CHVHP0389_Member Welcome Kit_South_Florida_BW_2015 :Layout 1 1/12/15 3:41 PM Page 1. Member Welcome Kit South Florida
|
|
|
- Jared Owen
- 8 years ago
- Views:
Transcription
1 CHVHP0389_Member Welcome Kit_South_Florida_BW_2015 :Layout 1 1/12/15 3:41 PM Page Member Welcome Kit South Florida

2

3 Table of Contents Important Definitions... 4 Your Child s VISTA ID Card... 4 Your Child s Doctor... 5 How To Change Your Child s Doctor... 5 Scheduling Your Child s First Appointment... 6 What to Expect at the Doctor s Office... 6 Getting a Referral from Your Child s Doctor Second Opinions Emergencies Getting Help in an Emergency When Your Child Gets Sick Away From Home Covered Services Summary of Benefits Benefits and Limitations Behavioral Health Durable Medical Equipment and Prosthetic Devices Emergency Services Home Health Services Hospice Services Inpatient Services Maternity Services and Newborn Care Skilled Nursing Facility Organ Transplantation Services Outpatient Services Refractions (Vision Testing) Substance Abuse Services Therapy Services Transportation Services Authorizations Case Management Program Adverse Determinations/Denials... 18

4 Grievances and Appeals Advance Directives Other Agencies Eligibility Policy Changes Canceling Your Child s Coverage Medical Bills/Claims Contacting VISTA Customer Service Need Help in a Language Other than English? If You are Hearing Impaired Important Phone Numbers Notice of Privacy Practices 26 2

5 Dear Parent/Guardian: Welcome to Coventry Health Care of Florida, Inc. d/b/a VISTA! Quality health care at your finger tips! This Guidebook explains your child s benefits with VISTA. Keep it handy. It contains important information to keep your child healthy. Your child s Coventry/VISTA ID card has been mailed to you. Check the ID card right away to make sure the information is accurate. If it is not, please call Customer Service at Your ID card will have: Your child s doctor Your child s membership start date with Coventry/VISTA The Customer Service telephone number Schedule your child s first doctor visit right away! Regular checkups will help your child s doctor know about problems early. You can also visit our website at You will find information on staying healthy. Visit our Kids Health site for more health information. It features lots of medically reviewed articles, moving pictures, and stories. They are written in a way that makes them just right for parents, kids, and teens. VISTA s Customer Service is available to answer any questions you may have. Call Monday through Friday from 8:00 a.m. to 7:00 p.m. If you are hearing or speech impaired and use a telephone device for the deaf, please call Relay. Our Nurse Line is available 24 hours a day to answer your medical questions when you cannot reach your doctor. To speak with a nurse, call Thanks for choosing VISTA!! 3

6 Important Definitions As you read this Guidebook, you may find it helpful to know the definitions of the following: Consultation - a visit to a doctor for an examination, testing, and advice Co-payment - the amount you have to pay for certain Covered Services. Covered Services - medical care, supplies, and/or products which VISTA will pay for as described in this Guidebook. Effective Date - the first day of your child s coverage with VISTA, which can be found on your child s VISTA ID Card. Emergency Medical Condition - a medical problem that is serious and/or painful and could lead to danger to your child s health or to the health of your child s unborn baby Health Professionals - persons licensed under the laws of the State of Florida to provide health care services. These people include doctors, dentists, optometrists, behavioral health providers, doctor assistants, nurse practitioners and other providers of care. Hospice - a facility which helps provide care and comfort to people who are dying or who are near to the end of their lives. Hospice care provides comfort measures for patients and supports families through the dying process. Medically Necessary - care your child needs that has been approved by VISTA. Participating Provider - health professionals, hospitals, other facilities, pharmacies, medical supply companies, and nursing agencies that have an agreement with VISTA to provide covered services to members. Service Area - the parts of Florida where VISTA offers the Healthy Kids Program. Specialist - any non-primary doctor (non-pcp) who provide covered services for VISTA members. VISTA - Coventry Health Care of Florida, Inc., a Health Maintenance Organization (HMO) in the State of Florida. Your Child s VISTA ID Card When your child becomes a member, VISTA will send you an ID card for your child in the mail. You will need the card when your child goes to a doctor, hospital, pharmacy, or anywhere else your child gets health care. Please keep it with you at all times. Never let anyone else use the 4


7 card. If your card is lost or stolen, please call VISTA Customer Service at right away so that you can get another card. Member: JOHN SAMPLE Member #: xxmbrxnbr-xx Group #: XXXXXXXX HEALTHY KIDS Eff. Date: 08/01/2012 PCP Name: NAMExxxxxxxxxxxxxxxxxxx PCP Phone: (000) Co-pays: $XX PCP $XX SPEC $XX ER $XX UC Rx:$X/$X Formulary Customer Service: (Mon-Fri 8am-7pm) FL-C40-XXXXXXXX---- M() D() V() 1035 *0* T15J Env [1] 2 of 1 Carrier [1] J013 Rx BIN: Rx Group: CVTYMCD J013 *0* T15J Env [1] 2 of 1 Carrier [1] 1089 FL-C40-XXXXXXXX---- M() D() V() 1036 Authorizations / Eligibility: Pharmacy Customer Service: Hearing or speech impaired (TDD): Relay Billing Information for Non-Contracted Providers: (Mon-Fri 8am-7pm) EMERGENCY SERVICES: Seek treatment at the nearest emergency room or network urgent care center or call 911. Notify us within 48 hours or as soon as reasonably possible if you are admitted to the hospital. Mail claims to: Coventry Health Care of Florida, Inc. P.O. Box 7403 London, KY Emdeon Payer ID: Express Scripts: Rx BIN: Rx Group: CVTYMCD Possession of an ID card does not guarantee eligibility or payment. Your Child s Doctor When your child becomes a member, VISTA will assign your child to a doctor near where you live. The name and phone number of your child s doctor will be on your child s ID card. When you go to your child s doctor, be sure to show your child s ID card. Your child s doctor will help you with all of your health care. You must use doctors in our network. Any services provided by a doctor that is not our network must be approved by us before you get the services. You may call customer service to request authorization to use a doctor that is not in our network. A list of the doctors in our network may be found in the Provider Directory. How To Change Your Child s Doctor If you want or need to change your child s doctor, follow these steps: Look through the VISTA Provider Directory and pick a doctor who is seeing new patients. Call VISTA s Customer Service Department at Monday through Friday from 8:00 a.m. to 7:00 p.m. If you are hearing or speech impaired and use a telephone device for the deaf, please call Relay. If you call on or before the 15th of the month, your doctor will be changed right away. If you 5
 D() V() 1035 *0* 20130604T15J013000000001000200011100 Env [1] 2 of 1 Carrier [1] J013 Rx BIN: 610014 Rx Group: CVTYMCD J013 *0* 20130604T15J013000000001000200011100 Env [1] 2")
8 call after the 15th of the month, your doctor will be changed on the 1st day of the following month. VISTA will then send you a new ID card showing the name and telephone number of your child s new doctor. Scheduling Your Child s First Appointment As soon as your child becomes a member, call your child s doctor to schedule a first visit. When you go for an appointment, your child s doctor will ask about your child s past health. He/she will start a medical record on your child. It is important for you to ask your child s past doctor (or doctors) to send all medical records to the new doctor s office. What to Expect at the Doctor s Office Regular well-child care can prevent problems with your child s long-term health. Your child should receive regular check-ups. Your child s doctor is the best person to help recommend the shots and preventive care your child needs. These charts show the check-up schedule recommended by the American Academy of Pediatrics. Well-child Check-ups Hearing Childhood Routine Care at: 3-5 days, 1 month, 2 months, 4 months, 6 months, 9 months, 12 months, 15 months, 18 months, 24 months, 30 months, 36 months - then yearly thereafter Screening in Newborn period recommended Vision Routine screening beginning at age 3 Lead Screening Screen all at risk children (all Medicaid children by law) for blood lead at age 12 months and at age 24 months In its efforts to improve member awareness of nationally established screening guidelines for common disease states, Vista supports the preventive care screening guidelines for children and adolescents recommended by the American Academy of Pediatrics. Members and providers may access the American Academy of Pediatrics website at Members are encouraged to familiarize themselves with these guidelines and to discuss them with their providers. As with all guidelines, they are intended to assist in the prevention of disease and in the identification and treatment of asymptomatic patients with pre-clinical disease. This guideline is referenced with the understanding that a physician s screening and treatment plan for any particular patient will be individualized. It is important to note that alternative screening guidelines exist, and physicians and members are encouraged to refer to other authoritative sources as their individual clinical situation may require. VISTA does not intent to exercise any control or direction over a treating provider s medical judgment or clinical decisions, or to interfere with the physician/patient relationship. Please note that not all health insurance and group health plans cover all recommended services. 6

