CMS Progress Toward Implementing Value-Based Purchasing
|
|
|
- Jean Strickland
- 7 years ago
- Views:
Transcription
1 Centers for Medicare & Medicaid Services CMS Progress Toward Implementing Value-Based Purchasing Thomas B. Valuck, MD, JD Medical Officer & Senior Adviser Center for Medicare Management 1 CMS Quality Improvement Roadmap Vision: The right care for every person every time Make care: Safe Effective Efficient Patient-centered Timely Equitable 2 1

2 CMS Quality Improvement Roadmap Strategies Work through partnerships Measure quality and report comparative results Value-Based Purchasing: improve quality and avoid unnecessary costs Encourage adoption of effective health information technology Promote innovation and the evidence base for effective use of technology 3 VBP Program Goals Improve clinical quality Reduce adverse events and improve patient safety Encourage more patient-centered care Avoid unnecessary costs in the delivery of care Stimulate investments in effective structural components or systems Make performance results transparent and comprehensible To empower consumers to make value-based decisions about their health care To encourage hospitals and clinicians to improve quality of care the quality of care 4 2

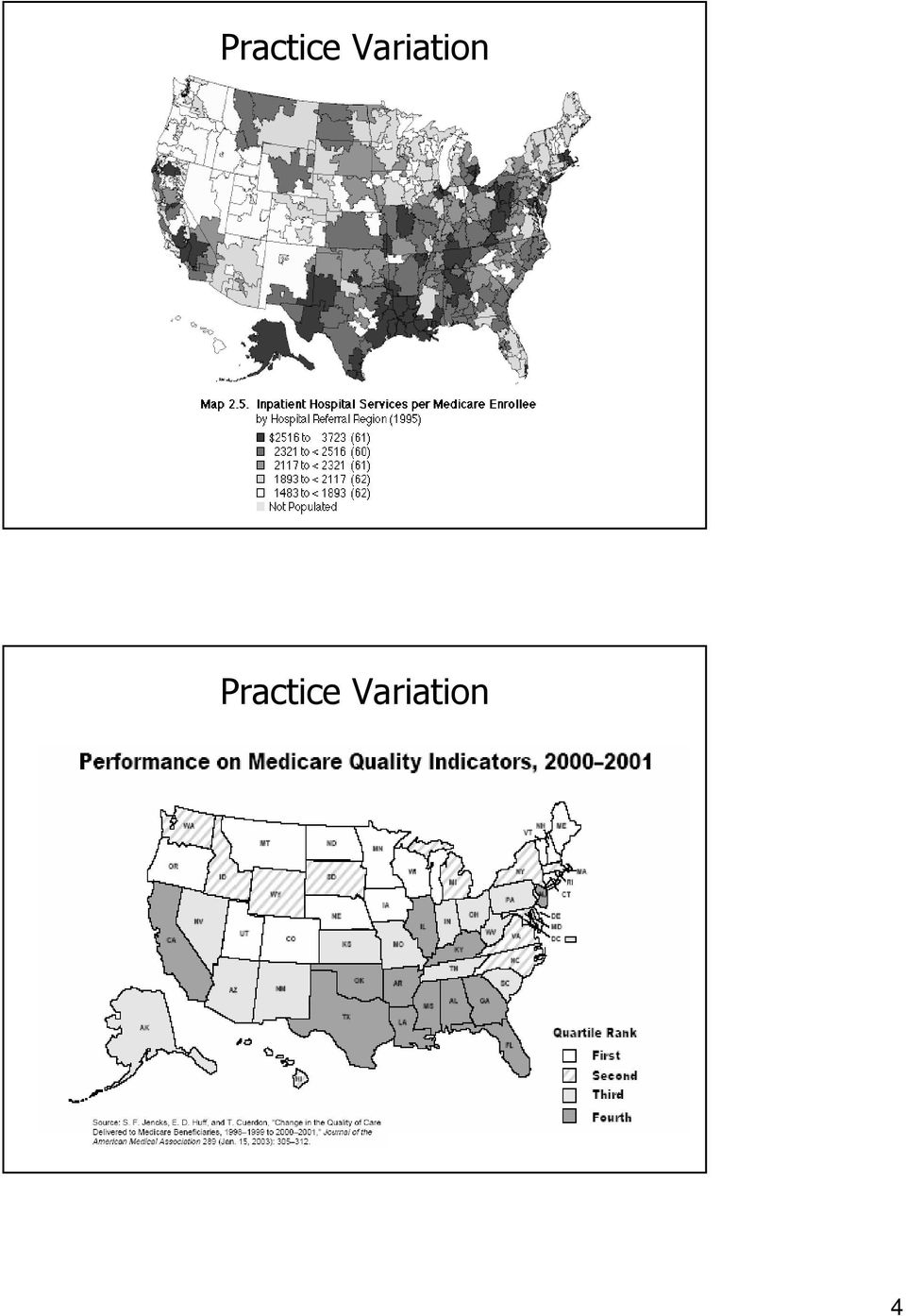
3 What Does VBP Mean to CMS? Transforming Medicare from a passive payer to an active purchaser of higher quality, more efficient health care Tools and initiatives for promoting better quality, while avoiding unnecessary costs Tools: measurement, payment incentives, public reporting, conditions of participation, coverage policy, QIO program Initiatives: pay for reporting, pay for performance, gainsharing, competitive bidding, coverage decisions, direct provider support 5 Why VBP? Improve Quality Quality improvement opportunity Wennberg s Dartmouth Atlas on variation in care McGlynn s NEJM findings on lack of evidence-based care IOM s Crossing the Quality Chasm findings Avoid Unnecessary Costs Medicare s various fee-for-service fee schedules and prospective payment systems are based on resource consumption and quantity of care, NOT quality or unnecessary costs avoided Physician Fee Schedule and Hospital Inpatient DRGs Medicare Trust Fund insolvency looms 6 3

4 Practice Variation Practice Variation 4
5 Support for VBP President s Budget FYs Congressional Interest in P4P and Other Value-Based Purchasing Tools BIPA, MMA, DRA, TRHCA, MMSEA MedPAC Reports to Congress P4P recommendations related to quality, efficiency, health information technology, and payment reform IOM Reports P4P recommendations in To Err Is Human and Crossing the Quality Chasm Report, Rewarding Provider Performance: Aligning Incentives in Medicare Private Sector Private health plans Employer coalitions 10 5

6 VBP Demonstrations and Pilots Premier Hospital Quality Incentive Demonstration Physician Group Practice Demonstration Medicare Care Management Performance Demonstration Nursing Home Value-Based Purchasing Demonstration Home Health Pay-for-Performance Demonstration ESRD Bundled Payment Demonstration ESRD Disease Management Demonstration 11 VBP Demonstrations and Pilots Medicare Health Support Pilots Care Management for High-Cost Beneficiaries Demonstration Medicare Healthcare Quality Demonstration Gainsharing Demonstrations Better Quality Information (BQI) Pilots Electronic Health Records (EHR) Demonstration Medical Home Demonstration 12 6
 Pilots Electronic Health Records (EHR) Demonstration Medical Home")
7 VBP Initiatives Hospital Quality Initiative: Inpatient & Outpatient Hospital VBP Plan & Report to Congress Hospital-Acquired Conditions & Present on Admission Indicator Physician Voluntary Reporting Program Physician Quality Reporting Initiative Physician Resource Use Home Health Care Pay for Reporting Ambulatory Surgical Centers Pay for Reporting Medicaid 13 VBP Initiatives Hospital Value-Based Purchasing 14 7

8 Hospital Quality Initiative MMA Section 501(b) Payment differential of 0.4% for reporting (hospital pay for reporting) FYs Starter set of 10 measures High participation rate (>98%) for small incentive Public reporting through CMS Hospital Compare website 15 Hospital Quality Initiative DRA Section 5001(a) Payment differential of 2% for reporting (hospital P4R) FYs subsequent years Expanded measure set, based on IOM s December 2005 Performance Measures Report Expanded measures publicly reported through CMS Hospital Compare website DRA Section 5001(b) Report for hospital VBP beginning with FY 2009 Report must consider: quality and cost measure development and refinement, data infrastructure, payment methodology, and public reporting 16 8
 Report for hospital VBP beginning with FY 2009 Report must consider:")
9 Hospital VBP Report to Congress The Hospital Value-Based Purchasing Report Congress can be downloaded from the CMS website at: 17 VBP Initiatives Hospital-Acquired Conditions and Present on Admission Indicator Reporting 18 9

