PEPPER, CASPER/ OSCAR, QM and 5 Star Reports. Lisa Thomson Vice President
|
|
|
- Scott Richard
- 7 years ago
- Views:
Transcription
1 PEPPER, CASPER/ OSCAR, QM and 5 Star Reports Lisa Thomson Vice President

2 Objectives Identify the purpose of the PEPPER and CASPER (OSCAR) report Identify the purpose of the Quality Measures and Five Star reports, incorporating the new public reporting requirements. Interpret the individual reports and identify the outlier data that places a facility at greater risk Discuss implementations strategies incorporating this data 2

3 The Journey Begins

4 Preparation for Change 4
5 5

6 New Era of Healthcare Quality and Efficiency is the value based modifier part 2/

7 VBP is Around the Corner

8 Stake Holders in Performance Measurement US Department of HHS CMS (also CMS 5 Star reporting and SNF VBP) AHRQ MedPAC GAO OIG State Medicaid programs NQF - NQS initiatives Affordable Care Act driving quality outcomes, increasing performance 8

9 9

10 Government Alignment Government Accountability Office Medicare Program is at high risk for fraud, waste, and abuse Office of Inspector General In 2012, 25% of SNF claims were billed in error Monitor COT, Add to FPS, CMS to instruct MAC, RAC to closely monitor SNFs Centers for Medicare and Medicaid Services In 2013, SNFs were required to have a compliance program 10

11 Compliance Program A SNF should conduct regular audits to ensure services provided are necessary and that charges for Medicare services are correctly documented and billed. PEPPER Program for Evaluating Payment Patterns Electronic Report First available to SNFs in 2013 SNF PEPPER Version Q4FY12 Latest report available May 2014 SNF PEPPER Version Q4FY13 August HX Data 11

12 PEPPER Compares SNF to SNF nationally, regional and individually 2013 (1 st PEPPER) received USPS around 8/30/13 Envelope with red print on the outside Your facility specific PEPPER Many perceived as junk mail Your facility specific PEPPER 12

13 Potentially Improper Payments PEPPER does not identify the presence of improper payments, but it can be used as a guide for auditing and monitoring efforts. A SNF can use PEPPER to compare its claims data over time to identify areas of potential concern and to identify changes in billing practices. 13

14 Facility-Specific Information PEPPERs are not available for public release They are released only to CEO, President, or Administrator TMF Health Quality Institute, a CMS contractor, produced the report SNFs received them by USPS in 2013 but will receive then on-line in 2014 TMF provides an Access database to MACs, FIs, and Recovery Auditors (RACs) FATHOM or First-look Analysis Tool for Hospital Outlier Monitoring (secured access point) 14
 FATHOM or First-look Analysis Tool for Hospital Outlier Monitoring (secured access")
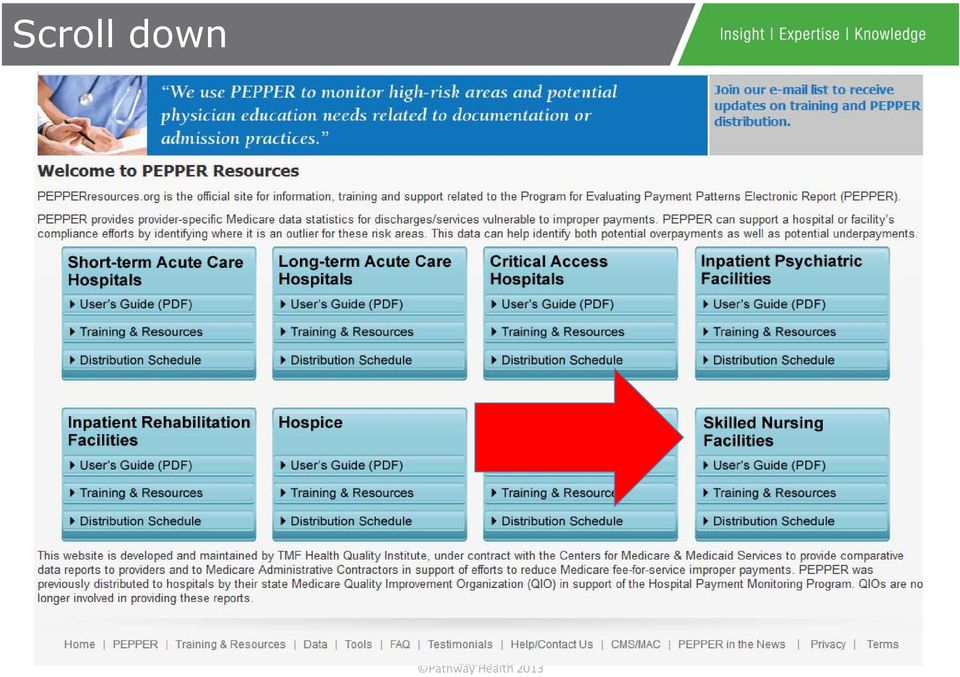
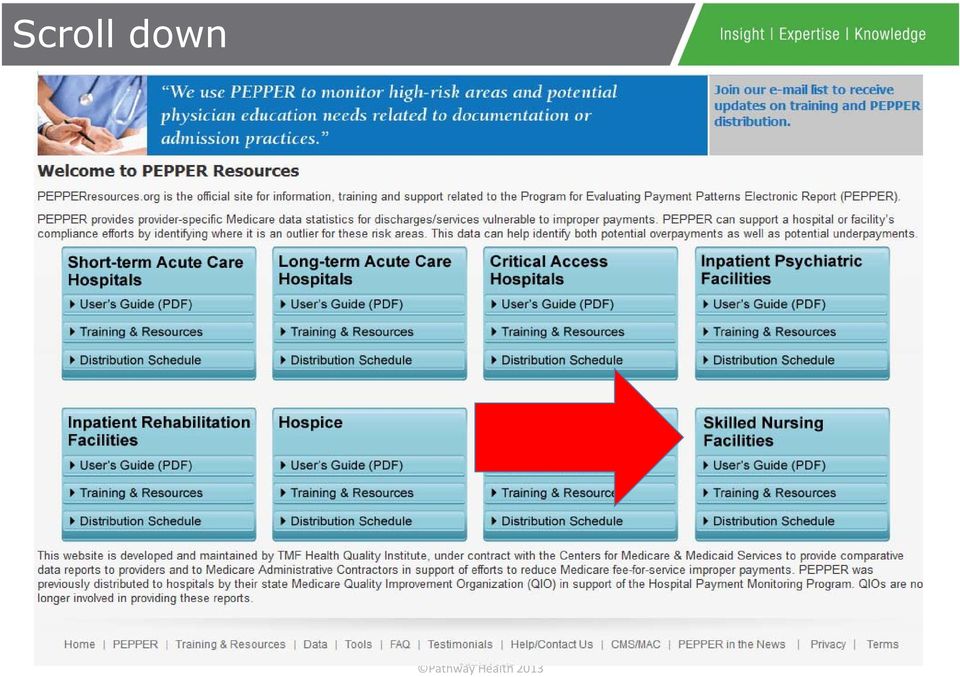
15 How To Obtain the PEPPER Report SNF Swing-Bed Units Via QualityNet Other SNFs Visit PEPPERresources.org Hover over PEPPER Select Secure PEPPER Access Review Instructions and access portal Join the listserv to receive notification when PEPPER reports are available 15

16 PEPPER Data and Rationale Based on OIG report CMS and OIG indicate high Medicare expenses could be suggestive of over coding CMS indicates that 20% highest expenses are questionable CMS identifies expenses above the 80% percentile as potential outliers CMS identifies that the bottom 20% of outliers are potential under coding The bottom 20 th percentile as outlier may be perceived as evidences of poor Quality of Care 16