9 Please check your benefit documents to determine whether your health insurance or group health plan covers these services. Recommended Immunization Schedule for Persons Aged 0 through 6 Years - United States For those who fall behind or start late, see the catch-up schedule 7

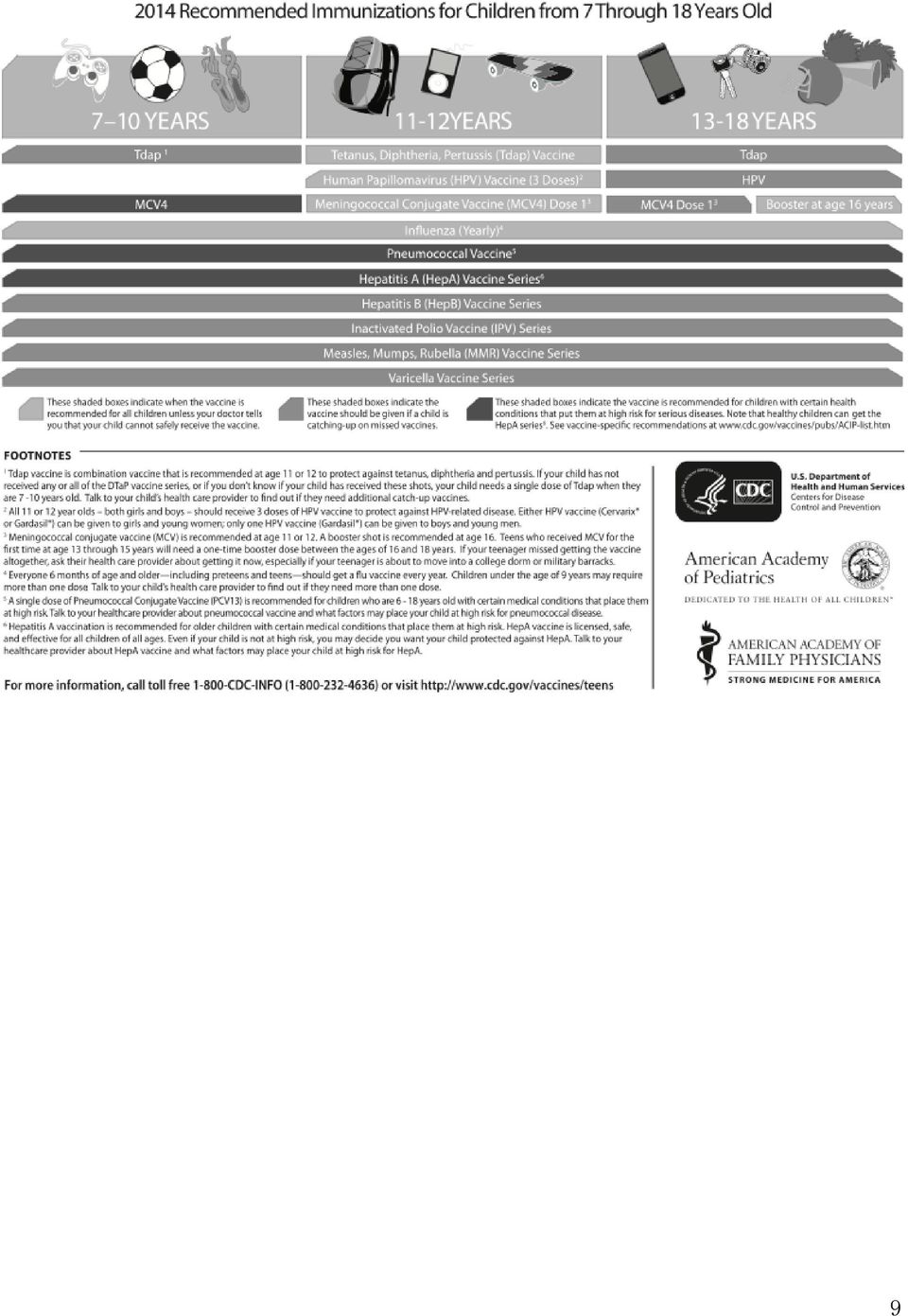
10 Recommended Immunization Schedule for Persons Aged 7 through 18 Years United States For those who fall behind or start late, see the schedule below and the catch-up schedule 8

11 9
12 Getting a Referral from Your Child s Doctor The referral process is one of the ways VISTA helps your child get the care and services that he/she needs. Your child s doctor is trained to treat most of your child s medical needs. Your child s doctor is the best person to help you decide if your child needs a referral. Your doctor will give you a referral if your child needs the care of a specialist. Here are the steps involved in getting care from a VISTA specialist: 1. Call your child s doctor for an appointment. 2. After seeing your child, if the doctor feels it is necessary, the doctor will give you a written referral for your child to see a specialist. 3. Call the specialist to schedule an appointment. *Please note that referrals can be used for 60 days after the date on the referral. After that, you will need to get another referral. 4. Take the referral form to the appointment with the Specialist. Seeing a Specialist without a Referral If your child goes to a specialist without a referral, you may have to pay for the services your 10

13 child receives, even if that specialist is a VISTA doctor. In some cases, you don t need a referral from your child s doctor to see a specialist. VISTA specialists that your child can see without a referral include: Chiropractors Podiatrists Behavioral Health/Substance Abuse Outpatient Care - Call PsychCare at (Please note that inpatient behavioral health services do need a referral). Dermatologists (first five visits each contract year). OB/GYN doctors for an annual well-woman visit and any follow-up care because of the well woman visit Optometrists for an annual eye examination if your child is a diabetic. (Children who are not diabetics need referrals). OB/GYN doctors if your child is pregnant Please Note: Sometimes your child s doctor may need to send your child to a non-vista provider. This must be approved by VISTA before your child sees the specialist. Your child s doctor must work with VISTA directly to arrange this referral. Second Opinions Sometimes families wish to see another doctor of the same type that they have already seen for a child s medical problem. This is known as a second opinion. As a VISTA member, your child can get a second opinion by a doctor of your choice inside the service area if: Your child is not getting better on the current treatment You don t agree that your child needs or should get surgery (an operation) You don t agree with the treatment your child s doctor has recommended The doctor who provides a second opinion must: Examine your child Not be part of the same practice as the doctor who first recommended surgery or treatment Not perform any surgery or treatment to correct the problem for which the second opinion was done To get a second opinion, speak with your child s doctor. A referral is needed. If your child gets a second opinion from a VISTA provider, you will need to pay your regular copayment for a doctor visit. If VISTA does not have a doctor inside the service area to meet your child s medical needs, VISTA will help arrange care from a doctor outside the service area, and your co-payment will not go up. However, if there is a doctor in your service area and you choose to go outside the service area anyway, VISTA will only pay 60% of the costs. You have to pay the 40% difference. Second opinions from non-vista doctors are limited to three (3) per calendar year. 11

