor of Nursing Villanova University Objectives Review normal kidney function. Define the pathophysiology of acute
NEPHROLOGY COMMON CLINICAL PRESENTATIONS AND CARDINAL MANIFESTATIONS OF RENAL DISEASES-
 NEPHOLOGY OON LINIAL PESENTATIONS AND ADINAL ANIFESTATIONS OF ENAL DISEASES- INITIAL EVALUATION AND DEISION-AKING SKILLS GOAL: The residents will learn the evaluation, diagnosis, and management of patients
NEPHOLOGY OON LINIAL PESENTATIONS AND ADINAL ANIFESTATIONS OF ENAL DISEASES- INITIAL EVALUATION AND DEISION-AKING SKILLS GOAL: The residents will learn the evaluation, diagnosis, and management of patients
Select the one that is the best answer:
 MQ Kidney 1 Select the one that is the best answer: 1) n increase in the concentration of plasma potassium causes increase in: a) release of renin b) secretion of aldosterone c) secretion of H d) release
MQ Kidney 1 Select the one that is the best answer: 1) n increase in the concentration of plasma potassium causes increase in: a) release of renin b) secretion of aldosterone c) secretion of H d) release
嘉 義 長 庚 醫 院 藥 劑 科 Speaker : 翁 玟 雯
 The Clinical Efficacy and Safety of Sodium Glucose Cotransporter-2 (SGLT2) Inhibitors in Adults with Type 2 Diabetes Mellitus 嘉 義 長 庚 醫 院 藥 劑 科 Speaker : 翁 玟 雯 Diabetes Mellitus : A group of diseases characterized
The Clinical Efficacy and Safety of Sodium Glucose Cotransporter-2 (SGLT2) Inhibitors in Adults with Type 2 Diabetes Mellitus 嘉 義 長 庚 醫 院 藥 劑 科 Speaker : 翁 玟 雯 Diabetes Mellitus : A group of diseases characterized
Interpretation of Laboratory Values
 Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Cardiovascular Risk in Diabetes
 Cardiovascular Risk in Diabetes Lipids Hypercholesterolaemia is an important reversible risk factor for cardiovascular disease and should be tackled aggressively in all diabetic patients. In Type 1 patients,
Cardiovascular Risk in Diabetes Lipids Hypercholesterolaemia is an important reversible risk factor for cardiovascular disease and should be tackled aggressively in all diabetic patients. In Type 1 patients,
Approach to the Patient with Acute Renal Failure. Michael Ornes Abbott Northwestern Hospital
 Approach to the Patient with Acute Renal Failure Michael Ornes Abbott Northwestern Hospital Definition Abrupt decrease in glomerular filtration rate Accumulation of urea and other metabolic byproducts
Approach to the Patient with Acute Renal Failure Michael Ornes Abbott Northwestern Hospital Definition Abrupt decrease in glomerular filtration rate Accumulation of urea and other metabolic byproducts
ACID- BASE and ELECTROLYTE BALANCE. MGHS School of EMT-Paramedic Program 2011
 ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
Care of an End Stage Renal Disease Patient. December 2012
 Care of an End Stage Renal Disease Patient 1 BARBARA BRECKLER RN BSN QUALITY IMPROVEMENT DIRECTOR NORTHWEST RENAL NETWORK December 2012 Objectives 2 Provide an overview of: Dialysis Basics Vascular Access
Care of an End Stage Renal Disease Patient 1 BARBARA BRECKLER RN BSN QUALITY IMPROVEMENT DIRECTOR NORTHWEST RENAL NETWORK December 2012 Objectives 2 Provide an overview of: Dialysis Basics Vascular Access
Disability Evaluation Under Social Security
 Disability Evaluation Under Social Security Revised Medical Criteria for Evaluating Endocrine Disorders Effective June 7, 2011 Why a Revision? Social Security revisions reflect: SSA s adjudicative experience.