17 17

18 Scroll down 18
19 User Guide 19

20 Scroll down 20
21 Training and Resources 21
22 Training and Resources 22
23 Scroll down 23
24 Distribution 24
25 25
26 Required Information for Portal Access (1 of 2) 6-digit CMS Certification Number Also referred to as the provider number or PTAN Provider Transaction Access Number Issued when the Medicare contractor approves facility enrollment Not the same as the tax id or NPI number Will have 3 rd digit of 5 or 6 Hospital-based swing bed unit PEPPERs, with 3 rd digit of U are not available on the portal; they are distributed via QualityNet 26
27 Required Information for Portal Access (2 of 2) Patient Control Number (form locator 03a) or Medical Record Number (form locator 03b) from the UB-04 claim of a traditional fee-for-service Medicare beneficiary receiving services during September 2013 ( from or through date between September 1 30, 2013) 27
28 Interpret the Individual Reports 28
29 SNF PEPPER Version Q4FY13 Episodes of care ending between October 1, 2010, through September 30, 2013 Federal fiscal years 2011, 2012, and 2013 Remember: 10/1/10 (FY 2011) RUGS III (53) to RUGS IV (66) 10/1/11 (FY 2012) Change of Therapy (COT) Assessments An episode of care is created from the UB04 claims submitted by a SNF for each beneficiary A beneficiary could have multiple episodes within this time frame 29
30 Six PEPPER Target Areas Identified by CMS as being potentially at risk for improper Medicare payments. Therapy RUGs with High ADLs Non Therapy RUGs with High ADLs COT Assessment Ultrahigh Therapy RUGs Numerator: Days billed of RUGs RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB Denominator: Days billed for all Therapy RUGS ADLs: Numerator: Days billed SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, IB1 in RUGs III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUGs IV Denominator: Days billed for all non therapy RUGS ADLs: in RUGs III; in RUGs IV Numerator: Count of assessments with AI second digit D Denominator: Count of all assessments Change of Therapy Assessments started 10/1/11 (FY 2012) Numerator: Days billed with RUGs RUX, RUL, RUC, RUB, RUA Denominator: Days billed for all therapy RUGs Ultra High Criteria: 720 minutes or more per week, at least 2 therapies, one of the them at least 5 days & the second at least 3 days Therapy RUGs Numerator: Days billed for all therapy RUGs Denominator: Days billed for all therapy and non therapy RUGs 90+ Day Episodes of Care Numerator: Episodes of care at the SNF with LOS 90+ days Denominator: All episodes of care at the SNF Maximum 100 days per benefit period 30
31 PEPPER Data Restrictions Statistics will not display when the numerator or denominator count is less than 11 for a target area in any time period. Some SNFs may not see any data for some target areas or time periods A few SNFs will not have a PEPPER available 31
32 Take Note (1) Payment rates for therapy RUGs are typically higher than those for non-therapy RUGs Medicare typically pays more for higher levels of therapy, and generally pays the most for ultrahigh therapy SNFs should ensure that the amount of therapy beneficiaries receive is: Appropriate, Necessary, and Documentation supports the level of care and services provided Medicare Benefit Policy Manual, Chapter 8, Section
33 Take Note (2) Medicare reimburses up to 100 days of skilled care per beneficiary spell of illness SNFs should ensure that beneficiaries are receiving services that are necessary SNFs should also ensure that beneficiaries receive skilled care the entire duration of their SNF stay 33
34 3 Types of Reports SNF Compare Report for Q4 FY 2013 (1) SNF Target Area Reports for FY 2011, 2012, & 2013 (6) Top RUG Reports for FY 2013 (4) SNF All Episodes 90+ Days Episodes Jurisdiction All Episodes 90+ Days Episodes 34
35 SNF Compare Targets Report Summarizes Medicare feefor-service claims data for SNF episodes of care Target Count is most recent fiscal year FY13 10/1/12 9/30/13 3 Comparison Groups National MAC Jurisdiction State 35
36 Calculating Percentages Target Area Percents are calculated by dividing the numerator by the denominator (See Slide 15), then multiplying by 100. Example: Numerator count = 20, and Denominator count = /100 X 100 = 20% Target Area Percent is 20% This lets the SNF know its billing patterns 36
37 PEPPER Data and Rationale Based on OIG report CMS and OIG indicate high Medicare expenses could be suggestive of over coding CMS indicates that 20% highest expenses are questionable CMS identifies expenses above the 80% percentile as potential outliers CMS identifies that the bottom 20% of outliers are potential under coding The bottom 20 th percentile as outlier may be perceived as evidences of poor Quality of Care 37
38 Calculating Percentiles The Percentiles give context by helping a provider understand how it compares to other providers. Definition of a Percentile: The percentage of providers with a lower target area percent To calculate Percentiles for all providers in a comparison group (nation, jurisdiction, or state) the target area percents are sorted from largest to smallest for each time period. Example: If 40% of the providers target area percents were lower than provider A, then provider A would be at the 40 th percentile. 38
39 Calculating 80 th & 20 th Percentiles 91% 90% 88% 83% 79% 73% 71% 68% 59% 32% 80 th percentile 20 th percentile The top two providers percents are at or above the 80th percentile. The bottom two providers percents are at or below the 20th percentile. 39
40 Risk for Improper Medicare Payments Target area percents for all SNFs with reportable data are ordered from highest to lowest. The target area percent below which 80% of all SNFs target area percents fall, is the 80 th percentile. SNFs whose target percents are at or above the 80 th percentile (that is, the top 20%) are considered at risk for improper Medicare payments. 40
41 Prioritizing Your SNF s Data - QAPI Percentile values at or above the 80 th percentile National Jurisdiction State Target Count If more than one area is at or above the 80 th percentile, the one with the higher/est target count should be given a higher priority than the other(s) 41
42 Detail of One Target Area PEPPER Report 42
43 Components of Each Report Graph SNF Data Table Comparative Data Table Interpretive Guidance & Suggested Interventions 43
44 Six PEPPER Target Areas Identified by CMS as being potentially at risk for improper Medicare payments. Therapy RUGs with High ADLs Non Therapy RUGs with High ADLs COT Assessment Ultrahigh Therapy RUGs Numerator: Days billed of RUGs RUX, RVX, RHX, RMX, RUC, RVC, RHC, RMC, RLB Denominator: Days billed for all Therapy RUGS ADLs: Numerator: Days billed SSC, CC2, CC1, BB2, BB1, PE2, PE1, IB2, IB1 in RUGs III; HE2, HE1, LE2, LE1, CE2, CE1, BB2, BB1, PE2, PE1 in RUGs IV Denominator: Days billed for all non therapy RUGS ADLs: in RUGs III; in RUGs IV Numerator: Count of assessments with AI second digit D Denominator: Count of all assessments Change of Therapy Assessments started 10/1/11 (FY 2012) Numerator: Days billed with RUGs RUX, RUL, RUC, RUB, RUA Denominator: Days billed for all therapy RUGs Ultra High Criteria: 720 minutes or more per week, at least 2 therapies, one of the them at least 5 days & the second at least 3 days Therapy RUGs Numerator: Days billed for all therapy RUGs Denominator: Days billed for all therapy and non therapy RUGs 90+ Day Episodes of Care Numerator: Episodes of care at the SNF with LOS 90+ days Denominator: All episodes of care at the SNF Maximum 100 days per benefit period 44
45 Therapy RUGs with High ADLs Suggested Interventions If At/Above 80 th Percentile Risk of potential over coding of ADL status Education orientation, at least quarterly Concurrent audits Suggested Interventions If At/Below 20 th Percentile Risk of potential under coding of ADL status Education orientation, at least quarterly Concurrent audits 45
46 Non-therapy RUGs with High ADLs Suggested Interventions If At/Above 80 th Percentile Risk of potential over coding of ADL status Education orientation, at least quarterly Concurrent audits Suggested Interventions If At/Below 20 th Percentile Risk of potential under coding of ADL status Education orientation, at least quarterly Concurrent audits 46
47 Change of Therapy Assessment Suggested Interventions If At/Above 80 th Percentile This could indicate the SNF is experiencing challenges with delivering services as anticipated Look at therapy availability, scheduling Can care planning be improved? Suggested Interventions If At/Below 20 th Percentile N/A Note: SNFs using the COT infrequently or not at all may be targeted by MACs or RACs for review to establish whether therapy assessments are being completed as required 47
48 Ultrahigh Therapy RUGs Suggested Interventions If At/Above 80 th Percentile This could indicate the SNF is improperly billing for therapy services Suggested Interventions If At/Below 20 th Percentile N/A Is the therapy provided reasonable and medically necessary? Is the amount of therapy reported on the MDS supported by documentation in the medical record? 48
49 Therapy RUGs Suggested Interventions If At/Above 80 th Percentile This could indicate the SNF is improperly billing for therapy services Suggested Interventions If At/Below 20 th Percentile N/A Is the therapy provided reasonable and medically necessary? Is the amount of therapy reported on the MDS supported by documentation in the medical record? 49
50 90+ Day Episodes of Care Suggested Interventions If At/Above 80 th Percentile This could indicate the SNF is continuing treatment beyond the point where those services are necessary. Suggested Interventions If At/Below 20 th Percentile N/A Review all documentation to ensure that beneficiaries continued care is appropriate and they received a skilled level of care. Review plans of care for appropriateness. Assess appropriateness of discharge plans 50
51 SNF Top RUGs Report Example FY /1/12 through 9/30/13 Total of 2 SNF Reports Top RUGS for the SNF (To the left) Top RUGs for the SNF for episodes of care with 90+days Each Report Up to 20 RUG Codes Must have at least 11 days billed to the respective RUG to appear 51
52 Jurisdiction-Wide Top RUGs Report FY /1/12 through 9/30/13 Total of 2 Reports Top RUGS for the Jurisdiction (To the left) Top RUGs for the Jurisdiction for episodes of care with 90+days Each Report Top 20 RUG Codes Must have at least 11 days billed to the respective RUG to appear 52
53 Jurisdictions MAC Jurisdictions E F K H L Process Medicare Part A & B Claims for These States California, Hawaii, Nevada, American Samoa, Guam, Northern Mariana Islands Alaska, Arizona, Idaho, Montana, North Dakota, Oregon, South Dakota, Utah, Washington, Wyoming Iowa, Kansas, Missouri, Nebraska Indiana, Michigan Illinois, Minnesota, Wisconsin Connecticut, New York, Maine, Massachusetts, New Hampshire, Rhode Island, Vermont Arkansas, Colorado, New Mexico, Oklahoma, Texas, Louisiana, Mississippi Delaware, District of Columbia, Maryland, New Jersey, Pennsylvania (Part B for Arlington & Fairfax counties & city of Alexandria in Virginia) MAC Noridian Healthcare Solutions, LLC Wisconsin Physicians Service Insurance Corporation National Government Services, Inc. Novitas Solutions, Inc. N Florida, Puerto Rico, U.S. Virgin Islands First Coast Service Option, Inc. 10 Alabama, Georgia, Tennessee Cahaba Government Benefit Administrators, LLC 11 North Carolina, South Carolina, Virginia, West Virginia (See Part B Virginia exclusions for L above) Palmetto GBA, LLC 15 Kentucky, Ohio GCS Administrators, LLC 53
54 Internal Audits -- QAPI Pre-Billing Audits Medicare Meeting 54
55 Pre-Billing Audit Clean Claim A claim that can be processed without obtaining additional information from the provider or a third party A focused Medicare Meeting Draft UB-04 Information confirmed by someone not directly responsible for data Examples: Administrator verifies therapy log for minutes & days DON verifies Validation Report Billing Office verifies Physician Certifications 55