14 Emergencies An emergency is a medical problem that is serious or painful and could be dangerous to your child s health or to the health of your child s unborn baby (if your child is pregnant). Examples of emergencies include injuries, high fevers, bleeding, or bad stomach pain. Getting Help in an Emergency Call 911 to get immediate help in an emergency. You do not need to get VISTA s permission for emergency care, even if you are on vacation or out of VISTA s service area. If your child receives care in an emergency department that is not in the VISTA service area, be sure that you call your child s doctor within 48 hours or as soon as possible after your child has received care. Remember that your child s doctor is available to you 24 hours a day to help arrange care with other providers if needed. If your child is admitted to a hospital for treatment, the doctor often calls VISTA to let us know that your child is in the hospital. We also ask that you or someone on your behalf contact VISTA at to be sure that we are notified. If your child is admitted to a hospital outside VISTA s service area, you or someone on your behalf must contact VISTA at within 48 hours, or as soon as possible. Letting us know is important since it allows VISTA and your child s doctor to help make arrangements for your child s medical care. VISTA may arrange to transfer your child to a participating hospital within VISTA s service area as soon as a move is safe for your child. The 24-Hour Nurse Line ( ) is also available for your medical questions when you cannot reach your doctor. Scheduling Appointments Here is a quick guide to scheduling appointments: Urgent Appointment - for a medical problem that is not an emergency but does need to be treated soon. Examples might include an earache or a cold that is getting worse. An urgent appointment should be scheduled within 24 hours from the time you call your doctor s office. Routine Appointment - for a health problem that is not urgent or emergent, including follow-up care. A routine appointment should be scheduled within seven days of your call Well Care Appointment (Routine) - for check-ups, an appointment should be scheduled within four weeks of your call When Your Child Gets Sick Away From Home Call 911 to get immediate help in an emergency. You do not need to get VISTA s permission for emergency care, even if you are on vacation or out of VISTA s service area. Sometimes, your child gets sick or hurt away from home, but it is not a true emergency. In this case, call your child s VISTA doctor to help you arrange care for your child. Your child s doctor may tell you to take your child to a doctor near where you are. In this case, VISTA will work 12

15 with your family to arrange payment for needed care. VISTA does not cover routine care and check-ups outside the VISTA service area. Sometimes providers will contact VISTA and arrange payment directly with us. Other providers will ask you to pay for the care up front. In this case, you will need to call VISTA Customer Service at after your child is seen. Customer Service will help you with the forms and information you may need so that VISTA can pay you back for medically necessary care. Covered Services The chart below explains VISTA s covered benefits for your child. Summary of Benefits Special Note: Native Americans or Alaskan Natives (that have been qualified by Healthy Kids) do not have cost sharing, including co-payments. All covered services for Native Americans or Alaskan Natives have a $0 co-payment. SUMMARY OF BENEFITS Lifetime Benefit Maximum: $1,000,000 I. PROFESSIONAL AND OUTPATIENT SERVICES CO-PAYMENT A. Office visit(s) to doctor for minor illness or accident care $5 B. Well child care and school-related physicals; visits to doctor for preventive care, including all immunizations recommended by American Academy of Pediatrics C. Routine vision screening (performed by doctor or Optometrist) $0 D. Routine hearing screening (performed by doctor) $0 E. Specialist office visit(s) (with referral) $5 F. Chiropractic services (per Florida Medicaid guidelines 24 visits per $5 contract year) G. Diagnostic testing (lab, x-rays, etc.) $0 H. Second medical opinion from a participating provider within the service $5 area (or outside the service area if a doctor can not be found in the service area) I. Second medical opinion from a non-participating provider 40% of usual and customary charges II. INPATIENT SERVICES CO-PAYMENT Inpatient medical and surgical care $0 $0 13

16 III. MATERNITY SUMMARY OF BENEFITS CO-PAYMENT Prenatal, delivery, postnatal and newborn care $0 IV. BEHAVIORAL HEALTH/SUBSTANCE ABUSE CO-PAYMENT Behavioral Health Inpatient $0 Outpatient $5 Substance Abuse Inpatient $0 Outpatient $5 V. EMERGENCY SERVICES CO-PAYMENT A. Emergency room visits in a hospital co-payment is waived if admitted or authorized by doctor B. Transportation for Emergencies $10 C. Urgent Care Centers $5 VI. OTHER BENEFITS $10 CO-PAYMENT A. Outpatient Physical, Occupational, Respiratory and Speech Therapy $5 B. Home Health Services $5 C. Hospice Care $5 D. Refraction (Vision Testing) $5 E. Corrective Lenses and Frames $10 F. Durable Medical Equipment and Prosthetic Devices $0 G. Hearing Aid $0 H. Nursing Facility $0 I. Pharmacy (covered drugs include all prescribed drugs covered by Florida Medicaid). Limitation: Florida Medicaid Formulary with generic substitution. Brand name products are covered if a generic substitution is not available or when the prescribing doctor indicates that a brand name is Medically Necessary. All prescriptions must be written by child s doctor, contracted specialist, consultant doctors or dental provider. $5 Generic $5 Brand The Summary of Benefits listed on the previous pages is intended to be read with the Benefits and Limitations section of this Guidebook. 14
 $5 E. Corrective Lenses and Frames $10 F.")
17 Benefits and Limitations Behavioral Health Covered services include inpatient and outpatient care for psychological or psychiatric conditions. You do not need a referral from your child s doctor to receive covered outpatient behavioral health services. Contact PsychCare, a company that contracts with VISTA to provide these services at All calls are confidential. A trained professional will help plan the care that is needed. Durable Medical Equipment and Prosthetic Devices Covered services include medically necessary equipment to treat your child s medical condition. Limitations: Must be provided by an authorized VISTA supplier. Covered prosthetic devices include artificial eyes and limbs. Low vision and telescopic lenses are not included. Hearing aids are covered only when medically needed to help with the treatment of a medical condition. Emergency Services Covered services include visits to an emergency room or other licensed facility needed right away due to an injury or sudden illness when delay could lead to permanent damage to the child s health. Limitation: Must use a VISTA facility or provider for emergency care unless the time to reach such facility or provider would mean the risk of damage to the child s health. Home Health Services Covered services include home visits by both registered and licensed practical nurses. Limitations: Skilled nursing services only Meals, housekeeping and personal comfort items are excluded Private duty nursing is limited to medically necessary conditions Services must be approved by VISTA Hospice Services Covered services include reasonable and necessary services for management of a terminal illness. 15

18 Limitations: Once a family decides on hospice services, other services to treat the terminal condition will not be covered Services needed for conditions totally unrelated to the terminal condition are covered if they would normally be covered by VISTA Inpatient Services Covered services provided for the medical care and treatment of a child when admitted as an inpatient to a hospital. Limitations: All admissions must be authorized by VISTA The length of stay shall be based on medical needs Room and board may be limited to semi-private rooms, unless a private room is medically necessary or semi-private rooms are not available Private duty nursing only if medically necessary Admissions for inpatient rehabilitation and physical therapy are limited to 15 days per Contract Year Maternity Services and Newborn Care Covered services include care for mother and newborn. The services include prenatal and postnatal care of the mother, nursery charges, and examination of the baby. Limitation: Infant is covered for up to three (3) days following birth or until the infant is transferred to another medical facility, whichever occurs first. Skilled Nursing Facility Coverage includes regular nursing services, therapy services, drugs, medical supplies and the use of the equipment furnished by the facility. Limitations: Must be provided by a VISTA participating facility. Member must need and receive skilled nursing services on a daily basis as ordered by a VISTA doctor; coverage limited to 100 days per Contract Year Specialized treatment centers and independent kidney disease treatment centers are excluded; private duty nurses, television and custodial care are excluded Admission for inpatient rehabilitation and physical therapy limited to 15 days per Contract Year Organ Transplantation Services Covered services include pre-transplant testing, transplant services, and post-transplant care. 16

19 Limitation: Coverage is available for transplants and medically related services if necessary within the guidelines set by the Organ Transplant Advisory Council or the Bone Marrow Transplant Advisory Panel. VISTA s Medical Director must approve the procedure and the facility. Outpatient Services Check-ups, testing, treatment, comfort care, and other services provided in the outpatient portion of a health facility. Limitation: Services must be provided by VISTA participating providers or upon referral Refractions (Vision Testing) Covered services include examination by a VISTA optometrist to determine the need for corrective lenses (eyeglasses). Limitations: Corrective lenses (eyeglasses) and frames are limited to one (1) pair every two (2) years unless head size or prescription changes Coverage is limited to the VISTA standard collection with plastic or SYL non-tinted lenses Substance Abuse Services Covered services include coverage for inpatient and outpatient care for drug and alcohol abuse including counseling and placement assistance. You do not need a referral from your child s doctor to receive covered substance abuse, detoxification and rehabilitation services. Contact PsychCare, a company that contracts with VISTA to provide these services at All calls are confidential. A trained professional will help plan the care that is needed. Therapy Services Covered services include physical, occupational, respiratory and speech therapy services for short-term rehabilitation. Limitations: 24 treatment sessions within 60 days of illness or injury 60 day period begins with the first treatment All treatments must be provided or authorized by VISTA participating providers Transportation Services Emergency transportation if medically necessary in response to an emergency. Authorizations VISTA requires members to contact Customer Service before scheduling certain services. 17
 Covered services include examination by a VISTA optometrist to determine the need")
20 Before your child receives some services, your child s doctor will contact VISTA for you. To be sure this has been done; you may also contact VISTA before your child has any of these services: All inpatient hospital admissions (non-emergency) Outpatient surgery (in a hospital setting or in a freestanding surgery center) Nursing Facility admissions Rehabilitation care (inpatient) Inpatient behavioral health, alcohol, or substance abuse treatment Home health care (nursing, physical therapy, occupational therapy, speech therapy, and infusion therapy) Hospice care Durable Medical Equipment (customized) All services provided by any non-vista provider/facility, except dialysis or emergencies Transplant evaluation and services Selected radiology services (example: x-rays, ultrasounds and MRI s) Case Management Program The Case Management Program helps those with complicated or serious conditions. VISTA watches the member population to find Healthy Kids members with conditions that case managers could help, such as those with heart disease, asthma or diabetes. Healthy Kids members with these conditions are assigned to a Case Management nurse. This nurse then works with the entire VISTA team to support your child s care. For more information about the Case Management services, please contact VISTA Customer Service at The 24-Hour Nurse Line ( ) is also available to answer your medical questions. Adverse Determinations/Denials It may be determined through Medical Management that a particular service is (or in the case of a review) not a covered benefit. You will be notified of any adverse determination/denial in writing. The notice will include: Reasons for the decision, including the clinical reason Instructions on how to have the decision reconsidered or appealed A notice of availability of the clinical review criteria used to make the determination (upon the request of you or your child s designee) What, if any, additional information is necessary for VISTA to make a decision on the appeal 18
 Hospice care Durable Medical Equipment (customized) All services provided by any non-vista provider/facility, except dialysis or")
21 Grievances and Appeals At VISTA, we are committed to member satisfaction. We will try to resolve any problems you may encounter over the telephone, but sometimes, additional steps are necessary. In these cases, we have a Grievance and Appeals Procedure available to you that provides channels for you to voice your concerns and have them reviewed and addressed at several different levels within the health plan. HOW TO FILE A GRIEVANCE VISTA s grievance and appeals process is designed to provide prompt, meaningful and confidential resolution of your concerns regarding quality of care, doctor behavior, office waiting times, claims payment, and other similar matters. What if you have a complaint about a doctor or your benefits? You can file a grievance if you are unhappy with your doctor. You can file an appeal if you want us to review the denial or limited authorization of a benefit. You can file a complaint verbally or in writing. You can file a grievance over the telephone by calling Monday through Friday from 8:00am to 7:00pm. If you want to file a complaint in writing, send it to: Coventry Health Care of Florida, Inc. dba VISTA Attention: Appeals and Grievance 1340 Concord Terrace Sunrise, FL With your permission, a doctor can file a complaint for you. VISTA will make sure that no action is taken against a doctor who files a complaint on your behalf. A grievance can be filed up to one year after the date of the incident. Upon request, VISTA employees can assist you with the filing of a grievance or appeal. All grievances will be addressed within 30 business days. APPEALS What if I disagree with a denial for a service request or payment of a claim? You can file an appeal within 30 days from the date VISTA issued the notice of action, or denial of a request for service or payment for services. You can file an appeal over the telephone by calling Monday through Friday from 8:00am to 7:00pm. If you file a verbal appeal, a written request must be filed within ten (10) business days after the health plan s receipt of the oral filing. If a written request is not received within 10 business days after the verbal appeal is filed, the appeal will be considered 19
22 withdrawn. If the appeal is sent to the health plan through the U.S. Mail, it must be received by the health plan within 15 days from the date on the notice of action. If you want to file an appeal in writing, send it to: Coventry Health Care of Florida, Inc. dba VISTA Attention: Appeals and Grievance 1340 Concord Terrace Sunrise, FL With your permission, a doctor can file an appeal for you. VISTA will make sure that no action is taken against a doctor who files an appeal on your behalf. Once your appeal has been reviewed, you will receive a written notice of the outcome within 60 days of VISTA s receipt of the original appeal. Extensions can only be granted when you request an extension, or when information regarding the Appeal must be collected from a nonparticipating provider or from outside the service area. If the original denial is overturned or decided in your favor you will be notified. If VISTA did not change its original decision, you will receive a letter that will explain the process for requesting another review. If you disagree with VISTA s decision, within 30 working days from the date you received the notice, you can request a review by the Grievance Review Panel and you have the right to appear in person to present your argument. If VISTA s original denial is upheld by the Grievance Review Panel, you may be liable for cost of continued benefits. What if your life, health or ability to regain maximum function is at risk? In these cases you can file an expedited appeal that will require VISTA to review your appeal within 72-hours. You can file an expedited appeal over the telephone by calling Monday through Friday from 8:00am to 7:00pm. If you want to file an appeal in writing, send it to: Coventry Health Care of Florida, Inc. dba VISTA Attention: Appeals and Grievance 1340 Concord Terrace Sunrise, FL Extensions can only be granted when you request an extension, or when information regarding the complaint must be collected from a non-participating provider or from outside the service area, only upon a showing of good cause by VISTA. State Appeals Subscriber Assistance Panel (SAP) Once you have completed VISTA s process, including the decision of the Grievance Review 20
The Healthy Michigan Plan Handbook
 The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). Eligibility for this program will be determined
The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). Eligibility for this program will be determined