Disability Evaluation Under Social Security Revised Medical Criteria for Evaluating Endocrine Disorders Effective June 7, 2011 Why a Revision? Social Security revisions reflect: SSA s adjudicative experience.
D. Vitamin D. 1. Two main forms; vitamin D2 and D3
 D. Vitamin D. Two main forms; vitamin D2 and D3 H H D3 - Cholecalciferol D2 - Ergocalciferol Technically, vitamin D is not a vitamin. It is the name given to a group of fat-soluble prohormones (substances
D. Vitamin D. Two main forms; vitamin D2 and D3 H H D3 - Cholecalciferol D2 - Ergocalciferol Technically, vitamin D is not a vitamin. It is the name given to a group of fat-soluble prohormones (substances
Managing Anemia When You Are on Dialysis. Stage 5
 Managing Anemia When You Are on Dialysis Stage 5 What is anemia? Anemia happens when your red blood cells are in short supply. Red blood cells carry oxygen from your lungs to all parts of your body, giving
Managing Anemia When You Are on Dialysis Stage 5 What is anemia? Anemia happens when your red blood cells are in short supply. Red blood cells carry oxygen from your lungs to all parts of your body, giving
Clinical Aspects of Hyponatremia & Hypernatremia
 Clinical Aspects of Hyponatremia & Hypernatremia Case Presentation: History 62 y/o male is admitted to the hospital with a 3 month history of excessive urination (polyuria) and excess water intake up to
Clinical Aspects of Hyponatremia & Hypernatremia Case Presentation: History 62 y/o male is admitted to the hospital with a 3 month history of excessive urination (polyuria) and excess water intake up to
PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement)
") 1 PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement) PHOSPHATE-SANDOZ PHOSPHATE-SANDOZ Tablets are a high dose phosphate supplement containing sodium phosphate monobasic. The CAS registry number
1 PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement) PHOSPHATE-SANDOZ PHOSPHATE-SANDOZ Tablets are a high dose phosphate supplement containing sodium phosphate monobasic. The CAS registry number
Clinical Performance Goals 2010-2011
 Clinical Performance Goals 2010-2011 Clinical Performance Goals 2010-2011 Table of Contents Table of Contents... 1 Health Care Quality Improvement Program... 2 Clinical Performance Measures... 6 Chapter
Clinical Performance Goals 2010-2011 Clinical Performance Goals 2010-2011 Table of Contents Table of Contents... 1 Health Care Quality Improvement Program... 2 Clinical Performance Measures... 6 Chapter
Hemodialysis: What You Need to Know
 Hemodialysis: What You Need to Know Healthy kidneys clean your blood and remove extra fluid in the form of urine. They also make hormones your body needs for some important functions. When kidney failure
Hemodialysis: What You Need to Know Healthy kidneys clean your blood and remove extra fluid in the form of urine. They also make hormones your body needs for some important functions. When kidney failure
Update in Contrast Induced Nephropathy
 Update in Contrast Induced Nephropathy Yves Pirson Service de Néphrologie, Clin. Univ. St-Luc - UCL A 76-year-old man with - type 2 diabetes - CKD (ser. creat.: 1.8 mg/dl; GFR: 32) presents with angina
Update in Contrast Induced Nephropathy Yves Pirson Service de Néphrologie, Clin. Univ. St-Luc - UCL A 76-year-old man with - type 2 diabetes - CKD (ser. creat.: 1.8 mg/dl; GFR: 32) presents with angina
High Blood Pressure and Kidney Disease
 High Blood Pressure and Kidney Disease National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH The kidneys play a key
High Blood Pressure and Kidney Disease National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH The kidneys play a key
The digestive system eliminated waste from the digestive tract. But we also need a way to eliminate waste from the rest of the body.