56 What to Check at Pre-Billing Audit Name, HICN, DOB, sex match CWF Admission dates & qualifying hospital stay dates Copy of Medicare card MD orders Therapy minutes match Section O of MDS MDS submitted & accepted RUG & modifiers match Correct number of days billed for each MDS Default days Provider liability days Physician certifications Therapy certifications Diagnoses sequenced Ancillary charges Medicare as Secondary Payer Nursing & therapy documentation Admission note Weekly note Discharge note/summary Re-instatement note 56
57 Nursing & Therapy Documentation Chapter 8 Coverage of Extended Care (SNF) Services New Section Documentation to support skilled care determinations Chapter 15 Covered Medical and Other Health Services (Part B Therapy) 57
58 Other Data Sources 58
59 Internal Sources for Trend Analysis CASPER (QEIS) Reason for Assessment Report (RFA) MDS 3.0 Software RUG Reports ADL Reports Financial Software Length of Stay 59
60 External Sources: The First PEPPER First PEPPER Q4FY12 Statistics for FY10, FY11, FY12 State comparison group included SNFs in the same state within the same MAC jurisdiction First page was a letter Majority were mailed in hard-copy format 8/13 This PEPPER Q4FY13 Statistics for FY11, FY12, FY13 State comparison group includes all SNFs in the same state, regardless of whether they are in the same jurisdiction First page is Purpose Electronic distribution as Microsoft Excel workbook via Secure PEPPER Portal or QualityNet 60
61 OSCAR to CASPER! 61
62 OSCAR 3 and 4 Online Survey Certification and Reporting Prior to 10/1/10 Provided by surveyors at the time of annual survey entrance conference OSCAR 3 All facility deficiencies from the last 4 years OSCAR 4 Most recent survey deficiencies and comparisons to state, CMS region, and nation 672 information A roadmap to previous survey issues 62
63 Common Acronyms CASPER Certification and Survey Provider Enhance Reporting system QIES Quality Improvement and Evaluation System ASAP ASPEN Assessment Submission and Processing System Automated Survey Processing Environment 63
64 OSCAR to CASPER Implementation of the MDS 3.0 on October 2010, Appendix P of the State Operations Manual was revised. CMS officially changed the terminology of Online Survey Certification and Reporting (OSCAR) to Certification and Survey Provider Enhanced Reporting (CASPER) per S&C letter CASPER/QEIS are part of a large relational database operating within CMS s Automated Survey Processing Environment (ASPEN) 64
65 CASPER DATA Types During the annual survey Facility is required to submit reports to the State Agencies, these reports are the 802, 671 and 672. It is important that these reports are submitted accurately to the State CMS analyzes the data The administrative purpose of survey data is to support the survey and certification function. Every "institutional" health care provider in the United States that is certified to provide services under either Medicare or Medicaid (or both) is listed in survey data. 65
66 Access your CASPER Reports MDS 3.0 Quality Measure Report Manual Instructions on how to access reports How to interpret your data Survey preparation Surveyors preparation based on your data Quality Improvement activities 66
67 CASPER Reports Password protected and encrypted MDS 3.0 reports are automatically purged after 60 days 67
68 CASPER Survey Data 68
69 OSCAR Data Today - CASPER National Associations and their state affiliates provide resources and support AHCA and Leading Age Updated on a quarterly basis 69
70 CASPER Survey Reports Survey History Complaint Trends Life Safety F Tags Cited Scope and Severity Why is this important? 70
71 Identifying Risk Compare your data against state, CMS region, and national data to help assess risk of survey deficiencies Facility s own trends State, regional, and national hot topics Remember: Repeat F Tag citations can lead to stronger penalties! Resident condition data (672) outliers may be indicative of your unique population, but does facility documentation and policies and procedures support this assumption 71
72 CMS Regional Offices 72
73 CMS 672 Form 73
74 Facility Responsibilities Track your F Tags as well as the severity and scope from year to year Annual surveys and Complaint surveys What does your latest Quality Assurance monitoring show? Are you still in compliance? Keep your 672 and 802 forms up to date MDS software Manual updates with admissions & discharges Increase the frequency of updates within survey window 74
75 CASPER MDS Specific Data 75
76 CASPER Certification and Survey Provider Enhanced Reports Accessed through the MDS 3.0 submission portal 13 reports are available and the provider can specify the date range for each report qtso.com for Chapter 6 of the QTSO Technical Support Manual 76
77 CASPER Reports Page 77
78 Data in different Directions 78
79 CASPER Reporting User s Guide 79
80 13 Reports MDS 3.0 Activity MDS 3.0 Admission/Re-Entry MDS 3.0 Assessments with Error Number XXXX Discharges MDS 3.0 Error Detail by Facility MDS 3.0 Error Number Summary by Facility by Vendor MDS 3.0 Errors b y Field by Facility MDS 3.0 Missing Assessments MDS 3.0 NH Assessment Print MDS 3.0 Reason for Assessment Statistics MDS 3.0 Roster MDS 3.0 Submission Statistics by Facility MDS 3.0 Vendor List 80
81 MDS 3.0 Activity Report Lists the accepted assessments, tracking records, and inactivation requests that were submitted by or on behalf of a facility during a specified timeframe. Use to determine workload. Use to determine if record was submitted. Run monthly or more frequently.
82 MDS 3.0 Assessments with Error Number XXXX Lists the assessments submitted with a specified error for a facility during a specified timeframe. Use to identify assessments with certain fatal errors that were submitted that need to be corrected and resubmitted. Use to determine which assessments were not completed under CMS timing rules (i.e., OBRA quarterly and yearly rules). Use to identify a pattern with coding or an area in need of training. Use to identify software-related errors.
83 MDS 3.0 Discharges Lists the residents discharged (A0310F = 10, 11, or 12) from a facility during a specified timeframe. When a discharged resident appears on the MDS 3.0 Roster report, use this report to determine if discharge was accepted in the ASAP database. Use to derive a list of all residents discharged since the last survey or other time period. Run monthly or more frequently.
84 References 1 Minimum Data Set (MDS) 3.0 Provider User s Guide on the QTSO MDS 3.0 web site at Section 5 contains the error and warning messages.
85 MDS 3.0 Missing OBRA Assessment Lists the residents in select facilities for whom the target date of the most recent OBRA assessment (other than a discharge or death record) is more than 138 days prior to the report run date. The report also includes residents for whom no OBRA record was submitted for a current episode that began more than 60 days prior to the report run date. Use as a QA tool to ensure all assessment have been successfully submitted.
86 MDS 3.0 RFA Statistics Summarizes for a facility the reasons for assessment for accepted assessments submitted during a specified timeframe. Use to monitor /evaluate workload during an identified timeframe. Great tool for leaders to use!!!
87 MDS 3.0 Roster Lists residents of a facility for whom the latest accepted, federally required assessment is not a Discharge assessment. (A0310F = 10, 11, or 12) Use to determine a list of all current residents at time of survey. Use as a QA tool to ensure all current residents have an entry record and all discharge residents have a discharge record in the ASAP database. CMS FOCUS!!!
88 References 2 CASPER Reporting User s Guide for MDS Providers at Section 6 contains MDS 3.0 NH provider reports (section 8 is swing bed provider reports). Section 7 contains the MDS 3.0 NH final validation report (section 9 is swing bed final validation report). Section 10 contains MDS 3.0 submitter validation report.
89 Quality Measures 89
90 Purpose of QMs Provide the public, information about: quality of care at nursing homes assist in choosing a nursing home care at a nursing home where they or family members already live to facilitate discussions with nursing home staff regarding the quality of care Provide data to the nursing home to help them in their quality improvement efforts 90
91 All Quality Measures 91
92 Measure Inventory for QMs 92
93 Summary of QMs 18 MDS 3.0-based 5 short-stay 13 long-stay 4 surveyor-only long-stay measures National and state benchmarks used for comparison purposes National benchmarks used for ranking purposes (percentiles) Surveyors are directed to focus on any QM at the 75 th percentile or greater 93
94 MDS 3.0-Based Short Stay QMs 1 Self report moderate to severe pain 2 Have pressure ulcers that are new or worsened* Newly received an anti psychotic medication Were assessed and appropriately given the seasonal influenza vaccine Were assessed and appropriately given the pneumococcal vaccine 94
95 MDS 3.0-Based Long Stay QMs (1 of 3) 1 Experienced one or more falls with major injury 2 Self report moderate or severe pain* Are high risk residents with pressure ulcers Were assessed and appropriately given the seasonal influenza vaccine Were assessed and appropriately given the pneumococcal vaccine 95
96 MDS 3.0-Based Long Stay QMs (2 of 3) Have a urinary tract infection Are low risk residents and lose control of bowel or bladder Have/Had a catheter inserted and left in the bladder* Were physically restrained Have an increased need for help with daily activities 96
97 MDS 3.0-Based Long Stay QMs (3 of 3) Lose too much weight Have depressive symptoms Received an antipsychotic medication 97
98 MDS 3.0-Based Survey Only QMs 1 2 Prevalence of falls Prevalence of psychoactive medication use, in the absence of psychotic or related conditions 3 Prevalence of antianxiety/hypnotic Use 4 Prevalence of behavior symptoms affecting others 98
99 Quality Measure Definitions Instruments/NursingHomeQualityInits/Downloads/MDS30QM-Manual.pdf 99
100 100
101 Admission & Re-Entry Admission Has never been admitted before OR Has been in this facility previously and is returning after a discharge return not anticipated OR Has been in this facility previously and was discharged return anticipated and is returning more than 30 days after discharge Re Entry Discharged return anticipated AND Returned to the facility within 30 days of discharge 101
102 Stay The period of time between a resident s entry into a facility and either a discharge or the end of the target period, whichever comes first A set of contiguous days in a facility Start of stay = either an admission or re entry End of stay = discharge, death in facility record or the end of the target period 102
103 Episode A period of time spanning one or more stays Begins with an Admission Entry Ends with Discharge return not anticipated OR Discharge return anticipated but did not return within 30 days of discharge OR A death in facility tracking record OR The end of the target period 103
104 CDIF: Cumulative Days in Facility Total number of days within an episode during which the resident was in the facility May contain one or more stays Only days in the facility count Outside days (home, hospital, etc.) do not count Entry day is counted, but discharge day is not unless it is the same day as entry Counting stops with the last record in the target period if that record is a discharge assessment or a death in facility record OR if the end of the period is reached, whichever is earlier 104
105 Short Stay and Long Stay Short Stay An episode with CDIF less than or equal to 100 days as of the end of the target period Long Stay An episode with CDIF greater than or equal to 101 days as of the end of the target period 105
106 Risk Adjustment 106
