PHARMACOLOGY OF COMMON ANTITHROMBOTICS KAMALES ARUMUGAM PRINCIPAL PHARMACIST ANTICOAGULATION WORKSHOP 19 TH SEP 2014
|
|
|
- Gwendoline Marsh
- 8 years ago
- Views:
Transcription
1 PHARMACOLOGY OF COMMON ANTITHROMBOTICS KAMALES ARUMUGAM PRINCIPAL PHARMACIST ANTICOAGULATION WORKSHOP 19 TH SEP 2014

2 INTRODUCTION Thrombus pathology Antiplatelet Anticoagulants HIT Switching Anticoagulants Fibrinolytics

3
4

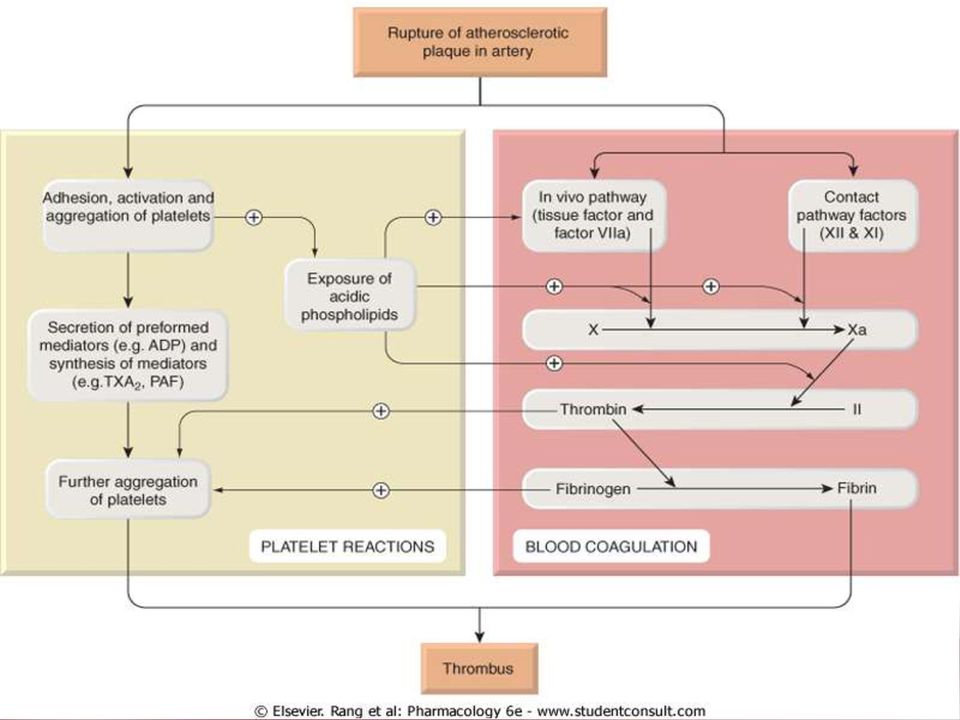
5 THROMBI PATHOLOGY ARTERIAL THROMBI VENOUS THROMBI FORMATION Artery Vein; tend to fragment creating an embolus INITIATION COMPOSITION Spontaneously or mechanical rupture of atherosclerotic plaques Mainly platelets, also contains fibrin & occasionally leukocytes & small amounts of coagulated erythrocytes Venous stasis or vascular injury after surgery or trauma Fibrin & erythrocytes KNOWN AS White thrombi Red thrombi MANIFESTS AS MI, Unstable angina, Ischaemic stroke, Peripheral artery disease e.g. acute limb ischaemia DVT, PE, AF related-thrombi

6 ANTITHROMBOTIC DRUGS

7 ANTIPLATELET DRUGS

8 ANTIPLATELET DRUGS



9

10 ANTIPLATELET DRUGS Aspirin P2Y 12 inhibitors: Clopidogrel Ticlopidine Thienopyridines Prasugrel Ticagrelor Dipyridamole Glycoprotein IIb/IIIa inhibitors: Abciximab Tirofiban Eptifibatide Antiplatelet drugs reduce mortality, risk of reinfarction & stroke


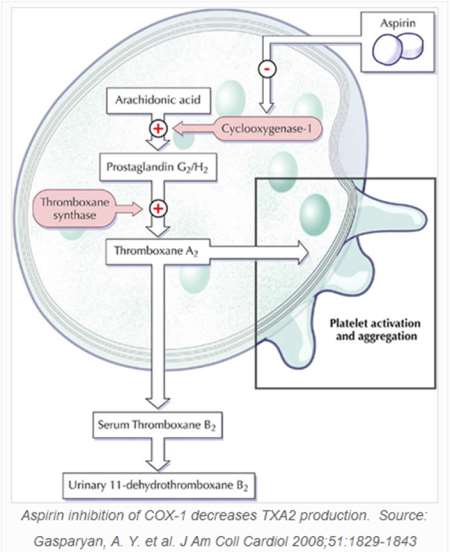
11 ASPIRIN MOA:

12 ASPIRIN ASPIRIN (ASA) PHARMACOKINETICS Action: rapid, peak plasma levels in 20 min Duration of action: 7-10 days Clearance: rapid Renal: caution in severe impairment; risk of bleeding & further deterioration of renal function INDICATIONS Acute MI, UA, Primary prevention of stroke & TIA, Secondary prevention of stroke, TIA & in IHD, Pain, Inflammation & fever DOSE Acute conditions: mg Long term: mg daily PRECAUTIONS ASA & NSAID allergies & aspirin-sensitive asthma Active peptic ulcer disease or other bleeding predispositions COMMON ADVERSE EFFECTS GI side effects (2 4x higher with ASA use; dose related) Asymptomatic blood loss Increased bleeding time PRACTICE POINTS No evidence that EC products decrease GI bleeding risk Patients with Hx of ASA-induced ulcer bleeding, clopidogrel causes more recurrent ulcer bleeding than ASA combined with PPI
 Asymptomatic blood loss Increased bleeding time PRACTICE POINTS No evidence that EC products decrease GI bleeding risk Patients with Hx of ASA-induced ulcer")
13 ADP P2Y 12 RECEPTOR ANTAGONISTS Clopidogrel, Ticlopidine, Prasugrel The active metabolites selectively inhibits the binding of adenosine diphosphate (ADP) to its platelet P2Y 12 receptor (irreversibly) and the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation

14 ADP P2Y 12 RECEPTOR ANTAGONISTS CLOPIDOGREL (PLAVIX ) PHARMACOKINETICS Action: rapid, peak plasma levels in 45 min Duration of action: 7-10 days Metabolised extensively in the liver INDICATIONS Prevention of vascular ischaemic evens in pts with symptomatic atherosclerosis, NSTEACS (with ASA), adjuvant to reperfusion for STEMI (with ASA), Prevention of thromboembolism after placement of stent DOSE Loading dose: mg Long term: 75mg daily PRECAUTIONS COMMON ADVERSE EFFECTS Combining clopidogrel with inhibitors of CYP2C19 or genetic lack of CYP2C19 activity may decrease clopidogrel's effectiveness in reducing the risk of CV events (evidence is conflicting) Diarrhoea, GI ulcers, dyspepsia, brusing, TTP (very rare) PRACTICE POINTS Optimal duration of treatment in ACS & after placement of coronary stent is debated; longer treatment is recommended with a DES than with a BMS
 Diarrhoea, GI ulcers, dyspepsia, brusing, TTP (very rare) PRACTICE POINTS Optimal duration of treatment in ACS")
15 ADP P2Y 12 RECEPTOR ANTAGONISTS TICLOPIDINE (TICLID ) PHARMACOKINETICS Action: peak plasma levels in 2 hours Duration of action: 7-10 days Metabolised extensively in the liver INDICATIONS DOSE Secondary prevention of ischaemic stroke and TIA in patients intolerant of or unresponsive to other antiplatelet drugs 250mg twice daily PRECAUTIONS COMMON ADVERSE EFFECTS Hematologic adverse reactions, including neutropenia, thrombocytopenia, TTP, aplastic anemia, agranulocytosis, pancytopenia, and leukemia, including fatalities, have been reported; monitoring recommended; therapy discontinuation may be necessary Diarrhoea, nausea, anorexia, vomiting, upper abdominal pain (tolerance may develop), mild-to-severe neutropenia PRACTICE POINTS Risk of neutropenia is greatest in the first 12 weeks of treatment; obtain FBC at baseline, then every 2 weeks for 4 months, then as indicated Stop ticlopidine if neutrophil count is <1.2x109/L or platelet count is <80x109/L; neutropenia is usually reversible on stopping ticlopidine
, mild-to-severe neutropenia PRACTICE POINTS Risk of neutropenia is greatest in the")
16 ADP P2Y 12 RECEPTOR ANTAGONISTS PRASUGREL (EFFIENT ) PHARMACOKINETICS Action: rapid, peak plasma levels in 30 mins Duration of action: 7 9 days; 5 days (depending loading/maintenance dose) Hydrolysed in the intestine INDICATIONS Prevention of atherothrombotic events (with ASA) in ACS (including STEMI and non-stemi) to be managed with PCI DOSE Give with low-dose ASA ( mg daily) Initially 60 mg, then 10 mg once daily >75 years or <60 kg: initially 60 mg, then 5 mg once daily PRECAUTIONS History of stroke or TIA contraindicated due to an increased risk of bleeding and stroke in trials Asian ethnicity may be at increased risk of bleeding COMMON ADVERSE EFFECTS PRACTICE POINTS Bleeding (may be severe and may cause anaemia) Hypersensitivity reactions (cross-reactivity can occur with other thienopyridines) In UA/NSTEMI patients, where coronary angiography is performed within 48 hours after admission, the loading dose should only be given at the time of PCI
 Hypersensitivity reactions (cross-reactivity can occur with")
17 ADP P2Y 12 RECEPTOR ANTAGONISTS Selective and reversibly binding P2Y 12 receptor antagonist that prevents ADP mediated P2Y 12 dependent platelet activation and aggregation