 Outline Urinary System Urinary System and Excretion Bio105 Lecture 20 Chapter 16 I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system 1
Outline Urinary System Urinary System and Excretion Bio105 Lecture 20 Chapter 16 I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system 1
Acid-Base Balance and the Anion Gap
 Acid-Base Balance and the Anion Gap 1. The body strives for electrical neutrality. a. Cations = Anions b. One of the cations is very special, H +, and its concentration is monitored and regulated very
Acid-Base Balance and the Anion Gap 1. The body strives for electrical neutrality. a. Cations = Anions b. One of the cations is very special, H +, and its concentration is monitored and regulated very
EXECUTIVE BLOOD WORK PANEL
 EXECUTIVE BLOOD WORK PANEL Below is a list of all blood and urine testing done on the day of your Executive Medical. MALE Serum Glucose Random Serum Glucose Fasting Creatinine Uric Acid Sodium Potassium
EXECUTIVE BLOOD WORK PANEL Below is a list of all blood and urine testing done on the day of your Executive Medical. MALE Serum Glucose Random Serum Glucose Fasting Creatinine Uric Acid Sodium Potassium
Parathyroid hormone (serum, plasma)
") Parathyroid hormone (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Parathyroid hormone (PTH) 1.2 Alternative names Parathormone 1.3 NMLC code 1.4 Description of analyte PTH is an
Parathyroid hormone (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Parathyroid hormone (PTH) 1.2 Alternative names Parathormone 1.3 NMLC code 1.4 Description of analyte PTH is an
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Cardiovascular disease physiology. Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011
 Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk
 Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk Behçet s Disease and the Kidneys How are the kidneys affected by Behçet s disease? Kidney disease
Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk Behçet s Disease and the Kidneys How are the kidneys affected by Behçet s disease? Kidney disease
Considerations With Calcium And Vitamin D Supplementation
 Considerations With Calcium And Vitamin D Supplementation Activity Preview Calcium is an electrolyte involved in many systems in the body including bone health, nerve signaling pathways, muscle contractions,
Considerations With Calcium And Vitamin D Supplementation Activity Preview Calcium is an electrolyte involved in many systems in the body including bone health, nerve signaling pathways, muscle contractions,
CASE B1. Newly Diagnosed T2DM in Patient with Prior MI
 Newly Diagnosed T2DM in Patient with Prior MI 1 Our case involves a gentleman with acute myocardial infarction who is newly discovered to have type 2 diabetes. 2 One question is whether anti-hyperglycemic
Newly Diagnosed T2DM in Patient with Prior MI 1 Our case involves a gentleman with acute myocardial infarction who is newly discovered to have type 2 diabetes. 2 One question is whether anti-hyperglycemic
Understanding Treatment Options for Renal Therapy
 Understanding Treatment Options for Renal Therapy Kidney failure happens to many different people for many different reasons 1 What causes kidney failure? Diabetes Chronic infection High blood pressure
Understanding Treatment Options for Renal Therapy Kidney failure happens to many different people for many different reasons 1 What causes kidney failure? Diabetes Chronic infection High blood pressure
Learning about Hepatitis C and Chronic Kidney Disease
 Learning about Hepatitis C and Chronic Kidney Disease Hepatitis C and Chronic Kidney Disease If you have chronic kidney disease (CKD), you want to learn all you can about your disease and what you can
Learning about Hepatitis C and Chronic Kidney Disease Hepatitis C and Chronic Kidney Disease If you have chronic kidney disease (CKD), you want to learn all you can about your disease and what you can
Information for Childhood Cancer Survivors. Kidney Problems