107 What Is Risk Adjustment? Risk adjustment refines quality measure rates to better reflect the prevalence of problems that facilities should be able to address Why? To ensure comparisons across facilities are fair and not skewed by the presence of special populations Example: If a facility has more short-stay residents with diabetes, their expected rate for pressure ulcers is higher than the average facility. Therefore, to level the playing field, their rate will be adjusted downward. 107
108 Three Types of Risk Adjustments Exclusions Risk Groups Covariates 108
109 Exclusions Residents removed from calculations if their outcomes are not under the facility s control Residents whose outcome may be unavoidable Residents removed if certain MDS items are missing All QMs except the vaccination QMs have some exclusions 109
110 Risk Groups QMs divided into high or low risk groups according to the diseases/conditions the residents have that make them likely to have the condition. Two QMs High risk pressure ulcers Low risk residents who lose control of their bladder or bowel 110
111 Covariates Resident level risk factors used to risk adjust facility QM rates higher or lower based on proportion of residents with the defined characteristics Three QMs Residents with pressure ulcers that are new or worsened (short Term) Residents who selfreport moderate to serve pain (Long Term) Residents who have/had a catheter inserted and left in their bladder (long Term) 111
112 Covariate Effect on Pain QM Higher Risk Adjusted Rate Expect lower rate if there are fewer cognitively intact residents reporting (or staff not identifying) pain Expect higher rate if there are more cognitively intact residents reporting more pain Lower Risk Adjusted Rate 112
113 Quality Measures Reports 113
114 CASPER Made possible by the national analytic reporting system, the Certification and Survey Provider Enhanced Reporting (CASPER) system Access via CMS Welcome screen same screen through which assessments are transmitted to QIES ASAP national database Click MDS link, then Click CASPER Reporting Online Reports link 114
115 Data in different Directions 115
116 QM Report Access 116
117 CASPER Reporting User s Guide 117
118 CASPER Three reports Facility Quality Measure Report Resident Level Quality Measure Report Monthly Comparison Report Reports default to a 6-month reporting period ending with the most recently ended month Users may change the dates of the reporting period manually 118
119 Facility Quality Measure Report Displays Each QM Numerator and denominator used for the calculation for each QM Facility percentage Comparison of facility score with all facilities in state and nation Assists to identify possible areas for further emphasis in facility quality improvement activities or investigation during the survey process 119
120 Sample QM Report 120
121 Facility QM Report Upper Left Facility ID information Date data was calculated Data is calculated weekly Upper Right Report Period Period of time covered by the report Comparison Group Data calculated monthly with two-month delay Run Date Date the report was accessed by the facility 121
122 Facility QM Report First two left-most columns QMs listed by name and ID numbers Remaining columns include facility data and comparison group information Num Numerator; top number of the fraction The number of residents with the QM condition in the reporting period Denom Denominator; number of residents with assessments evaluated for the QM condition Based on time frame of the reporting period and, for some QMs, focus on a specific subgroup of that number 122
123 Facility QM Report Observed Percent Numerator denominator x 100 For QMs not risk adjusted, this is the final score the percentage of residents with the QM condition Adjusted Percent Results after a covariate is applied to the observed percent as risk adjustment Pertains to three QMs; for them, this is the final QM score 123
124 Facility QM Report Comparison Group State Average Statewide percentage; the average of the QM percentages for all facilities in the state Should be used for comparison to the facility-specific score Comparison Group National Average National percentage; the average of the QM percentages for all facilities in the nation Should be compared to the facility-specific score 124
125 Facility QM Report State and national percentages are not benchmarks Percentile < 75 th or score the state or national average is not necessarily indicative of satisfactory performance If the state and/or nation are not doing particularly well on a certain QM issue, then those levels should not be viewed as the goal to achieve 125
126 Resident Level QM Report Identifies all residents, active and discharged, included in the QM calculations They are the residents in the numerator of the calculations Also indicates which QMs triggered for each resident Important tool that facilitates detailed record reviews of residents in the numerator of a QM for use in QA/QI activities and survey process 126
127 Resident Level QM Report 127
128 Monthly Comparison Report Summarizes comparison of facility s performance to state and national averages Made available to the public on NHC Not included Long-stay QMs with denominator 30 Short-stay QMs with denominator 20 High-triggered percentages 128
129 Monthly Comparison Report 129
130 How To Use the CASPER Reports State and National comparison group data are calculated monthly on the first day of the month. Data calculation is delayed by 2 months in order to allow for submission of late and corrected assessments. Your QM data is calculated weekly for the assessments submitted since the previous week s data calculation 130
131 How To Use The Data Strong programs of Performance Improvement (QAPI) Continuous monitoring of key aspects of key systems Correlate related QM scores with each other for clues to causative factors Identify and correct problems before they become trends Individual accountability for key systems put someone in charge of the system Quality Management is Key 131
132 MDS Excellence Misunderstandings about coding definitions can be disastrous QM scores are derived from MDS data Inaccurate coding can result in misleading Quality Measure scores Inaccurate MDS coding can result in inappropriate resident care 132
133 Educate on Coding the MDS ADLs (Section G) Rule of 3, ADL algorithm Pressure Ulcers (Section M) No back-staging, definition of worsening pressure ulcer Influenza Vaccine (Section O) Capturing vaccine from season just ended when new season hasn t started yet Restraints (Section P) Code only if the device meets the definition of daily restraint Urinary Tract Infection (Section I) Definition is very specific; code only if definition is met 133
134 Resources MDS 3.0 Quality Measures User s Manual RAI User s Manual CMS MDS 3.0 Training Materials
135 The Five Star Rating System 135
136 Five Star Ratings 136
137 Nursing Home Compare Website Each nursing home participating in Medicare and/or Medicare is a assigned an overall rating between one and five stars 5 Stars = Much above average* 1 Star = Much below average* * Compared to other nursing homes in the state 137
138 Three Categories 1 5 stars assigned to each category Health Inspections Staffing Quality Measures 138
139 Health Inspections Last 3 Years Standard Surveys and Complaint Surveys Health Inspections Most Recent Survey Findings Are Weighted More Than the Prior 2 Years Most Recent Year = 50% 2 Years Ago = 1/3 3 years Ago = 1/6 139
140 Survey Deficiency Score Severity/Scope Isolated Pattern Widespread Immediate jeopardy to resident health or safety Actual harm that is not immediate jeopardy No actual harm with potential for more than minimal harm that is not immediate jeopardy No actual harm with potential for minimal harm J 50 points (75 points if SQC) G 20 points D 4 points A 0 points K 100 points (125 points if SQC) H 35 points (40 points if SQC) E 8points B 0 points L 150 points (175 points if SQC) I 45 points (50 points if SQC) F 16 points (20 points if SQC) C 0 points 140
141 Staffing RN Hours/Resident/Day Total Staffing (RNs, LPNs, CNAs) /Resident/Day Staffing Staffing Data Submitted by the Facility at Time of Standard Survey Adjusted Based Upon Resident Acuity (RUG IV CMIs) 141
142 Quality Measures 5 Short Stay QMs 13 Long Stay QMs 9 of the 18 QMs Are Used to Calculate the Star Rating Quality Measures Charts Graphs 142
143 Five Star QMs Short Stay (2) Pain Pressure Ulcers Long Stay (7) Falls with Major Injury Pain Pressure Ulcers UTIs Catheters Physical Restraints ADL Assistance 143
144 Five Star Quality Rating System Scoring All 9 QMs are given equal weight 1 to 100 points are assigned to each QM based on facility performance Percentiles based on national distribution for all the QMs except for the ADL measure, which is state-specific More affected by case-mix variation Influenced by differences in State Medicaid policies Cut points for the QMs were set based on the QM distributions averaged across Q2, Q3, & Q4 of 2011 and will remain in effect until at least July
145 Calculating Overall 5 Star Rating Step Methods 1 Start with the Health Inspections Rating 2 Add 1 star if the Staffing Rating is 4 or 5 stars and greater than the Health Inspections Rating Subtract 1 star if the Staffing Rating is 1 star 3 Add 1 star if the Quality Measures Rating is 5 stars Subtract 1 star if the Quality Measures Rating is 1 star 4 If the Health Inspections Rating is 1 star, then the Overall Rating cannot be upgraded by more than 1 star based on the Staffing and Quality Measure Ratings 5 If a nursing home is a Special Focus Facility, the maximum Overall Rating is 3 stars 145
146 Updated Cut Points CMS Five Star quality ratings for the health inspection domain are based on the relative performance of facilities within a State. This approach helps to control for variation between States. Facility ratings are determined using these criteria: The top 10 percent (lowest 10 percent in terms of health inspection deficiency score) in each State receive a five star rating. The middle 70 percent of facilities receive a rating of two, three, or four stars, with an equal number (approximately percent) in each rating category. The bottom 20 percent receive a one star rating. Enrollment and Certification/CertificationandComplianc/Downloads/cutpointstable.pdf 146
147 147
148 148
149 Individual Facility Staffing Data 149
150 5 Star Performance Enrollment and Certification/CertificationandComplianc/Downl oads/nhc Year Five Report.pdf 150
151 Overall Ratings Nationally - 5 Years 151
152 Health Inspection Ratings 152
153 QM Ratings 153
154 154
155 Data Updates affecting 5 Star Rating 155
156 Use the QM Preview Reports Available in the facility s shared folders on CMS QIES website (Same way you got to CASPER) Allow provider to see quality measure percent values prior to being posted on NHC QM values for the most recent quarter Corresponds with the NHC reporting cycle 156
157 Resources 5 Star Quality Rating System Technical User s Guide 157
158 Leadership Thoughts 158
159 Data Driven Decisions 159
160 Leadership and Data Determine Quality Profile: Assess Organization Data Review Internal Processes: Optimize Data Establish an Information Agenda for Planning Plan to handle bad or inaccurate data GIGO Leadership today Data Driven Decisions! Your data is key to positive outcomes
161 Data Management Leader s Role Important Role in health care today and beyond Improving clinical and operational performance Collecting Analyzing Interpreting Acting Improvement 161
162 Data and Quality Strategy
163 Implementation and Innovation For Sustainability Preparation Operational Readiness Assessment Services Internal Systems Team composition Increase clinical competencies Validation and benchmark data Excellent outcomes quality and financial Evaluate, reposition, partner and implement 163
164
165 PEPPER, OSCAR/CASPER, QM and Five Star Reports Lisa Thomson Vice President
Differences in Resident Case-mix Between Medicare and Non-Medicare Nursing Home Residents