The Healthy Michigan Plan Handbook
 The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). The Healthy Michigan Plan provides health
The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). The Healthy Michigan Plan provides health
Healthy Michigan MEMBER HANDBOOK
 Healthy Michigan MEMBER HANDBOOK 2014 The new name for Healthy 1 TABLE OF CONTENTS WELCOME TO HARBOR HEALTH PLAN.... 2 Who Is Harbor Health Plan?...3 How Do I Reach Member Services?...3 Is There A Website?....
Healthy Michigan MEMBER HANDBOOK 2014 The new name for Healthy 1 TABLE OF CONTENTS WELCOME TO HARBOR HEALTH PLAN.... 2 Who Is Harbor Health Plan?...3 How Do I Reach Member Services?...3 Is There A Website?....
Policy & Procedure AUTUMN RIDGE RESIDENTIAL CARE. March, 2013
 AUTUMN RIDGE RESIDENTIAL CARE Policy & Procedure HIPAA / PRIVACY NOTICE OF PRIVACY PRACTICES FUNCTION NUMBER PRIOR ISSUE EFFECTIVE DATE March, 2013 PURPOSE To ensure that a Notice of Privacy Practices
AUTUMN RIDGE RESIDENTIAL CARE Policy & Procedure HIPAA / PRIVACY NOTICE OF PRIVACY PRACTICES FUNCTION NUMBER PRIOR ISSUE EFFECTIVE DATE March, 2013 PURPOSE To ensure that a Notice of Privacy Practices
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES This notice describes how your medical information may be used and disclosed, and how you can get access to this information. Chaparral House is required to provide you this
NOTICE OF PRIVACY PRACTICES This notice describes how your medical information may be used and disclosed, and how you can get access to this information. Chaparral House is required to provide you this
WELCOME TO STRAITH HOSPITAL FOR SPECIAL SURGERY OUR PHILOSOPHY JOINT NOTICE OF PRIVACY PRACTICES
 WELCOME TO STRAITH HOSPITAL FOR SPECIAL SURGERY During your stay with us, our goal is to make your hospital experience as favorable as possible by providing information and open channels of communication.
WELCOME TO STRAITH HOSPITAL FOR SPECIAL SURGERY During your stay with us, our goal is to make your hospital experience as favorable as possible by providing information and open channels of communication.
Covered Benefits. Covered. Must meet current federal and state guidelines. Abortions. Covered. Allergy Testing. Covered. Audiology. Covered.
 Covered Benefits Services Abortions Allergy Testing Audiology Birth Control Services Blood & Blood Plasma Bone Mass Measurement (bone density) Case Management Chemotherapy Chiropractor Services (manipulation/subluxation)
Covered Benefits Services Abortions Allergy Testing Audiology Birth Control Services Blood & Blood Plasma Bone Mass Measurement (bone density) Case Management Chemotherapy Chiropractor Services (manipulation/subluxation)
Trillium Community Health Plan: Oregon Standard Bronze Plan Vital Coverage Period: 01/01/2015-12/31/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.trilliumchp.com or by calling 1-800-910-3906. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.trilliumchp.com or by calling 1-800-910-3906. Important
South Florida Community Care Network
 South Florida Community Care Network Enrollee Services for Enrollees in Broward County- NBHD & MHS 2900 Corporate Way Miramar, FL 33025 Toll Free Phone 1-866-899-4828, Fax 954-602-2810 Hours of Operation:
South Florida Community Care Network Enrollee Services for Enrollees in Broward County- NBHD & MHS 2900 Corporate Way Miramar, FL 33025 Toll Free Phone 1-866-899-4828, Fax 954-602-2810 Hours of Operation:
Physicians Plus Insurance Corporation Coverage Period: 01/01/2016 12/31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pplusic.com or by calling 1-800-545-5015. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pplusic.com or by calling 1-800-545-5015. Important Questions
HUMANA MEDICAL PLAN, INC:
 HUMANA MEDICAL PLAN, INC: Humana Platinum 1000/South Florida HUMx (HMOx) Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
HUMANA MEDICAL PLAN, INC: Humana Platinum 1000/South Florida HUMx (HMOx) Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Michigan Medicaid. Fee-For-Service. Handbook
 Michigan Medicaid Fee-For-Service Handbook Table of Contents Introduction Getting Care Services Michigan Medicaid Covers Non-Emergency Transportation Services Emergency Room Care Dental Pharmacy Paying
Michigan Medicaid Fee-For-Service Handbook Table of Contents Introduction Getting Care Services Michigan Medicaid Covers Non-Emergency Transportation Services Emergency Room Care Dental Pharmacy Paying
Assurant Health. Time Insurance Company. Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans
 Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans View Summary of Benefits and Coverage for an individual plan View Summary
Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans View Summary of Benefits and Coverage for an individual plan View Summary
Covered Services. Health and Development History. Nutritional assessment. visit per year from 2 to 20 years of age
 You may receive covered services that are performed, prescribed or directed by a participating provider. As an Enrollee, you must receive your healthcare services from a participating PCP or medical provider.
You may receive covered services that are performed, prescribed or directed by a participating provider. As an Enrollee, you must receive your healthcare services from a participating PCP or medical provider.
Health First Health Plans : HF Silver HMO Select 85 5248 Coverage Period: On or after 01/01/2015
 Health First Health Plans : HF Silver HMO Select 85 5248 Coverage Period: On or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Members Only Plan
Health First Health Plans : HF Silver HMO Select 85 5248 Coverage Period: On or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Members Only Plan
NOTICE OF PRIVACY PRACTICES. for Sony Pictures Entertainment Inc.
 NOTICE OF PRIVACY PRACTICES for Sony Pictures Entertainment Inc. [Para recibir esta notificación en español por favor llamar al número proviso en este documento.] This notice describes how medical information
NOTICE OF PRIVACY PRACTICES for Sony Pictures Entertainment Inc. [Para recibir esta notificación en español por favor llamar al número proviso en este documento.] This notice describes how medical information
Assurant Health. Time Insurance Company. Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans
 Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans View Summary of Benefits and Coverage for an individual plan View Summary
Assurant Health Time Insurance Company Summary of Benefits and Coverage for Assurant Health individual major medical Silver plans View Summary of Benefits and Coverage for an individual plan View Summary
EVIDENCE OF COVERAGE. A complete explanation of your plan. Health Net Green (HMO) January 1, 2010 December 31, 2010
 January 1, 2010 December 31, 2010") EVIDENCE OF COVERAGE A complete explanation of your plan Health Net Green (HMO) January 1, 2010 December 31, 2010 Important benefit information please read H0755_2010_0389 10/2009 January 1 December 31,
EVIDENCE OF COVERAGE A complete explanation of your plan Health Net Green (HMO) January 1, 2010 December 31, 2010 Important benefit information please read H0755_2010_0389 10/2009 January 1 December 31,
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 Gold 80 PPO Network Name: Exclusive Coverage Period: Beginning on or after 1/1/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type:
Gold 80 PPO Network Name: Exclusive Coverage Period: Beginning on or after 1/1/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type:
Group Health Cooperative: Gold
 Group Health Cooperative: Gold Coverage Period: 1/1/2016 to 1/1/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Group Plan Type: HMO This is only a summary. If
Group Health Cooperative: Gold Coverage Period: 1/1/2016 to 1/1/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Group Plan Type: HMO This is only a summary. If
$25 copay. One routine GYN visit and pap smear per 365 days. Direct access to participating providers.
 HMO-1 Primary Care Physician Visits Office Hours After-Hours/Home Specialty Care Office Visits Diagnostic OP Lab/X Ray Testing (at facility) with PCP referral. Diagnostic OP Lab/X Ray Testing (at specialist)
HMO-1 Primary Care Physician Visits Office Hours After-Hours/Home Specialty Care Office Visits Diagnostic OP Lab/X Ray Testing (at facility) with PCP referral. Diagnostic OP Lab/X Ray Testing (at specialist)
UnitedHealthcare Community Plan Florida Healthy Kids Member Handbook
 UnitedHealthcare Community Plan Florida Healthy Kids Member Handbook FLORIDA FHK-H-O-3/14-8/15-096 910-2103 3/14 2014 United HealthCare Services, Inc. Important Information UnitedHealthcare of Florida,
UnitedHealthcare Community Plan Florida Healthy Kids Member Handbook FLORIDA FHK-H-O-3/14-8/15-096 910-2103 3/14 2014 United HealthCare Services, Inc. Important Information UnitedHealthcare of Florida,
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at PacificSource.com or by calling 1-888-977-9299 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at PacificSource.com or by calling 1-888-977-9299 Important
UAB MY HEALTH REWARDS BIOMETRIC SCREENING PROGRAM NOTICE OF HEALTH INFORMATION PRACTICES
 UAB MY HEALTH REWARDS BIOMETRIC SCREENING PROGRAM NOTICE OF HEALTH INFORMATION PRACTICES 1 Effective Date: January 26, 2015 THIS NOTICE APPLIES TO THE UAB MY HEALTH REWARDS BIOMETRIC SCREENING PROGRAM
UAB MY HEALTH REWARDS BIOMETRIC SCREENING PROGRAM NOTICE OF HEALTH INFORMATION PRACTICES 1 Effective Date: January 26, 2015 THIS NOTICE APPLIES TO THE UAB MY HEALTH REWARDS BIOMETRIC SCREENING PROGRAM
Arizona State Retirement System Plan Benefit Information for Medicare Eligible Members
 Arizona State Retirement System Plan Benefit Information for Medicare Eligible Members Benefits Effective January 1, 2012 UHAZ12HM3349753_000 H0303_110818_013543 Summary of the UnitedHealthcare plans
Arizona State Retirement System Plan Benefit Information for Medicare Eligible Members Benefits Effective January 1, 2012 UHAZ12HM3349753_000 H0303_110818_013543 Summary of the UnitedHealthcare plans
Important Questions Answers Why this Matters:
 Minimum Coverage PPO Network Name: Exclusive Coverage Period: Beginning on or after 1/1/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
Minimum Coverage PPO Network Name: Exclusive Coverage Period: Beginning on or after 1/1/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan
SURGICAL CENTER FOR EXCELLENCE PATIENT INFORMATION
 As a person with pain, you have the right to: SURGICAL CENTER FOR EXCELLENCE PATIENT INFORMATION PAIN CARE BILL OF RIGHTS Have your report of pain taken seriously and to be treated with dignity and respect
As a person with pain, you have the right to: SURGICAL CENTER FOR EXCELLENCE PATIENT INFORMATION PAIN CARE BILL OF RIGHTS Have your report of pain taken seriously and to be treated with dignity and respect
Member Handbook and Evidence of Coverage
 2016 www.hpsm.org Medi-Cal Member Handbook and Evidence of Coverage Last Updated 11/10/ 2015 Last Updated 11/10/ 2015 Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU
2016 www.hpsm.org Medi-Cal Member Handbook and Evidence of Coverage Last Updated 11/10/ 2015 Last Updated 11/10/ 2015 Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU
Florida Hospital Silver AV94 HMO 80 1545 Coverage Period: On or after 01/01/2016
 Florida Hospital Silver AV94 HMO 80 1545 Coverage Period: On or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Members Only Plan Type: HMO This is
Florida Hospital Silver AV94 HMO 80 1545 Coverage Period: On or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Members Only Plan Type: HMO This is
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the plan document at www.pebcinfo.com or by calling 214-653-6161. Important Questions Answers
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the plan document at www.pebcinfo.com or by calling 214-653-6161. Important Questions Answers
PLEASE COMPLETE AND RETURN
 PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
Benefits At A Glance Plan C
 Benefits At A Glance Plan C HIGHLIGHTS OF WELFARE FUND BENEFITS WELFARE FUND BENEFITS IN BRIEF Medical and Hospital Benefits Empire BlueCross BlueShield Plan C-1 Empire BlueCross BlueShield Plan C-2 All
Benefits At A Glance Plan C HIGHLIGHTS OF WELFARE FUND BENEFITS WELFARE FUND BENEFITS IN BRIEF Medical and Hospital Benefits Empire BlueCross BlueShield Plan C-1 Empire BlueCross BlueShield Plan C-2 All
HUMANA EMPLOYERS HEALTH PLAN OF GEORGIA, INC
 HUMANA EMPLOYERS HEALTH PLAN OF GEORGIA, INC and HUMANA INSURANCE COMPANY: Humana National Preferred Silver 4250/6250 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage:
HUMANA EMPLOYERS HEALTH PLAN OF GEORGIA, INC and HUMANA INSURANCE COMPANY: Humana National Preferred Silver 4250/6250 Plan Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage:
BridgeSpan Health Company: BridgeSpan Oregon Standard Gold Plan MyChoice Northwest
 BridgeSpan Health Company: BridgeSpan Oregon Standard Gold Plan MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at
BridgeSpan Health Company: BridgeSpan Oregon Standard Gold Plan MyChoice Northwest Summary of Benefits and Coverage: What this Plan Covers & What it Costs Questions: Call 1 (855) 857-9943 or visit us at
Make sure you re covered for this season s fun in the sun
 A Coventry Health Care Newsletter Spring 2015 Iowa INSIDE THIS ISSUE Make sure you re covered for this season s fun in the sun Your privacy matters to us 2 6 Need help? Turn to our website When rules for
A Coventry Health Care Newsletter Spring 2015 Iowa INSIDE THIS ISSUE Make sure you re covered for this season s fun in the sun Your privacy matters to us 2 6 Need help? Turn to our website When rules for
PPO Hospital Care I DRAFT 18973
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.ibx.com or by calling 1-800-ASK-BLUE. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.ibx.com or by calling 1-800-ASK-BLUE. Important Questions
State of Florida Employees' Group Health Insurance Privacy Notice
 This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. The Health Insurance Portability and Accountability
This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. The Health Insurance Portability and Accountability
Western Health Advantage: City of Sacramento HSA ABHP Coverage Period: 1/1/2016-12/31/2016
 Coverage For: Self Plan Type: HMO This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or
Coverage For: Self Plan Type: HMO This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.westernhealth.com or
Healthy Benefits HMO 6850.0
 Coverage Period: Beginning on or after 1/1/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://www.capbluecross.com/sbcsia
Coverage Period: Beginning on or after 1/1/2016 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at https://www.capbluecross.com/sbcsia
Important Questions Answers Why this Matters: Individual $6,850 Family of 2 or more $13,700 What is the overall
 Molina Healthcare of California: Minimum Coverage HMO Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family I
Molina Healthcare of California: Minimum Coverage HMO Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family I
Harris County - Texas HIPAA Notice of Privacy Practices
 Harris County - Texas HIPAA Notice of Privacy Practices Effective Date: September 23, 2013. THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
Harris County - Texas HIPAA Notice of Privacy Practices Effective Date: September 23, 2013. THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
Health First Insurance : Large Group HF24 PPO 500 20 30 4000 OOP 1500/80/60 w Co-pa
 Health First Insurance : Large Group HF24 PPO 500 20 30 4000 OOP 1500/80/60 w Co-pa Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: On or after 01/01/2015 Coverage
Health First Insurance : Large Group HF24 PPO 500 20 30 4000 OOP 1500/80/60 w Co-pa Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: On or after 01/01/2015 Coverage
What is the overall deductible? Are there other deductibles for specific services?
 : MyPriority POS RxPlus Silver 1800 Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Subscriber/Dependent Plan Type:
: MyPriority POS RxPlus Silver 1800 Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Subscriber/Dependent Plan Type:
What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at http://www.aetnastudenthealth.com/uva or by calling 1-800-466-3027.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at http://www.aetnastudenthealth.com/uva or by calling 1-800-466-3027.
Coventry Health Care of Missouri: Silver $10 Copay Carelink from Coventry
 Coventry Health Care of Missouri: Silver $10 Copay Carelink from Coventry Coverage Period : 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a
Coventry Health Care of Missouri: Silver $10 Copay Carelink from Coventry Coverage Period : 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a
Notice of Privacy Practices
 Notice of Privacy Practices Effective September 20, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Notice of Privacy Practices Effective September 20, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Consumer s Right to Know About Health Plans in Rhode Island
 Consumer s Right to Know bout Health Plans in Rhode Island BasicBlue BLUE CROSS & BLUE SHIELD of RHODE ISLND January 1, 2016 Consumer Disclosure Safe and Healthy Lives in Safe and Healthy Communities Consumer
Consumer s Right to Know bout Health Plans in Rhode Island BasicBlue BLUE CROSS & BLUE SHIELD of RHODE ISLND January 1, 2016 Consumer Disclosure Safe and Healthy Lives in Safe and Healthy Communities Consumer
$0 See the chart starting on page 2 for your costs for services this plan covers. Are there other. deductibles for specific No.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at capbluecross.com or by calling 1-800-730-7219. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at capbluecross.com or by calling 1-800-730-7219. Important
Summary of Services and Cost Shares
 Summary of Services and Cost Shares This summary does not describe benefits. For the description of a benefit, including any limitations or exclusions, please refer to the identical heading in the Benefits
Summary of Services and Cost Shares This summary does not describe benefits. For the description of a benefit, including any limitations or exclusions, please refer to the identical heading in the Benefits
United States Fire Insurance Company: International Technological University Coverage Period: beginning on or after 9/7/2014
 or after 9/7/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: PPO This is only a summary. If you want more detail about your coverage and
or after 9/7/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: PPO This is only a summary. If you want more detail about your coverage and
Coventry Health Care of Illinois: Gold $10 Copay PPO Plan
 Coventry Health Care of Illinois: Gold $10 Copay PPO Plan Coverage Period : 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary. If you
Coventry Health Care of Illinois: Gold $10 Copay PPO Plan Coverage Period : 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary. If you
The Empire Plan: for Groups in Non-Grandfathered Plans Coverage Period: 01/01/2015 12/31/2015
 The Empire Plan: for Groups in Non-Grandfathered Plans Coverage Period: 01/01/2015 12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Important Questions Coverage for: Individual
The Empire Plan: for Groups in Non-Grandfathered Plans Coverage Period: 01/01/2015 12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Important Questions Coverage for: Individual
What is the overall deductible? Are there other deductibles for specific services? Is there an out-ofpocket
 Regence BlueCross BlueShield of Oregon: Preferred Coverage Period: 08/15/2015-08/14/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible Family
Regence BlueCross BlueShield of Oregon: Preferred Coverage Period: 08/15/2015-08/14/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible Family
HUMANA HEALTH PLAN, INC:
 HUMANA HEALTH PLAN, INC: Humana Silver 4600/Lexington UK Healthcare HMOx Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
HUMANA HEALTH PLAN, INC: Humana Silver 4600/Lexington UK Healthcare HMOx Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage
Trustmark Life Insurance Company: LewerMark Coverage Period: Beginning on or after Aug 1, 2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.lewermark.com or by calling 1-800-821-7710. Request a
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.lewermark.com or by calling 1-800-821-7710. Request a
TotalIndependence Silver Plan: Health Republic Insurance of New York Coverage Period: 01/01/2015 12/31/2015 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-888-990-5702. Important Questions Answers Why this
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-888-990-5702. Important Questions Answers Why this
Student Health Insurance Plan: Moravian College & Theological Seminary Coverage Period: 8/24/14-8/24/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bollingercolleges.com/moravian or by calling 1-855-338-8015.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.bollingercolleges.com/moravian or by calling 1-855-338-8015.
Coverage level: Employee/Retiree Only Plan Type: EPO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan documents at www.dbm.maryland.gov/benefits or by calling 410-767-4775
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan documents at www.dbm.maryland.gov/benefits or by calling 410-767-4775
Glossary of Health Coverage and Medical Terms
 Glossary of Health Coverage and Medical Terms This glossary defines many commonly used terms, but isn t a full list. These glossary terms and definitions are intended to be educational and may be different
Glossary of Health Coverage and Medical Terms This glossary defines many commonly used terms, but isn t a full list. These glossary terms and definitions are intended to be educational and may be different
Healthy Benefits PPO 6000.0 - Zero Cost Sharing Plan Variation Coverage Period: Beginning on or after 1/1/2014 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at capbluecross.com or by calling 1-800-730-7219. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at capbluecross.com or by calling 1-800-730-7219. Important
Summaries of Benefits and Coverage
 Summaries of Benefits and Coverage Tufts Health Direct ConnectorCare Plan Type I Tufts Health Direct ConnectorCare Plan Type II Tufts Health Direct ConnectorCare Plan Type III Tufts Health Direct Silver
Summaries of Benefits and Coverage Tufts Health Direct ConnectorCare Plan Type I Tufts Health Direct ConnectorCare Plan Type II Tufts Health Direct ConnectorCare Plan Type III Tufts Health Direct Silver
Consumer s Right to Know About Health Plans in Rhode Island
 Consumer s Right to Know bout Health Plans in Rhode Island BlueCHiP BLUE CROSS & BLUE SHIELD of RHODE ISLND January 1, 2016 Consumer Disclosure Safe and Healthy Lives in Safe and Healthy Communities Consumer
Consumer s Right to Know bout Health Plans in Rhode Island BlueCHiP BLUE CROSS & BLUE SHIELD of RHODE ISLND January 1, 2016 Consumer Disclosure Safe and Healthy Lives in Safe and Healthy Communities Consumer
Consumers Mutual Insurance of Michigan: Choice Medium Deductible Coverage Period: 01/01/2015 12/31/2015 Summary of Benefits and Coverage:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.consumersmutual.org or by calling 1-877-371-9112. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.consumersmutual.org or by calling 1-877-371-9112. Important
Land of Lincoln Health : Family Health Network LLH 3-Tier Bronze PPO Coverage Period: 01/01/2016 12/31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.landoflincolnhealth.org or by calling 1-844-FHN-4YOU.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.landoflincolnhealth.org or by calling 1-844-FHN-4YOU.
Important Questions Answers Why this Matters: $3,000/ person $6,000/family Benefits not subject to deductible include: preventive care.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-888-990-5702. Important Questions Answers Why this
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-888-990-5702. Important Questions Answers Why this
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-888-990-5702. Important Questions Answers Why this
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document by calling 1-888-990-5702. Important Questions Answers Why this
What is the overall deductible? Are there other deductibles for specific services? Is there an out-ofpocket
 Regence BlueShield: Regence Direct Gold with Dental, Vision, Individual Assistance Program Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What
Regence BlueShield: Regence Direct Gold with Dental, Vision, Individual Assistance Program Coverage Period: Beginning on or after 01/01/2014 Summary of Benefits and Coverage: What this Plan Covers & What
What is the overall deductible? $250 per person/$500 per family. Are there other deductibles for specific services? No.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
In-network: $5,000 per insured/ $10,000 per family per calendar year. Out-of-network: $10,000 per insured / $20,000
 Regence BlueShield of Idaho: Coverage Period: Beginning on or after 01/01/2014 Regence Individual Direct Bronze HSA Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for:
Regence BlueShield of Idaho: Coverage Period: Beginning on or after 01/01/2014 Regence Individual Direct Bronze HSA Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for:
Welcome to Iowa Medicaid. Toll Free: 1 800 338 8366. Fax: 515 725 1351 Email: IMEMemberServices@dhs.state.ia.us
 Welcome to Iowa Medicaid Inside this booklet, you will find information about the Iowa Medicaid Managed Health Care (MHC) Program. You still have full Medicaid coverage! Managed Health Care only changes
Welcome to Iowa Medicaid Inside this booklet, you will find information about the Iowa Medicaid Managed Health Care (MHC) Program. You still have full Medicaid coverage! Managed Health Care only changes
Coventry Health Care of Illinois: Silver $10 Copay Carelink St. John's
 Coventry Health Care of Illinois: Silver $10 Copay Carelink St. John's Coverage Period : 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary.
Coventry Health Care of Illinois: Silver $10 Copay Carelink St. John's Coverage Period : 01/01/2014-12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary.
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 : VIVA HEALTH Access Plan Coverage Period: 01/01/2015 12/31/2015 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document
: VIVA HEALTH Access Plan Coverage Period: 01/01/2015 12/31/2015 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document
Important Questions Answers Why this Matters: What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.studentplanscenter.com or by calling 1-800-756-3702.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.studentplanscenter.com or by calling 1-800-756-3702.
Highmark Delaware: Shared Cost Blue EPO 3000 Coverage Period: 01/01/2016-12/31/2016
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbsde.com or by calling 1-888-601-2242. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbsde.com or by calling 1-888-601-2242. Important
POS. Point-of-Service. Coverage You Can Trust
 POS Point-of-Service Coverage You Can Trust Issued by Capital Advantage Insurance Company, a Capital BlueCross subsidiary. Independent licensees of the Blue Cross and Blue Shield Association. Coverage
POS Point-of-Service Coverage You Can Trust Issued by Capital Advantage Insurance Company, a Capital BlueCross subsidiary. Independent licensees of the Blue Cross and Blue Shield Association. Coverage
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.consumersmutual.org or by calling 1-877-371-9112. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.consumersmutual.org or by calling 1-877-371-9112. Important
State Managed Care Network and CHP+ Prenatal Care Program
 CHP ASO EOC CHPA_18 1-1-09 State Managed Care Network and CHP+ Prenatal Care Program CHP+ Member Benefits Booklet Welcome! Welcome to the Child Health Plan Plus (CHP+) State Managed Care Network, where
CHP ASO EOC CHPA_18 1-1-09 State Managed Care Network and CHP+ Prenatal Care Program CHP+ Member Benefits Booklet Welcome! Welcome to the Child Health Plan Plus (CHP+) State Managed Care Network, where
Kaiser Permanente: Platinum 90 HMO
 Kaiser Permanente: Platinum 90 HMO Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO
Kaiser Permanente: Platinum 90 HMO Coverage Period: Beginning on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: HMO
Banner Health - Choice Plus Coverage Period: 1/1/2015-12/31/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the plan document at www.bannerbenefits.com by clicking on the Resources tab and then Plan
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the plan document at www.bannerbenefits.com by clicking on the Resources tab and then Plan
Member Handbook. Amerigroup Florida, Inc. Florida Healthy Kids Program 1-800-600-4441. www.myamerigroup.com/fl FL-MHB-0037-15B 10.
 Member Handbook Amerigroup Florida, Inc. Florida Healthy Kids Program FL-MHB-0037-15B 10.15 1-800-600-4441 www.myamerigroup.com/fl www.myamerigroup.com Dear Parent/Guardian: Welcome to Amerigroup. Thank
Member Handbook Amerigroup Florida, Inc. Florida Healthy Kids Program FL-MHB-0037-15B 10.15 1-800-600-4441 www.myamerigroup.com/fl www.myamerigroup.com Dear Parent/Guardian: Welcome to Amerigroup. Thank
HPSM Medi-Cal Benefits
 HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care Health care and insurance benefits can be difficult to understand. This guide introduces you to your basic Medi-Cal benefits, to the Health
HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care Health care and insurance benefits can be difficult to understand. This guide introduces you to your basic Medi-Cal benefits, to the Health
HIPAA NOTICE OF PRIVACY PRACTICES
 HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This HIPAA Notice
HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This HIPAA Notice
Health Insurance - How Does This Plan Work
 : Nationwide Mutual Insurance - Georgia Coverage Period: 01/01/2015 12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: HMO This
: Nationwide Mutual Insurance - Georgia Coverage Period: 01/01/2015 12/31/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family Plan Type: HMO This
Massachusetts. Coverage Period: 7/1/2013 6/30/2014 Coverage for: Individual + Family Plan Type: HMO
 Harvard Pilgrim Health Care, Inc. The Harvard Pilgrim Best Buy Tiered Copayment ChoiceNet HMO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Massachusetts Coverage Period: 7/1/2013
Harvard Pilgrim Health Care, Inc. The Harvard Pilgrim Best Buy Tiered Copayment ChoiceNet HMO Summary of Benefits and Coverage: What this Plan Covers & What it Costs Massachusetts Coverage Period: 7/1/2013
Health First HF24 6350 PPO 6133 Coverage Period: On or after 01/01/2016
 Health First HF24 6350 PPO 6133 Coverage Period: On or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Members Only Plan Type: PPO This is only a
Health First HF24 6350 PPO 6133 Coverage Period: On or after 01/01/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Members Only Plan Type: PPO This is only a
LGC HealthTrust: MT Blue 5-RX10/20/45 Coverage Period: 07/01/2013 06/30/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-870-3057. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.anthem.com or by calling 1-800-870-3057. Important Questions
Important Questions Answers Why this Matters: What is the overall deductible? Are there other deductibles for specific services?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.etf.wi.gov or by calling 1-877-533-5020. Important Questions
Regence BlueCross BlueShield of Oregon: Regence Oregon Standard Bronze Plan Coverage Period: Beginning on or after 01/01/2014
 Regence BlueCross BlueShield of Oregon: Regence Oregon Standard Bronze Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: Beginning on or after 01/01/2014 Coverage
Regence BlueCross BlueShield of Oregon: Regence Oregon Standard Bronze Plan Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: Beginning on or after 01/01/2014 Coverage
Coverage Period : 01/01/2014-12/31/2014
 Coventry Health and Life Insurance Company: Silver Integrated $10 Co-pay PPO Exchange Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary. If you want more detail
Coventry Health and Life Insurance Company: Silver Integrated $10 Co-pay PPO Exchange Summary of Benefits and Coverage: What this Plan Covers & What it Costs This is only a summary. If you want more detail
Important Questions Answers Why this Matters: What is the overall deductible?
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at austintexas.gov/benefits or by calling 512-974-3284. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at austintexas.gov/benefits or by calling 512-974-3284. Important
The Health and Benefit Trust Fund of the International Union of Operating Engineers Local Union No. 94-94A-94B, AFL-CIO. Notice of Privacy Practices
 The Health and Benefit Trust Fund of the International Union of Operating Section 1: Purpose of This Notice Notice of Privacy Practices Effective as of September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL
The Health and Benefit Trust Fund of the International Union of Operating Section 1: Purpose of This Notice Notice of Privacy Practices Effective as of September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL
Group Health Cooperative: The Hearthstone
 Group Health Cooperative: The Hearthstone Coverage Period: 7/1/2015 to 7/1/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Group Plan Type: HMO This is only a
Group Health Cooperative: The Hearthstone Coverage Period: 7/1/2015 to 7/1/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Group Plan Type: HMO This is only a
Highmark West Virginia: Blue Cross Blue Shield Shared Cost 1500, A Multi-State Plan
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbswv.com or by calling 1-888-601-2321 Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.highmarkbcbswv.com or by calling 1-888-601-2321 Important
Important Questions Answers Why this Matters: What is the overall deductible?
 Molina Healthcare of Ohio, Inc.: Molina Gold Plan Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family ǀ Plan
Molina Healthcare of Ohio, Inc.: Molina Gold Plan Coverage Period: 01/01/2016-12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual + Family ǀ Plan
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW THIS NOTICE OF PRIVACY PRACTICES
NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW THIS NOTICE OF PRIVACY PRACTICES
Important Questions Answers Why this Matters:
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at http://www.peoplenotprofits.com or by calling 1-888-990-6635.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at http://www.peoplenotprofits.com or by calling 1-888-990-6635.