 Kidney problems Some chemotherapy drugs can affect the kidneys. The kidneys break down and remove many chemotherapy drugs from the body. When chemotherapy drugs get broken down, they may make products
Kidney problems Some chemotherapy drugs can affect the kidneys. The kidneys break down and remove many chemotherapy drugs from the body. When chemotherapy drugs get broken down, they may make products
Chapter 23. Composition and Properties of Urine
 Chapter 23 Composition and Properties of Urine Composition and Properties of Urine urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless to deep
Chapter 23 Composition and Properties of Urine Composition and Properties of Urine urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless to deep
High Blood Pressure and Chronic Kidney Disease
 High Blood Pressure and Chronic Kidney Disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
High Blood Pressure and Chronic Kidney Disease For People with CKD Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney
10/27/2010. CKD in the United States. Management of The Patient With Chronic Kidney Disease. CKD Patients Are More Likely to Die Than Progress to ESRD
 CKD in the United States Management of The Patient With Chronic Kidney Disease Paul J. Scheel, Jr., M.D., FASN Director,Division of Nephrology An estimated 26 million adults have CKD Many are unaware of
CKD in the United States Management of The Patient With Chronic Kidney Disease Paul J. Scheel, Jr., M.D., FASN Director,Division of Nephrology An estimated 26 million adults have CKD Many are unaware of
Kidney Cancer OVERVIEW
 Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Amylase and Lipase Tests
 Amylase and Lipase Tests Also known as: Amy Formal name: Amylase Related tests: Lipase The Test The blood amylase test is ordered, often along with a lipase test, to help diagnose and monitor acute or
Amylase and Lipase Tests Also known as: Amy Formal name: Amylase Related tests: Lipase The Test The blood amylase test is ordered, often along with a lipase test, to help diagnose and monitor acute or
HIGH BLOOD PRESSURE AND YOUR KIDNEYS
 HIGH BLOOD PRESSURE AND YOUR KIDNEYS www.kidney.org About the Information in this Booklet Did you know that the National Kidney (NKF) Foundation offers guidelines and commentaries that help your healthcare
HIGH BLOOD PRESSURE AND YOUR KIDNEYS www.kidney.org About the Information in this Booklet Did you know that the National Kidney (NKF) Foundation offers guidelines and commentaries that help your healthcare
Pseudohypoparathyroidism: A Variation on the Theme of Hypoparathyroidism
 Pseudohypoparathyroidism: A Variation on the Theme of Hypoparathyroidism Amanda Tencza MS IV 1 and Michael A. Levine, MD 2 1 Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
Pseudohypoparathyroidism: A Variation on the Theme of Hypoparathyroidism Amanda Tencza MS IV 1 and Michael A. Levine, MD 2 1 Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
Liver Function Essay
 Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
The sensitive marker for glomerular filtration rate (GFR) Estimation of GFR from Serum Cystatin C:
 Estimation of GFR from Serum Cystatin C:") The sensitive marker for glomerular filtration rate (GFR) Estimation of GFR from Serum Cystatin C: The good correlation allows close estimation of GFR Cystatin C GFR GFR in serum estimated* measured* n
The sensitive marker for glomerular filtration rate (GFR) Estimation of GFR from Serum Cystatin C: The good correlation allows close estimation of GFR Cystatin C GFR GFR in serum estimated* measured* n
1. PATHOPHYSIOLOGY OF METABOLIC SYNDROME
 1. PATHOPHYSIOLOGY OF METABOLIC SYNDROME Izet Aganović, Tina Dušek Department of Internal Medicine, Division of Endocrinology, University Hospital Center Zagreb, Croatia 1 Introduction The metabolic syndrome
1. PATHOPHYSIOLOGY OF METABOLIC SYNDROME Izet Aganović, Tina Dušek Department of Internal Medicine, Division of Endocrinology, University Hospital Center Zagreb, Croatia 1 Introduction The metabolic syndrome
TYPE 2 DIABETES MELLITUS: NEW HOPE FOR PREVENTION. Robert Dobbins, M.D. Ph.D.