 Differences in Resident Case-mix Between and Non- Nursing Home Residents Alan White Patricia Rowan Abt Associates Inc. A report by staff from Abt Associates for the Payment Advisory Commission MedPAC 425
Differences in Resident Case-mix Between and Non- Nursing Home Residents Alan White Patricia Rowan Abt Associates Inc. A report by staff from Abt Associates for the Payment Advisory Commission MedPAC 425
A/B MAC Jurisdiction 1 Original Medicare Claims Processor
 A/B MAC Jurisdiction 1 Jurisdiction 1 - American Samoa, California, Guam, Hawaii, Nevada and Northern Mariana Islands Total Number of Fee-For-Service Beneficiaries: 3,141,183 (as of Total Number of Beneficiaries
A/B MAC Jurisdiction 1 Jurisdiction 1 - American Samoa, California, Guam, Hawaii, Nevada and Northern Mariana Islands Total Number of Fee-For-Service Beneficiaries: 3,141,183 (as of Total Number of Beneficiaries
Public School Teacher Experience Distribution. Public School Teacher Experience Distribution
 Public School Teacher Experience Distribution Lower Quartile Median Upper Quartile Mode Alabama Percent of Teachers FY Public School Teacher Experience Distribution Lower Quartile Median Upper Quartile
Public School Teacher Experience Distribution Lower Quartile Median Upper Quartile Mode Alabama Percent of Teachers FY Public School Teacher Experience Distribution Lower Quartile Median Upper Quartile
Three-Year Moving Averages by States % Home Internet Access
 Three-Year Moving Averages by States % Home Internet Access Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware Florida Georgia Hawaii Idaho Illinois Indiana Iowa Kansas Kentucky Louisiana
Three-Year Moving Averages by States % Home Internet Access Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware Florida Georgia Hawaii Idaho Illinois Indiana Iowa Kansas Kentucky Louisiana
Model Regulation Service July 2005 LIFE INSURANCE MULTIPLE POLICY MODEL REGULATION
 Table of Contents Section 1. Section 2. Section 3. Section 4. Section 5. Section 6. Section 1. Model Regulation Service July 2005 Purpose Authority Exemptions Duties of Insurers Severability Effective
Table of Contents Section 1. Section 2. Section 3. Section 4. Section 5. Section 6. Section 1. Model Regulation Service July 2005 Purpose Authority Exemptions Duties of Insurers Severability Effective
Chex Systems, Inc. does not currently charge a fee to place, lift or remove a freeze; however, we reserve the right to apply the following fees:
 Chex Systems, Inc. does not currently charge a fee to place, lift or remove a freeze; however, we reserve the right to apply the following fees: Security Freeze Table AA, AP and AE Military addresses*
Chex Systems, Inc. does not currently charge a fee to place, lift or remove a freeze; however, we reserve the right to apply the following fees: Security Freeze Table AA, AP and AE Military addresses*
Exploring the Impact of the RAC Program on Hospitals Nationwide
 Exploring the Impact of the RAC Program on Hospitals Nationwide Overview of AHA RACTrac Survey Results, 4 th Quarter 2010 For complete report go to: http://www.aha.org/aha/issues/rac/ractrac.html Agenda
Exploring the Impact of the RAC Program on Hospitals Nationwide Overview of AHA RACTrac Survey Results, 4 th Quarter 2010 For complete report go to: http://www.aha.org/aha/issues/rac/ractrac.html Agenda
Real Progress in Food Code Adoption
 Real Progress in Food Code Adoption The Association of Food and Drug Officials (AFDO), under contract to the Food and Drug Administration, is gathering data on the progress of FDA Food Code adoptions by
Real Progress in Food Code Adoption The Association of Food and Drug Officials (AFDO), under contract to the Food and Drug Administration, is gathering data on the progress of FDA Food Code adoptions by
NON-RESIDENT INDEPENDENT, PUBLIC, AND COMPANY ADJUSTER LICENSING CHECKLIST
 NON-RESIDENT INDEPENDENT, PUBLIC, AND COMPANY ADJUSTER LICENSING CHECKLIST ** Utilize this list to determine whether or not a non-resident applicant may waive the Oklahoma examination or become licensed
NON-RESIDENT INDEPENDENT, PUBLIC, AND COMPANY ADJUSTER LICENSING CHECKLIST ** Utilize this list to determine whether or not a non-resident applicant may waive the Oklahoma examination or become licensed
American C.E. Requirements
 American C.E. Requirements Alaska Board of Nursing Two of the following: 30 contact hours 30 hours of professional nursing activities 320 hours of nursing employment Arizona State Board of Nursing Arkansas
American C.E. Requirements Alaska Board of Nursing Two of the following: 30 contact hours 30 hours of professional nursing activities 320 hours of nursing employment Arizona State Board of Nursing Arkansas
HCANJ. 44 th Annual 20-Hour Symposium March 16, 2016 FIVE-STAR RATING SYSTEM & QUALITY MEASURES
 HCANJ 44 th Annual 20-Hour Symposium March 16, 2016 FIVE-STAR RATING SYSTEM & QUALITY MEASURES NELIA ADACI RNC, BSN, CDONA, C-NE, RAC-CT VICE PRESIDENT, The CHARTS Group LEARNING OBJECTIVES: CURRENT 5-STAR
HCANJ 44 th Annual 20-Hour Symposium March 16, 2016 FIVE-STAR RATING SYSTEM & QUALITY MEASURES NELIA ADACI RNC, BSN, CDONA, C-NE, RAC-CT VICE PRESIDENT, The CHARTS Group LEARNING OBJECTIVES: CURRENT 5-STAR
NOTICE OF PROTECTION PROVIDED BY [STATE] LIFE AND HEALTH INSURANCE GUARANTY ASSOCIATION
![NOTICE OF PROTECTION PROVIDED BY [STATE] LIFE AND HEALTH INSURANCE GUARANTY ASSOCIATION](/thumbs/25/5402451.jpg "NOTICE OF PROTECTION PROVIDED BY [STATE] LIFE AND HEALTH INSURANCE GUARANTY ASSOCIATION") NOTICE OF PROTECTION PROVIDED BY This notice provides a brief summary of the [STATE] Life and Health Insurance Guaranty Association (the Association) and the protection it provides for policyholders. This
NOTICE OF PROTECTION PROVIDED BY This notice provides a brief summary of the [STATE] Life and Health Insurance Guaranty Association (the Association) and the protection it provides for policyholders. This
Impacts of Sequestration on the States
 Impacts of Sequestration on the States Alabama Alabama will lose about $230,000 in Justice Assistance Grants that support law STOP Violence Against Women Program: Alabama could lose up to $102,000 in funds
Impacts of Sequestration on the States Alabama Alabama will lose about $230,000 in Justice Assistance Grants that support law STOP Violence Against Women Program: Alabama could lose up to $102,000 in funds
Data show key role for community colleges in 4-year
 Page 1 of 7 (https://www.insidehighered.com) Data show key role for community colleges in 4-year degree production Submitted by Doug Lederman on September 10, 2012-3:00am The notion that community colleges
Page 1 of 7 (https://www.insidehighered.com) Data show key role for community colleges in 4-year degree production Submitted by Doug Lederman on September 10, 2012-3:00am The notion that community colleges
Model Regulation Service January 2006 DISCLOSURE FOR SMALL FACE AMOUNT LIFE INSURANCE POLICIES MODEL ACT
 Table of Contents Section 1. Section 2. Section 3. Section 4. Section 5. Section 6. Section 1. Model Regulation Service January 2006 Purpose Definition Exemptions Disclosure Requirements Insurer Duties
Table of Contents Section 1. Section 2. Section 3. Section 4. Section 5. Section 6. Section 1. Model Regulation Service January 2006 Purpose Definition Exemptions Disclosure Requirements Insurer Duties
Workers Compensation State Guidelines & Availability
 ALABAMA Alabama State Specific Release Form Control\Release Forms_pdf\Alabama 1-2 Weeks ALASKA ARIZONA Arizona State Specific Release Form Control\Release Forms_pdf\Arizona 7-8 Weeks by mail By Mail ARKANSAS
ALABAMA Alabama State Specific Release Form Control\Release Forms_pdf\Alabama 1-2 Weeks ALASKA ARIZONA Arizona State Specific Release Form Control\Release Forms_pdf\Arizona 7-8 Weeks by mail By Mail ARKANSAS
Five Star Rating System Tip Sheet
 Five Star Rating System Tip Sheet In December 2008, The Centers for Medicare & Medicaid Services (CMS) enhanced its Nursing Home Compare public reporting site to include a set of quality ratings for each
Five Star Rating System Tip Sheet In December 2008, The Centers for Medicare & Medicaid Services (CMS) enhanced its Nursing Home Compare public reporting site to include a set of quality ratings for each
Medicaid & CHIP: November Monthly Applications and Eligibility Determinations Report December 20, 2013
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 Medicaid & CHIP: December 20, 2013 Background This
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 Medicaid & CHIP: December 20, 2013 Background This
2014 CAHPS Health Plan Survey Database
 THE CAHPS DATABASE 214 CAHPS Health Plan Survey Database 214 Chartbook: What Consumers Say About Their Experiences with Their Health Plans and Medical Care AHRQ Contract No.: HHSA292133C Managed and prepared
THE CAHPS DATABASE 214 CAHPS Health Plan Survey Database 214 Chartbook: What Consumers Say About Their Experiences with Their Health Plans and Medical Care AHRQ Contract No.: HHSA292133C Managed and prepared
Medicare. If you have any other questions, please feel free to call us at 1-800-MEDICARE (1-800-633-4227). Sincerely,
. Sincerely,") Medicare Beneficiary Services:1-800-MEDICARE (1-800-633-4227) TTY/ TDD:1-877-486-2048 Thank you for your recent request for the Patient s Request for Medical Payment form (CMS-1490S). Enclosed is the form,
Medicare Beneficiary Services:1-800-MEDICARE (1-800-633-4227) TTY/ TDD:1-877-486-2048 Thank you for your recent request for the Patient s Request for Medical Payment form (CMS-1490S). Enclosed is the form,
The Obama Administration and Community Health Centers
 The Obama Administration and Community Health Centers Community health centers are a critical source of health care for millions of Americans particularly those in underserved communities. Thanks primarily
The Obama Administration and Community Health Centers Community health centers are a critical source of health care for millions of Americans particularly those in underserved communities. Thanks primarily
Licensure Resources by State
 Licensure Resources by State Alabama Alabama State Board of Social Work Examiners http://socialwork.alabama.gov/ Alaska Alaska Board of Social Work Examiners http://commerce.state.ak.us/dnn/cbpl/professionallicensing/socialworkexaminers.as
Licensure Resources by State Alabama Alabama State Board of Social Work Examiners http://socialwork.alabama.gov/ Alaska Alaska Board of Social Work Examiners http://commerce.state.ak.us/dnn/cbpl/professionallicensing/socialworkexaminers.as
MAINE (Augusta) Maryland (Annapolis) MICHIGAN (Lansing) MINNESOTA (St. Paul) MISSISSIPPI (Jackson) MISSOURI (Jefferson City) MONTANA (Helena)
 Maryland (Annapolis) MICHIGAN (Lansing) MINNESOTA (St. Paul) MISSISSIPPI (Jackson) MISSOURI (Jefferson City) MONTANA (Helena)") HAWAII () IDAHO () Illinois () MAINE () Maryland () MASSACHUSETTS () NEBRASKA () NEVADA (Carson ) NEW HAMPSHIRE () OHIO () OKLAHOMA ( ) OREGON () TEXAS () UTAH ( ) VERMONT () ALABAMA () COLORADO () INDIANA
HAWAII () IDAHO () Illinois () MAINE () Maryland () MASSACHUSETTS () NEBRASKA () NEVADA (Carson ) NEW HAMPSHIRE () OHIO () OKLAHOMA ( ) OREGON () TEXAS () UTAH ( ) VERMONT () ALABAMA () COLORADO () INDIANA
Census Data on Uninsured Women and Children September 2009
 March of Dimes Foundation Office of Government Affairs 1146 19 th Street, NW, 6 th Floor Washington, DC 20036 Telephone (202) 659-1800 Fax (202) 296-2964 marchofdimes.com nacersano.org Census Data on Uninsured
March of Dimes Foundation Office of Government Affairs 1146 19 th Street, NW, 6 th Floor Washington, DC 20036 Telephone (202) 659-1800 Fax (202) 296-2964 marchofdimes.com nacersano.org Census Data on Uninsured
Medicare may pay for inpatient hospital, doctor, or ambulance services you receive in Canada or Mexico:
 Medicare Beneficiary Services:1-800-MEDICARE (1-800-633-4227) TTY/ TDD:1-877-486-2048 Thank you for your recent request for the Patient s Request for Medical Payment form (CMS-1490S). Enclosed is the form,