10 Value-Based Purchasing and Hospital-Acquired Conditions The Hospital-Acquired Conditions provision is a step toward Medicare VBP for hospitals Strong public support for CMS to pay less for conditions that are acquired during a hospital stay Considerable national press coverage of HAC has prompted dialogue on how to further eliminate healthcare-associated conditions, including infections 19 Statutory Authority: DRA Section 5001(c) Beginning October 1, 2007, hospitals must begin submitting data on their claims for payment indicating whether diagnoses were present on admission (POA) Beginning October 1, 2008, CMS cannot assign a case to a higher DRG based on the occurrence of one of the selected conditions, if that condition was acquired during the hospitalization This provision does not apply to Critical Access Hospitals, Rehabilitation Hospitals, Psychiatric Hospitals, or any other facility not paid under the Medicare Hospital IPPS 20 10

11 Statutory Authority: DRA Section 5001(c) CMS is required to select conditions that are: 1. High cost, high volume, or both 2. Assigned to a higher paying DRG when present as a secondary diagnosis 3. Reasonably prevented through the application of evidence-based guidelines 21 Inpatient Prospective Payment System (IPPS) FY2008 Final Rule Complications, including infections, acquired in the hospital can trigger higher payments: MS-DRGs may split into three different levels of severity, based on complications or comorbidities (no CC, CC, or MCC major complication) The CCs and MCCs generate higher payment The more severe the complicating condition, the higher the payment assigned to that CC or MCC DRG 22 11

12 Questions to Address Burden Incidence, cost, morbidity, and mortality Preventability Guidelines and interventions exist Application can prevent these infections Interpretation of reasonably Measurement Events appropriately detected using ICD-9 codes 23 Hospital-Acquired Conditions Selection of Conditions 24 12

13 IPPS FY 2008 Final Rule Each condition considered was placed in one of three categories: 1. Conditions selected for implementation These conditions will have payment implications beginning in October 1, Conditions being considered during FY2009 IPPS rulemaking These conditions raise one or more implementation or policy issues that need to be resolved before they can be selected. We will work to address these issues and propose to reconsider these conditions during the FY 2009 IPPS rulemaking process. 3. Conditions needing further analysis After exhaustive consideration, we determined that further analysis is required before considering these conditions. 25 HACs Selected for FY 2009 to Date Foreign object retained after surgery Air embolism Blood incompatibility Catheter-associated urinary tract infection Pressure ulcers Vascular catheter-associated infection Surgical site infection mediastinitis after CABG Falls specific trauma codes 26 13

14 HACs Under Consideration for FY 2009 Ventilator-associated pneumonia (VAP) Staphylococcus aureus septicemia Deep vein thrombosis (DVT)/ pulmonary embolism (PE) Methicillin-resistant Staphylococcus aureus (MRSA) Clostridium difficile-associated disease (CDAD) Wrong surgery 27 Present on Admission (POA) CMS Implementation of POA Indicator Reporting 28 14
 Wrong surgery 27 Present on Admission (POA) CMS Implementation of POA")
15 POA Indicator General Requirements Present on admission is defined as present at the time the order for inpatient admission occurs -- conditions that develop during an outpatient encounter, including emergency department, observation, or outpatient surgery, are considered as present on admission. Phased implementation 29 POA Indicator General Requirements POA indicator is assigned to principal diagnosis secondary diagnoses external cause of injury codes (Medicare requires reporting only if E-code is reported as an additional diagnosis) 30 15

16 POA Indicator Reporting Options POA Indicator Options and Definitions Code Y N U W 1 Reason for Code Diagnosis was present at time of inpatient admission. Diagnosis was not present at time of impatient admission. Documentation insufficient to determine if condition was present at the time of inpatient admission. Clinically undetermined. Provider unable to clinically determine whether or not the condition was present at the time of inpatient admission or not. Unreported/Not used. Exempt from POA reporting. This code is equivalent code of a blank on the UB-04, however, it was determined that blanks are undesirable when submitting this data via the 4010A. POA Indicator Reporting Successful Documentation of Present on Admission 32 16

17 The Goal: Successful Documentation A joint effort between the healthcare provider and the coder is essential to achieve complete and accurate documentation, code assignment, and reporting of diagnoses and procedures. ICD-9-CM Official Guidelines for Coding and Reporting 33 Opportunities for HAC & POA Involvement IPPS Rulemaking Proposed rule in April Final rule in August Hospital Listserv Messages Updates to the CMS HAC & POA website Hospital Open Door Forums 34 17

18 HAC & POA Indicator Reporting Further information about HAC & POA indicator reporting is available on the CMS website at: 35 Thank You Thomas B. Valuck, MD, JD Medical Officer & Senior Adviser Center for Medicare Management Centers for Medicare & Medicaid Services 36 18

19 A Master Class in Hospital Reimbursement Compliance Present on Admission and Hospital-Acquired Conditions Thomas Valuck MD, JD Medical Officer and Senior Advisor Centers for Medicare and Medical Services Carol Eyer, RHIA, CHC Senior Manager, Clinical Compliance and Reimbursement Pershing Yoakley & Associates, P.C Moderator: Larry Vernaglia, Foley & Lardner LLP 37 Overview of POA Technical Aspects 38 19