 TYPE 2 DIABETES MELLITUS: NEW HOPE FOR PREVENTION Robert Dobbins, M.D. Ph.D. Learning Objectives Recognize current trends in the prevalence of type 2 diabetes. Learn differences between type 1 and type
TYPE 2 DIABETES MELLITUS: NEW HOPE FOR PREVENTION Robert Dobbins, M.D. Ph.D. Learning Objectives Recognize current trends in the prevalence of type 2 diabetes. Learn differences between type 1 and type
LECTURE 1 RENAL FUNCTION
 LECTURE 1 RENAL FUNCTION Components of the Urinary System 2 Kidneys 2 Ureters Bladder Urethra Refer to Renal System Vocabulary in your notes Figure 2-1,page10 Kidney Composition Cortex Outer region Contains
LECTURE 1 RENAL FUNCTION Components of the Urinary System 2 Kidneys 2 Ureters Bladder Urethra Refer to Renal System Vocabulary in your notes Figure 2-1,page10 Kidney Composition Cortex Outer region Contains
DIABETES. Eyes, Heart, Nerves, Feet, and Kidneys. www.kidney.org
 DIABETES Eyes, Heart, Nerves, Feet, and Kidneys www.kidney.org About the Information in this Booklet Did you know that the National Kidney Foundation (NKF) offers guidelines and commentaries that help
DIABETES Eyes, Heart, Nerves, Feet, and Kidneys www.kidney.org About the Information in this Booklet Did you know that the National Kidney Foundation (NKF) offers guidelines and commentaries that help
Understanding diabetes Do the recent trials help?
 Understanding diabetes Do the recent trials help? Dr Geoffrey Robb Consultant Physician and Diabetologist CMO RGA UK Services and Partnership Assurance AMUS 25 th March 2010 The security of experience.
Understanding diabetes Do the recent trials help? Dr Geoffrey Robb Consultant Physician and Diabetologist CMO RGA UK Services and Partnership Assurance AMUS 25 th March 2010 The security of experience.
NCD for Lipids Testing
 Applicable CPT Code(s): NCD for Lipids Testing 80061 Lipid panel 82465 Cholesterol, serum or whole blood, total 83700 Lipoprotein, blood; electrophoretic separation and quantitation 83701 Lipoprotein blood;
Applicable CPT Code(s): NCD for Lipids Testing 80061 Lipid panel 82465 Cholesterol, serum or whole blood, total 83700 Lipoprotein, blood; electrophoretic separation and quantitation 83701 Lipoprotein blood;
LIPID PANEL CHOLESTEROL LIPOPROTEIN, ELECTROPHORETIC SEPARATION LIPOPROTEIN, DIRECT MEASUREMENT (HDL) LDL DIRECT TRIGLYCERIDES
 LDL DIRECT TRIGLYCERIDES") Test Code Test Name CPT CHOL Cholesterol, Serum 82465 HDL HDL, (High Density Lipoprotein) 83718 TRIG Triglycerides, Serum 84478 FTRIG Triglycerides (Fluid) 84478 LIPID Lipid Panel 80061 LDL LDL (Low Density
Test Code Test Name CPT CHOL Cholesterol, Serum 82465 HDL HDL, (High Density Lipoprotein) 83718 TRIG Triglycerides, Serum 84478 FTRIG Triglycerides (Fluid) 84478 LIPID Lipid Panel 80061 LDL LDL (Low Density
Diagnostic Assessments Relating to Renal Function: Why we do them? What do they mean? Mohamud Karim MD, FRCPC. Feb 27, 2015
 Diagnostic Assessments Relating to Renal Function: Why we do them? What do they mean? Mohamud Karim MD, FRCPC Feb 27, 2015 Acknowledgements: Previous presentor Why are Patients Referred? Renal Syndromes:
Diagnostic Assessments Relating to Renal Function: Why we do them? What do they mean? Mohamud Karim MD, FRCPC Feb 27, 2015 Acknowledgements: Previous presentor Why are Patients Referred? Renal Syndromes:
What You Need to Know for Better Bone Health
 What You Need to Know for Better Bone Health A quick lesson about bones: Why healthy bones matter The healthier your bones The more active you can be Bone health has a major effect on your quality of life