Medicare Beneficiary Services:1-800-MEDICARE (1-800-633-4227) TTY/ TDD:1-877-486-2048 Thank you for your recent request for the Patient s Request for Medical Payment form (CMS-1490S). Enclosed is the form,
State by State Summary of Nurses Allowed to Perform Conservative Sharp Debridement
 State by State Summary of Nurses Allowed to Perform Conservative Sharp Debridement THE FOLLOWING ARE ONLY GENERAL SUMMARIES OF THE PRACTICE ACTS EACH STATE HAS REGARDING CONSERVATIVE SHARP DEBRIDEMENT
State by State Summary of Nurses Allowed to Perform Conservative Sharp Debridement THE FOLLOWING ARE ONLY GENERAL SUMMARIES OF THE PRACTICE ACTS EACH STATE HAS REGARDING CONSERVATIVE SHARP DEBRIDEMENT
Note: This Fact Sheet outlines a Proposed Rule. Any of the specifics of this fact sheet could change based on the promulgation of a Final Rule.
 Fact Sheet on Proposed Rule: Medicaid Payment for Services Furnished by Certain Physicians and Charges for Immunization Administration under the Vaccines for Children Program Note: This Fact Sheet outlines
Fact Sheet on Proposed Rule: Medicaid Payment for Services Furnished by Certain Physicians and Charges for Immunization Administration under the Vaccines for Children Program Note: This Fact Sheet outlines
Objectives. Objectives. The Facility Compliance Program Handbook 3/11/2016. Training 1
 Understanding the Five Star Quality Rating System Design For Nursing Home Compare Nathan Shaw RN, BSN, MBA, LHRM, RAC CT 3.0 Director of Clinical Reimbursement March 23rd, 2015 Objectives Objectives Provide
Understanding the Five Star Quality Rating System Design For Nursing Home Compare Nathan Shaw RN, BSN, MBA, LHRM, RAC CT 3.0 Director of Clinical Reimbursement March 23rd, 2015 Objectives Objectives Provide
Therapeutic Shoe and Insert Claim Form Preparation
 Therapeutic Shoe and Insert Claim Form Preparation NOTE: Claims cannot be submitted until AFTER the shoe has been dispensed. Claims for DME supplies cannot be billed paper based or electronic to your regular
Therapeutic Shoe and Insert Claim Form Preparation NOTE: Claims cannot be submitted until AFTER the shoe has been dispensed. Claims for DME supplies cannot be billed paper based or electronic to your regular
2014 INCOME EARNED BY STATE INFORMATION
 BY STATE INFORMATION This information is being provided to assist in your 2014 tax preparations. The information is also mailed to applicable Columbia fund non-corporate shareholders with their year-end
BY STATE INFORMATION This information is being provided to assist in your 2014 tax preparations. The information is also mailed to applicable Columbia fund non-corporate shareholders with their year-end
REPORT OF FINDINGS NURSING FACILITY STAFFING SURVEY 2010
 REPORT OF FINDINGS NURSING FACILITY STAFFING SURVEY 2010 October, 2011 ABSTRACT Approximately 2 million workers were employed at nursing facilities across the United States in 2010. 1.3 million nursing
REPORT OF FINDINGS NURSING FACILITY STAFFING SURVEY 2010 October, 2011 ABSTRACT Approximately 2 million workers were employed at nursing facilities across the United States in 2010. 1.3 million nursing
BUSINESS DEVELOPMENT OUTCOMES
 BUSINESS DEVELOPMENT OUTCOMES Small Business Ownership Description Total number of employer firms and self-employment in the state per 100 people in the labor force, 2003. Explanation Business ownership
BUSINESS DEVELOPMENT OUTCOMES Small Business Ownership Description Total number of employer firms and self-employment in the state per 100 people in the labor force, 2003. Explanation Business ownership
State Specific Annuity Suitability Requirements updated 10/10/11
 Alabama Alaska Ai Arizona Arkansas California This jurisdiction has pending annuity training legislation/regulation Initial 8 Hour Annuity Training Requirement: Prior to selling annuities in California,
Alabama Alaska Ai Arizona Arkansas California This jurisdiction has pending annuity training legislation/regulation Initial 8 Hour Annuity Training Requirement: Prior to selling annuities in California,
State-Specific Annuity Suitability Requirements
 Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware District of Columbia Effective 10/16/11: Producers holding a life line of authority on or before 10/16/11 who sell or wish to sell
Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware District of Columbia Effective 10/16/11: Producers holding a life line of authority on or before 10/16/11 who sell or wish to sell
Net-Temps Job Distribution Network
 Net-Temps Job Distribution Network The Net-Temps Job Distribution Network is a group of 25,000 employment-related websites with a local, regional, national, industry and niche focus. Net-Temps customers'
Net-Temps Job Distribution Network The Net-Temps Job Distribution Network is a group of 25,000 employment-related websites with a local, regional, national, industry and niche focus. Net-Temps customers'
Broadband Availability in America. With Rural Americans Looking for High-Speed Services, Adequate Broadband Speeds Remain Out of Reach for Many
 Broadband Availability in America With Rural Americans Looking for High-Speed Services, Adequate Broadband Speeds Remain Out of Reach for Many Federal Communications Commission January 30, 2015 High-speed
Broadband Availability in America With Rural Americans Looking for High-Speed Services, Adequate Broadband Speeds Remain Out of Reach for Many Federal Communications Commission January 30, 2015 High-speed
PUBLIC HOUSING AUTHORITY COMPENSATION
 PUBLIC HOUSING AUTHORITY COMPENSATION Background After concerns were raised about the level of compensation being paid to some public housing authority (PHA) leaders, in August 2011 HUD reached out to
PUBLIC HOUSING AUTHORITY COMPENSATION Background After concerns were raised about the level of compensation being paid to some public housing authority (PHA) leaders, in August 2011 HUD reached out to
Medicare- Medicaid Enrollee State Profile
 Medicare- Medicaid Enrollee State Profile The National Summary Centers for Medicare & Medicaid Services Introduction... 1 Data Source and General Notes... 2 Types and Ages of Medicare-Medicaid Enrollees...
Medicare- Medicaid Enrollee State Profile The National Summary Centers for Medicare & Medicaid Services Introduction... 1 Data Source and General Notes... 2 Types and Ages of Medicare-Medicaid Enrollees...
Englishinusa.com Positions in MSN under different search terms.
 Englishinusa.com Positions in MSN under different search terms. Search Term Position 1 Accent Reduction Programs in USA 1 2 American English for Business Students 1 3 American English for Graduate Students
Englishinusa.com Positions in MSN under different search terms. Search Term Position 1 Accent Reduction Programs in USA 1 2 American English for Business Students 1 3 American English for Graduate Students
STATE-SPECIFIC ANNUITY SUITABILITY REQUIREMENTS
 Alabama Alaska Arizona Arkansas California This jurisdiction has pending annuity training legislation/regulation Annuity Training Requirement Currently Effective Initial 8-Hour Annuity Training Requirement:
Alabama Alaska Arizona Arkansas California This jurisdiction has pending annuity training legislation/regulation Annuity Training Requirement Currently Effective Initial 8-Hour Annuity Training Requirement:
STATISTICAL BRIEF #273
 STATISTICAL BRIEF #273 December 29 Employer-Sponsored Health Insurance for Employees of State and Local Governments, by Census Division, 28 Beth Levin Crimmel, M.S. Introduction Employees of state and
STATISTICAL BRIEF #273 December 29 Employer-Sponsored Health Insurance for Employees of State and Local Governments, by Census Division, 28 Beth Levin Crimmel, M.S. Introduction Employees of state and
Understanding CMS 5-Star Rating System
 Understanding CMS 5-Star Rating System Michelle M. Pandolfi, LMSW, MBA, LNHA, PMP Director, Consulting Services Qualidigm This material was prepared by the New England Quality Innovation Network-Quality
Understanding CMS 5-Star Rating System Michelle M. Pandolfi, LMSW, MBA, LNHA, PMP Director, Consulting Services Qualidigm This material was prepared by the New England Quality Innovation Network-Quality
Peer Coaching: Leaders of Change
 Peer Coaching: Leaders of Change Part 3 Understanding CASPER Reports Disclaimer Nursing homes should always use: Resident Assessment Instrument User s Manual (RAI) MDS30Q 3.0 Quality Measures User s Manual
Peer Coaching: Leaders of Change Part 3 Understanding CASPER Reports Disclaimer Nursing homes should always use: Resident Assessment Instrument User s Manual (RAI) MDS30Q 3.0 Quality Measures User s Manual
Reading the Stars: Nursing Home Quality Star Ratings, Nationally and by State
 Reading the Stars: Nursing Home Quality Star Ratings, Nationally and by State Cristina Boccuti, Giselle Casillas, Tricia Neuman About 1.3 million people receive care each day in over 15,500 nursing homes
Reading the Stars: Nursing Home Quality Star Ratings, Nationally and by State Cristina Boccuti, Giselle Casillas, Tricia Neuman About 1.3 million people receive care each day in over 15,500 nursing homes
Real Progress in Food Code Adoption
 Real Progress in Food Code Adoption August 27, 2013 The Association of Food and Drug Officials (AFDO), under contract to the Food and Drug Administration, is gathering data on the progress of FDA Food
Real Progress in Food Code Adoption August 27, 2013 The Association of Food and Drug Officials (AFDO), under contract to the Food and Drug Administration, is gathering data on the progress of FDA Food
NAIC ANNUITY TRAINING Regulations By State
 Select a state below to display the current regulation and requirements, or continue to scroll down. Light grey text signifies states that have not adopted an annuity training program. Alabama Illinois
Select a state below to display the current regulation and requirements, or continue to scroll down. Light grey text signifies states that have not adopted an annuity training program. Alabama Illinois
(In effect as of January 1, 2004*) TABLE 5a. MEDICAL BENEFITS PROVIDED BY WORKERS' COMPENSATION STATUTES FECA LHWCA
 TABLE 5a. MEDICAL BENEFITS PROVIDED BY WORKERS' COMPENSATION STATUTES FECA LHWCA") (In effect as of January 1, 2004*) TABLE 5a. MEDICAL BENEFITS PROVIDED BY WORKERS' COMPENSATION STATUTES Full Medical Benefits** Alabama Indiana Nebraska South Carolina Alaska Iowa Nevada South Dakota
(In effect as of January 1, 2004*) TABLE 5a. MEDICAL BENEFITS PROVIDED BY WORKERS' COMPENSATION STATUTES Full Medical Benefits** Alabama Indiana Nebraska South Carolina Alaska Iowa Nevada South Dakota
United States Department of Justice Executive Office for United States Trustees. Public Report:
 United States Department of Justice Executive Office for United States Trustees Public Report: Debtor Audits by the United States Trustee Program Fiscal Year 2014 (As required by Section 603(a)(2)(D) of
United States Department of Justice Executive Office for United States Trustees Public Report: Debtor Audits by the United States Trustee Program Fiscal Year 2014 (As required by Section 603(a)(2)(D) of
REPORT OF FINDINGS 2008 NURSING FACILITY STAFF VACANCY, RETENTION AND TURNOVER SURVEY
 REPORT OF FINDINGS 2008 NURSING FACILITY STAFF VACANCY, RETENTION AND TURNOVER SURVEY American Health Care Association Department of Research October, 2010 ABSTRACT Approximately 2 million workers were
REPORT OF FINDINGS 2008 NURSING FACILITY STAFF VACANCY, RETENTION AND TURNOVER SURVEY American Health Care Association Department of Research October, 2010 ABSTRACT Approximately 2 million workers were
Recruitment and Retention Resources By State List
 Recruitment and Retention Resources By State List Alabama $5,000 rural physician tax credit o http://codes.lp.findlaw.com/alcode/40/18/4a/40-18-132 o http://adph.org/ruralhealth/index.asp?id=882 Area Health
Recruitment and Retention Resources By State List Alabama $5,000 rural physician tax credit o http://codes.lp.findlaw.com/alcode/40/18/4a/40-18-132 o http://adph.org/ruralhealth/index.asp?id=882 Area Health