20 Quick Added History POA isn t brand new? New York 1994 California 1996 (fully implemented) Individual state initiatives underway prior to 10/01/07 in Florida through state reporting, as well as Maryland and Massachusetts DRA essentially nationalized POA 39 Official Coding Guidelines POA Section Serves as a supplement to the ICD-9-CM Official Guidelines for Coding and Reporting to facilitate correct POA indicator assignment for each diagnosis and external cause of injury code reported on claim forms (UB-04) Not intended to replace any guidelines as otherwise reflected in the Official Guidelines Not intended to provide guidance on when a condition should be coded 40 20
 Not intended to replace")
21 Official ICD-9-CM CM Coding Guidelines Website Address: pserv/ftpicd9/icdguide07.pdf 41 Refresher on Indicators: POA Indicator Options and Definitions Code Y N U W 1 Reason for Code Diagnosis was present at time of inpatient admission. Diagnosis was not present at time of impatient admission. Documentation insufficient to determine if condition was present at the time of inpatient admission. Clinically undetermined. Provider unable to clinically determine whether or not the condition was present at the time of inpatient admission or not. Unreported/Not used. Exempt from POA reporting. This code is equivalent code of a blank on the UB-04, however, it was determined that blanks are undesirable when submitting this 42 data via the 4010A. Now let s walk through examples of when the Y indicator would be assigned 21
22 When to Assign the Y Indicator Condition is clearly documented by the provider Conditions diagnosed prior to inpatient admission, such as chronic, stable conditions Conditions diagnosed during the admission but clearly present before admission Diagnoses subsequently confirmed following admission are considered POA if at the time of admission they are documented as suspected, possible, rule out, differential diagnosis, or constitute an underlying cause of a symptom that is present at the time of admission (best sources of documentation - ED physician note, admitting physician note or history & physical report) Conditions that develop during outpatient encounter prior to inpatient admission 43 Combination codes Coding Specifics Identify all parts of the combination code as present on admission Ex: Diabetic nephropathy is admitted with uncontrolled diabetes One or more components of the combination code not present on admission Ex: Gastric ulcer that does not start bleeding until after admission Asthma patient develops status asthmaticus after admission Identifies the chronic condition and not the acute exacerbation Ex: Acute exacerbation of CHF 44 POA Indicator Y N Y Y N 22
23 Other Coding Specifics Impending or threatened diagnosis Based on symptoms or clinical findings that were present on admission POA Indicator Y N Based on symptoms or clinical findings that were not present on admission Comparative or contrasting diagnoses Both present, or suspected, at the time of admission Y Y Infection codes that include the causal organism Infection (or signs of the infection) present on admission, even though the culture results may not be known until after admission Ex: Patient admitted with pneumonia and the provider documents pseudomonas as the causal organism a few days later 45 Coding Specifics: E-codesE External cause of injury or poisoning occurred prior to inpatient admission: Ex. Patient fell out of bed at home Patient fell out of bed in emergency room prior to admission External cause of injury or poisoning occurred during inpatient hospitalization Ex. Patient fell out of hospital bed during hospitalization Patient experienced an adverse reaction to a medication administered after inpatient admission POA Indicator Y N 46 23
24 Sources of Chart Documentation ED notes condition(s) diagnosed or worked up H&P condition(s) diagnosed or worked up past medical history, current medications, etc. Progress notes follow-up on diagnosing initial condition new findings of existing conditions Consults for management of other conditions than that needing surgery Nursing admission, OR admission, & pre-anesthesia notes Lab and radiology reports 47 Uniform Billing Claim: Implemented last year through the National Uniform Billing Committee (NUBC); replaced the UB-92. Revised partly due to increased need to examine public health reporting requirements and efforts to establish a national approach on research data (example was the added field/requirement for Present on Admission). POA on the UB
25 POA on the UB-04 A closer look: 67 - Required Principal DX Code & Present on Admission Indicator Positions 1 7 are for the DX code(s); Position 8 (shaded area) are for POA Indicator's) 67 A-Q: Required Other Diagnosis 18 Total Dx s (9 New) Note the Shadowed Fields
26 Key Impact Considerations Documentation evaluation Quality of current physician documentation to provide enough clinical information to correctly assign POA Queries to obtain sufficiently detailed POA data Education of medical staff & support for improved documentation Auditing and monitoring of POA assignment accuracy Coding process & Health Information Management Operations Additional time for POA data assignment/collection Study at Mayo Clinic hospitals in Minnesota = 2 minutes per record Impact to coder productivity and/or staffing Impact DNFB (Discharged but not Final Billed) 51 Key Date Considerations October 1, 2007 IPPS hospitals were required to begin submitting POA information on all primary/secondary diagnoses on Medicare claims* January 1, 2008 CMS began processing POA data and providing feedback regarding POA reporting errors through Remark Codes on the Remittance Advice; hospitals were not subject to returned claims through March 31 st April 1, 2008 (TODAY!!) Claims submitted for payment that do not contain proper POA data will be returned to the provider for correct submission of POA information *Direct Data Entry (DDE) screens could not be updated until January 1, 2008, so hospitals submitting claims via DDE were unable to submit POA until January 1,
27 Compliance Officer Considerations Discuss POA with your HIM/coding professionals and business office to ensure appropriate mechanisms have been implemented Review findings from any internal evaluations performed of POA indicator claims feedback received between January and March 2008 be aware of patterns which may reflect poor documentation patterns or lack of understanding about POA Facilitate corrective action where needed and/or if not addressed elsewhere through department heads Facilitate the monitoring plan to periodically assess accurate POA assignment, or review findings of established monitoring plan Confirm appropriate training is provided with appropriate resources for new coding, finance and billing, and other pertinent staff (and that it s documented!) 53 Compliance Officer Considerations Confirm appropriate training resources are established and have been provided with existing coding, finance and billing, and other pertinent staff (and that it s documented!) Team with HIM/coding to evaluate physician POA education to date and ensure that initial physician education has been provided Reinforce POA with physicians in bite-sized chunks through newsletters, department meetings, summarized reports of audit findings, etc. Incorporate findings from POA accuracy audits into Compliance Committee meetings for the first year and as appropriate thereafter Support internal initiatives related to POA with senior management and HIM/coding to further the importance of appropriate provider documentation to effect accurate POA assignment Ensure that all education, training, procedural and other documentation of POA compliance efforts are documented and appropriately retained for reference 54 27
28 POA Monitoring Efforts Determine if audits have been performed, and if so, review and evaluate findings along with HIM/coding and others involved Or, prepare and audit method to include time frame, record selection process, sample size, indicators, data analysis techniques or tools used, qualifications of individuals performing the audit, how results will be communicated and used, and; report formats for tracking and analyzing audit reports Sample should include inpatient Medicare claims between October 1, 2007 to present Evaluate feedback received through the business office on remittance advices for trends perform further review as indicated Evaluate trends for potential overuse of the U and W POA indicators focus on high risk or problem areas 55 POA Monitoring Efforts Facilitate focused audit of detected U and W overuse trends to evaluate documentation and individualize trends by provider Communicate all pertinent feedback with senior management and medical staff leadership, as well as in medical staff forums as appropriate Establish an organizational data integrity process to remedy POA indicator corrections, or, ensure that the current process is efficient Be sure to include evaluation of any contract coders and ensuring that appropriate POA education has been provided through the vendor or otherwise 56 28