What You Need to Know for Better Bone Health A quick lesson about bones: Why healthy bones matter The healthier your bones The more active you can be Bone health has a major effect on your quality of life
Medicare s Preventive Care Services. Manage Your Chronic Kidney Disease (CKD stages 3-4) with Diet
 with Diet") s Preventive Care Services Manage Your Chronic Kidney Disease (CKD stages 3-4) with Diet What do the kidneys do? Your kidneys have important jobs to do in your body. Two of the kidneys most important jobs
s Preventive Care Services Manage Your Chronic Kidney Disease (CKD stages 3-4) with Diet What do the kidneys do? Your kidneys have important jobs to do in your body. Two of the kidneys most important jobs
EFFIMET 1000 XR Metformin Hydrochloride extended release tablet
 BRAND NAME: Effimet XR. THERAPEUTIC CATEGORY: Anti-Diabetic PHARMACOLOGIC CLASS: Biguanides EFFIMET 1000 XR Metformin Hydrochloride extended release tablet COMPOSITION AND PRESENTATION Composition Each
BRAND NAME: Effimet XR. THERAPEUTIC CATEGORY: Anti-Diabetic PHARMACOLOGIC CLASS: Biguanides EFFIMET 1000 XR Metformin Hydrochloride extended release tablet COMPOSITION AND PRESENTATION Composition Each
CHAPTER 20: URINARY SYSTEM
 OBJECTIVES: 1. Name the major function of the urinary system, and name and locate (on a diagram) the organs that compose the system. 2. Explain what the term renal refers to. 3. Define the term retroperitoneal.
OBJECTIVES: 1. Name the major function of the urinary system, and name and locate (on a diagram) the organs that compose the system. 2. Explain what the term renal refers to. 3. Define the term retroperitoneal.
Inpatient Heart Failure Management: Risks & Benefits
 Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Preoperative Laboratory and Diagnostic Studies
 Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Clinical Quality Measure Crosswalk: HEDIS, Meaningful Use, PQRS, PCMH, Beacon, 10 SOW
 Clinical Crosswalk: HEDIS, Meaningful Use, PQRS, PCMH, Beacon, 10 SOW NQF 0105 PQRS 9 NQF 0002 PQRS 66 Antidepressant Medication Management Appropriate Testing for Children with Pharyngitis (2-18 years)
Clinical Crosswalk: HEDIS, Meaningful Use, PQRS, PCMH, Beacon, 10 SOW NQF 0105 PQRS 9 NQF 0002 PQRS 66 Antidepressant Medication Management Appropriate Testing for Children with Pharyngitis (2-18 years)
Diagnostics: Page 2 of 5
 Proteinuria Proteinuria is a condition in which there are increased amounts of protein in the urine. There are a number of different diseases which can result in proteinuria. In the early stages of the
Proteinuria Proteinuria is a condition in which there are increased amounts of protein in the urine. There are a number of different diseases which can result in proteinuria. In the early stages of the
Renal syndromes leading to abnormal kidney function:
 Renal syndromes leading to abnormal kidney function: An abnormality in kidney function can be detected by the following: 1) changes in serum creatinine concentration, reflecting changes in GFR 2) abnormalities
Renal syndromes leading to abnormal kidney function: An abnormality in kidney function can be detected by the following: 1) changes in serum creatinine concentration, reflecting changes in GFR 2) abnormalities
Tuberculosis And Diabetes. Dr. hanan abuelrus Prof.of internal medicine Assiut University
 Tuberculosis And Diabetes Dr. hanan abuelrus Prof.of internal medicine Assiut University TUBERCULOSIS FACTS More than 9 million people fall sick with tuberculosis (TB) every year. Over 1.5 million die