How To Get A National Rac (And Mac)
") 7 th National RAC (and MAC) Summit December 5 6, 2012 Washington, DC Jane Snecinski P.O. Box 12078 Atlanta, GA 30355 www.postacuteadvisors.com National client base (both public and private sector) based
7 th National RAC (and MAC) Summit December 5 6, 2012 Washington, DC Jane Snecinski P.O. Box 12078 Atlanta, GA 30355 www.postacuteadvisors.com National client base (both public and private sector) based
********************
 THE SURETY & FIDELITY ASSOCIATION OF AMERICA 1101 Connecticut Avenue, N.W., Suite 800 Washington, D. C. 20036 Phone: (202) 463-0600 Fax: (202) 463-0606 Web page: www.surety.org APPLICATION Application
THE SURETY & FIDELITY ASSOCIATION OF AMERICA 1101 Connecticut Avenue, N.W., Suite 800 Washington, D. C. 20036 Phone: (202) 463-0600 Fax: (202) 463-0606 Web page: www.surety.org APPLICATION Application
High Risk Health Pools and Plans by State
 High Risk Health Pools and Plans by State State Program Contact Alabama Alabama Health 1-866-833-3375 Insurance Plan 1-334-263-8311 http://www.alseib.org/healthinsurance/ahip/ Alaska Alaska Comprehensive
High Risk Health Pools and Plans by State State Program Contact Alabama Alabama Health 1-866-833-3375 Insurance Plan 1-334-263-8311 http://www.alseib.org/healthinsurance/ahip/ Alaska Alaska Comprehensive
TO: FROM: DATE: RE: Mid-Year Updates Note: NCQA Benchmarks & Thresholds 2014
 TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: July 25, 2014 RE: 2014 Accreditation Benchmarks and Thresholds Mid-Year Update This document reports national benchmarks
TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: July 25, 2014 RE: 2014 Accreditation Benchmarks and Thresholds Mid-Year Update This document reports national benchmarks
Full Medical Benefits**
 (In effect as of January 1, 2006*) TABLE 5a. MEDICAL BENEFITS PROVIDED BY WORKERS' COMPENSATION STATUTES Full Medical Benefits** Alabama Indiana Nebraska South Carolina Alaska Iowa Nevada South Dakota
(In effect as of January 1, 2006*) TABLE 5a. MEDICAL BENEFITS PROVIDED BY WORKERS' COMPENSATION STATUTES Full Medical Benefits** Alabama Indiana Nebraska South Carolina Alaska Iowa Nevada South Dakota
CMS Payment Policies (By State)
") CMS Payment Policies (By State) To date, IAC is aware of the following states that have adopted CMS reimbursement directives. There are several states in which the Medicare carrier requires or recommends
CMS Payment Policies (By State) To date, IAC is aware of the following states that have adopted CMS reimbursement directives. There are several states in which the Medicare carrier requires or recommends
$7.5 appropriation $6.5 2011 2012 2013 2014 2015 2016. Preschool Development Grants
 School Readiness: High-Quality Early Learning Head Start $10.5 $9.5 $10.1 +$1.5 +17.7% $8.5 $7.5 +$2.1 +27.0% $6.5 for fiscal year 2010 Included in the budget is $1.078 billion to ensure that every Head
School Readiness: High-Quality Early Learning Head Start $10.5 $9.5 $10.1 +$1.5 +17.7% $8.5 $7.5 +$2.1 +27.0% $6.5 for fiscal year 2010 Included in the budget is $1.078 billion to ensure that every Head
Learning Objectives 4/19/2016. The Five-Star Ratings Have Changed IMPROVING YOUR CMS FIVE-STAR QUALITY RATING KAY HASHAGEN, PT, MBA, RAC-CT
 IMPROVING YOUR CMS FIVE-STAR QUALITY RATING KAY HASHAGEN, PT, MBA, RAC-CT Learning Objectives How to analyze the current Star Rating in each area Evaluate current operations to determine the most critical
IMPROVING YOUR CMS FIVE-STAR QUALITY RATING KAY HASHAGEN, PT, MBA, RAC-CT Learning Objectives How to analyze the current Star Rating in each area Evaluate current operations to determine the most critical
Nurse Aide Training Requirements, 2011
 Nurse Aide Training Requirements, 2011 Background Federal legislation (Omnibus Budget Reconciliation Act of 1987) and associated regulations (42 CFR 483.152) require that Medicare- and Medicaid-certified
Nurse Aide Training Requirements, 2011 Background Federal legislation (Omnibus Budget Reconciliation Act of 1987) and associated regulations (42 CFR 483.152) require that Medicare- and Medicaid-certified
Question by: Karon Beyer. Date: March 28, 2012. [LLC Question] [2012-03-29]
![Question by: Karon Beyer. Date: March 28, 2012. [LLC Question] [2012-03-29]](/thumbs/39/18786001.jpg "Question by: Karon Beyer. Date: March 28, 2012. [LLC Question] [2012-03-29]") Topic: LLC Question Question by: Karon Beyer : Florida Date: March 28, 2012 Manitoba Corporations Canada Alabama Alaska Arizona Arkansas California Colorado Arizona uses "manager" or "member," but not
Topic: LLC Question Question by: Karon Beyer : Florida Date: March 28, 2012 Manitoba Corporations Canada Alabama Alaska Arizona Arkansas California Colorado Arizona uses "manager" or "member," but not
Impact of the House Full-Year Continuing Resolution for FY 2011 (H.R. 1)
") U.S. DEPARTMENT OF EDUCATION DISCRETIONARY PROGRAMS Impact of the House Full-Year Continuing Resolution for (H.R. 1) Students Impacted* Job Losses Elementary & Secondary Education Programs Grants to Local
U.S. DEPARTMENT OF EDUCATION DISCRETIONARY PROGRAMS Impact of the House Full-Year Continuing Resolution for (H.R. 1) Students Impacted* Job Losses Elementary & Secondary Education Programs Grants to Local
Schedule B DS1 & DS3 Service
 Schedule B DS1 & DS3 Service SCHEDULE B Private Line Data Services DS1 & DS3 Service... 2 DS-1 Local Access Channel... 2 DS-1 Local Access Channel, New Jersey... 2 DS-1 Local Access Channel, Out-of-State...
Schedule B DS1 & DS3 Service SCHEDULE B Private Line Data Services DS1 & DS3 Service... 2 DS-1 Local Access Channel... 2 DS-1 Local Access Channel, New Jersey... 2 DS-1 Local Access Channel, Out-of-State...
Medical Industry Leadership Institute. Carlson School of Management. What Changes will Health Reform Bring to Medicare Advantage
 Medical Industry Leadership Institute Carlson School of Management What Changes will Health Reform Bring to Medicare Advantage Plan Benefits and Enrollment? WORKING PAPER SERIES Robert A. Book Senior Research
Medical Industry Leadership Institute Carlson School of Management What Changes will Health Reform Bring to Medicare Advantage Plan Benefits and Enrollment? WORKING PAPER SERIES Robert A. Book Senior Research
GOVERNMENT-FINANCED EMPLOYMENT AND THE REAL PRIVATE SECTOR IN THE 50 STATES
 GOVERNMENT-FINANCED EMPLOYMENT AND THE REAL PRIVATE SECTOR IN THE 50 STATES BY KEITH HALL AND ROBERT GREENE November 25, 2013 www.mercatus.org 0.7 2.4 4.2 FEDERAL CONTRACT FUNDED PRIVATE-SECTOR JOBS AS
GOVERNMENT-FINANCED EMPLOYMENT AND THE REAL PRIVATE SECTOR IN THE 50 STATES BY KEITH HALL AND ROBERT GREENE November 25, 2013 www.mercatus.org 0.7 2.4 4.2 FEDERAL CONTRACT FUNDED PRIVATE-SECTOR JOBS AS
State Tax Information
 State Tax Information The information contained in this document is not intended or written as specific legal or tax advice and may not be relied on for purposes of avoiding any state tax penalties. Neither
State Tax Information The information contained in this document is not intended or written as specific legal or tax advice and may not be relied on for purposes of avoiding any state tax penalties. Neither
A-79. Appendix A Overview and Detailed Tables
 Table A-8a. Overview: Laws Expressly Granting Minors the Right to Consent Disclosure of Related Information to Parents* Sexually Transmitted Disease and HIV/AIDS** Treatment Given or Needed Alabama 14
Table A-8a. Overview: Laws Expressly Granting Minors the Right to Consent Disclosure of Related Information to Parents* Sexually Transmitted Disease and HIV/AIDS** Treatment Given or Needed Alabama 14
NAIC Annuity Suitability Requirements by State
 NAIC Annuity Suitability Requirements by Specific Alabama Alaska 10/16/2011 TBD Arizona Arkansas If you obtained a life insurance license prior to 10/16/11, you must complete the NAIC course by 4/16/12.
NAIC Annuity Suitability Requirements by Specific Alabama Alaska 10/16/2011 TBD Arizona Arkansas If you obtained a life insurance license prior to 10/16/11, you must complete the NAIC course by 4/16/12.
IRS Request for Assistance re New EIN and True Owner. Question by: Sarah Steinbeck on behalf of Leslie Reynolds. Date: 5 August 2010
 Topic: IRS Request for Assistance re New EIN and True Owner Question by: Sarah Steinbeck on behalf of Leslie Reynolds Jurisdiction: Colorado/NASS Date: 5 August 2010 Jurisdiction Question(s) Have you spoken
Topic: IRS Request for Assistance re New EIN and True Owner Question by: Sarah Steinbeck on behalf of Leslie Reynolds Jurisdiction: Colorado/NASS Date: 5 August 2010 Jurisdiction Question(s) Have you spoken
STATE DATA CENTER. District of Columbia MONTHLY BRIEF
 District of Columbia STATE DATA CENTER MONTHLY BRIEF N o v e m b e r 2 0 1 2 District Residents Health Insurance Coverage 2000-2010 By Minwuyelet Azimeraw Joy Phillips, Ph.D. This report is based on data
District of Columbia STATE DATA CENTER MONTHLY BRIEF N o v e m b e r 2 0 1 2 District Residents Health Insurance Coverage 2000-2010 By Minwuyelet Azimeraw Joy Phillips, Ph.D. This report is based on data
Nurse Aide Training Requirements, October 2014
 Nurse Aide Training Requirements, October 2014 Background Federal legislation (Omnibus Budget Reconciliation Act of 1987) and associated regulations (42 CFR 483.152) require that Medicare- and Medicaid-certified
Nurse Aide Training Requirements, October 2014 Background Federal legislation (Omnibus Budget Reconciliation Act of 1987) and associated regulations (42 CFR 483.152) require that Medicare- and Medicaid-certified
What to Know About State CPA Reciprocity Rules. John Gillett, PhD, CPA Chair, Department of Accounting Bradley University, Peoria, IL
 What to Know About State CPA Reciprocity Rules Paul Swanson, MBA, CPA Instructor of Accounting John Gillett, PhD, CPA Chair, Department of Accounting Kevin Berry, PhD, Assistant Professor of Accounting
What to Know About State CPA Reciprocity Rules Paul Swanson, MBA, CPA Instructor of Accounting John Gillett, PhD, CPA Chair, Department of Accounting Kevin Berry, PhD, Assistant Professor of Accounting
Facing Cost-Sensitive Shoppers, Health Plan Providers Must Demonstrate Value
 w Reports: Health Insurance Marketplace Exchange Enrollment Satisfaction Improves Significantly in Second Year Facing Cost-Sensitive Shoppers, Health Plan Providers Must Demonstrate Value WESTLAKE VILLAGE,
w Reports: Health Insurance Marketplace Exchange Enrollment Satisfaction Improves Significantly in Second Year Facing Cost-Sensitive Shoppers, Health Plan Providers Must Demonstrate Value WESTLAKE VILLAGE,
Consent to Appointment as Registered Agent
 Consent to Appointment as Registered Agent This form is used by the person or business entity that agrees to act as the registered agent for a limited liability company. Every person or business entity
Consent to Appointment as Registered Agent This form is used by the person or business entity that agrees to act as the registered agent for a limited liability company. Every person or business entity
SECTION 109 HOST STATE LOAN-TO-DEPOSIT RATIOS. or branches outside of its home state primarily for the purpose of deposit production.
 SECTION 109 HOST STATE LOAN-TO-DEPOSIT RATIOS The Board of Governors of the Federal Reserve System, the Federal Deposit Insurance Corporation, and the Office of the Comptroller of the Currency (the agencies)
SECTION 109 HOST STATE LOAN-TO-DEPOSIT RATIOS The Board of Governors of the Federal Reserve System, the Federal Deposit Insurance Corporation, and the Office of the Comptroller of the Currency (the agencies)
NAIC Annuity Suitability Requirements by State
 NAIC Annuity Suitability Requirements by Specific Alabama Alaska 10/16/2011 TBD Arizona Arkansas If you obtained a life insurance license prior to 10/16/11, you must complete the NAIC course by 4/16/12.