18 ADP P2Y 12 RECEPTOR ANTAGONISTS TICAGRELOR (BRILINTA ) PHARMACOKINETICS Action: rapid, peak plasma levels in 30 mins Platelet function recovery 3-4 days after cessation Metabolised in the liver by CYP3A4 INDICATIONS ACS (with aspirin) DOSE Give with low-dose ASA ( mg daily) Loading dose 180 mg, then 90 mg twice a day PRECAUTIONS Patients at risk of bradycardia (e.g. SSS without pacemaker, 2 nd or 3 rd -degree COMMON ADVERSE EFFECTS AV block) asymptomatic ventricular pauses Asthma, COPD ticagrelor may cause dyspnoea Weight <60 kg increases risk of bleeding Hyperuricaemia ticagrelor may increase uric acid concentration Treatment with CYP3A4 strong inhibitors contraindicated Bleeding (may be severe & cause anaemia), dyspnoea, nausea, diarrhoea, noncardiac chest pain, headache, raised uric acid concentration, raised creatinine concentration PRACTICE POINTS 12-month study: ticagrelor+asa more effective than clopidogrel+asa in preventing CV events in patients with ACS: Sig. reduction in MI & vascular death, but a non-sig. increase in stroke Incidence total major bleeding similar, rate of major IC haemorrhage was higher with ticagrelor

19 DIPYRIDAMOLE It inhibits the uptake of adenosine into the platelet & erythrocytes stimulate platelet adenylate cyclase & increase levels of platelet camp prevent activation and aggregation of platelet

20 DIPYRIDAMOLE DIPYRIDAMOLE PHARMACOKINETICS Action: peak 2 3 hours (CR) Extensively metabolized in the liver INDICATIONS Prevention of thromboembolism in patients with prosthetic heart valves (with warfarin) Secondary prevention of ischaemic stroke & TIA, including combination with ASA Cardiac stress testing (IV) DOSE Prevention of thromboembolism : PO mg daily in 3-4 doses Secondary prevention of stroke & TIA: PO 200mg CR twice daily PRECAUTIONS Vasodilatory effect (used with caution in patients with severe CAD) Beer s Criteria (short-acting dipyridamole): Not recommended, poorly tolerated & may cause orthostatic hypotension Aortic stenosis dipyridamole-induced vasodilation may increase pressure gradient across aortic valve and worsen organ perfusion. Unstable angina, recent MI use with caution; vasodilation may induce myocardial ischaemia. COMMON ADVERSE EFFECTS Headache, diarrhoea, nausea, vomiting, hot flushes, hypotension, tachycardia