29 Other POA Efforts Establish a process (or evaluate the effectiveness of an existing process) for clinical documentation improvement initiatives Include evaluation of an existing or develop/implement a new query process for inconsistent, missing, conflicting, or unclear documentation, and; a related auditing and monitoring process using audit methodology and tools, along with a process to monitor responses to queries as well as appropriateness of queries Project financial impact by analyzing ICD-9-CM code frequency from the 12 months prior to 10/01/07 for the nine CMS conditions; evaluate potential reimbursement impact of accurate physician documentation and correct POA assignment share internally as appropriate Provide education and training for identified opportunities Develop and implement trending and reporting mechanisms 57 Bottom Line Considerations Payment for the CMS designated conditions (hospital acquired or otherwise not identified as POA) will be adjusted* starting October 1, 2008: Serious preventable event, object left in surgery Serious preventable event, air embolism Serious preventable event, blood incompatibility Catheter-associated urinary tract infection Pressure ulcers (decubitus) Vascular catheter-associated infection Mediastinitis after cardiac artery bypass grafting - surgical site infection Hospital acquired injuries (fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes) * Not assigned to the higher-paying MS-DRG 58 29
30 Bottom Line Considerations Potential lost revenue for missing or inadequate physician documentation of conditions that were clinically present at time of admission Increase in accounts receivables days for returned claims and those resulting delays for needed corrections to POA indicator data (negative cash flow impact) Physician report card impact POA can play a significant role in demonstrating why variations exist 59 CMS POA Fact Sheet Website Address: Cond/Downloads/hac_fact_sheet.pdf 60 30
31 Federal Register August 22, 2007 pg 48168, section VII., Effects of Other Policy Changes Website Address: tion=all&page= Conclusions January to March has been the training wheels period 2008 claims data is now building the repository upon which CMS will draw in part to determine POA success as well as formulate 2009 considerations and beyond Anticipate increased POA awareness with claims return after April 1 st great opportunity for compliance to get involved (if not already)! 62 31
32 Carol Eyer, RHIA, CHC Senior Manager, Clinical Compliance & Reimbursement Pershing Yoakley & Associates Two Ravinia Drive, Suite 200 Atlanta, Georgia (678)
CMS Progress Toward Implementing Value-Based Purchasing
 Centers for Medicare & Medicaid Services CMS Progress Toward Implementing Value-Based Purchasing Thomas B. Valuck, MD, JD Medical Officer & Senior Adviser Center for Medicare Management Presentation Overview
Centers for Medicare & Medicaid Services CMS Progress Toward Implementing Value-Based Purchasing Thomas B. Valuck, MD, JD Medical Officer & Senior Adviser Center for Medicare Management Presentation Overview
CMS Progress Toward Implementing Value-Based Purchasing
 Centers for Medicare & Medicaid Services CMS Progress Toward Implementing Value-Based Purchasing Lisa Grabert, MPH Health Insurance Specialist Hospital & Ambulatory Policy Group Presentation Overview CMS
Centers for Medicare & Medicaid Services CMS Progress Toward Implementing Value-Based Purchasing Lisa Grabert, MPH Health Insurance Specialist Hospital & Ambulatory Policy Group Presentation Overview CMS
Value Based Purchasing: Combining Cost and Quality
 Value Based Purchasing: Combining Cost and Quality Michael T. Rapp, MD, JD, FACEP Director, Quality Measurement and Health Assessment Group Office of Clinical Standards & Quality Centers for Medicare &
Value Based Purchasing: Combining Cost and Quality Michael T. Rapp, MD, JD, FACEP Director, Quality Measurement and Health Assessment Group Office of Clinical Standards & Quality Centers for Medicare &
Medicare Value-Based Purchasing Programs
 By Jane Hyatt Thorpe and Chris Weiser Background Medicare Value-Based Purchasing Programs To improve the quality of health care delivered to Medicare beneficiaries, the Centers for Medicare and Medicaid
By Jane Hyatt Thorpe and Chris Weiser Background Medicare Value-Based Purchasing Programs To improve the quality of health care delivered to Medicare beneficiaries, the Centers for Medicare and Medicaid
Linking Quality to Payment
 Linking Quality to Payment Background Our nation s health care delivery system is undergoing a major transformation as reimbursement moves from a volume-based methodology to one based on value and quality.
Linking Quality to Payment Background Our nation s health care delivery system is undergoing a major transformation as reimbursement moves from a volume-based methodology to one based on value and quality.
HOSPITAL-ACQUIRED CONDITION PAYMENT POLICY
 Health Care Purchaser Toolkit: HOSPITAL-ACQUIRED CONDITION PAYMENT POLICY August 2009 Developed for NBCH by: Developed with support from: www.discernconsulting.com 410-542-4470 Health Care Purchaser Toolkit:
Health Care Purchaser Toolkit: HOSPITAL-ACQUIRED CONDITION PAYMENT POLICY August 2009 Developed for NBCH by: Developed with support from: www.discernconsulting.com 410-542-4470 Health Care Purchaser Toolkit:
NEVER EVENT LISTS ENDORSED BY NATIONAL QUALITY FORUM & MEDICARE
 Never Events : Medicare s and Health Plan s Policies on Providing Payment for Serious and Preventable Hospital Errors BACKGROUND Preventable medical errors are a leading cause of death in the United States
Never Events : Medicare s and Health Plan s Policies on Providing Payment for Serious and Preventable Hospital Errors BACKGROUND Preventable medical errors are a leading cause of death in the United States
CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM
 For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
Thomas B. Valuck, MD, JD. Medical Officer & Senior Adviser Center for Medicare Management
 Thomas B. Valuck, MD, JD Medical Officer & Senior Adviser Center for Medicare Management Presentation Overview CMS Value-Based Purchasing (VBP) CMS/Premier Hospital Quality Incentive Demonstration ( HQID
Thomas B. Valuck, MD, JD Medical Officer & Senior Adviser Center for Medicare Management Presentation Overview CMS Value-Based Purchasing (VBP) CMS/Premier Hospital Quality Incentive Demonstration ( HQID
Cognos Web-based Analytic Tool Overview
 Cognos Web-based Analytic Tool Overview Market, Quality and Physician Data Analysis with Drill-thru Feature Mari Tietze, PhD, RN-BC Director, Nursing Research and Informatics DFWHC ERF 2009 1 UB-04 Source
Cognos Web-based Analytic Tool Overview Market, Quality and Physician Data Analysis with Drill-thru Feature Mari Tietze, PhD, RN-BC Director, Nursing Research and Informatics DFWHC ERF 2009 1 UB-04 Source
How Regulations Affect Coding and Documentation
 How Regulations Affect Coding and Documentation Byline Deborah Neville, RHIA, CCS-P Director Revenue Cycle, Coding and Compliance for Elsevier, Inc. INTRODUCTION Regulations, laws, mandates, and guidelines
How Regulations Affect Coding and Documentation Byline Deborah Neville, RHIA, CCS-P Director Revenue Cycle, Coding and Compliance for Elsevier, Inc. INTRODUCTION Regulations, laws, mandates, and guidelines
Improving Hospital Performance
 Improving Hospital Performance Background AHA View Putting patients first ensuring their care is centered on the individual, rooted in best practices and utilizes the latest evidence-based medicine is
Improving Hospital Performance Background AHA View Putting patients first ensuring their care is centered on the individual, rooted in best practices and utilizes the latest evidence-based medicine is
FY2015 Final Hospital Inpatient Rule Summary
 FY2015 Final Hospital Inpatient Rule Summary Interventional Cardiology (IC) Peripheral Interventions (PI) Rhythm Management (RM) On August 4, 2014, the Centers for Medicare & Medicaid Services (CMS) released
FY2015 Final Hospital Inpatient Rule Summary Interventional Cardiology (IC) Peripheral Interventions (PI) Rhythm Management (RM) On August 4, 2014, the Centers for Medicare & Medicaid Services (CMS) released
Chapter Seven Value-based Purchasing
 Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Chapter Seven Value-based Purchasing Value-based purchasing (VBP) is a pay-for-performance program that affects a significant and growing percentage of Medicare reimbursement for medical providers. It
Contents. Part 1. Billing Instructions for PPCs for Inpatient Hospitals
 Appendix V: Billing Instructions V-1 This appendix describes the billing instructions (PPCs), as they apply to providers. This appendix is subdivided into three parts, listed below. This appendix is also
Appendix V: Billing Instructions V-1 This appendix describes the billing instructions (PPCs), as they apply to providers. This appendix is subdivided into three parts, listed below. This appendix is also