Tuberculosis And Diabetes Dr. hanan abuelrus Prof.of internal medicine Assiut University TUBERCULOSIS FACTS More than 9 million people fall sick with tuberculosis (TB) every year. Over 1.5 million die
PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION
 Hull & East Riding Prescribing Committee PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION For guidance on Primary Prevention please see NICE guidance http://www.nice.org.uk/guidance/cg181
Hull & East Riding Prescribing Committee PRESCRIBING GUIDELINES FOR LIPID LOWERING TREATMENTS for SECONDARY PREVENTION For guidance on Primary Prevention please see NICE guidance http://www.nice.org.uk/guidance/cg181
GUIDELINES FOR THE TREATMENT OF DIABETIC NEPHROPATHY*
 71 GUIDELINES FOR THE TREATMENT OF DIABETIC NEPHROPATHY* Ryuichi KIKKAWA** Asian Med. J. 44(2): 71 75, 2001 Abstract: Diabetic nephropathy is the most devastating complication of diabetes and is now the
71 GUIDELINES FOR THE TREATMENT OF DIABETIC NEPHROPATHY* Ryuichi KIKKAWA** Asian Med. J. 44(2): 71 75, 2001 Abstract: Diabetic nephropathy is the most devastating complication of diabetes and is now the
IM 655 Nephrology Clerkship. Selective/Elective Clerkship Rotation Syllabus
 IM 655 Nephrology Clerkship Selective/Elective Clerkship Rotation Syllabus Osteopathic Medical Specialties Mary Hughes DO Chairperson, Instructor of Record Mary Hughes DO hughesm@msu.edu (100% for CLIFMS
IM 655 Nephrology Clerkship Selective/Elective Clerkship Rotation Syllabus Osteopathic Medical Specialties Mary Hughes DO Chairperson, Instructor of Record Mary Hughes DO hughesm@msu.edu (100% for CLIFMS
DR. Trinh Thi Kim Hue
 TYPE 2 DIABETES IN THE CHILD AND ADOLESCENT DR. Trinh Thi Kim Hue CONTENTS Definition Diagnosis Treatment Comorbidities and Complications Comorbidities and Complications Screening for T2D References DEFINITION
TYPE 2 DIABETES IN THE CHILD AND ADOLESCENT DR. Trinh Thi Kim Hue CONTENTS Definition Diagnosis Treatment Comorbidities and Complications Comorbidities and Complications Screening for T2D References DEFINITION
Chronic Kidney Disease: A New Classification and Staging System
 Clinical Review Article Series Editor: Mark A. Perazella, MD, FACP Chronic Kidney Disease: A New Classification and Staging System Mark A. Perazella, MD, FACP Robert F. Reilly, MD Chronic kidney disease
Clinical Review Article Series Editor: Mark A. Perazella, MD, FACP Chronic Kidney Disease: A New Classification and Staging System Mark A. Perazella, MD, FACP Robert F. Reilly, MD Chronic kidney disease
Metabolic Syndrome Overview: Easy Living, Bitter Harvest. Sabrina Gill MD MPH FRCPC Caroline Stigant MD FRCPC BC Nephrology Days, October 2007
 Metabolic Syndrome Overview: Easy Living, Bitter Harvest Sabrina Gill MD MPH FRCPC Caroline Stigant MD FRCPC BC Nephrology Days, October 2007 Evolution of Metabolic Syndrome 1923: Kylin describes clustering
Metabolic Syndrome Overview: Easy Living, Bitter Harvest Sabrina Gill MD MPH FRCPC Caroline Stigant MD FRCPC BC Nephrology Days, October 2007 Evolution of Metabolic Syndrome 1923: Kylin describes clustering
Protocol for the safe administration of iodinated contrast media in diagnostic radiology
 Protocol for the safe administration of iodinated contrast media in diagnostic radiology Protocol statement: This protocol applies to all staff within Radiology Departments at Heart of England NHS Foundation
Protocol for the safe administration of iodinated contrast media in diagnostic radiology Protocol statement: This protocol applies to all staff within Radiology Departments at Heart of England NHS Foundation
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains