Discuss differences in pharmacokinetics and pharmacodynamics in the elderly Describe key considerations associated with anticoagulation in elderly
|
|
|
- Eunice Francine Murphy
- 8 years ago
- Views:
Transcription
1 Giovanni Lares, PharmD Anticoagulation Clinic, Internal Medicine, ACC October 30,

2 Discuss differences in pharmacokinetics and pharmacodynamics in the elderly Describe key considerations associated with anticoagulation in elderly patients Apply cultural sensitivity concepts to engage in discussions related to anticoagulation in elderly patients Determine an optimal anticoagulation regimen in an elderly patient Identify risks and benefits associated with new anticoagulation agents 2

3 Increase in clotting factors I, V, VIII, IX, XIIIa Increased platelet activity Increased IL 6 increased fibrinogen, PAI 1, CRP, platelet aggregation 3

4 Decreased serum albumin Increased serum concentration of protein bound drugs Increased total body fat Increased Vd of lipophilic drugs Decreased Vd for hydrophilic drugs Comorbidities (e.g. heart failure, diabetes, etc) Decreased hepatic first pass metabolism Decreased liver mass, perfusion Increased bioavailability of some drugs Impaired phase 1 metabolism Decreased renal excretion Increased bioavailability of some drugs Drug Metab Rev 2009;41:67 4

5 Treatment/prevention of thrombosis DVT, PE Prevention of stroke in patients with artificial heart valves Lifelong anticoagulation indicated in patients with mechanical valves Prevention of stroke in patients with atrial fibrillation (AF) and concomitant risk factors CHADS 2 score 1 5
 and concomitant risk factors")
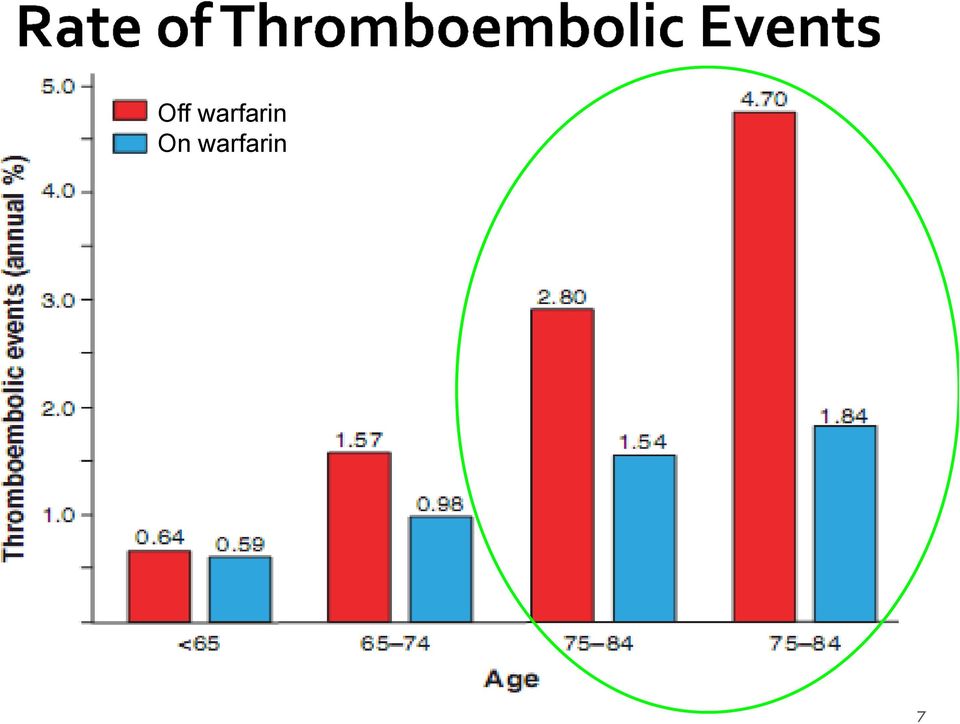
6 Atrial fibrillation is highly prevalent in older adults 1.5% of adults aged 60 to 70 years 10% of adults aged >80 years AF increases the risk of stroke 4 to 5 fold, across all age groups Risk of stroke attributable to AF increases with age 1.5% risk in ages 50 to 59 years 23.5% in ages 80 to 89 years Strokes in AF are more severe and disabling, and associated with high mortality ~50% at 1 year Circulation 2011;123:

7 Off warfarin On warfarin 7
8 CHADS 2 Congestive Heart Failure = 1 point Hypertension = 1 point Age >75 years = 1 point Diabetes = 1 point Stroke or TIA = 2 points CHA 2 DS 2 VASC Congestive Heart Failure = 1 point Hypertension = 1 point Age >75 years = 2 points Diabetes = 1 point Stroke/TIA/systemic thromboembolism = 2 points Vascular disease = 1 point Age years = 1 point Sex Category (female) = 1 point Moderate-high risk: 2 points Low risk: 0 1 point 8
 = 1 point Moderate-high risk: 2 points Low risk: 0 1")
9 Despite its benefit in elderly patients, warfarin is underutilized Used in only one third of eligible patients >85 years despite lack of contraindications Providers & Patients Physicians underestimate stroke prevention by as much as 22% and overestimate bleeding risk by as much as 670% AF patients aged years, when educated on risk/benefits, 61% chose warfarin, 47% of those not on warfarin would have chosen it Interview study of physicians and patients with high risk of stroke Minimum number of strokes prevented (100 pts/2y) to justify warfarin was lower for patients than for physicians (1.8 vs. 2.5, p=0.009) Maximum number of bleeds acceptable to patients (100 pts/2y) was higher than for physicians (17.4 vs. 10.3, p<0.001) Ann Intern Med 1999;131: BMJ 2000;320: BMJ 2001;323:1-7 9
 Maximum number of bleeds acceptable to patients (100 pts/2y) was higher than for physicians (17.4 vs. 10.3, p<0.")
10 HAS BLED Score (AF) Hypertension = 1 point Abnormal renal/hepatic function = 1 point 1 point for each Stroke = 1 point Bleeding history or anemia = 1 point Labile INR = 1 point Elderly (age > 75 years) = 1 point Drugs (NSAIDs, antiplatelet, EtOH) = 1 point 1 point for each High risk (> 4%/year) 4 points Moderate risk (2 4%/year) 2 3 points Low risk (< 2%/year) 0 1 point HEMHORR(2)HAGES Score Hepatic or renal disease = 1 point 1 point for each Ethanol abuse = 1 point Malignancy = 1 point Older age (>75 years) = 1 point Reduced platelet count/function = 1 point Platelets<75,000, use of antiplatelets, NSAID Rebleeding = 2 points Hypertension = 1 point Anemia = 1 point Genetic factors = 1 point CYP2C9*2, CYP2C9*3 Excessive fall risk = 1 point Alzheimer s, Parkinson s, etc. Stroke = 1 point Chest 2010;138(5):

11 Patients >80 years II Chest 2010;138(5): Circulation 2007;115:

12 Limited data in elderly patients Risk ranges per 100 person years Increased risk with INR>4, first 90 days of warfarin use Risk of intracranial hemorrhage (ICH) is about 0.5% per year with INR 2 3 Increased risk: SBP 160mmHg, DBP 90mmHg (4 fold), concurrent high dose ASA Circulation 2007;115: Ann Intern Med1994;120:
, concurrent")
13 Fall risk is frequently listed as a barrier to anticoagulation in the elderly 33% of people >65 fall each year Average number of falls is 1.8 per year A Markov decision model using 49 published studies: Average stroke risk 6%, average fall risk 33%, life expectancy average 13 years Conclusion: A patient with AF would have to fall 295 times in one year for the risk of anticoagulation to outweigh its benefits Arch Intern Med 1999;159:

14 57 elderly patients enrolled in an anticoagulation clinic were screened with the mini mental state exam (MMSE): Conclusion: The presence of cognitive impairment should not necessarily preclude the use of warfarin in elderly patients enrolled in an anticoagulation clinic. Drugs Aging 2012; 29(4):

15 15

16 Tablet Strength Color 1mg 2mg 2.5mg 3mg 4mg 5mg 6mg 7.5mg 10mg Pink Purple Green Tan Blue Peach Teal Yellow White 16

17 Mechanism of Action Interferes with the production of vitamin-k dependent clotting factors (II, VII, IX, and X) by inhibiting vitamin K oxide reductase Route PK PO Onset of anticoagulant effect: h Full therapeutic effect: 5 7 days Duration: 2 5 days Metabolism: CYP2C9, CYP1A2, CYP3A4 Adverse Effects Skin necrosis and limb gangrene 17

18 Chest 2012; 141(2):e44s-e88s 18

19 Warfarin interferes with the production of clotting factors from their inactive form it has no effect on existing, active clotting factors Anticoagulant activity relies on the natural catabolism of existing clotting factors and their corresponding half lives. Protein Half-Life (hr) VII 4 6 IX X II Protein C 9 Protein S 60 19

20 Consider warfarin 2.5mg daily in the following: Age >75 years old BMI<18.5, Body weight <50kg CHF Liver disease Clinical hyperthyroidism GI, genitourinary, or CNS bleed within last 2 months Concomitant meds known to increase warfarin sensitivity E.g. amiodarone High bleeding risk 20

21 Drug Drug interactions Major: Antibiotics, NSAIDs, steroids, OCs, Amiodarone EtOH, smoking Warfarin Disease interactions Warfarin Diet interactions Consistency in vitamin K intake, NOT avoidance 21
22 Complete blood count Monitor for possible bleeding complications PT and INR Monitor for therapeutic effectiveness 22
23 Advantages (relative to warfarin) Less interactions with drugs and foods No routine monitoring; fixed dosing Reduced risk of intracranial hemorrhage Faster onset Disadvantages (relative to warfarin) No readily available test to monitor dosing No antidote Dosage adjustment for CKD III IV; CKD V contraindicated Limited data in older patients with comorbidities Cost Increased risk of stroke with abrupt discontinuation Black Box warning 23
24 Mechanism of Action Approved Indications Dosing Dabigatran* (Pradaxa ) Direct Thrombin Inhibitor Non-valvular AF 110mg BID 150mg BID Rivaroxaban (Xarelto ) Factor Xa inhibitor Non-valvular AF DVT/PE treatment DVT prophylaxis 10mg daily 15mg daily 20mg daily Apixaban (Eliquis ) Factor Xa inhibitor Non-valvular AF 2.5mg BID 5mg BID Metabolism Renal Renal/Hepatic Renal Drug-Drug Interactions P-gp inhibitor CYP3A4 substrate P-gp inhibitor CHADS2 studied CYP3A4 substrate P-gp inhibitor *Listed on 2012 Beers Criteria as Use with caution due to increased risk of bleeding in adults 75 years, lack of evidence of safety in CrCl<30ml/min NEJM 2009; 361: , NEJM 2011;365:883-90, NEJM 2011;365:
25 RE LY (Dabigatran) ROCKET AF (Rivaroxaban) ARISTOTLE: (Apixaban) Inclusion Criteria AF + 1 of: TIA/CVA, LVEF <40%, or HF Age 75 or DM, HTN, or CAD AF and prior TIA /CVA/systemic embolus or AF and CHADS 2 2 or AF and Age 75 or plus DM, HTN, or CAD AF and CHADS 2 1 Exclusion Criteria Valvular disease CVA within 14 days CrCl<30ml/min Active liver disease Pregnancy Valvular disease/prosthetic valve CVA within 14 days or severe CVA within 3 months CrCl <30 ml per minute Known significant liver disease Pregnancy Condition with bleeding predisposition Aspirin >100 mg qd Valvular disease/prosthetic valve CVA within 7 days CrCl <25 ml per minute Condition with bleeding predisposition Aspirin >165 mg qd, or aspirin plus clopidogrel 25
26 Outcome (RR ± 95% CI) RE-LY (Dabigatran 150mg BID) ROCKET AF (Rivaroxaban 20mg/day) ARISTOTLE (Apixaban 5mg BID) Warfarin TTR 64% 55% 62.2% Stroke/Systemic 0.66 ( ) 0.88 ( ) 0.79 ( ) Embolic Event Ischemic stroke 0.76 ( ) 0.94 ( ) 0.92 ( ) Hemorrhagic 0.26 ( ) 0.59 ( ) 0.51 ( ) stroke Major bleeding 0.93 ( ) 1.04 ( ) 0.69 ( ) Intracranial hemorrhage 0.40 ( ) 0.67 ( ) 0.42 ( ) NEJM 2009; 361: NEJM 2011;365: NEJM 2011;365:
27 Close monitoring & lifestyle modification when using warfarin Management of excessive anticoagulation Control of hypertension Interventions to reduce the risk of falls Avoid NSAIDs Treatment of GI pathology (Ulcers, H. Pylori) Close attention to patients with cognitive impairment Interventional procedures Catheter ablation Left atrial appendage closure devices (still being investigated) Surgical MAZE and LAA resection Treatment decisions are not final they should evolve and adapt as patient s risk factors and therapy goals change. 27
28 28
29 Circulation 2011;123:e269-e367 29
30 ACC/AHA/ESC 2011 Focused Update Recommendation: CHADS 2 = 0 May also use with CHADS 2 = 1, though warfarin is preferred Use in addition to clopidogrel in patients with AF in whom warfarin therapy is considered unsuitable due to patient preference or assessment of patient s ability to safely sustain anticoagulation Aspirin and low intensity warfarin (INR<2) not recommended Circulation 2011;123:e269-e367 Lancet 1996;348:633 30
31 Circulation 2011;123:e269-e367 31
32 32
33 AA is a healthy 72 year old male with a history of non valvular atrial fibrillation and hypertension. He has been on warfarin for 10 years (TTR 70%) and is interested in starting Pradaxa. He is currently taking the following medications: Hydrochlorothiazide 25mg daily Amiodarone 200mg daily Warfarin 2.5mg QHS Pertinent labs (10/30/13): <98 Hct/Hgb/PLT: 40.6/14.0/ INR 2.0 BP: 132/79 HR: 65 Ht: 6 0 Wt: 82kg 33
34 Stroke Risk: CHA 2 DS 2 VASC = 2 (HTN, age) 2.2% risk of stroke Bleed Risk: HAS BLED = 1 (low risk) Is this patient eligible for Pradaxa? Non valvular afib CrCl=48.9mL/min CrCl>30mL/min: dabigatran 150mg BID CrCl 15 30mL/min: dabigatran 75mg BID CrCl<15mL/min: not recommended 34
35 The decision has been made to start AA on Pradaxa. How do you instruct him to start? Pradaxa should be started when INR<2 INR = 2.0 on 10/30/13 Have patient skip tonight s warfarin dose, start Pradaxa tomorrow evening 35
36 AA returns to the clinic several weeks later. He states that he developed a fungal infection a couple days ago and was prescribed ketoconazole 200mg daily by the local urgent care facility. Dose adjustments for concomitant administration with strong P gp inhibitors (dronedarone, ketoconazole) CrCl 30 50mL/min: Decrease dose to dabigatran 75mg BID No dose adjustments necessary for other P gp inhibitors (verapamil, amiodarone, quinidine, clarithromycin) 36
37 A few months later, AA returns to the clinic. He states that his insurance will lapse at the end of the month and he will no longer be able to afford Pradaxa. How do you proceed? CrCl>50mL/min: start warfarin 3 days before discontinuing Pradaxa CrCl 30 50mL/min: start warfarin 2 days before discontinuing Pradaxa CrCl 15 30mL/min: start warfarin 1 day before discontinuing Pradaxa 37
38 BB is an 84 year old woman recently discharged from the hospital for new onset atrial fibrillation. She is discharged with warfarin 3mg daily and referred to your office for INR monitoring. PMH: HTN, OA, DM Home Meds: Aspirin 81mg daily, amlodipine 10mg daily, metoprolol 50mg daily, Ibuprofen 400mg Q8hr prn Social Hx: Ambulates with walker, occasional mechanical falls, grand daughter helps with medications Pertinent Labs (10/30/13): <108 Hct/Hgb/PLT: 40.6/14.0/ INR 2.2 BP: 153/85 HR: 65 Ht: 5 2 Wt: 50kg 38
39 Stroke Risk: CHA 2 DS 2 VASC = 5 HTN, age, DM, female 6.7% risk of stroke Bleed Risk: HAS BLED = 4 (high risk) HTN, elderly (age>75 years), Drugs (Aspirin, Ibuprofen) Is the patient a candidate for novel anticoagulants? Dabigatran: not recommended in patients >75 years Rivaroxaban, apixaban No absolute contraindications, though caution with: Advanced age, low body weight, concomitant antiplatelet/nsaid use, renal insufficiency (CrCl 33mL/min) 39
40 What can be done to minimize risk in this patient? OA: switch ibuprofen to acetaminophen (gold standard) 500mg q 6 hr prn BP 153/85: optimize BP medication Increased blood pressure increases risk of ICH Increase metoprolol 100mg daily Minimize fall risk Close INR follow up (1 2 weeks) Recently started on warfarin at hospital discharge 40
41 BB returns to clinic 2 weeks later for anticoagulation follow up. Her INR is 2.3 and her BP is now 135/80. She reports that the acetaminophen given at last visit has not helped with her OA. She states that she is now bed ridden all day and is requesting to switch back to her ibuprofen. 41
42 Arch Intern Med 2002;162:
43 Three weeks following her last visit, BB returns to the clinic for anticoagulation follow up. Her INR is 6.1. What questions should be asked? Are you experiencing any bleeding? What dose of warfarin are you taking? Did you take an extra warfarin dose by mistake? Have any of your medications changed? What about over thecounter medications? Have you had any alcohol recently? Have you experienced any illness recently? E.g. vomiting, diarrhea, flu symptoms 43
44 BB denies any signs and symptoms of bleeding, denies doubling up on her warfarin dose, recent alcohol or medication changes, or recent illness. Both she and her granddaughter insist that she has been taking warfarin 3mg daily since her initial hospital discharge 5 weeks ago. How do you proceed? 44
45 GOAL INR 2 3 INR WEEKLY WARFARIN DOSE < % %* 2 3 NO CHANGE %* HOLD X 1 DOSE, THEN 5 15% HOLD X 1 2 DOSES, THEN 10 20% HOLD X 3 4 DOSES, RECHECK INR, THEN 25 50% >10.0 RECOMMEND VITAMIN K PO 2.5 5MG 45
46 BB returns to clinic 3 days later as instructed for anticoagulation follow up. Her INR is 3.1 and she still denies any signs or symptoms of bleeding. What is her new warfarin dose? Previous dose: warfarin 3mg daily (21mg/wk) New dose should be ~30% less than original weekly dose 0.7 x 21mg/wk = 14.7mg/wk Warfarin 1.5mg daily except 3mg on Mon/Wed/Fri (15mg/wk) 1.5mg x 4 days = 6mg 3mg x 3 days = 9mg INR follow up: 1 week 46
47 Assess need for oral anticoagulation (CHA2DS2VASC) Assess bleeding risk (HAS BLED) Is there a compelling indication for a newer anticoagulant? Patient refuses warfarin Patient has unstable INRs on warfarin Are there contraindications to newer agents? Severe renal and/or liver disease, valve disease Do NOT use if history of noncompliance Remember, the benefit of anticoagulation will most often outweigh the risk 47
48 References 1. Abbate R, Prisco D, Rostagno, et al. Age related changes in the hemostatic system. Intl J Clin Lab Res 1993;23(1): Go AS, Hylek EM, Borowsky LH, et al. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Ann Intern Med1999;131: Sinnaeve PR, Brueckmann M, Clemens A, et al. Stroke prevention in elderly patients with atrial fibrillation: challenges for anticoagulation. J Int Med 2011;271: Jones M, McEwan P, Morgan CL, et al. Evaluation of the pattern of treatment, level of anticoagulation control, and outcome of treatment with warfarin in patients with non valvular atrial fibrillation: a record linkage study in a large British population. Heart 2005; Wann LS, Curtis AB, January CT, et al ACCF/AHA/HRS Focused Update on the Management of Patients With Atrial Fibrillation. Circulation 2011;123: Pisters R, Lane DA, Nieuwlaat R, et al. A Novel user friendly score (HAS BLED) to assess 1 year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138(5): Fuster V, Ryden LE, Cannom DS, et al ACCF/AHA/HRS Focused Updates Incorporated Into the ACC/AHA/ESC 2006 Guidelines for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011;123:e Hylek EM, Evans Molina C, Shea C, et al. Major Hemorrhage and Tolerability of Warfarin in the First Year of Therapy Among Elderly Patients With Atrial Fibrillation. Circulation 2007;115: Hylek EM, Singer DE, et al. Risk factors for intracranial hemorrhage in outpatients taking warfarin. Ann Intern Med1994;120: Man Son Hing M, at al. Choosing antithrombotic therapy for elderly patients with atrial fibrillation who are at risk for falls. Arch Intern Med 1999; 159: Khreizat HS, Whittaker P, Curtis KD, et al. The Effect of Cognitive Impairment in the Elderly on the Initial and Long Term Stability of Warfarin Therapy. Drugs Aging 2012; 29(4): Protheroe J, Fahey, Montgomery AA, et al. The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis. BMJ 2000;320: Devereaux PJ, Anderson DR, Gardner MJ, et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ 2001;323: Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361: Granger CB, Alexander JH, McMurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365: Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365: Man Son Hing M, Laupacis A. Balancing the risks of stroke and upper gastrointestinal tract bleeding in older patients with atrial fibrillation. Arch Intern Med 2002;162:
STROKE PREVENTION IN ATRIAL FIBRILLATION
 STROKE PREVENTION IN ATRIAL FIBRILLATION OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention of ischemic stroke and arterial thromboembolism in patients
STROKE PREVENTION IN ATRIAL FIBRILLATION OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention of ischemic stroke and arterial thromboembolism in patients
Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013
 Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013 Family physician with Rivergrove Medical Clinic Practice in the north end since 1985 Medical Director of the Wellness
Kevin Saunders MD CCFP Rivergrove Medical Clinic Wellness Institute @ SOGH April 17 2013 Family physician with Rivergrove Medical Clinic Practice in the north end since 1985 Medical Director of the Wellness
STROKE PREVENTION IN ATRIAL FIBRILLATION. TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: ABBREVIATIONS: BACKGROUND:
 STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation. Joy Wahawisan, Pharm.D., BCPS April 25, 2012
 New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
New Anticoagulation Options for Stroke Prevention in Atrial Fibrillation Joy Wahawisan, Pharm.D., BCPS April 25, 2012 Stroke in Atrial Fibrillation % Stroke 1991;22:983. Age Range (years) CHADS 2 Risk
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation
 Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for Stroke Prevention in Atrial Fibrillation Drew Baldwin, MD Virginia Mason Seattle, Washington NCVH May 29,
Antiplatelet and Antithrombotic Therapy. Dr Curry Grant Stroke Prevention Clinic Quinte Health Care
 Antiplatelet and Antithrombotic Therapy Dr Curry Grant Stroke Prevention Clinic Quinte Health Care Disclosure of Potential for Conflict of Interest Dr. F.C. Grant Atrial Fibrillation FINANCIAL DISCLOSURE:
Antiplatelet and Antithrombotic Therapy Dr Curry Grant Stroke Prevention Clinic Quinte Health Care Disclosure of Potential for Conflict of Interest Dr. F.C. Grant Atrial Fibrillation FINANCIAL DISCLOSURE:
Anticoagulants in Atrial Fibrillation
 Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
The author has no disclosures
 Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
FDA Approved Oral Anticoagulants
 FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
FDA Approved Oral Anticoagulants Generic (Trade Name) Warfarin (Coumadin, Jantoven ) 1 FDA approved indication Prophylaxis and treatment of venous thromboembolism (VTE) Prophylaxis and treatment of thromboembolic
1/7/2012. Objectives. Epidemiology of Atrial Fibrillation(AF) Stroke in AF. Stroke Risk Stratification in AF
 Stroke in AF. Stroke Risk Stratification in AF") Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
Objectives Atrial Fibrillation and Prevention of Thrombotic Complications: Therapeutic Update Andrea C. Flores Pharm.D Pharmacy Resident at the Miami VA Healthcare System Review the epidemiology, pathophysiology
3/25/14. To Clot or Not What s New In Anticoagulation? Clotting Cascade. Anticoagulant drug targets. Anita Ralstin, MS CNS CNP. Heparin.
 To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
The Role of the Newer Anticoagulants
 The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
The Role of the Newer Anticoagulants WARFARIN = Coumadin DAGIBATRAN = Pradaxa RIVAROXABAN = Xarelto APIXABAN = Eliquis INDICATION DABIGATRAN (Pradaxa) RIVAROXABAN (Xarelto) APIXABAN (Eliquis) Stroke prevention
Anticoagulation Therapy Update
 Anticoagulation Therapy Update JUDY R. WALLING, FNP-BC ARRHYTHMIA MANAGEMENT MUSC CARDIOLOGY Outline Who do we anticoagulate? Review classes of Anticoagulants Review examples of Anticoagulants Review CHADS2
Anticoagulation Therapy Update JUDY R. WALLING, FNP-BC ARRHYTHMIA MANAGEMENT MUSC CARDIOLOGY Outline Who do we anticoagulate? Review classes of Anticoagulants Review examples of Anticoagulants Review CHADS2
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below
 RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below") Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
New Anticoagulants: Are we Ready to Replace Warfarin? Carole Goodine, RPh Horizon Health Network Stroke Conference 2011
 New Anticoagulants: Are we Ready to Replace Warfarin? Carole Goodine, RPh Horizon Health Network Stroke Conference 2011 Warfarin Decreases stroke risk by 60-70% Superior to ASA and ASA plus clopidogrel
New Anticoagulants: Are we Ready to Replace Warfarin? Carole Goodine, RPh Horizon Health Network Stroke Conference 2011 Warfarin Decreases stroke risk by 60-70% Superior to ASA and ASA plus clopidogrel
Oral Anticoagulation in Older Persons The Next Generation
 Oral Anticoagulation in Older Persons The Next Generation Luis Viana B.Sc. Phm., Pharm D (candidate), M.Ed., ACPR, CGP Clinical Consultant Pharmacist, Medical Pharmacies Group Limited Adjunct Clinical
Oral Anticoagulation in Older Persons The Next Generation Luis Viana B.Sc. Phm., Pharm D (candidate), M.Ed., ACPR, CGP Clinical Consultant Pharmacist, Medical Pharmacies Group Limited Adjunct Clinical
How To Treat Aneuricaagulation
 Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
Speaker Introduction Jessica Wilhoite, PharmD, BCACP Doctor of Pharmacy: Purdue University Postgraduate Residency Training: PGY1 Pharmacy Practice St. Vincent Hospital PGY2 Ambulatory Care St. Vincent
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations
 for stroke prevention in atrial fibrillation Special situations") Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial
 Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial Camillo Autore Università di Roma Sapienza II Facoltà di Medicina e Chirurgia
Long term anticoagulant therapy in patients with atrial fibrillation at high risk of stroke: a new scenario after RE-LY trial Camillo Autore Università di Roma Sapienza II Facoltà di Medicina e Chirurgia
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
Anticoagulation: How Do I Pick From All the Choices? Jeffrey H. Neuhauser, DO, FACC BHHI Primary Care Symposium February 28, 2014
 Anticoagulation: How Do I Pick From All the Choices? Jeffrey H. Neuhauser, DO, FACC BHHI Primary Care Symposium February 28, 2014 Atrial Fibrillation 2 Atrial Fibrillation The most common arrhythmia encountered
Anticoagulation: How Do I Pick From All the Choices? Jeffrey H. Neuhauser, DO, FACC BHHI Primary Care Symposium February 28, 2014 Atrial Fibrillation 2 Atrial Fibrillation The most common arrhythmia encountered
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical
 Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
Devang M. Desai, MD, FACC, FSCAI Chief of Interventional Cardiology Director of Cardiac Catheterization Lab St. Mary s Hospital and Regional Medical Center A.Fib affects 2.2 million Americans. The lifetime
GRASP-AF Coming to a PCT near you.
 GRASP-AF Coming to a PCT near you. ADAS Anticoagulation dosing advisory service Blackpool Teaching Hospitals Trust Sean O'Brien; Anticoagulation Specialist BMS Grasp-AF and the implications on our Anticoagulation
GRASP-AF Coming to a PCT near you. ADAS Anticoagulation dosing advisory service Blackpool Teaching Hospitals Trust Sean O'Brien; Anticoagulation Specialist BMS Grasp-AF and the implications on our Anticoagulation
Objectives. Epidemiology. Pathophysiology 4/1/2013
 Objectives The New CHEST Guidelines, The Bleeding War Continues Ginger Warren, PharmD., MCSR gwarren@valleyhealthlink.com PGY1 Pharmacy Resident Valley Health System/Bernard J Dunn School of Pharmacy,
Objectives The New CHEST Guidelines, The Bleeding War Continues Ginger Warren, PharmD., MCSR gwarren@valleyhealthlink.com PGY1 Pharmacy Resident Valley Health System/Bernard J Dunn School of Pharmacy,
4/9/2015. Risk Stratify Our Patients. Stroke Risk in AF: CHADS2 Scoring system JAMA 2001; 285: 2864-71
 Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
Anticoagulation in the 21 st Century Adam Karpman, D.O. Saint Francis Medical Center/Oklahoma State University Medical Center Disclosures: None Atrial Fibrillation Most common arrhythmia in clinical practice.
AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation
 AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation A Statement for Healthcare Professionals from the American Heart Association/American Stroke
AHA/ASA Scientific Statement Oral Antithrombotic Agents for the Prevention of Stroke in Atrial Fibrillation A Statement for Healthcare Professionals from the American Heart Association/American Stroke
Failure or significant adverse effects to all of the alternatives: Eliquis and Xarelto
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Service Ansell, J. Hematology Copyright 2010 American Society of Hematology.
Novel OAC s : How should we use them?
 Novel OAC s : How should we use them? Jean C. Grégoire MD, FRCP(c), FACC, FACP Associate Professor, Université de Montréal, IntervenJonal Cardiologist, InsJtut de cardiologie de Montréal Disclosures Speaker
Novel OAC s : How should we use them? Jean C. Grégoire MD, FRCP(c), FACC, FACP Associate Professor, Université de Montréal, IntervenJonal Cardiologist, InsJtut de cardiologie de Montréal Disclosures Speaker
Optimizing Anticoagulation Selection for Your Patient. C. Andrew Brian MD, FACC NCVH 2015
 Optimizing Anticoagulation Selection for Your Patient C. Andrew Brian MD, FACC NCVH 2015 Who Needs to Be Anticoagulated and What is the Patient s Risk? 1. Atrial Fibrillation ( nonvalvular ) 2. What regimen
Optimizing Anticoagulation Selection for Your Patient C. Andrew Brian MD, FACC NCVH 2015 Who Needs to Be Anticoagulated and What is the Patient s Risk? 1. Atrial Fibrillation ( nonvalvular ) 2. What regimen
Goals 6/6/2014. Stroke Prevention in Atrial Fibrillation: New Oral Anti-Coagulants No More INRs. Ashkan Babaie, MD
 Stroke Prevention in Atrial Fibrillation: New Oral Anti-Coagulants No More INRs Ashkan Babaie, MD Arrhythmia Service Providence Heart Clinic June 8 th, 2014 Goals Discuss the data behind approval of NOACs
Stroke Prevention in Atrial Fibrillation: New Oral Anti-Coagulants No More INRs Ashkan Babaie, MD Arrhythmia Service Providence Heart Clinic June 8 th, 2014 Goals Discuss the data behind approval of NOACs
Non- Valvular Atrial Fibrillation and Stroke Prevention: Which OAC Do I Choose. Warfarin vs the NOACs
 Non- Valvular Atrial Fibrillation and Stroke Prevention: Which OAC Do I Choose Warfarin vs the NOACs Dr. Lori McIntosh D.O. Board Certified Neurologist Objectives Be able to list the current options of
Non- Valvular Atrial Fibrillation and Stroke Prevention: Which OAC Do I Choose Warfarin vs the NOACs Dr. Lori McIntosh D.O. Board Certified Neurologist Objectives Be able to list the current options of
RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) 3.75
 P=0.051 (superiority) 3.75") ALL-CAUSE MORTALITY RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) Rate per year (%) 5.0 4.0 3.0 2.0 1.0 0 3.64 D150 mg BID 3.75 D110 mg BID RR 0.91 (95% CI: 0.80 1.03) P=0.13 (superiority) 4.13 Warfarin
ALL-CAUSE MORTALITY RR 0.88 (95% CI: 0.77 1.00) P=0.051 (superiority) Rate per year (%) 5.0 4.0 3.0 2.0 1.0 0 3.64 D150 mg BID 3.75 D110 mg BID RR 0.91 (95% CI: 0.80 1.03) P=0.13 (superiority) 4.13 Warfarin
Appendix C Factors to consider when choosing between anticoagulant options and FAQs
 Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Management of Antithrombotics with Procedures. Jordan Weinstein, MD
 Management of Antithrombotics with Procedures Jordan Weinstein, MD Presenter Disclosure Information Cardiology Update 2013 I have no relevant financial interest and/or arrangement with industry. Novel
Management of Antithrombotics with Procedures Jordan Weinstein, MD Presenter Disclosure Information Cardiology Update 2013 I have no relevant financial interest and/or arrangement with industry. Novel
TSOAC Initiation Checklist
 Task Establish appropriate dose based on anticoagulant selected, indication and patient factors such as renal function. Evaluate for medication interactions that may necessitate TSOAC dose adjustment.
Task Establish appropriate dose based on anticoagulant selected, indication and patient factors such as renal function. Evaluate for medication interactions that may necessitate TSOAC dose adjustment.
PHARMACOLOGICAL Stroke Prevention in Atrial Fibrillation STROKE RISK ASSESSMENT SCORES Vs. BLEEDING RISK ASSESSMENT SCORES.
 PHARMACOLOGICAL Stroke Prevention in Atrial Fibrillation STROKE RISK ASSESSMENT SCORES Vs. BLEEDING RISK ASSESSMENT SCORES. Hossam Bahy, MD (1992 2012), 19 tools have been identified 11 stroke scores 1
PHARMACOLOGICAL Stroke Prevention in Atrial Fibrillation STROKE RISK ASSESSMENT SCORES Vs. BLEEDING RISK ASSESSMENT SCORES. Hossam Bahy, MD (1992 2012), 19 tools have been identified 11 stroke scores 1
Stroke Risk Scores. CHA 2 DS 2 -VASc. CHA 2 DS 2 -VASc Scoring Table 2
 Bleeding/Clotting Risk Evaluation Tools for Atrial Fibrillation Patients Before prescribing anticoagulants, providers should weigh the risk of thrombosis against the risk of bleeding. The tools below can
Bleeding/Clotting Risk Evaluation Tools for Atrial Fibrillation Patients Before prescribing anticoagulants, providers should weigh the risk of thrombosis against the risk of bleeding. The tools below can
Traditional anticoagulants
 TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
TEGH Family Practice Clinic Day April 4, 03 Use of Anticoagulants in 03: What s New (and What Isn t) Bill Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University
Dorset Cardiac Centre
 P a g e 1 Dorset Cardiac Centre Patients with Atrial Fibrillation/Flutter undergoing DC Cardioversion or Ablation procedures- Guidelines for Novel Oral Anti-coagulants (NOACS) licensed for this use February
P a g e 1 Dorset Cardiac Centre Patients with Atrial Fibrillation/Flutter undergoing DC Cardioversion or Ablation procedures- Guidelines for Novel Oral Anti-coagulants (NOACS) licensed for this use February
New Anticoagulants and GI bleeding
 New Anticoagulants and GI bleeding DR DANNY MYERS MD FRCP(C) CLINICAL ASSISTANT PROFESSOR OF MEDICINE, UBC Conflicts of Interest None I am unbiased in the use of NOAC s vs Warfarin based on risk benefit
New Anticoagulants and GI bleeding DR DANNY MYERS MD FRCP(C) CLINICAL ASSISTANT PROFESSOR OF MEDICINE, UBC Conflicts of Interest None I am unbiased in the use of NOAC s vs Warfarin based on risk benefit
Cardiology Update 2014
 Cardiology Update 2014 Update on the Novel Oral Anticoagulants (NOACS) Raymond Kawasaki, MD AMG Cardiology December 6, 2014 Disclosures I have no disclosures relevant to this presentation Contents I. The
Cardiology Update 2014 Update on the Novel Oral Anticoagulants (NOACS) Raymond Kawasaki, MD AMG Cardiology December 6, 2014 Disclosures I have no disclosures relevant to this presentation Contents I. The
Objectives. New and Emerging Anticoagulants. Objectives (continued) 2/18/2014. Development of New Anticoagulants
 2/18/2014. Development of New Anticoagulants") Objectives New and Emerging Anticoagulants Adraine Lyles, PharmD, BCPS Clinical Pharmacy Specialist VCU Medical Center Describe the pharmacology of the novel oral anticoagulants Discuss the clinical evidence
Objectives New and Emerging Anticoagulants Adraine Lyles, PharmD, BCPS Clinical Pharmacy Specialist VCU Medical Center Describe the pharmacology of the novel oral anticoagulants Discuss the clinical evidence
New Oral Anticoagulants: Thinning out the competition
 New Oral Anticoagulants: Thinning out the competition Ashlee D. Gerfen, Pharm.D. University of Arizona Medical Center PGY2 Critical Care Pharmacy Resident DISCLOSURE I have no financial interest, arrangement,
New Oral Anticoagulants: Thinning out the competition Ashlee D. Gerfen, Pharm.D. University of Arizona Medical Center PGY2 Critical Care Pharmacy Resident DISCLOSURE I have no financial interest, arrangement,
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Anticoagulation in Atrial Fibrillation
 Anticoagulation in Atrial Fibrillation Parag P. Patel, MD FACC Disclosures Eliquis Speakers Bureau 1 Clinical Scenario Ms. L is a 76F admitted to the stroke service with a dense right sided hemiparesis
Anticoagulation in Atrial Fibrillation Parag P. Patel, MD FACC Disclosures Eliquis Speakers Bureau 1 Clinical Scenario Ms. L is a 76F admitted to the stroke service with a dense right sided hemiparesis
Speaker Disclosure. Outline. Pharmacist Objectives. Patient Case. Outline 9/4/2014
 Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS mpitlick@stlcop.edu Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Speaker Disclosure Matthew K. Pitlick, Pharm.D., BCPS St. Louis College of Pharmacy/VA St. Louis HCS mpitlick@stlcop.edu Matthew K. Pitlick, Pharm.D., BCPS declares no conflicts of interest, real or apparent,
Antiplatelet and Antithrombotics From clinical trials to guidelines
 Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008:
 have been licensed in Ireland since 2008:") Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
Key Points to consider when prescribing NOACs Introduction Three new/novel oral anticoagulants (NOAC) have been licensed in Ireland since 2008: Dabigatran Etexilate (Pradaxa ) 75mg, 110mg, 150mg. Rivaroxaban
NOAC S For Stroke Prevention in. Atrial Fibrillation. Peter Cohn M.D FACC Associate Physician in Chief Cardiovascular Care Center Southcoast Health
 NOAC S For Stroke Prevention in Atrial Fibrillation Peter Cohn M.D FACC Associate Physician in Chief Cardiovascular Care Center Southcoast Health New Oral Anti Coagulant Formal Definition: Atrial Fibrillation
NOAC S For Stroke Prevention in Atrial Fibrillation Peter Cohn M.D FACC Associate Physician in Chief Cardiovascular Care Center Southcoast Health New Oral Anti Coagulant Formal Definition: Atrial Fibrillation
Dabigatran (Pradaxa) Guidelines
 Guidelines") Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
FOR THE PREVENTION OF ATRIAL FIBRILLATION RELATED STROKE
 www.bpac.org.nz keyword: warfarinaspirin FOR THE PREVENTION OF ATRIAL FIBRILLATION RELATED STROKE Key Concepts In atrial fibrillation (AF) warfarin is more effective than aspirin for stroke prevention.
www.bpac.org.nz keyword: warfarinaspirin FOR THE PREVENTION OF ATRIAL FIBRILLATION RELATED STROKE Key Concepts In atrial fibrillation (AF) warfarin is more effective than aspirin for stroke prevention.
} Most common arrhythmia. } Incidence increases with age. } Anticoagulants approved for AF
 Deniz Yavas, PharmD PGY-2 Ambulatory Care Pharmacy Resident Detroit Veterans Affairs Medical Center } Most common arrhythmia 0.4-1% of Americans (2.2 mil people) 1,2 } Incidence increases with age 6% (65
Deniz Yavas, PharmD PGY-2 Ambulatory Care Pharmacy Resident Detroit Veterans Affairs Medical Center } Most common arrhythmia 0.4-1% of Americans (2.2 mil people) 1,2 } Incidence increases with age 6% (65
Xarelto (Rivaroxaban)
") Xarelto (Rivaroxaban) Hightly selective, reversible, direct oral FXa inhibitor Maxium concentratiion after 2 to 4 hrs High bioavailability(66%),increase with food ( suggest with food) 1/3 from renal excretion,
Xarelto (Rivaroxaban) Hightly selective, reversible, direct oral FXa inhibitor Maxium concentratiion after 2 to 4 hrs High bioavailability(66%),increase with food ( suggest with food) 1/3 from renal excretion,
The New Kids on the Block: Oral Anticoagulants
 The New Kids on the Block: Oral Anticoagulants Lauren E. Odum, PharmD, BCPS Clinical Assistant Professor UMKC School of Pharmacy at MU April 11, 2014 Objectives Be able to Understand the major trials leading
The New Kids on the Block: Oral Anticoagulants Lauren E. Odum, PharmD, BCPS Clinical Assistant Professor UMKC School of Pharmacy at MU April 11, 2014 Objectives Be able to Understand the major trials leading
How To Compare Warfarin To Dabigatran
 Page 1 WOMEN AT RISK Anticoagulation Issues In Atrial Fibrillation WOMEN AT RISK Anticoagulation Issues In Atrial Fibrillation J E A N N A P P I, P H A R M. D., F C C P, B C P S Accreditation: Pharmacists:
Page 1 WOMEN AT RISK Anticoagulation Issues In Atrial Fibrillation WOMEN AT RISK Anticoagulation Issues In Atrial Fibrillation J E A N N A P P I, P H A R M. D., F C C P, B C P S Accreditation: Pharmacists:
DOACs. What s in a name? or TSOACs. Blood Clot. Darra Cover, Pharm D. Clot Formation DOACs work here. Direct Oral AntiCoagulant
 DOACs NOACs or TSOACs Generic Name DOACs Brand Name Mechanism of Action Direct Xa Inhibitor Direct Thrombin Inhibitor Dabigatran Pradaxa X Rivaroxaban Xarelto X Darra Cover, Pharm D Apixaban Eliquis X
DOACs NOACs or TSOACs Generic Name DOACs Brand Name Mechanism of Action Direct Xa Inhibitor Direct Thrombin Inhibitor Dabigatran Pradaxa X Rivaroxaban Xarelto X Darra Cover, Pharm D Apixaban Eliquis X
Anticoagulation For Atrial Fibrillation
 Anticoagulation For Atrial Fibrillation New Agents In A New Era Arjun V Gururaj, MD Arrhythmia and Electrophysiology Nevada Heart and Vascular Center Disclosures Biotronik Speaker Clinical investigator
Anticoagulation For Atrial Fibrillation New Agents In A New Era Arjun V Gururaj, MD Arrhythmia and Electrophysiology Nevada Heart and Vascular Center Disclosures Biotronik Speaker Clinical investigator
CCPN SPAF Tool. www.ccpn.ca STROKE PREVENTION IN ATRIAL FIBRILLATION (SPAF): POCKET REFERENCE
: POCKET REFERENCE") SEPTEMBER 2012 CCPN SPAF Tool STROKE PREVENTION IN ATRIAL FIBRILLATION (SPAF): POCKET REFERENCE Approximately 20% of all strokes are attributable to Atrial Fibrillation (AF). 1 Of these, 20% will result
SEPTEMBER 2012 CCPN SPAF Tool STROKE PREVENTION IN ATRIAL FIBRILLATION (SPAF): POCKET REFERENCE Approximately 20% of all strokes are attributable to Atrial Fibrillation (AF). 1 Of these, 20% will result
Novel Anticoagulation Agents DISCLOSURES. Objectives ATRIAL FIBRILLATION TRIALS. NOAC Comparison 6/12/2015
 Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Novel Anticoagulation Agents DISCLOSURES James W. Haynes, MD Department of Family Medicine Univ of TN Health Science Center (Chattanooga) Objectives Understand mechanism of action behind the NOAC agents
Rivaroxaban (Xarelto ) by
 by") Essentia Health Med Moment Short Video Tune-Up A brief overview of a new medication, or important new medication information Rivaroxaban (Xarelto ) by Richard Mullvain RPH BCPS (AQC) Current - August 2011
Essentia Health Med Moment Short Video Tune-Up A brief overview of a new medication, or important new medication information Rivaroxaban (Xarelto ) by Richard Mullvain RPH BCPS (AQC) Current - August 2011
DABIGATRAN ETEXILATE TARGET Vitamin K epoxide reductase WARFARIN RIVAROXABAN APIXABAN
 TARGET SPECIFIC ORAL ANTICOAGULANTS (TSOACs) This document is intended as a guideline only and should not replace sound clinical judgment Please refer to UNMH formulary in Lexicomp for approved use(s)
TARGET SPECIFIC ORAL ANTICOAGULANTS (TSOACs) This document is intended as a guideline only and should not replace sound clinical judgment Please refer to UNMH formulary in Lexicomp for approved use(s)
Bridging the Gap: How to Transition from the NOACs to Warfarin
 Bridging the Gap: How to Transition from the NOACs to April 24 th 2015 UAN: 0048-0000-15-034-L01-P Amanda Styer, Pharm.D. Marion General Hospital, OhioHealth Objectives: 1. Review labeling regarding transition
Bridging the Gap: How to Transition from the NOACs to April 24 th 2015 UAN: 0048-0000-15-034-L01-P Amanda Styer, Pharm.D. Marion General Hospital, OhioHealth Objectives: 1. Review labeling regarding transition
New Oral Anticoagulants. How safe are they outside the trials?
 New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation
 Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation Goal Statement Pharmacists and technicians will gain knowledge in the use of target specific oral anticoagulants
Out with the Old and in with the New? Target Specific Anticoagulants for Atrial Fibrillation Goal Statement Pharmacists and technicians will gain knowledge in the use of target specific oral anticoagulants
Update on Antiplatelets and anticoagulants. Outlines. Antiplatelets and Anticoagulants 1/23/2013. Timir Paul, MD, PhD
 Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
NIL. Dr Chuks Ajaero FMCP FRACP Cardiologist QEH, NALHN, SA Heart & Central Districts. Approach. Approach. 06-Nov-14
 Stroke Prevention in Atrial Fibrillation: Commencing Non- Oral Anticoagulants in GP setting Dr Chuks Ajaero FMCP FRACP Cardiologist QEH, NALHN, SA Heart & Central Districts Disclosures NIL Classification
Stroke Prevention in Atrial Fibrillation: Commencing Non- Oral Anticoagulants in GP setting Dr Chuks Ajaero FMCP FRACP Cardiologist QEH, NALHN, SA Heart & Central Districts Disclosures NIL Classification
Anticoagulation at the end of life. Rhona Maclean Rhona.maclean@sth.nhs.uk
 Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM
 NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
NEWER ANTICOAGULANTS: FOCUS ON STROKE PREVENTION IN ATRIAL FIBRILLATION AND DEEP VEIN THROMBOSIS/PULMONARY EMBOLISM Carol Lee, Pharm.D., Jessica C. Song, M.A., Pharm.D. INTRODUCTION For many years, warfarin
22-Oct-14. Oral Anticoagulation Which Drug for Which Patient in the era of New Oral Anti-coagulants. Atrial Fibrillation. AF as an embolic risk factor
 Oral Anticoagulation Which Drug for Which Patient in the era of New Oral Anti-coagulants Dr Scott McKenzie BSc MBBS FRACP FCSANZ Cardiologist, Vascular Physician, Telehealth Specialist, Advanced Heart
Oral Anticoagulation Which Drug for Which Patient in the era of New Oral Anti-coagulants Dr Scott McKenzie BSc MBBS FRACP FCSANZ Cardiologist, Vascular Physician, Telehealth Specialist, Advanced Heart
AF, Stroke Risk and New Anticoagulants
 Carmarthen Cardiac Update Course AF, Stroke Risk and New Anticoagulants Dr Hamsaraj Shetty, B.Sc, FRCP (London & Edinburgh) Consultant Physician & Honorary Senior Lecturer University Hospital of Wales,Cardiff
Carmarthen Cardiac Update Course AF, Stroke Risk and New Anticoagulants Dr Hamsaraj Shetty, B.Sc, FRCP (London & Edinburgh) Consultant Physician & Honorary Senior Lecturer University Hospital of Wales,Cardiff
ΠΟΙΟ ΑΝΤΙΠΗΚΤΙΚΟ ΓΙΑ ΤΟΝ ΑΣΘΕΝΗ ΜΟΥ? ΚΛΙΝΙΚΑ ΠΑΡΑΔΕΙΓΜΑΤΑ. Σωκράτης Παστρωμάς Καρδιολόγος Νοσοκομείο Ερρίκος Ντυνάν
 ΠΟΙΟ ΑΝΤΙΠΗΚΤΙΚΟ ΓΙΑ ΤΟΝ ΑΣΘΕΝΗ ΜΟΥ? ΚΛΙΝΙΚΑ ΠΑΡΑΔΕΙΓΜΑΤΑ Σωκράτης Παστρωμάς Καρδιολόγος Νοσοκομείο Ερρίκος Ντυνάν The AF epidemic Mayo Clinic data (assuming a continued increase in the AF incidence) Mayo
ΠΟΙΟ ΑΝΤΙΠΗΚΤΙΚΟ ΓΙΑ ΤΟΝ ΑΣΘΕΝΗ ΜΟΥ? ΚΛΙΝΙΚΑ ΠΑΡΑΔΕΙΓΜΑΤΑ Σωκράτης Παστρωμάς Καρδιολόγος Νοσοκομείο Ερρίκος Ντυνάν The AF epidemic Mayo Clinic data (assuming a continued increase in the AF incidence) Mayo
None. Dual Antiplatelet Therapy Plus Systemic Anticoagulation: Bleeding Risk and Management. 76 year old male LINGO 1/5/2015
 Financial Disclosure Information Dual Antiplatelet Therapy Plus Systemic Anticoagulation: Bleeding Risk and Management Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Dual Antiplatelet
Financial Disclosure Information Dual Antiplatelet Therapy Plus Systemic Anticoagulation: Bleeding Risk and Management Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Dual Antiplatelet
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
The speakers have attested that their presentation will be free of all commercial bias toward a specific company and its products.
 Update on New Anticoagulants (Apixaban, Dabigatran and Rivaroxaban) Patient Safety Daniel B. DiCola, MD and Paul Ament,, Pharm.D Excela Heath, Latrobe, PA Disclosures: Paul Ament discloses that he receives
Update on New Anticoagulants (Apixaban, Dabigatran and Rivaroxaban) Patient Safety Daniel B. DiCola, MD and Paul Ament,, Pharm.D Excela Heath, Latrobe, PA Disclosures: Paul Ament discloses that he receives
VOLUME No: 21 04 written by Sara Wilds & Kathryn Buchanan. Date of issue: June 2012 (updated November 2012 following NICE TA 256)
") Prescribing Points A NEWSLETTER FOR ALL HEALTH CARE PROFESSIONALS IN OXFORDSHIRE, WRITTEN BY THE MEDICINES MANAGEMENT TEAM, OXFORDSHIRE PCT, JUBILEE HOUSE, OXFORD BUSINESS PARK SOUTH, OXFORD, OX4 2LH.
Prescribing Points A NEWSLETTER FOR ALL HEALTH CARE PROFESSIONALS IN OXFORDSHIRE, WRITTEN BY THE MEDICINES MANAGEMENT TEAM, OXFORDSHIRE PCT, JUBILEE HOUSE, OXFORD BUSINESS PARK SOUTH, OXFORD, OX4 2LH.
Efficacy in Hip Arthroplasty. Efficacy in Knee Arthroplasty. Adverse Effects. Drug Interactions
 Objectives Just for the RECORD: Rivaroxaban joins the US Anticoagulation Arsenal Anne P. Spencer, PharmD, FCCP, BCPS (AQ Cardiology) Cardiovascular Care Pharmacy Specialist Roper Saint Francis Healthcare
Objectives Just for the RECORD: Rivaroxaban joins the US Anticoagulation Arsenal Anne P. Spencer, PharmD, FCCP, BCPS (AQ Cardiology) Cardiovascular Care Pharmacy Specialist Roper Saint Francis Healthcare
48 th Annual Meeting. Non-VKA Oral Anticoagulants: Prevention & Treatment of Bleeding. Terminology. Disclosure. Public Health Impact.
 48 th Annual Meeting Terminology Non-VKA Oral Anticoagulants: Prevention & Treatment of Bleeding Stacy A. Voils, PharmD, MS, BCPS Navigating the Oceans of Opportunity Target-specific oral anticoagulants
48 th Annual Meeting Terminology Non-VKA Oral Anticoagulants: Prevention & Treatment of Bleeding Stacy A. Voils, PharmD, MS, BCPS Navigating the Oceans of Opportunity Target-specific oral anticoagulants
NOACS AND AF PEARLS AND PITFALLS DR LAURA YOUNG HAEMATOLOGIST
 NOACS AND AF PEARLS AND PITFALLS DR LAURA YOUNG HAEMATOLOGIST NGAIRE IS 70 YEARS OLD AND IN AF. SHE HAS NO MURMURS, NORMAL BLOOD PRESSURE, EGFR OF 65ML/MIN AND NO SIGNIFICANT PAST MEDICAL HISTORY. REGARDING
NOACS AND AF PEARLS AND PITFALLS DR LAURA YOUNG HAEMATOLOGIST NGAIRE IS 70 YEARS OLD AND IN AF. SHE HAS NO MURMURS, NORMAL BLOOD PRESSURE, EGFR OF 65ML/MIN AND NO SIGNIFICANT PAST MEDICAL HISTORY. REGARDING
Financial Disclosures
 Financial Disclosures Consulting: AstraZeneca, Bayer, Boehringer Ingleheim, Bristol-Myers Squibb, Daiichi Sankyo, Eli Lilly, Glaxo Smith Kline, Johnson & Johnson, Merck, Novartis, Ortho/McNeill, Pfizer,
Financial Disclosures Consulting: AstraZeneca, Bayer, Boehringer Ingleheim, Bristol-Myers Squibb, Daiichi Sankyo, Eli Lilly, Glaxo Smith Kline, Johnson & Johnson, Merck, Novartis, Ortho/McNeill, Pfizer,
Atrial Fibrillation: Stroke and Thromboprophylaxis. Derek Waller
 Atrial Fibrillation: Stroke and Thromboprophylaxis Derek Waller Atrial Fibrillation in the Elderly: Risk of Stroke Framingham study AGE 50-59 60-69 70-79 80-89 Prevalence of AF % Attributable Risk of AF
Atrial Fibrillation: Stroke and Thromboprophylaxis Derek Waller Atrial Fibrillation in the Elderly: Risk of Stroke Framingham study AGE 50-59 60-69 70-79 80-89 Prevalence of AF % Attributable Risk of AF
Management of atrial fibrillation. Satchana Pumprueg, MD Sirin Apiyasawat, MD Thoranis Chantrarat, MD
 Management of atrial fibrillation Satchana Pumprueg, MD Sirin Apiyasawat, MD Thoranis Chantrarat, MD Antithrombotic therapy in atrial fibrillation Satchana Pumprueg, MD AF has serious consequences Independent
Management of atrial fibrillation Satchana Pumprueg, MD Sirin Apiyasawat, MD Thoranis Chantrarat, MD Antithrombotic therapy in atrial fibrillation Satchana Pumprueg, MD AF has serious consequences Independent
Disclosure/Conflict of Interest
 NEW ORAL ANTICOAGULANTS: WHAT EVERY PHARMACIST SHOULD KNOW LORI B. HORNSBY, PHARMD, BCPS ASSOCIATE CLINICAL PROFESSOR AUHSOP CLINICAL PHARMACIST MIDTOWN MEDICAL CENTER OUTPATIENT CLINIC COLUMBUS, GEORGIA
NEW ORAL ANTICOAGULANTS: WHAT EVERY PHARMACIST SHOULD KNOW LORI B. HORNSBY, PHARMD, BCPS ASSOCIATE CLINICAL PROFESSOR AUHSOP CLINICAL PHARMACIST MIDTOWN MEDICAL CENTER OUTPATIENT CLINIC COLUMBUS, GEORGIA
Committee Approval Date: September 12, 2014 Next Review Date: September 2015
 Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
Medication Policy Manual Policy No: dru361 Topic: Pradaxa, dabigatran Date of Origin: September 12, 2014 Committee Approval Date: September 12, 2014 Next Review Date: September 2015 Effective Date: November
How To Compare The New Oral Anticoagulants
 Disclosures The New Oral Anticoagulants: Are they better than Warfarin? Alan P. Agins, Ph.D. does not have any actual or potential conflicts of interest in relation to this CE activity. Alan Agins, Ph.D.
Disclosures The New Oral Anticoagulants: Are they better than Warfarin? Alan P. Agins, Ph.D. does not have any actual or potential conflicts of interest in relation to this CE activity. Alan Agins, Ph.D.
COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS. TARGET AUDIENCE: All Canadian health care professionals.
 COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS AND PHYSICIANS TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVES: To provide a comparison of the new
COMPARISON OF NEW ORAL ANTICOAGULANTS AND FREQUENTLY- ASKED QUESTIONS FROM PATIENTS AND PHYSICIANS TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVES: To provide a comparison of the new
Comparative Anticoagulation
 Comparative Anticoagulation Laurajo Ryan, PharmD, MSc, BCPS, CDE Clinical Associate Professor The University of Texas at Austin College of Pharmacy The University of Texas Health Science Center Pharmacotherapy
Comparative Anticoagulation Laurajo Ryan, PharmD, MSc, BCPS, CDE Clinical Associate Professor The University of Texas at Austin College of Pharmacy The University of Texas Health Science Center Pharmacotherapy
New Anticoagulants- Dabigatran/Rivaroxaban
 New Anticoagulants- Dabigatran/Rivaroxaban JOHN NOVIASKY, PHARMD, BCPS, FNYSCHP CGH AT UPSTATE UNIVERSITY HOSPITAL SYRACUSE NY Objectives Describe the risks and benefits of dabigatran therapy Describe
New Anticoagulants- Dabigatran/Rivaroxaban JOHN NOVIASKY, PHARMD, BCPS, FNYSCHP CGH AT UPSTATE UNIVERSITY HOSPITAL SYRACUSE NY Objectives Describe the risks and benefits of dabigatran therapy Describe
NHS FORTH VALLEY Rivaroxaban for Stroke Prevention in Atrial Fibrillation
 NHS FORTH VALLEY Rivaroxaban for Stroke Prevention in Atrial Fibrillation Date of First Issue 06/06/2012 Approved 06/06/2012 Current Issue Date 29/10/2014 Review Date 29/10/2016 Version 1.4 EQIA Yes 01/06/2012
NHS FORTH VALLEY Rivaroxaban for Stroke Prevention in Atrial Fibrillation Date of First Issue 06/06/2012 Approved 06/06/2012 Current Issue Date 29/10/2014 Review Date 29/10/2016 Version 1.4 EQIA Yes 01/06/2012
I NUOVI ANTICOAGULANTI ORALI
 AGGIORNAMENTI in CARDIOLOGIA I NUOVI ANTICOAGULANTI ORALI F. BELLANDI U.O.CARDIOLOGIA OSPEDALE DI PRATO NOVEL ORAL ANTICOAGULANTS RISK SCORE STRATIFICATION TRULY LOW RISK PATIENTS CHA 2 DS 2 -VASc vs
AGGIORNAMENTI in CARDIOLOGIA I NUOVI ANTICOAGULANTI ORALI F. BELLANDI U.O.CARDIOLOGIA OSPEDALE DI PRATO NOVEL ORAL ANTICOAGULANTS RISK SCORE STRATIFICATION TRULY LOW RISK PATIENTS CHA 2 DS 2 -VASc vs
9/8/2014. None. Identify the under-recognized risk of cardioembolic stroke in untreated and undertreated. morbidity, mortality and cost burdens
 Optimizing Anticoagulation Therapy for Older Adults with Atrial Fibrillation: The New Oral Agents" None Disclosures Brad Hein, PharmD Associate Professor of Pharmacy The University of Cincinnati Winkle
Optimizing Anticoagulation Therapy for Older Adults with Atrial Fibrillation: The New Oral Agents" None Disclosures Brad Hein, PharmD Associate Professor of Pharmacy The University of Cincinnati Winkle
Introduction. Methods. Study population
 New Technologies, Diagnostic Tools and Drugs Schattauer 2012 1 Net clinical benefit of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus no treatment in a real world atrial fibrillation
New Technologies, Diagnostic Tools and Drugs Schattauer 2012 1 Net clinical benefit of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus no treatment in a real world atrial fibrillation
Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis )
: Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis )") Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis ) The contents of this CPG are to be used as a guide. Healthcare professionals
Guideline for the Prescribing of Novel Oral Anticoagulants (NOACs): Dabigatran (Pradaxa ), Rivaroxaban (Xarelto ), Apixaban (Eliquis ) The contents of this CPG are to be used as a guide. Healthcare professionals
The New Oral Anticoagulants: When and When Not to Use Them Philip C. Comp, M.D., Ph.D. Professor of Medicine, University of Oklahoma Health Sciences
 The New Oral Anticoagulants: When and When Not to Use Them Philip C. Comp, M.D., Ph.D. Professor of Medicine, University of Oklahoma Health Sciences Center September 25, 2015 Question: With which of the
The New Oral Anticoagulants: When and When Not to Use Them Philip C. Comp, M.D., Ph.D. Professor of Medicine, University of Oklahoma Health Sciences Center September 25, 2015 Question: With which of the
Novel Oral Anticoagulants (NOACs) Prescriber Update 2013
 Prescriber Update 2013") Novel Oral Anticoagulants (NOACs) Prescriber Update 2013 Indications/Contraindications Indications Orthopedic VTE Prophylaxis VTE Treatment Stroke Prevention for non-valvular AF Contraindications 150 mg
Novel Oral Anticoagulants (NOACs) Prescriber Update 2013 Indications/Contraindications Indications Orthopedic VTE Prophylaxis VTE Treatment Stroke Prevention for non-valvular AF Contraindications 150 mg
Anticoagulation and Reversal
 Anticoagulation and Reversal John Howard, PharmD, BCPS Clinical Pharmacist Internal Medicine Affiliate Associate Clinical Professor South Carolina College of Pharmacy Disclosures I have no Financial, Industry,
Anticoagulation and Reversal John Howard, PharmD, BCPS Clinical Pharmacist Internal Medicine Affiliate Associate Clinical Professor South Carolina College of Pharmacy Disclosures I have no Financial, Industry,
The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era. CCRN State of the Heart 2012 June 2, 2012
 The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era CCRN State of the Heart 2012 June 2, 2012 Disclosures I have I have been involved in trials of new anticoagulants and have received
The 50-year Quest to Replace Warfarin: Novel Anticoagulants Define a New Era CCRN State of the Heart 2012 June 2, 2012 Disclosures I have I have been involved in trials of new anticoagulants and have received
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. A. Prescriptions That Require Prior Authorization
 MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants
MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Anticoagulants A. Prescriptions That Require Prior Authorization Prescriptions for Anticoagulants
Oral Anticoagulants: What s New?
 Oral Anticoagulants: What s New? Sallie Young, Pharm.D., BCPS (AQ-Cardiology) Clinical Pharmacy Specialist, Cardiology Penn State Hershey Medical Center syoung1@hmc.psu.edu August 2012 Oral Anticoagulant
Oral Anticoagulants: What s New? Sallie Young, Pharm.D., BCPS (AQ-Cardiology) Clinical Pharmacy Specialist, Cardiology Penn State Hershey Medical Center syoung1@hmc.psu.edu August 2012 Oral Anticoagulant
Comparison between New Oral Anticoagulants and Warfarin
 Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several
Comparison between New Oral Anticoagulants and Warfarin Warfarin was the mainstay of oral anticoagulant therapy until the recent discovery of more precise targets for therapy. In recent years, several