Medicare Long-Term Care Hospital Prospective Payment System
 Medicare Long-Term Care Hospital Prospective Payment System May 5, 2015 Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview, Resources, and Comment Submission On May 17, the Centers for Medicare
Medicare Long-Term Care Hospital Prospective Payment System May 5, 2015 Payment Rule Brief PROPOSED RULE Program Year: FFY 2016 Overview, Resources, and Comment Submission On May 17, the Centers for Medicare
Highlights of the Revised Official ICD-9-CM Guidelines for Coding and Reporting Effective October 1, 2008
 Highlights of the Revised Official ICD-9-CM Guidelines for Coding and Reporting Effective October 1, 2008 Please refer to the complete ICD-9-CM Official Guidelines for Coding and Reporting posted on this
Highlights of the Revised Official ICD-9-CM Guidelines for Coding and Reporting Effective October 1, 2008 Please refer to the complete ICD-9-CM Official Guidelines for Coding and Reporting posted on this
Preventing Readmissions
 Emerging Topics in Healthcare Reform Preventing Readmissions Janssen Pharmaceuticals, Inc. Preventing Readmissions The Patient Protection and Affordable Care Act (ACA) contains several provisions intended
Emerging Topics in Healthcare Reform Preventing Readmissions Janssen Pharmaceuticals, Inc. Preventing Readmissions The Patient Protection and Affordable Care Act (ACA) contains several provisions intended
THE EVOLUTION OF CMS PAYMENT MODELS
 THE EVOLUTION OF CMS PAYMENT MODELS December 3, 2015 Dayton Benway, Principal AGENDA Legislative Background Payment Model Categories Life Cycle The Models LEGISLATIVE BACKGROUND Medicare Modernization
THE EVOLUTION OF CMS PAYMENT MODELS December 3, 2015 Dayton Benway, Principal AGENDA Legislative Background Payment Model Categories Life Cycle The Models LEGISLATIVE BACKGROUND Medicare Modernization
June 10, 2015. Dear Mr. Slavitt:
 1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 10, 2015 Andrew M. Slavitt Acting Administrator Centers for Medicare &
1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 10, 2015 Andrew M. Slavitt Acting Administrator Centers for Medicare &
Fiscal Year 2016 proposed Inpatient and Long-term Care Hospital policy and payment changes (CMS-1632-P)
") Fiscal Year 2016 proposed Inpatient and Long-term Care Hospital policy and payment changes (CMS-1632-P) Date 2015-04-17 Title Fiscal Year 2016 proposed Inpatient and Long-term Care Hospital policy and
Fiscal Year 2016 proposed Inpatient and Long-term Care Hospital policy and payment changes (CMS-1632-P) Date 2015-04-17 Title Fiscal Year 2016 proposed Inpatient and Long-term Care Hospital policy and
Roadmap for Implementing Value Driven Healthcare in the Traditional Medicare Fee-for-Service Program
 Centers for Medicare & Medicaid Services Roadmap for Implementing Value Driven Healthcare in the Traditional Medicare Fee-for-Service Program vision for america: GOALS FOR VALUE-BASED PURCHASING: Patient-centered,
Centers for Medicare & Medicaid Services Roadmap for Implementing Value Driven Healthcare in the Traditional Medicare Fee-for-Service Program vision for america: GOALS FOR VALUE-BASED PURCHASING: Patient-centered,
Updates on CMS Quality, Value and Public Reporting
 Updates on CMS Quality, Value and Public Reporting Federation of American Hospitals Policy Conference Kate Goodrich, MD MHS Director, Quality Measurement and Value Based Incentives Group, CMS June 17,
Updates on CMS Quality, Value and Public Reporting Federation of American Hospitals Policy Conference Kate Goodrich, MD MHS Director, Quality Measurement and Value Based Incentives Group, CMS June 17,
Value Based Care and Healthcare Reform
 Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
No. 108 June 6, 2011. Centers for Medicare & Medicaid Services
 Vol. 76 Monday, No. 108 June 6, 2011 Part III Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 434, 438, and 447 Medicaid Program; Payment Adjustment for Provider-Preventable
Vol. 76 Monday, No. 108 June 6, 2011 Part III Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 434, 438, and 447 Medicaid Program; Payment Adjustment for Provider-Preventable
HAI LEADERSHIP PARTNERING FOR ACCOUNTABLE CARE
 HAI LEADERSHIP PARTNERING FOR ACCOUNTABLE CARE Cepheid s Government Affairs Department Advocating for Patient Access to Molecular Diagnostics in the Era of Healthcare Reform A TEAM APPROACH Legislative
HAI LEADERSHIP PARTNERING FOR ACCOUNTABLE CARE Cepheid s Government Affairs Department Advocating for Patient Access to Molecular Diagnostics in the Era of Healthcare Reform A TEAM APPROACH Legislative
Interventional Cardiology Peripheral Interventions Rhythm Management
 FY2016 Hospital Inpatient Final Rule (IPPS) Interventional Cardiology Peripheral Interventions Rhythm Management On July 31, 2015, the Centers for Medicare and Medicaid Services (CMS) released the Final
FY2016 Hospital Inpatient Final Rule (IPPS) Interventional Cardiology Peripheral Interventions Rhythm Management On July 31, 2015, the Centers for Medicare and Medicaid Services (CMS) released the Final
what value-based purchasing means to your hospital
 Paul Shoemaker what value-based purchasing means to your hospital CMS has devised an intricate way to measure a hospital s quality of care to determine whether the hospital qualifies for incentive payments
Paul Shoemaker what value-based purchasing means to your hospital CMS has devised an intricate way to measure a hospital s quality of care to determine whether the hospital qualifies for incentive payments
Narrow network health plans: New approaches to regulating adequacy and transparency. Michael S. Adelberg
 Compliance TODAY October 2015 a publication of the health care compliance association www.hcca-info.org Combating healthcare fraud in New Jersey an interview with Paul J. Fishman United States Attorney
Compliance TODAY October 2015 a publication of the health care compliance association www.hcca-info.org Combating healthcare fraud in New Jersey an interview with Paul J. Fishman United States Attorney
Hospital Quality Initiative Overview CENTERS FOR MEDICARE & MEDICAID SERVICES December 2005
 Hospital Quality Initiative Overview CENTERS FOR MEDICARE & MEDICAID SERVICES December 2005 Background Quality health care is a high priority for the Bush administration, the Department of Health and Human
Hospital Quality Initiative Overview CENTERS FOR MEDICARE & MEDICAID SERVICES December 2005 Background Quality health care is a high priority for the Bush administration, the Department of Health and Human
The Why and How of a CDI Program. Deb Neville, RHIA, CCS-P, Elsevier/MC Strategies Donna Bonno, CPC- CPC-I, QuadraMed September 12, 2012
 The Why and How of a CDI Program Deb Neville, RHIA, CCS-P, Elsevier/MC Strategies Donna Bonno, CPC- CPC-I, QuadraMed September 12, 2012 Objectives Understand the reasons behind a Clinical Documentation
The Why and How of a CDI Program Deb Neville, RHIA, CCS-P, Elsevier/MC Strategies Donna Bonno, CPC- CPC-I, QuadraMed September 12, 2012 Objectives Understand the reasons behind a Clinical Documentation
Healthcare Reform Update Conference Call VI
 Healthcare Reform Update Conference Call VI Sponsored by the Healthcare Reform Educational Task Force October 9, 2009 2:00-2:45 2:45 pm Eastern Healthcare Delivery System Reform Provisions in America s
Healthcare Reform Update Conference Call VI Sponsored by the Healthcare Reform Educational Task Force October 9, 2009 2:00-2:45 2:45 pm Eastern Healthcare Delivery System Reform Provisions in America s
Overview of the Hospital Value-Based Purchasing (VBP) Fiscal Year (FY) 2017
 Fiscal Year (FY) 2017") Overview of the Hospital Value-Based Purchasing (VBP) Fiscal Year (FY) 2017 Bethany Wheeler Hospital VBP Program Support Contract Lead HSAG February 17, 2015 2 p.m. ET Purpose This event will provide an
Overview of the Hospital Value-Based Purchasing (VBP) Fiscal Year (FY) 2017 Bethany Wheeler Hospital VBP Program Support Contract Lead HSAG February 17, 2015 2 p.m. ET Purpose This event will provide an
Evidence Based Practice to. Value Based Purchasing. Barb Rogness BSN MS Building Bridges May 2013
 Evidence Based Practice to Value Based Purchasing Barb Rogness BSN MS Building Bridges May 2013 Why this topic? Value based Purchasing is here and not going away. It will grow by leaps and bounds. The
Evidence Based Practice to Value Based Purchasing Barb Rogness BSN MS Building Bridges May 2013 Why this topic? Value based Purchasing is here and not going away. It will grow by leaps and bounds. The
TUTORIAL: How to Code an Emergency Department (ED) Record
 Record") TUTORIAL: How to Code an Emergency Department (ED) Record Welcome! Assigning ICD-10-CM codes to diagnoses and CPT/HCPCS Level II codes to procedures/services for emergency department office records can
TUTORIAL: How to Code an Emergency Department (ED) Record Welcome! Assigning ICD-10-CM codes to diagnoses and CPT/HCPCS Level II codes to procedures/services for emergency department office records can
Value-Based Payment and Health System Transformation
 Value-Based Payment and Health System Transformation National Health Policy Forum Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for
Value-Based Payment and Health System Transformation National Health Policy Forum Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for
Healthcare Financial Management Association Southern California. Implementation of MS-DRGs. November 20, 2008
 Healthcare Financial Management Association Southern California Implementation of MS-DRGs November 20, 2008 John Valenta, CPA, MBA, Director Health Sciences Regulatory Practice Deloitte & Touche LLP Agenda
Healthcare Financial Management Association Southern California Implementation of MS-DRGs November 20, 2008 John Valenta, CPA, MBA, Director Health Sciences Regulatory Practice Deloitte & Touche LLP Agenda
U.S. Department of Health & Human Services May 7, 2014. New HHS Data Shows Major Strides Made in Patient Safety, Leading to Improved Care and Savings
 U.S. Department of Health & Human Services May 7, 2014 New HHS Data Shows Major Strides Made in Patient Safety, Leading to Improved Care and Savings The data in this report shows a substantial nine percent
U.S. Department of Health & Human Services May 7, 2014 New HHS Data Shows Major Strides Made in Patient Safety, Leading to Improved Care and Savings The data in this report shows a substantial nine percent
National Provider Call: Hospital Value-Based Purchasing (VBP) Program
 Program") National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
Present on Admission Reporting
 Present on Admission Reporting Audio Seminar/Webinar February 21, 2008 Practical Tools for Seminar Learning Copyright 2008 American Health Information Management Association. All rights reserved. Disclaimer
Present on Admission Reporting Audio Seminar/Webinar February 21, 2008 Practical Tools for Seminar Learning Copyright 2008 American Health Information Management Association. All rights reserved. Disclaimer
The electronic health record (EHR) has been a game-changer for CDI specialists.
 has been a game-changer for CDI specialists.") Physician queries and the use of prior information: Reevaluating the role of the CDI specialist WHITE PAPER Summary: The following white paper examines the issue of whether to use information from a prior
Physician queries and the use of prior information: Reevaluating the role of the CDI specialist WHITE PAPER Summary: The following white paper examines the issue of whether to use information from a prior
Healthcare Reform & Value Based Purchasing: Are You Ready?
 Healthcare Reform & Value Based Purchasing: Are You Ready? Premier, Inc Jan Englert, Director-QUEST Poudre Valley Health System Sonja Wulff, VP Center for Performance Excellence Federal Register Statement:
Healthcare Reform & Value Based Purchasing: Are You Ready? Premier, Inc Jan Englert, Director-QUEST Poudre Valley Health System Sonja Wulff, VP Center for Performance Excellence Federal Register Statement:
Reporting Adverse Events and Concerns at Stroger Hospital
 Reporting Adverse Events and Concerns at Stroger Hospital Case Pt on coumadin comes in for community acquired pneumonia and is started on levaquin After several days, you note a lot of bruising.. You realize
Reporting Adverse Events and Concerns at Stroger Hospital Case Pt on coumadin comes in for community acquired pneumonia and is started on levaquin After several days, you note a lot of bruising.. You realize
Montana Hospital Discharge Data System
 Montana Hospital Discharge Data System Surveillance Report July, 2011 Results of the E-Code Quality Improvement Survey, 2011 Introduction Cody L. Custis, MS, Epidemiologist, MHDDS Hannah Yang, BS Carol
Montana Hospital Discharge Data System Surveillance Report July, 2011 Results of the E-Code Quality Improvement Survey, 2011 Introduction Cody L. Custis, MS, Epidemiologist, MHDDS Hannah Yang, BS Carol
ICD-9 Basics Study Guide
 Board of Medical Specialty Coding ICD-9 Basics Study Guide for the Home Health ICD-9 Basic Competencies Examination Two Washingtonian Center 9737 Washingtonian Blvd., Ste. 100 Gaithersburg, MD 20878-7364
Board of Medical Specialty Coding ICD-9 Basics Study Guide for the Home Health ICD-9 Basic Competencies Examination Two Washingtonian Center 9737 Washingtonian Blvd., Ste. 100 Gaithersburg, MD 20878-7364
Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium
 Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium October 30, 2008 Barry Libman, RHIA, CCS, CCS-P President, Barry Libman Inc. Stroke Coding Issues Outline Medical record documentation
Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium October 30, 2008 Barry Libman, RHIA, CCS, CCS-P President, Barry Libman Inc. Stroke Coding Issues Outline Medical record documentation
Using Medicare Hospitalization Information and the MedPAR. Beth Virnig, Ph.D. Associate Dean for Research and Professor University of Minnesota
 Using Medicare Hospitalization Information and the MedPAR Beth Virnig, Ph.D. Associate Dean for Research and Professor University of Minnesota MedPAR Medicare Provider Analysis and Review Includes information
Using Medicare Hospitalization Information and the MedPAR Beth Virnig, Ph.D. Associate Dean for Research and Professor University of Minnesota MedPAR Medicare Provider Analysis and Review Includes information
Abstraction 101 An Introduction for New Abstractors
 California and Florida In the Know Webinar Series Abstraction 101 An Introduction for New Abstractors September 2011 Becky Ure, RN, BSN, MEd 1 Topics The driving forces behind abstraction and public reporting
California and Florida In the Know Webinar Series Abstraction 101 An Introduction for New Abstractors September 2011 Becky Ure, RN, BSN, MEd 1 Topics The driving forces behind abstraction and public reporting
FY2015 Proposed Hospital Inpatient Rule Summary
 FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
June 25, 2012. Dear Acting Administrator Tavenner,
 June 25, 2012 Marilyn B. Tavenner, RN, Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-1588-P P.O. Box 8011 Baltimore, MD 21244-1850
June 25, 2012 Marilyn B. Tavenner, RN, Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-1588-P P.O. Box 8011 Baltimore, MD 21244-1850
The Impact of Value- Based Purchasing in the Healthcare Industry
 The Impact of Value- Based Purchasing in the Healthcare Industry Presented By: Kim Charland, BA, RHIT, CCS Senior Vice President Clinical Innovation for Panacea Healthcare Solutions and Editor of VBPmonitor
The Impact of Value- Based Purchasing in the Healthcare Industry Presented By: Kim Charland, BA, RHIT, CCS Senior Vice President Clinical Innovation for Panacea Healthcare Solutions and Editor of VBPmonitor
September 12, 2011. Dear Dr. Corrigan:
 September 12, 2011 Janet M. Corrigan, PhD, MBA President and Chief Executive Officer National Quality Forum 601 13th Street, NW Suite 500 North Washington, D.C. 20005 Re: Measure Applications Partnership
September 12, 2011 Janet M. Corrigan, PhD, MBA President and Chief Executive Officer National Quality Forum 601 13th Street, NW Suite 500 North Washington, D.C. 20005 Re: Measure Applications Partnership
Creating a Hybrid Database by Adding a POA Modifier and Numerical Laboratory Results to Administrative Claims Data
 Creating a Hybrid Database by Adding a POA Modifier and Numerical Laboratory Results to Administrative Claims Data Michael Pine, M.D., M.B.A. Michael Pine and Associates, Inc. mpine@consultmpa.com Overview
Creating a Hybrid Database by Adding a POA Modifier and Numerical Laboratory Results to Administrative Claims Data Michael Pine, M.D., M.B.A. Michael Pine and Associates, Inc. mpine@consultmpa.com Overview
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY
 A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
Preparing for the Conversion from ICD-9 to ICD-10: What You Need to Be Doing Today
 Preparing for the Conversion from ICD-9 to ICD-10: What You Need to Be Doing Today Currently in the United States, ICD-9 is the code set used to report diagnoses and inpatient procedures. ICD-9 stands
Preparing for the Conversion from ICD-9 to ICD-10: What You Need to Be Doing Today Currently in the United States, ICD-9 is the code set used to report diagnoses and inpatient procedures. ICD-9 stands
ICD-10 Preparation for Non- Coders in the Revenue Cycle
 ICD-10 Preparation for Non- Coders in the Revenue Cycle September 24, 2015 Arkansas HFMA Revenue Cycle Seminar Susan Wallace, MEd, RHIA, CCS, CCDS, CDIP, FAHIMA Program Objectives Explain the impact of
ICD-10 Preparation for Non- Coders in the Revenue Cycle September 24, 2015 Arkansas HFMA Revenue Cycle Seminar Susan Wallace, MEd, RHIA, CCS, CCDS, CDIP, FAHIMA Program Objectives Explain the impact of
CMS Quality Measurement and Value Based Purchasing Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 CMS Quality Measurement and Value Based Purchasing Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS American Urological Association Quality Improvement Summit