21 GLYCOPROTEIN IIb/IIIa INHIBITORS Prevent binding of fibrinogen to platelet, by occupying glycoprotein IIb/IIIa receptor, thereby blocking platelet aggregation
22 GLYCOPROTEIN IIb/IIIa INHIBITORS ABCIXIMAB (REOPRO ) PHARMACOKINETICS Chimeric monoclonal antibody Action: within 10 mins Duration of action: Platelet function recovers over 48 hours Remains in the circulation for 15 days in a platelet-bound state INDICATIONS PTCA and intracoronary stenting Unstable angina refractory to treatment where PCI is planned DOSE PCI: IV bolus 250 mcg/kg before procedure, then 0.125mcg/kg/min for 12 hours Planned PCI in refractory unstable angina: Start hours before intervention; IV bolus of 250 mcg/kg, followed by infusion of 10 mcg/min; stop 1 hour after intervention PRECAUTIONS Abciximab infusion within 30 days increases risk & severity of thrombocytopenia Thrombocytopenia from previous abciximab increases risk of recurrence COMMON ADVERSE EFFECTS PRACTICE POINTS Bleeding, thrombocytopenia Give low-dose ASA & heparin infusion with abciximab Monitor baseline PT, APTT, CrCl, platelet count, Hb & HCT; after starting, monitor Hb & HCT at 12 & 24 hrs, & platelet count at 2 4 hrs & 24 hrs
23 GLYCOPROTEIN IIb/IIIa INHIBITORS EPTIFIBATIDE (INTEGRILIN ) PHARMACOKINETICS Action: immediate Duration of action: Return of platelet function 4 hours after stopping continuous inf Clearance: Renal INDICATIONS Unstable angina and non-stemi in high-risk patients Elective PCI with stenting DOSE PCI: IV bolus 180mcg/kg just before intervention, then 2nd bolus of 180mcg/kg 10 mins later. Start IV inf, 2mcg/kg/min, with first bolus until hospital DC or up to a max of hrs post intervention UA, non-stemi: IV bolus 180mcg/kg followed by 2mcg/kg/min IV inf for up to 72 hrs until initiation of CABG or DC from hospital. If PCI is performed during that time, continue inf for hrs after intervention for an overall max duration of 96 hrs PRECAUTIONS Renal: Same bolus but reduce inf to 1mcg/kg/min Hepatic: Avoid in patients with significant hepatic disease COMMON ADVERSE EFFECTS Bleeding, thrombocytopenia PRACTICE POINTS Give low-dose ASA and heparin infusion with eptifibatide Monitor PT, APTT, CrCl, platelet, Hb & HCT before treatment; monitor Hb, HCT and platelet within 6 hrs after start of treatment & at least once daily thereafter
24 GLYCOPROTEIN IIb/IIIa INHIBITORS TIROFIBAN (AGGRASTAT ) PHARMACOKINETICS Chimeric monoclonal antibody Action: rapid, within 30 mins Duration of action: Returns of platelet function within 8 hrs after discontinuation Clearance: Renal and biliary INDICATIONS DOSE PRECAUTIONS COMMON ADVERSE EFFECTS Unstable angina and non-stemi in high-risk patients IV 0.4mcg/kg/min for 30 minutes, followed by 0.1mcgkg/min for hrs Renal: Reduce dose by 50% when CrCl <30 ml/min Bleeding, thrombocytopenia PRACTICE POINTS Give low-dose ASA and heparin infusion with tirofiban Monitor PT, APTT, CrCl, platelet, Hb & HCT before treatment; monitor Hb, HCT and platelet within 6 hrs after start of treatment & at least once daily thereafter
25 ANTICOAGULANTS
26 ANTICOAGULANTS
27 ANTICOAGULANTS HISTORICAL DEVELOPMENT Oral Spoiled sweet clover Warfarin clinical use Dicoumarol discovered Warfarin / Vitamin K mechanism High / low dose Warfarin / INR Warfarin clinical trials Ximelagatran clinical trials Dabigatran Rivaroxaban Apixaban AZD s 1970s s 1990s Heparin discovered Heparin clinical use Continous heparin infusion/ aptt LMWH discovered LMWH clinical trials Pentasaccharide clinical trials Injection
28 ANTICOAGULANTS Heparins: UFH Enoxaparin Tinzaparin Warfarin Direct Thrombin Inhibitors: Dabigatran Bivalirudin Argatroban Lepirudin NA in Malaysia Melagatran Factor Xa Inhibitors: Fondaparinux Rivaroxaban Apixaban
29 HEPARIN (UFH) When heparin sodium is combined with antithrombin III (heparin cofactor), thrombosis is blocked through inactivation of Factor Xa and inhibition of prothrombin's conversion to thrombin (Factor IIa). This also prevents fibrin formation from fibrinogen during active thrombosis
30 HEPARINS HEPARIN (UFH) PHARMACOKINETICS Action: immediate Elimination T½: 1.5 hr (anticoagulation effect half-life) Metabolised in the liver; inactive metabolic products are excreted in the urine INDICATIONS Prevention of VTE & other thromboses in surgical and high-risk medical patients (including during procedures, eg haemodialysis) Treatment of VTE, ACS, peripheral arterial occlusion & disseminated intravascular coagulation (DIC) DOSE PRECAUTIONS COMMON ADVERSE EFFECTS Refer to PI/local protocols & indications for dose recommendations HIT Thrombocytopenia, bleeding, HIT, increased liver transferases PRACTICE POINTS Unexpectedly high APTT may be due to blood sample being taken from same limb as heparin infusion Preferred over LMWH in severe renal impairment Monitor APTT (6 hrs) after dose changes, platelet counts, HCT, signs & symptoms of bleeding
31 LMWH LMWH has greater capacity to potentiate factor Xa inhibition by antithrombin than thrombin because, with a mean molecular weight of , at least half of the LMWH chains are too short to bridge antithrombin to thrombin
32 LMWH ENOXAPARIN (CLEXANE ) PHARMACOKINETICS Action: anti-xa activity occurs 1 to 4 hours after injection Elimination T½: 4 5 hrs Metabolism: renal (40%) & hepatic INDICATIONS Prevention of VTE in surgical patients & in medical patients bedridden due to acute illness Treatment of venous thrombosis Prevention of extracorporeal thrombosis during haemodialysis Treatment of acute STEMI, non-stemi and unstable angina Treatment of PE DOSE Prophylaxis dose: mg once daily Treatment dose: 1mg/kg every 12 hrs Adjusted by weight & CrCl (if <30ml/min use 50% dose) PRECAUTIONS COMMON ADVERSE EFFECTS PRACTICE POINTS Caution in patients with renal impairment due to increased risk for bleeding; monitoring recommended (antifactor Xa) Bleeding, bruising and pain at injection site, hyperkalaemia, mild reversible thrombocytopenia, increased aminotransferases Consider heparin IV if an invasive procedure is anticipated as the anticoagulant effect diminishes more quickly after stopping
33 LMWH TINZAPARIN (INNOHEP ) PHARMACOKINETICS Action: peak plasma activity being observed after 4 to 6 hours Elimination T½: 1.5 hrs Excreted in urine primarily unchanged drug INDICATIONS Treatment of DVT and PE Prevention of postoperative DVT in patients undergoing general and orthopaedic surgery Prevention of extracorporeal thrombosis DOSE Prophylaxis dose: 75 anti Xa-units/kg/d or 3500 units/day Treatment dose: 175 anti Xa-units/kg/d PRECAUTIONS COMMON ADVERSE EFFECTS Caution in patients with renal or hepatic insufficiency; consider dose reduction Erythema, increased LFTs, localised pain, injection site hematoma
34 COMPARISONS BETWEEN UFH & LMWH ISSUES Bleeding incidence Protamine Renal impairment Severe HIT Osteoporosis General surgery (prevention) Orthopaedic surgery (prevention) DVT (treatment) NSTEACS VTE in cancer COMMENTS similar for heparin and LMWHs only partially effective in reversing effect of LMWHs risk of severe bleeding is higher with LMWHs lower with LMWHs; LMWHs should not be used as an alternative; cross-reactivity occurs in 90% of cases; incidence is even lower with danaparoid & it is used for treatment of HIT seems lower with LMWHs heparin & LMWHs have similar efficacy in preventing VTE LMWHs more effective than heparin or warfarin LMWHs as effective as heparin in preventing recurrent thromboembolism and in reducing overall mortality Enoxaparin appears to be slightly more effective than heparin in reducing the combined endpoint of death or MI but it increases the risk of major bleeding Long-term treatment with LMWHs (dalteparin) may be more effective than vitamin K antagonists
35 HIT Digital Ischemia in a Patient with Heparin-Induced Thrombocytopenia
36 HIT
37 HIT Occurs in <1% of patients with short-term use HIT should be suspected: Thrombocytopenia Thrombosis with thrombocytopenia Platelet count has fallen >50% Necrotic skin lesions at injection sites (heparin was started preceding 5-10 days) Diagnosis is initially made on clinical ground Assays with highest sensitivity and specificity may not be available & have slow turnaround time 1. Warkentin, TE, et al. Treatment and prevention of heparin-induced thrombocytopenia. ACCP Evidence-based clinical practice guidelines (8th edition) 2008;133 (6 Suppl): 340S..
38 HIT Delayed onset HIT has also occurred up to several weeks after stopping heparin May result in major ischaemic complications (eg stroke, limb ischaemia), bleeding or death Monitoring: Early recognition is important Baseline platelet count is a MUST Daily platelet count starting from Day 1 in patients with history of past heparin exposure within 3 months (occurs earlier if patient has been recently (<100 days) exposed to heparin) Otherwise, start on Day 4 Withhold heparin or LMWH if platelet count drops 30 50% below baseline and substitute alternative anticoagulant
39 HIT Treatment options: Lepirudin, Argatroban (both FDA approved) or Bivalirudin (limited data) Danaparoid (cross-reactivity 10%) Fondaparinux (weaker evidence) Warfarin alone should not be used Risk of causing venous limb gangrene and/or skin necrosis Safe to be use when patient is adequately and stably anticoagulated with a drug that reduces thrombosis & when platelet count is > 150,000/microL Prophylactic platelet transfusions should not be administered for patient with HIT who do not have active bleeding If heparin-induced thrombocytopenia (HIT) is confirmed, future use of heparin or LMWH is contraindicated
40 WARFARIN
41 ELIMINATION T½ OF VIT-K DEPENDANT PROTEINS PROTEIN T½ (hours) Factor VII 4 6 Factor IX 24 Factor X Factor II 60 Protein C 8 Protein S 30 Warfarin 40 (range 20 60)

42 LOADING DOSE VS MAINTENANCE DOSE
43 WARFARIN WARFARIN PHARMACOKINETICS Action: onset 24 hrs; peak 3 4 days; stabilised effect in days (ave days) Elimination T½: hrs (mean 40hrs) Metabolism: Hepatic (primarily via CYP2C9; minor pathway: CYP2C8, 2C18, 2C19, 1A2 & 3A4) INDICATIONS Prevention and treatment of VTE Prevention of thromboembolism in patients with prosthetic heart valves Prevention of stroke in patients with previous MI and increased embolic risk Prevention of stroke in non-valvular AF DOSE Follow local protocols & individualise according to TTR PRECAUTIONS Alcoholism contraindicated Compliance likely to be poor avoid unless supervised administration Protein C or protein S deficiency increases risk of skin necrosis COMMON ADVERSE EFFECTS Bleeding, skin necrosis (stop treatment), purple discolouration of toes, alopecia, fever, rash, nausea, vomiting, diarrhoea, hepatic dysfunction, allergic reactions, eg hypersensitivity PRACTICE POINTS Different brands are not bioequivalent and should not be interchanged Many drugs interactions; monitor the INR when changing drug treatment Consider use of a warning bracelet or necklace (Yayasan MedicAlert) Advise patients of the intended duration of anticoagulation, and the potential risks of stopping treatment without medical advice Review the need for continued warfarin treatment regularly
44 DIRECT THROMBIN INHIBITORS Reversibly inhibit both free and fibrin-bound thrombin, preventing conversion of fibrinogen to fibrin, preventing thrombus formation. Thrombin-induced platelet aggregation is also inhibited
45 DIRECT THROMBIN INHIBITORS DABIGATRAN (PRADAXA ) PHARMACOKINETICS Action: peak hrs Elimination T½: hrs Excretion: renal (primary); reduce dose in renal impairment INDICATIONS Prevention of VTE after elective total hip or knee replacement Non-valvular AF or high risk of stroke or systemic embolism DOSE Prevention of VTE after knee/hip replacement: initially 110mg within 1 4 hrs after surgery, then 220mg once daily; CrCl ml/min: 150 mg once daily Prevention of emboli in AF: 150mg BD; CrCl ml/min & >75 yrs: 110mg BD PRECAUTIONS GI haemorrhage within previous 12 months CI (more common than with warfarin in a clinical trial comparing their use in AF) Prosthetic heart valve CI COMMON ADVERSE EFFECTS Gastritis, dyspepsia, GI bleeding, oesophageal ulcers, increased liver enzymes & bilirubin PRACTICE POINTS Watch for drug interactions: verapamil, amiodarone, ketoconazole, P-gp inhibitors, clarithromycin, dronedarone, etc. Swallow capsule whole; oral bioavailability may be increased by 75 % when the pellets are taken without capsule shell; increased risk of bleeding
46 SWITCHING ANTICOAGULANTS (DABIGATRAN) SWITCHING From dabigatran to parenteral anticoagulant From parenteral anticoagulant to dabigatran From dabigatran to warfarin From warfarin to dabigatran RECOMMENDATIONS Prevention of VTE after knee/hip replacement: wait for 24 hours after the last dabigatran dose Prevention of emboli in AF: wait for 12 hours after the last dabigatran dose Start dabigatran within the 2 hours before the due time of the next dose of parenteral anticoagulant CrCl >50 ml/min: start warfarin 3 days before stopping dabigatran CrCl ml/min: start warfarin 2 days before stopping dabigatran CrCl ml/minute: start warfarin the day before stopping dabigatran Stop warfarin and start dabigatran when INR <2
47 FACTOR Xa INHIBITORS Selectively inhibit factor Xa, blocking thrombin production, conversion of fibrinogen to fibrin, and thrombus development
48 FACTOR Xa INHIBITORS FONDAPARINUX (ARIXTRA ) PHARMACOKINETICS Action: peak 3 hr Elimination T½: hr Excretion: renal (primary); may need to reduce dose in renal impairment INDICATIONS Prevention of VTE in high-risk orthopaedic surgery (hip fracture, knee or hip replacement) and abdominal surgery Treatment of VTE Treatment of high-risk unstable angina or non-stemi (NSTEACS) if PCI is not immediate DOSE PRECAUTIONS COMMON ADVERSE EFFECTS PRACTICE POINTS Prevention of VTE: 2.5mg SC once daily for 5 9 days; CrCl ml/min, 1.5mg once daily Treatment of VTE: <50 kg, 5mg SC once daily kg, 7.5mg SC once daily >100 kg, 10mg SC once daily >100 kg and CrCl ml/minute, initial 10mg SC, then 7.5mg SC once daily Treatment of high-risk NSTEACS: 2.5mg SC once daily Contraindicated when CrCl <30 ml/minute Thrombocytopenia, allergy NSTEACS additional dose of heparin must be given before an angiogram or PCI are performed
49 FACTOR Xa INHIBITORS APIXABAN (ELIQUIS ) PHARMACOKINETICS Action: peak 3 4 hrs Elimination T½: 12 hrs Excretion: hepatic & renal (30%) INDICATIONS Prevention of VTE following elective hip or knee replacement Non-valvular AF or high risk of stroke or systemic embolism DOSE Prevention of VTE after hip/knee replacement: 2.5mg BD Prevention of emboli in AF: 5mg BD PRECAUTIONS COMMON ADVERSE EFFECTS PRACTICE POINTS If at least 2 of: Weight <60 kg, age >80 years, SeCr>133 µmol/l, reduce dose to 2.5mg BD Nausea, thrombocytopenia, abnormal LFTs Apixaban is not indicated for patients with hip fracture (no clinical trial data
50 SWITCHING ANTICOAGULANTS (APIXABAN) SWITCHING From apixaban to parenteral anticoagulant (and vice versa) RECOMMENDATIONS Start at time of the next scheduled dose From apixaban to warfarin Give warfarin with apixaban for 2 days, then check INR before the next apixaban dose. Continue both drugs until INR >2. From warfarin to apixaban Stop warfarin and start apixaban when INR <2
51 FACTOR Xa INHIBITORS RIVAROXABAN (XARELTO ) PHARMACOKINETICS Action: peak 2 4 hrs Elimination T½: 5 12 hrs Excretion: Hepatic & renal (30%) INDICATIONS Prevention of VTE following elective hip or knee replacement Treatment of acute VTE and prevention of subsequent VTE Non-valvular AF or high risk of stroke or systemic embolism DOSE PRECAUTIONS COMMON ADVERSE EFFECTS Prevention of VTE after hip/knee replacement: 10mg once daily Treatment of acute VTE & prevention of subsequent VTE: 15mg BD for 3 weeks, then 20 mg once daily Prevention of emboli in AF: 20 mg once daily CrCl ml/minute: 15mg once daily Treatment with azoles (e.g. itraconazole) or HIV-PIs (e.g. ritonavir) CI Peripheral oedema, itch, skin blisters, muscle spasm PRACTICE POINTS Rivaroxaban & warfarin given together affect the INR more than additively: INR will be misleadingly high (e.g. up to 12) if measured <24 hours after the previous rivaroxaban dose; vitamin K treatment or reduction in warfarin dose is not required INR is not a measure of rivaroxaban's anticoagulant effect
52 SWITCHING ANTICOAGULANTS (RIVAROXABAN) SWITCHING From rivaroxaban to parenteral anticoagulant RECOMMENDATIONS Give first dose of parenteral anticoagulant when the next rivaroxaban dose would have been due. From rivaroxaban to warfarin Limited data. Give warfarin with rivaroxaban until INR >2; use standard warfarin dose for the first 2 days, then adjust dose according to INR. While both drugs are being taken, check INR at least 24 hours after the previous rivaroxaban dose. From parenteral anticoagulant to rivaroxaban Start rivaroxaban within the 2 hours before the due time of the next dose of parenteral anticoagulant or when an infusion is stopped. From warfarin to rivaroxaban Prevention of emboli in AF, stop warfarin and start rivaroxaban when INR <3 Treatment of DVT, stop warfarin and start rivaroxaban when INR <2.5
53 FIBRINOLYTICS
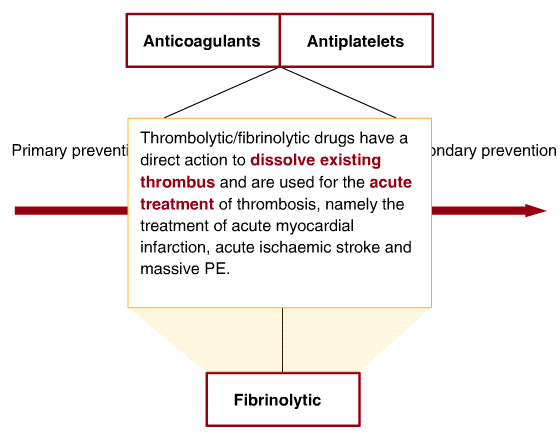
54 FIBRINOLYTICS
, reteplase and tenecteplase cleave plasminogen to produce plasmin, which")
55 FIBRINOLYTICS Streptokinase binds plasminogen, which converts free plasminogen to plasmin. Alteplase, urokinase, recombinant urokinase (r-uk), reteplase and tenecteplase cleave plasminogen to produce plasmin, which catalyses the breakdown of fibrin
56 FIBRINOLYTICS Non- fibrin specific Streptokinase (SK) Urokinase (UK) Fibrin-specific Alteplase (r-tpa) Tenecteplase Reteplase NA in Malaysia
57 FIBRINOLYTICS STREPTOKINASE (STREPTASE ) PHARMACOKINETICS Action: peak 20 mins Elimination T½: 80 mins Excretion: degraded to peptides & excreted renally INDICATIONS Treatment of acute MI within 12 hours of onset, with persistent STsegment elevation or recent left bundle-branch block DOSE Systemic: single dose of 1.5 million IU IV over 60 mins Local intracoronary: bolus of 20,000 IU followed by a maintenance infusion of 2,000 IU to 4,000 IU/min over 30 to 90 mins PRECAUTIONS Development of antibodies thus not if administered more than 5 days, particularly between 5 days and 12 months after initial treatment & effect reduced in patients with recent streptococcal infections CI in severe active bleeding disorders or disease states with an increased risk of bleeding COMMON ADVERSE EFFECTS PRACTICE POINTS Hypotension, tachycardia, bradycardia (initial infusion), haemorrhage Allergic reactions pre-treat with Hydrocortisone 100mg Active heparinisation neutralised with protamine sulphate APTT <2x normal control value before thrombolytic is started Warfarin treatment the INR <1.3 before starting the streptokinase
58 FIBRINOLYTICS UROKINASE PHARMACOKINETICS Action: rapid Elimination T½: mins Excretion: Hepatic INDICATIONS Thrombosed IV cannulae, central venous catheters and haemodialysis shunts Peripheral arterial thromboembolism DVT, PE DOSE Adjust individually depending on the clinical condition PRECAUTIONS COMMON ADVERSE EFFECTS PRACTICE POINTS CI in severe active bleeding disorders or disease states with an increased risk of bleeding e.g. severe uncontrolled hypertension, severe hepatic disease, severe thrombocytopenia. Bleeding, including bleeding at injection sites, intracerebral bleeding, internal bleeding (e.g. GI, genitourinary), transient hypotension Stop heparin before giving urokinase; check APTT (should <2X the normal control value before beginning thrombolytic treatment & before reinstituting heparin
59 FIBRINOLYTICS ALTEPLASE (ACTILYSE ) PHARMACOKINETICS Action: rapid Elimination T½: 4 5 mins Excretion: Hepatic INDICATIONS Acute STEMI Massive pulmonary embolism Acute ischaemic stroke DOSE PRECAUTIONS COMMON ADVERSE EFFECTS Adjust individually depending on the clinical condition Due to an increased haemorrhagic risk, treatment with platelet aggregation inhibitors should not be initiated within the first 24 hours following thrombolysis with alteplase Bleeding, including bleeding at injection sites, intracerebral bleeding, internal bleeding (e.g. GI, genitourinary), transient hypotension PRACTICE POINTS Avoid IM injections & other invasive procedures during thrombolytic treatment In case of severe bleeding not controlled by local pressure, stop infusion of thrombolytic; fibrinogen, platelets, coagulation factors, tranexamic acid may be useful (or protamine if heparin has been used)
60 FIBRINOLYTICS PHARMACOKINETICS INDICATIONS DOSE PRECAUTIONS COMMON ADVERSE EFFECTS TENECTEPLASE (METALYSE ) Action: rapid Elimination T½: mins Excretion: Hepatic Acute STEMI Based on body weight, with a maximum dose of 10,000 units CI in severe active bleeding disorders or disease states with an increased risk of bleeding Bleeding, including bleeding at injection sites, intracerebral bleeding, internal bleeding (eg GI, genitourinary), transient hypotension PRACTICE POINTS Avoid IM injections & other invasive procedures during thrombolytic treatment In case of severe bleeding not controlled by local pressure, stop infusion of thrombolytic; fibrinogen, platelets, coagulation factors, tranexamic acid may be useful (or protamine if heparin has been used)
61 SUMMARY The development of various anti-thrombotic agents has great impact in prevention & treatment of thrombosis-related diseases. Such agents markedly reduced death from heart attacks, the risk of stroke in people with atrial fibrillation and the risk of major stroke in patients with mini-strokes, pulmonary embolism etc. Emergence of new agents provides more options and convenience for patients in the future.
62 REFERENCES 1. Australian Medicines Hanbook Andrew D Blann et al. ABC of antithrombotic therapy. An overview of antithrombotic therapy. British Medical Journal 2001;325: Patrono C et al. Antiplatelet drugs: American College of Chest Physicians evidence-based clinical practice guidelines (8 th ed). Chest.2008;118: Jefrey l, Weitz, et al. New Antithrombotic Drugs. ACCP Evidence-based clinical practice guidelines (8 th edition) 2008; 133:234S 256S 5. Warkentin, TE, et al. Treatment and prevention of heparin-induced thrombocytopenia. ACCP Evidence-based clinical practice guidelines (8 th edition) 2008;133 (6 Suppl): 340S. 6. Ann K.Wittkowsky. New oral anticoagulants: a practical guide for clinicians. J Thromb Thrombolysis. Published online: 04 November Zikria and Ansell. Oral anticoagulation with factor Xa and thrombin inhibitors: on the threshold of change. Current Opinion in Hematology 2009, 16: electronic Medicines Compendium (emc) [Internet database]. Stocks House, 9 North Street, Leatherhead, Surrey, England KT22 7AX. Updated periodically 9. Baskin, JL, et al. Thrombolytic therapy for central venous catheter occlusion. Haematologica May : ;doi: /haematol
Anticoagulant therapy
 Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Update on Antiplatelets and anticoagulants. Outlines. Antiplatelets and Anticoagulants 1/23/2013. Timir Paul, MD, PhD
 Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia
 Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia Insertion, removal or presence of a catheter in selected sites can place a patient who is antithrombotic agent at risk for a local bleeding
Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia Insertion, removal or presence of a catheter in selected sites can place a patient who is antithrombotic agent at risk for a local bleeding
Time of Offset of Action The Trial
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant Amgen Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What I am Talking About
New Oral Anticoagulants. How safe are they outside the trials?
 New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Low Molecular Weight Heparin. All Wales Medicines Strategy Group (AWMSG) Recommendations and advice
 Recommendations and advice") Low Molecular Weight Heparin All Wales Medicines Strategy Group (AWMSG) Recommendations and advice Starting Point Low Molecular Weight Heparin (LMWH): Inhibits factor Xa and factor IIa (thrombin) Small
Low Molecular Weight Heparin All Wales Medicines Strategy Group (AWMSG) Recommendations and advice Starting Point Low Molecular Weight Heparin (LMWH): Inhibits factor Xa and factor IIa (thrombin) Small
3/25/14. To Clot or Not What s New In Anticoagulation? Clotting Cascade. Anticoagulant drug targets. Anita Ralstin, MS CNS CNP. Heparin.
 To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
East Kent Prescribing Group
 East Kent Prescribing Group Rivaroxaban (Xarelto ) Safety Information Approved by the East Kent Prescribing Group. Approved by: East Kent Prescribing Group (Representing Ashford CCG, Canterbury and Coastal
East Kent Prescribing Group Rivaroxaban (Xarelto ) Safety Information Approved by the East Kent Prescribing Group. Approved by: East Kent Prescribing Group (Representing Ashford CCG, Canterbury and Coastal
Traditional anticoagulants
 TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
Prescriber Guide. 20mg. 15mg. Simply Protecting More Patients. Simply Protecting More Patients
 Prescriber Guide 20mg Simply Protecting More Patients 15mg Simply Protecting More Patients 1 Dear Doctor, This prescriber guide was produced by Bayer Israel in cooperation with the Ministry of Health as
Prescriber Guide 20mg Simply Protecting More Patients 15mg Simply Protecting More Patients 1 Dear Doctor, This prescriber guide was produced by Bayer Israel in cooperation with the Ministry of Health as
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
Dabigatran (Pradaxa) Guidelines
 Guidelines") Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical
 Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Anticoagulation Dosing at UCDMC Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h
 Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
Heparin Induced Thrombocytopenia
 Heparin Induced Thrombocytopenia Ann-Marie Liberman B.Sc.Phm., ACPR Clinical Pharmacist, Cardiac Surgery Clinical Trials Pharmacist Royal Columbian Hospital Fraser Health Disclosure Participated in research
Heparin Induced Thrombocytopenia Ann-Marie Liberman B.Sc.Phm., ACPR Clinical Pharmacist, Cardiac Surgery Clinical Trials Pharmacist Royal Columbian Hospital Fraser Health Disclosure Participated in research
To aid practitioners in prescribing unfractionated heparin and low-molecular-weight heparins to patients.
 UNFRACTIONATED HEPARIN AND LOW-MOLECULAR-WEIGHT HEPARIN TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To aid practitioners in prescribing unfractionated heparin and low-molecular-weight
UNFRACTIONATED HEPARIN AND LOW-MOLECULAR-WEIGHT HEPARIN TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To aid practitioners in prescribing unfractionated heparin and low-molecular-weight
Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008:
 have been licensed in Ireland since 2008:") Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
Antiplatelet and Antithrombotics From clinical trials to guidelines
 Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below
 RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below") Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Disclosure. New Agents for Treatment of DVT. Prevalence of DVT VTE. Normal Hemostasis 7/17/2015. Mark Oliver, MD, RVT, RPVI,FSVU
 New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
New Agents for Treatment of DVT Disclosure PI Adopt and Amplify trials Mark Oliver, MD, RVT, RPVI,FSVU BMS and Pfizer Speaker VTE Venous Thromboembolism Recognized DVT s New : 170,000 Recurrent : 90,000
LAMC Reversal Agent Guideline for Anticoagulants 2013. Time to resolution of hemostasis (hrs) Therapeutic Options
 Therapeutic Options") LAMC Reversal Agent Guideline for Anticoagulants 2013 Medication resolution of hemostasis (hrs) Intervention Administration Instructions Heparin 3-4 Protamine 1mg IV for every 100 units of heparin Slow
LAMC Reversal Agent Guideline for Anticoagulants 2013 Medication resolution of hemostasis (hrs) Intervention Administration Instructions Heparin 3-4 Protamine 1mg IV for every 100 units of heparin Slow
The author has no disclosures
 Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Rivaroxaban (Xarelto ) by
 by") Essentia Health Med Moment Short Video Tune-Up A brief overview of a new medication, or important new medication information Rivaroxaban (Xarelto ) by Richard Mullvain RPH BCPS (AQC) Current - August 2011
Essentia Health Med Moment Short Video Tune-Up A brief overview of a new medication, or important new medication information Rivaroxaban (Xarelto ) by Richard Mullvain RPH BCPS (AQC) Current - August 2011
New Anticoagulants: When and Why Should I Use Them? Disclosures
 Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
Winship Cancer Institute of Emory University New Anticoagulants: When and Why Should I Use Them? Christine L. Kempton, MD, MSc Associate Professor of Pediatrics and Hematology and Medical Oncology Hemophilia
New Anticoagulants: What to Use What to Avoid
 New Anticoagulants: What to Use What to Avoid Bruce Davidson, MD, MPH Clinical Professor of Medicine Pulmonary and Critical Care Medicine Division University of Washington School of Medicine Seattle USA
New Anticoagulants: What to Use What to Avoid Bruce Davidson, MD, MPH Clinical Professor of Medicine Pulmonary and Critical Care Medicine Division University of Washington School of Medicine Seattle USA
Reversal of Antiplatelet and Anticoagulant Therapy: What You Need To Know. Ronald Walsh, MD Chief Medical Officer Community Blood Services
 Reversal of Antiplatelet and Anticoagulant Therapy: What You Need To Know Ronald Walsh, MD Chief Medical Officer Community Blood Services HEMOSTATIC PROCESS Initiation and formation of the platelet plug
Reversal of Antiplatelet and Anticoagulant Therapy: What You Need To Know Ronald Walsh, MD Chief Medical Officer Community Blood Services HEMOSTATIC PROCESS Initiation and formation of the platelet plug
To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
 DEEP VEIN THROMBOSIS: TREATMENT TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
DEEP VEIN THROMBOSIS: TREATMENT TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
2.5mg SC daily. INR target 2-3 30 mg SC q 12 hr or 40mg daily. 10 mg PO q day (CrCl 30 ml/min). Avoid if < 30 ml/min. 2.
. Avoid if < 30 ml/min. 2.") Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Anticoagulants in Atrial Fibrillation
 Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
QUICK REFERENCE. Mary Cushman 1 Wendy Lim 2 Neil A Zakai 1. University of Vermont 2. McMaster University
 QUICK REFERENCE Clinical Practice Guide on Antithrombotic Drug Dosing and Management of Antithrombotic Drug- Associated Bleeding Complications in Adults February 2014* Mary Cushman 1 Wendy Lim 2 Neil A
QUICK REFERENCE Clinical Practice Guide on Antithrombotic Drug Dosing and Management of Antithrombotic Drug- Associated Bleeding Complications in Adults February 2014* Mary Cushman 1 Wendy Lim 2 Neil A
Anticoagulation and Reversal
 Anticoagulation and Reversal John Howard, PharmD, BCPS Clinical Pharmacist Internal Medicine Affiliate Associate Clinical Professor South Carolina College of Pharmacy Disclosures I have no Financial, Industry,
Anticoagulation and Reversal John Howard, PharmD, BCPS Clinical Pharmacist Internal Medicine Affiliate Associate Clinical Professor South Carolina College of Pharmacy Disclosures I have no Financial, Industry,
DABIGATRAN ETEXILATE TARGET Vitamin K epoxide reductase WARFARIN RIVAROXABAN APIXABAN
 TARGET SPECIFIC ORAL ANTICOAGULANTS (TSOACs) This document is intended as a guideline only and should not replace sound clinical judgment Please refer to UNMH formulary in Lexicomp for approved use(s)
TARGET SPECIFIC ORAL ANTICOAGULANTS (TSOACs) This document is intended as a guideline only and should not replace sound clinical judgment Please refer to UNMH formulary in Lexicomp for approved use(s)
Appendix C Factors to consider when choosing between anticoagulant options and FAQs
 Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
The Role of the Newer Anticoagulants
 The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
Guideline for managing patients on a factor Xa inhibitor Apixaban (Eliquis ) or Rivaroxaban (Xarelto )
 or Rivaroxaban (Xarelto )") Guideline [Optional heading here. Change font size to suit] Document Number # QH-GDL-950:2014-2 Guideline for managing patients on a factor Xa inhibitor Apixaban (Eliquis ) or Rivaroxaban (Xarelto ) 1.
Guideline [Optional heading here. Change font size to suit] Document Number # QH-GDL-950:2014-2 Guideline for managing patients on a factor Xa inhibitor Apixaban (Eliquis ) or Rivaroxaban (Xarelto ) 1.
COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS. TARGET AUDIENCE: All Canadian health care professionals.
 COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS AND PHYSICIANS TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVES: To provide a comparison of the new
COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS AND PHYSICIANS TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVES: To provide a comparison of the new
Novel Anticoagulation Agents DISCLOSURES. Objectives ATRIAL FIBRILLATION TRIALS. NOAC Comparison 6/12/2015
 Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Comparison between New Oral Anticoagulants and Warfarin
 Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
DOACs. What s in a name? or TSOACs. Blood Clot. Darra Cover, Pharm D. Clot Formation DOACs work here. Direct Oral AntiCoagulant
 DOACs NOACs or TSOACs Generic Name DOACs Brand Name Mechanism of Action Direct Xa Inhibitor Direct Thrombin Inhibitor Dabigatran Pradaxa X Rivaroxaban Xarelto X Darra Cover, Pharm D Apixaban Eliquis X
DOACs NOACs or TSOACs Generic Name DOACs Brand Name Mechanism of Action Direct Xa Inhibitor Direct Thrombin Inhibitor Dabigatran Pradaxa X Rivaroxaban Xarelto X Darra Cover, Pharm D Apixaban Eliquis X
Management for Deep Vein Thrombosis and New Agents
 Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Management for Deep Vein Thrombosis and New Agents Mark Malesker, Pharm.D., FCCP, FCCP, FASHP, BCPS Professor of Pharmacy Practice and Medicine Creighton University 5 th Annual Creighton Cardiovascular
Thrombosis management: A time for change practical management with NOACs Dr Wala Elizabeth Medical Director, Bayer Healthcare
 Thrombosis management: A time for change practical management with NOACs Dr Wala Elizabeth Medical Director, Bayer Healthcare Kenya Association of Physicians Conference 10 th May 2013 New anticoagulants:
Thrombosis management: A time for change practical management with NOACs Dr Wala Elizabeth Medical Director, Bayer Healthcare Kenya Association of Physicians Conference 10 th May 2013 New anticoagulants:
New oral anticoagulants and antiplatelets: Where do they fit? Meredith Hollinger, PharmD BCPS
 New oral anticoagulants and antiplatelets: Where do they fit? Meredith Hollinger, PharmD BCPS Clinical Pharmacy Specialist, Cardiology September 2012 Objectives Describe the mechanisms of action for novel
New oral anticoagulants and antiplatelets: Where do they fit? Meredith Hollinger, PharmD BCPS Clinical Pharmacy Specialist, Cardiology September 2012 Objectives Describe the mechanisms of action for novel
Comparative Anticoagulation
 Comparative Anticoagulation Laurajo Ryan, PharmD, MSc, BCPS, CDE Clinical Associate Professor The University of Texas at Austin College of Pharmacy The University of Texas Health Science Center Pharmacotherapy
Comparative Anticoagulation Laurajo Ryan, PharmD, MSc, BCPS, CDE Clinical Associate Professor The University of Texas at Austin College of Pharmacy The University of Texas Health Science Center Pharmacotherapy
FDA Approved Oral Anticoagulants
 FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants
 Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers Relevant Licensed Indications
Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers Relevant Licensed Indications
Management of Patients on Anticoagulants. Haemostasis. Coagulation cascade. Cell-based model 19/11/2013
 Management of Patients on Anticoagulants National Coal Mining Museum 11 Nov 2013 Navneet Lad StR Special Care Dentistry Aims: Discuss the different anti-platelet drugs available. Discuss the new generation
Management of Patients on Anticoagulants National Coal Mining Museum 11 Nov 2013 Navneet Lad StR Special Care Dentistry Aims: Discuss the different anti-platelet drugs available. Discuss the new generation
Session 3 Topics. Argatroban. Argatroban. Drug Use and Adverse Effects. Laboratory Monitoring of Anticoagulant Therapy
 ~~Marshfield Labs Presents~~ Laboratory Monitoring of Anticoagulant Therapy Session 3 of 4 Michael J. Sanfelippo, M.S. Technical Director, Coagulation Services Session 3 Topics Direct Thrombin Inhibitors:
~~Marshfield Labs Presents~~ Laboratory Monitoring of Anticoagulant Therapy Session 3 of 4 Michael J. Sanfelippo, M.S. Technical Director, Coagulation Services Session 3 Topics Direct Thrombin Inhibitors:
Oral Anticoagulants: What s New?
 Oral Anticoagulants: What s New? Sallie Young, Pharm.D., BCPS (AQ-Cardiology) Clinical Pharmacy Specialist, Cardiology Penn State Hershey Medical Center syoung1@hmc.psu.edu August 2012 Oral Anticoagulant
Oral Anticoagulants: What s New? Sallie Young, Pharm.D., BCPS (AQ-Cardiology) Clinical Pharmacy Specialist, Cardiology Penn State Hershey Medical Center syoung1@hmc.psu.edu August 2012 Oral Anticoagulant
Guideline for Anticoagulation and Prophylaxis Using Low Molecular Weight Heparin (LMWH) in Adult Inpatients
 in Adult Inpatients") Guideline [Optional heading here. Change font size to suit] Document Number # QH-GDL-951:2015 Guideline for Anticoagulation and Prophylaxis Using Low Molecular Weight Heparin (LMWH) in Adult Inpatients
Guideline [Optional heading here. Change font size to suit] Document Number # QH-GDL-951:2015 Guideline for Anticoagulation and Prophylaxis Using Low Molecular Weight Heparin (LMWH) in Adult Inpatients
Dabigatran: Amber Drug Guidance for the prevention of stroke and systemic embolism in patients with non-valvular AF
 Leeds Dabigatran: Amber Drug Guidance for the prevention of stroke and systemic embolism in patients with non-valvular AF Amber Drug Level 3 (amber drug with monitoring requirements) We have started your
Leeds Dabigatran: Amber Drug Guidance for the prevention of stroke and systemic embolism in patients with non-valvular AF Amber Drug Level 3 (amber drug with monitoring requirements) We have started your
Guideline for managing patients on Dabigatran (Pradaxa ) Statewide
 Statewide") Guideline for managing patients on Dabigatran (Pradaxa ) Statewide Custodian: Medication Safety, Medicines Regulation and Quality medicationsafety@health.qld.gov.au Developed by Medication Safety, Medicines
Guideline for managing patients on Dabigatran (Pradaxa ) Statewide Custodian: Medication Safety, Medicines Regulation and Quality medicationsafety@health.qld.gov.au Developed by Medication Safety, Medicines
More information for patients and caregivers can be accessed at http://www.xarelto-us.com/.
 Janssen Research & Development Submits Application to U.S. FDA for XARELTO (rivaroxaban) to Reduce Secondary Cardiovascular Events in Patients with Acute Coronary Syndrome RARITAN, DECEMBER 29, 2011 -
Janssen Research & Development Submits Application to U.S. FDA for XARELTO (rivaroxaban) to Reduce Secondary Cardiovascular Events in Patients with Acute Coronary Syndrome RARITAN, DECEMBER 29, 2011 -
Anticoagulation at the end of life. Rhona Maclean Rhona.maclean@sth.nhs.uk
 Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Duration of Dual Antiplatelet Therapy After Coronary Stenting
 Duration of Dual Antiplatelet Therapy After Coronary Stenting C. DEAN KATSAMAKIS, DO, FACC, FSCAI INTERVENTIONAL CARDIOLOGIST ADVOCATE LUTHERAN GENERAL HOSPITAL INTRODUCTION Coronary artery stents are
Duration of Dual Antiplatelet Therapy After Coronary Stenting C. DEAN KATSAMAKIS, DO, FACC, FSCAI INTERVENTIONAL CARDIOLOGIST ADVOCATE LUTHERAN GENERAL HOSPITAL INTRODUCTION Coronary artery stents are
NHS FORTH VALLEY RIVAROXABAN AS TREATMENT FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN ADULTS
 NHS FORTH VALLEY RIVAROXABAN AS TREATMENT FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN ADULTS Date of First Issue 01/12/ 2012 Approved 15/11/2012 Current Issue Date 29/10/2014 Review Date 29/10/2016
NHS FORTH VALLEY RIVAROXABAN AS TREATMENT FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN ADULTS Date of First Issue 01/12/ 2012 Approved 15/11/2012 Current Issue Date 29/10/2014 Review Date 29/10/2016
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM OPTIONAL CE ADVANCED LEVEL (EMTP, PHRN, ECRN) August 2013. Anticoagulants
 August 2013. Anticoagulants") MCHENRY WESTERN LAKE COUNTY EMS SYSTEM OPTIONAL CE ADVANCED LEVEL (EMTP, PHRN, ECRN) August 2013 Anticoagulants Anticoagulants are agents that prevent the formation of blood clots. Before we can talk about
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM OPTIONAL CE ADVANCED LEVEL (EMTP, PHRN, ECRN) August 2013 Anticoagulants Anticoagulants are agents that prevent the formation of blood clots. Before we can talk about
Speaker Disclosure. Outline. Pharmacist Objectives. Patient Case. Outline 9/4/2014
 Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS mpitlick@stlcop.edu Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS mpitlick@stlcop.edu Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Critical Bleeding Reversal Protocol
 Critical Bleeding Reversal Protocol Coagulopathy, either drug related or multifactorial, is a major contributing factor to bleeding related mortality in a variety of clinical settings. Standard therapy
Critical Bleeding Reversal Protocol Coagulopathy, either drug related or multifactorial, is a major contributing factor to bleeding related mortality in a variety of clinical settings. Standard therapy
Stop the Bleeding: Management of Drug-induced Coagulopathy. Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery
 Stop the Bleeding: Management of Drug-induced Coagulopathy Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery Objectives Discuss contemporary management of warfarin reversal in patients
Stop the Bleeding: Management of Drug-induced Coagulopathy Stacy A. Voils, PharmD, BCPS Critical Care Specialist, Neurosurgery Objectives Discuss contemporary management of warfarin reversal in patients
An#- Coagulant An#- Thrombo#c An#- Platelet Drugs
 An#- Coagulant An#- Thrombo#c An#- Platelet Drugs 1 ANTICOAGULANT CLASSES INHIBITORS OF CLOTTING FACTOR SYNTHESIS WARFARIN (COUMADIN ) Rivaroxaban (Xarelto ) INHIBITORS OF THROMBIN HEPARIN, LEPIRUDIN (REFLUDAN
An#- Coagulant An#- Thrombo#c An#- Platelet Drugs 1 ANTICOAGULANT CLASSES INHIBITORS OF CLOTTING FACTOR SYNTHESIS WARFARIN (COUMADIN ) Rivaroxaban (Xarelto ) INHIBITORS OF THROMBIN HEPARIN, LEPIRUDIN (REFLUDAN
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults
 Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis )
: Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis )") Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis ) The contents of this CPG are to be used as a guide. Healthcare professionals
Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis ) The contents of this CPG are to be used as a guide. Healthcare professionals
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013
 Clinical Practice Guideline August 2013") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation. Joy Wahawisan, Pharm.D., BCPS April 25, 2012
 New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation
 Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
A practice tool for the new oral anticoagulants
 Peer-reviewed A practice tool for the new oral anticoagulants Anne Massicotte, BPharm, MSc Although warfarin has been the king of oral anticoagulation for the past few decades, its reign is now jeopardized
Peer-reviewed A practice tool for the new oral anticoagulants Anne Massicotte, BPharm, MSc Although warfarin has been the king of oral anticoagulation for the past few decades, its reign is now jeopardized
How To Compare The New Oral Anticoagulants
 Disclosures The New Oral Anticoagulants: Are they better than Warfarin? Alan P. Agins, Ph.D. does not have any actual or potential conflicts of interest in relation to this CE activity. Alan Agins, Ph.D.
Disclosures The New Oral Anticoagulants: Are they better than Warfarin? Alan P. Agins, Ph.D. does not have any actual or potential conflicts of interest in relation to this CE activity. Alan Agins, Ph.D.
Xarelto (Rivaroxaban): Effective in a broad spectrum. Joep Hufman, MD Medical Scientific Liason
: Effective in a broad spectrum. Joep Hufman, MD Medical Scientific Liason") Xarelto (Rivaroxaban): Effective in a broad spectrum Joep Hufman, MD Medical Scientific Liason Xarelto : Effective in a broad spectrum Introduction Therapeutic areas SPAF VTE Prevention VTE treatment Practical
Xarelto (Rivaroxaban): Effective in a broad spectrum Joep Hufman, MD Medical Scientific Liason Xarelto : Effective in a broad spectrum Introduction Therapeutic areas SPAF VTE Prevention VTE treatment Practical
CHADS score of 5 or 6 Recent (within 3mo) stroke or TIA Rheumatic valvular heart disease CHADs score of 3 or 4
 stroke or TIA Rheumatic valvular heart disease CHADs score of 3 or 4") LAMC Department of Pharmacy Services: ANTICOAGULATION: Surgical Intervention Table 1: Classification of Surgical interventions according to bleeding risk t required to discontinue anticoagulation Dental
LAMC Department of Pharmacy Services: ANTICOAGULATION: Surgical Intervention Table 1: Classification of Surgical interventions according to bleeding risk t required to discontinue anticoagulation Dental
Cardiology Medications New Drugs, New Guidelines
 Cardiology Medications New Drugs, New Guidelines Ken Kester, PharmD, JD Pharmacy Team Leader Nebraska Heart Hospital August 4, 2014 Cardiology Medications Objectives The attendee will understand Indications,
Cardiology Medications New Drugs, New Guidelines Ken Kester, PharmD, JD Pharmacy Team Leader Nebraska Heart Hospital August 4, 2014 Cardiology Medications Objectives The attendee will understand Indications,
Warfarin and Novel Anti-Coagulants: Management Before and After the Cath Lab
 Warfarin and Novel Anti-Coagulants: Management Before and After the Cath Lab Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 28, 2015 2:30 pm I have no disclosures. Stroke risk reduction in
Warfarin and Novel Anti-Coagulants: Management Before and After the Cath Lab Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 28, 2015 2:30 pm I have no disclosures. Stroke risk reduction in
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. A. Prescriptions That Require Prior Authorization
 MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants
MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants
Getting smart about dyspnea and life saving drug therapy in ACS patients. Kobi George Kaplan Medical Center Rehovot
 Getting smart about dyspnea and life saving drug therapy in ACS patients Kobi George Kaplan Medical Center Rehovot 78 year old female Case description Presented with resting chest pain and dyspnea Co morbidities:
Getting smart about dyspnea and life saving drug therapy in ACS patients Kobi George Kaplan Medical Center Rehovot 78 year old female Case description Presented with resting chest pain and dyspnea Co morbidities:
Thrombosis and Hemostasis
 Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Anticoagulation Therapy Update
 Anticoagulation Therapy Update JUDY R. WALLING, FNP-BC ARRHYTHMIA MANAGEMENT MUSC CARDIOLOGY Outline Who do we anticoagulate? Review classes of Anticoagulants Review examples of Anticoagulants Review CHADS2
Anticoagulation Therapy Update JUDY R. WALLING, FNP-BC ARRHYTHMIA MANAGEMENT MUSC CARDIOLOGY Outline Who do we anticoagulate? Review classes of Anticoagulants Review examples of Anticoagulants Review CHADS2
2/17/2015 ANTICOAGULATION UPDATE OBJECTIVES BRIEF REVIEW: CLASSES OF ORAL ANTICOAGULANTS
 ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
ANTICOAGULATION UPDATE C AR R I E P AL M E R, D N P, RN, AN P - BC OBJECTIVES At the end of the presentation, the NP will be able to: Identify new indications for target-specific oral anticoagulants (TSOACs),
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM
 Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
The Brave New (Anticoagulant) World
 World") The Brave New (Anticoagulant) World Diane M. Birnbaumer, M.D., FACEP Emeritus Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA
The Brave New (Anticoagulant) World Diane M. Birnbaumer, M.D., FACEP Emeritus Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA
Breadth of indications matters One drug for multiple indications
 Breadth of indications matters One drug for multiple indications Sylvia Haas, MD, PhD Formerly of the Technical University of Munich Munich, Germany Disclosures: Sylvia Haas 1 Novel oral anticoagulants:
Breadth of indications matters One drug for multiple indications Sylvia Haas, MD, PhD Formerly of the Technical University of Munich Munich, Germany Disclosures: Sylvia Haas 1 Novel oral anticoagulants:
Program Objectives. Why Use Anticoagulants? 6/5/2014
 Larry Reis RPh CGP FASCP Prepared June 2014 for NADONA REIS RXCARE CONSULTING Reisrxcare@comcast.net 1 Program Objectives Discuss complications of current anticoagulant Rx Identify risks of using anticoagulants
Larry Reis RPh CGP FASCP Prepared June 2014 for NADONA REIS RXCARE CONSULTING Reisrxcare@comcast.net 1 Program Objectives Discuss complications of current anticoagulant Rx Identify risks of using anticoagulants
Venous Thromboembolic Treatment Guidelines
 Venous Thromboembolic Treatment Guidelines About the NYU Venous Thromboembolic Center (VTEC) The center s mission is to deliver advanced screening, detection, care, and management services for patients
Venous Thromboembolic Treatment Guidelines About the NYU Venous Thromboembolic Center (VTEC) The center s mission is to deliver advanced screening, detection, care, and management services for patients
The speakers have attested that their presentation will be free of all commercial bias toward a specific company and its products.
 Update on New Anticoagulants (Apixaban, Dabigatran and Rivaroxaban) Patient Safety Daniel B. DiCola, MD and Paul Ament,, Pharm.D Excela Heath, Latrobe, PA Disclosures: Paul Ament discloses that he receives
Update on New Anticoagulants (Apixaban, Dabigatran and Rivaroxaban) Patient Safety Daniel B. DiCola, MD and Paul Ament,, Pharm.D Excela Heath, Latrobe, PA Disclosures: Paul Ament discloses that he receives
Antiplatelet and Antithrombotic Therapy. Dr Curry Grant Stroke Prevention Clinic Quinte Health Care
 Antiplatelet and Antithrombotic Therapy Dr Curry Grant Stroke Prevention Clinic Quinte Health Care Disclosure of Potential for Conflict of Interest Dr. F.C. Grant Atrial Fibrillation FINANCIAL DISCLOSURE:
Antiplatelet and Antithrombotic Therapy Dr Curry Grant Stroke Prevention Clinic Quinte Health Care Disclosure of Potential for Conflict of Interest Dr. F.C. Grant Atrial Fibrillation FINANCIAL DISCLOSURE:
Committee Approval Date: September 12, 2014 Next Review Date: September 2015
 Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
EMMC Guide on Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults. February, 2013
 EMMC Guide on Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults February, 2013 1 Quick Index To Reversal Recommendations Anti-Platelet Medications Page P2Y12
EMMC Guide on Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults February, 2013 1 Quick Index To Reversal Recommendations Anti-Platelet Medications Page P2Y12
GUIDELINES IN ANTIPLATELET AND ANTICOAGULATION RX IN CARDIAC SURGERY
 BLOOD CONSERVATION STRATEGIES IN CARDIAC SURGERY: MORE IS BETTER GUIDELINES IN ANTIPLATELET AND ANTICOAGULATION RX IN CARDIAC SURGERY DIMITRIOS V. AVGERINOS MD, PhD, FACS, FACC Department of Cardiac Surgery,
BLOOD CONSERVATION STRATEGIES IN CARDIAC SURGERY: MORE IS BETTER GUIDELINES IN ANTIPLATELET AND ANTICOAGULATION RX IN CARDIAC SURGERY DIMITRIOS V. AVGERINOS MD, PhD, FACS, FACC Department of Cardiac Surgery,
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM
 NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. A. Prescriptions That Require Prior Authorization
 MEDICAL ASSISTANCE HBOOK I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants which meet any of the following conditions
MEDICAL ASSISTANCE HBOOK I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants which meet any of the following conditions
TSOAC Initiation Checklist
 Task Establish appropriate dose based on anticoagulant selected, indication and patient factors such as renal function. Evaluate for medication interactions that may necessitate TSOAC dose adjustment.
Task Establish appropriate dose based on anticoagulant selected, indication and patient factors such as renal function. Evaluate for medication interactions that may necessitate TSOAC dose adjustment.
What You Should NOAC About the New Anticoagulants. Dr Calum Young Cardiologist
 What You Should NOAC About the New Anticoagulants Dr Calum Young Cardiologist Overview The Burden of AF What s Wrong With Warfarin? The Era of NOACs NOACs in New Zealand Clinical Trials with NOACs Potential
What You Should NOAC About the New Anticoagulants Dr Calum Young Cardiologist Overview The Burden of AF What s Wrong With Warfarin? The Era of NOACs NOACs in New Zealand Clinical Trials with NOACs Potential
Failure or significant adverse effects to all of the alternatives: Eliquis and Xarelto
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
STROKE PREVENTION IN ATRIAL FIBRILLATION. TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: ABBREVIATIONS: BACKGROUND:
 STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
The Anti coagulated Patient: The Cardiologist s View. February 28, 2015
 The Anti coagulated Patient: The Cardiologist s View February 28, 2015 Conflicts Dr. McMurtry has no conflicts to disclose. CanMeds Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS
The Anti coagulated Patient: The Cardiologist s View February 28, 2015 Conflicts Dr. McMurtry has no conflicts to disclose. CanMeds Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS
New Anticoagulants: Are we Ready to Replace Warfarin? Carole Goodine, RPh Horizon Health Network Stroke Conference 2011
 New Anticoagulants: Are we Ready to Replace Warfarin? Carole Goodine, RPh Horizon Health Network Stroke Conference 2011 Warfarin Decreases stroke risk by 60-70% Superior to ASA and ASA plus clopidogrel
New Anticoagulants: Are we Ready to Replace Warfarin? Carole Goodine, RPh Horizon Health Network Stroke Conference 2011 Warfarin Decreases stroke risk by 60-70% Superior to ASA and ASA plus clopidogrel
Rivaroxaban for the treatment of Deep Vein Thrombosis in patients unsuitable for vitamin K antagonists
 Rivaroxaban for the treatment of Deep Vein Thrombosis in patients unsuitable for vitamin K antagonists Traffic light classification- Amber 2 specialist initiation Information sheet for Primary Care Prescribers
Rivaroxaban for the treatment of Deep Vein Thrombosis in patients unsuitable for vitamin K antagonists Traffic light classification- Amber 2 specialist initiation Information sheet for Primary Care Prescribers
Xarelto (rivaroxaban) Prescriber Guide November 2012
 Prescriber Guide November 2012") Xarelto (rivaroxaban) Prescriber Guide November 2012 Simple Protection for More Patients 2 Xarelto Prescriber Guide Patient Alert Card 4 Dosing Recommendations 4 Dosing in patients with atrial fibrillation
Xarelto (rivaroxaban) Prescriber Guide November 2012 Simple Protection for More Patients 2 Xarelto Prescriber Guide Patient Alert Card 4 Dosing Recommendations 4 Dosing in patients with atrial fibrillation