NAIC Annuity Suitability Requirements by Specific Alabama Alaska 10/16/2011 TBD Arizona Arkansas If you obtained a life insurance license prior to 10/16/11, you must complete the NAIC course by 4/16/12.
State Pest Control/Pesticide Application Laws & Regulations. As Compiled by NPMA, as of December 2011
 State Pest Control/Pesticide Application Laws & As Compiled by NPMA, as of December 2011 Alabama http://alabamaadministrativecode.state.al.us/docs/agr/mcword10agr9.pdf Alabama Pest Control Alaska http://dec.alaska.gov/commish/regulations/pdfs/18%20aac%2090.pdf
State Pest Control/Pesticide Application Laws & As Compiled by NPMA, as of December 2011 Alabama http://alabamaadministrativecode.state.al.us/docs/agr/mcword10agr9.pdf Alabama Pest Control Alaska http://dec.alaska.gov/commish/regulations/pdfs/18%20aac%2090.pdf
Research Brief. Gap in Dental Care Utilization Between Medicaid and Privately Insured Children Narrows, Remains Large for Adults.
 Gap in Dental Care Utilization Between Medicaid and Privately Insured Children Narrows, Remains Large for Adults Authors: Marko Vujicic, Ph.D.; Kamyar Nasseh, Ph.D. The Health Policy Institute (HPI) is
Gap in Dental Care Utilization Between Medicaid and Privately Insured Children Narrows, Remains Large for Adults Authors: Marko Vujicic, Ph.D.; Kamyar Nasseh, Ph.D. The Health Policy Institute (HPI) is
Healthcare. State Report. Anthony P. Carnevale Nicole Smith Artem Gulish Bennett H. Beach. June 2012
 Healthcare State Report June 2012 Anthony P. Carnevale Nicole Smith Artem Gulish Bennett H. Beach B Table of Contents Healthcare: State Level Analysis... 3 Alabama... 12 Alaska... 14 Arizona... 16 Arkansas...
Healthcare State Report June 2012 Anthony P. Carnevale Nicole Smith Artem Gulish Bennett H. Beach B Table of Contents Healthcare: State Level Analysis... 3 Alabama... 12 Alaska... 14 Arizona... 16 Arkansas...
OPT Extension Application Process 11/22/2010
 OPT Extension Application Process 11/22/2010 Step One: Request an I-20 recommending OPT Extension from Designated School Officer (DSO) (Pi-Shin pishin@npu.edu or Bill wjw@npu.edu or Jessie jessie@npu.edu)
OPT Extension Application Process 11/22/2010 Step One: Request an I-20 recommending OPT Extension from Designated School Officer (DSO) (Pi-Shin pishin@npu.edu or Bill wjw@npu.edu or Jessie jessie@npu.edu)
Subject: Military Personnel Strengths in the Army National Guard
 United States General Accounting Office Washington, DC 20548 March 20, 2002 The Honorable John McHugh Chairman The Honorable Vic Snyder Ranking Member Military Personnel Subcommittee Committee on Armed
United States General Accounting Office Washington, DC 20548 March 20, 2002 The Honorable John McHugh Chairman The Honorable Vic Snyder Ranking Member Military Personnel Subcommittee Committee on Armed
Annual Rate of Serious Disciplinary Actions by State Medical Boards: 2000-2011
 Public Citizen s Health Research Group Ranking of the Rate of State Medical Boards Serious Disciplinary Actions, 2009-2011 May 17, 2012 Sidney M. Wolfe, M.D., Cynthia Williams, Alex Zaslow Using an analysis
Public Citizen s Health Research Group Ranking of the Rate of State Medical Boards Serious Disciplinary Actions, 2009-2011 May 17, 2012 Sidney M. Wolfe, M.D., Cynthia Williams, Alex Zaslow Using an analysis
Prepared by : Michael R. Fowlkes CBP / Fraudulent Document Officer San Ysidro Port of Entry 720 E. San Ysidro Blvd. San Ysidro, CA 92173 (619)
") Prepared by : Michael R. Fowlkes CBP / Fraudulent Document Officer San Ysidro Port of Entry 720 E. San Ysidro Blvd. San Ysidro, CA 92173 (619) 662-7342 Social Security Facts: The Social Security act was
Prepared by : Michael R. Fowlkes CBP / Fraudulent Document Officer San Ysidro Port of Entry 720 E. San Ysidro Blvd. San Ysidro, CA 92173 (619) 662-7342 Social Security Facts: The Social Security act was
Medicare Advantage Plan Landscape Data Summary
 Medicare Advantage Plan Landscape Data Summary Table of Contents Report Overview............................................ 3 Methodology............................................... 6 Medicare Advantage
Medicare Advantage Plan Landscape Data Summary Table of Contents Report Overview............................................ 3 Methodology............................................... 6 Medicare Advantage
Center for Medicaid, CHIP, and Survey & Certification/Survey & Certification Group. Memorandum Summary
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2 12 25 Baltimore, Maryland 21244 1850 Center for Medicaid, CHIP, and Survey & Certification/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2 12 25 Baltimore, Maryland 21244 1850 Center for Medicaid, CHIP, and Survey & Certification/Survey
Medicare Advantage Cuts in the Affordable Care Act: March 2013 Update Robert A. Book l March 2013
 Medicare Advantage Cuts in the Affordable Care Act: March 2013 Update Robert A. Book l March 2013 The Centers for Medicare and Medicaid Services (CMS) recently announced proposed rules that would cut payments
Medicare Advantage Cuts in the Affordable Care Act: March 2013 Update Robert A. Book l March 2013 The Centers for Medicare and Medicaid Services (CMS) recently announced proposed rules that would cut payments
PROVIDERS TERMINATED FROM ONE STATE MEDICAID PROGRAM CONTINUED PARTICIPATING IN OTHER STATES
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL PROVIDERS TERMINATED FROM ONE STATE MEDICAID PROGRAM CONTINUED PARTICIPATING IN OTHER STATES Suzanne Murrin Deputy Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL PROVIDERS TERMINATED FROM ONE STATE MEDICAID PROGRAM CONTINUED PARTICIPATING IN OTHER STATES Suzanne Murrin Deputy Inspector General
Summary of Laws Regarding International Adoptions Finalized Abroad 50 States and 6 U.S. Territories
 Summary of Laws Regarding International Adoptions Finalized Abroad 50 States and 6 U.S. Territories (7/01) Effect of Foreign Adoption Decree Twenty-five States and one territory (Commonwealth of the Northern
Summary of Laws Regarding International Adoptions Finalized Abroad 50 States and 6 U.S. Territories (7/01) Effect of Foreign Adoption Decree Twenty-five States and one territory (Commonwealth of the Northern
Medicaid Topics Impact of Medicare Dual Eligibles Stephen Wilhide, Consultant
 Medicaid Topics Impact of Medicare Dual Eligibles Stephen Wilhide, Consultant Issue Summary The term dual eligible refers to the almost 7.5 milion low-income older individuals or younger persons with disabilities
Medicaid Topics Impact of Medicare Dual Eligibles Stephen Wilhide, Consultant Issue Summary The term dual eligible refers to the almost 7.5 milion low-income older individuals or younger persons with disabilities
STATISTICAL BRIEF #435
 STATISTICAL BRIEF #435 April 2014 Premiums and Employee Contributions for Employer-Sponsored Health Insurance: Private versus Public Sector, 2012 Karen E. Davis, MA Introduction Employer-sponsored health
STATISTICAL BRIEF #435 April 2014 Premiums and Employee Contributions for Employer-Sponsored Health Insurance: Private versus Public Sector, 2012 Karen E. Davis, MA Introduction Employer-sponsored health
US Department of Health and Human Services Exclusion Program. Thomas Sowinski Special Agent in Charge/ Reviewing Official
 US Department of Health and Human Services Exclusion Program Thomas Sowinski Special Agent in Charge/ Reviewing Official Overview Authority to exclude individuals and entities from Federal Health Care
US Department of Health and Human Services Exclusion Program Thomas Sowinski Special Agent in Charge/ Reviewing Official Overview Authority to exclude individuals and entities from Federal Health Care
SECTION 109 HOST STATE LOAN-TO-DEPOSIT RATIOS. The Board of Governors of the Federal Reserve System (Board), the Federal Deposit
, the Federal Deposit") SECTION 109 HOST STATE LOAN-TO-DEPOSIT RATIOS The Board of Governors of the Federal Reserve System (Board), the Federal Deposit Insurance Corporation (FDIC), and the Office of the Comptroller of the Currency
SECTION 109 HOST STATE LOAN-TO-DEPOSIT RATIOS The Board of Governors of the Federal Reserve System (Board), the Federal Deposit Insurance Corporation (FDIC), and the Office of the Comptroller of the Currency
Outpatient dialysis services
 O n l i n e A p p e n d i x e s 6 Outpatient dialysis services 6-A O n l i n e A p p e n d i x Medicare spending by dialysis beneficiaries is substantial FIGURE 1-3 Figure 6 A1 Medicare population Dialysis
O n l i n e A p p e n d i x e s 6 Outpatient dialysis services 6-A O n l i n e A p p e n d i x Medicare spending by dialysis beneficiaries is substantial FIGURE 1-3 Figure 6 A1 Medicare population Dialysis
14-Sep-15 State and Local Tax Deduction by State, Tax Year 2013
 14-Sep-15 State and Local Tax Deduction by State, Tax Year 2013 (millions) deduction in state dollars) claimed (dollars) taxes paid [1] state AGI United States 44.2 100.0 30.2 507.7 100.0 11,483 100.0
14-Sep-15 State and Local Tax Deduction by State, Tax Year 2013 (millions) deduction in state dollars) claimed (dollars) taxes paid [1] state AGI United States 44.2 100.0 30.2 507.7 100.0 11,483 100.0
State Individual Income Taxes: Treatment of Select Itemized Deductions, 2006
 State Individual Income Taxes: Treatment of Select Itemized Deductions, 2006 State Federal Income Tax State General Sales Tax State Personal Property Tax Interest Expenses Medical Expenses Charitable Contributions
State Individual Income Taxes: Treatment of Select Itemized Deductions, 2006 State Federal Income Tax State General Sales Tax State Personal Property Tax Interest Expenses Medical Expenses Charitable Contributions
Employment and Earnings of Registered Nurses in 2010
 Employment and Earnings of Registered Nurses in 2010 Thursday, May 25, 2011 The Bureau of Labor Statistics (BLS) released 2010 occupational employment data on May 17, 2011. This document provides several
Employment and Earnings of Registered Nurses in 2010 Thursday, May 25, 2011 The Bureau of Labor Statistics (BLS) released 2010 occupational employment data on May 17, 2011. This document provides several
Question for the filing office of Texas, Re: the Texas LLC act. Professor Daniel S. Kleinberger. William Mitchell College of Law, Minnesota
 Topic: Question by: : Question for the filing office of Texas, Re: the Texas LLC act Professor Daniel S. Kleinberger William Mitchell College of Law, Minnesota Date: March 18, 2012 Manitoba Corporations
Topic: Question by: : Question for the filing office of Texas, Re: the Texas LLC act Professor Daniel S. Kleinberger William Mitchell College of Law, Minnesota Date: March 18, 2012 Manitoba Corporations
We do require the name and mailing address of each person forming the LLC.
 Topic: LLC Managers/Members Question by: Jeff Harvey : Idaho Date: March 7, 2012 Manitoba Corporations Canada Alabama Alaska Arizona Arkansas California Colorado Arizona requires that member-managed LLCs
Topic: LLC Managers/Members Question by: Jeff Harvey : Idaho Date: March 7, 2012 Manitoba Corporations Canada Alabama Alaska Arizona Arkansas California Colorado Arizona requires that member-managed LLCs
State Agency Name Link to and/or Information about Complaint Process
 Alabama Alabama Alabama Commission on Higher - Office of Institutional Effectiveness and Planning Alabama Department of Postsecondary - Office of Private School Licensing Division Complaints for out of
Alabama Alabama Alabama Commission on Higher - Office of Institutional Effectiveness and Planning Alabama Department of Postsecondary - Office of Private School Licensing Division Complaints for out of
State Insurance Department Websites: A Consumer Assessment
 State Insurance Department Websites: A Consumer Assessment By J. Robert Hunter Director of Insurance November 2008 1 of 10 EXECUTIVE SUMMARY This report analyzes Internet websites for the nation s 51 major
State Insurance Department Websites: A Consumer Assessment By J. Robert Hunter Director of Insurance November 2008 1 of 10 EXECUTIVE SUMMARY This report analyzes Internet websites for the nation s 51 major