CMS Quality Measurement and Value Based Purchasing Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS American Urological Association Quality Improvement Summit
Introduction. The History of CMS/JCAHO Measure Alignment
 Release Notes: Introduction - Version 2.2 Introduction The History of CMS/JCAHO Measure Alignment In early 1999, the Joint Commission solicited input from a wide variety of stakeholders (e.g., clinical
Release Notes: Introduction - Version 2.2 Introduction The History of CMS/JCAHO Measure Alignment In early 1999, the Joint Commission solicited input from a wide variety of stakeholders (e.g., clinical
ICD-10 Compliance Date
 ICD-10 Implementation Frequently Asked Questions Updated September 2015 ICD-10 Compliance Date The U.S. Department of Health and Human Services (HHS) issued a rule on July 31, 2014 finalizing October 1,
ICD-10 Implementation Frequently Asked Questions Updated September 2015 ICD-10 Compliance Date The U.S. Department of Health and Human Services (HHS) issued a rule on July 31, 2014 finalizing October 1,
Value Based Purchasing and Accountable Care Organizations
 Value Based Purchasing and Accountable Care Organizations P R E S E N T E D B Y: Mary Carol Todd, MSN, RN Senior Vice President, Clinical Efficiency Catholic Healthcare West San Francisco, California CHW
Value Based Purchasing and Accountable Care Organizations P R E S E N T E D B Y: Mary Carol Todd, MSN, RN Senior Vice President, Clinical Efficiency Catholic Healthcare West San Francisco, California CHW
See page 331 of HEDIS 2013 Tech Specs Vol 2. HEDIS specs apply to plans. RARE applies to hospitals. Plan All-Cause Readmissions (PCR) *++
 *++") Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
APPENDIX E DATA REPORTING REGULATIONS
 APPENDIX E DATA REPORTING REGULATIONS DATA REPORTING REGULATION Section 4602(e) of the Balanced Budget Act of 1997 authorizes the Secretary of the Department of Health and Human Services (HHS) to require
APPENDIX E DATA REPORTING REGULATIONS DATA REPORTING REGULATION Section 4602(e) of the Balanced Budget Act of 1997 authorizes the Secretary of the Department of Health and Human Services (HHS) to require
GUIDE TO HOME HEALTH DIAGNOSIS CODES
 GUIDE TO HOME HEALTH DIAGNOSIS CODES Proper selection of diagnoses codes for the Medicare OASIS Assessment The process of selecting correct diagnosis codes for the OASIS Start of Care, Re-Certification
GUIDE TO HOME HEALTH DIAGNOSIS CODES Proper selection of diagnoses codes for the Medicare OASIS Assessment The process of selecting correct diagnosis codes for the OASIS Start of Care, Re-Certification
Reimbursement for Medical Products: Ensuring Marketplace
 Reimbursement for Medical Products: Ensuring Marketplace Success by Securing Coverage and Payment Christopher J. Panarites, Ph.D. Director, Endovascular Products Health Economics and Outcomes Research
Reimbursement for Medical Products: Ensuring Marketplace Success by Securing Coverage and Payment Christopher J. Panarites, Ph.D. Director, Endovascular Products Health Economics and Outcomes Research
AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY
 AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY Adult Medicaid Quality Grants Program The Adult Medicaid Quality Grants Program is a 2-year funding opportunity designed to support grantee Medicaid
AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY Adult Medicaid Quality Grants Program The Adult Medicaid Quality Grants Program is a 2-year funding opportunity designed to support grantee Medicaid
The Future of Population-Based Reimbursement
 Thomas Jefferson University Jefferson Digital Commons Jefferson College of Population Health Forum Jefferson College of Population Health 11-12-2014 The Future of Population-Based Reimbursement David Chin,
Thomas Jefferson University Jefferson Digital Commons Jefferson College of Population Health Forum Jefferson College of Population Health 11-12-2014 The Future of Population-Based Reimbursement David Chin,
Defining the Core Clinical Documentation Set
 Defining the Core Clinical Documentation Set for Coding Compliance Quality Healthcare Through Quality Information It is time to examine coding compliance policy and test it against the upcoming challenges
Defining the Core Clinical Documentation Set for Coding Compliance Quality Healthcare Through Quality Information It is time to examine coding compliance policy and test it against the upcoming challenges
National Action Plan to Prevent Health Care-Associated Infections: ROAD MAP TO ELIMINATION
 National Action Plan to Prevent Health Care-Associated Infections: ROAD MAP TO ELIMINATION 2013 National Action Plan to Prevent Health Care-Associated Infections: Road Map to Elimination April 2013 http://www.hhs.gov/ash/initiatives/hai/index.html
National Action Plan to Prevent Health Care-Associated Infections: ROAD MAP TO ELIMINATION 2013 National Action Plan to Prevent Health Care-Associated Infections: Road Map to Elimination April 2013 http://www.hhs.gov/ash/initiatives/hai/index.html
ICD-10... What Are You Waiting For?
 ICD-10... What Are You Waiting For? What is it? International classification for all general epidemiological, many health management purposes, and clinical use Published by the World Health Organization
ICD-10... What Are You Waiting For? What is it? International classification for all general epidemiological, many health management purposes, and clinical use Published by the World Health Organization
Trends in Medical Malpractice. Patients versus Profits
 Trends in Medical Malpractice Patients versus Profits CAS 2008 Spring Meeting Quebec City, Quebec Presented by: Greg Larcher, FCAS, Aon Global Tammi Dulberger, FCAS, IronHealth How about Patients and Profits?
Trends in Medical Malpractice Patients versus Profits CAS 2008 Spring Meeting Quebec City, Quebec Presented by: Greg Larcher, FCAS, Aon Global Tammi Dulberger, FCAS, IronHealth How about Patients and Profits?
Interventional Cardiology Peripheral Interventions Rhythm Management
 FY2016 Hospital Inpatient Rule (IPPS) Interventional Cardiology Peripheral Interventions Rhythm Management On April 17, 2015 the Centers for Medicare and Medicaid Services (CMS) released the Hospital Inpatient
FY2016 Hospital Inpatient Rule (IPPS) Interventional Cardiology Peripheral Interventions Rhythm Management On April 17, 2015 the Centers for Medicare and Medicaid Services (CMS) released the Hospital Inpatient
Patient Criteria: Modeling in LTRAX
 Patient Criteria: Modeling in LTRAX Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant Overview Objectives Review background on upcoming LTCH patient criteria Examine LTRAX
Patient Criteria: Modeling in LTRAX Mary Dalrymple Managing Director, LTRAX Kristen Smith, MHA, PT Senior Consultant Overview Objectives Review background on upcoming LTCH patient criteria Examine LTRAX
HCIM ICD-10 Training Online Course Catalog August 2015
 HCIM ICD-10 Training Online Course Catalog August 2015 Course/Content Duration Quiz Duration CME Credits Assessments: Assessment: Provider - Baseline - E/M Emergency Department 45 5/1/2015 Assessment:
HCIM ICD-10 Training Online Course Catalog August 2015 Course/Content Duration Quiz Duration CME Credits Assessments: Assessment: Provider - Baseline - E/M Emergency Department 45 5/1/2015 Assessment:
Data Analysis Project Summary
 of Introduction The notion that adverse patient safety events result in excess costs is not a new concept. However, more research is needed on the actual costs of different types of adverse events at an
of Introduction The notion that adverse patient safety events result in excess costs is not a new concept. However, more research is needed on the actual costs of different types of adverse events at an
Continuous Quality Monitoring
 Continuous to Maximize ICD-10 Proficiency and Organizational Benefits 1 2 The New Role of 3 Continuous ! A common strategy to maintain coding accuracy, continuous quality reviews have taken on greater
Continuous to Maximize ICD-10 Proficiency and Organizational Benefits 1 2 The New Role of 3 Continuous ! A common strategy to maintain coding accuracy, continuous quality reviews have taken on greater
Value Based Insurance Design Key concepts & their application at HealthPartners Health Insurance Plan
 Value Based Insurance Design Key concepts & their application at HealthPartners Health Insurance Plan Shaun Frost, MD Associate Medical Director for Care Delivery Systems HealthPartners Health Plan Minneapolis,
Value Based Insurance Design Key concepts & their application at HealthPartners Health Insurance Plan Shaun Frost, MD Associate Medical Director for Care Delivery Systems HealthPartners Health Plan Minneapolis,
Present on Admission Reporting Guidelines
 Introduction Present on Admission Reporting Guidelines These guidelines are to be used as a supplement to the ICD-9-CM Official Guidelines for Coding and Reporting to facilitate the assignment of the Present
Introduction Present on Admission Reporting Guidelines These guidelines are to be used as a supplement to the ICD-9-CM Official Guidelines for Coding and Reporting to facilitate the assignment of the Present
2016 PERITONEAL DIALYSIS CATHETERS CODING AND REIMBURSEMENT GUIDE
 2016 PERITONEAL DIALYSIS CATHETERS CODING AND REIMBURSEMENT GUIDE Contents Overview of Peritoneal Dialysis 2 Physician Reimbursement for Peritoneal Dialysis s Under Resource-based Relative Value Scale
2016 PERITONEAL DIALYSIS CATHETERS CODING AND REIMBURSEMENT GUIDE Contents Overview of Peritoneal Dialysis 2 Physician Reimbursement for Peritoneal Dialysis s Under Resource-based Relative Value Scale
ENGAGING PHYSICIANS FOR ICD-10: ALL ABOARD Engaging Physicians for ICD-10: All Aboard
 ENGAGING PHYSICIANS FOR ICD-10: ALL ABOARD Engaging Physicians for ICD-10: All Aboard ICD-10 Lisa Kozakoff Principal Consultant Siemens Healthcare Lisa Kozakoff Principal Consultant Agenda Introduction
ENGAGING PHYSICIANS FOR ICD-10: ALL ABOARD Engaging Physicians for ICD-10: All Aboard ICD-10 Lisa Kozakoff Principal Consultant Siemens Healthcare Lisa Kozakoff Principal Consultant Agenda Introduction
Medicare Advantage Risk Adjustment Data Validation CMS-HCC Pilot Study. Report to Medicare Advantage Organizations
 Medicare Advantage Risk Adjustment Data Validation CMS-HCC Pilot Study Report to Medicare Advantage Organizations JULY 27, 2004 JULY 27, 2004 PAGE 1 Medicare Advantage Risk Adjustment Data Validation CMS-HCC
Medicare Advantage Risk Adjustment Data Validation CMS-HCC Pilot Study Report to Medicare Advantage Organizations JULY 27, 2004 JULY 27, 2004 PAGE 1 Medicare Advantage Risk Adjustment Data Validation CMS-HCC
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Hospital Value-Based Purchasing (VBP) Program
 Program") Medicare Spending per Beneficiary (MSPB) Measure Presentation Question & Answer Transcript Moderator: Bethany Wheeler, BS Hospital VBP Program Support Contract Lead Hospital Inpatient Value, Incentives,
Medicare Spending per Beneficiary (MSPB) Measure Presentation Question & Answer Transcript Moderator: Bethany Wheeler, BS Hospital VBP Program Support Contract Lead Hospital Inpatient Value, Incentives,
Supplemental Technical Information
 An Introductory Analysis of Potentially Preventable Health Care Events in Minnesota Overview Supplemental Technical Information This document provides additional technical information on the 3M Health
An Introductory Analysis of Potentially Preventable Health Care Events in Minnesota Overview Supplemental Technical Information This document provides additional technical information on the 3M Health
June 2, 2014. RE: File Code CMS-1608-P. Dear Ms. Tavenner:
 . June 2, 2014 Marilyn Tavenner Centers for Medicare & Medicaid Services Room 445-G, Hubert H. Humphrey Building 200 Independence Avenue SW Washington, DC RE: File Code CMS-1608-P Dear Ms. Tavenner: The
. June 2, 2014 Marilyn Tavenner Centers for Medicare & Medicaid Services Room 445-G, Hubert H. Humphrey Building 200 Independence Avenue SW Washington, DC RE: File Code CMS-1608-P Dear Ms. Tavenner: The
Accountable Care Organizations and Future Healthcare Delivery
 Accountable Care Organizations and Future Healthcare Delivery Introduction Accountable care organizations (ACOs) are a key component of healthcare reform. This module covers the establishment of accountable
Accountable Care Organizations and Future Healthcare Delivery Introduction Accountable care organizations (ACOs) are a key component of healthcare reform. This module covers the establishment of accountable
UB-04 Claim Form Instructions
 UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
UB-04 Claim Form Instructions FORM LOCATOR NAME 1. Billing Provider Name & Address INSTRUCTIONS Enter the name and address of the hospital/facility submitting the claim. 2. Pay to Address Pay to address
National Council for Behavioral Health
 National Council for Behavioral Health Preparing your Organization for ICD-10 Implementation Presented by: Michael D. Flora, MBA, M.A.Ed, LCPC, LSW Senior Operations and Management Consultant David R.
National Council for Behavioral Health Preparing your Organization for ICD-10 Implementation Presented by: Michael D. Flora, MBA, M.A.Ed, LCPC, LSW Senior Operations and Management Consultant David R.
RE: Medicare s Post-acute Transfer Policy and Condition Code 42 BACKGROUND
 Memorandum TO: FROM: Glenn Hendrix Doug M. Hance DATE: RE: Medicare s Post-acute Transfer Policy and Condition Code 42 BACKGROUND Medicare s post-acute transfer policy distinguishes between discharges
Memorandum TO: FROM: Glenn Hendrix Doug M. Hance DATE: RE: Medicare s Post-acute Transfer Policy and Condition Code 42 BACKGROUND Medicare s post-acute transfer policy distinguishes between discharges
Long term care coding issues for ICD-10-CM
 Long term care coding issues for ICD-10-CM Coding Clinic, Fourth Quarter 2012 Pages: 90-98 Effective with discharges: October 1, 2012 Related Information Long Term Care Coding Issues for ICD-10-CM Coding
Long term care coding issues for ICD-10-CM Coding Clinic, Fourth Quarter 2012 Pages: 90-98 Effective with discharges: October 1, 2012 Related Information Long Term Care Coding Issues for ICD-10-CM Coding
Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program
 Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program Cristina Boccuti and Giselle Casillas For Medicare patients, hospitalizations can be stressful; even more so when
Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program Cristina Boccuti and Giselle Casillas For Medicare patients, hospitalizations can be stressful; even more so when
Institutional Billing Guide
 Program KANSAS MEDICAL ASSISTANCE PROGRAM Institutional Billing Guide Updated 10.2013 Institutional Billing The Kansas Medical Assistance Program (KMAP) offers different billing options to all providers.
Program KANSAS MEDICAL ASSISTANCE PROGRAM Institutional Billing Guide Updated 10.2013 Institutional Billing The Kansas Medical Assistance Program (KMAP) offers different billing options to all providers.
How CDI is Revolutionizing the Transition to Value-Based Care
 How CDI is Revolutionizing the Transition to Value-Based Care How CDI is Revolutionizing the Transition to Value-Based Care Creating a state-of-the-art clinical documentation improvement (CDI) program
How CDI is Revolutionizing the Transition to Value-Based Care How CDI is Revolutionizing the Transition to Value-Based Care Creating a state-of-the-art clinical documentation improvement (CDI) program
The Changing Face of Medical Necessity under ICD-10
 The Changing Face of Medical Necessity under ICD-0 Sponsored by 95 N. Fine Ave #04 Fresno CA 93720-565 Phone: (559) 25-5038 Fax: (559) 25-5836 www.californiahia.org Program Handouts Monday, June 8, 205
The Changing Face of Medical Necessity under ICD-0 Sponsored by 95 N. Fine Ave #04 Fresno CA 93720-565 Phone: (559) 25-5038 Fax: (559) 25-5836 www.californiahia.org Program Handouts Monday, June 8, 205
Overview and Legal Context
 Impact of ACOs on Physician/Provider Membership Decisions 0 Overview and Legal Context Michael R. Callahan Katten Muchin Rosenman LLP Vice Chair, Medical Staff Credentialing and Peer Review Practice Group
Impact of ACOs on Physician/Provider Membership Decisions 0 Overview and Legal Context Michael R. Callahan Katten Muchin Rosenman LLP Vice Chair, Medical Staff Credentialing and Peer Review Practice Group
ZEPHYRLIFE REMOTE PATIENT MONITORING REIMBURSEMENT REFERENCE GUIDE
 ZEPHYRLIFE REMOTE PATIENT MONITORING REIMBURSEMENT REFERENCE GUIDE Overview This guide includes an overview of Medicare reimbursement methodologies and potential coding options for the use of select remote
ZEPHYRLIFE REMOTE PATIENT MONITORING REIMBURSEMENT REFERENCE GUIDE Overview This guide includes an overview of Medicare reimbursement methodologies and potential coding options for the use of select remote
Health and Technology
 profile July 2010 Health and Technology A Blue Shield of California Foundation Legacy Program Background In 2004, the Blue Shield of California Foundation (BSCF) Board of Trustees approved the creation
profile July 2010 Health and Technology A Blue Shield of California Foundation Legacy Program Background In 2004, the Blue Shield of California Foundation (BSCF) Board of Trustees approved the creation
Moving Towards Bundled Payment
 ISSUE BRIEF Moving Towards Bundled Payment Introduction The fee-for-service system of payment for health care services is widely thought to be one of the major culprits in driving up U.S. health care costs.
ISSUE BRIEF Moving Towards Bundled Payment Introduction The fee-for-service system of payment for health care services is widely thought to be one of the major culprits in driving up U.S. health care costs.
Abu Dhabi Clinical Coding Audit
 Abu Dhabi Clinical Coding Audit 1 st January, 2014 Clinical Coding Steering Committee v4 1 Contents Section or Table 1. Objective 3 2. Who May Ask for an Audit? 3 3. Who May Conduct the Audits? 3 4. Payers
Abu Dhabi Clinical Coding Audit 1 st January, 2014 Clinical Coding Steering Committee v4 1 Contents Section or Table 1. Objective 3 2. Who May Ask for an Audit? 3 3. Who May Conduct the Audits? 3 4. Payers